evidence-based wound care laura bolton, ph.d., adjunct associate professor, dept. of surgery,...
TRANSCRIPT
EVIDENCE-BASED WOUND CARE
EVIDENCE-BASED WOUND CARE
Laura Bolton, Ph.D., Adjunct Associate Professor, Dept. of Surgery, Bioengineering Section
University of Medicine & Dentistry of New JerseyPresident, BoltonSCI, LLC
E-mail: [email protected]
Laura Bolton, Ph.D., Adjunct Associate Professor, Dept. of Surgery, Bioengineering Section
University of Medicine & Dentistry of New JerseyPresident, BoltonSCI, LLC
E-mail: [email protected]
GOALSGOALS
1. Define evidence-based (EB) wound care
2. Describe EB wound care principles and how to integrate them into your wound care practice.
3. Review results reported using EB protocols of wound care
1. Define evidence-based (EB) wound care
2. Describe EB wound care principles and how to integrate them into your wound care practice.
3. Review results reported using EB protocols of wound care
“EVIDENCE-BASED MEDICINE IS…“EVIDENCE-BASED MEDICINE IS…
The conscientious, explicit, and judicious use of current best evidence in making
decisions about the care of individual patients.” 1
The conscientious, explicit, and judicious use of current best evidence in making
decisions about the care of individual patients.” 1
1Sackett DL et al. Br Med J, 1997; 312:71-77.

Sir Isaac Newton1642-1727
Sir Isaac Newton1642-1727
If I have seen further,
It is by standing upon
The shoulders of giants.
If I have seen further,
It is by standing upon
The shoulders of giants.

DIAGNOSE,CARE FORWOUND, PATIENT
DIAGNOSE,CARE FORWOUND, PATIENT
PROVIDE CAREPROVIDE CARE MORE CARE...MORE CARE...
YOU CAN CHOOSE…
CARE FOR WOUNDS
YOU CAN CHOOSE…
CARE FOR WOUNDS
OR
HEAL WOUNDS
using evidence-based practice.
OR
HEAL WOUNDS
using evidence-based practice.

Scope Of Evidence-Based Wound CareScope Of Evidence-Based Wound Care
• WHO can use EB wound care? – All disciplines: MD, RN, ET, APN, PT, DPM ...
• WHERE– All settings: Home, Hospital, Skilled Care...– All indications: Post-op, traumatic, chronic ...
• HOW– Diagnosis, predicting outcomes and therapy
• WHAT IS USED– Evidence of both benefits and risks– To derive patient-centered wound outcomes
• WHO can use EB wound care? – All disciplines: MD, RN, ET, APN, PT, DPM ...
• WHERE– All settings: Home, Hospital, Skilled Care...– All indications: Post-op, traumatic, chronic ...
• HOW– Diagnosis, predicting outcomes and therapy
• WHAT IS USED– Evidence of both benefits and risks– To derive patient-centered wound outcomes

How Does EB Wound Care Differ From Traditional Wound Practice?1
How Does EB Wound Care Differ From Traditional Wound Practice?1
Traditional
• Focus on practice• Parental approach• Clinician oriented • Expert opinion-based
Traditional
• Focus on practice• Parental approach• Clinician oriented • Expert opinion-based
Evidence-Based
• Focus on outcomes• Informed decision• Patient oriented• Science-based
Evidence-Based
• Focus on outcomes• Informed decision• Patient oriented• Science-based
1 1 Jaeschke R, Guyatt GH, Meade M. Jaeschke R, Guyatt GH, Meade M. Adv Wound CareAdv Wound Care 1999; 11(5):214 1999; 11(5):214

Doctor's Visit Traditional Evidence-Based
Doctor's Visit Traditional Evidence-Based
"I think you should take this therapy."
"Be sure you follow the instructions."
"I think you should take this therapy."
"Be sure you follow the instructions."
Based on the evidence,
•Therapies A or B may help you achieve your wound care goals.
•The risks, benefits and costs of each therapy are...
•Which would you be most comfortable using?

HALLMARKS OF GOOD EVIDENCE1,2HALLMARKS OF GOOD EVIDENCE1,2
• Randomized assignment of patients• Independent blinded comparison of treatment effects
or comparison to accepted standard• Efficacy and safety measured and reported• Valid outcomes measured reliably• Clinically relevant, patient-centered outcomes• Representative, similar patient samples• Adequate timing and scope of follow up
1Jaeschke R et al. Adv Wound Care, 1998; 11(5):214-2182 Gray M. et al. JWOCN 2004; 31(2):53-61.
• Randomized assignment of patients• Independent blinded comparison of treatment effects
or comparison to accepted standard• Efficacy and safety measured and reported• Valid outcomes measured reliably• Clinically relevant, patient-centered outcomes• Representative, similar patient samples• Adequate timing and scope of follow up
1Jaeschke R et al. Adv Wound Care, 1998; 11(5):214-2182 Gray M. et al. JWOCN 2004; 31(2):53-61.

Benefits Of EB Wound CareBenefits Of EB Wound Care
• Reliable, safe patient outcomes
• Consistently managed patients
• Reduced recurrence
• Improved professional reputation
• Reduce legal liability
• Economically sound outcomes
• Reliable, safe patient outcomes
• Consistently managed patients
• Reduced recurrence
• Improved professional reputation
• Reduce legal liability
• Economically sound outcomes
Some EBM Resources: http://www….Some EBM Resources: http://www….
• Cochrane Initiative– cochrane.org/
• McMasters– shef.ac.uk/uni/academic/R-Z/scharr/
triage/index/EBM.htm
• National Library of Med. (MEDLINE)– ncbi.nlm.nih.gov/PubMed/
• National Guideline Clearinghouse
– guideline.gov/
• Cochrane Initiative– cochrane.org/
• McMasters– shef.ac.uk/uni/academic/R-Z/scharr/
triage/index/EBM.htm
• National Library of Med. (MEDLINE)– ncbi.nlm.nih.gov/PubMed/
• National Guideline Clearinghouse
– guideline.gov/
BRIDGING THE GAP BETWEEN EVIDENCE AND PRACTICE
INTEGRATING EVIDENCE-BASED PRINCIPLES INTO WOUND PRACTICE
BRIDGING THE GAP BETWEEN EVIDENCE AND PRACTICE
INTEGRATING EVIDENCE-BASED PRINCIPLES INTO WOUND PRACTICE
Implementing EB Principles In Wound Care Practice
Implementing EB Principles In Wound Care Practice
G: Identify patient-oriented GOAL
A: Evidence-based ACTION PLAN
P: Measure PROGRESS
Hermans MHE, Bolton LL, Establishing a skin integrity program. Remington Report, 2001; 9(6) Suppl. 1:6-8

Patient-oriented Goal Guides the Action PlanPatient-oriented Goal Guides the Action Plan
If the GOAL is...
• Reduce edema• Reduce pressure• Protect wound• Protect skin• Minimize pain, odor• Manage excess fluid• Reduce infection risk• Heal the wound• Minimize scar
If the GOAL is...
• Reduce edema• Reduce pressure• Protect wound• Protect skin• Minimize pain, odor• Manage excess fluid• Reduce infection risk• Heal the wound• Minimize scar
ACTION plan requires...
• High multi-layer compression• Pressure relief surface or shoe• Off-load insensate extremity• Moisturizing skin barrier• Moisture barrier wound dressing• With optional absorbent primary
dressing• Moisture barrier wound dressing
ACTION plan requires...
• High multi-layer compression• Pressure relief surface or shoe• Off-load insensate extremity• Moisturizing skin barrier• Moisture barrier wound dressing• With optional absorbent primary
dressing• Moisture barrier wound dressing

Evidence-based (EB)
Action To Manage Patient and Wound
Evidence-based (EB)
Action To Manage Patient and Wound
• Diagnose & correct tissue damage causes
• Optimize wound bed & surrounding skin
• Provide moist healing environment

Diagnose….Diagnose….

