evidence for persistence of infectious agents in …
TRANSCRIPT

Vol. 100, No. 3Printed in U.SA.
AMERICAN JOURNAL OF EPIDEMIOLOGYCopyright @ 1974 by The Johns Hopkins University
EVIDENCE FOR PERSISTENCE OF INFECTIOUS AGENTS IN ISOLATEDHUMAN POPULATIONSl
FRANCIS L. BLACK,. WALTER J. HIERHOLZER,. FRANCISCO DEP. PINHEIRO,. ALFRED S.EVANS,. JOHN P. WOODALL,' EDWARD M. OPTON,. JEAN E. EMMONS,. BERNICE S. WEST"
GEOFFREY EDSALL,. WILBUR G. DOWNS. AND GORDON D. WALLACE7
Black, F. L. (Dept. of Epidemiology and Public Health, Vale UniversitySchool of Medicine, 60 College Street, New Haven, Conn. 065101, W. J.Hierholzer, F. deP. Pinheiro, A. S. Evans, J. P. Woodall, E. M. Opton, J. E.Emmons, B. S. West, G. Edsall, W. G. Downs and G. D. Wallace. Evidencefor persistence of infectious agents in isolated human populations. Am JEpidemio! 100 :230-250, 1974.-More than 900 members of three Cariband four Kayapo Indian tribes, living on the periphery of the Amazon basin,have been studied for immunity to various viral, bacterial and protozoalagents. These tribes are isolated from the main Brazilian culture, and severa Ihad remained hostile and dependent on stone tools until less than 10 yearsprior to the study. The prevalence of antibodies to herpesvirus types 1 and 2,Epstein-Barr virus, cytomegalovirus, varicella and hepatitis B antigen wasvery high in every tribe studied. The age of acquisition of immunity was lowerthan in previously studied cosmopolitan communities. These agents seem tomaintain a very stable relation with their host populations. Antibodies tomeasles, mumps, rubella, influenza Ao, A2 and B, parainfluenza 1., 2 and 3and poliovirus 1 were nearly or totally absent from one or more tribes. Whenthese antibodies were found in anyone who had not been outside the tribialarea, they were usually found in nearly everyone over a specific age. Theseagents seem to maintain an unstable relation with their hosts, appearing onlywhen introduced from the outside and then disappearing again. There wasno evidence of smallpox in any tribe. Antibodies to the arboviruses (yellowfever viruses, Ilhéus, and Mayarol were found with high frequency in certainareas. Prevalence of antibody to these viruses increased gradually with age,suggesting endemicitv of a different arder from that of the herpes group vi-ruses. Antibody to Toxoplasma was absent from children but was frequentlypresent in older adults. Antibody to treponema had a very high prevalence inthe Kayapo tribes 'without evidence of pathology, suggesting that the para-site present in these communities was well adapted to its host. Malaria andtuberculosis, on the other hand, caused extensive and severe morbidity and
Received for publication February 1, 1974, and infinal forrn May 10, 1974.
Abbreviations: EBV, Epstein-Barr virus; FTA-ABS, fluorescent treponemal antibody absorption;HI, hemagglutination inhibition; VDRL, VenerealDisease Research Laboratory.
1 This work was supported by a traveI grant from
the Pan American Health Organization and researchgrants from the United States Public Health Service(AI-OO701 and CA-I2952), The Rockefeller Founda-tion, and U.S. Army DADA 17-70-C-OO42.
.Department of Epidemiology and Public Health,Yale University,.New Haven, Conn. 06510.
.Instituto Evandro Chagas, FIOCRUZ, BrazilianMinistry of Health, Belem, Para, Brazil.
.State of New York Dept. of Health, Albany, N. Y.12201.
.State of Connecticut Dept. of Health, Hartford,Conn.
e Department of Public Health, State LaboratoryInstitute, The Commonwealth ofMassachusetts, Bos-ton, Mass. 02130. Present address: London School ofHygiene and Tropical Medicine, London, England.
7 Pacific Research Station, NIAID, Honolulu,
Hawaii.
230

INTRODUCTION
Since the studies ofPanum on measles inthe Faroes (1) and of Paul and Freese onthe common cold in Spitzbergen (2), it hasbeen clear that many infectious agents donot persist in small isolated communitiesbut must be reintroduced from larger pop-ulations at the onset of every epidemic. Onthe other hand, Hope Simpson (3) foundthat varicella-zoster vírus remained en-demic in a small population in the Shet-land Islands. Expressed in quantitativeterms, it has been estimated that at least200,000 people would be needed to sustainmeasles vírus (4, 5), but that a populationof 2000 sustained varicella vírus.
Population groups of the size needed tosustain measles vírus first arose with thedevelopment of urbanized societies only4000-5000 years ago. It seems improbablethat agents dependent on large aggrega-tions of the people could have existed intheir present form prior to that time. Onlythose microorganisms which, like varicella,can exist in small groups, and those which,like yellow rever vírus, have a non-humanreservoir, are likely to have played a role inthe development of mankind through hismuch longer evolutionary history.
The purpose of this study is to determinewhich of our modem disease agents areable to persist in small, isolated communi-ties. The emphasis has been placed onviruses. because specific, durable serologicreactions more commónly follow vírus in-fection than infection with more complexorganisms, and these have provided ourbest index of past history. For this study, itwas necessary to identify populationgroups sufficiently isolated that viruseswere rarely introduced from the outside.
Island populations have served this pur-pose in the past, but with improved meansof communication, most common virusesare introduced to even the most isolatedislands every few years (6-9). Mufson andassociates (10-12) and Brown and Taylor-Robinson (13) have studied various iso-lated African tribes and found serologicevidence of recent infection with alI but afew of the viruses for which they tested. Incontrast, however, Neel et aI. (14) foundlittle or no influenza antibody in one SouthAmerican Indian tribe and we found noserologic evidence of influenza, measles, ormumps in another such tribe (15). Thepresent report is an extension of our earlierstudy (66) of seven tribes living on the pe-riphery of the lower Amazon basin. Gen-erally, these groups are sufficiently iso-lated to have been protected from manydiseases. They offer a further advantage inthe reconstruction of man's heritage ofdisease, in that they are still hunters andgatherers, as were alI men through mostof their evolutionary history.
When Dane or very few positive serologicreactions were found with a vírus known toinduce a 10ng-lived response, one could nottell whether that vírus was incapable ofmaintaining itself in the community, orwhether the vírus had Dever been intro-duced to the community. However, when ahigh proportion of the population over aspecific age had antibody, while very fewpersons below that age gave specific reac-tiDOS, it was quite certain that the agenthad been introduced but that it had diedout or become inactive since the birth ofthe youngest immune person. Conversely,if high antibody prevalence lates werefound even in very young children, or if theproportion of the immune population in-
INFECTIOUS AGENTS IN ISOLATED HUMAN POPULATIONS 231
threatened destruction of their host populations. Tetanus antibodies werevirtually absent.
Indians, South American; malaria; tetanU$; treponema; tuberculosis; virusdiseases

232
creased steadily with increasing age, onecould be quite confident that the vírus wassuriviving within the community.
POPULATIONS STUDIED AND SPECIMENS USED
The tribes under consideration variedgreatly in size and in the duration of theircontact with civilization (table 1). TheEwarhoyana and Kaxuyana were bothremnants of much larger groups. Thesetribes moved to the Tiriyo village in 1970and 1966, respectively, and it was therethat the specimens were collected (figure1).
The Xikrin tribe split from the Gorotireabout 1900 and was scattered into ~everal8mall groups between 1930 and 1962. TheKuben Kran Kegn represent the productof a later split of the Gorotire, havingseparated in 1936.
The Kaxuyana had had contact with nutcollectors for many years. They had num-bered about 400 persons prior to a severemeasles epidemic in 1924. This epidemicleft only 80 to 90 persons alive, and thetribe has never recovered its numbers. TheXikrin, too, suffered from a series of epi-demics in 1962 and 1963 that reduced theirpopulation from 164 to 86. Measles epi-demics were recorded in Gorotire andKuben Kran Kegn in 1962. A rubellaepidemic occurred in Tiriyo in 1963. Epi-demics characterized as "grippe" had af-fected alI the tribes except, perhaps, theEwarhoyana, for whom our history covereda period of only a few weeks.
The home territory of the Ewarhoyana,Kuben Kran Kegn and Tiryo was savannahcountry with riverine forest belts. Theother tribes lived in continuous tropicalforest. AlI used a slash and burn agricul-ture, with manioc the dominant crop of thenorthem tribes and sweet potatoes mostimportant south of the Amazon. The Goro-tire, Kaxuyana and Kuben Kran Kegnvillages were accessible by river most of theyear, and the Xikrin were accessible. for afew months. Air strips capable of handlinglight planes existed at each village exceptthe Ewarhoyana and Kaxuyana. SeveralIndian Service and missionary personnellived at Gorotire, Kuben Kran Kegn andTiriyo. Single missionaries lived at Mek-ranoti and Xikrin at the time the collec-tions were made.
Specimens available from the Mekranotiand the Xikrin represent essentially thewhole population over one year of age ofthese tribes. The Tiriyo collection includesnearly alI members of the tribe who lived inBrazil, plus a number of young men whovisited from Surinam. The collections fromthe other tribes represent themembers whohappened to be near the central village ona particular day and these collections oftenunder-represented young hunters. Veryyoung children may siso be under-repre-sented in these collections.
