extensive farming systems
TRANSCRIPT

CONTROL of EAST COAST FEVER and CORRIDOR DISEASE in
EXTENSIVE FARMING SYSTEMS
NICK McHARDY BSc PhD
Global Excellence in Animal Health
Evolution of strategies for the control of ECF and CD
_______________________________________________________
• Up to 1984 - tick control only
• 1984 parvaquone (Clexon) first product to cure ECF and CD
• 1993 buparvaquone (Butalex) single injection, short milk withhold
• 2003 parvaquone + frusemide (Parvexon Plus) for advanced cases
• 2012 ECF vaccine introduced after 40 years’ development
• But the ECF vaccine does not protect against Corridor Disease
• Natural exposure and treatment (NEAT) may protect against ECF and CD
Attitudes and misconceptions re. ECF vaccine and curative drugs
_______________________________________________________
• “Curative drugs are :- toxic, liable to drug resistance, of low efficacy and
very expensive”
• “ECF vaccination can enable substantial cost savings on tick control”
• “One shot of the vaccine is for life”
• “The ECF vaccine is cheaper than treating animals”
• “ECF can kill 30-60% of cattle”
• “No East Coast fever vaccine – no cattle. No cattle – no Maasai”

Picture taken 2011
Many cattle – many Maasai ! •
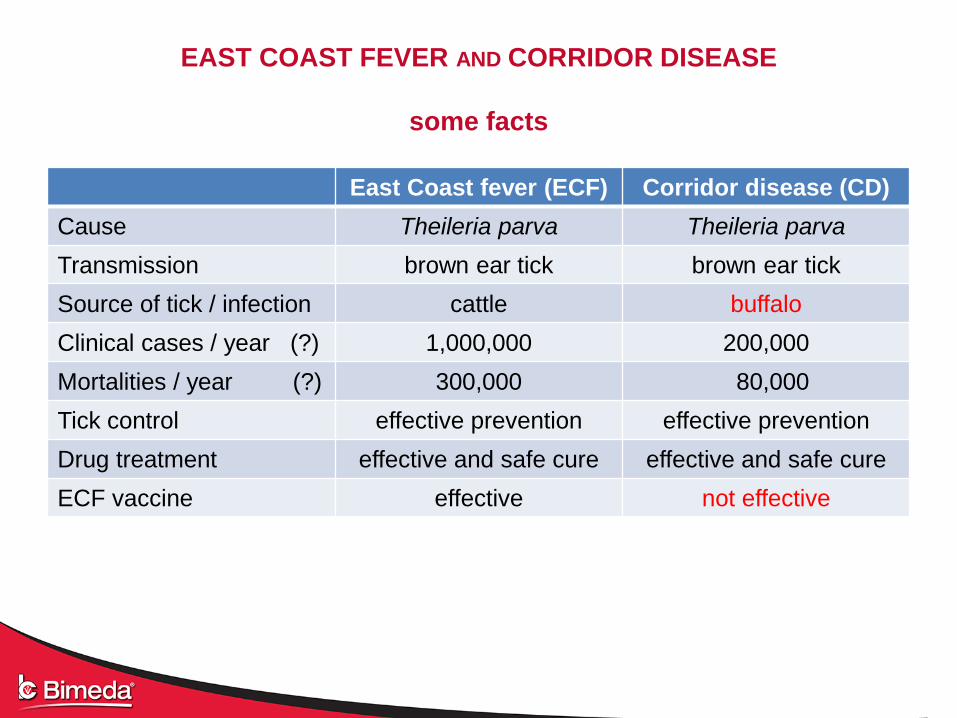
EAST COAST FEVER AND CORRIDOR DISEASE
some facts
East Coast fever (ECF) Corridor disease (CD)
Cause Theileria parva Theileria parva
Transmission brown ear tick brown ear tick
Source of tick / infection cattle buffalo
Clinical cases / year (?) 1,000,000 200,000
Mortalities / year (?) 300,000 80,000
Tick control effective prevention effective prevention
Drug treatment effective and safe cure effective and safe cure
ECF vaccine effective not effective

