慢性腎臟病與糖尿病藥物 - ktgh.com.t · 05/12/2017 1 慢性腎臟病與糖尿病藥物...
TRANSCRIPT

05/12/2017
1
慢性腎臟病與糖尿病藥物
光田綜合醫院 新陳代謝科
曾士婷醫師
2017.5.
1
藥物動力學
2

05/12/2017
2
全球糖尿病盛行率
Lancet. 2016 Apr 5. pii: S0140-6736(16)00618-8. doi: 10.1016/S0140-6736(16)00618-8.
從1億8百萬到 4億2千2百萬人
人口結構改變39.7%
兩者互動31.8%
盛行率改變 28.5%
Prevalence of diabetes in East Asian countries compared
to the United States and Europe: Estimates for 2015
Country
Diabetes
prevalence in
2015 (%)
Diabetes
comparative
prevalence in
2015 (%)
Adults with
undiagnosed
diabetes (20-79)
in 1,000s
China 10.6 9.8 57 813.6
Hong Kong 10.2 8.0 273.5
Taiwan 10.0 8.4 828.3
Singapore 12.8 10.5 253.8
Japan 7.6 5.7 3 353.8
Korea 8.7 7.2 1559.0
Australia 6.3 5.1 493.9
USA 12.8 10.8 8 284.6
UK 6.2 4.7 1 068.9
IDF Diabetes Atlas I Seventh edition I Atlas, IDF Diabetes. “7th." International Diabetes Federation (2015).

05/12/2017
3
5
Chronic Complications of DM
Diabetic
Retinopathy
Leading cause
of blindness
in working age
adults1
Diabetic
Nephropathy
Cardiovascular
Disease
Stroke
2 to 4 fold increase in cardiovascular mortality and stroke3
Diabetic
Neuropathy
Leading cause of
non-traumatic lower
extremity amputations5
8/10 diabetic patients
die from CV events4
1 Fong DS, et al. Diabetes Care 2003; 26 (Suppl. 1):S99–S102. 2Molitch ME, et al. Diabetes Care 2003; 26 (Suppl. 1):S94–S98. 3 Kannel WB, et al. Am Heart J 1990; 120:672–676. 4Gray RP & Yudkin JS. In Textbook of Diabetes 1997.5Mayfield JA, et al. Diabetes Care 2003; 26 (Suppl. 1):S78–S79.
30% of Type 1 Diabetes40% of Type 2 Diabetes
Progression of DN
6The kidney at a glance. 2000; 82-2000 Blackwell Science Ltd.
Hyperfiltration
GBM thickening,Mesengial expansion
020 1015 525Years from diagnosis of diabetes
Stage 2 Microalbuminuria-BP rising
Stage 2 Hypertension
Stage 3 Proteinuria
Stage 4 Rising creatinine
Stage 5 ESRD
Pro
gression
of d
iabetic n
eph
rop
athy

05/12/2017
4
• Optimize glucose control
• Optimize blood pressure control (<140/90 mmHg)
• Dietary protein intake
–Not dialysis dependent: 0.8 g/kg body weight per
day.
– on dialysis: higher levels of dietary protein intake
should be considered
• ACEI or ARB
RecommendationsDiabetic Kidney Disease
American Diabetes Association Standards of Medical Care in Diabetes. Microvascular
complications and foot care. Diabetes Care 2016; 39 (Suppl. 1): S72-S80
Prevalence of ESRD
per
mil
lion
pop
ula
tion
https://www.usrds.org/2007/view/12_intl.asp
Atlas of End-Stage Renal Disease in the United States
05/12/2017
5
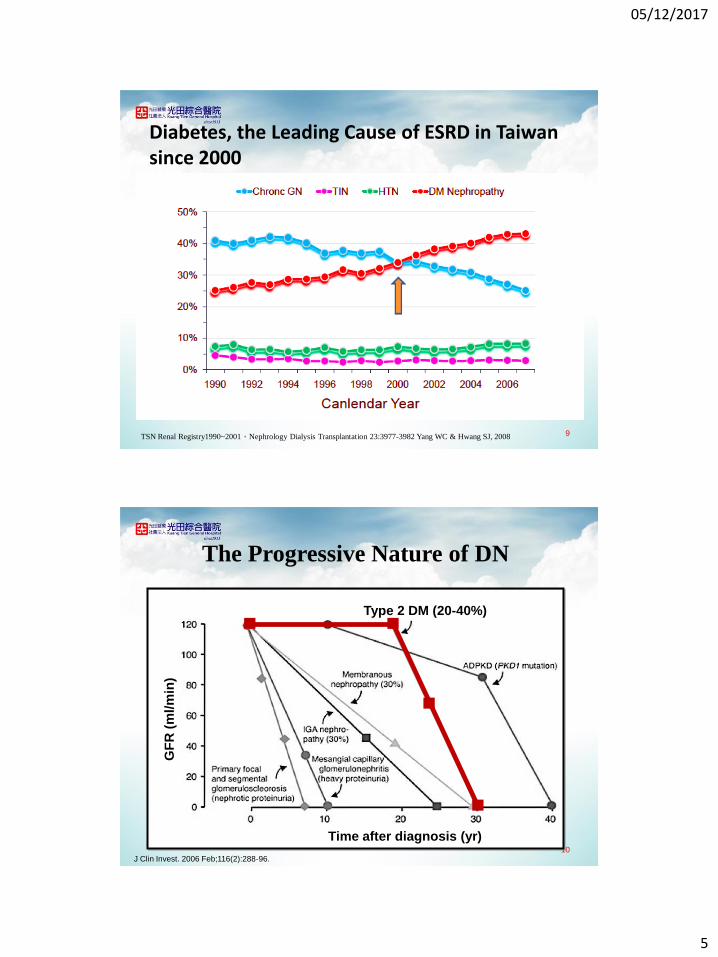
Diabetes, the Leading Cause of ESRD in Taiwan since 2000
9TSN Renal Registry1990~2001,Nephrology Dialysis Transplantation 23:3977-3982 Yang WC & Hwang SJ, 2008
The Progressive Nature of DN
10J Clin Invest. 2006 Feb;116(2):288-96.
Type 2 DM (20-40%)
GF
R(m
l/m
in)
Time after diagnosis (yr)

