efqm excellence model - iese blog networkwebprofesores.iese.edu/mba/health/master/sessions/efqm...
TRANSCRIPT

Prof. M Rosenmöller IESE
EFQM Model in Health Care 1
Universidad de Navarra
EFQM Excellence Model
SANIT – Management in the Health Sector 2004
(Case Hospital Comarcal de Igualada)
Prof. Magdalene Rosenmöller
14University of Navarra
EFQM EFQM ExcellenceExcellence ModelModelEuropean Quality Award Model (www.efqm.org)
Structure Processes Results

Prof. M Rosenmöller IESE
EFQM Model in Health Care 2
15University of Navarra
The EFQM Model (efqm)
• Is based on a self assessment • Conclusions are as good as the analysis done• The focus is on processes• Is client oriented• Uses the means of continuous improvement
(benchmarking or reengineering of processes)• Is based on group work (with people from different
departments
16University of Navarra
The EFQM Model (efqm)
• Allows to integrate (not substitute) other quality improvement initiatives.
• Is focused on results and on facilitators. It´s not only about to do things, but look at the effects of it.
• Depends on the level of leadership in the organisation –(and gives details on how to evaluate this level)
• Promote the continuous improvement, instead of compliance with some standards.
• Expects the institutions to demonstrate positive tendencies.

Prof. M Rosenmöller IESE
EFQM Model in Health Care 3
17University of Navarra
The health sector is somehow difficult
• Bases of TQM– Dominance of management aspects over
technical ones– Rational process of decision making
• Challenges in Health– Conceptual aspects– Structural aspects– Implementation aspects
18University of Navarra
Problems and Challenges of the implementation
of the EFQM model in Hospitals
–Conceptual Aspects–Structural Aspects–Implementation Aspects

Prof. M Rosenmöller IESE
EFQM Model in Health Care 4
19University of Navarra
Conceptual Aspects
• Professionals are not identifying with the way the efqm model is seeing the company (or institution)
• Quality Vision • Physicians think they are always doing quality work • Relation with other quality initiatives• The models and the system of auto evaluation is only
a means to make a diagnosis and establish the base line situation.
• TQM is seen as a way to reduce costs.
20University of Navarra
Conceptual Aspects
• Professionals are not identifying with the way the efqm model is seeing the company (or institution)
• Quality Vision • Physicians think they are always doing quality work. • Relation with other quality initiatives• The models and the system of auto evaluation is only
a means to make a diagnosis and establish the base line situation.
• TQM is seen as a way to reduce costs
• A health centre is not a business and cannot be managed as if itwould be one.
• The physician – patient relationship is very special.• The professional engagement of the physicians is to always act
in the best interest of the patient.• Health is a completely different product to those ¨manufactured
by other companies.• It is unacceptable that the management vision is above the
clinical (technical) vision.

Prof. M Rosenmöller IESE
EFQM Model in Health Care 5
21University of Navarra
Conceptual Aspects
• Quality Vision • Physicians think they are always doing quality
work. • Relation with other quality initiatives• The models and the system of auto
evaluation is only a means to make a diagnosis and establish the base line situation.
• TQM is seen as a way to reduce costs.
Different perception on what quality means:• Quality in the client perspective• Quality in the provider perspective• Quality in the funding institutions´perspective
Usually it is the client, who in the end defines quality, but inhere he has limited information and does not understand it
Internal quality vision.
22University of Navarra
Conceptual Aspects
• Physicians think they are always doing quality work.
• Relation with other quality initiatives• The models and the system of auto
evaluation is only a means to make a diagnosis and establish the base line situation.
• TQM is seen as a way to reduce costs.
There is not a unique way to do things right. The physician redefines it in each moment. The acceptable practices not a point but an area.
Start quality improvement actions in the clinical area – means that we are doing now is not the best quality......
Don´t even start to think this !!!
Do the minimum necessary
Not do anything
inappropriate
Area of acceptable practices
Prof. M Rosenmöller IESE
EFQM Model in Health Care 6
23University of Navarra
Conceptual Aspects
• Relation with other quality initiatives• The models and the system of auto
evaluation is only a means to make a diagnosis and establish the base line situation.
• TQM is seen as a way to reduce costs
• Professional qualifications, (licenses, etc.. )• Certification of continuous education • Protocols• Commissions• Audits• Peer review• Accreditations• ........
24University of Navarra
Conceptual Aspects
• The models and the system of auto evaluation is only a means to make a diagnosis and establish the base line situation.
• TQM is seen as a way to reduce costs
• TQM is not quick way to solve problems.
• The objective is to establish a better (common) knowledge of the functioning of the institutions and the subsequent identification of improvement areas.

