employer trends and best practices in health benefits and wellness initiatives cheryl larson vice...
TRANSCRIPT

Employer Trends and Best Practices
in Health Benefits and
Wellness Initiatives
Cheryl LarsonVice President Michigan Purchasers Health AllianceMidwest Business Group on Health September 18, 2008
Why Are Employers Changing Why Are Employers Changing Benefit Strategies?Benefit Strategies?
• Their costs continue to increase
• Their population is not getting healthier
• The marketplace is not meeting their expectations
• Employees don’t recognize the real cost of health services
• Few patients take responsibility for own health
• Serious and systemic quality problems exist
• Employers have the unique opportunity to impact workers’ health since they see employees over 1000 hours a year, while the average person sees their doctor only several hours each year!

How Have EmployersHow Have EmployersContributed to the Problem?Contributed to the Problem?
Been reluctant to direct employees to better performing plans, giving them the same contributions for any plan they selected
Continued the ongoing perception of “entitlement,” instead of encouraging and communicating to them that “we’re in this together”
Carved out services to obtain customized programs, better information and services – resulting in fragmentation and confusion, the loss of integrated data and poor coordination of vendor services
Treated wellness as a fringe benefit, not an integral part of human capital management
Expected employees would participate in health management programs just because they were offered
Treated health benefits as an expense, not an investment

The New Employer FoundationThe New Employer Foundation
Is built on the maintenance of health and the integration of data
Includes key support beams:◦ Integrating benefit designs and financial strategies
that drive behavior change and increase compliance through the use of strategic incentives and disincentives
◦ Implementing proven, best-practice programs for prevention, wellness, lifestyle and disease management
◦ Including key consumerism/engagement strategies, along with targeted communications

MBGH Annual Member MBGH Annual Member Survey - 2007Survey - 2007
95% of member employers believe all Americans should have access to health care
59% support a “play or pay” requirement that would require employers who do not offer health benefits to pay into a government fund that would provide such coverage
Of those that support “pay or play” 24% believe the amount of “pay” should be a fixed amount based on the size of the employer
49% support requiring all employers to offer benefits to full time employees, while 44% do not support an employer mandate
64% support the government providing tax credits to encourage employers to offer health benefits to part-time workers
Only 26% support requiring employers to provide coverage to part-time workers

Annual Survey 2007Annual Survey 2007
64% support the government providing a premium subsidy to low income individuals to pay for coverage from their employer or the marketplace
66% do not believe there is sufficient quality information on doctors to enable patients to make knowledgeable choices
100% believe physicians and hospitals should make prices and the quality and safety of their services publicly available
94% believe patients need to know their out-of-pocket costs to make informed decisions on obtaining and selecting health care services
76% think all physician offices should be required to use interoperable electronic medical records, with 49% supporting the govt. providing funds
Annual Survey 2007Annual Survey 2007
79% think physicians should be paid more for reaching certain quality targets
77% think evidence-based preventive care services should be covered in benefit plans with no cost to patients
79% think a physician should be paid the same for a procedure regardless of whether the patient is uninsured, underinsured or fully insured
92% believe every person should have access to portable medical records
46% would rather pay patients for selecting higher performing doctors and hospitals than paying more to physicians and hospitals
89% believe there should be caps on non-economic damages in med-malpractice suits

MBGH Key Employer TrendsMBGH Key Employer TrendsSurvey - 2008Survey - 2008

Employer Trends 2008Employer Trends 2008Key Clinical Areas of InterestKey Clinical Areas of Interest
Arthritis Asthma Birth Cancer CVD Depres- Diabetes Fatigue Fitness GI Hyper- Infer- Muscu- Obesity Smoking
Control sion tension tility loskeletal
#1 #2#3

