endoeconomics fall 2015_lowres
TRANSCRIPT
FALL 2015A Journal Dedicated to Economic Issues Impacting GI ASCs and Practices
Project SonarA Solution for ChangePage 5
Treatment Using FMTPage 12
Clinical Co-Management AgreementsPage 14
The GI Journal of: “Improving the landscape of healthcare one surgery center at a time.”
FALL 2015 EndoEconomics | 3
Content
4 Message from the President
5 Project Sonar, A Solution for Change
8 What Every GI Physician Should Know from the
2015 GI Outlook Conference
12 Fecal Microbial Transplantation, Beyond the Treatment
of Recurrent Clostridium Difficile
14 Clinical Co-Management Agreements: Sharing Power,
Sharing Responsibility
16 Marketing Buzz: Best Practices for Building a Nimble
Marketing Strategy
18 Business Briefs: Addressing the GERD Treatment Gap
19 Business Briefs: Congress and Obama Administration
Agree on Two-Year Budget Deal
20 Front and Center
22 Current GI Opportunities
FALL 2015 ISSUE
EndoEconomicsby Physicians Endoscopy
Editorial Staff
Carol StopaEditor in [email protected]
Lori TrzcinskiManaging [email protected]
EndoEconomics™, a free quarterly publication, is published by Physicians Endoscopy, 2500 York Road, Suite 300, Jamison, PA 18929.
The views expressed in this publication are not necessarily those of Physicians Endoscopy, EndoEconomics™ or the editorial staff.
POSTMASTER: Send address changes to: Physicians Endoscopy, Attn: EndoEconomics, 2500 York Road, Suite 300, Jamison, PA 18929. Periodical postage paid at Merrill, WI. While every effort has been made to ensure the accuracy of EndoEconomics contents, neither the editor nor staff can be held responsible for the accuracy of information herein, or any consequences arising from it.
Advertisers assume liability and responsibility for all content (including text, illustrations, and representations) of their advertisements published.
Printed in the U.S.A.
Copyright © 2015 by Physicians Endoscopy.
All rights reserved.
All copyright for material appearing in EndoEconomics belongs to Physicians Endoscopy, and/or the individual contributor/clients and may not be reproduced without the written consent of the Physicians Endoscopy. Reproduction in whole or in part of the contents without expressed permission is prohibitied.
To request reprints or the rights to reprint- such as copying for general distribution, advertising, promotional purposes-- should be submitted in writing by mail or sent via email to [email protected].
5
12
14
Find out more at endocenters.com or find us on
The 2016 presidential election campaign has kicked into high gear, and the issue of healthcare in America has continued to be a prominent topic of discussion. As you would expect, accessibility and cost of care typically take center stage in the discussions. Although it is extremely unlikely that the words “ambulatory surgery center” (ASC) will ever cross the lips of any candidate, behind the scenes the data supporting ASCs as a growing part of the overall solution to both cost and quality continues to build.
In a recent study published in the journal Health Affairs, Kathleen Carey, PhD, a professor of health policy and management at Boston University, found that the average price increase for six common types of elective surgeries has increased substantially less in ASCs versus HOPDs between 2007 and 2012. To those of us on the ASC provider side of the healthcare industry, this comes as no surprise. Dr. Carey cited that insurers paid ASCs for a colonoscopy procedure an average reimbursement increase of 15.5% during the six years ending with 2012, while hospital outpatient departments (HOPDs) during the same period were paid an average increase of 35.7% for the same procedure. For other procedures the contrast was even more striking.
Within the same six-year period, insurers paid price increases averaging 76.7% for knee arthroscopies performed in HOPDs, while the same insurers experienced price increases of only 32.3% for the same procedure performed in an ASC. Dr. Carey concluded from the
study that ASCs have had a very limited, if any, success in pressuring HOPDs to lower prices, and further concluded that because of the tremendous leverage that hospitals enjoy in bargaining with third-party payers for improved reimbursement, the gap between the two sites of service continues to widen. Dr. Carey also suggested that CMS policies contribute to widening the gap.
At times there have been reasons to believe that the ASC versus HOPD reimbursement gap might be closed or at least narrowed. In April 2014, the Department of Health and Human Services – Office of Inspector General (OIG) published a report declaring that Medicare and Medicaid beneficiaries could save billions of dollars if CMS were to reimburse HOPDs for ASC approved procedures at ASC payment rates. The OIG report was careful to distinguish that their recommendation would only apply to patients for whom the clinical assessment suggested that the procedure could be safely performed in an ASC setting. For patients whose clinical needs suggest that the procedure should be performed in an HOPD setting, the higher Outpatient Prospective Payment System (OPPS) payment would be retained. While I felt strongly that the OIG report and recommendation made common sense, it clearly has gone nowhere and the playing field is increasingly unleveled via CMS annual updates.
In September 2015, Senator Crapo from Idaho introduced Bill S.2071 entitled “Ambulatory Surgical Center Quality and Access Act of 2015”. This proposed legislation contains several elements; however, three things struck me as key to all ASCs and patients.
• The first provision is that CMS’ annual updates (reimbursement adjustments) for ASCs be equal to
the HOPD fee schedule increase beginning in 2016 and for each year thereafter. This would help stop widening the gap.
• The second key feature is that it requires, to the extent that there are quality measures implemented by CMS for HOPDs, that they are also applicable, measurable and reportable by ASCs. All such data, including side-by-side comparisons for each measure, must be made available on the website Medicare.gov by geographic regions within the US.
• The third proposed legislation would require that CMS publish (along with the quality reporting indications mentioned above) comparisons of the Medicare payment and beneficiary copayment amounts by procedure when performed in an ASC versus an HOPD within the same geographic area.
Once again, I found this proposed legislation, which has been sent to committee, to be an important recognition of the need for better knowledge, better data and increased transparency within healthcare. But don’t get too excited, because Washington lawmakers give the bill only a 2% chance of getting through committee and only a 1% chance of enactment. Hopefully that will change.
As we move closer to 2016 and the next big election, maybe we can share some measure of renewed hope that politics as usual won’t prevail this time around, and someday logical, common sense solutions to the problems we try to confront in healthcare today will get the attention they deserve.
I hope you enjoy this edition of EndoEconomics!
4 | EndoEconomics FALL 2015
BARRY TANNERPresident and CEO,
Physicians Endoscopy
the PresidentMessage from
FALL 2015 EndoEconomics | 5
Introduction
Driven by mul-tiple indepen-dent forces, gastroenterolo-gists today are being forced to deal with mas-sive change to the way we man-age and structure our practices and the way we provide care for our patients.
Changes in reimbursement, driven by a desire by the CMS and commercial payers to control costs, have pushed our reimbursements down and com-pressed our margins. No procedure is more vulnerable to these market forc-es than colonoscopy, a mature service that drives most of the revenue of a GI practice.
Structural changes driven by the Triple Aim and the Affordable Care Act have
resulted in a focus on population health defined as “the health outcomes of a group of individuals, including the distribution of such outcomes within the group,”i thus requiring providers to focus on their entire population of patients with specific diseases rather than the traditional “one at a time” approach.
The focus on population health will impact our reimbursement as we move from fee for service (FFS) to value based payments (VBP). The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA)ii signed in April creates a Merit-Based Incentive Payment System (MIPS) which, beginning in 2019, will convert FFS into a VBP system with the goal of the majority of physician income being value based, and provides incentives for practices to embrace Alternative Payment Models (APM) for patients across their commercial and Medicare patientsiii.
By Lawrence Kosinski, MD, MBA, AGAF, FACG
A Solution for Change
Project Sonar
LAWRENCE KOSINSKI, MD,
MBA, AGAF, FACG
6 | EndoEconomics FALL 2015
Power shifts driven by consolidation in the hospital industry have spurned the development of powerful health systems, well-funded and focused on building market share through the pur-chase of our primary care base and se-lect hospital-based specialists. The new power of the health systems is threaten-ing the previous power and position of the payers as they are both competing in the same space. This can open op-portunity for well managed large gas-troenterology practices to build a better relationship with their payers.
Disruptive technologies, funded by The Recovery Act which injected over $30B into the Health Information Technol-ogy industry, have revolutionized how we document the care we provide and communicate with each other and with our patients. Much like Moneyball in baseball, big data will drive very signifi-cant change in the way we provide care.
The management of chronic disease is the “elephant in the room,” responsible for over two-thirds of the total cost of healthcare expenditures today. Gastro-enterologists can assume a key posi-tion in this space, but it will require us to change our focus from preventive care to chronic care management. This is critical for our futures as it will allow us to move from the commoditization of our procedures to the development of a competitive advantage for our cogni-tive skills.
The wild card in all of this is consumer-ism which will be a major game-changer. High deductible plans which have re-sulted in a new focus on retail pricing will drive us to compete in this space. Social media has replaced our previous proprietary patient satisfaction tools and has exposed our weaknesses. We have to adapt to the power of the consumer if we are going to survive and thrive.
Management of Chronic Disease
The major chronic disease category which drives significant revenue in a GI
practice is Inflammatory Bowel Disease (IBD). A typical GI practice may derive about 25% of their revenue from the management/treatment of IBDiv, which requires significant knowledge and ex-pertise and, as such, should represent a competitive advantage for GIs. Un-fortunately, most GI practices have not leveraged this opportunity.
Data from BlueCross BlueShield of Il-linois (BCBSIL) obtained in 2012 re-vealed that their average IBD spend is $11,000 per commercial patient per year for Crohn’s Diseasev. Over 50% of this spend is on inpatient treatment for complications of this condition. Unfor-tunately, gastroenterologists receive only 3.5% of this spend despite our being the most knowledgeable physi-cians of IBD. Tremendous variation in physician practice and hospitalization rates exists, which may persist even when normalized for patient risk and comorbidities. Clearly there is an opportunity to improve care management and de-liver value.
We cannot master this op-portunity without engaging our patients. Only a third of patients who are admitted to a hospital for a compli-cation of IBD were seen by a provider within 30 days prior to the admission. This is the result of our “reactive medicine model” where physicians are often not engaged until the patient realizes they have a problem that they cannot fix themselves. Like submarines, patients “run silent and run deep” surfacing only when they are in trouble and need help. Unfortunately, by that time serious complications may have already ensued and they need hos-pitalization.
Project Sonar
Recognizing the need to address care management and patient engagement for patients with IBD, the 45 physician Illinois Gastroenterology Group (IGG)
developed Project Sonar, a care man-agement solution for patients with IBD in 2013. Project Sonar utilizes a team-based approach with Nurse Care Man-agers (NCMs) and Physician Medical Directors (PMDs) to coordinate care for patients with IBD, along with Clinical Decision Support (CDS) and enhanced patient engagement.
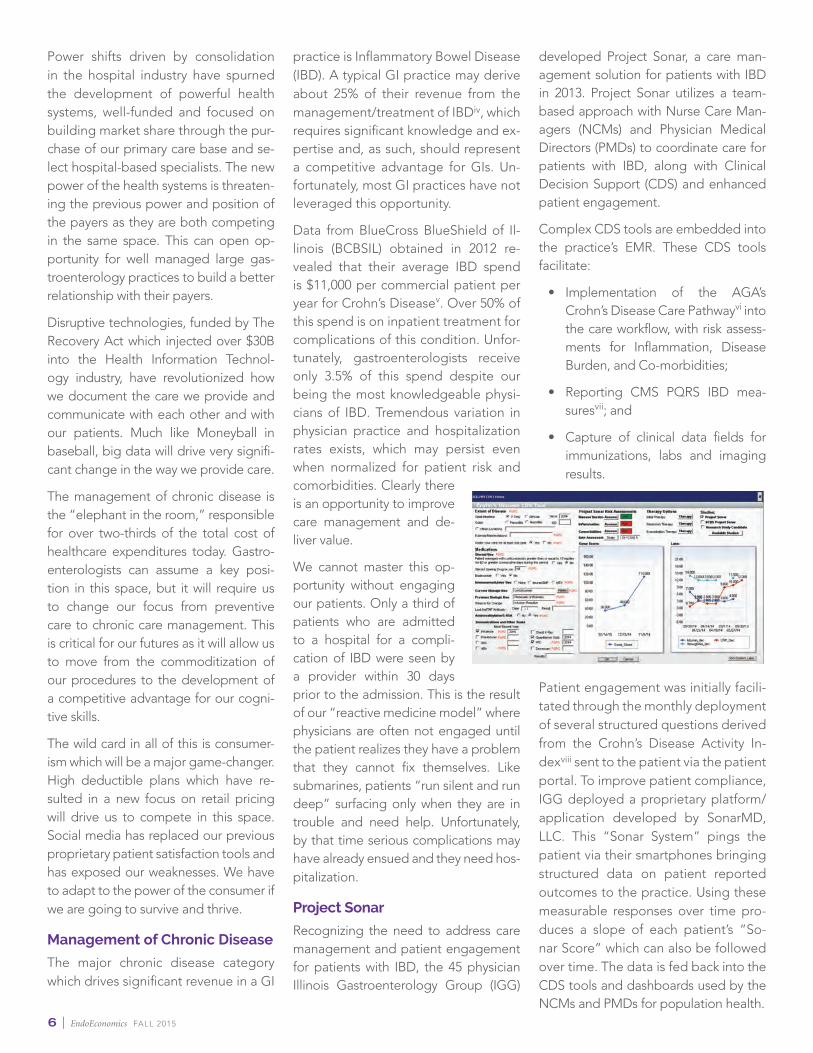
Complex CDS tools are embedded into the practice’s EMR. These CDS tools facilitate:
• Implementation of the AGA’s Crohn’s Disease Care Pathwayvi into the care workflow, with risk assess-ments for Inflammation, Disease Burden, and Co-morbidities;
• Reporting CMS PQRS IBD mea-suresvii; and
• Capture of clinical data fields for immunizations, labs and imaging results.
Patient engagement was initially facili-tated through the monthly deployment of several structured questions derived from the Crohn’s Disease Activity In-dexviii sent to the patient via the patient portal. To improve patient compliance, IGG deployed a proprietary platform/application developed by SonarMD, LLC. This “Sonar System” pings the patient via their smartphones bringing structured data on patient reported outcomes to the practice. Using these measurable responses over time pro-duces a slope of each patient’s “So-nar Score” which can also be followed over time. The data is fed back into the CDS tools and dashboards used by the NCMs and PMDs for population health.

