ehva project overview · ehva jan2016-dec2020 4 28 million euros 22 million euros from the european...
TRANSCRIPT
This project has received funding from the European Union’s horizon 2020 research and innovation programme under grant agreement No 681032.
EHVA Project Overview
1

EHVA Consortium
2
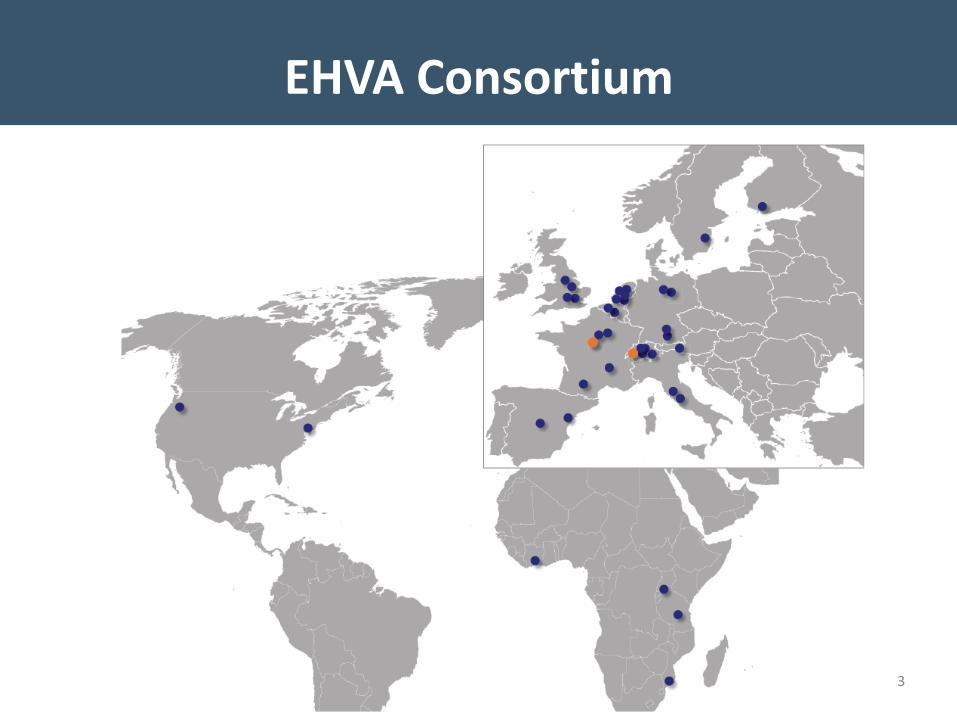
39 partners 11 countries3 continents
Infinite enthusiasm spanning basic, clinical, biostatistical and
community disciplines
EHVA Consortium
3

EHVA Jan2016-Dec2020
4
28 million Euros22 million Euros from
the European Commission(Grant nr 681032)
6 million Euros from the Swiss government for
the Swiss partners (Grant nr 15.0337).
Primary Goals
• To Develop a Multidisciplinary Vaccine Platform (MVP) in the fields of Prophylactic and Therapeutic HIV Vaccines
• To move at least two novel prophylactic vaccine candidates to clinical development
• To identify immune correlates associated with the control of HIV replication following immunological intervention
