evolving strategies for immunotherapy: side-effect management
TRANSCRIPT

Oncology Nursing Society 43nd Annual CongressMay 17–20, 2018 • Washington, DC 1Clinical Practice
Rowena Schwartz, PharmD, BCOPAssociate Professor of Pharmacy Practice University of Cincinnati [email protected]
Key Session Takeaways1. Immune checkpoint inhibitors are evolving in the treatment of
many cancers, including in combination with other cancer ther-apies. The adverse event profiles of these agents require consider-ation with the evolution in treatment.
2. Immune checkpoint inhibitors require a coordinated approach to care, as many of the immune-related adverse events (irAEs) are rare. In addition, the more common toxicities (e.g., fatigue) may be overlooked as practitioners focus on irAEs.
3. CAR T-cells are an important therapy in the treatment of cancer. The toxicities of cytokine release syndrome include management of symptoms and, if needed, management of T-cell mediated inflammation.
Evolving Strategies for Immunotherapy: Side-Effect ManagementSaturday, May 19 • 2:45–4 pm
Note one action you’ll take after attending this session: ____________________________________________________
________________________________________________________________________________

ONS 43rd Annual Congress
Clinical Practice 1
Evolving Strategies for Immunotherapy Side Effect Management
Rowena N. Schwartz, PharmD, BCOPUniversity of Cincinnati
Disclosures
• Rowena N. Schwartz, PharmD, BCOP has no disclosures.

ONS 43rd Annual Congress
Clinical Practice 2
Approaching Side Effects of Immunotherapy
• Identification of “important” side effects for immunotherapy– Frequent complications– Severe toxicities
• Development of strategies to identify at-risk individuals• Optimize:
– Patient and caregiver education– Monitoring and identification of toxicity– Management
Approaching Side Effects of Immunotherapy
• Individual agents and/or strategies:– CAR T cell– Vaccines– Immune Checkpoint Inhibitors:
• CTLA-4 Inhibitors (ipilimumab)• PD-1 Inhibitors (nivolumab, pembrolizumab)• PD-L1 inhibitors (atezolizumab, avelumab, durvalumab)
• Combination anticancer therapy including immunotherapy– Immunotherapy + immunotherapy– Immunotherapy + chemotherapy– Immunotherapy + targeted therapy– Impact of radiation– Sequencing of therapy
• Select populations– Disease specific– Patient specific
The Cancer-Immunity Cycle
Chen DS, Mellman I. Immunity 2013

ONS 43rd Annual Congress
Clinical Practice 3
T Cell Activation
●Mapped out the molecular mechanism of T cell recognition, regulation and function
●Blocking negative immune regulators (checkpoints) may give the human immune system the power to fight cancer
Focus on T-cell Activation
Callahan MK, et al. Clinic Dermatology 2013;31:191‐99
Immune Checkpoint Inhibition Strategies
• Cytotoxic T Lymphocyte Antigen 4 inhibition:– Ipilimumab
• PD-1 inhibition:– Nivolumab– Pembrolizumab
• PD-L1 inhibition:– Atezolizumab– Avelumab– Durvalumab
• Combination immune checkpoint inhibition– Ipilimumab + nivolumab
ONS 43rd Annual Congress
Clinical Practice 4
Dual Checkpoint Inhibition
• CTLA-4 and PD-1 have distinct roles in regulating adaptive immunity.• Dual checkpoint inhibition → synergistic activity
Melanoma: Nivolumab + Ipilimumab
• Results:– Objective response in patients with BRAF WT tumors
• Ipilimumab + nivolumab: 61%• Ipilimumab + placebo: 11%
– CR was seen in 22% in the combination arm
Postow MA, et al. N Engl J Med 2015 Postow MA, et al. N Engl J Med 2015
Melanoma: Nivolumab + Ipilimumab
• Hodi FS, et al. Combined nivolumab and ipimumab versus ipilimumab alone in patients with advanced melanoma: 2-year overall survival outcomes in a multicentre, randomized, controlled phase 2 trial. Lancet Oncol 2016;17:1558.
• Wolchok JH, et al. Overall survival with combined nivolumaband ipilimumab in advanced melanoma. N Engl J Med 2017;377:1345.
• Bohensky MA, et al. A cost-effectiveness analysis of nivolumab compared with ipilimumab for the treatment of BRAF wild-type advanced melanoma in Australia. Value Health 2016; 19:1009.

