elderly acute myeloid leukemia
TRANSCRIPT
MIGUEL A SANZ, MDValencia, Spain
• Professor and Head of Department, of Oncology, Hematology and Bone Marrow Transplant Unit, University Hospital La Fe in Valencia, Spain
• Professor Sanz is chairman of the Spanish PETHEMA Group and leads the working parties of acute promyelocyticleukemia, acute myeloid leukemia and infections in neutropenic patients. He is currently a reviewer for numerous high-profile medical journals including all top hematology journals, and has authored more than 470 peer-reviewed papers, numerous book chapters, and in excess of 1000 abstracts at national and international meetings. Professor Sanz has also lectured widely in Europe, North, central and South America, as well as in Middle East and Asia, serving as lecturer at the American Society of Hematology in 2004, 2005 and 2010.
AML: Best of 2014
Elderly Patients with AML
The 6th International Hematologic Malignancies Conference: Bridging the Gap 2015 (BTG2015)
Beijing, China (January 31, 2014)
Miguel A. Sanz
Departamento de Medicina de la Universidad de Valencia
Servicio de Hematología y Hemoterapia
Hospital Universitario La Fe
Valencia, Spain
Original Article
Clonal Hematopoiesis and Blood-Cancer Risk Inferred from Blood DNA Sequence
Giulio Genovese, Ph.D., Anna K. Kähler, Ph.D., Robert E. Handsaker, B.S., Johan Lindberg, Ph.D., Samuel A. Rose, B.S., Samuel F. Bakhoum, M.D., Ph.D., Kimberly
Chambert, M.S., Eran Mick, B.S., Benjamin M. Neale, Ph.D., Menachem Fromer, Ph.D., Shaun M. Purcell, Ph.D., Oscar Svantesson, M.S., Mikael
Landén, Ph.D., Martin Höglund, M.D., Ph.D., Sören Lehmann, M.D., Ph.D., Stacey B. Gabriel, Ph.D., Jennifer L. Moran, Ph.D., Eric S. Lander, Ph.D., Patrick F.
Sullivan, M.D., Pamela Sklar, M.D., Ph.D., Henrik Grönberg, M.D., Ph.D., Christina M. Hultman, Ph.D., and Steven A. McCarroll, Ph.D.
N Engl J MedVolume 371(26):2477-2487
December 25, 2014
We analyzed data from whole-exome sequencing of DNA in peripheral-blood cells from 12,380 persons, unselected for cancer or hematologic phenotypes.
3
Study Overview
• Clonal hematopoiesis with somatic mutations was observed in 10% of otherwise healthy people > 65 years of age but in only 1% of those < 50 years of age.
• Detectable clonal expansions most frequently involved somatic mutations in three genes (DNMT3A , ASXL1 , and TET2 ) that have previously been implicated in hematologic cancers.
• The risk of hematologic cancer was substantially increased among these persons:
- Clonal hematopoiesis was a strong risk factor for subsequent hematologic cancer (HR, 12.9; 95% CI, 5.8 to 28.7).
- 42% of hematologic cancers in persons with previous detectable clonality.
Genovese G et al. N Engl J Med 2014;371:2477-2487 4
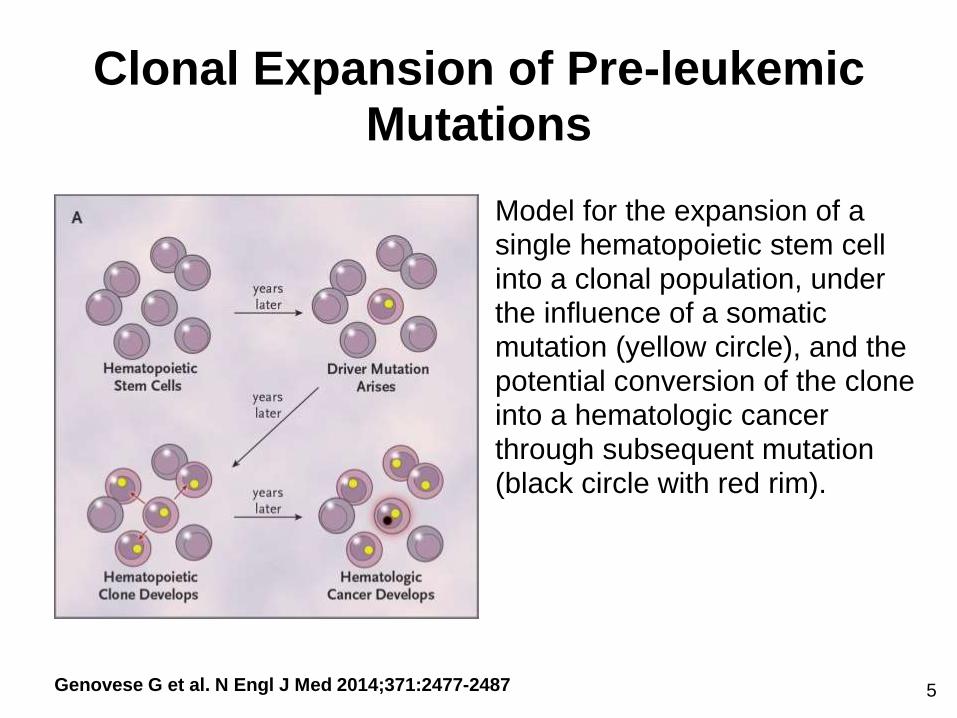
Clonal Expansion of Pre-leukemic Mutations
Genovese G et al. N Engl J Med 2014;371:2477-2487
Model for the expansion of a single hematopoietic stem cell into a clonal population, under the influence of a somatic mutation (yellow circle), and the potential conversion of the clone into a hematologic cancer through subsequent mutation (black circle with red rim).