FALL 2015 EndoEconomics | 7
The success of Project Sonar on a 50 patient pilot in 2013 led to a partnership between IGG and BCBSIL in 2014 to develop a specialty-based Intensive Medical Home (IMH), a joint initiative to improve the care of patients with Crohn’s Diseaseix. The IMH utilizes the Project Sonar structure in an attributed population of IBD patients. IGG receives a sup-plemental PMPM care management payment for each at-tributed/enrolled patient and a shared savings opportunity at the end of each study period.
The data produced from the CDS tools and Sonar Scores creates a unique set of physician risk assessments, medi-cal decisions and patient reported outcomes not typically available in most EMRs. These data are used to refine the care provided through the development of care algorithms, which update the CDS tools and the content of the smart-phone app.
Conclusion
It is time for GI practices to differentiate and add chronic disease management to their portfolio of services. This will provide the market what it needs in this time of cost con-tainment. This strategy can actually increase the revenue of our practices by saving cost that is currently being spent on the care provided by others. Three pillars are essential to our success:
1. Changing our focus from one patient at a time to im-proving the health of populations;
2. A team approach that embraces mid-level professionals, care managers, social workers, dieti-tians, pharmacists and others is required; and
3. Engaging patients as partners in their care alongside their healthcare team is crucial.
All of this requires changes to how we structure the policies, procedures and compensation models for our practices. In ad-dition, we need to move out of the constraints of our EMRs and embrace technologies that are developed specifically for pop-ulation health. Incorporating CDS tools and a patient engage-ment platform will be essential components for GIs to manage chronic disease.
Gastroenterologists can survive and thrive in the new popu-lation health. Through engaging patients, decision support and demonstrating value, we can establish our competitive advantage.
i http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1447747/ii https://www.congress.gov/bill/114th-congress/house-bill/2iii Gastroenterology, Vol. 147, Issue 4, p927–929iv Illinois Gastroenterology Group Data v BCBSIL Datavi http://campaigns.gastro.org/algorithms/IBDCarePathway/vii http://www.gastro.org/practice-management/quality/quality-reportng/digestive-
health-recognition-program-dhrpviii Best WR, Becktel JM, Singleton JW, Kern F Jr. (March 1976). “Development of
a Crohn’s disease activity index. National Cooperative Crohn’s Disease Study.” Gastroenterology 70 (3): 439–444. PMID 1248701.
ix http://www.bcbsil.com/company-info/news/news?lid=i18dwg7e
Lawrence Kosinski, MD, MBA, AGAF, FACG is one of the managing partners of the Illinois Gastroenterology Group, a 48 physician GI practice in Chicago that owns multiple endoscopy centers. Dr. Kosinski is also the Clinical Practice Coun-cilor on the board of the American Gastroenterological Association and is a mem-ber of the board of directors of Advocate Sherman Hospital.
8 | EndoEconomics FALL 2015
Each year, I have the privilege of attend-ing two outstanding practice manage-ment conferences specific to the GI industry: GI Roundtable (GIRT) and GI Outlook (GO). These meetings pro-vide high-quality information relevant to health policy and practice manage-ment for gastroenterology practice leaders and administrators. Both con-ferences attract the best of the best in terms of thought leaders, industry ex-perts and physicians.
GO, held this past August, is co-spon-sored by the ASGE and the AGA Insti-tute, while GIRT, held this past March, is run by Thomas Deas, MD, MMM; Klaus Mergener, MD, PhD, MBA; and Bergein Overholt, MD.
Year after year, these conferences in-creasingly provide excellent information and resources. However, it’s unfortunate that only a few hundred out of almost 13,000 gastroenterologists practicing in
this country usually attend. This leaves those physicians who do not at-tend less in-formed of what is happening across the industry and on the radar of our GI leaders.
Many physicians who do participate tend to be from the larger practices — those that have succeeded in merging practices or bringing together a large consortium of physicians within a spe-cific geographic location. However, it has become noticeable that there is a growing presence among the solo prac-tice physicians and those from smaller groups, most likely because they are feeling the pain of remaining indepen-dent and challenged to find ways to keep their practices afloat. All who do
participate in these conferences, clinical and non-clinical, recognize the informa-tion provided to be of significant value and appreciate the ability to network with like-minded peers.
I’ve been fortunate to attend both these conferences over the years, which brings the added pleasure of catching up with the partners of Physicians Endoscopy and speaking with a number of physi-cians and practice administrators over a few days of intense discussions. It’s amazing to learn what physicians can do and are doing when they band togeth-er, which isn’t easy as it requires strong leadership, valuable time and a lot of determination, as well as a balanced sense of compromise.
I had the opportunity to sit and listen to what the experts said at the recent GO conference.
Topics of significant attention included the continued transformation of the
CAROL STOPA
By Carol Stopa, VP, Business Development, Physicians Endoscopy
The 2015 GI Outlook ConferenceWhat Every GI Physician Should Know From