ECF and CD in extensive farming systems
Considerations
________________________________________________________
• Buffalo presence – always ? sometimes ? Never ???
• Buffalo are not dipped or sprayed
• Buffalo likely to be a constant source of infected ticks
• Buffalo may be the principal source of ticks
• CD therefore likely to be more common than ECF
• ….. but less than 2% of brown ear ticks are likely to carry either CD or ECF
• Dipping may not kill all the ticks all the time
• CD (and ECF) therefore a constant danger
• ….. so, what should be done to minimise the problem ?
Strategy to control CD and ECF in extensive systems
______________________________________________________
• Maintain best possible tick control programme
• Keep constant watch for cases of CD and ECF
….. and other tick-borne diseases
• Treat all observed cases with proven curative drugs
….. and continue to watch for new cases
• Implicitly, if any cases of ECF or CD do occur, tick control has “failed”
….. so review tick control strategy
• Consider - is there any point in using ECF vaccine when CD is present ?

Drugs for treatment of ECF and CD
and concurrent conditions
Active Product Features
parvaquone Parvexon quick-acting, 2 injections*, 1ml / 15kg im,
buparvaquone Buparvex long acting, 1 injection*, 1ml / 20kg im,
short milk withhold (2 days)
parvaquone
+ frusemide
Parvexon Plus best product for advanced cases with
pulmonary oedema
tetracycline Tetroxy LA for concurrent conditions – particularly
anaplasmosis and bacterial infections
(has no direct effect on clinical ECF or CD)

Diagnosis and treatment of ECF and CD
________________________________________________________
• Diagnose early
• Diagnose accurately
• Treat immediately on confirmation of diagnosis
• Treat correctly - give additional injections if clinically indicated
• Consider treatment for concurrent infections – tetracycline, imidocarb
• Nurse carefully, provide water and food, minimise stress
• If response to treatment is poor, review diagnosis

Expected cure rates – ECF and CD
(composite of studies at NVRC Muguga, and elsewhere)
_____________________________________________________
___
No safety issues
Mild Moderate Advanced Advanced (with oedema)
Parvexon near 100% 90% 70-90% 40-50%
Buparvex near 100% 90% 70-90% 40-50%
Parvexon Plus near 100% 90% 70-90% ca. 75%

So …. what is the best strategy to control ECF and CD ?
_______________________________________________________
• Ticks and tick-borne diseases will always be a problem
in extensive farming systems
• An effective tick control strategy is essential
• Some cases of TBDs are likely, no matter how good your tick control
• Effective and safe drugs are available to cure all four of the major TBDs
• Early treatment minimises costs – drug, vet, and production losses
• A reliable diagnostic system and correct treatment will minimise losses
• Is this enough to manage the ECF / CD problem in extensive systems ?
• What else can be done ? ECF vaccine ?

Is the ECF vaccine the answer ? Points to consider
_______________________________________________________
• ECF vaccine only protects against ECF
• It gives no protection against Corridor Disease
• ….. so ECF vaccine has limited value on a farm with CD
• ECF vaccine does not protect against any other tick-borne disease
e.g. redwater, gallsickness, heartwater
• Maintain tick control to prevent these diseases, as well as ECF and CD,
and to prevent damage caused by ticks themselves
• “ECF can kill 30-60% of cattle” – ECF vaccine advert
• …... true, if cattle are not dipped, but cattle are dipped
• …… when cattle are dipped, rarely more than 0-5% cases

Cost comparison
_______________________________________________________
• “The ECF vaccine is cheaper than treating animals” - ECF vaccine advert
• Vaccine cost $10 (???) per animal
• Treatment cost $25-50 depending on weight of animal (including vet. fees)
• But If vaccine is used it must be given to every animal
If vaccine is not used only sick animals have to be treated with drug
• Assume an effective dipping programme, so maximum 5% cases of ECF :-
cost per 100 cattle is :-
• Vaccination $1,000 assumes 100% protection – if not, add treatment costs
• Treatment $250 likely maximum i.e. 5 x 400kg cattle @ $50
(but max. $25 if just one 50kg animal needs treatment !)