5

Candidate Driver Somatic Mutations
Genovese G et al. N Engl J Med 2014;371:2477-2487 6
DNMT3A in NPM1mut AMLHigh stability & persistence in remission
Schnittger S, et al.-MLL lab (abst. 122, session 617)
• DNMT3A is a stable mutation in NPM1 AML cases
- DNMT3A is retained at relapse in 57/61 (93%) cases with paired
diagnosis – relapse samples.
• DNMT3A as a potential pre-leukemic mutation
- DNMT3A persisted in remission samples in 32/54 (59%)
patients with NPM1 clearance.
• Persistence of DNMT3A at remission is associated to
worse prognosis:
- EFS: 38 vs 96 mos (p=0.03)
- OS: 69 vs. 96 mos (p=0.053)
7
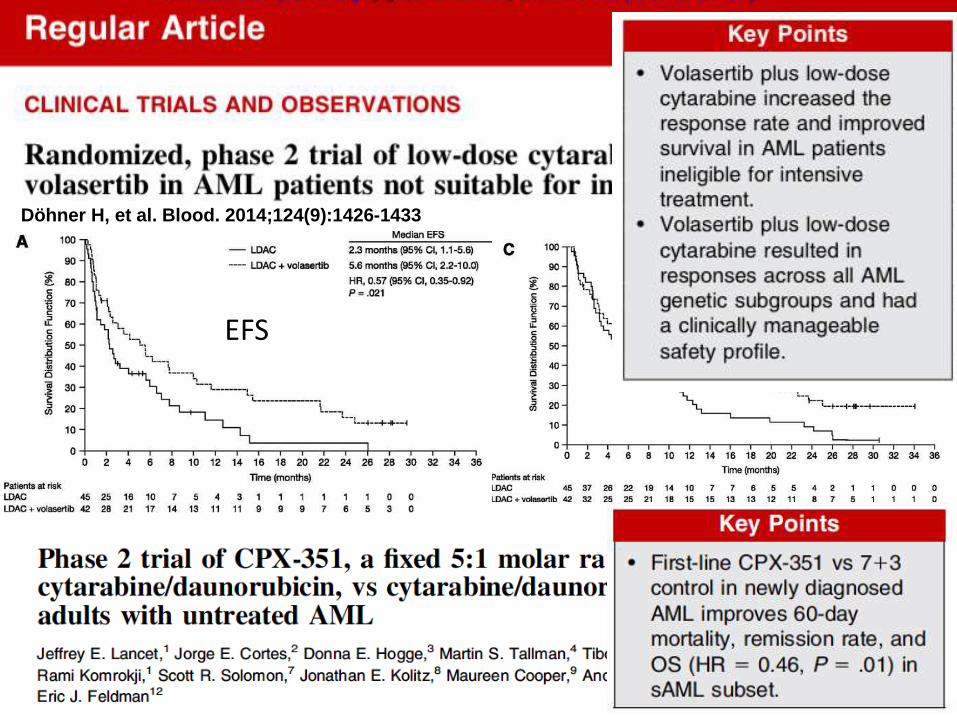
Döhner H, et al. Blood. 2014;124(9):1426-1433
EFS OS
8
RESULTS OF A PHASE 3, MULTICENTER, RANDOMIZED, OPEN-LABEL STUDY OF AZACITIDINE
VS CONVENTIONAL CARE REGIMENS IN OLDER PATIENTS WITH NEWLY DIAGNOSED ACUTE MYELOID
LEUKEMIA
Hervé Dombret1, John F. Seymour2, Aleksandra Butrym3, Agnieszka Wierzbowska4, Dominik Selleslag5, Jun Ho Jang6, Rajat Kumar7, James Cavenagh8, Andre Schuh9, Anna Candoni10,
Christian Récher11, Irwindeep Sandhu12, Teresa Bernal del Castillo13, Haifa Kathrin Al-Ali14, Giovanni Martinelli15, Richard M. Stone16, Mark D. Minden9, Heidi McIntyre17, Steve Songer17,
Lela Lucy17, CL Beach17, Hartmut Döhner18
1Hôpital Saint Louis, Paris Cedex 10, France; 2Peter MacCallum Cancer Centre, East Melbourne, Australia; 3Wroclaw Medical University, Wroclaw, Poland; 4Medical University of Lodz, Lodz, Poland; 5Algemeen Ziekenhuis Sint-Jan, Brugge, Belgium; 6Samsung Medical Center, Seoul,
Republic of Korea; 7Cancer Care Manitoba, Winnipeg, Canada; 8Barts Health NHS Trust, London, United Kingdom; 9Princess Margaret Cancer Centre, Toronto, Canada; 10Azienda Ospedaliero Universitaria S. Maria della Misericordia di Udine, Udine, Italy; 11Centre Hospitalier Universitaire