FALL 2015 EndoEconomics | 9
healthcare delivery system, shifts in re-imbursement, consolidation and lever-aging economies of scale. GI physicians and practices will have to adjust to the new realities, including financial, as-sociated with providing high-quality GI care. More than ever, the GI clinical and practice operations teams must work together to ensure the continued success of the GI practice. Physicians will need to not only learn to survive the changing healthcare delivery sys-tem, but thrive in it.
I thought it might be beneficial to provide a brief sampling of some of the presentations and discussions from GO for those who did not have a chance to attend.
Consolidation and Transparency James Leavitt, MD, from Gastro Health in Miami presented on “The Future Be-longs to the Doctor.” He discussed how healthcare reform will affect our future. I’ve listened to Dr. Leavitt present many times, and he always delivers a passion-ate and well-attended session.
Dr. Leavitt states that over the next five years, consolidation and transparency will be the dominant theme. There will be massive consolidation of health sys-tems, and payers will mandate a tightly managed referral network. Practices will need to demonstrate and deliver value (quality/cost) as there is a shift from volume-based to value-based reim-bursement models. Dr. Leavitt believes it is the obligation of physicians to take control of their future, and why wouldn’t they want to? If physicians want to be a real force and have a voice at the table, he says physicians need to think and act bigger — take control and position themselves as a stronger, unified force who can negotiate and demand what they want and need.
If physician groups don’t consolidate, Dr. Leavitt believes it will results in a loss of autonomy. Hospitals are motivated to employ physicians, resulting in doctors under pressure to act in compliance with the goals of their employer rather than the interest of their patients. Physicians will lose autonomy and leverage, reduc-ing competition from effective physician
group aggregation. Reduced competition will convert to higher prices. Employment of physicians and acqui-sition of practices by hospitals, along with hospitals purchasing ambulatory surgery centers, are resulting in more and more ser-vices paid at higher outpatient rates. This results in a significantly diminished harmony with what Dr. Leavitt refers to as the “Triple Aim” — to control the experience of care, population health and per capita cost.
Dr. Leavitt, who is part of a large, suc-cessful practice organization of over 60 GI physicians, discussed the im-portance of becoming the group of choice, which requires hard work and discipline. Consolidation and a strat-egy to remain independent are driving factors. Physicians need to continually demonstrate value, and leverage their strength by joining forces to ensure the doctor remains in control.
According to Dr. Leavitt, a strategy to remain independent takes a tightly in-tegrated practice governance with in-ternal accountability, EMR with robust regional connectivity, highest tier payer recognition, strong physician leadership and a turnkey solution for Accountable Care Organizations/Clinical Integrated Networks (ACO/CIN) or payment meth-odology. Dr. Leavitt outlined what he considers five required competencies: 1) ability to design, organize and manage an efficient and effective clinical delivery system; 2) ability to integrate care across time, settings, providers and geogra-phy; 3) ability to innovatively price and cost account for care delivery; 4) abil-ity to rationally distribute premium and potential dollar savings; and 5) ability to live and thrive simultaneously in two potentially contradictory models for a significant period of time.
Understanding Your Online Reputation
Several interesting presentations were delivered related to social media and the physician’s online presence. When you think about a changing landscape, this is probably one of the most relevant year over year, as our world of connect-ing with one another via the Internet continues to advance. The Internet has become a significant resource for infor-mation, making it easy to connect with people while providing a platform for personal opinions and commentary.
An important use of social media that many physicians overlook relates to

10 | EndoEconomics FALL 2015
understanding your online reputation. David Johnson, MD, MACG, FASGE, chief of gastroenterology at Eastern Virginia Medical School in Norfolk, discussed why physicians should care about their online reputation. During his presentation, “Understanding Phy-sician Online Reputation: Boot Camp for the GI,” he stated that physician evaluation websites (PEWs) are grow-ing in their influence. Over 80% of in-ternet users search online for health information, and 20% of their searches are about a specific provider.
Dr. Johnson believes the most sig-nificant values for which physicians are graded online are doctor punctuality/wait times, quality of nursing and non-nursing staff, knowledge/makes correct diagnosis and bedside manner.
The bottom line is creating a great on-line reputation for yourself. Dr. Johnson provided eight starter tips: 1) remember an ounce of prevention is worth a pound of cure; 2) be proactive about asking for honest feedback; 3) consider giving pa-
tients a “pop-off valve” — a means for them to vent frustration — such as an email address like [email protected]; 4) don’t try to attack nega-tive reviews; rather aim to provide overwhelming positive information; 5) on PEWs that receive a lot of traffic, respond to negative reviews in a posi-tive way; 6) claim/create free profiles on PEWs with highest impact; 7) consider purchasing advanced profiles; and 8) aim to control search results by creating a variety of positive outlets for informa-tion about yourself.
The Key to Population Health
In his presentation on “Payment Re-form: Contracting for Population Health Management,” Lawrence Kosinski, MD, MBA, AGAF, FACG, from Illinois Gas-troenterology Group in Elgin (a group of 45 GI physicians) gave an enlight-ening presentation stating that the key to population health is providing value in a risk-based environment. The objective is to increase the amount of health people receive out of each dol-
lar spent; it is the aggre-gate management of that population and its respective components.
To find their place in the population health chain, Dr. Kosinski be-lieves physicians must accept risk – becoming accountable, explor-ing alternative payment models, considering a practice redesign, focus-ing on patient engage-ment, providing data reporting/data analytics and showing financial responsibility.
Dr. Kosinski further dis-cussed alternative pay-ment models and the ex-pected path of payment
transformation from a fee-for-service to a fee-for-value model. Particularly inter-esting was his discussion on “Project Sonar,” an intensive medical home busi-ness model based on shared savings that he has created. Note: Read more on Project Sonar in this issue.
In summary, Dr. Kosinski says it’s time for physicians to abandon their depen-dence on fee-for-service reimburse-ment. He advises physicians to work with payers and to solve problems, and consider redesigning their practice with a focus on team-based integrat-ed care, technology, data and patient engagement.
Defining a Model Bundle
In an engaging session by Charles Accurso, MD, FACG from Digestive HealthCare Center in Hillsborough, New Jersey, he discussed a growing national movement towards value-based contracts and defining a model bundle that includes all costs connect-ed to providing the colonoscopy.
According to Dr. Accurso, physician leadership is a key driver to effective-ly implement such a program. While changing physician behavior can be difficult, it has the highest potential re-turn, and alignment of financial incen-tives reduces the difficulty.
In the presentation titled “Implement-ing Bundled Colonoscopy Contracts into GI Practice,” Dr. Accurso also states that it is important to refocus care and understand how to create success in a fee-for-quality/value mod-el. Physicians need to work together towards shared/full risk, change the spirit of the relationship between the payer and the provider, and to always remember that patients are at the cen-ter of care. Dr. Accurso will share more on this topic in the next edition of EndoEconomics.

