effect of two different attachments on the supporting
TRANSCRIPT
The British University in Egypt The British University in Egypt
BUE Scholar BUE Scholar
Dentistry Health Sciences
4-2014
Effect of Two Different Attachments on the Supporting Structures Effect of Two Different Attachments on the Supporting Structures
and Masticatory Capacity of Implant Retained Mandibular and Masticatory Capacity of Implant Retained Mandibular
Overdenture Overdenture
Fardos N. Rizk The British University in Egypt, [email protected]
Follow this and additional works at: https://buescholar.bue.edu.eg/dentistry
Part of the Prosthodontics and Prosthodontology Commons
Recommended Citation Recommended Citation Rizk, Fardos N., "Effect of Two Different Attachments on the Supporting Structures and Masticatory Capacity of Implant Retained Mandibular Overdenture" (2014). Dentistry. 97. https://buescholar.bue.edu.eg/dentistry/97
This Article is brought to you for free and open access by the Health Sciences at BUE Scholar. It has been accepted for inclusion in Dentistry by an authorized administrator of BUE Scholar. For more information, please contact [email protected].

* Associate Professor, Head of Prosthodontics Department, Faculty of Dentistry, British University in Egypt
ملاحظاتصور 4 لونصور 1 لونص الألوانعدد الصفحاتالترقيمرقم المقالة
7816274
EFFECT OF TWO DIFFERENT ATTACHMENTS ON THE SUPPORTING STRUCTURES AND MASTICATORY CAPACITY OF IMPLANT
RETAINED MANDIBULAR OVERDENTURE
Fardos N. Rizk*
ABSTRACTAim: This study was conducted to compare the effect of ball and socket attachment and GPS
attachment in implant retained mandibular overdenture cases regarding changes in: crestal bone height and density surrounding implants, electromyographic activity of temporalis and masseter muscles and occlusal biting force.
Materials and Methods: Following two stage surgical protocol twelve completely edentulous patients received two implants placed bilaterally in the canine region (24 implants) to retain mandibular overdenture. Four months following the surgery patients were randomly divided into two equal groups; Group-I received ball and socket attachment while Group-II received GPS attachment upon which mandibular overdentures were retained. Once patients were comfortable to the prosthesis, they were placed on zero, three, six and twelve month follow-up period to measure: - Crestal bone height and density surrounding the implants using cone beam computed tomography. - Muscle activity of masseter and temporalis muscle using electromygraphic device. -Occlusal biting force using occlusal force-meter. Measurements were taken then the results were statistically analyzed.
Results: Both attachment designs showed crestal bone resorption and increase in bone density during all intervals of follow-up period however, there was statistically significant difference between the two designs in favour of GPS attachment which showed less crestal bone resorption but, there was statistically none significant difference between them regarding the increase in bone density. By time, the muscle activity decreased in both attachment designs with statistically none significant difference between them during all intervals of follow-up period. The occlusal biting force increased in both attachment designs with statistically significant difference between them in favour of GPS attachment which showed more increase during all intervals of follow-up period.
Conclusion: GPS attachment is less destructive to crestal bone surrounding the implants and has higher biting force than ball and socket attachment however, there is no difference between the two attachments in terms of muscle activity of masseter and temporalis muscles.
KEY WORDS: implants, GPS attachment, ball and socket attachment, overdenture, cone beam computed tomography, electromyograph , occlusal force-meter.

(2) Fardos N. RizkE.D.J. Vol. 60, No. 2
INTRODUCTION
The multitude of benefits to the edentulous population from implant supported overdenture is overwhelming in terms of better quality of life, emotional stability, improved function, enhanced esthetics and significantly clinical comfort to the patient. 1-7 The clinical comfort achieved is dependent on many factors including the degree of retention provided by proper location and orientation of implants, fitness of the prosthesis and the use of attachment elements as bar and clips, or solitary attachments. 8
Individual implants with solitary attachments have had the same favorable clinical results in mandible as rigidly splinted implants, in addition to being less costly, less technique sensitive, less dependent on implant position, easier to clean and to replace, easier to adjust and to control the amount of retention, and finally requires less inter-arch space. 9-11 Moreover, Takanashi et al.,12 estimated that the time required to fabricate mandibular overdenture retained by implants with solitary attachments was not significantly different than the time needed for conventional denture treatment.
Solitary attachments are available in various designs including ball, locator, equator and GPS attachments. Ball attachments drive their name from the shape of the male portion of the attachment which consists of a metal ball, whereas the female part is frictionally retained over the male stud and is incorporated in the denture resin. The use of ball attachments is advantageous regarding optimizing stresses and minimizing denture movement. Patient’s appreciation of their ball retained mandibular overdenture remained high over ten years follow-up period and clinical parameters revealed healthy mucosal conditions, high retentive measures and stable marginal bone levels.13-15
GPS attachment consists of female metallic abutment available in variable cuff heights and male nylon caps available in different colors each representing different degree of retention. This
attachment provides low profile design which offers multiple solutions for overdenture treatment planning where inter-occlusal space limitations are considered. It has the advantage of being resilient thus transferring more occlusal load to the soft tissues and lowering the stress placed on bone surrounding the implants than rigid attachments. It is also compatible with the hex tool which eliminates the need for special insertion tool as locator attachment and it enhances esthetics by its pink anodized metal housing of the male nylon cap which blends with denture acrylic allowing natural profile.
Three dimensional visualization of jaw areas has improved the clinical success of implants and their associated prostheses, and led to more accurate outcomes. Cone beam computed tomography (CBCT) accurately pinpoints vital structures and evaluates the surgical site underneath the soft tissues making it possible to pre-surgically determine with a high degree of accuracy and with 3D views the best position and inclination for implant placement based on the final prosthetic outcome.16-21
In general, the main motivation of the patients who look forward mucous supported implant rehabilitation is to increase the retention of the lower denture and to improve the masticatory capacity.22,25 Mastication is a highly coordinated neuromuscular function involving fast effective movements of the jaw, tongue and facial movements that vary depending on the food ingested. 26, 27On contraction of muscle, physical, chemical, thermal, and electrical changes take place in the individual muscle fibers. As a result of polarization changes associated with the contraction of the muscle, an electrical energy appears which is known as action potential. Recording this action potential is the basis for electromyographic measurements. The action potentials are picked up by the electrodes, amplified, and then recorded by electromyographic muscle activity recording device.28Since electromyography was introduced for dental research, several investigators have examined the relation between dental conditions and jaw muscle electrical activity.

