epidemiology of inflammatory bowel disease in … - fda - pediatric ibd... @cheoibd. eric benchimol,...
TRANSCRIPT

Evidence Guiding Health Carewww.cheo-ibd.ca@CHEOibd
ERIC BENCHIMOL, MD, PhD, FRCPCAssociate Professor of Pediatrics and Epidemiology,
University of Ottawa
Pediatric Gastroenterologist, CHEO IBD Centre,Children’s Hospital of Eastern Ontario
Senior Scientist and Program Director, CHEO Research Institute
Core Scientist, ICES
EPIDEMIOLOGY OFINFLAMMATORY BOWEL DISEASE
IN PEDIATRIC PATIENTS
Evidence Guiding Health Care
DISCLOSURES
• I have no conflicts of interest to disclose.

Evidence Guiding Health Care
WORLDWIDE EPIDEMIOLOGY
Ng et al. Lancet 2017; 390: 3769-78.

Evidence Guiding Health Care
Montreal Classification
Under 17Pediatric Cohort
Slide courtesy of Dr. Aleixo Muise.www.neopics.org
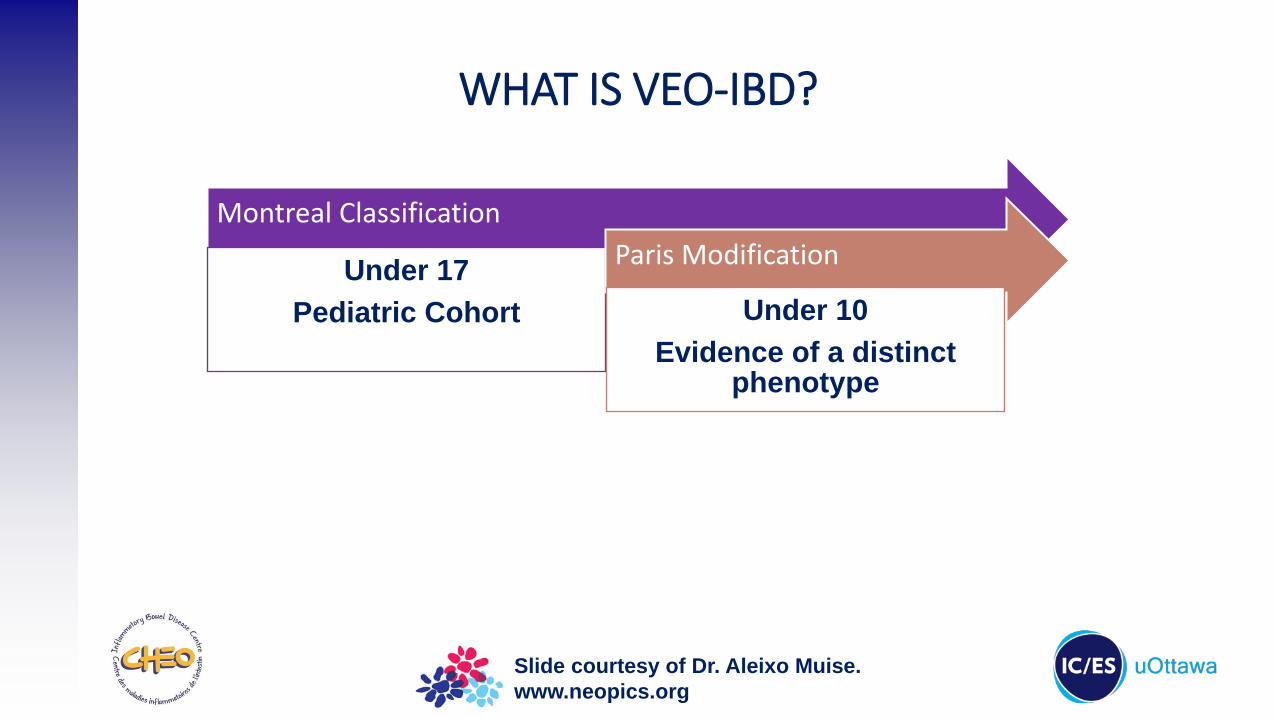
WHAT IS VEO-IBD?
Evidence Guiding Health Care
WHAT IS VEO-IBD?
Montreal Classification
Under 17Pediatric Cohort
Paris Modification
Under 10Evidence of a distinct
phenotype
Slide courtesy of Dr. Aleixo Muise.www.neopics.org