Diagnose and correct the cause(s) of tissue damage!
Diagnose and correct the cause(s) of tissue damage!

Chronic wounds require a multidisciplinary team to diagnose and
correct the cause.
Chronic wounds require a multidisciplinary team to diagnose and
correct the cause.
• Contributing factors– Vasculature– Nutrition– Endocrinology– Immune Disorders– Infection– Excessive/Prolonged
Pressure/Moisture– Repeated Physical or
Chemical Trauma
• Contributing factors– Vasculature– Nutrition– Endocrinology– Immune Disorders– Infection– Excessive/Prolonged
Pressure/Moisture– Repeated Physical or
Chemical Trauma
The wound is attached to A PATIENT.
Local care can’t do this alone!
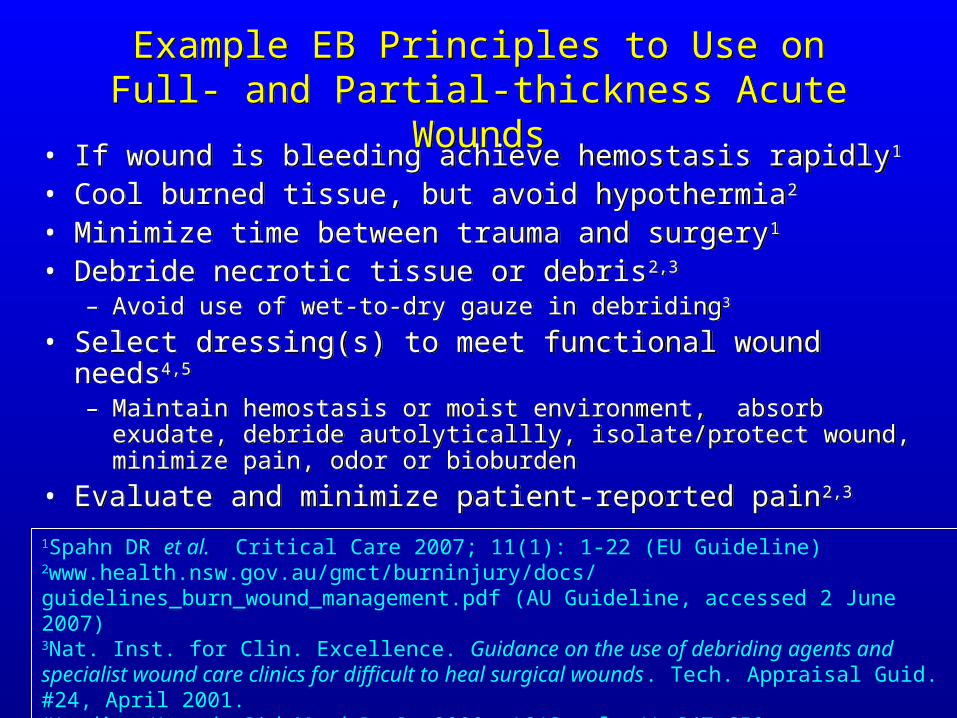
Example EB Principles to Use on Full- and Partial-thickness Acute Wounds
Example EB Principles to Use on Full- and Partial-thickness Acute Wounds
• If wound is bleeding achieve hemostasis rapidly1
• Cool burned tissue, but avoid hypothermia2
• Minimize time between trauma and surgery1
• Debride necrotic tissue or debris2,3
– Avoid use of wet-to-dry gauze in debriding3
• Select dressing(s) to meet functional wound needs4,5
– Maintain hemostasis or moist environment, absorb exudate, debride autolyticallly, isolate/protect wound, minimize pain, odor or bioburden
• Evaluate and minimize patient-reported pain2,3
• If wound is bleeding achieve hemostasis rapidly1
• Cool burned tissue, but avoid hypothermia2
• Minimize time between trauma and surgery1
• Debride necrotic tissue or debris2,3
– Avoid use of wet-to-dry gauze in debriding3
• Select dressing(s) to meet functional wound needs4,5
– Maintain hemostasis or moist environment, absorb exudate, debride autolyticallly, isolate/protect wound, minimize pain, odor or bioburden
• Evaluate and minimize patient-reported pain2,3
1Spahn DR et al. Critical Care 2007; 11(1): 1-22 (EU Guideline)2www.health.nsw.gov.au/gmct/burninjury/docs/guidelines_burn_wound_management.pdf (AU Guideline, accessed 2 June 2007)3Nat. Inst. for Clin. Excellence. Guidance on the use of debriding agents and specialist wound care clinics for difficult to heal surgical wounds. Tech. Appraisal Guid. #24, April 2001.4Harding K et al. Diab Metab Res Rev 2000; 16(Suppl. 1):S47-S50. 5van Rijswijk L, Beitz J. J. W. O. C. N. 1998; 25(3):116-122.
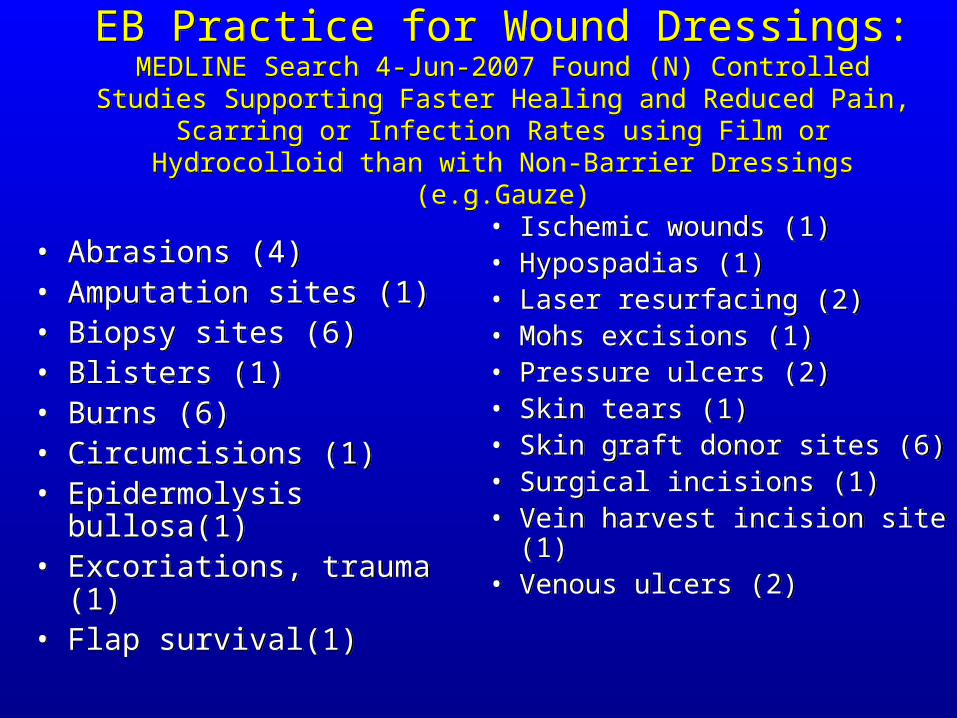
EB Practice for Wound Dressings:MEDLINE Search 4-Jun-2007 Found (N) Controlled Studies Supporting
Faster Healing and Reduced Pain, Scarring or Infection Rates using Film or Hydrocolloid than with Non-Barrier Dressings (e.g.Gauze)
EB Practice for Wound Dressings:MEDLINE Search 4-Jun-2007 Found (N) Controlled Studies Supporting
Faster Healing and Reduced Pain, Scarring or Infection Rates using Film or Hydrocolloid than with Non-Barrier Dressings (e.g.Gauze)
• Abrasions (4)• Amputation sites (1)• Biopsy sites (6)• Blisters (1)• Burns (6)• Circumcisions (1)• Epidermolysis bullosa(1)• Excoriations, trauma (1)• Flap survival(1)
• Abrasions (4)• Amputation sites (1)• Biopsy sites (6)• Blisters (1)• Burns (6)• Circumcisions (1)• Epidermolysis bullosa(1)• Excoriations, trauma (1)• Flap survival(1)
• Ischemic wounds (1)• Hypospadias (1)• Laser resurfacing (2)• Mohs excisions (1) • Pressure ulcers (2)• Skin tears (1)• Skin graft donor sites (6)• Surgical incisions (1)• Vein harvest incision site (1) • Venous ulcers (2)
• Ischemic wounds (1)• Hypospadias (1)• Laser resurfacing (2)• Mohs excisions (1) • Pressure ulcers (2)• Skin tears (1)• Skin graft donor sites (6)• Surgical incisions (1)• Vein harvest incision site (1) • Venous ulcers (2)
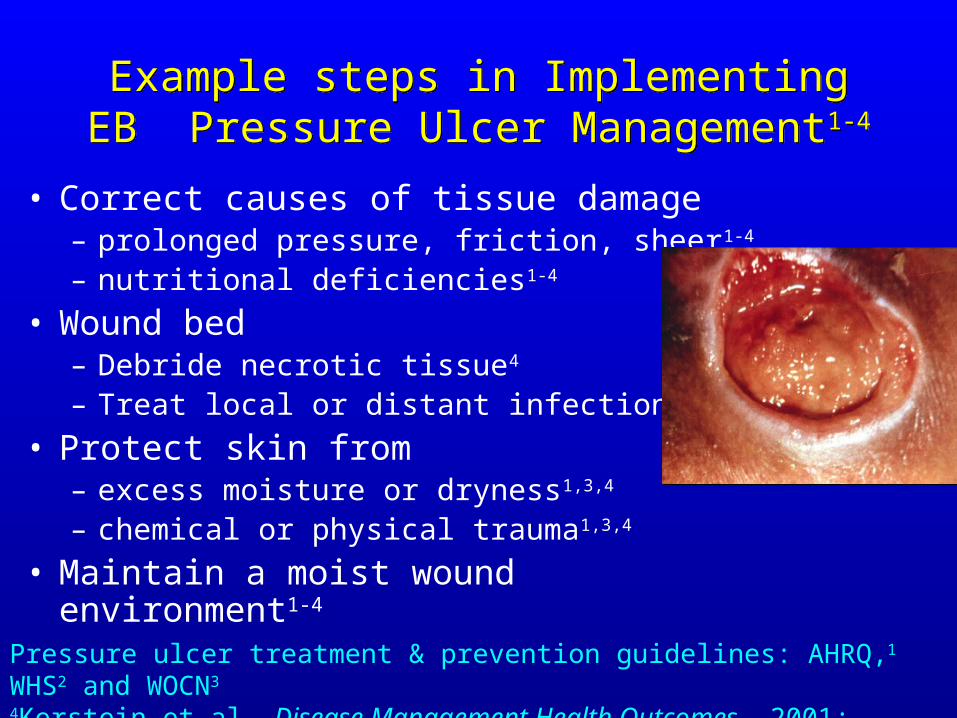
Example steps in ImplementingEB Pressure Ulcer Management1-4
Example steps in ImplementingEB Pressure Ulcer Management1-4
• Correct causes of tissue damage – prolonged pressure, friction, sheer1-4
– nutritional deficiencies1-4
• Wound bed – Debride necrotic tissue4
– Treat local or distant infection2
• Protect skin from– excess moisture or dryness1,3,4
– chemical or physical trauma1,3,4
• Maintain a moist wound environment1-4
Pressure ulcer treatment & prevention guidelines: AHRQ,1 WHS2 and WOCN3
4Kerstein et al. Disease Management Health Outcomes, 2001; 9(11):651-663

