ecmo basics
DESCRIPTION
picuTRANSCRIPT
ECMO – An Overview
Nicole Shilkofski, M.D. MEd.
Pediatric Critical Care
Johns Hopkins School of Medicine
Perdana University School of Medicine
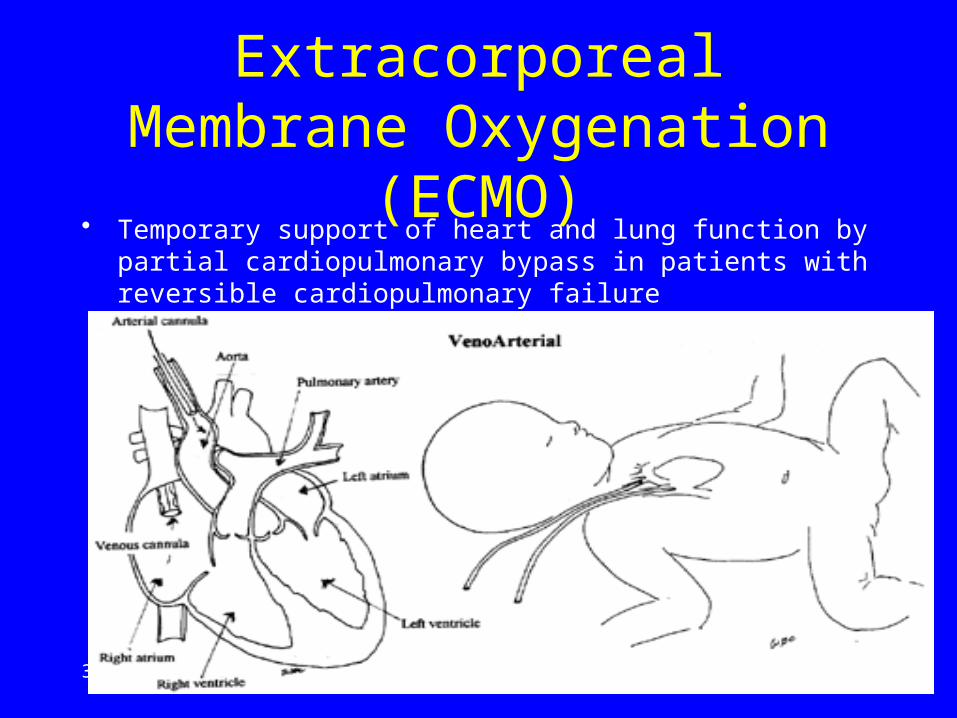
Extracorporeal Membrane Oxygenation (ECMO)
• Temporary support of heart and lung function by partial cardiopulmonary bypass in patients with reversible cardiopulmonary failure
April 17, 2023 2
History of ECMO
• 1930’s-1950’s: research into bypass for cardiac surgery; invention of roller-pump
• 1956: Invention of membrane lung
History
• 1957 – cardiopulmonary bypass used in OR• 1965-75 – ECMO tried in premature infants
(universally fatal)• 1972 – 1st human survivor – adult patient• 1975 – 1st term neonate survivor• 1981- Began use for PPHN• By 1986 used in 715 newborns at 18 centers
