endosopy - validating surveillance patients
TRANSCRIPT
Improving access to endoscopy
services – win – win situation.
Irene Dunkley
Nurse Consultant Gastroenterology
The Team
• Irene Dunkley – Nurse Consultant
• Julie Maddocks – Lead Nurse BCSP.
• Janet Jones – Nurse Practitioner - BCS
• Rose Haggett – Admin support BCSP
• GICU
Problem
• 6 month backlog of validation of referrals for surveillance colonoscopy - colorectal 2011.
• Resulting in Global ratings score for Timeliness fell from A to C in 2011 as surveillance patients waiting >13 weeks in some cases.
• Without A score in timelines risk to continued participation as BCSP site.
• Constant challenges to meet waiting list targets:– cancer pathway seen within 2 week of referral.
– all routine patients seen within 6 weeks or referral
– all surveillance procedure done within 6 weeks of due date.
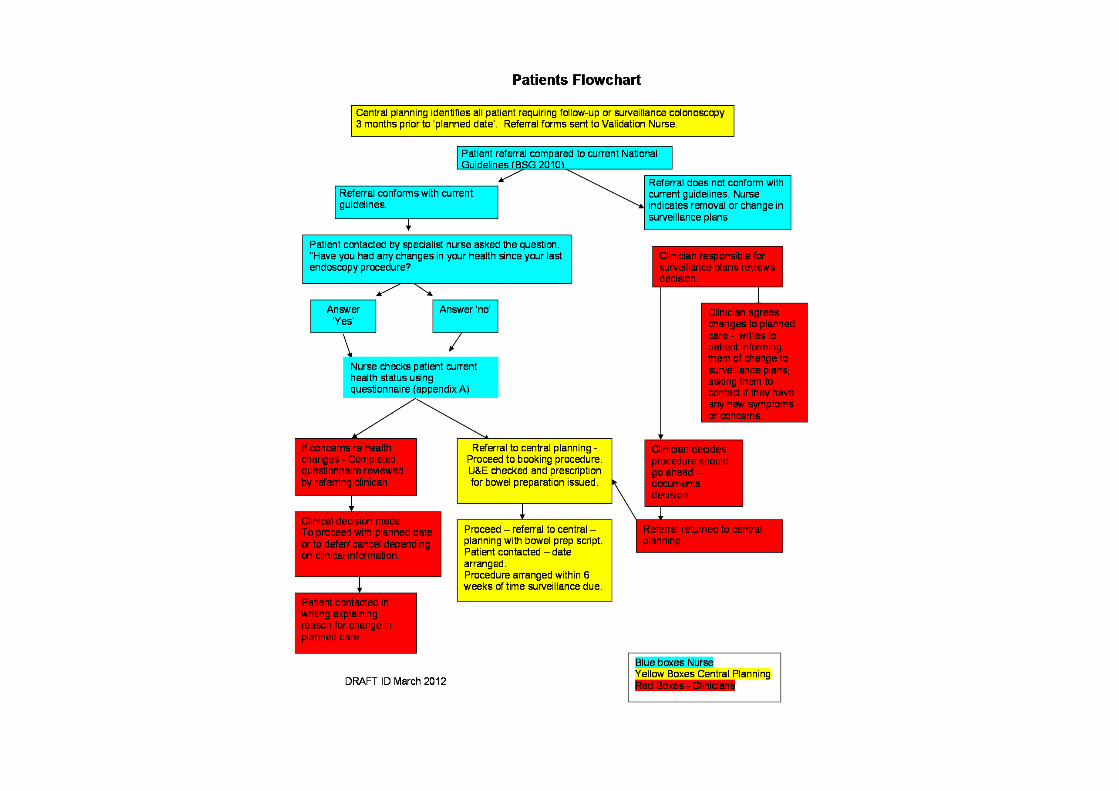
Validation Process
• Three months before surveillance
colonoscopy.
• Referrals sent to consultant to ensure
colonoscopy still needed under current
guidance.
• Problem was this was not being done by
colorectal team – backlog of referrals not
vetted.

What to do?
Idea!
Adapt current practice
• BSCP NP- good knowledge of colorectal cancer and surveillance procedure guidance.
• Lull in their own workload meant they had enough time to take on this task.
• Protocol adapted and approve by GICU. And clinicians.
• Proforma completed by NP with recommendations based on current guidelines.
• ‘Responsible’ clinician to write to patient if any changes in planned care.