ONS 43rd Annual Congress
Clinical Practice 5
irAE with Checkpoint Inhibitors*
* melanoma* melanoma Rubin KM. CJON 2015;19:709‐717Rubin KM. CJON 2015;19:709‐717
Immune Checkpoint Inhibition: Adverse Events
Weber J, PostowM, Lao C et al.. Oncologist. 2016 Jul 8;21(1)
Avelumab: Merkel Cell Carcinoma
Kaufman HL, et al. Lancet Oncol 2016:17:1374 -85.

ONS 43rd Annual Congress
Clinical Practice 6
Immune Checkpoint Inhibition Strategies
• Cytotoxic T Lymphocyte Antigen 4 inhibition:– Ipilimumab
• PD-1 inhibition:– Nivolumab – Pembrolizumab
• PD-L1 inhibition:– Atezolizumab – Avelumab– Durvalumab
• Combination therapy:– Dual immune checkpoint inhibition: Ipilimumab + nivolumab– Chemotherapy + immunotherapy: carboplatin + pemetrexed + pembrolizumab– Chemotherapy followed by immunotherapy: chemoradiation → durvalumab – Targeted therapy + immune checkpoint inhibitors
ONS Resources for Practitioners
Immune Checkpoint Inhibitor and Immunotherapy: Adverse Effects
Clinical Journal of Oncology Nursing. (2017). Supplement to Vol 21(2).• Reimschissel E, et al. Immunotherapy toxicities: A new electronic documentation template to improve patient care. pg
41-44• Gordon R, et al. Checkpoint inhibitors: Common immune-related adverse events and their management. pg 45-52.• Mistry HE, et al. Toxicity management: Development of a novel and immune-mediated adverse events algorithym. pg
53-59.• Smith LT, et al. Cytokine release syndrome: Inpatient care for side effects of CAR T-cell therapy. pg 29-34.Society for Immunotherapy of Cancer (SITC)• Puzanov I, et al. Managing toxicities associated with immune checkpoint inhibitors: consensus recommendations from
the Society for Immunotherapy of Cancer Toxicity Management Working Group. J Immunotherapy Can 2017;5:95ASCO:• Brahmer JR, et al. Management of immune-related adverse events in patients treated with immune checkpoint
inhibitor therapy: American Society of Clinical Oncology Clinical Practice Guidelines. J Clin Oncol 2018; 36:1

ONS 43rd Annual Congress
Clinical Practice 7
Immune-Related Adverse Effects
• Mechanism: infiltration of “normal” tissue by activated T cells responsible for autoimmunity• Tissues:
– Skin – Gastrointestinal tract– Endocrine glands– Lung– Nervous system– Liver– Kidney– Hematological cells– Musculo-articular system– Heart– Eyes
ASCO Guidelines for Immune Checkpoint Inhibitor Therapy
The Bottom Line:• patient and family caregivers should receive
timely and up-to-date education about immunotherapies
• High level of suspicion that new symptoms are treatment related
ASCO Guidelines for Immune Checkpoint Inhibitor Therapy
The Bottom Line:• Grade 1 toxicities: continue therapy
– Except some neurologic, hematologic and cardiac toxicities• Grade 2 toxicities:
– Consider resuming therapies when toxicities become grade 1 or less– Corticosteroids
• Grade 3 toxicities:– High dose corticosteroids → tapering within 4 – 6 weeks– If needed → infliximab
• Grade 4 toxicities:– May warrant permanent discontinuation of immune checkpoint inhibitor– Exception of endocrinopathies that have been controlled by hormone replacement