FALL 2015 EndoEconomics | 11
Understanding Your Value
An enlightening presentation was pro-vided by Tom Deas, MD, director of physician development at North Texas Specialty Physicians in Fort Worth. In his presentation “Know Your Practice, Know Your Strength,” Dr. Deas recommends that physicians need to understand their value to the payers in terms of cost ef-ficiency, quality of care, quality of service and patient satisfaction. In other words, to know your practice is to understand your costs to the health plan — it is un-derstanding your costs of doing busi-ness, and knowing your patient sources and keeping them satisfied. Equally important is knowing your healthcare market, as well as the people you will need to deal with on the payer’s side. Dr. Deas believes physicians need to be prepared for the future as fee-for-service payments will continue to decline for both government and commercial pay-ers; new value-based payment method-
ologies will evolve, such as bundled pay-ments, performance-based payments, capitation and global payments; and electronic records, decision-support and population management tools will produce added value to payers.
Plan Now for 2016
These are just a sampling of the type of quality and intuitive presentations you will hear at a GO and GIRT conference. There will be many relevant discussions that shouldn’t be missed, including topics on private payer perspectives, successful negotiating strategies, phy-sicians experience in ACOs, patient en-gagement strategies and preparing for future challenges.
The GI Roundtable 2016 (http://gir-oundtable.com) is scheduled for March 10-12 in Fort Worth, Texas, while GI Out-look 2016 (http://asge.org) is planned for August 5-7 in Washington, D.C. If you
haven’t had the chance to attend in the past, make it a point to go to at least one of these conferences next year, or have someone from your practice attend. In any case, as Physicians Endoscopy’s on-going commitment to all GI physicians, we will continue to provide relevant information from each of these confer-ences, as well as other business-focused meetings. While you continue to work in your business daily, we can help you work on the business year round.
Carol Stopa is a vice president of business development at Physicians Endoscopy. Carol is responsible for developing new market initiatives as well as identifying and generating qualified business opportunities within the physician community in regards to new partnerships, acquisitions and hospital/health system joint ventures. She is also the editor-in-chief for EndoEconomics. Prior to joining the PE team, Ms. Stopa worked in clinical and administrative healthcare including mental health centers, correctional facilities, and psychiatric healthcare management companies. She may be reached at [email protected].

12 | EndoEconomics FALL 2015
Do your patients ask you a lot of strange questions? Since I’ve begun doing fecal microbiota transplants (FMT), here are some of the typical questions I’ve been getting: • “Is the FMT donor fat?”• “Was the FMT donor breastfed?”• “I have two great FMT donors
and don’t want to hurt anybody’s feelings. Could you mix their stools?”
• “How do you extract the stool from the FMT donor?”
• “What if it doesn’t agree with my own poop?”
Today, FMT has one approved use: the treatment of recurrent Clostridium Difficile colitis. For that use, the suc-cess rates are extremely high. Of all the things we prescribe as doctors, this is one we can feel unambigu-
ously proud of. It’s fast, effective, and inexpensive. This is no small mat-ter: about 30,000 Americans die every year of Clostridium Difficile. Millions of dollars are spent treating this infec-tion, which can be devastating. One can administer FMT though the up-per GI tract or directly into the colon. Since Clostridium Difficile colitis affects the colon, today most gastroenterolo-gists administer it via colonoscopy.
As a result of this success, some patients will now try anything to convince you that they need a fecal transplant to cure a whole host of maladies. Others will refuse one even when they have been debilitated by years of infectious colitis and multiple hospital admissions.
But will there be other clinical uses for fecal transplant?
To do justice to this question, it is important first to consider the topic of the mi-crobiome.
Recently, FMT has inspired the medical commu-nity to look at this “newly discovered organ” we had been ignoring for so long. The “organ” is our microbiota: an enormous number of cells living in an organized dynamic ecosystem and playing so many roles in virtually ev-ery aspect of our health and disease. Our gut microbes interact with each other and with us, the host. We have coevolved and developed a mutu-ally beneficial relationship: we provide them with food and shelter and they help with our nutrition, our ability to fight infections, our metabolism, and
By Caterina Oneto, MD
Beyond the Treatment of Recurrent Clostridium Difficile
Fecal Microbial Transplantation
CATERINA ONETO, MD

FALL 2015 EndoEconomics | 13
even our neurologic development. Their study is particularly fascinating because it brings together medicine, ecology, and evolution.
To better understand the microbiota, we have used several tools that have allowed us to gather an enormous amount of information: more information than we can actually interpret. In a sense one could say that technology is ahead of science. Today, for example, we have the ability to sequence the genetic material of the organisms that live in the gut instead of culturing them.
We have observed that the microbio-ta of patients with IBS, IBD, metabolic syndrome, obesity, autoimmune dis-eases, and even autism is different from the “normal” microbiome, but associa-tion and causation are, of course, two different things.
Moreover, it has become clear that in order to understand the effects of the microbiota, we need to not only identify these microorganisms but also measure the products of their metabolism. The mere presence of a particular microbe or a group of microbes may not be as important as what they are doing.
FMT has also helped to advance our understanding of the microbiome and its role. For example, if a disease or a trait can be transmitted though FMT, that could support at least some role of the microbiota in causing that disease or trait.
But studying the effects of stool transplant is a lot more complicated than studying the effects of a regular drug. Even though stool when used for FMT is now considered a drug, there are many unknowns: dose, ideal route of administration, mechanism of action, etc. Also, each individual person’s stool is different, like a fingerprint. Therefore, it may interact in a unique way with the recipient’s microbiota.
A few months ago, we started to enroll patients in a multicenter study with doctors at Montefiore, Yale, and Concorde Medical Group to investigate the possible use of FMT in IBS-D (diarrhea predominant IBS).
IBS-D, especially when it is moderate to severe, can be a debilitating disease and very frustrating to treat. Most pa-tients have typically tried conventional therapies like special diets, probiot-ics, antidiarrheals, antispasmodics, and sometimes antibiotics like rifaxi-min, which was recently approved for this use.
Why are there currently so many differ-ent conventional therapies prescribed for IBS? Likely this is because the patho-genesis of IBS is so little understood. Visceral hypersensitivity, low-grade inflammation, and dysbiosis have been thought to play a role. Regard-ing dysbiosis, we know that there is an abnormal microbiota. The num-bers of lactobacilli and bifidobacteria, for example, are lower in patients who suffer from IBS than in those who don’t. Also their microbiota seems to be less diverse. Replacing “good bacteria” is the idea behind the use of probiotics, which seem to help some patients. But why are they not sufficient to cure IBS in most patients? The answer is not clear today. Perhaps the numbers of bacteria that survive the passage through the GI tract are not sufficient. Or maybe in order to change that whole ecosystem that is our microbiota in a permanent way, one has to modify it more radical-ly instead of just adding a few specific strains of bacteria.
Despite the unanswered questions about IBS-D, we hypothesize that IBS-D is a condition that occurs secondary to an altered microbiota in the small bowel. Therefore, instead of adminis-tering the FMT via colonoscopy as we would do for recurrent Clostridium Dif-
ficile colitis, we are using “poop cap-sules.” It’s a 6-month randomized, pla-cebo-controlled trial and at 3 months there is a crossover, so by the end of the study 100% of the patients will have re-ceived the active drug.
As doctors and investigators, we are eager to help our patients with this very debilitating disease. In the process, we also hope to learn more about the microbiota, its effects on our health, and how this new knowledge will lead to exciting new therapies.
To learn more about this trial, go to clinicaltrials.gov
Dr. Caterina Oneto is a board certified gastroenterologist affiliated with NYU Langone Medical Center and a member of Concorde Medical Group. Her special interests include IBD (Crohn’s disease and Ulcerative Colitis), IBS (irritable bowel syndrome) and FMT (Fecal Microbiota Transplantation).
Caterina Oneto, M.D. @caterina_oneto | Twitter