05/12/2017
6
Prediction Probability for Incidence or
Progression of CKD After 5.5 years in
T2DM
11Modified from Clin J Am Soc Nephrol. 2015 Aug 7;10(8):1371-9.
5 2515
For incidence of CKD
UACR (mg/g)
UACR (mg/g)
For progression of CKD
50 100 200
eGFR CKD-EPI eGFR CKD-EPI
Predicted Probabilities for
Death within 5.5 years in T2DM
12
eGFR CKD-EPI eGFR CKD-EPI
For death
For death
UACR (mg/g)
5 15 25
UACR (mg/g)
50 100 200
Modified from Clin J Am Soc Nephrol. 2015 Aug 7;10(8):1371-9.
05/12/2017
7
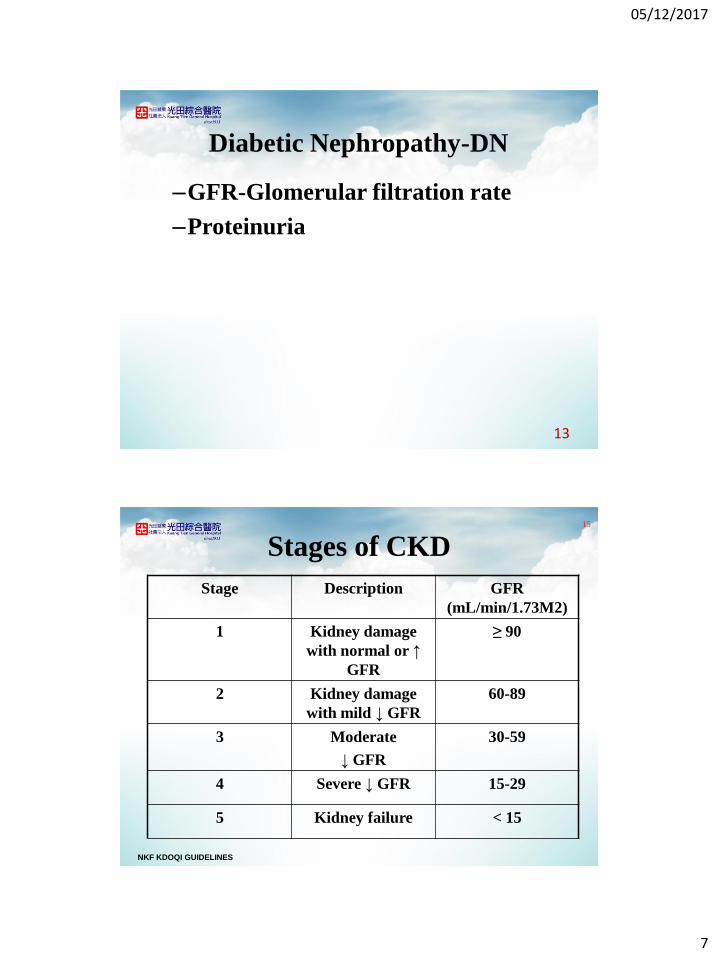
Diabetic Nephropathy-DN
–GFR-Glomerular filtration rate
–Proteinuria
13
Stages of CKD
Stage Description GFR
(mL/min/1.73M2)
1 Kidney damage
with normal or ↑
GFR
≥ 90
2 Kidney damage
with mild ↓ GFR
60-89
3 Moderate
↓ GFR
30-59
4 Severe ↓ GFR 15-29
5 Kidney failure < 15
15
NKF KDOQI GUIDELINES

05/12/2017
8
Hyperglycemic Damage Pathway
Clinical diabetes, Vivian A. Fonseca, 2006
13
Vasopressor peptide
Sympathetic activation
Elevation in blood pressure
Hyperglycemia
Metabolic change Hemodynamic change
Diabetic Nephropathy (DN)
Type 1 DM Type 2 DM
Reactive oxygen species
Inflammatory cytokines
Growth & apopototic factor
17Clinical Diabetes , Vivian A. Fonseca, 2006