Prof. M Rosenmöller IESE
EFQM Model in Health Care 7
25University of Navarra
Conceptual Aspects
• TQM is seen as a way to reduce costs
• Concept of “value” for the client.
• Diminish costs may result in a better perception of the value.
• Back to the different vision what is means to do it well (quality) in a hospitals.
26University of Navarra
Structural Aspects• The responsibility for the health of the patient is with the
physicians not with the manager.• In a hospitals there are 2 organisations – not always
compatible: the hospital and the physicians.• Complex structures and highly hierarchical with subcultures.• Special patient – physician relation• Professional autonomy (exist as well in universities)• Lack of (formal) authority of the manager over the physician• Conflict of the TQM philosophy and the management of
health institutions.

Prof. M Rosenmöller IESE
EFQM Model in Health Care 8
27University of Navarra
Implementation Aspects• Need to know TQM in order to be able to implement
it with success. The experience in training is important.
• Need to focus on the clients of the institutions and their needs.
• Perception that the professionals will loose with TQM – turn to be very critical
• The manager can loose as well: power goes to the improvement groups
28University of Navarra
Implementation Aspects
• Assure a ambience of “empowerment”.• The concept of measurement is not well
established in health management• Mostly the focus is on non clinical aspects,
which are the most accessible, but ignoring the most critical activity : health care provision.
• All problems inherent of bad project management.

Prof. M Rosenmöller IESE
EFQM Model in Health Care 9
29University of Navarra
Different Quality Strategies
• Accreditation• Certification• Peer Review• Clinical Guidelines• Performance Indicators• Patient SurveysOthers – External Mechanism• ISO certification• EFQM – European Foundation for Quality
Management
30University of Navarra
Quality in the HITs• Spain
– Catalonia first introducing quality indictors– 1998 Plan of Quality Improvement
• incl monitoring and incentives (prospective payment)– Accreditation
• UK– Internal market to improve quality of services provided– Emphasis on measuring and improving quality standards– 1998 A First Class service: Quality in the new NHS– June 1999 – 6 main clinical indicators
• death J30 post op; emergency readmission (hip fracture > 65);• inpatient waiting lists/1000 pop., • 5y survival breast/cervical cancer
New method of clinical governance: NICE – National Institute for Clinical ExcellenceCHImP – Commission for Health improvement
Accreditation - hospital standards, …• Germany
– Contracts including quality assurance measures– Licensing of medical services– Länder & ‘self administration’ – representation of hospitals and professionals

Prof. M Rosenmöller IESE
EFQM Model in Health Care 10
31University of Navarra
QUALITY OF CARE, PATIENT ORIENTATION, INFORMATION TO PATIENTS AND
PROFESSIONALS.
a) Approval and regulation of pharmaceuticals.
b) Trained professionals.
c) Quality assurance systems:
- Approval of safety
- Health Technology Assessment
- Use of guidelines on effectiveness
- Basic training
- System of licensing/revalidation
e) Internal and external performance.
Overview on Quality of Care
32University of Navarra
QUALITY OF CARE: AN OVERVIEW
Definitions

Prof. M Rosenmöller IESE
EFQM Model in Health Care 11
33University of Navarra
QUALITY OF CARE: AN OVERVIEW
Sources: Saturno et al. 1994, NHS 1997, European Commission 1998, David et al. 2001 and Oxford Handbook of Public Health 2001.
Dimensions
34University of Navarra
QUALITY OF CARE: AN OVERVIEW
Source: European Commission 1998
Levels of analysis

Prof. M Rosenmöller IESE
EFQM Model in Health Care 12
35University of Navarra
QUALITY OF CARE: AN OVERVIEW
Source: "The Quality of Care: How can it be assessed?" in Donabedian (1988;1744)
Levels of analysis
36University of Navarra
Structure: This denotes the attributes of the settings in which care occurs. Structure includes:
•Material resources (facilities, equipment and money)
•Human resources (number and qualifications of personnel)
•Organizational structure (medical staff organization, methods of peer review, methods of reimbursement).
Process: It denotes what is done in giving and receiving care. Process includes the patient’s activities in seeking care and carrying it out as well as the practitioner’s activities in making a diagnosis and recommending or implementing treatment.
Outcome: refers to what results are achieved (performance).
QUALITY OF CARE: AN OVERVIEW
The assessment of quality of care (Donabedian)