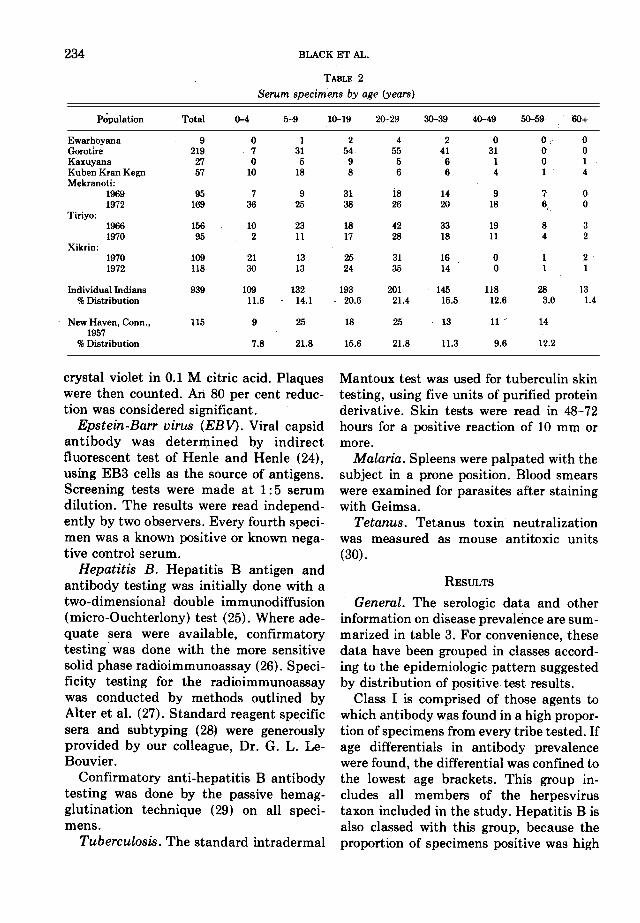
Except for very young children, no spe-cific data on age were available in any ofthese tribes. Age estimates in table 2 arebased on the opinion oftwo or more observ-
Ewarhoyana 14 1970 1970 Carib 16Gorotire 400 1937 1965 Kayapo (Ge) 17Kaxuyana 40 1725 1970 Carib 16KubenKranKegn 300 1955 1970 Kayapo(Ge) 17Mekranoti 190 1958 1969; 1972 Kayapo (Ge) 18Tiriyo 1000 1951 1966; 1970 Carib 19Xikrin 123 1962 1970; 1972 i Kayapo (Ge) 20New Haven, Conn. 250,000 1957 21
Population No. of members Initiation ot f Pteaceful Date of specimen Linguistic group Referencecon ac
BLACK ET AL.
TABLE 1
Populations studied and dates of specimens

233INFECTIOUS AGENTS IN ISOLATED HUMAN POPULATIONS
ers and take into account the estimatedages of the relatives of each individual.
SeTa from Connecticut cities are in-cluded in certain key tests as representa-tive of modero urban communities. TheNew Haven collection was made beforepoliomyelitis, measles, mumps or rubellavaccine were distributed. The sample isbalanced by social class and by age (21).
Herpes simplex. Aplaque reduction testin Vero cells was used with Nahmias' type1 strain E 377 (22) and Gudnadottir's type2 strain X 263 (23). Vírus suspension con-taining 100-200 plaque-forming units per0.1
ml was incubated with equal volumes ofserial serum dilutions for 1 hour at roamtemperature. Two-tenths ml ofthemixturewas placed on drained culture sheets andincubated for 1 hour at 37 C. Cultures werefed with 5 ml Eagle's medium, with 10 percent calí serum and with 0.2 or 1 per centhuman gamma globulin (Merck "Gam-magee") for types 1 and 2, respectively,and were incubated 3 days. They were thendrained and were stained with 1 per cent
METHODS
Serologic methods were as used pre-viou~ly (15) except as noted below. AlItests were quantitative, although only asingle leveI was chosen as the dividing linebetween positive and negative in table 3.
\\, /
('\, ( ATLANTIC.,.--, I '.J '
VENEZUELA ,,' : ,.- (..-/' \-.: (
, ,'- \, GI U I A N A \S--, I ," '"
(', ',// , I (I I "\ \ / I, , -'
\ \ ,--,-/ ""-, ,, " "\ J'Tiriyo ' '.../"
"-,-~--''Ewarhoyono
, Xikrin
't',Gorotire ~
, c(Kuben Kron Kegn ;:)
(O~~...o 100 200 KM
FIGURE 1. Map of a section of northem Brazil indicating home territory of tribes studied.
Mantoux test was used for tuberculin skintesting, using five units of purified proteinderivative. Skin tests were read in 48-72hours for a positive reaction of 10 mm ormore.
Malaria. Spleens were palpated with thesubject in a prone position. Blood smearswere examined for parasites after stainingwith Geimsa.
Tetanus. Tetanus toxin neutralizationwas measured as mouse antitoxic units(30).
RESULTS
General. The serologic data and otherinformation on disease prevalence are sum-marized in table 3. For convenience, thesedata have been grouped in classes accord-ing to the epidemiologic pattern suggestedby distribution of positive test results.
Class I is comprised of those agents towhich antibody was found in a high propor-tion of specimens from every tribe tested. Ifage differentials in antibody prevalencewere found, the differential was confined tothe lowest age brackets. This group in-cludes alI members of the herpesvirustaxon included in the study. Hepatitis B isalso classed with this group, because theproportion of specimens positive was high
crystal violet in 0.1 M citric acid. Plaqueswere then counted. An 80 per cent reduc-tion was considered significant.
Epstein-Barr virus (EBV). Viral capsidantibody was deterI1;lined by indirectfluorescent test of Renle and Renle (24),using EB3 cells as the source of antigens.Screening tests were made at 1:5 serumdilution. The results were read independ-ently by two observers. Every fourth speci-men was a known positive or known nega-tive control serum.
Hepatitis B. Repatitis B antigen andantibody testing was initially done with atwo-dimensional double immunodiffusion(micro-Ouchterlony) test (25). Where ade-quate sela were available, confirmatorytesting was done with the more sensitivesolid phase radioimmunoassay (26). Speci-ficity testing for the radioimmunoassaywas conducted by methods outlined byAlter et aI. (27). Standard reagent specificsela and subtyping (28) were generouslyprovided by our colleague, Dr. G. L. Le-Bouvier.
Confirmatory anti-hepatitis B antibodytesting was done by the passive hemag-glutination technique (29) on alI speci-mens.
Tuberculosis. The standard intradermal
Ewarhoyana 9 O 1 2 4 2 O O OGorotire 219 7 31 54 55 41 31 O OKaxuyana 27 O 5 9 5 6 1 O 1Kuben Kran Kegn 57 10 18 8 6 6 4 1 4Mekranoti:
1969 95 7 9 31 18 14 9 7 O1972 169 36 25 38 26 20 18 6 OTiriyo: c
1966 156 10 23 18 42 33 19 8 31970 95 2 11 17 28 18 11 4 2
Xikrin:1970 109 21 13 25 31 16 O 1 21972 118 30 13 24 35 14 O 1 1
Individual Indians 939 109 132 193 201 145 118 28 13% Distribution 11.6 14.1 -20.6 21.4 15.5 12.6 3.0 1.4
New Haven, Conn., 115 9 25 18 25 13 11 ~ 14
1957% Distribution 7.8 21.8 15.6 21.8 11.3 9.6 12.2
Population Total 0-4 5-9 10-19 20-29 30-39 40-49 50-59 60+
234 BLACK ET AL.
TABLE 2
Serum specimens by age (years)

~
~ ;};; fõ~ ~ ~ ~~~> .
:!§flu o;:;; :9 :9 ~~~ '2 fz z .'" '15 '15 '15 !2 .~
i c;};; ~~'i)~~~~ ~~~~~~"'~QQ~:8:;; =i~~~ ~~~... g ~
-= ~ g.
<] ~ i;j~~~:;;lili §gj!§~~~~~~~~~~ liiliiliilii~ ~~~!:: ] !.!:;3 "'j
f + ~ ~ ...~!;;~ = :~.-~ B 'z <~ .z := Q,
~ o O)O)O)O).!... Z ~ ~ s Q,~NNNN.. ..~o;; .a "a. ~ o:"õ% ~;};; ~ ~ ~§~ Q~~~ ~ i ~].S Q .! j!
~ ~ ~ ~ ~ ~~~ $$$i! ~ :i ~iti ~
~ :;3 ~ ~~~ ~~ Q"'~ .~g ~~~~~ ~~~ ~ ~~.~ ~ .; ~ iE~ ~~ Zo ~~~ gg !;;~~ ~~~ i~~m~ ~~~ ~ .~]~ ~ ~... --
.c >. ~c~ I o o:;) =;:J
:~ ~ ~!::'i)~ ~~ MQ~~~~Q:9QQi~~ !;;~~~~ ~~~Q § ~i
~ ] a]a~ ~ >< ~ s~~~ ~~ ~~~~~a;a;a;a;a;~~~ ~~~~~ ~~~:;; :~ ~~~e 1 ~t
M ~~ c g 5;,
~~ ~Q.H c + ~ 8 CQ QQ"'OQQQ é .~..~ c -o >. ~ ,
111 .-o ~ ..'..-< o... ..: < E-o "O oS ~ ..~ :;
~;S ~ .c "":~ Q. ~ ~ ~~ '... ...O) ~ O) O) O) O) O) ~ O) ~ ~.2 ~ Q,Qjo -..,,"...Q. B .,~~ ~ + ~ O)...MN...~Q...QQ Q ~ a~-c ~ O) ~"""M...'" ..'"..