ONS 43rd Annual Congress
Clinical Practice 8
Immune Checkpoint Inhibitors: irAE
SKIN• Maculopapular rash• Vitiligo• Psoriasis• Lyell syndrome• DRESS
Immune Checkpoint Inhibitors: irAE
GASTROINTESTINAL TRACT toxicities include:• Enterocolitis• Gastritis• Pancreatitis• Coeliac disease
The challenge of diarrhea with ICI
• Differential: diarrhea vs colitis• Presentation:
– Frequent, watery bowel movements– Abdominal cramping– Blood or mucus in stool– Incidental finding on imaging
• Assessment:– Review of symptom (duration, onset, self-management strategies)– Review of bowel patterns– Review of diet– Review of medications
ONS 43rd Annual Congress
Clinical Practice 9
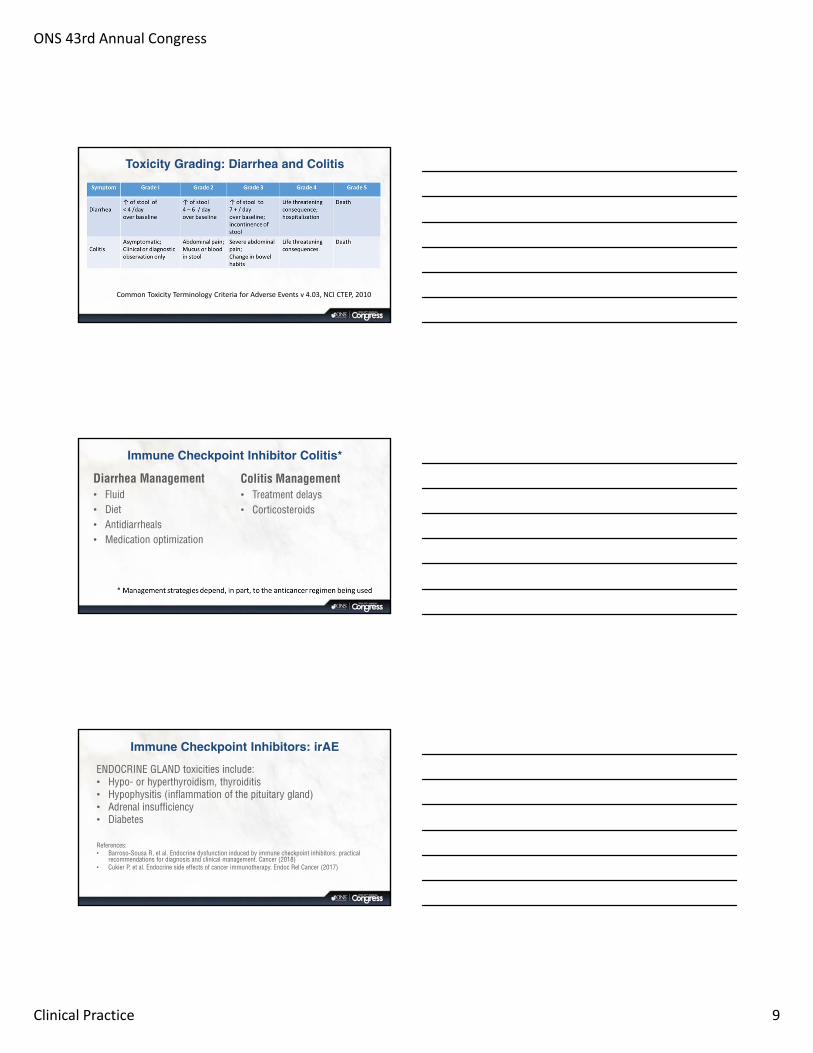
Toxicity Grading: Diarrhea and Colitis
Common Toxicity Terminology Criteria for Adverse Events v 4.03, NCI CTEP, 2010
Immune Checkpoint Inhibitor Colitis*
Colitis Management• Treatment delays • Corticosteroids
Diarrhea Management• Fluid • Diet• Antidiarrheals• Medication optimization
Immune Checkpoint Inhibitors: irAE
ENDOCRINE GLAND toxicities include:• Hypo- or hyperthyroidism, thyroiditis• Hypophysitis (inflammation of the pituitary gland)• Adrenal insufficiency• Diabetes
References:• Barroso-Sousa R, et al. Endocrine dysfunction induced by immune checkpoint inhibitors: practical
recommendations for diagnosis and clinical management. Cancer (2018)• Cukier P, et al. Endocrine side effects of cancer immunotherapy. Endoc Rel Cancer (2017)

ONS 43rd Annual Congress
Clinical Practice 10
Incidence of Endocrine ir-AE with Immune Checkpoint Inhibitors
Cukier P, et al. Endoc Rel Cancer (2017)
Incidence of Endocrine ir-AE with Immune Checkpoint Inhibitors
Cukier P, et al. Endoc Rel Cancer (2017)* Investigational agent as of 2/2018
Immune Checkpoint Inhibitors: Thyroid• Incidence does not appear to be the same for all immune checkpoint inhibitors, but
does appear to increase with combination immune checkpoint inhibitor.• Pathogenesis is thought be due to destructive thyroiditis mediated by cytotoxic T
cells against the thyroid gland• Presentation can vary among patients:
- With monitoring increase in TSH may proceed symptoms- Cases have been reported of thyroid storm or severe hypothyroidism
• Monitoring: TSH, free T4, assessment of pituitary, adrenal, gondal functional status• Management is dependent on diagnosis
- Hypothyroidism → thyroid replacement‐ Thyrotoxicosis → beta blockers may be required (control symptoms)
Barroso‐Sousa R, et al.. Cancer (2018), Cukier P, et al. Endoc Rel Cancer (2017)

