evaluation of the incidental solitary liver...
TRANSCRIPT

1
Lewis R. Roberts, PhD, FAASLD
Evaluation of the Incidental
Solitary Liver Lesion
Postgraduate Course:
Challenges in Management of Common Liver Diseases
347

© 2016 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES
WWW.AASLD.ORG 2
Questions for Reviewers:
1. Is it ok to leave out simple cyst
and abscess slides – 23,24,25?
2. Are LIRADS slides needed –
30,31?
3. Any other suggested changes?
348

A 39 year old female with a 2 cm solitary lesion
on ultrasound and normal liver chemistries
Key Questions/Content Focus:
• Present an algorithm for investigation of
incidental solitary solid liver lesions.
• How does one differentiate a benign from a
malignant lesion?
• Do adenomas and focal nodular hyperplasia
need to be followed and if so, how? © 2016 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES
WWW.AASLD.ORG 3
Case
349

© 2016 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES
WWW.AASLD.ORG 4
Objectives
• Clinical classification of liver masses
• Evaluation of liver mass lesions
• Common benign mass lesions • Clinical features • Imaging characteristics • Optimal management
• Common malignant mass lesions • Hepatocellular Carcinoma • Cholangiocarcinoma • Metastases from other Primary Sites
350

© 2016 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES
WWW.AASLD.ORG 5
Three Categories of Liver Masses
1. Benign lesions usually requiring no further intervention
2. Benign lesions requiring further investigation and therapy
3. Malignant lesions requiring appropriate management
351

© 2016 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES
WWW.AASLD.ORG 6
1. Benign lesions usually requiring no further intervention
• Cavernous hemangioma
• Focal nodular hyperplasia
• Simple cyst
• Focal fatty change or sparing
352

© 2016 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES
WWW.AASLD.ORG 7
2. Benign lesions requiring further
investigation and therapy
• Hepatic adenoma and adenomatosis
• Biliary cystadenoma
• Hepatic abscess – pyogenic or amebic
• Echinococcal cyst
• Granulomatous inflammation
• Inflammatory pseudotumor
353

© 2016 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES
WWW.AASLD.ORG 8
3. Malignant lesions requiring appropriate
management
• Metastases from other primary sites
• Hepatocellular carcinoma
• Cholangiocarcinoma
• Biliary cystadenocarcinoma
• Lymphoma
• Hepatic angiosarcoma
354
© 2016 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES
WWW.AASLD.ORG 9
Clinical Approach to Liver Mass Lesions
• Symptoms
• Physical examination
• Laboratory studies
• Imaging characteristics: Ultrasound, CT,
MRI (especially with newer hepatobiliary
contrast agents)
• Need for biopsy
• Optimal management 355

© 2016 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES
WWW.AASLD.ORG 10
356

Phasic Vascular Perfusion of the Liver
357

Cavernous Hemangioma: Histology
Large hemangiomas
may have areas of
thrombosis, scarring,
and calcification
Network of vascular spaces separated by thin, fibrous stroma
358
Cavernous Hemangioma
359

