feasibility of diabetes prevention in arab americans: final focus group report
DESCRIPTION
Sills, S. 2010. "Feasibility of Diabetes Prevention in Arab Americans: Final Focus Group Report" Report for National Diabetes and Digestive and Kidney Diseases Grant #1-R34-DK076663-01A1TRANSCRIPT

FEASIBILITY OF DIABETES PREVENTION IN ARAB AMERICANS
National Diabetes and Digestive and Kidney Diseases Advisory Council
PI: Linda A. Jaber, Pharm.D. Associate Professor ‐ Pharmacy Practice ‐ Wayne State University NIH Grant # 1‐R34‐DK076663‐01A1

R I S K AWAR EN E S S , B A R R I E R S TO P A R T I C I P A T I ON , AND F E A S I B I L I T Y OF I N T E R V EN T I ON :
Focus Group Analysis Report
Prepared by
Stephen J. Sills, PhD Assistant Professor of Sociology
University of North Carolina at Greensboro 320 Graham Building
Greensboro, NC 27402‐6170 Phone 336.792.1191• Fax 336.334.5283
March ∙ 2010

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
i
Table of Contents TABLE OF CONTENTS.................................................................................................................................................. I
TABLES..................................................................................................................................................................... III
FIGURES................................................................................................................................................................... III
BACKGROUND .......................................................................................................................................................... 1
ARAB AMERICANS IN THE DETROIT METROPOLITAN AREA ..............................................................................................................1 FOCUS GROUPS IN DIABETES HEALTH RESEARCH ..........................................................................................................................2
PILOT STUDY............................................................................................................................................................. 3
PROCEDURES .........................................................................................................................................................................4 RESULTS ...............................................................................................................................................................................6 Turn‐Taking ....................................................................................................................................................................6 Verbosity ........................................................................................................................................................................7 Self‐Disclosure ................................................................................................................................................................7
SEPARATE INTERVENTIONS BY SEX..............................................................................................................................................8 PILOT TESTING CONCLUSIONS ...................................................................................................................................................9
INTERVENTION FOCUS GROUPS .............................................................................................................................. 10
PURPOSE OF THE FOCUS GROUPS IN THIS STUDY ........................................................................................................................10 PROCEDURES .......................................................................................................................................................................10 CHARACTERISTICS OF THE PARTICIPANTS ...................................................................................................................................11 GROUP CHARACTERISTICS ......................................................................................................................................................11 Pre‐intervention Groups ...............................................................................................................................................11 Education Conversion Groups.......................................................................................................................................12 Refusal to Participate Groups.......................................................................................................................................12 Post‐Ramadan Group ...................................................................................................................................................13 Lifestyle Completer Groups ..........................................................................................................................................13
POST SESSION EXIT SURVEYS ..................................................................................................................................................13
DIABETES KNOWLEDGE AND HEALTH BELIEFS.......................................................................................................... 15
WHAT IS DIABETES? .............................................................................................................................................................15 Symptoms.....................................................................................................................................................................15 Blood Sugar ..................................................................................................................................................................16 Types of Diabetes .........................................................................................................................................................16 Genetic Predisposition..................................................................................................................................................17 Lifestyle ........................................................................................................................................................................17
ACCULTURATIVE STRESS AS A FACTOR.......................................................................................................................................18 PREVALENCE........................................................................................................................................................................18 RISK PERCEPTION .................................................................................................................................................................19 COMMUNITY AWARENESS......................................................................................................................................................19 DIABETES PREVENTION AND TREATMENT ..................................................................................................................................19 MYTHS...............................................................................................................................................................................20 Herbal Remedies...........................................................................................................................................................21 Stigma ..........................................................................................................................................................................21
BARRIERS TO CARE ...............................................................................................................................................................22
REASONS FOR PARTICIPATION IN INTERVENTION.................................................................................................... 22
FEAR OF THE RISK OF DIABETES FOR SELF OR FAMILY ...................................................................................................................23

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
ii
CONVERSION FROM THE EDUCATION PROGRAM.........................................................................................................................23 OTHER REASONS ..................................................................................................................................................................23
BARRIERS TO PARTICIPATION IN INTERVENTION ..................................................................................................... 24
ISSUES WITH TIME OR SCHEDULING..........................................................................................................................................24 MIXED‐SEX GROUPS .............................................................................................................................................................25
EDUCATIONAL INTERVENTION FEEDBACK................................................................................................................ 25
SUGGESTIONS FOR IMPROVEMENT...........................................................................................................................................27 REASONS TO CONTINUE IN THE LIFESTYLE PROGRAM...................................................................................................................28
LIFESTYLE INTERVENTION FEEDBACK....................................................................................................................... 29
FEEDBACK SURVEY................................................................................................................................................................29 FOCUS GROUP FEEDBACK ......................................................................................................................................................30 Encouragement ............................................................................................................................................................30 Learning How to Count Calories and Shop ...................................................................................................................31 Accomplishing Personal Goals......................................................................................................................................32 Additional Health Benefits............................................................................................................................................33 Impact on Family and Beyond ......................................................................................................................................33
SUGGESTIONS FOR IMPROVEMENTS .........................................................................................................................................34 More Dynamic Content ................................................................................................................................................34 Additional Health Experts.............................................................................................................................................35 Cooking Classes ............................................................................................................................................................35 More Time for Exercise.................................................................................................................................................35 Calorie Count for Arab Foods .......................................................................................................................................36 More Training on How to Teach Others .......................................................................................................................36 Better Cultural Fit of the Intervention ..........................................................................................................................37
CONCLUSIONS AND RECOMMENDATIONS............................................................................................................... 40
KEY FACTORS WHICH INFLUENCED PARTICIPATION .......................................................................................................................40 BARRIERS TO PARTICIPATION...................................................................................................................................................41 OVERALL PROGRAM FEEDBACK ...............................................................................................................................................41
REFERENCES............................................................................................................................................................ 43
APPENDIX A PROJECT DELIVERABLES....................................................................................................................... 45
APPENDIX B TRANSCRIPT CONCORDANCE ............................................................................................................... 47

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
iii
Tables Table 1 ‐ Select Post‐Focus Group Survey Measures.......................................................... 8 Table 2 ‐ Focus Group Scripts ........................................................................................... 10 Table 3 ‐ Post Session Exit Survey Summary Table........................................................... 14 Table 4 ‐ Feedback Survey Summary Table ...................................................................... 29 Table 5 ‐ Concordance of Scripts, Filenames, Group Descriptions, and Project Goals .... 48
Figures Figure 1: Age Distribution of Focus Group Participants ................................................... 11

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
1
Background This analysis of focus group data was completed per the request of Dr. Linda A. Jaber, Principal
Investigator of the Feasibility of Diabetes Prevention in Arab Americans project (NIH R34 Grant #
1‐R34‐DK076663‐01A1). The focus group protocol was designed by Dr. Stephen J. Sills at the University
of North Carolina Greensboro and based on the project proposal submitted to the National Diabetes and
Digestive and Kidney Diseases Advisory Council in 2007. The goal of the focus groups, as stated in the
NIH proposal, was to “identify barriers to participation in a diabetes prevention program and to
demonstrate the feasibility of recruitment and retention by pilot testing a community‐based, culturally
specific diabetes prevention intervention.” In particular, focus groups sought information from
participants that would help in refining the Lifestyle Intervention Program and its complementary
educational intervention for diabetes prevention among Arab Americans.
Arab Americans in the Detroit Metropolitan Area
Arab immigrants have been settling in the United States since the late nineteenth century. According to
the United States Census Bureau estimates for 2008, there were about 1.6 million individuals who claim
Arab ancestry in the US (U.S. Census Bureau, 2008). However, it is recognized that this figure is
inaccurate and well below the actual total. According to the Arab American Institute the true figure of
those who have Arab ancestry is at least 3.5 million (Arab American Institute 2009a). Arab Americans,
both foreign‐born and their descendents, are a steadily growing population in the United States.
Between 1990 and 2000 this population grew by 38% (de la Cruz and Brittingham 2003). While
temporary visitors from the Middle East have dropped in recent years, the number of individuals
permanently immigrating from Arabic‐speaking countries has remained constant post 2001 (Kayyali
2006).
Michigan is home to the largest Arab population in the United States and the second highest
concentration of Arabs outside of the Middle East. The Arab‐American community represents the third
largest minority population in Michigan. About 400,000 Arab Americans live in the Detroit Metropolitan
Area (Arab American Institute 2009b). A previous cross‐sectional, population‐based study of Arab
Americans of Dearborn, Michigan found that the community is largely homogenous with striking

