editor’s page - iap...
TRANSCRIPT

1 June 2013
Dr. Remesh Kumar R.Medical Superintendent & PediatricianNSS Medical Mission Hospital, Pandalam Mob : 94474 57594Email : [email protected]
E D I T O R ’ S P A G E
design & production : pixel studio, cochin @ 0484-2806301
Dear colleague,
Warm Greetings in a cool monsoon !. The best thing we at the Editorial desk of Pediatric Companion can offer our colleagues in this season is sensible reading material in the cozy comforts of their office room. We hope we are doing justice to the task entrusted to us through the columns of our dear ‘Companion’.
The initial half of the academy year has seen IaP Kerala moving swiftly with a wide array of academic & community programs. almost all the branches have planned & executed the IMNCI & NSSK Workshops mooted at State level by the vibrant Prez Dr.S.S. Kamath & Sec Dr. Suresh Kumar E.K. ably liaisoned with NRHM by Dr. M.a. Mathew. The immunization, asthma, Down’s Syndrome & autism days are quickly catching up as a regular feature in the branch calendars. apart from the conventional ORS, Breastfeeding & Teenage Day Celebrations, these new awareness programs have surely taken our academy to a different height in community perspective.
We at state level have got 400 more colleagues this year to share the academic & social festivities in the IaP Kerala umbrella fold. Dr. Narayanan who heads the membership campaign committee deserves all credit for bringing this many friends to our midst in a short period.
As for our journal, we are trying to beautify it every issue with the best possible attire. This volume carries a new feature “Practitioner’s column” in addition to all the ongoing regular columns. My sincere thanks to all those who are involved with the journal proceedings especially those who are contributing through material and moral support. I owe a lot to Dr. anandakesavan & Dr. Suresh Kumar E.K. for guiding me through the release of each issue of Pediatric Companion.
Wish You all a Happy Reading !
Yours in the academy,
President : Dr. S.S. KamathVice President : Dr. T.M. ananda KesavanSecretary : Dr. Suresh Kumar E.K.Treasurer : Dr. Riyaz I.Joint Secretary : Dr. Shimmy Paulose Imm. Past President : Dr. M.R. Nair
IAP StAte OffIce beArerS 2013Imm. Past Secretary : Dr. Jose O.President Elect : Dr. Shaji Thomas JohnVice President Elect : Dr. Prasad K.N.Editor : Dr. Remesh Kumar R.Website Editor : Dr. Muhamed IsmailNational EB Members : Dr. S.S. Kamath Dr. Santhosh M.K., Dr. Jayaraman T.P.
PeDIAtrIc cOMPANION OffIce beArerS 2013
Dr. M.K.C. NairDr. T.U. SukumaranDr. Kurian ThomasDr. abraham K. PaulDr. S.S. KamathDr. Sushama BaiDr. Parvathy V.K.Dr. Lalitha KailasDr. a. Riyaz
Dr. T.M. anandakesavanDr. Babu GeorgeDr. Sr. Betty JoseDr. Jayakumar C.Dr. Jayakumar P.R.Dr. Jayakrishnan M.P.Dr. Jayaram ShankarDr. Mohammed Kunju
Dr. Muhamed Ismail Dr. Narayanan M.Dr. Naushad K.Dr. Prashanth PavithranDr. Preetha RemeshDr. Pisharody P.N.N.Dr. Radhakrishnan V.V.Dr. Sajikumar J.
Dr. Santhosh M.K.Dr. Suresh Kumar E.K. Dr. Sushama PrabhuDr. Silvan Mathews GeorgeDr.Shaji Thomas JohnDr. Tonny Mampilly Dr. Venkiteswaran M.N.Dr. Zulfikar Ahmed M.
Advisory BoArd EditoriAl BoArd
2 Pediatric Companion
Dear Colleagues,I thank each and every
member of the academy for supporting all IaP activities
and appreciate your commitment for the betterment of children in Kerala.
I congratulate all the branch office bearers and Pediatricians for their whole hearted commitment towards president’s action Plan, Single Digit IMR. a document for IMR reduction was presented to the Government of Kerala. The government has decided to do a micro level planning and Health Secretary has requested IaP to do the initial work for the same.
The govt. has requested to furnish details on the infrastructure development, equipment and manpower required. Dr. M.K.C. Nair, Dr. Rajmohan and their team are working on this.
IaP in association with NRHM is a model for child health development in most States. IMNCI, FMNCI & NSSK programs are going extremely well and funds to these programs are already allotted. NRHM has appreciated the commitment of the members for the success of these programs. all these surveys shows that IaP is a better stakeholder. I feel that the private hospitals also need to be included in the IMNCI program. Tertiary Neonatal care to support the IMNCI program.
a review of vaccinology update teaching module is being prepared by Dr. Geetha and Dr. Suresh Kumar, State Secretary who are fully involved in it.
Regarding management protocol for common pediatric illnesses, Govt. has given permission
to IaP to formulate a protocol and publish it by august 2013.
I take this opportunity to congratulate Dr. Rajagopal, Dr. Jayaraman, Dr. Riyaz, Dr. Krishna Kumar, Dr. Suresh Kumar E.K., Dr. Geetha, Dr. Bijili, Dr. Krishnan and their team who raised to the occasion at attapadi and with no publicity did real work to help the needy.
I request all the members to take the Family Benefit Scheme seriously which is the dream project of Dr T.U. Sukumaran, with Dr. George F. Moolayil as the Chairman. We need to inform all our colleagues regarding this great project and help them to enrol.
All the activities and projects started by Dr. M.R. Nair, efficient immediate past president of Kerala IaP will be continued. ‘Touch’ programmes are allotted to many branches in Kerala state and this prestigious project will help to improve the quality of care in the hospitals in periphery.
as you all are aware, I am coming out with many activities to help young children who need special care. My seniors in the profession are guiding me and with their blessings and support, I feel I can achieve the targets set in stipulated time. I expect your wholehearted support in all the ventures I take up.
I once again thank you all for giving me this opportunity to work for our prestigious academy.
Thanking you, Jai IaP,
Dr. S. Sachidananda KamathPresident, IaP Kerala
M E S S A G E F R O M P R E S I D E N T
Welcome 400 odd neonate Central IAP members from Kerala !Hats off to the Membership Drive Team of IAP Kerala who have enrolled more than 400 members in Central IAP rolls from April 2012 to Mar. 2013. IAP Kerala whole heartedly welcome the newly enrolled fellow pediatricians to march under IAP flag. Kudos to Dr. Narayanan M. & Dr. Remesh Kumar R. who planned & executed the membership campaign in a meticulous manner.
IAP Kerala 2013 State EB
3 June 2013
Dear Colleagues,Greetings from the office bearers of IaP
Kerala!almost all Sundays we have one or other
IaP conference or CME. Kerala IaP is touching all areas of child health and all IaP members are updated on recent developments in medicine.
all the members of IaP Kerala worked hard for last few months. It was really hectic for each of you. IaP Kerala membership drive, guided by Dr. Narayanan and Dr. Remesh Kumar gathered momentum in the last two months and we were able to add around 200 new members. Membership of IaP Kerala is 1680, and IaP Trivandrum must be congratulated for adding 39 new members. Dr. Bennet and Dr. Remesh Kumar require special appreciation for adding maximum number of new members. It is a commendable achievement. I thank all my colleagues for achieving this. IMNCI, IYCN, NSSK programmes conducted at various branches with the support of NRHM helped IaP to serve the community by sharing knowledge with health care workers.
We are now looking forward to bring down IMR in Kerala. President Dr. Sachidananda Kamath is working 24x7 to achieve the target of single digit IMR as it is the President’s action plan for the year. For the same he has already done the first stage consultative meeting on single digit IMR involving eminent faculty from various states and HODs of Medical Colleges, senior Neonatologists and senior Pediatricians from the State. It has reached a stage of final document preparation.
Vaccicon TOT program conducted at Cochin was also a grand success. We have trained more than 75 Pediatricians to conduct programs at their respective branches. The support we got from Dr. Rohit Agrawal, Dr. Pravin Mehta and Dr. Vijay Yewale was encouraging.
TOT programs on disability detection were conducted at Kozhikode and Pathanamthitta recently. again a well appreciated programme under the leadership of Dr. M.K.C. Nair and D. Remesh Kumar.
Prevention of neonatal deaths is the most important task ahead. We need to look into even the minute aspects of factors responsible for the death of neonates. IaP will be coming out with disease management protocols and proper transport guidelines for Neonatal Nurseries.
We are proud of our senior member Dr. K.C. Rajagopal and CIAP EB member Dr. T.P. Jayaraman for conducting a Medical camp at attappadi to detect malnutrition. They also conducted classes for health care workers. IaP is the only medical organization conducting many public activities and keen to develop strategies to prevent diseases.
IaP EB meeting and family get-together was well organized by Wynad IaP team under Dr. Sr Betty, Dr. Yaswanth and Dr. Sajith. 1st planning meeting on protocols for common diseases was also conducted at Wynad on May 26th.
Safe injection practices training for house surgeons and junior doctors are being conducted at various medical colleges under the supervision of Dr. M.a. Mathew.
It is a great news that our Pediatric companion is being appreciated by academicians all over India. Also our prestigious journal is now giving profit to IAP. Editor, Dr. Remesh Kumar needs to be appreciated for the efforts taken.
I place on record the support I get from seniors Dr. T.U. Sukumaran, Dr. M.K.C .Nair, Dr. Remesh, Dr. Jose, Dr. Shaji Thomas John, Dr. Santhosh and and many others. Under the able supervision of Dr P.M. Muhamed Ismail, website editor, we are coming out with a modified look for our webste in the coming days. Under the leadership of National IaP President, Dr. C.P. Bansal, State IaP President Dr. Sachidananda Kamath and IaP Secretary General Dr. Sailesh Guptha we can do more in the coming months.
Jai IaP, Jai India!Dr. Suresh Kumar E.K.Secretary, IaP Kerala
S E C R E T A R Y ’ S M E S S A G E

4 Pediatric Companion
Asthma and Allergic Rhinosinusitis in Children
dr. t.U.sukumaranProf. of Pediatrics,
Pushpagiri Institute of Medical SciencesThiruvalla
Rhinitis is defined as inflammation of the membranes lining the nose and is characterized by nasal congestion, rhinorrhea, sneezing, itching of the nose and/or postnasal drainage. atopy is an important risk factor for rhinitis and allergic rhinitis (aR) is the most common form. although a cause of significant and widespread morbidity, aR is often viewed, rather erroneously as a trivial disease. It may significantly affect the quality of life of the patient by causing fatigue, headache, cognitive impairment and other occasional symptoms.
Epidemiology of Ar in indiaIn India, ISaaC study was conducted in 14
centers. Phase I included 30,879 children in the 6-7 year age group while there were 37,171 children in 13-14 year age group. Data from India reveled that nasal symptoms were present in 12.5% children in 6-7 years age group & 18.6% in the 13-14 years age group. Allergic rhinoconjunctivitis was seen in 3.3% and 5.6% respectively. ISSaC study in our centre showed a prevalence 35% and 40% respectively.
Diagnosis of allergic Rhinitis is by: 1.Clinical evaluation – History and physical examination, 2.Lab investigations, 3.Categorisation of severity and duration and 4.assessment of co morbidities
Clinical FeaturesAllergic rhinitis is defined as a symptomatic
disorder of nose induced by IgE mediated inflammation, after allergen exposure of the nasal mucous membrane . It is a condition manifested by 1.Nasal blockage, 2.Running nose (Rhinorrhoea), 3.Sneezing, 4.Itching.
To diagnose allergic rhinitis, any 2 of the above 4 symptoms must be present for >1 hr every day for >2 wks. also there has to be some associated symptoms such as facial pain, loss of sense of smell, and postnasal drip. Some individuals may develop sinus infection and disturbed sleep as well.
Nasal Examination :a careful external and internal examination
of nose is essential in diagnosing allergic rhinitis.1. a deviated nasal septum can sometimes be
apparent externally.2. Gross nasal polyps can produce expansion of
nasal bones.
3. a horizontal crease above the tip of the nose called ‘Darrier’s Line’ is characteristic feature of marked allergic rhinitis. The darrier’s line is caused by the patient persistently rubbing the nose from below upwards with the palm of the hand.
4. ‘allergic salute’ is done to relieve itching and free oedematous turbinates from the septum.
5. The patient may exhibit facial grimaces like nose wrinkling and mouth wrinkling which relieves the nasal itching of the rhinitis. (allergic Mannerism).
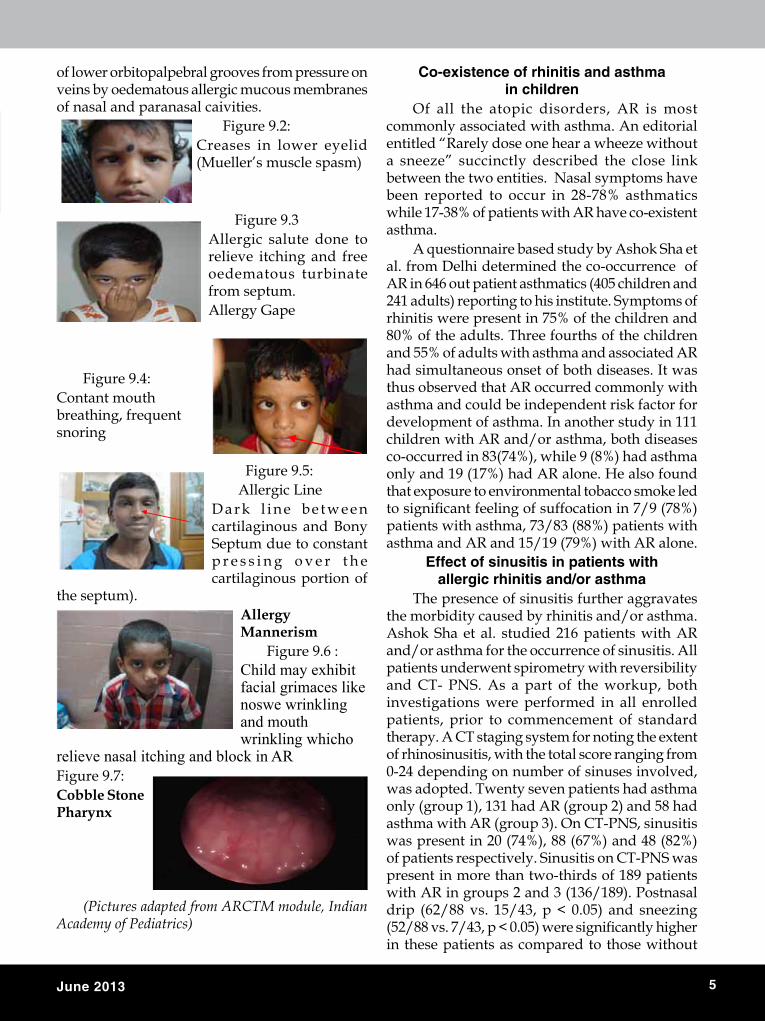
6. With the worsening of symptoms, many chi ldren may develop bluish-black discolorations under the lower eye lids which are termed ‘allergic shiners’. These discolorations are caused by venous stasis in the areolar tissue of the lower palpebral grooves from pressure on veins by oedematous allergic mucous membranes of the nasal and paranasal cavities.
7. an internal examination using a simple nasal speculum can show an anterior deviation of the septum, narrowing of the nasal valve and inferior turbinate hypertrophy.
8. Nasal polyps can easily be confused with swollen inferior turbinates. Nasal polyps are non tender and grayish, whereas swollen turbinates are tender and pale purple or pink.Figure 9.1:
B l u i s h - b l a c k d i s c o l o r a t i o n s u n d e r l o w e r eyelids which are termed “alergic shiners”, caused by various stasis in areolar tissues
5 June 2013
of lower orbitopalpebral grooves from pressure on veins by oedematous allergic mucous membranes of nasal and paranasal caivities.
Figure 9.2:Creases in lower eyelid (Mueller’s muscle spasm)
Figure 9.3allergic salute done to relieve itching and free oedematous turbinate from septum.allergy Gape
Figure 9.4:Contant mouth breathing, frequent snoring
Figure 9.5:allergic Line
D a r k l i n e b e t w e e n cartilaginous and Bony Septum due to constant p r e s s i n g o v e r t h e cartilaginous portion of
the septum).Allergy Mannerism
Figure 9.6 :Child may exhibit facial grimaces like noswe wrinkling and mouth wrinkling whicho
relieve nasal itching and block in ARFigure 9.7:Cobble Stone Pharynx
(Pictures adapted from ARCTM module, Indian Academy of Pediatrics)
Co-existence of rhinitis and asthma in children
Of all the atopic disorders, aR is most commonly associated with asthma. an editorial entitled “Rarely dose one hear a wheeze without a sneeze” succinctly described the close link between the two entities. Nasal symptoms have been reported to occur in 28-78% asthmatics while 17-38% of patients with aR have co-existent asthma.
a questionnaire based study by ashok Sha et al. from Delhi determined the co-occurrence of aR in 646 out patient asthmatics (405 children and 241 adults) reporting to his institute. Symptoms of rhinitis were present in 75% of the children and 80% of the adults. Three fourths of the children and 55% of adults with asthma and associated aR had simultaneous onset of both diseases. It was thus observed that aR occurred commonly with asthma and could be independent risk factor for development of asthma. In another study in 111 children with aR and/or asthma, both diseases co-occurred in 83(74%), while 9 (8%) had asthma only and 19 (17%) had aR alone. He also found that exposure to environmental tobacco smoke led to significant feeling of suffocation in 7/9 (78%) patients with asthma, 73/83 (88%) patients with asthma and aR and 15/19 (79%) with aR alone.
Effect of sinusitis in patients with allergic rhinitis and/or asthma
The presence of sinusitis further aggravates the morbidity caused by rhinitis and/or asthma. ashok Sha et al. studied 216 patients with aR and/or asthma for the occurrence of sinusitis. all patients underwent spirometry with reversibility and CT- PNS. as a part of the workup, both investigations were performed in all enrolled patients, prior to commencement of standard therapy. a CT staging system for noting the extent of rhinosinusitis, with the total score ranging from 0-24 depending on number of sinuses involved, was adopted. Twenty seven patients had asthma only (group 1), 131 had aR (group 2) and 58 had asthma with aR (group 3). On CT-PNS, sinusitis was present in 20 (74%), 88 (67%) and 48 (82%) of patients respectively. Sinusitis on CT-PNS was present in more than two-thirds of 189 patients with aR in groups 2 and 3 (136/189). Postnasal drip (62/88 vs. 15/43, p < 0.05) and sneezing (52/88 vs. 7/43, p < 0.05) were significantly higher in these patients as compared to those without