Summary – Control of ECF and CD
TINA – “there is no alternative”
________________________________________________________
• Robust tick control programme TINA
• Early and accurate diagnosis of ECF and CD (and other TBDs) TINA
• Correct treatment of ECF and CD (and other TBDs) TINA
If an animal has ECF or CD – treat it immediately !!! TINA
• ECF vaccine - CD absent - perhaps, if many cases of ECF despite dipping
ECF vaccine - CD present - unlikely to be worthwhile
• NEAT - ECF and / or CD present - may be an option when fully tested
Possible NEAT strategy to protect against ECF and CD
(strategy not yet proven)
_____________________________________________________
• Withdraw tick control to allow ticks to transmit ECF and CD
• Observe for attaching ticks
• First ticks likely to attach after about 7 days
• Disease transmission (ECF and / or CD) begins about 2 days later
• “Block” the infection by drug treatment
• Cattle develop immunity to ECF and CD
• Resume tick control
• Continue to observe for new cases, and treat them if necessary
• Look out for other tick-borne diseases too, and treat if necessary
• Some Which drug should be used as the block ?
questions When should the blocking drug be injected ?
How to tell which animals have become immunised ?

Candidate blocking drugs in NEAT system for ECF and CD
tetracycline or buparvaquone
________________________________________________________
TETRACYCLINE 20% or 30%
• Used as block for ECF vaccine
• But effective only if injected immediately after infection
• Infections that are not blocked progress to clinical ECF or CD
• But exact time of infection cannot be known
• Therefore, at least 2 doses must be given to block reliably
BUPARVAQUONE e.g. Buparvex
• Kills all stages of ECF and CD parasites (but does not eradicate infection)
• Effective from a few days before infection, throughout incubation period
and in early clinical stages (and clinical cases, of course)
• Therefore, if tick challenge is “high”, one dose should be effective

When should NEAT blocking drug be given ?
______________________________________________________
TETRACYCLINE 20%, 30%
• Every few days from when first ticks attach and begin to feed until
infection of “all” the animals is “assured”
BUPARVAQUONE (Buparvex)
• Either treat animals individually as each shows first signs
of ECF or CD (i.e. enlarged lymph nodes, raised temperature)
• Or treat the whole group when the first one shows early clinical
signs of ECF or CD
• With both drugs, look out for, and treat, other infections
• …. and for ECF / CD in any animals not infected when block injected

Control of ECF and CD
CONCLUSION_______________________________________________________
• Different strategies will suit different farming systems
• Different strategies will suit individual farms
• Tick control, drugs and vaccine all “work” but none of
them is completely effective on its own
• We should all help farmers to choose and to operate
the best strategy for their farm
THEILERIOSIS – THE DISEASE
--------------------------------------------------------------------------------------------------------------------
CAUSE Theileria parva
TRANSMISSION Brown ear ticks
SYMPTOMS Pyrexia, up to 42º C
Enlarged lymph nodes
Milk yield falls to near zero
Oedema - laboured respiration, bottle jaw,
Frothing at nostrils and mouth
Ocular opacity
Leucopoenia and severe immunodepression
Death, usually 14 – 28 days after infection
IMMUNITY Cured and recovered cattle are strongly immune
----------------------------------------------------------------------------------------------------------------
----

TRIALS CATTLE ON DAY 10, BEFORE CLINICAL SIGNS

SAME CATTLE 5 DAYS LATER, WITH SEVERE ECF

ENLARGED PRESCAPULAR LYMPH NODE

‘BOTTLE-JAW’ OEDEMA

DIAGNOSIS OF CD (and ECF, JD)
Sign CD JD / ECF
Enlarged lymph nodes +++ +++
High fever +++ +++
Oedema, cough etc + +++
Anaemia (++) -
Petechiation ++ +
Lymph smear - lymphoblasts +++ +++
Lymph smear - schizonts - / + + / +++
Blood smear - piroplasms - / + + / +++
Loss of condition +++ (-) +++ (-)
Drop in milk yield +++ +++