Employer Trends 2008Employer Trends 2008Importance of key employer challengesImportance of key employer challenges
Creating Using Relying Collect- Helping Offering Staying Working Working Sharing a culture VBD & on vendors ing and workers convenient current with other with others info on of health incentives to change using become care that’s on policy employers to improve best practices to improve behaviors data for better personal- changes to improve the health with other health /improve activities consu- ized health of the purchasers
health mers system community
Creating Using Relying Collect- Helping Offering Staying Working Working Sharing a culture VBD & on vendors ing and workers convenient current with other with others info on of health incentives to change using become care that’s on policy employers to improve best practices to improve behaviors data for better personal- changes to improve the health with other health /improve activities consu- ized health of the purchasers
health mers system community
#1 #3 #2

Employer Trends 2008Employer Trends 2008Importance of key employer challengesImportance of key employer challenges
82% Creating a culture of health
77% Helping workers become better consumers
72% Using value-based benefit designs and incentives to improve population health
69% Staying current on policy changes
64% Relying on vendors to change behaviors to improve population health
52% Collecting and using data for activities
46% Sharing information on best practices with other purchasers
43% Working with other employers to improve the health care system
36% Offering convenient care that’s personalized
34% Working with others to improve the health of the community
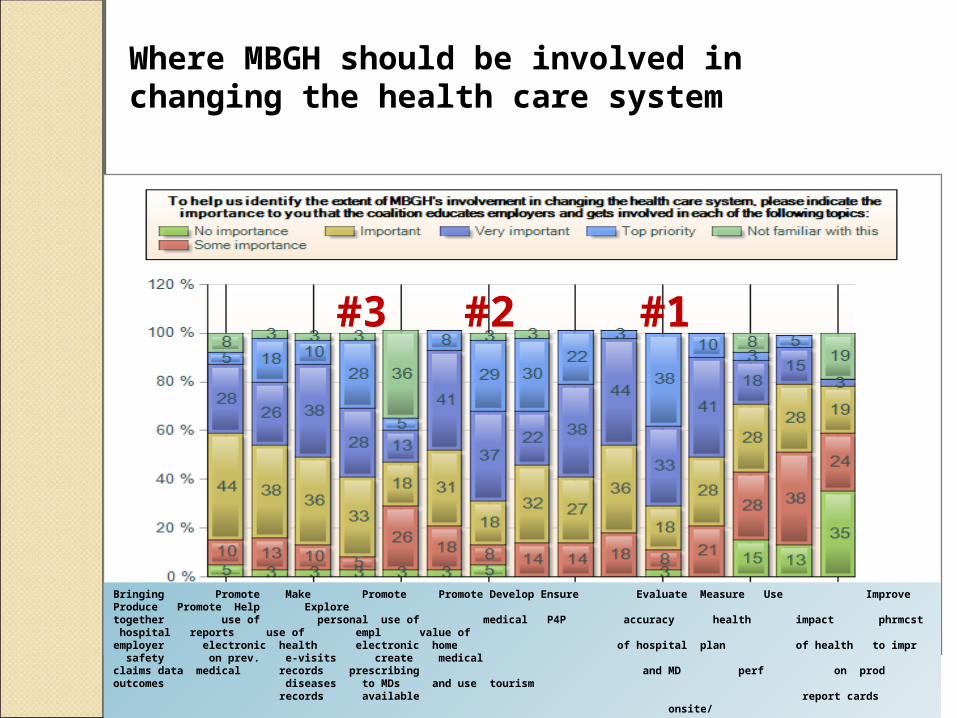
Where MBGH should be involved in changing the health care system
Bringing Promote Make Promote Promote Develop Ensure Evaluate Measure Use Improve Produce Promote Help Explore together use of personal use of medical P4P accuracy health impact phrmcst hospital reports use of empl value of employer electronic health electronic home of hospital plan of health to impr safety on prev. e-visits create medicalclaims data medical records prescribing and MD perf on prod outcomes diseases to MDs and use tourism records available report cards onsite/
retail clinics
#1#2#3

