extradigestive manifestations of gastroesophageal reflux ... · pdf fileextradigestive...
TRANSCRIPT
1
„GRIGORE T. POPA” UNIVERSITY OF MEDICINE AND PHARMACY IAŞI
EXTRADIGESTIVE MANIFESTATIONS OF
GASTROESOPHAGEAL REFLUX DISEASE
Ph. D. Thesis Summary
Scientific coordinator:
Prof. MD. Ph.D. GHEORGHE BĂLAN
Ph. D. Candidate:
OANA-BOGDANA LEONTE (BĂRBOI)
2016

2
3
SUMMARY
LIST OF ABBREVIATIONS……………………………………………………………….i
INTRODUCTION…………………………………………………………………………..ii
GENERAL PART
I. GENERAL INFORMATION. HISTORY. DEFINITIONS 1
II. EPIDEMIOLOGY 3 II.1. Gastroesophageal reflux disease 3
II.2. Gastroesophageal reflux disease with extradigestive manifestations 5
III. ETHIO-PHYSIO-PATHOGENICITY 7
III.1. Physio-pathogenic mechanisms 7
III.1.1. Incompetence of the anti reflux barrier 7
III.1.2. Imbalance between the factors of aggression and defense of the
esophageal lining 9
III.2. Ethio-pathogenic factors 9
III.2.1. Nitric oxide 9
III.2.2. Behavioral factors 9
III.2.3. Helicobacter pylori infection 10
III.2.4. Mental stress 11
III.2.5. Genetic factors 11
III.3. Gastroesophageal reflux disease with extradigestive manifestations 11
III.3.1. Gastroesophageal reflux disease and chronic laryngitis 12
III.3.2. Gastroesophageal reflux disease and chronic cough 12
III.3.3. Gastroesophageal reflux disease and asthma 13
III.3.4. Gastroesophageal reflux disease and dental erosions 13
III.3.5. Gastroesophageal reflux disease and pseudo-angina 13
IV. DIAGNOSIS 13
IV.1. Clinical diagnosis 13
IV.1.1. Gastroesophageal reflux disease and chronic laryngitis 14
IV.1.2. Gastroesophageal reflux disease and asthma 15
IV.1.3. Gastroesophageal reflux disease and chronic cough 15
IV.1.4. Gastroesophageal reflux disease and pseudo-angina 15
IV.1.5. Gastroesophageal reflux disease and dental erosions 16
IV.1.6. Gastroesophageal reflux disease and sleep disorders 16
IV.1.7. Other symptoms 16
IV.1.8. Impaired quality of life 16
IV.2. Para-clinical diagnosis 17
4
IV.2.1. Diagnosis techniques 17
IV.2.2. Gastroesophageal reflux disease and chronic laryngitis 24
IV.2.3. Gastroesophageal reflux disease and asthma 26
IV.2.4. Gastroesophageal reflux disease and chronic cough 27
IV.2.5. Gastroesophageal reflux disease and pseudo-angina 28
IV.2.6. Gastroesophageal reflux disease and dental erosions 29
V. TREATMENT 29
V.1. Lifestyle changes 29
V.2. Medical treatment 30
V.2.1. Antiacids 30
V.2.2. Alginates 30
V.2.3. H2 histamine receptor antagonists 30
V.2.4. Prokinetics 30
V.2.5. Proton pump inhibitors 31
V.2.6. New agents 31
V.3. Endoscopic treatment 32
V.4. Surgery treatment 32
V.5. Treatment of gastroesophageal reflux disease associated with chronic laryngitis 32
V.6 Treatment of gastroesophageal reflux disease associated with asthma 34
V.7 Treatment of gastroesophageal reflux disease associated with chronic cough 35
V.8. Treatment of gastroesophageal reflux disease associated with pseudo-angina 35
V.9. Treatment of gastroesophageal reflux disease associated with dental erosion 36
VI. GASTROESOPHAGEAL REFLUX DISEASE AND ATRIAL FIBRILLATION 36
VI.1. Patho-physiological mechanisms 37
VI.1.1. Sympatico-vagal imbalance 37
VI.1.2. Hiatal hernia 37
VI.1.3. Inflammation 38
VI.1.4. Other possible mechanisms 38
VI.2. Evidence of association between gastroesophageal reflux disease and atrial
fibrillation 38
VI.3. Treatment of gastroesophageal reflux disease associated with atrial fibrillation 39
PERSONAL CONTRIBUTION
VII. PERSONAL RESEARCH MOTIVATION. STRUCTURE OF THE PERSONAL
STUDY. GENERAL OBJECTIVES 40
VIII. EVALUATION OF PATIENTS WITH CHRONIC LARYNGITIS
WITH AN ETHIOLOGIC POTENTIAL OF GASTRO ESOPHAGEAL REFLUX
DISEASE 42
VIII.1. Purpose 42
VIII.2. Material and Method 42
VIII.2.1. Patients 42
VIII.2.2. Study protocol 43

5
VIII.2.3. Statistical processing 46
VIII.3. Results 47
VIII.4. Discussions 80
VIII.5. Conclusions 93
IX. EVALUATION OF PATIENTS WITH ASTHMA WITH AN ETHIOLOGIC
POTENTIAL OF GASTRO ESOPHAGEAL REFLUX DISEASE 95
IX.1. Purpose 95
IX.2. Material and Method 95
IX.2.1. Patients 95
IX.2.2. Study protocol 96
IX.2.3. Statistical processing 97
IX.3. Results 97
IX.4. Discussions 127
IX.5. Conclusions 136
X. EVALUATION OF PATIENTS WITH CHRONIC COUGH WITH AN
ETHIOLOGIC POTENTIAL OF GASTRO ESOPHAGEAL REFLUX DISEASE 138
X.1. Purpose 138
X.2. Material and Method 138
X.2.1. Patients 138
X.2.2. Study protocol 138
X.2.3. Statistical processing 139
X.3. Results 139
X.4. Discussions 167
X.5. Conclusions 175
XI. COMPARATIVE EVALUATION OF EXTRA DIGESTIVE
MANIFESTATIONS POSSIBLY INDUCED BY GASTROESOPHAGEAL
REFLUX DISEASE 176
XI.1. Purpose 176
XI.2. Material and Method 176
XI.3. Results 176
XI.4. Discussions 183
XI.5. Conclusions 185
XII. GASTRO ESOPHAGEAL REFLUX DISEASE AND ATRIAL FIBRILLATION 186
XII.1. Purpose 186
XII.2. Material and Method 186
XII.2.1. Patients 186
XII.2.2. Study protocol 187
XII.2.3. Statistical analysis 188
XII.3. Results 188
XII.4. Discussions 202
XII.5. Conclusions 206
6
XIII. DIFFICULTIES AND LIMITATIONS OF RESEARCH 208
XIV. ORIGINALITY OF THE STUDY 208
XV. PERSPECTIVES OPEN BY PERSONAL RESEARCH AND FUTURE
DIRECTIONS OF STUDY 209
XVI. GENERAL CONCLUSIONS
211
XVII. BIBLIOGRAPHIC REFERENCES 212
7
LIST OF ABBREVIATIONS
BA – bronchitis asthma
Ao - aorta
LA - left atrium
CVA – cerebrovascular stroke
PAD - peripheral arterial disease
CAD - coronary artery disease
GERD – gastroesophageal reflux disease
CRP - C-reactive protein
SD - standard deviation
DM – diabetes mellitus
E - velocity peak of the early diastolic filling wave of the mitral flow
Ea – early diastolic velocity peak of the mitral ring longitudinal movement
EB – Barrett esophagus
UGE - upper gastrointestinal endoscopy
AF - atrial fibrillation
H pylori - Helicobacter pylori
HH - hiatal hernia
AHT – arterial hypertension
MII-pH - multichannel intra-luminal pH- impedance
PPI - proton pump inhibitors
LA - Los Angeles classification of esophagitis
LF / HF - ratio of low frequency / high frequency power
ENT - ear, nose and throat
proBNP - B-type natriuretic peptide
LFR – laryngopharyngeal reflux
SR - sinus rhythm
SAP - symptom association probability
SDNN - standard deviation of the mean of all ranges of normal R-R in 24 hours
SI - symptom index
VRR - R-R variability
8
INTRODUCTION
The gastroesophageal reflux disease (GERD) is a chronic complex clinical condition,
which is also recurrent, multi-factorial, with risk of complications and a significant morbidity
level.
The gastroesophageal reflux disease has become undoubtedly the most commonly
diagnosed disease by the gastroenterologist in the specialized ambulatory care, being one of the
most common diseases of modern civilization. It is considered that GERD negatively affects the
patient’s quality of life as much as osteoarthritis or acute coronary events, representing a public
health problem, with important socio-economic and psychological impact. In many cases,
requiring long-term therapy, this pathology involves periods of absenteeism, repeated
hospitalizations, explorations and costly treatments, unnecessarily burdening the health system
budget.
The gastroesophageal reflux disease with extradigestive manifestations remains a
controversial issue in terms of epidemiology, diagnosis and treatment, the literature on this
pathology being contradictory. GERD with extradigestive manifestations remains an important
issue for diagnosis and treatment for both gastroenterologists and other physicians: ENT,
cardiology, pulmonology, dentistry, as evidenced by the growing number of patients with
suspected reflux disease who are referred to Gastroenterologists from these services. Numerous
articles published in international medical literature devoted to this subject reflect growing
concerns over scientific researchers of this pathology, still incompletely understood.
Since GERD has become in recent decades one of the most widespread diseases in the
world, an algorithm for diagnosis and treatment must be unanimously accepted immediately.
Despite a wide range of diagnostic tests available, none is so far considered "gold standard" in
the diagnosis of GERD with extradigestive manifestations, making it difficult for clinicians.
The doctoral thesis contains a number of 171 figures, 52 tables and 529 references. The
thesis summary retains the original numbering of the chapters and subchapters, as well as figures
and tables.
9
GENERAL PART
I. GENERAL INFORMATION. HISTORY. DEFINITIONS
This chapter provides general information related to GERD, a brief history of the
evolution of this pathology over time and definitions that have been issued by experts in recent
decades to describe GERD or GERD with extradigestive manifestations.
II. EPIDEMIOLOGY
This chapter reveals epidemiological data known to date, in the medical international and
national literature on GERD, with and without extradigestive manifestations.
III. ETHIO-PHYSIO-PATHOGENICITY
This chapter addresses the patho-physiological mechanisms and etiologic factors
involved in triggering GERD.
IV. DIAGNOSIS
This chapter addresses, according to literature, the role of clinical symptoms in the
diagnosis of GERD with extradigestive manifestations, as well as the contribution of the latest
laboratory techniques for obtaining a proper diagnosis.
V. TREATMENT
Chapter V presents the principles of treatment used in GERD with extradigestive
manifestations and the response to various therapies of patients presenting associations of GERD
with chronic laryngitis, asthma, chronic cough, pseudo-angina, erosions dental, according to the
latest studies published in literature.
VI. GASTRO ESOPHAGEAL REFLUX DISEASE AND ATRIAL
FIBRILLATION
The chapter analyses the most relevant and current scientific evidence on the association
between GERD and atrial fibrillation (AF) in terms of epidemiology, diagnosis and treatment.
10
PERSONAL CONTRIBUTION
VII. PERSONAL RESEARCH MOTIVATION
GERD has progressed in the last decades from a seemingly trivial disease status to a
prevalent disease, dominating today the pathology diagnosed in the gastroenterology ambulatory
care.
Increasing prevalence could be explained by the increased medical interest and by the
degree of recognition of GERD with extradigestive manifestations, not only of the
gastroenterology specialists, but also by other physicians, and also by the increased accuracy and
availability of diagnosis methods.
As a disease of modern civilization, GERD has become a public health problem, with
socio-economic and psychological implications, in that it adversely affects the quality of life of
the working population, generating periods of absenteeism from work, with lower work
productivity. Repeated need healthcare, costly explorations conducted in order to establish the
correct diagnosis or testing multiple therapies to achieve disease symptom resolution generate
high costs, which are detrimental to the health system budget.
Although this topic is widely discussed in international medical literature, the
epidemiology, diagnosis and treatment of GERD with extradigestive manifestations remain
controversial; moreover, in Romania, the existing data so far are limited. The lack of a
standardized national protocol for diagnosis and treatment, and the diagnosis methods with, often
exceeded, which are available in health centers in our country, make the task of clinicians more
difficult.
Starting from these premises and with the help of the data in literature, I decided to
evaluate prospectively the association between GERD and certain extradigestive manifestations
(chronic laryngitis, chronic cough and asthma) and to analyze the possibility of grouping atrial
fibrillation as an extradigestive manifestation of GERD.
STRUCTURE OF THE PERSONAL STUDY
The thesis section dedicated to personal contribution included five studies, with the first
four studies pursuing the same objectives and the same study protocol, while the fifth study has
different research objectives and a different protocol.
GENERAL OBJECTIVES
The main objectives of this doctoral research were as follows:
assessment of the association between GERD and chronic laryngitis, asthma, chronic
cough
assessment of the usefulness of Gastrointestinal investigations in patients showing extra
digestive manifestations (chronic laryngitis, asthma and chronic cough) possibly induced
by GERD
11
evaluation of the effect of treatment with proton pump inhibitors on extradigestive
manifestations (chronic laryngitis, asthma, chronic cough) with a potential GERD
etiology
assessing the relationship between GERD and paroxysmal non-valvular atrial fibrillation
and verifying the possibility of classification of atrial fibrillation as an extradigestive
manifestation of GERD.
The secondary objectives were represented by:
determining the demographic, clinical, biological and endoscopic characteristics of
patients that associate GERD with chronic laryngitis, bronchitis asthma poorly controlled
therapeutically, chronic cough, and paroxysmal non-valvular atrial fibrillation and
analyzing the correlations between them
assessment of the risk factors involved in the association between GERD and chronic
laryngitis, asthma, chronic cough or paroxysmal non-valvular atrial fibrillation
research on the impact of GERD associated with chronic laryngitis, asthma or chronic
cough, on sleep and daily activities of patients
assessment of the structural, electrical and mechanical remodeling of the left atrium in
patients with GERD and atrial fibrillation.
Ethical considerations
All patients enrolled in the study have expressed verbal and written informed consent for
participation in the study, after they were explained the details regarding the purpose and
methodology of the study, the risks and benefits involved in the study and after they were offered
information on the confidential results. The present doctoral study was approved by the Ethics
Committee of "Grigore T. Popa" University of Medicine and Pharmacy and the Ethics
Committee of "Sf. Spiridon" Hospital.
VIII. EVALUATION OF PATIENTS WITH CHRONIC LARYNGITIS
WITH AN ETHIOLOGIC POTENTIAL OF GASTROESOPHAGEAL
REFLUX DISEASE

12
VIII.1. The aim of this study was to evaluate the association between GERD and chronic
laryngitis.
VIII.2. MATERIAL AND METHOD
VIII.2.1. Patients
We conducted a prospective case-control study over a period of 37 months (November 1,
2012 - November 30, 2015) at the Institute of Gastroenterology and Hepatology of "St. Spiridon"
Hospital, in collaboration with the ENT Clinic of "St. Spiridon" Hospital in Iaşi.
Inclusion criteria:
patients older than 18 who have signed the informed consent
patients diagnosed with chronic laryngitis and suggestive lesions of GERD in ENT
examination:
edema and erythema of the posterior commissure - arytenoids and the
interarytenoid area
edema and erythema of the posterior pharyngeal wall
arytenoidian granuloma
diffuse congestion of the endolarynx or of the vocal cords.
Exclusion criteria:
refusal from patient/uncooperative patient/patient with documented psychiatric
pathology
presence of laryngeal formations or other ENT injuries that may explain laryngitis
oropharyngeal infections of bacterial, viral or fungal causes
history of laryngeal surgery or oro-tracheal intubation maneuvers
chronic exposure to toxic or allergic environmental factors
patients with alarm symptoms (unexplained weight loss, upper gastrointestinal bleeding,
dysphagia)
history of gastric or esophageal surgery
pathological personal history of movement disorders (achalasia cardia, scleroderma,
myopathies)
pregnant or lactating women
patients on chronic medications that can impair motor function of the esophagus and SEI
(anticholinergics, NSAIDs, calcium channel blockers, beta-blockers, nitrates,
barbiturates, progesterone)
patients receiving treatment with PPIs in the last 8 weeks prior to enrollment.