LYMPH NODE 7–10 DAYS POST-INFECTION
LYMPHOBLASTS, BUT NO SCHIZONTS, VISIBLE

LYMPH NODE DAY 8-12
FIRST SCHIZONTS IN SOME LYMPHOBLASTS

LYMPH NODE DAY 10-16
MANY SCHIZONTS PRESENT
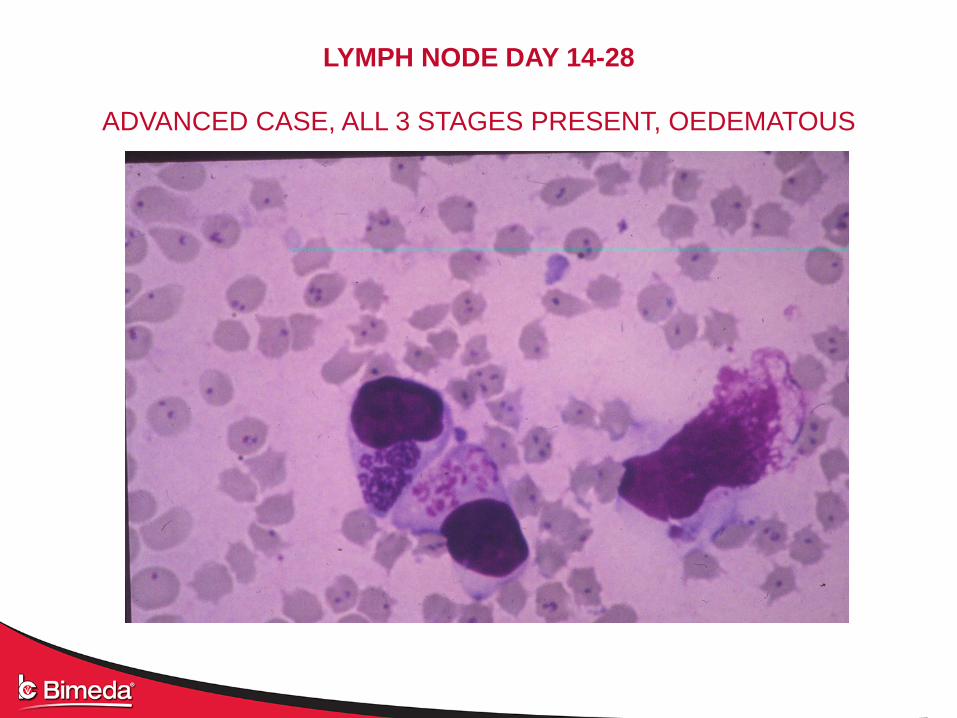
LYMPH NODE DAY 14-28
ADVANCED CASE, ALL 3 STAGES PRESENT, OEDEMATOUS
BUPARVEX---------------------------------------------------------------------------------------------------------------------
• Buparvaquone 50mg / ml
Kills all stages of Theileria
• 1ml / 20kg bodyweight
Inject into neck muscles
• Repeat after 48 – 72 hours, if necessary.
Consider supportive treatment for
anaemia, other infections, etc.
Minimise stress, give plenty of water,
good food, etc.

LYMPH NODE 24-48 H AFTER BUPARVEX TREATMENT

LYMPH NODE 3-4 DAYS AFTER BUPARVEX TREATMENT
Theileria schizonts eliminated, lymphoblasts still present

RESPONSE TO TREATMENT WITH BUPARVEX
• Temperature falls within 1-2 days – if not, re-treat
• Schizonts clearly damaged in 1-2 days, then eliminated
• Piroplasms killed, but remain in eythrocytes for several days
• Anaemia stabilised, then begins slow resolution (CD)
• Body condition improves over several days
• Milk yield increases after a few days
• Some signs may return after 10-20 days, usually do not need treatment