ONS 43rd Annual Congress
Clinical Practice 11
Incidence of Thyroid Disease with Immune Checkpoint Inhibitors
Barroso‐Sousa R, et al. Cancer 2018
Immune Checkpoint Inhibitors: Pituitary Gland
Hypophysitis• Incidence does not appear to be the same for all immune checkpoint inhibitors, but
does appear to increase with combination immune checkpoint inhibitor.– Dose related for CTLA-4 inhibitor ipilimumab?
• Pathogenesis → autoimmune based mechanism• Presentation:
- Panhypopituitarism- Isolated anterior pituitary hormone deficiency- Pituitary enlargement
• Monitoring: TSH, free T4• Management is dependent on diagnosis
Barroso‐Sousa R, et al.. Cancer (2018), Cukier P, et al. Endoc Rel Cancer (2017)
Immune Checkpoint Inhibitors: Pituitary GlandClinical presentation of hypophysitis (Ipilimumab):• Central hypothyroidism (>90%)• Hypogonadotropic hypogonadism (>80%)• Central adrenal insufficiency (75%)• Less commonly:
– Diabetes insipidus– Posterior pituitary hormone deficiency (↓ sodium)– Adrenal crisis presenting with hypotension, shock, abdominal or flank
or back pain, fever, anorexia, nausea, vomiting, lethargy, confusion, disorientation, coma, electrolyte disorder.
Faje AT, et al. J Clin Endocrin Metab (2104);99:4078; Joshi MN, et al. Clin Endocrinol (2016);85:331.

ONS 43rd Annual Congress
Clinical Practice 12
Management of Adrenal Insufficiency: Example Approach
* Patient and caregiver education about management of replacement hormone at times of stress
Care of the Individual on Chronic Physiologic Corticosteroids
• Long-term corticosteroid and mineralocorticoid replacement is often required
• Provide patient AND caregiver with instructions (oral and written):– Advising all caregivers and healthcare team members of therapy– Instructions for increasing corticosteroid doses in situations of acute
illness, stress or medical procedures.– Medical alert bracelet – Identification card – Emergency hydrocortisone IM injection kit
Immune Checkpoint Inhibitors: Diabetes
Autoimmune Diabetes Mellitus• Incidence: uncommon• Pathogenesis → autoimmune based mechanism
‐ Destruction of pancreatic β cells mediated by autoreactive T cells‐ Role of PD‐1/PD‐L1 axis in protection against autoimmune DM
• Presentation:- Hyperglycemia- Diabetic ketoacidosis (DKA)- Increased hemoglobin A1c (not seen in all patient suggesting rapid onset)
• Monitoring: glucose• Management is dependent on diagnosis
- Insulin regimen - DKA management if present
Barroso‐Sousa R, et al.. Cancer (2018), Cukier P, et al. Endoc Rel Cancer (2017)

ONS 43rd Annual Congress
Clinical Practice 13
Immune Checkpoint Inhibitors: irAE
KIDNEY toxicities include:• Granulomatous interstitial nephritis• Lupus-like glomerulonephritis
References:• Murakami N, et al. Renal complications of immune checkpoint
blockade. Curr Probl Cancer (217);41:100
Immune Checkpoint Inhibitors : renal irAE• Presentation:
- Asymptomatic - Worsening or new-onset hypertension- Oliguria
• Pathological features:- Acute interstitial nephritis (AIN) pattern on biopsy (± granulomatous features)- Systemic lupus erythematosus like changes- Acute thrombotic microangiopathy
• Monitoring:- Urinalysis - Serum creatinine- Proteinuria (mild)
• Management:- r/o other possible causes of acute kidney injury- Steroids (± response)- Holding immunotherapy (dependent on severity)
Murakami N, et al. Curr Probl Cancer (217);41:100, Perazella M. Kidney Intern (2016); 90:466.
Pathological Features of Acute Kidney Injury (AKI) with Immune Checkpoint Inhibitors in Case Series
Description of 13 individuals with immune checkpoint inhibitors AKI who had kidney biopsy:• Median time to initiation: 91 days (range, 21 – 245 days)• Pyuria present in 8 of 13 patients• Extra renal immune related adverse event occurred prior to AKI in 7 of 13
patients• Prevalent pathologic lesion:
– Acute tubulointerstitial nephritis (12 of 13)• 10 treated with corticosteroids with complete (2) or partial (7) response• 2 patients did not receive corticosteroids and did not respond
Cortazar FB, et al. Kidney International (2016):90:638