Employer Trends 2008Employer Trends 2008Where MBGH should be involved in changing Where MBGH should be involved in changing the health care systemthe health care system71% Improve hospital safety
66% Ensure accuracy of hospital and MD report cards
60% Measuring impact of health on productivity
56% Promote use of electronic medical records
52% Evaluate health plan performance
51% Produce reports on prevalence of diseases
49% Develop P4P
48% Make personal health records available
47% Use pharmacists to improve outcomes
44% Promote use of electronic prescribing
33% Bring together employers’ claims data
21% Promote use of e-visits to doctors
20% Help employers create and use onsite and retail clinics
18% Promote medical home
3% Explore the value of medical tourism
Keys to Creating a “Culture of Keys to Creating a “Culture of Health”Health” Secure senior management endorsement and
participation through:
◦ Educating management
◦ Tying the health of the worksite to management’s performance bonuses
◦ Identifying and using local health champions
◦ Ensuring a supportive environment
◦ Making sure health policies support the culture Work with all vendors - health plan, PBM, EAP, DM,
TPA, to gather data and coordinate efforts Engage local providers – hospitals, medical groups,
disease-specific organizations – for resources, screenings, programs, etc.

Keys to Creating a “Culture of Keys to Creating a “Culture of Health”Health” Include in program offerings:
◦ Health coaching for lifestyle and acute/chronic conditions
◦ Self-directed program options
◦ Access to on-line resources, nurseline and EAP – as appropriate
Evaluate and address stress and anxiety levels of workplace
Offer incentives for participation Offer healthy foods, at lower cost than others Offer health fairs and screenings Include spouses and dependents over 18 in offerings Communication – ongoing, comprehensive, transparent

Culture & Your EmployeesCulture & Your Employees

Copyright MBGH 2007 17
MBGH Readiness to Adopt Value-MBGH Readiness to Adopt Value-Based Benefits Survey - 2007-08Based Benefits Survey - 2007-08Characteristics of Self-Identified “Leading Edge” Characteristics of Self-Identified “Leading Edge” FirmsFirms
The organization is highly supportive of improving employee health
Senior leadership is highly influential in designing health benefits
They see a link between an employee's health and his/her productivity
In addition to company data, they look to experiences of other “leading edge” firms and academic research to determine their benefit directions
Health benefits are seen a necessary cost of doing business and an investment in human capital, with a measurable outcome

Copyright MBGH 2007 18
Readiness SurveyReadiness SurveyEmployers Views on the Value of HealthEmployers Views on the Value of Health
There is a link between an employee’s health and their productivity
◦ 95% of employers agree Health benefits are a necessary cost of doing business
◦ 84% of employers agree Health benefits are an investment in human capital with a
measurable outcome
◦ 85% of employers agree Our company is highly supportive of improving employee
health
◦ 75% of employers agree We should provide cash or other incentives to motivate
employees’ use of preventive services
◦ 62% of employers who view themselves as “Leading Edge” agree, versus 40% of other employers

Copyright MBGH 2007 19
Readiness SurveyReadiness SurveyKey Findings on Cost SharingKey Findings on Cost Sharing
Drug co-pays are not considered barriers to optimal care by most employers
◦ However, employers viewing themselves as “leading edge” currently have or plan to adopt strategies to waive co-pays to encourage participation in DM programs, use of generics and to improve adherence in chronic disease treatments
Employers see cost-sharing as reducing physician visits
Employees need to know their out-of-pocket costs to make informed decisions to obtain health services
Mandating use of generics is a major employer strategy

Copyright MBGH 2007 20
Readiness SurveyReadiness SurveyKey Findings on IncentivesKey Findings on Incentives
Employers prefer incentives rather than disincentives
An increasing number of employers will provide strong incentives for completing health risk assessments
Employers would rather pay employees to select better physicians and hospitals, than to pay providers for higher quality care
Employers want to incentivize employees to select quality providers – but they don’t believe there is sufficient information on doctors and hospitals to enable people to make informed decisions
Employer believe workers would be willing change providers if they understood how quality varies and impacts outcomes
“Leading Edge” employers are twice as likely as others to provide incentives for encouraging preventive care, use of quality providers and designated Centers of Excellence