EFFECT OF TWO DIFFERENT ATTACHMENTS ON THE SUPPORTING STRUCTURES (3)
They demonstrated that after rehabilitation with a new denture electromyographic parameters usually approach those observed in dentate subjects however, many factors play a role, such as denture mobility and subjective experience of wearing dentures.29-31The poor fit and the lack of stability of the denture clearly affects the masticatory function.32
Bite force measurements is one of the methods used for analyzing mas ticatory function. It is an indicator of the functional state of the masticatory system that results from the action of jaw elevator muscles modified by the craniomandibular biomechanics.33 It is often recorded with one or two transducers placed between pairs of opposing teeth during clenching.34 Maximum bite force level in complete denture wearers has been limited to an extent due to the sensitivity or pain of the mucoperiosteum covering the mandibular edentulous ridge which gets sandwiched in between the dentures and bone. However, the maximum bite force level is higher in patients wearing implant-retained mandibular overdentures than conventional dentures due to improved retention and stability of the prosthesis.35,36
To provide further insight on the masticatory capacity and the supporting structures of implant retained mandibular overdenture, this study was conducted to draw comparison between ball and socket attachment and GPS attachment regarding their effect on:• Crestal bone height and density surrounding
implants.• Electromyographic activity of temporalis and
masseter rmuscles.• Occlusal biting force.
MATERIALS AND METHODS
Patients Selection
Patients eligible for the study were male completely edentulous patients with age ranging between 55 to 65 years and for whom a decision had
already been made to incorporate dental implants for the treatment of complete edentulism. Following Misch37 rules of bone classification patients with bone density ranging from 850-1250 HU (D2) and bone height and width more than 10mm and 5mm respectively in the anterior region of the mandible (Division A) were included in the study. Exclusion criteria included severe maxillomandibular skeletal discrepancy, clenching habits, bruxism, tempromandibular joint disorders, smokers, drug abuse, history of head and neck radiation and systemic disorders that may prevent surgery, affect bone quality or contribute to bone resorption. Following this criteria twelve qualified patients were chosen and motivated to the treatment.
Prosthetic Procedures
Complete dentures were fabricated for all patients prior to implant installation to assure ideal implant placement in harmony with osseous anatomy, denture esthetics and abutment connection. For each patient upper and lower primary impressions were taken using alginate (Alginmax, Major Prodotti. Dentari SPA. Moncalieri. Italy) in stock trays and upper and lower secondary impressions were taken using medium body rubber base (Swiss TEC, Coltene, Whaledent, Altstatten, Switzerland) in specially constructed special trays. Occlusion blocks were fabricated on the poured master casts. Centric occluding relation was recorded following the conventional wax wafer technique. Upper casts were mounted on semi-adjustable articulator (Dentatus type ARH, AB, Dentatus, Stockholm, Sweden) according to face bow record (Dentatus face bow, Dentatus, Stockholm, Sweden) while the lower casts were mounted using the wax wafer centric occluding record. Setting up of teeth was done following modified lingualized occlusion using modified anatomic teeth (Vita-pan acrylic teeth, Vita Bad Sackingen-Germany).38 Waxed up denture was tried in the patient’s mouth, then flasked and processed into high impact heat cure
(4) Fardos N. RizkE.D.J. Vol. 60, No. 2
acrylic resin (Lucitone 199, Dentsply, York, PA-USA). Laboratory remounting was done before finishing the denture and occlusal discrepancies were adjusted.
Any necessary adjustments were carried out to eliminate occlusal interference and the denture was delivered to the patient. It was checked after twenty four and seventy two hours for any needed adjustment and to ensure that the patient was satisfied with esthetics, stability and retention of the denture. Following denture placement and patient adaptation, the mandibular denture was duplicated in clear acrylic resin (Vertex Rapid Simplified; Vertex-Dental BV, Zeist, The Netherlands) to act as a surgical guide for implant positioning to assure proper implants installation beneath the planned position which was determined by ideal denture contour and esthetics.
Surgical Procedures
For each patient two implants (Legacy I Implant Direct LLC, USA, Canada) with dimensions (3.7 x 13mm) were inserted bilaterally in the canine region at equal distance from the mid line, parallel to each other and perpendicular to the occlusal plane. All implants were placed by the same oral surgeon using surgical guide and following two stage surgical protocol. Covering screws were threaded into the implants which were left to heal for four months.
During the initial healing period (two weeks after surgery) no prosthesis was used over the implants so that early healing can occur without functional loading. After the two weeks period the tissue surface of the existing denture was relieved in the area overlying the installed implants. Resilient relining material (Permsoft Myerson Chicago IL. USA) was placed into the relieved areas to assure intimate tissue contact. Implants were left to integrate for four months and osseointegration of the implants was verified by digital panoramic radiographs.
Following the four months healing period patients were randomly divided into two equal groups according to the type of attachments they received.
Group I: Received ball and socket attachment (Im-plant Direct LLC, USA, Canada) in the form of
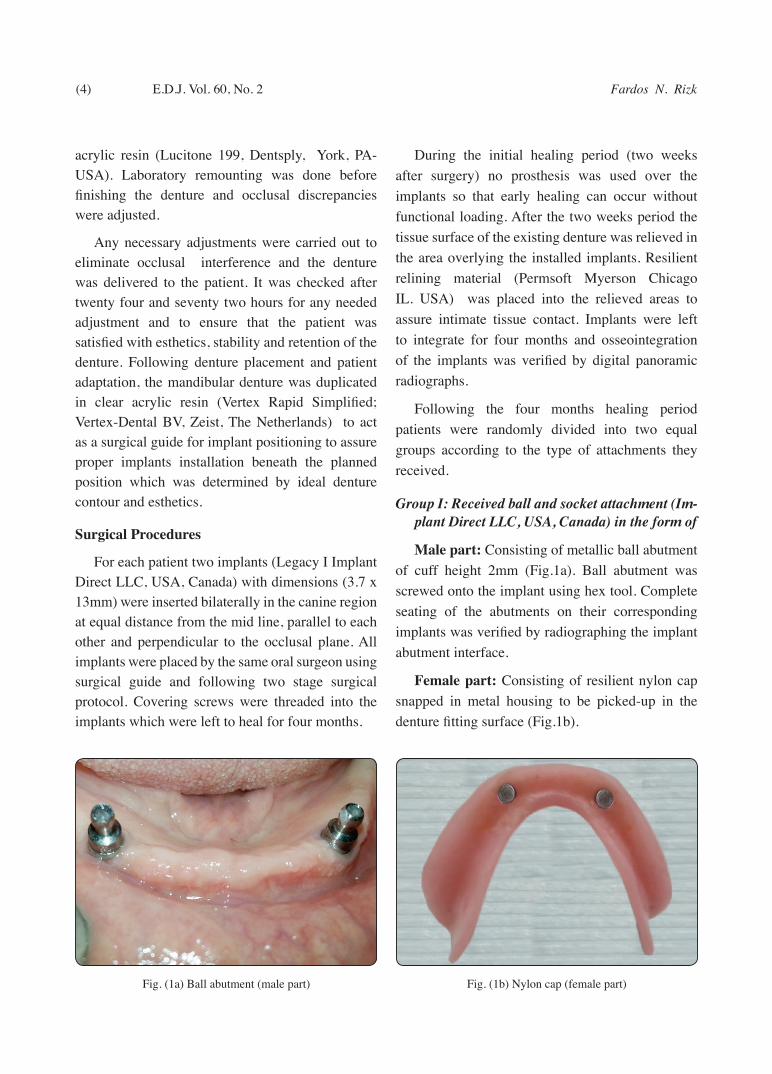
Male part: Consisting of metallic ball abutment of cuff height 2mm (Fig.1a). Ball abutment was screwed onto the implant using hex tool. Complete seating of the abutments on their corresponding implants was verified by radiographing the implant abutment interface.