05/12/2017
9
CKD造成血糖異常之各項因素
37 1
CKD造成血糖異常之各項因素
37 1
低血糖 監測困難

05/12/2017
10
20
Diabetes and ESKD
• Reducing insulin requirements
• Difficult vascular access
• Accelerated macrovascular disease
• Advanced microvascular disease
• Frequent sepsis
• Silent ischaemia
• 2-3 x death rate vs non-DM patients
Burnt-Out Diabetes
Semin Dial. 2014 March ; 27(2): 135–145. doi:10.1111/sdi.12198. 1
05/12/2017
11
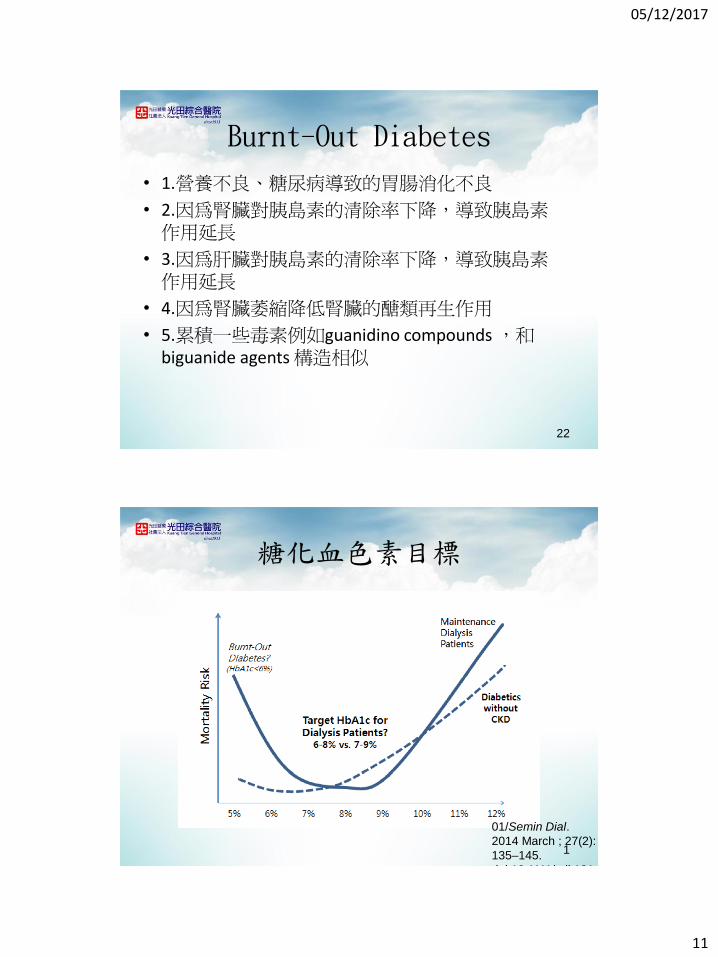
Burnt-Out Diabetes
• 1.營養不良、糖尿病導致的胃腸消化不良
• 2.因為腎臟對胰島素的清除率下降,導致胰島素作用延長
• 3.因為肝臟對胰島素的清除率下降,導致胰島素作用延長
• 4.因為腎臟萎縮降低腎臟的醣類再生作用
• 5.累積一些毒素例如guanidino compounds ,和biguanide agents 構造相似
22
糖化血色素目標
01/Semin Dial.
2014 March ; 27(2):
135–145.
doi:10.1111/sdi.121
1

05/12/2017
12
與糖代謝有關的實驗室及臨床數據
• 糖化血色素(A1C)
• 空腹血糖 (AC sugar)
• 餐後血糖 (PC sugar)
• 血漿C-peptide濃度
• 血漿insulin濃度
24
A
B
C
建議的血糖控制目標
Adapted from 中華民國糖尿病學會 2006 第2型糖尿病照護指
引p.9.

05/12/2017
13
口口服抗糖尿病藥物Oral Antidiabetic Drugs (OAD)服
抗糖尿病藥物Oral Antidiabetic Drugs (OAD)
26
01/11/2013 1Nephrol Dial Transplant (2014) 29: 1284–
1300

05/12/2017
14
口服降血糖藥物的種類
• 胰島素分泌促進劑(insulin secretagogues)
– 磺醯尿素(sulfonylureas)
– Glinides (又稱Meglitinides類似物)
• 胰島素敏感劑 (insulin sensitizer)
– 雙胍類 ( Biguanides)
– Glitazones (Thiazolidinediones, TZD)
• 阿爾發-葡萄糖甘酶抑制劑(α-glucosidase inhibitor )
• 二肽基肽酶抑制劑(DPP-4 Inhibitor)28
Major Targeted Sites of Oral Drug
Classes
29Buse JB et al. In: Williams Textbook of Endocrinology. 10th ed. Philadelphia: WB Saunders; 2003:1427–1483; DeFronzo RA. Ann Intern Med.
1999;131:281–303; Inzucchi SE. JAMA 2002;287:360-372; Porte D et al. Clin Invest Med. 1995;18:247–254.
DPP-4=dipeptidyl peptidase 4; TZDs=thiazolidinediones.
Glucose
absorption
Hepatic glucose
overproduction
Impaired insulin
secretion
Insulin
resistance
Pancreas
↓Glucose level
Muscle
and fatLiver
Biguanides
TZDs Biguanides
TZDs
α-Glucosidase
inhibitors
Gut
Sulfonylureas
Meglitinides
DPP-4 inhibitors
DPP-4 inhibitors
Biguanides