Basic mechanics• Blood is drained from the right atrium• Blood is warmed and oxygenated• Excess CO2 is removed
• Oxygenated blood is returned to the aorta– (or for VV ECMO into the right atrium)
• ECMO blood mixes with blood ejected from the left ventricle
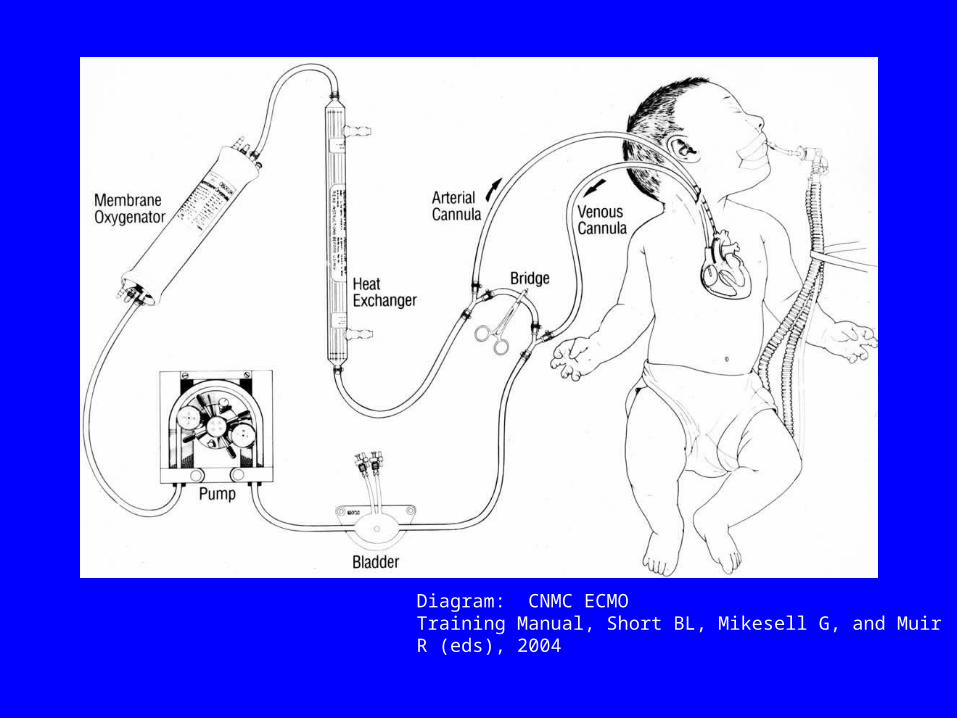
Diagram: CNMC ECMOTraining Manual, Short BL, Mikesell G, and Muir R (eds), 2004
VA ECMO• Used for respiratory failure• Used for cardiac failure• Used for both
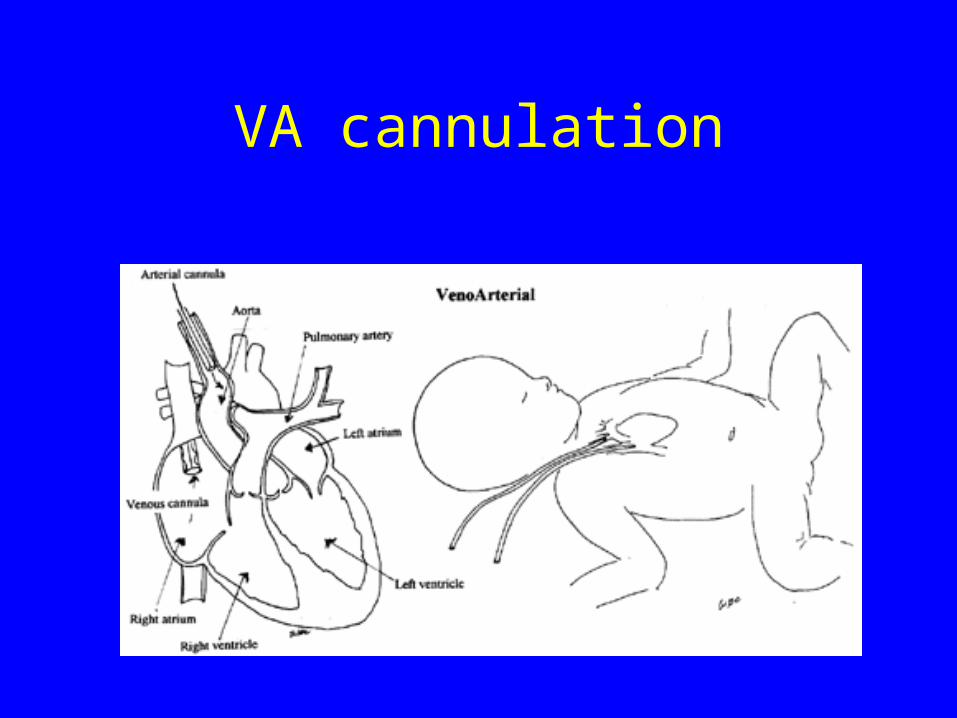
VA cannulation
VV ECMO
• Used primarily for respiratory failure• Indirectly improved cardiac function
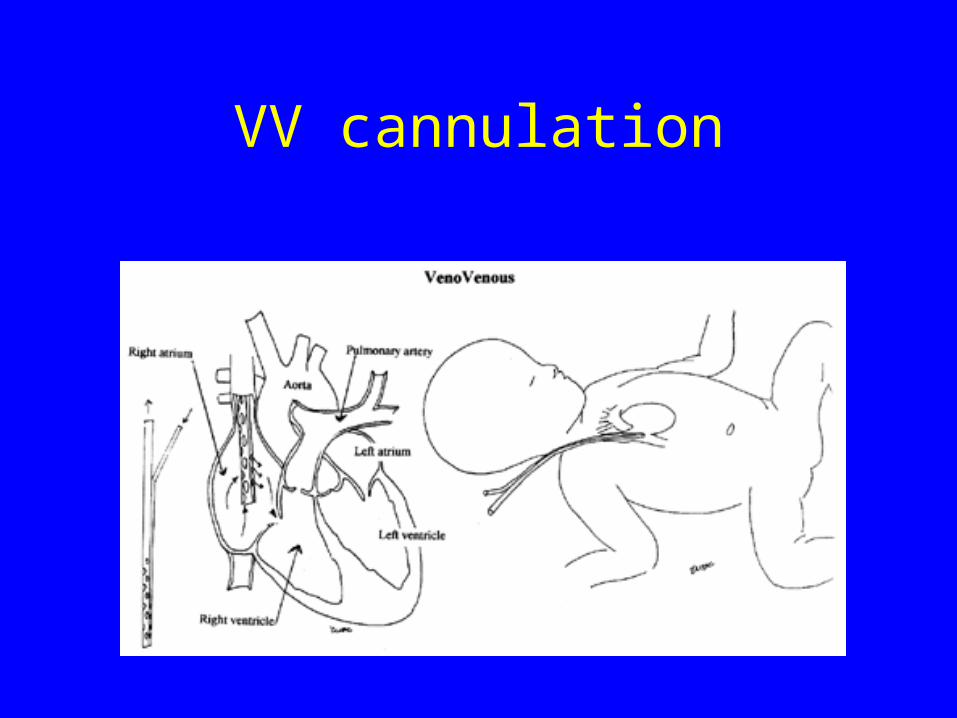
VV cannulation
Venous drainage
• Primarily a passive process• Depends on sufficient preload (volume)• Lack of venous return results in drop in
pressure in the bladder pump stops• Improved by height of patient• Improved by intravascular volume

