etidronate for prevention of ectopic mineralization in patients … · best corrected visual acuity...
TRANSCRIPT
Listen to this manuscript’s
audio summary by
JACC Editor-in-Chief
Dr. Valentin Fuster.
J O U R N A L O F T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y VO L . 7 1 , N O . 1 0 , 2 0 1 8
ª 2 0 1 8 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N
P U B L I S H E D B Y E L S E V I E R
Etidronate for Prevention ofEctopic Mineralization in Patients WithPseudoxanthoma Elasticum
Guido Kranenburg, MD,a Pim A. de Jong, MD, PHD,b Jonas W. Bartstra, MD,a Suzanne J. Lagerweij, MD,bMarnix G. Lam, MD, PHD,b Jeannette Ossewaarde-van Norel, MD, PHD,c Sara Risseeuw, MD,c
Redmer van Leeuwen, MD, PHD,c Saskia M. Imhof, MD, PHD,c Harald J. Verhaar, MD, PHD,d Job J. de Vries, BSC,b
Riemer H.J.A. Slart, MD, PHD,e Gert Luurtsema, PHD,e Annemarie M. den Harder, MD,b Frank L.J. Visseren, MD, PHD,a
Willem P. Mali, MD, PHD,b Wilko Spiering, MD, PHDa
ABSTRACT
ISS
FrobDcD
Ge
Ce
Gr
ve
UN
ma
the
au
Ma
BACKGROUND In pseudoxanthoma elasticum (PXE), low pyrophosphate levels may cause ectopic mineralization,
leading to skin changes, visual impairment, and peripheral arterial disease.
OBJECTIVES The authors hypothesized that etidronate, a pyrophosphate analog, might reduce ectopic mineralization
in PXE.
METHODS In the Treatment of Ectopic Mineralization in Pseudoxanthoma Elasticum trial, adults with PXE and leg
arterial calcifications (n ¼ 74) were randomly assigned to etidronate or placebo (cyclical 20 mg/kg for 2 weeks every
12 weeks). The primary outcome was ectopic mineralization, quantified with 18fluoride positron emission tomography
scans as femoral arterial wall target-to-background ratios (TBRfemoral). Secondary outcomes were computed tomography
arterial calcification and ophthalmological changes. Safety outcomes were bone density, serum calcium, and phosphate.
RESULTS During 12 months of follow-up, the TBRfemoral increased 6% (interquartile range [IQR]: �12% to 25%) in the
etidronate group and 7% (IQR: �9% to 32%) in the placebo group (p ¼ 0.465). Arterial calcification decreased 4%
(IQR: �11% to 7%) in the etidronate group and increased 8% (IQR: �1% to 20%) in the placebo group (p ¼ 0.001).
Etidronate treatment was associated with significantly fewer subretinal neovascularization events (1 vs. 9, p ¼ 0.007).
Bone density decreased 4% � 12% in the etidronate group and 6% � 9% in the placebo group (p ¼ 0.374). Hypocal-
cemia (<2.20 mmol/l) occurred in 3 versus 1 patient (8.1% vs. 2.7%, p ¼ 0.304). Eighteen patients (48.6%) treated with
etidronate, compared with 0 patients treated with placebo (p < 0.001), experienced hyperphosphatemia (>1.5 mmol/l)
and recovered spontaneously.
CONCLUSIONS In patients with PXE, etidronate reduced arterial calcification and subretinal neovascularization
events but did not lower femoral 18fluoride sodium positron emission tomography activity compared with placebo,
without important safety issues. (Treatment of Ectopic Mineralization in Pseudoxanthoma elasticum; NTR5180)
(J Am Coll Cardiol 2018;71:1117–26) © 2018 by the American College of Cardiology Foundation.
N 0735-1097/$36.00 https://doi.org/10.1016/j.jacc.2017.12.062
m the aDepartment of Vascular Medicine, University Medical Center Utrecht, Utrecht University, Utrecht, the Netherlands;
epartment of Radiology and Nuclear Medicine, University Medical Center Utrecht, Utrecht University, Utrecht, the Netherlands;
epartment of Ophthalmology, University Medical Center Utrecht, Utrecht University, Utrecht, the Netherlands; dDepartment of
riatric Medicine, University Medical Center Utrecht, Utrecht University, Utrecht, the Netherlands; and the eMedical Imaging
nter, Department of Nuclear Medicine and Molecular Imaging, University of Groningen, University Medical Center Groningen,
oningen, the Netherlands. This study was supported by the Dutch Innovation Fund of Health Insurers (Innovatiefonds Zorg-
rzekeraars), Dutch Foundation PXE Fund, Dutch Eye Association, and Foundation Friends of University Medical Center Utrecht.
I-Pharma Kleon Tsetis Pharmaceutical Laboratories SA (Greece) provided all etidronate and placebo capsules for free, as
nufacturer of the finished product (OSTOPOR hard capsules, 400 mg/capsule). UNI-Pharma SA was not involved in the design,
execution, the analysis, or the reporting of the Treatment of Ectopic Mineralization in Pseudoxanthoma Elasticum trial. The
thors have reported that they have no relationships relevant to the contents of this paper to disclose.
nuscript received December 14, 2017; accepted December 19, 2017.

ABBR EV I A T I ON S
AND ACRONYMS
18F-NaF PET = 18fluoride
sodium positron emission
tomography
ALT = alanine transaminase
AST = aspartate transaminase
BCVA = best corrected visual
acuity
CT = computed tomography
eGFR = estimated glomerular
filtration rate
IMT = intima-media thickness
IQR = interquartile range
PPi = inorganic pyrophosphate
PWV = pulse wave velocity
PXE = pseudoxanthoma
elasticum
SF-36 = Short Form 36
TBRfemoral = femoral arterial
wall target-to-background
ratio
VEGF = vascular endothelial
growth factor
Kranenburg et al. J A C C V O L . 7 1 , N O . 1 0 , 2 0 1 8
Etidronate for Prevention of Ectopic Mineralization M A R C H 1 3 , 2 0 1 8 : 1 1 1 7 – 2 6
1118
P seudoxanthoma elasticum (PXE,OMIM #264800) is an autosomalrecessive systemic calcification disor-
der. PXE is characterized by skin involve-ment (e.g., yellowish papules/plaques), eyeinvolvement (e.g., angioid streaks), andvascular involvement (arterial calcification),and has a considerable morbidity, includingsevere visual impairment and blindness, pe-ripheral arterial disease, ischemic stroke,and vascular dementia (1,2). The prevalenceis approximately 1:25,000 to 100,000 (2). Toprevent progression of visual impairmentcaused by choroidal neovascularization inpatients with PXE, injections with antivascu-lar endothelial growth factor (VEGF) are used(3); however, there is no specific and preven-tive treatment available for patients withPXE.