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
2
uniformity in cultural identity based on commonality of the spoken Arabic language, the Muslim faith,
and adherence to traditional values and practices. Most (95%) were immigrants with a mean length of
stay in the US of only 11 years. The majority were Lebanese (65%) followed by Yemenis and Iraqis. A
large proportion came from rural areas of the Middle East. Approximately 69% of men and 49% of
women had completed high school education. About 80% of men were employed, compared to 19% of
women. Acculturation, measured by multiple factors including age at immigration, language proficiency
and preference, friends’ ancestry, and socioeconomic status, was low in men and women (Jaber, Brown,
Hammad, Nowak, Zhu, Ghafoor, and Herman 2003; Jaber, Brown, Hammad, Zhu, and Herman 2003).
Focus Groups in Diabetes Health Research
The focus group, or group interview, is a common methodology that has been used as a means of data
collection in the social sciences for at least a century. Focus groups gained popularity in the 1930s and
40s with Robert K. Merton who used them as a tool for gauging reactions to wartime propaganda
materials (Morgan, 1988; Hollander 2004). Since then, the methodology has been employed in a wide
variety of research settings that call for a deep understanding of a groups’ perspective on a particular
issue. It is through the synergistic, collaborative, and interactive atmosphere of the focus group that
participants are influenced to express many ideas that may have been more difficult to express
individually (Morgan, 1988).
There are many advantages to using focus groups in health‐related research as they provide an effective
method for assessing needs, identifying barriers, framing appropriate health messages, and designing
relevant strategies for outreach (Garfield, Malozowski, Chin, Narayan,Glasgow, Green, Hiss, and
Krumholz 2003). Vincent, Clark, Zimmer, and Sanchez (2006) note that focus groups are an “efficient
method of obtaining information about an underserved population’s experience” (96). Focus groups
produce more in‐depth information than quantitative research methods, yet the value of focus group
research is largely dependent on how well the focus groups are designed and executed and how
carefully the data are collected and analyzed.
Focus groups have often been used when conducting research in ethnic or immigrant communities
especially when developing culturally tailored interventions or instruments (Willgerodt 2003; Rice,
Weglicki, Templin, Hammad, Jamil, & Kulwicki 2003). Health‐related focus group studies in the Arab‐

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
3
American community have included investigations of tobacco use among adolescents (Rice et al 2003),
elders' views about health and social support (Ajrouch 2005), cultural considerations for mental health
counseling (Nassar‐McMillan and Hakim‐Larson 2003), ways in which to enhance health services
(Kulwicki, Miller, and Schim 2000), and on the importance of culturally and linguistically appropriate
health interventions (Shah, Ayash, Pharaon, and Gany 2008).
Investigators have used focus groups to explore diabetes care and behavior change issues among various
cultural groups. Past research has demonstrated the effectiveness of the focus group technique in
identifying important health beliefs and nutrition practices of urban Caribbean Latinos and Native
Americans with diabetes (Quatromoni, Milbauer, Posner, Carballeira, Brunt, Chipkin 1994; Hosey 1993).
They have also been used to identify diabetes care issues for urban African Americans (Anderson,
Satterfield, German, and Anderson, 1996) and Latinos with diabetes (Anderson, Goddard, Garcia,
Guzman, and Vazquez 1998). They are especially useful in studying the cultural, psychosocial, and
contextual influences on self‐care practices relevant to diabetes prevention (Anderson, 2001). Focus
groups can help identify culturally specific health beliefs and which health beliefs are amenable to
change.
Pilot Study Focus groups, though commonly used in health research and quite useful in developing culturally
appropriate interventions, may also present “methodological challenges” (Peek and Fothergill 2009). The
focus group is a social interaction in which customs and normative behaviors of a society may be
reenacted, limiting voice of some within the group. Smithson (2000), notes that some individuals tend to
dominate the discourse in the focus group setting resulting in the silencing of others. Hollander (2004) in
fact says that focus groups are less a methodology and more the site of social process that is being
observed by the facilitator. Hollander (2004) advises researchers to consider the social context of the
focus groups asking:
Who has status or power in the situation? Who speaks first in the discussion? What kinds of thoughts, feelings, or experiences might be expected in the context, and what kinds might not be expected? Are these expectations the same for all participants? What are the

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
4
consequences (both immediate and long term) for individual participants of disclosing sensitive information? What are the potential rewards for conformity or nondisclosure? (627)
The achieved and ascribed statuses of focus group participants may determine the amount of power and
voice one has in the interaction (Peek and Fothergill 2009). The sex of the speaker (or their gender
identity) may play a significant role, in particular when discussing gendered issues. As Morgan notes,
"group interaction requires mutual self‐disclosure, it is undeniable that some topics will be unacceptable
for discussion among some categories of research participants" (1996:140).
Some methodologists recommend segmentation of focus groups (separation on the basis of gender or
other attributes) as a solution to power imbalances or in the case of sensitive topics (Goldman and
McDonald 1987; Morgan 1996). Yet, as Bristol points out, “evidence in support of the gender
assumption is nonexistent” (1999:479). Hollander also notes that segmentation does not necessarily
lead to more disclosure though it may make some participants feel more comfortable (Hollander 2004).
In the case of research with Arab‐Americans though, many researchers have chosen to segment their
groups. While most researchers do not explain their rationale for gender segmentation, Peek and
Fothergill (2009) elaborate on how they decided to segment Arab women from men:
Some of the groups said it would be easier to meet as a mixed male‐female group, while others requested that the interview be conducted with an all‐female or all‐male group. One student told Peek over the telephone that she did not think the Muslim women would be comfortable talking about some of the issues they had faced in front of their male counterparts. Thus, Peek segmented the groups according to sex in part at the request of the students, but she tried to conduct all‐female or all‐male groups if possible because it became apparent that the students in the sex‐segregated groups seemed more comfortable and talked more openly about sensitive topics. (39‐40)
Procedures
During the pilot phase of the project, a series of tests were conducted to determine the degree of
“silencing”, or lack of self‐disclosure, that may occur in mixed‐sex, focus group sessions. Based on our
understanding of gendered roles and behaviors in the Arab‐American community, we contemplated that
in some instances women may feel less likely to disclose health information, health beliefs, or provide
D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
5
candied feedback when men would be present. We also examined if participants felt strong preferences
for delivery of the intervention and educational components of the project in single‐sex or mixed‐sex
settings. Thus, we devised a test in which focus groups were conducted with participants in three
conditions: a male‐only group, female‐only group, and a mixed‐sexed group. The content of the pilot
script dealt primarily with diabetes awareness, perceptions of risk, diabetes health beliefs, and perceived
barriers to health care.
A total of three pilot focus groups were conducted. The groups ranged from eight to twelve participants
and from 90 minutes to 115 minutes in duration. The test compared the volume of linguistic output and
the number of turns taken by each sex in male‐only, female‐only, and mixed‐sex focus groups.
Participants were randomly assigned to a male‐only, female‐only, or mixed group. Most indicated having
families in the USA (19 of 29 mentioned family in the warm‐up). The majority of the women indicated
that they were homemakers (12 of 18). Of those who indicated that they work working outside of the
home, nine were in professional occupations (teachers, engineers, etc.), two were in business, and one
was in a service occupation.
Focus groups were digitally recorded, transcribed, and then translated into English. Qualitative analysis
was performed using MAXqda2 software. The analysis included the generation of thematic codes and
subcodes grounded in the participant’s discourse. Content analysis was also performed using MAXDictio.
All text was coded as being generated by males or females. Character, word, line, and paragraph counts
were made as well as the number of turns per individual. Averages were computed per person per
minute.
In addition, post‐focus group surveys were administered to explore issues of self‐disclosure and to assess
issues with silencing, comfort, and willingness to participate in future focus groups. This strategy has
been a common technique for comparing individual level data to that produced in the group. For
example, Corfman (as cited in Bristol 1999) employed pre‐and post surveys to “gather information on
member characteristics and reactions to the group” (479). The survey also collected demographic
information. Survey responses were coded and entered into a spreadsheet. Simple descriptive and
bivariate analysis was conducted with the survey data using SPSS.

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
6
Results
The primary goal of the series of pilot focus groups was to determine the degree of silencing that may
occur in mixed‐sex Arab focus groups as a result of perceived male dominance. The pilot focus group
design was meant to create a test with male‐only and female‐only control groups and a mixed‐sex
experimental group. However, several complications affected the research design. First, the groups were
not of equal size (one group of 12, one of 8, and one of 9 members), thus the measure (amount of text in
turns, lines, or words) was averaged by the number of group members. Second, the focus groups were
not of the same duration (the women‐only group lasting for 1 hour and 45 minutes, the men‐only for 1
hour and 30 minutes, and the mixed group for 1 hour and 40 minutes). The mixed group was also
imbalanced, with only three males and six females. Finally, at one point about three‐quarters of the way
into the discussion in the experimental mixed group, the facilitator may have biased the outcome by
interjecting that the men were not talking very much:
Facilitator‐ (talking to men) You thought that women are reluctant to speak when men are present… well in this session, women are talking more than you
FG3‐Man3‐ (Smiling) Good
FG3‐Man1‐ Because we are outnumbered
FG3‐Woman2‐ No no it is not about numbers. Women can express themselves freely in front of men.
FG3‐Man1‐ Excuse me I am just joking.
ALL LAUGHING
None‐the‐less, two separate approaches to discourse analysis were performed to compare males and
females and the amount of text produced by each: one looking at turn taking, the other at the amount
of text or utterances produced (verbosity). By all measures, men were found to speak more than women
in all conditions.
Turn‐Taking
On average men took 30 turns in the male‐only group compared to 23 turns for women in the female‐
only group. Men in the mixed group took 41 turns, while women took only 20. Thus, in the mixed group,