• To establish a strong scientific basis for further development of EHVA vaccine candidates in larger clinical trials
5
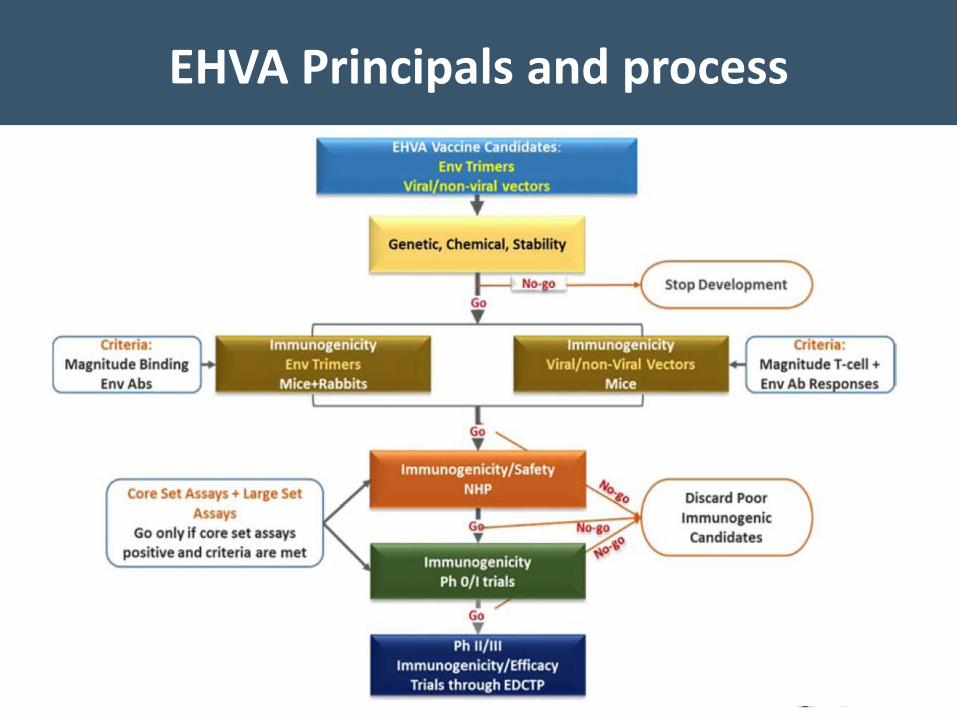
EHVA Principals and process
6
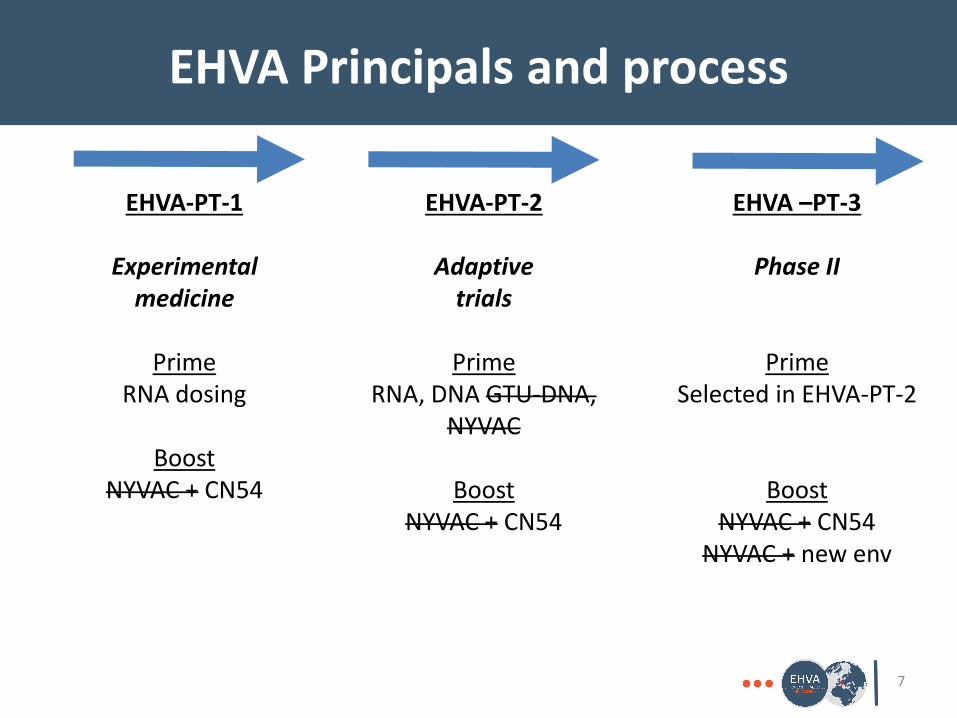
EHVA Principals and process
7
EHVA-PT-1
Experimental medicine
Prime RNA dosing
BoostNYVAC + CN54
EHVA-PT-2
Adaptive trials
PrimeRNA, DNA GTU-DNA,
NYVAC
BoostNYVAC + CN54
EHVA –PT-3
Phase II
PrimeSelected in EHVA-PT-2
BoostNYVAC + CN54
NYVAC + new env
EHVA T01 Trial
8
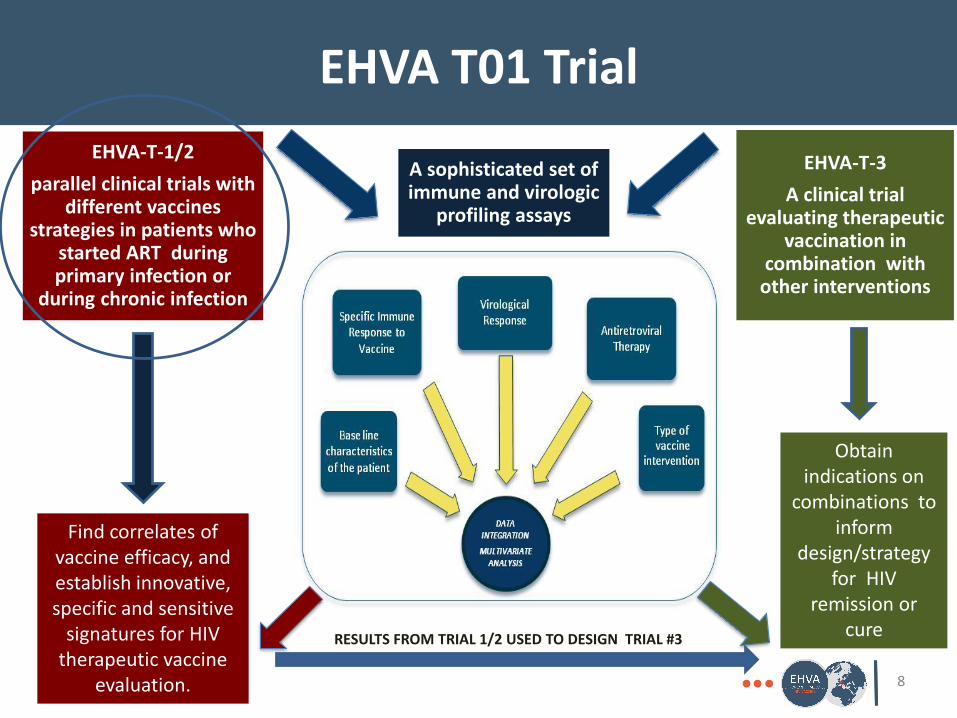
A sophisticated set of immune and virologic
profiling assays
EHVA-T-1/2
parallel clinical trials with different vaccines
strategies in patients whostarted ART duringprimary infection or
during chronic infection
Find correlates of vaccine efficacy, and establish innovative, specific and sensitive
signatures for HIV therapeutic vaccine
evaluation.
