echo-doppler de l’aorte abdominale et des - amcar.maamcar.ma/ressources/att/ateliers/2015/serge...
TRANSCRIPT

Echo-Doppler de l’Aorte Abdominale et des
Carotides
Serge Kownator
Centre cardiologique et vasculaire - Thionville
AMCAR Marrakech
Octobre 2015

About Femoral Artery
• SFA is mainly a transport vessel to the below-knee muscles and has very few branches
• Profunda is the most important artery in case of SFA occlusion
• Persistent sciatic artery is a very rare condition, where the superficial femoral artery is hypoplastic and localised to the thigh.

Cas

Natural history of femoral
lesions • Pressure is dropping for >50% stenosis
• The collateral circulation provides a parallel pathway via branches from the deep femoral.
• This reserve capacity is the main reason why patients who develop chronic occlusion of the SFA without affecting the deep femoral artery have either no symptoms or mild symptoms of intermittent claudication.
• As the origin of the deep femoral artery is also stenosed, the symptoms worsen.
• Critical limb ischaemia is rarely a consequence of isolated occlusion of the superficial femoral artery but does occur when the deep femoral artery is also affected
• Don’t forget upstream lesions +++
Epidemiology of femoral
stenosis
• Prevalence increases with age,
• Male predominance
• Prevalence varies between 0-5% and 6-
9%
• 72% of SFA lesions remain stable.
• 12% diameter reduction per year
J Vasc Surg 1997; 25:512-21.

Progression of femoral disease
(vs carotid disease) • 30 pts – High FRS (29.5)- standard
medical Rx
Bianda L et al. European Heart Journal (2012) 33, 230–237
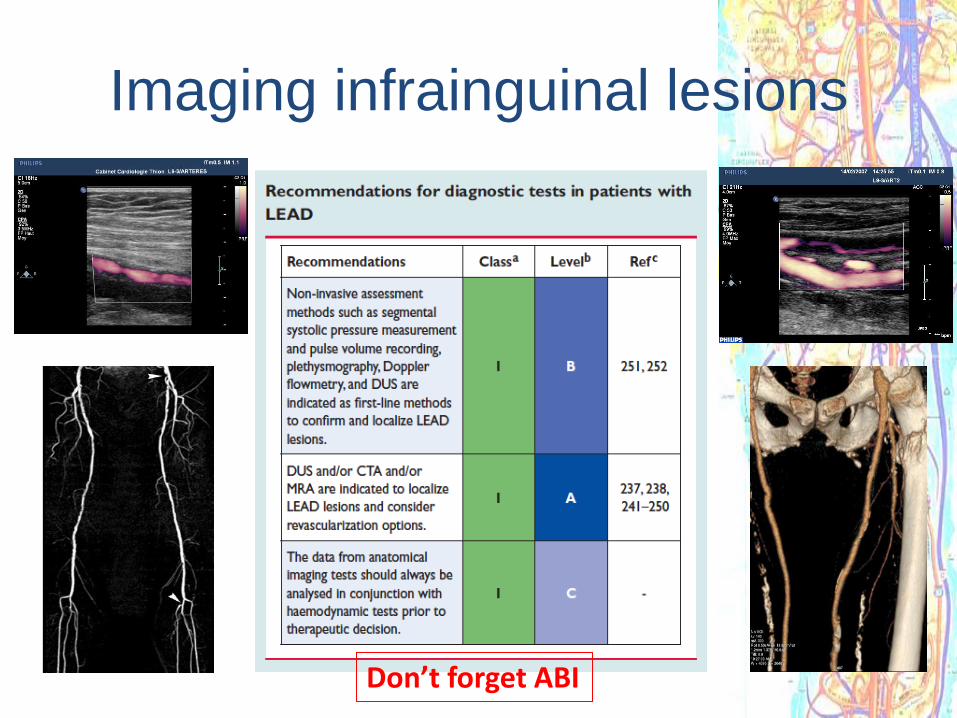
Imaging infrainguinal lesions
Don’t forget ABI

Prediction of SFA stenosis
progression • 19 patients with arteriography for severe SFA
occlusive disease in 20 legs 32 months following
initial arteriography performed when the SFA
under study caused minimal or no symptoms.
Walsh DB et al. J Vasc Surg 1997; 25:512-21

Factors of progression
• Complex lesions
• Inside the adductor canal
Walsh DB et al. J Vasc Surg 1997; 25:512-21