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
7
where men were the minority, they spoke more than twice as often as women. Individual analysis shows
that several participants dominated the conversations in their respective focus groups; particularly Man7
in the men‐only group; and Man 3 in the mixed group. Women’s turn taking was more equitably
distributed, though some women clearly took fewer turns than others (see for example Woman 10 and
12 in the female‐only group, and Woman 6 in mixed‐sex group.
Verbosity
Utterances could be measured by the number of words, characters, paragraphs, or lines produced by a
speaker. This quantifies the amount of language an individual contributed to the transcription. A rate can
also be computed based on the average number of words generated per individual per minute (See
Table 3). Using this approach we see that men in both the men‐only as well as the mixed group
produced more utterances. In particular, men in the Mixed group contributed twice as much text to the
transcripts given that were half as many of them. Women’s utterances were, however, consistent in
both the mixed group and the women‐only group.
Self‐Disclosure
It is difficult for a focus group moderator to really tell if someone is holding back information. Often, if
the moderator focuses in on one person alone, the dynamic atmosphere of a focus group will be lost.
We determined that a brief post‐focus group survey would be most helpful in determining if there was
information that was not disclosed during the focus group. Analysis of the post‐test survey shows that
women were more likely to agree with the statement “I had things to say which I kept to myself” than
men (47.0 percent of women compared with 37.5 percent of men). Women were more likely to agree
with the statements “I could have said more than I did” (55.6 percent of women compared with 50.0
percent of men), “I felt awkward sharing in front of the group” (27.8 percent of women compared with
10.0 percent of men) and “I feel more comfortable in same‐sex groups” (64.7 percent of women
compared with 45.5 percent of men). Yet males were more likely to agree with the statement that “I felt
others dominated the discussion” (31.1 percent of women compared with 36.4 percent of men).

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
8
Table 1 ‐ Select Post‐Focus Group Survey Measures
Percent Agree or Strongly Agree
Question F M I had things to say which I kept to myself 47.0 37.5 I could have said more than I did 55.6 50.0 I felt awkward sharing in front of the group 27.8 10.0 I felt others dominated the discussion 31.3 36.4 I feel more comfortable in same‐sex groups 64.7 45.5
Within the mixed group, all three men disagreed with the statement “I had things to say which I kept to
myself,” while three of the six women agreed. Similarly, all of the men disagreed with the statement “I
felt awkward sharing in front of the group” while the same three women agreed. Four of the six women
agreed that “there were uncomfortable moments during the focus group,” while none of the men
agreed. Finally, all three men in the mixed group were neutral on the issue of feeling more comfortable
in same‐sex groups; however, three of the six women strongly agreed that they would be more
comfortable in same‐sex groups.
Separate Interventions by Sex
About a quarter of the participants expressed a clear preference for same‐sex intervention and
education groups. A little more than half of the men in the male‐only group (5 of 8), and two of the
women in the women‐only group seemed to prefer a separation of the sexes for informational sessions.
As one women noted; “possibly we can express ourselves more freely in women session.” Most of the
remaining 29 participants seemed to agree that mixed‐sex groups were acceptable. A male participant in
the mixed group notes, “You should define the community you will deliver the speech to. As an example
in the ICD, we have mixed gender lectures where men and women are seated separately, but in the
same place, where they listen to the same lecture at the same time. However, there are separate
lectures for women only on Wednesdays at 1:00 PM that deals with topics important to women, so it
depends on the place and topic.”
Part of the Lifestyles Intervention Program includes consultation and courses on healthy food
preparations. There was a general consensus that cooking was the “women’s realm” and that many men

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
9
“would not be interested” in attending a course on healthy food preparation. One female participant
commented, “It is a part of the Arabic culture that men are not interested in cooking.” However, another
female participant also observed, “When men attend these sessions, they will communicate with us
better, listen and accept the meals we cook... I think you should invite women and their husbands.” Yet,
this also presented a problem for childcare. One father said, “In my case [only] one of us could attend
because of the children.”
There was an agreement among participants regarding same‐sex versus mixed‐sex exercise classes.
Most felt that separate classes should be offered. The only exception was in walking groups. While there
was debate over who walked faster, men or women, there was agreement that this activity was not
gendered and that mixed groups were fine: “Walking in groups around the neighborhood is encouraging
and supportive. It can be done in group with family, or friends, certainly.” On the other hand, anything
that involved “physical activities that require bending or movements,” were considered to be best
practiced separately.
Pilot Testing Conclusions
By all measures, Arab‐American men were found to take more turns and to speak with more verbosity
than Arab‐American women. Speech in groups with men (male only and mixed sex), tended to be
dominated by a few speakers, while the female group was more equitable in the turn‐taking and
amount of discourse per participant. Women were more reluctant to share in general, yet the male
domination of the mixed‐sex group made the discussion even more awkward for the women and limited
their responses. Thus, the reluctance to self‐disclose in mixed‐sex groups may result in loss of important
information as women were more likely to talk less, more likely to feel awkward, and more likely to keep
information to themselves. Moreover, they indicate preference for same‐sex groups.
These finding have direct implications for future studies with Arab‐American populations using focus
group methods as well as for interventions that include male and female participants. It was clear from
the focus group participants that separate or segmented focus group sessions would work best so as not
to alienate a significant proportion of the Arab‐American community. The findings provide empirical
evidence for the current practices of many qualitative researchers in the Arab‐American community who
already gender‐segment their focus groups.
D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
10
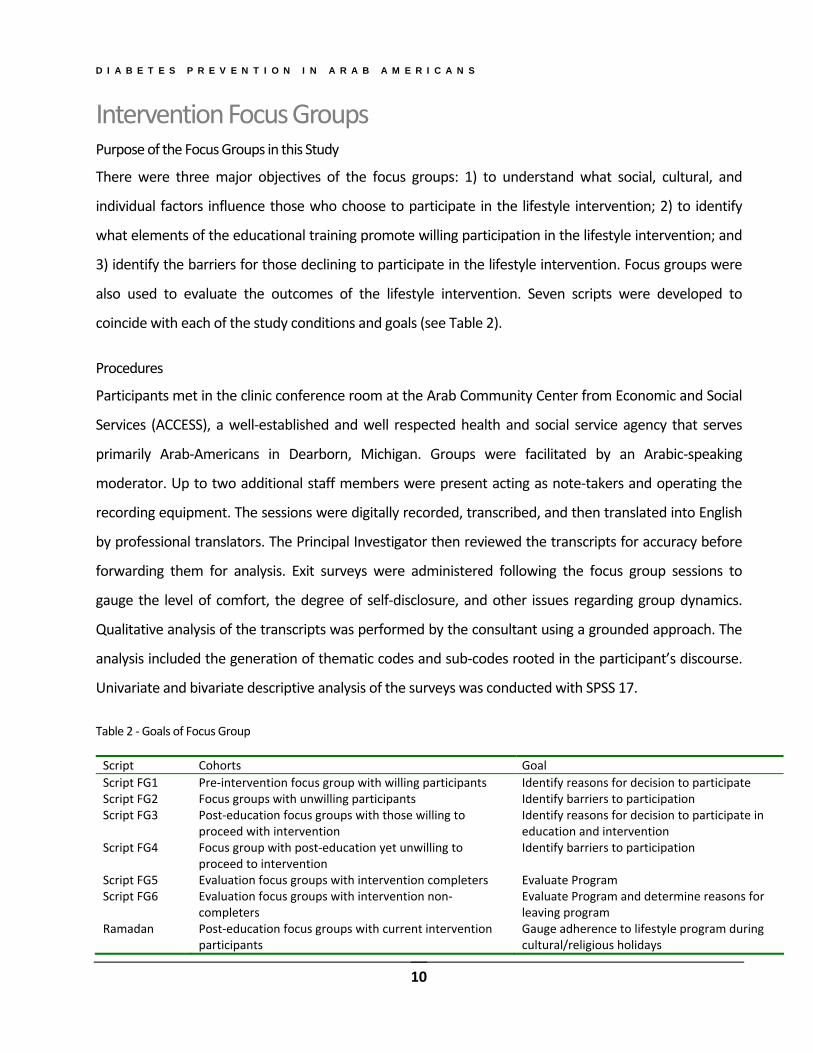
Intervention Focus Groups Purpose of the Focus Groups in this Study
There were three major objectives of the focus groups: 1) to understand what social, cultural, and
individual factors influence those who choose to participate in the lifestyle intervention; 2) to identify
what elements of the educational training promote willing participation in the lifestyle intervention; and
3) identify the barriers for those declining to participate in the lifestyle intervention. Focus groups were
also used to evaluate the outcomes of the lifestyle intervention. Seven scripts were developed to
coincide with each of the study conditions and goals (see Table 2).
Procedures
Participants met in the clinic conference room at the Arab Community Center from Economic and Social
Services (ACCESS), a well‐established and well respected health and social service agency that serves
primarily Arab‐Americans in Dearborn, Michigan. Groups were facilitated by an Arabic‐speaking
moderator. Up to two additional staff members were present acting as note‐takers and operating the
recording equipment. The sessions were digitally recorded, transcribed, and then translated into English
by professional translators. The Principal Investigator then reviewed the transcripts for accuracy before
forwarding them for analysis. Exit surveys were administered following the focus group sessions to
gauge the level of comfort, the degree of self‐disclosure, and other issues regarding group dynamics.
Qualitative analysis of the transcripts was performed by the consultant using a grounded approach. The
analysis included the generation of thematic codes and sub‐codes rooted in the participant’s discourse.
Univariate and bivariate descriptive analysis of the surveys was conducted with SPSS 17.
Table 2 ‐ Goals of Focus Group
Script Cohorts Goal
Script FG1 Pre‐intervention focus group with willing participants Identify reasons for decision to participate Script FG2 Focus groups with unwilling participants Identify barriers to participation Script FG3 Post‐education focus groups with those willing to
proceed with intervention Identify reasons for decision to participate in education and intervention
Script FG4 Focus group with post‐education yet unwilling to proceed to intervention
Identify barriers to participation
Script FG5 Evaluation focus groups with intervention completers Evaluate Program Script FG6 Evaluation focus groups with intervention non‐
completers Evaluate Program and determine reasons for leaving program
Ramadan Post‐education focus groups with current intervention participants
Gauge adherence to lifestyle program during cultural/religious holidays