ONS 43rd Annual Congress
Clinical Practice 14
Immune Checkpoint Inhibitors : renal irAE
Safety of using immune checkpoint inhibitors in patients with pre-existing renal dysfunction?• Limited data on the use of immune checkpoint inhibitors in
patients with chronic kidney disease (often excluded from clinical trial)
• Dose reduction is not recommended in patients with renal dysfunction
• Role in patients post kidney transplantation?
Immune Checkpoint Inhibitors: irAE
HEART toxicities include:• Pericarditis• Cardiomyopathy• Myocarditis
References:• Heinzerling L, et al. Cardiotoxicity associated with CTLA4 and PD1 blocking immunotherapy. J
Immunother Cancer (2016);4:50.• Varricchi G, et al. Immune checkpoint inhibitors and cardiac toxicity: an emerging issue. Curr Med
Chem (2017)
Immune Checkpoint Inhibitors:Autoimmune Cardiomyopathy
A case report from the literature:• A 72 year old with metastatic melanoma treated with combination of nivolumab +
ipilimumab on clinical trial- PR for 4 months
• At 10th infusion:- dyspnea, edema, ascites and wt gain secondary to decreased EF (~ 50% to 15%)- r/o ischemia and viral infection
• Histopathology:- Hypertrophic myocarditis with interstitial lymphocytes
• Management:- Steroids - Treatment held
• Retreatment:- re-induction of antiPD1 therapy → flare of myocardi s
Tajmir-Riahi A, et al. J Immunother (2018);41:35

ONS 43rd Annual Congress
Clinical Practice 15
Immune Checkpoint Inhibitors: Hepatotoxicity
Retrospective observational study in individuals with melanoma treated between March 2011 – March 2016 that were treated with ipilimumab, nivolumab, pembrolizumab or combination ipilimumab + nivolumab.• Hepatotoxicity → increased LFTs and bilirubin• Onset of hepatotoxicity: median time from first dose 52 days• Clinical presentation: variable, including concurrent other irAE• Management: steroids, discontinuation of therapy (most),
additional immunosuppression
Huffman BM, et al. Am J Clin Oncol (2017)
Immune Checkpoint Inhibitors: irAE
LUNG toxicities include:• Pneumonitis• Pleural effusion• Sarcoidosis
Immune Checkpoint Inhibitors: irAE
NERVOUS SYSTEM toxicities include:• Peripheral neuropathy• Aseptic meningitis• Guillain-Barre syndrome• Encephalopathy• Myelitis• Meningo-radiculo-neuritis• Myasthenia

ONS 43rd Annual Congress
Clinical Practice 16
Immune Checkpoint Inhibitors: irAE
HEMATOLOGIC SYSTEM toxicities include:• Hemolytic anemia• Thrombocytopenia• Neutropenia• Pancytopenia
Immune Checkpoint Inhibitors: irAE
MUSCULO-ARTICULAR SYSTEM toxicities include:• Arthritis• Myopathies
Immune Checkpoint Inhibitors: irAE
EYE toxicities include:• Uveitis• Conjunctivitis• Belpharitis• Retinitis• Choroiditis• Orbital myositis