Pre-contrast
Arterial phase
Venous phase
Peripheral nodular arterial phase enhancement,
with fill-in to the center in the venous phase
45 y o F with a Liver Mass
360
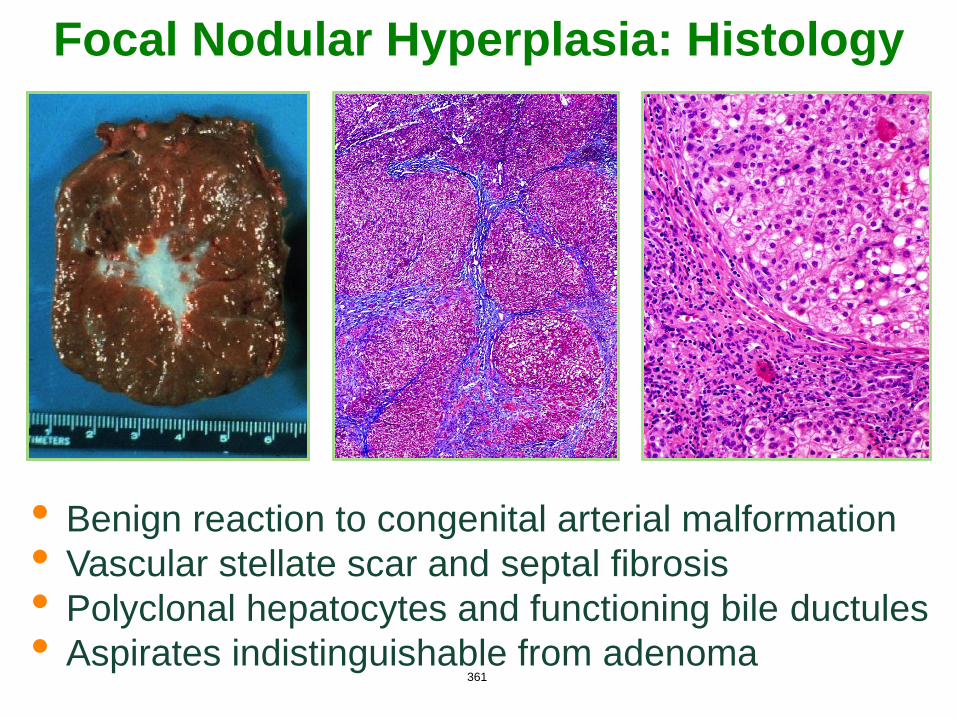
Focal Nodular Hyperplasia: Histology
• Benign reaction to congenital arterial malformation
• Vascular stellate scar and septal fibrosis
• Polyclonal hepatocytes and functioning bile ductules
• Aspirates indistinguishable from adenoma 361

MRI of Focal Nodular Hyperplasia
362

Sodium Gadoxetate MRI for
Distinguishing FNH from Adenoma
• Brightly enhancing in arterial phase
• Homogeneous enhancement with central scar
• Isointense in portal venous phase
• Retained intensity in the hepatobiliary phase supports the diagnosis of FNH
Arterial Portal Venous Hepatobiliary
363

Histopathology of Adenoma
Monoclonal hepatocytes
Prominent “naked” arteries
No normal portal tracts or bile ducts
Adenoma
364

β-catenin Exon 3 Mutated Adenomas
have Higher Risk of Malignancy
Normal Membrane
Staining
Positive Nuclear
Staining 365
MRI of Hepatic Adenoma
366

Gadobenate Dimeglumine MRI for
Distinguishing FNH from Adenoma
• Heterogeneous arterially enhancing mass • Isointense in portal venous phase • Decreased intensity in the hepatobiliary
phase suggests HNF1A mutated adenoma • Inflammatory and β-catenin mutated
adenomas may retain contrast
Arterial Portal Venous Hepatobiliary
367

Management of Hepatic Adenomas
• Follow up 6 mo, q 1 yr x 5 yrs, then q 2 yrs
• High Risk: Resect
• Lesions ≥ 5 cm (or increasing size)
• Hemorrhage
• Male Gender (increased malignant risk)
• β-Catenin mutated adenomas
• Older females with no history of OCP use
• Low Risk: Stop OCPs, lose weight
• Young Females, lesions < 5 cm on OCP
• Follow w US q 6-12 weeks during pregnancy
• Alternatives to Resection: RFA, embolization 368

Imaging Characteristics of Liver Cysts
Ultrasound
• Best test
• No internal echoes
• No flow on color flow
or duplex Doppler
• Through transmission
• Well-defined posterior
walls
• May have thin
echogenic septa 369

Symptomatic Cyst in a 72 y o F with Painless Jaundice and Leg Edema
Presentation
1 year after cyst aspiration
& EtOH sclerosis 2 years later
370

Pyogenic Liver Abscess
• Rupture or leak of
bile duct or bowel
• Biliary stenting,
instrumentation, or
chemoembolization
• Increased risk in
diabetes mellitus
• Biliary: enteric gram
-ves & enterococci
• Other sites: mixed
aerobic & anaerobic
41 yo F with new diagnosis of type 1 diabetes mellitus with ketoacidosis and liver mass
371