de Toulouse, Toulouse Cedex 09, France; 12University of Alberta Hospital, Edmonton, Canada; 13Hospital Central de Asturias, Oviedo, Spain; 14Universitätsklinikum Leipzig, Leipzig, Germany; 15Azienda Ospedaliero-Universitaria di Bologna - Policlinico S.Orsola-Malpighi, Bologna, Italy;
16Dana Farber Cancer Institute, Boston, United States; 17Celgene Corporation, Summit, United States; 18Universitätsklinikum Ulm, Ulm, Germany
Presented at the 19th Congress of the European Hematology Association; June 12-15, 2014; Milan, Italy
9
9
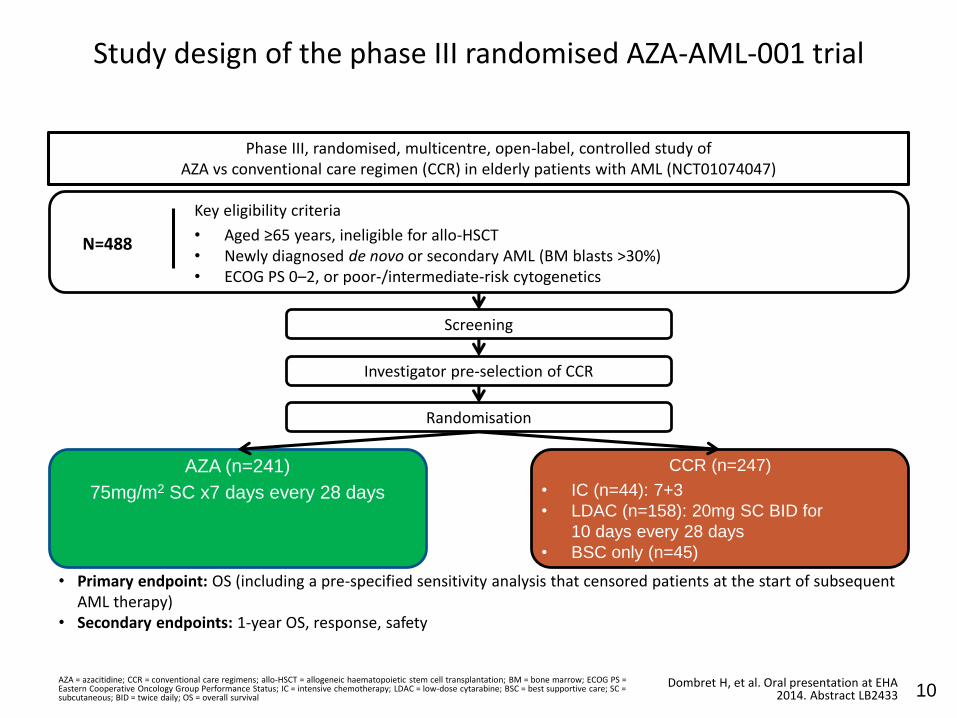
Study design of the phase III randomised AZA-AML-001 trial
AZA = azacitidine; CCR = conventional care regimens; allo-HSCT = allogeneic haematopoietic stem cell transplantation; BM = bone marrow; ECOG PS = Eastern Cooperative Oncology Group Performance Status; IC = intensive chemotherapy; LDAC = low-dose cytarabine; BSC = best supportive care; SC = subcutaneous; BID = twice daily; OS = overall survival
Dombret H, et al. Oral presentation at EHA 2014. Abstract LB2433
Key eligibility criteria
• Aged ≥65 years, ineligible for allo-HSCT• Newly diagnosed de novo or secondary AML (BM blasts >30%)• ECOG PS 0–2, or poor-/intermediate-risk cytogenetics
Screening
N=488
• Primary endpoint: OS (including a pre-specified sensitivity analysis that censored patients at the start of subsequent AML therapy)
• Secondary endpoints: 1-year OS, response, safety
Phase III, randomised, multicentre, open-label, controlled study of AZA vs conventional care regimen (CCR) in elderly patients with AML (NCT01074047)
Investigator pre-selection of CCR
CCR (n=247)
• IC (n=44): 7+3
• LDAC (n=158): 20mg SC BID for
10 days every 28 days