.c >. o: "cE ~ ..-5.-~ ~ ~ ~ ~~?~~~~~~~ ~ t ~i'. a c e~ oi o ~ ;;~'i)~~Q~ .~~o)M~N~QQ~~~ ~~~g~ ~ ...8. ~ i~ >. r.. .!~...:s U ""'~~ ~ O.~QM~"""'" .~...MMM~~MM"""'" ~~~~Q O) ~ ~ t]Z M~M~~~~ ~...~~~~~~~~ ~ ~ ~ ] ..:c >. ~ ~ ~ ~ ~..' .~ co :..E ...,~..a.. = ~:Jo: ~>'" ..e~~ a:~~ ~~~ ~~QOQQQQQQ QQQQ~ ~ c'""2 :§~'z ~ ~... ;s ~=~ ~ .J ~ ~ ~;~ ~~ ;:J f.: °e,.~ < .,.-'"' ~< o: -< ~>
...~x <Qt~ r.. '>.B~ ZZ~~~:,;~ ~~=~~~~~~~zzz ~~~~! t~~~ ~ ~~
!Q,~ .~ ":=~oP~C-I ~ < f:;3=Q
~~ "'c-IM Q, Q, ~~~"õ~ f: f: ., ~ ~ ~ 5 ~ ~ .5 ~ ]~ ~ ~ Q Eo."""'~c .!!.!!.~ c c c ~ ~ +- ~ .,.~
Z 9'~ ~., Q,Q, > ~ e eo" .E-o
5 a ~ ~ ~~ ccC~<~~"'c-I'" ~ c.; .~+-f.-"c ., ~ ~., > ó' >" ~ o o I'..';; .;; ~ c .~ ,~ ~ ~ ~ ~ ~ ~ ~ " e ~ o! .B +- .B]. ~"3 c w ~ ~~ 11 ~ ~ =i ,~ ,~ 1. ~ a. ~ ~ "ã c c ~ =.~.~'S ~"e" Q, c ~ .1: "
ã. ""C C w .~,~.~ ccc> cc.s -'" > 9.": Q, Q,~ c ~ a c c c ~ " " ".~.~.~ 53 ~ >. >. >. ~ -8.~ -Si~"~~c~"~~"~~~~~~~~õõõ~~~c~oi~~c~~xx~u>~~]~~~~~~~.s~~~~~]><~<E-o~~~~E-o
U U U U
INFECTlOUS AGENTS IN ISOLATED HUMAN POPULATlONS 235

relative to that which has been found withthe same tests in other population groupsand because this high late occurred in alIage categories.
Class 11 agents include the viruses ofmeasles, rubella, mumps, parainfluenza 1,2 and 3, influenza A and B, and poliomyeli-tis. Antibodies to these viruses were eithertotally missing or had very low frequencyin some tribes, but in other tribes showedvery high prevalence lates in persons over aspecific age. We infer that these are viroseswhich were not present prior to introduc-tion from larger communities and whichspread readily when introduced but whichdo not persist in these small communitiesafter a sharp epidemic.
The prevalence of antibodies against thearboviroses varied considerably from onetribe to another, but where the overallprevalence was substantial, a clear agegradient was apparent with increasingprevalence in older people. These virosesinfect forest animaIs as well as man, so thatin examining the human population, welooked at only one portion of this picture.Isolation from other human populationswould not isolate the Indian tribes fromthese viroses. We surmise from the agepattem of antibody that the viroses hadbeen active in these communities at vari-Qus times over the years but not generallyin the form of intense epidemics. They areidentified as Class 111. The distribution ofToxoplasma antibody algo depended on ageand this disease probably algo belongs withthis class.
In Class IV are agents that cause pro-tracted disease with extended infectiousperiods. Resolution of epidemic pattemsfrom available data is difficult because thetime required for the complete epidemiccycle would be proportionally longo Immu-nity to tuberculosis and malaria is notsufficiently solid to prevent reinfection andthe epidemic pattems would be quite dif-ferent from those of the viros diseases.
Tetanus is uniqu~ in that infection with
this agent might involve such a high mor-tality rate that absence of antibody cannotbe taken to indicate that the disease isabsent.
In the section that follows, selected dataon individual diseases are examined withrespect to age and titer distribution.
Class I
Herpes simplex. Herpes simplex type 1antibody was found in a high proportion ofthe sera from alI tribes tested (figure 2). Asnoted by Buddingh in bis study of NewOrleans children (31), few low titers wereencountered; thus minor differences in sen-sitivity of the test have little effect on theproportion recorded positive. The propor-tion of the Indian sera positive was higherfor alI age groups in alI three major tribesthan in our own urban series tested by thesame method or in published series testedby different methods (31, 32). Neverthe-less, there remained a clear relationshipbetween antibody prevalence and age inchildren of the Indian tribes. Fifty per centof the children acquired herpes antibodyby two years of age and 75 per cent byfour years in the Kayapo tribes. It took alittle longer in the Tiriyo.
The distribution of herpes type 2 anti-body was closely correlated with that oftype 1 both by age (table 4) and byindividual specimens. Very few specimensqualified as "type 2" sera by Nahmias'criterion that only sera with higher titeragaipst type 2 than type 1 are clearlyindicative of type 2 infection (22). AI-though most type 2 titers were lowe~ thantype 1 in alI age groups, the difference wassmaller in the older age groups, and manyreli into Nahmias' "Intermediate" class(i.e., type 1 titers O to 3 times the type 2)(table 4). There was no sharp change inprevalence of these relatively high type 2antibody titers after puberty, such asmight be characteristic of an infectionacquired by venereal transmission. It isimpossible to say whether this change in
236 BLACK ET AL.

INFECTIOUS AGENTS I~ ISOLATED HUMAN POPULATIONS 237
tOO ~ -:~~o.o ~;-;-;-,-;-o~--&-;-.-;-;-'""'t1--:'t~ o o o, -.., e--" poo '..~~~ o 'f' " 'o 0,0-.. / e" _ .- ~ I ' o
/I, I ..' I o, o O'"-.'..' '",I&J dI, "o> ' oE I ri'cn oo IQ. 50 p-,-cI&J ...J /
~ 1ct ocn /ILo~
oo tO 20 30 40 50 60
AGE IN YEARS
I Number tested in eoch oge brocket ,
Mekronoti .--~ 24 7 20 8 t9 17 tO 6 ~
Tiriyo e-e 6 2t 7 7 39 3t 16 tO
Xikrin 0""-0 t4 13 7 7 13 6
New Hoven 0-0..0 9 23 6 t2 10 tI 10 tO
FIGURE 2. Prevalence of neutralizing antibody to herpes simplex type 1 in three lndian tribes and one urbanpopulation. ln this and subsequent figures, the number or tests incorporated in each point is given in the tablebelow.
TABLE 4 the data on high risk populations studiedHerpes simplex vírus type 2 neutralizing antibody. by Nahmias (22) and by Rawls (33).
Number tested and percentage o~ type 2 titers within EBV. A previous report (15) indicated1.. 3 01 type 1 tlter that 67 per cent of the Tiriyo had EBV
Ali Indiana NewHaven antibody. At the time those tests wereAge No. % No. % made, this population had one of the
0-4 30 17 9 O highest proportions of positive sela on5-9 27 35 23 O recordo The sensitivity of the method has
10-14 9 46 6 O been substantially increased in the present15-19 14 50 12 O study, and 98 per cent of the Tiriyo were20-29 21 67 21 4.8 found positive. Similar prevalence lates30-39 9 67 10 O ..40+ 14 36 10 20 were found m each of the other tnbes
tested, including the recently contactedEwarhoyana. The percentage EBV anti-
relative titer was the result of superinfec- body nega tive was too small to permittion with type 2 virus of type 1 positive analysis of individual tribes by age, andpersons, or if it simply represents a broad- even after data from the tive tribes wereening of the type 1 response with prolonged pooled, it was doubtful whether any evi-antigenic stimulation. No corresponding dence of tbe age of acquisition of immunitybroadening was observed in the New could be detected (table 5). Overall, 98.3Haven population. The number of interme- per cent of the 291 specimens were re-diate titer ratios was low in New Haven, as corded as positive, but even under twomight be expected from extrapolation from years of age 95 per cent of 19 sela had

Age (years)%+ %+
among remote populations in both Africaand South America has led LeBouvier tosuggest that this may have been the "an-cient subtype" (39).
The increasing antibody prevalence withincreasing age in children, and the rela-tively high incidence of antigen carriage inthe youngest age group suggest early infec-tion and high endemic lates of hepatitis Bin these people. One individual of theXikrin tribe demonstrated antigen pres-ence on both occasions tested, suggestingthe occurrence of chronic carriage and anendemic means of continuance of this in-fection in these groups.
Class 11
Measles. No measles antibody was foundin any member of the Mekranoti whentheir tribe was first tested. The one mem-ber of the Ewarhoyana who was positivewas algo uniquely positive for rubella,mumps and parainfluenza antibody, andthe only member of the three Carib tribeswith Rh negative blood (40). It seemsprobable that this individual had joinedthe tribe from some other group and hadbeen exposed to vírus infections elsewhere.The three Xikrin who had measles anti-body had lived and worked for a time withNeo-Brazilian nut collectors, and the fewTiriyo who had measles antibody were alIyoung adults, the most mobile age group(figure 3). We conclude this pattern indi-cates that measles vírus had never spreadwithin any of these tribes. Infections in-curred outside the tribal territory were notcarried back with the retuming traveler ina state infectious for fellow tribesmen.