VIII.2.2. Study protocol
Chronic laryngitis possible deriving from GERD was considered by the ENT specialist
for patients who have:
13
Clinically: dysphonia (especially in the morning), globus, hemming, foreign body
sensation in the throat or sore throat, lasting at least 8 weeks, with or without typical
symptoms of GERD (heartburn and / or regurgitation).
ENT exam (which consisted of indirect laryngoscopy and videofibrolaryngoscopy):
lesions suggestive of GERD - edema and erythema of the posterior commissure
(arytenoids and interarytenoidian area), edema and erythema of the rear wall of the
pharynx, arytenoidian granuloma, diffuse congestion of vocal cords or of the endolarynx.
Each patient included in the study was compiled a data sheet that recorded information
related to: personal data (name, age, gender, environment, BMI), personal history and family
history, history of their disease, living and working conditions (using voice for vocational
purposes, behaviors towards the environment: smoker / non-smoker, consumption of coffee,
alcohol and drugs, how the symptoms of the disease influenced the sleep of patients and
therefore everyday work, biological data (Ac anti-Helicobacter pylori, cholesterol and
triglycerides)).
In our clinic, patients with possibly GERD-induced chronic laryngitis have been
evaluated differently depending on the presence or absence of typical symptoms of reflux
(heartburn and / or regurgitation occurred with a frequency of at least 2-3 times / week and
considered "troublesome" by the patient). All patients included in the study were clinically
evaluated every month and 3 months, in IGH Iasi Ambulatory Hospital.
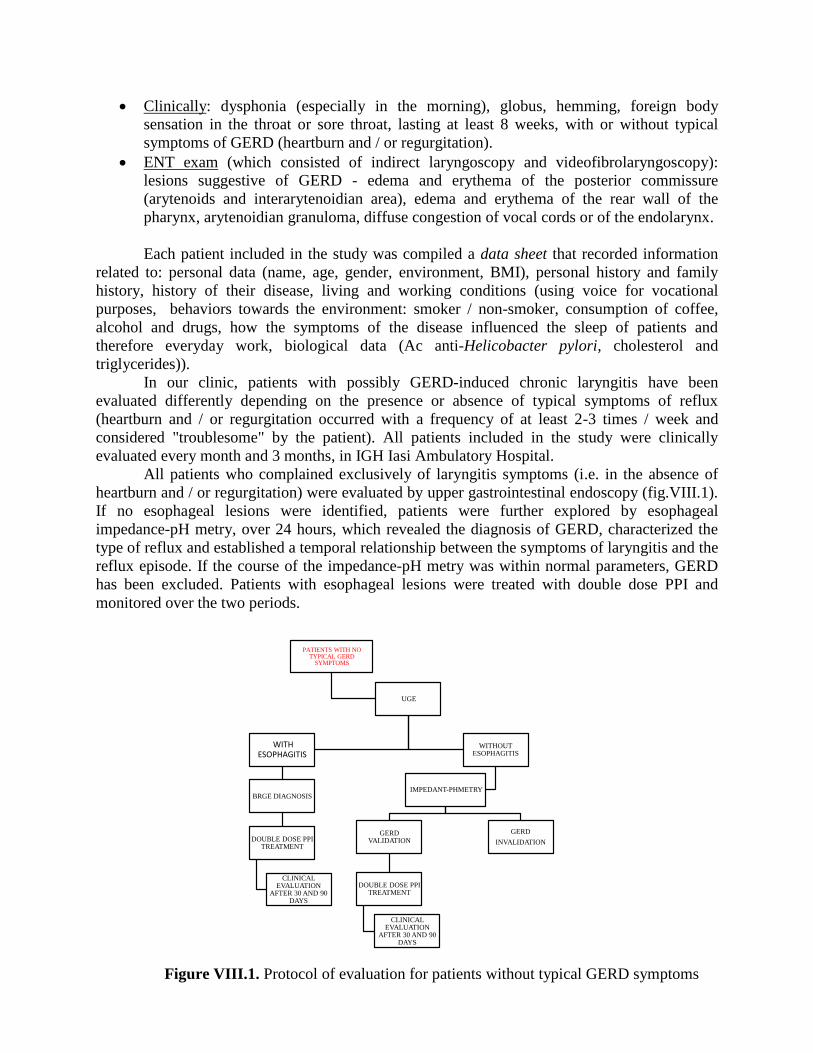
All patients who complained exclusively of laryngitis symptoms (i.e. in the absence of
heartburn and / or regurgitation) were evaluated by upper gastrointestinal endoscopy (fig.VIII.1).
If no esophageal lesions were identified, patients were further explored by esophageal
impedance-pH metry, over 24 hours, which revealed the diagnosis of GERD, characterized the
type of reflux and established a temporal relationship between the symptoms of laryngitis and the
reflux episode. If the course of the impedance-pH metry was within normal parameters, GERD
has been excluded. Patients with esophageal lesions were treated with double dose PPI and
monitored over the two periods.
PATIENTS WITH NO TYPICAL GERD
SYMPTOMS
UGE
WITH ESOPHAGITIS
BRGE DIAGNOSIS
DOUBLE DOSE PPI TREATMENT
CLINICAL EVALUATION
AFTER 30 AND 90 DAYS
WITHOUT ESOPHAGITIS
IMPEDANT-PHMETRY
GERD VALIDATION
DOUBLE DOSE PPI TREATMENT
CLINICAL EVALUATION
AFTER 30 AND 90 DAYS
GERD
INVALIDATION
Figure VIII.1. Protocol of evaluation for patients without typical GERD symptoms
14
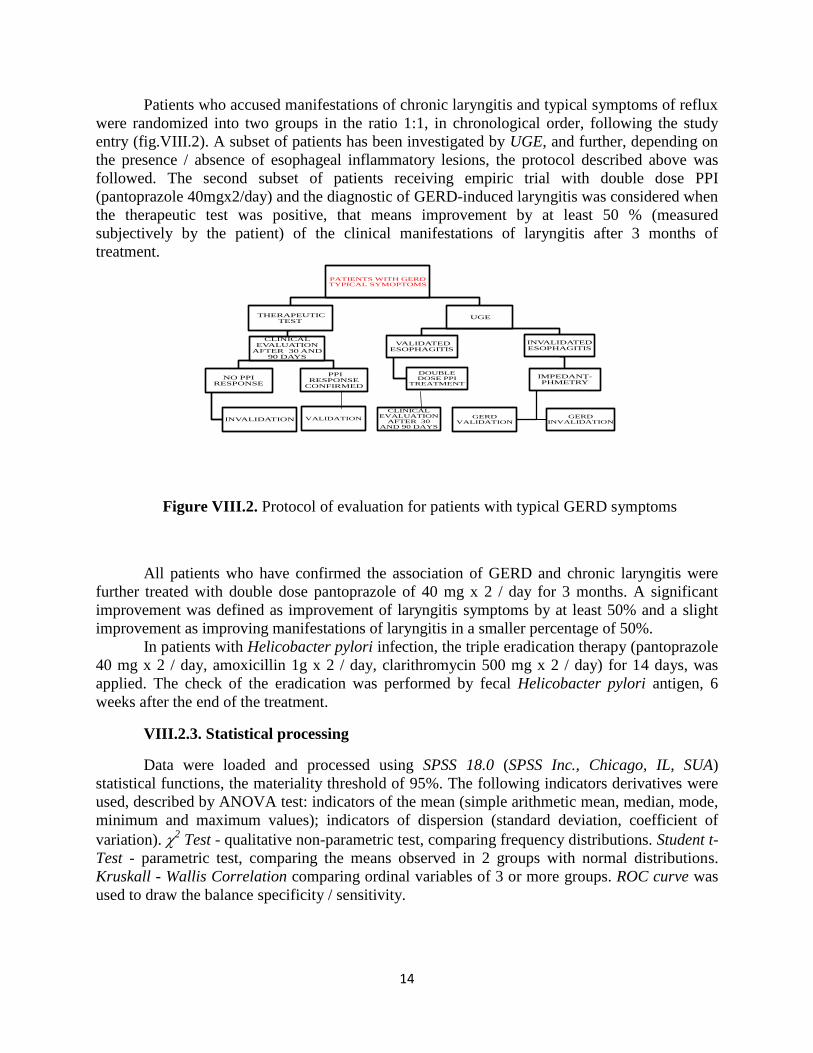
Patients who accused manifestations of chronic laryngitis and typical symptoms of reflux
were randomized into two groups in the ratio 1:1, in chronological order, following the study
entry (fig.VIII.2). A subset of patients has been investigated by UGE, and further, depending on
the presence / absence of esophageal inflammatory lesions, the protocol described above was
followed. The second subset of patients receiving empiric trial with double dose PPI
(pantoprazole 40mgx2/day) and the diagnostic of GERD-induced laryngitis was considered when
the therapeutic test was positive, that means improvement by at least 50 % (measured
subjectively by the patient) of the clinical manifestations of laryngitis after 3 months of
treatment.
PATIENTS WITH GERD TYPICAL SYMOPTOMS
THERAPEUTIC TEST
CLINICAL EVALUATION
AFTER 30 AND 90 DAYS
NO PPI RESPONSE
INVALIDATION
PPI RESPONSE
CONFIRMED
UGE
INVALIDATED ESOPHAGITIS
IMPEDANȚ-PHMETRY
GERD VALIDATION
GERD INVALIDATION
VALIDATED ESOPHAGITIS
DOUBLE DOSE PPI
TREATMENT
VALIDATION
CLINICAL EVALUATION
AFTER 30 AND 90 DAYS
All patients who have confirmed the association of GERD and chronic laryngitis were
further treated with double dose pantoprazole of 40 mg x 2 / day for 3 months. A significant
improvement was defined as improvement of laryngitis symptoms by at least 50% and a slight
improvement as improving manifestations of laryngitis in a smaller percentage of 50%.
In patients with Helicobacter pylori infection, the triple eradication therapy (pantoprazole
40 mg x 2 / day, amoxicillin 1g x 2 / day, clarithromycin 500 mg x 2 / day) for 14 days, was
applied. The check of the eradication was performed by fecal Helicobacter pylori antigen, 6
weeks after the end of the treatment.
VIII.2.3. Statistical processing
Data were loaded and processed using SPSS 18.0 (SPSS Inc., Chicago, IL, SUA)
statistical functions, the materiality threshold of 95%. The following indicators derivatives were
used, described by ANOVA test: indicators of the mean (simple arithmetic mean, median, mode,
minimum and maximum values); indicators of dispersion (standard deviation, coefficient of
variation). 2 Test - qualitative non-parametric test, comparing frequency distributions. Student t-
Test - parametric test, comparing the means observed in 2 groups with normal distributions.
Kruskall - Wallis Correlation comparing ordinal variables of 3 or more groups. ROC curve was
used to draw the balance specificity / sensitivity.
Figure VIII.2. Protocol of evaluation for patients with typical GERD symptoms

15
VIII.3. RESULTS
VIII.3.1. General characteristics of the group of patients with chronic laryngitis
We included 112 patients who met the selection criteria, which were characterized by the
predominance of males and of urban origin, with ages between 20-83 years and an average age
of about 50 years. Most patients did not show typical symptoms of GERD.
VIII.3.2. Diagnosis protocol for possibly GERD-induced chronic laryngitis
Following established protocol diagnosis, we identified an association between chronic
laryngitis and GERD of 80.4%, a percentage that is much higher than that reported in literature
(fig.VIII.9).
Figure VIII.9. Distribution of chronic laryngitis possibly GERD-induced cases
By randomizing patients with laryngitis and typical reflux symptoms and by their
different investigation, using either the therapeutic test or UDE, we assessed the sensitivity and
specificity of these two techniques for the diagnosis of laryngitis with GERD etiologic potential.
By plotting the ROC curve, we found a sensitivity of 57% and a specificity of 60% for UDE and
a much lower sensitivity and specificity, of only 42% and 40% for empiric PPI trial (Fig.
VIII.10).
Figure VIII.10. The balance sensitivity/specificity for
UDE and the therapeutic test in the diagnosis of GERD-induced laryngitis
With symptoms, therapeutic test +
17.9%With symptoms,
UDE with esophagitis 15.2%
With symptoms, IIM-pH+
0.9%Without symptoms,
UDE with esophagitis 34.8%
Without symptoms,IIM-pH+11.6%
No GERD19.6%
Area Under the Curve
.601 .091 .540 .378 .734
.444 .091 .540 .266 .622
Test Result Variable(s)
EDS
TestTerapeutic
Area Std. Errora
Asy mptotic
Sig.b
Lower Bound Upper Bound
Asy mptotic 95% Conf idence
Interv al
The test result v ariable(s): EDS, TestTerapeutic has at least one tie between the posit iv e actual
state group and the negativ e actual state group. Stat istics may be biased.
Under the nonparametric assumptiona.
Null hy pothesis: t rue area = 0.5b.
1.00.80.60.40.20.0
1 - Specificity
1.0
0.8
0.6
0.4
0.2
0.0
Se
ns
itiv
ity
TestTerapeutic
EDS
Source of the Curve
ROC Curve
16
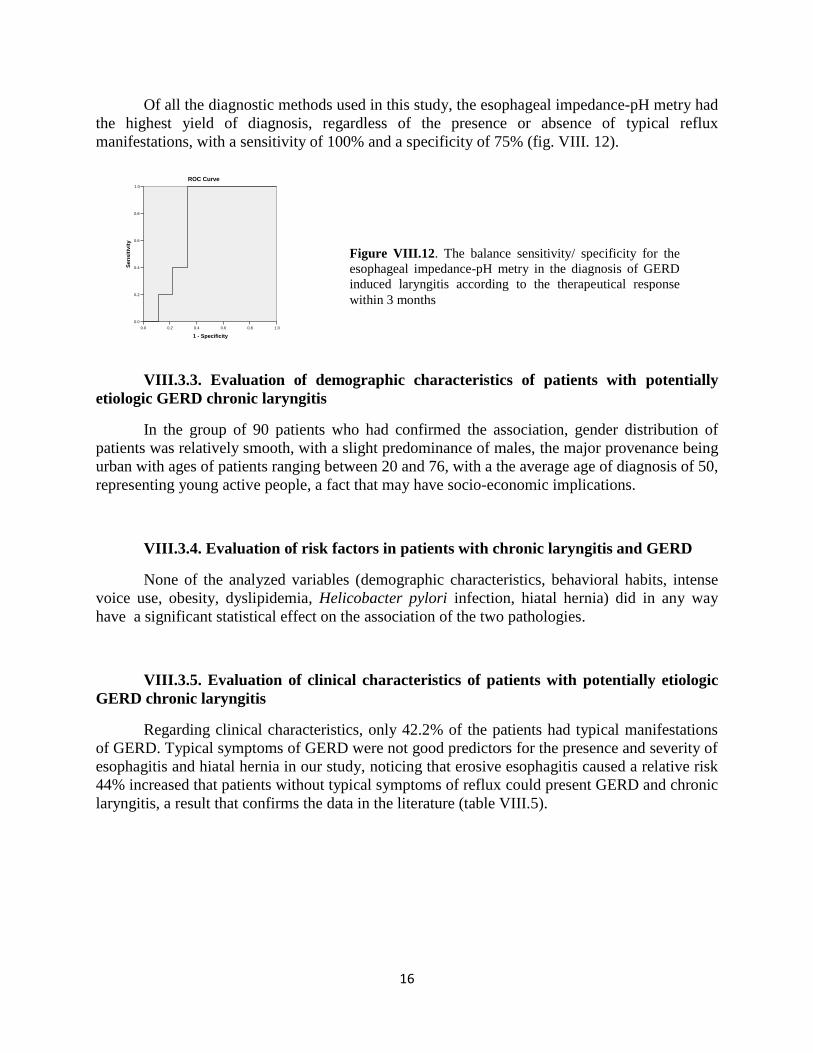
Of all the diagnostic methods used in this study, the esophageal impedance-pH metry had
the highest yield of diagnosis, regardless of the presence or absence of typical reflux
manifestations, with a sensitivity of 100% and a specificity of 75% (fig. VIII. 12).
VIII.3.3. Evaluation of demographic characteristics of patients with potentially
etiologic GERD chronic laryngitis
In the group of 90 patients who had confirmed the association, gender distribution of
patients was relatively smooth, with a slight predominance of males, the major provenance being
urban with ages of patients ranging between 20 and 76, with a the average age of diagnosis of 50,
representing young active people, a fact that may have socio-economic implications.
VIII.3.4. Evaluation of risk factors in patients with chronic laryngitis and GERD
None of the analyzed variables (demographic characteristics, behavioral habits, intense
voice use, obesity, dyslipidemia, Helicobacter pylori infection, hiatal hernia) did in any way
have a significant statistical effect on the association of the two pathologies.