ONS 43rd Annual Congress
Clinical Practice 17
Immune Checkpoint Inhibitors: Fatigue
• Fatigue is one of the most frequent adverse effect of immune checkpoint inhibitors
• Meta-analysis evaluated fatigue in 17 clinical trials with ipilimumab, pembrolizumab, nivolumab and tremelimumab- Incidence of all grade treatment-associated fatigue ranges from 14 – 42%
- Incidence of high-grade treatment-associated fatigue varied from 1 – 11%- Incidence dependent on a variety of issues including :
- Agent- Dose- Scheduled- Combination vs single agent
Abdel‐Rahman O, et al. Clinical Oncology 2016; 28:e127.
Immune Checkpoint Inhibition Strategies• Cytotoxic T Lymphocyte Antigen 4 inhibition:
– Ipilimumab• PD-1 inhibition:
– Nivolumab– Pembrolizumab
• PD-L1 inhibition:– Atezolizumab– Avelumab– Durvalumab
• Combination therapy:– Ipilimumab + nivolumab– Chemotherapy + immunotherapy: carboplatin + pemetrexed + pembrolizumab– Chemotherapy followed by immunotherapy: chemoradiation → durvalumab – Targeted therapy + immune checkpoint inhibitors
Advanced, non-squamous NSCLC (KEYNOTE-021): Carboplatin + pemetrexed + pembrolizumab
Methods:• Randomized, open-label, phase II cohort of multicohort study (n=123)• Pts stage IIIB or IV non-squamous NSCLC (chemotherapy naïve)• Regimen:
– Pembrolizumab 200 mg IV q 3 wk x 4 → 24 months or placebo– Carboplatin (AUC = 5) IV q 3 x 4 – Pemetrexed 500 mg/m2 IV q 3 weeks → indefinite pemetrexed maintenance
Findings:– Increase objective response to chemotherapy + pembrolizumab vs chemotherapy (estimated treatment
difference of 26%)– Incidence of grade 3 or worse treatment related adverse effects similar
• Impact:– Change in package insert– Inclusion in NCCN guidelines for NSCLC
Langer C, et al. Lancet Oncology 2016; 17: 1497

ONS 43rd Annual Congress
Clinical Practice 18
Durvalumab: Stage III NSCLC• PACIFIC Trial: Phase III placebo controlled trials (n=709)• Interim analysis • Patient Population:
- Individuals with locally advanced, unresectable stage III NSCLC • Methods:
- Patients randomly assigned 2:1 to durvalumab or placebo q 2 weeks for up to 12 months following chemoradiation (1 to 42 days) between 5/2014 – 5/2016
- Primary endpoints: PFS and OS- Secondary endpoints: 12 month PFS, 18 month PFS, ORR, DOR, time to death or distant metastasis, safety
• Results:- Increased median PFS in treatment group- Increase in ORR in treatment group- Increase DOR in treatment group- Increase time to death in treatment group
Antonia SJ, et al. NEJM 2017;377(20):1919‐1929
Durvalumab: Stage III NSCLC
Data cutoff point for interim analysis was feb 13, 2017
Antonia SJ, et al. NEJM 2017;377(20):1919‐1929
Durvalumab: Stage III NSCLC
Antonia SJ, et al. NEJM 2017;377(20):1919‐1929

ONS 43rd Annual Congress
Clinical Practice 19
Durvalumab: Stage III NSCLC
Antonia SJ, et al. NEJM 2017;377(20):1919‐1929
Durvalumab: Stage III NSCLC• Among patients with locally advanced, unresectable NSCLC, PFS was 11
months longer among patients who received durvalumab vs placebo.- Responses were durable- Responses irrespective of baseline expression of PD-L1 on tumor cells- Durvalumab had a favorable effect on frequency of new metastases, including
lower incidence of new brain metastases.• Difference in PFS was seen across all pre-specified groups • Data on OS was immature at time of analysis• Safety profile of durvalumab was consistent with other immune checkpoint
inhibitors– Increased incidence of pneumonitis / radiation pneumonitis in both durvalumab
and placebo group.
Antonia SJ, et al. NEJM 2017;377(20):1919‐1929
Breakthrough Therapy Designation:Combination in Renal Cell Carcinoma
Strategy: multiple receptor TKI + immune checkpoint inhibitor
Clinical Trials: Phase I• Multicenter, open-label Ib/II clinical trial that evaluated the efficacy and safety of
lenvatinib + pembrolizumab in patients with unresectable solid tumors who had disease progression after treatment with approved therapies
• Primary objective: determine MTDPhase II • Combination therapy in patients who had select solid tumors with 0-2 prio lines of
systemic therapy : lenvatinib 20 mg po daily + pembrolizumab 200 mg IV q 3 weeks • Primary objective: Objective response rates at 24 weeks
ONS 43rd Annual Congress
Clinical Practice 20
Immune Checkpoint Inhibitors + PARP Inhibition
Rationale: • Preclinical studies demonstrated DNA damage promotes neoantigens expression• Oral poly (ADP-ribose) polymerase – inhibitors increase DNA damage• Potential that increase DNA damage with PARP inhibitors could increase
mutational burden and expand neoantigens expression leading to greater immune recognition by the tumor.
Clinical trial: • Phase I : Combination of durvalumab + PARP inhibitor and combination of
durvalumab + VEGF inhibitor Lee JM, et al. J Clin Oncol 2017 35;2193
Immune Checkpoint Inhibitors in the Elderly
Rationale for Use• Evidence :
– clinical trials include older patients
– older adults maybe underrepresented in some trials
• Tolerability: – common toxicities of immune
checkpoint inhibitors are mild
Concern about the Use• Efficacy:
– immune checkpoint inhibitors rely on presence of ongoing immune response
– aging associated with decreased effectiveness of the immune system
Daste A, et al. Eur J Cancer (2017); 82:155, Elias R, et al. J Geriat Oncol (2017); 8:229.
Immune Checkpoint Inhibitors: Young vs “Seasoned”
• Meta-analysis and review of nine trials including:– Anti CTLA4 mAb: ipilimumab or tremelimumab– Anti PD-1 mAb: nivolumab or pembrolizumab
Nishijima TF, et al. Cancer Treat Rev (2016);45:30