The other three tribes tested for measlesantibody alI had high prevalence lates inthe adults and low lates in young children.In Gorotire, specimens were collected 3years after a measles epidemic, and alI butone person over the age of. three years hadantibody. In Kuben Kran Kegn, 10 yearshad elapsed since the last recorded epi-demic, and 80 per cent of the adults but
<2 19 95 126 112-4 37 97 640 195-9 37 97 898 32
10-14 21 100 32 5715-19 39 10020-24 24 96 120 8625-29 36 100 335 8830-39 42 93 517 9140-49 23 96 160 9650+ .13 100
antibody. This remaiJ;ls one of the earliestacquisition rates recorded and is distinctlyaccelerated rei ative to the situation in theConnecticut urban community of Danbury(34).
Cytomegalovirus and varicella. Thecomplement fixation tests for cytomegalo-vírus and varicella do not measure stableantibody (35, 36), so it must be presumedthat many persons who were recorded asnegative had had experíence with the vírusin the pasto
There was a minor inverse relationshipbetween cytomegalovirus antibody preva-lence and age suggestive of waning titersafter infection early in life. No correlationcould be shown with varicella, wherenearly as many children as adults hadantibody. The overall antibody prevalencerates are similar to those observed in openpopulations (37).
Hepatitis B. The results of hepatitis Bantigen and antibody testing are shown intable 6. Rates for both hepatitis B antigenand antibody are higher than those re-ported for industrialized populations, al-though antigen prevalence does not reachthose highest levels previously reported forseveral lndian and tropical populations(38).
Subtyping of antigen positive sera re-vealed only the antigen combination"adw." The finding of this antigen subtype
TABLE 5
Number tested andpercentage of sera positive (+) forEBVantibody by fluorescence test
238 BLACK ET AL.
Ali Indians Danbury, Conn.

~~~~~~~~
..1 11 Çl Çl ~I ~I 9 ç~ 6 o-.~ U8AOH M8N
..ç ç ç 9 ~I ~I U68~UOj~u8qn>l
ç ~I g~ çç gç 11 I --8J!IOJ09
i~ ~ç 69 ~Ol ~L 18 e-e .I. 9 X 'w '3\ '8~~OJq 860 4~08 U! p81181 J8QwnN I
SijW3A NI 39~09 Oç O" Oç O~ 01 O
.~ I .O ~1 o
..iJ .....:,:f Ch o. >
,- j ~ 'C "U..,r
..!TI
'I"U ..O ..Ch
..=iOg "<:o,.. , !TI ,.0.
p ~..",,., ~ ,
I~
c.4,o..I'r .." c
..0 .,.' .I... o.. .../ õ.."-0 '..J 00 I Z
°saq!.I~ u.laq~.l°N WO.lJ ZI sapnl'JuI °a'Juo AluO pa~uno'J lunp!A!pu! awus aq~ uo s-.S3~ ~u3d31{ .
~.9 1~/St 906 9°t EOt E09> Eo9 90S % .IIVEoE E~I/t LI/E 00/1 1~/0 8/0 tI/O EE/O ~L61tOt 89/E 91/6 t~/1 01/0 9/0 8/0 tiO OL61
U!.lll!XE.L 091/11 LE/6 ZE/1 9~/6 11/0 lZ/1 E~/9 !~ouu.lllaw
ua~!~uy9E ~86/601 tOL~ LoLE tOL9 0"9Jr 9°LE 9°~1 % .IIVlE 911/9E Ll/9 EE!OI Ll/61 6/E tl/t 9~/6 ~L61Z~ E9/tl El/6 E~/t 6/E 9/6 8/6 t/1 0L61
U!.i1\!X6E 091/69 LE/61 ZE/91 9~/91 1.1/9 1~/6 ~/E !~ouu.lllaw
Apoq!~uy
+(.: ~~ 6t-g1 .1~1 6~ t~" IIV-(8.lvaÂ) aJy
ÁpoqJ1UO pilo u38J1uO fi BJ1J10d31{ /0 3Ju31on3.ld
9 3111V.L
6E~ SNOLLV"IfidOd NVWfiH 03.LV'lOSI NI S.I.N8DV SfiOIJ.::>uNI
FIGURE 3. Prevalence of measles HI antibody. E, M, X & T represents combined data for tribes with very lowprevalence (Ewarhoyana, Mekranoti, Xikrin and Tiriyo, respectively.)
only two children under 10 years old had studies in island populations (7, 41, 42), weantibody. In Kaxuyana, no history was believe that the measles epidemics com-available, and everyone over the age of 9 monly involve essentially everyone in anyears had measles antibody and no one affected viii age. The unaffected Kubenunder 9 years had antibody. Kran Kegn may have been away at the
On the basis of the high rates in adult time of epidemic. It is algo evident theG.orotire and Kaxuyana and by analogy to vírus does not commonly persist in a latent

infectious form after an epidemic. Childrenbom later remain without their own anti-body to the disease.
Rubella. There was a history of a rubellaepidemic among the Tiriyo in 1962 or 1963.Specimens collected in 1966 and 1970 pro-vided serologic confirmation of this epi-demic and evidence that the vírus was notactive in the community after 1963 (table7). Ninety-three per cent of the specimensfrom persons bom before 1961 had rubellahemagglutination inhibition (HI) anti-body, whereas there was only one uncon-firmed positive titer in specimens fromchildren bom after 1963.
Rubella HI antibody was found in onlyone member of the Xikrin or Mekranotitribes.
Poliovirus. The neutralization test forpoliomyelitis is not altogether type spe-cific; infection with one type sometimesgives antibody to another type (43). There-Core, some positive reactions are to beexpected against types with which therehas been no experience. Furthermore, somelive vaccine had been distributed amongthe Tiriyo making antibody prevalence inthat tribe irrelevant to the present study.
Type 1 poliovirus neutralizing antibodywas found in very few persons of any age inMekranoti, only in persons over the age of
20 in Xikrin (with two exceptions) and,with one exception, only in persons over 12years of age in Kuben Kran Kegn (figure4). This antibody was found in alI KubenKran Kegn 18 years or older, but in onlyhalf the adult Xikrin. Twenty years priorto the date of specimen collections, theXikrin were living in small scatteredgroups, whereas the Kuben Kran Kegnwere in a consolidated village.
Type 2 poliovirus antibody was verywidely distributed in alI age groups of theMekranoti, Xikrin and Kuben Kran Kegn.However, prevalence of this antibody waslow in the Tiriyo and what was found maybe attributable to vaccine-derived immu-nity.
Type 3 poliovirus antibody was absentfrom children under age 5 in Xikrin (withone exception) but was found in older agegroups, including 11 of 13 children aged 5to 9. In Kuben Kran Kegn, the cut-off fortype 3 antibody was about 10 years of age.In Mekranoti, it was prevalent in alI agegroups.
Mumps and parainfluenza. The HI anti-bodies induced by mumps and by theparainfluenza viruses are neither as spe-cific nor as durable as the antibody sys-tems described above. On several occa-sions, paired serum specimens showedboosts in titer against one or another ofthese viruses that were confined to personswho already had detectable antibody (44).Reconstructions of the history of the tribeswith respect to these viruses must, there-Core, be more limited and more tenuous.
Only two of the Mekranoti, the eldestmember of the tribe and one who hadtraveled most widely, had mumps anti-body, and these had only a titer of 1: 10, avalue which may be nonspecific (45). Ti-ters greater than 1: 10 in the Tiriyo collec-tion were confined to sela from personsover 17 years old, and in the Xikrin werelimited to persons over 6 (figure 5). How-ever, even over these ages, the proportionpositive and the average titer of positive
240 BLACK ET ALo
TABLE 7
Number tested and percentage of seTa positive (+) forrubella HI antibody
Danbury. Tiriyot Xikrin andAle Conn.* Mekranoti
No. %+ No. %+ No. %+
1-43 378 ~.2 17 29 16 O3-4 488 32.0
5-95-6 488 37 .37-8379 46.2 19 79 17 O
1~14 80 68 8 100 18 O15-19 17 71 8 100 35 320--29 160 73 46 98 51 O30-39 39 69 26 92 24 O40-49 14 93 11 O50+ 8 88 10 O
* Data from McCollum et ai. (64).t Tiriyo ages a8 of 1966. three years after reported rubella
epidemic.