Evidence Guiding Health Care
WHAT IS VEO-IBD?
Montreal Classification
Under 17Pediatric Cohort
Paris Modification
Under 10Evidence of a
distinct phenotype
VEO-IBD
Under 6More colonic involvementLong-term
outcomes???
Slide courtesy of Dr. Aleixo Muise.www.neopics.org

Evidence Guiding Health Care
WHAT IS VEO-IBD?
Montreal Classification
Under 17Pediatric Cohort
Paris Modification
Under 10Evidence of a
distinct phenotype
VEO-IBD
Under 6More colonic involvementLong-term
outcomes???
Slide courtesy of Dr. Aleixo Muise.www.neopics.org
Infants diagnosed under 1 year of age are very unique subset of VEO-IBD –“Infantile IBD”

Evidence Guiding Health Care
0
Stan
dard
ised
inci
denc
e pe
r 100
,000
per
son
year
s
IBD incidenceper 100,000 PYs
CD incidenceper 100,000 PYs
UC incidenceper 100,000 PYs
Percentage changeper year
* p<0.05** p<0.001
*** p<0.0001
5
10
15
20
25
30
35
40
0
12
2
4
6
8
10
Percentage change in IBD
incidence per year0–9 10–19 20–29 30–39 40–49 50–59 60–69 70–79 80–89
Age (years)
***
***
**
** ***
ONTARIO, CANADAONTARIO CROHN’S AND COLITIS COHORT (1999-2008)
Benchimol et al., Inflamm Bowel Dis 2014; 20(10): 1761-9.
Evidence Guiding Health Care
0
Stan
dard
ised
inci
denc
e(p
er 1
00,0
00 p
opul
atio
n)
4
8
16
1999 2010
20
18
2
6
10
14
12
2009200820072006200520042003200220012000
Alberta
Manitoba
Nova Scotia
Ontario
Quebec
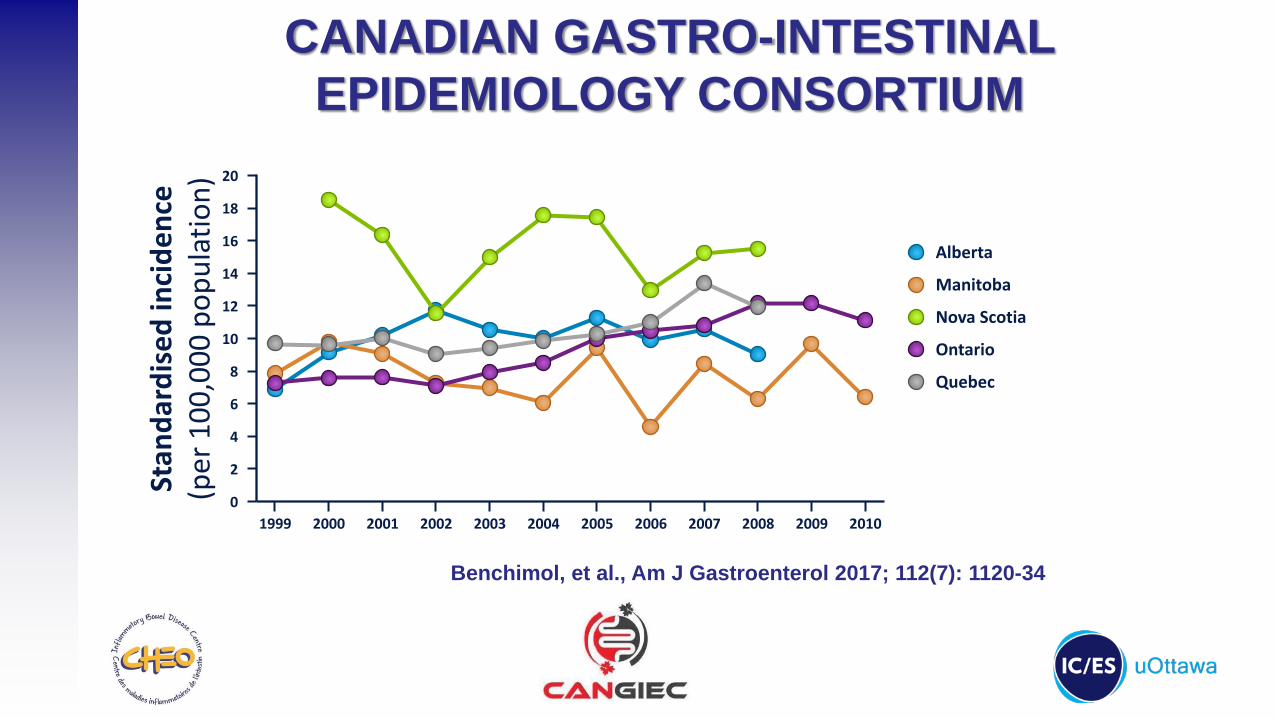
Benchimol, et al., Am J Gastroenterol 2017; 112(7): 1120-34
CANADIAN GASTRO-INTESTINAL EPIDEMIOLOGY CONSORTIUM
Evidence Guiding Health Care
0
Stan
dard
ised
inci
denc
e(p
er 1
00,0
00 p
opul
atio
n)
4
8
16
1999 2010
20
18
2
6
10
14