ONS 43rd Annual Congress
Clinical Practice 21
Immune Checkpoint Inhibitors in Older Adults: Impact of Toxicities
Helissey C, et al. J Geriatric Oncol (2016); 7:325
Anticipating and recognizing potential obstacles…
Immune-Related Adverse Events
Is there a correlation between irAE and efficacy?• NSCLC:
– Small single center prospective observational study (n=38) suggest relationship between irAE and efficacy in NSCLC pts treated with nivolumab.
Sato K, et al. Lung Cancer (2018);115:71.• Solid tumors:
– Single center study retrospective review (n=167) suggest relationship between lymphocyte count and treatment related toxicities and clinical response in patients with solid tumor treated with nivolumab or pembrolizumab.
Diehl A, et al. Oncotarget (2017); 8:114268.

ONS 43rd Annual Congress
Clinical Practice 22
Cell Surface Antigens on B Cell
Tisagenlecleucel (Kymriah)
• CD19-directed genetically modified autologous T cell immunotherapy– Autologous T cells from patients peripheral mononuclear cells
(leukaphereses)– Genetically modified using lentiviral vector to encode an anti-CD19
chimeric antigen receptor (CAR)– CAR is fused to intracellular signaling domains that activate T cells and
enhance response
Goal: Reprogramming a patients own T cells to identify and eliminate CD-19 expressing cells (normal cells + malignant cells)
Tisagenlecleucel (Kymriah)

ONS 43rd Annual Congress
Clinical Practice 23
Tisagenlecleucel: ALLMethods: • Phase II, single-cohort, 25 center, global study• pediatric and young adult patients with CD19+ relapsed or refractory B-cell
ALL (n=75)• Primary endpoint: overall remission rate within 3 monthsResults:• Overall remission rate within 3 months: 81%• Event-free survival: 73% (6 months) → 50% (12 months)• Overall survival: 90% (6 months) → 76% (12 months)• Persistence of tisagenlecleucel in blood was observed for “as long as 20
month”
Maude SL, et al. N Engl J Med (2018); 5:439
Tisagenlecleucel: ALL
Safety
Event Any Time (n=75) ≤ 8 week after infusion (n=75)
> 8 week to 1 year after infusion (n=70)
Adverse event (any grade) 100% 99% 93%
Adverse event believed to be attributed to tisagenlecleucel
95% 92% 43%
Adverse event Grade 3 or 4 88% 83% 44%
Adverse event Grade 3 or 4Believed to be attributed to tisagenlecleucel
73% 69% 17%
Maude SL, et al. N Engl J Med (2018); 5:439