Female part: Consisting of resilient nylon cap snapped in metal housing to be picked-up in the denture fitting surface (Fig.1b).
Fig. (1b) Nylon cap (female part)Fig. (1a) Ball abutment (male part)

EFFECT OF TWO DIFFERENT ATTACHMENTS ON THE SUPPORTING STRUCTURES (5)
Group II: Received GPS attachment (Implant Di-rect LLC, USA, Canada) in the form of
Female part: Consisting of metallic GPS abutment of cuff height 2mm (Fig.2a). The female part was screwed onto the implant using hex screw driver. Complete seating of the abutments on their corresponding implants was verified by radiographing the implant abutment interface.
Male part: Consisting of male clear nylon cap of standard retention. Using male seating tool, the male cap was firmly pushed into the empty metal housing to be picked-up in the fitting surface of the denture (Fig.2b).
Pick-up Procedures
The mandibular overdenture base was relieved to accommodate the newly inserted attachments. The denture was tried in the patient’s mouth to ensure complete seating. Any undercuts were blocked out using temporary filling (Litark, Lascod SpA-Vita L. Longo, Sesto F. no Firenze Italy). A mix of self cure acrylic resin (Lucitone 199; Dentsply, York, PA-USA)) was applied in the relieved region for direct pick- up of the nylon caps of ball and GPS attachments following close-mouth technique. Necessary adjustments were carried out to eliminate occlusal interference and the denture was delivered to the patient and checked after 24 and 72 hours for any needed adjustment and to ensure that the patient was satisfied with esthetics, stability and retention of the denture.
Follow-Up Evaluation Schedule
Evaluation was scheduled at the denture insertion, three, six and twelve months following denture insertion. At these intervals, patients return for assessment of implant, prosthesis’ function and standardized evaluation of his oral health. For each patient crestal bone height and density surrounding the implants were measured using cone beam computed tomography (Scanora 3D, Sorredex-Finland). Activity of the superficial masseter and anterior temporalis muscles was recorded using electromyographic device (Cadwell Excel High-Power EMG/EP device, USA). Maximum bite force was determined using occlusal force-meter (model GM, NaGONO Keiki Seisakusho, LTd, J. Morita Corporation, 33-18-3-Chome-Torumi-Cho Suita City, Osaka 564-8650, Japan).
1- Radiographic evaluation using cone beam computed tomography (CBCT)
Images were acquired using the Scanora 3D Imaging system (voxel size 133um-350 um) which allows the recording of linear bone height and density measurements of images. The personal
Fig. (2a) GPS abutment (female part)
Fig. (2b) GPS nylon cap (male part)
(6) Fardos N. RizkE.D.J. Vol. 60, No. 2
computer utilized was an Intel Core Duo- 2.13 Mhz-3.25 Gbites-21 inches flat screen 9 Hewlett-Packard Pavilion Elite m9200t series (Hewlett-Packard Pavilion Elite m9200t series USA).
Image Analysis
Linear measurements for evaluation of crestal bone height
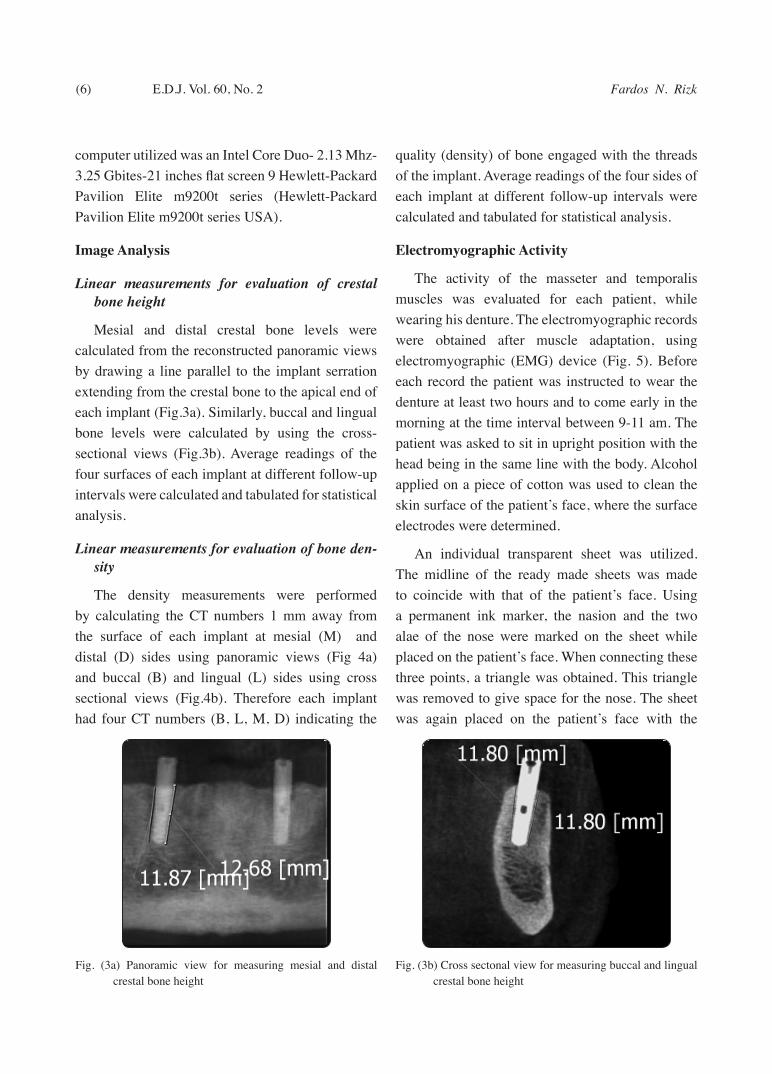
Mesial and distal crestal bone levels were calculated from the reconstructed panoramic views by drawing a line parallel to the implant serration extending from the crestal bone to the apical end of each implant (Fig.3a). Similarly, buccal and lingual bone levels were calculated by using the cross-sectional views (Fig.3b). Average readings of the four surfaces of each implant at different follow-up intervals were calculated and tabulated for statistical analysis.