~
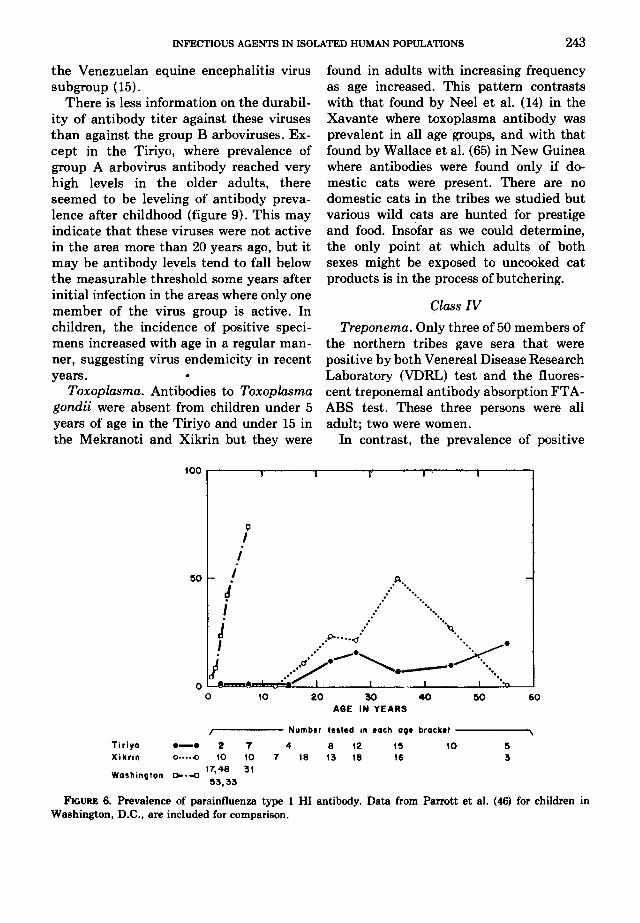
specimens was low relative to that found in assurance when these viruses were lastNew Haven. The number of specimens active in each of these tribes, but it is clearfrom Gorotire children under age 5 was too that the prevalence of antibody is unusu-small to give meaningful data, but the ally low in alI of them. ln contrast to thesedistribution of positive tests and titer in results, Parrott et aI. (46) found that mostolder Gorotire was indistinguishable from children in their Washington, D.C., studythat in New Haven. Most Kuben Kran had neutralizing antibody against theseKegn adults had mumps antibody in mod- viroses by their fourth birthday, and Tay-erate titer and most children did noto lor-Robinson (47) reported 100 per cent of
Parainfluenza 1 antibody was found in adult sera from various countries positivevery few Tiriyo of any age and none under for alI three viruses by the RI testo20 (figure 6). ln the Xikrin, too, there was Influenza. Very few persons had anti-no evidence of parainfluenza 1 under age body to any of the influenza antigens used17, but it was commonly found in persons in our tests. No one had influenza Bof 30 to 40 years. antibody. The fact that influenza A2 was
Parainfluenza 2 was frequently found in slightly more common than Ao confirmsXikrin of alI ages, but was almost entirely the supposition that the tribes have beenabsent from the northem tribes (figure 7). less isolated since 1957 than they wereParainfluenza 3 was present in most Kax- earlier. These results echo similar findingsuyana sera but relatively few Tiriyo or by Neel et aI. in the Xavante lndians oftheXikrin. ln the latter tribes, positive results Mato Grosso who were devoid of influenzawere found at alI ages, but high titers were A2 antibody and had a very low prevalencealmost entirely confined to specimens from of influenza B antibody (14).adults. Smallpox; No pock scars indicative of
lt is not possible to state with any varíola were seen in any member of any
INFECTIOUS AGENTSIN ISOLATED HUMAN POPULATIONS 24.1
z 100 .8 , ",!"",,8 ! 8O ..'i= ..~ ..-J ."Õ ."...cio. .-.o.. .j --' .""D". -'cf- q,... ~ e- -ect ". jc. Li! :
~ 50 :f- .0 :. eO . /Q. : Li! : -J .
Q. :~ :ct :(/) :...:O e !.:;i~ ~~'---"-, ~~A "'---ae O I~;~~~. I -'~-"T-- I -i--~.
O 10 20 30 40 50 60
AGE IN YEARS
, Number lesled in each age brackel \
'Kuben K K 8 8 5 15 6 7 3 4Mekranoli A---A 7 15 6 20 14 12 17 15 4
Xikrin e-e 14 13 7 18 1417 11 8New Haven C-.-C 37 114 95 69 86 108
FIGURE 4. Prevalence of poliovirus type 1 neutralizing antibody.

242 BLACK ET AL
tribe. Vaccinia had not been administeredto the Northern tribes, the Xikrin or theMekranoti.
Class 111
Group B arbovirus. Yellow rever vírusaccounted for most of the Group B ar-bovirus antibody in Tiriyo and Xikrin,although broad group reactionswere com-monly found. Ilhéus HI antibody wassometimes found without antibody to othermembers of the group and may have beenchiefly responsible, with yellow rever forthe group-specific reactions characteristicof multiple infections. Ilhéus was the mostcommonly encountered member of thegroup in Kuben Kran Kegn, Gorotire andMekranoti. Yellow rever HI antibodieswere algo found in a small proportion ofthelatter two tribes, and the specificity ofthese reactions was confirmed by neutral-ization tests. There were no yellow.reverpositive specimens from Kuben KranKegn. Tests for antibody to St. Louisencephalitis and Bussaquera were algo car-
ried out, but specific reactions were notobserved.
Antibody to yellow fever is known to bemaintained for many years without re-exposure (48) and, hence, it is reasonableto assume that the pattems observed rep-resent cumulative life-time histories.There was a steady progression towardincreasing antibody prevalence with in-creasing age in each of the tribes studied(figure 8). There was no evidence of asudden increase in prevalence at any oneage bracket that mighi indicate a majorepidemic in the pasto The curves suggestthat these viroses are endemic as a groupand that the chances that any one personhas encountered them are proportional tobis life span.
Arbovirus group A. Mayaro antibodieswere the most frequently encountered ofthe group A arboviros HI antibodies in alItribes studied. There was some broadeningof the response to include other members ofthe group in Tiriyo. This seemed to beattributable to activity of some memqer of
z 100Oi= .0.,..3 ~ . /\ , ...D.õ k.. .-O' D, t\ '~ 'oo :1" / \ .10'\ ,~ 11 ,~/ \ I, o,~ ;1 \1"\ ". 6LII.1 " )r~_o_D~ 50 ' I \. I- ;n I1O .a. I I .p
OLII d I ..". ..0.0-J .' e'. ..0"a.
I ~L~;~=~;:.."'... 0 o.ooao.o~ o' ..,~ 00cn I p'10. .0. e O 0.0 --e
at O .' e-" e
O 10 20 30 40 50 60
AGE IN YEARS
, Number 'e.'ed in each age bracket \Gorotire b--ó 2 10 22 14 '1 22 14 1I 1I 3Tiriyo e-e 10 22 7 7 16 23 20 12 19 1IXikrin 0 0(} 16 13 25 30 16 3Ne. Haven 0-.-0 9 25 6 12 12 13 13 'I 14
FIGURE 5. Prevalence ar mumps HI antibady.
243INFECTIOUS AGENTS IN ISOLATED HUMAN POPULATIONS
the Venezuelan equine encephalitis vírussubgroup (15).
There is less information on the durabil-ity of antibody titer against these virusesthan against the group B arboviruses. Ex-cept in the Tiriyo, where prevalence ofgroup A arbovirus antibody reached veryhigh levels in the older adults, thereseemed to be leveling of antibody preva-lence after childhood (figure 9). This mayindicate that these viruses were not activein the area more than 20 years ago, but itmay be antibody levels tend to falI belowthe measurable threshold some years afterinitial infection in the areas where only onemember of the vírus group is active. Inchildren, the incidence of positive speci-mens increased with age in a regular man-ner, suggesting vírus endemicity in recentyears. .
Toxoplasma. Antibodies to Toxoplasmagondii were absent floro children under 5years of age in the Tiriyo and under 15 inthe Mekranoti and Xikrin but they were
100
""q.
found in adults with increasing frequencyas age increased. This pattern contrastswith that found by Neel et aI. (14) in theXavante where toxoplasma antibody wasprevalent in alI age groups, and with thatfound by Wallace et aI. (65) in New Guineawhere antibodies were found only if do-mestic cats were present. There are nodomestic cats in the tribes we studied butvarious wild cats are hunted for prestigeand food. Insofar as we could determine,the only point at which adults of bothsexes might be exposed to uncooked catproducts is in the process of butchering.
Class IV
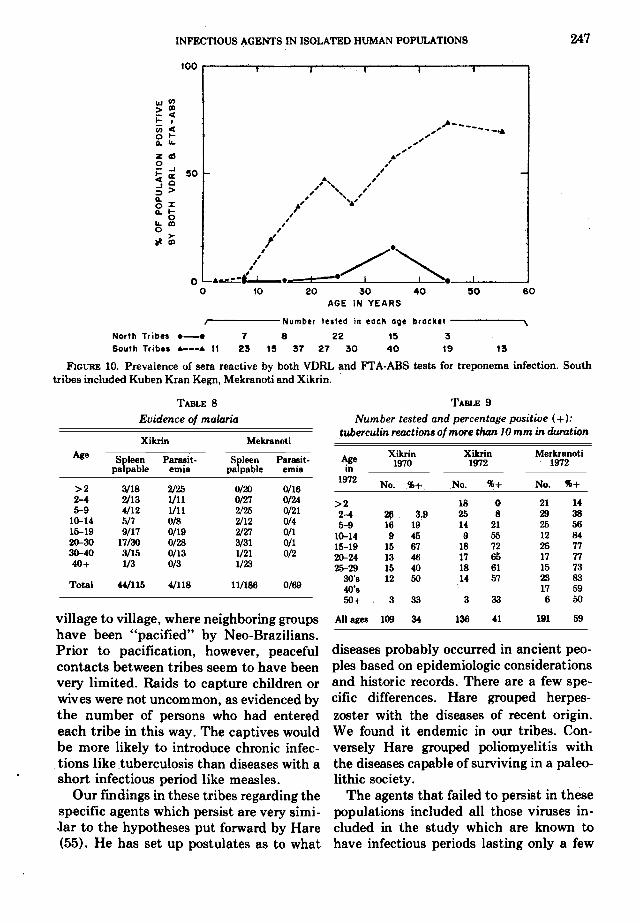
Treponema. Only three of 50 members ofthe northern tribes gave gera that werepositive by both Venere aI Disease ResearchLaboratory (VDRL) test and the fluores-cent treponemal antibody absorption FT A-ABS testo These three persons were alIadult; two were women.