Imaging Characteristics of Focal Fat:
65 y o Woman Referred for Presumed
Gallbladder Adenocarcinoma
Ultrasound Hyperechoic
T1 Weighted In & Out of Phase
3 Month Follow-Up
372

© 2016 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES
WWW.AASLD.ORG 27
• Epidemiology:
• Fatty liver is increasingly common
• Focal fatty infiltration looks like a mass
• Also focal sparing in diffuse fatty infiltration
• Associations:
• Obesity
• Diabetes mellitus
• High alcohol consumption
• Altered metabolism due to chemotherapy
Focal Fat or Fat Sparing
373

Hepatocellular Carcinoma
374

Non-Invasive Diagnosis: Arterial Enhancement, Venous Washout, Capsule and Threshold Growth
Arterial
Portal
Late venous phase 375
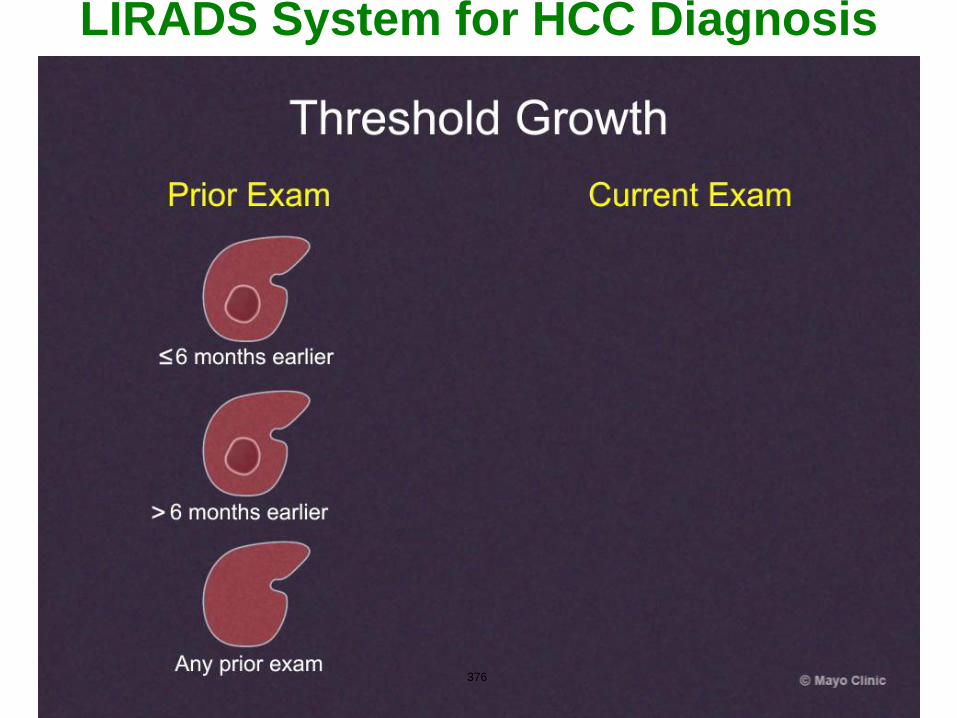
LIRADS System for HCC Diagnosis
Threshold Growth
376
© 2016 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES
WWW.AASLD.ORG 31
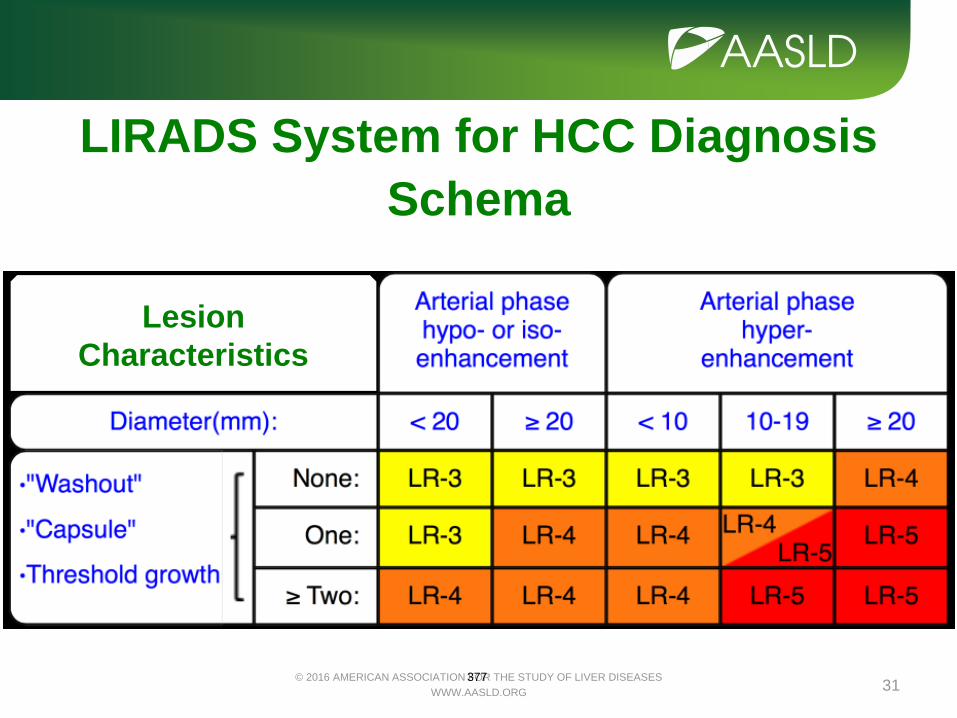
Lesion
Characteristics
LIRADS System for HCC Diagnosis
Schema
377