SEE PAGE 1127
PXE is caused by mutations in the ABCC6gene and associated with ectopic minerali-zation of elastic fibers in the skin, the Bruch
membrane beneath the retina, and the medial layer ofarteries (4). Recently, major steps have been made indeciphering the etiology of PXE. ABCC6 mutationshave been shown to result in reduced adenosinetriphosphate secretion in the liver causing low levelsof inorganic pyrophosphate (PPi) (5). PPi is a stronginhibitor of ectopic mineralization (6–8). Thedecreased levels of PPi in PXE may therefore causethe ectopic mineralization in PXE (9).
Bisphosphonates, well-established drugs for thetreatment of osteoporosis and bone metastases, arestable PPi analogs and could thus stimulate theinhibitory effects on ectopic mineralization (10). Infact, bisphosphonates have been shown to reduce softtissue calcifications in rats even before their effect onbone resorption was known (11). Of the currentlyavailable bisphosphonates, etidronate may have thelargest potential to delay ectopic mineralization givenits predominant inhibition of calcium precipitationand hydroxyapatite binding. This is different fromnewer bisphosphonates, such as alendronate, whichpredominantly inhibit osteoclasts (12,13).
Several nonrandomized and uncontrolled reportsdescribe beneficial effects of etidronate in patientswith rare diseases with ectopic mineralizationresulting from a deficiency in PPi homeostasis. Inpatients with basal ganglia calcifications or primarybrain calcifications (OMIM #213600), treatment withetidronate alleviates neurological symptoms (12,14).In generalized arterial calcification of infancy (OMIM
#208000) etidronate treatment reduces arterialcalcification and is associated with improved survival(15,16). Generalized arterial calcification of infancycan be seen as an aggressive form of PXE with aconsiderable overlap in genotype and phenotype(17,18). Treatment with etidronate in PXE mousemodels results in prevention of ectopic mineraliza-tion and in alterations in bone microarchitecture(19,20). The effectiveness of etidronate remains to beestablished in patients with PXE in a randomized,placebo-controlled trial.
We therefore hypothesized that synthetic PPisupplementation with etidronate treatment couldreduce ectopic mineralization in patients with PXE.To be able to investigate this hypothesis in a ran-domized, placebo-controlled trial, we used femoralarterial wall 18
fluoride sodium positron emissiontomography (18F-NaF PET) activity and computedtomography (CT)-based femoral calcium scores asmarkers of ectopic mineralization (21–25). Imagingwith 18F-NaF PET may be more sensitive to changes inectopic mineralization compared with traditional CTbecause it is believed to be able to visualize the activeand ongoing calcification process and discriminatebetween the active and the more indolent calcifica-tions (22,26).
Here, we report the results of the Treatment ofEctopic Mineralization in Pseudoxanthoma elasticum(TEMP) trial in which we set out to investigate theeffectiveness and safety of 1 year’s treatment withetidronate (cyclical 20 mg/kg for 2 weeks every12 weeks) on ectopic mineralization among partici-pants with PXE.
METHODS
TRIAL DESIGN AND STUDY POPULATION. The TEMPtrial was a single-center, randomized, double-blind,placebo-controlled trial conducted in the PXE exper-tise center at the University Medical Center Utrecht,the Netherlands. Participants eligible for participationhad a confirmed clinical diagnosis of PXE, were $18years of age, and had evidence of arterial calcificationon a CT scan of the legs that was acquired in all patientsduring the first visit in our center. PXE was diagnosedif 2 of the following were present: skin involvement(e.g., yellowish papules/plaques), eye involvement(e.g., angioid streaks), and genetically confirmation(biallelic ABCC6mutations) (1). Exclusion criteria weresevere renal impairment, known abnormality of theesophagus, known sensitivity to etidronate, use ofbisphosphonates during the past 5 years, osteoma-lacia, chronic diarrhea, pregnancy, claustrophobia,hypocalcemia (calcium <2.20 mmol/l), and vitamin D

FIGURE 1 Flowchart Eligibility, Randomization, and Follow-Up
77 Patients were assessed foreligibility
74 Underwent randomization
37 Were assigned to etidronate(cyclical 20 mg/kg for 2 weeks
every 12 weeks)
1 Discontinued intervention (after second treatment period)
37 were included in the(primary endpoint) analysis
36 were included in the(primary endpoint) analysis
1 Refused further participation(after ophthalmological event at
3 months of follow-up)
37 Were assigned to placebo(for 2 weeks every 12 weeks)
3 were ineligible or declinedto participate- 1 Declined to participate- 1 Did not meet PXE criteria- 1 Had claustrophobia
Seventy-seven patients were screened for eligibility and 74 patients underwent
randomization. Eventually, 37 patients in the etidronate group and 36 patients in the
placebo group were included in the (primary endpoint) analysis. PXE ¼ pseudoxanthoma
elasticum.
J A C C V O L . 7 1 , N O . 1 0 , 2 0 1 8 Kranenburg et al.M A R C H 1 3 , 2 0 1 8 : 1 1 1 7 – 2 6 Etidronate for Prevention of Ectopic Mineralization
1119
deficiency (25-OH vitamin D <35 nmol/l). TheTEMP trial was approved by the institutional reviewboard of the University Medical Center Utrecht (num-ber 15/522). All participants provided written informedconsent.
RANDOMIZATION AND INTERVENTION. Eligibleparticipants were randomized in a 1:1 ratio to either acyclical regime of 2 weeks 20 mg/kg etidronate withoral administration of 400 mg capsules every12 weeks or to an identical treatment regime andcapsules without the active pharmacological sub-stance (i.e., placebo). Thus, patients were given20 mg/kg every day for 2 weeks. Etidronate (OSTO-POR hard capsules, 400 mg/capsule) and placebocapsules were provided by Uni-Pharma Kleon TsetisPharmaceutical Laboratories SA (Athens, Greece).Randomization with random permuted blocks for sexwas performed using a random number generator atthe pharmacy department, where the randomizationlist was stored during the entire duration of the trial.
PROCEDURES. Full body 18F-NaF PET/CT scans wereperformed at baseline and after 12 months of follow-up on a Siemens Biograph 40 scanner (SiemensHealthcare, Erlangen, Germany). Images were recon-structed according to the European Association ofNuclear Medicine Research Ltd recommendations(27). Ninety minutes before imaging, an intravenousinjection of 2.0 MBq/kg 18F-NaF (maximum dosage:200 MBq) was administered. A conventional full-bodyCT scan was performed after 6 months of follow-up.
Measurements of carotid intima-media thickness(IMT) and carotid-femoral pulse wave velocity (PWV)were performed at baseline and after 12 months offollow-up. IMT was measured with ultrasound(Esaote, Florence, Italy) in the left and right carotidarteries. PWV was measured using applanationtonometry with a micromanometer (Millar In-struments Inc., Houston, Texas) in combination withSphygmocor software (Atcore Medical Pty. Ltd., Syd-ney, New South Wales, Australia).