6 Pediatric Companion
sinusitis. Co-existent sinusitis increased the severity and morbidity caused by aR especially, in those who were predominantly “blockers”.
MANAGEMENt allergic rhinitis is mainly a clinical diagnosis
and management is mainly four fold. 1. Environment control, 2. Pharmacotherapy,
3. Treatment of co-morbid conditions, 4. Immunotherapy
Recognizing allergy triggers and avoiding them is the first step towards controlling Allergic symptoms. avoid allergic triggers like dust mite, pollen grain, animal dander, cockroach, moulds, cold air, cigarette smoke, firewood smoke, mosquito coils, etc.
Pharmacotherapy1. Second Generation antihistamines (SGa)2. Intra Nasal Steroids (INS)3. Leukotriene Inhibitors1. Second Generation Antihistamines It should be prescribed due to their favorable
efficacy and safety rate. SGa have greater selectivity for peripheral H1 receptors. It has anti-allergic effect independent of action at histamine receptors and long term treatment with SGa is safe. Drugs used are Cetrizine, Levocetrizine, Fexofenadine, Loratidine and Ebastin.
2. Intranasal SteroidsINS are the first line drug for treatment
of moderate to severe allergic rhinitis. It is the most efficacious medication available and it can improve all symptoms of allergic rhinitis as well as allergic conjunctivitis. Quality of life is better compared to antihistamines. Main INS are Budesonide, Beclomethasone, Fluticosone Propionate and Mometasone.
3.Anti-Leukotrienes (Monteleukast)It is indicated in seasonal allergic rhinitis,pre
school children and allergic rhinitis associated with other comorbid conditions like asthma and conjunctivitis. Although combinations of antihistamines with monteleukast is beneficial in several studies, it is not recommended.
table 9.2: treatment of Allergic rhinitis (AriA Guidelines)
indications for immunotherapy Q Definite specific allergen trigger Q Inadequate response to environment control Q Inadequate response to pharmacotherapy Q Undesirable side effects to pharmacotherapy Q Poor compliance to long term pharmacotherapy Q Patients who have perennial disease Q Possible prevention of asthma from aR
references1. allergic Rhinitis and its impact on asthma. aRIa
guidelines. 1999, available at http://www.whiar.com February 28,2004.
2. Beasly R, Keil U, Von Mutius E, Pearce N. World wide variation in prevalence of symptoms of asthma, al-lergic Rhinoconjunctivitis and atopic eczema, ISACC. Lancet 1998, 351: 1225-32
3. ashok Sha, Ruby Pawankar, allergic Rhinitis and co-morbid asthma: Perspective from India- aRIa asia-Pacific Workshop Report, Asia Pacific Journal of Allergy and Immunology (2009) 27:71-77.
Intermittent• <4days per week• <4 weeks per year
Persistent• > or =4 days per week• And > or = 4 weeks per year
MildNormal sleep and no impairment
of daily activities,sports,leisures and normal work at school and no troublesome symptoms.
Moderate - Severe one or more items• Abnormal sleep• Impairment of daily activities,
sports, leisures.• Abnormal work at school and
troublesome symptoms.
Table 9.1: ARIA classification
Mild Intermittent
Moderate –Severe Intermittent
Mild Persistent
Moderate – Severe Persistent
Intranasal Steroids and LTRA
Oral 2nd generation antihistamines or LTRA
Environmental control
Immunotherapy

7 June 2013
Pharmacological management of Attention Deficit Hyperactivity Disorder
dr. P. Krishnakumar Addl. Professor of Pediatrics
Govt. Medical College, Kozhikode & Director, Institute of Mental Health and
Neurosciences(IMHANS), Kozhikode
Attention Deficit Hyper activity Disorder (aDHD) is the most common child psychiatric disorder with a prevalence rate of 5-10% among school aged children. The three cardinal clinical features of aDHD are hyperactivity, impulsivity and inattention. There are three sub-types of aDHD - Predominantly hyperactive - impulsive type, predominantly inattentive type and the combined type. In majority of children all the three features are present. Children with hyperactivity present early to the pediatrician whereas children with predominantly inattention are noted when attention problems affect academic functioning and hence usually during the primary school or secondary school age. as the age advances hyperactivity comes down and attention problems become more predominant.
diagnosisThere are no diagnostic tests for aDHD
and diagnosis is made based on clinical criteria. according to DSM IV, to make a diagnosis of aDHD, the symptoms should be present for more than six months duration and should be present in more than one situation. (eg. school and home). The symptoms must begin before the age of 7 years and should not be secondary to other medical or psychological disorders. The symptoms should cause impairment in social, academic or occupational functioning. Co-morbid psychiatric disorders like oppositional defiant disorder, conduct disorder, learning disorder, anxiety disorders and depression are common in children with aDHD. Tics disorder and seizure disorder may coexist.
EtiologyGenetic factors, perinatal brain insult,
environmental toxins, endocrine abnormalities and structural brain defects are implicated in the etiology of aDHD. Thyroid hormone disorders and heavy metal poisoning like lead poisoning can lead to symptoms of aDHD and should be ruled out. Micronutrient deficiencies like iron deficiency, zinc deficiency may be associated with aDHD and should be treated. Food coloring agents and preservatives are reported to cause aDHD symptoms and should be looked for while treating children with aDHD.
abnormalities in the level of various neuro-transmitters like dopamine, nor-epinephrine and epinephrine in the CNS are associated with aDHD. Drugs effective for aDHD act through modifying the functioning of neural circuits involving these neurotransmitters.
treatmentT h e t r e a t m e n t o f aD H D i n c l u d e s
psychosocial interventions and pharmacotherapy. Pharmacotherapy should be combined with psychosocial interventions.
Drugs used to control the symptoms of aDHD are usually divided into two groups - CNS Stimulant drugs and the non- stimulant drugs. CNS stimulant drugs include methylphenidate, dextroamphitamine and their combinations. The non stimulants include atomoxetin, clonidine, and risperidone. Tricyclic antidepressants like imipramine are now not advised for the treatment of aDHD due to potential cardiovascular side effects.
stimulant drugsStimulant drugs act by increasing synaptic
level of dopamine and nor-epinephrine in the central nervous system. They are effective in controlling hyperactivity and impulsivity and improving attention span in children with aDHD.
MethylphenidateDuration of action of methylphenidate is 3-4
hours only and hence should be given in multiple doses. The usual recommended dose is 0.3 to 1 mg per Kg three times a day up to 60 mg per day. 5,10and 20 mg tablets are available. The drug is usually given three times a day but the doses could be adjusted according to school time so that the maximum effect of the drug occurs during the school hours. One common brand available in India is aDDWISE. Methylphenidate is not indicated in children below the age of 6 years.

8 Pediatric Companion
Sustained release preparations of methyl-phenidate are available now. Sustained release preparations could be given once daily or twice daily dose. One preparation available in India is with brand name Inspiral SR. Methylphenidate is effective in controlling symptoms in three fourth of children with aDHD.
The most common immediate side effects of methylphenidate include head ache, stomach ache, nausea and insomnia. Sedation may also be complained. Loss of appetite and growth suppression are potential side effects of long term treatment with methylphenidate. Drug holidays during school vacation period are suggested to tide over loss of appetite and the resultant growth suppression. Methylphenidate therapy can lead to emergence of or exacerbation of tics. Hence should not be prescribed when associated tics disorder is present. Cardiovascular side effects can occur very rarely and hence regular monitoring of cardiovascular function is indicated. Rebound hyperactivity can occur in some children on starting methylphenidate.
MonitoringBefore starting stimulant medication detailed
physical examination should be done. Cardiac work up should be done if cardiovascular diseases suspected. Baseline blood pressure, pulse, weight and height should be documented. Child should be on regular follow up. Blood pressure, pulse, weight and height should be checked once in three months.
dextroamphitamineDextroamphitamine is the second line of drug
approved for treatment of children with aDHD. It can be prescribed for children above the age of three years. The drug got addictive potential in higher doses. The side effect profile is the same as methylphenidate. Dextroamphitamine is currently not available in India. The dose is 0.15 – 0.5 mg per kg twice daily up to 40 mg per day.
Non stimulant medications for AdHdNon stimulant drugs effective in the treatment
of aDHD include atomoxetine, clonidine and tricyclic antidepressants (imipramine). Tricyclics like imipramine are currently not recommended for treatment of aDHD due to potential cardiac side effects.
Atomoxetineatomoxetine is a non-adrenergic reuptake
inhibitor and is effective in controlling all the
three symptoms of aDHD. It could be prescribed in children above the age of 6 years. atomoxetin is considered as the second line drug in the management of aDHD. The drug is initiated at a dose of 0.5mg per Kg per day as a single daily dose or twice daily dose and gradually increased to 1.8 mg per Kg per day. Maximum dose of 80 mg per day could be given. 10mg, 18mg and 25 mg tablets/capsules / sachets are available. It is effective in adolescents and adults with aDHD. The common side effects are diminished appetite, fatigue, sleep disturbances, abdominal discomfort, dizziness and dry mouth. Irritability and increased behavior problems can occur rarely. Increase in heart rate and blood pressure has been reported. Severe liver injury can occur rarely. Suicidal ideation is reported associated with atomoxetine. Regular follow up and monitoring of pulse, BP and liver functions is essential.
ClonidineClonidine is an alpha adrenergic receptor
agonist. It is effective in controlling hyperactivity in children with aDHD. It can be prescribed for children below 6 years also. The common side effects are sedation and hypotension. Rebound hypertension can occur while discontinuing the drug. Hence slow withdrawal advised. The dose is 3-10 micrograms per Kg per day. 0.1 mg tablet is available. The drug may be started as a single bed time dose of 0.025mg(one fourth tablet) and gradually increased.
risperidone Respiridone and other antipsychotic drugs
will help to control the hyperactivity. Long term use will impair cognitive functions and extrapyramidal side effects can occur. Hence these drugs are not routinely advised for treatment of aDHD.
other drugs which have possible roleSelective Serotonin Reuptake Inhibitors
(SSRI) like fluoxetine will be effective when associated anxiety or depressive symptoms are present. Carbamazepine or sodium valproate will help to control impulsive behavior in certain children.
How to initiate drug therapyStart with methylphenidate or a long acting
preparation of methylphenidate if available. Initially prescribe the minimum required dose

9 June 2013
and gradually increase the dose over a period of four weeks. If there is improvement in symptoms the dose is gradually increased till optimum improvement is obtained. Drug is discontinued if any side effects occur. If no improvement after one month or if side effects occur then the second line drug is initiated. atomoxetine is the usual second line drug. If there is no improvement after a one month trial or if side effects occur third line drugs are tried. Clonidine could be used as a third line drug. If methylphenidate is not available atomoxetine could be tried as the first line drug.
Counseling on drug therapyChildren and especially adolescents do
not like taking medicines for long periods. In the case of aDHD there is the issue of child being labeled as “mad” or “abnormal” since the disease is associated with behavior problems. Hence counseling to both parents and children is important. Before starting drug therapy discuss the side effects, usefulness and compliance problems with parents. Children should be assured that drug therapy will not adversely affect their ability to study or play and stress the fact that drugs will only help to improve academic functioning. The child should be convinced of the need for drug therapy and also that regular drug treatment does not mean psychiatric illness.
Monitoring for AdHd symptoms
Rating scales like Connor rating scale or Vanderbilt rating scale should be used to rate the severity of symptoms at the time of starting
treatment. Rating is done on follow up visits to monitor improvement in symptoms.
Teacher reports about academic functioning at the time of starting treatment and on follow up visits could be used to monitor improvement in academic functioning and class room behavior.
Psychosocial interventionsFor optimum results, pharmacotherapy
should be combined with psychosocial interventions. Psychosocial treatments include behavior therapy, psychotherapy, family therapy and school and family based interventions.
Treatment of ADHD is not just prescribing drugs. academic and school problems and problems in the family environment can precipitate and exacerbate the behavior problems in a child with aDHD. These issues should be addressed along with pharmacotherapy. Most of the time pediatricians stop by prescribing drugs alone and hence the poor outcome. Counseling regarding the importance of balanced diet, avoiding junk foods and food preservatives should be part of the treatment program. Correction of iron deficiency, zinc deficiency and other micronutrient deficiencies will go a long way in improving the behaviour and attention span. advice regarding life style modification should be given. The importance of rest, play, TV time, and adequate sleep should be discussed with parents and children.
reference1. Kaplan & Sadock’s Synopsis of Psychiatry, 10th Edition2. Nelson text book of Pediatrics, 19th Edition
42nd Annual Conference of iAP Kerala state Branch Theme: Translating Science into Clinical Practice
date: 4th,5th, 6th oct,2013 Q CoNtoUr BACKWAtErs, CHANGANACHErry, KottAyAM
Organized by : IAP Kottayam Branch Q Dept. of Pediatrics, ICH, Medical College, Kottayam Q IAP Kerala
For Regn contact : Org Chair : dr C. Jayakumar, Mob: 9446053602 Org Secretary : dr. d. Balachandar Mob : 9447030371
For Free paper/Poster/Thesis presentation, contact Scientific Committee Chair dr. Jayakumar P.r. Mob:8281165957, [email protected]
From June 1: Rs 3700/- Workshop : Rs 750/- . From Sept 1 :Rs 4500/- Online transfer by : SBT, Amancherry, Kottayam, Pedicon 2013 . IFS code SBTR0000473 A/C No: 00000067213204905
KErAlA PEdiCoN 2013