EB Venous Ulcer Management1,2,3EB Venous Ulcer Management1,2,3
• Diagnose and correct the cause– Rule out arterial cause:
• Ankle/brachial index (ABI) > 0.9• ABI 0.7-0.9 compress with care
– Sustained, graduated, high, 2- to 4- layer elastic compression
– Elevate limb, flex ankle or walk– Elastic stockings prevent recurrence
• Manage exudate and dermatitis• Moist wound environment
• Diagnose and correct the cause– Rule out arterial cause:
• Ankle/brachial index (ABI) > 0.9• ABI 0.7-0.9 compress with care
– Sustained, graduated, high, 2- to 4- layer elastic compression
– Elevate limb, flex ankle or walk– Elastic stockings prevent recurrence
• Manage exudate and dermatitis• Moist wound environment
11McGuckin M, et al. McGuckin M, et al. Amer J SurgeryAmer J Surgery 2002; 183:132-137. 2002; 183:132-137.
22Bolton et al. Bolton et al. Ostomy/Wound Mgmt , , 2006; 52(11):32-48 (AAWC Guideline)33Kerstein MD Kerstein MD et al. Dis. Manage. Health Outcomeset al. Dis. Manage. Health Outcomes, 2001;9(11),651-63, 2001;9(11),651-63
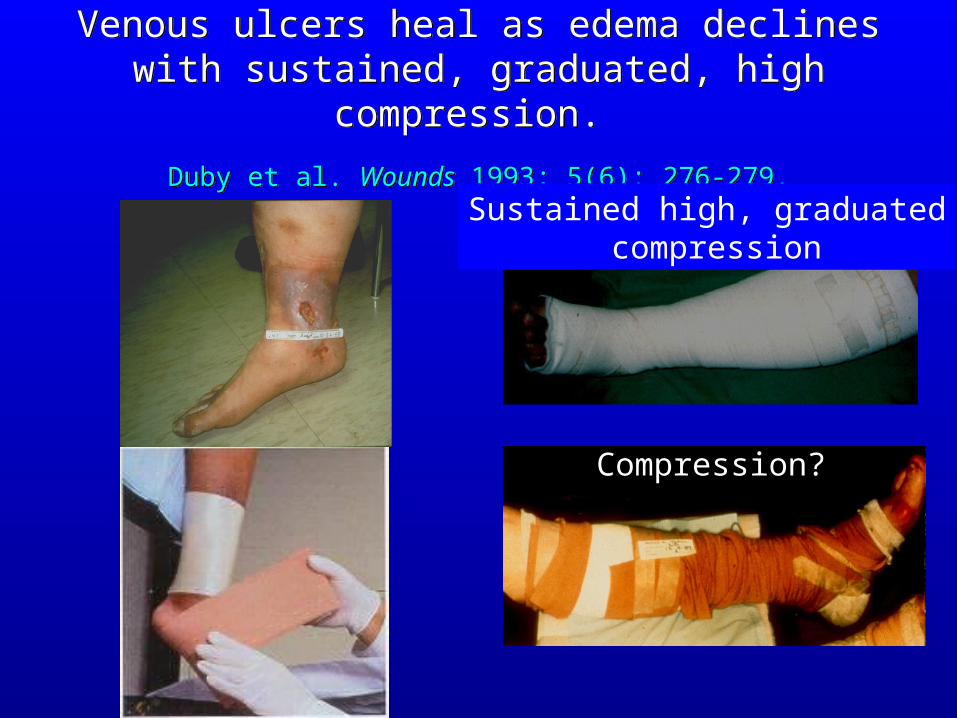
Venous ulcers heal as edema declineswith sustained, graduated, high compression.
Duby et al. Wounds 1993; 5(6): 276-279.
Venous ulcers heal as edema declineswith sustained, graduated, high compression.
Duby et al. Wounds 1993; 5(6): 276-279.
Sustained high, graduated compression
Compression?