BLOOD SMEAR 1-2 DAYS AFTER BUPARVEX TREATMENT
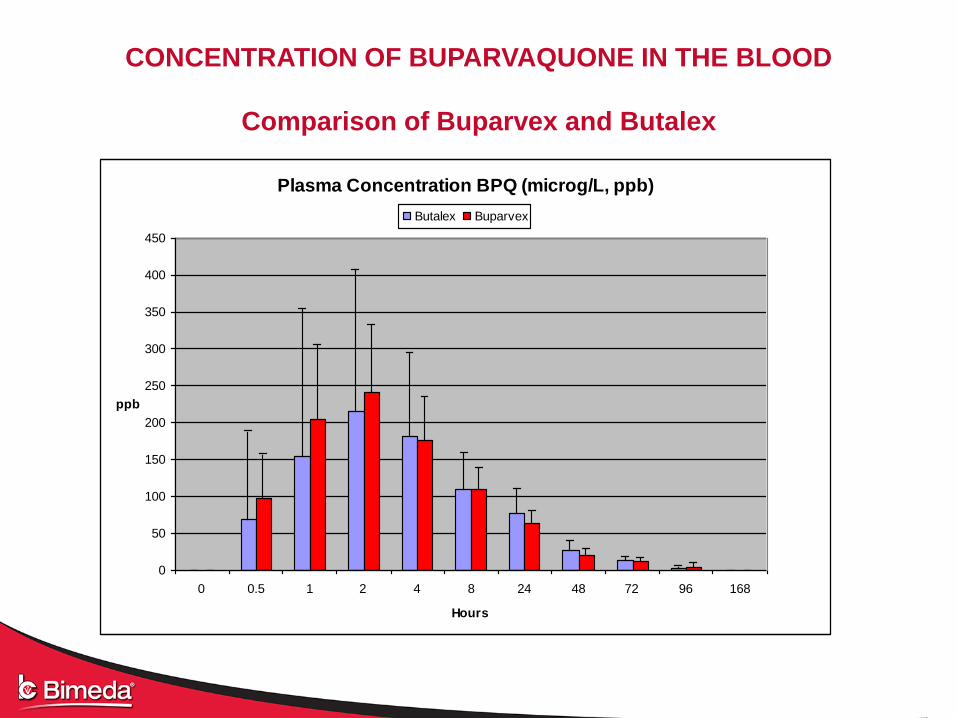
CONCENTRATION OF BUPARVAQUONE IN THE BLOOD
Comparison of Buparvex and Butalex
Plasma Concentration BPQ (microg/L, ppb)
0
50
100
150
200
250
300
350
400
450
0 0.5 1 2 4 8 24 48 72 96 168
Hours
ppb
Butalex Buparvex

MANAGEMENT OF CLINICAL ECF
--------------------------------------------------------------------------------------------------------------------------
• Diagnose early – reduced milk yield, swollen lymph nodes, rising temperature
• Diagnose accurately – if unsure, prepare and examine lymph node and blood smears
• Treat immediately - on positive diagnosis
• Treat correctly – and give repeat injections if necessary
• Diagnose and treat concurrent conditions – due to immunodepression
• Review diagnosis - if recovery is unexpectedly slow
• Give supportive treatment – as necessary for anaemia, anorexia, dehydration, etc.
• Observe the rest of the herd - for signs of theileriosis, and treat if necessary
• Review tick control strategy
--------------------------------------------------------------------------------------------------------------------------
36

INTERCURRENT INFECTIONS IN 100 CASES OF ECF (Theileria parva)
TREATED WITH BUPARVEX, IMIDOCARB or TETROXY LA, as clinically indicated
37
Concurrent
disease(s)
Number
treated
Number
cured
%
cured
Anaplasmosis 10 10 100
Babesiosis 3 3 100
Bacterial - respiratory 29 26 89.5
Bacterial - enteric 12 11 91.5
Anaplasmosis + bacterial 6 5 83.5
TOTAL 60 55 91.5

PARVEXON PLUS“The drug that cures dead cattle” – quote by happy Ugandan farmer.
-------------------------------------------------------------------------------------------------------------------
• Parvaquone 150 mg /ml
- kills all stages of Theileria
Frusemide 55 mg / ml
- resolves oedema
• 1 ml / 15 Kg, intramuscular
injection
- repeat after 48 hours, then
as necessary
• Pulmonary oedema usually
resolved in 1–2 days
- give supportive treatment
as necessary

Independent field trials
Parvexon (PQ) and Parvexon Plus (PQ + frusemide)
to treat advanced ECF, with or without pulmonary oedema
-----------------------------------------------------------------------------------------------------------
Treatment Number of cases Number cured % Cured
-----------------------------------------------------------------------------------------------------------
Advanced cases WITHOUT pulmonary oedema
-----------------------------------------------------------------------------------------------------------
Parvexon 17 17 100
Parvexon Plus 19 17 90
----------------------------------------------------------------------------------------------------------
Advanced cases WITH pulmonary oedema
----------------------------------------------------------------------------------------------------------
Parvexon 22 10 45
Parvexon Plus 28 21 75----------------------------------------------------------------------------------------------------------