Ophthalmological examination took place at base-line and after 3, 6, 9, and 12 months. The frequency ofsubretinal neovascularization events was monitoredwith optical coherence tomography scans and fundusphotography during all visits. The frequency of anti-VEGF injections in the year before the baseline visitand during the trial was obtained. If needed, medicalinformation was retrieved from other hospitals. Bestcorrected visual acuity (BCVA) was measured atbaseline and after 12 months follow-up using EarlyTreatment Diabetic Retinopathy Study letter charts(Online Appendix) (28). Quality of life was assessed atbaseline and after 12 months of follow-up using the
validated Dutch version of the 36-Item Short Formsurvey (SF-36) questionnaire (29).
Laboratory measurements for serum calcium andphosphate were performed at baseline, and after 3, 6,9, and 12 months of follow-up. Estimated glomerularfiltration rate (eGFR calculated using the ChronicKidney Disease Epidemiology Collaboration formula),aspartate transaminase (AST), and alanine trans-aminase (ALT) were measured at baseline, after6 months, and after 12 months of follow-up.
OUTCOMES. The primary outcome was change infemoral 18F-NaF PET activity. The femoral arterytarget-to-background ratio (TBRfemoral) as a measureof femoral 18F-NaF PET activity was determinedblinded for treatment status using previouslydescribed methods (Online Appendix) (24,30).
Change in arterial calcification on conventional CTscan was a secondary outcome. Calcifications in boththe left and right femoral arteries were quantifiedblinded for treatment status using the femoral artery
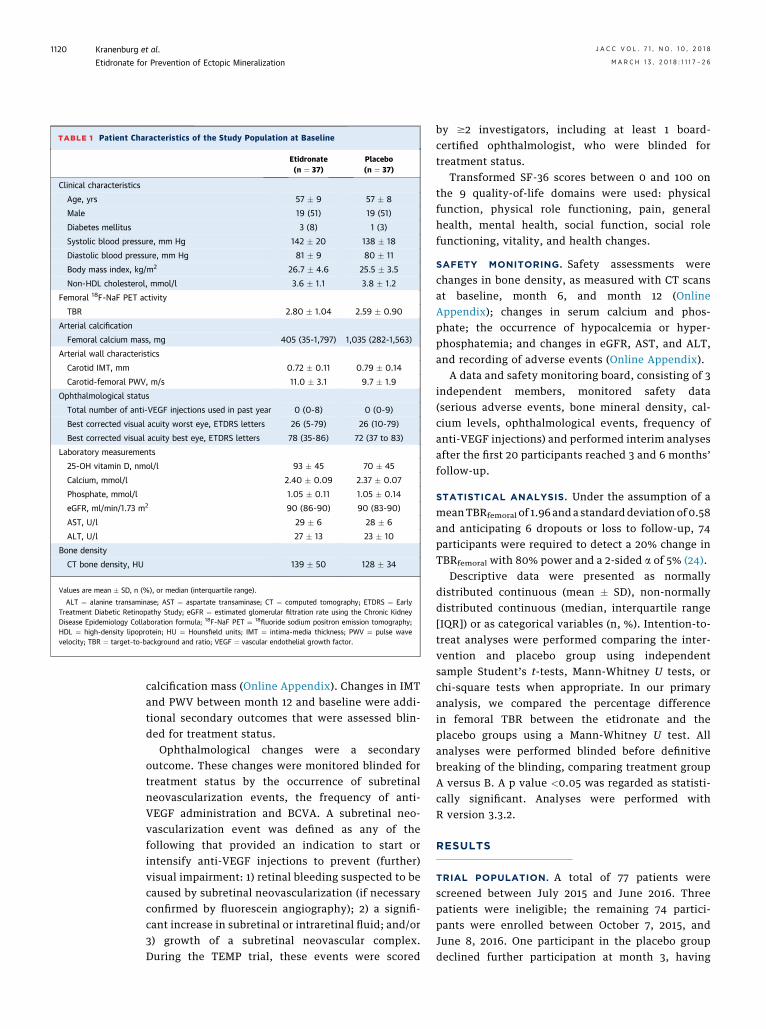
TABLE 1 Patient Characteristics of the Study Population at Baseline
Etidronate(n ¼ 37)
Placebo(n ¼ 37)
Clinical characteristics
Age, yrs 57 � 9 57 � 8
Male 19 (51) 19 (51)
Diabetes mellitus 3 (8) 1 (3)
Systolic blood pressure, mm Hg 142 � 20 138 � 18
Diastolic blood pressure, mm Hg 81 � 9 80 � 11
Body mass index, kg/m2 26.7 � 4.6 25.5 � 3.5
Non-HDL cholesterol, mmol/l 3.6 � 1.1 3.8 � 1.2
Femoral 18F-NaF PET activity
TBR 2.80 � 1.04 2.59 � 0.90
Arterial calcification
Femoral calcium mass, mg 405 (35-1,797) 1,035 (282-1,563)
Arterial wall characteristics
Carotid IMT, mm 0.72 � 0.11 0.79 � 0.14
Carotid-femoral PWV, m/s 11.0 � 3.1 9.7 � 1.9
Ophthalmological status
Total number of anti-VEGF injections used in past year 0 (0-8) 0 (0-9)
Best corrected visual acuity worst eye, ETDRS letters 26 (5-79) 26 (10-79)
Best corrected visual acuity best eye, ETDRS letters 78 (35-86) 72 (37 to 83)
Laboratory measurements
25-OH vitamin D, nmol/l 93 � 45 70 � 45
Calcium, mmol/l 2.40 � 0.09 2.37 � 0.07
Phosphate, mmol/l 1.05 � 0.11 1.05 � 0.14
eGFR, ml/min/1.73 m2 90 (86-90) 90 (83-90)
AST, U/l 29 � 6 28 � 6
ALT, U/l 27 � 13 23 � 10
Bone density
CT bone density, HU 139 � 50 128 � 34
Values are mean � SD, n (%), or median (interquartile range).
ALT ¼ alanine transaminase; AST ¼ aspartate transaminase; CT ¼ computed tomography; ETDRS ¼ EarlyTreatment Diabetic Retinopathy Study; eGFR ¼ estimated glomerular filtration rate using the Chronic KidneyDisease Epidemiology Collaboration formula; 18F-NaF PET ¼ 18
fluoride sodium positron emission tomography;HDL ¼ high-density lipoprotein; HU ¼ Hounsfield units; IMT ¼ intima-media thickness; PWV ¼ pulse wavevelocity; TBR ¼ target-to-background and ratio; VEGF ¼ vascular endothelial growth factor.
Kranenburg et al. J A C C V O L . 7 1 , N O . 1 0 , 2 0 1 8
Etidronate for Prevention of Ectopic Mineralization M A R C H 1 3 , 2 0 1 8 : 1 1 1 7 – 2 6
1120
calcification mass (Online Appendix). Changes in IMTand PWV between month 12 and baseline were addi-tional secondary outcomes that were assessed blin-ded for treatment status.