14 | EndoEconomics FALL 2015
In healthcare, “gainsharing” has be-come somewhat of a dirty word over the past decade. Though the nega-tive characterization may be unjust, calling any relationship a “gainsharing arrangement” has fallen out of vogue in many circles due to pushback from legal counsel. However, the tenets that drive gainsharing are back in a big way, and often they are being effectu-ated through clinical co-management agreements (CCMAs). CCMAs are contractual agreements wherein a phy-sician or, more likely, a group of phy-sicians are engaged to provide man-agement and oversight for a particular set of clinical services. In this model, physicians, often in strategic partner-ship with a hospital, work to achieve greater efficiencies, cost savings, im-proved quality, and greater operating
efficiency. This article debunks some of the common myths about CCMAs. Myth #1: CCMAs are only applicable to orthopedic surgery. The most predominant specialty to embrace CCMAs as well as the earli-est adopter of the model has been orthopedics. As a result of the signifi-cant expenses traditionally tied to the implants used in orthopedic surgery cases, the magnitude of potential sav-ings when orthopedic surgeons are en-gaged under a CCMA has been exten-sive. These savings have helped fund many orthopedic CCMAs (sometimes directly, sometimes indirectly), which is one reason they have become so popular with both hospitals and phy-sicians. However, orthopedics is cer-
tainly not the only specialty that can benefit from the CCMA. Cardi-ology, urology, oncology, and gastroenterology are other exam-ples of specialties that have embraced CCMAs and have demonstrated benefits for their par-ticipants. While there may not be the same expansive opportunity for direct savings for these specialties in com-parison to orthopedics (although there are certainly savings to be achieved for any specialty or service), there are any number of benefits to be achieved that make the CCMA economically viable and strategically imperative for a host of specialties.
By Aimee Greeter, MPH
Sharing Power, Sharing Responsibility
Clinical Co-Management Agreements
AIMEE GREETER, MPH

FALL 2015 EndoEconomics | 15
Myth #2: CCMAs only apply to a hospital’s inpatient service line. Many people believe that CCMAs only apply to an inpatient service line. For example, when a hospital’s cardiovas-cular service line is being co-managed, there is sufficient scope of work to be done as well as resources to fund this work, and thus, the CCMA appears to be a natural “fit.” However, many am-bulatory surgery centers (ASCs), either wholly or jointly owned by hospitals, are also viable avenues for CCMAs. This practicality makes sense because ASCs, like hospital service lines, can also be made more efficient and more effec-tive as a direct result of active physician input and interaction into their opera-tions. And, as ASCs become a more popular location for a broader extent of clinical services, it is important that they are well-managed. Since many physician-owned ASCs have achieved this, ASCs that are owned (in total or in part) by a hospital also seek this same efficiency, and the CCMA provides the vehicle for achieving that goal. Myth #3: CCMAs are a great alterna-tive source of revenue. Compensation under a CCMA often includes two components: administra-tive services and incentive payments. Administrative services typically are compensated at a fixed rate per hour, up to a maximum number of hours per month. In contrast, the incentive pay-ments are normally a pool of funds held at-risk based on the physicians’ ability to reach pre-determined performance metrics. Previously, some physicians have thought that because of this pay-ment structure, CCMAs provide a po-tential “windfall” in terms of remunera-tion, that participating in a CCMA is a type of “get rich quick” scheme. While CCMAs yield an economic return to physician participants, in many cases,
on a per-hour basis, the return is less than what physicians could achieve by staying in the procedure or operating room and completing another case. Thus, a trade-off needs to be made wherein physicians recognize that while the compensation under a CCMA may not have the same economic benefit as their procedural work, there are other benefits to participating. As many phy-sicians have noted, this trade-off is well worthwhile when the time they spend on the CCMA helps improve their quality of life, improve staff relations, and makes the procedure room run more efficiently, among other benefits typically realized as a result of CCMA participation. Myth #4: CCMAs allow participants to maintain their own methods and independent goals. When a hospital or ASC engages phy-sicians through a CCMA, they agree to a partnership in which the physicians now have an influential voice. Success-ful CCMAs are those in which the phy-sician participants are enabled to make decisions that impact the services and operations that they are managing. This empowerment requires the hospi-tal or ASC to turn over the reins and allow the physicians to have the au-thority to effectuate true change. This change takes significant trust, but it is necessary to maximize success under a CCMA. In this model, there isn’t room for micromanaging, minimizing physi-cian participation, or soliciting but then not responding to physician input. On the contrary, the hospital or ASC agrees to give up some of their power and control in exchange for greater physician involvement and definitive improvements. Thus, suddenly there is shared power, but also a shared re-sponsibility for success, between the parties. Often this change in mindset
is significant, though it is necessary under a CCMA.
CCMAs frequently are considered a moderate form of alignment because they do not entail the same bound-aries seen in employment (i.e., a full form of alignment), but they are also much more robust than a simple medi-cal directorship (i.e., a limited form of alignment). These agreements, when correctly executed, allow physicians to have more decision-making power while also holding them accountable for demonstrable results. CCMAs achieve many of the benefits that have previously been associated with gain-sharing arrangements and do so in a legally permissible model that offers benefits for all participants.
For more information regarding clinical co-management agreements or other forms of alignment, contact Aimee Greeter ([email protected]) or visit our website (www.cokergroup.com).

16 | EndoEconomics FALL 2015
Gone are the days when you can build a five-year marketing plan and follow it goal-by-goal and tactic-by-tactic from day one through to the end. Marketing has evolved significantly in recent years, due in large part to the growing digital landscape and ever-evolving world of social me-dia; and these changes are requir-ing everyone from small grassroots nonprofits to Fortune 500 companies and everyone in-between to adopt nimble, adaptable strategies that are platform-agnostic. So, what exactly does that mean? As social media and PR guru Peter Shankman once said during a professional development workshop, “Embrace the concept not the medium.” Shank-man went on to say that if Twitter goes away, organizations will be tasked with finding new and equally effective ways to communicate with their stakeholders in 140-characters or less, i.e., Twitter isn’t what’s working – communicating in 140-characters or less is.
While the longevity of Twitter and other social media marketing channels remains to be seen, the pressure for organizations to be social and think digitally continues to mount. Think about your own practices, for example. Online reviews influence where patients go for care and younger generations are increasingly turning to their social networks for practitioner and facility recommendations. You certainly don’t want to be overlooked because you aren’t socially savvy and, as we often say, just because you aren’t present on a certain platform doesn’t guarantee people aren’t talking about you in that space. So, where does one start building a marketing strategy that’s ready for a digital world, addresses the needs and communication preferences of multiple generations and ultimately moves the needle? Research. Now, let’s discuss the role of data in forming your strategy.
Becoming data-driven
Without exception, research is the foundation of an effective marketing strategy. Research is, of course, multi-faceted. There’s the primary research you conduct with your existing stakeholders (patients, referral sources, affiliated practices, etc.), as well as the third-party research that helps you understand the climate, including any environmental factors and/or competitive threats that may augment or inhibit your ability to achieve the goals you will set in your marketing plan.
When establishing your primary research methods – think online surveys, phone interviews and, depending on the circumstances, focus groups – focus on gathering a representative sample of stakeholders. With your group(s) defined, it’s time to develop your questions. This is an opportunity to ask about everything from preferred communication channels and frequency to information gaps and further communication needs. This is also a great opportunity to address any pervasive myths and misconceptions. Once you have your data in-hand, it’s time to identify the strategies and tactics that will be used to help achieve your marketing goals. Which means we should take a few moments to talk about goal setting.
By Danielle M. Cyr, Vice President of Integrated Marketing, Co-Communications
BuzzMarketing
DANIELLE M. CYR
Marketing StrategyBest Practices for Building a Nimble