Linear measurements for evaluation of bone den-sity
The density measurements were performed by calculating the CT numbers 1 mm away from the surface of each implant at mesial (M) and distal (D) sides using panoramic views (Fig 4a) and buccal (B) and lingual (L) sides using cross sectional views (Fig.4b). Therefore each implant had four CT numbers (B, L, M, D) indicating the
quality (density) of bone engaged with the threads of the implant. Average readings of the four sides of each implant at different follow-up intervals were calculated and tabulated for statistical analysis.
Electromyographic Activity
The activity of the masseter and temporalis muscles was evaluated for each patient, while wearing his denture. The electromyographic records were obtained after muscle adaptation, using electromyographic (EMG) device (Fig. 5). Before each record the patient was instructed to wear the denture at least two hours and to come early in the morning at the time interval between 9-11 am. The patient was asked to sit in upright position with the head being in the same line with the body. Alcohol applied on a piece of cotton was used to clean the skin surface of the patient’s face, where the surface electrodes were determined.
An individual transparent sheet was utilized. The midline of the ready made sheets was made to coincide with that of the patient’s face. Using a permanent ink marker, the nasion and the two alae of the nose were marked on the sheet while placed on the patient’s face. When connecting these three points, a triangle was obtained. This triangle was removed to give space for the nose. The sheet was again placed on the patient’s face with the
Fig. (3a) Panoramic view for measuring mesial and distal crestal bone height
Fig. (3b) Cross sectonal view for measuring buccal and lingual crestal bone height

EFFECT OF TWO DIFFERENT ATTACHMENTS ON THE SUPPORTING STRUCTURES (7)
nose passing through the created triangle space. The positions of the outer canthus of the eyes, the two angles of the mouth, the tragus of both ears and the most contractile sites of the four muscles were marked on the sheet. Holes were then drilled through the marks denoting the positions of the recording electrodes. In each subsequent visit, this sheet was used for accurate repositioning of the surface electrodes.
Six electrodes were used for each patient, four were fixed at the most contractile and palpable sites of the superficial masseter and anterior temporalis muscles of both right and left sites as predetermined on the sheet and two reference electrodes, one was fixed on the patient’s forehead and the last one on the skin of the neck. The inner sides of the electrodes were filled with a conductive gel and the electrodes were fixed on patient’s skin using adhesive tapes.
The activity of the four muscles was recorded in the following sequence: right masseter, right temporalis, left masseter and left temporalis. For each muscle, the patient was asked to perform the following:
Chew soft food approximately equal sized pieces of bananas (about one cubic centimetre in volume).
Chew hard food equal sized pieces of carrots (about one cubic centimetre in volume).
The patient was instructed to place one piece per time in the same position of one side and chew it. For each examination, three runs were made and the excel displays the mean and standard deviation for each parameter. Then the mean and standard deviation of the area were recorded. For each patient, the mean value of both right and left masseter and the mean value of both right and left temporalis muscles during chewing soft and hard food at different follow-up intervals were collected and tabulated for statistical analysis.Fig. (5) Electromyographic device
Fig. (4a) Panoramic view for measuring mesial and distal bone density
Fig. (4b) Cross sectonal view for measuring buccal and lingual bone density

(8) Fardos N. RizkE.D.J. Vol. 60, No. 2
3-Bite Force
The bite forces were measured with an occlusal force-meter instrument as shown in (Fig. 6).During testing, the patient was seated in upright position on a dental stool without a back rest. The occlusal force-meter with its disposable cap and four wood tongue depressors were positioned bilaterally (one in each side of the mouth) in correspondence of the mandibular second premolars/first molars with a symmetric disposition.39 (Fig.7).
Before the actual data collection, all patients were allowed to familiarize with the measurement procedure and the instruments. The peak force measurements were displayed on the screen of a computerized interface. The occlusal force-meter and four tongue depressors were positioned posteriorly in the mouth and the patients were asked to clench at different force levels which were displayed on the screen of the force-meter in Newton. The actual peak value was recorded for further quantitative analysis. Between each force level, a minute of rest was allowed. During performance, the patients were encouraged to maintain the desired force level for all the test period and a buzzer will sound if the biting force has exceeded the set-point. For each patient at each follow-up period, the mean of 10 records of the right and left sides was collected to be considered as one record for statistical analysis. 34
Statistical analysis
All the data was collected and tabulated. Statistical analysis was performed by Microsoft Office 2013 (Excel) and Statistical Package for Social Science (SPSS) version 20.
The significant level was set at P ≤ 0.05.
Kolmogorov-Smirnova and Shapiro-Wilk tests was used to assess data normality.
Independent t test was used to compare between groups with parametric data.
Mann Whitney test was used to compare between groups with non-parametric data.
RESULTS
I-Crestal Bone Height
There was decrease in crestal bone height surrounding the implants throughout the study period in both studied groups. However, group I with ball and socket attachment showed more crestal bone resorption than group II with GPS attachment with statistically significant difference between them through all intervals of follow-up period except at delivery to three months as shown in table I.
Fig. (6) Occlusal force-meter device with its disposable cap Fig. (7) Bite force- meter at its position on premolar-molar area in the patient’s mouth

EFFECT OF TWO DIFFERENT ATTACHMENTS ON THE SUPPORTING STRUCTURES (9)
II-Bone density
There was increase in bone density surrounding the implants throughout the study period in both studied groups with statistically none significant difference between them through all intervals of follow-up period as shown in table II.
III-Muscle activity
1-Masseter muscle
There was decrease in masseter muscle activity throughout the study period in both studied groups
with statistically none significant difference between them during eating soft and hard food through all intervals of follow-up period as shown in table III,IV.