• BSC only (n=45)
AZA (n=241)
75mg/m2 SC x7 days every 28 days
Randomisation
10
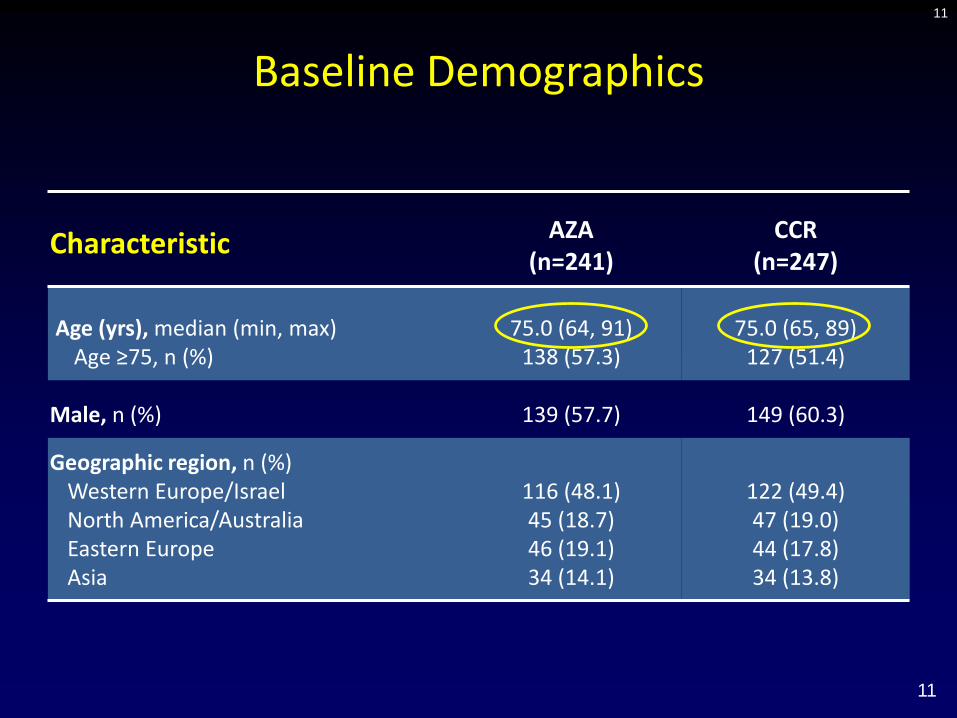
Baseline Demographics
Characteristic AZA(n=241)
CCR(n=247)
Age (yrs), median (min, max)Age ≥75, n (%)
75.0 (64, 91)138 (57.3)
75.0 (65, 89)127 (51.4)
Male, n (%) 139 (57.7) 149 (60.3)
Geographic region, n (%)Western Europe/IsraelNorth America/AustraliaEastern EuropeAsia
116 (48.1)45 (18.7)46 (19.1)34 (14.1)
122 (49.4)47 (19.0)44 (17.8)34 (13.8)
11
11
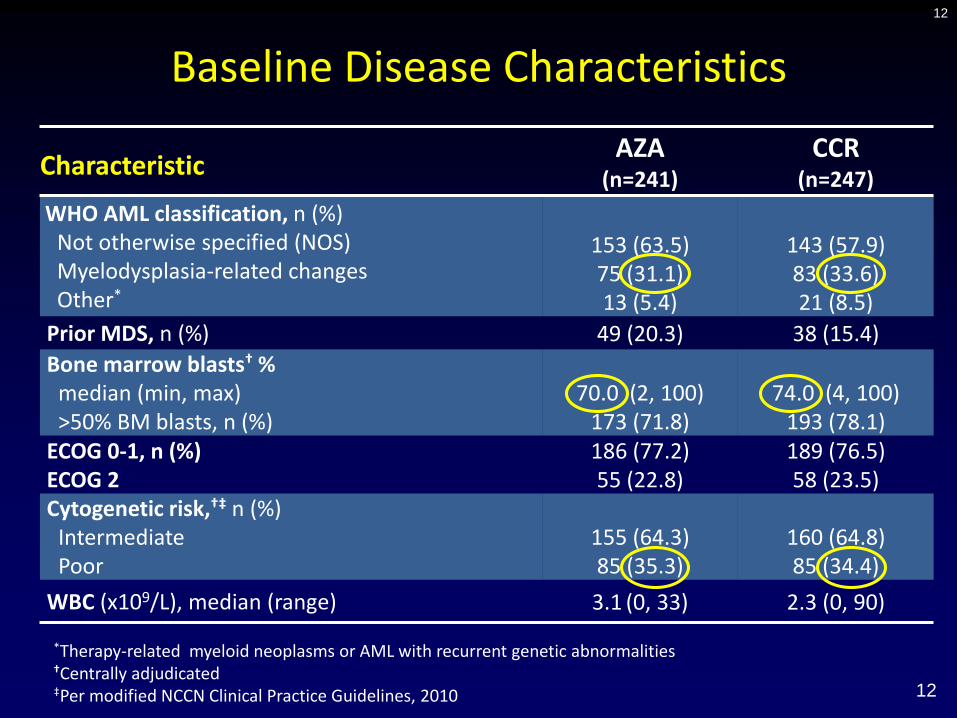
Baseline Disease Characteristics
CharacteristicAZA
(n=241)
CCR(n=247)
WHO AML classification, n (%)Not otherwise specified (NOS)Myelodysplasia-related changesOther*
153 (63.5)75 (31.1)13 (5.4)
143 (57.9)83 (33.6)21 (8.5)
Prior MDS, n (%) 49 (20.3) 38 (15.4)
Bone marrow blasts† %median (min, max)>50% BM blasts, n (%)
70.0 (2, 100)173 (71.8)
74.0 (4, 100)193 (78.1)
ECOG 0-1, n (%)ECOG 2
186 (77.2)55 (22.8)
189 (76.5)58 (23.5)
Cytogenetic risk,†‡ n (%)IntermediatePoor
155 (64.3)85 (35.3)
160 (64.8)85 (34.4)
WBC (x109/L), median (range) 3.1 (0, 33) 2.3 (0, 90)
12
*Therapy-related myeloid neoplasms or AML with recurrent genetic abnormalities†Centrally adjudicated‡Per modified NCCN Clinical Practice Guidelines, 2010 12
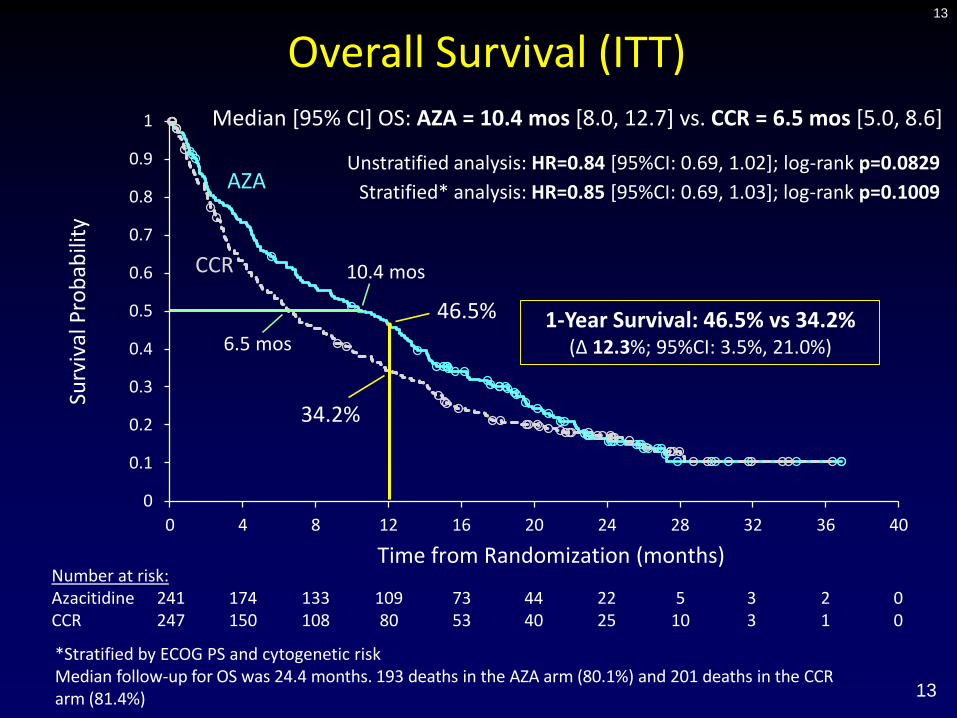
Overall Survival (ITT)13
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 4 8 12 16 20 24 28 32 36 40
Surv
ival
Pro
bab
ility
Time from Randomization (months)Number at risk:Azacitidine 241 174 133 109 73 44 22 5 3 2 0CCR 247 150 108 80 53 40 25 10 3 1 0
AZA
CCR
*Stratified by ECOG PS and cytogenetic riskMedian follow-up for OS was 24.4 months. 193 deaths in the AZA arm (80.1%) and 201 deaths in the CCRarm (81.4%)
Median [95% CI] OS: AZA = 10.4 mos [8.0, 12.7] vs. CCR = 6.5 mos [5.0, 8.6]