20 year old F with Long History of Vague Symptoms and Large Liver Mass
Fibrolamellar Subtype of HCC
Arterial phase Portal phase
• Young females
• Lymph node metastases
• Aggressive surgery recommended
• DNAJB1-PRKACA Chimeric Transcripts 378

Intrahepatic CCA
Perihilar CCA
Distal CCA
Image Courtesy of Dr. Gregory Gores
Gall bladder
Cystic duct
Pancreas
Cholangiocarcinoma (CCA)
Small
intestine
Liver
Bile duct
379
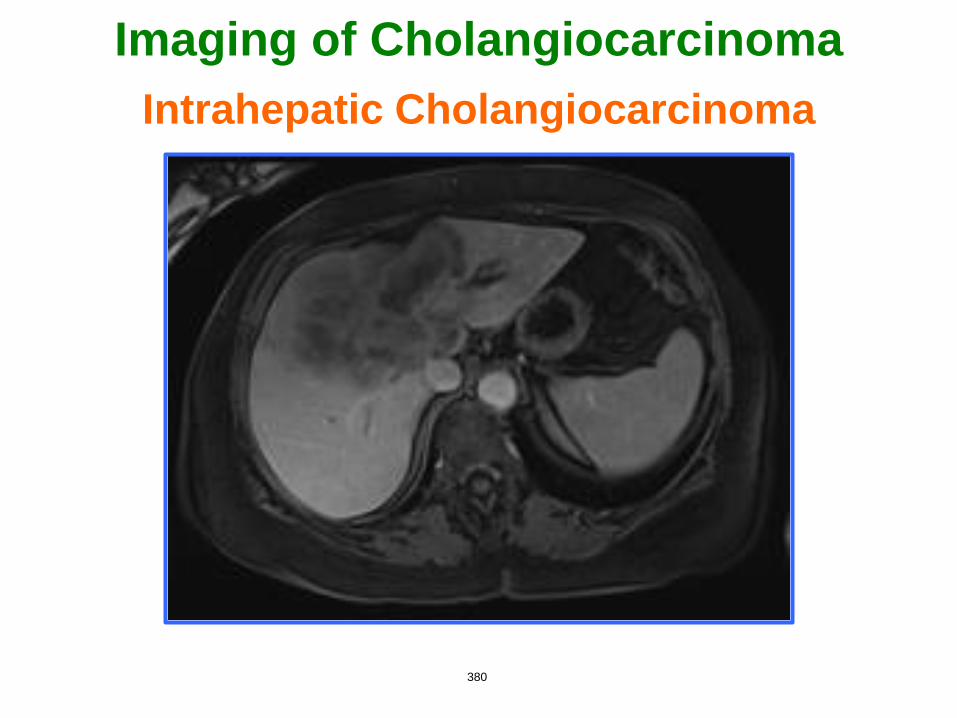
Imaging of Cholangiocarcinoma
Intrahepatic Cholangiocarcinoma
380
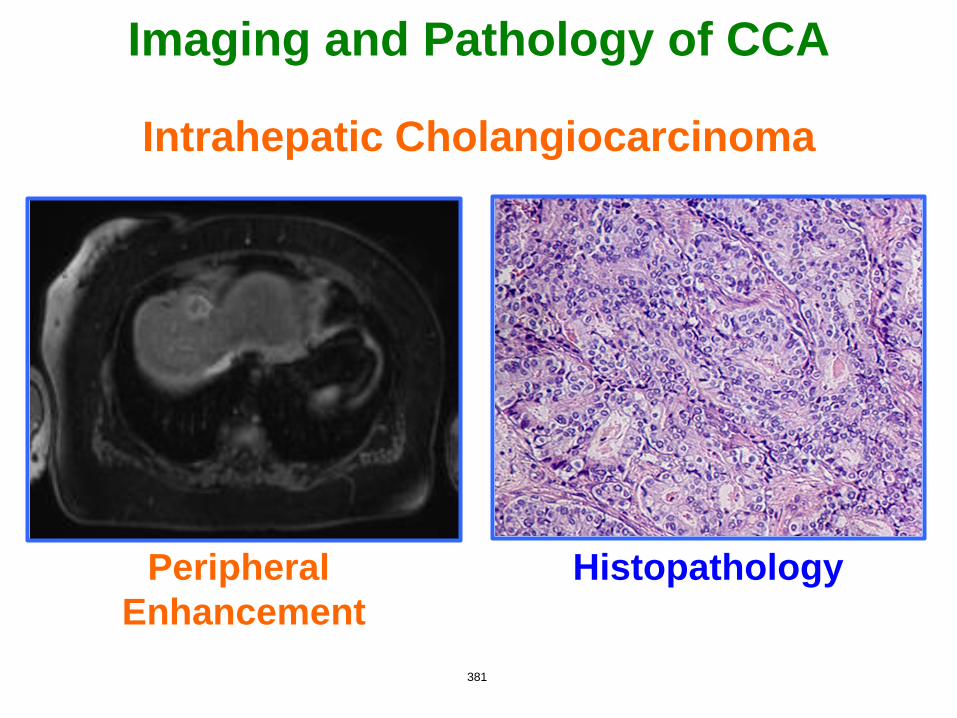
Imaging and Pathology of CCA
Intrahepatic Cholangiocarcinoma
Histopathology Peripheral
Enhancement
381

© 2016 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES
WWW.AASLD.ORG 36
Case
A 39 year old female with a 2 cm solitary lesion
on ultrasound and normal liver chemistries
Key Questions/Content Focus:
• Present an algorithm for investigation of
incidental solitary solid liver lesions.
• How does one differentiate a benign from a
malignant lesion? Imaging and/or biopsy
• Do adenomas and focal nodular hyperplasia
need to be followed and if so, how? Follow
adenomas – 6 mo, q 1 yr x 5 yrs, then q 2 yr 382

© 2016 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES
WWW.AASLD.ORG 37
Summary
• History, physical, and laboratory tests are important in the evaluation of liver masses
• Imaging techniques allow distinction between most benign and malignant liver masses
• Repeat imaging after an interval or biopsy when the diagnosis remains uncertain
• The commonest conundrum is the distinction between FNH and adenoma
• Focal fat or sparing in a fatty liver frequently masquerade as a mass
• HCCs show distinct differences from adenocarcinomas such as cholangiocarcinoma
383

© 2016 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES
WWW.AASLD.ORG 38
Thank You for Your Attention!
384

© 2016 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES
WWW.AASLD.ORG 39
Questions for Reviewers:
1. Is it ok to leave out simple cyst
and abscess slides – 23,24,25?
2. Are LIRADS slides needed –
30,31?
3. Any other suggested changes?
385