2-Temporalis muscle
There was decrease in temporalis muscle activity throughout the study period in both studied groups with statistically none significant difference between them during eating soft and hard food through all intervals of all follow-up period as shown in table V,VI.
TABLE (I) Comparison between crestal bone height changes surrounding the implants in both studied groups at different intervals of follow-up period .
Group I (ball & socket attachment) Group II (GPS attachment) P value
Mean Difference (mm)
Sd. Mean Difference (mm)
Sd.
Delivery to 3months 0.1908 0.05334 0.1450 0.06789 0.079
3months to 6months 0.2433 0.11888 0.1567 0.03627 0.024*
6months to 12months 0.5142 0.06908 0.2950 0.04359 <0.001*
Delivery to 12months 0.9483 0.08548 0.5967 0.07703 <0.001*
Independent t test, *significant
TABLE (II) Comparison between changes in bone density surrounding the implants in both studied groups at different intervals of follow-up period.
Group I (ball & socket attachment) Group II (GPS attachment) P value
Mean Difference (HU)
Sd. (IQ) Mean Difference(HU)
Sd.(IQ)
delivery to 3months -29.9792(29.8) 8.35602(12.59) -38.9375(29.5) 31.14007(27.97) 0.843m
3months to 6months -36.7692(34.8) 8.50305(15.87) -34.7417(43.25) 35.74883(31.87) 0.551m
6months to 12months -66.7508(70.98) 19.16102(30.6) -59.3750(55.8) 14.47243(19.45) 0.29t
Delivery to 12months -133.4992(129.7) 28.36125(46.9) -133.0542(119.65) 31.39499(63.03) 0.97t
T independent t test, m Mann Whitney test

(10) Fardos N. RizkE.D.J. Vol. 60, No. 2
Masseter muscle activity while eating Soft food:
TABLE (III) Comparison between changes in masseter muscle activity with soft food in both studied groups at different intervals of follow-up period.
Group I (ball & socket attachment) Group II (GPS attachment) P value
Mean Difference(Amp)
Sd. Mean Difference(Amp)
Sd.
delivery to 3months 4.4250 0.86668 4.2000 0.84423 0.526
3months to 6months 4.3000 1.09045 4.3833 1.44022 0.874
6months to 12months 1.4333 0.53824 2.5417 3.30934 0.264
Delivery to 12months 10.2667 1.28865 11.125 3.1672 0.394
T independent t test
Masseter muscle activity while eating hard food:
TABLE (IV) Comparison between changes in masseter muscle activity with hard food in both studied groups at different intervals of follow-up period.
Group I (ball & socket attachment) Group II (GPS attachment) P value
Mean Difference (Amp)
Sd. Mean Difference (Amp)
Sd.
delivery to 3months 4.7000 0.60453 4.5917 0.90800 0.734
3months to 6months 4.5750 0.82476 5.3500 3.10557 0.412
6months to 12months 1.3583 0.50535 1.1000 0.57840 0.256
Delivery to 12months 10.5 0.87 11.04 2.949 0.548
T independent t test
Temporalis muscle activity while eating soft food:
TABLE (V) Comparison between changes in temporalis muscle activity with soft food in both studied groups at different intervals of follow-up period.
Group I (ball & socket attachment) Group II (GPS attachment) P valueMean Difference
(Amp)Sd. Mean Difference
(Amp) Sd.
delivery to 3months 5.2333 0.69978 5.0917 0.75854 0.6393months to 6months 5.1167 1.01250 4.6150 0.95507 0.2256months to 12months 0.8000 0.31042 1.1183 0.62322 0.128Delivery to 12months 11.0667 1.062 10.825 0.819 0.539
T independent t test

EFFECT OF TWO DIFFERENT ATTACHMENTS ON THE SUPPORTING STRUCTURES (11)
IV-Occlusal biting force
There was increase in biting force in both studied groups throughout the study period however, group II with GPS attachment showed increased mean
DISCUSSION
Only male patients participated in this study to avoid the effect of female hormonal changes on oral mucosa40and bone.41 Also, the maximum bite force is generally higher in men than in women because of men’s longer jaw dimensions. In addition, the greater bite force in men seems to correspond with
value of change in biting force in relation to group
I with ball and socket attachment with statistically
significant difference between them through all
intervals of follow-up period as shown in table VII.
the greater diameter and cross-sectional area of the type II fibres in the masseter muscle.42
CBCT was chosen in this study to determine the amount of marginal bone loss and density around the studied implants based on its reported accuracy and precision. 43 It is utilized successfully whenever direct measurements of bone height and density are
Temporalis muscle activity while eating hard food:
Table (VI) Comparison between changes in temporalis muscle activity with hard food in both studied groups at different intervals of follow-up period.
Group I (ball & socket attachment) Group II (GPS attachment)
P valueMean Difference (Amp)
Sd. Mean Difference
(Amp)Sd.
delivery to 3months 4.7167 0.49513 4.6250 0.55288 0.673
3months to 6months 3.9667 1.04389 4.6417 0.54682 0.06
6months to 12months 1.7250 1.25924 1.1583 0.60672 0.174
Delivery to 12months 10.408 0.814 10.425 0.506 0.953
T independent t test
TABLE (VII) Comparison between changes in occlusal biting force in both studied groups at different intervals of follow-up period.
Group I (ball & socket attachment) Group II (GPS attachment) P value
Mean Difference(N)
Sd. Mean Difference(N)
Sd.
delivery to 3months -19.3333 3.44656 -32.9167 4.42017 <0.001*
3months to 6months -20.4167 3.08835 -23.5833 3.20393 0.022*
6months to 12months -1.0000 0.60302 -1.9167 0.90034 0.008*
Delivery to 12months -40.75 4.351 -58.4167 3.3967 <0.001*
T independent t test, * significant

(12) Fardos N. RizkE.D.J. Vol. 60, No. 2
required due to the fact that periapical and panoramic radiography ignore the bone density and height at the buccal and lingual surfaces however, CBCT measures the crestal bone height and calculates the Hounsfield units at the four surfaces of the implant.44,45 It is precise and fast method which can be used to assess with high resolution digital images representing the trabecular structure in detail and allowing three-dimensional reconstruction of the bone structure to be achieved. Consequently, using CBCT for assessment of bone changes around the studied implants added accuracy to the results.