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
11
Figure 1: Age Distribution of Focus Group Participants
Characteristics of the Participants
Based on exit surveys 65% of participants were female and 35% male. Lebanese participants comprised
the majority (72%); a slightly greater proportion than presented than in the Detroit MSA data reported
earlier. Iraqis were the next largest group (15% of participants), followed by Yemenis (6%). The
remaining 7% included participants from Egypt, Jordan, Kuwait, Sierra Leone, Syria, and the United
States. The average age of participants was 49 years (mean) with a range from 31 years old to 82 years
old (see Figure 1).
Group Characteristics
Including the three pilot groups, a total of seventeen focus groups were conducted between November
2007 and April of 2009 (See Appendix C for a concordance of transcripts, scripts, file names, and stage of
project). The groups ranged from six to fourteen participants.
Pre‐intervention Groups
Three focus groups were conducted in the pre‐intervention stage with participants willing to begin the
Lifestyle Intervention Program (labeled as "Lifestyle Accept"). The goal of these focus groups was to
identify the reasons for participation in the intervention. The first group met on March 20, 2008. All
seven participants were female and from Lebanon. They identified principally as mothers and
D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
12
housewives and were between the ages of thirty‐three and fifty‐two. All but one spoke Arabic in the
home. The second group also met on March 20, 2008 with seven participants ‐ six male and one female
of whom five were Lebanese, one Iraqi, and one Yemeni. No other background information was
collected for the second group. The third group met on October 30, 2008 with fourteen participants;
four men and ten women. The group was divided between Lebanese (6) and Iraqis (4), with one
Jordanian and three others who did not report their nationality. They had been in the United States
between six and thirty‐three years. This group included a mix of stay‐at‐home mothers, skilled
professionals, business owners, and a student.
Education Conversion Groups
There were three focus groups with participants willing to continue to the Lifestyle Intervention Program
after they completed a series of education sessions (labeled as “Education Conversion”). The goal of
these focus groups was to identify the reasons for their decision to participate in the education sessions
and continue to the intervention. Feedback regarding the efficacy of the educational program was also
discussed. The first group met on May 16, 2008. All but one of the nine participants was from Lebanon.
Three of the nine were males. The second group met on June 20, 2008 with six participants. No
demographic information was recorded for this group. The last group met on August 12, 2008 with ten
participants: seven female, three male. The majority of the group members were again from Lebanon,
with one participant from Iraq and another from Syria.
Refusal to Participate Groups
Three focus groups were conducted with individuals who declined participation in the intervention
program (labeled as “Refusal to Participate”). The goal of these focus groups was to identify the reasons
for refusal. The first group was held on June 20, 2008 and included six participants (four males and two
females). Four of these participants were from Lebanon, one was Syrian, and the other Iraqi. All of the
members in this group had attended educational sessions, but declined further participation. On June
27, 2008, another group was held with six participants (three male and three female). Five were from
Lebanon and the sixth was Egyptian. None had participated in the educational sessions. The last group
was held on July 1, 2008 with four females and one male. Five of the groups were Lebanese and the
other was Yemeni. One participant spoke English only.

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
13
Post‐Ramadan Group
Nine participants (four male and five female) were present for the Post‐Ramadan group to gauge their
adherence to Lifestyle Intervention program during this cultural and religious holiday. In particular, the
discussion explored their traditional and customary observance of Ramadan and how they may have
altered these practices as a result of the program.
Lifestyle Completer Groups
Four focus groups were conducted between August of 2008 and April of 2009 with participants who had
completed the Lifestyle Intervention program. The goal of these focus groups was to provide formative
feedback on the program. Participants discussed the things they liked about the program as well as areas
for improvement. Groups varied from 9 to 12 participants. No additional background information was
collected as these individuals were previous attendees of Pre‐Intervention or Educational Conversion
groups.
Post Session Exit Surveys
Following each of the focus groups a post‐session survey was completed by the participants. This was
the same survey as found in the Pilot Focus group sessions. The survey explored the participant’s
comfort level in the group setting, group dynamics, and degree of self‐disclosure.
Complete surveys results are presented by sex in Table 3 on the following page. Overall participants
were comfortable sharing with the groups (88.3% strongly agreed), felt free to express their opinions
(87.5% strongly agreed), and felt that others were open to what they had to say (69.6% strongly agreed).
Some participants did report withholding information. For example, 28.8% agreed or strongly agreed
that they had things to say which they kept to themselves and 37.1% agreed or strongly agreed that they
could have said more than they did. A few (15.7% agreed or strongly agreed) felt awkward sharing in
from of the group while more (21.2% agreed or strongly agreed) felt that others in the group dominated
the discussions. Similarly, a few (13.1% agreed or strongly agreed) felt that there were uncomfortable
moments during the focus group session. Group size was not a major issue as only 9.6% agreed or
strongly agreed that there were too many people in the group. About a third (30.6% agreed or strongly
agreed) would have felt more comfortable in same‐sex groups. This figure was higher for females
(33.3%) than for males (25.7%). Most were happy to participate in the project (85.3% strongly agreed)
and reported that they would participate in a future focus group (78.2% strongly agreed).

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
14
Table 3 ‐ Post Session Exit Survey Summary Table
Strongly Disagree Disagree
Neither Disagree
nor Agree Agree
Strongly Agree
Female 1.3% 0.0% 1.3% 5.1% 92.3%
Male 0.0% 0.0% 0.0% 19.0% 81.0% I was comfortable sharing my perspective in this group setting
Total 0.8% 0.0% 0.8% 10.0% 88.3%
Female 1.3% 0.0% 0.0% 9.0% 89.7%
Male 0.0% 0.0% 0.0% 16.7% 83.3% I felt free to express my own opinions Total 0.8% 0.0% 0.0% 11.7% 87.5%
Female 1.3% 1.3% 0.0% 26.7% 70.7%
Male 0.0% 2.5% 5.0% 25.0% 67.5% I felt others were open to what I had to say Total 0.9% 1.7% 1.7% 26.1% 69.6%
Female 37.7% 23.4% 6.5% 26.0% 6.5%
Male 39.0% 29.3% 9.8% 17.1% 4.9% I had things to say which I kept to myself Total 38.1% 25.4% 7.6% 22.9% 5.9%
Female 30.7% 29.3% 5.3% 18.7% 16.0%
Male 13.2% 31.6% 13.2% 28.9% 13.2% I could have said more than I did Total 24.8% 30.1% 8.0% 22.1% 15.0%
Female 59.2% 21.1% 9.2% 5.3% 5.3%
Male 51.3% 17.9% 5.1% 7.7% 17.9% I felt awkward sharing in front of the group Total 56.5% 20.0% 7.8% 6.1% 9.6%
Female 53.8% 12.8% 6.4% 15.4% 11.5%
Male 50.0% 27.5% 12.5% 5.0% 5.0% I felt others dominated the discussion Total 52.5% 17.8% 8.5% 11.9% 9.3%
Female 65.3% 18.7% 4.0% 5.3% 6.7%
Male 57.5% 12.5% 15.0% 7.5% 7.5% There were uncomfortable moments during the focus group
Total 62.6% 16.5% 7.8% 6.1% 7.0%
Female 56.0% 30.7% 4.0% 6.7% 2.7%
Male 53.8% 28.2% 7.7% 7.7% 2.6% I felt there were too many people in the group
Total 55.3% 29.8% 5.3% 7.0% 2.6%
Female 36.1% 25.0% 5.6% 13.9% 19.4%
Male 46.2% 23.1% 5.1% 15.4% 10.3% I feel more comfortable in same‐sex groups Total 39.6% 24.3% 5.4% 14.4% 16.2%
Female 3.9% 0.0% 0.0% 9.1% 87.0%
Male 0.0% 2.6% 0.0% 15.4% 82.1% I was happy to participate in this research Total 2.6% 0.9% 0.0% 11.2% 85.3%
Female 1.3% 1.3% 2.6% 11.5% 83.3%
Male 2.4% 4.9% 7.3% 17.1% 68.3% I will participate in a future focus group Total 1.7% 2.5% 4.2% 13.4% 78.2%

