neonatal ecmo : an update - florida association of ... neonatal ecmo-an update.pdf · neonatal ecmo...
TRANSCRIPT
Neonatal ECMO: An Update Amir M. Khan, MD Associate Professor of Pediatrics UT Houston Medical School Medical Director NICU, Neonatal Transport and Respiratory Care Children’s Memorial Hospital, Houston, TX
The speaker has signed a disclosure form and indicated he has no significant financial interest or relationship with the companies or the manufacturer(s) of any commercial product and/or service that will be discussed as part of this presentation.
Session Summary
During this session the presenter will review the historical trend and current uses of ECMO and changes in approach such as VV versus VA, changes in diagnoses, and change in management while on ECMO.
Session Objectives
Upon completion of this presentation, the participant will be able to:
give a brief history of ECMO;
understand common indications of ECMO;
understand typical management and outcome on ECMO;
evaluate the outcome and utilization data of ECMO;
recognize indications for ECMO.
References
Bartlett, R., Roloff, D., Cornell, R., Andrews, A., Dillon, P. & Zwischenberger, J. (1985). Extracorpeal circulation in neonatal respiratory failure: A prospective randomized study. Pediatrics, 76(4): 479-87.
O'Rourke, P., Crone, R., Vacanti, J., Ware, J., Lillehei, C., Parad, R. & Epstein, M. (1989). Extracorpeal membrane oxygenation and conventional medical therapy in neonates with persistent pulmonary hypertension of the newborn: A prospective randomized study. Pediatrics, 84(6): 957-63.
UK Collaborative ECMO Trial Group (1996). UK collaborative randomized trial of neonatal extracorpeal membrane oxygenation. Lancet, 348(9020): 75-82.
Session Outline
See presentation handout on the following pages.
A9 FANNP 24TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A9: NEONATAL ECMO: AN UPDATE Page 1 of 8

Neonatal ECMOAn Update
Amir M. Khan, MD
INTRODUCTION TO ECMO
What is ECMO?
• A constellation of biomedical devices(heart, lung, kidney, GI tract) compiled to provide life support when biologic organs are failing despite maximal “conventional” care
• A form of extrathoracic partial cardiopulmonary bypass designed as an oxygen delivery system to meet tissue needs
• A system based on a non-porous silicone oxygenator to allow prolonged life support
ECMOHistorical Background
1937 - Gibbon - 1st Oxygenator 1956 - Clowes - Membrane Oxygenator 1972 - 1st Adult Survivor 1974 - 1st Neonatal Survivor 1979 - NIH Trial 1980’s (Early) - Bartlett, Others 1980’s (Late) - Boston/Michigan Trials
Explosion of ECMO Centers 1996 - Lancet/UK Trial
FANNP 24TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A9: NEONATAL ECMO: AN UPDATE Page 2 of 8
ECMO UtilityRandomized Trials
• Bartlett, et al Pediatrics 1985; 76:479-487
• O’Rourke, et al Pediatrics 1989; 84:957-963
• UK Trial Lancet 1996; 348:75-82
Neonatal ECMOUK Trial
ECMO C ti lECMO Conventional
63/93 (68%) 38/92 (41%) p<0.0005
59/75 (79%) 38/75 (51%) p<0.0006)
(No CDH)
Lancet 1996
ELSO
Extracorporeal LifeSupport Organization
Est. 1989Membership Voluntary
Data CollectionStandards
Scientific Exchange
ECMO Circuit
PumpVenous Reservoir
OxygenatorHeat Exchanger
Safety MechanismsCannula
FANNP 24TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A9: NEONATAL ECMO: AN UPDATE Page 3 of 8
FANNP 24TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A9: NEONATAL ECMO: AN UPDATE Page 4 of 8
When is ECMO needed (generally)?