Ophthalmological changes were a secondaryoutcome. These changes were monitored blinded fortreatment status by the occurrence of subretinalneovascularization events, the frequency of anti-VEGF administration and BCVA. A subretinal neo-vascularization event was defined as any of thefollowing that provided an indication to start orintensify anti-VEGF injections to prevent (further)visual impairment: 1) retinal bleeding suspected to becaused by subretinal neovascularization (if necessaryconfirmed by fluorescein angiography); 2) a signifi-cant increase in subretinal or intraretinal fluid; and/or3) growth of a subretinal neovascular complex.During the TEMP trial, these events were scored
by $2 investigators, including at least 1 board-certified ophthalmologist, who were blinded fortreatment status.
Transformed SF-36 scores between 0 and 100 onthe 9 quality-of-life domains were used: physicalfunction, physical role functioning, pain, generalhealth, mental health, social function, social rolefunctioning, vitality, and health changes.
SAFETY MONITORING. Safety assessments werechanges in bone density, as measured with CT scansat baseline, month 6, and month 12 (OnlineAppendix); changes in serum calcium and phos-phate; the occurrence of hypocalcemia or hyper-phosphatemia; and changes in eGFR, AST, and ALT,and recording of adverse events (Online Appendix).
A data and safety monitoring board, consisting of 3independent members, monitored safety data(serious adverse events, bone mineral density, cal-cium levels, ophthalmological events, frequency ofanti-VEGF injections) and performed interim analysesafter the first 20 participants reached 3 and 6 months’follow-up.
STATISTICAL ANALYSIS. Under the assumption of ameanTBRfemoral of 1.96 and a standarddeviation of 0.58and anticipating 6 dropouts or loss to follow-up, 74participants were required to detect a 20% change inTBRfemoral with 80% power and a 2-sided a of 5% (24).
Descriptive data were presented as normallydistributed continuous (mean � SD), non-normallydistributed continuous (median, interquartile range[IQR]) or as categorical variables (n, %). Intention-to-treat analyses were performed comparing the inter-vention and placebo group using independentsample Student’s t-tests, Mann-Whitney U tests, orchi-square tests when appropriate. In our primaryanalysis, we compared the percentage differencein femoral TBR between the etidronate and theplacebo groups using a Mann-Whitney U test. Allanalyses were performed blinded before definitivebreaking of the blinding, comparing treatment groupA versus B. A p value <0.05 was regarded as statisti-cally significant. Analyses were performed withR version 3.3.2.
RESULTS
TRIAL POPULATION. A total of 77 patients werescreened between July 2015 and June 2016. Threepatients were ineligible; the remaining 74 partici-pants were enrolled between October 7, 2015, andJune 8, 2016. One participant in the placebo groupdeclined further participation at month 3, having

TABLE 2 Primary and Secondary Outcomes
Etidronate Placebo p Value
Femoral arterial wall 18F-NaF PET activity
Change in target-to-background ratio, % 6 (�12 to 25) 7 (�9 to 32) 0.465
CT arterial calcification
Change in femoral calcification mass(month 12 vs. baseline), %
�4 (�10 to 7) 8 (�1 to 20) 0.001
Arterial wall characteristics
Change in carotid IMT, mm 0.00 � 0.09 0.02 � 0.09 0.530
Change in carotid-femoral PWV, m/s 0.6 � 2.2 0.6 � 2.1 0.990
Ophthalmological status
Subretinal neovascularization events during follow-up 1 (2.7) 9 (24.3) 0.007
Change in frequency of VEGF inhibitors 0 (�2 to 0) 0 (�1 to 1) 0.137
Change in best corrected visual acuityworst eye, ETDRS letters
�1 � 5 �1 � 7 0.900
Change in best corrected visual acuitybest eye, ETDRS letters
�2 � 4 �3 � 7 0.460
Values are median (interquartile range), mean � SD, or n (%). Treatment groups were compared using inde-pendent sample Student’s t-tests and Mann-Whitney U tests when appropriate. Change is displayed as % forfemoral arterial wall 18F-NaF PET activity and femoral calcium mass.
Abbreviations as in Table 1.
J A C C V O L . 7 1 , N O . 1 0 , 2 0 1 8 Kranenburg et al.M A R C H 1 3 , 2 0 1 8 : 1 1 1 7 – 2 6 Etidronate for Prevention of Ectopic Mineralization
1121
experienced severe uveitis following an anti-VEGFinjection. One participant in the etidronate groupdiscontinued treatment because of a hypersensitivityskin reaction at month 6 but remained in the study(Figure 1). Baseline characteristics are presented inTable 1. The mean age in both groups was 57 years;both groups were 51% male.
EFFICACY. The TBRfemoral increased with 6%(IQR: �12% to 25%) in the etidronate group and with7% (IQR: �9% to 32%) in the placebo group in the12 months of follow-up (p ¼ 0.465) (Table 2, Figure 2).During the 12 months of follow-up, arterial calcifica-tion decreased 4% (IQR: �11% to 7%) in the etidronategroup and increased 8% (IQR: �1% to 20%) in theplacebo group (p ¼ 0.001) (Figure 2).
Carotid IMT increased 0.00 � 0.09 mm in the eti-dronate group and 0.02 � 0.09 mm in the placebogroup (p ¼ 0.523). The PWV increased with 0.6 �2.2 m/s in the etidronate group and 0.6 � 2.1 m/s inthe placebo group (p ¼ 0.990).
During follow-up, 1 patient (2.7%) in the etidronategroup had a subretinal neovascularization eventcompared with 9 patients (24.3%) in the placebogroup (p ¼ 0.007). The median number of anti-VEGFinjections administered per year did not change inthe etidronate group (0; IQR: �2 to 0) or in theplacebo group (0; IQR: �1 to 1) (p ¼ 0.137). The BCVAin LogMAR number of letters of the worse eyedecreased with 1 � 5 letters in the etidronate groupand with 1 � 7 letters in the placebo group (p ¼ 0.900).The BCVA of the best eye decreased with 2 � 4 lettersin the etidronate group and with 3 � 7 letters in theplacebo group (p ¼ 0.460).
No significant differences between the etidronateand placebo group were found in quality of life do-mains of the SF-36 questionnaire (Online Table 1).
SAFETY. From baseline to 12 months of follow-up,the bone mineral density changed with �4 � 12%(�7 � 16 HU) in the etidronate group comparedwith �6 � 9% (�9 � 16 HU) in the placebo group(p ¼ 0.374) (Table 3).
No significant differences were found between theetidronate and placebo group when comparing base-line with values after 12 months of follow-up of cal-cium, phosphate, eGFR, AST, and ALT (Table 3). Duringfollow-up, hypocalcemia (calcium <2.20 mmol/l)occurred in 3 patients (8.1%) in the etidronate groupand in 1 (2.7%) in the placebo group (p ¼ 0.304).Hyperphosphatemia (phosphate >1.5 mmol/l)occurred in 18 patients (48.6%) in the etidronate groupcomparedwith 0 (0%) in the placebo group (p<0.001).All cases were monitored and recovered without anymedical intervention.