12
2009200820072006200520042003200220012000
Alberta
Manitoba
Nova Scotia
Ontario
Quebec
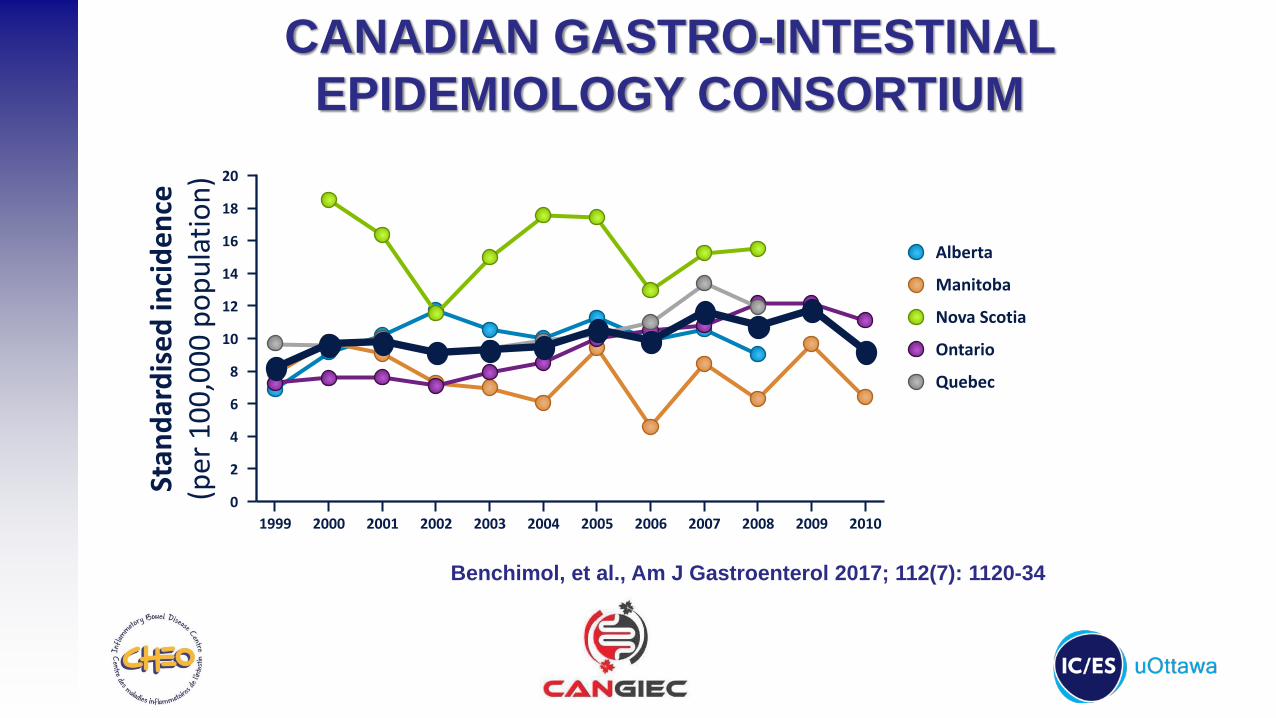
Benchimol, et al., Am J Gastroenterol 2017; 112(7): 1120-34
CANADIAN GASTRO-INTESTINAL EPIDEMIOLOGY CONSORTIUM
Evidence Guiding Health Care
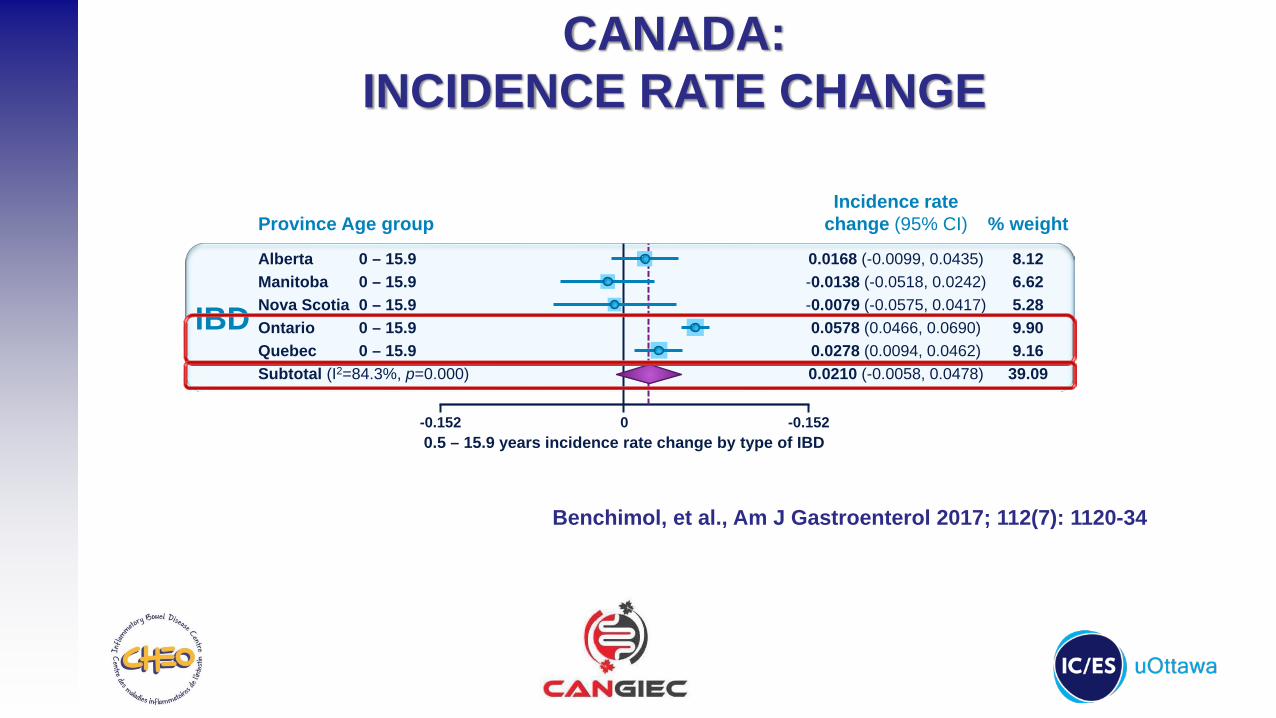
CANADA:INCIDENCE RATE CHANGE
0.5 – 15.9 years incidence rate change by type of IBD0
AlbertaManitobaNova ScotiaOntarioQuebecSubtotal (I2=84.3%, p=0.000)
IBD
Province
0 – 15.90 – 15.90 – 15.90 – 15.90 – 15.9
Age group
8.126.625.289.909.1639.09
% weight
0.0168 (-0.0099, 0.0435)-0.0138 (-0.0518, 0.0242)-0.0079 (-0.0575, 0.0417)0.0578 (0.0466, 0.0690)0.0278 (0.0094, 0.0462)0.0210 (-0.0058, 0.0478)
Incidence ratechange (95% CI)
-0.152 -0.152
Benchimol, et al., Am J Gastroenterol 2017; 112(7): 1120-34

