edward camacho mina 1061 md4 windsor university hodgkin lymphoma
TRANSCRIPT

Edward Camacho Mina1061
MD4
WINDSOR UNIVERSITY
HODGKIN LYMPHOMA

Lymphoma
Clonal malignant disorders that are derived from lymphoid cells: either precursor or mature T-cell or B-cell
Majority are of B- cell origin
Hodgkin lymphoma
It is a neoplastic disorder and proliferation of Reed-Sternberg (RS) cells, which are large B cells with multilobed nuclei and prominent nucleoli ('owl-eyed nuclei.classically
It usually arises in lymph nodes and spreads to contiguous groups. Extranodal presentation are rare. Disease is associated with defective cellular immunity.

Hodgkin Disease
Incidence:
2-4 cases per 100.000 population / year
Bimodal age distribution :
15-35 years and above 50 years
male predominance M:F = 1,7:1

Etiology
most Hodgkin's lymphoma occurs when an infection-fighting cell called a B cell develops a mutation in its DNA.
Infection with EBV

Hodgkin's lymphoma
It is divided into two groups:
1. Classical Hodgkin's lymphoma
2. Lymphocyte-predominant

Classical Hodgkin's lymphoma
This is the most common type of this disease. And patients diagnosed with classical Hodgkin's lymphoma have large and abnormal cells called Reed-Sternberg cells in the lymph nodes.

classical Hodgkin's lymphoma
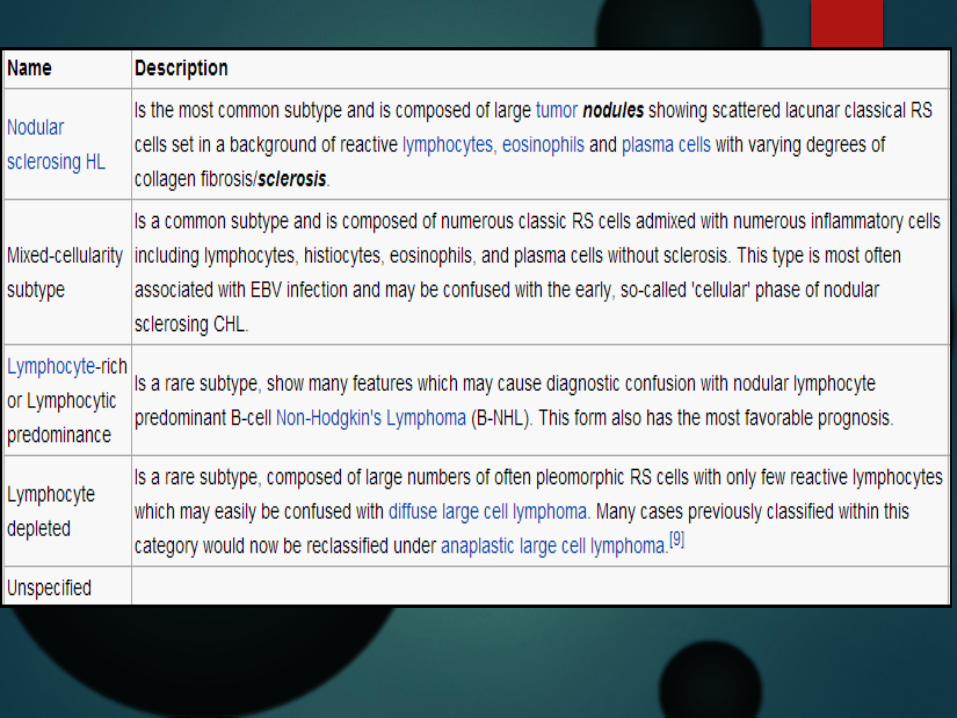
Subtypes of include:
Nodular sclerosis Hodgkin's lymphoma (70% of all cases).
Mixed cellularity Hodgkin's lymphoma
Lymphocyte-depleted Hodgkin's lymphoma
Lymphocyte-rich classical Hodgkin's lymphoma
.

Lymphocyte-predominant Hodgkin's lymphoma
This is a rarer type of Hodgkin's lymphoma . In this type of lymphoma, there are very few Reed-Sternberg cells. But there are other abnormal, and large cells with the appearance of popcorn cells.
This lymphoma has better prognosis if diagnosed at an early stage.

Popcorn cells
Risk factors
age.
Hodgkin's lymphoma is most often diagnosed in people between the ages of 15 and 35, as well as those older than 55.
A family history of lymphoma.
patients with a relative presenting Hodgkin's lymphoma or non-Hodgkin's lymphoma have an increased risk of developing Hodgkin's lymphoma.
Risk factors
sex.
Males are more likely to develop Hodgkin's lymphoma than women.
Epstein-Barr infection.
People who have had exposure to Epstein-Barr virus, which causes infectious mononucleosis, are more likely to develop Hodgkin's lymphoma.