Gastrointestinal complaints (reflux, stomach pain,diarrhea) presented in 2 patients (5.4%) in the eti-dronate and 2 patients (5.4%) in the placebo group(p ¼ 1.000). A hypersensitivity dermatological reac-tion occurred in 1 patient (2.7%) in the etidronategroup compared with 0 (0%) in the placebo group(p ¼ 0.304).
DISCUSSION
The TEMP trial, a randomized double-blind, placebo-controlled trial including 74 PXE participants,showed that etidronate did not lower femoral arterialwall 18F-NaF PET activity compared with placebo af-ter 12 months of follow-up (Central Illustration);however, etidronate significantly decreased ectopicmineralization as quantified by arterial calcificationcompared to placebo. Also, etidronate treatment inPXE was associated with significantly lower rates ofsubretinal neovascularization events (1 vs. 9 pa-tients). There were no important safety issues of eti-dronate treatment during the year of follow-up.Although in these dosages etidronate is known toincrease the risk of bone-related adverse events andhypocalcemia, no significant differences wereobserved between the etidronate and placebo group.Eighteen patients in the etidronate group comparedwith 0 in the placebo group experienced hyper-phosphatemia (>1.5 mmol/l), but all patients recov-ered without any medical intervention.
The body has several inhibiting pathwaysfor ectopic mineralization including vitaminK–dependent pathways, the Klotho protein, Fetuin-A,
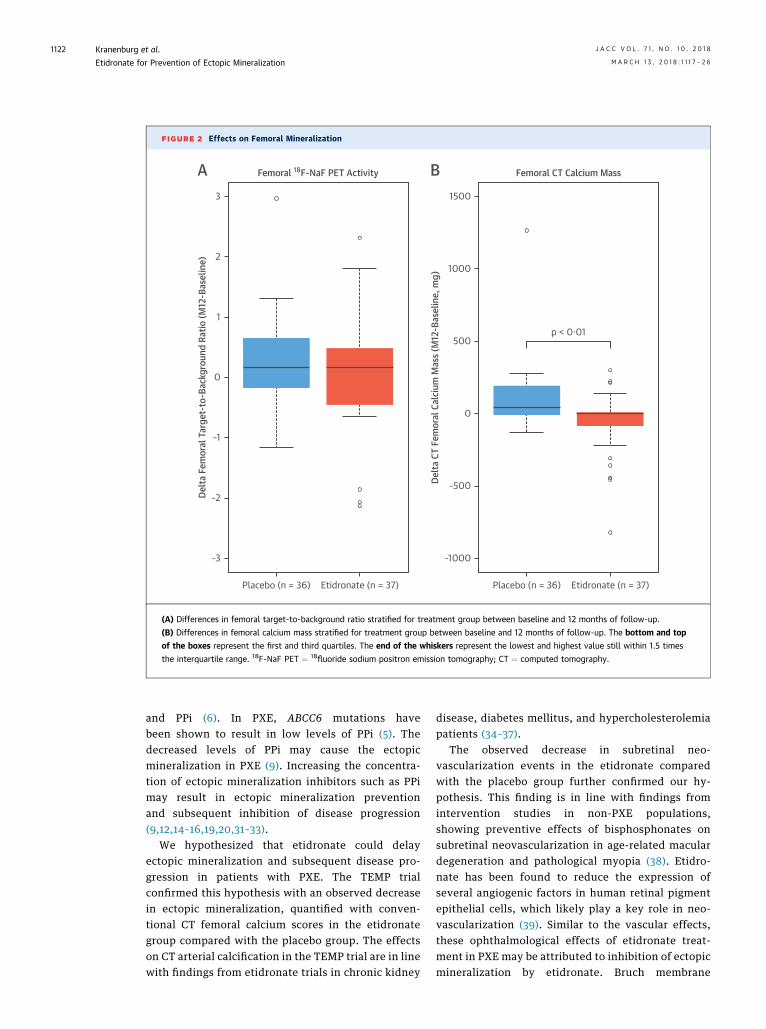
FIGURE 2 Effects on Femoral Mineralization
Placebo (n = 36)
–3
–2
–1
Delta
Fem
oral
Tar
get-
to-B
ackg
roun
d Ra
tio (M
12-B
asel
ine)
Femoral 18F-NaF PET Activity
0
1
2
A B3
Etidronate (n = 37) Placebo (n = 36)
–1000
–500
0
p < 0·01
Delta
CT
Fem
oral
Cal
cium
Mas
s (M
12-B
asel
ine,
mg)
Femoral CT Calcium Mass
500
1000
1500
Etidronate (n = 37)
(A) Differences in femoral target-to-background ratio stratified for treatment group between baseline and 12 months of follow-up.
(B) Differences in femoral calcium mass stratified for treatment group between baseline and 12 months of follow-up. The bottom and top
of the boxes represent the first and third quartiles. The end of the whiskers represent the lowest and highest value still within 1.5 times
the interquartile range. 18F-NaF PET ¼ 18fluoride sodium positron emission tomography; CT ¼ computed tomography.
Kranenburg et al. J A C C V O L . 7 1 , N O . 1 0 , 2 0 1 8
Etidronate for Prevention of Ectopic Mineralization M A R C H 1 3 , 2 0 1 8 : 1 1 1 7 – 2 6
1122
and PPi (6). In PXE, ABCC6 mutations havebeen shown to result in low levels of PPi (5). Thedecreased levels of PPi may cause the ectopicmineralization in PXE (9). Increasing the concentra-tion of ectopic mineralization inhibitors such as PPimay result in ectopic mineralization preventionand subsequent inhibition of disease progression(9,12,14–16,19,20,31–33).
We hypothesized that etidronate could delayectopic mineralization and subsequent disease pro-gression in patients with PXE. The TEMP trialconfirmed this hypothesis with an observed decreasein ectopic mineralization, quantified with conven-tional CT femoral calcium scores in the etidronategroup compared with the placebo group. The effectson CT arterial calcification in the TEMP trial are in linewith findings from etidronate trials in chronic kidney
disease, diabetes mellitus, and hypercholesterolemiapatients (34–37).