10 Pediatric Companion
Gynaecomastia - An Overview
dr. G. reetha MD, DCH, Fellowship (Paed endocrinology)
Asso. Professor Pariyaram Medical College
introductionGynaecomastia is a benign condition in
males in which the glandular tissue of the breast proliferate ,resulting in a concentric enlargement of one or both the breasts.The term is derived from Greek which means ‘with breast like a woman’.
Pathogenesis Parenchymal and stromal cells with potential
for full breast development are present in both boys and girls. an appropriate stimulus can produce breast enlargement in both sexes. Gynaecomastia results from an imbalance between estrogen and androgen action .an absolute or relative increase in estrogen levels ;hypersensitivity of breast tissue to normal concentrations of estrogens;or decrease in the production,circulating concentrations or action of free androgens can cause gynaecomastia.
Pubertal gynaecomastiaThe exact etiology of pubertal gynaecomastia
remains to be fully elucidated.It may be due to alteration in the ratio of free testosterone to estrogen seen during puberty or due to hypersensitivity of the breast tissue to estrogens.Increased aromatisation of androgens to estrogens in the breast tissue may also be of significance.
Pubertal gynaecomasia may first appear as early as 10 years of age with a peak between 13-14 years.The glandular enlargement can be asymmetric ,unilateral and tender. Signs of pubertal development usually preceds the breast enlargement. Transient increase in glandular breast tissue may occur in as many as 75% of normal boys during the pubertal period and typically resolves in 2 years,though occasionally it might persist.
diagnosisGynaecomastia is clinically apparent when the
diameter of the glandular tissue exceeds 0.5 cm.With the patient lying supine, with the
hands locked together underneath the back of his head,the examiner should palpate with the thumb and forefinger at opposite corners of the breast.
In true gynaecomastia there will be a firm rubbery disk of tissue beneath the nipple. Pseudogynaecomastia or lipomastia is breast enlargement due to fat accumulation which seen in obesity,where there will be no resistance between the palpating fingers .
Causes of gynaecomastiaPhysiological Newborn,pubertal, old ageTumours Testis,adrenal,liverEndocrinopathies Hyperthyroidism,acromegaly,
cushing syndromeNon endocrine disorders
Chronic liver disease,CRF,malnutrition and refeeding,HIV,local trauma
androgen deficiency
Disorders of testosterone biosynthesis androgen insensitivity syndrome Hypogonadism -primary and secondary Ovotesticular DSD
Drug induced Hormones – androgens, estrogens, hCG, anabolic steroids,growth hormone Testosterone antagonists - cimetidine, ketoconazole Psychoactive drugs -tricyclic antidepressants ,phenothazine Others - phenytoin,digitalis,calcium channel blockers ,aCE inhibitorsDrugs of abuse
Idiopathic factors & heredity
Prepubertal gynaecomastia is rare and gynaecomastia prior to 10 years of age should be thoroughly investigated.
History should include details about drug intake,genital ambiguity,undescended testis,chronic illness.
Physical examination should include the following:
Q Examination of the breasts- size and consistency
Q assessment for any nipple discharge or axillary lymphadenopathy
Q Examination of the testicles,- size and consistency, nodules or asymmetry
Q Pubertal staging Q Observation of any signs of feminization Q Checking for any stigmata of chronic liver

11 June 2013
disease, thyroid disease, or renal disease or other endocrinopathies
Q Laboratory tests are performed in accordance with the c l in ica l f indings .Puberta l gynaecomastia usually does not need any detailed evaluation Hormonal test include hCG,LH FSH, testosterone, estradiol,DHEaS ,TFT. Karyotying and imaging of testis,adrenal or liver may be undertaken as required
treatmentPubertal gynaecomastia does not need
any treatment other than reassurance.It usually resolves within 18 -24 months in 90% of case .Specific treatment in indicated if the gynaecomastia causes significant pain or embarrassment to the patient.Treatment options available are medical and surgical.
Medical therapy Medical therapy is more successful during
the early proliferative phase.Therapeutic options include androgens, -dihydrotestosterone
Estrogen receptor antagonists- clomiphene citrate (100mg/day), tamoxifen(10-20 mg bd)for 3-6 months
aromatase inhibitors.-testolactone, ana-strozole
surgical therapyLong standing gynaecomastia is unlikely to
respond to medical therapy.Subcutaneous mastectomy through a
circumareolar incision has satisfactory results.Liposuction procedures also has been tried with variable results.Operative therapy before completion of puberty might result in recurrence of gynaecomastia.
references 1. MP Desai, PSN Menon,V Bhatia Pediatric endocrine
disorders second edition page 242-2462. Pediatric endocrinology.1; Pescovitz ora Hirsch,11
Eugster,Erica a page 349 -3593. Barros a C,Sampio Mde.C Sao Paulo Med. J. vol.130
(3):187-97 gynaecomastia- pathophysiology, evaluation and treatment
From June 20139th June Disability Detection TOT (South Zone) - Pathanamthitta 16th June Hematology Chapter State Conference - Kannur22-23 June Sessional Conference of IAP Kerala and Pedimedicine - Cochin 30th June Respiratory Chapter - Manjery7th July PALS provider course - Thiruvananthapuram28th July Adolescent Health Care Chapter State Conference - Madhya Kerala 4th August Pediatric Ophthalmology Chapter State CMe - Tiruvalla11th August Protocol CMe - Cochin18th August Nephrology Chapter State Conference - Trichur 25th August Dermatology Chapter State Conference - Vadakara 1st Sept. endocrinology Chapter State Conference - Thiruvananthapuram8th Sept. Nutrition Chapter State Conference - Thiruvananthapuram 7-8 Sept. Infectious Disease Chapter Stae Conference - Tellicherry22nd Sept. Gastroenterology Chapter - Kozhikode28-29 Sept. IAP Childhood Disability Group Conference, Cochin29th Sept. Critical Care chapter state CMe - Kozhikode 4-6th Oct. IAP Kerala State Conference - Changanacherry (Kottayam Branch) 19-20 Oct. South Pedicon - Belgaum 27th Oct. Neurology Chapter State Conference - Kasargod 17th Nov. Cardiology Chapter - Pariyaram1st Dec. environment & Child Health Group National Conference - Cochin
U P C O M I N G E v E N T S

12 Pediatric Companion
WBCs – The Flag bearers
dr. suresh Kumar E.K.Dept.of Pediatrics MIMS, Kozhikode
introduction
White Blood Cells are part of our immune system and plays an important role in protecting us from different types of infections. Pleuripotent hematopoietic stem cells arising from the bone marrow or, during fetal development, from the liver and marrow space undergo proliferation and differentiation to give rise to all lineages of peripheral white blood cells - Lymphocytes, monocytes, dendritic cells and polymorphonuclear leukocytes (neutrophils, basophils, and eosinophils). The number of white cells and the proportion of each cell type in the circulating blood are helpful in the diagnosis and management of many illnesses.
Total leucocyte count vary in different age groups.
Age Leukocyte count (x1000/mm3 µL0-30 days 9.1- 34.01-23 months 6.0- 14.02-9 yrs 4.0- 12.010-99 yrs 4.0- 10.5
WBC differential counts indicate the relative proportions of different kinds of leukocytes in the blood.The absolute count of each cell type is obtained by multiplying the total WBC by the percentage of that cell type in the differential count and is expressed as a multiple of 109/L. absolute values for neutrophils and lymphocytes are more clinically relevant than percentage values. The absolute neutrophil count (aNC) decreases during the first day of life and then remains almost same for 2 years and reaches the adult mean at about 3 years of age. african-americans have slightly lower aNC than other races. a few metamyelocytes and even myelocytes are common in the peripheral blood of the newborn. In premature infants, more of these immature neutrophils and even myelocytes and blast cells may occasionally be seen. The absolute lymphocyte count (aLC) in early infancy is more than twice that found in the adult. Monocytes, basophils, and eosinophils are relatively abundant in the first weeks after birth and then gradually decline to the lower adult values.
disorders of white blood cells
Disorders of white blood cells can be classified into two broad categories.
1. Proliferative disorders (Leukocytosis), in which there is an expansion of leukocytes.
2. Leukopenias, which are defined as a deficiency of leukocytes.
Proliferations of white cells can be reactive or neoplastic. Since the major function of leukocytes is host defence, reactive proliferation in response to an underlying primary, often microbial, disease is fairly common. Neoplastic disorders, though less frequent, are much more important clinically. an abnormally low white cell count (leukopenia) usually results from reduced numbers of neutrophils (neutropenia, granulocytopenia). Lymphopenia is less common. It is important to discuss each type of cells as the variation in count of each cell line affects the total WBC count.
Neutrophils
Neutrophils are myeloid-lineage cells characterized by the presence of granules containing enzymes and other potentially toxic agents involved in host defence.Mature neutrophils can be found in the bones of 11-week fetuses. Circulating hematopoietic progenitors, as evidenced by either CD34+ cells or CFU, are high in fetuses and neonates. Neutrophils function in acute inflammation and provide an essential defence against acute bacterial infections. abnormalities of neutrophil function are uncommon and associated with impaired ability to respond to life-threatening infections. a key function of neutrophils is to ingest foreign particles such as bacteria and degrade them through activation of proteases, activation of other antibiotic molecules and generation of toxic oxygen radicals.
Causes of Neutrophilia include Infections (Bacterial infections, particularly Streptococcus pneumoniae and staphylococci, fungal infections,

13 June 2013
some viral infections and rickettsial infections), Tissue damage or necrosis (surgery, burns, trauma, myocardial infarction, other tissue necrosis and hyperthermia),Inflammatory disorders (rheumatoid arthri t is , other autoimmune diseases, gout etc.) acute stress or physical exertion, seizures, acute haemorrhage, Hemolysis , Metabolic disorders like diabetic ketoacidosis , Hodgkin’s disease, Non-hematologic malignancies, Medications( lithium, corticosteroids, epinephrine, hematopoietic growth factors), Chronic idiopathic neutrophilia, Hereditary neutrophilia etc.
absolute neutrophil counts between 1.0 and 1.5 x 109/L are classified as mild neutropenia, between 0.5 and 1.0 x 109/L moderate neutropenia and below 0.5 x 109/L severe neutropenia. a wide variety of acquired conditions result in neutrophill dysfunction, depletion, or both including malignancies (myeloid leukemias), metabolic abnormalities (diabetes) and drugs (corticosteroids, chemotherapy). Many congenital disorders are also identified. Neutrophil function defects causes increased incidence of bacterial and fungal infections but not parasitic and viral infections. Heritable disorders of neutropenia include Severe congenital neutropenia (Kostmann’s syndrome), Benign congenital neutropenia, and Cyclic neutropenia. Diagnosis of Kostman syndrome is by mutation analysis and the treatment is with G-CSF. Leukocyte adhesion deficiencies, chemotaxis deficiency like Hyper IgE syndrome, Granule disorders like, Chédiak-Higashi syndrome, Myeloperoxidase deficiency, p14 deficiency and Oxidase Defects like Chronic granulomatous disease (multiple types) etc. are also heritable.
lymphocytes
Lymphocytes are found in large numbers in blood, lymph and in lymphoid organs such as the thymus, lymph nodes and spleen. They are essential for immunity. B-lymphocytes produce antibody against a specific antigen (humoral immunity) while T-lymphocytes are the cells of the cell-mediated response. Following an appropriate antigenic stimulus, B-lymphocytes transform into plasma cells and secrete antibody specific to that antigen.
an increase in lymphocytes in the blood (lymphocytosis) is generally a reaction to infection (Chronic infections like tuberculosis and toxoplasmosis, acute viral infections like infectious mononucleosis, rubella and bacterial infections likepertussis) or is part of a malignancy (Chronic lymphocytic leukemia and variants, Non-Hodgkin’s lymphoma, acute lymphoblastic leukaemia etc). a polyclonal T-cell lymphocytosis is a common response to viral infection, particularly in childhood.
Peripheral lymphocyte count seems to be maintained in a narrow range at 2000 to 4000/µL, 20% of which are B cells and 70% of which are T cells. Lymphocytopenia,, is a total lymphocyte count of less than 1500/µL. It can be the result of decreased production, defective trafficking, or increased loss or destruction. Decreased production can occur as a result of protein and calorie malnutrition; lymphocyte progenitor pool injury secondary to radiation, chemotherapy, or immunosuppressive agents; and congenital immunodeficiency states. Endogenous or exogenous glucocorticoid excess can cause lymphocytopenia by altering lymphocyte trafficking. This can also occur as the result of acute bacterial or fungal infections, certain viral infections and granulomatous disease.
Eosinophils
Eosinophils have proinflammatory and cytotoxic potential in the pathogenesis of allergic, parasitic, neoplastic and a variety of other idiopathic disease processes. Eosinophilia is defined as the presence of greater than 450 to 500 eosinophils/µL of blood as normally measured by sampling peripheral blood.
Diseases, Syndromes, and Conditions commonly associated with peripheral blood Eosinophilia and/or tissue Eosinophilia include, Infections (Parasitic Infections -Tropical eosinophilia, Visceral larval migrans, Helminth infections, Filariasis, Onchocerciasis, Schistosomiasis, Fascioliasis, Paragonimiasis, Strongyloidiasis, Trichinosis, Hookworm, ascariasis, Echinococcosis/hydatid disease etc, Fungal Infections – Coccidioidomycosis, Cryptococcosis ),allergic diseases (asthma, Urticarias, atopic dermatitis), Respiratory tract disorders (Hypersensitivity pneumonitis
14 Pediatric Companion
, aBPa, Eosinophilic pneumonia, Transient pulmonary infiltrates (Löeffler syndrome), Tropical pulmonary eosinophilia , Bronchiectasis, Cystic fibrosis), Addison disease,Inflammatory bowel disease (IBD), Eosinophilic gastroenteritis, eosinophilic esophagitis, allergic gastroenteritis, toxins, Connective tissue disorders, skin disorders, immunodeficiency syndromes, Solid tumors (mucin-secreting, epithelial cell origin), Chronic eosinophil leukemia, Idiopathic hypereosinophilic syndromes (HES) and Systemic mastocytosis.
other blood cells
Basophil granulocytes develop in the bone marrow and are released into circulation as mature end-stage cells that represent <1% of the leukocytes in blood. While their exact role in in vivo processes remains an enigma, basophils secrete a variety of mediators and cytokines that are central in allergic disease. Evidence indicates that basophils are particularly capable of generating IL-4 and IL-13, cytokines that promote IgE synthesis. Increased basophil count may be seen in asthma, urticarial, myeloproliferative disease (e.g., chronic myeloid leukemia) etc.
Transient monocytosis is common in many viral infections, usually during the recovery phase. Monocytosis also occurs with tuberculosis, infective endocarditis, syphilis, brucellosis, malaria, trypanosomiasis, and Rocky Mountain spotted fever.
Monocytopenia, eosinopenia, and baso-philopenia can be seen in the setting of bone marrow failure syndromes or as a result of acute infection, malignancy, or severe injury. Monocytopenia is less frequently seen, probably owing to the diverse roles monocytes play in normal human physiology; prolonged and extreme monocytopeniamay not be compatible with life.
summary
Even though it is impossible to come to a complete diagnosis with analysis of leukocytes in most of the situations, a clinical correlation of this simple laboratory test will give us valuable information during evaluation and lead us in the right direction.
oBitUArydr. P.P. George , Con-s u l t a n t P a e d i a t r i c i a n , Kothamangalam passed away on 14th March 2013.
He took his MBBS from Kakinada Medical College,
Andhra Pradesh, MD in Paediatrics from KMC Mangalore. He worked in St. George Hospital, Muvattupuzha and MBMM Hospital, Kothamangalam.He was an active member in IAP Malanad Branch. He is survived by his wife, Dr. Sheela George, Gynaecologist, doughter Aneeta, Software engineer and son Ashish, engineering Student.
dr. Jose Kuruvila, Prof of Pediatrics at Pushpagiri I n s t i t u t e o f M e d i c a l Sciences, Tiruvalla (former Prof of Pediatrics at ICH Kottayam) expired on 17th Apri l 2013 fol lowing a massive heart attack. He is survived by wife Mrs. Annamma V.D. ( Retd. Nursing Supdt. District Hospital, Kottayam), son Dr. Kiron T. Jose & daughter Soya Mary Jose.
dr. Muraleedharan, Retd Civil Surgeon and Senior Pediatrician, expired on April 21st, 2013. He was an active member of IAP Thrissur Branch. He is b lessed with a daughter (Sandya,
Pathologist) and son (Arun, engineer).
We at IAP Kerala pay loving tributes to these fellow members who flew to their heavenly abode and express our heartfelt condolences to the bereaved family.