• When tissue oxygen requirements are not being met by biologic organs and “conventional” care ... usually manifest by progressive metabolic acidosis mixed venousmanifest by progressive metabolic acidosis, mixed venous desaturation (SvO2), and multiple organ failure
• When irreversible biologic organ damage is occurring with conventional care
• When expected mortality likelihood approached 80-90% with conventional care
Indications for ECMO
• Severe Respiratory Failure
• Severe Barotrauma
• Cardiac Failure
Neonatal ECMO
• No lethal anomaly
• No cyanotic heart diseaseNo cyanotic heart disease
• No bleeding diathesis
• No intracranial hemorrhage (relative)
• < 10 days of mechanical ventilation (relative)
Criteria for ECMO
• Alveolar-arterial gradient• Oxygenation indexyg• Barotrauma• Cardiac arrest• Acute deterioration• Failure to respond
Contraindicationsfor ECMO*
• Severe PrematuritySevere Prematurity• Profound Neurological Deficit• Severe Anomalies• Bleeding Diathesis
*( Never Rule it Out!)
FANNP 24TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A9: NEONATAL ECMO: AN UPDATE Page 5 of 8
Oxygenation Index
Mean Airway Pressure x FiO2 x 100y 2
Postductal paO2
ECMO Complications
Patient
Mechanical
Patient Complications
• Seizures
• Intracranial hemorrhage
• Renal failure
• Bleeding
• Hypertension
• Hemolysis
• Others
Mechanical Complications
• Oxygenator failure
• Pump malfunction
• Cl t• Clots
• Air in circuit
• Cannula problems
• Cracks in tubing
• Raceway rupture
• Others
Time on ECMO
Neonates
Survivors Non-SurvivorsSurvivors Non Survivors128 Hours 172 Hours
Cause of Death
• Intracranial Hemorrhage
• Sepsisp
• Cardiac Failure
• Failure To Respond
• Other
FANNP 24TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A9: NEONATAL ECMO: AN UPDATE Page 6 of 8

ELSO Registry Data Summaryy
July 2011
Active ECLS Centers
2000
2500
3000
3500
80
100
120
140
160
of
Ru
ns
f C
en
ters
0
500
1000
1500
0
20
40
60
80
90 92 94 96 98 00 02 04 06 08 10
Nu
mb