Probability of occlusion
• Probability of occlusion
depends on stenosis severity,
lesion morphology and
location in the adductor canal
Walsh DB et al. J Vasc Surg 1997; 25:512-21

Occlusion
• Can be outweighted by collateral developement

Factor of clinical worsening
• Deep femoral artery stenosis

Suivi des lésions sous inguinales
• La clinique est au premier plan
– CI – ischémie d’effort
– Ischémie critique – ischémie
chronique
• L’apparition ou l’aggravation des
symptômes sont les éléments
marquants de l’évolution

Therapeutic strategy for intervention in
femoral popliteal lesions
TASC II. J Vasc Surg 2007;45:S5–S67.

Quantification des sténoses • Doppler: ratio +++ sténoses étagées
• St > 50% : PSV > 200 cm/s - PSV ratio > 2 – 3
• St > 70% : PSV > 350 - PSV ratio > 3,5 – 4
Sacks et al. J Ultrasound Med 1992 ; 11 (3) : 95-103

Signes indirects
• Signes indirects – Amortissement et démodulation du flux en aval:
• temps de montée systolique (Acceleration Time)
– 110 ms : sténose < 50 % ;
– 150 ms : sténose comprise entre 50 et 79 % ;
– 180 ms : sténose entre 80 et 99 % ;
– 225 ms : occlusion
• Flux monophasique ± flux diastolique – Valeur ++ si > 40 cm/s
• Sensibilisation à l’effort
Schneider PA et al. J Vasc Surg 1998 ; 28 (1) : 28-34

Anévrismes de l’aorte
abdominale

Quelques chiffres
• En France
– Prévalence 3,7 à 5,9 % chez les sujets de plus de 65 ans
– 6 à 7000 opérés par an (chirurgie ou endovasculaire)
• Mortalité 8,4 % – 75 à 90 % si rupture
– 2 – 6 % pour les interventions réglées
– 0,4 à 6,5 % des causes de DC/an
– Parmi les AAA opérés, environ 8 % sont des AAA rompus.
– La part des traitements endovasculaires est > 50 %

Initial Diagnosis of AAA
• 38% patients AAAs initially detected by PE
• 23% AAAs were not palpable on preoperative PE,
even when the diagnosis was known.
• AAAs detected by PE had lower BMIs but there was
no difference in AAA size
• 43 % of AAAs detected on radiologic examination
had palpable AAAs that should have been detected
on PE.
• Obese patients had only 15% of AAAs detected by
PE, and only 33% were palpable.
Chervu A et al. Surgery 1995 Apr;117(4):454-7

AAA Quelle définition?
• Diamètre maximal > 30 mm (McGregor et al Scott Med J1975;20:133-7)
• Diamètre > à 1.5 x le diamètre de l’aorte sus rénale (Sterpetti et
al Surg Res 1987;43:211-9)
• 1.5 X le diamètre de l’aorte sous rénale normale (ou à défaut
1.5 X le diamètre établi grâce à un normogramme) (ISCVS/SVS J
Vasc Surg 1991;13:452-8)
Aorte sous rénale non anévrismale Anévrisme

Anévrismes de l’aorte
abdominale

Imaging Modalities

Echo-Doppler de l’aorte abdominale
Rappel d’écho-anatomie




Tronc coeliaque
Hépatique
Splénique
Coronaire stomachique




Renal artery disease
• Renal artery stenosis (RAS) is increasingly
related to atherosclerosis with advancing
age and prevalent hypertension, diabetes
mellitus, renal disease, LEAD, and CAD. Less
frequent causes are fibromuscular dysplasia
and arteritis.
• RAS may cause or deteriorate arterial
hypertension and/or renal failure.
• RAS is a marker of very high CV Risk