The observed decrease in subretinal neo-vascularization events in the etidronate comparedwith the placebo group further confirmed our hy-pothesis. This finding is in line with findings fromintervention studies in non-PXE populations,showing preventive effects of bisphosphonates onsubretinal neovascularization in age-related maculardegeneration and pathological myopia (38). Etidro-nate has been found to reduce the expression ofseveral angiogenic factors in human retinal pigmentepithelial cells, which likely play a key role in neo-vascularization (39). Similar to the vascular effects,these ophthalmological effects of etidronate treat-ment in PXE may be attributed to inhibition of ectopicmineralization by etidronate. Bruch membrane

TABLE 3 Safety Measurements and Adverse Events
Etidronate Placebo p Value
Bone mineral density
%D CT bone density, HU �4 � 12 �6 � 9 0.374
Laboratory measurements*
Hypocalcemia (calcium <2.20 mmol/l) 3 (8.1) 1 (2.7) 0.304
Hyperphosphatemia (phosphate >1.5 mmol/l)† 18 (48.6) 0 (0.0) <0.001
Renal impairment (eGFR �20%) 0 (0.0) 0 (0.0) 1.000
Liver impairment (AST/ALT þ50%)† 1 (2.7) 0 (0.0) 0.304
D Calcium, mmol/l �0.03 � 0.08 �0.01 � 0.07 0.438
D Phosphate, mmol/l �0.01 � 0.14 �0.03 � 0.14 0.707
D eGFR, ml/min/1.73 m2 0 (0 to 0) 0 (�1 to 0) 0.864
D AST, U/l 0 � 5 0 � 4 0.841
D ALT, U/l �1 � 9 2 � 8 0.147
Adverse events
Gastrointestinal complaints 2 (5.4) 2 (5.4) 1.000
Hypersensitivity dermatological reaction‡ 1 (2.7) 0 (0.0) 0.304
Posterior vitreous detachment 1 (2.7) 0 (0.0) 0.304
Suspected uveitis after anti-VEGF injection 0 (0.0) 1 (2.7) 0.304
Blurry sight after anti-VEGF injection,disappearing within a day
0 (0.0) 1 (2.7) 0.304
Drop in visual acuity not relatedto neovascularization
0 (0.0) 1 (2.7) 0.304
Hospital admission§ 0 (0.0) 1 (2.7) 0.304
Values are mean � SD, n (%), or median (interquartile range). Treatment groups were compared using inde-pendent sample Student’s t-tests, chi-square tests, and Mann-Whitney U tests when appropriate. *Calcium andphosphate were measured at baseline and after 3, 6, 9, and 12 months of follow-up. Renal function and liverfunction were measured at baseline and after 6 and 12 months of follow-up. †All cases were followed andrecovered without any medical intervention. ‡Skin rash arising during second treatment period, after which thestudy medication was discontinued and the rash disappeared. Restart of study medication again resulted in rash,after which this participant continued the study off study medication. §Hospital admission because of (planned)hip operation.
D Delta ¼ month 12 minus baseline value; other abbreviations as in Table 1.
J A C C V O L . 7 1 , N O . 1 0 , 2 0 1 8 Kranenburg et al.M A R C H 1 3 , 2 0 1 8 : 1 1 1 7 – 2 6 Etidronate for Prevention of Ectopic Mineralization
1123
mineralization in PXE may impede the transport ofoxygen and waste products across Bruch membrane.Inhibition of this mineralization might thus preventthe growth or recurrence of activity of a choroidalneovascularization (3).
We assumed that 18F-NaF PET activity wouldvisualize the active calcification process and thuswould be sensitive to small changes in arterial calci-fication, providing an efficient marker of ectopicmineralization in the TEMP trial (22). The TEMP trialis the first interventional trial that reports on femoral18F-NaF PET activity as an outcome. The absence ofan effect of etidronate treatment on femoral arterialwall 18F-NaF PET activity is remarkably discrepantwith the observed effects of etidronate on CT arterialcalcification and subretinal neovascularizationevents. This discrepancy questions our assumptionon the value of femoral 18F-NaF PET activity as anintermediate outcome in such an interventional trial.Although femoral 18F-NaF PET activity relates tocardiovascular risk scores (24), regional 18F-NaF PETactivity and regional conventional CT arterial calcifi-cation scores are not correlated, suggesting that thebiological processes measured with 18F-NaF PETscans are not exactly known (40,41). Recent evidenceshows that arterial wall 18F-NaF PET activity coloc-alize closely and preferentially bind to pathologicalmineralization, but also that the increased surfacearea of microcalcifications relative to macro-calcifications resulted in increased tracer uptake and,therefore, does not necessarily represent activecalcification (41). Our assumptions on the 18F-NaFPET measurements as a reflection of disease activityproved to be incorrect as a result. Another explana-tion for the discrepancy between effects of etidronateon 18F-NaF activity and CT arterial calcification scoremay be that etidronate treatment increases dissolu-tion of existing mineral deposits while not loweringnew calcium deposition; however, this remainsspeculative and potential biological mechanisms areunknown. Taking the effects of etidronate treatmenton conventional CT arterial calcification into account,even in the absence of an effect on the primaryoutcome, the TEMP trial showed that etidronatetreatment can delay ectopic mineralization in PXE.
Based upon our findings, all patients with PXEshould be considered for etidronate treatment. Pref-erably, all patients with PXE treated with etidronateshould be carefully monitored in a research settingfor long-term efficacy and safety. Being one of theoldest bisphosphonates, etidronate has been on themarket for almost 40 years and is easily available atlow cost. Given the large effect on quality of life ofophthalmological and vascular involvement in PXE,
etidronate treatment may eventually enhance qualityof life in patients with PXE (42). Other potentialtreatment strategies considered in patients with PXEshould be weighed against the efficacy and safetyprofile of etidronate.
The TEMP trial provides proof of the concept thatbisphosphonates can reduce arterial calcificationsand may reduce subsequent vascular risk. Pop-ulations other than patients with PXE may benefitfrom this potential of bisphosphonates. Medial arte-rial calcification is a prevalent process occurring inrenal failure, diabetes mellitus, and aging, which re-lates to an increased vascular risk (43,44). In-vestigations on the effects of bisphosphonates inthese populations, associated with a high residualvascular risk, seem warranted.
STUDY STRENGTHS AND LIMITATIONS. The TEMP trial isthe first randomized placebo-controlled trial thatinvestigates the efficacy and safety of bisphospho-nates in patients with PXE. Strengths of the TEMP trialinclude the relatively large number of patients withPXE and its success to achieve a low dropout rate.Limitations include the limited treatment and

CENTRAL ILLUSTRATION PXE: Treatment of Ectopic Mineralization
Kranenburg, G. et al. J Am Coll Cardiol. 2018;71(10):1117–26.
PXE is characterized by ectopic mineralization of elastic fibers in the skin, the Bruch membrane beneath the retina, and the medial layer of arteries. PXE is caused by a
biallelic mutation in the ABCC6 genes, causing reduced levels of inorganic pyrophosphate and ectopic mineralization. Clinical manifestations are present in the skin,
eyes, and vascular system. In the TEMP trial, 74 adult patients with PXE with leg arterial calcifications were randomly assigned to etidronate or placebo (cyclical
20 mg/kg for 2 weeks every 12 weeks) during 1 year. 18F-NaF PET ¼ 18fluoride sodium positron emission tomography; CT ¼ computed tomography;
Events ¼ subretinal neovascularization events; PXE ¼ pseudoxanthoma elasticum; TEMP ¼ Treatment of Ectopic Mineralization in Pseudoxanthoma Elasticum.