Evidence Guiding Health Care
CANADA:INCIDENCE RATE CHANGE (0-5y)
0.5 – 4.9 years incidence rate change by type of IBD0
AlbertaNova ScotiaOntarioQuebecSubtotal (I2=9.5%, p=0.346)
AlbertaOntarioQuebecSubtotal (I2=0.0%, p=0.838)
AlbertaOntarioQuebecSubtotal (I2=0.0%, p=0.501)
IBD
CD
UC
Province0.5 – 4.90.5 – 4.90.5 – 4.90.5 – 4.9
0.5 – 4.90.5 – 4.90.5 – 4.9
0.5 – 4.90.5 – 4.90.5 – 4.9
Age group14.251.5033.325.9655.03
6.159.364.8520.37
3.4720.091.0424.60
% weight0.0596 (-0.0174, 0.1366)0.1166 (-0.1207, 0.3540)0.0959 (0.0455, 0.1463)
-0.0188 (-0.1379, 0.1003)0.0719 (0.0282, 0.1156)
0.0566 (-0.0606, 0.1738)0.0314 (-0.0637, 0.1265)0.0031 (-0.1289, 0.1351)0.0323 (-0.0322, 0.0967)
0.0732 (-0.0828, 0.2292)0.0606 (-0.0043, 0.1255)-0.1111 (-0.3964, 0.1742)0.0551 (-0.0035, 0.1138)
Incidence ratechange (95% CI)
-0.396 0.396
Benchimol, et al., Am J Gastroenterol 2017; 112(7): 1120-34