VIII.3.5. Evaluation of clinical characteristics of patients with potentially etiologic
GERD chronic laryngitis
Regarding clinical characteristics, only 42.2% of the patients had typical manifestations
of GERD. Typical symptoms of GERD were not good predictors for the presence and severity of
esophagitis and hiatal hernia in our study, noticing that erosive esophagitis caused a relative risk
44% increased that patients without typical symptoms of reflux could present GERD and chronic
laryngitis, a result that confirms the data in the literature (table VIII.5).
1.00.80.60.40.20.0
1 - Specificity
1.0
0.8
0.6
0.4
0.2
0.0
Sen
sit
ivit
y
ROC Curve
Figure VIII.12. The balance sensitivity/ specificity for the
esophageal impedance-pH metry in the diagnosis of GERD
induced laryngitis according to the therapeutical response
within 3 months
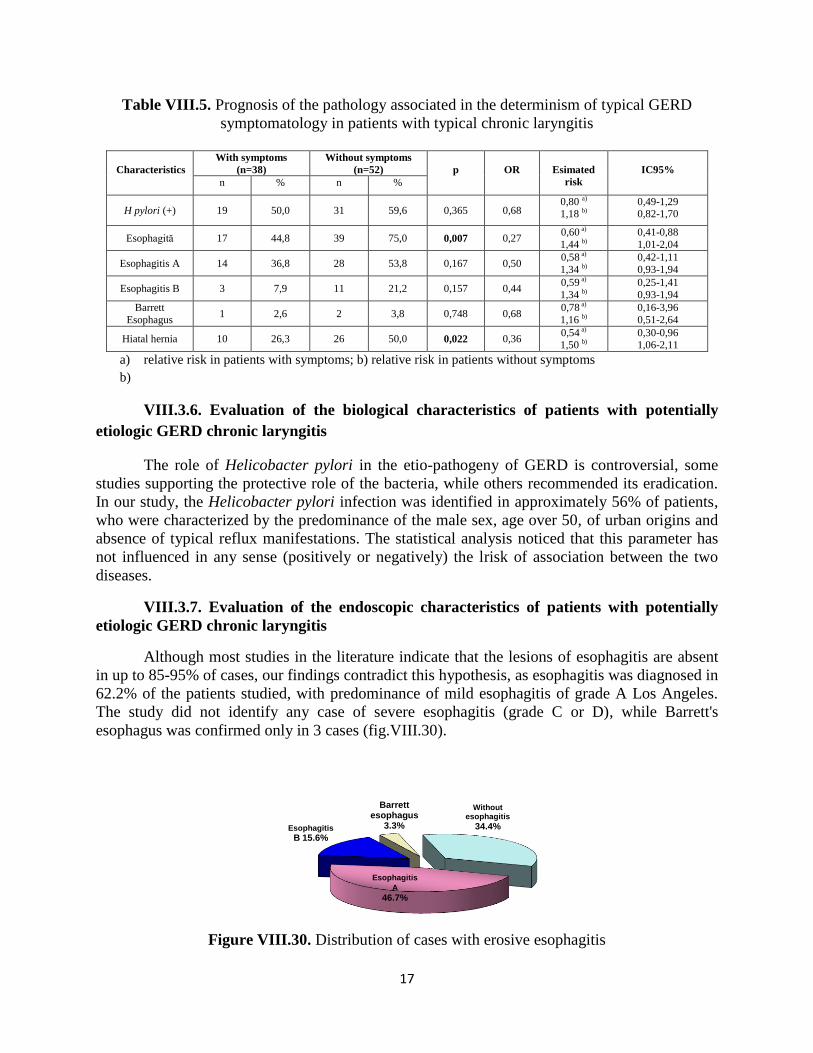
17
Table VIII.5. Prognosis of the pathology associated in the determinism of typical GERD
symptomatology in patients with typical chronic laryngitis
Characteristics
With symptoms
(n=38)
Without symptoms
(n=52)
p
OR
Esimated
risk
IC95%
n % n %
H pylori (+) 19 50,0 31 59,6 0,365 0,68 0,80 a)
1,18 b) 0,49-1,29 0,82-1,70
Esophagită 17 44,8 39 75,0 0,007 0,27 0,60 a)
1,44 b)
0,41-0,88
1,01-2,04
Esophagitis A 14 36,8 28 53,8 0,167 0,50 0,58 a)
1,34 b)
0,42-1,11
0,93-1,94
Esophagitis B 3 7,9 11 21,2 0,157 0,44 0,59 a)
1,34 b)
0,25-1,41
0,93-1,94
Barrett
Esophagus 1 2,6 2 3,8 0,748 0,68
0,78 a)
1,16 b)
0,16-3,96
0,51-2,64
Hiatal hernia 10 26,3 26 50,0 0,022 0,36 0,54 a)
1,50 b) 0,30-0,96 1,06-2,11
a) relative risk in patients with symptoms; b) relative risk in patients without symptoms
b)
VIII.3.6. Evaluation of the biological characteristics of patients with potentially
etiologic GERD chronic laryngitis
The role of Helicobacter pylori in the etio-pathogeny of GERD is controversial, some
studies supporting the protective role of the bacteria, while others recommended its eradication.
In our study, the Helicobacter pylori infection was identified in approximately 56% of patients,
who were characterized by the predominance of the male sex, age over 50, of urban origins and
absence of typical reflux manifestations. The statistical analysis noticed that this parameter has
not influenced in any sense (positively or negatively) the lrisk of association between the two
diseases.
VIII.3.7. Evaluation of the endoscopic characteristics of patients with potentially
etiologic GERD chronic laryngitis
Although most studies in the literature indicate that the lesions of esophagitis are absent
in up to 85-95% of cases, our findings contradict this hypothesis, as esophagitis was diagnosed in
62.2% of the patients studied, with predominance of mild esophagitis of grade A Los Angeles.
The study did not identify any case of severe esophagitis (grade C or D), while Barrett's
esophagus was confirmed only in 3 cases (fig.VIII.30).
Figure VIII.30. Distribution of cases with erosive esophagitis
Esophagitis
A
46.7%
Esophagitis
B 15.6%
Barrett esophagus
3.3%
Without esophagitis
34.4%
18
Hiatal hernia, which was identified in 40% of patients, correlated significantly with the
presence of reflux esophagitis, inducing a risk of association of chronic laryngitis with erosive
GERD 67% higher, a result that is consistent with the data in the medical literature.
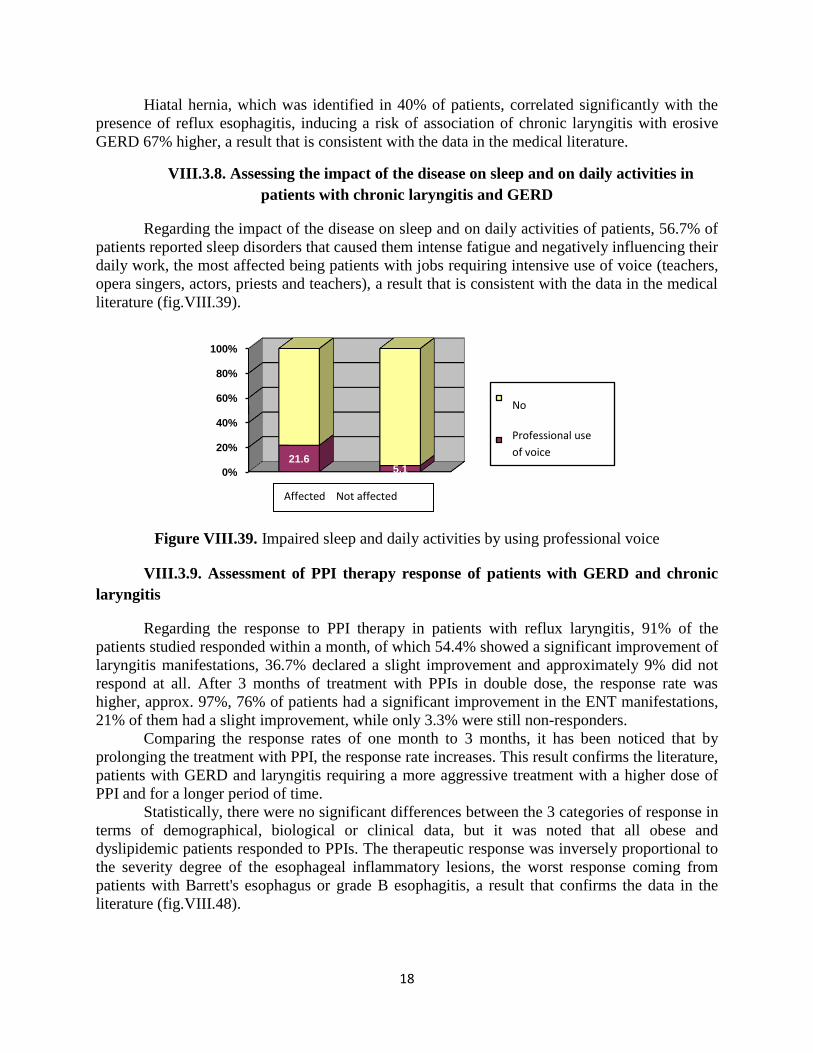
VIII.3.8. Assessing the impact of the disease on sleep and on daily activities in
patients with chronic laryngitis and GERD
Regarding the impact of the disease on sleep and on daily activities of patients, 56.7% of
patients reported sleep disorders that caused them intense fatigue and negatively influencing their
daily work, the most affected being patients with jobs requiring intensive use of voice (teachers,
opera singers, actors, priests and teachers), a result that is consistent with the data in the medical
literature (fig.VIII.39).
Figure VIII.39. Impaired sleep and daily activities by using professional voice
VIII.3.9. Assessment of PPI therapy response of patients with GERD and chronic
laryngitis
Regarding the response to PPI therapy in patients with reflux laryngitis, 91% of the
patients studied responded within a month, of which 54.4% showed a significant improvement of
laryngitis manifestations, 36.7% declared a slight improvement and approximately 9% did not
respond at all. After 3 months of treatment with PPIs in double dose, the response rate was
higher, approx. 97%, 76% of patients had a significant improvement in the ENT manifestations,
21% of them had a slight improvement, while only 3.3% were still non-responders.
Comparing the response rates of one month to 3 months, it has been noticed that by
prolonging the treatment with PPI, the response rate increases. This result confirms the literature,
patients with GERD and laryngitis requiring a more aggressive treatment with a higher dose of
PPI and for a longer period of time.
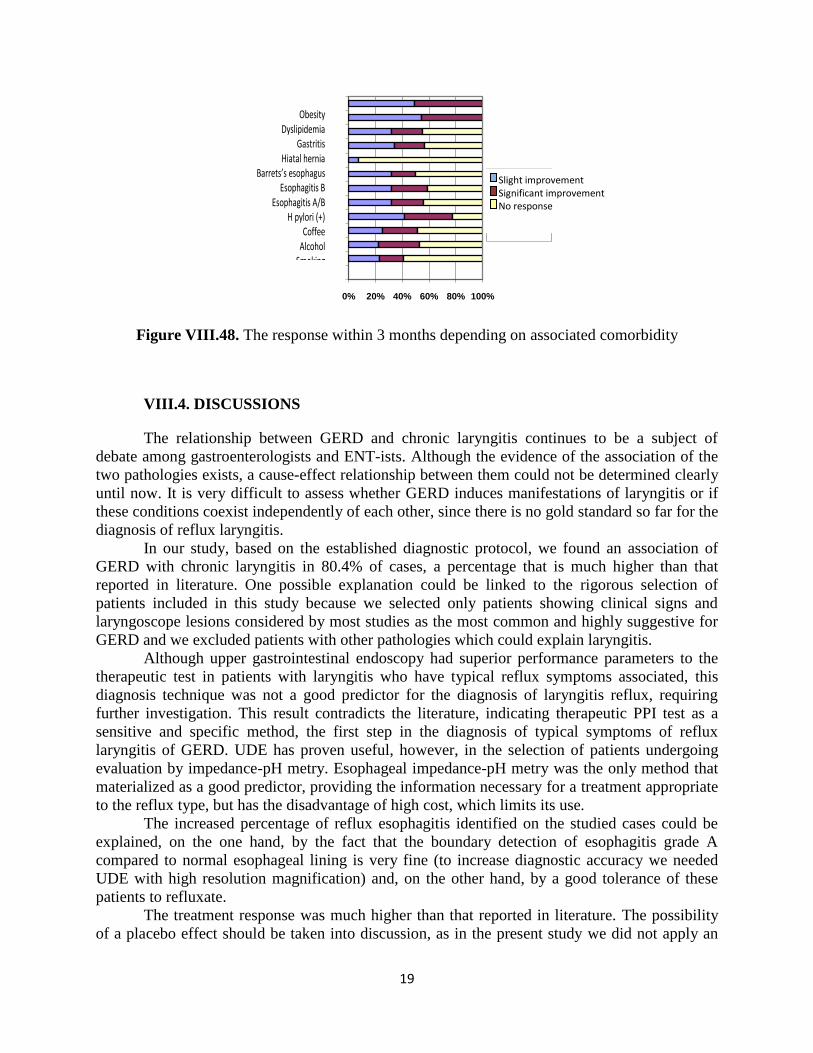
Statistically, there were no significant differences between the 3 categories of response in
terms of demographical, biological or clinical data, but it was noted that all obese and
dyslipidemic patients responded to PPIs. The therapeutic response was inversely proportional to
the severity degree of the esophageal inflammatory lesions, the worst response coming from
patients with Barrett's esophagus or grade B esophagitis, a result that confirms the data in the
literature (fig.VIII.48).
0%
20%
40%
60%
80%
100%
21.65.1
Nu
Folosirea profesională a vocii
Affected Not affected
No
Professional use
of voice
19
Figure VIII.48. The response within 3 months depending on associated comorbidity
VIII.4. DISCUSSIONS
The relationship between GERD and chronic laryngitis continues to be a subject of
debate among gastroenterologists and ENT-ists. Although the evidence of the association of the
two pathologies exists, a cause-effect relationship between them could not be determined clearly
until now. It is very difficult to assess whether GERD induces manifestations of laryngitis or if
these conditions coexist independently of each other, since there is no gold standard so far for the
diagnosis of reflux laryngitis.
In our study, based on the established diagnostic protocol, we found an association of
GERD with chronic laryngitis in 80.4% of cases, a percentage that is much higher than that
reported in literature. One possible explanation could be linked to the rigorous selection of
patients included in this study because we selected only patients showing clinical signs and
laryngoscope lesions considered by most studies as the most common and highly suggestive for
GERD and we excluded patients with other pathologies which could explain laryngitis.
Although upper gastrointestinal endoscopy had superior performance parameters to the
therapeutic test in patients with laryngitis who have typical reflux symptoms associated, this
diagnosis technique was not a good predictor for the diagnosis of laryngitis reflux, requiring
further investigation. This result contradicts the literature, indicating therapeutic PPI test as a
sensitive and specific method, the first step in the diagnosis of typical symptoms of reflux
laryngitis of GERD. UDE has proven useful, however, in the selection of patients undergoing
evaluation by impedance-pH metry. Esophageal impedance-pH metry was the only method that
materialized as a good predictor, providing the information necessary for a treatment appropriate
to the reflux type, but has the disadvantage of high cost, which limits its use.
The increased percentage of reflux esophagitis identified on the studied cases could be
explained, on the one hand, by the fact that the boundary detection of esophagitis grade A
compared to normal esophageal lining is very fine (to increase diagnostic accuracy we needed
UDE with high resolution magnification) and, on the other hand, by a good tolerance of these
patients to refluxate.
The treatment response was much higher than that reported in literature. The possibility
of a placebo effect should be taken into discussion, as in the present study we did not apply an
0% 20% 40% 60% 80% 100%
Fumat
Alcool
Cafea
H pylori (+)
Esofagită A/B
Esofagită A
Esofagită B
Esofag Barrett
Hernie hiatală
Gastrită
Dislipidemie
Obezitate
Ameliorare uşoară
Ameliorare semnificativă
Fără răspuns
Obesity Dyslipidemia
Gastritis Hiatal hernia
Barrets’s esophagus Esophagitis B
Esophagitis A/B H pylori (+)
Coffee Alcohol
Smoking
Slight improvement Significant improvement No response
20
objective method for quantifying this response (laryngoscopy exam, validated questionnaire), the
degree of improvement of laryngitis symptoms being appreciated in a subjective way by the
patient. In addition, this study was not a double-blind trial placebo-controlled.