FALL 2015 EndoEconomics | 17
What are realistic marketing objectives?
Of course you want to have more positive online reviews floating in cyberspace than any of your competitors. And, you want your social media communications to be richly populated with raving fans. And, you want to be the go-to source for the “A-list” of media. And, you want your marketing to translate into increased patient and procedure volume. We get it. But, how does one know what is a realistic and reasonable goal?
When setting marketing goals and objectives, the two most important considerations are bandwidth and budget. For example, what is your practice capable of taking on? What are you willing/able to invest in making it work? While 20 percent of total revenue is a fairly common amount to allocate to one’s marketing budget, there are no hard and fast rules. Every organization has a different comfort level (and risk tolerance), as well as a set of preferred marketing channels to which these dollars should be allocated.
With all of this in mind, align your marketing goals and objectives with both your budget and bandwidth. Have your research findings in mind when you set these goals and objectives, and ensure you have benchmarks set up along the way. Don’t arrive at the end of the calendar/fiscal year finding that you either didn’t achieve your goals or invested significant marketing dollars in under-performing tactics when the data clearly showed an opportunity for budget reallocation early on in the execution process.
My goals are set. Now what?
With your goals clearly-defined, it’s time to determine what your overall strategy will be for achieving them. Focus primarily on patient communications, practitioner recruitment communications and/or referral source communications, to name a few. With your primary, secondary and tertiary audiences outlined, you can assess the communication channels and tactics that will allow you to reach and engage these audiences most effectively.
As you begin to assemble this list of channels and tactics, you want to maintain a laser focus on adopting and sustaining an integrated approach. What exactly does that mean? You
want synergy between your online and offline marketing activities and, regardless of the channel(s) through which you are communicating, you want the messaging to be consistent and your audiences to clearly understand that the messages are coming from one organization.
I figured out what to say and where to say it. How do I actually know if it’s working?
Every bit as important as what you say, how you say it and where you say it, is how you know if any or all of the strate-gies and tactics you have implemented are working. From the onset, it is imperative to know how your organization will define and measure success. The metrics you put in place should be both realistic and capable of being as-sessed on a periodic basis. As mentioned before, you don’t want to land at year-end only to realize your marketing bud-get could have been better allocated and the data-driven proof has been there for weeks or months if not quarters.
Given you will be implementing an integrated program, you’ll want to have your success metrics and benchmarks defined both by channel and goal. That is to say, you’ll want to know if your custom blend of strategies and tactics was effective in achieving your end goal AND which channel(s) made the greatest impact in achieving your objective(s). While some things are more challenging to measure quantifiably than others, take the time to make things as quantifiable as humanly possible.
While marketing requires a commitment of both time and resources to move the needle and generate tangible ROI, it is critical for preventing one’s practice from being a best kept secret and one’s expertise from being overlooked in the media space, on the speaking circuit and the list goes on. Be consistent, be creative, remain on-brand and be ready to reap the rewards of implementing a multi-channel marketing plan that moves the needle and takes your practice to the next level.
Danielle M. Cyr is vice president of integrated marketing for Co-Communications, a full-service marketing and public relations agen-cy with offices in Connecticut and New York. She can be reached at [email protected].
BuzzMarketing

Addressing the GERD Treatment Gap
Since their introduction to the market in the 1980’s, proton pump inhibitors (PPI) have become the mainstay of GERD treatment, moving the decades of sleep positioning research somewhat to the sidelines. Though PPIs are effective for the majority of the GERD population, approximately 20-30% of patients, referred to as refractory patients, continue to experience mild to moderate symptoms despite regular PPI usage, with 92% of these patients experiencing nighttime symptoms25. These patients fall into what has been called the Treatment Gap and present a significant clinical challenge for the PCP and GI medical communities due to the lack of treatment options for patients who continue to suffer26.
As a former professor of medicine at UC San Diego and a refractory GERD patient himself, Carl Melcher, MD, has experienced this Treatment Gap firsthand. Dr. Melcher’s story is like so many refractory patients. Dr. Melcher suffered with GERD for decades before being diagnosed with Barrett’s Esophagus in 2007. Luckily, his Barrett’s resolved itself after several years of high dose PPI therapy and lifestyle changes. Throughout his PPI therapy, Dr. Melcher remained symptomatic with extra-esophageal symptoms, including chronic rhinitis and throat clearing. In 2010, Dr. Melcher developed Clostridium difficile, two years before the FDA Safety Announcement regarding use of PPIs and the risk of developing of Clostridium difficile was issued.
Dr. Melcher wanted to find another treatment alternative to high dose PPIs for nocturnal GERD patients. As a strong proponent of positional therapy research, he founded Amenity Health to create an effective positional therapy system for patients with nocturnal symptoms. After several years of R&D, MedCline™ was developed to address the Treatment Gap in the GERD landscape.
MedCline™ is a positional therapy device for the treatment of nocturnal reflux, which is clinically proven to significantly reduce reflux symptoms27, episodes28 and esophageal acid exposure34. Its Cradle-Loc™ technology properly positions patients at an effective incline and on the left side for natural symptom relief. MedCline™ offers a practical solution allowing patients to easily implement lifestyle modifications in the comfort of their own bed.
Most of us know that a significant percentage of the population suffers from Gastroesophageal Reflux Disease (GERD), with some studies showing up to 28%1 with a diagnosis the US. But did you know that the majority (89%2) of GERD patients suffer with nocturnal symptoms? Such symptoms, including heartburn and regurgitation of liquid and/or food, not only make getting quality sleep difficult, but also expose patients to an increased risk of developing more serious health complications down the road.
Nocturnal reflux has been found to be an underlying risk factor for developing erosive esophagitis, peptic stricture, esophageal ulcerations, Barrett’s esophagus and adenocarcinoma of the esophagus3. In fact, while the risk of esophageal adenocarcinoma increases eightfold for those suffering with daytime acid reflux symptoms, the risk increases to 11-fold for those with nighttime symptoms4.
Current medical guidelines recommend lifestyle changes as the first line of defense against GERD. The two lifestyle modifications proven to be effective are weight loss and sleep positioning for nighttime symptom relief5. Incline positioning has been written into the clinical guidelines for both the American Association of Gastroenterologists6
(AGA) and American College of Gastroenterologists7 (ACG) due to its effectiveness at reducing esophageal acid exposure by helping the body naturally return refluxed content back to the stomach8, 9, 10, 11, 12, 13, 14, 15, 16.
Several medical organizations, such as John Hopkins Medical Center, Penn State Hershey Medical Center, the US Department of Veteran Affairs, the McKinley Health Center, the American Journal of Medical Sciences and Gastroenterology and Endoscopy News, include left-lateral positioning in their respective guidelines. Left-lateral positioning has been found to significantly decrease the frequency of acid reflux episodes as compared to sleeping on the right side or the back17, 18,
19, 20, 21, 22, 23, 24.
By Aaron Clark
BriefsBusiness
AARON CLARK
18 | EndoEconomics FALL 2015