1-Year Survival: 46.5% vs 34.2% (Δ 12.3%; 95%CI: 3.5%, 21.0%)
Unstratified analysis: HR=0.84 [95%CI: 0.69, 1.02]; log-rank p=0.0829
Stratified* analysis: HR=0.85 [95%CI: 0.69, 1.03]; log-rank p=0.1009
6.5 mos
10.4 mos
34.2%
46.5%
13

Subanalysis of AZA-AML-001 trialOutcomes according to cytogenetic risk
CI = confidence interval Döhner H, et al. Oral presentation at ASH 2014. Abstract 621
Median OS of patients with int-risk cytogenetics treated with AZA was prolonged by 2.9 months compared with those treated with CCR
0.0
0.2
0.4
0.6
0.8
1.0
0 4 8 12 16 20 24 28 32 36 40
Surv
ival
Pro
bab
ility
Time from randomisation, months
13.0 months
10.1 months log-rank p=0.4119
AZA (n=155)CCR (n=160)
• 1-year OS: AZA: 55.2%; CCR: 45.5% (Δ9.7%; 95% CI: –1.4%, 20.8%)
OS: intermediate-risk cytogenetics
14
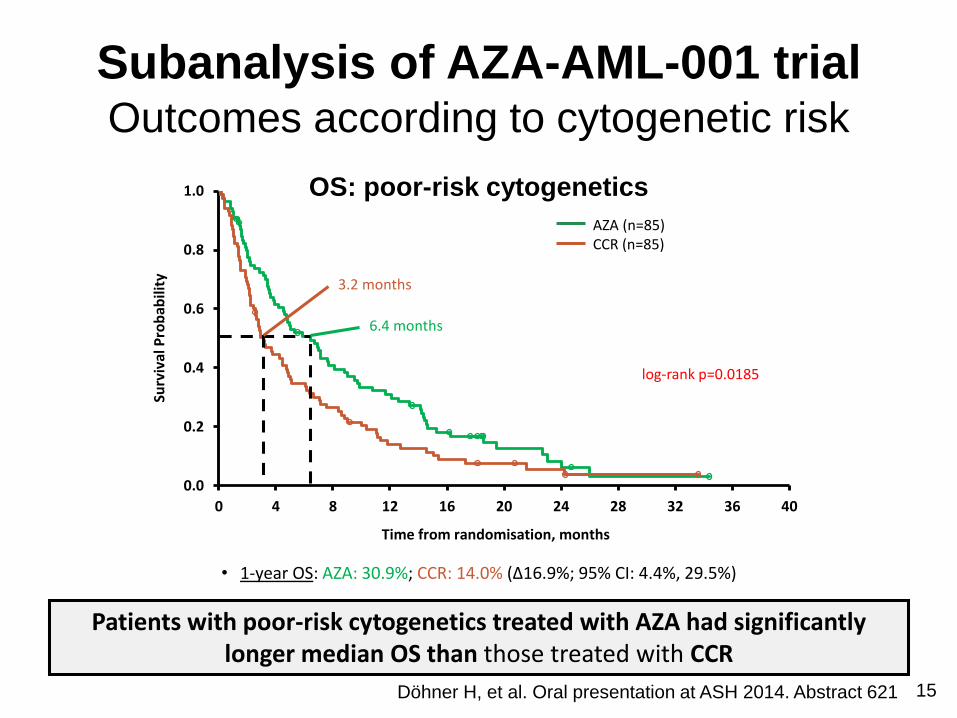
Subanalysis of AZA-AML-001 trialOutcomes according to cytogenetic risk
Patients with poor-risk cytogenetics treated with AZA had significantly longer median OS than those treated with CCR
0.0
0.2
0.4
0.6
0.8
1.0
0 4 8 12 16 20 24 28 32 36 40
Surv
ival
Pro
bab
ility
Time from randomisation, months
log-rank p=0.0185
6.4 months
3.2 months
AZA (n=85)CCR (n=85)
• 1-year OS: AZA: 30.9%; CCR: 14.0% (Δ16.9%; 95% CI: 4.4%, 29.5%)
15Döhner H, et al. Oral presentation at ASH 2014. Abstract 621
OS: poor-risk cytogenetics
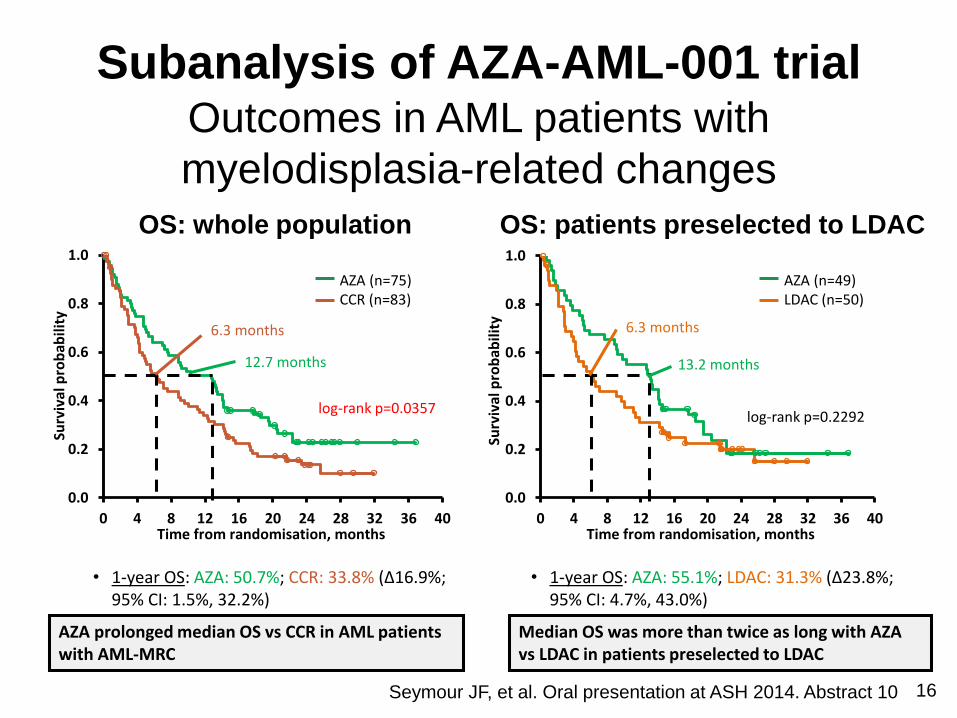
Subanalysis of AZA-AML-001 trialOutcomes in AML patients with
myelodisplasia-related changes
Seymour JF, et al. Oral presentation at ASH 2014. Abstract 10
OS: whole population OS: patients preselected to LDAC
• 1-year OS: AZA: 50.7%; CCR: 33.8% (Δ16.9%; 95% CI: 1.5%, 32.2%)
• 1-year OS: AZA: 55.1%; LDAC: 31.3% (Δ23.8%; 95% CI: 4.7%, 43.0%)
0.0
0.2
0.4