VIII.5. CONCLUSIONS
The diagnosis of GERD induced-laryngitis is a difficult task, requiring a close
interdisciplinary collaboration between the gastroenterologist and the ENT-ist. The increased
percentage identified for the association between GERD and chronic laryngitis reflects the
importance of gastroenterological evaluation in patients with chronic laryngitis without a clear
etiology. Contrary to previous research data reported, the present study did not show therapeutic
test with proton pump inhibitors as a sensitive and specific method for the diagnosis of reflux
laryngitis with typical GERD symptoms. The esophageal impedance-pH metry proved an
important diagnosis tool in patients with normal endoscopy and laryngitis; it has identified and
characterized the type of reflux, stating a correct diagnosis, provided the information necessary
for appropriate treatment of reflux type and hasset a temporal relationship between the reflux
episode and the extradigestive manifestation. However, impedance-pH metry remains a difficult
method to reach in local hospitals in Romania.
Helicobacter pylori infection did not influence the risk of association, the role of
Helicobacter pylori in the etiopathogeny of GERD with ENT manifestations remaining
controversial still. Esophagitis lesions were objectified in a much higher percentage than that
reported in literature, all cases being mild esophagitis. The typical symptoms of GERD, found in
more than half of the cases, were not good predictors of the presence and severity of esophagitis
and hiatal hernia in our study.
GERD manifestations of chronic laryngitis had negative consequences for patients by
developing sleep disorders and by altering their daily activity, patients with professions that
require use of the voice intensively (teachers, opera singers, actors, priests, teachers) with
preference being affected, a result that is consistent with the data in the medical literature.
The resolution of symptoms of GERD-induced chronic laryngitis requires a more
aggressive treatment with PPIs, with a higher dose and for a longer period of time. The
therapeutic response to PPI was inversely proportional to the degree of severity of esophageal
lesions, results confirmed by numerous studies in the literature.
21
IX. ASSESSMENT OF ASTHMA PATIENTS WITH POTENTIALLY
ETIOLOGIC GASTROESOPHAGEAL REFLUX DISEASE
IX.1. THE AIM of the second study was to evaluate the association between poorly
controlled / uncontrolled asthma and GERD, as a clinical condition may induce other.
IX.2. MATERIAL AND METHOD
IX.2.1. Patients
We conducted a prospective case-control study over a period of 37 months (November 1,
2012 - November 30, 2015), at the Institute of Gastroenterology and Hepatology of "St.
Spiridon" Hospital, in collaboration with Iasi Pneumology Hospital.
Inclusion criteria:
patients older than 18 who have signed informed consent
patients diagnosed with asthma according to GINA 2015 guideline (Global Initiative for
Asthma) at least 6 months with significant reversibility inhaled bronchodilator (FEV1
(forced expiratory volume in one second) > 200 ml and > 12%)
uncontrolled or partially controlled asthma patients with maximal therapeutic dose of
inhaled corticosteroids (CIS) and beta2-agonists long-acting (BDLA)
CSI treatment and / or BDLA initiated at least 3 months prior to enrollment
patients who had at least one exacerbation of symptoms of asthma in the past year.
Exclusion criteria:
patient refusal / uncooperative patient / patient with documented psychiatric pathology
active tuberculosis or other acute lower respiratory tract infection
chronic bronchitis or lung cancers
use of oral corticosteroids 30 days prior to study entry
patients with alarm symptoms (unexplained weight loss, upper gastrointestinal bleeding,
dysphagia)
history of gastric or esophageal surgery
pathological personal history of motility disorders (achalasia cardia, scleroderma,
myopathies)
pregnant or lactating women
patients on chronic medications that can impair motor function of the esophagus and SEI
(anticholinergics, NSAIDs, calcium channel blockers, beta-blockers, nitrates,
barbiturates, progesterone)
patients receiving treatment with PPIs in the last 8 weeks.

22
IX.2.2. Study protocol
We included patients diagnosed with bronchial asthma at least 6 months prior to the
study, according to GINA criteria 2015.
The diagnosis of GERD induced- asthma was considered under the following conditions:
• historically positive for respiratory symptoms (particularly nocturnal or postprandial):
wheezing, shortness of breath , tightness of the chest.
• alteration objectified in spirometry lung function by lowering FEV1 (forced expiratory volume
in one second) and the ratio FEV1 / FVC (forced vital capacity) and was reversible inhaled
bronchodilators.
• lack of therapeutic or partial therapeutic control of asthma treatment with maximum doses of
anti-asthma properly.
• irrespective of the presence or absence of typical symptoms of reflux (heartburn and / or
regurgitation).
Patients with possibly GERD-induced asthma have been investigated following the same
protocol as in the previous study (fig.VIII.1 and VIII.2) .
IX.2.3. Statistical processing
The results were centralized in a SPSS 18.0 database (SPSS Inc., Chicago, IL, USA) and
processed with statistical functions to which they report, to the materiality threshold of 95%. In
the statistical analysis, we used descriptive as well as analytical methods.
IX.3. RESULTS
IX.3.1. General characteristics of patients with asthma
The present study included 44 patients diagnosed with asthma suspected of GERD origin.
This group of patients revealed the clear predominance of male sex and urban provenance, aged
between 18 and 77, with an average age of approx. 50 years. Most patients did not have typical
symptoms of GERD.
IX.3.2. Diagnosis protocol for asthma with potentially etiologic GERD
Following the same protocol as for the diagnosis of chronic laryngitis, we have identified
an association between the prevalence of GERD and asthma 88.6%, falling in the range of
variance of the prevalence reported by the international literature, but superior to that reported in
our country (fig.IX.7).

23
Figure IX.7. Distribution of asthma possibly GERD-induced cases
By plotting ROC curve, it was found that both the therapeutic test, and UDE are
ineffective for diagnosis of GERD-induced asthma. UDE had a sensitivity of 55% and a
specificity of 45%, while therapeutic test had a lower sensitivity and specificity of 50% and,
respective, 40% (fig.IX.8).
Only 3 patients were tested by esophageal impedance-pH metry. Of these, in 2 patients
the association between GERD and asthma was established.
IX.3.3. Evaluation of the demographic characteristics of patients with potentially
etiologic GERD asthma
In the group of 39 patients with uncontrolled or partially therapeutically controlled
asthma and GERD, there was noted a slightly higher percentage of males and the clear
predominance of urban provenance. The age of the patients ranged between 23 and 77, with an
average value of 51 years in the study group.
IX.3.4. Evaluation of risk factors in patients with asthma and GERD
Of all risk factors analyzed, only alcohol consumption and hiatal hernia induced a
statistically significant risk of association between GERD and asthma.
With symptoms, therapeutic
test+17.9%
With symptoms,UDE with
esophagitis15.2%
With symptoms,
IIM-pH+0.9%
Without symptomsUDE with
esophagitis34.8%
Without symptoms,
IIM-pH+11.6%
Without GERD
confirmation10.4%
1.00.80.60.40.20.0
1 - Specificity
1.0
0.8
0.6
0.4
0.2
0.0
Se
ns
itiv
ity
TestTerapeutic
EDSSource of the Curve
ROC Curve
Area Under the Curve
.545 .088 .606 .374 .717
.455 .088 .606 .283 .626
Test Result Variable(s)
EDS
TestTerapeutic
Area Std. Errora
Asy mptotic
Sig.b
Lower Bound Upper Bound
Asy mptotic 95% Conf idence
Interv al
The test result v ariable(s): EDS, TestTerapeutic has at least one tie between the posit iv e actual
state group and the negativ e actual state group. Stat istics may be biased.
Under the nonparametric assumptiona.
Null hy pothesis: t rue area = 0.5b.
Figure IX.8. The balance
sensitivity/ specificity for UDE
and the therapeutic test in the
diagnosis of the association
between GERD and asthma
24
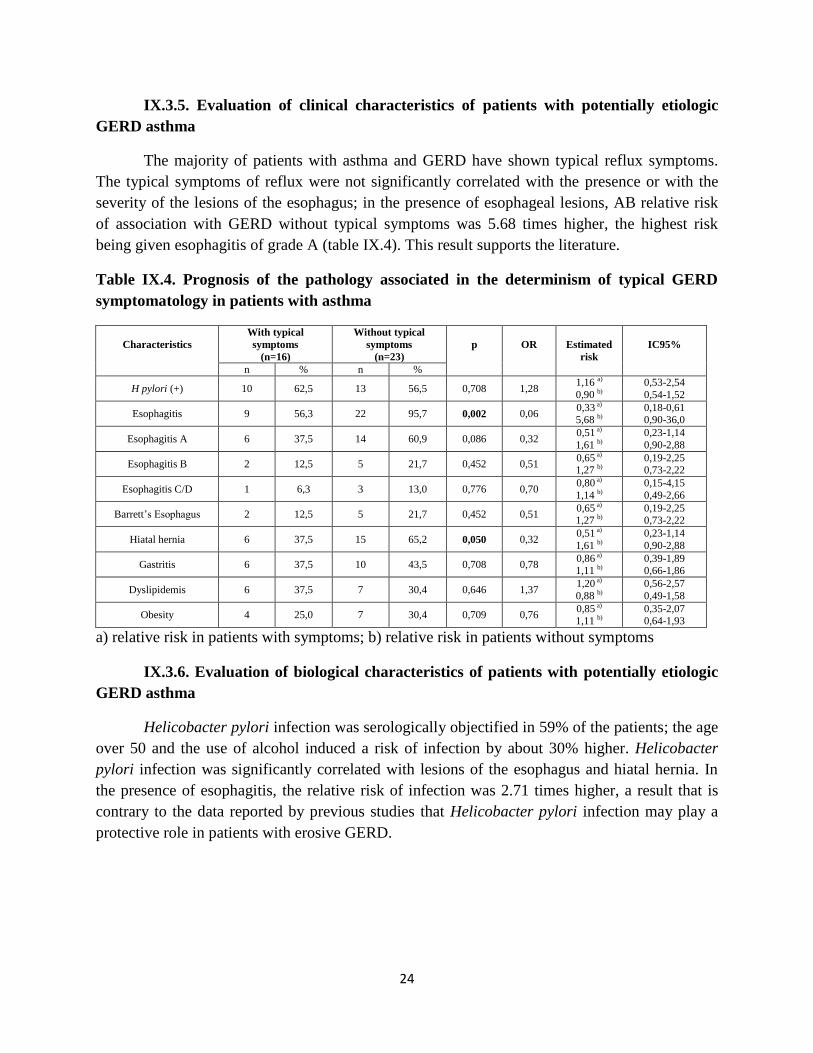
IX.3.5. Evaluation of clinical characteristics of patients with potentially etiologic
GERD asthma
The majority of patients with asthma and GERD have shown typical reflux symptoms.
The typical symptoms of reflux were not significantly correlated with the presence or with the
severity of the lesions of the esophagus; in the presence of esophageal lesions, AB relative risk
of association with GERD without typical symptoms was 5.68 times higher, the highest risk
being given esophagitis of grade A (table IX.4). This result supports the literature.
Table IX.4. Prognosis of the pathology associated in the determinism of typical GERD
symptomatology in patients with asthma
Characteristics
With typical
symptoms
(n=16)
Without typical
symptoms
(n=23)
p
OR
Estimated
risk
IC95%
n % n %
H pylori (+) 10 62,5 13 56,5 0,708 1,28 1,16 a)
0,90 b)
0,53-2,54
0,54-1,52
Esophagitis 9 56,3 22 95,7 0,002 0,06 0,33 a)
5,68 b) 0,18-0,61 0,90-36,0
Esophagitis A 6 37,5 14 60,9 0,086 0,32 0,51 a)
1,61 b)
0,23-1,14
0,90-2,88
Esophagitis B 2 12,5 5 21,7 0,452 0,51 0,65 a)
1,27 b) 0,19-2,25 0,73-2,22
Esophagitis C/D 1 6,3 3 13,0 0,776 0,70 0,80 a)
1,14 b)
0,15-4,15
0,49-2,66
Barrett’s Esophagus 2 12,5 5 21,7 0,452 0,51 0,65 a)
1,27 b) 0,19-2,25 0,73-2,22
Hiatal hernia 6 37,5 15 65,2 0,050 0,32 0,51 a)
1,61 b)
0,23-1,14
0,90-2,88
Gastritis 6 37,5 10 43,5 0,708 0,78 0,86 a)
1,11 b) 0,39-1,89 0,66-1,86
Dyslipidemis 6 37,5 7 30,4 0,646 1,37 1,20 a)
0,88 b)
0,56-2,57
0,49-1,58
Obesity 4 25,0 7 30,4 0,709 0,76 0,85 a)
1,11 b) 0,35-2,07 0,64-1,93
a) relative risk in patients with symptoms; b) relative risk in patients without symptoms
IX.3.6. Evaluation of biological characteristics of patients with potentially etiologic
GERD asthma
Helicobacter pylori infection was serologically objectified in 59% of the patients; the age
over 50 and the use of alcohol induced a risk of infection by about 30% higher. Helicobacter
pylori infection was significantly correlated with lesions of the esophagus and hiatal hernia. In
the presence of esophagitis, the relative risk of infection was 2.71 times higher, a result that is
contrary to the data reported by previous studies that Helicobacter pylori infection may play a
protective role in patients with erosive GERD.
25
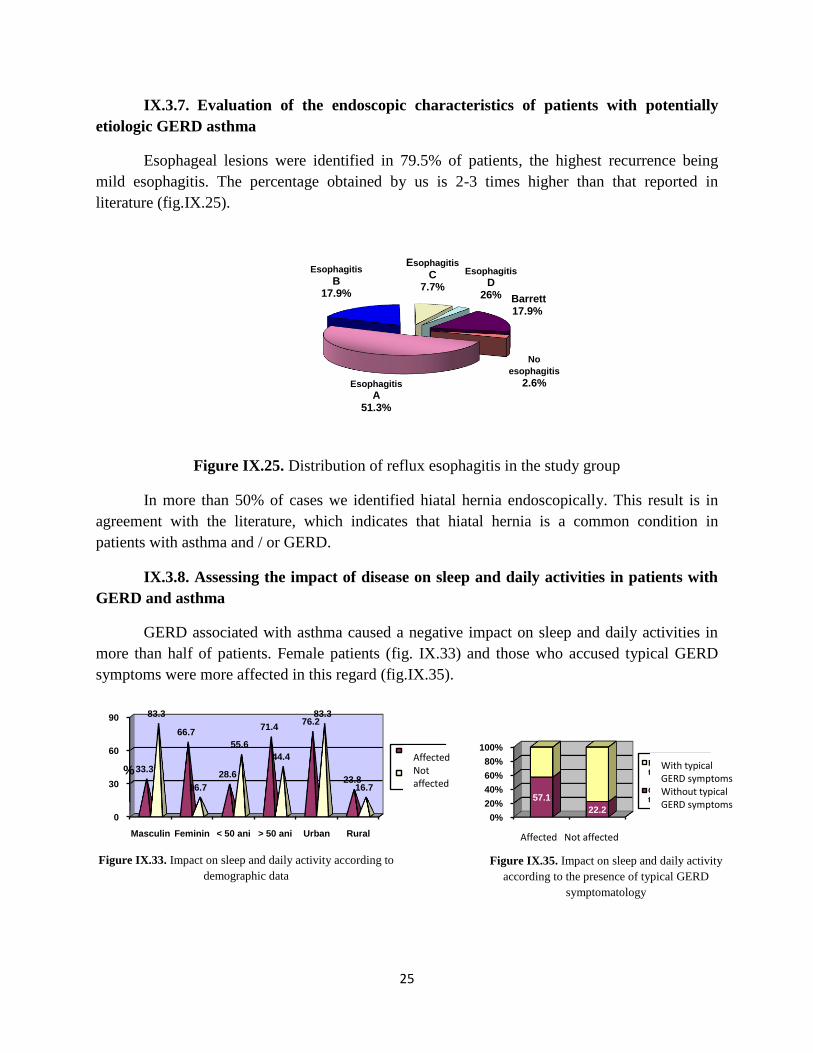
IX.3.7. Evaluation of the endoscopic characteristics of patients with potentially
etiologic GERD asthma
Esophageal lesions were identified in 79.5% of patients, the highest recurrence being
mild esophagitis. The percentage obtained by us is 2-3 times higher than that reported in
literature (fig.IX.25).
Figure IX.25. Distribution of reflux esophagitis in the study group
In more than 50% of cases we identified hiatal hernia endoscopically. This result is in
agreement with the literature, which indicates that hiatal hernia is a common condition in
patients with asthma and / or GERD.