10 Johnson L, De Meester T. Evaluation of elevation of the head of the bed, bethanicol and antacid foam tablets on gastro esophageal reflux. Dig Dis Sci 1981, 26:673-680.
11 Harvey RF, Gordon PC, Hadley N, et al. Effects with the Bed-Head Raised and of Ranitidine in patients with severe peptic esophagitis. The Lancet 1987, 2(8569): 1200-1203.
12 Stanciu C, Bennett JR: Effect of posture on gastro esophageal reflux, Digestion 1977, 15: 104-109.13 Kaltenbach T, Crockett S, Gerson LB. Are life style measures effective in patients with gastro
esophageal reflux disease? An evidence based approach. Arch Intern Med 2006, 166:965-71.14 Castell DO: Medical therapy of reflux esophagitis. Ann Intern Med 93:926-927, 1980.15 Richter JE, Castell DO: Gastroesophageal reflux: Pathogenesis, diagnosis, and therapy. Ann Intern
Med 97i93-103, 1982.16 Pope CE: Gastro esophageal reflux disease: Pathophysiology, diagnosis, management. Philadelphia,
WB Saunders 1983, 449-490.17 Khoury, Ramez M. Influence of Spontaneous Sleep Positions on Nighttime Recumbent Reflux in
Patients With Gastroesophageal Reflux Disease. The American Journal of Gastroenterology. Vol. 94, No. 8, 1999.
18 Patrick FG. Investigation of gastroesophageal reflux in various positions with a two lumen pH electrode. Gut 1970;11:659–67.
19 Shay SS, Conwell DL, Mehidru V, et al. The effect of posture on gastroesophageal reflux frequency and composition during fasting. Am J Gastroenterol 1996;91:54–60.
20 Kapur K, Trudgill N, Smith L, et al. Effect of sleep position on nocturnal acid reflux. Gastroenterology 1998;114:A167.
21 Skinner DB, Camp TF. Relation of esophageal reflux to lower esophageal sphincter pressures decreased by atropine. Gastroenterology 1968;54:543–51.
22 Tobin JM, McCloud P, Cameron DJS. Posture and gastrooesophageal reflux: A case for left lateral positioning. Arch Dis Child 1997;76:254–8.
23 Katz LC, Just R, Castell DO. Body position affects recumbent postprandial reflux. J Clin Gastroenterol 1994;18:280 –3.
24 Van Herwaarden, MA, Katzka, DA, Smout, AJPM. Samsom, M, Gideon, M, Castell, DO. Effect of Different Recumbent Positions on Postprandial Gastroesophageal Reflux in Normal Subjects. The American Journal of Gastroenterology 2000; Vol. 95, No. 10, 2000.
25 Toghanian S, Johnson DA, Stålhammar NO, Zerbib F.Brook RA, et al. Burden of gastro-oesophageal reflux disease in patients with persistent and intense symptoms despite proton pump inhibitor therapy: A post hoc analysis of the 2007 national health and wellness survey. Clin Drug Investig. 2011 Oct 1;31(10):703-15. ?
26 Subramanian, Charumathi Raghu, Triadafilopoulos, George. Refractory gastroesophageal reflux disease. Gastroenterology Report (2014) 1–13, doi:10.1093/gastro/gou061.
27 Allampati SK, Lopez R, Ray M, Birgisson S, Gabbard SL. Use of a Sleep Positioning Device Significantly Improves Nocturnal Gastroesophageal Reflux Symptoms. Am J Gastroenterol 2014; 109:S1–S39.
28 Person, EB, Rife CC, Castell DO, et al. A novel sleep-assist device prevents gastroesophageal reflux: A randomized controlled trial. Am J Gastroenterology 2013; 108:S1-S36.
Congress and Obama Administration Agree on Two-Year Budget DealLate evening (Oct 26th), Congressional leaders and the Obama administration announced a bipartisan agreement on legislation that funds the federal government for two years, raises the nation’s debt ceiling and staves off Medicare premium increases for beneficiaries, among other things. The final legislation, which responds to a number of quickly approaching fiscal deadlines and to upcoming leadership changes in the House that might have impacted the ability to strike such a deal, was passed by the House on Wednesday and is expected to pass in the Senate. President Obama has stated that he will sign the legislation into law.
Of great interest to ASCs is a site-neutral provision that stops the practice of hospitals purchasing off-campus facilities, such as ASCs and physician offices, and then charging the Medicare program and beneficiaries the higher hospital rates. The provision will apply to any outpatient department/physician practice acquired or established and wholly owned by a hospital after the enactment of the legislation.
BriefsBusiness
Available by prescription only, MedCline™ can be used as appropriate by PCPs and GIs as part of a patient’s treatment plan to provide much needed relief of nocturnal GERD symptoms for those patients suffering in the Treatment Gap.
Aaron Clark is the chief operating officer for Amenity Health, Inc. Mr. Clark leads all product development, clinical research, sales and marketing efforts at Amenity Health. Mr. Clark has a BSME from University of California at San Diego. For more information, he can be reached at [email protected].
1 Storr M, Meining A, Allescher HD. Pathophysiology and pharmacological treatment of gastroesophageal reflux disease. Dig Dis Sci 2000; 18: 93–102.
2 Mody, R., et al., Clinical Gastroenterol and Hepatol 2009;7:953-959.3 Lagergren, J, Bergstrom R, Lindgren A, et al. Sympomatic gastroesophageal reflux as a risk factor for
esophageal adenocarcinoma. N Engl J Med 1999; 340: 825-831.4 Lagergren J, Bergstrom R, Lindgren A, Nyren O. Symptomatic GER as a risk factor for esophageal
adenocarcinoma. N Engl J Med 1999; 340:825–831.5 Kaltenbach T, Crockett S, Gerson LB. Are life style measures effective in patients with gastro
esophageal reflux disease? An evidence based approach. Arch Intern Med 2006, 166:965-71.6 American Gastroenterological Association: Kahrilas PJ, Shaheen NJ, Vaezi MF, Hiltz SW, Black E,
Modlin IM, Johnson SP, Allen J, Brill JV. American Gastroenterological Association Medical Position statement on the management of gastroesophageal reflux disease. Gastroenterology 2008 Oct; 135(4):1383-91, 1391.e1-5.
7 American College of Gastroenterology: DeVault KR, Castell DO. Updated Guidelines for the Diagnosis and Treatment of Gastroesophageal Reflux Disease. American Journal of Gastroenterology, 2005; 100:190-200.
8 Hamilton, John W. et al. Sleeping on a Wedge Diminishes Exposure of the Esophagus to Refluxed Acid. Digestive Diseases and Sciences, Vol. 33, No. 5 (May 1988), pp. 518-522.
9 Khan, Bashir A. et al. Journal of Gastroenterology and Hepatology, Accepted article. doi: 10.1111/j.1440-1746.2011.06968.
FALL 2015 EndoEconomics | 19
As drafted, on January 1, 2017, Medicare will begin paying hospital-owned facilities bought or built after the bill is signed into law according to the ‘applicable payment system’ – the physician fee schedule rate for office visits and the ASC rate for outpatient surgical procedures. Outpatient departments, ASCs, physician offices or other off-campus facilities that are currently operating will be exempted from the payment changes.
For ASCs, this means that a hospital purchase and conversion would not result in the hospital being reimbursed by Medicare beyond the current ASC rate. With regard to physician offices, this provision responds to the concerns of many that hospitals were buying up physician practices and limiting the ability of those physicians to refer patients outside the hospital.
Reprinted with permission of ASCA. For more information www.ascassociation.org/budgetdeal.

20 | EndoEconomics FALL 2015
Sarah Malaniak, CASC, Administra-tor for Ambulatory Center for Endoscopy, was appointed to the Board of Directors of the NJ ASC Society. She was also named one of Becker’s ASC Review’s “Rising Stars: 62 ASC leaders under 40.” She obtained her CASC certification in 2014, is an active member of the NJAASC Association and serves as the ASCAPAC representative for New Jersey.
ASGE Endoscopy Unit – Recognition Program: Center Congratulations!The American Society for Gastrointestinal Endoscopy (ASGE) has recognized each of the centers below as part of its program, specifically dedicated to promoting quality in endoscopy in all settings where it is prac-ticed in the United States. Each of these centers is one of more than 400 endoscopy units to be granted the recognition since 2009. The ASGE Endoscopy Unit Recog-nition Program honors endoscopy units that have demonstrated a commitment to patient safety and quality in endoscopy as evidenced by meeting the program’s rigorous criteria, which includes following the ASGE guidelines on privileging, quality assurance, endoscope reprocessing, CDC infection control guidelines and ensuring endoscopy staff competency.
• Berks Center for Digestive Health, Wyomissing, PA
• Burlington County Endoscopy Center, Lumberton, NJ
• The Endoscopy Center at Bainbridge, Chagrin Falls, OH
Berks Center for Digestive Health sponsored and participated in Nirav’s Run—a 5 mile run, 1 mile run, and
DHA Endoscopy Center par-ticipated in Get Your Rear in Gear Boston 2015, which was held on September 19th at DCR Mother’s Rest at Carson Beach in Boston, MA. The event featured a 5k run/walk and a one mile walk to help raise funds for colon cancer awareness efforts in the Boston area. Monies raised stays in the community, helping with prevention, early detection and treatment, and healthy living projects for this disease.
The Endoscopy Center of West-ern New York attended the 2015 Fall Western New York Health Expo at the East-ern Hills Mall in October. The fair offered an opportunity to educate the public on colon cancer screening.
Endoscopy Center of Niagara celebrated International Infection Prevention
wellness fair. The Dr. Nirav Patel Founda-tion was created in memory of Nirav Patel, MD, who cared deeply about medicine and public health. He was passionate about addressing health issues and developing changes to improve people’s quality of life and thereby improving whole communi-ties. The event proceeds go to local health related organizations.
Scott Williams, MPH, CASC, Ad-ministrator for Carnegie Hill Endoscopy and Helen Lowenwirth, MBA, CASC, Administrator for East Side Endoscopy, spoke at the Fall Course of the New York Metropolitan SGNA Region 40 conference in New York City. Scott discussed the topic of bridging the gap in GI endoscopy care for the underserved, while Helen examined in more detail operations in endoscopy and patient satisfaction. The event took place in the Muhlenberg Auditorium at Mount Sinai St. Luke’s Hospital.
East Side Endoscopy has added pain management as a second specialty offered at the center. The center—officially re-named East Side Endoscopy and Pain Management Center—will begin offering pain management solutions in early 2016.
Congratulations to Cindy Durham of Digestive Disease Endoscopy Center! She was recently promoted to Administrator/Director of Nursing for the center. Cindy’s growth over the past three years as Clinical Director, and through added responsibil-ity for oversight of the front office, facility and its operations, has been significant. Cindy always demonstrates her absolute dedication to the success of DDEC through her seemingly tireless commitment to its patients, physicians, and owners.
CenterFront and

