e:kims new ackup 6janclinical meetings 201501.10.2015 to … · hemiparesis. rash: petechial or...
TRANSCRIPT

Clinical featuresClinical features
The classic clinical triad of meningitis is fever, The classic clinical triad of meningitis is fever, headache, and nuchal rigidity (headache, and nuchal rigidity (““stiff neckstiff neck””). ).
Altered Altered consciousnessconsciousness headache headache photophobia photophobia irritabilityirritability LethargyLethargy poor feeding /weak sucking poor feeding /weak sucking high-pitched cry high-pitched cry skin rashes skin rashes

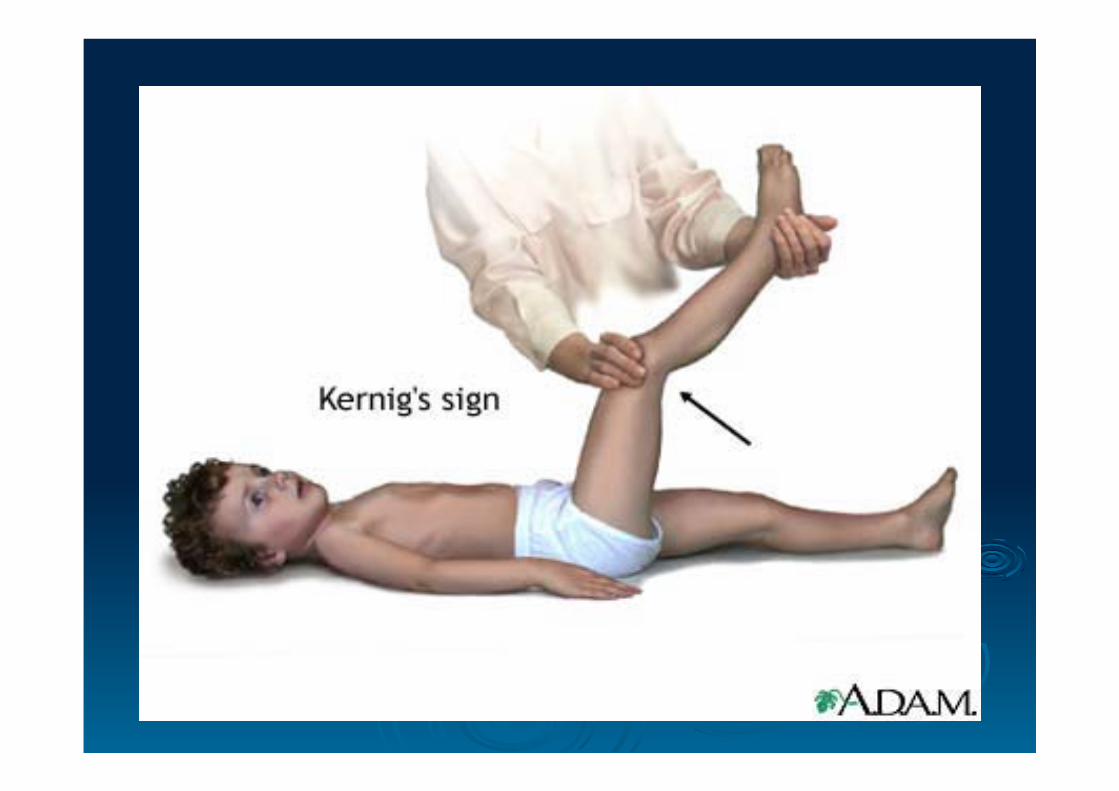
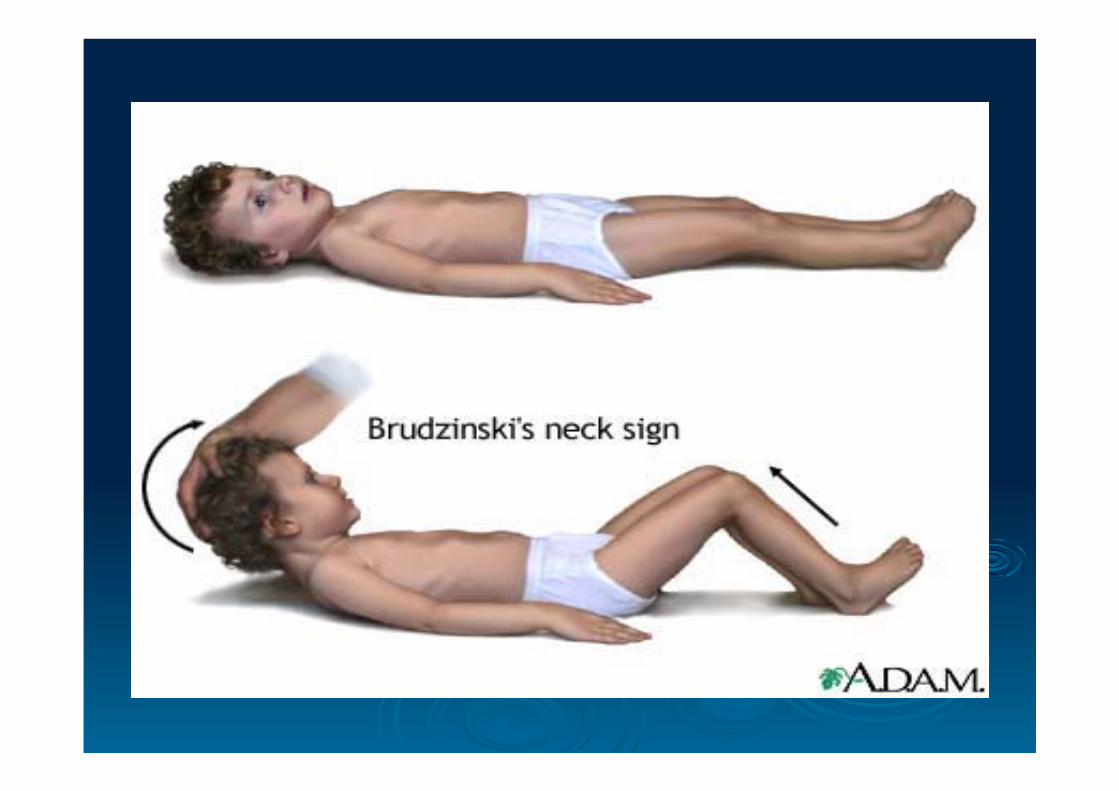
Signs & symptomsSigns & symptoms Brudzinski signBrudzinski sign Kernig sign Kernig sign Apnea Apnea Abnormal temperature (hypo/hyperthermia)Abnormal temperature (hypo/hyperthermia) bulging bulging fontanellesfontanelles Poor reflexes Poor reflexes