Clinical situations where the diagnosis of RAS should be considered

Diagnostic strategies for RAS
Recommendations Class Level
DUS is recommended as the first-line imaging test to establish the diagnosis of RAS.
I B
CTA (in patients with creatinine clearance >60 mL/min) is recommended to establish the diagnosis of RAS.
I B
MRA (in patients with creatinine clearance >30 mL/min) is recommended to establish the diagnosis of RAS.
I B
When the clinical index of suspicion is high and the results of non-invasive tests are inconclusive, DSA is recommended as a diagnostic test (prepared for intervention) to establish the diagnosis of RAS.
I C
Captopril renal scintigraphy, selective renal vein renin measurements, plasma renin activity, and the captopril test are not recommended as useful screening tests to establish the diagnosis of RAS.
III B
1 CTA = computed tomography angiography; DSA = digital subtraction angiography; DUS = duplex
ultrasonography; MRA = magnetic resonance angiography; RAS = renal artery stenosis.
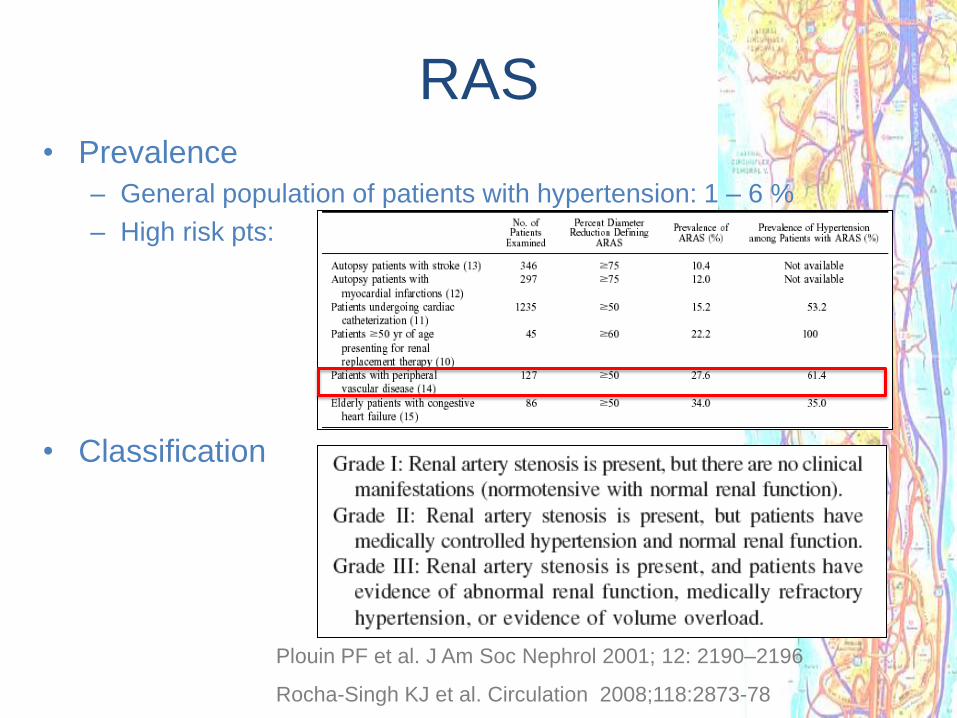
• Prevalence
– General population of patients with hypertension: 1 – 6 %
– High risk pts:
• Classification
Plouin PF et al. J Am Soc Nephrol 2001; 12: 2190–2196
Rocha-Singh KJ et al. Circulation 2008;118:2873-78
RAS

Renal arteries
Anatomy
• Anatomy
– Accessory (ies) renal artery (ies) in 25 %
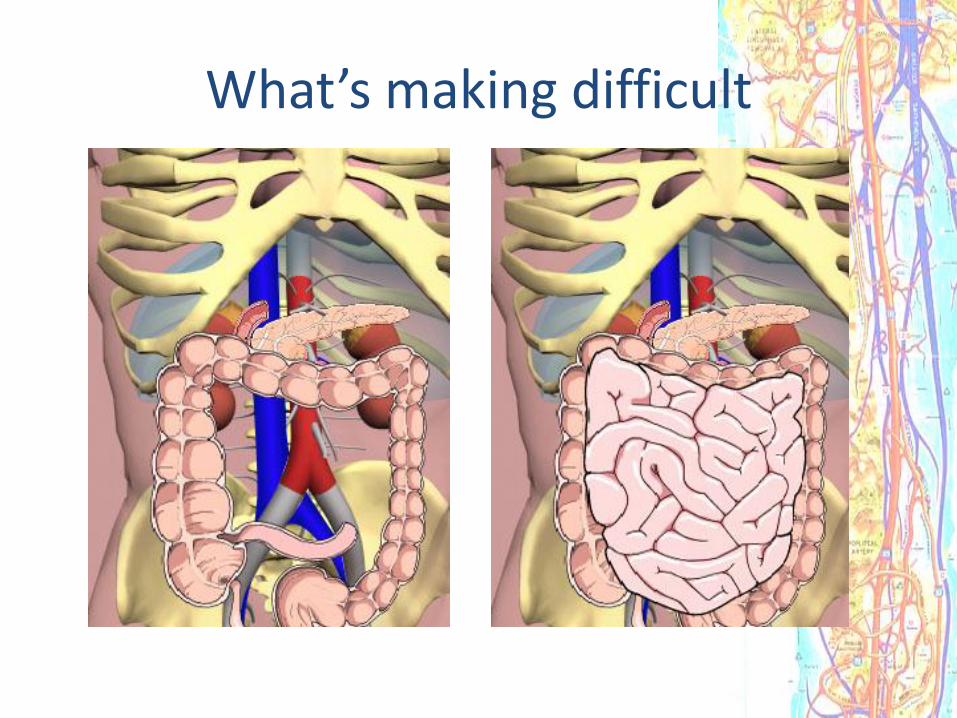
What’s making difficult