05/12/2017
15
醫院常見之口服降血糖藥物 (1)
學名 商品名 劑量範圍
(mg/day)
Peak
level
(h)
Half-
life
(h)
代謝途徑
(腎/肝)
健保價
(元)
Sulfonylurea
Glipizide GliDiab 2.5-40 1-3 2-4 80/20 2.18/ 5mg
Gliclazide Mezide 80-320 4–6 10.4 65/25 5/ 80mg
Glibenclamide Gliben 1.25-20 ~4 10 50/50 1.74/ 5mg
Glimepiride Amaryl 1-8 2-3 9 60/40 10.5/ 2mg
Meglitinide
Repaglinide Novonorm 1.5-12 0.75 1 -/100 5.8/ 1mg
D-phenylalanine
derivative
Nateglinide Starlix 360 1.0 1.4 80/10 7.3/
120mg30
醫院常見之口服降血糖藥物 (2)
學名 商品名 劑量範圍
(mg/da
y)
Peak
level
(h)
Half-
life
(h)
代謝途徑
(腎/肝)
健保價
(元)
Biguanide
Metformin Glibudon 750-
2550
1-2 6 90/10 2.35/
500mg
a-glucosidase
Inhibitor
Acarbose Glucobay 75-300 ~ ~ ~ 5.8/ 50mg
Thiazolidinedio
ne
Rosiglitazone Avandia 4-8 1 3-4 ~ 39/ 4mg
Pioglitazone Actos 15-45 2 3-7 20/80 59/ 30mg31

05/12/2017
16
選擇口服降血糖藥物之考量原則
需依據患者之病情
• 胰島素分泌不足 ( Insulin deficiency) 或胰島素作用不良( Insulin resistance)?
• 血糖之高低與糖尿病症狀之嚴重程度
• 飲食習慣與進食狀況
• 肝、腎、心臟功能與併發之疾病
• 自理生活之能力與居家照顧之品質
• 藥物之療效
• 低血糖等副作用的風險
• 價格因素
32
胰島素分泌促進劑
• 磺醯尿素(sulfonylureas)– A1C 降低約1-2%
– 最大降糖效果通常在仿單建議最大劑量的1/2~2/3時便已達到
• Glinides (Meglitinides analogue)– A1C 降低約0.8%
– 作用快速,須隨餐服用,可降低餐後高血糖
– 短效,較少低血糖副作用
– Repaglinide 不可與gemfibrozil 併用
33

05/12/2017
17
SU的作用機轉
34
Insulin Secretagogues類
01/11/2013 1

05/12/2017
18
SFU in CKD
• Depends on Renal or Hepatic metabolism
• Depends also on whether metabolites have hypoglycemic effects
36
37

05/12/2017
19
38
Insulin Sensitizers類
01/11/2013 1

05/12/2017
20
Metformin
• 常用於過重或肥胖的(準)糖尿病患者
• 並不刺激胰島素分泌,單獨使用少見低血糖副作用
• 抑制肝糖新生與製造,因而降低空腹血糖
• 治療後不會增加體重
• 可改善血脂肪異常,對內皮細胞功能等心血管危險因子有正向的影響
• 常見腸胃道一過性副作用,低劑量起始可避免
• 肝腎心肺功能不良不宜使用,以免發生40
Biguanide(雙胍類)的作用機轉
1. Metformin降低肝臟中
的葡萄糖新生作用
2. 降低或延遲腸道葡萄糖吸收
3. 促進GLUT4移動到細胞表面而增加胰島素敏感性

05/12/2017
21
Thiazolidinediones
• 活化peroxisome proliferative-activated receptor-γ (PPAR-γ),而增加胰島素之敏感度,降低空腹血糖及血中胰島素濃度
• 降糖效果較緩慢,通常需6至8週才見成效
• 需在內生或外源性胰島素存在下才有作用
• 可改善內皮細胞功能,發炎指摽等心血管疾患危險因子
• 與metformin 併用對改善胰島素阻抗性有加成作用
• 常見副作用有體重增加、水腫等,需密切追蹤肝指數如ALT,若ALT值超過正常上限的三倍,應停藥
• 重度心臟衰竭者不宜使用
42
43

05/12/2017
22
44
45

05/12/2017
23
46
Acarbose
• 抑制近端小腸澱粉及雙醣類之分解,延緩葡萄糖的吸收,降低飯後血糖、胰島素濃度,甚至空腹血糖
• 不被腸胃道吸收(<1%)
• 無體重增加之副作用
• 副作用為輕至中度的脹氣、腹瀉;自低劑量起始可減緩(start low, go slow)
• 低血糖僅出現於合併療法時,須使用葡萄糖或牛奶治療
• 使用於輕中度糖尿病之單一治療或合併治療
• 可減低葡萄糖耐量異常患者轉變為第2型糖尿病的機率及發生心血管疾患的風險 ,減緩頸動脈內膜厚度增加速率 (STOP-NIDDM)
• 可減低第2型糖尿病患者心肌梗塞風險(MeRIA)47

