epigenetic alteration of dna in mucosal wash fluid...
TRANSCRIPT

Research Article
Epigenetic Alteration of DNA in Mucosal Wash Fluid PredictsInvasiveness of Colorectal Tumors
Seiko Kamimae1, Eiichiro Yamamoto1,2, Hiro-o Yamano5, Masanori Nojima3, Hiromu Suzuki1,2,Masami Ashida1, Tomo Hatahira1, Akiko Sato1, Tomoaki Kimura5, Kenjiro Yoshikawa5, Taku Harada5,Seiko Hayashi5, Hiroyuki Takamaru2, Reo Maruyama1,2, Masahiro Kai1, Morie Nishiwaki6, Tamotsu Sugai7,Yasushi Sasaki4, Takashi Tokino4, Yasuhisa Shinomura2, Kohzoh Imai8, and Minoru Toyota1
AbstractAlthough conventional colonoscopy is considered the gold standard for detecting colorectal tumors,
accurate staging is often difficult because advanced histology may be present in small colorectal lesions.
We collected DNA present in mucosal wash fluid from patients undergoing colonoscopy and then assessed
the methylation levels of four genes frequently methylated in colorectal cancers to detect invasive tumors.
We found thatmethylation levels inwash fluidwere significantly higher in patients with invasive than those
with noninvasive tumors. Cytologic and K-ras mutation analyses suggested that mucosal wash fluid from
invasive tumors contained greater numbers of tumor cells thanwash fluid fromnoninvasive tumors. Among
the four genes, levels ofmir-34b/cmethylation had the greatest correlationwith the invasion and showed the
largest area under the receiver operating characteristic curve (AUC¼ 0.796).Using cutoff points ofmir-34b/c
methylation determined by efficiency considerations, the sensitivity/specificity were 0.861/0.657 for the
13.0%(high sensitivity) and0.765/0.833 for the 17.8%(well-balanced) cutoffs. In the validation test set, the
AUCwas also very high (0.915), the sensitivity/specificity were 0.870/0.875 for 13.0% and 0.565/0.958 for
17.8%. Using the diagnostic tree constructed by an objective algorithm, the diagnostic accuracy of the
invasiveness of colorectal cancer was 91.3% for the training set and 85.1% for the test set. Our results suggest
that analysis of the methylation of DNA in mucosal wash fluid may be a good molecular marker for
predicting the invasiveness of colorectal tumors. Cancer Prev Res; 4(5); 674–83. �2011 AACR.
Introduction
Colorectal cancer is one of the most common neoplasiasworldwide (1), and its early detection and accurate pre-operative staging are essential for reducing the incidencesof invasion and metastasis. The fecal occult blood test iswidely used to screen for colorectal tumors, though itssensitivity and specificity are not high (2, 3). Conventionalcolonoscopy is considered the gold standard for detectingcolorectal cancers and adenomas, whereas several other
methods, including computed tomography, ultrasonogra-phy, and 3D magnetic resonance, have been used forstaging (4, 5). Generally, tumor size is used as the markerfor invasion and lymph node metastasis; however, accuratestaging is often difficult because advanced histologymay bepresent in as much as 10% of small (5–10 mm) colorectaladenomas (6–8).
Magnified endoscopy is a highly useful method fordiagnosing invasive colorectal cancer (9, 10). Althoughconventional endoscopic examination with indigo carminedye is not sufficient to determine whether or not a color-ectal cancer is invasive, pit pattern analysis, using high-magnification observation with crystal violet, reportedlyenables the diagnosis of invasive colorectal cancers.Recently, narrow-band imaging magnification endoscopyhas also been used to predict the invasiveness of colorectaltumors (11). However, it has been suggested that the skillsrequired for pit pattern analysis will limit the number ofendoscopists who use the technique.
DNA methylation plays a critical role in the tumorigen-esis of colorectal cancer (12, 13). For example, promoterhypermethylation is associated with the silencing of var-ious cancer-related genes (14, 15), and aberrant methyla-tion of the CpG islands of genes in stool and serum/plasmacan be used as a molecular marker for detection of color-ectal tumors (16–20). On the contrary, because DNA
Authors' Affiliations: 1Department of Biochemistry, 2First Department ofInternal Medicine, 3Department of Public Health, and 4Department ofMolecular Biology, Cancer Research Institute, Sapporo Medical Univer-sity; 5Akita Red Cross Hospital, Akita; 6GeneticLab Co. Ltd., Sapporo;7Department of Pathology, Iwate Medical University, Morioka; and 8TheInstitute of Medical Science, The University of Tokyo, Tokyo, Japan
Note: Supplementary data for this article are available at Cancer Preven-tion Research Online (http://cancerprevres.aacrjournals.org/).
S. Kamimae, E. Yamamoto, and H. Yamano contributed equally to thiswork.
Corresponding Author: Minoru Toyota, Department of Biochemistry,Sapporo Medical University, South-1, West-17, Chuo-ku, Sapporo 060-8556, Japan. Phone: 81-11-611-2111 (Ext. 2680); Fax: 81-11-622-1918.E-mail: [email protected]
doi: 10.1158/1940-6207.CAPR-10-0214
�2011 American Association for Cancer Research.
CancerPreventionResearch
Cancer Prev Res; 4(5) May 2011674
Association for Cancer Research. on November 7, 2018. © 2011 Americancancerpreventionresearch.aacrjournals.org Downloaded from

methylation is an early event (21–23), it does not enableone to distinguish between premalignant lesions and inva-sive tumors. As yet, there is no study describing a moleculartest for predicting the invasiveness of colorectal tumors.In this study, we examined the methylation levels of 4
genes frequently methylated in colorectal cancers by usingDNA obtained frommucosal wash fluid. We found that themethylation level of DNA in the wash fluid was signifi-cantly higher in patients with invasive than those withnoninvasive tumors. Our results suggest that methylationof DNA in mucosal wash fluid could be a good molecularmarker for predicting the invasiveness of colorectal tumors.