Imaging Renal arteries with DUS
3 steps to scan!
• Step 1:
– Supine position:
• Feasibility of 60 to 80 %
– Coronal (transverse) view:
• SMA arise from the anterior wall of
the aorta
• Make an angulation of the probe to
identify the origin of the right and left
renal arteries
• Look for aliasing with the adapted
PRF
– Sagital (longitudinal) view
• Record the Doppler folw in the aorta
at the level of the SMA – Renal-
aortic ratio

• Right RA at 10 h
• Left RA at 4 h

Imaging Renal arteries with DUS
3 steps to scan! • Record the Doppler flow with an angle ≤ 60 ° at the origin and
proximal portion of the renal arteries
• Renal artery velocities:
– PSV: 80 – 120 cm/s
– EDV: 20 – 40 cm/s
• Resistive Index : syst V – diastV = 0.5 - 0,7
syst V
• Intra renal velocities
– PSV et VTD
– Ascension time : N < 70 ms

Imaging Renal arteries with DUS
3 steps to scan! • Step 2: Left lateral decubitus:
• Coronal view =>Right renal artery from the aorta and right kidney short axis – Record the Doppler flow with a ≤ 60 ° angle all along the artery
• Turn to sagital ± oblique view => Right renal artery from aorta and right kidney long
axis – Record the intra renal Doppler flow and measure carefully the kidney’s height

Imaging Renal arteries with DUS
3 steps to scan!
• Step 2 bis
– Left lateral decubitus
• Trans hepatic approach - Sagital view
– Origin and proximal right and, most of the time, left renal artery
– Allows an optimal angle for Doppler flow recording

Imaging Renal arteries with DUS
3 steps to scan! • Step 3
– Right lateral decubitus:
• Sagital ± oblique view => Left renal artery from aorta and left kidney long axis • Record the intra renal Doppler flow and measure carefully the kidney’s height
• Coronal view =>Left renal artery from the aorta and right kidney short axis in
different plans – Record the Doppler flow with a ≤ 60 ° angle all along the artery

Left RA
left lateral approach

Pittfals
• One missing renal artery…
– Look to the pelvis !
– Renal artery issue from the iliac artery
• Accessory (ies) renal arteries
– Up to 25 %
– Low probability if the diameter is over 4 mm
– Scan in short axis from the the SMA to the bifurcation -
– Lateral sagital views

DUS & RAS
• > 60 % : PSV = 200 cm/s – RAR = 3.5
• Sens : .98 – Spec: .98 - PPV:.99 - NPV .97
Olin, J. W. et. al. Ann Intern Med 1995;122:833-838

RAS
DUS vs Angiography
(1) 34 >60 % stenosis
– Mean PSV: 272 cm/s – mean RAR : 3.7
(2) 219 cm/sec :
– sensitivity 89%, specificity 89%, accuracy 89%
(1) Soares et al J Ultrasound Med 2006; 25:293–298
(2) Kawarada O, Catheter Cardiovasc Interv. 2006 Aug;68(2):311-8

Reapraisal of the cut-off values
Drieghe B et al. European Heart Journal (2008) 29, 517–524