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
Diabetes Knowledge and Health Beliefs A series of questions were designed to examine the understanding of diabetes and health beliefs
regarding the disease. Specifically, the participants were asked to explain what they knew about the
disease, its symptomatology, the perceived prevalence in the Arab community, their personal risk for
becoming diabetic, and what they understood of ways to lower risk of becoming diabetic. The questions
were asked during the Pilot, Life‐Style Accept, Life‐Style or Education Refuse, and Education Conversion
groups.
What Is Diabetes?
Participants showed a range of understandings, and misunderstandings, about the disease. Some
admitted no knowledge. For example, one participant said she had no personal experience or exposure
to diabetes and had no relatives who had suffered from the disease. Meanwhile others had many family
members who had been afflicted, serving as motivation for them to learn about it. One participant noted
that the death of a family member was partial motivation for them to be present in the study: "…my
brother died because of Diabetes, but I do not know about Diabetes…. I will tell you honestly, because my
brother died from Diabetes. I did not want to know anything about it. I came so that to learn."
Symptoms
Many participants, however, were fairly accurate in reporting the symptoms of diabetes. One participant
identified the following symptoms: “dryness of the mouth, eyes blurring, using the bathroom a lot to
urinate, they feel thirsty a lot.” Another said, "dryness of the mouth, and urinating a lot, in an abnormal
way. In spite of drinking, as if the person has not drank. These are the symptoms. Dizziness. Fatigue
happens towards the end. It raises the blood pressure. Perhaps lowers it."
Several members understood these symptoms as a result of personal contact with someone who is
diabetic:
My husband who is diabetic has dry mouth. He has dry skin. His skin splits. He has dry feet. He has blurred vision. During the night, no matter what he eats, he feels hungry. He wants to eat anything, mostly something sweet.

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
16
Blood Sugar
While participants were generally knowledgeable of the symptoms of diabetes, they did not always
understand its causes. Answers touched on many of the factors associated with increased risk of
diabetes including genetics/family history, stress, high blood pressure, diet, drinking alcohol, lack of
exercise, obesity, and age. Many seemed to understand that the disease is related to the pancreas and
that it results in difficulty regulating blood glucose levels. Thus, they also knew that blood sugar
imbalances are related to food and metabolic processes:
The first thing is the way we eat, the quality of food we eat, eating sweet products more than it is necessary. It is the lack of balance in the body between what is necessary food to eat the necessary food and the sweet products that one eats more.
Participants identified that diabetes results from an imbalance of sugars and is related to the secretion of
insulin: “The body may not secrete sufficient insulin.” They were also aware that this imbalance results
from problems with the pancreas: “It is the malfunctioning of pancreas. To be more specific, when
pancreas malfunctions, there will be sugar either in the blood or in the urine.”
Yet, participants attributed diabetes to a number of causes. One participant felt it was due to the over
consumption of sugar: As the sister mentioned:
I used to think that if one ate more sweets would have more energy. I remember when I used to work in a hotel in Amsterdam, Holland, I would put approximately 6, 7, 8 cubes of sugar. Everyday I would increase sugar cubes. A Belgian told me to be careful. In this way, at the end you will become diabetic. I paid attention. I was young that time and I did not know.
Types of Diabetes
Members of the focus groups comprised of individuals who had not attended education sessions were
very unclear about the types of diabetes: “I think there are two types of diabetes. The most known is
sugar in the urine or in the blood.” Another refuser explained: “There are two types; one when the level
of sugar rises and the other when the level of sugar lowers.” Still others were very unclear as to how
many types: Another “There is up to the limit of seven. The seventh type is the most dangerous.”

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
17
Meanwhile, those who had attended the education sessions correctly identified the two types, as well as
gestational diabetes:
A type for children and a type for adults. For adults, as we said, it is hereditary from third or fourth generation, or it happens from the amount of insulin the liver secretes. Or at the time a baby is born, the mother may have diabetes so the baby is born very big.
A participant in one pre‐intervention group noted that diabetes may develop when a woman is
pregnant. Both groups correctly identified that there were two types of diabetes, but there was
misinterpretation on what the two types were with thinking that they were related to advancement of
the disease: "I think type two is the first stage of Diabetes and type one is the more advanced."
Genetic Predisposition
Participants correctly identified that some people have a genetic predisposition to the disease: "…it is
hereditary. This is more difficult. In case of hereditary, one has to protect oneself more from the normal
person, because he has it in the family." One member of the pre‐intervention focus group explained that
diabetes is inherited from parents: “All I know that some have it through hereditary from parents that
may affect the children. Some people have diabetes from hereditary.”
Lifestyle
The participants clearly recognized that diabetes is in many ways a "preventable" lifestyle disease
making them open to the intervention approach: "I have to care what I should eat, to lessen eating
sweets, fat, and to prevent so as not to have diabetes early on." They also noted that without medication
and modification of lifestyle there would be a long‐term impact on the body: "If one has Diabetes and is
not treated and did not take the right medications, over time, the person will have kidney failure."
Another identified elevated blood pressure and body fat as factors: “Whoever has blood pressure is at
risk for diabetes disease. When a person has other diseases, he is at risk to diabetes disease. Fatness, or
mostly when a person has a large belly is at risk for disease.”

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
18
Acculturative Stress as a Factor
Several participants eluded to their status as immigrants as increasing the risk of diabetes. This was
attributed to a lack of adherence to traditional practices in the homeland as well as a lack of
acculturation to an American way of life. One participant explained:
Since we came to this country [the United States], we have to live a different way of life and in consideration of the American way of life, whether moving by cars, etc. However, over there [in home country], one could walk a long distance. The closeness of life there [in home country], makes you exert an effort. The fats are secreted from the body. Here, it is not so. The Americans controlled this life style. They go to the gym, for example, whether men or women. They know the equation because of lack of activity limited to the office and home. Hence, they go to the gym daily for an hour. We, as Arabs, between parenthesis, we took their disadvantages. Their disadvantage is lack of activity, for example. The advantages and the disadvantages of the Americans. Their disadvantage is lack of activity, for example. We do not go to the gym because we either do not have time or we do not care or each one has a special reason. Our problem, as Arabs in America, we did not live as Americans 100%, nor we kept our Arabic lives; walking, seeing our walking friend, going to the next appointment by walking to a neighbor or to a friend, etc. We neither kept our Arabic life nor did we walk with the Americans.
He went on to add that the economic difficulties that many migrant face today necessitates a longer
working day and perhaps even more stress, and to greater risk of diabetes:
…the reality of the American life is that I have work and have no free time. I do not work 15 hours in my home country. Here, I must work from 12 to 15 hours a day. This cumulative stressful situation causes تراآمات in me sluggishness/laziness خمول. Sluggishness will lead to cholesterol like we just said in this hour.
Prevalence
Participants were asked to estimate the prevalence of diabetes in the community. They felt the
prevalence of the disease was so high that every family was affected: “I think in every home there is one
who is diabetic whether a mother, a father, a child or one of the relatives. I think everyone became aware
of diabetes because they have someone in the family who is diabetic.” Most said that there were many
people they knew with the disease. Participants felt that diabetes was a common ailment in the Arab
world that had recently become more prevalent with changes in diet.

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
19
The general consensus of those in the pilot focus groups was that the rate was above 50 percent among
Arabs with most respondents estimating in the 60 to 70 percent range. Estimates in other groups ran as
high as 50 percent or more: "half of the people. I think more than half of the people." However,
education sessions seemed to help dispel this myth. A member of a post‐education group placed the
rate at “between 18‐28%” for the Arab community.
Risk Perception
The perception of personal risk for developing diabetes was quite high. Almost all participants felt they
were at risk due to their weight, high blood pressure, heredity, lack of a healthy diet, or lack of exercise.
One female respondent noted that many within her own family were diabetic, causing a fear that she or
her children would become diabetic: "My grandmother died from Diabetes. My uncle died from
Diabetes. My second uncle has Diabetes. My mother, now, has Diabetes. My sister has Diabetes. We do
not have fear from Diabetes. But we have four twins." Nearly all felt that they were at some personal risk
of developing the disease. Most felt this personal risk due to heredity and lifestyle. Only one person out
of the pre‐intervention groups felt she was not a risk for the disease. As she explained: "Because the
world is beautiful and good for us. Its sweetness is more than enough for us. All my family has Diabetes, I
do not have."
Community Awareness
Awareness was also seen as an issue. A member of a post‐education group said that only about half of
the Arab community is aware: “I think that 50% of people know about diabetes and 50% of the people
are ignorant.” They noted that ACCESS has played a significant role in raising awareness:
I come frequently to the center here [Arab Community Center for Economic and Social Services]. I pick up flyers that give information and calls for meetings, seminars to battle against diabetes. Mostly it is at this center. Then, there are clinics that you visit. The very first thing they have put there for you is about diabetes and what must be done.
Diabetes Prevention and Treatment
Participants were well‐versed in ways in which to prevent diabetes, yet indicated that willpower, time,
and other factors limited their attempts to diet and exercise. They listed regular walking and exercise,