EHVA-T-3
A clinical trial evaluating therapeutic
vaccination in combination with
other interventions
Obtain indications on
combinations to inform
design/strategy for HIV
remission or cure
RESULTS FROM TRIAL 1/2 USED TO DESIGN TRIAL #3
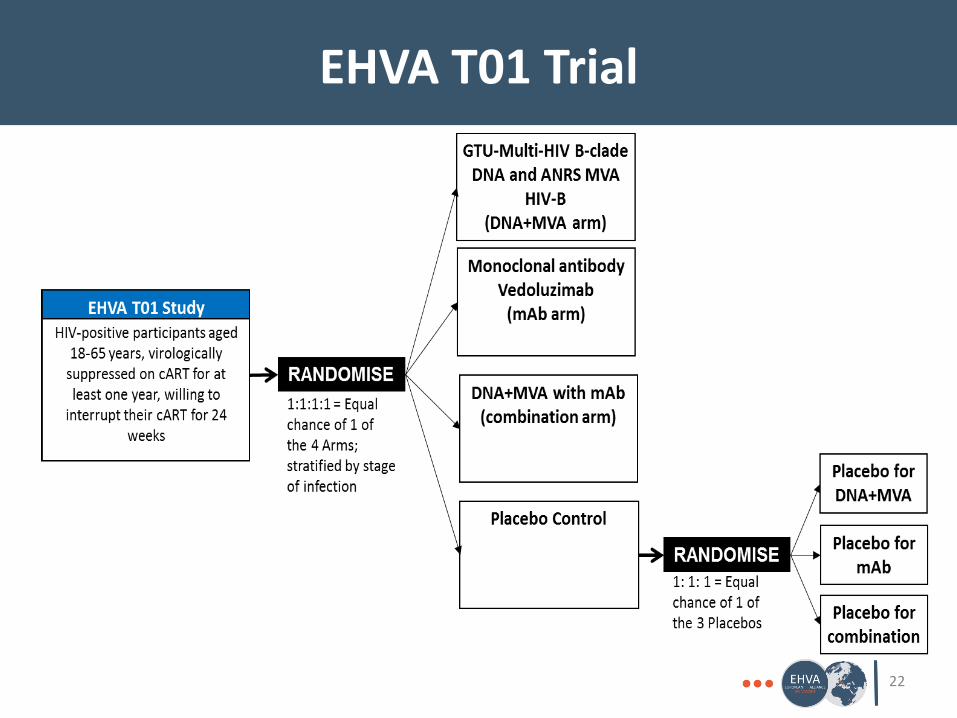
EHVA T01 Trial
A Phase I/II randomised therapeutic HIV vaccine trial in individuals who
started antiretrovirals during primary or chronic infection
9

EHVA T01 Trial
10
EHVA T01 Trial
11
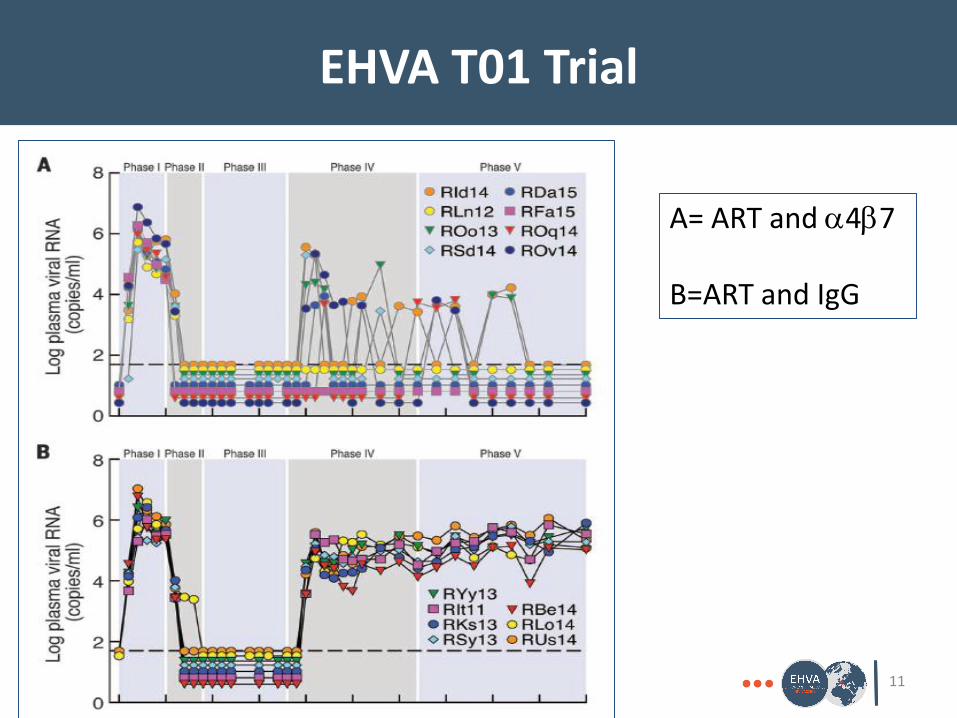
A= ART and a4b7
B=ART and IgG
EHVA T01 Trial
A Phase I/II randomised therapeutic HIV vaccine trial, alone and in
combination with vedolizumab, in individuals who started antiretrovirals
during primary or chronic infection
12
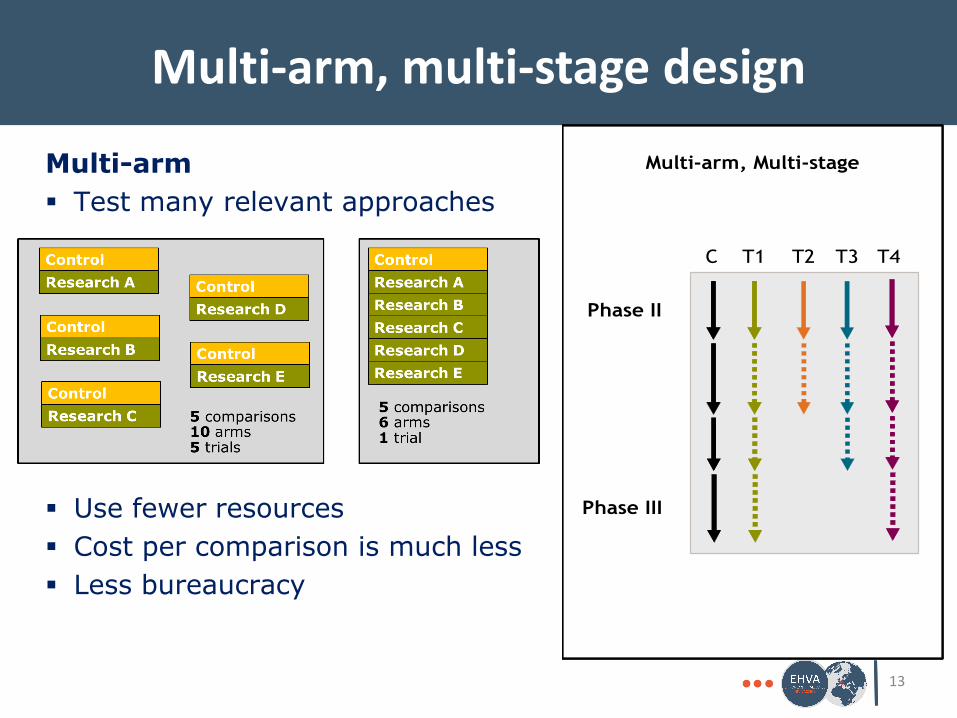
Multi-arm, multi-stage design
13
Multi-arm
Test many relevant approaches
Use fewer resources
Cost per comparison is much less
Less bureaucracy
Multi-arm, Multi-stage
T2 T3T1C T4
Phase II
Phase III
Multi-arm, Multi-stage
T2 T3T1C T4
Phase II
Phase III
EVHA T01 Hypothesis
14
Therapeutic vaccination will induce de novo immune responses and boost existing responses to improve the control of HIV replication
A clinically relevant viral load response to vaccine is defined as a delay to rebound of at least 10,000 copies/ml, confirmed
Vedolizumab acts through a different mechanism to limit the viral replication and it is very likely that these two interventions will be synergistic
Primary outcome measures
15
• Efficacy:
Confirmation of HIV RNA ≥ 10,000 copies/ml on a separate sample
Resuming antiretroviral therapy for any reason over a period of 24 weeks
Safety:
A clinical decision to discontinue the regimen for an adverse event that is considered related to product.