Indirect criteria • RI
• Intra renal flow analysis: « Tardus Parvus »
1 Baxter GM et al. Br J Radiol 1996 Sep;69(825):810-5
2 Ripoles T et al. Eur J Radiol 2001 Oct;40(1):54-63
AT > 120 ms high probability of > 70 % stenosis1
AT> 80 ms => > 75 % stenosis : sens 89%, spec 98 % 2
106 ms
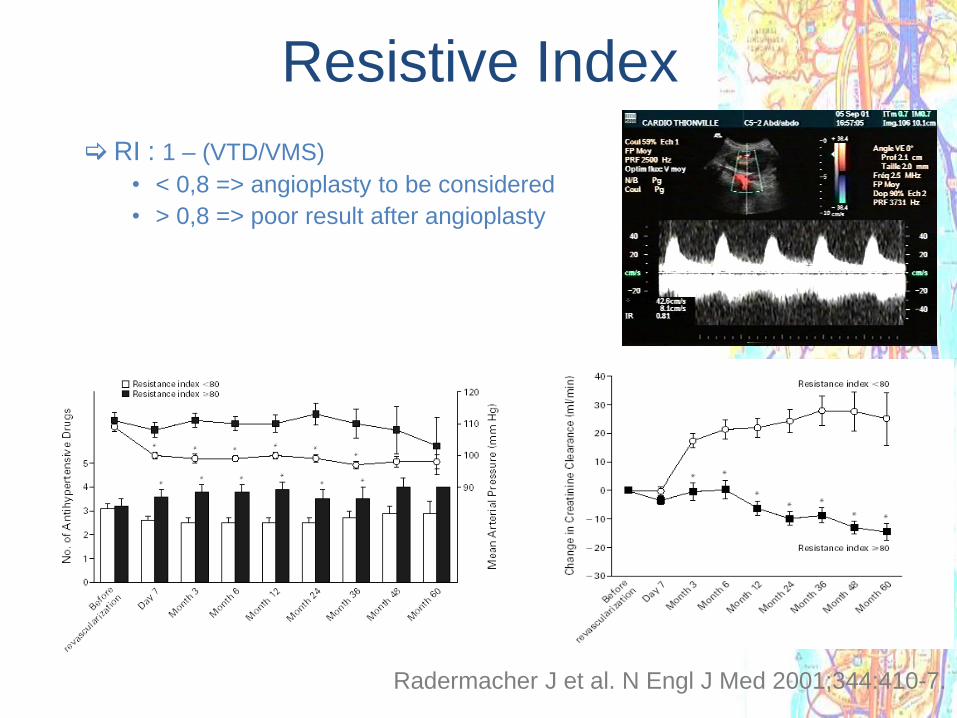
Resistive Index
RI : 1 – (VTD/VMS)
• < 0,8 => angioplasty to be considered
• > 0,8 => poor result after angioplasty
Radermacher J et al. N Engl J Med 2001;344:410-7.

RAS
• What are we applying for RAS > 60 % in
our lab.
– PSV > 250 cm/s
– RAR > 3.5
– Turbulences +++
– Intrarenal wave form
– Renal dimension and pattern
Case # 1
• Mrs Mul…65
• Retired MD
• Resistant hypertension
– .
• ABP: mean 24h 183/101 mmHg
• Biology N
– Clck: 55 ml/mn….