15 June 2013
Infant with Atypical Genitalia – An Emergency ?
dr. riaz i.Ped. endocrinologist & Asst. Professor
Dept. of Pediatrics, SAT Hospital GMC, Thiruvananthapuram
Disorders of Sex Development (DSD) is the currently accepted general term for conditions in which infants present with atypical genitalia. Under this there are a wide range of specific diagnoses with diverse pathophysiology. a newborn infant with atypical genitalia often poses a major challenge to the treating physician as well as the parents.
Establishing a diagnosis, providing the emergency life saving treatment whenever needed, ascertaining the sex of rearing and following up these children providing adequate emotional support to the family are all as complex as the condition itself.
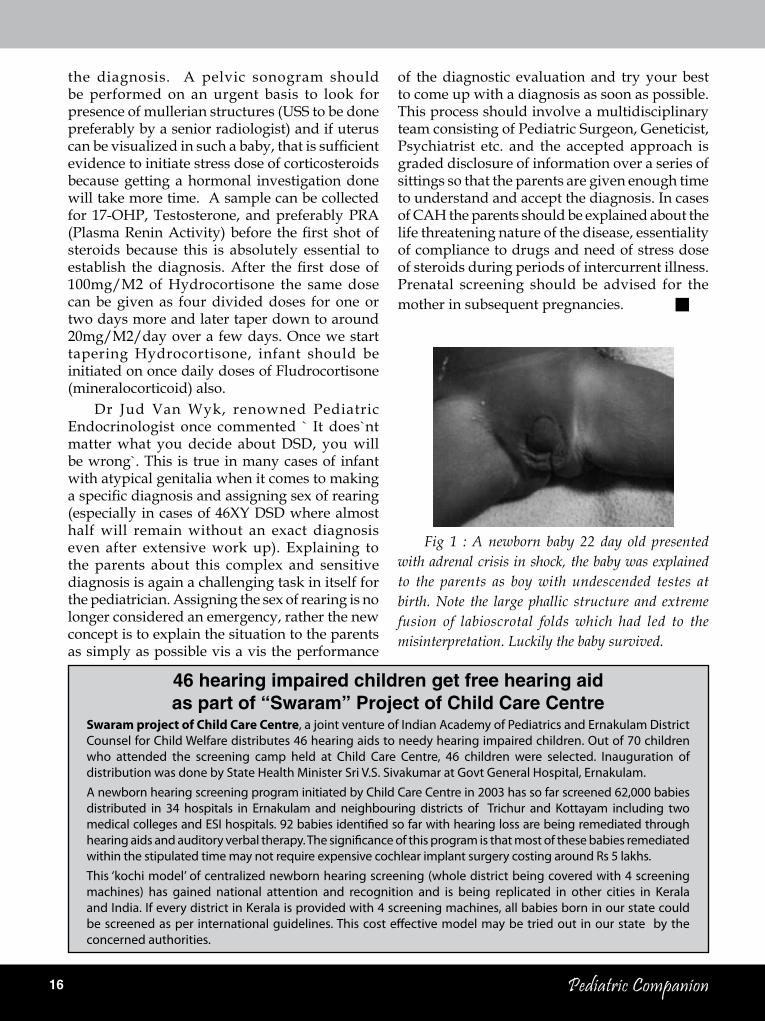
The birth prevalence of truly ambiguous genitalia which could arise a doubt regarding sex of rearing is rare, approximately one in 5000. a newborn with CaH with severe clitoromegaly could be misinterpreted as an apparent boy with undescended testes and later detected. It is our primary duty as a pediatrician attending delivery or doing the first newborn exam to perform a complete physical examination including genitalia. If we find any atypical features one has to use terms like labioscrotal folds (rather than labia or scrotum) and phallus (rather than clitoris or penis) to describe the external genitalia and examine for presence of gonads in the labioscrotal folds, the degree of fusion of the labioscrotal folds, size of the phallus and the site of the urinary meatus on the phallus, if possible. It is better to do this exercise in an objective way , for example calculating the External Masculinisation Score.
(Fig.1).an EMS of < 11 should prompt us to do further evaluation.
Congenital adrenal Hyperplasia, salt losing type is the most common cause of atypical genitalia and also the dangerous type. Infants with 46XY karyotype will have normal genitalia at birth. Infants with 46XX karyotype and severe virilisation could be labeled as ̀ normal boys` with undescended testes and could crash with a salt losing crisis during the initial weeks of life. When evaluating a baby for CaH it is very important to obtain samples only after 48 hours of life, and usually these babies will not develop adrenal crisis in the first week of life and their electrolytes could be normal initially.
These mishaps can be prevented if we do a systematic examination and scoring for any baby with slightest atypical features of genitalia at birth. a family history of consanguinity, stillbirths, neonatal deaths abortions, infertility, atypical genitalia or delayed puberty etc. should prompt the pediatrician to be more vigilant. associated dysmorphic features, limb anomalies, increased pigmentation of nipples and areola, axilla, umbilicus, genitalia and oral mucosa should be looked for. In a few weeks old infant failure to thrive, dehydration and acidotic breathing could be valuable clues for diagnosis of a salt losing type of CaH in adrenal crisis.
For any infant presenting in the Emergency Department in shock with any of the fore mentioned features Congenital adrenal Hyperplasia should definitely get a place in the list of DDs. Genital examination in such a child will reveal phallus (enlarged clitoris) with varying degrees of labioscrotal fusion with no palpable gonads. In such a case suspecting the condition, prompt investigations – basic and hormonal and immediate initiation of treatment will be life saving. Presence of hyperkalemia, hypoglycemia and acidosis in such a child strongly suggests
16 Pediatric Companion
of the diagnostic evaluation and try your best to come up with a diagnosis as soon as possible. This process should involve a multidisciplinary team consisting of Pediatric Surgeon, Geneticist, Psychiatrist etc. and the accepted approach is graded disclosure of information over a series of sittings so that the parents are given enough time to understand and accept the diagnosis. In cases of CaH the parents should be explained about the life threatening nature of the disease, essentiality of compliance to drugs and need of stress dose of steroids during periods of intercurrent illness. Prenatal screening should be advised for the mother in subsequent pregnancies. Q
Fig 1 : A newborn baby 22 day old presented with adrenal crisis in shock, the baby was explained to the parents as boy with undescended testes at birth. Note the large phallic structure and extreme fusion of labioscrotal folds which had led to the misinterpretation. Luckily the baby survived.
the diagnosis. a pelvic sonogram should be performed on an urgent basis to look for presence of mullerian structures (USS to be done preferably by a senior radiologist) and if uterus can be visualized in such a baby, that is sufficient evidence to initiate stress dose of corticosteroids because getting a hormonal investigation done will take more time. a sample can be collected for 17-OHP, Testosterone, and preferably PRa (Plasma Renin Activity) before the first shot of steroids because this is absolutely essential to establish the diagnosis. After the first dose of 100mg/M2 of Hydrocortisone the same dose can be given as four divided doses for one or two days more and later taper down to around 20mg/M2/day over a few days. Once we start tapering Hydrocortisone, infant should be initiated on once daily doses of Fludrocortisone (mineralocorticoid) also.
Dr Jud Van Wyk, renowned Pediatric Endocrinologist once commented ` It does`nt matter what you decide about DSD, you will be wrong`. This is true in many cases of infant with atypical genitalia when it comes to making a specific diagnosis and assigning sex of rearing (especially in cases of 46XY DSD where almost half will remain without an exact diagnosis even after extensive work up). Explaining to the parents about this complex and sensitive diagnosis is again a challenging task in itself for the pediatrician. assigning the sex of rearing is no longer considered an emergency, rather the new concept is to explain the situation to the parents as simply as possible vis a vis the performance
46 hearing impaired children get free hearing aid as part of “swaram” Project of Child Care Centre
Swaram project of Child Care Centre, a joint venture of Indian Academy of Pediatrics and Ernakulam District Counsel for Child Welfare distributes 46 hearing aids to needy hearing impaired children. Out of 70 children who attended the screening camp held at Child Care Centre, 46 children were selected. Inauguration of distribution was done by State Health Minister Sri V.S. Sivakumar at Govt General Hospital, Ernakulam.A newborn hearing screening program initiated by Child Care Centre in 2003 has so far screened 62,000 babies distributed in 34 hospitals in Ernakulam and neighbouring districts of Trichur and Kottayam including two medical colleges and ESI hospitals. 92 babies identified so far with hearing loss are being remediated through hearing aids and auditory verbal therapy. The significance of this program is that most of these babies remediated within the stipulated time may not require expensive cochlear implant surgery costing around Rs 5 lakhs.This ‘kochi model’ of centralized newborn hearing screening (whole district being covered with 4 screening machines) has gained national attention and recognition and is being replicated in other cities in Kerala and India. If every district in Kerala is provided with 4 screening machines, all babies born in our state could be screened as per international guidelines. This cost effective model may be tried out in our state by the concerned authorities.

17 June 2013
2013 is half way thru... moments to cherish @ IAP Kerala
17 June 2013
IAP Kerala Medical Camp at Attappady
Family Get-together at Vythiri
Cheers to the State Treasurer : Dr.Wasim, President, IaP Kozhikode handing over the cheque for Rs.3 lacs to Stae President Dr. S.S. Kamath as contribution from Kerala Pedicon 2012 to the State IaP exchequer.IPP Dr. M.R. Nair & State Secretary Dr. Suresh Kumar happily sharing the moment at the EB Meeting at Trichur on Feb. 17th.
Sate level inauguration of free distribution of hearing aids to needy hearing impaired children at General Hospital Ernakulam in March 2013. Dr.abraham K. Paul addressing the meeting with Chief Guest Shri Sivakumar, Minister for Health, Govt. of Kerala, Shri Dominic Presentation MLa, Dr.Junaid Rahman etc. as keen listeners.
‘Exhausted but satisfied‘. Team from IaP Kozhikode led by Dr. Rajagopal & Dr. Riaz gearing up to leave Attappady after the camp.
True to its motto ‘child welfare for the uncared’, Team IaP Kerala had a medical camp & health education program on 23rd May 2013. Dr.Suresh Kumar E.K., State Secretary paying keen attention to a mother’s woes.
Family Get-together of IaP Kerala EB Members at Vythiri on 25.5.2013. Dr.Raveendra Varma, the neonatologist live with his melodies. The organizing core group of Dr. Sr. Betty, Dr.Sajith, Dr. Madhusoodanan & Dr. Surendran with the program anchor Dr. Shaji Thomas John enjoying it out at the front.
Renowned pediatricians on the dance floor.Dr.Jose O., Dr. Padmanabhan, Dr. Sugathan, Dr. Rakesh, Dr.Ittoop, Dr. Suresh & a genuine ped, Dr. Padmanabhan’s son making it merry!
Dr. Lalitha Kailas receiving the World TB Day award from Minister of Health Shri.V.S. Sivakumar at Tvpm on 23.3.2013 in the presence of Mr. K. Muraleedharan, M.L.A. & other senior officials of Dept. of Health, Govt of Kerala.
Dr.K.N.Prasad, Vice President, IaP Kerala receiving the Dr. E.G. Suresh Memorial award for the Best Doctor (instituted by IMa & Health for all Foundation) from Dr.Thomas Issac, MLa at alappuzha on 19th May 2013.
Congratulations

18 Pediatric Companion
Thymus Gland in Xrays
18 Pediatric Companion
R E F R E S H U R R A D I O L O G Y dr. t.M. Ananda Kesavan editor-in-Chief
IAP Text Book of Pediatric RadiologyFig 1: Normal ThymusF r o n t a l c h e s t radiograph shows t h e t h y m i c w a v e sign (arrowheads), which is created by the impression of the anterior ribs on the normal thymus, and the thymic sail sign which is created by the right lobe of the thymus abutting the minor fissure (Different sail sign also described in pneumomediastinum and elbow radiograph)
Fig 3 : 4 months old child with presenting with noisy respiration. a large thymus mimicking a mediastinal mass (noisy respiration may be due to laryngomalacia)
Fig 7 A,B : 10 year old while screening for pneumonia, suggested to be right sided mass.RaO view for barium swallow, showed it to be a normal thymus gland and there is no pressure effect over the oesophagus
Fig 8 : 6 month old child with Transposition of Great vessels(TGV). Hypoplastic thymus may be seen in TGV and thymic aplasia in DiGeorge syndrome
Fig 5 : Mediastinal mass like appearance
due to thymus obliterating cardiac
silhouette
Fig 2 : Thymus lateral view: Normal position
of the thymus in the anterior,
superior mediastinal compartment with
its undulating lower edge
Fig 4 : Pneumonia like appearance due to rotation : gives an appearance of right upper lobe pneumonia by normal thymus(arrow).
Fig 6 : Superior mediastinal
widening due to normal thymus
Ref: IAP Text Book of Pediatric Radiology; Jaypee Bros,2013

19 June 2013
Neurology series
(Answers on Page 33)
19 June 2013
P E D I A T R I C P H O T O q U I z dr. d. KalpanaAddl. Professor of Pediatric Neurology
Govt. Medical College, Thiruvananthapuram
1. Five year old boy with developmental delay and dystonia. Spot the diagnosis? What is the mode of inheritance
3. What is the abnormality in the cranial USS of a preterm 34 week baby?
5. Spot the diagnosis
2. Describe the abnormality in the MR imaging in a child with dyakinetic cerebral palsy and deafness? What is the most probable etiology?
4. Can you name the neuro cutaneous syndrome from the CT findings? What is the lesion pointed?
6. Examination of hair under polarized light helped in making the diagnosis in a 1 year old child with hypotonia, developmental delay and sparse hypopigmented hair. Please tell the diagnosis and the abnormality in hair

20 Pediatric Companion
S n a p s f r o m t h e b r a n c h e s
20 Pediatric Companion
IAP Pariyaram : Dr. Urmila KE, Dr.Mohammed MTP & Dr. Sudhakaran K, at CME on Enuresis in children on Mar. 31st at
Pariyaram Medical College.
IAP Kollam : Science of Vaccinology Workshop on 3rd Feb. 2013. Faculty Dr. Srinivas Kasi,
Dr. Jagdish Chinnappa , Dr.T.U. Sukumaran & Dr. Remesh Kumar at the inagural function.
IAP Alappuzha : Inauguration of IMNCI Training Program on 22nd Mar. at TD Medical College. Dr. Jose O., Dr. Suma and Dr. Girija Mohan on the dias.
IAP Thrissur : Rally on ashtma awareness month at amala Medical College on 7th May 2013 led by Dr.V.K. Parvathy & Dr.Sunil Menon.
IAP Wynad : Immunisation week celebrations being inaugurated by
Dr. Omana Madhusoodanan, President, Wynad OBG Club on 1st Mar. 2013.
IAP Badagara: Hands on experience of farming methods to school students conducted on 24.02.13 at Maruthomkara Panchayat Hall, near Kuttiady.
IAP Pathanamthitta : South Zone Childhood Disability Detection TOT on 9th June 2013. adv. Sivadasan Nair M.L.a & Shri Pazhakulam Madhu, Jilla Panchayath Health Committee Chairman with Course Director Dr. M.K.C. Nair at inaugural function.
IAP Thrissur : World autism awareness Day celebrations on 2nd April 2013. Scientific session by Dr. Sasidharan, Clinical Psychologist. Dr. Ittoop a.K. & Dr. anandakesavan also on the dais.
IAP Trichur : Dr. ananda Kesavan (Vice President -Elect, IaP Kerala) planting saplings at Govt Medical College campus on World Environment Day on June 5th. about 3000 saplings were planted in the campus on the same day.
IAP Madhyakerala : CME on Obesity & its Management on 16th Dec 2012. Book on Obesity authored by Dr. Sebastian Lukose being released by 2012 State President Dr.
M.R. Nair.
IAP Wynad : Dr. Madhusoodanan inaugurating the NSSK Workshop at Vinayaka Hospital auditorium, Sulthan Bathery on 30th april.
IAP Pathanamthitta : Dr. Rajaram, DMO inaugurating the NSSK Workshop at Pandalam on 17.4.2013. DPM Dr.Vidyadharan, Dr.Carol Cheriyan, Dr. Remesh Kumar & Dr. Naveen Diwakar sharing the dias.