Secondary outcome measures
16
• Virological: Level of HIV total DNA Cell Associated (CA) HIV RNA Quantification
Immunological: Response rate, magnitude and polyfunctionality of
vaccine induced CD4 and CD8 T-cell responses
Safety: ≥ severe solicited AEs; AEs leading to interruption AE leading to resuming treatment during the ATI Time to VL suppression after restarting ART SAEs, other AEs
Selected inclusion criteria
17
HIV-1-infected, aged 18 – 65 at screening, >50kg
Nadir CD4 count > 300 CD4 count > 600, Viral load <50 at screening Started cART after 2009 and on cART for at least
one year prior to screening
Willing to take precautions to prevent onward transmission during ATI
Willing to avoid pregnancy
Selected exclusion criteria
18
• HIV-2 infection (either isolated or associated with HIV-1) or receipt of previous HIV vaccines
• VL >200 copies/ml on 2 occasions in the 12 months prior to screening, previous interruptions in cART or virologicalfailure with resistance
• Current medical conditions or lab abnormalities, including active infection or presence of pathogenic bacteria or parasites in the stool, active hep B or C
• Past history of PML, cardiac, neurological, cancer, severe reaction to vaccination
• Family history of rheumatoid arthritis
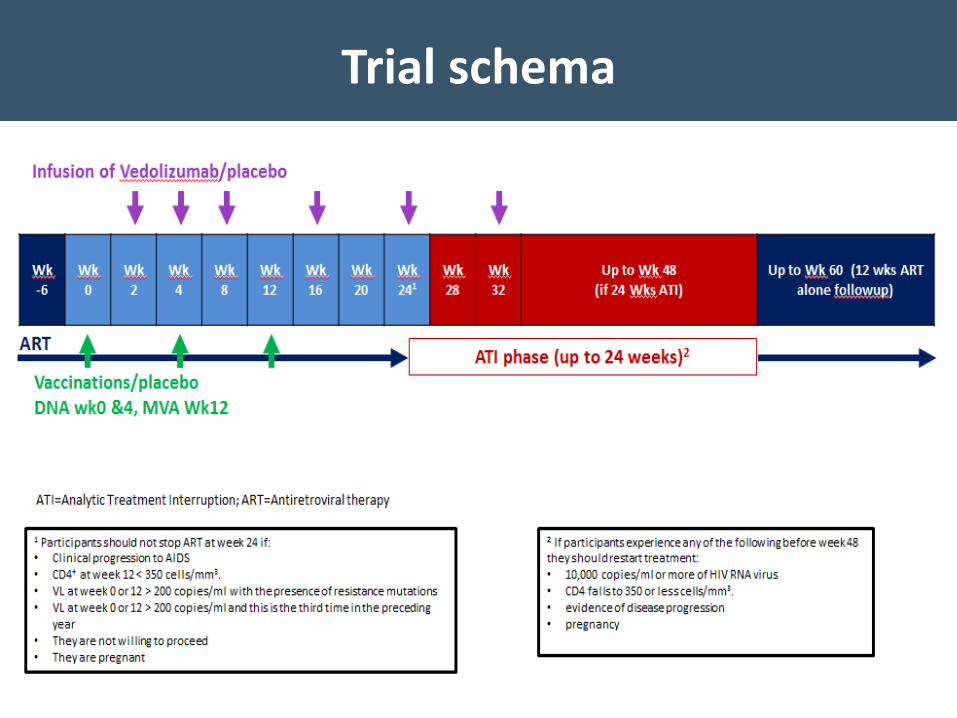
Trial schema
19
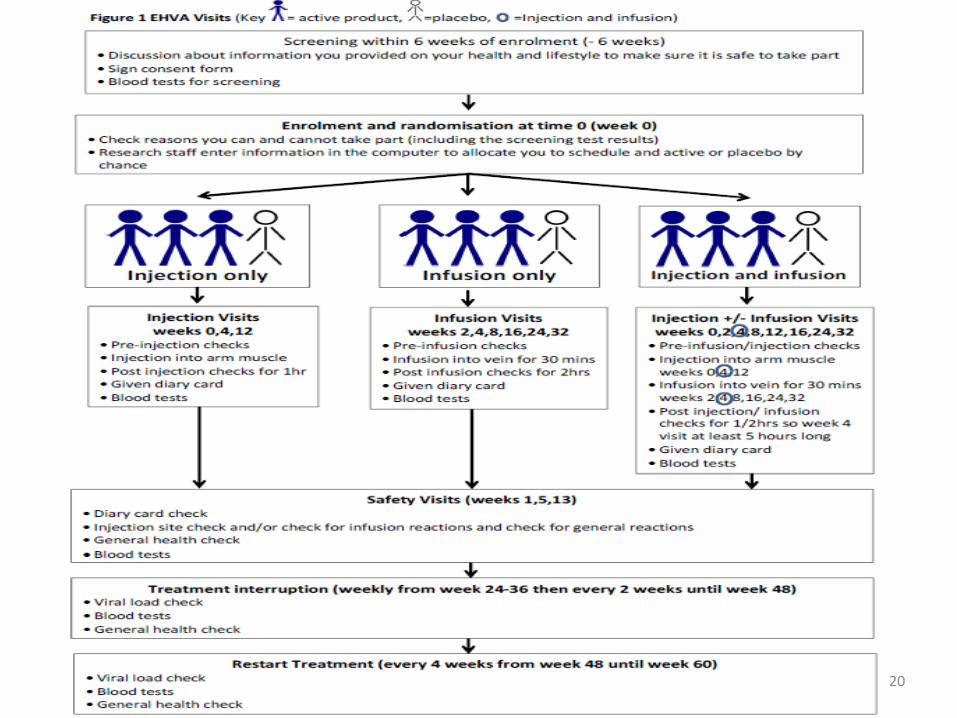
Trial schema – add PIS diagram
20
EHVA T01 Trial Size
• 88-192 participants will be enrolled across the 6 centers and randomised to active product or placebo in a ratio of 3:1 within each schedule