EB Action Plan To Manage Arterial or Ischemic Ulcers
• Diagnose, correct related conditions1,2
– Peri-wound TcPO2 < 20 mmHg predicts non-healing1
– Vascular specialist locate, correct arterial blockage
• Prompt referral if rest pain and/or gangrene2
• Remove necrotic tissue– limit microorganisms2
• Avoid nicotine1,2
• Diagnose, correct related conditions1,2
– Peri-wound TcPO2 < 20 mmHg predicts non-healing1
– Vascular specialist locate, correct arterial blockage
• Prompt referral if rest pain and/or gangrene2
• Remove necrotic tissue– limit microorganisms2
• Avoid nicotine1,2
1Hopf H. et al. Wound Rep Regen, 2006; 14: 693-710. (WHS Guideline)2Kerstein MD. Kerstein MD. Ostomy/Wound MgmtOstomy/Wound Mgmt 1996; 42(10A Suppl):19S-35S 1996; 42(10A Suppl):19S-35S

EB Diabetic Foot Ulcer Management1,2,3EB Diabetic Foot Ulcer Management1,2,3
• Diagnose and correct the cause– Control diabetes (HbA1c < 6.5%)– ABI > 0.9 rules out arterial insufficiency– ABI > 1.3 rigid vessel wall; use great toe– No ABI, use TcPO2 > 40 mmHg
• Check for neuropathy– Semmes-Weinstein 10 g (#5.07) fiber– Protect skin and off load
• Wound/Skin:– Gel debridement speeds DFU healing4 – No healing progress: suspect infection
• Moist wound environment3
• Diagnose and correct the cause– Control diabetes (HbA1c < 6.5%)– ABI > 0.9 rules out arterial insufficiency– ABI > 1.3 rigid vessel wall; use great toe– No ABI, use TcPO2 > 40 mmHg
• Check for neuropathy– Semmes-Weinstein 10 g (#5.07) fiber– Protect skin and off load
• Wound/Skin:– Gel debridement speeds DFU healing4 – No healing progress: suspect infection
• Moist wound environment3
1Steed et al. Wound Rep Reg (2006) 14 680–692 (WHS Guideline)2Crawford et al. WOCN Guideline 3 …Lower extremity neuropathic disease3Amer Diab Assn Consensus Dev. Conf., Diabetes Care 1999; 22(8):1354-1360.42Smith J, Thow J. The Diabetic Foot 2003; 6(1):12-16

Consistent, Continuous Off-loading
Consistent, Continuous Off-loading
One barefoot walk to the bathroom can One barefoot walk to the bathroom can undo a week of healing.undo a week of healing.

Evidence For Minimizing Wound InfectionsEvidence For Minimizing Wound Infections
Infection is 5x more likely in DFU than in non-diabetic chronic wounds4
• Passive Mechanisms– Isolate and protect wound 1,2
– Debride necrosis, foreign matter3 • Active Mechanisms3
– Topical antimicrobial agents– If signs of infection are present,
• Biopsy or quantitative swab to identify infecting organism
• Prescribe correct systemic antibiotic
• Passive Mechanisms– Isolate and protect wound 1,2
– Debride necrosis, foreign matter3 • Active Mechanisms3
– Topical antimicrobial agents– If signs of infection are present,
• Biopsy or quantitative swab to identify infecting organism
• Prescribe correct systemic antibiotic
1Hutchinson JJ, McGuckin M. Amer J Infec Control 1990; 18(4):257-268.2 Wilson P, et al. The Pharmaceutical Journal December 17, 1988; 787-788. 3 Steed et al. Wound RepRegen, (2006) 14 680–692 4 Rubinstein, Am. J. Med. 1983; 75(1):161

Moist Environment to Protect, Isolate Wound: Fewer Infections in Diabetic Neuropathic UlcersMoist Environment to Protect, Isolate Wound:
Fewer Infections in Diabetic Neuropathic Ulcers
BOULTON et al. Wound Rep Reg 1999;7:7-16
Retrospective study• Clinical infections
– diabetic foot ulcers
• Off-load + Dressings:– Hydrocolloid (HCD)– Traditional Gauze
BOULTON et al. Wound Rep Reg 1999;7:7-16
Retrospective study• Clinical infections
– diabetic foot ulcers
• Off-load + Dressings:– Hydrocolloid (HCD)– Traditional Gauze
Percent Clinical Infections Reported
6
2.5
0
1
2
3
4
5
6
Gauze HCD
Protocols of CareProtocols of Care

Moist Environment to Protect, Isolate Wound Reduces Risk of Infection: All Wounds
Moist Environment to Protect, Isolate Wound Reduces Risk of Infection: All Wounds
Hutchinson & McGuckinAmer J Infect Control, 1990; 18:257
• Retrospective 30 yr literature review
• Clinical infections• 1085 gauze (all types)• 1351 hydrocolloid (HCD)• 617 foam dressings• 1021 film dressings
Hutchinson & McGuckinAmer J Infect Control, 1990; 18:257
• Retrospective 30 yr literature review
• Clinical infections• 1085 gauze (all types)• 1351 hydrocolloid (HCD)• 617 foam dressings• 1021 film dressings
Percent Clinical Infections Reported
HCD
7.1
1.32.4
4.5
0
2
4
6
8
Gauze Foams Films
ProtocolProtocol
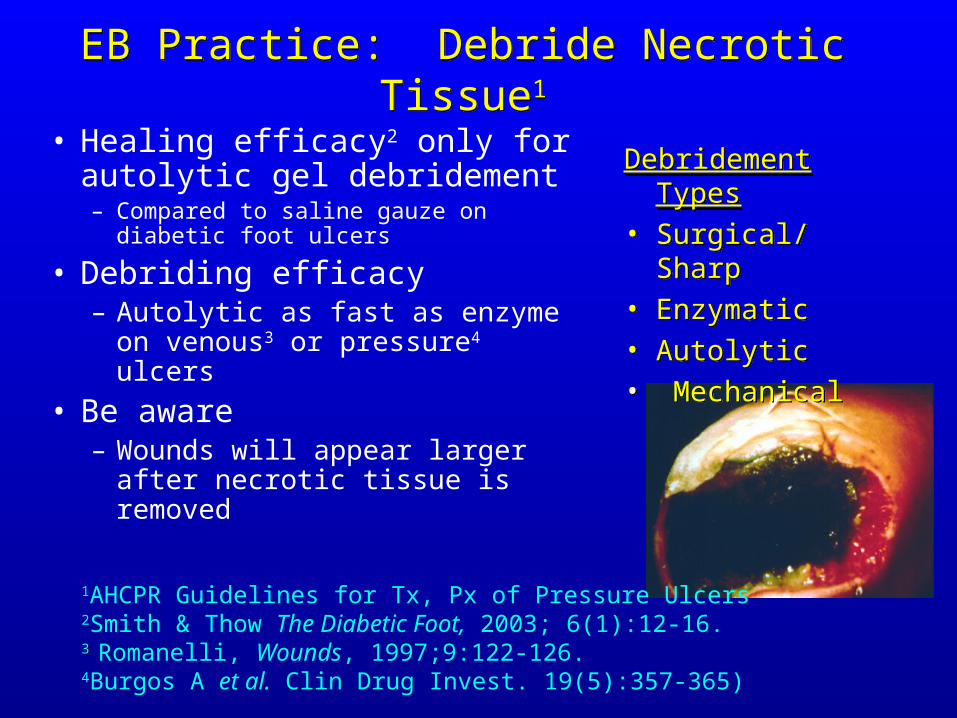
EB Practice: Debride Necrotic Tissue1EB Practice: Debride Necrotic Tissue1
• Healing efficacy2 only for autolytic gel debridement– Compared to saline gauze on
diabetic foot ulcers
• Debriding efficacy– Autolytic as fast as enzyme on
venous3 or pressure4 ulcers
• Be aware – Wounds will appear larger after
necrotic tissue is removed
1AHCPR Guidelines for Tx, Px of Pressure Ulcers2Smith & Thow The Diabetic Foot, 2003; 6(1):12-16.3 3 Romanelli, Wounds, 1997;9:122-126.4Burgos A et al. Clin Drug Invest. 19(5):357-365)
Debridement Types• Surgical/ Sharp• Enzymatic• Autolytic• Mechanical
Debridement Types• Surgical/ Sharp• Enzymatic• Autolytic• Mechanical