Materials and Methods
Specimens and sample preparationColorectal tumor tissues and washing fluid were col-
lected from Japanese patients who underwent endoscopicmucosal resection (EMR) or surgical resection of colorectaltumors at Akita Red Cross Hospital. Informed consent wasobtained from all patients before collection of the speci-mens. Approval for this study was obtained from theInstitutional Review Board of Akita Red Cross Hospitaland Sapporo Medical University.We used 2 methods to obtain DNA from mucosal
washing fluid. When a colorectal tumor was detected dur-ing colonoscopy, the tumor’s surface mucus was eitherwashed away by using 20 mL of water, which was aspiratedthrough the suction channel of the endoscope, and sus-pended in ThinPrep PreservCyt solution (Hologic, Inc.;method 1) or washed away with 20 mL of normal salineby using anNT tube and collected (method 2). Each sampleof collected washing fluid was placed in a Non-GYN Pre-servCyt vial (Hologic, Inc.) for a minimum of 15 minutes,after which the solution was transferred to a disposablecentrifuge tube and centrifuged at 500 � g for 20 minutes.The resultant supernatant was discarded, and the cell pelletwas suspended in ThinPrep solution until DNA extraction.After collection of the washing fluid and endoscopic obser-vation, biopsies of the colorectal tumor and correspondingnormal colonic mucosa were carried out by using biopsyforceps under endoscopic guidance. For cytology analysis, aThinPrep slide was prepared by a T2000 ThinPrep proces-sor (Hologic, Inc.) and a nongynecologic ThinPrep Filterwith 5-mm pores. The slide was then Papanicolaou stainedand examined by GLab cytotechnologists and a pathologist(GeneticLab Co. Ltd.), and atypical cells were identified.Nuclei were stained by 40,6-diamidino-2-phenylindole(DAPI) and visualized under a fluorescence microscope(Olympus) as described previously (24).A total of 337 biopsy specimens including 150 colorectal
tumors and 187 normal colonic mucosa specimens wereexamined. We also examined 88 samples of washing fluidfrom 70 colorectal tumor patients and 18 healthy patients.For testing the clinical usefulness of the study, we examinedan additional 47 colorectal tumor biopsy samples as thetest set, which were independently obtained severalmonths after the collection of prior samples. On the basis
of histologic examination after any type of resection,biopsy specimens and wash fluid samples from a colorectaltumor were divided into 2 groups: invasive tumors andnoninvasive tumors. Invasive tumors were defined as sub-mucosal invasive tumors.
Bisulfite pyrosequencingDNA was extracted from biopsy specimens and washing
fluid by using the standard phenol-chloroform procedure,after which 1-mg samples of genomic DNA were modifiedwith sodium bisulfite by an EpiTect Bisulfite Kit (Qiagen).Bisulfite pyrosequencing was then carried out as describedpreviously (25). Primers for pyrosequencing were designedby PSQ Assay Design software (Qiagen). Following PCR,the biotinylated PCR product was purified, made single-stranded, and then used as a template in a pyrosequencingreaction run according to the manufacturer’s instructions.The PCR products were bound to streptavidin Sepharosebeads HP (Amersham Biosciences), after which beads withthe immobilized PCR product were purified, washed, anddenatured by using a 0.2 mol/L NaOH solution. Afteraddition of 0.3 mmol/L sequencing primer to the purifiedPCR product, pyrosequencing was carried out by aPSQ96MA system (Qiagen) and Pyro Q-CpG software(Qiagen). The primer sequences are listed in Supplemen-tary Table S1.
K-ras mutation analysisMutation of codons 12 and 13 of K-ras was examined by
using direct sequencing and pyrosequencing, as describedpreviously (26). Pyrosequencing was done by a K-rasmuta-tion detection kit (Qiagen) as suggested by the supplier.
Statistical analysisAll statistical analyses were carried out by SPSSJ 15.0
(SPSS Japan Inc.). To compare differences in methylationlevels or other continuous values between groups, t tests orANOVAwith a post hoc Tukey test were carried out. Fisher’sexact test was used for analysis of categorical data. Toevaluate correlations between continuous values, Pearson’scorrelation coefficients were calculated. Receiver operatingcharacteristic (ROC) curves for the diagnosis of invasivetumors were constructed on the basis of methylation levels,followed by area under the curve (AUC) calculation. Adiagnostic tree to discriminate invasive tumors was con-structed by using the training set based on the followingobjective algorithm. Step 1: classify the samples based onthe most efficient cutoff of tumor size. Step 2: classify thesamples based on the most efficient cutoffs of methylationlevels in 4 sequences under the classification of the pre-vious step. Step 3: repeat step 2 until no additional efficacyis observed. P < 0.05 (2-sided) were considered significant.
Results
Preparation of specimensWe first compared the 2 methods used to obtain tumor
cells from colonoscopy wash fluid. When tumors were
Epigenetic Alterations in Mucosal Washing Fluid
www.aacrjournals.org Cancer Prev Res; 4(5) May 2011 675
Association for Cancer Research. on November 7, 2018. © 2011 Americancancerpreventionresearch.aacrjournals.org Downloaded from
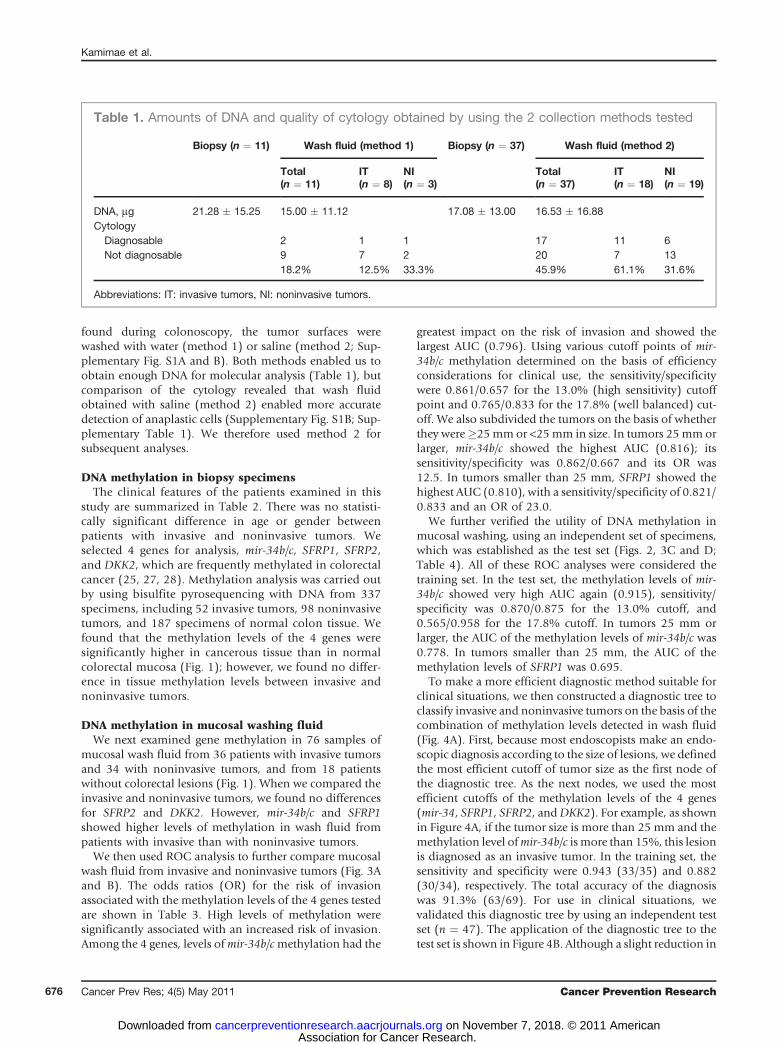
found during colonoscopy, the tumor surfaces werewashed with water (method 1) or saline (method 2; Sup-plementary Fig. S1A and B). Both methods enabled us toobtain enough DNA for molecular analysis (Table 1), butcomparison of the cytology revealed that wash fluidobtained with saline (method 2) enabled more accuratedetection of anaplastic cells (Supplementary Fig. S1B; Sup-plementary Table 1). We therefore used method 2 forsubsequent analyses.