Oxygen delivery
• Depends on dissolved O2 in plasma and O2 bound to hemoglobin
• CaO2 = (SaO2 x Hb x 1.36) + (PaO2 x 0.003)
• On ECMO depends on– Lungs– Membrane oxygenator
Ventilation
• CO2 removal– Via lungs
• May be quite limited• Depends on minute ventilation
– Membrane oxygenator• Very efficient• May be excessive- can put CO2 back into circuit if
needed
Rationale and Indications
• ECMO is purely supportive therapy• Ensures delivery of adequate oxygenated systemic
blood flow • ECMO does nothing for underlying primary
cardiac or respiratory pathology• Allows reduction in vent settings avoiding
volutrauma, barotrauma and oxygen toxicity-• ECMO indicated in acute severe reversible
cardiac or respiratory failure when risk of dying from primary disease despite optimal conventional treatment is high (50-100%)
Indications
• Hypoxic respiratory failure not manageable by other means– Neonates (Pulmonary hypertension -meconium
aspiration, asphyxia, HMD, sepsis, D hernia)– Older children (ARDS, pneumonia, status asthmaticus)
• Cardiac failure not manageable by other means– Post cardiac surgery, myocarditis, cardiomyopathy,
intractable arrythmias, drug overdose– Unlikely to be successful if not off in 5-7 days post
bypass– Should not be a bridge to cardiac transplant
• Septic shock not manageable by other means• Cardiac arrest ??????????????
Extracorporeal CPR (ECPR)
• Use of ECMO to support failed conventional CPR
• PALS guidelines recommend consideration when conditions leading to CPA are potentially reversible or amenable to heart transplant
• Recent series report survival 33% to 55%
Fiser and Morris, Ped Clin N Am, 2008
Respiratory ECMO Criteria
Oxygenation Index ≥ 40
OI = MAP x FiO2 x 100
PaO2
Common Conditions in Infants
• Hyaline membrane disease• Meconium Aspiration• Persistant Fetal Circulation• Congenital Diaphragmatic Hernia• Cardiac Anomalies
Common Conditions in Older Children and Adults
• Adult Respiratory Distress Syndrome (ARDS)
• Non-necrotizing pneumonias• Pulmonary contusion• Other reversible respiratory and cardiac
failure not responsive to other measures• Post cardiac surgery