Prof. M Rosenmöller IESE
EFQM Model in Health Care 13
37University of Navarra
System performance done at national level, European level and global level. Issues addressed include: the general environment of the country, system planning and financing and resource allocation, legislation, other regulatory mechanisms, health priorities, professional recognition and overall quality management.
Organisational and Clinical level of performance there is a wide variety of mechanisms which carry out assessment. There are two different approaches: External Assessment and Internal Assessment.
External Assessment consists of external inspection to ensurepublic accountability, transparency, self regulation, qualityimprovement and value for money.
Internal approaches are used inside healthcare organizations and focus on bringing change from within.
QUALITY OF CARE: AN OVERVIEW
Measurement Tools
38University of Navarra
• The International Organization for Standardization (ISO) model provides standards against which organizations or functions may be certificated by accredited auditors.
• The European Foundation for Quality Management (EFQM)model is a framework for self-assessment and it is also used by facilities applying for external review in order to achieve the European Quality Award or national awards.
• The Accreditation model is a voluntary procedure external to an establishment, for the purpose of obtaining public and peer recognition of the quality of that establishment.
• The Peer review or Visitatie model of clinical departments consists of standards based on-site survey conducted by medical professionals in order to assess the quality of professional performance of peers.
•The Registration and licensing statutory model consists of programmes to ensure that professional staff or provider organizations achieve minimum standards of competence.
QUALITY OF CARE: AN OVERVIEW
Measurement Tools: External Assessment
Prof. M Rosenmöller IESE
EFQM Model in Health Care 14
39University of Navarra
Internal approaches to performance at an institutional level include notions of corporate performance such as:
• Patients’ rights
• Risk management
• Benchmarking
• Clinical governance
• Clinical measures at the micro level: clinical audit of evidence-based processes, quality teams and quality circles, continuous quality improvement, and numerical outcomes indicators of performance.
QUALITY OF CARE: AN OVERVIEW
Measurement Tools: Internal Assessment
40University of Navarra
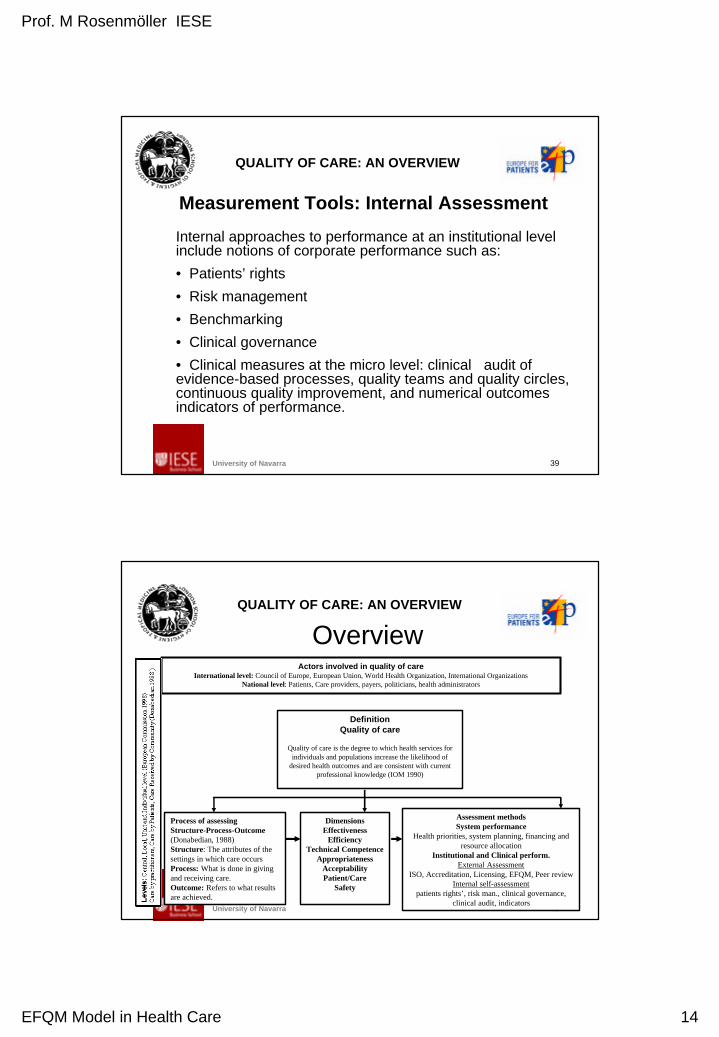
QUALITY OF CARE: AN OVERVIEW
Actors involved in quality of care International level: Council of Europe, European Union, World Health Organization, International Organizations
National level: Patients, Care providers, payers, politicians, health administrators
DefinitionQuality of care
Quality of care is the degree to which health services for individuals and populations increase the likelihood of
desired health outcomes and are consistent with current professional knowledge (IOM 1990)
Process of assessingStructure-Process-Outcome(Donabedian, 1988)Structure: The attributes of the settings in which care occurs Process: What is done in giving and receiving care.Outcome: Refers to what results are achieved.
Dimensions Effectiveness
EfficiencyTechnical Competence
AppropriatenessAcceptabilityPatient/Care
Safety
Assessment methods System performance
Health priorities, system planning, financing and resource allocation
Institutional and Clinical perform.External Assessment
ISO, Accreditation, Licensing, EFQM, Peer reviewInternal self-assessment
patients rights’, risk man., clinical governance, clinical audit, indicators
Overview