The amount of peri-implant bone loss has been found to be time related in the two groups. This bone reduction might be an immediate bone reaction after insertion of the prosthesis resulting from functional loading of implants. 43, 46 In this study the bone height changes remained within the clinically permissible range which may be attributed to many factors including proper patient selection, proper selection of implant site with good bone quality and quantity, following correct surgical and loading protocols,47,48 proper design, number and dimensions of implants, 49 proper prosthetic design,50 and finally reduction of occlusal load by following modified lingualzed concept of occlusion,38 sharing the load between the ridge and the implant and restricting the opposing occlusion to complete dentures.51,52
The decreased amount of crestal bone resorption with GPS attachment in comparison to ball and socket attachment might be attributed to the difference in the abutment designs of the two groups. In case of ball and socket attachment the abutment connected to the implant is the male part which forms lever arm of 2mm cuff height while in case of GPS attachment the abutment connected to the implant is the female part which transfers the fulcrum point close to the fixture thus reducing lever arm and torque and allowing less crestal bone resorption.53
Both groups showed increase in bone density with statistically none significant difference between
them. This agrees with other authors54,55 who found statistically significant increase in the bone density surrounding delayed loaded implants. They explained that this might be due to positive response of bone to load applied within its physiologic limit and adaptive capacity as new bone formation and active remodelling may be observed when the bone is mechanically stimulated during the first 6 months to one year of loading. These results are inconsistent with the findings of Quirynen et al.,56
who demonstrated an increase in density of peri-implant bone structures over six months to four years period after implant placement and explained this that the thickness and closeness of the bone trabeculae vary directly with the stresses transmitted to them thus, the proper distribution of the load falling on the implants might have enhanced the structural orientation of bone trabeculae and hence increased the bone density around the implants. These findings supported the findings of Misch 57
who reported higher bone density as well as reduced amounts of crestal bone loss around the delayed loaded implants and also the findings of Appleton et al.,58 who noted that progressively loaded implants had increased bone density as well as reduced amount of crestal bone loss.
Masster and temporalis muscles were chosen for representing the masticatory muscle activity since they are the largest and strongest masticatory muscles and thus play a major role in mandibular movement, this is in addition to their accessibility during recording. Records were made for the masseter and temporalis muscles bilaterally at each interval of follow-up, collected and the mean was calculated to avoid variation in the activity of the recorded muscles as a result of variation in the preferable chewing side for each patient.59,60
Besides, the activity in both sides will be nearly the same as the mandible is one unit, so for one side to move by the action of the muscles, the other side should also move.61

EFFECT OF TWO DIFFERENT ATTACHMENTS ON THE SUPPORTING STRUCTURES (13)
The decreased activity of masseter and temporalis muscles indicated improvement of the functional state of the masticatory system, because the muscles are able to do the same action with less electrical activity .i.e. less number of fibers participated performing the same function. This indicates that the patient was accommodated to the denture and could control it well to the extent that he did not need that much muscular activity to masticate either soft or hard food. This agrees with the findings of Perrez et al., 62 who stated that improved stability of the overdenture gives better chewing of soft and hard food and improves masticatory ability. None significant difference between both groups during chewing soft or hard food is explained by rapid muscle adaptation and achievement of patient’s comfort with both attachment designs. This is in agreement with Boucher et al., 63 who reported that the adaptive behavior for the patients, the learned skill of denture manipulation and forming a memory for the mandibular movements are very detective factors for improving the muscular activity.
Chewing hard food showed higher electromyographic activity of masseter and temporalis muscles than chewing soft food. This can be attributed to increasing the contractile force of the muscle and/or increasing the muscle fibers evoked during contraction as a result of increasing the resistance of the food. Tallgren 64 revealed this to reflex mechanism elicited providing a pressure sensitive proprioceptive response. This agrees with the results obtained by Nagasaw et al., 65 who found that chewing fresh raw carrots and peanuts showed higher activity than chewing kamaboko. This was also in accordance with Kapur, 66 who found that chewing crisp wafers showed higher activity than chewing soggy wafers.
Maximum bite force showed significant improvement in this study which was in agreement with other studies67-69 that reported significant increases in maximum bite force and chewing
performance in patients wearing implant supported overdenture. This marked increase in biting force is most likely related to improved denture stability and retention. The increased values of biting force with GPS in comparison to ball and socket attachment might be attributed to the improved retention of GPS in relation to ball and socket as proved by other studies.70,71
CONCLUSION
The following conclusions could be drawn from the results of this study:
1- GPS attachment is less destructive to crestal bone surrounding the implants.
2- Patients wearing overdentures retained by GPS attachment have higher biting force than patients wearing overdentures retained by ball and socket attachment.
3- There is no difference between GPS and ball and socket attachments in terms of muscle activity of masseter and temporalis muscles.
REFERENCES
1- Boerrigter EM, Stegenga B, Raghoebar GM, Boering G. Patient satisfaction and chewing ability with implant-retained mandibular overdentures: a comparison with new complete dentures with or without preprosthetic surgery. J Oral Maxillofac Surg 95;53:1167-1173.
2- Meijer HJ, Raghoebar GM, Van’t Hof MA, Geertman ME, Van Oort RP. Implant-retained mandibular overdentures compared with complete dentures; a 5-years’ follow-up study of clinical aspects and patient satisfaction. Clin Oral Implants 1999; 10:238-244.
3- Naert I, Gizani S, Vuylsteke M, Van Steenberghe D. A 5-year prospective randomized clinical trial on the influence of splinted and unsplinted oral implants retaining a mandibular overdenture: prosthetic aspects and patient satisfaction. J Oral Rehabil 1999;26:195-202.
4- Awad MA, Locker D, Korner-Bitensky N, Feine JS. Measuring the effect of intra-oral implant rehabilitation on health-related quality of life in a randomized controlled clinical trial. J Dent Res 2000; 79:1659-1663.

(14) Fardos N. RizkE.D.J. Vol. 60, No. 2
5- Awad MA, Lund JP, Shapiro SH, Locker D, Klemetti E, Chehade A, et al. Oral health status and treatment satisfaction with mandibular implant overdentures and conventional dentures: a randomized clinical trial in a senior population. Int J Prosthodont 2003; 16:390-396.
6- Heydecke G, Locker D, Awad MA, Lund JP, Feine JS. Oral and general health related quality of life with conventional and implant dentures. Community Dent Oral Epidemiol 2003;31:161-168.
7- Feine JS, Carlsson GE, Awad MA, Chehade A, Duncan WJ, Gizani S, et al. The McGill consensus statement on overdentures. Mandibular two-implant overdentures as first choice standard of care for edentulous patients. Gerodontology 2002;19:3-4.