er
o
Nu
mb
er
o
Centers
Cases
ELSO Registry July 2011
Texas ECMO Centers
Overall Patient Outcomes
Total Surv ECLS Surv to DC Neonatal Respiratory 24,770 20,951 85% 18,558 75% Cardiac 4,375 2,649 61% 1,723 39% ECPR 694 438 63% 270 39% Pediatric Respiratory 5,009 3,251 65% 2,785 56% Cardiac 5,423 3,468 64% 2,609 48% ECPR 1,347 720 53% 539 40% Adult Respiratory 2,620 1,655 63% 1,428 55% Cardiac 1,680 894 53% 660 39% ECPR 591 225 38% 173 29% Total 46,509 34,251 74% 28,745 62%
ELSO Registry July 2011
Initial Mode of Neonatal Respiratory Support
VA, 67%VA
VV
VVDL
ELSO Registry July 2011
VV, 2%VVDL, 23%
VA+V, 5%
VV-VA, 3%Other, 0%
VA+V
VV-VA
Other
Runs by Year
60%
80%
100%
Card (16 years and over)
Card (1 year < 16 years)
Card (31 days < 1 year)
Card (0 - 30 days)
Adult Pulm
Ped Pulm
0%
20%
40%
Ped Pulm
Neo Pulm
ELSO Registry July 2011
FANNP 24TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A9: NEONATAL ECMO: AN UPDATE Page 7 of 8
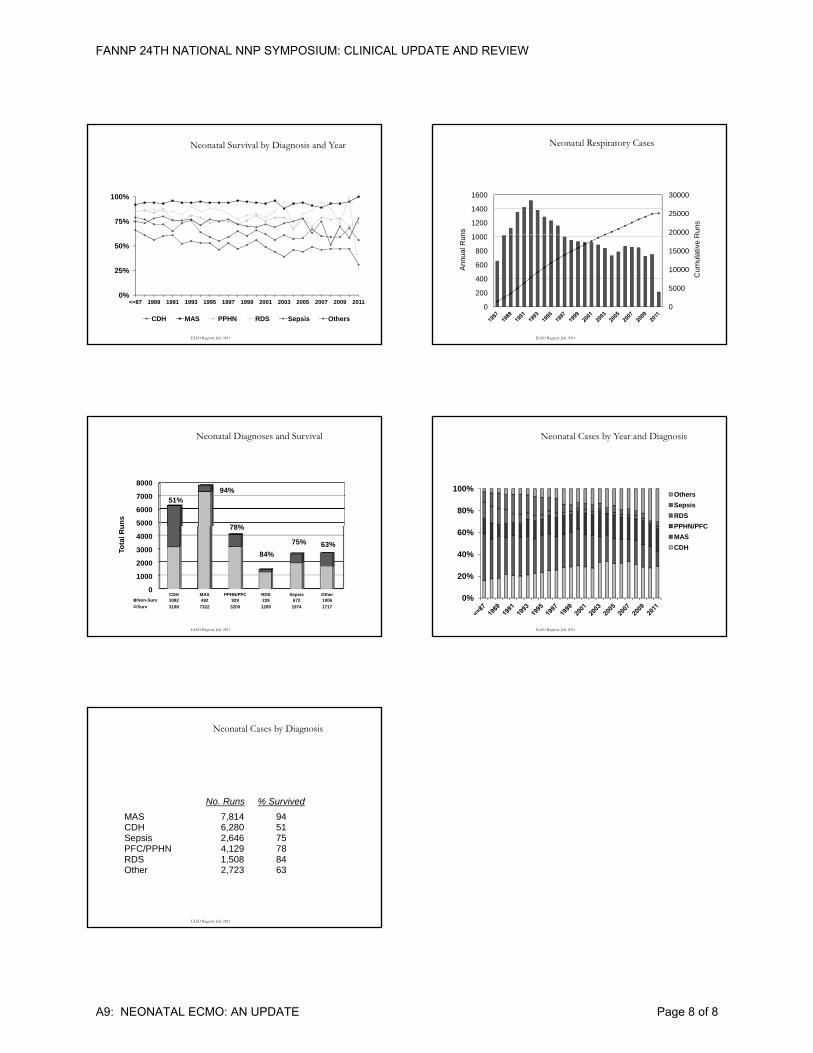
Neonatal Survival by Diagnosis and Year
75%
100%
0%
25%
50%
<=87 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011
CDH MAS PPHN RDS Sepsis Others
ELSO Registry July 2011
Neonatal Respiratory Cases
20000
25000
30000
1000
1200
1400
1600
Run
s
ns
0
5000
10000
15000
20000
0
200
400
600
800
1000
Cum
ulat
ive
R
Annu
al R
un
ELSO Registry July 2011
Neonatal Diagnoses and Survival
5000
6000
7000
8000
un
s
51%94%
78%
0
1000
2000
3000
4000
CDH MAS PPHN/PFC RDS Sepsis OtherNon-Surv 3082 492 929 239 672 1006
Surv 3198 7322 3200 1269 1974 1717
Tota
l Ru
75%
84%
78%
63%
ELSO Registry July 2011
Neonatal Cases by Year and Diagnosis
80%
100%Others
Sepsis
RDS
PPHN/PFC
0%
20%
40%
60%PPHN/PFC
MAS
CDH
ELSO Registry July 2011
Neonatal Cases by Diagnosis
No. Runs % Survived
MAS 7 814 94
ELSO Registry July 2011
MAS 7,814 94 CDH 6,280 51 Sepsis 2,646 75 PFC/PPHN 4,129 78 RDS 1,508 84 Other 2,723 63
FANNP 24TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A9: NEONATAL ECMO: AN UPDATE Page 8 of 8