Implementing EB Wound Care: Measure
Progress Toward Goal
Implementing EB Wound Care: Measure
Progress Toward GoalWhy measure?
• Support care decisions• Encourage patient• Early warning of:
– infection – non-healing (4 wk <20%
decrease in wound area)
• Benchmark outcomes• Identify problems
Why measure?
• Support care decisions• Encourage patient• Early warning of:
– infection – non-healing (4 wk <20%
decrease in wound area)
• Benchmark outcomes• Identify problems
What to Measure
• Wound dimensions• Wound bed
– Necrotic tissue– Granulation– Epithelization
• Exudate• Odor• Pain
What to Measure
• Wound dimensions• Wound bed
– Necrotic tissue– Granulation– Epithelization
• Exudate• Odor• Pain
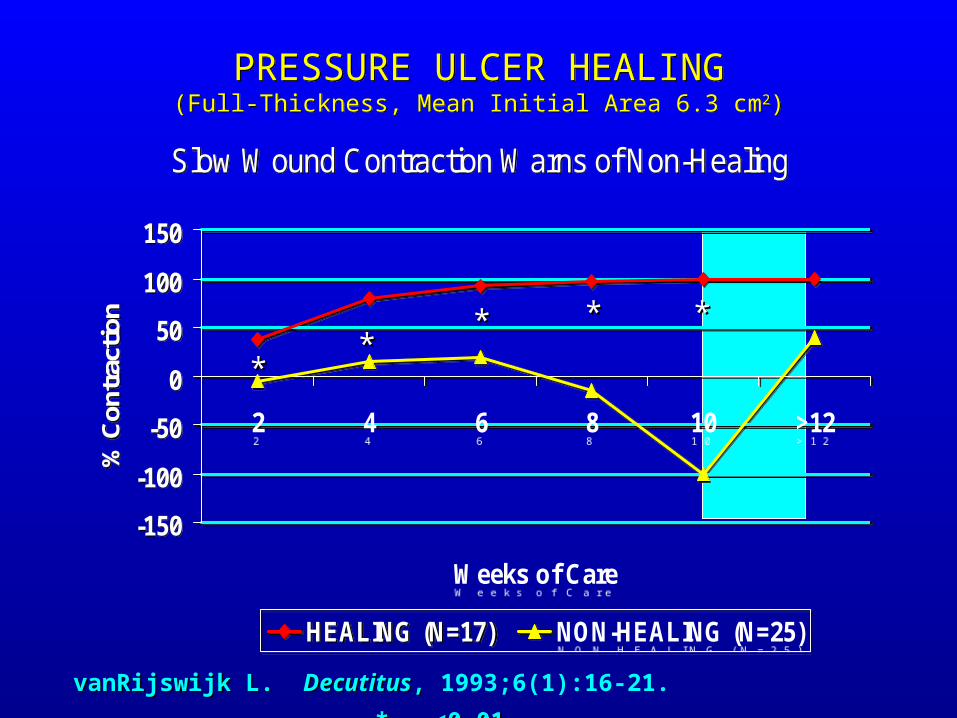
PRESSURE ULCER HEALING(Full-Thickness, Mean Initial Area 6.3 cm2)
PRESSURE ULCER HEALING(Full-Thickness, Mean Initial Area 6.3 cm2)
Slow Wound Contraction Warns of Non-Healing
-150
-100
-50
0
50
100
150
2 4 6 8 10 >12
Weeks of Care
% C
ontr
actio
n
HEALING (N=17) NON-HEALING (N=25)
Slow Wound Contraction Warns of Non-Healing
-150
-100
-50
0
50
100
150
2 4 6 8 10 >12
Weeks of Care
% C
ontr
actio
n
HEALING (N=17) NON-HEALING (N=25)
****
** ** **
vanRijswijk L. vanRijswijk L. DecutitusDecutitus, , 1993;6(1):16‑21. * * <0.01 <0.01
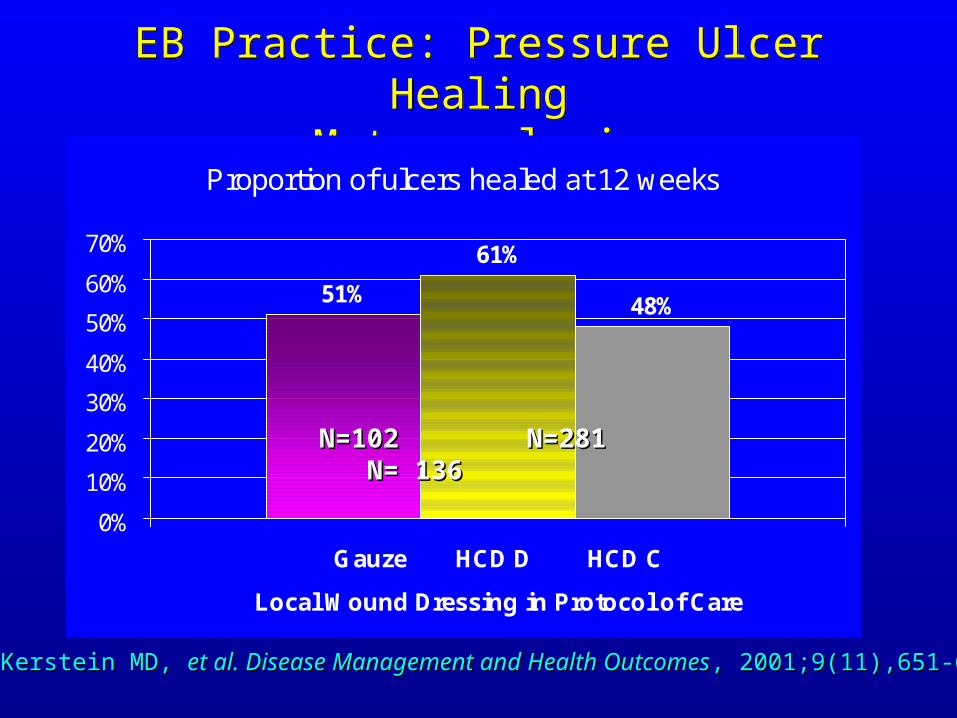
EB Practice: Pressure Ulcer HealingMeta-analysis
EB Practice: Pressure Ulcer HealingMeta-analysis
Proportion of ulcers healed at 12 weeks
51%
61%
48%
0%
10%
20%
30%
40%
50%
60%
70%
Gauze HCD D HCD C
Local Wound Dressing in Protocol of Care
Kerstein MD, Kerstein MD, et al. Disease Management and Health Outcomeset al. Disease Management and Health Outcomes, 2001;9(11),651-663, 2001;9(11),651-663
N=102 N=281 N= 136N=102 N=281 N= 136