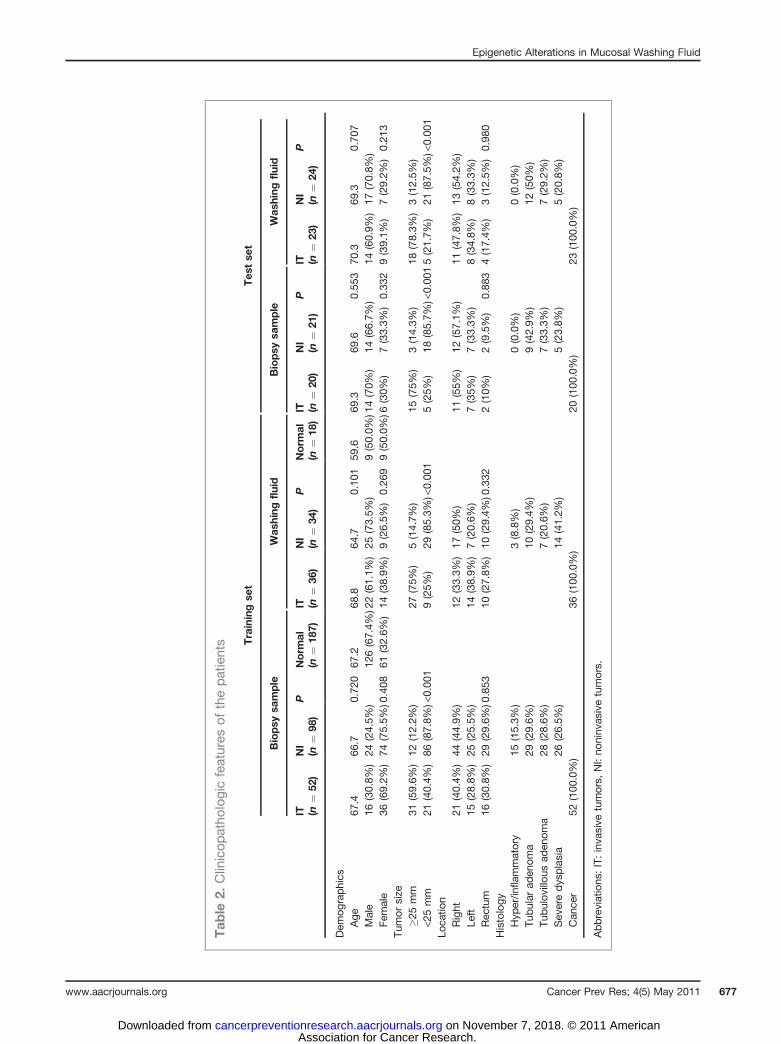
DNA methylation in biopsy specimensThe clinical features of the patients examined in this
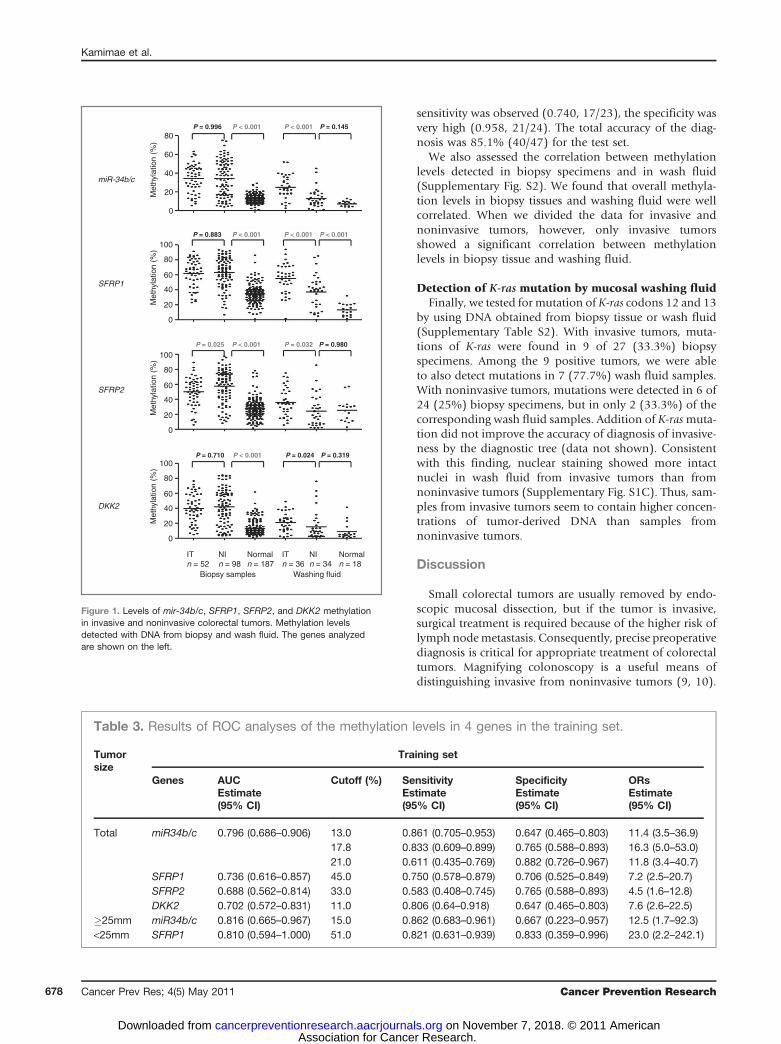
study are summarized in Table 2. There was no statisti-cally significant difference in age or gender betweenpatients with invasive and noninvasive tumors. Weselected 4 genes for analysis, mir-34b/c, SFRP1, SFRP2,and DKK2, which are frequently methylated in colorectalcancer (25, 27, 28). Methylation analysis was carried outby using bisulfite pyrosequencing with DNA from 337specimens, including 52 invasive tumors, 98 noninvasivetumors, and 187 specimens of normal colon tissue. Wefound that the methylation levels of the 4 genes weresignificantly higher in cancerous tissue than in normalcolorectal mucosa (Fig. 1); however, we found no differ-ence in tissue methylation levels between invasive andnoninvasive tumors.
DNA methylation in mucosal washing fluidWe next examined gene methylation in 76 samples of
mucosal wash fluid from 36 patients with invasive tumorsand 34 with noninvasive tumors, and from 18 patientswithout colorectal lesions (Fig. 1). When we compared theinvasive and noninvasive tumors, we found no differencesfor SFRP2 and DKK2. However, mir-34b/c and SFRP1showed higher levels of methylation in wash fluid frompatients with invasive than with noninvasive tumors.
We then used ROC analysis to further compare mucosalwash fluid from invasive and noninvasive tumors (Fig. 3Aand B). The odds ratios (OR) for the risk of invasionassociated with the methylation levels of the 4 genes testedare shown in Table 3. High levels of methylation weresignificantly associated with an increased risk of invasion.Among the 4 genes, levels ofmir-34b/cmethylation had the
greatest impact on the risk of invasion and showed thelargest AUC (0.796). Using various cutoff points of mir-34b/c methylation determined on the basis of efficiencyconsiderations for clinical use, the sensitivity/specificitywere 0.861/0.657 for the 13.0% (high sensitivity) cutoffpoint and 0.765/0.833 for the 17.8% (well balanced) cut-off. We also subdivided the tumors on the basis of whetherthey were�25mm or <25mm in size. In tumors 25mm orlarger, mir-34b/c showed the highest AUC (0.816); itssensitivity/specificity was 0.862/0.667 and its OR was12.5. In tumors smaller than 25 mm, SFRP1 showed thehighest AUC (0.810), with a sensitivity/specificity of 0.821/0.833 and an OR of 23.0.