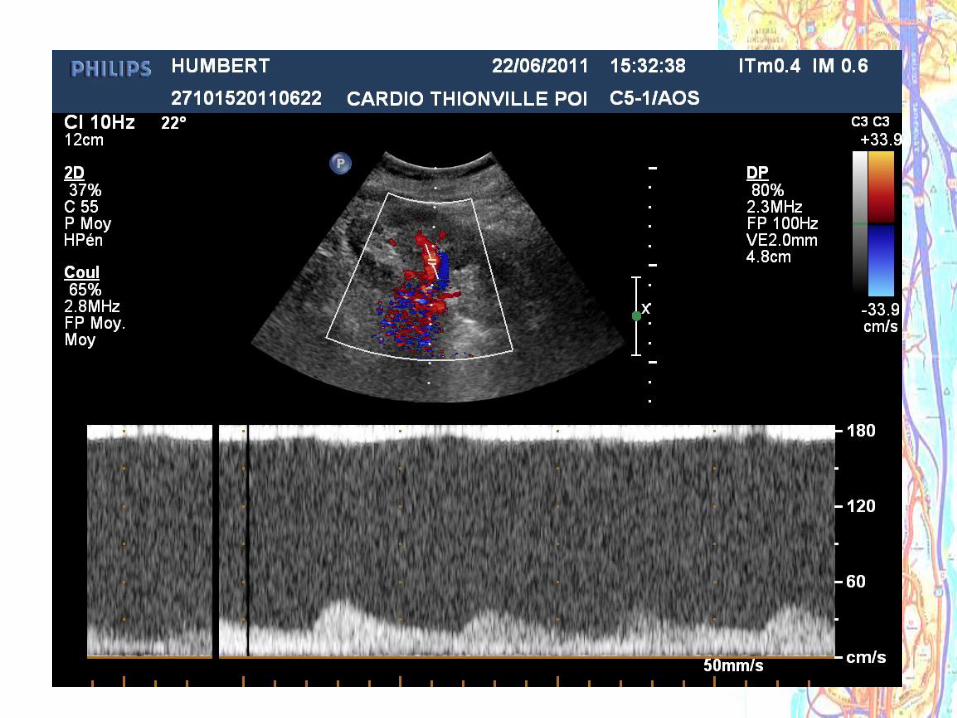
Case # 1

Case # 1
PSV 300 cm/s - RAR 4

Case # 1
Case # 1
• Normalization of blood pressure after
angioplasty
• 1 month later:
– ABPM :
• 24 h: 144/84 mmHg
• Day time: 151/89 mmHg
– Rx : ARB
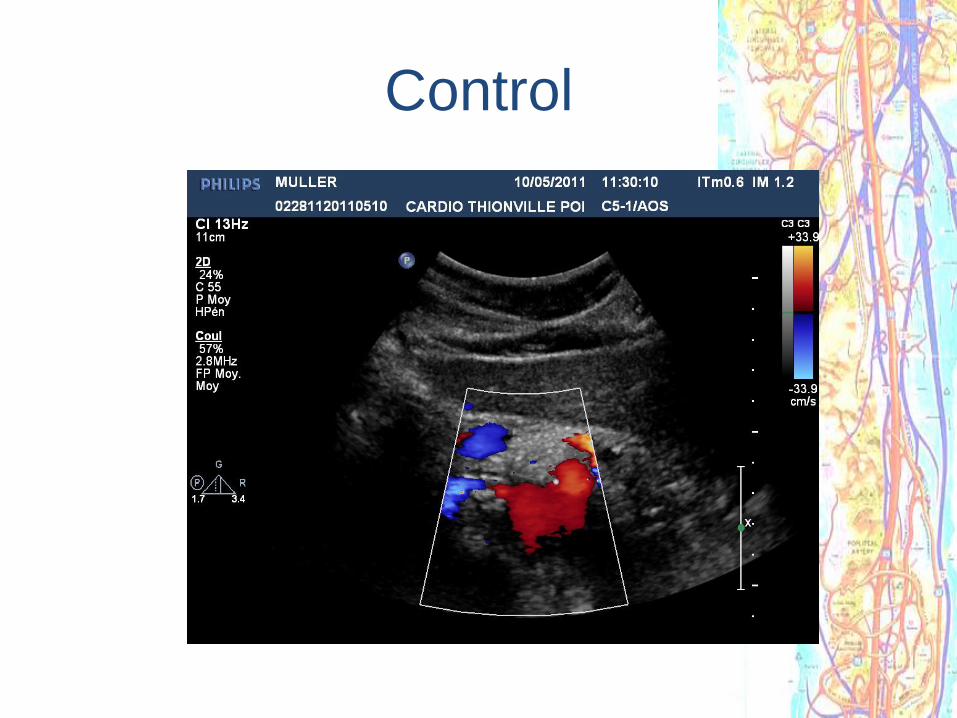
Control

Case # 2
• Mrs Mas. 45 yrs
– Hypertension

Case # 2 • Mrs HUM …70
• Left renal angioplasty in 2002
• Uncontroled hypertension since 6 months