IX.3.8. Assessing the impact of disease on sleep and daily activities in patients with
GERD and asthma
GERD associated with asthma caused a negative impact on sleep and daily activities in
more than half of patients. Female patients (fig. IX.33) and those who accused typical GERD
symptoms were more affected in this regard (fig.IX.35).
Esophagitis
A51.3%
Esophagitis
B17.9%
Esophagitis
C7.7%
Esophagitis
D26% Barrett
17.9%
No
esophagitis
2.6%
0%
20%
40%
60%
80%
100%
Cu afectare
Fără afectare
57.1
22.2
Fără simptome tipice de BRGE
Cu simptome tipice de BRGE
0
30
60
90
Masculin Feminin < 50 ani > 50 ani Urban Rural
33.3
66.7
28.6
71.476.2
23.8
83.3
16.7
55.6
44.4
83.3
16.7
%
Cu afectare
Fără afectare
Male Female <50years >50years Urban Rural
Affected Not affected
Affected Not affected
With typical GERD symptoms Without typical GERD symptoms
Figure IX.33. Impact on sleep and daily activity according to
demographic data Figure IX.35. Impact on sleep and daily activity
according to the presence of typical GERD
symptomatology
26
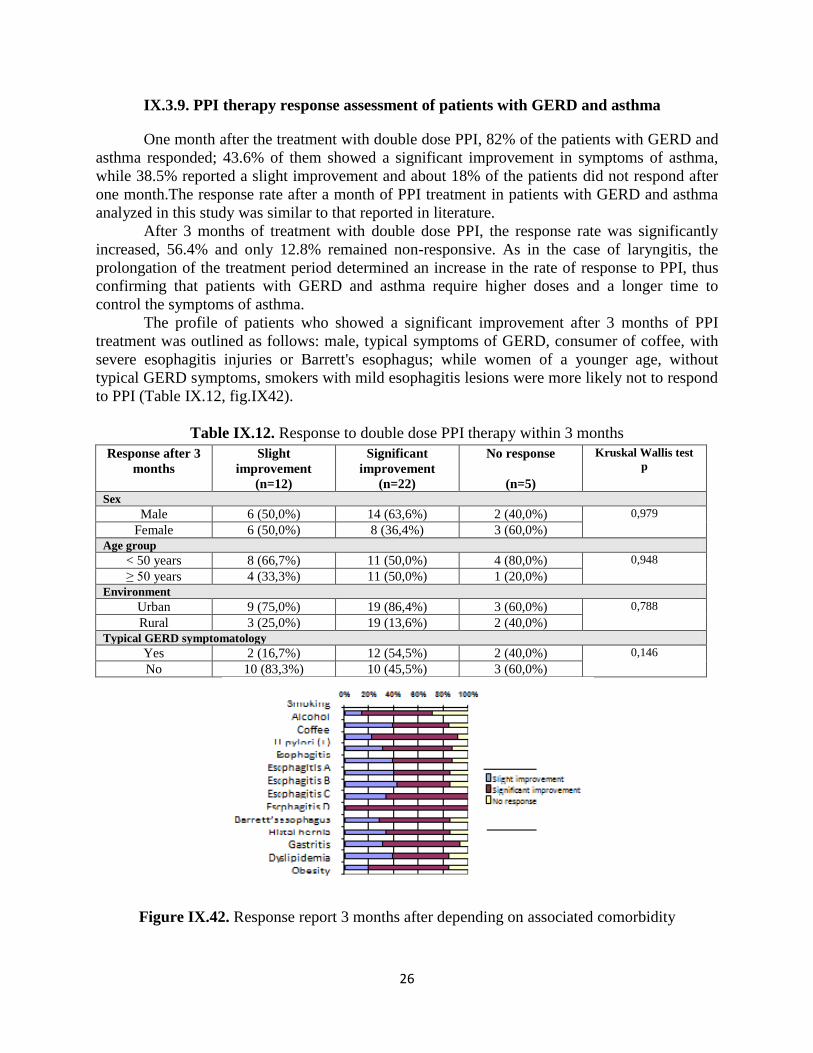
IX.3.9. PPI therapy response assessment of patients with GERD and asthma
One month after the treatment with double dose PPI, 82% of the patients with GERD and
asthma responded; 43.6% of them showed a significant improvement in symptoms of asthma,
while 38.5% reported a slight improvement and about 18% of the patients did not respond after
one month.The response rate after a month of PPI treatment in patients with GERD and asthma
analyzed in this study was similar to that reported in literature.
After 3 months of treatment with double dose PPI, the response rate was significantly
increased, 56.4% and only 12.8% remained non-responsive. As in the case of laryngitis, the
prolongation of the treatment period determined an increase in the rate of response to PPI, thus
confirming that patients with GERD and asthma require higher doses and a longer time to
control the symptoms of asthma.
The profile of patients who showed a significant improvement after 3 months of PPI
treatment was outlined as follows: male, typical symptoms of GERD, consumer of coffee, with
severe esophagitis injuries or Barrett's esophagus; while women of a younger age, without
typical GERD symptoms, smokers with mild esophagitis lesions were more likely not to respond
to PPI (Table IX.12, fig.IX42).
Table IX.12. Response to double dose PPI therapy within 3 months
Response after 3
months
Slight
improvement
(n=12)
Significant
improvement
(n=22)
No response
(n=5)
Kruskal Wallis test
p
Sex
Male 6 (50,0%) 14 (63,6%) 2 (40,0%) 0,979
Female 6 (50,0%) 8 (36,4%) 3 (60,0%)
Age group
< 50 years 8 (66,7%) 11 (50,0%) 4 (80,0%) 0,948
≥ 50 years 4 (33,3%) 11 (50,0%) 1 (20,0%)
Environment
Urban 9 (75,0%) 19 (86,4%) 3 (60,0%) 0,788
Rural 3 (25,0%) 19 (13,6%) 2 (40,0%)
Typical GERD symptomatology
Yes 2 (16,7%) 12 (54,5%) 2 (40,0%) 0,146
No 10 (83,3%) 10 (45,5%) 3 (60,0%)
Figure IX.42. Response report 3 months after depending on associated comorbidity

27
IX.4. DISCUSSIONS
The present study identified a prevalence of GERD associated with poorly controlled
asthma (with maximal treatment) of 88.6%, a percentage that falls in the range of variation in the
prevalence reported by the international literature, but it is significantly higher than that reported
in our country.
The diagnosis of GERD-induced asthma is very challenging, especially when typical
symptoms of GERD are absent. A case of asthma difficult to control with maximal doses of
specific therapy should raise suspicion of GERD secondary asthma, limiting the chance of
diagnosis and therapeutic error. Here lies the importance of the interdisciplinary approach to this
pathology, which can save lives or at least improve the quality of life of affected patients.
Although the current guidelines indicate the therapeutic test with inhibitors of proton
pump as a first stage of diagnosis in patients with asthma possibly secondary to GERD, in the
present study the PPI test was shown to be an effective technique for diagnosis in patients with
typical symptoms of reflux. UDE performance parameters were superior to those of therapeutic
PPI test, but they confirmed literature, reaffirming that UDE is not a method efficient enough to
diagnose GERD-induced asthma in patients with typical symptoms of reflux. Esophageal
impedance-pH metry is the diagnosis technique that can establish a temporal relationship
between symptoms of asthma and the production of the reflux episode, acid or non-acid.
Unfortunately, the number of patients who were evaluated by impedance-pH metry was very
small and did not allow calculating performance parameters for this method.
Studies show that the presence of esophagitis is not common in patients with GERD and
asthma. This study contradicts this result, identifying a rate 2-3 times higher of esophagitis
lesions, with mild esophagitis prevalence. A possible explanation is similar to the case of chronic
laryngitis.
Multiple controversies have been reported in literature also for the case of the efficacy of
PPI in patients with GERD-induced asthma. In our study, the response rate in patients with
GERD and asthma to PPI was similar to that reported in literature. Extending the duration of
treatment to 3 months we noticed an increase in the percentage of patients that reported
improvement of the manifestations of asthma.
IX.5. CONCLUSIONS
Establishing a relationship of cause-effect between GERD and asthma is an extremely
difficult task, given that there is no gold standard method for diagnosis, to prove the meaning of
the link between events in this two-way relationship or if the two clinical conditions coexist
independently of each other. The prevalence of the association between asthma and GERD was
placed in the range of variation in the prevalence reported by the international literature, but was
higher than that reported in our country. Patients with uncontrolled/ partially controlled asthma
with maximal therapeutic anti-asthma treatment require gastroenterological assessment by
excluding other possible factors of exacerbation of asthma symptoms, the interdisciplinary
approach being essential.
Both the therapeutic test and EDS are ineffective methods for the diagnosis of GERD-
induced asthma. Although the very small number of patients evaluated by esophageal
impedance-pH metry did not allow calculation of performance parameters for this method, the
esophageal impedance-pH metry had an important role in revealing the diagnosis and
28
establishing a temporal relationship between the episode of reflux and the manifestations of
asthma in patients without endoscopic GERD mark.
From a demographic perspective, patients with GERD and asthma were characterized by
the predominance of males and urban origin, with a mean age segment of the population that is
active in working with the socio-economic repercussions not insignificant.
The typical symptoms of GERD were absent in more than half of the cases, suggesting
the important role of silent reflux and did not correlate with the presence or severity of lesions of
the esophagus, a result which is consistent with the medical literature.
More than half of patients reported sleep disturbances and decreased yield due to socio-
occupational disease manifestations, female patients and those who have typical reflux
symptoms charged with being more affected.
The response to PPI therapy was similar to that reported in literature, patients requiring
higher doses and a longer time to resolution of symptoms of asthma.
X. ASSESSMENT OF PATIENTS WITH POTENTIALLY ETIOLOGIC
CHRONIC COUGH GERD
X.1. THE AIM of the third study was to evaluate the association between chronic cough
and GERD, in order to analyze the possibility of GERD involvement in the etiology of chronic
cough.
X.2. MATERIAL AND METHOD
X.2.1. Patients
The prospective case-control study was conducted over a period of 37 months (November
1, 2012 - November 30, 2015) at the Institute of Gastroenterology and Hepatology of "St.
Spiridon" Hospital in collaboration with the Iaşi Pneumology Hospital.
Inclusion criteria:
patients older than 18 who have signed informed consent
patients diagnosed with chronic cough (cough, lasting at least 8 weeks) without a clear
etiology.
Exclusion criteria:
patient refusal / uncooperative patient / patient with documented psychiatric pathology
active tuberculosis or other acute respiratory tract infection
history of asthma, chronic bronchitis or lung cancers
postnasal syndrome or rhinosinusitis
smokers
chronic exposure to toxic or allergic environmental factors
treatment with angiotensin-converting inhibitors
history of left ventricular failure or mitral stenosis
alarm symptoms (unexplained weight loss, gastrointestinal bleeding upper dysphagia)
history of gastric or esophageal surgery
29
pathological personal history of motiliyy disorders (achalasia cardia, scleroderma,
myopathies)
pregnant or lactating women
patients on chronic medications that can impair motor function of the esophagus and SEI
(anticholinergics, NSAIDs, calcium channel blockers, beta-blockers, nitrates,
barbiturates, progesterone)
patients receiving treatment with PPI in the last 8 weeks.
X.2.2. Study protocol
The present study included patients with chronic cough which were excluded from
possible breathing etiologies (clinical examination, chest radiography, spirometry and sputum
examination normal), ENT etiologies (indirect and direct laryngoscopy without change), allergic
etiologies (skin tests for allergies negative) and heart etiologies (echocardiography normal in the
absence of angiotensin converting enzyme inhibitor therapies).
Once these causes of chronic cough were excluded, patients were evaluated in our
service, following the same protocol for diagnosis, treatment and monitoring as in previous
studies (fig.VIII.1 and VIII.2) and GERD was considered under the same criteria.
X.2.3. Statistical processing
In the statistical analysis we used descriptive and analytical methods. The data were
collected in the SPSS 18.0 database (SPSS Inc., Chicago, IL, USA) and processed to materiality
threshold 95% (CI 95%).
X.3. RESULTS
X.3.1. General characteristics of the group of patients with chronic cough
The study group comprised 35 patients diagnosed with chronic cough suspected of
GERD otigin, which were characterized by the predominance of males and urban origin. The age
of patients with chronic cough varying widely, with extremes of 28 and 81 years old and with an
average of about 48 years. In contrast to the above mentioned extradigestive manifestations, the
cough patients included in the study had their most typical symptoms of reflux.
X.3.2. Diagnosis protocol for possibly GERD-induced chronic cough
According to the established study protocol, we found an association between GERD and
chronic cough in 85.7% of cases, a percentage that is higher than estimated literature (fig.X.7).
30
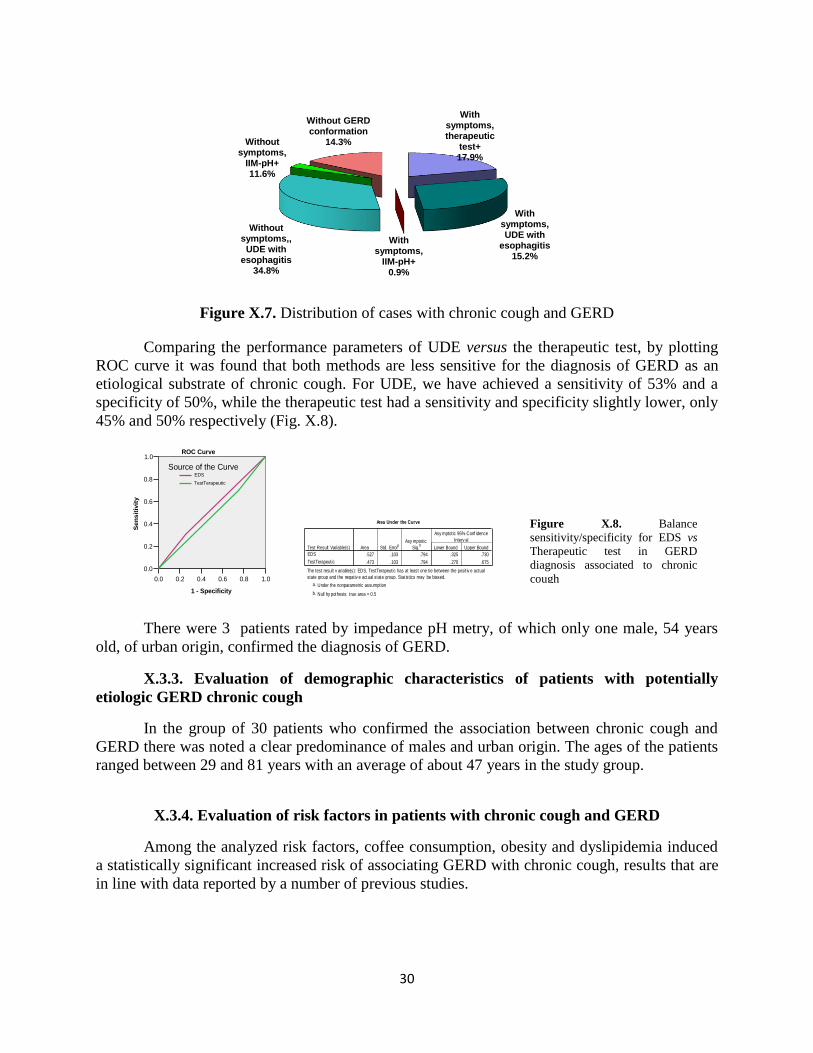
Figure X.7. Distribution of cases with chronic cough and GERD
Comparing the performance parameters of UDE versus the therapeutic test, by plotting
ROC curve it was found that both methods are less sensitive for the diagnosis of GERD as an
etiological substrate of chronic cough. For UDE, we have achieved a sensitivity of 53% and a
specificity of 50%, while the therapeutic test had a sensitivity and specificity slightly lower, only
45% and 50% respectively (Fig. X.8).
There were 3 patients rated by impedance pH metry, of which only one male, 54 years
old, of urban origin, confirmed the diagnosis of GERD.
X.3.3. Evaluation of demographic characteristics of patients with potentially
etiologic GERD chronic cough
In the group of 30 patients who confirmed the association between chronic cough and
GERD there was noted a clear predominance of males and urban origin. The ages of the patients
ranged between 29 and 81 years with an average of about 47 years in the study group.
X.3.4. Evaluation of risk factors in patients with chronic cough and GERD
Among the analyzed risk factors, coffee consumption, obesity and dyslipidemia induced
a statistically significant increased risk of associating GERD with chronic cough, results that are
in line with data reported by a number of previous studies.