NeonatesNeonates Suspect meningitis with temperature more than Suspect meningitis with temperature more than
100.7100.700 F(38.2 F(38.200C).C).
Risk factors:Risk factors: Infective illness in motherInfective illness in mother PROMPROM Difficult deliveryDifficult delivery Premature babiesPremature babies Spina bifidaSpina bifida

ExaminationExamination General physical- General physical- Check for Consciousness
level according to GCS scoring, irritability, dullness.
Vitals: temperature , HR, BP, RR.Vitals: temperature , HR, BP, RR.
Signs of Increased ICP- Signs of Increased ICP- Bulging fontanelle, headache, nausea, vomiting, Bulging fontanelle, headache, nausea, vomiting, ocular palsies, altered level of consciousness, ocular palsies, altered level of consciousness, and papilledema and papilledema
Fundus: papilloedemaFundus: papilloedema CN palsies: (occulomotor, facial, and auditory)CN palsies: (occulomotor, facial, and auditory)

ExaminationExamination Meningismus - check for nuchal rigidity with Meningismus - check for nuchal rigidity with
passive neck flexion (gives 'involuntary passive neck flexion (gives 'involuntary resistance).resistance).
Brudzinski sign (hip & knee flexion with neck Brudzinski sign (hip & knee flexion with neck movement) movement)
Kernig sign (extend knee with hip flexed)Kernig sign (extend knee with hip flexed)
Hemiparesis.Hemiparesis.
Rash: petechial or purpuric rashRash: petechial or purpuric rash

Contraindication for LPContraindication for LP
Increase intracranial pressure.Unstable patient. Skin infection at site of LP. Thrombocytopenia. Papilloedema.