EB Practice: Venous Ulcer HealingMeta-analysis
EB Practice: Venous Ulcer HealingMeta-analysis
Proportion of ulcers healed at 12 weeks
39%
51%45%
0%
10%
20%
31%
41%
51%
61%
Gauze HCD D Skin Construct
Local Wound Dressing in Protocol with Compression
Kerstein MD, Kerstein MD, et al. Disease Management and Health Outcomeset al. Disease Management and Health Outcomes, 2001;9(11),651-663, 2001;9(11),651-663
N=223 N=530 N=130N=223 N=530 N=130
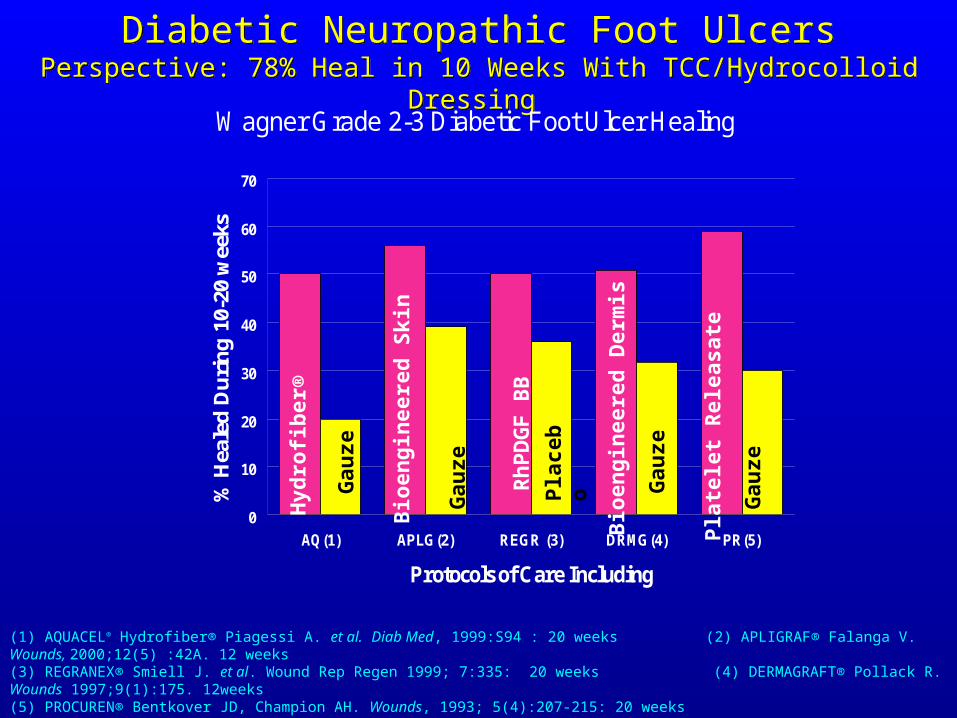
Diabetic Neuropathic Foot UlcersPerspective: 78% Heal in 10 Weeks With TCC/Hydrocolloid Dressing
Diabetic Neuropathic Foot UlcersPerspective: 78% Heal in 10 Weeks With TCC/Hydrocolloid Dressing
Wagner Grade 2-3 Diabetic Foot Ulcer Healing
0
10
20
30
40
50
60
70
AQ(1) APLG(2) REGR (3) DRMG(4) PR(5)
Protocols of Care Including
% H
eale
d D
uri
ng
10-
20 w
eeks
(1) AQUACEL® Hydrofiber® Piagessi A. et al. Diab Med, 1999:S94 : 20 weeks (2) APLIGRAF® Falanga V. Wounds, 2000;12(5) :42A. 12 weeks(3) REGRANEX® Smiell J. et al. Wound Rep Regen 1999; 7:335: 20 weeks (4) DERMAGRAFT® Pollack R. Wounds 1997;9(1):175. 12weeks(5) PROCUREN® Bentkover JD, Champion AH. Wounds, 1993; 5(4):207-215: 20 weeks
Hyd
rofi
ber
®
Gau
ze
Bio
engi
nee
red
Sk
in
Gau
ze
Rh
PD
GF
BB
Bio
engi
nee
red
Der
mis
Pla
tele
t R
elea
sate
Pla
ceb
o
Gau
ze
Gau
ze
Implementing Evidence-Based
Wound Practice
Implementing Evidence-Based
Wound Practice
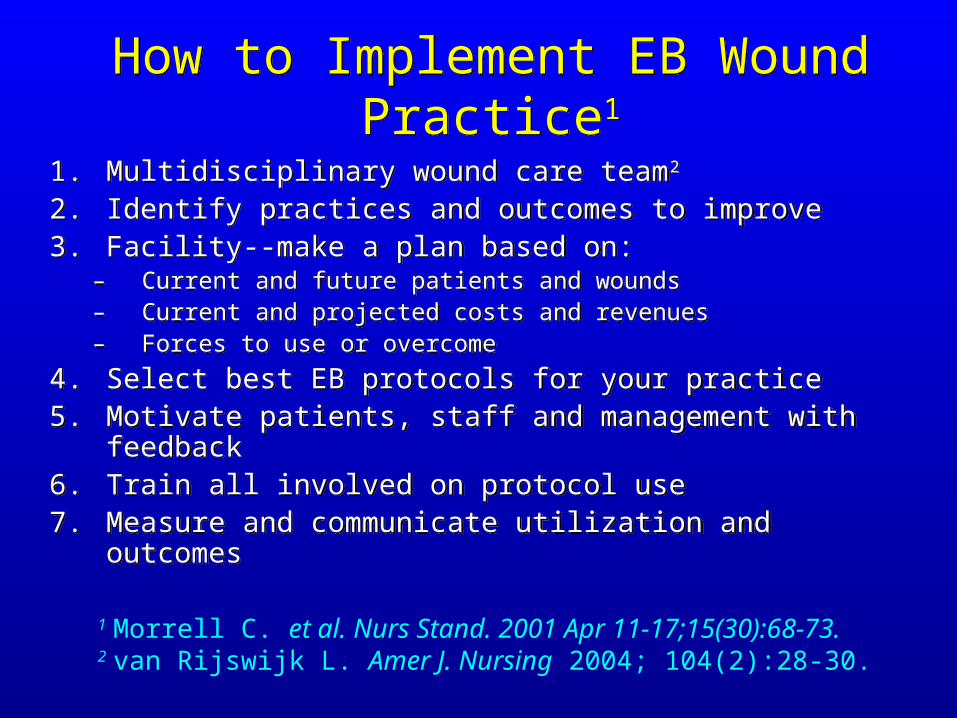
How to Implement EB Wound Practice1How to Implement EB Wound Practice1
1. Multidisciplinary wound care team2
2. Identify practices and outcomes to improve3. Facility--make a plan based on:
– Current and future patients and wounds– Current and projected costs and revenues– Forces to use or overcome
4. Select best EB protocols for your practice5. Motivate patients, staff and management with feedback6. Train all involved on protocol use 7. Measure and communicate utilization and outcomes
1. Multidisciplinary wound care team2
2. Identify practices and outcomes to improve3. Facility--make a plan based on:
– Current and future patients and wounds– Current and projected costs and revenues– Forces to use or overcome
4. Select best EB protocols for your practice5. Motivate patients, staff and management with feedback6. Train all involved on protocol use 7. Measure and communicate utilization and outcomes
1 Morrell C. et al. Nurs Stand. 2001 Apr 11-17;15(30):68-73.2 van Rijswijk L. Amer J. Nursing 2004; 104(2):28-30.