21 June 2013
Virginia ApgarF R O M T H E A R C H I v E S
dr. Mohandas NairAssoc. Professor, Dept. of Pediatrics
IMCH, Medical CollegeKozhikode
for Infantile Paralysis. This foundation, originally the heart child of Franklin D. Roosevelt, was founded in 1938 to fight polio and promote medical research through large nationwide collections under the name of March of Dimes. Since polio was almost eliminated from USa by then, she reoriented the activity towards congenital malformations and low birth weight. These are the priorities of March of Dimes even now. Being a renowned orator, she could attract huge funds for the foundation.
In 1964-65, during the Rubella pandemic, she became the out spoken advocate for universal rubella vaccination, by which she could bring down the incidence of congenital rubella syndrome to a great extend. She also promoted Rh testing to predict hydrops fetalis and neonatal hyperbilirubinemia. In 1973, she was appointed lecturer in medical genetics at the Johns Hopkins School of Public Health.
She got various awards from the academies of anesthesia, pediatrics, genetics and obstetrics. In 1973 she was the first woman to receive the Gold Medal for Distinguished achievement in Medicine from the College of Physicians and Surgeons, Columbia University. In 1994, apgar was pictured on a U.S. postage stamp, as part of the Great americans series.
She had wide scope of interest beyond medicine. She was an eminent lecturer- though at a machine gun like pace. She was invited for speech to various places and she enjoyed travelling. She was an avid stamp collector. Her greatest interest was in music. She built her own stringed instruments, violin, mezzo violin, cello and viola.
She continued to learn various diverse subjects throughout her life but never learned how to cook. In her fifties, she started learning flying lessons.
Throughout her career, apgar maintained, with her characteristic optimism, that “women are liberated from the time they leave the womb,” and that being female had not imposed any limitation in her medical career, but at times expressed her frustration in gender inequalities. She never married. She died of liver disease on august 7, 1974 but was quite active till the end.
When asked why she kept basic resuscitation equipment with her at all times her answer was “Nobody, but nobody, is going to stop breathing on me!”
There is no doubt that every baby born in a modern hospital anywhere in the world is looked at first through the eyes of Dr. Virginia Apgar. She only introduced the simple and rapid way of assessing the well being of a newly born baby, the apgar score. It helped a lot in reducing neonatal mortality and also laid the foundation stone for neonatology.
Virginia apgar, better known among her friends and colleagues as Ginny was born on June 7, 1909 in Westfield, New Jersey. She was graduated in Zoology. Because of the poor financial status of the family she had to do many extra works to support herself, one among them was catching cats for the physiology laboratory. She graduated in Medicine from the Columbia University’s College of Physicians and Surgeons, in 1933 when few women even attended college. She specialized in Surgery, but her professor, Dr. alan Whipple advised her to switch to the new field, Anesthesiology, as he felt that it is difficult for a woman to succeed the male dominated field of Surgery. Till then anesthesiology was a nursing field.
She got board certification in anesthesiology in 1939 and she was appointed as the chief of the division of anesthesiology in a hospital in Columbia, becoming the first woman heading the department. She got attracted to obstetric anesthesia and worked for ten years in this field at the Sloane Hospital for Women. It was at this time, in 1953, she introduced the apgar score. By that time she had attended nearly 20,000 deliveries. She also researched in neonatal acid base balance in HIE and also on the effect of maternal anesthesia on neonate.
During a sabbatical year (1959) she got a master’s degree in Public Health. This along with her experience in neonatology led her to The National Foundation

22 Pediatric Companion
Oral Iron Preparations
dr. t.M. AnandaKesavan dr. A. Anju
Dept. of Pediatrics Govt Medical College, Thrissur
History: Iron lacks the glitter of gold and the sparkle of silver, but it outshines both in terms of its biologic importance. The importance of iron was recognized since time immemorial as exemplified by the use of Lauhabhasma (calcinediron) in ancient Indian medicine. Greek belief considers Mars as the God of strength and iron symbolizes Mars:thus iron was used for improving lethargy, which is common in anemia. The use of iron is mentioned in Greek mythology, in the story of Iphiclus, who was cured of impotence by drinking iron rust dissolved in wine. In 1713 iron was shown to be present in blood. In early 19th century Blaud developed his famous “Blaud’s pill” consisting of ferrous sulfate and potassium carbonate for anemia. all important aspects of iron metabolism have been learned in the past few decades.
Iron Deficiency Anemia (IDA) is a major health problem in India, especially among women and children. The third National FamilyHealth Survey (NFHS-3; 2005–06) found that the prevalence of anemia among under-5 children approached 70 %. In children, IDa can result in different spectrum of illnesses as summarized in (Table I).
table i: Manifestation of iron deficiency anemia
FatigabilityanorexiaReduced attention
spanIrritabilityGrowth retardation
(weight> Height)Behavioral changesDevelopmental delayLearning disability
( w r i t i n g , mathematics)
P o o r S c h o l a s t i c performance
Cognitive impairmentSenso-neural hearing lossRestless leg syndromeFebrile seizureStrokeBreath-holding episodesPseudotumorcerebriCranial nerve palsies
different oral iron preparationsThe preferred route of iron administration is
oral. Indian market is flooded with more than 200 oral iron preparations and similar preparations by the same pharmaceutical company are marketed in more than one brand name. Marked variation in elemental iron content and combination is also common in the drug field.
Preparations of iron salt used are: Ferrous sulfate, Ferrous fumarate, Ferrous gluconate, Ferrous glycine sulfate, Ferrous succinate, Ferrous calcium citrate, Ferrous ammoniate, Ferric ammonium citrate and Ferrousascorbate.The elemental iron content of different preparations are given in table II.
The newer formulations include Iron polysaccharide complex (iron polymaltose), Carbonyl iron, Sodium feredetate,Combination of iron salts &Vit C, succinate, fructose andHaemoglobin preparations(no more advised)
table ii : Percentage and amount of iron in some commonly used oral iron
preparations5
Preparation Iron compound
(mg/tab)
Elemental iron
mg/tab (%)
Fe-ulfate(hydrous) 300 60 (20%) Fe-sulfate(dried) 200 65 (32.5%) Fe-fumarate 200 66 (33%) Fe-gluconate 300 36 (12%) Fe-succinate 100 35 (35%) Fe-bisglycinate 300 60 (20%) Carbonyl iron 100 98 (98%) Na-feredetate 3314%)
Dissociable ferrous salts are inexpensive, have high iron content and are better absorbed than ferric salts, especially in high doses. Gastric irritation and constipation are related to the total quantity of elemental iron administered.
P R A C T I T I O N E R S C O L U M N

23 June 2013
If viewed in terms of iron content, nearly all preparations have the same degree of gastric tolerance, the limits of which are fairly well defined in individual patients
• Ferrous sulfate:The most common iron salt used for oral administration. It is known to produce intestinal side effects (nausea, vomiting, constipation, bloating) in many users. Ferrous fumarate and gluconate have less gastrointestinal side effects and are readily absorbed compared to ferrous sulfate.Ferrous succinate is completely absorbed, but is expensive and has no added advantage over ferrous fumarate and ferrous sulfate. Ferrous calcium citrate has very low iron content, necessitating multiple tablets to be taken to provide adequate elemental iron making it a non-compliant approach.
• Colloidal ferric hydroxide has high elemental iron(52.26%). Iron in colloidal form undergoes ready conversion to soluble form by the action of gastric acid and is easily reduced to ferrous form by mucoproteins present in the secretions of the stomach and small intestine. This might be the mechanism behind its greatest and better absorption with minimal gastric irritation.
• Ironpolymaltosecomplex(IPC)- among ferric iron preparations, iron polymaltose complex has very poor bioavailability. Thus therapeutic efficacy of IPC is questionable and is 4 to 5 times costlier than other iron salts.
• Carbonyliron-Carbonylironis a small particle preparation of highly purified metallic iron. In the process of gastric acid solubilization of carbonyl iron, H+ ions are consumed, there by increasing the pH and as a result the absorption of iron is slow but complete (permitting continued release for 1to3 days) with less side effects. However the rise in Hb level will be a slow response.
• Ferrousbisglycinate-Fe bisglycinate is an amino acid chelate. When ferrous iron reacted with glycine (smallest of all amino acids), it forms a bisglycinate chelate, which is more stable. This higher stability of amino acid chelate prevents the molecule from being destroyed in the gut, produces less GI irritation. Thus absorption of bisglycinate is not reduced in presence of phytates. Ferrous bisglycinate has shown greater efficacy than conventional iron in reducing iron deficiency and iron deficiency anaemiaby short-term treatment using significantly low doses
exhibiting high bioavailability and regulation, but this is an expensive iron preparation.
• Feredetate: Ideal iron for food fortification without any color or taste.Newer iron Preparation and Combinations:
any advantage?= The newer preparations are claimed to be
better absorbed and /or produce less bowel upset, but this is primarily due to lower iron content. all of these newer generation iron products are very expensive.
= There is a wide-spread misunderstanding that the costlier preparations are “more effective,have less side effects”. On the choice of preparation of iron Goodman and Gliman comments-“Variation in the particular ferrous salts have relatively little effect on bioavailability, and the sulphate,fumarate,succinate,gluconate and other ferrous salts are absorbed approximately to the same extent.although a great variety of preparations are being promoted in the present times, their so called advantage over ferrous sulphate or related salts have no foundation in fact.”.a technical advisory board(India)has recommended that B complex vitamins, zinc and calcium should not be included in iron and folic acid containing hematinic preparations.
= Iron polymaltose Complex (IPC) has been marketed and vigorously promoted for its high iron content, absence of metallic taste, good GI tolerability and direct absorption from the intestine. Because the complexreleases little iron in the gut lumen, GI irritation is minimal. The high bio-availabilty observed in rats has not beenfound in humans and reports of its poor efficacy in treating IDa have been well recognized. Preparations of IPCare 4-5 times costlier than iron salts and its therapeutic efficacy is questionable.
= The efficacy of many slow release preparations are also not very good. Slow release preparation disintegrate in the lower intestine and release iron. We know that iron absorption mainly occurs in the first part of small intestine.
= The amount of iron absorbed is biologically limited. There is no benefit by increasing the amount of iron per dose. However, maximum benefit will be obtained when the required iron is divided in to 3 doses. In children 2-3 mg/kg is an ideal dose while small children and infants can tolerate relatively large doses of iron

24 Pediatric Companion
3/4 for example, 5 mg/kg. The dose used is a compromise between the desired therapeutic action and the toxic effects. Prophylaxis and mild nutritional iron deficiency may be managed with modest doses. Further increase in dose will only result in more side effects
Factors that affect the absorption of iron supplements
The amount of iron absorbed decreases as doses get larger. For this reason, it is recommended that most people take their prescribed daily iron supplement in two or three equally spaced doses.
Oral iron supplements must dissolve rapidly in the stomach so that the iron can be absorbed in the duodenum or upper jejunum. Enteric-coated preparations and long-acting supplements may be ineffective, since they do not dissolve in the stomach.
ascorbic acid is an enhancer of iron absorption and can reverse the inhibiting effects of substances such as tea and calcium. ascorbic acid facilitates iron absorption by forming a chelate with ferric iron at acid pH that remains soluble at the alkaline pH of the duodenum. However, the increased uptake is associated with a significant increase in the incidence of side effects; therefore, the addition of ascorbic acid seems to have little advantage over increasing the amount of iron administered.
To minimize side effects, iron supplements are often taken with food. This may decrease iron absorption by as much as 40-66%.
Food and drug interactions may reduce the efficacy of oral iron.Caffeinated beverages (especially tea), calcium containing foods and beverages, calcium supplements, antacids, H-2 receptor blockers and proton pump inhibitors, all will reduce iron absorption.
Ways to Minimize Adverse Effects of oral iron
Q Start with half the recommended dose and gradually increase to the full dose
Q Take iron supplements with food to alleviate gastrointestinal distress
Q Change to a different iron preparation Q Take the supplement in divided doses Q Give liquid preparations using filler to reduce
staining of teeth.Conclusion
Oral iron supplementation is the standard
treatment for patients with iron deficiency. Ferrous salts (sulfate and fumarate) are the treatment of choice given their high effectiveness, acceptable tolerability, and low cost. Preparations with iron III hydroxide polymaltose generally display poorer bioavailability and their clinical efficacy is yet to be established. as far as possible use pure iron preparations with out any combinations. Only preparations for which efficacy and tolerability have been proven should be used in the treatment of iron deficiency.
references: 1) Goodman & Gilman’s the Pharmacological Basis of
Therapeutics - 11th ed. (2006)2) MIMS:Vol 33,Number 3, March 20133) Medical Pharmacology: SK Srivastava,avichal Publish-
ing company, Surat,20124) Mehta BC. Ineffectiveness of iron polymaltose in treat-
ment of iron deficiency anemia. J Assoc Physicians India 2003; 51: 419-421.
5) Choudhury P, Gera T. Rationale of iron dosage and formulations in under three children. available from: URL: http://www.idpas.org/pdf/985Rationale.pdf. accessed January 13, 2011.
iAP CHildHood disABility GroUP 9th National Conference
iMA House, Kochi on 28-29sept. 2013
HiGHliGHts oF CoNFErENCE
symposia
Autism Spectrum Disorders
Cerebral Palsy Speech And Language Disorders
Learing Disabilities
early Intervention Therapy
Workshops
Deveopmental Screening In Office Practice Learing Disabilities
Parent Interraction Sessions Autism Spectrum Disorders
Learing Disabilitis
Please keep the dates free. Details follow.
For details contact
dr. s.s. Kamath : 98470 57766
dr. Abraham Paul : 98460 23388
25 June 2013
J O R N A L S C A N
all infants of lower target groups had reduced rate of Retinopathy of prematurity at the same time this group had increased rate of necrotising enterocolitis.
authors concluded that targeting an oxygen satuaration below 90% with the use of current oximeters in extremely preterm infants was associated with an increased risk of death.3. race mic Adrenaline and inhalation strategies in acute bronchiolitis
Harvard Ove Skjerven,Jon Olav Gjengsto Hunderi et al N Eng J Med 2013;368:2286-2293,June 13 ,2013
Eventhough acute bronchiolitis frequently results in hospitalisation,consensus lacks on inhalation therapy.authors aimed to assess the effectiveness of inhaled recemic adrenaline as compared with inhaled saline and the strategy for frequency of inhalation(on demand vs fixed schedule) in infants hospitalised with acute bronchiolitis.
Study design:a randomised double blind multicenter trial ,the primary outcome being length of hospital stay .any use of oxygen therapy,nasogastric feeding or ventilators support were recorded.
Length of hospital stay, use of oxygen, nasogastric feeding, ventilatory support and relative improvement were similar in both groups.
On demand inhalation ,as compared with fixed schedule inhalation,was associated with a significantly shorter estimated mean length of stay,as well as less use of oxygen,nasogastric feeding and ventilation and fewer inhalation treatments.
The study concludes that 1)recemic adrenaline is not a better choice than inhaled normal saline and 2)on demand inhalation is preferable compared to a fixed schedule.
1. Non steroidal Anti inflammatory drugs are an important cause of Acute Kidney injury in Children
Jason M Misurac,Chad A Knoderer,JeffreyD Leiser et al ,The. Journal of Pediatrics,vol162,issue 6,pages 1153-1159.june 2013
The use of NSaID in children has increased to enormous proportion in day to day practice,This article is a word of caution.
authors have conducted a retrospective study of the records from 1999 to 2010.Medical records were reviewed to confirm the diagnosis of aKI and to quantify NSaID administration.Pediatric RIFLE criteria were used to codify aKI..
This study concludes that NSaID admini-stration is an important cause of acute kidney injury in children.
It occurred after correctly dosed administration of NSaID .
Young children with NSaID associated aKI. may have increased disease severity.2. oxygen saturation and outcomes in preterm infants
The BOOST United Kingdom,Australia and New Zealand collaborative groups
N England J Medicine 2013;368:2094-2104. May 30,2013
The clinically appropriate range of oxygen saturation in preterms is unknown.Previous studies have shown infants had reduced rate of retinopathy of prematurity when lower targets of oxygen satuaration were used.
In three international randomised,controlled trials, evaluated the effects of targeting an oxygen satuaration of 85 to 89 % as compared with a range 91 to 95% on disability free survival at 2 years in infants born before 28 weeks gestation.Half way through the trials oximeter calibration algorithm was revised.Recruitment was stopped early when an interim analysis showed an increased rate of death at 36 weeks in the group with lower oxygen concentration.
a total of 2448 infants were recruited.among 1187 infants whose treatment used the revised oximeter calibration algorithm the rate of death was significantly higher in the lower target group than in the higher target group.
dr. Jayaraman t.P.Thangam Hospital
Palakkad