TETROXY LA---------------------------------------------------------------------------------------------------------------------
• Oxytetracycline 200mg / ml
Treats intercurrent bacterial infections and anaplasmosis
• 1ml / 10 Kg, intramuscular injection
• Repeat after 2-3 days, if necessary
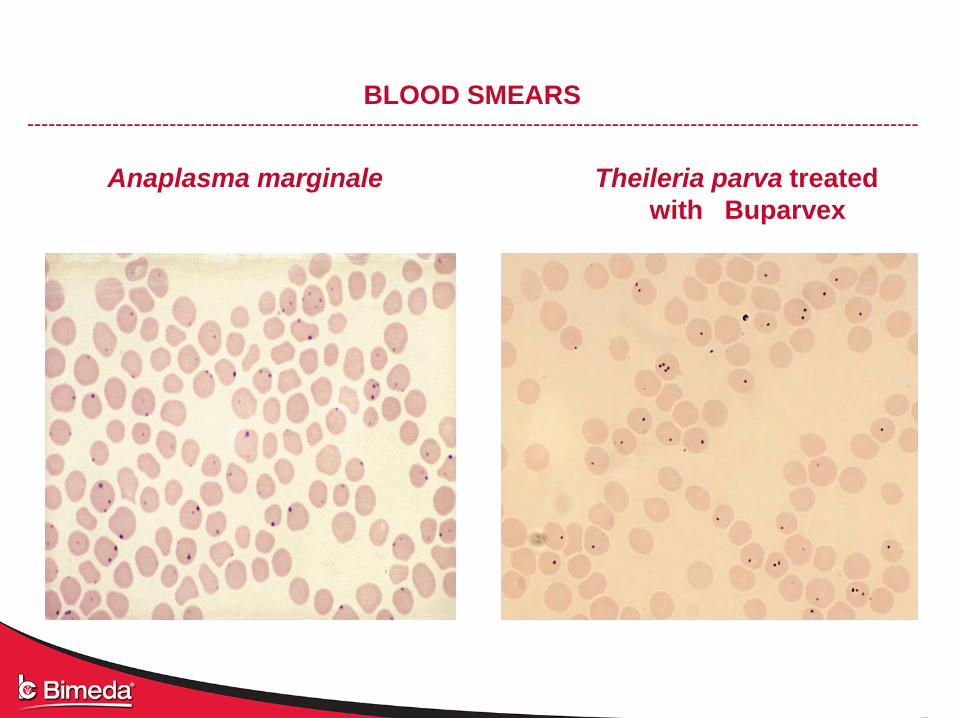
BLOOD SMEARS -----------------------------------------------------------------------------------------------------------------------------
Anaplasma marginale Theileria parva treated
with Buparvex

TOXICITY / SAFETY OF BUPARVAQUONE (BPQ)
---------------------------------------------------------------------------------------------------------------------------
Mode of action On electron transport (energy generation) of Theileria
No effect on electron transport of mammalian cells
---------------------------------------------------------------------------------------------------------------------------
Toxicity Slight inhibition of blood clotting
(BPQ is a distant analogue of vitamin K)
---------------------------------------------------------------------------------------------------------------------------
Therapeutic index Curative dose 2.5 mg / Kg
Minimum toxic dose > 200 mg / Kg
Minimum lethal dose ca. 2000 mg / Kg
---------------------------------------------------------------------------------------------------------------------------