Clinical Presentation
Nontender lymph nodes enlargement ( localised ) neck and supraclavicular area 60-80% mediastinal adenopathy 50% other ( abdominal, extranodal disease )
systemic symptoms (B symptoms) 30% fever night sweats unexplained weight loss (10% per 6 months)
other symptoms fatigue, weakness, pruritus cough , chest pain, shortness of breath, vena cava syndrome abdominal pain, bowel disturbances, ascites bone pain


Diagnosis of Hodgkin's lymphoma
It is based on microscopic examination of lymph node or other involved tissue
it requires identification of diagnostic Reed-Sternberg cells
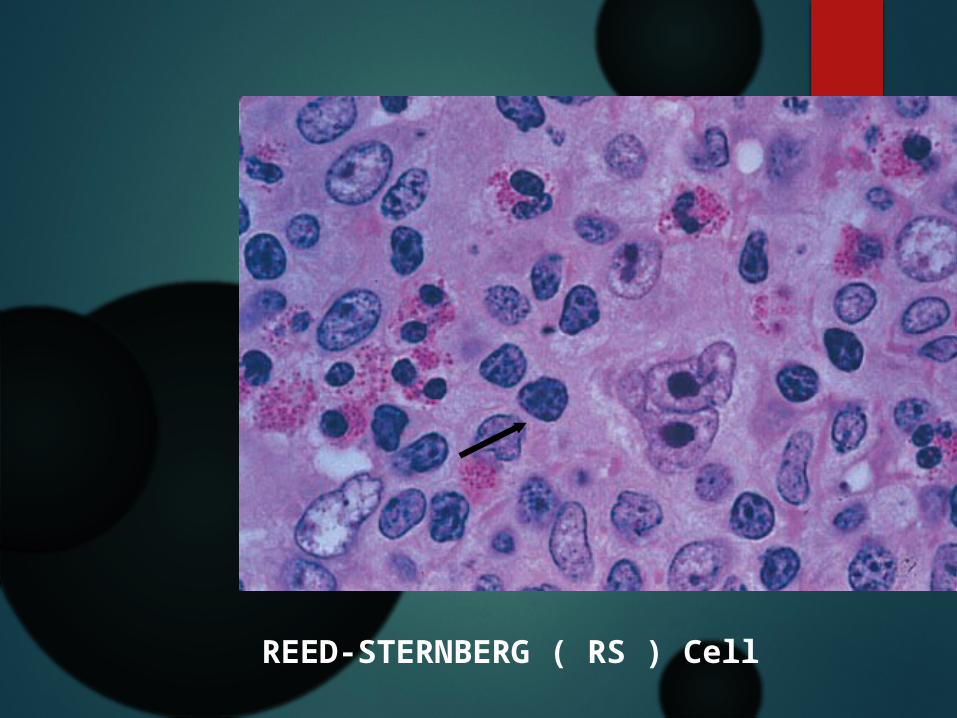
REED-STERNBERG ( RS ) Cell
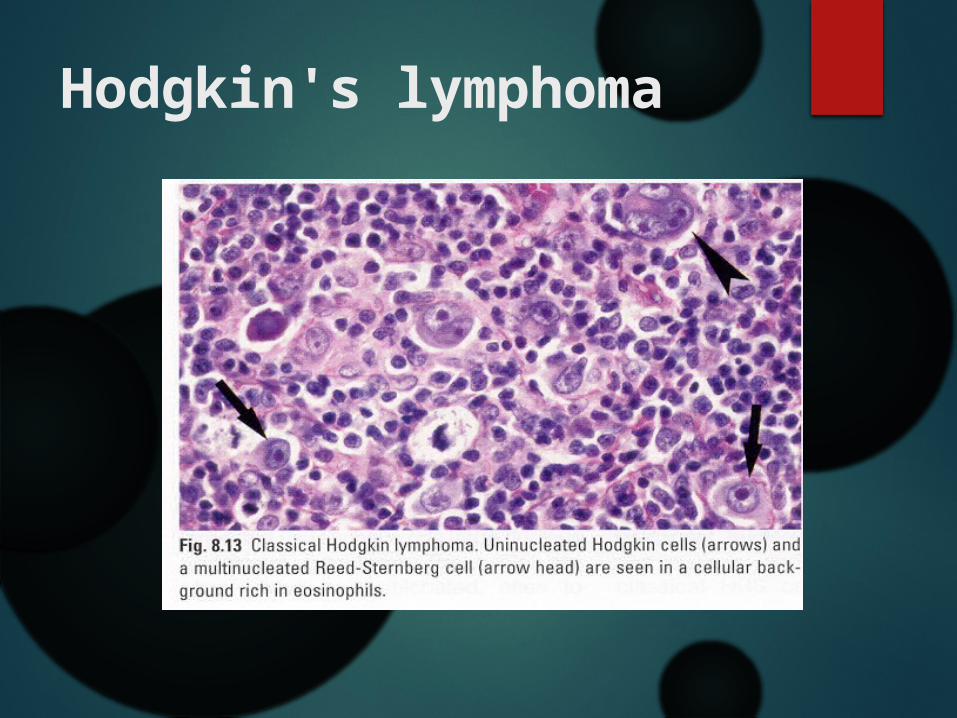
Hodgkin's lymphoma