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
20
healthy diet (including reduction of fried foods, portion control, reduction in sweets and carbohydrates,
and fewer “junk foods”), regular checkups, reduction in stressors, and increasing personal knowledge or
awareness. Many participants noted that while they understood that prevention was possible and
necessary, the issue became laziness, time, and/or lack of will power.
Participants in the pre‐intervention focus groups were well aware of many of the lifestyle changes that
could help to prevent or reduce the chances of becoming diabetic. They correctly identified that
prevention was dependent upon exercise and changes in diet. One participant noted: "One must pay
attention about his life style. One must not eat too much sugar. One must watch about everything,
because this disease is very sensitive. The sugar level rises very fast and to lower the level is very difficult."
They also noted that changes to diet and exercise not only reduced the chances of becoming diabetic,
but increased health in general: "Gym helps a lot to fight Diabetes; using the sauna, the steam room and
swimming pool. I did all these at the gym. I used to go for a number of years, 10 years. When I used to go
there I lost weight and felt better." One participant noted that successful treatment of a diabetic
depended upon both lifestyle changes and medication, but that there was no way to "cure" diabetes:
"He must not eat sweets, carbohydrates. He must watch his food. He must go to the doctor and follow
the doctor's instructions. Diabetes does not have a medication that completely treats it."
Members of all three refusal groups were also quite clear that lifestyle changes could help in prevention
or lowering of risks. They discussed diet and exercise, as well as monitoring for signs of diabetes.
Members of the post‐education group also noted that there is no cure: “What we understood from the
seminar that I heard from the doctor that there is no 100% treatment for diabetes.”
Myths
There was a commonly held belief that being upset, anxious, worried, or under stress could cause
diabetes. One participant felt, "90% is one being upset or sad." Others believed that diabetes could result
from an emotional shock or surprise. They gave anecdotes of this kind of occurrence: "… my brother
when he had a shock, he became diabetic." Another member of Pilot noted that, “if one of my sons has
an accident, this will be like ‘volcano eruption’ and I might develop the disease at once.” A member in the
post‐education group correctly refuted the myth that shock or emotional duress causes diabetes: “Being
D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
21
upset does not cause diabetes. Diabetes is how much you store food, how much you eat. It is not that
when a person is upset, he becomes diabetic. It has no connection with diabetes...” However, some in
other groups still held the belief that diabetes was related to emotional trauma: “Diabetes is the result of
shocks. In addition, being upset has an effect. Any person, who experiences a shock and being upset
regarding a loved one, becomes diabetic. This greatly affects a person.” Other myths linked diabetes to
blood‐pressure or cholesterol medications, eating before bedtime, use of sugar substitutes, and sudden
anger or sadness.
Herbal Remedies
Beyond diet, exercise, and medication, another theme emerged from discussions of diabetes
prevention: the use of naturopathic remedies. There were several herbs mentioned, though the
transcriptions of the names of these herbs may not be accurate (please reference original Arabic
transcripts). By name, azagan (also spelled as ataman), and quat [khat] were mentioned. One female
noted that medical doctors in her home country used these herbal remedies: "My mother's sugar level
reached 600. They could not lower the sugar level in the old fashioned way, and the "azaqan" lowered it.
Now, when my mother goes to the female doctor, if the doctor finds it [sugar level] high she tells her go
and drink from it. This is something popular." This remedy was mentioned by several focus group
members as way of not only treating, but preventing diabetes: "Drink every day a glass of "azaqan" you
prevent it in all your life totally. Quat [khat or تاق] was another folk treatment was mentioned not as a
cure, but as a way to lower the sugar level in the blood: "Quat, you know, Quat lowers the level of sugar
in the blood….It lowers a little bit. It is bitter, bitter herbs. Everything that is bitter lowers Diabetes. It does
not cure, but it lowers Diabetes a little bit."
Stigma
There was also recognition that within the Arab‐ American community there is stigma to illness: "they
used to keep secret about the diseases. There are things that could be in the family [hereditary], however,
but they do not tell anyone, especially someone died from something, fearing that someone would know.
They do not tell." This stigma resulting in a reluctance not only to disclose information but to asking
questions about diseases like diabetes: "…here, in our community there is shame. We have shame in our
community to ask."

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
22
Barriers to Care
The major barrier to health care was lack of health insurance and the high cost of seeing a physician:
“many do not have medical insurance and so cannot see doctors regularly… they pay to see a doctor.”
This lack of insurance causes many to delay care until it is absolutely necessary. A male participant noted
that this problem is especially acute among recent arrivals who are searching for employment: “When
people come from the old country they do not find a job right away or find a job without health
insurance; most companies are now cutting back anyway. All things that relate to health insurance such
as the financial factor, the person does not find job.”
Other barriers discussed included a fear or dislike of doctors or medicine; a lack of awareness;
negligence, laziness, or stubbornness, and transportation issues. Language issues, while acknowledge to
be a concern, were not seen as a true barrier to care. About half of the participants expressed a
preference for co‐ethnic caregivers. It was seen that most routine medical care was the domain of the
wife/mother, yet there was sentiment for shared responsibility between men and women, especially in
making decisions about serious health issues.
Reasons for Participation in Intervention Three Pre‐Intervention sessions were conducted with participants. As stated previously, the goal of
these pre‐intervention focus groups was to identify the reasons for participation in the intervention. Two
principal reasons emerged: (1) to gain more information about the prevention of the disease and (2) to
help the Arab community by spreading accurate information to others. One participant succinctly
underscored the collective nature of the Arab‐American community and that information that an
individual learns will be useful to all:
Honestly, to gain information. The first thing you can give information to a person. Secondly, I will have general information about this disease even though the person did not happen to have this illness. If one is among people, one has knowledge about it or can help someone. You can give simple information that could teach and help someone else. It is not only necessarily you. For that reason….We are all Arabs. We need to encourage each other in order to build our future, our community.

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
23
Fear of the Risk of Diabetes for Self or Family
Fear of the risk of diabetes may have been a motivator many. As noted, most participants in the pre‐
intervention groups felt that their personal risk for eventually becoming diabetic were quite high. About
half of the participants agreed that this fear was a factor for joining in the intervention or educational
sessions: “In fact, my grandmother died from Diabetes and I don't want to take her place. As the saying
says "An ounce of prevention is worth a pound of cure." Another, in a later group, noted: “It was the
danger for me. If one has not improved [in knowledge] or does not have information, he may experience
this disease or other diseases. So, I wanted to increase my knowledge about the dangers of diabetes
disease so as to improve my health.” This concern also extended to the future of their children as well: “I
have children and I am afraid that they may be at risk. I will try as much as possible to teach my children
and protect them from these all.”
Conversion from the Education Program
The Education Program seemed to be an effective method for recruiting individuals who were initially
uncertain about committing to the Intervention. When offered the choice between Lifestyle Program
and Education program, chose to enroll in the Education program as a gateway to understanding the
issues associated with Diabetes. They explained: “When you talked about education, I changed from
Lifestyle to Education. One has to have enough education in order to enroll in Lifestyle.” Similarly others
explained that they were not yet ready to commit to a six‐month program so they signed up for the
Education Program to see if there was a benefit before agreeing to continue: “Thank God, we found that
it was good and now we requested to join the second program because we benefited. It was better not to
start the six months program and stop. Now, we are ready to continue the six months program, if God
willing.”
Other Reasons
One participant noted that the personal appeals and telephone calls from the staff persuaded her to
join: “When you called, you called me more than once for which I thank you. You know, I hesitated
because of the house work and the children. At the end I was convinced by you 100%.” Interestingly, the
offer of incentives played little role in their decision to participate: “They [the gifts] are nice but they are
not the reason that one joins the program.” However, a participant did say that money for gasoline
D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
24
would make a good incentive. “Mutual support” was commonly given as a reason for perseverance in
the program among the converters. Group members said that there were many ways to learn things, but
that working together in a group reinforced their commitment to completing the program. Finally, the
location and timing were simply convenient for some while not for others: “timing was convenient. In
the morning is good.”
Barriers to Participation in Intervention Three focus groups were conducted with those who refused to participate in the Intervention Program.
These groups sought to examine the barriers to participation.
Issues with Time or Scheduling
The major barrier to continued participation in the program was time: “This subject is important. As you
noticed that we care about these subjects and listen. However, we do not have time.” There were a
number of responsibilities that were limiting participation: family and childcare, work, school,
businesses, and one person even mentioned that some people would rather watch television. A
participant tried to explain:
I think it was good for the community; however each one had an excuse. The housewives have children and did not have time. I am at my work. Naturally, during the day I do not have the time. I think there are many people who would like to attend however they do not have time to come and attend. And there are people who may not know about the program or are not receiving information about the program.
Suggestions were made to have several time slots available, preferably with weekend hours or evening
hours: “It is possible if it can be on a Saturday. Some people are off and may be convenient to many
people. Not all people can come during the week because of the work.” Also, as some participants
explained they needed flexibility to attend different time slots each week as their schedules were
variable: “My work does not allow me. My shift does not allow. Sometimes I work from 12 midnight until
10 am. Other days I work from 12 noon until 10 evening. Approximately, every month my schedule is
different.”