Case # 2
PSV > 350 cm/ s – RAR 4.2 - turbulences

DSA
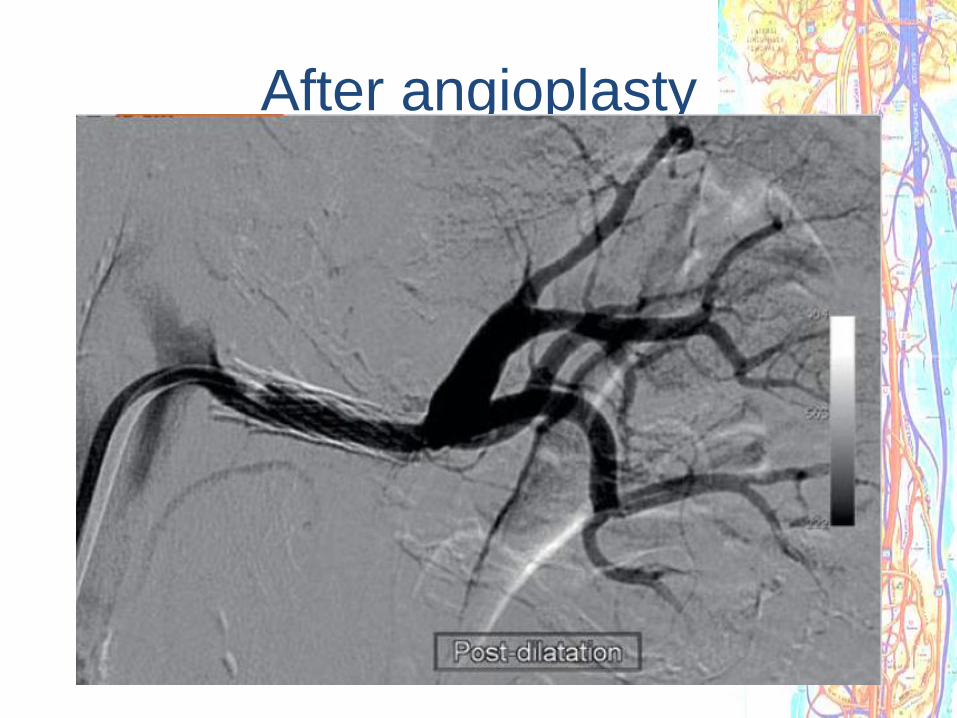
After angioplasty

Control
Case # 3
• Mrs Mas. 45 yrs
– Hypertension

Case # 3

Case # 4
• Mrs Sim. – 62 yrs
– Hypertension
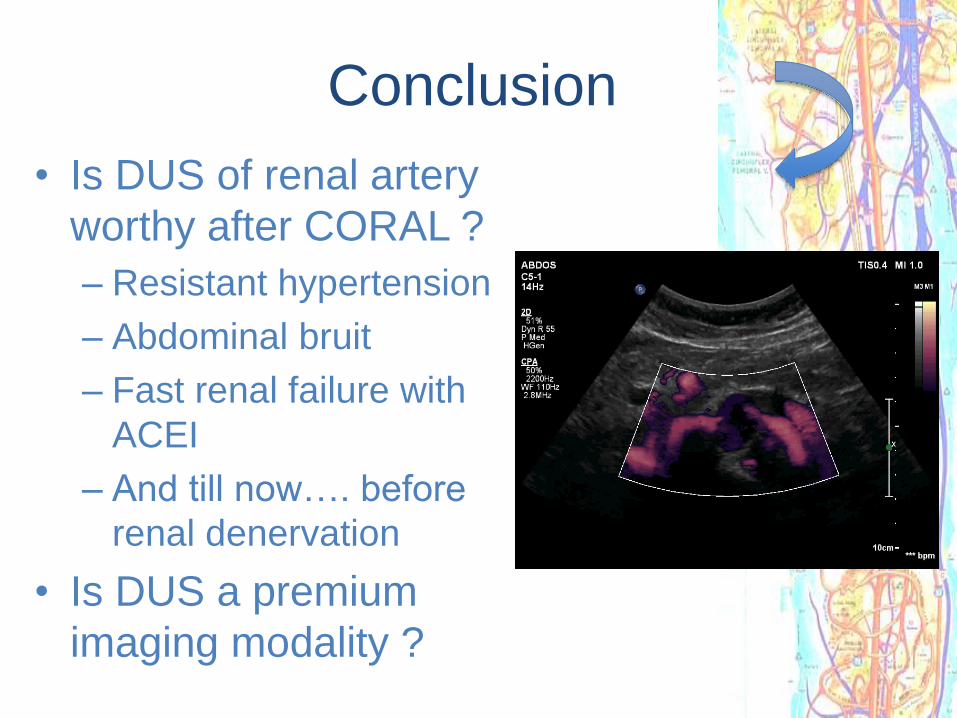
Conclusion
• Is DUS of renal artery
worthy after CORAL ?
– Resistant hypertension
– Abdominal bruit
– Fast renal failure with
ACEI
– And till now…. before
renal denervation
• Is DUS a premium
imaging modality ?