Keys to Effective Value-Based Keys to Effective Value-Based Benefit DesignBenefit Design
Getting individuals engaged in producing good health outcomes
Using economic incentives to influence consumer behavior and aligning them with outcomes the employer wants to achieve
Aligning consumer incentives with economic incentives for providers and other suppliers of health and health care services
Tiering medical services/coverage by evidence of effectiveness - and providers by evidence of performance
Using co-pay levels to steer individuals toward effective services and high performing providers
Linking timely information, coaching and support with economic incentives to create educated, skilled consumers to make knowledgeable choices and self manage their health and utilization

A Few Words about IncentivesA Few Words about Incentives
Rewards or Penalties…Incentives or Disincentives…
Carrots or Sticks …
“We use both - we just paint the stick “orange”

Copyright MBGH 2007 23
Keys to Using IncentivesKeys to Using Incentives
Incentives must be viewed as meaningful to individuals – based on culture, company loyalty, reduction of expenses, increase in benefits
Offer a variety to motivate employee engagement in wellness programs and encourage lifestyle-related behavior changes
Both financial and non-financial incentives seek to reward and penalize a variety of personal activities and/or achievements
Employers expect their financial investment will be offset by economic and other benefits of wellness
Employers want to emphasize a strong connection between healthy living and their ultimate objective of reducing the cost of health care
Align the reward with the cost of the underlying health benefit –e.g. premium differentials or contributions to HSA/HRA

Types of Incentives being offered Types of Incentives being offered by Employers Todayby Employers Today
Rewarding activity by reimbursing costs
Providing discounts on health coverage – i.e. premium differentials (increase or decrease)
Indicating eligibility for coverage or benefit contingent is on completing an activity – e.g. program participation, completing HRA
Making contribution to FSA or HRA
Making contribution to HSA through cafeteria plan
Offering cash, prizes, points or paid time off
Providing recognition on individual or team reaching goal

Copyright MBGH 2007 25
MBGH Smoking Cessation MBGH Smoking Cessation ProgramProgramSurvey - 2008Survey - 2008
Survey sent to MBGH members and employers of sister coalitions
51 respondents total
Mid to large, self-insured employers – primarily in the Midwest

Smoking Cessation SurveySmoking Cessation Survey

27Copyright@MBGH 2008

28Copyright@MBGH 2008

29Copyright@MBGH 2008

30Copyright@MBGH 2008

31Copyright@MBGH 2008

32Copyright@MBGH 2008

33Copyright@MBGH 2008

34Copyright@MBGH 2008

35Copyright@MBGH 2008

36Copyright@MBGH 2008

37Copyright@MBGH 2008

38Copyright@MBGH 2008

39Copyright@MBGH 2008
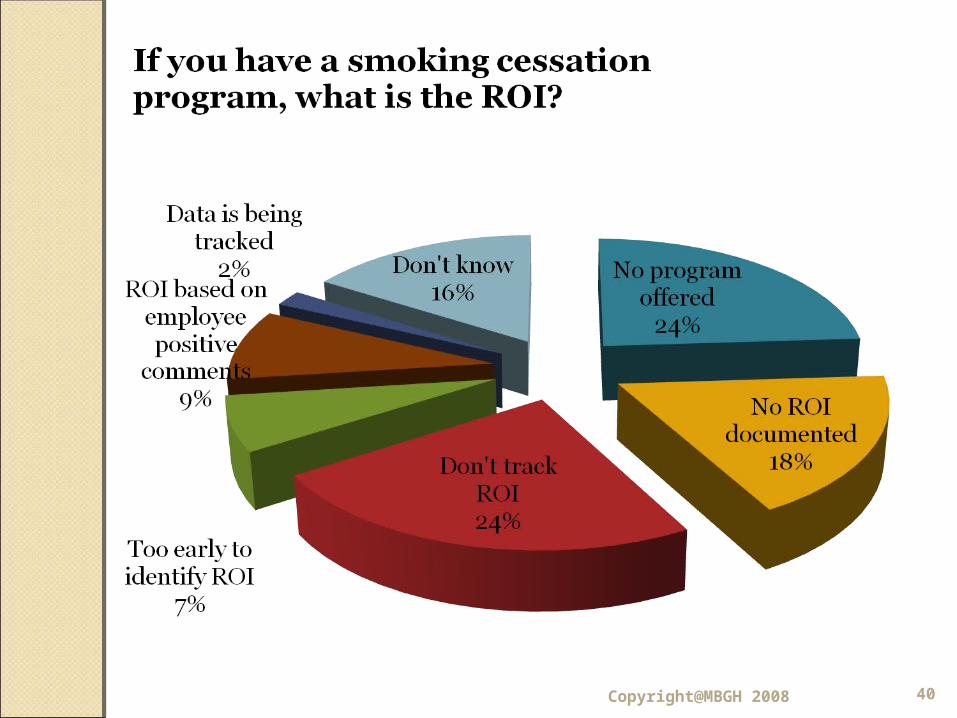
40Copyright@MBGH 2008