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
25
Mixed‐Sex Groups
Mixed‐sex groups were brought up as another possible barrier specifically for the Yemeni and Iraqi
communities. Some participants felt that the presence of men may prohibit participation by women
from these communities. There was considerable discussion on this topic in one of the groups:
FGRefuser.01: Yes for some people but not the majority. There could be some women who would not like to mix with men; however they are not a big number. Some people are used to come to a public place to take lessons. It does not matter to them if there are men or women; however, some women may not come to class if there are men.
FGRefuser.02: This is not a barrier that a woman sits with men.
FGRefuser.01: I am not saying it is a barrier for all people. I will say that for some people it may.
FGRefuser.02: I know some people. For example you are a man and you are far away from me and them. They listen and I listen. I do not think there is a barrier.
FGRefuser.01: Even at Islamic centers, at mosques, people come. Men come with their wives to pray. They come because of special occasions. I do not think it is a problem. The person is not doing something wrong.
FGRefuser.03: It is not that a person is doing something wrong. I think it is the culture of the Arabs. It’s their culture. We Yemenis, men and women do not mix. Always they are separated.
FGRefuser.02: The Iraqis likewise.
FGRefuser.03: The same thing. We don’t mix men and women.
FGRefuser.04: This is a principle.
FGRefuser.02: We, the Lebanese, no. We mix.
FGRefuser.03: If you did separate classes for women, you might get some.
Educational Intervention Feedback A key element of the education conversion focus groups was to gather feedback regarding the education
sessions. Participants said that they had learned a lot about diabetes in these few sessions and that they

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
26
had already begun changing their cooking and exercise practices in the home. For example, one
participant notes how she has begun to walk regularly and change the foods she and her family eat:
At the beginning I did not know how much walking helps. How healthy walking is for your body. Now, for example, I have my children, and their health is very well. I did not know how to regulate their food. I did not know how to prepare the food.
Participants noted that the sessions were well paced and were neither “too long nor too short.” One
participant said, “One hour is enough because more than one hour it may become boring.” They agreed
that the time, day of the week, and location of the sessions were convenient. They were happy with the
amount of content that they received, but did not feel overwhelmed. They especially liked that the
seminars were in the form of a discussion more than instruction. There was also general agreement in
the groups that the educational program was appropriately tailored to the Arab community. One person
pointed out that, “there is nothing that conflicts with the community or anything.”
Participants explained that several myths or misbeliefs they held previously had been dispelled by the
information received during the sessions: “There were many things which were somehow unclear. They
were clarified in this program.” For example one participant recounted the new things she had learned:
Prevention by changing food, for example excess fat is not good. How diabetes disease starts with a person. We have to take precautions. If the level of sugar passes 100 or 120 means that the person started becoming diabetic. All these things we did not know about.
Importantly, those in the education program were better able to indicate that diabetes is related to
insulin levels, that the body converts carbohydrates into sugars, that high blood pressure and high
cholesterol are associated with risk, that there are two types of diabetes (correctly identified by their
causes), and that lifestyle changes were an effective way to reduce risk:
We did not know, for example, that the sugar that is stored in the body, hits the pancreas, the liver. We thought that if someone ate sugar/sweets, he has to reduce it because he may become diabetic. We did not know about carbohydrates, fats that pile in the body and is transformed into diabetes in the future.
D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
27
The myth that at single emotional shock or trauma could cause diabetes was also dispelled: “Most of us
(I am one of them) thought that diabetes disease has a relationship with the psychological condition and
being upset.” While the program dispelled myths it also highlighted risk that participants face. One focus
group member said the educational program was “like a stop sign,” telling them to stop and take note of
bad habits.
Suggestions for Improvement
While feedback was positive, there were a few suggestions for improving the educational program.
Several suggestions were made with the goal of helping to improve the program:
One participant felt that among program participants there was too broad a range of educational
backgrounds making it difficult for instruction. She explained: “if you are going to do a program,
the educational level of the participants in a group [needs] to be comparable; groups that
comprehend ideas fast and groups that want to know exactly what to eat and what they have to
cook in spite of it is very good and very beneficial.”
It was suggested by a younger member of the focus group that alternative ways of
communication be explored. The participant suggested, “electronic communication, electronic
conferences, e‐mail to be once a week” as a way for some to maintain the needed support.
Participants also felt that for the program to be effective it should research a larger and broader
audience: “It could have been better in regards to the number of participants. It could be more
awareness among the people so as to attend these programs. It could be that this number is
sufficient; however, the program is very important.” One participant suggested groups of up to
30 or 40 people. This invoked a discussion on the proper size of the group with some saying it is
better to have smaller more focused groups and others arguing for greater outreach into the
Arab community. They did agree that information was quick to spread in the Arab community:
“… [a] good thing in the Arabic community is that there is a difference from learning a fact and
like to pass it to a brother, sister, neighbor, and a friend. That is especially good for a woman to
have general education. That is a person (i.e woman) to pay attention to.”

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
28
Several felt that the outreach efforts of the current program were too limited: “We are 10 out of
100,000. It is nothing.” There was discussion on the serious need within the community to
engage in broader dissemination: “When I come and sit at the table, I meet about 180 women,
among them 35 or 40 women are diabetic. Sometimes, I help them to learn what to do. Really,
there is ignorance, especially, especially among our women.”
Participants were also eager to learn more about specific food products they should buy. It is
acknowledged that this is covered later in the Lifestyle Intervention, yet participants were not
aware of this.
There was also concern over starting on time, primarily as a concern of some participants that
others were causing the program to start late or that they were not present for every session:
“Even if somebody is late, start without them. That’s very important. We all have lives outside
this.”
Reasons to Continue in the Lifestyle Program
Participants in these three groups agreed to continue learning about diabetes through the Lifestyle
Intervention Program after they completed the education sessions. They explained that what they had
learned in the few classes had given them enough information to encourage them to continue. Others
spoke about the need for enough “basic information” before progressing to the “implementation.”
Family and community also played a role. Several participants talked about the need to learn more in
order to protect their children or to help educate their community: “I am mother and I have my children
so as I educate them from now. This is the reason.” Several were convinced to continue based on the
lifestyle changes they had already begun at home and the desire to learn more:
I noticed that there is benefit, and I started to change my lifestyle in order to reduce this disease among us and coming to our house. I followed a special calorie diet, and regular exercise and food. For this reason, I am going to enroll in the second program of Lifestyle.
The promise of hands‐on learning was also an enticement: “What also encouraged me is that the doctor
[Dr. Jaber] said that we will go to stores and we will learn about which food is healthy and which is not.

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
29
Also, the exercise classes encouraged me.” A few, however, expressed possible limitations to their
further participation. In particular scheduling was a concern. Busy work lives as well as summer travel
plans posed limitations to their ability to attend all sessions of the intervention.
Lifestyle Intervention Feedback Feedback on the Lifestyle Intervention program was obtained both through a series of four focus groups
with completers (N=42) and through a post‐focus group feedback survey.
Feedback Survey
Following the final focus group with intervention completers, a post‐session survey was completed by
the participants. The survey sought feedback from them on the impact and outcomes of the program.
Complete survey results are presented in Table 4 below.
All 42 participants, felt that their knowledge of diabetes had increased as a result of the program (100%
strongly agreed). All had changed the way they eat (100% agreed or strongly agreed). Most had also
Table 4 ‐ Feedback Survey Summary Table
Strongly Disagree
Disagree Neither Disagree nor Agree
Agree Strongly Agree
This program increased my knowledge about diabetes 0.0% 0.0% 0.0% 0.0% 100.0%
As a result of this program, I changed the way I eat 0.0% 0.0% 0.0% 14.3% 85.7%
As a result of this program, I changed the way I exercise 0.0% 0.0% 2.5% 32.5% 65.0%
As a result of this program, I believe my risk of diabetes has been reduced
0.0% 0.0% 2.4% 17.1% 80.5%
As a result of this program, I feel healthier 0.0% 0.0% 2.4% 19.0% 78.6%
I achieved my goals as a result of this program 0.0% 0.0% 0.0% 24.4% 75.6%
Because of my participation in the program, members of my family have changed their lifestyle
2.4% 0.0% 4.9% 46.3% 46.3%
Because of my participation in the program, members of my community have changed their lifestyle
0.0% 5.0% 15.0% 42.5% 37.5%
The instructors in this program were informative 0.0% 0.0% 2.4% 2.4% 95.1%
The peer mentors in this program provided good support in achieving my goals
0.0% 0.0% 0.0% 0.0% 100.0%
The materials in this program were culturally appropriate 0.0% 0.0% 2.4% 7.1% 90.5%
The lessons in this program taught me things I did not know 0.0% 0.0% 2.4% 12.2% 85.4%
I would recommend this program to others in my community 0.0% 0.0% 0.0% 4.9% 95.1%