Diagnosis of Hodgkin's lymphoma
Physical exam.
Checking for swollen lymph nodes, including in the neck, underarm and groin, as well as a swollen spleen or liver.
Blood tests.
A sample of your blood is examined in a lab to see if anything in the blood indicates the possibility of cancer.
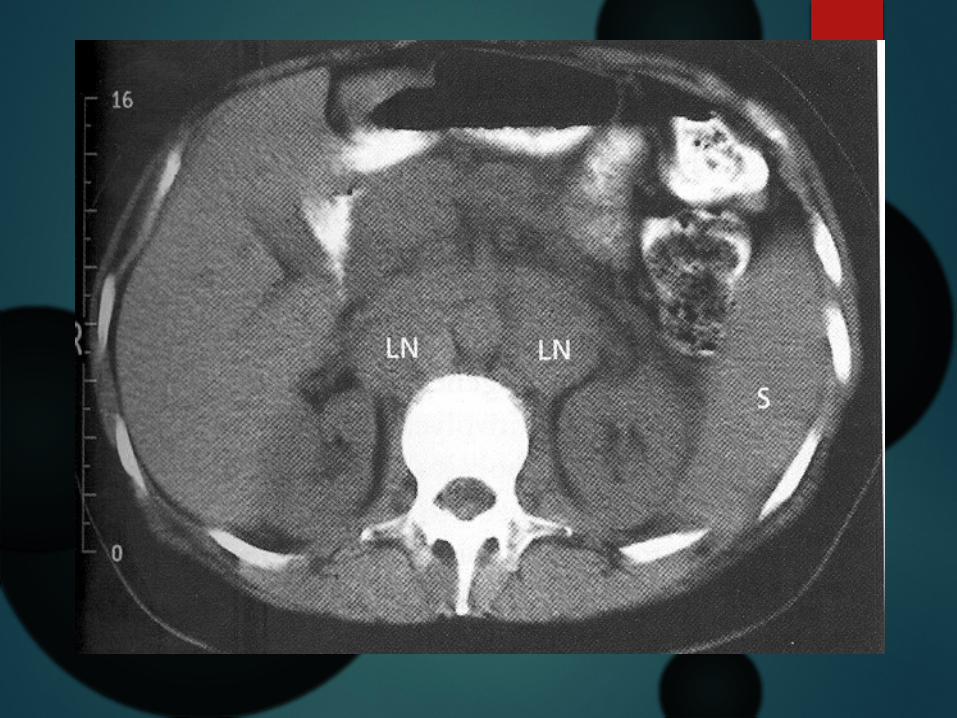
Diagnosis of Hodgkin's lymphoma
Imaging tests.
Imaging tests used to diagnose Hodgkin's lymphoma include X-rays, computerized tomography (CT) scan, magnetic resonance imaging (MRI) and positron emission tomography (PET).
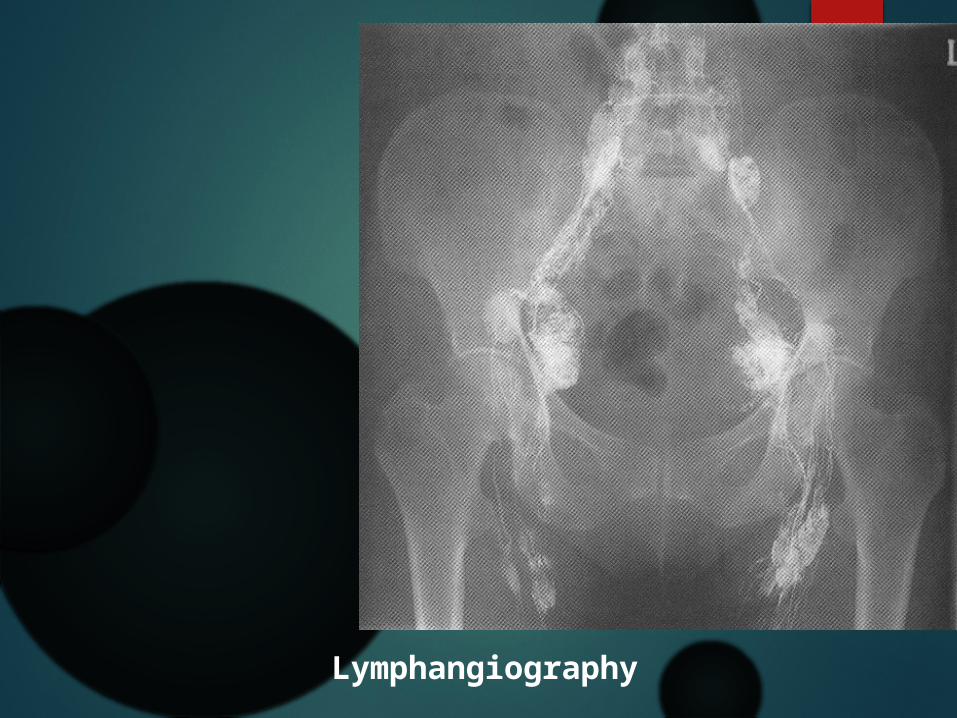
Lymphangiography