TreatmentTreatment
Supportive therapy:Supportive therapy:Maintain fluid & electrolyte balance as Maintain fluid & electrolyte balance as
requiredrequired Transfuse whole blood, PRC, FFP or Transfuse whole blood, PRC, FFP or
platelets as required.platelets as required.Maintain temperature.Maintain temperature.Monitor OFCMonitor OFC




Duration of RxDuration of Rx
N meningitidisN meningitidis - 7 days- 7 days H influenzaeH influenzae - 7 days- 7 days S pneumoniaeS pneumoniae - 10-14 days- 10-14 days S agalactiaeS agalactiae (GBS) - 14-21 days(GBS) - 14-21 days Aerobic gram-negative bacilli - 21 days or Aerobic gram-negative bacilli - 21 days or
2 weeks beyond the first sterile culture 2 weeks beyond the first sterile culture (whichever is longer)(whichever is longer)
L monocytogenesL monocytogenes - 21 days or longer- 21 days or longer

Viral meningitisViral meningitis
HSV encephalitis : Acyclovir (10 mg/kg HSV encephalitis : Acyclovir (10 mg/kg every 8 h) . minimum 14-day course of every 8 h) . minimum 14-day course of therapy. therapy.
Arbovirus: RibavarinArbovirus: Ribavarin CMV: Gancyclovir.CMV: Gancyclovir.
TreatmentTreatment
SteroidsSteroids::
Dexamethasone useful for H.influenzae type b, Dexamethasone useful for H.influenzae type b, First dose should be given 1 hr prior to starting First dose should be given 1 hr prior to starting antibiotics.antibiotics.
ComplicationsComplications Cranial nerve palsies Cranial nerve palsies Subdural empyema Subdural empyema Brain abscess Brain abscess Hearing loss Hearing loss Obstructive hydrocephalus Obstructive hydrocephalus Learning disability, CP, seizures, Mental Learning disability, CP, seizures, Mental
retardation.retardation. Septic shock/ DIC Septic shock/ DIC AtaxiaAtaxia StrokeStroke SIADH SIADH

Tuberculous Tuberculous MeningitisMeningitis

CLINICAL FEATURES OF TBMAlways sec. to primary tuberculosis.Always sec. to primary tuberculosis.First Phase:First Phase:Vague symptomsVague symptomsChild doesnChild doesn’’t play, is irritable, restless or t play, is irritable, restless or
drowsy.drowsy.Fever, anorexia & vomitingFever, anorexia & vomitingHeadache.Headache.Possibly preceding history of Measles or Possibly preceding history of Measles or
another illness with incompletely recoveryanother illness with incompletely recovery

SECOND PHASESECOND PHASE:: Later drowsy with neck stiffness & rigidity.Later drowsy with neck stiffness & rigidity.Kernig & Brudzinski sign may become Kernig & Brudzinski sign may become
positive, anterior fontanels bulgespositive, anterior fontanels bulgesTwitching of muscles, convulsions, raised Twitching of muscles, convulsions, raised
temperature.temperature.strabismus, nystagmus, and papilloedema strabismus, nystagmus, and papilloedema
may be present.may be present.Fundoscopy: Choroidal TB may be seenFundoscopy: Choroidal TB may be seen

TERMINAL PHASETERMINAL PHASE
Comatose Comatose opisthotonus opisthotonus multiple focal paresis.multiple focal paresis.Cranial nerve palsies.Cranial nerve palsies.High grade fever often occurs High grade fever often occurs
terminally.terminally.