Contraindications
• Severe Bleeding (Contraindication to anticoagulation)– Neonates-intraventricular hemorrhage > Grade 1 or 2– Major trauma, severe burns??, head injury with bleeds– Major coagulopathy
• Size limitation (neonates)– < 2 kg, < 34 weeks gestation
• Irreversible lung disease– Mechanical ventilation > 10 days– Other irreversible lung diseases such as necrotizing pneumonia
• Immunosuppression? (Cancer, transplantation, primary immunodeficiencies)
Survival
• Neonatal respiratory failure – 80%• Pediatric respiratory failure – 60%• Adult respiratory failure – 50%• Pediatric cardiac – 45%• Adult cardiac – 40%
Univ. of Michigan ECMO website
Neonatal Outcomes- vary with underlying disease
• Aspiration syndromes 90%• Persistent pulm HTN 80%• Infection 65%• Congenital D Hernia 50%• Congenital Heart Dz 40%• Cardiomyopathy 50%
Pre-cannulation preparation
• Neonates:– Head ultrasound- r/o bleed– Echocardiogram – evaluate for structural heart disease – Labs: Hb, platelets, coags and metabolic panel
• Lines, tubes, procedures BEFORE bypass– Foley catheter with balloon– Nice to have a central line and arterial line– Need peripheral access at minimum
Pre-cannulation preparation
• Prepare anesthetic– Fentanyl – Pancuronium/vecuronium
• Volume for resuscitation– 5% albumin, saline, blood
• Resuscitation meds – Epinephrine, CaCl, NaHCO3
• Heparin 100u/Kg • Ensure access to IV
Circuit Components