05/12/2017
24
α-Glucosidase inhibitors類
01/11/2013 1
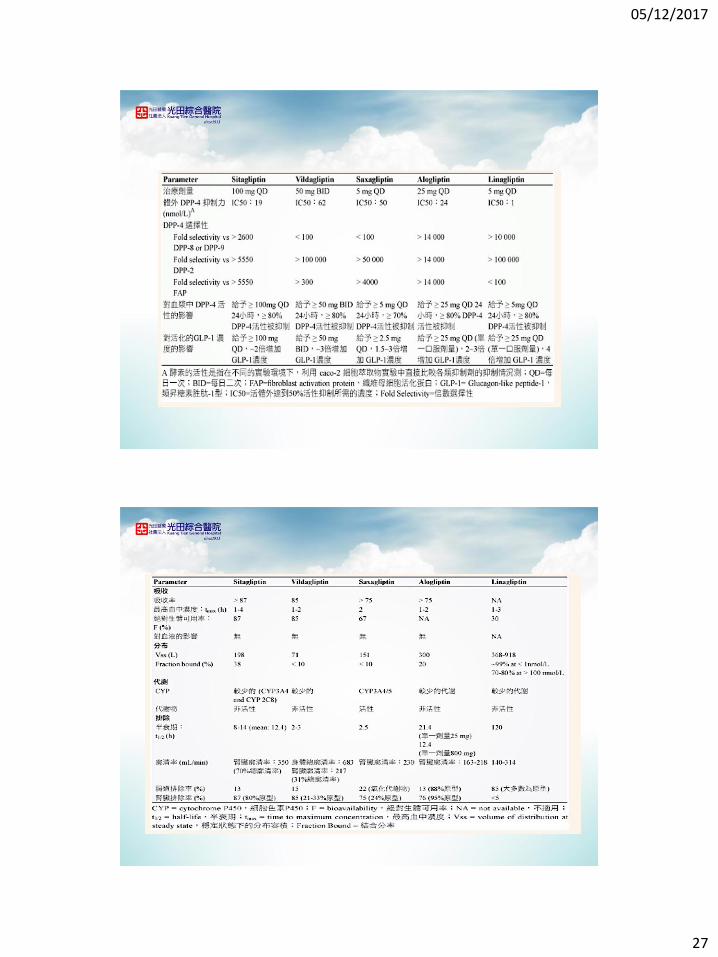
DPP-4 Inhibitor 二肽基肽酶抑制劑
作用機轉
•抑制DPP-4酵素提昇incretins濃度,包括GLP-1及GIP的濃度。
•incretins是體內平衡葡萄糖生理調節之內因系統一部份,當血糖升高時,GLP-1與GIP會提高胰臟β細胞合成及釋出胰島素作用;GLP-1也會降低α細胞昇糖素分泌作用,進而降低肝臟葡萄糖生成
副作用
•對照性臨床研究中,不論單一或合併療法,表現出良好耐受性,出現臨床不良反應而停藥者與安慰劑相當
49

05/12/2017
25
50
DPP-4 Inhibitor 二肽基肽酶抑制劑:提升活性incretin濃度
51
*Refers to amino acid number.
Deacon CF et al. Diabetes. 1995;44:1126–1131.
Meal
Intestinal
GIP and GLP-1
release
GIP and GLP-1
Actions
DPP-4
Enzyme
GIP-(1-42*)
GLP-1(7-36)*
Intact (active)
GIP-(3-42)*
GLP-1(9-36)*
metabolites
Rapid InactivationX
DPP-4
Inhibitor

05/12/2017
26
Incretin-Based Insulin Secrtagogues類
01/11/2013 1
53
05/12/2017
27

05/12/2017
28
Nephrol Dial
Transplant (2014)
29: 1284–1300
1
低血糖副作用及策略• 危險因子
– 老年、營養狀況不佳、餐無定時、或合併有肝腎功能異常者
• 低劑量起始
• 高危險族群考慮使用glinide
• 腎功能不良者考慮短效、具不活性代謝物、由肝臟排除者尤佳,可使用glinide
• 餐無定時或常誤餐者,可使用glinide
• 注意藥物交互作用– Alcohol, anticoagulant, trimethoprim
57

05/12/2017
29
• 抗糖尿病藥物胰島素
•
58
何時需使用胰島素?• 第1型糖尿病患者
• 第2型糖尿病患者– 空腹血糖超過300 毫克/毫升 和合併酮體血症或酮體尿
症。
– 持續性出現空腹血糖超過 300 毫克/毫升 和出現多尿、多喝、及體重減輕的症狀
• 糖尿病酮酸血症患者
• 肝腎功能不良的糖尿病患者
• 因急性病症住院的糖尿病或高血糖患者
• 口服抗糖尿病藥物療效不佳者
• 願意接受胰島素做為第一線治療的患者
• 妊娠性糖尿病患者無法以飲食控制者
• 糖尿病婦女懷孕時59

05/12/2017
30
60
Insulin in pt. on hemodialysis
•Insulin inhibitors – dialyzable
•Insulin resistance diminishes after the start of dialysis.
•half-life of insulin is prolonged.
•the potential for hypoglycemia with both oral agents and insulin increases in the presence of CKD (with the exception of gliquidone and glimepiride).
•Self-monitoring of blood glucose concentration is imperative.