MBGH Obesity Management MBGH Obesity Management Benefits Survey - 2006Benefits Survey - 2006
Employer respondents offering obesity/weight management programs
◦61% - Weight watchers
◦52% - Onsite fitness facility
◦47% - Bariatric surgery
◦28% - Weight loss medications◦23% - Health club membership/medical
weight management programs
41 Copyright MBGH 2007

Obesity Management SurveyObesity Management Survey
Employer respondents offering obesity/weight
management programs19% of employers track employee BMI
Indicate the main entities that drive education/compliance with these programs is:
◦Employee self motivation
◦Physician direction
◦Peers
◦ Incentives
◦Spouse42 Copyright MBGH 2007

Finally….A Word on Finally….A Word on MeasurementMeasurement
ROI is More Than the Dollars Saved
Periodically review programs to determine efficiency and effectiveness
Best program measurements looks at:
◦ Process Measures - How well the program is working
◦ Outcome Measures - Whether or not it is achieving expected results
Don’t forget Self-Report – Getting feedback from employees is still valuable data!
Other ways to measure programs:
• Aggregate clinical and cost changes in the population
• Program enrollment & participant engagement
• Program utilization & web site visits• Number of participants reaching
goals• Reduction in overall trend• Reduction in emergency room use
and inpatient stays• Percent completing health risk
assessment• Absenteeism rate• Compliance and adherence with
medications• Satisfaction with programs

ResourcesResources
U.S. Dept of Health & Human Services - www.hhs.gov www.nih.gov
Partnership for Prevention - www.prevent.org/
Leading by Example: CEOs on the Business Case for Worksite Health Promotion - www.prevent.org/content/view/31/60
Centers for Disease Control and Health Promotion -www.cdc.gov/node.do/id/0900f3ec80059b1a – View CDC’s “Healthiest Nation” initiative
American Cancer Society Workplace Solutions- www.acsworkplacesolutions.com
AHRQ “Questions Are the Answer” – website to help consumers get involved in their health care - www.ahrq.gov/questionsaretheanswer/
AHRQ’s Consumer Engagement - www.ahrq.gov/consumer/
Article on Engaging Employees in Wellness http://hshackleford.wordpress.com/2008/02/01/byline-overcoming-challenges-in-engaging-employees-in-health-wellness/

ResourcesResources Welcoa – The Wellness Councils of America - http://welcoa.org
Wellsteps - ROI Calculator and wellness toolkit - http://wellsteps.com
HERO – Health Enhancement Research Organization -Wellness Audit/Scorecard - http://www.the-hero.org/scorecard.htm
Midwest Business Group Health – General Health, Benefits Info/Health Calculators http://www.mbgh.org
Integrated Benefits Institute – Information on Health and Productivity - http://ibiweb.org/
Publications and resources on nutrition, physical activity, and weight control listed by subject - http://win.niddk.nih.gov/publications/index.htm

Thank You!Thank You!
Cheryl Larson, Vice PresidentMidwest Business Group on Health
Phone: 312-372-9090 x3Email: [email protected]