In contrast, the prevalence of positive
tOO
Q
II
50 ! A.I " '.
~ ;' ."'.I ' ".: "..:. "'"J :' ~
p ~' .'.I .' "V '. e
j. '/-;ct"'" e--e,- e"';~<..' "' "
.' '.O' '.
O 10 20 30 40 50 60
AGE IN YEARS
, Number lelled in eoch oQe brocktl ,Tiriyo e-e 2 7 4 8 '2 t5 tO 5Xikrin 0.,...0 10 tO 7 t8 13 18 16 3
17,48 31Wo$hlnQlon 0-.-0
53,33
FIGURE 6. Prevalence of paraintluenza type 1 HI antibody. Data from Parrott et aI. (46) for children inWashington, D.C., are included for comparison.

244' BLACK ET AL.
gera in the southem tribes was very high in 11 instances, but they differed from each(figure 10). In the Xikrin, 35 per cent, in other in 14 instances. Both were negative inthe Mekran<;>ti 54 per cent, and in the two instances. Sixteen of 32 offspring ofKuben Kran Kegn 84 per cent of the adults positive mothers were themselves positive,were positive by both tests. In addition to whereas only 6 of 21 offspring of negativethe specimens that were positive for both mothers were positive for both tests. How-tests, 6.9 per cent of the specimens from ever, there was a strong age correlationthese three tribes were positive by VDRL within the offspring groups, suggestingonly and 12.2 per cent by FI'A only. The that the antibody was acquired years afterVDRL "false positive" tests were usually birth. The familial correlation could not below in titer and they were found most confirmed by comparison of sibs. Physicalfrequently in young children. Malaria may examination revealed no evidence of con-have caused the false positives, although genital syphilis or pinta, and only onethe rate of spleen enlargement was not lesion that might have been caused eitherunusually high in false positive subjects. by yaws or by leishmaniasis.The larger proportion positive by FT A Malaria. Examinations for splenomegalyonly were distributed by age in a pattern were carried out on members of the Xikrinsimilar to reactions by both tests. and Mekranoti at the end of the rainy
The prevalence of treponemal antibody season and blood smears were prepared atin children ofthe southern tribes was much the same time. Parasite positive smearslower than in adults, although positive were found only in young Xikrin, and thereactions by the two tests were noted in four infections encountered were alI Plas-children as young as 9 years of age. There modium falciparum with scant numbers ofwas no correlation of test results between gametocytes. None of these four childrenspouses. Of 27 couples for whom full data had enlarged spleens. However,38 per centare available, both partners were positive of the Xikrin had palpable spleens. Twenty
100
000.0'0
?50 i
~ i, o ..M
,D,,
o ~o 10 20 30 40 50 60
AGE IN YEARS
, Number tested in each age bracket ,Tiriya e-e 2 7 4 8 12 15 10 5
Xikrin 0 <> 10 10 7 18 13 18 16 3
25,48 31WashIngton c-.-c
53,33
FIGURE 7. Prevalence of parainfluenza type 2 HI antibody.

245INFECTIOUS AGENTS IN ISOLATED HUMAN POPULATIONS
of these spleens were characterized aslarge, 12 being at or below the umbilicus.Among the Mekranoti, the spleen lateswere lower and the gizes smaller (table 8).
In the absence of definitive informationabout possible malaria control activities,including both insecticide spraying andantimalarial drug administration, it is notpossible to identify a specific leveI of en-demicity as outlined by the WHO techni-cal committee (49). Antimalarials, includ-ing chloroquine-treated salt, have beenwidely distributed in poorly controlled butnonetheless significant volume.
The detection of parasites only in theyoung, and only gametocytes, coupled witha significant number of large spleens, sug-gests a high degree of malaria endemicityin the Xikrin. The position of the Mek-ranoti is less clear, but malaria, presum-ably present, would appear to be at a lowerleveI of endemicity.
According to the WHO classification(49), these spleen lates indicate that ma-laria is hypoendemic in Mekranoti and
mesoendemic in Xikrin. However, thisclassification presumes the acquisition ofimmunity by adults, and the ability of theSouthem American lndian to develop suf-ficient immunity to prevent splenomegalyis unproved. Neel (14) has suggested thatspleen enlargement rates, such as those ofthe Xikrin which Schaad (50) also found inlndians of Surinam, may represent a muchgreater burden to these people than similarrates in faces who have more resistance tothe disease.
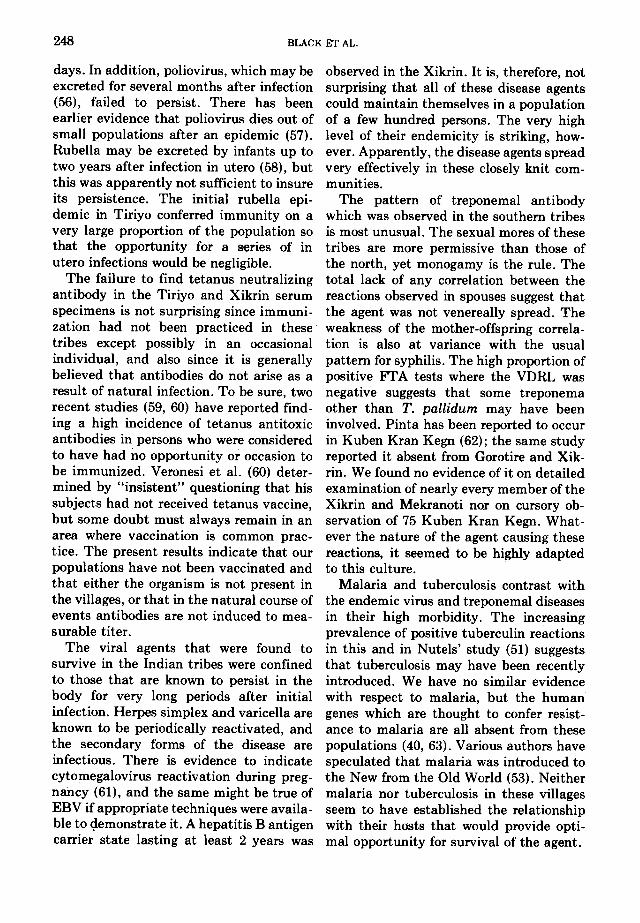
Tuberculosis. Tuberculosis probablyrepresents the most serious immediatethreat to the survival of the lndian tribes.The increasing prevalence of positive tu-berculin reactions and the fact that thehighest rates are found in the teen-agegroup (table 9) sugges.t that this is aninfection which has not yet established anequilibrium with its host. Nutels has dis-cussed this problem in relation to theIndians of the Xingu Park (51, 52), wherehe also found a rapidly increasing propor-tion of tuberculin reactors in serial tests.
100
e
e"~.-o'"-- e ..0.0'
e o..' _&_-- ..h :.0_- :'& ~&.." 0..0'
~-O:' 0050 ,~ 0~. ...&~ ". -",,--.::.~' ' 0_-
~ ..C1 00 .0.. --t~.. '...I ,' ,d
I .0-,I e... ...,~ .""'" .'"", 00.. ~' ;" ,e.. .,-'..0' .,-
...,-O ~-"
O 10 20 30 40 5 60AGE IN YEARS
I Number lested in each age brackel ,Goratire i'---ó 7 33 54 55 41 3'KubenKK.o.ooo.,515 11 8 9 11Mekronoti &---A 44 23 48 36 22 17Tiriyo e-e 25 20 40 49 35 17Xikrin 0 0 30 35 29 8
FIGURE 8. Prevalence of HI antibody to yellow rever or Ilhéus viruso

246 BLACK ET AL.
few infectious diseases. Diseases of softtissues have been studied in Egyptianmummies, but these carne from a relativelyadvanced culturallevel. Polunin has con-sidered contemporary primitive societies inMalaysia as a model for the conditions ofantiquity (54). He has emphasized theimportance of isolation of small groups indetermining disease patterns, but the pop-ulations he studied were less isolated thanthose considered in the present reporto
The fact that many common diseaseshad been absent for very long periods oftime from the tribes we have studied doesby itself prove that the agents causingthem could not have persisted in thesecultures. The absence of any evidence ofsmallpox, for instance, may mean that thevírus evolved since the dispersal of thesepeople from the old world population cen-ters and that it has yet to reach thesetribes. Another possibility to be consideredis a slow movement of these viruses in anarrow stream over a large area so thatintervals appro~mating a life span mightoccur between epidemics in any one tribe.Measles has been observed to spread from
Tetanus. Antibody against tetanus, asmeasured by toxin neutralization in mice,was only found at a low leveI (0.0025 units)in one out of77 persons in two tribes tested.
Filiariasis. The blood smears examinedfor plasmodia were also scanned for filaria-siso None was falindo This is in accordancewith nega tive findings by Schaad in Suri-nam (50) and Neel in the Xavante (14).Approximately one third of 187 specimensexamined were collected after dark, whenWuchereria bancrofti, if present, mighthave been active.