0.6
0.8
1.0
0 4 8 12 16 20 24 28 32 36 40
Surv
ival
pro
bab
ility
Time from randomisation, months
12.7 months
6.3 months
log-rank p=0.0357
AZA (n=75)CCR (n=83)
0.0
0.2
0.4
0.6
0.8
1.0
0 4 8 12 16 20 24 28 32 36 40
Surv
ival
pro
bab
ility
Time from randomisation, months
log-rank p=0.2292
13.2 months
6.3 months
AZA (n=49)LDAC (n=50)
AZA prolonged median OS vs CCR in AML patients with AML-MRC
16
Median OS was more than twice as long with AZA vs LDAC in patients preselected to LDAC
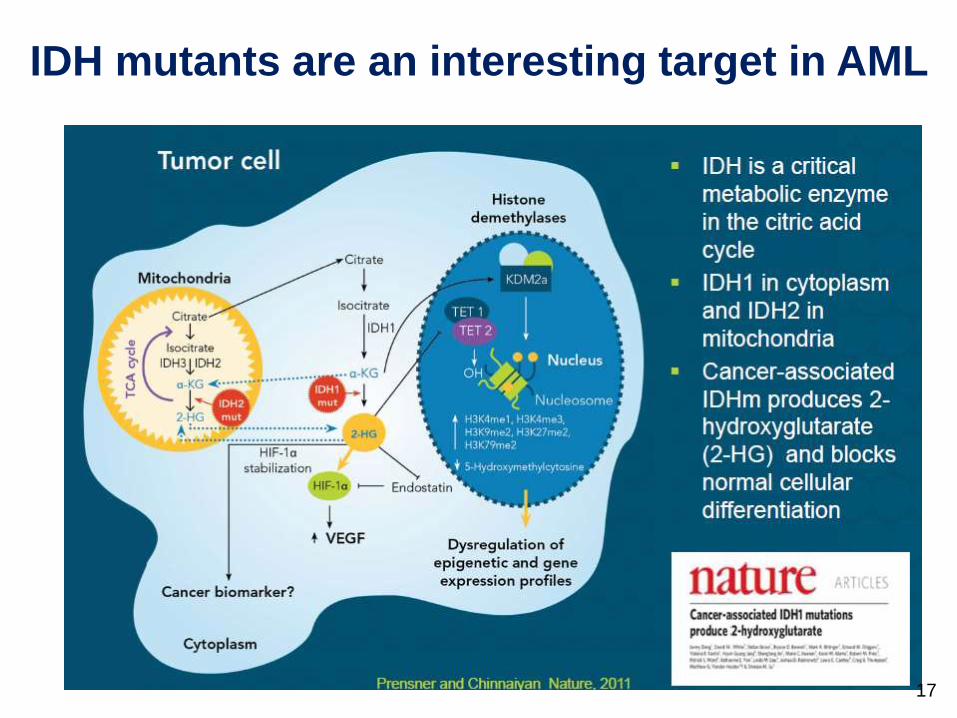
IDH mutants are an interesting target in AML
17
AG-221, an Oral, Selective, First-in-Class,
Potent Inhibitor of the IDH2 Mutant Enzyme,
Induces Durable Remissions in a Phase 1
Study of IDH2 Mutation Positive Advanced
Hematologic Malignancies
Eytan M Stein1, Jessica K Altman2, Robert Collins3, Daniel J DeAngelo4, Amir T Fathi5,
Ian Flinn6, Arthur Frankel3, Ross L Levine1, Bruno C Medeiros7, Manish Patel8,
Daniel A Pollyea9, Gail Roboz10, Richard M Stone4, Ronan T Swords11, Martin S Tallman1,
Sam Agresta12, Bin Fan12, Meredith Goldwasser 12, Hua Yang12, Katharine Yen12 and
Stéphane de Botton13
1Memorial Sloan-Kettering Cancer Center, New York, NY; 2Robert H. Lurie Comprehensive Cancer Center, Chicago, IL; 3University of
Texas Southwestern, Dallas, TX; 4Dana-Farber Cancer Institute, Boston, MA; 5Massachusetts General Hospital Cancer Center, Harvard
Medical School, Boston, MA; 6Sarah Cannon Research Institute, Nashville, TN; 7Stanford Comprehensive Cancer Center, Stanford
University, Stanford, CA; 8Florida Cancer Specialists, Sarasota, FL; 9University of Colorado Cancer Center, Aurora, CO; 10Weill Cornell
Medical College, New York Presbyterian Hospital, New York, NY; 11Sylvester Comprehensive Cancer Center, University of Miami Hospitals,