8- Brian H, Williams, Kent T, Ochiai, Satoru Hojo, Russell Nishimura, Angelo A. Retention of maxillary implant overdenture bars of different designs. J Prosthet Dent 2001;86:603-7.
9- Sadowsky SJ. The implant-supported prosthesis for the edentulous arch: design considerations. J Prosthet Dent 1997; 78:28-33.
10- Wismeijer D, Van Waas MA, Vermeeren JI, Mulder J, Kalk W. Patient satisfaction with implant-supported mandibular overdentures. A comparison of three treatment strategies with ITI-dental implants. Int J Oral Maxillofac Surg 1997;26:263-7.
11- Menicucci G, Lorenzetti M, Pera P, Preti G. Mandibular implant-retained overdenture: a clinical trial of two anchorage systems. Int J Oral Maxillofac Implants 1998;13:851-6.
12- Takanashi Y, Pernord JR, Chehade A, Klemetti E, Savard A, Lund JP. Does a prosthodontist spend more time providing mandibular two-implant overdenture than conventional dentures? Int J Prosthodont 2002; 15: 397-403.
13- Cune M, Burgers M, Van Kampen F, de Putter C, Van Der Bilt A. Mandibular overdentures retained by two implants: 10-year results from a crossover clinical trial comparing ball-socket and bar-clip attachments. Int J Prosthodont 2010; 23: 310-317.
14- Cune MS, de Putter C, Hoogstraten J. Treatment outcome with implant retained overdentures: part I-clinical findings and predictability of clinical treatment outcome. J Prosthet Dent 1994; 72: 144-195.
15- Cune, M, Van Kampen, Van der Bilt A, Bosman F. Patient
satisfaction and preference with magnet, bar-clip and ball-socket retained mandibular overdentures: A cross-over clinical trial. Int. J. Prosthodont 2005; 18: 99-105.
16- Wittwer G, Adeyemo WL, Wagner A, Enislidis G. Computer-guided flapless placement and immediate loading of four conical screw-type implants in the edentulous mandible. Clin Oral Implants Res 2007; 18: 534-539.
17- Ganz SD: Conventional CT and cone beam CT for improved dental diagnostics and implant planning. Dent Implantol Update 2005; 16:89-95.
18- Rossi R, Morales RS, Frascaria M, Benzi R, Squadrito N. Planning implants in the esthetic zone using a new implant 3D navigation system. Eur J Esthet Dent 2010; 5: 172-188.
19- Loubele M, Van Assche N, Carpentier K, Maes F, Jacobs R, van Steenberghe D. Suetens P. Comparative localized linear accuracy of small-field cone-beam CT and multislice CT for alveolar bone measurements. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105:512-8.
20- Ludlow JB. Regarding ‘Influence of CBCT exposure conditions on radiation dose. Oral Surg, Oral Med, Oral Pathol, Oral Radiol, and Endod 2008 106: 627-628.
21- Viegas VN, Dutra V, Pagnoncelli RM, de Oliveira MG. Transference of virtual planning and planning over biomedical prototypes for dental implant placement using guided surgery. Clinical Oral Implants Research 2010; 21: 290-295.
22- Boerrigter EM, Geertman ME, Van Oort RP, Bouma J, Raghoebar GM, Van Waas MA, et al. Patient satisfaction with implant retained mandibular overdentures. A comparison with new complete dentures not retained by implants—a multicentre randomized clinical trial. Br J Oral Maxillofac Surg 1995; 33: 282-8.
23- Thomason JM, Lund JP, Chehade A, Feine JS. Patient satisfaction with mandibular implant overdentures and conventional dentures 6 months after delivery. Int J Prosthodont 2003; 16: 467-73.
24- Slagter AP, Bosman F, Van der Bilt A. Comminution of two artificial test foods by dentate and edentulous subjects. J Oral Rehabil 1993; 20: 159-76.
25- Fontijn-Tekamp FA, Slagter AP, Van Der Bilt A, Van ‘T Hof MA, Witter DJ, Kalk W, Jansen JA. Biting and chewing in overdentures, full dentures, and natural dentitions. J Dent Res 2000; 79: 1519-24.

EFFECT OF TWO DIFFERENT ATTACHMENTS ON THE SUPPORTING STRUCTURES (15)
26- Karkazis HC, Kossioni AE. Surface EMG activity of the masseter muscle in denture wearers during chewing of hard and soft food. J Oral Rehabil 1998;25:8-14
27- Nakamura Y, Sessle GJ. Neurobiology of mastication. From molecular to system approach. Tokyo: Elsevier Science; 1999.
28- Boucher C O, Hieckey J C, Zarb, G. A. Prosthodontic treatment for edentulous patients. 2th. Ed. C. V. Mosby Co. St. Louis , 1975.
29- Jemt T. Chewing patterns in dentate and complete denture wearers – recorded by light-emitting diodes. Swed Dent J 1981;5:199-205.
30- Jemt T, Karlsson S. Mandibular movements during mastication before and after rehabilitations with new complete dentures recorded by light-emitting diodes. Swed Dent J 1980;4:195–200.
31- Geertman M, Slagter A, Van’T Hof MA, Van Waas M, Kalk W. Masticatory performance and chewing experience with implant retained mandibular overdentures. J Oral Rehabil 1999; 26:7-13.
32- Fujimori T, Hirano S, Hayakawa I. Effects of a denture adhesive on mastication functions for complete denture wearers. J Med Dent Sci 2002; 49:151-156.
33- Duygu K, Arife D, Bulent B. Bite force and influential factors on bite force measurements: A literature review. Eur J Dent 2010;4:223-32.
34- Hagberg C. Assessment of bite force: a review. J Cranio-26. mandib Disord 1987; 1:162-169.
35- Fontijn-Tekampl FA, Slagter AP, vant Hof MA, Geertman ME, Kalk W. Bite forces with mandibular implant-retained overdentures. J Dent Res 1998;77:1832-39.
36- Rismanchian M, Bajoghli F, Mostajeran Z, Fazel A, Eshkevari S. Effect of implants on maximum bite force in edentulous patients. Journal of Oral Implantology 2009;35 (4).
37- Mish,C. 11. Classification of partially and completely edentulous arches in implant dentistry In: Contemporary implant dentistry. St. Louis. C.V. Mosby, 1993; 201-221.
38- Mish,C. Maxillary denture opposing an implant prosthesis: Hydroxyapatite augmentation and modified occlusal concepts. In: Contemporary implant dentistry. St.Louis.C.V.Mosby, 1999; 629-746.