Implementing EB Protocols Venous Ulcer Care If expected outcomes not achieved, e.g. little progress in 2-4
weeks, re-evaluate etiology, care
Implementing EB Protocols Venous Ulcer Care If expected outcomes not achieved, e.g. little progress in 2-4
weeks, re-evaluate etiology, care
Beitz JM, Bates-Jensen B. O/WM, 2001; 47(4):33-40Beitz JM, Bates-Jensen B. O/WM, 2001; 47(4):33-40
Example EB VU Protocol
Patient Wound
Goals Based on evaluation
Rule out arterial (ABI)
Reduce edema
Reduce pain
Manage exudate
Heal venous ulcer
Action plan Evidence-Based
Elastic compression agreeable to patient
Absorbent primary dressing, moisture barrier secondary
Progress Measures
Patient-reported pain
Ankle circumference
Length, width, depth
Healing time

Implementing Evidence-Based GuidelinesAvoid Pitfalls
Implementing Evidence-Based GuidelinesAvoid Pitfalls
• Credit protocol only if it was clear cause
• Use objective benchmarks
• Listen to what missing data tells you.
• Listen to and use feedback from– Patients– Staff– Management
• Credit protocol only if it was clear cause
• Use objective benchmarks
• Listen to what missing data tells you.
• Listen to and use feedback from– Patients– Staff– Management

Clinical Outcomes Using Evidence-Based
Protocols of Wound Care
Clinical Outcomes Using Evidence-Based
Protocols of Wound Care

Japan Pressure Ulcer Outcomes Using EB ProtocolOhura T, Sanada H, Mino Y.Wounds 2004; 16(5):157-73
MC/A
TC/A
TC/NA
10
15
20
25
30
35
At time ofenrollment
At the end of study
26.9
31.5
15.8
21.9
MC/A (n=29): modern dressings with a standardized wound management algorithmTC/A (n=34): traditional dressings with a standardized wound management algorithmTC/NA (n=20): traditional dressings without using a standardized wound management algorithm
29.8
22.5
Mea
n P
SS
T S
core
s
MCA improved PUoutcomes at less than half
the total (labor +
materials) cost of TC/NA
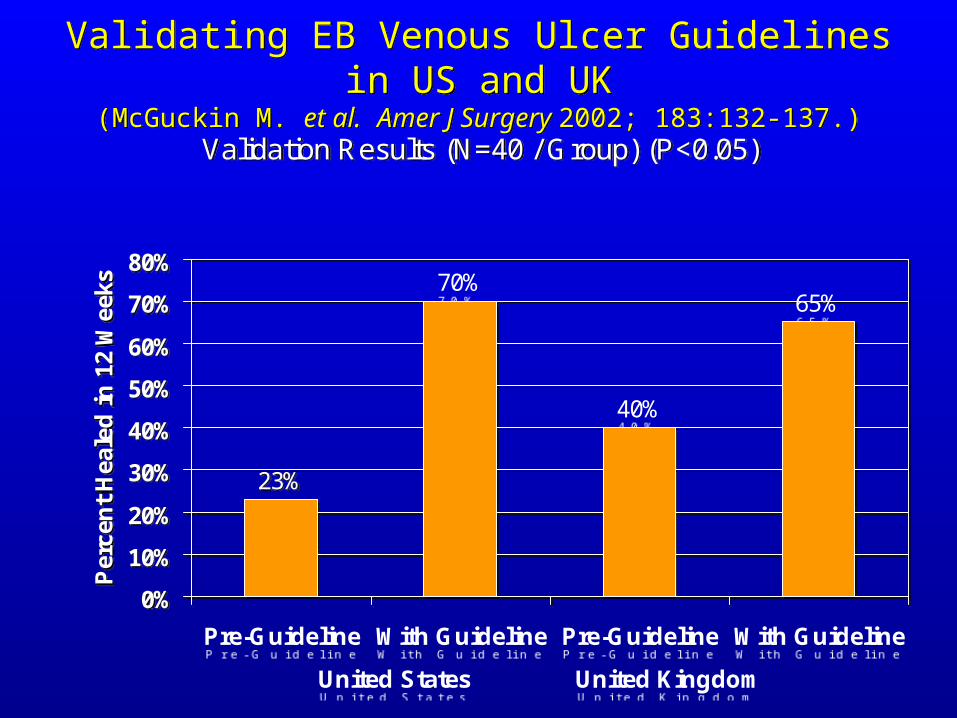
Validation Results (N=40 / Group) (P<0.05)
23%
70%
40%
65%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Pre-Guideline With Guideline Pre-Guideline With Guideline
United States United Kingdom
Per
cen
t H
eale
d i
n 1
2 W
eeks
Validation Results (N=40 / Group) (P<0.05)
23%
70%
40%
65%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Pre-Guideline With Guideline Pre-Guideline With Guideline
United States United Kingdom
Per
cen
t H
eale
d i
n 1
2 W
eeks
Validating EB Venous Ulcer Guidelines in US and UK(McGuckin M. et al. Amer J Surgery 2002; 183:132-137.)
Validating EB Venous Ulcer Guidelines in US and UK(McGuckin M. et al. Amer J Surgery 2002; 183:132-137.)
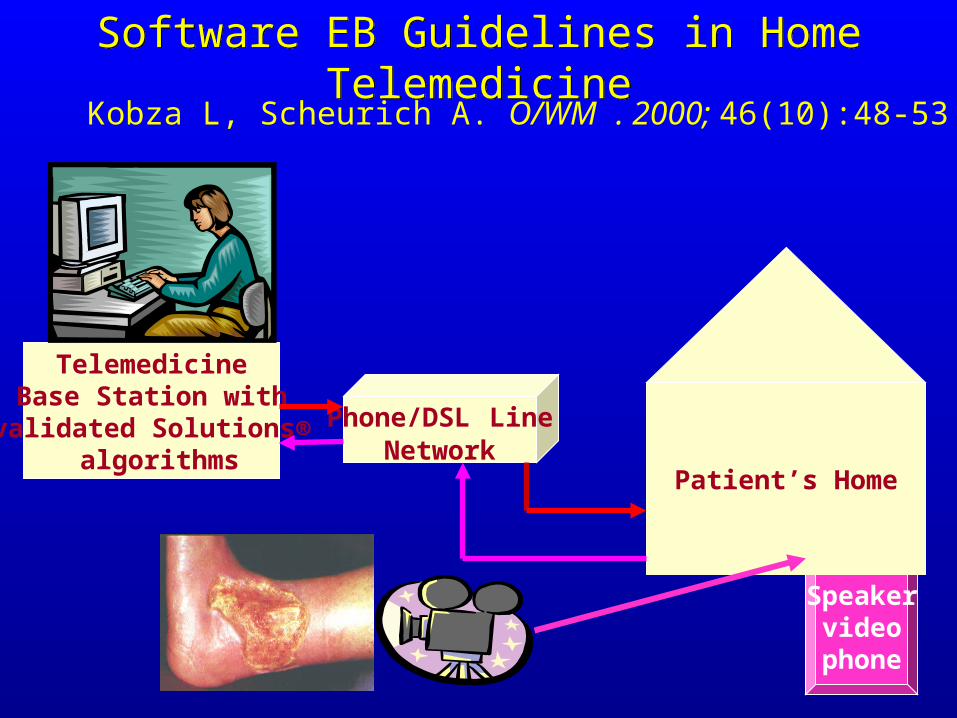
Phone/DSL LineNetwork
Speakervideophone
TelemedicineBase Station with
validated Solutions® algorithms
Patient’s Home
Software EB Guidelines in Home TelemedicineSoftware EB Guidelines in Home TelemedicineKobza L, Scheurich A. O/WM . 2000; 46(10):48-53
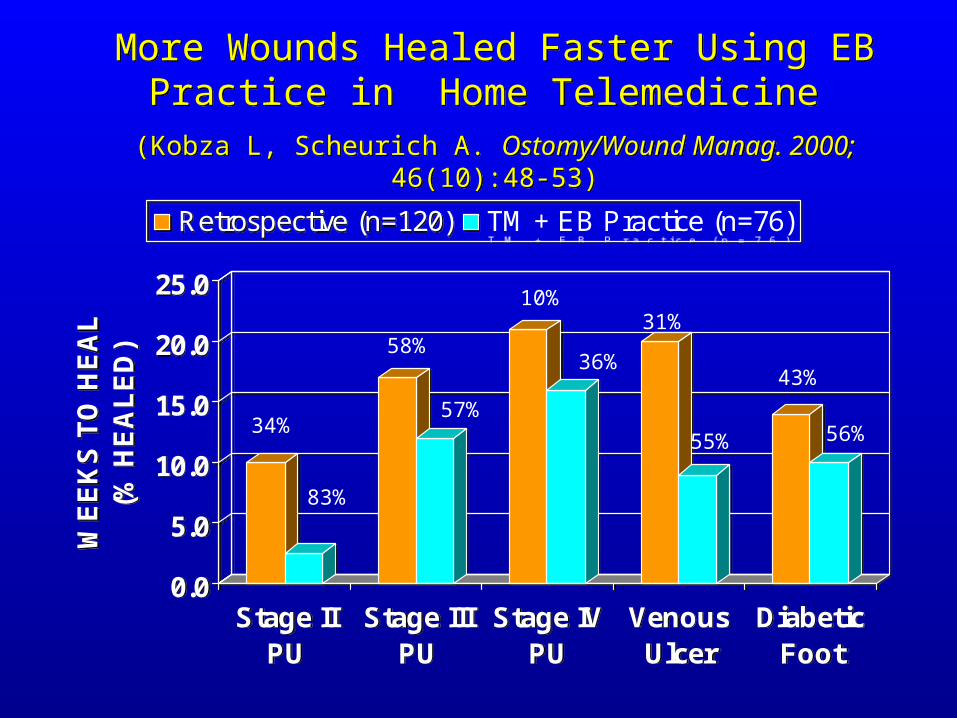
More Wounds Healed Faster Using EB Practice in Home Telemedicine
(Kobza L, Scheurich A. Ostomy/Wound Manag. 2000; 46(10):48-53)
More Wounds Healed Faster Using EB Practice in Home Telemedicine
(Kobza L, Scheurich A. Ostomy/Wound Manag. 2000; 46(10):48-53)
0.0
5.0
10.0
15.0
20.0
25.0
WE
EK
S T
O H
EA
L
(
% H
EA
LE
D)
Stage IIPU
Stage IIIPU
Stage IVPU
VenousUlcer
DiabeticFoot
Retrospective (n=120) TM + EB Practice (n=76)
0.0
5.0
10.0
15.0
20.0
25.0
WE
EK
S T
O H
EA
L
(
% H
EA
LE
D)
Stage IIPU
Stage IIIPU
Stage IVPU
VenousUlcer
DiabeticFoot
Retrospective (n=120) TM + EB Practice (n=76)
34%
83%
58%
57%
10%
36%
31%
55%
43%
56%
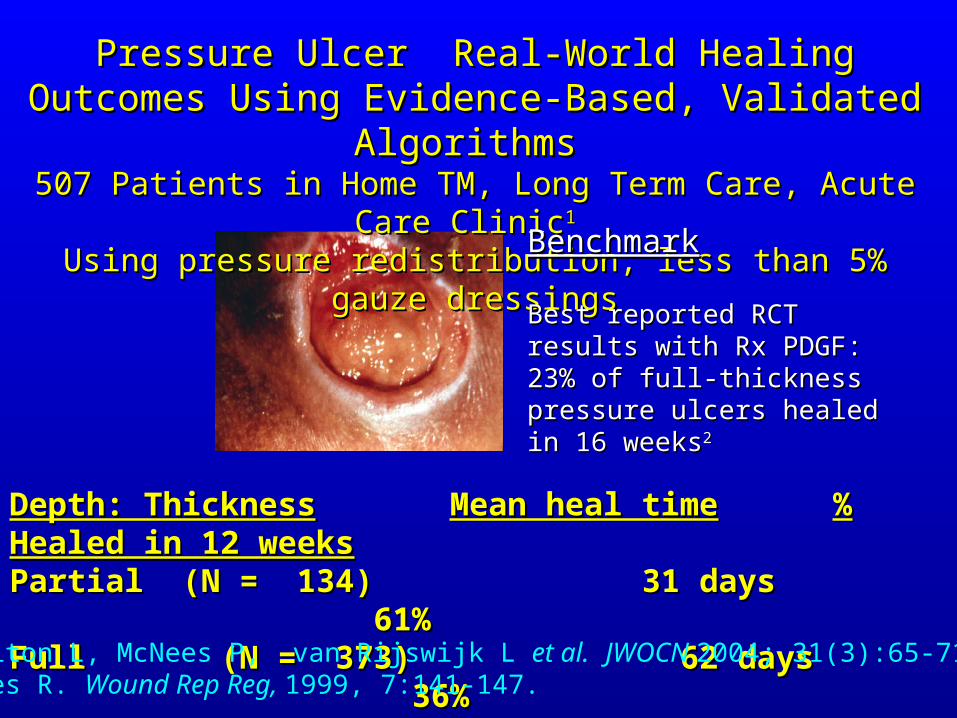
Depth: ThicknessDepth: Thickness Mean heal timeMean heal time % Healed in 12 % Healed in 12 weeksweeksPartial (N = 134) 31 days 61% Partial (N = 134) 31 days 61% Full (N = 373) 62 days 36%Full (N = 373) 62 days 36%
Pressure Ulcer Real-World Healing Outcomes Using Pressure Ulcer Real-World Healing Outcomes Using Evidence-Based, Validated AlgorithmsEvidence-Based, Validated Algorithms
507 Patients in Home TM, Long Term Care, Acute Care Clinic507 Patients in Home TM, Long Term Care, Acute Care Clinic11 Using pressure redistribution, less than 5% gauze dressingsUsing pressure redistribution, less than 5% gauze dressings
BenchmarkBenchmark
Best reported RCTBest reported RCTresults with Rx PDGF:results with Rx PDGF:23% of full-thickness23% of full-thicknesspressure ulcers healedpressure ulcers healedin 16 weeksin 16 weeks22
1Bolton L, McNees P, van Rijswijk L et al. JWOCN 2004; 31(3):65-7122Rees R. Wound Rep Reg, 1999, 7:141-147.