GENERAL DISCUSSION
Populations as primitive and isolated asthose studied in this report are fast disap-pearing and their health status might beconsidered of little lasting consequence.However, until 7000 years ago alI mankindlived in settings sociologically much morelike those of these modern primitive survi-vors than like any cosmopolitan commu-nity. Efforts to reconstruct the environ-ment in which man and his pathogensevolved have been largely dependent onbony remains (53), but these shed light on
100
//---~ 00 o,. &
.' ,.,.&--- --& " ,,,' ", .,.0. ,,';.,. P.. , ' ,-'
, O .,"
..' ,00. O." ,,~, ,.""""O ~ '.. " , "I ...",' "0' -'
O .0. -,. .I o' 00I O ---ó- O'
\ I O': ç..,.." " ---'" 00.00\; .." '00 ~ .0.1'-' " '. 00.I O ~ vi' ." .., , .' "
Ic! " ,I ..
I "I O'I.
OO 10 20 30 40 50 60
AGE IN VEARS
, Number te~ted in eoch oQe brocket ,Gorolire 6--6 7 33 54 55 41 31Kuben KK 8 ,. 15 15 11 8 9 IIMekronoti 44 23 48 36 22 17Tiriyo e-e 25 20 40 49 35 17XikriR 0.'..-0 30 35 29 8
FIGURE 9. Prevalence of HI antibody to Mayaro or Pixuna.
,1',,-No.No.
TABLE 8 TABLE 9
Evidence 01 maioria Number tested and percentage positive (+):...tuberculin reactions 01 more than 10 mm in durotio~
Xlknn MekranotlAge.. .Xikrin Xikrin Merkranoti
Spleen Para.slt- Spleen Par~lt- A..ge 1970 1972 1972palpable emla palpable emla m
1972>2 3/18 2/25 0/20 0/16 No. %+ No. %+ No. %+2-4 2/13 1/11 0/27 0/24 >2 18 O 21 145-9 4/12 1/11 2/25 0/21 2-4 26 3.9 25 8 29 38
10-14 5n 0/8 2/12 0/4 5-9 16 19 14 21 25 5615-19 9/17 0(19 2/27 0/1 10-14 9 45 9 55 12 8420-00 17/00 0/28 3/31 0/1 15-19 15 67 18 72 26 7730-40 3/15 0/13 1/21 0/2 20-24 13 46 17 65 17 7740+ 1/3 0/3 1/23 25-29 15 40 18 61 15 73
OO's 12 50 14 57 23 83Total 44/115 4/118 11/186 0/69 40's 17 59
50+ 3 33 3 33 6 50
village to village, where neighboring groups Ali ages 109 34 136 41 191 59have been "pacified" by Neo-Brazilians.Prior to pacification, however, peaceful diseases probably occurred in ancient peo-contacts between tribes seem to have been pIes based on epidemiologic considerationsvery limited. Raids to capture children or and historic records. There are a few spe-wives were not uncommon, as evidenced by cific differences. Hare grouped herpes-the number of persons who had entered zoster with the diseases of recent originoeach tribe in this way. The captives would We found it endemic in our tribes. Con-be more likely to introduce chronic infec- versely Hare grouped poliomyelitis withtions like .tuberculosis than diseases with a the diseases capable of surviving in a paleo-
.short infectious period like measles. lithic society.Our fmdings in these tribes regarding the The agents that failed to persist in these
specific agents which persist are very simi- populations included alI those viruses m-.lar to the hypotheses put forward by Hare cluded in the study which are known to(55). He has set up postulates as to what have infectious periods lasting only a few
INFECTlOUS AGENTS IN ISOLATED HUMAN POPULATIONS 247
100
1olC/)>aI-<~ I C/) < " o ~ ,
Q. ~ ""z ~ .'
o "i::" ~ so "~o ,."-I > ,,' ,j , ' ,ft , ,-:r ,,-.'o~ I'Q. o '
~ GI "o ,~~ F, .
o ...L +-/ ~.o 10 20 30 40 ~O 60
AGE IN YEARS
,- Number tested in each age brack8' '\
North Tribes .-7 8 22 15 3
South Trib8S 6 11 23 15 37 27 30 40 19 13
FIGURE 10. Prevalence of sela reactive by both VDRL and FT A-ABS tests for treponema infection. Southtribes included Kuben Kran Kegn, Mekranoti and Xikrin.
248 BLACK ET AL.
days. ln addition, poliovirus, which may beexcreted for several months after infection(56), failed to persisto There has beenearlier evidence that poliovirus dies out ofsmall populations after an epidemic (57).Rubella may be excreted by infants up totwo years after infection in utero (58), butthis was apparently not sufficient to insuleits persistence. The initial rubella epi-demic in Tiriyo conferred immunity on avery large proportion of the population sothat the opportunity for a series of inutero infections would be negligible.
The failure to find tetanus neutralizingantibody in the Tiriyo and Xikrin serumspecimens is not surprising since immuni-zation had not been practiced in thesetribes except possibly in an occasionalindividual, and algo since it is generallybelieved that antibodies do not alise as aresult of natural infection. To be Bule, tworecent studies (59, 60) have reported find-ing a high incidence of tetanus antitoxicantibodies in persons who were consideredto have had no opportunity or occasion tobe immunized. Veronesi et aI. (60) deter-mined by "insistent" questioning that bissubjects had not received tetanus vaccine,but some doubt must always remain in anarea where vaccination is common prac-tice. The present results indicate that ourpopulations have not been vaccinated andthat either the organism is not present inthe villages, or that in the natural course ofevents antibodies are not induced to mea-surable titer.
The viral agents that were found tosurvive in the lndian tribes were confinedto those that are known to persist in thebody for very long periods after initialinfection. Herpes simplex and varicella areknown to be periodically reactivated, andthe secondary forms of the disease areinfectious. There is evidence to indicatecytomegalovirus reactivation during preg-nancy (61), and the same might be true ofEBV if appropriate techniques were availa-ble to «;iemonstrate it. A hepatitis B antigencarrier state lasting at least 2 years was
observed in the Xikrin. 1t is, therefore, notsurprising that alI of these disease agentscould maintain themselves in a populationof a few hundred persons. The very highleveI of their endemicity is striking, how-ever. Apparently, the disease agents spreadvery effectively in these closely knit com-munities.
The pattern of treponemal antibodywhich was observed in the southem tribesis most unusual. The sexual mores of thesetribes are more permissive than those ofthe north, yet monogamy is the rule. Thetotal lack of any correlation between thereactions observed in spouses suggest thatthe agent was not venereally spread. Theweakness of the mother-offspring correla-tion is algo at variance with the usualpattem for syphilis. The high proportion ofpositive FI' A tests where the VDRL wasnega tive suggests that some treponemaother than T. pallidum may have beeninvolved. Pinta has been reported to occurin Kuben Kran Kegn (62); the garoe studyreported it absent from Gorotire and Xik-riDo We found no evidence of it on detailedexamination of nearly every member of theXikrin and Mekranoti Dor on cursory ob-servation of 75 Kuben Kran Kegn. What-ever the nature of the agent causing thesereactions, it seemed to be highly adaptedto this culture.
Malaria and tuberculosis contrast withthe endemic virus and treponemal diseasesin their high morbidity. The increasingprevalence of positive tuberculin reactionsin this and in Nutels' study (51) suggeststhat tuberculosis may have been recentlyintroduced. We have no similar evidencewith respect to malaria, but the humangenes which are thought to confer resist-ance to malaria are alI absent from thesepopulations (40, 63). Various authors havespeculated that malaria was introduced tothe New from the Old World (53). Neithermala ria Dor tuberculosis in these villagesse em to have established the relationshipwith their hosts that would provide opti-mal opportunity for survival of the agent.