Miami, FL; 12Agios Pharmaceuticals, Cambridge, MA; 13Institut Gustave Roussy, Villejuif, France
Oral presentation:
Dec 7, 2014
4:30 PM
West Building, 2001-2003-2014-2016
Moscone CenterStein EM., et al. AG-221, an Oral, Selective, First-in-Class, Potent Inhibitor of the IDH2 Mutant Enzyme, Induces Durable Remissions in a Phase 1 Study of
IDH2 Mutation Positive Advanced Hematologic Malignancies. Oral Presentation at: Annual Meeting and Exposition of the American Society of Hematology 2014;
December 6-9; San Francisco, CA.18
AG-221 for AML patients with mutatedIDH-2
• AG-221, an oral inhibitor of mutated IDH2, is well
tolerated in pts with advanced myeloid malignancies
• Leads to effective 2-HG inhibition >90% in pts with
IDH2-R140 or -R172 mutation (≥100 mg/day)
• Significant clinical activity
- Overall response rate 56% (25/45)
- 6 CR + 9 CR with incomplete recovery
- Durable responses (6 pts on-study >6 mos.)
Stein E, et al. ASH 2014 (abst. 115, session 616) 19

Vosaroxin (LBA-6) in combination with cytarabine improves survival in patients with first
relapsed/refractory AML: results of phase III VALOR trial
• Vosaroxin is a novel anticancer quinolone derivative
• Topoisomerase II inhibitor
• Non P-glycoprotein substrate
• P53-independent activity
• Additive/synergistic effect with cytarabine
Ravandi F, et al. ASH 2014 (Late breaking abstracts) 20
Vosaroxin (LBA-6) in combination with cytarabine improves survival in patients with first
relapsed/refractory AML: results of phase III VALOR trial
• Refractory or AML in first relapse
• Dec 2010-Sept 2013
• 711 pts randomized in a 1:1 ratio
• Up to 2 induction & 2 consolidation courses
Cytarabine 1 g/m2 IV d 1-5Cytarabine 1 g/m2 IV days 1-5
+Vosaroxin 90 (70)mg/m2 IV d1 & d4
Vs.