Evidence Guiding Health Care
EPIMAD:CROHN’S DISEASE TRENDS
0
Stan
dard
ised
inci
denc
e ra
tes
(eve
nts/
100,
000)
5
10
15
1988–1990
0 – 910 – 19
20 – 2930 – 39≥40
1991–1993 1994–1996 1997–1999 2000–2002 2003–2005 2006–2007
p<0.0001
p=0.02
Age category (years)
Chouraki V et al. Aliment Pharm Ther 2011;33:1133-42.

Evidence Guiding Health Care
SCOTLAND:VEO-IBD TRENDS
1981
-1985
1986
-1990
1991
-1995
2003
-2007
2008
-2013
0
1
2
3Crohn's disease
Non-Crohn's colitis
p<0.0001 NS
p=0.002 NS
Epoch
Adj
uste
d in
cide
nce
of A
1a C
D a
nd N
CC
per 1
00,0
00 p
opul
atio
n at
risk
Henderson P et al. ECCO 2015 oral abstract OP027.Slide courtesy of David Wilson

Evidence Guiding Health Care
VEO-IBD: PROGRESSION
Baumgart and Sandborn, Lancet 2012; 380:1590-1605.
Evidence Guiding Health Care
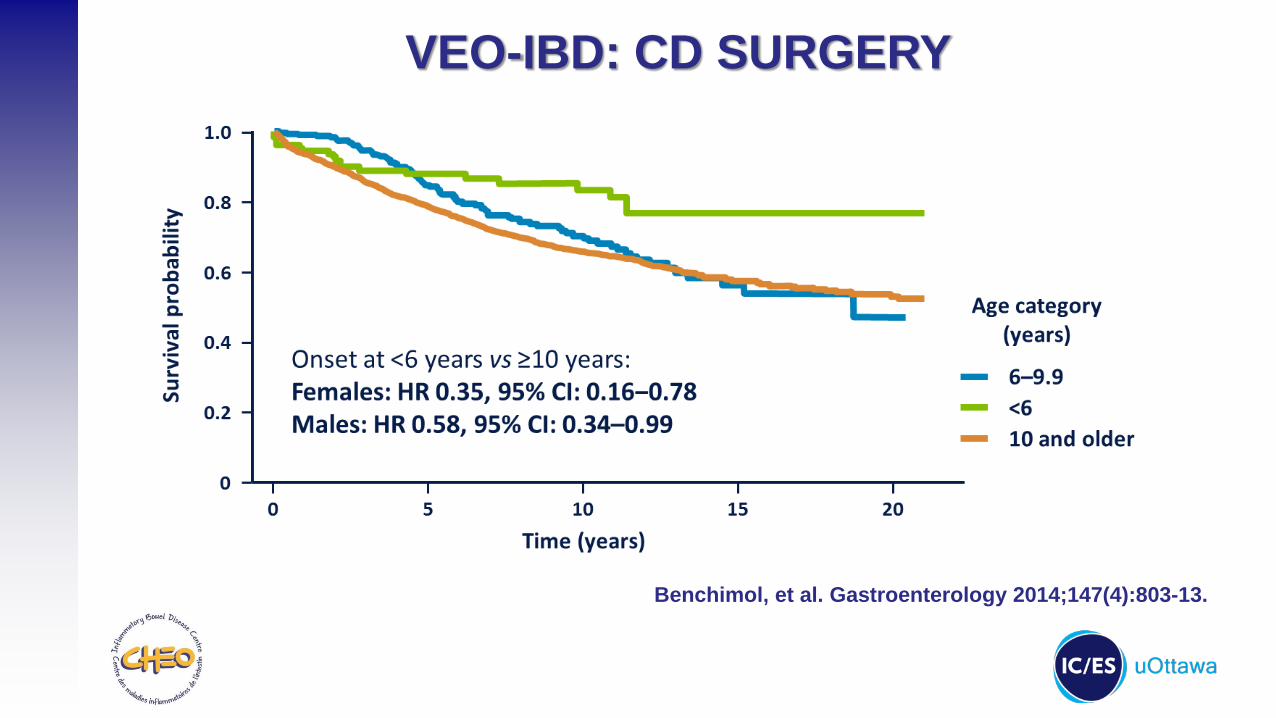
VEO-IBD: CD SURGERY
Benchimol, et al. Gastroenterology 2014;147(4):803-13.
Evidence Guiding Health Care
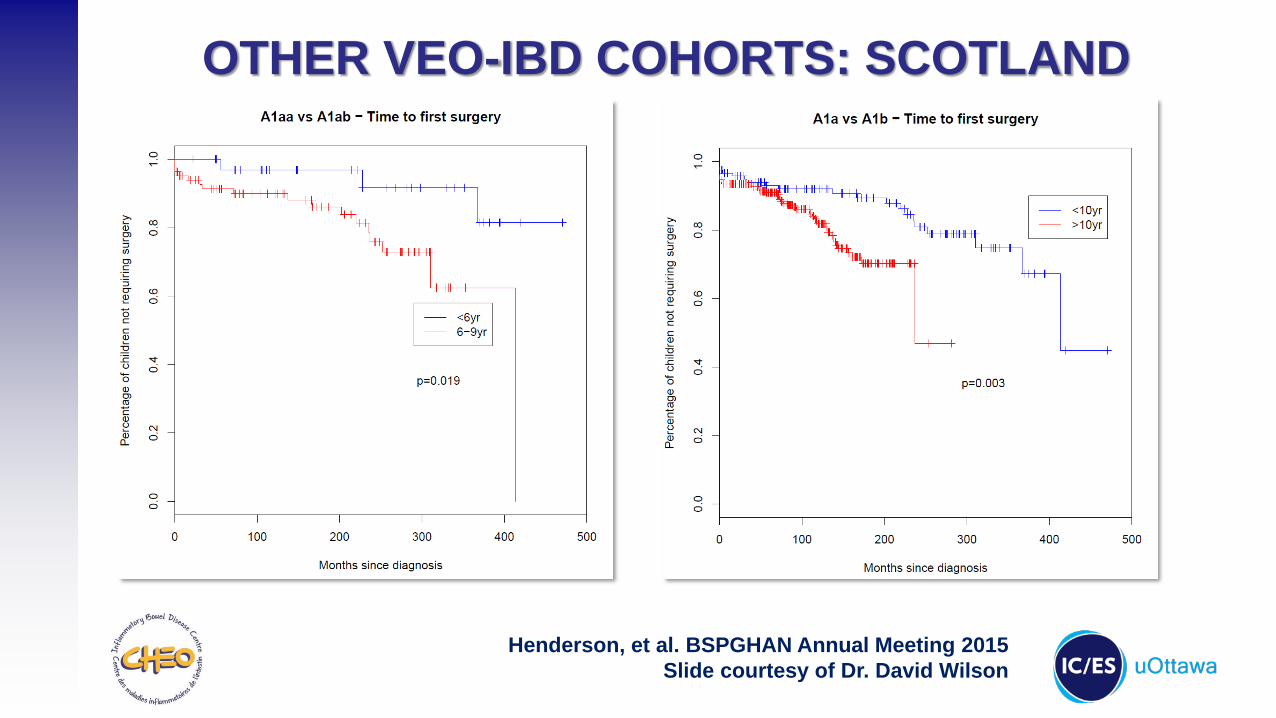
OTHER VEO-IBD COHORTS: SCOTLAND
Henderson, et al. BSPGHAN Annual Meeting 2015Slide courtesy of Dr. David Wilson