We further verified the utility of DNA methylation inmucosal washing, using an independent set of specimens,which was established as the test set (Figs. 2, 3C and D;Table 4). All of these ROC analyses were considered thetraining set. In the test set, the methylation levels of mir-34b/c showed very high AUC again (0.915), sensitivity/specificity was 0.870/0.875 for the 13.0% cutoff, and0.565/0.958 for the 17.8% cutoff. In tumors 25 mm orlarger, the AUC of the methylation levels of mir-34b/c was0.778. In tumors smaller than 25 mm, the AUC of themethylation levels of SFRP1 was 0.695.
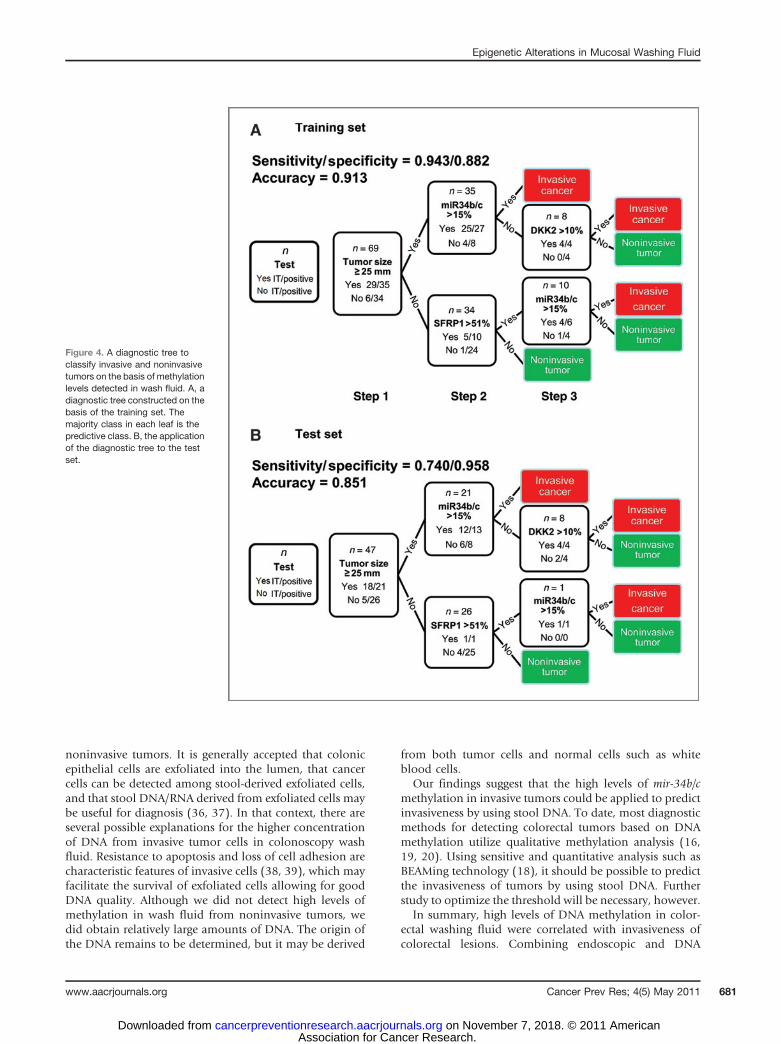
To make a more efficient diagnostic method suitable forclinical situations, we then constructed a diagnostic tree toclassify invasive and noninvasive tumors on the basis of thecombination of methylation levels detected in wash fluid(Fig. 4A). First, because most endoscopists make an endo-scopic diagnosis according to the size of lesions, we definedthe most efficient cutoff of tumor size as the first node ofthe diagnostic tree. As the next nodes, we used the mostefficient cutoffs of the methylation levels of the 4 genes(mir-34, SFRP1, SFRP2, andDKK2). For example, as shownin Figure 4A, if the tumor size is more than 25 mm and themethylation level ofmir-34b/c is more than 15%, this lesionis diagnosed as an invasive tumor. In the training set, thesensitivity and specificity were 0.943 (33/35) and 0.882(30/34), respectively. The total accuracy of the diagnosiswas 91.3% (63/69). For use in clinical situations, wevalidated this diagnostic tree by using an independent testset (n ¼ 47). The application of the diagnostic tree to thetest set is shown in Figure 4B. Although a slight reduction in
Table 1. Amounts of DNA and quality of cytology obtained by using the 2 collection methods tested
Biopsy (n ¼ 11) Wash fluid (method 1) Biopsy (n ¼ 37) Wash fluid (method 2)
Total(n ¼ 11)
IT(n ¼ 8)
NI(n ¼ 3)
Total(n ¼ 37)
IT(n ¼ 18)
NI(n ¼ 19)
DNA, mg 21.28 � 15.25 15.00 � 11.12 17.08 � 13.00 16.53 � 16.88Cytology
Diagnosable 2 1 1 17 11 6Not diagnosable 9 7 2 20 7 13
18.2% 12.5% 33.3% 45.9% 61.1% 31.6%
Abbreviations: IT: invasive tumors, NI: noninvasive tumors.
Kamimae et al.
Cancer Prev Res; 4(5) May 2011 Cancer Prevention Research676
Association for Cancer Research. on November 7, 2018. © 2011 Americancancerpreventionresearch.aacrjournals.org Downloaded from
Tab
le2.
Clinicop
atho
logicfeatures
ofthepatients Trainingse
tTes
tse
t
Biopsy
sample
Was
hing
fluid
Biopsy
sample
Was
hing
fluid
IT (n¼
52)
NI
(n¼
98)
PNorm
al(n
¼18
7)IT (n
¼36
)NI
(n¼
34)
PNorm
al(n
¼18
)IT (n
¼20
)NI
(n¼
21)
PIT (n
¼23
)NI
(n¼
24)
P
Dem
ograph
ics
Age
67.4
66.7
0.72
067
.268
.864
.70.10
159
.669
.369
.60.55
370
.369
.30.70
7Male
16(30.8%
)24
(24.5%
)12
6(67.4%
)22(61.1%
)25
(73.5%
)9(50.0%
)14(70%
)14
(66.7%
)14
(60.9%
)17
(70.8%
)Fe
male
36(69.2%
)74
(75.5%
)0.408
61(32.6%
)14
(38.9%
)9(26.5%
)0.26
99(50.0%
)6(30%
)7(33.3%
)0.33
29(39.1%
)7(29.2%
)0.21
3Tu
mor
size
�25mm
31(59.6%
)12
(12.2%
)27
(75%
)5(14.7%
)15
(75%
)3(14.3%
)18
(78.3%
)3(12.5%
)<2
5mm
21(40.4%
)86
(87.8%
)<0.00
19(25%
)29
(85.3%
)<0.00
15(25%
)18
(85.7%
)<0.00
15(21.7%
)21
(87.5%
)<0.00
1Lo
catio
nRight
21(40.4%
)44
(44.9%
)12
(33.3%
)17
(50%
)11
(55%
)12
(57.1%
)11
(47.8%
)13
(54.2%
)Le
ft15
(28.8%
)25
(25.5%
)14
(38.9%
)7(20.6%
)7(35%
)7(33.3%
)8(34.8%
)8(33.3%
)Rec
tum
16(30.8%
)29
(29.6%
)0.853
10(27.8%
)10
(29.4%
)0.332
2(10%
)2(9.5%
)0.88
34(17.4%
)3(12.5%
)0.98
0Histology
Hyp
er/in
flammatory
15(15.3%
)3(8.8%)
0(0.0%)
0(0.0%)
Tubu
larad
enom
a29
(29.6%
)10
(29.4%
)9(42.9%
)12
(50%
)Tu
bulovillo
usad
enom
a28
(28.6%
)7(20.6%
)7(33.3%
)7(29.2%
)Sev
eredys
plasia
26(26.5%
)14
(41.2%
)5(23.8%
)5(20.8%
)Can
cer
52(100
.0%
)36
(100
.0%
)20
(100
.0%
)23
(100
.0%
)
Abbreviations
:IT:inva
sive
tumors,
NI:no
ninv
asivetumors.