26 Pediatric Companion
C A S E R E P O R T
as limes, oranges, grapes, mango, gooseberry, tomatoes, potatoes, cabbage, spinach etc. that are rich in vitamin C in the diet.
This case is reported due to the rarity of the case in recent era and its unusual presentation.
Legend
Fig. 1. Profile of the child showing irritability and joint swellings
Fig. 2. Spongy gingival swelling that bled to touch
Fig. 3. X-Ray Knee and long bones showing features of Scurvy
An Unusual Case of Painful Limbs and Oral Cavity Bleed
dr. Elizabeth K.E., dr. Prasanth v.r.Dept of Pediatrics, SAT Hospital
Govt.Medical College Thiruvananthapuram
a 5 ½ year old boy was referred from Orthopedics Department with low grade fever, painful swelling of ankle and knee joints and bleeding from the mouth of 1 week duration. He was very irritable, had joint swellings (Fig. 1) and spongy gingiva that was bleeding to touch (Fig. 2). He was a 900 g preterm low birth weight baby with growth and developmental retardation, who started walking at the age of 5 years. His dietary intake was very poor and had Grade IV malnutrition according to IaP Classification, 3rd degree stunting according to Waterlow Classification and weight for height was 70%. Investigations showed; hemoglobin 7.7 g/dL, total leukocyte count of 11,000/cumm with polymorphs 70% and lymphocyte 30%, platelet count 300,000/cumm, ESR 55 mm/1st Hr, CRP 1.2, aSO titer 800 IU, Rheumatoid factor negative, Mantoux test negative, HIV ELISa negative, synovial fluid sterile, X- Ray Chest and ECG normal and peripheral smear: microcytic hypochromic anemia and no blast cells. He had 1 week of Inj. Crystalline penicillin and anti-inflammatory drugs without any relief.
In view of the clinical presentation and very poor dietary intake, the possibility of scurvy was considered. X- ray knee and long bones showed features suggestive of scurvy; pencil thin cortex with ground glass appearance, Corner sign of Park, Trummerfeld zone of rarefaction, white line of Frankel and Wimberger ring sign around epiphysis (Fig.3). He had no scorbutic rosaries in the chest or subperiosteal bleeds. Vitamin C level was not done due to financial constrains. He was given oral vitamin C 500 mg in 2 divided doses initially till recovery. after 24 hours, bleeding from the spongy gingiva stopped and the lesion healed in 5 days. The joint swellings and pain disappeared in a week’s time and he became asymptomatic and started walking. His appetite also improved and he became cheerful. Vitamin C 100 mg daily was continued for 2 months and mother was instructed to include items such

27 June 2013
C A S E R E P O R T
He was investigated with an MRI Brain (contrast).This showed a heterogenous lesion in the right cerebellar hemisphere measuring 3.5 x 3.1 x 4 cm.Lesion extending laterally to the cerebellopontine angle and compressing the fourth ventricle.along with mild dilatation of lateral and third ventricles suggestive of obstructive hydrocephalus.
Conclusion-astrocytoma.The patient was advised surgery and
chemotherapy.discussion
Torticollis in childhood may be a sign of many disorders. Five cases, with torticollis as the initial sign of a posterior fossa tumor, are presented (3).
astrocytomas account for approximately 40% of CNS tumors.Juvenile pilocytic astrocytoma (JPa)is the most common(20%).The classic site of presentation is the cerebellum.Based on their clinicopathologic characteristics ,they are grouped as low-grade astrocytomas,malignant astrocytomas, and glioblastoma multiforme.JPa is a low-grade astrocytomas.Surgery is the primary treatment as well as radiation and chemotherapy.Complete surgical resection the overall survival approaches 80-100 %.
In newborns or infants with congenital torticollis, ultrasonography (US) is the modality of choice. In nontraumatic acquired torticollis, computed tomography (CT) of the neck or cervical spine is the initial imaging study. If CT findings are negative, magnetic resonance (MR) imaging of the brain and cervical spine should be performed(4).1. UijaIPoddar. SurjitSingh. Lata Kumar Paroxysmal
Torticollis of Infancy .Indian Pediatrics 1999; 36:86-882. HermanMJ:Torticollis in infants and children: common
and unusual cause.Instr Course Lect. 2006;55:647-533. K.Gupta. D R Roy . E S Conhan .a H Crawford .Torticol-
lis secondary to posterior fossa tumors. J PediatrOrthop. 1996 Jul-aug;16(4):505-73.
4. Imaging of torticollis in children.Haque S, Bilal Shafi BB, Kaleem M. Radiographics.2012 Mar-apr;32(2):557-71.
Paroxysmal Torticollis – A masquerader
dr. insy MBBS (DNB Trainee) dr. Cherian Joseph MD, DCH
dr. silvan Mathews George MD, DCH Senior Consultants
Little Flower Hospital, Angamaly
Abstract : Paroxysmal torticollis is a self-limiting condition which presents in infancy and generally resolves spontaneously by two to three years of age (I). The differential diagnosis includes trauma (clavicle fracture or brachial plexopathy), tumors or malformations of the central nervous system, ocular disorders, congenital bony abnormalities (Klippel-Feil syndrome), inflammatory conditions, and other diagnoses such as atlantoaxial rotatory displacement or Sandifer syndrome resulting from gastroesophageal reflux(2). The authors report a similar case of paroxysmal torticollis in a 18 month old boy associated with unilateral lower motor neuron facial palsy, which turned out to be a space occupying lesion.
Case reportan 18-month-old boy presented with history
of head tilting to the left side since 4 months and inability to close right eye since 1 week.He was the only child to his parents born after 13 years of marriage.Mother had history of gestational diabetes mellitus and pregnancy induced hypertension.Baby was a preterm gestation and weighed 2.3 kg at birth.There was history of being admitted 3 months back for 5 days in another hospital for fever and vomiting .No other history of pallor, seizures, trauma and drug intake. His development was normal. On examination he weighed 8.5 kg; other anthropometric measurements were within normal limits. He was keeping his head tilted to left and did- not cry on manipulation.There was lower motor neuron facial palsy on the left, characterised by deviation of angle of mouth to right, loss of nasolabial fold on left and inability to close left eye tightly. There was no other abnormalities on systemic examination. There was no family history of similar illness or of migraine or paroxysmal vertigo.
MRI showing obstructive MRI showing Hydrocepalus midline shift

28 Pediatric Companion
eye for which artificial tears were started. Dermatologist advised appropriate skin protection with emollients. The child improved steadily with the supportive care and had no further episodes of fever.
disCUssioNHypohidrotic ED is a heterogeneous group
of inherited disorders characterized by defect in the development of two or more structures of ectodermal origin. Major structures involved are hair follicles, nail, teeth, sweat glands, sebaceous glands, conjunctiva and or lens. Three of the well defined types include – Hypohidrotic ED, Hidrotic ED, Ectodactyly cleft lip cleft palate syndrome. Hypohidrotic ED is inherited as XLR. Incidence of 1:100000 males. It manifests in the first year of life. Triad includes – complete or partial absence of sweat glands, anomalous dentition and hypotrichosis. There may be severe peeling or scaling of skin. Skin may be pale dry with a prominent venous pattern over most of the body. Hyper pigmentation and wrinkling may be present in the periorbital area.
Children are unable to sweat and hyperpyrexia may occur. Other features include frontal bossing, depression of midface, flattened nasal bridge, malar hypoplasia, low set ears with thick protruding lips and prominent chin associated hypodentia. Other associations include atrophic rhinitis, diminished lacrimation, atopic dermatitis , decrease in T cell function with absent or hypo plastic mammary glands, cataract and corneal opacity.
The only management which can be offered to such children are a supportive care in terms of prevention of hyperpyrexia, treatment of defective lacrimation and regular dental evaluation.
A Case of Hypohidrotic Ectodermal Dysplasia
dr. Uma Mohandas dr. Nabil F., dr. Jose o.
dr. Girija Mohan GTDMCH Alappuzha
Hypohidrotic Ectodermal Dysplasia- Hypohidrotic ED (Christ-Siemens-Touraine syndrome), is a heterogeneous group of inherited disorders characterized by defect in the development of two or more structures of ectodermal origin They are about 200 in Case
number of which Hypohidrotic ED is commonly seen. It is commonly inherited as X-linked Recessive disorder. It is one amongst the several causes of fever in newborns.
CAsE rEPort a term LSCS, 3.25 kg male baby born of Non
consanguineous marriage with an uneventful antenatal history other than a history of leaking PV of 14 hours and maternal pyrexia at the time of delivery. Baby presented with fever since PND-1. On examination, the baby had a peculiar facial appearance with sparse and thin scalp hair, eye lashes and eye brows, periorbital wrinkling and generalized peeling was present. He had a depressed nasal bridge with thick everted lips and prominent chin and absent breast nodule.
Baby was investigated for routine causes of fever. His sepsis screen was negative, CSF study normal and triple cultures later came as negative. There was no evidence of any cranial malformation/ hemorrhages or evidence of dehydration. On account of the persistent fever and peculiar facial appearance – Palmar skin biopsy was done, which revealed hypo plastic eccrine glands which is the histopathological evidence of Hypohidrotic ED. Baby’s mother also had certain facial features like thick everted lips and sparse hair.antibiotics were given till cultures came as negative and then he was treated conservatively. Ophthalmological evaluation revealed the presence of dry
C A S E R E P O R T

29 June 2013
S h a r i n g U r C l i n i c a l E x p e r i e n c e sBreastfeeding and Maternal Fluid Intake
dr. Newton luiz Senior Consultant Paediatrician
Dhanya Mission Hospital, Chalakudy
It’s a common scenario. The infant is brought for immunization at 1½ months of age, and his mother complains that since 15 days now he is only passing stools every alternate day. “So you reduced your fluid intake 15 days back?” you ask cheerfully, and she grins with surprise and sudden comprehension. She was unaware that decreased maternal fluid intake can lead to thickened breast milk with reduced fluid content resulting in dry infrequent stools. “But he passes plenty of urine”, she claims. Urine output is not decreased significantly in dehydrated infants, except in severe cases.
“He cries a lot these days, Doctor, especially at night, sometimes for 2-3 hours non-stop till he falls asleep from sheer exhaustion”. Infantile colic in our society is most commonly caused by decreased stooling due to decreased maternal fluid intake. In the West, where mothers are routinely advised to increase their fluid intake after delivery – and where exclusive breast feeding is rare anyway – it is not a significant cause. Perhaps 2/3 of babies in our state will respond dramatically to an increased fluid intake by their mothers; the rest need Dicyclomine drops and parental reassurance.
“He is very thirsty Doctor, feeds all the time, day and night, he is never satisfied, he leaves me exhausted”. Well, what should she expect? She takes less fluids, her baby gets less fluids, he is thirsty all the time, so he feeds all the time. The baby who takes multiple but brief feeds gets more fluid as the earliest breast milk at every feed is high in water content (and low in calories and fat: fat content increases dramatically after the first two minutes of feeding). Breast milk has an average caloric content of 67 calories per 100 ml, but hind milk has 10 times more calories than fore milk – 100 calories v/s 10 calories. Initially his persistent feeding may gain him adequate calories, but as his hunger increases his weight gain too will slow down.
“He’s not taking much feeds since one month; he prefers to sleep all the time”. Poor fellow, he is so frustrated from not getting enough milk, or getting thick milk when he is more thirsty than hungry, that he has stopped trying. Don’t blame him if he is not gaining weight properly.
“Poor weight gain”. Breast fed babies gain weight astonishingly fast in the first four months, 3.5 – 4 kg, much faster than bottle-fed babies. (In the second half of infancy bottle-fed babies overtake them, as breast milk production slows). This is especially true of babies that are thin at birth; they show amazing catch-up for the first 2 months. A sudden slowing of weight gain any time in the first few months is usually a sign of sudden reduction in maternal fluid intake. It can also occur because the mother’s capacity for milk production is on the lower side, but this is uncommon.
“He strains and cries before passing urine.” This is an uncommon manifestation of decreased maternal fluid intake. Usually they only strain and cry before passing stools.
“His breathing has become very noisy recently, I think he has nose block” – but nasal examination of the neonate shows dry and clear nostrils. There is
often a clear relationship to the date of reducing fluid intake (usually Day 28 in Thrissur district), and a good response to increasing maternal fluid intake and using Saline nasal drops for the neonate.
So how much fluid does a lactating mother need, anyway?
Nelson tells us (19th edition, 2011. Table 41-7) that the fluid requirement of a woman is 2.7 litres/day in a non-pregnant woman and 3.8 litres/day after delivery. As invisible fluid intake (fluid present in rice, fruits, vegetables etc) is estimated at 1 litre/day, the actual requirement is about 1.7 litres in an average woman, and 2.8 litres after delivery. (In the Western diet food is expected to provide only 20% of fluid requirement, or 500 ml, but rice is an excellent source of water).
Lesser quantities result in dehydration, manifesting in the mother as excessive tiredness, giddiness while walking, eye pain while reading or even watching TV, all of which she is told are normal in the postpartum period. This is why traditionally women are encouraged to keep to the bed for two months after delivery, and are not permitted to read or to watch TV.
Greater quantity of fluids than needed does not increase breast milk quantity (as was wrongly taught to us by Western textbooks 30 years ago) but only increases maternal urine output day and night, something she finds very annoying. Why such large quantities, one may ask. Well, for the first two months she has increased BMR as her body struggles to return to normalcy. But a greater reason is that she has to take fluids for her baby: if he needs 750 ml of breast milk, his mother will have to ingest an extra 750 ml of fluid. This excessive fluid requirement will persist so long as she is breastfeeding him; BM production slows down after 6 months but continues to be significant even at 1½ - 2 years.
But why are mothers so reluctant to take fluids if they are thirsty? Because while Western beliefs traditionally promoted excessive fluid intake after delivery (4-5 litres/day of water, light tea, and even light beer and ale!), ayurvedic beliefs are exactly the opposite. Fluids should be restricted as severely as possible, preferably 3 – 5 glasses of water per day, and the rice should be deliberately overcooked to further reduce fluid intake. This is because “vellum kudichaal vayaru chaadum” – as though the vayaru is not already chaadi irrikkunnu and can further chaadu. also, “vellum kudichaal vayaru pazhakkum” because the water goes into the abdomen, and a baby has just come out of the abdomen, creating a raw wound in the vayaru, and everyone knows you should not wet a raw wound. Finally, it is not good to drink fluids while taking ayurvedic ‘prasava raksha’, which is often started on Day 28 ( though the date varies from district to district).