05/12/2017
31
正常人血糖與胰島素濃度曲線
62
Continuous basal insulin secretion
Incremental prandial insulin secretion
Starting Dose
1 x Basal 10 IU (bedtime)
FBG value in millimoles per liter
0.16 IU/Kg
1 x Premix 10 IU ( Presupper)
2 x Premix 10 IU ( Prebreakfast), 10 IU ( Presupper)
MDI Individualized
63

05/12/2017
32
Scheme for Adding Basal or Intermediate-Acting Insulin to Oral Agents
64
Start with 5–10 units; increase by 2–3 units every 3 days
until FPG is between 110 and 120 mg/dl
Clinic- vs. Patient-driven Titration of Basal Insulin
--AT.LANTUS Study
24
140 and <180 mg/dl
(7.8 and <10 mmol/l)
Increase in daily basal insulin glargine dose (U)
26–8
180 mg/dl
(10 mmol/l)
22120 and <140 mg/dl
(6.7 and <7.8 mmol/l)
0–20–2100 and <120 mg/dl
(5.5 and <6.7 mmol/l)
Algorithm 2:
Patient-driven titration
every 3 days
Algorithm 1:
Clinic-driven titration
at every visit
Mean FBG for the
previous
3 consecutive days
Davies M et al. Diabetes Care2005;28:1282–8

05/12/2017
33
Self-Titration of Insulin Detemir:
The PREDICTIVE 303 Study• 303 Algorithm Sites: Patients to adjust dose every 3 days based on mean FPG values
• Standard-of-Care sites: Physician to adjust dose based on standard-of-careMeneghini et al. Diabetes Obes Metab. 2007;
9:902-13
FPG (mg/dL) Basal Dose Adjustment
< 80 Reduce detemir dose by 3U
80-110 No change
>110 Increase detemir dose by 3U
Key Learning Points
• There are clinical advantages of pens over vial-and-syringe dosing1,2
• You may need to consider features, advantages, and disadvantages of insulin pens as well as patient needs when selecting an insulin pen
• There are unique features in the insulin pens demonstrated today that may help you individualise care for your patients
1. Summers KH, et al. Clin Ther. 2004;26(9):1498-1505. 2. Cobden D, et al. Pharmacotherapy. 2007;27(7):948-962.
67