FALL 2015 EndoEconomics | 21
Week - October 18th-24th - with a set of cen-ter activities, including educating center staff and visitors on the importance of practicing good hygiene and stressing ways to avoid contamination.
Hudson Valley Center for Digestive Health recently presented at an education booth at the Peekskill Riverfront Green Festival (Hudson Valley Exposition) as well as at the Yorktown Street Fair. Staff members delivered the message on the importance of Colon Screening and distributed physician contact information for their offices—a great opportunity to expand community outreach.
This year, over 900 healthcare facilities were eligible for the award and 104 were selected as winners.
Giving back to the community, Physicians Endoscopy held a suit drive where hun-dreds of pieces of professional clothing were donated by employees to low-income job seekers through Robert Half, Dress for Success and other nonprofit organizations. For more information, visit www.dressforsuccess.org and www.roberthalf.com.
South Broward Endoscopy has been named as one of Modern Healthcare’s Best Places to Work in Healthcare for 2015. This is the third year in a row and the fifth time the cen-ter has been nominated and chosen in six years.
Island Digestive Health Center and its five physicians, along with Physi-cians Endoscopy, held a ribbon cutting ceremony on October 8th to announce the center’s official re-opening now partnered with Good Samaritan Hospital Medical Center as of June 1, 2015.
Long Island Center for Digestive Health has been recognized as a 2014/2015 National APEX Quality Award Winner by SPH Analytics (SPHA). The APEX Quality Award distinguishes them as one of the highest performing healthcare entities in their healthcare peer group. Winners are determined solely on patient feedback.
CenterFront and
At the 5th annual NJAASC meeting held on October 29, 2015, Ambulatory Center for Endoscopy (ACE) won the first ever Quality Improvement Award from the NJAASC Society. The goal of the program was to share best practices and cultivate a community of quality amongst the NJAASC members. At the meeting, ACE was presented with an award and had the opportunity to give a brief presentation about their study to the membership. The QI study submitted was on patient privacy.

22 | EndoEconomics FALL 2015
For more information, contact:Annie Sariego, CASC, VP, Operations(215) 589-9008 • [email protected]
North Bergen, NJAn outstanding opportunity for a gastroenterologist!
For more information, contact:Annie Sariego, CASC, VP, Operations(215) 589-9008 • [email protected]
Cortlandt Manor, NYAn opportunity in Northern Westchester with a two-physician practice.
The physicians of Gastroenterology Consultants of Laredo, a private gastroenterology group, are seeking a gastroenterologist to expand the practice. This candidate will have ownership opportunity in the affiliated endoscopic ambulatory surgery center.
This two-room facility is located in Laredo, Texas in the Northtown Professional Plaza on McPherson Avenue.
• Physician-owned and controlled center• State-of-the-art endoscopic equipment• Medicare licensed and AAAHC accredited• Anesthesia services for patient comfort• Physician efficiency and optimal patient quality of care• Nursing staff has extensive experience in GI endoscopy• An outstanding benefits package is offered• Professionally operated and managed• Group participates in research• High population to GI Doctor ratio 60,000:1• 2 Nurse Practitioners with over 11 years of GI experience
Laredo, TXGastroenterology Consultants of Laredo – Laredo Digestive Health Center
• Full-time or part-time: perfect for young families• State-of-the-art endoscopic equipment• Physician efficiency and optimal patient quality of care• Light call schedule: 1:3• One hour to New York City• Beautiful scenic area
Ambulatory Center for Endoscopy, LLC Advanced Center for Endoscopy (ACE) has an immediate opportunity available for GI physicians looking for an outstanding ASC in which to perform procedures. Our single specialty GI center is the perfect environment for you and your patients.
ASCs provide physicians the predictability and efficiency in scheduling that most hospitals do not. Specialized focus by nurses and other support staff further increases efficiency. Our center can help drive additional patient volume to you through the ASC, allowing you to increase your procedure volume in the environment that is more convenient. Our center can provide your patients a better outcome, and you will have satisfied and loyal patients.
ACE is ideally located in North Bergen along the banks of the Hudson River—the “gold coast” of Northern NJ, with a spectacular view of the NYC skyline.
The nine physicians at Advanced Center for Endoscopy are partnered with Physicians Endoscopy (PE) in their state-of-the art endoscopy center. This is an excellent opportunity for a motivated physician.
For more information, contact:Monte Allen, DO - Medical Director(956) 795-4776 • [email protected]
For more information, contact:Kathy Harren, Office Manager(576) 248-3737 • [email protected]
Garden City, NYGastroenterology Associates – Long Island Center for Digestive Disease
The physicians of Gastroenterology Associates, a large single specialty private gastroenterology group, are seeking a BC/BE physician to start immediately or July 2015.
This candidate will have partnership/ownership opportunity in the affiliated endoscopic ambulatory surgery center. This three-room facility, located in Garden City, NY offers: • Physician-owned and controlled center • State-of-the-art endoscopic equipment • Physician efficiency and optimal patient quality of care • Professionally operated and managed
Gastroenterology Associates, one of the oldest and most respected GI practices on Long Island, has always prided themselves on being leaders in delivering the highest quality of specialized patient care.
GI OpportunitiesCurrent

FALL 2015 EndoEconomics | 23
Williamsville, NYGastroenterology Associates, LLP
A well-established practice with a solid referral base, Gastroenterology Associates, LLP, located in western New York, seeks a board-certified/board-eligible gastroenterologist to join our growing 11 physician practice. ERCP experience is a plus.
With two clinical sites and two physician-owned state-of-the-art endoscopy centers, this opportunity includes: • Partnership track in a premier quality driven group • Competitive compensation and benefits package • Nursing staff in our Centers with extensive GI experience • Fully integrated EMR environment. Meaningful Use attested • Professional management staff • 9 mid-level providers including registered dietician
Western New York offers four beautiful seasons, a wide variety of cultural and recreational opportunities and tremendous housing values. The area has many public and private colleges and universities, museums, galleries and major league professional sports teams. We are located within easy driving distance of The Finger Lakes Region, The Adirondack Mountains, The Great Lakes and Toronto.
For more information, contact:Peg Centola, Human Resources Manager [email protected] • Phone: 716-626-5250 • Fax: 716-565-0665
Seeking a GASTROENTEROLOGIST
The physicians of Gastro-Intestinal Associates, Inc., a dominant GI group serving Lima, Ohio and surrounding counties, is seeking a BE/BC gastroenterologist to join our six physician, four CNP single-specialty practice.
Established in 1977, the practice has an outstanding reputation with the local Lima community. This is an opportunity to join a GI physician-owned 18,000 square foot combined office and three-room endoscopy center. The center, built in 2008, is AAAHC and ASGE certified. In the area are two local hospitals with state-of-the-art facilities.
This opportunity offers:• 1:7 call rotation• First year salary guarantee• Outstanding earning potential• Professionally operated and managed
Lumberton, NJGastroenterology Consultants of South Jersey
Lima, OHGastro-Intestinal Associates, Inc.
Gastroenterology Consultants of South Jersey (GCSJ) is a privately owned, eight physician practice located in Lumberton, NJ. GCSJ is a well-established practice located among several growing communities in southern New Jersey.
• Located within thirty minutes of Philadelphia and within one hour of New York City.• We are affiliated with Burlington County Endoscopy Center, a three room Ambulatory Surgical Center• The ASC is physician owned and operated.• Our practice is seeking to add a full or part time gastroenterologist.• Our large practice offers an attractive call schedule of 1:7 and an opportunity to perform ERCP and EUS (not required).• Partnership will be offered in the practice and endoscopy center.
For more information, contact: Monica Awsare, MD • [email protected]
For more information, contact: Robert Neidich, MDPresident of Gastro-Intestinal AssociatesPhone: (419) 999-1088Fax: (419) 222-6007
GI OpportunitiesCurrent

2500 York Road, Suite 300Jamison, PA 18929
PRSRT STDUS Postage
PAIDMerrill WI
54452Permit No 24