• 4-arm, 2-stage design with an interim analysis when 11 participants in the placebo group resume treatment Expected after 88 participants have been enrolled, so
there will be a pause in enrolment when n=88
• The final sample size will depend on how many arms proceed beyond the interim analysis
21
EHVA T01 Trial
22
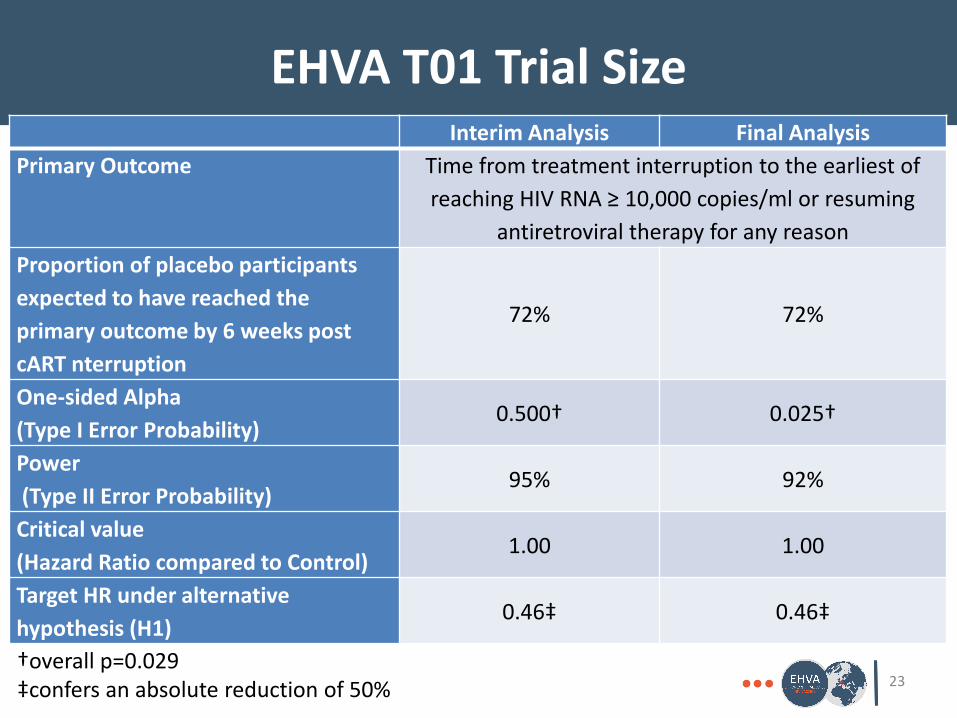
EHVA T01 Trial Size
23
Interim Analysis Final Analysis
Primary Outcome Time from treatment interruption to the earliest of
reaching HIV RNA ≥ 10,000 copies/ml or resuming
antiretroviral therapy for any reason
Proportion of placebo participants
expected to have reached the
primary outcome by 6 weeks post
cART nterruption
72% 72%
One-sided Alpha
(Type I Error Probability)0.500† 0.025†
Power
(Type II Error Probability)95% 92%
Critical value
(Hazard Ratio compared to Control)1.00 1.00
Target HR under alternative
hypothesis (H1)0.46‡ 0.46‡
†overall p=0.029‡confers an absolute reduction of 50%

EHVA T01 Organization
• Trial Sponsor: Inserm-ANRS, France• Clinical Centers:
France: 3 Inserm-ANRS Centres, Paris Spain: Hospital Clinic de Barcelona UK: Imperial College (St Mary’s and St Stephens Clinical
Research/Chelsea and Westminster Hospital), London Italy: Instituto Nazionale Malattie Infettive Lazaro
Spallanzani, Rome Germany: Universitätsklinikum Hamburg-Eppendorf Switzerland: CHUV, Lausanne
• Trial Coordinating Center: MRC CTU at UCL, London• Community partner: EATG
24
EHVA T01 Sub-studies
• Leukopheresis: (Spain), Germany, Switzerland, France• LN biopsy: (Spain), Germany, Switzerland • GI biopsy: (Spain), Germany, France
• Microbiome: not flagged as substudy in the main protocol, but not all ppts/centres will take part