Epigenetic Alterations in Mucosal Washing Fluid
www.aacrjournals.org Cancer Prev Res; 4(5) May 2011 677
Association for Cancer Research. on November 7, 2018. © 2011 Americancancerpreventionresearch.aacrjournals.org Downloaded from
sensitivity was observed (0.740, 17/23), the specificity wasvery high (0.958, 21/24). The total accuracy of the diag-nosis was 85.1% (40/47) for the test set.
We also assessed the correlation between methylationlevels detected in biopsy specimens and in wash fluid(Supplementary Fig. S2). We found that overall methyla-tion levels in biopsy tissues and washing fluid were wellcorrelated. When we divided the data for invasive andnoninvasive tumors, however, only invasive tumorsshowed a significant correlation between methylationlevels in biopsy tissue and washing fluid.
Detection of K-ras mutation by mucosal washing fluidFinally, we tested for mutation of K-ras codons 12 and 13
by using DNA obtained from biopsy tissue or wash fluid(Supplementary Table S2). With invasive tumors, muta-tions of K-ras were found in 9 of 27 (33.3%) biopsyspecimens. Among the 9 positive tumors, we were ableto also detect mutations in 7 (77.7%) wash fluid samples.With noninvasive tumors, mutations were detected in 6 of24 (25%) biopsy specimens, but in only 2 (33.3%) of thecorresponding wash fluid samples. Addition of K-rasmuta-tion did not improve the accuracy of diagnosis of invasive-ness by the diagnostic tree (data not shown). Consistentwith this finding, nuclear staining showed more intactnuclei in wash fluid from invasive tumors than fromnoninvasive tumors (Supplementary Fig. S1C). Thus, sam-ples from invasive tumors seem to contain higher concen-trations of tumor-derived DNA than samples fromnoninvasive tumors.
Discussion
Small colorectal tumors are usually removed by endo-scopic mucosal dissection, but if the tumor is invasive,surgical treatment is required because of the higher risk oflymph nodemetastasis. Consequently, precise preoperativediagnosis is critical for appropriate treatment of colorectaltumors. Magnifying colonoscopy is a useful means ofdistinguishing invasive from noninvasive tumors (9, 10).
80P = 0.996 P < 0.001 P < 0.001 P = 0.145
P = 0.883 P < 0.001
P = 0.025
P = 0.710 P < 0.001 P = 0.024 P = 0.319
P < 0.001 P = 0.032 P = 0.980
P < 0.001 P < 0.001
100
80
60
40
20
0
Met
hyla
tion
(%)
Met
hyla
tion
(%)
100
80
60
40
20
0
Met
hyla
tion
(%)
100
80
60
40
20
0
ITn = 52
NIn = 98
Biopsy samples Washing fluid
ITn = 36
NIn = 34
Normaln = 18
Normaln = 187
Met
hyla
tion
(%)
60
40
20
miR-34b/c
SFRP1
SFRP2
DKK2
0
Figure 1. Levels of mir-34b/c, SFRP1, SFRP2, and DKK2 methylationin invasive and noninvasive colorectal tumors. Methylation levelsdetected with DNA from biopsy and wash fluid. The genes analyzedare shown on the left.
Table 3. Results of ROC analyses of the methylation levels in 4 genes in the training set.
Tumorsize
Training set
Genes AUC Cutoff (%) Sensitivity Specificity ORsEstimate(95% CI)
Estimate(95% CI)
Estimate(95% CI)
Estimate(95% CI)
Total miR34b/c 0.796 (0.686–0.906) 13.0 0.861 (0.705–0.953) 0.647 (0.465–0.803) 11.4 (3.5–36.9)17.8 0.833 (0.609–0.899) 0.765 (0.588–0.893) 16.3 (5.0–53.0)21.0 0.611 (0.435–0.769) 0.882 (0.726–0.967) 11.8 (3.4–40.7)
SFRP1 0.736 (0.616–0.857) 45.0 0.750 (0.578–0.879) 0.706 (0.525–0.849) 7.2 (2.5–20.7)SFRP2 0.688 (0.562–0.814) 33.0 0.583 (0.408–0.745) 0.765 (0.588–0.893) 4.5 (1.6–12.8)DKK2 0.702 (0.572–0.831) 11.0 0.806 (0.64–0.918) 0.647 (0.465–0.803) 7.6 (2.6–22.5)
�25mm miR34b/c 0.816 (0.665–0.967) 15.0 0.862 (0.683–0.961) 0.667 (0.223–0.957) 12.5 (1.7–92.3)<25mm SFRP1 0.810 (0.594–1.000) 51.0 0.821 (0.631–0.939) 0.833 (0.359–0.996) 23.0 (2.2–242.1)
Kamimae et al.
Cancer Prev Res; 4(5) May 2011 Cancer Prevention Research678
Association for Cancer Research. on November 7, 2018. © 2011 Americancancerpreventionresearch.aacrjournals.org Downloaded from

However, invasive colorectal tumors show a heterogeneouspit pattern, making it difficult to determine a therapeuticstrategy based on pit pattern diagnosis alone (29). Notably,surface mucus is washed away during magnifying endo-scopic analysis, so that utilization of the wash fluid couldbe an effective noninvasive approach to diagnosis. It hasbeen recommended that nearly all colorectal cancerpatients who receive EMR receive periodic endoscopy forearly detection of relapses (30). Examination of the methy-lation levels in the wash fluid could provide helpful infor-mation as to how often the patient should receive thefollow-up endoscopy (e.g., the lower the methylation level,
the less frequently endoscopic examination may beneeded). In addition, although we did not include fol-low-up in our study, it is possible that wash fluid analysiscould help physicians detect mucosal relapse after EMRduring follow-up endoscopy.