30 Pediatric Companion
Vancomycin and teicoplanin are the glycopeptides of clinical use in pediatrics. They are active against an extremely broad range of gram positive organisms but it affords no gram negative cover. They are used to treat staphylococci, including MRSa, coagulase negative staphylococci, streptococci, enterococci and clostridia. Glycopeptide resistant coagulase negative staphylococci (especially teicoplanin resistant) and enterococci are becoming important pathogens in hospital acquired infections. MRSa with reduced susceptibility are also being reported.
Vancomycin should be reserved for the treatment of multi-antibiotic resistant staphylococci and coagulase negative staphylococcal septicaemia, and as prophylaxis against endocarditis). Oral vancomycin is the second line agent for treating pseudomembranous colitis. Metronidazole is, however, as effective for treating pseudomembranous colitis. It is cheaper and does not risk promoting emergence of glycopeptide resistant enterococci. Vancomycin or teicoplanin have become important agents used in combination with other antibiotics when initiating therapy for infections caused by various access devices (eg, central venous catheters, ventriculoperitoneal shunts) because of its activity against coagulase-negative staphylococci. It is also used in bacterial meningitis because of its activity against penicillin-nonsusceptible S pneumoniae, and in selected episodes of febrile neutropenia because of the possibility of resistant viridans streptococci.
vancomycin in comparison to teicoplaninA meta-analysis of trials comparing the efficacy
and safety of teicoplanin and vancomycin suggested
Glycopeptides in pediatric practice
dr. Jeeson C. Unnieditor-in-chief, IAP Drug Formulary
Dr. Kunhalu’s Nursing Home Cochin
that teicoplanin is as effective as vancomycin for treating MRSa infections. Side effects were less in the teicoplanin-treated group. Systematic reviews have shown that teicoplanin is not inferior to vancomycin with regard to efficacy for the treatment of suspected or proven infections and is associated with a lower adverse event rate than vancomycin.
Study of the distribution of teicoplanin and vancomycin resistant strains among coagulase negative staphylococci (CONS) have shown that teicoplanin is less effective than vancomycin against CONS and most resistant strains of S. hemolyticus. However a recent study found teicoplanin was more effective against CONS.
Teicoplanin is very effective in preventing experimental streptococcal, enterococcal, and staphylococcal endocarditis and may be an attractive alternative antibiotic in patients allergic to beta-lactams, especially in the outpatient setting.
Teicoplanin appears to be the best choice for treatment of Clostridium difficile-associated diarrhea because the available evidence suggests that it is better than vancomycin for bacteriologic cure and has borderline superior effectiveness in terms of symptomatic cure.
K N O W U R D R U GFrom IAP Drug Formulary
The IAPDF Mobile apps are currently available on iOS, Android and Symbian, and will be launched on Blackberry shortly. The Apps are free to download and available in the App store on both iOS and Android. The Symbian app can be downloaded and installed from www.iapdrugformulary.com/app/iapdf_symbian_ver3_29_2.wgz.On first launch after apps are installed, user will have to register with an App key. Purchase the App Key online at www.iapdrugformulary.com - Rs. 300 ? IAP Member; Rs. 500 ? Non IAP Member. App Key will be sent by email. An App key may be
used for only 1 device. For use on multiple devices contact us at our site.Internet data connection (2G / 3G / WiFi) has to be active during the initial registration and subsequent usage of the app for most android and all symbian mobiles. All IAP DF data gets installed on iOS; hence no internet connection required for iOS.The App key installation is just a one time process, the next time you open the app, it will straightaway direct you to the home page where you can click on the Search tab and go ahead with your Search.
IAP Drug Formulary Mobile Apps

31 June 2013
Medical cum Health Education Camp at Attappady
IaP Calicut Branch in association with Kerala State IaP, NRHM & Dept of Pediatrics, Medical College, Kozhikode conducted a medical camp for tribal children of attappady & a health education program for tribal mothers & health care personnels in Attappady area on 23.5.2013. Prof. K.C. Rajagpolan, Dr. Riyaz a., Dr. Sureshkumar E.K. and a team of doctors from Calicut Medical College (Dr.Geeta M.G., Dr. Krishnakumar, Dr. Krishnan C., Dr. Shareth, Dr. Gayathri, Dr. Vivek, Dr. Jestlin) participated.There were 281 tribal children who attended the camp. Free drugs and food were distributed. Feeding pattern, nutritional status, immunization status of tribal children were studied in the camp. also stool microscopy and Hb were done to study the nutritional anemia and soil transmitted Helminthiasis in tribal children. Health education: Dr. K.C. Rajagopalan took a class on nutrition, Dr. a. Riyaz conducted a class on Hepatitis,Dr. Sureshkumar took class on Immunization and Dr. Krishnakumar spoke on behavioral problems for the JPHNs, JHIs, anganwadi workers and a large no. of tribal mothers. Team also visited the tribal colonies (ooru) . Camp started at 9.30 am and concluded at 4.30 pm.
PAriyArAMOn Feb 7th , CME was conducted. Dr Sudhakaran
delivered a lecture on childhood tuberculosis and RNTCP. Immunization week was observed from March 1-7, Dr Mohammed MTP, took awareness classes for the parents. Dr Ranjith spoke on Measles, on world measles day.
Mar. 12-14th - IMNCI training program was conducted. There were about 20 participants. President Dr Sudhakaran, and Dr, Mohammed MTP, Dr. Kavitha Pavithran, Dr. Urmila KV were the faculty.
World Down Syndrome Day observed on Mar 21st. Dr aiswarya delivered a lecture. a CME was conducted on March 31st. Prof. Dr. Urmila KE presented a talk on Enuresis in Children. april 2nd was observed as World Autism Awareness Day. Child Psychiatrist Dr. Arun Kumar talked on the subject. Dr. Druhin, Prof. of Psychiatry felicitated. President Dr Sudhakaran chaired.
vAdAKArAas part of promoting basic knowledge, awareness
and skills, on various extra curricular fields for school children, a class on the basics of agriculture and hands on experience of farming methods to school students was conducted by IaP Vadakara on 24.02.2013 at Maruthomkara Panchayat Hall, near Kuttiady. The meeting was presided over by Dr. Sachith, President IaP Vadakara. The meeting was inaugurated by the Maruthomkara Panchayat President, Mr. Sajith. He spoke on the importance of creating interest in agriculture in the younger generations. Felicitated by Dr. Saleem P.M., Secretary, IaP Vadakara, adv. Jamal, and Mr. Noushad, Agricultural Officer. A class
introducing the various farming methods was given by Mr. Noushad, after which the children were taken to the fields for the live demonstration of farming methods and equipments. The different methods of tilling the soil, cultivation, seasonal farming, maintanence of crops, spraying methods etc. were demonstrated and explained by the local farmers and the agricultural officer. There were about 60 students including girls, actively participated in the proceedings and also tried their hands in using the different types of tilling and spraying machines.They were also taught to climb coconut trees using machine.all the students who attended, appreciated the classes and agreed that it was an experience of a different kind and expressed their desire for more such classes. The programme ended with tea and refreshments for all.
KozHiKodEIaP Kozhikode Branch in association with NRHM
conducted a NSSK program for nurses on 4th & 5th March, 2013 in Jubilee Hall, IMCH, Calicut. There were 46 participants. Dr. M.P. Jayakrishnan was the lead instructor, Dr. Babu Francis, Dr. Girish S., Dr. Gireeshan V.K. & Dr. Mohandas K. & Dr. Kasim Rezvi were the other faculty members. DMO Dr. Mohanan K.P. inaugurated the program. Dr. a. Baburaj, NRHM District Program Manager, Dr. A.V Gopalan, Prof. of Pediatrics, Medical College, Calicut, Dr. E.K. Suresh Kumar, State IaP Secretary, felicitated the occasion. Dr. Wasim K., President, IaP Kozhikode & Dr. Krishnan C., Secretary IaP Kozhikode also participated in the function. Dr. Mohandas K. was the District Co-ordinator.
WyNAd CME on Communication Skills in Pediatric
Healthcare by Dr. Manoj Narayanan, Asst. Professor of Paediatrics, DM WIMS, Meppadi on 27th Feb 2013 at S.Bathery. Syposium on Autism by Dr. Krishnakumar,Director,IMHaNS, Calicut on 1st april 2013 at Kalpetta.CME on Hypothyroidism by Dr.Vijayakumar, Asso. Prof. of Paediatrics, MCH, Calicut on 5th april 2013 at Chundale.CME on Asthma by Dr. Praveen, Pulmonologist, BMH, Calicut on 7th May 2013 at Kalpetta.
Days and week celebrations: World Cancer Day was celebrated at Cosmopolitan Club, Kalpetta by Dr. Betty Jose on 4th Feb 2013 : Immunization Week Celebration : Inaugural function was conducted on 1st March 2013 at Vinayaka Nursing College, S.Bathery. The programme was inaugurated by Dr. Omana Madhusudanan, President Obg Club Wayanad and Class on Immunisation was taken by Dr.Madhusudanan for nursing college students.
On 2nd March 2013, class on immunisation at assumption Hospital, S.Bathery by Dr.Betty Jose.On 3rd March 2013, class on immunisation at Fatima Mata Mission Hospital, Kalpetta by Dr.Betty Jose.On 4th March 2013, Rubella Vaccination Camp for around 100 girls was conducted at Vinayaka Hospital, S.Bathery. Measles Day was celebrated at Taluq
b R A N C H A C T I v I T I E S
32 Pediatric Companion
b R A N C H A C T I v I T I E SHospital, S. Bathery on 7th March 2013 by Dr. Suraaj and Dr.Yashwanth Kumar.On 7th March 2013, awareness programme on immunisation was conducted at District Hospital, Mananthavady by Dr P. Narayanan Nair, Dr Jyothi Ignatious and Dr.Chandrashekaran.On 14th March 2013 World Kidney Day - Radio talk on UTI by Dr Betty Jose. On 15th March 2013 (World Disability Day) entertainment programmes for childrens at Govt Childrens Home, Kaniyambetta by Dr Betty Jose.On 21st March 2013(World Downs Syndrome Day) radiotalk on Downs Syndrome by Dr Betty Jose. On 24th March 2013(World TB Day) awareness programme were conducted at District Hospital,Mananthavady and Taluq Hospital, S.Bathery On 24th March 2013,Dr Betty Jose gave radiotalk on Tuberculosis. On 2nd april 2013 (World Autism Day), Dr Betty Jose gave radiotalk on Autism.World Health Day was celebrated at Chundale on 7th april 2013. The programme was inaugurated by Dr Bhaskaran, Past National Vice President and Dr Madhusudanan presented powerpoint discussion on various aspects of Hypertension. On 7th May 2013(Asthma Day) Dr Betty Jose gave a radiotalk on Asthma. 12th May 2013, Asthma Awareness Camp was organised by Dr Betty Jose at Tharapuzha. Radio programs on Asthma are telecasted weekly this month, with Dr. Betty Jose as speaker.On 31st May 2013(No Tobacco Day) radiotalk by DR Betty Jose. Workshops: 5 IYCN workshops & 5 NSSK workshops were conducted by the branch. IaP Wayanad Branch hosted this year’s Family Meet of IAP Kerala State at Vythiri Village, Vythiri on 25-26 May 2013. IaP Wayanad Branch presented mementos to all the family members who attended the meet
triCHUrIYCN Training programme for nurses at Hotel
Elite International on 28,29,30 Jan. 2013 at Thrissur.KERALA NEoCoN 2013 - 16,17 Feb. 2013, 19th
State Conference of NNF at Hotel Joys Palace, Thrissur. Over 400 delegates participated in the conference.
IMNCI ToT was conducted on 6.3.2013, at GMC Thrissur. 30 doctors took training.
Immunization Week observation (March)Dr. anandakesavan organised at GMC Thrissur
on 6-3-13 and at Wadakkanchery on 7-3-13.At Amala Medical College,Thrissur on 1.3.2013 -
talk by Dr.V.K. Parvathy on vaccines in the paediatric ward. Dr. Sunil Menon spoke on newer vaccines. Dr. anette spoke on measles on Measles Day - 7.3.2013.
World Downs Syndrome Day observed on 21.3.2013 at Sahithya academyHasll, Thrissur, organized by Dept of Paediatrics, GMC, Thrissur and IaP Thrissur Branch.
World Tuberculosis Day : a study class was conducted at anganwadi, Nadathara Panchayath on 24th March 2013 by Dr. anandakesavan and Dr. Ittoop.
IAP World Autism Awareness Day was celebrated at ‘Sloka’, a centre for mentally challenged children at Poonkunnam,Thrissur.
World Health Day was celebrated on april 7th, 2013 at Pallotine Youth Center, Ollukkara, Thrissur. 30 young boys and girls attended. Dr. Betty and Dr. anandakesavan took classes. Dr. V.K. Parvathy and Dr. Sunil Menon took classes at amala Medical College.
Medical Camp for disabled children and parents at anganwadi on 21.3.2013 at Viyyur, Near Thrissur.
Medical Camp at 2 Tribal Colonies on 25.4.2013. Dr. Ittoop and Dr. Sunil Menon organised the medical camps at Thirumani Tribal colony, anganwadi No.99, Thrissur; Kalapara Tribal Colony, anganwadi No.167, Thrissur.
CME on Endocrinology on 28.4.2013 by IaP Thrissur Branch. Dr. Prof. Muraleedharan, Seniormost Endocrinologist of the State and Prof of Endocrinology, aIMS, Kochi inaugurated the CME.
World Asthma Day - 7.5.2013 at amala Institute of Medical Sciences,Thrissur, on 7.5.2013 organized a rally on asthma awareness month and thereby educating the public using various cutouts on asthma and distributed these pamphlets in taxi stands, autorickshaw stands, houses and on the roads motivated by Dr.Sunil Menon (Secretary IaP Thrissur Branch)
Adolescence Programme for Boys and Girls of Don Bosco HS School at Mannuthy On 14.5.2013, classes by Dr. Newton, Dr. Ittoop and Dr. Prabitha.
World No Tobacco observation Day on 31.5.2013 at Public Library, Nallankara ward of Thrissur Corporation. Dr anandakesavan and Dr. Ittoop took classes.
Praveshanolsavam-2013 on 3rd June at Nallankara LP School and on 4th June at Kalathode LP School. Free bag, books, pencils etc were distributed to the children by IaP Thrissur Branch under Dr. Ittoop.
World Environment Day observed on 5.6.2013 at Govt Medical College, Thrissur. about 3000 saplings were planted in the campus. Staff members from all the depts. participated. Dr. anandakesavan (asso. Professor, Vice President IaP) motivated the staff in planting saplings at Govt Medical College Campus .
Total of 7 NSSK training programmes conducted till date.
AlAPPUzHAapart from last years programs, IaP alappuzha
could successfully organize three more IYCN programs in the months of February and March this year. March 7th - the `Measles day` was celebrated by the branch. Dr. anil Vincent took an awareness class on this day for the health workers and public at Taluk Hospital, Thuravoor. A Pediatric CME program was organized by Dept. of Pediatrics and IaP alappuzha Branch on the occasion of Golden Jubilee Year Celebrations of Govt TD Medical College, alappuzha on 10th March 2013 at Vandanam. The program was inaugurated by the Superintentdent of TDMCH, Dr. Suma T.K. HOD Pediatrics, Dr. Girija Mohan welcomed the gathering Dr. Jose O., President, IaP alappuzha Branch presided