With symptoms,therapeutic
test+17.9%
With symptoms, UDE with
esophagitis15.2%
With symptoms,
IIM-pH+0.9%
Without symptoms,,
UDE with esophagitis
34.8%
Without symptoms,
IIM-pH+11.6%
Without GERD conformation
14.3%
1.00.80.60.40.20.0
1 - Specificity
1.0
0.8
0.6
0.4
0.2
0.0
Sen
sit
ivit
y
TestTerapeutic
EDS
Source of the Curve
ROC Curve
Area Under the Curve
.527 .103 .794 .325 .730
.473 .103 .794 .270 .675
Test Result Variable(s)
EDS
TestTerapeutic
Area Std. Errora
Asy mptotic
Sig.b
Lower Bound Upper Bound
Asy mptotic 95% Conf idence
Interv al
The test result v ariable(s): EDS, TestTerapeutic has at least one tie between the posit iv e actual
state group and the negativ e actual state group. Stat istics may be biased.
Under the nonparametric assumptiona.
Null hy pothesis: t rue area = 0.5b.
Figure X.8. Balance
sensitivity/specificity for EDS vs
Therapeutic test in GERD
diagnosis associated to chronic
cough
31
X.3.5. Evaluation of clinical characteristics of patients with potentially etiologic GERD
chronic cough
Typical symptoms were present in over half of patients falling within the ranges reported
in the literature. The same inverse relationship was noticed between typical reflux symptoms the
and presence of esophagitis, like in the case of the other extradigestive manifestations (Table
X.4).
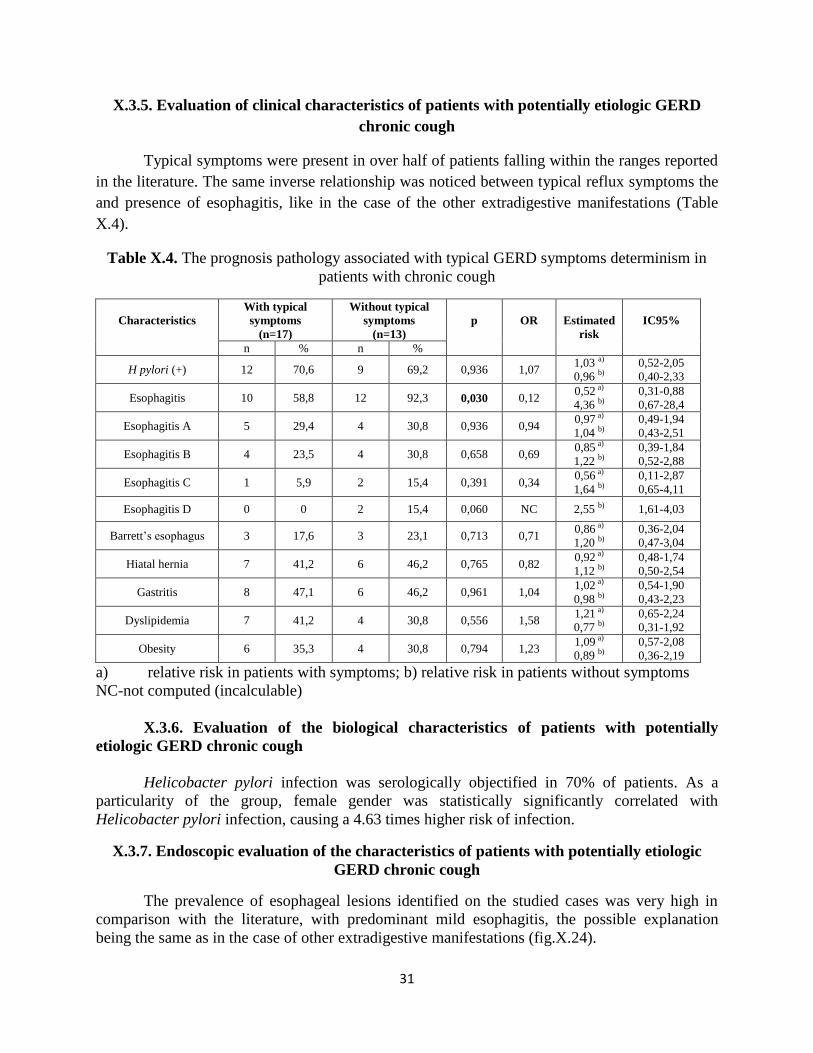
Table X.4. The prognosis pathology associated with typical GERD symptoms determinism in
patients with chronic cough
Characteristics
With typical
symptoms
(n=17)
Without typical
symptoms
(n=13)
p
OR
Estimated
risk
IC95%
n % n %
H pylori (+) 12 70,6 9 69,2 0,936 1,07 1,03 a)
0,96 b)
0,52-2,05
0,40-2,33
Esophagitis 10 58,8 12 92,3 0,030 0,12 0,52 a)
4,36 b)
0,31-0,88
0,67-28,4
Esophagitis A 5 29,4 4 30,8 0,936 0,94 0,97 a)
1,04 b)
0,49-1,94
0,43-2,51
Esophagitis B 4 23,5 4 30,8 0,658 0,69 0,85 a)
1,22 b)
0,39-1,84
0,52-2,88
Esophagitis C 1 5,9 2 15,4 0,391 0,34 0,56 a)
1,64 b)
0,11-2,87
0,65-4,11
Esophagitis D 0 0 2 15,4 0,060 NC 2,55 b) 1,61-4,03
Barrett’s esophagus 3 17,6 3 23,1 0,713 0,71 0,86 a)
1,20 b)
0,36-2,04
0,47-3,04
Hiatal hernia 7 41,2 6 46,2 0,765 0,82 0,92 a)
1,12 b)
0,48-1,74
0,50-2,54
Gastritis 8 47,1 6 46,2 0,961 1,04 1,02 a)
0,98 b)
0,54-1,90
0,43-2,23
Dyslipidemia 7 41,2 4 30,8 0,556 1,58 1,21 a)
0,77 b)
0,65-2,24
0,31-1,92
Obesity 6 35,3 4 30,8 0,794 1,23 1,09 a)
0,89 b)
0,57-2,08
0,36-2,19
a) relative risk in patients with symptoms; b) relative risk in patients without symptoms
NC-not computed (incalculable)
X.3.6. Evaluation of the biological characteristics of patients with potentially
etiologic GERD chronic cough
Helicobacter pylori infection was serologically objectified in 70% of patients. As a
particularity of the group, female gender was statistically significantly correlated with
Helicobacter pylori infection, causing a 4.63 times higher risk of infection.
X.3.7. Endoscopic evaluation of the characteristics of patients with potentially etiologic
GERD chronic cough
The prevalence of esophageal lesions identified on the studied cases was very high in
comparison with the literature, with predominant mild esophagitis, the possible explanation
being the same as in the case of other extradigestive manifestations (fig.X.24).
32
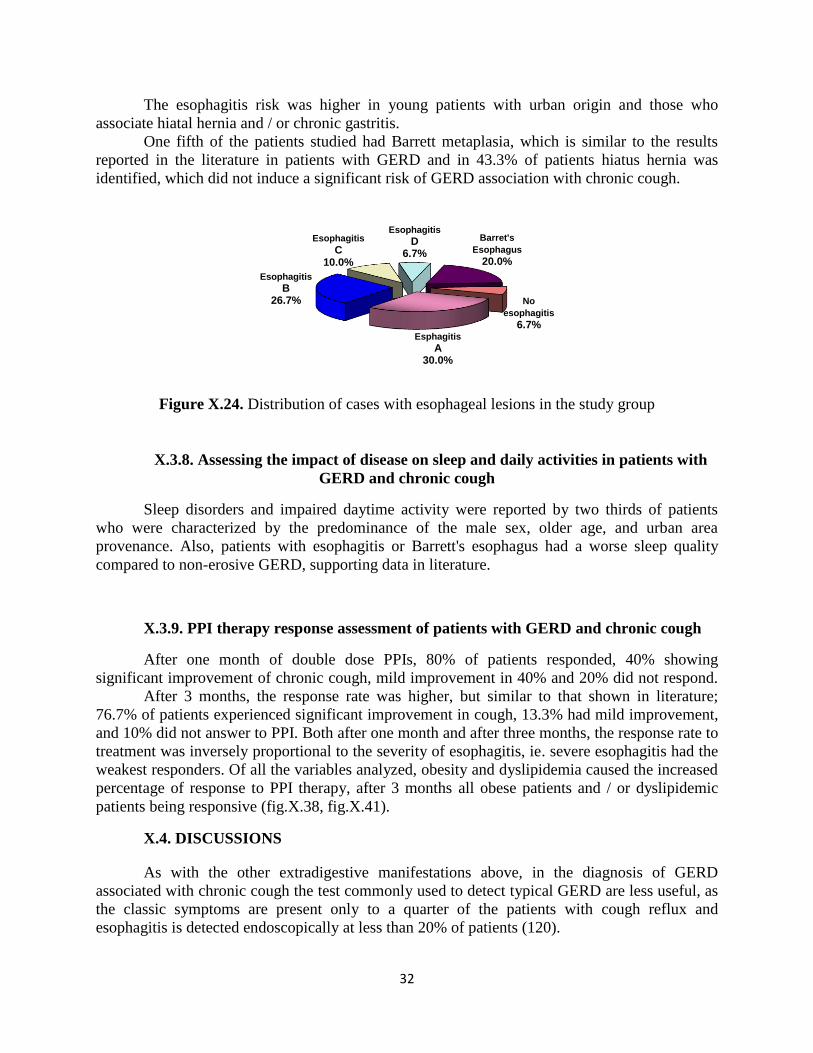
The esophagitis risk was higher in young patients with urban origin and those who
associate hiatal hernia and / or chronic gastritis.
One fifth of the patients studied had Barrett metaplasia, which is similar to the results
reported in the literature in patients with GERD and in 43.3% of patients hiatus hernia was
identified, which did not induce a significant risk of GERD association with chronic cough.
Figure X.24. Distribution of cases with esophageal lesions in the study group
X.3.8. Assessing the impact of disease on sleep and daily activities in patients with
GERD and chronic cough
Sleep disorders and impaired daytime activity were reported by two thirds of patients
who were characterized by the predominance of the male sex, older age, and urban area
provenance. Also, patients with esophagitis or Barrett's esophagus had a worse sleep quality
compared to non-erosive GERD, supporting data in literature.
X.3.9. PPI therapy response assessment of patients with GERD and chronic cough
After one month of double dose PPIs, 80% of patients responded, 40% showing
significant improvement of chronic cough, mild improvement in 40% and 20% did not respond.
After 3 months, the response rate was higher, but similar to that shown in literature;
76.7% of patients experienced significant improvement in cough, 13.3% had mild improvement,
and 10% did not answer to PPI. Both after one month and after three months, the response rate to
treatment was inversely proportional to the severity of esophagitis, ie. severe esophagitis had the
weakest responders. Of all the variables analyzed, obesity and dyslipidemia caused the increased
percentage of response to PPI therapy, after 3 months all obese patients and / or dyslipidemic
patients being responsive (fig.X.38, fig.X.41).
X.4. DISCUSSIONS
As with the other extradigestive manifestations above, in the diagnosis of GERD
associated with chronic cough the test commonly used to detect typical GERD are less useful, as
the classic symptoms are present only to a quarter of the patients with cough reflux and
esophagitis is detected endoscopically at less than 20% of patients (120).
Esphagitis
A30.0%
Esophagitis
B26.7%
Esophagitis
C10.0%
Esophagitis
D6.7%
Barret's
Esophagus
20.0%
No
esophagitis
6.7%

33
The percentage of association between GERD and chronic cough we found is higher than
that estimated in literature. This may be due to the study methodology, selection of patients for
enrollment being very rigorous. We excluded the most common etiologies possible that could
explain chronic cough and factors that could influence the association between GERD and
cough. Also, this percentage reflects the prevalence of the association between GERD and cough
and not the temporal relationship between them, which was established by esophageal
impedance-pH metry, according to the protocol, in only one patient.
In front of a patient with unexplained chronic cough, the doctor should suspect GERD as
etiologic substrate of cough and refer the patient to accurately assess and establish the
gastroenterology therapeutic conduct.
Comparing the performance parameters of the therapeutic test versus UDE, it was found
that both methods are less sensitive for the diagnosis of GERD as an etiologic substrate of
chronic cough.
As a feature of our casuistry, female gender increased the risk of infection with
Helicobacter pylori in patients studied. The explanation of this difference can only be
speculated, possibly due to the different hormonal status of the two sexes, knowing that oxytocin
plays an important role in gastric emptying.
Treatment of chronic cough suspected to be GERD induced remains a controversial topic
in literature, although it has been widely studied in numerous clinical trials. The results reported
by are more varied and inconsistent, because of important limitations and methodological
problems, the most common being the small number of patients included and the lack of placebo
control group.
After 3 months, the response rate was higher than that in a month, but similar to that
shown by the literature. The response to PPI was inversely proportional to the severity of
esophagitis, ie severe esophagitis had the weakest responders. Of all the variables analyzed,
obesity and dyslipidemia caused the increased percentage of response to PPI therapy, after 3
months all obese patients and / or dyslipidemic patients being responsive.
X.5. CONCLUSIONS
GERD-induced chronic cough is a true diagnostic challenge, the usual tests commonly
applied to detect typical GERD being less useful in this case; the therapeutic test with PPI and
UDE proved not sufficiently efficient for the diagnosis of reflux cough. The asociation between
GERD and chronic cough was identified in our study in a high percentage of patients,
emphasizing the importance of gastroenterological evaluation of patients with chronic cough
who were excluded from other causes (ENT, respiratory, allergic or cardiac).
Most patients was characterized by the following traits: male, average age under 50 years
and urban origin. Coffee consumption, obesity and dyslipidemia are factors which induced an
increased risk of GERD with the combination of a chronic cough, respectively, which are in
agreement with data reported by a number of previous studies.
Typical symptoms were present in over half of patients falling within the range of values
reported in literature. An inverse relationship was noted between the presence of typical
symptoms of GERD and reflux esophagitis.
Helicobacter pylori infection has been objectified in an increased number of patients,
female gender increased the risk of infection, which is a feature of the study group.
34
The prevalence of esophageal lesions was very high in comparison with the literature, the
majority of cases falling within the degrees of mild esophagitis. Esophagitis risk was higher in
patients with younger age, urban origin or hiatus hernia.
Sleep disorders and impaired daytime activity were declared by two thirds of patients,
mostly males, of older age and of urban origin. Also, patients with esophagitis or Barrett's
esophagus had a worse sleep quality compared to non-erosive GERD.
PPI therapy was followed by an increased response rate after 3 months, similar to the data
presented by the literature. Extending treatment with PPI to 90 days increased the response rate
of the patients studied. The response rate to treatment was inversely proportional to the severity
of esophagitis, severe esophagitis having the weakest responders, while obesity and dyslipidemia
caused the highest percentage of increased response to therapy with PPI.
XI. COMPARATIVE ASSESSMENT OF EXTRADIGESTIVE
MANIFESTATIONS POSSIBLY INDUCED BY THE
GASTROESOPHAGEAL REFLUX DISEASE
XI.1. The aim of this study was the comparative analysis in demographic, clinical,
biological, endoscopic and therapeutic terms of the patients with extradigestive manifestations
(chronic laryngitis, asthma and chronic cough respectively) supposedly induced by GERD.
XI.2. MATERIAL AND METHOD
We performed a prospective descriptive case-control study comparing patients with
extradigestive manifestations to which we confirmed the diagnosis of GERD according to the
previously established protocol. Patients were analyzed in demographic data, clinical, biological,
endoscopic and therapeutic response terms.
Statistical analysis
The data were statistically analyzed using a centralized SPSS 18.0 database (SPSS Inc.,
Chicago, IL, USA) F ANOVA -test and the correlation Kruskall-Wallis.
XI.3. RESULTS
Study groups were constituted as follows:
• Group I - 90 patients with GERD and chronic laryngitis, which represents 80.4% of the 112
patients who were suspected of GERD etiologic substrate laryngitis
• Group II - 39 patients, representing 88.6% of the 44 patients known to have bronchial asthma
which confirmed suspicion of GERD
• Group III - 30 patients, representing 85.7% of the 35 patients known to have chronic cough,
which confirmed suspicion of GERD.
35
Demographic characteristics
The gender distribution of study groups showed homogeneity, registering slightly higher
frequency of male patients in all groups.