05/12/2017
34
Clinical advantages of pens over vial-and-syringe dosing
Ease of use2
Social acceptability2
Lifestyle adaptability2
Why Use an Insulin Pen?
•Patients with diabetes may benefit from modern insulin injection pens that provide an accurate way to inject insulin.1
1. Hänel H, et al. J Diabetes Sci Technol. 2008;2(3):478-481. 2. Summers KH, et al. Clin Ther. 2004;26(9):1498-505. 3. Cobden D, et al.
Pharmacotherapy. 2007;27(7):948-962.
Reduced risk for
hypoglycaemic events3
Overall reduced healthcare
costs3
68
Why Use an Insulin Pen? (continued)
Insulin pens:
Accurate dosing1-
4
Flexible2,3,5,6
Convenient2,3,5,6
1. Shelmet J, et al. Diabet Res Clin Pract. 2004;63(1):27-35. 2. Hänel H, et al. J Diabetes Sci Technol. 2008;2(3):478-481. 3. Korytkowski M, et
al. Clin Ther. 2005;27(Suppl B):S89-S100. 4. Lombardo F, et al. Acta Biomed. 2005;76(S3):S66-S69. 5. Korytkowski M, et al. Clin Ther.
2003;25(11):2836-2848. 6. Bohannon NJ, et al. Clin Ther. 2000;22(9):1049-1067. 7. Fox C, et al. Practical Diabetes International.
2002;19(4):104-107.
Discreet2,4,5,6
Easy to use1-7
69
05/12/2017
35
Humalog KwikPen
•Humalog KwikPen is an easy-to-use, easy-to-inject pre-filled pen1
•For patients who want a portable device
•For patients desiring discreet insulin delivery
1. Data on file, Lilly USA, LLC; KwikPen Design Validation User Study. HUM20071024A.
Select Safety Information:
Pens and needles are for single-patient use only and should not be
shared, even in healthcare facilities, as infection or disease can be
spread from one person to another.
Do not withdraw insulin from the pen.
70
Humalog KwikPen (continued)
• Humalog KwikPen has the following advantages:
• Easy to set the dose
• Easy to see numbers
• Easy to dispense maximum dose of 60 units*
• Easy to dispense dose*
*Humalog KwikPen Design Validation User Study included adult male and female participants with type 1 and type 2 diabetes. Of the total 150 study
participants, 56 were insulin-naïve, 42 were currently administering insulin with a vial and syringe, and 52 were experienced insulin pen users.
Data on file, Lilly USA, LLC; KwikPen Design Validation User Study. HUM20071024A.
Easy to dial up and back down for
dose correction
Short thumb-reach at high doses
Small, lightweight, and portable
71
05/12/2017
36
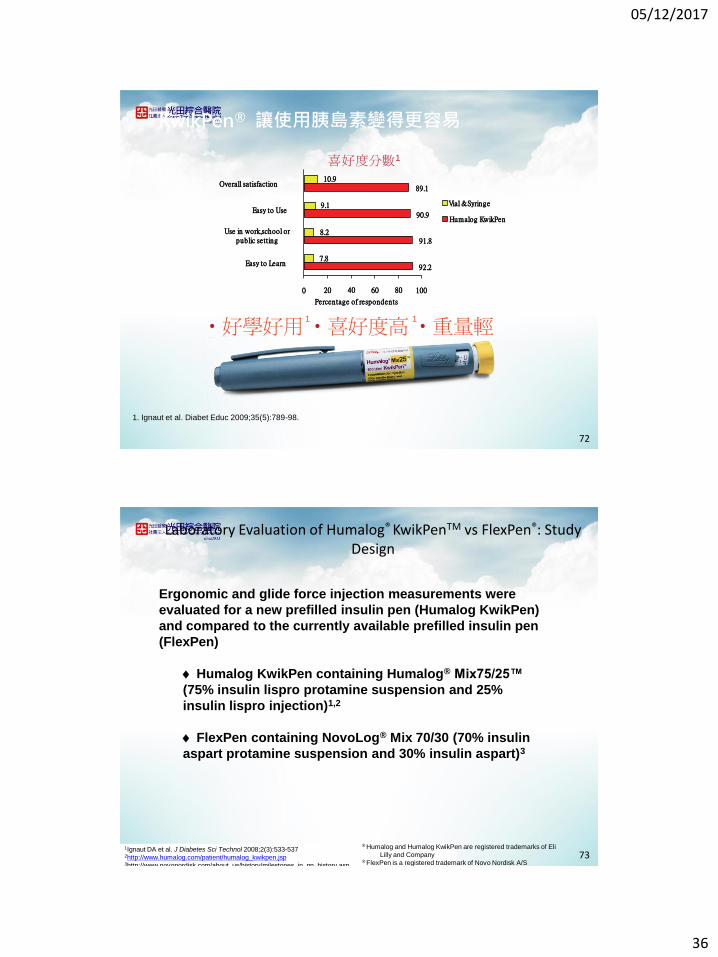
KwikPen® 讓使用胰島素變得更容易
1. Ignaut et al. Diabet Educ 2009;35(5):789-98.
‧好學好用 ‧喜好度高 ‧重量輕 1 1
喜好度分數1
Overall satisfaction
Easy to UseVial & Syringe
Humalog KwikPen
Easy to Learn
Percentage of respondents
Use in work,school orpublic setting
0 20 40 60 80 100
92.2
91.8
90.9
89.1
10.9
9.1
8.2
7.8
72
Laboratory Evaluation of Humalog® KwikPenTM vs FlexPen®: Study Design
Ergonomic and glide force injection measurements were
evaluated for a new prefilled insulin pen (Humalog KwikPen)
and compared to the currently available prefilled insulin pen
(FlexPen)
Humalog KwikPen containing Humalog® Mix75/25™
(75% insulin lispro protamine suspension and 25%
insulin lispro injection)1,2
FlexPen containing NovoLog® Mix 70/30 (70% insulin
aspart protamine suspension and 30% insulin aspart)3
1Ignaut DA et al. J Diabetes Sci Technol 2008;2(3):533-5372http://www.humalog.com/patient/humalog_kwikpen.jsp3http://www.novonordisk.com/about_us/history/milestones_in_nn_history.asp
® Humalog and Humalog KwikPen are registered trademarks of Eli
Lilly and Company® FlexPen is a registered trademark of Novo Nordisk A/S
73

05/12/2017
37
Humalog KwikPen (A)
FlexPen (B)
Overall Length (in) 5.69 6.23
Weight w/ cap (g) 31.12 23.98
Diameter across cartridge holder (in)
0.56 0.51
Data from Ignaut DA et al. J Diabetes Sci Technol 2008;2(3):533-537® Humalog and Humalog KwikPen are registered trademarks of Eli Lilly and Company ® FlexPen is a registered trademark of Novo Nordisk A/S
Laboratory Evaluation of Humalog® KwikPenTM vs FlexPen®
Ergonomic Testing Results
74
Distance (in) Humalog KwikPen (A)
FlexPen (B)
At 30 units 0.95 1.20
At 60 units 1.50 1.83
Data from Ignaut DA et al. J Diabetes Sci Technol 2008;2(3):533-537® Humalog and Humalog KwikPen are registered trademarks of Eli Lilly and Company ® FlexPen is a registered trademark of Novo Nordisk A/S
Laboratory Evaluation of Humalog® KwikPenTM vs FlexPen®
“Thumb Reach” Distances
75