Venous Ulcer Real-World Healing Outcomes Venous Ulcer Real-World Healing Outcomes Using Evidence-Based, Validated Algorithms Using Evidence-Based, Validated Algorithms
154 Patients in Home TM, Long Term Care, Acute Care Clinic154 Patients in Home TM, Long Term Care, Acute Care ClinicUsing compression and less than 5% gauze dressings Using compression and less than 5% gauze dressings
Depth: ThicknessDepth: Thickness Mean + SE heal timeMean + SE heal time % Healed in 12 weeks% Healed in 12 weeksPartial (N = 30) 29 Partial (N = 30) 29 ++ 7 days 77% 7 days 77% Full (N = 124) 57 Full (N = 124) 57 ++ 7 days 44% 7 days 44%
Bolton L, McNees P, van Rijswijk L et al. Wound healing outcomes using standardized care JWOCN 2004; 31(3):65-71.

Implementing an adaptation of EB validated wound care guideline in Nova Scotia home care reduced time
and costs to healing or discharge to family care1
Implementing an adaptation of EB validated wound care guideline in Nova Scotia home care reduced time
and costs to healing or discharge to family care1
0
200
400
600
800
1000
1200
1400
1999 (6)
2000 (3)
2001 (33)
2002(435)
2003(250)
Ave
rage
Day
s to
Hea
ling
or T
o D
isch
arge
to F
amily
Car
e Pressure Ulcer
Venous Ulcer
Diabetic Foot Ulcer
Ischemic/Mix Ulcer
Surgical Wound
Burn Wound
Other Wound
0
200
400
600
800
1000
1200
1400
1999 (6)
2000 (3)
2001 (33)
2002(435)
2003(250)
Ave
rage
Day
s to
Hea
ling
or T
o D
isch
arge
to F
amily
Car
e Pressure Ulcer
Venous Ulcer
Diabetic Foot Ulcer
Ischemic/Mix Ulcer
Surgical Wound
Burn Wound
Other Wound
1Numbers in parentheses are total clients healed during specified year, not total receiving care.
(McIsaac C. O/WM 2005 Apr;51(4):54-6, 58, 59 passim. )

Hippocrates 460-400 BCELaw, Book IV
Hippocrates 460-400 BCELaw, Book IV
“There are in fact two things, science and opinion; the former begets knowledge, the latter ignorance.”
“There are in fact two things, science and opinion; the former begets knowledge, the latter ignorance.”