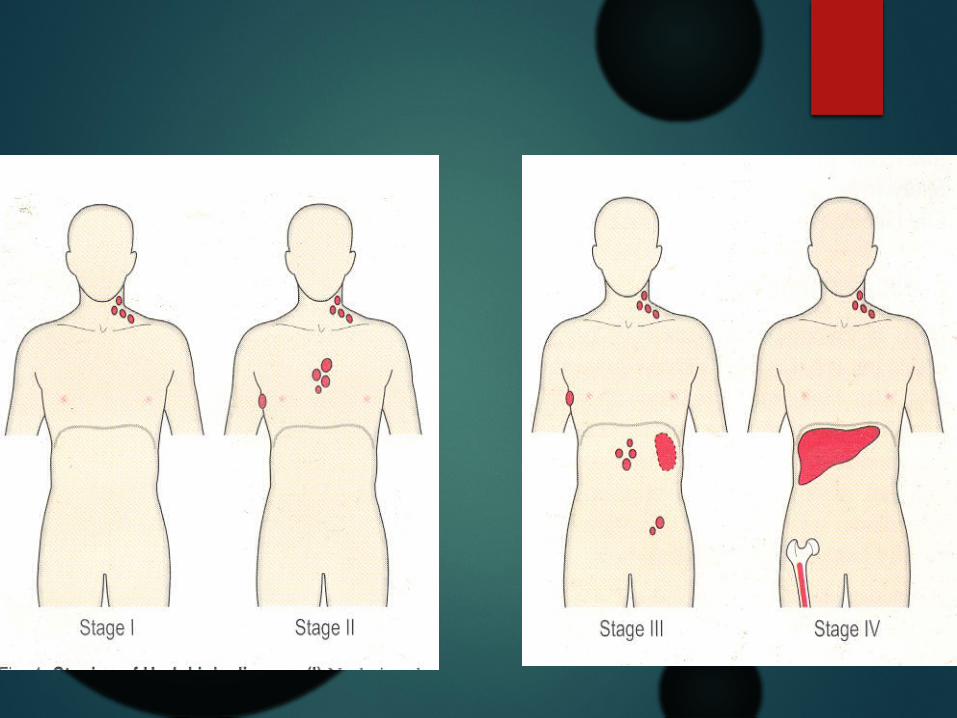
Staging
Stage I : Involvement of single LN region
Stage II : Two or more LN regions involved on the same side of diaphragm
Stage III : Involvement of lymph node regions on both sides of diaphragm.
Stage IV : Involvement outside LN areas (Liver, bone marrow)

Treatment
RT
Chemo
Antibody treatment: Rituximab target CD-20
Supportive

Treatment - Guidelines
Indications for RT: Stage I disease
Stage II disease with 3 or lesser areas involved
Indications for CT Stage II disease with >3 areas involved
Stage III and IV disease

Mr. Smith, a 25 year old man, presented with malaise, night sweats, weight loss and intermittent fever dating for 3 months. On examination, he had bilateral, cervical and axillary lymphadenopathy. His liver and spleen were not enlarged. Investigation showed that his hemoglobin was low (113g/l) and the white-cell count was normal (4.2 x 109/l. The blood film did not show any abnormal cells. A cervical lymph node was removed for histology. The gross architecture of the node was destroyed; the tissue consisted of histiocytes, eosinophils, lymphocytes and giant binucleate cells known as Reed-Sternberg cells. A bone marrow examination was normal and a tomography showed no involvement of other lymph nodes.