Sténoses carotidiennes

72
D
A
B C
Que mesure-t-on?
Méthodes angiographiques

73
Que mesure-t-on en Doppler ?
95 98 100 % of stenosis
PSV
Spencer MP et al. Stroke. 1979 ;3:326-330
Bernouilli’s Equation

DUS
Validation
• Extensive literature
• Overall sensitivity > 85 %
• Overall specificity > 90 %
75
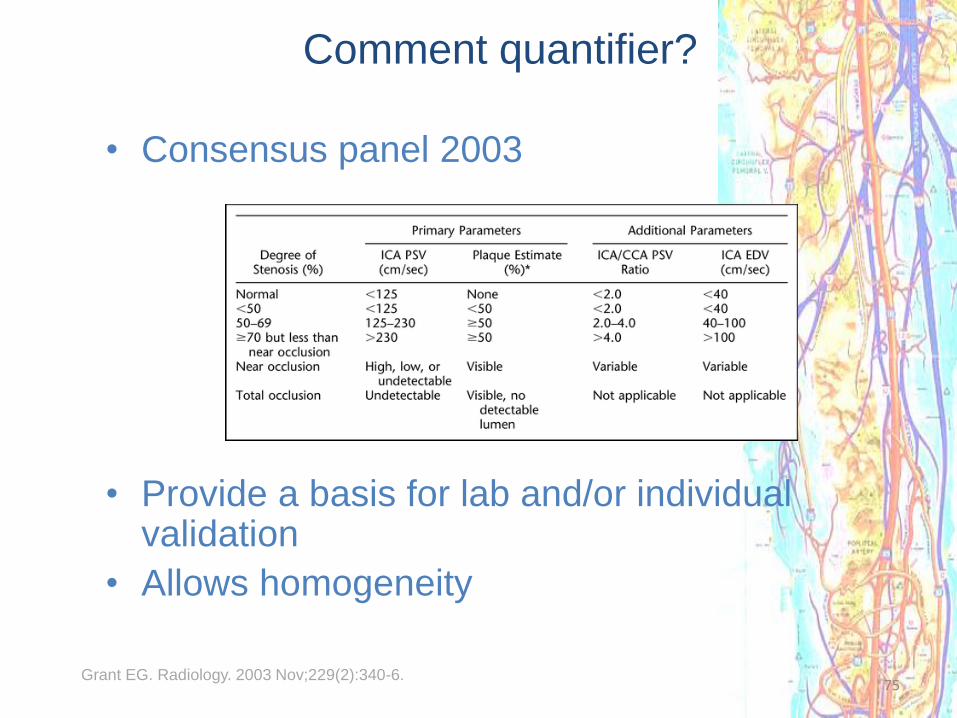
Comment quantifier?
• Consensus panel 2003
• Provide a basis for lab and/or individual validation
• Allows homogeneity
Grant EG. Radiology. 2003 Nov;229(2):340-6.
76
Critères 2008
• La comparaison n’est plus faite avec l’artériographie
mais avec l’échographie haute résolution et
l’angioscanner
• Le diamètre est mesuré au bulbe
– Echo et angio scanner ont une bonne corrélation : r = 0,9
– Bonne reproductibilité intra et inter observateur pour écho et CT
(0,8 – 0,9)
• Sténose > 50 % :
– PSV of ≥ 155 cm/s and ICA/CCA ratio of ≥ 2
• Sténose > 80 % :
– EDV ≥ 140 cm/s, PSV ≥ 370 cm/s, ICA/CCA ratio ≥ 6
J Vasc Surg. 2008 Jul;48(1):104 Shaalan WE et al. J Vasc Surg. 2008 Jul;48(1)

Recommendations UK 2009
Oates CP et al. Eur J Vasc Endovasc Surg. 2009 Mar;37(3):251-61.

DUS and Carotid stenosis
New consensus 2012 Neurosonology Research Group of the World Federation of Neurology
Von Reutern G et al. Stroke. 2012;43:916-921

Mr EL. 72 ans – Asymptomatique
Souffle carotidien gauche