WHY RESISTANCE TO
PARVAQUONE (PQ) AND BUPARVAQUONE (BPQ)
DRUG RESISTANCE IS UNLIKELY IN THEILERIA PARASITES
---------------------------------------------------------------------------------------------------------------------
Method of use PQ and BPQ are used for cure, not prevention, of ECF
on a single occasion. Cured cattle are immune, so
selection pressure for resistance is very low.
---------------------------------------------------------------------------------------------------------------------
Life cycle Theileria life-cycle can take a year or more, but parasites
are exposed to drug for only 3-4 days. So, most of the
cycle, in cattle and tick, is in the absence of drug.
--------------------------------------------------------------------------------------------------------------------
Mode of action PQ and BPQ block two enzymes, one on each branch of
the electron transport chain. The chance of a resistance
mutation occurring to both enzymes at the same time is
very small.
---------------------------------------------------------------------------------------------------------------------
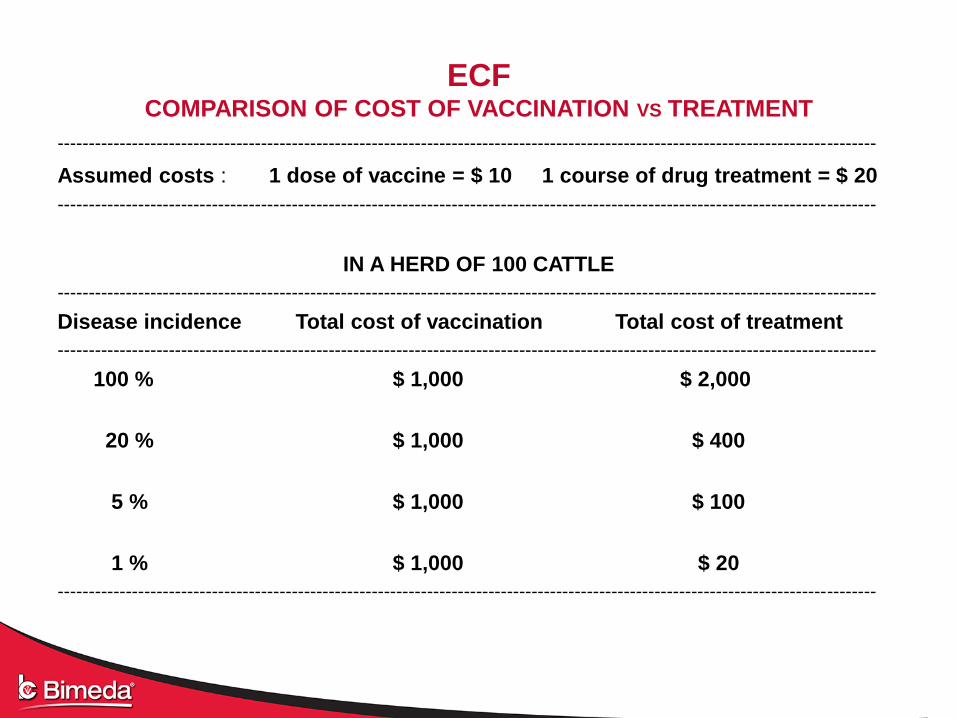
ECFCOMPARISON OF COST OF VACCINATION VS TREATMENT
-------------------------------------------------------------------------------------------------------------------------------------
Assumed costs : 1 dose of vaccine = $ 10 1 course of drug treatment = $ 20
-------------------------------------------------------------------------------------------------------------------------------------
IN A HERD OF 100 CATTLE
-------------------------------------------------------------------------------------------------------------------------------------
Disease incidence Total cost of vaccination Total cost of treatment
-------------------------------------------------------------------------------------------------------------------------------------
100 % $ 1,000 $ 2,000
20 % $ 1,000 $ 400
5 % $ 1,000 $ 100
1 % $ 1,000 $ 20
-------------------------------------------------------------------------------------------------------------------------------------

SUMMARY
DIAGNOSIS AND TREATMENT OF ECF
---------------------------------------------------------------------------------------------------------------------------------------
• Diagnose early - reduced milk yield, swollen lymph nodes, fever
• Diagnose accurately - if unsure, prepare and examine lymph and blood smears
• Treat immediately - on positive diagnosis
• Treat correctly - give repeat injections if necessary
• Diagnose and treat intercurrent diseases - immunodepression
• Review diagnosis - if recovery is slow
• Give supportive treatment - for anaemia, anorexia, dehydration, etc.
• Observe the whole herd - for signs of theileriosis, and treat if necessary
• Review tick control strategy
---------------------------------------------------------------------------------------------------------------------------------------