249INFECTIOUS AGENTS IN ISOLATED HUMAN POPULATIONS
REFERENCF.s1. Panum PL: Observations Made during the Epi-
demic of Measles on the Faroe lslands in the Year1846. New York, American Publishing Associa-tion, 1940
2. Paul JH, Freese HL: An epidemiological andbacteriological study of "common cold" in anisolated Arctic community (Spitzbergen) Am JHyg 17:517-535,1933
3. Hope Simpson RE: Studies on shingles. ls thevirus ordinary chickenpox? Lancet 2: 1299-1302,1954
4. Bartlett MS: The critica! community size formeasles in the United States. J Roy Stat Soc SerA 123:37-44, 1960
5. Black FL: Measles endemicity in insular popula-tions. Critical community size and its evolution-ary implication. J Theor Bio.lll:207-211, 1966
6. Rosen L, Thooris C: Poliomyelitis in FrenchOceania. Epidemiologic observations on an out-break with notes on the incidence of paralysisfollowing intramuscular injections. Am J Hyg57:237-252, 1953
7. Adels NR, Francis JW, Gajdusek DC: Measles inAustralasian indigenes. Am J Dis Child 103:255-260, 1962
8. Brown P, Gajdusek DC, Morris JA: Epidemic A.influenza in isolated Pacific island populationswithout pre-epidemic antibody to influenza vinIstypes A and B, and discovery of other still unex-po,sed populations.. Am J Epidemiol 83:176-188,1966
9. Tyrell DAJ, Feto M; King N: Serologic studies oninfections by respiratory viroses of the inhabi-tants of Tristan da Cunha. J Hyg (Camb)65:327-341, 196710. IIIman D, Mufson MA: Viral antibodies in theKorekore tribe of Northern Rhodesia. Trop GeogrMed 23:64-70, 197111. Anderson N, Mufson MA: Viral antibodies amongthe Turkana people of Northern Kenya. TropGeogr Med 24:168-177,197212. Van Reken D, Mufson MA: Viral antibodies inthe Mano tribe of Northem Liberia. Trop GeogrMed 24:303-310, 1972
13. Brown PK, Taylor-Robinson D: Respiratory vinIsantibodies in sera of persons living in isolatedcommunities. Buli WHO 34:895-900, 1966
14. Neel JV, Salzano FM, Juqueira PC, et ai: Studieson the Xavante lndians of the Brazilian MatoGrosso. Hum Genet 16:52-140, 1964
15. Black FL, Woodall JP, Evans AS, et ai: Preva-lence of antibody against viruses in the.Tiriyo, anisolated Amazon tribe. Am J Epidemiol91:430-438, 1970
16. Frikel P: Os Kaxuyana Nota etnohistoricas.Museu Paraense E Goeldi Belem Publ Avulsas14:1-82, 1972
17. Diniz ES: Os Kayapo-Gorotire. Aspectos socio-
cult~is do momento actual. Boi Mus E GoeldiBelém 18NS:I-40, 1962
18. Rocha FJ da,Salzano FM: Anthropometric stud-ies in Brazilian Kayapo Indians. Am J PhysAnthropol 36:95-101, 1972
19. Frikel P: Fases culturais e aculturacão intertribalno tumucumaque. Boi Mus E Goeldi Belém16NS:I-90, 1961
20. Frikel P: Notas sobre a situacão actual dos índiosXikrin do rio Caetete. Rev Mus Paulista SãoPaulo 14NS:145-158, 1963
21. Niederman JC, Horstmann DM, Opton EM: Asurvey of poliovirus antibody levels in New Ha-ven, Connecticut, 1957-58. Am J Hyg 72:218-230,1960
22. Nahmias AJ, Josey WE, Naib ZM, et ai: Anti-bodies to herpesvirus hominis types 1 and 2 inhumans. I. Patients with genital herpes infec-tions. Am J EpidemioI91:539-546, 1970
23. Gudnadottir M, Helgadottir H, Bjamason D, etai: Vírus isolated from the brain of a patient withmultiple sclerosis. Exp Neurol 9:85-95, 1964
24. Henle G, Henle W: Immunofluorescence in cellsderived from Burkitt's lymphoma. J Bacteriol91:1248-1256, 1966
25. LeBouvier GL, McCollum RW: Australia (hepati-tis associated) antigen: physicochemical and im-munological characteristics. Adv Vírus Dis16:357-396, 1970
26. Ling CM, Overby LR: Prevalenc~ of hepatitis Bvírus antigen as revealed by direct radioimmuneassay with 125I-antibody. J Immunoll09:834-841;1972
27. Alter HJ, Holland PV, Purcell RH, et ai: TheAusria test: critical evaluation of sensitivity andspecificity. Blood 42:947-957,1973
28. LeBouvier GL: The heterogeneity of Australiaantigen. J Infect Dis 123:671-675, 1971
29. Vyas GN, Shulman NR: Hemagglutination assayfor antigen and antibody associated with viralhepatitis. Science 170:332-333, 197030. Clenny AT, Stevens MF: Laboratory contrai oftetanus prophylaxis. J Roy Army Med Corps70:308-310, 1938
31. Buddingh GJ, Schrum DI, Lanier JC, et ai:Studies of the natural history of herpes simplexinfection. Pediatrics 11:595-610, 1953
32. Yoshino K, Kaniguchi S, Furuse R, et ai: Aserological survey for antibodies against herpessimplex vírus with special reference to compara-tively heat-labile complement-fixing antibodies.Jap J Med Sci BioI15:235-247, 1970
33, Rawls WE, Gardner HL, Flanders RW, et ai:Genital herpes in two social groups. Am J ObstetGynecoll00:682-689, 1971 '
34. Nimminitra S: A survey of EBV antibodiesamong healthy children. Thesis for MPH degree,Yale Univ School of Med, 1969
35. Weller TH, Witton HM: The etiologic agents of

reactions, x-ray and bacteriological studies in theKayapo Indians of Brazil. Tubercle 48:195-200,1967
53. Janssens PA: Paleopathology, Diseases and Inju-ries ofPrehistoric mano London, John Baker, 1970
54. Polunin IV: Health and disease in contemporaryprimitive societies. In Diseases in Antiquity.Edited by D Brothwell and AT Sandison. Spring-field, Ill, Charles C Thomas, 1967, pp 69-97
55. Hare R: The antiquity of diseases caused bybacteria and viroses, a review of the problem flOrothe bacteriologist's point of view. In Diseases inAntiquity. Edited by D Brothwell and AT Sandi-sono Springfield, lli, Charles C Thomas, 1967, pp115-131
56. Paul JR: The epideIIiiology of poliomyelitis.WHO Monograph No 26:1955
57. Paul JR, Riordan JT, Melnick JL: Antibodies tothree different antigenic types of poliomyelitisyirus in serum flOro North Alaskan Eskimos. AmJ Hyg 54:275-285, 1951
58. Phillips CA, MelnickJL, Yow MD, et al:Persist-ence of virus in infants with congenital rubellaand in normal infants with a history of maternalrubella. JAMA 193:1027-1029, 1965
59. Vakil BJ, Tulpule TH: A eomparison of 1500 unitsand 5000 units of tetanus antitoxin in simultane-ous active and passive immunization againsttetanus. Indian J Med Res 56:1-14, 1968.
60. Veronesi R, Cecin H, Corres A, et ai: Newapproaches on tetanus immunization: Nàturallyacquired immunity. Preliminary reporto RevHosp Clin 28:313-318, 1973
61. Reynolds DW, Stagno S, Hosty TS, et aI: Mater-nal cytomegalovirus excretion and perinatal in-fections. N Engl JMed 285:1-5, 1973
62. Bellizzi AM: Alguns dados sobre a incidencianosologica nos indios Kayapo. J Brazil Med5:197-211, 1961
63. Salzano FM, Neel JV, Weitkamp LR, et aI:Serum proteins, hemoglobins and erythrocyteenzymes of Brazilian Kayapo Indians. Hum Biol44:443-458, 1972
64. McCollum RW, Randolf MF, Byrne EB,et aI:Antigenic and protective efficacy of live at-tenuated rubella virus vaccine (HPV 77-DE 5)Am J Dis Child 118:186-189, 1969
65. Wallace GD, Zigas V, Gajdusek DC: Toxoplas-mosis and cats in New Guinea. Am J Trop Med
Hyg 23:8-14,197466. Black FL, Hierholzer WJ, Woodall P, et ai: In-
tensified reactions to measles vaccine in unex-posed populations of American Indians. J InfectDis 124:306-317, 1971
varicella and herpes zoster. Serologic studies withthe viruses as propagated in vitro. J Exp Med108:869-890, 1958~. Starr JG, Calafiore, D, Casey HL: Experiencewith a human cytomegalovirus complement-fix-ing antigen. Am J Epidemiol 86:507-512, 1967
37. Wentworth BB, Alexander ER: Seroepidemiologyof infections due to members of herpesvirusgroup. Am J Epidemiol 94:496-507, 1971
38. Blumberg BS, Sutnick AI, London wf: Hepatitisand leukemia: their relation to Australia antigen.BulI NY Acad Med 44:1566-1586, 1968
39. LeBouvier G: The subtypes of hepatitis B anti-gen. Ann Int Med 79:894-896, 1973
40. Salzano FM, Woodall JP, Biack FL, et ai: Bioodgroups, serum proteins and hemogiobins of Bra-zilian Tiriyo Indians. Hum Biol (in press)
41. Christensen PE, Schmidt H, Bang HO, et aI: Anepidemic of measles in southern Greenland.Measles in virgin soil. 11. The epidemic proper.Acta Med Scand 144:430-449, 1952
42. Black FL, Rosen L: Patterns of measles anti-bodies inresidents of Tahiti and- their stability inthe absence of reexposure. J ImmunoI88:725-731,1962
43. Melnick JL, Ramos-Alvarez M, Black FL, et aI:Poliomyelitis viroses in tissue culture. VII. Ex-periences with viral and serological diagnosticprocedures. Yale J Biol Med 26:465-485, 1954
44. Black FL, Woodall JP, Pinheiro FP: Measlesvaccine reactions in a virgin population. Am JEpidemioI89:168-175, 1969
45. Black FL, Houghton WJ: The significance ofmumps hemagglutinin inhibition titers in normalpopulations. Am J EpidemioI85:101-107, 1967
46. Parrott RH, Vargosko AJ, Kim.HW, et aI: Acuterespiratory diseases of viral etiology. 111. Myx-oviruses: parainfluenza. Am J Public Health52:907-917, 1962
47. Taylor-Robinson D: Respiratory virus antibodiesin human serum from different regions of theworid. Buii WHO 32:833-847, 1965
48. Downs WC, Anderson CR, Deipeche KA, et ai:Arthropod-borne encephaiitis virus in the WestIndies ares. 11. A seroiogicai survey of Barbados.West Indian Med J 11:117-122, 1962
49. Covell G, Russeii PF, Sweliengrebei NH: Malariaterminology. WHO Monograph No 13:1953
50. Schaad JDG: Epidemiological observations inbush Negroes and Amerindians in Surinam. TropGeogr Med 12:38-46, 1960
51. Nutels N: Medical problems of newly contactedIndian groups. PAHO Sci PubI165:68-76, 1968
52. Nutels N, Ayres M, Salzano FM: Tuberculin