05/12/2017
38
Humalog KwikPen FlexPen
Ignaut DA et al. J Diabetes Sci Technol 2008;2(3):533-537® Humalog and Humalog KwikPen are registered trademarks of Eli Lilly and Company ® FlexPen is a registered trademark of Novo Nordisk A/S
Laboratory Evaluation of Humalog® KwikPenTM vs FlexPen®
“Thumb Reach” Dialed Out to 60 Units
76
Laboratory Evaluation of Humalog® KwikPenTM vs FlexPen®
Injection Force Characteristics
30-Unit Dose 60-Unit Dose
Humalog KwikPen
FlexPen Humalog KwikPen
FlexPen
Maximum Glide Force (lbs)
3.42 ± 0.35 5.36 ± 0.76 3.61 ± 0.40 5.62 ± 0.77
Average Glide Force (lbs)
3.31 ± 0.35 4.95 ± 0.65 3.39 ± 0.38 5.08 ± 0.66
Glide Force Variability at Plateau Curve (lbs)
0.30 ± 0.06 0.76 ± 0.32 0.57 ± 0.15 1.01 ± 0.42
Data represent the mean ± standard deviation;
All treatment comparisons were statistically significant, P<0.0001
Data from Ignaut DA et al. J Diabetes Sci Technol 2008;2(3):533-537® Humalog and Humalog KwikPen are registered trademarks of Eli Lilly and Company ® FlexPen is a registered trademark of Novo Nordisk A/S
77

05/12/2017
39
30 Units
Time (s)
0 1 2 3 4 5 6
Gli
de
Fo
rce (
lbs
)
0
2
4
6
8
10
Time (s)
0 1 2 3 4 5 6
KwikPen
FlexPen
60 Units
Abbreviation: s, seconds. Data from Ignaut DA et al. J Diabetes Sci Technol 2008;2(3):533-537® Humalog and Humalog KwikPen are registered trademarks of Eli Lilly and Company ® FlexPen is a registered trademark of Novo Nordisk A/S
Laboratory Evaluation of Humalog® KwikPenTM vs FlexPen® Glide Force Profile
78
FlexPen
● Lighter in weight
● Smaller in diameter at the cartridge holder
Humalog KwikPen
● Shorter in overall length
● Shorter “thumb reach”
● Requires less effort to inject
● Provides smoother and more consistent delivery
Ignaut DA et al. J Diabetes Sci Technol 2008;2(3):533-537® Humalog and Humalog KwikPen are registered trademarks of Eli Lilly and Company ® FlexPen is a registered trademark of Novo Nordisk A/S
Laboratory Evaluation of Humalog® KwikPenTM vs FlexPen® Key Results Summary
79

05/12/2017
40
Primary Objective: Response to the Final Preference Question (FPQ)
Humalog KwikPen vs NovoLog® FlexPen®
Patient Preference
n=76
n=155
0
20
40
60
80
100
FPQ
Pe
rce
nta
ge
of
Re
sp
on
de
nts
NovoLogFlexPen
HumalogKwikPen
Ignaut DA, et al. Diabet Educ. 2009;35(5):789-798.
Which Insulin Pen Would You Prefer?
80
Humalog KwikPen vs NovoLog FlexPen
• Secondary Objective
• To what extent do you agree that the pen just assessed has these features?
• Overall ease of use1
• Ease of holding in hand when injecting1
• Ease of pressing injection button when injecting dose1,2
1. Ignaut DA, et al. Diabet Educ. 2009;35(5):789-798. 2. Ignaut DA, et al. J Diabetes Sci Technol. 2008;2(3):533-537.
Adapted from J Diabetes Sci Technol, 2008.2
81

05/12/2017
41
Humalog KwikPen vs NovoLog FlexPenPen Use Scores
n=38n=13
n=46 n=39
n=147
n=179
0
20
40
60
80
100
NovoLog FlexPen Humalog KwikPenPe
rce
nta
ge
of
Re
sp
on
de
nts
Was the Pen Overall Easy to Use?
Other
Agree
Strongly Agree
P=.006 Humalog KwikPen vs FlexPen for users who either agreed or strongly agreed.
*IDAB Question 14.Ignaut DA, et al. Diabet Educ. 2009;35(5):789-798.
82
Humalog KwikPen vs NovoLog FlexPenPen Use Scores (continued)
n=62 n=29
n=48 n=49
n=122
n=153
0
20
40
60
80
100
NovoLog FlexPen Humalog KwikPenPe
rce
nta
ge
of R
esp
on
de
nts
Was the Pen Easy to Hold in Your Hand When You Injected?
Other
Agree
Strongly Agree
P=.002 Humalog KwikPen vs FlexPen for users who either agreed or strongly agreed.
*IDAB Question 4.Ignaut DA, et al. Diabet Educ. 2009;35(5):789-798.
83

05/12/2017
42
Humalog KwikPen vs NovoLog FlexPenPen Use Scores (continued)
n=78
n=34n=48 n=47
n=106
n=150
0
20
40
60
80
100
NovoLog FlexPen Humalog KwikPen
Pe
rce
nta
ge
of
Re
sp
on
de
nts
Was It Easy to Press theInjection Button?
Other
Agree
Strongly Agree
P<.001 Humalog KwikPen vs FlexPen for users who either agreed or strongly agreed.
*IDAB Question 5.Ignaut DA, et al. Diabet Educ. 2009;35(5):789-798.
84
謝謝大家
85