It has been reported that DNAmethylation in wash fluidcontaining pancreatic juice, saliva, or gastric juice is usefulfor diagnosis and risk assessment in cancer (34–36). Forexample, Watanabe and colleagues reported that DNAmethylation in gastric wash fluid is useful for detectionof early gastric cancer (36). The unique feature of our studyis that it suggests DNAmethylation in colon mucosal washfluid can be used to predict the invasiveness of tumors.Further study will be necessary to determine whether DNAmethylation of colon mucosal wash might also be usefulfor screening or risk assessment in cancer.
Here we showed that levels of mir-34b/c gene methyla-tion were predictive of the invasiveness of colorectaltumors (Figs. 3 and 4; Tables 3 and 4). The sensitivity(0.833) and specificity (0.765) of this approach (wellbalanced cutoff), as well as the ROC AUC value (0.796),suggest methylation of this gene in colonoscopic wash fluidis a goodmolecularmarker that distinguishes invasive fromnoninvasive colorectal tumors. We also showed that adiagnostic tree constructed by the combination of methy-lation levels was highly accurate for predicting invasive-ness. To avoid unneeded surgery, it is important that theprediction of invasiveness is highly specific. In this regard,the specificities of the diagnostic tree were 0.882 in thetraining set, and 0.958 in the test set.
There is currently no molecular test that distinguishesinvasive from noninvasive colorectal tumors. DNA methy-lation can be used as a biomarker for detection of colorectallesions (16–20), but genes frequently methylated in cancerare also frequently methylated in early lesions (e.g., ade-nomas), and even in normal colorectal mucosa from agedpatients (21, 22). It is therefore difficult to distinguishinvasive tumors from noninvasive ones. We previouslyshowed that SFRP1 and SFRP2 are frequently methylatedin colorectal cancer (28). However, they are also oftenmethylated in normal colorectal mucosa in an age-relatedmanner (34), which is consistent with our present findings.The mir-34b/c gene is a putative tumor suppressor whoseexpression is induced by p53 (35). We previously showedthatmir-34b/c is silenced by DNAmethylation in colorectalcancers and adenomas (25). In this study, we found thatmethylation of mir-34b/c in noninvasive tumors is as highas that in invasive tumors. By contrast, levels of mir-34b/cmethylation in normal colorectal mucosa are low. Thus,given the high frequency of methylation in tumors, tumor-specific methylation of mir-34b/c may be a highly usefulmolecular marker for colorectal cancer.
The molecular mechanism underlying the high levels ofDNA methylation in wash fluid from invasive tumors isnot fully understood. Analysis of nuclear staining, DNAmethylation, and K-ras mutation suggest that wash fluid–derived DNA from invasive tumors contains higher con-centrations of tumor-derived DNA than wash fluid from
100
150
100
50
0
80
60
40
20
0
Met
hyla
tion
(%)
100
80
60
40
20
0
Met
hyla
tion
(%)
Met
hyla
tion
(%)
100
80
60
40
20
0
Met
hyla
tion
(%)
miR-34b/c
SFRP1
SFRP2
DKK2
P = 0.634
Test set
P < 0.001
P = 0.733 P = 0.001
P = 0.586 P = 0.644
P = 0.630 P = 0.198
ITn = 20
ITn = 23
NIn = 24
NIn = 21
Biopsy samples Washing fluid
Figure 2.Methylation levels ofmir-34b/c, SFRP1, SFRP2, andDKK2 in thetest set. Methylation levels detected with DNA from biopsy tissues andwash fluid. The genes analyzed are shown on the left.
Epigenetic Alterations in Mucosal Washing Fluid
www.aacrjournals.org Cancer Prev Res; 4(5) May 2011 679
Association for Cancer Research. on November 7, 2018. © 2011 Americancancerpreventionresearch.aacrjournals.org Downloaded from
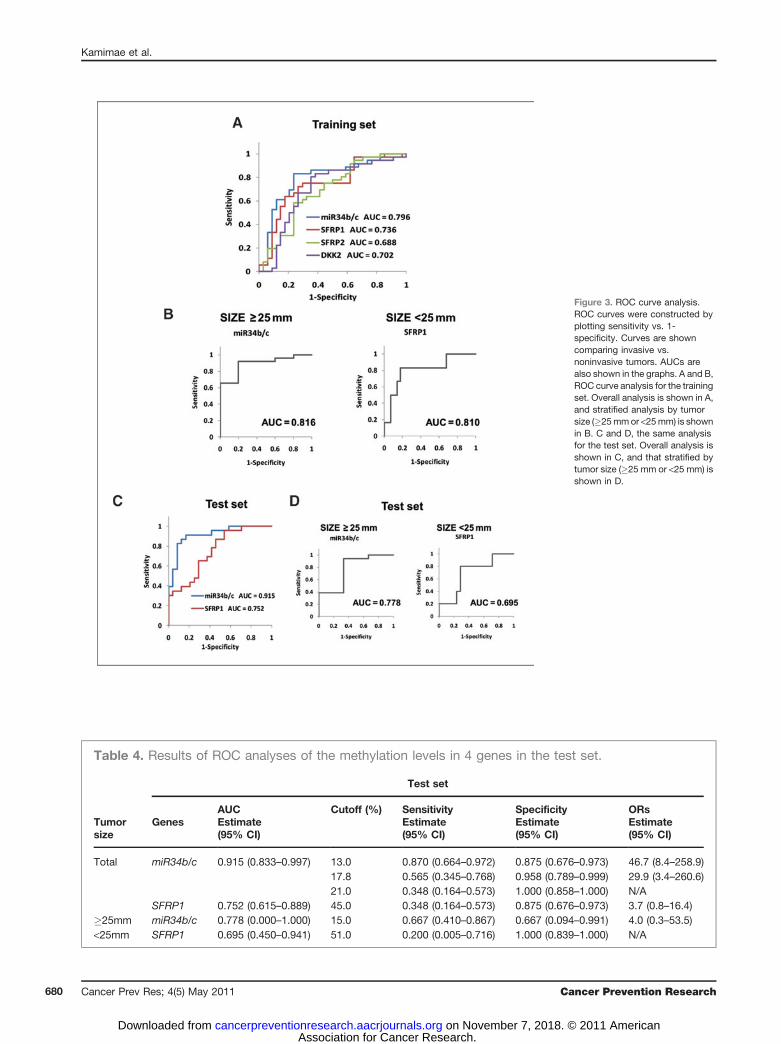
Figure 3. ROC curve analysis.ROC curves were constructed byplotting sensitivity vs. 1-specificity. Curves are showncomparing invasive vs.noninvasive tumors. AUCs arealso shown in the graphs. A and B,ROC curve analysis for the trainingset. Overall analysis is shown in A,and stratified analysis by tumorsize (�25mmor <25mm) is shownin B. C and D, the same analysisfor the test set. Overall analysis isshown in C, and that stratified bytumor size (�25 mm or <25 mm) isshown in D.
Table 4. Results of ROC analyses of the methylation levels in 4 genes in the test set.