• Social Science: not yet submitted, all centres willing to take part
• Genital secretions: recently proposed for French centresonly
25
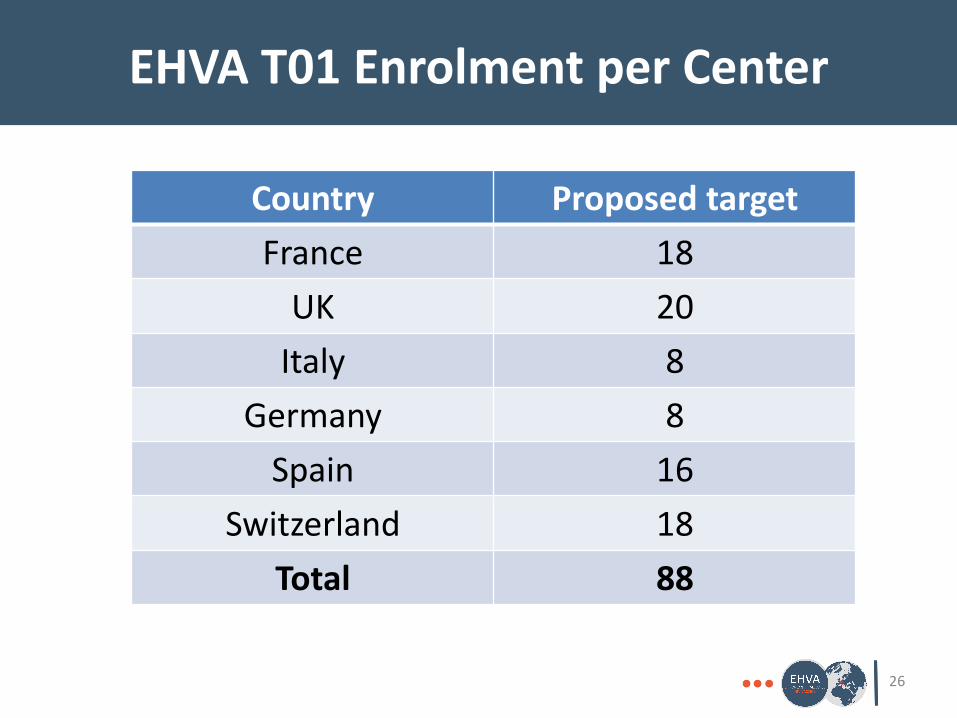
EHVA T01 Enrolment per Center
26
Country Proposed target
France 18
UK 20
Italy 8
Germany 8
Spain 16
Switzerland 18
Total 88
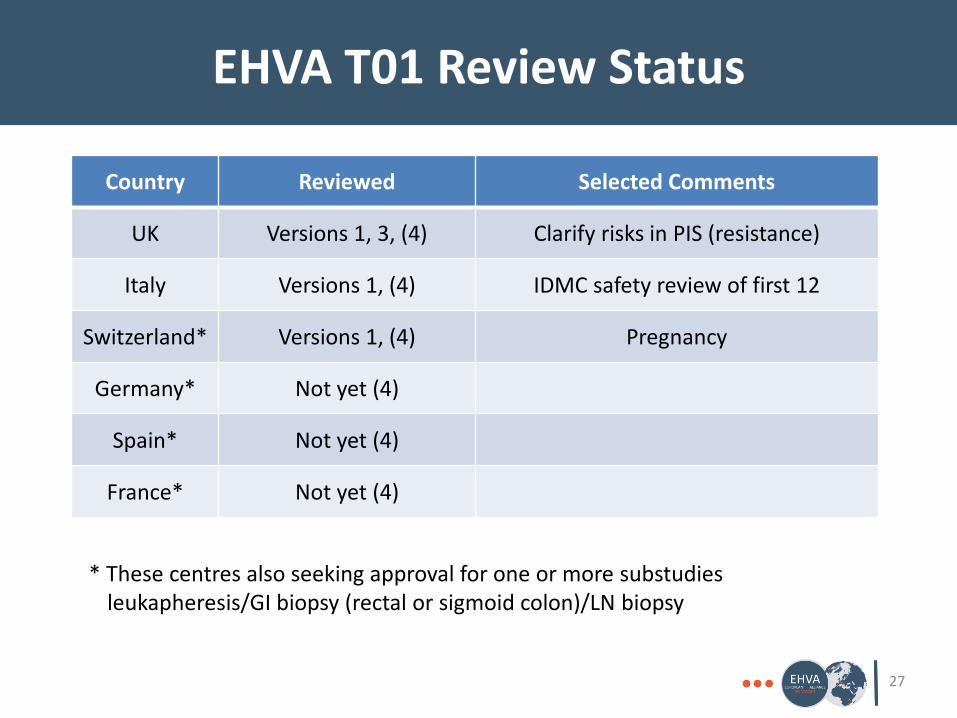
EHVA T01 Review Status
27
Country Reviewed Selected Comments
UK Versions 1, 3, (4) Clarify risks in PIS (resistance)
Italy Versions 1, (4) IDMC safety review of first 12
Switzerland* Versions 1, (4) Pregnancy
Germany* Not yet (4)
Spain* Not yet (4)
France* Not yet (4)
* These centres also seeking approval for one or more substudiesleukapheresis/GI biopsy (rectal or sigmoid colon)/LN biopsy
EHVA T01 Issues
• ART interruption CD4 and VL eligibility criteria to mitigate against risk, but
still an issue for those who started in primary?
Weekly VL monitoring, monthly CD4
Resume at 10,000 copies or CD4 350 or symptomatic –acceptable to EATG
Need to avoid resistance, so patients may have to switch
Transmission to negative partners
PML and JCV antibodies
• Recruitment Will be challenging because of intensity
28
EHVA T01 Next steps
• Initiation
Will follow approval of v4 and product release late June (if all goes to plan)
• Enrolment
Pause 1 after 12 have been (slowly) enrolled and passed their first safety visit for IDMC to review local and systemic reactogenicity
o1 individual/week for the first 4 weeks
o2 individuals/week for 4 weeks
Pause 2 after 88 have been enrolled at 4 or more per week for interim analysis