Kranenburg et al. J A C C V O L . 7 1 , N O . 1 0 , 2 0 1 8
Etidronate for Prevention of Ectopic Mineralization M A R C H 1 3 , 2 0 1 8 : 1 1 1 7 – 2 6
1124

PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE: Compared with
placebo, etidronate can prevent progression of arterial
calcification and subretinal neovascularization in patients with
PXE without significant adverse effects.
TRANSLATIONAL OUTLOOK: Further research is needed to
assess the long-term efficacy and safety of etidronate in patients
with PXE and to evaluate the potential therapeutic utility of
bisphosphonates on arterial calcification and vascular risk in
patients with diabetes mellitus and renal failure.
J A C C V O L . 7 1 , N O . 1 0 , 2 0 1 8 Kranenburg et al.M A R C H 1 3 , 2 0 1 8 : 1 1 1 7 – 2 6 Etidronate for Prevention of Ectopic Mineralization
1125
follow-up period. With this limited follow-up time, wewere unable to show effects of etidronate treatment onother outcomes besides CT arterial calcification andsubretinal neovascularization events. Also, no safetyinformation for etidronate treatment in patients withPXE for$1 year is available. The lack of generalizabilityto patients with PXE not eligible for the TEMP trial,such as patients without leg arterial calcification orwith osteomalacia, is another limitation.
CONCLUSIONS
In patients with PXE, etidronate treatment did notchange femoral arterial wall 18F-NaF PET activitycompared with placebo after 12 months of follow-up;however, etidronate significantly reduced arterialcalcification and the number of subretinal neo-vascularization events compared to placebo. Noimportant safety issues of etidronate treatmentoccurred during the year of follow-up. Furtherresearch in the long-term effects and safety of eti-dronate seems warranted.
ACKNOWLEDGMENTS The authors gratefullyacknowledge the contribution of all participantsand the contributions of C.A.M. Joosten, I.P. Klaassen,E.T. Koene, and I. Janse-Seip (research nurses);A. Lalmohamed, PhD (pharmacist); G. Berkelmans,MD,
and C. Koopal, MD, PhD (subinvestigators); J.Westerink, MD, PhD (independent study physician);M.J.C Eijkemans, MD, PhD; G.K. Hovingh, MD, PhD;and R.O. Schlingemann, MD, PhD (members of thedata and safety monitoring board).
ADDRESS FOR CORRESPONDENCE: Dr. WilkoSpiering, Department of Vascular Medicine,University Medical Center Utrecht, PO Box85500, 3508 GA Utrecht, the Netherlands. E-mail:[email protected].
RE F E RENCE S
1. Plomp AS, Toonstra J, Bergen AA, van Dijk MR,de Jong PT. Proposal for updating the pseudox-anthoma elasticum classification system and areview of the clinical findings. Am J Med GenetPart A 2010;152a:1049–58.
2. Uitto J, Varadi A, Bercovitch L, Terry PF,Terry SF. Pseudoxanthoma elasticum: progress inresearch toward treatment: summary of the 2012PXE international research meeting. J Invest Der-matol 2013;133:1444–9.
3. Mimoun G, Ebran JM, Grenet T, Donati A,Cohen SY, Ponthieux A. Ranibizumab for choroidalneovascularization secondary to pseudoxanthomaelasticum: 4-year results from the PIXEL study inFrance. Graefe’s archive for clinical and experi-mental ophthalmology ¼ Albrecht von GraefesArch Clin Exp Ophthalmol 2017;225:1651–60.
4. Bergen AA, Plomp AS, Schuurman EJ, et al.Mutations in ABCC6 cause pseudoxanthoma elas-ticum. Nat Genet 2000;25:228–31.
5. Jansen RS, Kucukosmanoglu A, de Haas M, et al.ABCC6 prevents ectopic mineralization seen inpseudoxanthoma elasticum by inducing cellularnucleotide release. Proc Natl Acad Sci U St A 2013;110:20206–11.
6. Evrard S, Delanaye P, Kamel S, Cristol JP,Cavalier E. Vascular calcification: from patho-physiology to biomarkers. Clin Chim Acta 2015;438:401–14.
7. Fleisch H, Schibler D, Maerki J, Frossard I. In-hibition of aortic calcification by means of pyro-phosphate and polyphosphates. Nature 1965;207:1300–1.
8. Lomashvili KA, Narisawa S, Millan JL,O’Neill WC. Vascular calcification is dependent onplasma levels of pyrophosphate. Kidney Int 2014;85:1351–6.
9. Jansen RS, Duijst S, Mahakena S, et al. ABCC6-mediated ATP secretion by the liver is the mainsource of the mineralization inhibitor inorganic py-rophosphate in the systemic circulation-brief report.Arterioscler Thromb Vasc Biol 2014;34:1985–9.
10. Elmariah S, Delaney JA, O’Brien KD, et al.Bisphosphonate use and prevalence of valvularand vascular calcification in women MESA (TheMulti-Ethnic Study of Atherosclerosis). J Am CollCardiol 2010;56:1752–9.
11. Schenk R, Merz WA, Muhlbauer R, Russell RG,Fleisch H. Effect of ethane-1-hydroxy-1,1-diphosphonate (EHDP) and dichloromethylenediphosphonate (Cl 2 MDP) on the calcification andresorption of cartilage and bone in the tibialepiphysis and metaphysis of rats. Calcif Tissue Res1973;11:196–214.
12. Oliveira JR, Oliveira MF. Primary brain calcifi-cation in patients undergoing treatment with thebiphosphanate alendronate. Scie Rep 2016;6:22961.
13. Drake MT, Clarke BL, Khosla S. Bisphospho-nates: mechanism of action and role in clinicalpractice. Mayo Clin Proc 2008;83:1032–45.
14. Loeb JA. Functional improvement in a patientwith cerebral calcinosis using a bisphosphonate.Mov Disord 1998;13:345–9.
15. Edouard T, Chabot G, Miro J, et al. Efficacy andsafety of 2-year etidronate treatment in a childwith generalized arterial calcification of infancy.Eu J Pediatr 2011;170:1585–90.
16. Rutsch F, Boyer P, Nitschke Y, et al. Hypo-phosphatemia, hyperphosphaturia, and bisphosph-onate treatment are associated with survival beyondinfancy in generalized arterial calcificationof infancy.Circ Cardiovasc Genet 2008;1:133–40.
17. Nitschke Y, Baujat G, Botschen U, et al.Generalized arterial calcification of infancy andpseudoxanthoma elasticum can be caused bymutations in either ENPP1 or ABCC6. Am J HumGenet 2012;90:25–39.