With a wide variation, the age of patients with chronic laryngitis ranged between 20-76
years, with a mean of 49.94 ± 14.36 years and a median of 50 years. In the group of patients with
asthma, the average age was slightly higher (51 ± 13.43 years), with a median of 50 years. In
patients with chronic cough, age ranged from 28-81 years, with a median of 49 years and a mean
of 47.37 ± 13.06 years, which was slightly lower compared to other study groups (p = 0.546)
(table XI.1).
Table XI.1. Statistical indicators, descriptive of age (years) by study groups
Study group N
Median
St.
deviation
St. error
Confidence interval Min Max
p
FANOVA
test - 95%CI +95%CI
Group I 90 49,94 14,36 1,51 46,94 52,95 20 76
0,546 Group II 39 51,00 13,43 2,15 46,65 55,35 23 77
Group III 30 47,37 13,06 2,38 42,49 52,24 28 81
Total 159 49,72 13,87 1,10 47,54 51,89 20 81
Depending on the area of origin, the structure of the groups was homogenous, the urban
origin being predominant in all groups (74.4%, 79.5% and 76.7%; p = 0.694).
Clinical characteristics
Depending on the presence of typical GERD symptoms, the structure of the groups was
fairly homogeneous, however it should be noted that in the group with GERD and chronic
cough, typical reflux manifestations were more frequent (p = 0.337) (Fig. XI.5).
Group 1 Group 2 Group 3
Figure XI.5. Structure of groups depending on the presence of typical GERD symptoms
The share of smokers was relatively small in the groups with laryngitis and asthma, while
in the group with chronic cough smoking was an exclusion criterion for the group (23.3%;
17.9%; p = 0.490 0% respectively). The proportion of patients that were coffee consumers was
increased in all study groups, without statistical significance (55.6%; 59%; 68.7% respectively p
= 0.296).
Obesity was significantly more frequent in patients with chronic cough versus the other
groups (15.6%, 28.2% and 33.3%; p = 0.025).
36
Biological features
Helicobacter pylori infection has been objectified in the highest percentage (70%) in
patients with chronic cough; differences between groups did not reach statistical significance
(55.6% and 59%; p = 0.184) (fig.XI.10).
Figure XI.10. The distribution of patients with Helicobacter pylori by study groups
The distribution of cases with dyslipidemia showed a share of 36.7% in patients with
chronic cough, but the percentage was not significantly increased compared to that of the group
with laryngitis (26.7%) or asthma (33.3% ) (p = 0.260).
Endoscopic characteristics
Esophagitis was more frequently observed in patients with chronic cough (73.3%), but
the percentage differences were not significant compared with other study groups (62.2% and
71.5%) (p = 0.154) (Fig.XI.12).
Figure XI.12. The distribution of patients with esophagitis by study groups
Barrett's esophagus was noted in 20% of patients with chronic cough and 17.9% in those
with poorly controlled asthma therapy, a significantly higher frequency of chronic laryngitis
compared to group (p = 0.002). Hiatal hernia was more frequently observed in patients with
asthma (53.8%), but the percentage differences were not statistically significant compared with
other study groups (40.0% and 43.3%) (p = 0.094).
Impact of the disease on sleep and daily activities of patients
The share of impaired sleep and impact on daily activity was increased in all study
groups (56.7%; 53.8%; 66.7% respectively p = 0.531).
0
20
40
60
80
55.6 59
70
%
Lot I
Lot II
Lot III
0
20
40
60
80
55.6 59
70
%
Lot I
Lot II
Lot III
37
Response to treatment with PPI
The response after a month was generally the same in the groups analyzed, being
dominated by the significant improvement with shares of 40% in patients with chronic cough and
54.4% in those with laryngitis (p = 0.519). After 3 months of treatment with PPI significant
improvements were noted in 75.6% of patients with laryngitis and in 76.7% of those with
chronic cough, slightly higher frequencies compared to the lot with asthma, where significant
improvement was observed only in 56.4% of patients. However, percentage distributions did not
statistically differ significantly.
XI.4. DISCUSSIONS
Comparing confirmation percentages of GERD in patients with extradigestive
manifestations, it was noticed that the most increased percentage was recorded in the group of
patients with asthma, followed by the group with chronic cough, the group of patients with
chronic laryngitis having the lowest rate of diagnosis confirmation.
Depending on the presence of typical symptoms of GERD, the groups with laryngitis and
asthma were homogeneous, with predominance patients without classic manifestations of GERD,
but the group with chronic cough distinguished by a higher percentage of patients who accused
heartburn and/ or regurgitation. Maybe this was why confirmatory diagnostic rate of GERD in
patients with cough was increased, the diagnosis being relatively easy.
Esophagitis lesions were endoscopically identified with an increased frequency in the
group of patients with chronic cough, followed by the group with asthma and finally the group of
patients with GERD and laryngitis. Relating to the severity of esophagitis, it was observed that
mild esophagitis was found at an increased proportion in patients with asthma, laryngitis
respectively, while severe esophagitis was significantly more frequent in the group with chronic
cough.
If in the group with laryngitis the prevalence of Barrett's esophagus was lower than that
reported in literature, in the other two groups, this complication of GERD was above the value
indicated by data from other studies. It seems therefore that patients with GERD and chronic
cough are more likely to develop severe lesions of esophagitis and Barrett's esophagus compared
with patients showing one of the other extra-digestive manifestations.
Hiatal hernia was most often diagnosed in patients with GERD and asthma versus those
with GERD and cough or GERD and laryngitis, but the percentage differences were not
significant in statistical terms, a result that is consistent with previously published data in the
literature.
Over 50% of patients of all three groups have declared a bad sleep quality and thus an
impairment of their daily activities because of chronic fatigue. In the group with chronic cough
the highest percentage of affected patients was noted, cough is therefore the extra-digestive
manifestation that prompted the most frequent awakenings from sleep with major socio-
professional consequences.
Response rates after one month of treatment with PPI in patients in the three study groups
were comparable. The increased rate of significant improvement was noted in patients with
chronic laryngitis, and the highest percentage of non-responsive patients had GERD and chronic
cough. Patients with GERD and laryngitis, and those with GERD and cough had the highest
percentages of significant improvement (75%) after 3 months of therapy with PPI.
38
XI.5. CONCLUSIONS
Extradigestive manifestations associated with GERD were common and generally
homogeneous in our study; similar to the literature, the groups were marked by the
predominance of males. Although the group of patients who associated GERD and chronic
cough recorded the highest share of young people, and the group with asthma included most
elderly patients, all three categories of extradigestive manifestations affected mostly the young,
representing the active population segment. The diagnosis of GERD with extradigestive
manifestations was established much more in males versus females. Like in the literature data,
we identified a high prevalence of patients with GERD and extradigestive manifestations from
urban areas.
Typical symptoms of GERD were met with preference in patients with GERD and
chronic cough, unlike those with GERD and laryngitis or asthma who were mostly asymptomatic
from a digestive point of view..
Behavioral habits (alcohol, coffee, tobacco) have not resulted in significant differences
between the study groups, while obesity was more common in patients with GERD and cough
compared to other groups. Also, Helicobacter pylori infection and dyslipidemia were noted more
in the group with chronic cough.
The most increased frequency of esophageal lesions overall, and the most severe of them
(C and D grade esophagitis, Barrett's esophagus) was found in the group with chronic cough, and
the lowest in the group with chronic laryngitis. Hiatal hernia was found especially in patients
with GERD and asthma, while chronic gastritis in patients with GERD and cough.
Although more than half the patients in each group declared a bad sleep quality, and
impaired social and professional activities, patients with GERD and cough were the most
affected.
After one month of treatment with double dose PPI, patients with GERD and chronic
cough had the lowest rate of significant improvement, after 3 months these patients had
increased the percentage of significant improvement or complete resolution of extradigestive
manifestations. Of all extradigestive manifestations studied, asthma had the weakest response to
PPI therapy.
XII. GASTRO-ESOPHAGEAL REFLUX DISEASE AND ATRIAL
FIBRILLATION
XII.1. The aim of this study was to evaluate the association between GERD and
paroxysmal non-valvular atrial fibrillation, to investigate whether atrial fibrillation can be
classified as an extradigestive manifestation of GERD.
XII.2. MATERIAL AND METHOD
We conducted a prospective case-control trial, with the inclusion of consecutive patients
over a period of 13 months (July 1, 2014 - July 31 2015), at the Institute of Gastroenterology and
Hepatology Iasi, in collaboration with 3 rd
Medical Clinic from "St. Spiridon" Hospital.
39
XII.2.1. Patients
Inclusion of patients in the study was carried out by a joint team: gastroenterologist and
cardiologist based on the inclusion and exclusion criteria agreed.
Inclusion criteria:
We included patients older than 18 years diagnosed with paroxysmal non-valvular AF
from the Medical Clinic III of the Hospital "St. Spiridon ", to which we confirmed (GERD + AF)
or disproved (non-GERD + AF) the diagnosis of GERD, at the Institute of Gastroenterology and
Hepatology of “St. Spiridon” Hospital, as well as patients without AF, but diagnosed with GERD
(GERD + RS) or without GERD (non-GERD + RS), who gave their consent for consensual
enrollment.
Exclusion criteria:
patients aged under 18
documented valvular AF
persistent or permanent AF
hemodynamically unstable patients with acute coronary syndrome / aortic dissection,
sick sinus syndrome, pericarditis, myocarditis, endocarditis, congenital heart disease,
cardiac surgery, cardiac pacemaker or defibrillator, Wolff-Parkinson-White pre-
excitation syndrome
chronic pulmonary heart, pulmonary embolism, pneumonia
endocrine disorders (hyperthyroidism, pheochromocytoma)
dyselectrolytemia (hypokalemia, hypomagnesemia, hypocalcemia)
neoplasia
psychiatric and neurological pathology (subarachnoid haemorrhage)
history of esophageal surgery
abuse of alcohol or other stimulants (cocaine)
pregnant or lactating women
uncooperative patients / patients who refused enrollment
treatment with PPI in the last 8 weeks.
XII.2.2. Study protocol
All patients were investigated in the cardiology service by history and physical
examination, ECG, Holter ECG, echocardiography and biological dosages and in the
gastroenterology service by history, clinical examination and UDE. Paroxysmal non-valvular
atrial fibrillation was defined according to the current guidelines as paroxysmal AF (ECG
presence of three elements: irregular RR intervals, the absence of P waves and fibrillation
irregular activity, with a frequency of 400-600/ minute, with spontaneous remission or under
antiarrhythmic medication in less than 7 days), without rheumatic mitral stenosis, prosthetic
valve or mitral valve repair (475). The diagnosis of GERD was determined on the basis of
clinical symptoms (according to the Montreal Consensus) (7): heartburn and/ or regurgitation of
at least 2-3 times / week, perceived as "troublesome" by patients.
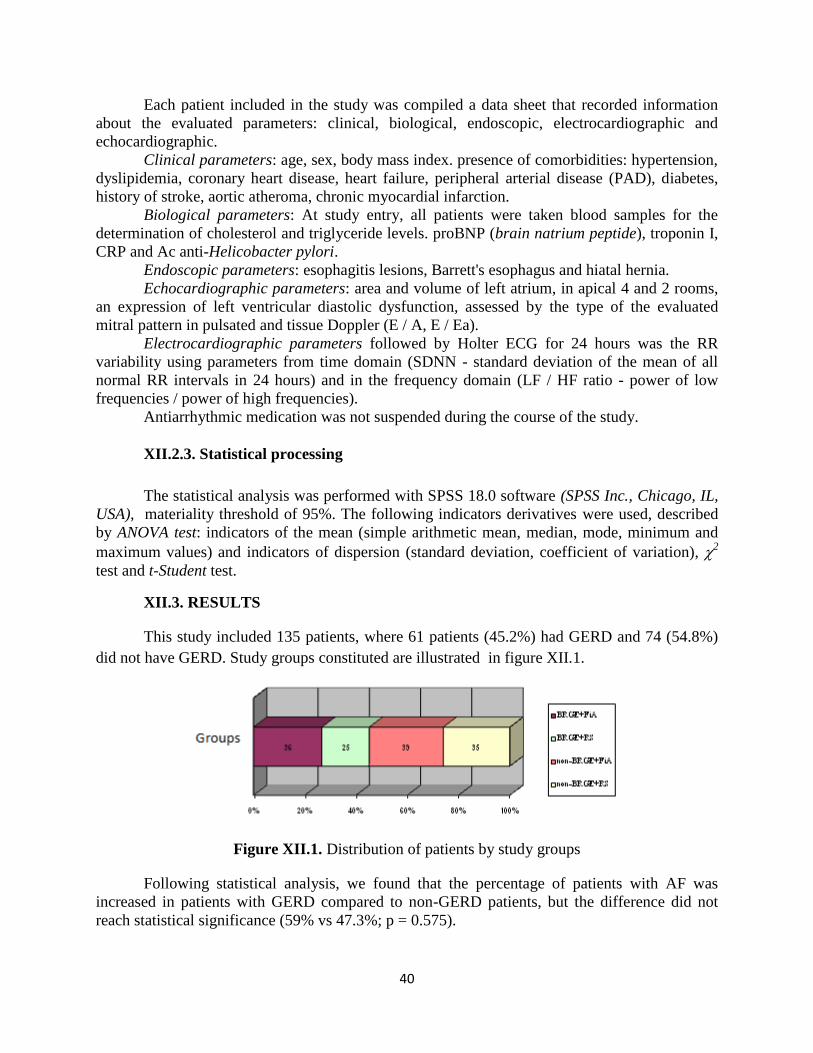
40
Each patient included in the study was compiled a data sheet that recorded information
about the evaluated parameters: clinical, biological, endoscopic, electrocardiographic and
echocardiographic.
Clinical parameters: age, sex, body mass index. presence of comorbidities: hypertension,
dyslipidemia, coronary heart disease, heart failure, peripheral arterial disease (PAD), diabetes,
history of stroke, aortic atheroma, chronic myocardial infarction.
Biological parameters: At study entry, all patients were taken blood samples for the
determination of cholesterol and triglyceride levels. proBNP (brain natrium peptide), troponin I,
CRP and Ac anti-Helicobacter pylori.
Endoscopic parameters: esophagitis lesions, Barrett's esophagus and hiatal hernia.
Echocardiographic parameters: area and volume of left atrium, in apical 4 and 2 rooms,
an expression of left ventricular diastolic dysfunction, assessed by the type of the evaluated
mitral pattern in pulsated and tissue Doppler (E / A, E / Ea).
Electrocardiographic parameters followed by Holter ECG for 24 hours was the RR
variability using parameters from time domain (SDNN - standard deviation of the mean of all
normal RR intervals in 24 hours) and in the frequency domain (LF / HF ratio - power of low
frequencies / power of high frequencies).
Antiarrhythmic medication was not suspended during the course of the study.
XII.2.3. Statistical processing
The statistical analysis was performed with SPSS 18.0 software (SPSS Inc., Chicago, IL,
USA), materiality threshold of 95%. The following indicators derivatives were used, described
by ANOVA test: indicators of the mean (simple arithmetic mean, median, mode, minimum and
maximum values) and indicators of dispersion (standard deviation, coefficient of variation), 2
test and t-Student test.
XII.3. RESULTS
This study included 135 patients, where 61 patients (45.2%) had GERD and 74 (54.8%)
did not have GERD. Study groups constituted are illustrated in figure XII.1.
Figure XII.1. Distribution of patients by study groups
Following statistical analysis, we found that the percentage of patients with AF was
increased in patients with GERD compared to non-GERD patients, but the difference did not
reach statistical significance (59% vs 47.3%; p = 0.575).

41
Clinical parameters
AF patients with GERD and AF were characterized by the predominance of females, at
an average age of 60 years and overweight status.
Regarding comorbidities, heart failure was significantly more prevalent in patients with
GERD and AF, entailing a risk of association estimated 1.65 times higher. In patients with AF,
aortic atheroma statistically significantly increased relative risk of GERD, 42%, making the
aortic atheroma a possible risk factor for the combination of the two pathologies.
Biological parameters
In the studied cases, we found the most increased medium values of proBNP in patients
with AF, irrespective of the presence of GERD.
By analyzing the relationship between the average value of troponin I and the presence of
AF in patients with GERD, we found that structural remodeling of the left atrium through atrial
fibrosis was not influenced by the presence of GERD.
We found no statistically significant differences between patients with GERD and AF
versus other study groups regarding CRP value.
Although the literature indicates that Helicobacter pylori infection increases the risk of
GERD association with AF, our study did not confirm this hypothesis.
Dyslipidemia, a risk factor for AF and GERD, increased the risk of association solely on
the basis of hypertriglyceridemia, a relationship that could not also be established in the case of
serum cholesterol.