Evidence Guiding Health Care
Henderson, et al. BSPGHAN Annual Meeting 2015Slide courtesy of Dr. David Wilson
OTHER VEO-IBD COHORTS: SCOTLAND
Evidence Guiding Health Care
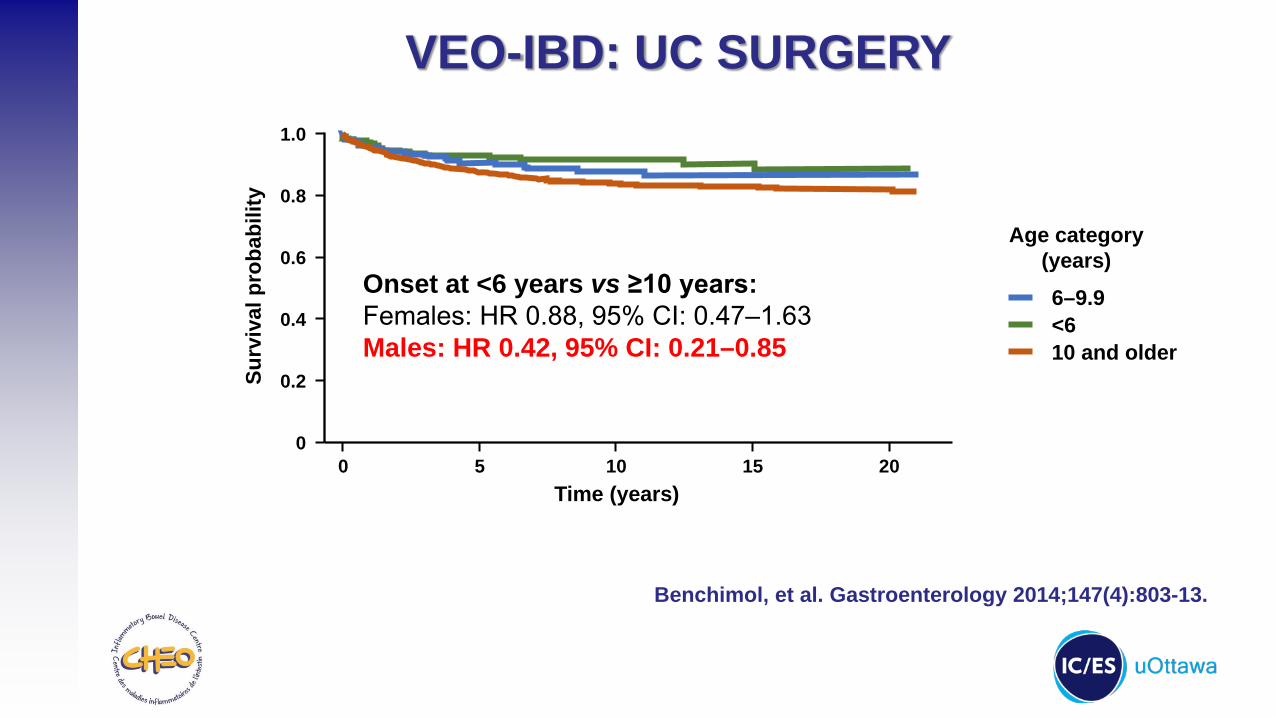
VEO-IBD: UC SURGERY
Benchimol, et al. Gastroenterology 2014;147(4):803-13.
Onset at <6 years vs ≥10 years:Females: HR 0.88, 95% CI: 0.47‒1.63Males: HR 0.42, 95% CI: 0.21–0.85
0
Surv
ival
pro
babi
lity
0.4
0.8
0
1.0
0.2
0.6
2015105
6–9.9<610 and older
Time (years)
Age category (years)
Evidence Guiding Health Care
WHAT DOES THE FUTURE HOLD?
Evidence Guiding Health Care
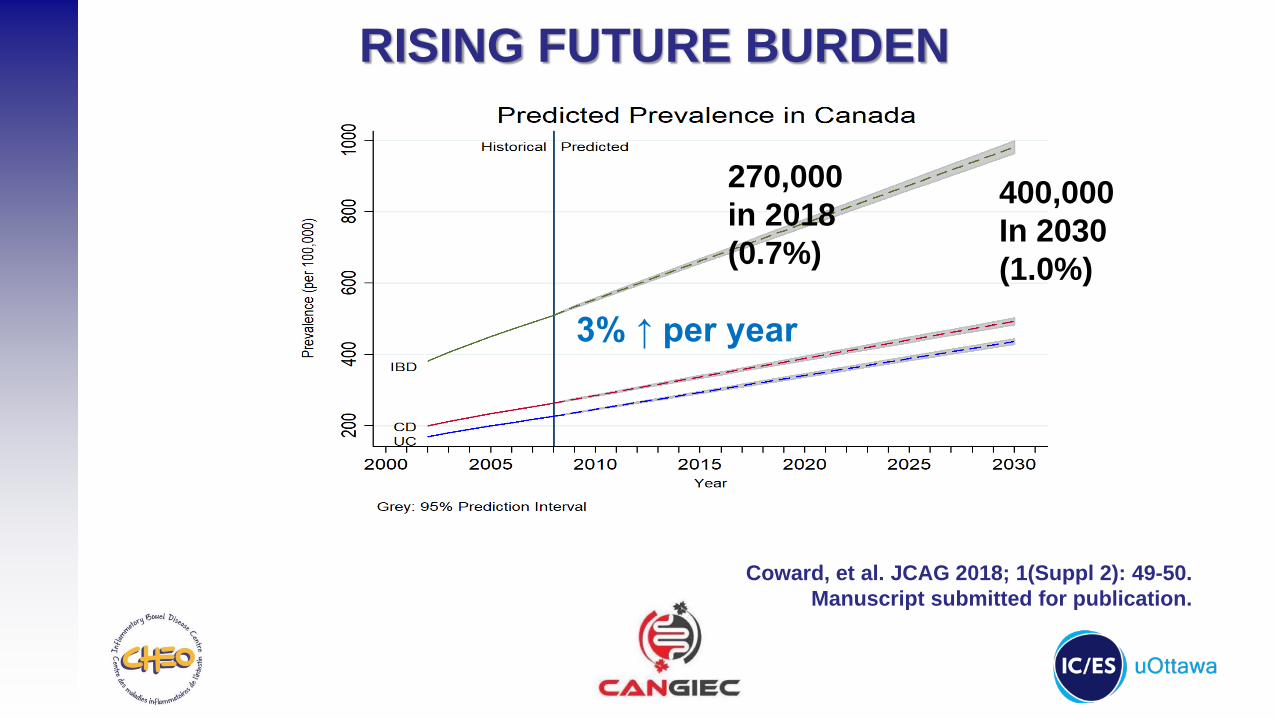
RISING FUTURE BURDEN
Coward, et al. JCAG 2018; 1(Suppl 2): 49-50.Manuscript submitted for publication.
3% ↑ per year
270,000in 2018(0.7%)
400,000In 2030(1.0%)