TreatmentTreatment2 mo of Isoniazid, Rifampin, 2 mo of Isoniazid, Rifampin,
Pyrazinamide and an Aminoglycoside Pyrazinamide and an Aminoglycoside or ethionamide, once a day, or ethionamide, once a day, f/ b 7f/ b 7––10 mo of isoniazid and rifampin, 10 mo of isoniazid and rifampin,
once a day or twice a week (9once a day or twice a week (9––12 mo 12 mo total) total)

STEROIDSSTEROIDS:: reduce cerebral edemareduce cerebral edemaprevent fibrosis & subsequent obstruction prevent fibrosis & subsequent obstruction to CSFto CSF
Dose:2mg/kg/24 hours of prednisolone for Dose:2mg/kg/24 hours of prednisolone for 6-8 weeks6-8 weeks

PrognosisPrognosis It depends on the It depends on the •• age, age, •• duration, duration, •• complications, complications, •• micro-organism & micro-organism & •• immune status. immune status. Viral meningitis: good prognosis .Viral meningitis: good prognosis . Worse : Age (ie, <2 y, >60 y), Worse : Age (ie, <2 y, >60 y), Significant Comorbidities , Significant Comorbidities , Immunodeficiency. Immunodeficiency.
Impaired level of consciousness. Impaired level of consciousness. Seizures Seizures

PreventionPrevention
The vaccines against Hib, measles, mumps, polio, The vaccines against Hib, measles, mumps, polio, meningococcus, and pneumococcus can protect meningococcus, and pneumococcus can protect against meningitisagainst meningitis
Hib vaccine: all infants should receive at 2,4,6 Hib vaccine: all infants should receive at 2,4,6 months of age & booster 1 year later.months of age & booster 1 year later.
After 1 year 1 dose is given till the age of 5 years.After 1 year 1 dose is given till the age of 5 years.
Pneumococcal vaccine: 0.5 ml is given IM Pneumococcal vaccine: 0.5 ml is given IM

PreventionPrevention High-risk children should also be immunized High-risk children should also be immunized
routinely.routinely.
Vaccination before travelling to an endemic areaVaccination before travelling to an endemic area
Chemoprophylaxis for susceptible individuals or Chemoprophylaxis for susceptible individuals or close contacts:close contacts:
H influenzae type b : Rifampin(20 mg/kg/d) for 4 days H influenzae type b : Rifampin(20 mg/kg/d) for 4 days N meningitidis: Rifampin (600 mg PO q12h) for 2 days N meningitidis: Rifampin (600 mg PO q12h) for 2 days Ceftriaxone (250 mg IM) single dose or Ceftriaxone (250 mg IM) single dose or
Ciprofloxacin(500-750 mg) single dose. Ciprofloxacin(500-750 mg) single dose.

FUNGAL MENINGITISFUNGAL MENINGITIS
Amphotericin B ( Amphotericin B (0.7 mg/kg/day0.7 mg/kg/day) + ) + flucytosine (flucytosine (100 mg/kg/day100 mg/kg/day) -- 6) -- 6––10 wk 10 wk ((induction)induction), ,
f/b Fluconazole f/b Fluconazole (400 mg/day(400 mg/day)-- 8-10wk)-- 8-10wk ( (consolidationconsolidation)) Fluconazole Fluconazole (200(200––400 mg/day400 mg/day) continued ) continued
for life (for life (maintenance therapymaintenance therapy) after the ) after the completion of consolidation therapycompletion of consolidation therapy

Parasitic meningitisParasitic meningitis
Amphotericin B, rifampin, and fluconazole or Amphotericin B, rifampin, and fluconazole or ketoconazole; amphotericin B, rifampin, and ketoconazole; amphotericin B, rifampin, and chloramphenicol and amphotericin B alone. chloramphenicol and amphotericin B alone.
The The optimal duration optimal duration of treatment is of treatment is unknownunknown..
ReferencesReferences
Nelson textbook of pediatricsNelson textbook of pediatrics O P Ghai text book of pediatricsO P Ghai text book of pediatrics Harrisons text book of internal medicineHarrisons text book of internal medicine