Enrolment will be competitive, if necessary29
EHVA T01 Acknowledgments• MRC CTU at UCL: Nafisah Atako, Liz Brodnicki, Silvia Forcat, Sue Fleck, Denise Ward, Mary Rauchenberger, Cecilia
Moore, Wolfgang Stohr
• INSERM-ANRS: Mireille Centlivre, Veronique Rieux, Laure Bourdery, Alpha Diallo, Imane Amri, Yves Levy, Jean-Daniel Lelievre, Laurence Weiss, Jean-Michel Molina, Christel Protiere, Bruno Spire, Rodolphe Thiebault, Fabien Barbier, Laura Richert, Christine Lacabaratz, Hakim Hocini, Christianne Moog
• EuroVacc Foundation: Song Ding, Gepi Pantaleo
• CHUV: Gepi Patnaleo, Matthias Cavassini, Deolinda Alves, Sandra Bettinelli-Riccardi, Dolon Das, Fabio Candotti, Craig Fenwick, Gonzalo Tapia, Francesco Procopio
• IDIBAPS: Felipe Garcia, Florencia Etcheverry, Jose Gatel
• ISS/INMI: Stefano Vella, Giuseppe Ippolito, Alessandra Mallano, Andrea Antinori, Carmela Pinnetti, Adriana Ammassari, Raffaella Libertone
• UKE: Julian Schulze zur Wiesch, Veronika Schlicker, Olaf Degen, Johanna Eberhard, Sandra Hertling, Thomas Brehm, Janne Rathjens, Sindy Bartel
• Imperial College including IAVI: Alan Winston, Ken Legg, Michael Wood, Cherry Kingsley, Jonathan Weber, Sarah Joseph, Debbie King, Fran Lala, Jill Gilmour
• Chelsea and Westminster (SSAT): Marta Boffito, Tom Morrish, Carl Fletcher
• ULVI: Bill Paxton, Georgios Pollakis
• HPI: Marcus Altfield
• Erasmus: Rob Gruters, Charles Boucher
• EATG: Giulio Maria Corbelli, Giorgio Barbareschi, Maria Dutarte, Mariana Vicente, Simon Collins, Richard Jefferys
• Fit Biotech: Kalevi Reijonen, Matti Lahde, Andres Mannik, Jussi Seitsonen, Santtu Kiviluoto
30