Endoscopic parameters
Half of the patients with GERD + AF showed esophagitis lesions in endoscopic
examination, the risk that patients with GERD develop AF in the presence of esophagitis was 2.5
times higher (Table XII.7).
Hiatal hernia was found in a small percentage of patients with GERD + AF and there was
no significant difference compared with the group with AF and without GERD.
Table XII.7. Endoscopic parameters by study groups
Endoscopic
result
BRGE+FiA non-BRGE+FiA χ
2 p RR IC95%
n % N %
Esophagitis 18 50,0 3 7,7 17,88 0,001 2,57 1,70-3,90
Barrett’s
esophagus
2 5,6 1 2,6 0,44 0,506 1,41 0,61-3,26
Hiatal hernia 7 19,4 6 15,4 0,22 0,643 1,15 0,65-2,03
Echocardiographic parameters
Of all the echocardiographic parameters analyzed, the area and the average volume of
AS, as markers of LA structural remodeling, and the parameters of velocity, E / A and E / Ea, as
markers of diastolic dysfunction of the left ventricle, only in the case of AS volume was there
registered an average higher in patients with GERD + AF compared to other study groups, but
the differences did not reach statistical significance (fig.XII.14).
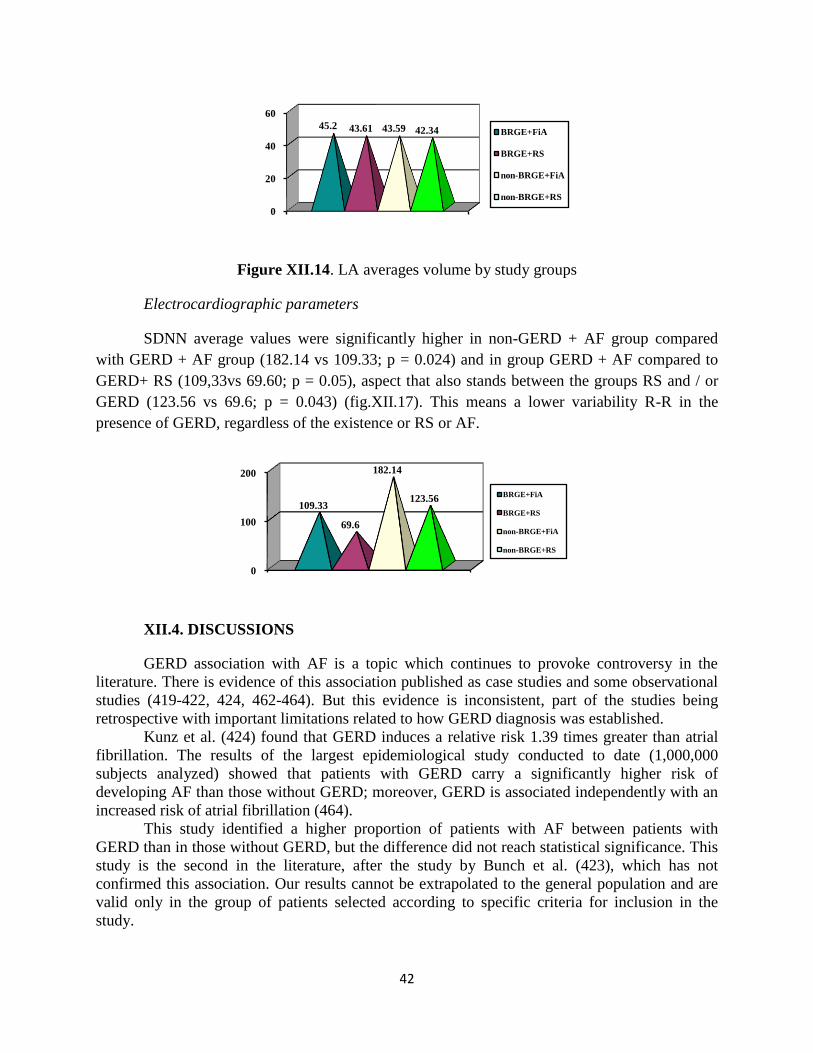
42
Figure XII.14. LA averages volume by study groups
Electrocardiographic parameters
SDNN average values were significantly higher in non-GERD + AF group compared
with GERD + AF group (182.14 vs 109.33; p = 0.024) and in group GERD + AF compared to
GERD+ RS (109,33vs 69.60; p = 0.05), aspect that also stands between the groups RS and / or
GERD (123.56 vs 69.6; p = 0.043) (fig.XII.17). This means a lower variability R-R in the
presence of GERD, regardless of the existence or RS or AF.
XII.4. DISCUSSIONS
GERD association with AF is a topic which continues to provoke controversy in the
literature. There is evidence of this association published as case studies and some observational
studies (419-422, 424, 462-464). But this evidence is inconsistent, part of the studies being
retrospective with important limitations related to how GERD diagnosis was established.
Kunz et al. (424) found that GERD induces a relative risk 1.39 times greater than atrial
fibrillation. The results of the largest epidemiological study conducted to date (1,000,000
subjects analyzed) showed that patients with GERD carry a significantly higher risk of
developing AF than those without GERD; moreover, GERD is associated independently with an
increased risk of atrial fibrillation (464).
This study identified a higher proportion of patients with AF between patients with
GERD than in those without GERD, but the difference did not reach statistical significance. This
study is the second in the literature, after the study by Bunch et al. (423), which has not
confirmed this association. Our results cannot be extrapolated to the general population and are
valid only in the group of patients selected according to specific criteria for inclusion in the
study.
0
20
40
60
45.2 43.61 43.59 42.34 BRGE+FiA
BRGE+RS
non-BRGE+FiA
non-BRGE+RS
0
100
200
109.33
69.6
182.14
123.56BRGE+FiA
BRGE+RS
non-BRGE+FiA
non-BRGE+RS
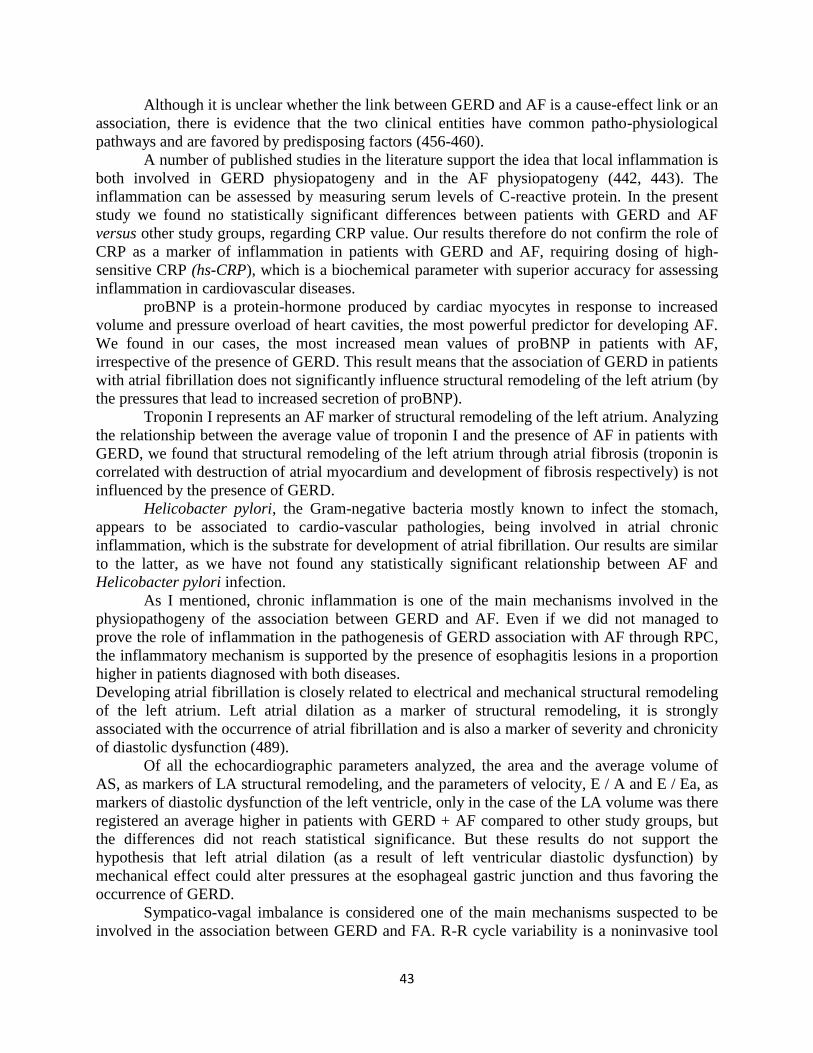
43
Although it is unclear whether the link between GERD and AF is a cause-effect link or an
association, there is evidence that the two clinical entities have common patho-physiological
pathways and are favored by predisposing factors (456-460).
A number of published studies in the literature support the idea that local inflammation is
both involved in GERD physiopatogeny and in the AF physiopatogeny (442, 443). The
inflammation can be assessed by measuring serum levels of C-reactive protein. In the present
study we found no statistically significant differences between patients with GERD and AF
versus other study groups, regarding CRP value. Our results therefore do not confirm the role of
CRP as a marker of inflammation in patients with GERD and AF, requiring dosing of high-
sensitive CRP (hs-CRP), which is a biochemical parameter with superior accuracy for assessing
inflammation in cardiovascular diseases.
proBNP is a protein-hormone produced by cardiac myocytes in response to increased
volume and pressure overload of heart cavities, the most powerful predictor for developing AF.
We found in our cases, the most increased mean values of proBNP in patients with AF,
irrespective of the presence of GERD. This result means that the association of GERD in patients
with atrial fibrillation does not significantly influence structural remodeling of the left atrium (by
the pressures that lead to increased secretion of proBNP).
Troponin I represents an AF marker of structural remodeling of the left atrium. Analyzing
the relationship between the average value of troponin I and the presence of AF in patients with
GERD, we found that structural remodeling of the left atrium through atrial fibrosis (troponin is
correlated with destruction of atrial myocardium and development of fibrosis respectively) is not
influenced by the presence of GERD.
Helicobacter pylori, the Gram-negative bacteria mostly known to infect the stomach,
appears to be associated to cardio-vascular pathologies, being involved in atrial chronic
inflammation, which is the substrate for development of atrial fibrillation. Our results are similar
to the latter, as we have not found any statistically significant relationship between AF and
Helicobacter pylori infection.
As I mentioned, chronic inflammation is one of the main mechanisms involved in the
physiopathogeny of the association between GERD and AF. Even if we did not managed to
prove the role of inflammation in the pathogenesis of GERD association with AF through RPC,
the inflammatory mechanism is supported by the presence of esophagitis lesions in a proportion
higher in patients diagnosed with both diseases.
Developing atrial fibrillation is closely related to electrical and mechanical structural remodeling
of the left atrium. Left atrial dilation as a marker of structural remodeling, it is strongly
associated with the occurrence of atrial fibrillation and is also a marker of severity and chronicity
of diastolic dysfunction (489).
Of all the echocardiographic parameters analyzed, the area and the average volume of
AS, as markers of LA structural remodeling, and the parameters of velocity, E / A and E / Ea, as
markers of diastolic dysfunction of the left ventricle, only in the case of the LA volume was there
registered an average higher in patients with GERD + AF compared to other study groups, but
the differences did not reach statistical significance. But these results do not support the
hypothesis that left atrial dilation (as a result of left ventricular diastolic dysfunction) by
mechanical effect could alter pressures at the esophageal gastric junction and thus favoring the
occurrence of GERD.
Sympatico-vagal imbalance is considered one of the main mechanisms suspected to be
involved in the association between GERD and FA. R-R cycle variability is a noninvasive tool
44
useful for assess the balance between the two components of the autonomic nervous system: the
sympathetic and parasympathetic, and for assessing vulnerability and arythmogenicity
fibrillation. VRR decreases when there is a predominance of sympathetic activity and
conversely, increases when the parasympathetic prevails, a lower value of VRR signifying an
increase of atrial vulnerability and arythmogenicity.
According to the European Society of Cardiology, the most used methods for
determining VRR are those in time and frequency domain in Holter ECG monitoring. In the time
domain, we analyzed the SDNN parameter (standard deviation of the mean R-R normal intervals
within 24 hours) and in the frequency domain, we calculated the ratio between the powers of low
and high frequencies, LF / HF. We obtained statistically significant differences only in the case
of the variable of time. SDNN value was statistically significantly lower in patients with GERD
than in those without GERD, regardless of the presence of AF. This shows a greater
arythmogenicity given by GERD and supports the theory of autonomic system imbalance as a
mechanism of association of GERD with AF.
XII.5. CONCLUSIONS
Atrial fibrillation was more common in patients with GERD, but without statistically
significant difference compared with patients without GERD. The present study is the second
study that does not demonstrate a statistically significant association relationship between GERD
and AF.
A feature of the sample studied was the predominance of females in patients with GERD
and AF, contrary to data reported by most studies published so far, which might suggest that the
female population in the region of N-E Romania is more prone to develop this association.
Inclusion criteria for this study could still create biases in data interpretation. Similar to the
literature, the average age of patients with GERD and AF in our study was 60 years, indicating
the older age as factor for the combination of the two pathologies.
Overweight status was not found to be a risk factor for GERD association with AF, but a
feature of the study is the absence of obesity in patients of the study group. Dyslipidemia on the
basis of hypertriglyceridemia was correlated in our study with the presence of GERD and AF.
Regarding associated comorbidities, heart failure induced an increased risk of developing
a paroxysm of AF in patients with GERD, while aortic atheroma increased risk of GERD in
patients with AF, results that are consistent with the literature. Helicobacter pylori infection has
not been shown to be a risk factor for the combination of GERD and AF.
The theory of inflammation as a pathophysiological mechanism involved in the
association between GERD and AF was sustained in our study by the presence of esophagitis
lesions identified in a higher percentage in patients with GERD and AF, but could not be
supported by CRP, as a marker of biological inflammation of the left atrium. The theory of the
mechanical effect of dilatation of the left atrium on the esophagus has not proven to be one of the
pathophysiological mechanisms involved in the association of the two pathologies in terms of
biological or echocardiographic parameters analyzed. Patients with GERD showed a reduced R-
R cycles variability, regardless of the presence of AF, which reflects an increased
arythmogenicity induced by GERD and supports the theory of the autonomic system imbalance
as a mechanism of association of GERD with AF.

45
XVI. GENERAL CONCLUSIONS
1. Our study revealed an increased prevalence of the association between GERD and
extradigestive manifestations, stressing the importance of gastroenterological evaluation in
patients with chronic laryngitis, poorly controlled asthma, chronic cough, potentially etiologic
GERD.
2. The diagnosis of GERD with extradigestive manifestations was an extremely difficult
task, challenging, given that at present there is no gold standard method to demonstrate the
causality of these clinical conditions.
3. Of all the diagnosis methods used in the present study, the esophageal impedance-pH
metry has proven to be the tool with the best diagnostic yield, being a good predictor regardless
of the presence or absence of typical symptoms of reflux.
4. Helicobacter pylori infection did not significantly influenced the risk of association
between GERD and extradigestive manifestations.
5. Typical GERD symptoms were met with preference in patients with GERD and
chronic cough, unlike those with GERD and laryngitis or asthma who were mostly asymptomatic
from a digestive point of view and were not good predictors for the presence and severity of
reflux esophagitis and hiatal hernia.
6. In our study, esophagitis lesions were identified in a percentage much higher than that
reported in literature, with mild esophagitis being predominant. The presence of hiatal hernia
was statistically significantly associated with GERD and asthma, GERD and laryngitis
respectively, while chronic gastritis was statistically significantly more frequently associated
with GERD and cough.
7. GERD with extra-digestive manifestations caused a negative impact on sleep and
consequently on daily activities due to decreased professional efficiency and labor productivity,
which is why GERD currently represents a major public health problem, burdening state budget.
8. The rate of favorable response to treatment with double dose PPI was increased in
patients with GERD, regardless of the extra-digestive manifestation, while prolonging therapy
for 3 months resulted in an increased responsiveness to treatment. The therapeutic response to
PPI was inversely proportional to the degree of esophagitis lesions severity.
9. Atrial fibrillation was a clinical condition more common in patients with GERD, but
the association did not reach statistical significance.
10. The results of our study confirmed the theory of inflammation as a pathophysiological
mechanism involved in the association between GERD and AF and also the theory of the
autonomic nervous system imbalance, but did not support the theory of the mechanical effect of
the left atrial dilation on the esophagus.