39- Tortopidis D, Lyons MF, Baxendale RH. A coustic myography 32. electromyography and bite force in the masseter muscle. J Oral Rehabil 1988; 25:940-945.
40- Hatch JP, Shinkai RS, Sakai S. Determinants of 24. masticatory performance in dentate adults. Arch Oral Biol 2001; 46:641-648.
41- Tortopidis D, Lyons MF, Baxendale RH. The variability of bite force measurement between sessions indifferent positions within the dental arch. J Oral Rehabil 1998; 25:681-686.
42- Shinogaya T, Bakke M, Thomson CE. Effects of ethnicity, gender and age on clenching force and load distribution. Clin Oral Investig 2001; 5:63-68.
43- Hohlweg MC, Metzger b T, Kummerc D, Schulze B. Hohlweg- Majert B. Article in press as: Hohlweg-Majert B et al., Morphometric analysis- Cone beam computed tomography to predict bone quality and quantity, Journal of Craniomaxillofacial Surg 2010; 10:1016.
44- Shahlaie M, Gantes B, Schulz E, Riggs M, Crigger M. Bone density assessments of dental implant sites; Quantitative computed tomography. Int.J.Oral Maxillofac.Implants 2003; 18:224-31.
45- Song Y.D, Jun SH, Kwon JJ. Correlation between bone qualities evaluated by cone-beam computerized tomogra-phy and implant primary stability. Int.J.Oral Maxillofac.Implants 2009; 24:59-64.
46- Jonkman RE, van Waas MA, Plooij J, Kalk W. Measuring mandibular ridge reduction on oblique cephalometric ra-diographs. J Craniomaxillofac Surg 1991;19: 27-30.
47- Burns DR. Mandibular implant overdenture treatment: consensus and controversy. J Prosthodont 2000; 9:37–46.
48- Wolfinger GJ. Implant prosthodontic and restorative com-plications. Int J Oral Maxillofac Implants 2003; 18:766-7.
49- Chiapasco M, Abati S, Romeo E, Vogel G. Implant-retained mandibular overdentures with Branemark System MK II implants. A prospective comparative study between delayed and immediate loading. Int J Oral Maxillofac Implants 2001; 16:537–46.
50- Rungcharassaeng K, Lozada J, Kan JIK and Kim J. Peri implant tissue response of immediate loaded threaded HA coated implants. 1 year results. J Prosthet Dent 2002; 87:173-81.
51- Romanos GE, Toh CG, Siar CH and Swaminathan D. Histological and histomorphometric evaluation of peri-implant bone subjected to immediate loading: An experimental study with Macaca fascicularis. Int J Oral Maxillofac Implants 2002; 17: 44-51.

(16) Fardos N. RizkE.D.J. Vol. 60, No. 2
52- Phay YM, Tan BTK. Rehabilitation of the edentulous mandible with implant-supported overdentures using prefabricated telescopic copings Singapore Dental Journal 2005;27:30-5.
53- Jingade RK, Rudraprasad IV, Sangur R. Biomechanics of dental implants: A FEM study. J. Indian Prosthodont.Soc 2005; 5:18-22.
54- Romanos GE, Toh CG, Siar CH, Swaminathan D. Histological and histomorphometric evaluation of peri-implant bone subjected to immediate loading: An experimental study with Macaca fascicularis. Int J Oral Maxillofac Implants 2002; 17: 44-51.
55- Page ME. Systemic and prosthodontic treatment to prevent bone resorption in edentulous patients. J Prosthet Dent 1975; 33: 483-488.
56- Quirynen M, Naert I, Van Steenberghe D, Nys L. A study of 589 consecutive implants supporting complete fixed prosthesis. Part I: Peridontal aspects. J Prosthet. Dent 1992; 68: 655-663.
57- -Misch C. Dental implants prosthetics. Mosby Co, St Louis, Chicago, Toronto, 2005.
58- Appleton RS, Nummikoski PV, Pigno MA, Cronin RJ, Chung KH. A radiographic assessment of progressive loading on bone around single osseointegrated implants in the posterior maxilla. Clin Oral Implants Res 2005; 16: 161-167.
59- Pond LM, Barghi N, Barnwell GM. Occlusion & chewing side preference. J Prosthet Dent 1986; 55: 498-500.
60- Delvin H, Wastell DG, Duxbury AJ, Grant AA. Chewing side preference and muscle activity incomplete denture wearing subjects. J Prosthet Dent 1987; 15:23.
61- Eriksson RO, Thornell LE. Histochemical and morphological muscle-fiber characteristics of the human masseter, the medical pterygoid and the temporal muscles. Archs Oral Biol 1983; 28:781.
62- Perrez P, Kapur KK. Occlusal adjustment, base retention and fit on masseter muscle activity and masticatory performance. J Prosthet Dent 1985; 53:69.
63- Boucher CO, Hieckey J C, Zarb G A. Prosthodontic treatment for edentulous patients. 2th. Ed. C. V. Mosby Co. St. Louis , 1975.
64- Tallgren A, Tryde G. Chewing and swallowing activity of masticatory muscles in patients with a complete upper and a partial lower denture. J. Oral Rehab 1991; 18: 285.
65- Nagasawa T, Okane H, Tsuro H. The role of the periodontal ligament in overdenture treatment. J Prosthet Dent 1979; 42:12.
66- Kapur KK. Studies of biologic parameters for denture design, part I: Comparison of masseter muscle activity during chewing crisp and soggy wafers in denture and dentition groups. J Prosthet Dent 1975; 33:242.
67- Fueki K, Kimoto K, Ogawa T, Garrett NR. Effect of implant-supported or retained dentures on masticatory performance: a systematic review. J Prosthet Dent 2007; 98:470-477.
68- Bakke M, Holm B, Gotfredsen, K. Masticatory function and patient satisfaction with implant-supported mandibular overdentures: a prospective 5-year study. Int J Prosthodont. 2002; 15: 575-581.
69- Stellingsma K, Slagter AP, Stegenga B, Raghoebar GM, Meijer, HA. Masticatory function in patients with an extremely resorbed mandible restored with mandibular implant-retained overdentures: comparison of three types of treatment protocols. J Oral Rehabil 2005; 32: 403-410.
70- Kleis WK, Kammerer PW, Hartmann S. A comparison of three different attachment systems for mandibular two-implant overdentures: one-year report. Clin Implant Dent Relat Res. 2010; 12: 209-218.
71- Sadig W. A comparative in vitro study on the retention and stability of implant-supported overdentures. Quintessence Int. 2009; 40: 313-322.