Cannulae :VA ECMO
• Neonates: Usual location for VA ECMO:– Venous – right internal jugular to RA– Arterial – right carotid to aortic arch
• Older child /adult– Venous – R internal jugular or femoral vein– Arterial – Femoral, right carotid– Monitor distal leg perfusion (Pulse oximeter,
dorsalis pedis arterial line)
Cannulae:VV ECMO
• VV ECMO:– Double lumen right atrial– RA femoral; femoral femoral or RA
• Available double lumen: 12 – 31 Fr• Usually placed by surgical cutdown in
neonates• Can be percutaneous in children / adults • CXR, sometimes echo, to check position


Venous Reservoir• Also known as “bladder”• On most ECMO circuits, venous return from the
patient is completely passive, by gravity• Bladder acts as venous resevoir to avoid negative
pressure generated by pump, which could cavitate air out of the blood
• Automatic feedback control to shut off pump when bladder collapses (“chirping”)

Roller Pump• Reliable use for many years
• Correct occlusion essential to calculate correct blood flow rate,( flow rate is CALCULATED and NOT MEASURED–revolutions/min, tubing diameter, occlusion) and avoid hemolysis
• Hand crank available for power failure


How much flow?
• Normal cardiac output – Neonates 150-200 cc/kg/min, infants 100 cc/kg/min, older children 75 cc/kg/min, adults 50 cc/kg/min
• Pump flow often expressed as % of presumed CO• VA ECMO – increase flow to improve
oxygenation or blood pressure• VV ECMO – inotropes to increase CO• Titrate flows using
– Pulse oximetry, ABGs– Mixed venous sats ≥ 65%, normal lactate, no acidosis– BP and perfusion


“Oxygenator”• More accurate name: membrane lung• Oxygenation:
– FiO2 to oxygenator
– Blood flow rate– Membrane surface area (can add second oxygenator)
• CO2 removal– Very efficient removal– Affected by gas “sweep” flow– Usually have to add some CO2 back to gas mixture

Heat exchanger
Required Monitoring
• Mixed venous sats• Pressure monitoring (prepump, postpump,
postmembrane)• Bubble detector• 3 sets of blood gases: post-oxygenator, patient,
mixed venous• End tidal CO2 – very low while on ECMO - low
pulmonary blood flows• Daily Head U/S in infants
CAVH
• Most patients on ECMO develop fluid overload, sometimes anuria, despite diuretics
• Non-pulsatile flow to kidneys may affect their function
• Possible to put hemofilter in line with ECMO pump for UF, CAVH or CAVHD
• Diuretics vs. Ultrafiltration
CAVH circuit in-line with pump

Heparinization
• Heparin bolus (100 units/kg) given just before bypass
• Activated clotting time at bedside hourly
• Usual ACT goal: 180-220
• Circuit usually needs to be changed every 7-10 days due to clots
Ventilator management on ECMO
“Rest” vent settings on VA ECMO:
– Goal: minimal settings to keep lungs recruited but also avoid volutrauma
– Typical: PEEP 10, PIP ~ 20, Rate ~ 10, FiO2 < 40%
Higher settings needed for VV ECMO

Venovenous ECMO• Advantages:
– Coronary arteries & lungs receive oxygenated blood– Spare carotid– Less risk of embolic stroke, air embolus– Pulsatile flow to organs
• Disadvantages:– No cardiac support- only use for pulmonary indications– Lower patient pO2
• Conversion rate from VV to VA: 5-15%
PROBLEMS and COMPLICATIONS
Complications of ECMO
• Hemorrhage (pulmonary, intracranial, GI, surgical site)
• CNS infarction• Seizures (metabolic or CNS cause)• Renal failure• Hyperbilirubinemia• Sepsis
Bleeding
• Topical agents• Lower ACT goal (180-200, or even 160-180)• Set platelet goal higher• FFP or fibrinogen/cryoprecipitate• Add Amicar • Surgical exploration• Don’t discontinue heparin, give more cryo and
platelets• Discontinue ECMO
Cardiac Stun
• Case: Neonate on VA ECMO x 24 hours, heart rate falls to 20. What do you do?
• 5-10% of patients on VA ECMO• More common in neonates• Worsened by hypertension• Don’t do CPR turn up pump flow
ELSO registry
• Founded 1989• 145 participating centers worldwide• Goal: include All ECMO patients• To date:
– 18,000 newborns– 4,000 pediatric patients– 1,000 adults
• www.elso.med.umich.edu












Team Training for ECMO Deployment – Role of
Simulation
April 17, 2023
Practicing on Plastic: In Situ Simulation



Summary Points
• ECMO is supportive therapy considered for cardiorespiratory failure with reversible cause
• Consider VA vs VV ECMO depending on underlying pathophysiology
• Circuit components are complex and require multidisciplinary team effort for effective routine and emergency management