epidemiology of poliomyelitis
TRANSCRIPT
Epidemiology of Poliomyelitis
Joint Program for Family and Community MedicineOct. 17, 09
Ghaiath M. A. HusseinMBBS, MHSc. (Bioethics)


Overview
• Global situation• Definition of Poliomyelitis • Epidemiology of Polio• The Global Polio Eradication Initiative• Challenges to stay ‘Polio-Free’ country

Worldwide situation
• The Americas were certified polio-free in 1994. (36 countries)
• the western pacific was certified polio-free in 2000. (37 countries and areas including china)
• Europe, composed of 51 countries, was certified polio-free in June 2002. (51 countries)
• with only six polio endemic countries left in the world, polio transmission could be stopped by end 2005. The world could then be certified polio-free by end-2008.

Key facts
• Polio (poliomyelitis) mainly affects children under five years of age.
• One in 200 infections leads to irreversible paralysis (usually in the legs). Among those paralysed, 5% to 10% die when their breathing muscles become immobilized.
• Polio cases have decreased by over 99% since 1988, from an estimated 350 000 cases then, to 1997 reported cases in 2006.
• In 2008, only four countries in the world remain polio-endemic, down from more than 125 in 1988.

• Endemic countries• Afghanistan• India• Nigeria• Pakistan
• Importation countries• Angola• Burundi• Cameroon• Central African Republic
(CAR)• Chad• Democratic Republic of the
Congo (DRC)• Horn of Africa• West Africa

Global Status 1988

GLOBAL STATUS 2004


"Poliomyelitis" comes from the Greek word for gray, polio, and myelo, meaning spinal cord. The Latin suffix itis refers to inflammatory diseases.
Among children who are paralyzed by polio:30% make a full recovery • 30% are left with mild paralysis • 30% have medium to severe paralysis • 10% die
What is Polio?


EPIDEMIOLOGY
• Agent: poliovirus• Type : three sero types(type-1,type-2,type-3)• Reservoir: man• Infectious material: faeces, oro-pharyngeal
secretions• Incubation period: 7 to 14 days( 3- 35 days)• Period of communicability: 7 to 10 days• Host age : 6 months to 3 years• Environment : rainy season (June to
September)• Mode of transmission: faeco – oral route,
droplet infection

The virion consists of a single strand of RNA containing genetic information and a protein coat. Humans are its only natural host. - The poliovirus is a member of a larger family known as Picornaviruses, which also includes rhinoviruses (such as influenza) and the hepatitis A virus. - Polio belongs to the enterovirus subgroup, made up of over 70 viruses that infect the intestines. - It is one of the smallest RNA viruses, measuring around 25 nm in diameter.
AGENT: POLIO VIRUS

Group: Group IV ((+)ssRNA)
Family: Picornaviridae
Genus: Enterovirus
Species: Poliovirus
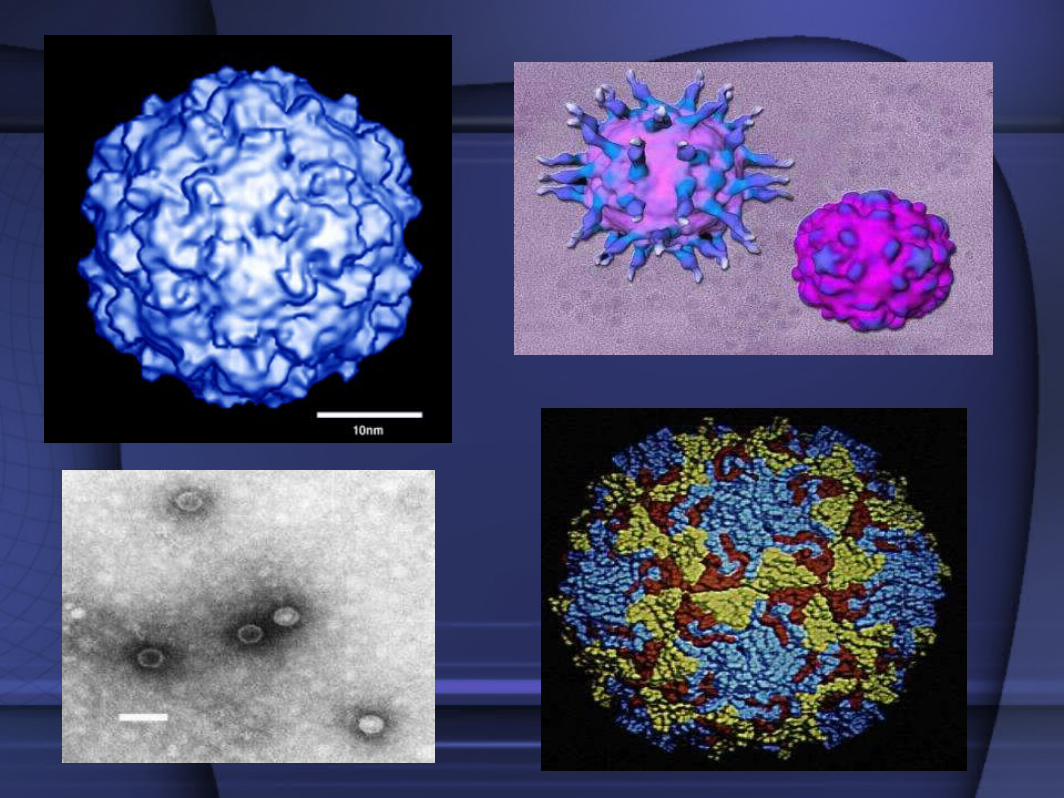