Management of Surveillance Patients
• Protocol developed.
• BCSP - CNS’s make recommendations based on current guidelines.
• Recommendation reviewed by responsible clinician – who writes to patient if changes to planned care are made.
• To date 296 sets of notes have been reviewed.
• 18 sets of notes are awaiting consultant validation (not included).

Validation of Surveillance Referrals
March to November 2012: Results
126
43%170
57%
Is the referral appropriate?
Yes - met guidelines
No/unsure open to interpretation
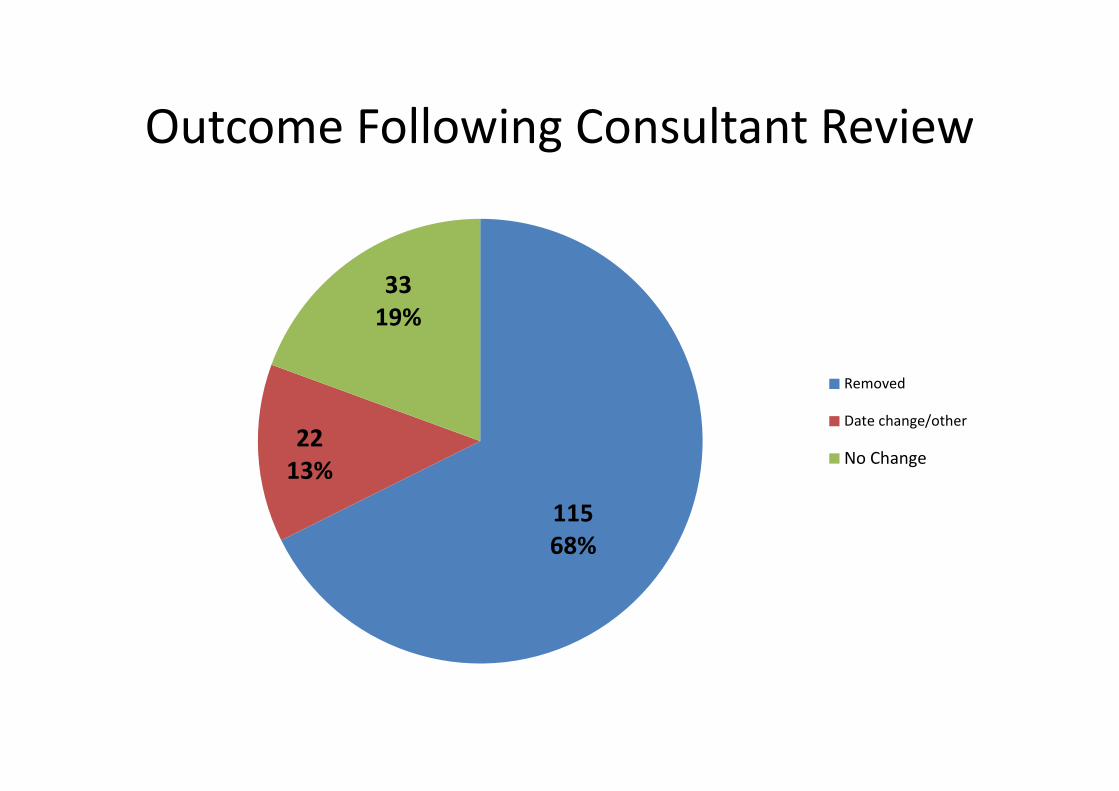
Outcome Following Consultant Review
115
68%
22
13%
33
19%
Removed
Date change/other
No Change

Summary of success To date
• Nurses are able to identify changes to planned surveillance colonoscopy referrals.
• Reducing risk to patients through inappropriate colonoscopy procedures.
• Reducing waiting list and releasing capacity to other patients.
• Cost saving in our case of 115 less colonoscopies equating to 23 lists = weeks work.

Further changes ?
• nurse reviewers contacting patients by
telephone or in appropriate clinics.
• Improvements in documentation.
• Electronic data bases for surveillance patients
which include family history of colorectal
cancer to inform decision making.
• Roll out to Endoscopy staff as part of pre-
assessment process
Need more bright ideas…got any?

Let’s talk….