Evidence Guiding Health Care
RISING FUTURE BURDEN
Coward, et al. JCAG 2018; 1(Suppl 2): 49-50.Manuscript submitted for publication.

Evidence Guiding Health Care
PEDIATRIC IBD EPIDEMIOLOGY2003-2004 2008 2018 2030
Canada(per 100,000)
62 101 159
USA(per 100,000)
Canada(raw number)
4,730 7,254 12,647
USA**(raw number)

Evidence Guiding Health Care
PEDIATRIC IBD EPIDEMIOLOGY2003-2004 2008 2018 2030
Canada(per 100,000)
62 101 159
USA(per 100,000)
71* 71 115 181
Canada(raw number)
4,730 7,254 12,647
USA**(raw number)
*In people <20 years, from: Kappelman et al., Clin Gastroenterol Hepatol 2008;135:1907-13

Evidence Guiding Health Care
PEDIATRIC IBD EPIDEMIOLOGY2003-2004 2008 2018 2030
Canada(per 100,000)
62 101 159
USA(per 100,000)
71* 71 115 181
Canada(raw number)
4,730 7,254 12,647
USA**(raw number)
52,043 52,611 84,870 138,103
*In people <20 years, from: Kappelman et al., Clin Gastroenterol Hepatol 2008;135:1907-13**Based on estimated population of children <18 years according to childstats.gov

Evidence Guiding Health Care
CONCLUSIONS• Pediatric IBD is increasing internationally
Rates are rising most rapidly in young children
• Children with disease onset <10y: More often have colonic involvement More inflammatory, less stricturing UC: More mild endoscopic findings
• Rising prevalence may result in strain on the health system

Evidence Guiding Health Care
QUESTIONS?
ACKNOWLEDGEMENTS:
IBD Impact Reporthttp://crohnsandcolitis.ca/impactreport