18. Li Q, Brodsky JL, Conlin LK, et al. Mutations inthe ABCC6 gene as a cause of generalized arterialcalcification of infancy: genotypic overlap withpseudoxanthoma elasticum. J Invest Dermatol2014;134:658–65.
19. Li Q, Sundberg JP, Levine MA, Terry SF,Uitto J. The effects of bisphosphonates on ectopicsoft tissue mineralization caused by mutations inthe ABCC6 gene. Cell Cycle 2015;14:1082–90.

Kranenburg et al. J A C C V O L . 7 1 , N O . 1 0 , 2 0 1 8
Etidronate for Prevention of Ectopic Mineralization M A R C H 1 3 , 2 0 1 8 : 1 1 1 7 – 2 6
1126
20. LiQ,KingmanJ,Sundberg JP, LevineMA,Uitto J.Etidronate prevents, but does not reverse, ectopicmineralization in amousemodel of pseudoxanthomaelasticum (Abcc6-/-). Oncotarget 2016.
21. Oudkerk SF, de Jong PA, Blomberg BA,Scholtens AM, Mali WP, Spiering W. Whole-bodyvisualization of ectopic bone formation of arteriesand skin in pseudoxanthoma elasticum. J Am CollCardiol Img 2016;9:755–6.
22. Joshi NV, Vesey AT, Williams MC, et al. 18F-fluoride positron emission tomography for identi-fication of ruptured and high-risk coronaryatherosclerotic plaques: a prospective clinical trial.Lancet 2014;383:705–13.
23. Agatston AS, Janowitz WR, Hildner FJ,Zusmer NR, Viamonte M Jr., Detrano R. Quantifi-cation of coronary artery calcium using ultrafastcomputed tomography. J Am Coll Cardiol 1990;15:827–32.
24. Janssen T, Bannas P, Herrmann J, et al. Asso-ciation of linear (1)(8)F-sodium fluoride accumula-tion in femoral arteries as a measure of diffusecalcification with cardiovascular risk factors: a PET/CT study. J Nucl Cardiol 2013;20:569–77.
25. Guzman RJ, Brinkley DM, Schumacher PM,Donahue RM, Beavers H, Qin X. Tibial arterycalcification as a marker of amputation risk in pa-tients with peripheral arterial disease. J Am CollCardiol 2008;51:1967–74.
26. Dweck MR, Chow MW, Joshi NV, et al. Coro-nary arterial 18F-sodium fluoride uptake: a novelmarker of plaque biology. J Am Coll Cardiol 2012;59:1539–48.
27. Boellaard R, Delgado-Bolton R, Oyen WJ, et al.FDG PET/CT: EANM procedure guidelines fortumour imaging: version 2.0. Eur J Nucl MedicineMolec Imaging 2015;42:328–54.
28. Ferris FL 3rd, Kassoff A, Bresnick GH, Bailey I.New visual acuity charts for clinical research. Am JOphthalmol 1982;94:91–6.
29. Aaronson NK, Muller M, Cohen PDA, et al.Translation, validation, and norming of the Dutch
language version of the SF-36 Health Survey inCommunity and Chronic Disease Populations.J Clin Epidemiol 1998;51:1055–68.
30. Rudd JH, Myers KS, Bansilal S, et al. Athero-sclerosis inflammation imaging with 18F-FDG PET:carotid, iliac, and femoral uptake reproducibility,quantification methods, and recommendations.J Nucl Med 2008;49:871–8.
31. Kranenburg G, Bartstra JW, Weijmans M, et al.Bisphosphonates for cardiovascular risk reduction:A systematic review and meta-analysis. Athero-sclerosis 2016;252:106–15.
32. Villa-Bellosta R, Rivera-Torres J, Osorio FG,et al. Defective extracellular pyrophosphatemetabolism promotes vascular calcification in amouse model of Hutchinson-Gilford progeriasyndrome that is ameliorated on pyrophosphatetreatment. Circulation 2013;127:2442–51.
33. Schurgers LJ, Spronk HM, Soute BA,Schiffers PM, DeMey JG, Vermeer C. Regression ofwarfarin-induced medial elastocalcinosis by highintake of vitamin K in rats. Blood 2007;109:2823–31.
34. Hashiba H, Aizawa S, Tamura K, Kogo H. In-hibition of the progression of aortic calcificationby etidronate treatment in hemodialysis patients:long-term effects. Ther Apher Dial 2006;10:59–64.
35. Ariyoshi T, Eishi K, Sakamoto I, Matsukuma S,Odate T. Effect of etidronic acid on arterial calci-fication in dialysis patients. Clin Drug Invest 2006;26:215–22.
36. Koshiyama H, Nakamura Y, Tanaka S,Minamikawa J. Decrease in carotid intima-mediathickness after 1-year therapy with etidronate forosteopenia associated with type 2 diabetes. J ClinEndocrinol Metab 2000;85:2793–6.
37. Kawahara T, Nishikawa M, Kawahara C,Inazu T, Sakai K, Suzuki G. Atorvastatin,etidronate, or both in patients at high risk foratherosclerotic aortic plaques: a randomized,controlled trial. Circulation 2013;127:2327–35.
38. Miki A, Honda S, Nagai T, Tsukahara Y, Negi A.Effects of oral bisphosphonates on myopicchoroidal neovascularisation over 2 years offollow-up: comparison with anti-VEGF therapyand photodynamic therapy. A pilot study. Br JOphthalmol 2013;97:770–4.
39. Or C, Cui J, Matsubara J, Forooghian F. Pro-inflammatory and anti-angiogenic effects ofbisphosphonates on human cultured retinalpigment epithelial cells. Br J Ophthalmol 2013;97:1074–8.
40. Morbelli S, Fiz F, Piccardo A, et al. Divergentdeterminants of 18F-NaF uptake and visible cal-cium deposition in large arteries: relationship withFramingham risk score. Int J CardiovascI Imaging2014;30:439–47.
41. Irkle A, Vesey AT, Lewis DY, et al. Identifyingactive vascular microcalcification by (18)F-sodiumfluoride positron emission tomography. Nat Com-mun 2015;6:7495.
42. Finger RP, Fenwick E, Marella M, et al. Therelative impact of vision impairment and cardio-vascular disease on quality of life: the example ofpseudoxanthoma elasticum. Health Qual LifeOutcomes 2011;9:113.
43. Lanzer P, Boehm M, Sorribas V, et al. Medialvascular calcification revisited: review and per-spectives. Eur Heart J 2014;35:1515–25.
44. Rennenberg RJ, Kessels AG, Schurgers LJ, vanEngelshoven JM, de Leeuw PW, Kroon AA.Vascular calcifications as a marker of increasedcardiovascular risk: a meta-analysis. Vasc HealthRisk Manage 2009;5:185–97.
KEY WORDS arterial calcification,bisphosphonates, etidronate, PXE
APPENDIX For an expanded Methods sectionas well as a supplemental table, please see theonline version of this paper.