Left: Picture of poliovirus. The poliovirus is
extremely small, about 50 nm (nanometer = one-
billionth of a meter) Courtesy of David Belnap
and James Hogle
Right: Cross-section of the poliovirus showing the RNA, capsid, and nerve cell
receptors Illustration courtesy of Link Studio

• Inapperent(sub-clinical) Infection: this occurs approximately in 95 per cent of poliovirus infection. There are no presenting symptoms. Recognition only by isolation.
• Abortive Polio Or Minor Illness: occurs approximately in 4-8 per cent of the infection. It causes only a mild or self limiting illness due to viraemia. The patient recovers quickly.
• Non paralytic polio: occurs approximately in one per cent of all infections. The presenting features are stiffness and pain in neck and back. The disease lasts for two to ten days. Recovery is rapid.
• Paralytic polio: occurs in less then one per cent of infections. The virus enters the brain and causes varying degree of disability.

TREATMENT
• No specific antiviral agent is available • Treatment focuses on management of
complications (e.g., meningitis, abnormal cardiac rhythms, and heart failure).
• Intravenous administration of immune globulin may have a use in preventing severe disease in immunocompromised individuals or those with life-threatening disease.

The Global Polio Eradication Initiative

OBJECTIVES: • To interrupt transmission of the wild poliovirus as
soon as possible and certify all who regions polio-free by the end of 2005;
• To implement the polio endgame programme of work, including containment of wild poliovirus, global polio-free certification, and the development of a post-eradication immunization policy;
• To contribute to health systems development by strengthening routine immunization and surveillance for communicable diseases.

Strategies: • High infant immunization coverage with four doses
of oral polio vaccine in the first year of life; • Supplementary doses of oral polio vaccine to all
children under five years of age during national immunization days (NIDs);
• Surveillance for wild poliovirus through reporting and laboratory testing of all cases of acute flaccid paralysis (AFP) among children under fifteen years of age;
• Targeted “mop-up” campaigns once wild poliovirus transmission is limited to a specific focal area.

Before a WHO region can be certified polio-free, three conditions must be satisfied:( A) at least three years of zero polio cases due to wild poliovirus( B) excellent certification standard surveillance ( c) each country must illustrate the capacity to detect, report and respond to “imported” polio cases. Laboratory stocks must be contained and safe management of the wild virus in inactivated polio vaccine (IPV) manufacturing sites must be assured before the world can be certified polio-free.

• 1. Substantial external financial resources are required to support the efforts of developing countries to eradicate polio.
• 2. India is the highest priority country, because it has the highest number of cases in the world (83%), and for the first time in the Initiative’s history, previously polio-free areas were reinfected.
• 3. As the world is nearing polio-free status, effective surveillance becomes even more important
• 4. To rapidly mount massive immunization response campaigns to manage any wild poliovirus importations quickly and efficiently in polio-free areas
GLOBAL PRIORITIES TO STOP TRANSMISSION OF THE WILD POLIOVIRUS:

Case Definition:In the Global Polio Eradication Initiative (PEI), acute flaccid paralysis is defined as:Any case of AFP in a child aged <15 years, or any case of paralytic illness in a person of any age when polio is suspected.Acute: rapid progression of paralysis from onset to maximum paralysisFlaccid: loss of muscle tone, “floppy” – as opposed to spastic or rigidParalysis: weakness, loss of voluntary movementAny case meeting this definition undergoes a thorough investigation to determine if the paralysis is caused by polio.

Components of AFP Surveillance • detect the exact geographic locations where wild
polioviruses are circulating in the human population.
• All cases of acute flaccid paralysis in children aged <15 years are rigorously investigated by a trained personeel, with
• collection of stool specimens to determine if poliovirus is the cause of the paralysis.
• Analysis of the location of polioviruses isolated from AFP cases allows programme managers to plan immunization campaigns (Pulse Polio Immunization) to prevent continuing circulation of virus in these areas.

Components of AFP surveillance
1.The AFP surveillance network and case notification2.Case and laboratory investigation3.Outbreak response and active case search in the community4.60-day follow-up, cross-notification and tracking of cases 5.Data management and case classification6.Virologic case classification scheme7. Surveillance performance indicators

Samples are considered adequate if both the specimens are :• collected within 14 days of paralysis onset
and at least 24 hours apart; • of adequate volume (8-10g) and • arrives at a WHO-accredited laboratory in
good condition (ie, no desiccation, no leakage), with adequate documentation and evidence of cold-chain maintenance.


Current challenges in KSA
• Surveillance of AFP cases (zero reporting)• Access to immunization and health facilities
(illegal residents)• Location and function Sentinel Sites • Trained personel on AFP case definition• Imported cases• Polio-Free is not a granted ‘blanket cheque’.
We can be re-infected!

resources
• www.who.int • www.polioeradication.org • www.unicef.org/immunization• Super course/ Pittsburgh
university(www.pitt.edu/~super1)• http://www.polionet.org/vaccine.htm