21Ravandi F, et al. ASH 2014 (Late breaking abstracts)
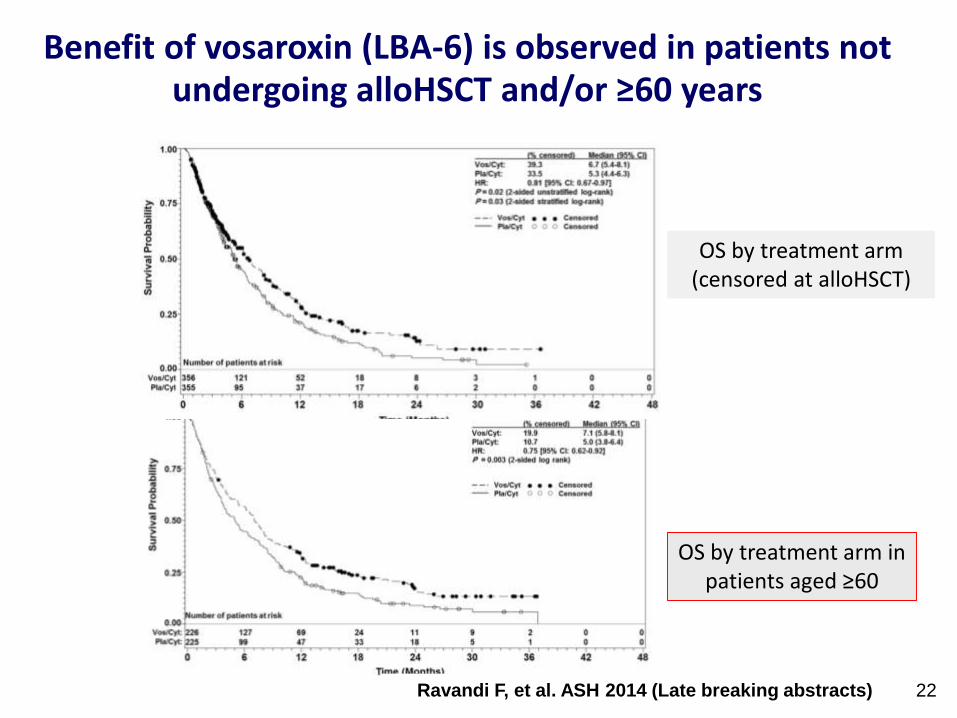
Benefit of vosaroxin (LBA-6) is observed in patients not undergoing alloHSCT and/or ≥60 years
OS by treatment arm (censored at alloHSCT)
OS by treatment arm in patients aged ≥60
22Ravandi F, et al. ASH 2014 (Late breaking abstracts)
Improved Overall Survival with Gemtuzumab Ozogamicin (GO) Compared with Best Supportive Care (BSC) in Elderly Patients with Untreated Acute Myeloid Leukemia (AML) Not Considered Fit for Intensive Chemotherapy: Final Results from the Randomized Phase III Study (AML-19) of the EORTC
and Gimema Leukemia Groups
Conclusions:
• Compared with BSC including hydroxyurea as necessary, GO 6 mg/m2 day 1 and 3 mg/m2 day 8 significantly improved OS in elderly AML pts not considered fit for intensive chemotherapy, with an acceptable safety profile.
• The benefit of GO were greater in pts presenting with better-risk cytogenetics, high CD33 expression on blast cells, or secondary disease.
23Amadori S et al. Oral presentation at ASH 2014.
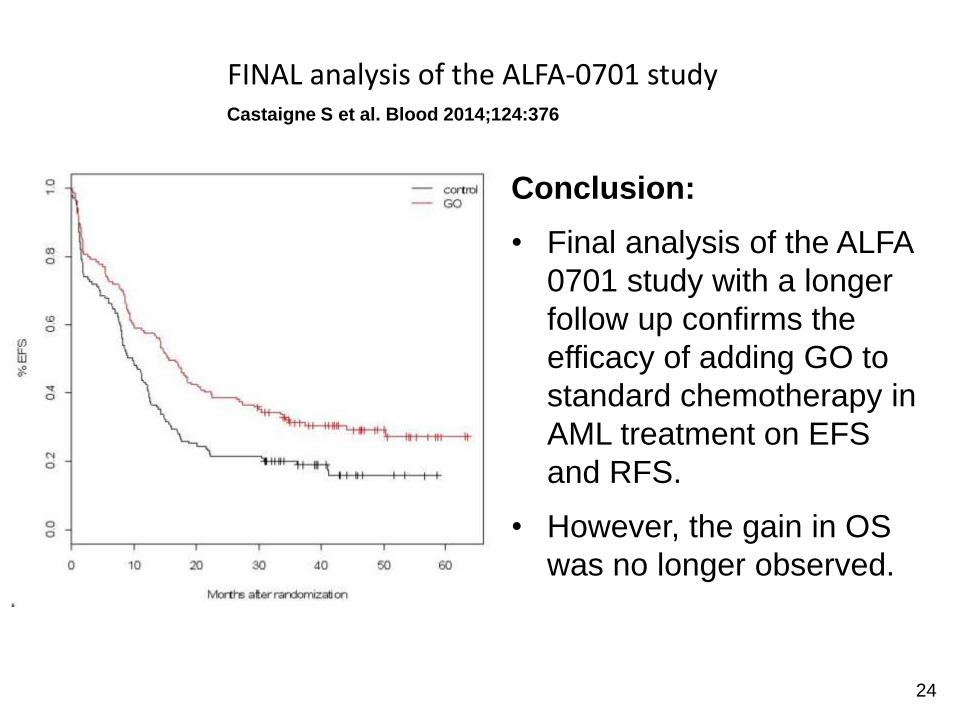
Castaigne S et al. Blood 2014;124:376
FINAL analysis of the ALFA-0701 study
Conclusion:
• Final analysis of the ALFA
0701 study with a longer
follow up confirms the
efficacy of adding GO to
standard chemotherapy in
AML treatment on EFS
and RFS.
• However, the gain in OS
was no longer observed.
24