33 June 2013
and Dr. anil Vincent, Secreatry has felicitated the meeting. `World Asthma day` was observed at TD MCH alappuzha on 7th May 2013. District President, Dr. Jose delivered a talk, ’asthma how to control`‚ and BSc Nursing students has conducted a skit on asthma for public. about 100 people attended the meeting.
IMNCI training programme was organized by IaP alappuzha Branch for the Medical Officers of Ernakulam and alappuzha district on 22,23 & 24th March 2013, at Govt. TD Medical College, alappuzha.The State IMNCI Programme Coordinator and IaP Branch President, Dr. Jose, presided and Dr. Suma T K, Supt. of TDMCH has inagurated the meeting. another remarkable event was the `Grand Gala Family Getogether ` organized by the branch on the occasion of the Golden Jubilee Celebrations of IaP, on 28th april, at Vasundhara Sarovar Premiere Resorts, at Vayalar. a Golden Jubilee Mementos were presented to all families. Colourful programs and games were arranged. It was a grand function which rendered everlasting memories. The branch has completed 6 NSSK programmes till now. Two were for the Doctors. More programmes are scheduled.
KollAM On 3rd February, Science of Vaccinology was
conducted at the Quilon Beach Hotel. Dr. Kasi, Dr. Jagadish Chinnappa, both from Banglore, Dr. T.U.Sukumaran and Dr. Remesh Kumar, conducted classes. On 14 Feb, thefirstCMEcumGBMof IaP Kollam was held at Bishop Jerome Hall. Dr. Lalitha Kailas, HOD, SaT Hospital,Trivandrum spoke about ‘Not to be missed cases‘. Both programs were well attended.
PAtHANAMtHittA March: InstallationofOfficebearerson 10.3.2013
by State President Dr S.S. Kamath. Immunisation week & measles day celebrations - Classes for mothers. Talk by NPSP SMO Dr. asha Raghavan. Medical Camp.Talk on Radio Macfast 90.4 on immunsation on 23.3.2013. Down Syndrome Day : CME on Down Syndrome. Health checkup for children with Down Syndrome.World Tuberculosis Day : Intergrated Teaching for UG Students on 22-03-2013.
April : World Autism Awareness Day - conducted medical Camp in special school in Kaviyoor for mentally challenged children. Conducted classes for mothers at the school on autism. Created public awareness about the myths and facts of autism through the malayalam medical publication (Pushpavani) . Interactive phone in program about autism through the community radio 90.4. World Health Day - conducted a week long health checkup in Pushpagiri Medical College where the children were examined by senior doctors, giving importance to the detection of hypertension. all children especially adolescents who were detected to have high BP were evaluated further. Conducted medical camp at Nooranad. NSSK workshop was conducted at NSS Hospital Pandalam on 17,18 april under the leadership of Dr. Remesh Kumar. The DMO and the DPM of Pathamanthita were present at the inaugural ceremony. Dr. Jacob abraham Neonatologist of Pushpagiri lead the classes.
May : World Asthma Day - CME on bronchial asthma in association with the Dept. of Chest Medicine Pushpagiri Institute of Medcial Sciences. Health Camp for children with Bronchial asthma , health education for mothers with emphasis on bronchial asthma.
b R A N C H A C T I v I T I E S
1. Lesch Nyhan syndrome. Note the characteristic self mutilation of the lips. Lesch Nyhan syndrome is an X linked recessive disorder characterized by HGPRTase. Male children present with develop-mental delay, extrapyramidal movements and self mutilation. The serum uric acid level will be very high. Other differential diagnoses for self mutilation include neuro acanthocytosis and hereditary sensory autonomic neuropathy.
2. The T2 weighted MR image shows symmetrical hyperintensity of bilateral globus pallidus. The MR finding is characteristic of kernicterus. Neonatal hyperbilirubinemia.
3. The cranial USS shows evidence of intraventricular hemorrhage with parenchymal extension. according to Papile grading system it is Grade IV . Cranial USS is a very useful modality in the identification and follow up of intraventricular hemorrhage in preterm babies.
4. Tuberous sclerosis. The CT scan shows the calcifi-cations jutting into the ventricle. In addition there is hydrocephalus also. The lesion pointed is a sub-ependymal giant cell astrocytoma which produces hydrocephalus by blocking the Foramen of Monroe.
5. Joubert syndrome. The characteristic molar tooth sign can be easily appreciated. Joubert syndrome is associated with hypoplasia of vermis of cerebellum. The molar tooth sign is produced by the deep inter-peduncular fossa, thick and short superior cerebellar peduncles and hypoplasia of vermis. The babies with Joubert syndrome present with episodic hyperpnea and tongue thrusting movements.
6. The hair shows “Tiger tailed” appearance which is characteristic in Trichothiodystrophy. The children presents with developmental delay, failure to thrive, sparse hypo pigmented or de pigmented hair with or without photosensitivity. The hair is brittle and is deficient in cysteine.
P H O TO Q U I Z A N S W E R S (Page 19)

34 Pediatric Companion
lasts 4 to 6 days and is often precipitated by vaccination, minor trauma, or stress. It is usually associated with abdominal pain, vomiting, diarrhea and cervical lymphadenopathy. Other common symptoms include hepatosplenomegaly, headache, arthralgia and rashes. Occasionally, patients present with aphthous ulcers. after the attack, the patients are free of symptoms, although skin and joint symptoms resolve only slowly. Few of the adult patients also develop neurological abnormalities of varying degree, such as mental retardation, ataxia, ocular symptoms and epilepsy, reflecting the existence of a continuous spectrum between MVa and HIDS.
Mevalonic ac iduria - MVa shows considerable clinical heterogeneity. Severely affected patients present from birth with congenital malformations such as microcephaly, dolichocephaly and wide irregular fontanels, as well as low set and posteriorly rotated ears, downslanted palpebral fissures, blue sclerae, and central cataracts. Cholestatic liver disease may be present, and patients may die from recurrent septicemia. Children with MVa who are severely affected with multiple problems may live only into early childhood; mildly affected individuals may have a normal life expectancy.
Important manifestations from late infancy include mild to severe psychomotor retardation, recurrent crises (fever, vomiting and diarrhea), failure to thrive, hypotonia and myopathy. Sometimes hematological abnormalities predominate with normocytic hypoplastic anemia, leukocytosis, thrombocytopenia and abnormal blood cell forms.
after preschool age, short stature, ataxia due to a progressive cerebellar atrophy and ocular involvement with uveitis, and cataracts become predominant findings, and can be the major manifestations in milder cases. Most patients
Life with Fever
dr. sajikumar J.Parabrahma Specialty Hospital
Oachira
It is quite usual for a bride to be in tears on the day of her wedding. But for Julianne* there was a strange reason to cry. “I was so happy that my one wish had come true. That day I did not have a fever. I was able to enjoy the festivity.”
The fact that Julianne had a normal temperature on that day may seem insignificant, but not for her. She suffers from a very rare disease called the Hyper-IgD syndrome. It is characterized by periodic fever attacks. Julianne: “On average I’m about 10 days free of fever, and then I get a fever attack which lasts some 5 days”. On a good number of days she will be in bed, crippled by pain and by a fever of 40 degrees Celsius. The constant disappointments make the disorder mentally exhausting too.
Hyper igd syndrome & Mevalonic aciduriaHyperimmunoglobulinaemia D with periodic
fever (Hyper-IgD syndrome) is a rare inherited autoinflammatory syndrome that presents with recurrent episodes of fever, skin rash, abdominal pain, headaches and enlarged lymph glands that begin in infancy. It is now recognized that HyperIgD syndrome represents one end of a clinical spectrum of disease caused by deficiency of Mevalonate kinase (MVK), the first committed enzyme of cholesterol biosynthesis. Mevalonic aciduria (MVa) is a severe often fatal variant of HIDS. Children who have approximately 1 to 20 percent of normal mevalonate kinase activity typically develop HIDS and those who have less than 1 percent of enzyme activity usually develop MVa.
Genetics and Molecular biologyMevalonate kinase deficiency is an autosomal
recessively inherited disorder. The MVK gene is located on chromosome 12 (12q24) and produces the enzyme mevalonate kinase. Mutations in the MVK gene and reduced activity of MVK have been identified as underlying cause of both MVA and HIDS syndrome.
Clinical PictureHyper-IgD syndrome - In HIDS, the clinical
picture is dominated by recurrent febrile attacks that usually start late in the infancy. The fever

35 June 2013
suffer from frequent crises characterized by fever, vomiting and diarrhea. These episodes appear to be noninfectious in origin, and are often accompanied by arthralgia, subcutaneous edema and a morbilliform rash.
diagnosisThe characteristic recurrent acute febrile
attacks without a clear infectious or autoimmune cause suggest the need for investigation. The diagnosis of HIDS is confirmed by the continuously high IgD values (more than 100 IU/ml). However, IgD may be normal in patients under three years of age. The key for diagnosis of MVa is the elevated level of Mevalonic acid in the urine, plasma and cerebrospinal fluid, which can be detected through organic acid analysis or more sensitively by isotope dilution mass spectrometry. Urinary excretion of leukotriene E4 is elevated in most patients. Radiometric assay testing can demonstrate reduced mevalonate kinase activity in white blood cells or cultured fibroblasts. DNA analysis showing two disease-linked mutations in the MVK gene is used to confirm the diagnosis.
Genetic counselingGenetic counseling should be offered to
families at risk of MVa. as MVa is an autosomal recessive disorder, the risk for future pregnancies is 25% for families who already have a child with MVa. Prenatal diagnosis of an affected fetus is possible for MVa but is usually not considered to be appropriate for HIDS.
treatmentEffective treatment has not yet been devised.
Trials of supplemental cholesterol, bile acids and inhibitors of HMG Coa reductase have not been therapeutic. Corticosteroids often control the symptoms of an acute crisis. Long-term therapy with ubiquinone-50, with vitamin C and vitamin E, appeared to calm down the clinical course and improve somatic and psychomotor development. Treatment of HIDS is largely supportive with the symptomatic treatment of febrile episodes. Various standard anti-inflammatory drugs including colchicine, NSaIDs, steroids and thalidomide have failed to suppress the attacks. Beneficial effect of anakinra, a recombinant interleukin-1 receptor antagonist is described in
a few patients. Reports of successful treatment of Mevalonic aciduria through allogenic bone marrow transplantation have also surfaced. Enzyme replacement therapy is not currently available.
What we do not know yetIt is yet to be known how the deficiency of
MVK causes the inflammatory periodic fever syndrome.
* Original name withheld.references
1. Haas D, Hoffmann GF. Mevalonic aciduria. Orphanet. http://www.orphanet.net/consor/cgi-bin/OC_Exp.php?lng=EN&Expert=29.
2. Van der Meer JW, Vossen JM, Radl J, et al. (May 1984). “Hyperimmunoglobulinaemia D and periodic fever: a new syndrome”. Lancet 1 (8386): 1087–90. doi:10.1016/S0140-6736(84)92505-4. PMID 6144826.
3. Drenth JP, van der Meer JW (December 2001). “Heredi-tary periodic fever”. N. Engl. J. Med. 345 (24): 1748–57. doi:10.1056/NEJMra010200. PMID 11742050.
4. http://en.wikipedia.org/wiki/Mevalonate_kinase_de-ficiency
5. http://rarediseases.info.nih.gov/gard/3588/mevalon-ic-aciduria/resources/1
IAP Kerala Election NotificationNominations are invited for the following posts
in IAP Kerala :President 2015 & Vice President 2015Last date for submitting Nominations - July 31st 2013 Scrutiny - Aug 3rd 2013 Last date for withdrawal of Nomination- Aug 15th 2013Sending ballot paper - Aug 25th - Sept 5th 2013Last date for receiving filled up ballot papers – Sept. 25th 2013Counting of votes - September 29th, 2013
Deposit of Rs.5000/- & Rs.2500/- to be paid by the candidates vying for the post of President & Vice President respectively.
Nomination forms can be downloaded from IAP Kerala website www.iapkerala.org
Completed Nomination forms to be sent to :Dr.George F. Moolayil
Emvee House, Kizhthadiyoor P.O. Palai 686 574, Kottayam Dist.

36 Pediatric Companion
dr. sajikumar J.Parabrahma Speciality Hospital
Oachira
1. Periorbital swelling in Chagas’ disease is ___ sign
2. Test for hearing impairment4. Test for vertigo/vestibular
dysfunction5. Horizontal scarring of the upper
tarsal conjunctiva in trachoma is ___line
8. Mastoid ecchymosis in basal skull fracture is ___sign
9. Nodules found in neurofibromatosis type 1
12. Test to detect achilles tendon rupture
14. Punctate bleeding when psoriatic scales are scraped is ___sign
Down
JANUAry 2013 issUE solUtioN
15. Bluish discolouration of the gingival border in lead poisoning
17. Inability to maintain convergence of eyes in thyrotoxicosis is ___ sign
18. Expressive aphasia due to lesions in frontal cortical areas
21. Dilated pupil, poorly reactive but with normal near accommodation
P E D I - C R O S S W O R DThe theme for this month’s Pedicrossword is ‘Eponymous Clinical signs. Eg. If the answer to a question is ‘Koplik’s spots’ then the solution would be Koplik. Please send in your answers by August 2013. An attractive prize awaits the winner. Across
3. Quick shallow respirations followed by period of apnea
6. Epigastric pain with pressure on McBurney’s point is ___sign
7. Pulse in aortic insufficiency 8. Abnormal plantar reflex10. Sign that detects neuritis or nerve compression11. Test to detect fixed flexion deformity of hip13. The increase in the intensity of the tricuspid
regurgitation murmur during inspiration is ___sign
16. Hyperaesthesia at inferior angle of right scapula in acute cholecystitis is ___sign
19. Triad which describes the factors that contributes to thrombosis
20. Dermatographic sign in urticaria pigmentosa22. Painless symmetrical joint swellings in
congenital syphilis23. Sign in muscular dystrophy
Pedicrossword January 2013
Winner
Dr. N.RAMACHANDRANPediatrician & Retd. Dy DHS
18/469, Nataraj, West YakkaraPalakkad - 678001
The theme for this month’s Pedi -crossword is ‘Eponymous Clinical signs. Eg. If the answer to a question is ‘Koplik's spots’ then the solution would be Koplik. Please send in your answers by _____. An attractive prize awaits the winner.
Dr. Saji Kumar .J
Parabrahma Specialty Hospital
Oachira
1 2 3 4
5 6
7
8
9 10
11 12 13 14
15
16 17
18 19
20 21
22 23
ACROSS 3. Quick shallow respirations followed by period of apnea 6. Epigastric pain with pressure on McBurney's point is ___sign 7. Pulse in aortic insufficiency 8. Abnormal plantar reflex 10. Sign that detects neuritis or nerve compression 11. Test to detect fixed flexion deformity of hip 13. The increase in the intensity of the tricuspid regurgitation murmur during inspiration is ___sign 16. Hyperaesthesia at inferior angle of right scapula in acute cholecystitis is ___sign 19. Triad which describes the factors that contributes to thrombosis 20. Dermatographic sign in urticaria pigmentosa 22. Painless symmetrical joint swellings in congenital syphilis 23. Sign in muscular dystrophy
DOWN 1. Periorbital swelling in Chagas' disease is ___ sign 2. Test for hearing impairment 4. Test for vertigo/vestibular dysfunction 5. Horizontal scarring of the upper tarsal conjunctiva in trachoma is ___line 8. Mastoid ecchymosis in basal skull fracture is ___sign 9. Nodules found in neurofibromatosis type 1 12. Test to detect achilles tendon rupture 14. Punctate bleeding when psoriatic scales are scraped is ___sign 15. Bluish discolouration of the gingival border in lead poisoning 17. Inability to maintain convergence of eyes in thyrotoxicosis is ___ sign 18. Expressive aphasia due to lesions in frontal cortical areas 21. Dilated pupil, poorly reactive but with normal near accommodation
1E C Z E 2M A 3L
4H E 5C H T U 6Q A 7T O R C H M U S
A 8K A 9T E X 10P H I P P S
11R N R S N A
12F O R C H H E I M E R S
U R P 13L Y M 14E 15P O X E O 16P B
17R I N D E R P E S T O
18I M 19N I L 20T A O 21H A N T A
O 22J E R Y L L Y N N
X G 23Y E L L O W
O 24B L A D D E R A
I E W 25A T 26S 27D A M R O S C H 28R E S O M A L A
I U R 29R O M A N A 30B O R N H O L M S