ONS 43rd Annual Congress
Clinical Practice 24
Tisagenlecleucel: ALL
Selected Adverse Events seen within 8 Weeks after tisagenlecleucel infusion
Type of Event Any Grade (n=75) Grade 3 (n=75) Grade 4 (n=75)
Cytokine release syndrome 77% 21% 25%
Neurologic event 40% 13% 0%
Infection 43% 21% 3%
Febrile neutropenia 35% 32% 3%
Cytokine NOT resolving by day 28
37% 16% 16%
Tumor lysis syndrome 4% 4% 0%
Maude SL, et al. N Engl J Med (2018) 378:439
Tisagenlecleucel (Kymriah) • Current indication:
– Treatment of patients up to 25 years with B-cell precursor acute lymphoblastic leukemia that is refractory or in second or later relapse
• Warnings → restricted program – Cytokine release syndrome (CRS)
• tocilizumab– Neurologic toxicities – Infections– Prolonged cytopenias– Hypogammaglobulinemia– Secondary malignancy
CD19-specific CAR T cells: Follow-up• Methods:
– Phase 1 trial in adults with relapsed ALL from MSKCC– Safety and long term outcomes in 53 adults
• Results:– After infusion: CRS in 26% (one death)– CR in 83% patients– Median follow-up of 29 months:
- Median event-free survival was 12.9 months (95% CI, 8.7 – 23.4)- Patients with low disease burden prior to treatment had increased remission
duration and survival- Patient with higher disease burden prior to treatment had increased CRS and
neurologic toxicity and shorter long-term survival.Park JH, et al. N Engl J Med (2018); 378:449.
ONS 43rd Annual Congress
Clinical Practice 25
Axicabtagene ciloleucel (Yescarta)
• Chimeric antigen receptor T cell immunotherapy – Autologous T cells genetically modified to produce a CAR protein– CAR T cells identify and eliminate CD19-expressing normal and malignant cells
Indication:• Treatment of adult patients with relapsed or refractory large B cell
lymphoma after two or more lines of systemic therapy – Diffuse large B-cell lymphoma (DLBCL)– Primary mediastinal large B-cell lymphoma– High-grade B-cell lymphoma– DLBCL arising from follicular lymphoma
Not indicated for the treatment of individuals with primary CNS lymphoma
Axicabtagene Ciloleucel CAR T-Cell in Refractory Large B-Cell Lymphoma
• Methods:– Multicenter Phase 2 trial (n=111)– Pts with DLBCL, primary mediastinal B-cell lymphoma, transformed follicular lymphoma (refractory disease)– Target dose of 2 x 106 anti-CD19 CAR T cells per kg (after conditioning regimen of low dose cyclophosphamide +
fludarabine)– Primary endpoint: ORR
• Results– Axicabtagene ciloleucel was successfully manufactured for 99% pts, administered to 91%– ORR: 82%– CR rate: 54%– OS at 18 months: 52%– Most common adverse effects (grade 3 or higher): neutropenia (78%), anemia (43%), thrombocytopenia (38%)– Cytokine release syndrome (grade 3 or higher): 13%– Neurologic events: 28%
Neelapu SS, et al. NEJM 2017;377:2531
Cytokines

ONS 43rd Annual Congress
Clinical Practice 26
Cytokines
• A large family of low molecular weight soluble proteins involved in the regulating cellular activity and mediates the immune and inflammatory reactions
• Act as messengers within the immune system and between the immune system and other systems of the body
• Some cytokines have direct role in immune defense (e.g. interferon are released by virally infected cells to establish viral resistance)
• Cytokines are produced by many immune cells including mast cells, dendritic cells, macrophages
CAR T-Cell Therapy: Cytokine Release Syndrome
• Cytokine release syndrome (CRS) is group of symptoms resulting from stimulation of T cells → general inflammatory response.
• Presentation:
– Fatigue, myalgia, arthralgia
– Anorexia, nausea, vomiting
– Fever
– Capillary leak syndrome → sequeale
Aldesleukin (rIL2): Toxicity

ONS 43rd Annual Congress
Clinical Practice 27
CAR T-Cell Therapy: Cytokine Release Syndrome
Management:• Goal: symptom management without suppressing CAR T cells• Initial approach: supportive care• Targeting the cause:
– Tocilizumab (Actemra): mAB that targets IL-6 receptor to minimize IL-6 mediated inflammation
– Steroids: blocks T cell activation → inflamma on
Smith LT, Clin J Oncol Nurs (2017); 21 supplement 2:29; Brudno JN, et al. Blood (2016); 127:3321.
CAR T-Cell Therapy: Neurologic Toxicities
• Encephalopathy• Hallucinations• Delirium• Seizures
Key Takeaways• Immune checkpoint inhibitors are rapidly evolving in the
treatment of many cancers, and are now being combined with other cancer therapies.
• Immune checkpoint inhibitors management require a coordinated approach to care.
• CAR T Cells are a new and important therapy in the treatment of cancer.