Test set
AUC Cutoff (%) Sensitivity Specificity ORsTumorsize
Genes Estimate(95% CI)
Estimate(95% CI)
Estimate(95% CI)
Estimate(95% CI)
Total miR34b/c 0.915 (0.833–0.997) 13.0 0.870 (0.664–0.972) 0.875 (0.676–0.973) 46.7 (8.4–258.9)17.8 0.565 (0.345–0.768) 0.958 (0.789–0.999) 29.9 (3.4–260.6)21.0 0.348 (0.164–0.573) 1.000 (0.858–1.000) N/A
SFRP1 0.752 (0.615–0.889) 45.0 0.348 (0.164–0.573) 0.875 (0.676–0.973) 3.7 (0.8–16.4)�25mm miR34b/c 0.778 (0.000–1.000) 15.0 0.667 (0.410–0.867) 0.667 (0.094–0.991) 4.0 (0.3–53.5)<25mm SFRP1 0.695 (0.450–0.941) 51.0 0.200 (0.005–0.716) 1.000 (0.839–1.000) N/A
Kamimae et al.
Cancer Prev Res; 4(5) May 2011 Cancer Prevention Research680
Association for Cancer Research. on November 7, 2018. © 2011 Americancancerpreventionresearch.aacrjournals.org Downloaded from
noninvasive tumors. It is generally accepted that colonicepithelial cells are exfoliated into the lumen, that cancercells can be detected among stool-derived exfoliated cells,and that stool DNA/RNA derived from exfoliated cells maybe useful for diagnosis (36, 37). In that context, there areseveral possible explanations for the higher concentrationof DNA from invasive tumor cells in colonoscopy washfluid. Resistance to apoptosis and loss of cell adhesion arecharacteristic features of invasive cells (38, 39), which mayfacilitate the survival of exfoliated cells allowing for goodDNA quality. Although we did not detect high levels ofmethylation in wash fluid from noninvasive tumors, wedid obtain relatively large amounts of DNA. The origin ofthe DNA remains to be determined, but it may be derived
from both tumor cells and normal cells such as whiteblood cells.
Our findings suggest that the high levels of mir-34b/cmethylation in invasive tumors could be applied to predictinvasiveness by using stool DNA. To date, most diagnosticmethods for detecting colorectal tumors based on DNAmethylation utilize qualitative methylation analysis (16,19, 20). Using sensitive and quantitative analysis such asBEAMing technology (18), it should be possible to predictthe invasiveness of tumors by using stool DNA. Furtherstudy to optimize the threshold will be necessary, however.
In summary, high levels of DNA methylation in color-ectal washing fluid were correlated with invasiveness ofcolorectal lesions. Combining endoscopic and DNA
Figure 4. A diagnostic tree toclassify invasive and noninvasivetumors on the basis of methylationlevels detected in wash fluid. A, adiagnostic tree constructed on thebasis of the training set. Themajority class in each leaf is thepredictive class. B, the applicationof the diagnostic tree to the testset.
Epigenetic Alterations in Mucosal Washing Fluid
www.aacrjournals.org Cancer Prev Res; 4(5) May 2011 681
Association for Cancer Research. on November 7, 2018. © 2011 Americancancerpreventionresearch.aacrjournals.org Downloaded from

methylation analyses may facilitate accurate preoperativestaging of colorectal cancer.
Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed.
Acknowledgments
The authors thank Dr. William F. Goldman for editing the manuscript.
Grant Support
This study was supported in part by Grants-in-Aid for Scientific Research onPriority Areas (T. Tokino, K. Imai, and M. Toyota), Grants-in-Aid for ScientificResearch (S) from the Japan Society for Promotion of Science (K. Imai), a Grant-in-Aid for the Third-term Comprehensive 10-year Strategy for Cancer Control(M. Toyota), and a Grant-in-Aid for Cancer Research from the Ministry ofHealth, Labor, and Welfare, Japan (M. Toyota).
The costs of publication of this article were defrayed in part by the paymentof page charges. This article must therefore be hereby marked advertisementin accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received August 25, 2010; revised January 19, 2011; accepted January 27,2011; published online May 4, 2011.
References1. Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, et al. Cancer
statistics, 2008. CA Cancer J Clin 2008;58:71–96.2. Davies RJ, Miller R, Coleman N. Colorectal cancer screening: pro-
spects for molecular stool analysis. Nat Rev Cancer 2005;5:199–209.
3. Osborn NK, Ahlquist DA. Stool screening for colorectal cancer:molecular approaches. Gastroenterology 2005;128:192–206.
4. Kwok H, Bissett IP, Hill GL. Preoperative staging of rectal cancer. Int JColorectal Dis 2000;15:9–20.
5. Yamada I, Okabe S, EnomotoM, Sugihara K, Yoshino N, Tetsumura A,et al. Colorectal carcinoma: in vitro evaluation with high-spatial-resolution 3D constructive interference in steady-state MR imaging.Radiology 2008;246:444–53.
6. Hurlstone DP, Cross SS, Adam I, Shorthouse AJ, Brown S, SandersDS, et al. A prospective clinicopathological and endoscopic evalua-tion of flat and depressed colorectal lesions in the United Kingdom.Am J Gastroenterol 2003;98:2543–9.
7. Kudo S, Kashida H, Tamura T, Kogure E, Imai Y, Yamano H, et al.Colonoscopic diagnosis andmanagement of nonpolypoid early color-ectal cancer. World J Surg 2000;24:1081–90.
8. Soetikno R, Friedland S, Kaltenbach T, Chayama K, Tanaka S. Non-polypoid (flat and depressed) colorectal neoplasms. Gastroenterology2006;130:566–76; quiz 88–9.
9. Bianco MA, Rotondano G, Marmo R, Garofano ML, Piscopo R, deGregorio A, et al. Predictive value of magnification chromoendoscopyfor diagnosing invasive neoplasia in nonpolypoid colorectal lesionsand stratifying patients for endoscopic resection or surgery. Endo-scopy 2006;38:470–6.
10. Matsuda T, Fujii T, Saito Y, Nakajima T, Uraoka T, Kobayashi N, et al.Efficacy of the invasive/non-invasive pattern by magnifying chro-moendoscopy to estimate the depth of invasion of early colorectalneoplasms. Am J Gastroenterol 2008;103:2700–6.
11. Kanao H, Tanaka S, Oka S, Hirata M, Yoshida S, Chayama K. Narrow-band imaging magnification predicts the histology and invasion depthof colorectal tumors. Gastrointest Endosc 2009;69:631–6.
12. Markowitz SD, Bertagnolli MM. Molecular origins of cancer: Molecularbasis of colorectal cancer. N Engl J Med 2009;361:2449–60.
13. Wong JJ, Hawkins NJ, Ward RL. Colorectal cancer: a model forepigenetic tumorigenesis. Gut 2007;56:140–8.
14. Issa JP. CpG island methylator phenotype in cancer. Nat Rev Cancer2004;4:988–93.
15. Jones PA, Baylin SB. The epigenomics of cancer. Cell 2007;128:683–92.
16. Gl€ockner SC, Dhir M, Yi JM, McGarvey KE, Van Neste L, LouwagieJ, et al. Methylation of TFPI2 in stool DNA: a potential novelbiomarker for the detection of colorectal cancer. Cancer Res2009;69:4691–9.
17. Hellebrekers DM, Lentjes MH, van den Bosch SM, Melotte V, WoutersKA, Daenen KL, et al. GATA4 and GATA5 are potential tumor sup-pressors and biomarkers in colorectal cancer. Clin Cancer Res2009;15:3990–7.
18. Li M, Chen WD, Papadopoulos N, Goodman SN, Bjerregaard NC,Laurberg S, et al. Sensitive digital quantification of DNAmethylation inclinical samples. Nat Biotechnol 2009;27:858–63.
19. M€uller HM, Oberwalder M, Fiegl H, Morandell M, Goebel G, Zitt M,et al. Methylation changes in faecal DNA: a marker for colorectalcancer screening? Lancet 2004;363:1283–5.
20. Zou HZ, Yu BM, Wang ZW, Sun JY, Cang H, Gao F, et al. Detection ofaberrant p16 methylation in the serum of colorectal cancer patients.Clin Cancer Res 2002;8:188–91.
21. Ahuja N, Li Q, Mohan AL, Baylin SB, Issa JP. Aging and DNAmethylation in colorectal mucosa and cancer. Cancer Res 1998;58:5489–94.
22. Issa JP, Ottaviano YL, Celano P, Hamilton SR, Davidson NE, BaylinSB. Methylation of the oestrogen receptor CpG island links ageingand neoplasia in human colon. Nat Genet 1994;7:536–40.
23. Park SJ, Rashid A, Lee JH, Kim SG, Hamilton SR, Wu TT. FrequentCpG islandmethylation in serrated adenomas of the colorectum. Am JPathol 2003;162:815–22.
24. Satoh A, Toyota M, Itoh F, Sasaki Y, Suzuki H, Ogi K, et al. Epigeneticinactivation of CHFR and sensitivity to microtubule inhibitors in gastriccancer. Cancer Res 2003;63:8606–13.
25. Toyota M, Suzuki H, Sasaki Y, Maruyama R, Imai K, Shinomura Y,et al. Epigenetic silencing of microRNA-34b/c and B-cell translocationgene 4 is associated with CpG island methylation in colorectal cancer.Cancer Res 2008;68:4123–32.
26. Kusano M, Toyota M, Suzuki H, Akino K, Aoki F, Fujita M, et al.Genetic, epigenetic, and clinicopathologic features of gastric carci-nomas with the CpG island methylator phenotype and an associationwith Epstein-Barr virus. Cancer 2006;106:1467–79.
27. Sato H, Suzuki H, Toyota M, Nojima M, Maruyama R, Sasaki S,et al. Frequent epigenetic inactivation of DICKKOPF family genesin human gastrointestinal tumors. Carcinogenesis 2007;28:2459–66.
28. Suzuki H, Watkins DN, Jair KW, Schuebel KE, Markowitz SD, ChenWD, et al. Epigenetic inactivation of SFRP genes allows constitu-tive WNT signaling in colorectal cancer. Nat Genet 2004;36:417–22.
29. Tanaka S, Kaltenbach T, Chayama K, Soetikno R. High-magnifica-tion colonoscopy (with videos). Gastrointest Endosc 2006;64:604–13.
30. Winawer SJ, Zauber AG, Fletcher RH, Stillman JS, O’Brien MJ, LevinB, et al. Guidelines for colonoscopy surveillance after polypectomy: aconsensus update by the US Multi-Society Task Force on ColorectalCancer and the American Cancer Society. Gastroenterology 2006;130:1872–85.
31. Matsubayashi H, Canto M, Sato N, Klein A, Abe T, Yamashita K,et al. DNA methylation alterations in the pancreatic juice ofpatients with suspected pancreatic disease. Cancer Res 2006;66:1208–17.
32. Pattani KM, Zhang Z, Demokan S, Glazer C, Loyo M, Goodman S,et al. Endothelin receptor type B gene promoter hypermethylation insalivary rinses is independently associated with risk of oral cavitycancer and premalignancy. Cancer Prev Res 2010;3:1093–103.
33. Watanabe Y, Kim HS, Castoro RJ, Chung W, Estecio MR, Kondo K,et al. Sensitive and specific detection of early gastric cancer with DNAmethylation analysis of gastric washes. Gastroenterology 2009;136:2149–58.
Kamimae et al.
Cancer Prev Res; 4(5) May 2011 Cancer Prevention Research682
Association for Cancer Research. on November 7, 2018. © 2011 Americancancerpreventionresearch.aacrjournals.org Downloaded from

34. Shen L, Toyota M, Kondo Y, Lin E, Zhang L, Guo Y, et al. Integratedgenetic and epigenetic analysis identifies three different subclasses ofcolon cancer. Proc Natl Acad Sci U S A 2007;104:18654–9.
35. He L, He X, Lim LP, de Stanchina E, Xuan Z, Liang Y, et al. A microRNAcomponent of the p53 tumour suppressor network. Nature 2007;447:1130–4.
36. White V, Scarpini C, Barbosa-Morais NL, Ikelle E, Carter S, Laskey RA,et al. Isolation of stool-derived mucus provides a high yield ofcolonocytes suitable for early detection of colorectal carcinoma.Cancer Epidemiol Biomarkers Prev 2009;18:2006–13.
37. Zhao C, Ivanov I, Dougherty ER, Hartman TJ, Lanza E, Bobe G, et al.Noninvasive detection of candidate molecular biomarkers in subjectswith a history of insulin resistance and colorectal adenomas. CancerPrev Res 2009;2:590–7.
38. Brown JM, Attardi LD. The role of apoptosis in cancer deve-lopment and treatment response. Nat Rev Cancer 2005;5:231–7.
39. Christofori G. Changing neighbours, changing behaviour: cell adhe-sion molecule-mediated signalling during tumour progression. EMBOJ 2003;22:2318–23.
Epigenetic Alterations in Mucosal Washing Fluid
www.aacrjournals.org Cancer Prev Res; 4(5) May 2011 683
Association for Cancer Research. on November 7, 2018. © 2011 Americancancerpreventionresearch.aacrjournals.org Downloaded from
2011;4:674-683. Cancer Prev Res Seiko Kamimae, Eiichiro Yamamoto, Hiro-o Yamano, et al. Invasiveness of Colorectal TumorsEpigenetic Alteration of DNA in Mucosal Wash Fluid Predicts
Updated version
http://cancerpreventionresearch.aacrjournals.org/content/4/5/674
Access the most recent version of this article at:
Material
Supplementary
http://cancerpreventionresearch.aacrjournals.org/content/suppl/2011/05/05/4.5.674.DC1
Access the most recent supplemental material at:
Cited articles
http://cancerpreventionresearch.aacrjournals.org/content/4/5/674.full#ref-list-1
This article cites 36 articles, 11 of which you can access for free at:
Citing articles
http://cancerpreventionresearch.aacrjournals.org/content/4/5/674.full#related-urls
This article has been cited by 4 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
SubscriptionsReprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. (CCC)Click on "Request Permissions" which will take you to the Copyright Clearance Center's
.http://cancerpreventionresearch.aacrjournals.org/content/4/5/674To request permission to re-use all or part of this article, use this link
Association for Cancer Research. on November 7, 2018. © 2011 Americancancerpreventionresearch.aacrjournals.org Downloaded from