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
30
changed the way in which they exercise (97.5% agreed or strongly agreed). Nearly all felt as if their risk of
diabetes had diminished as a result of the intervention (97.6% agreed or strongly agreed). Likewise
97.6% agreed or strongly agreed that they were currently feeling healthier as a result of the program. All
reported that they had achieved their personal goals for the program (100% agreed or strongly agreed).
The impact of the program extended well beyond the immediate participants. Most (92.7%) agreed or
strongly agreed that members of their family had changed their lifestyle as a result of the Lifestyle
Intervention. Similarly, many (80%) reported that because of their own participation, members of the
community had changed their lifestyles as well.
Feedback regarding the instructors and materials was also overwhelmingly positive. Instructors were
seen as informative (97.6% agreed or strongly agreed), and peer mentors as providing good support
(100% strongly agreed). The materials were perceived to be cultural appropriate (97.6% agreed or
strongly agreed). The lessons were seen to present material that was new to the participants ((97.6%
agreed or strongly agreed). All would recommend the program to others in the community (100%
agreed or strongly agreed).
Focus Group Feedback
As found in the surveys, participants were overwhelmingly positive about the program yet survey results
alone are insufficient in providing formative evaluation feedback for the purposes of refining this
program for future application. Thus, focus groups were held to elicit more detailed input from the
participants. In general, they felt the pacing and content was appropriate. They liked many of the
practical aspects of the program such as exercise sessions, calorie counting, and shopping trips. They felt
well supported and encouraged in their efforts.
Encouragement
The respondents in all groups said they liked the mutual support and camaraderie: “Working as a
collective was more beneficial than one‐on‐one.” Another person concurred: “Working together as a
group was encouraging to each other.” A participant in another group echoed a similar sentiment, “This
way is better because the group encourage each other more. The group setting is better. I prefer like
this.” They also agreed that there was a lot of encouragement by program staff and other participants:
D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
31
“The presence of the group. The instructors were good. The subject was scientific, and we encouraged
each other.” Moreover, the program made them feel comfortable by not being commercial and instilling
a feeling of trust:
I have participated in 20 programs and in different countries; in Iran, Iraq, and in Dubai. I have seen the programs of different cultures, exercise issues; a part was related to specialties because teaching was my profession. This program was very useful to me. I felt comfortable. I did not feel any pressure. It was really nice and was not commercial. You do not feel that the program is commercial. It is scientific. You feel assured. It is not the money. It is about the education, giving accurate knowledge. Almost you are in the safe side. There is the feeling of safety or trust.
Learning How to Count Calories and Shop
Participants also liked the practical aspects of the program. In particular they discussed the “calorie
count” and “how to select food” activities. The participants liked these tools as they provided the ability
to do things for themselves. One likened the experience to being provided the materials to fish rather
than being given fish: “…in the former programs that I participated in, they offered us the fish ready
made, everything 1, 2, 3, 4, 5, whereas in these meetings, we obtained the hook and learned how to
fish.” For example, in one group most agreed that the calorie book and the activity of recording their
daily intake was useful:
Writing the calories helped me a lot. I counted the number of calories I ate for breakfast. I counted the number of calories I ate for dinner. I count my daily calorie intake of about 1500 calorie. This believe me is too much food. It is more than enough. If I ate 2000 calories, I regret it the second day. I try to eat 500 calories less during the following day. It helped me a lot.
The shopping trip also came up often and in several of the groups as a favorite activity. One participant
explained that this was the most useful part of the intervention: “Mostly it is the manner of shopping.
The points that we learned were how to shop and prepare foods. One reads and watches what is very
useful.” Another echoed a similar sentiment about the shopping trip:

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
32
I liked the most when we went to Kroger. I used to only pay attention to the fat or the cholesterol content being low, because I have high blood cholesterol. I did not watch for the transfat, the salt, the calories and these things. Now, I watch for everything; every element in the kind of food that I get.
Accomplishing Personal Goals
Participants estimated that they attained 60% to 90% of their goals in weight reduction, cutting calorie
intake, and maintaining their exercise regimens. They felt supported by mutual reinforcement, but
admitted that some elements of the program were difficult at first: “At the beginning I found it a little bit
difficult. Every time that you eat something you have to write it. You keep on writing back and forth.
Later, I got used to it. I learned it and I wrote them.”
Most participants reported shedding weight. One noted, “I lost 10 pounds, which is good, and I felt
good.” Another noted, “My size was 24, now it became 18.” Many had received compliments from
family and friends that reinforced their desire to stick to the calorie counting regimen. This weight loss
was the most important feature of the program to some: “Regarding the topic, the most important thing
that was helpful to us was losing weight. We felt comfortable. We felt ourselves more active. We
regulated our food in an incredible way.” For some, the weight loss and modifications to the diet began
during the Educational Program and continued during the Lifestyle Intervention with dramatic results:
I attended the program and initially I lost about 15 pounds. My weight before was about 164 pounds. My weight went down to 152 or 150 pounds. Then I followed the Lifestyle Program and my weight lowered to 136 pounds; from 152 pounds to 136 pounds and even less 135.5 pounds. The program is very good. First, the program strengthened my determination. Whenever I desired to eat something, I would remember that my weight would increase, so I would just taste it or eat just a little bit. Then, everyday I do half an hour exercise. This also helps me and strengthens my determination also. I do not let myself go as it wishes.
Temptations such as sweets were difficult for some to avoid at first and might prove to be a problem still
in the future. One participant explained, “I am afraid from one thing that after the program I will not be
able to control over myself regarding eating sweets. I am afraid from this only.” Also, some participants
felt that exercising for an hour would be difficult for them: “It is the time element. Sometimes I do not

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
33
have the time to do the exercise. I could exercise for half an hour or for smaller intervals. An hour exercise
is difficult.”
Additional Health Benefits
In addition to the loss of weight, many reported feeling stronger and more energetic. Moreover, in each
of the focus groups with completers there was discussion over the reduction in blood pressure and
cholesterol. One participant, since beginning the program, had stopped needing as much of her blood
pressure medications: “My blood pressure went down; instead of taking the complete medication dose
that I used to take, I am taking half of the dose.” Several described dramatic reductions in cholesterol:
My cholesterol was 264. Fat was high. The doctor told me that I had to watch for fatty foods and also my sugar. Either you have to watch or I will prescribe you medication. I followed the methodology of this program. A month ago or less, I did tests. Everything is normal. Truly, thank God, cholesterol, sugar, everything is normal. This is not an advertisement. I am telling you what happened with me.
Impact on Family and Beyond
Nearly all reported the ancillary impact of changes in lifestyle among family members and friends. As
they changed their eating habits at home, their families also became a part of the intervention. “This
program is very useful. It helped us. It helped our children. It helped our friends because we sat together
and talked about the program and encouraged them to join this program.” This was particularly evident
with female participants who were more often the cooks in the home: “Whatever we cook at home, the
family eats.”
Beyond the family, neighbors and friends were impacted as they noticed the loss of weight or changes in
eating habits: “I tell my friends about the program that I have joined and what we do. So, they started
watching their food. If they had to use fat in the food, they use instead a little bit oil. Also, they
benefited.” Likewise, family and friends were recruited to become exercise partners: “My sister in law,
she came with me to the park to Maysoon’s class. Now, she calls me asking: “Don’t you have any more
exercise classes? When are we going? Let us go.” She comes to me and asks me to walk together. The
exercise raised her enthusiasm in many things.

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
34
While there were several discussions in the focus groups regarding the need for additional health
marketing in the community, it was recognized that the participation of a few in the initial program had a
great impact on the entire community:
We do not need religious centers. We do not need advertisement. We became the advertisement. We are the ones that we give. First of all we started with our children, our husbands, our families. Now, my sisters say, this method I followed and I benefited. Let me try with my husband and children. My brother is the same thing. My neighbors followed, too. Slowly, it is being found.... it spreads more and more.
Suggestions for Improvements
More Dynamic Content
There were several suggestions for improving the program. First, there were a number of comments
that alluded to the program lacking dynamism. As one participant put it: “It lacked a little bit of the
excitement elements.” Another participant felt that some sessions were too much like going to school:
“writing on the board kills me when I come to attend sessions.” Others talked about the classes being too
long: “The program could be shorter so that one does not get bored.” A suggestion was made to spread
out the dense or complicated topics over the course of several sessions with activities interspersed to
make it more fun. Since much of the content of the program was “front loaded” rather than spread out
throughout, it was felt that some participants may have dropped out early. A focus group member
explains, “if the information material is heavy, everybody is gonna come, but toward the end less and less
people came; somebody would come, somebody wouldn’t come. I think sessions should be spread over
the six months rather than do everything in the beginning.”
Several people commented on the handouts saying there was “too much paper work” and that the
handouts were “tiresome.” Another participant suggested making the course livelier by reducing the
number of handouts, making the handouts that were passed around more engaging, and using videos.
She explains: “a video makes teaching interesting for the person and not only learning from reading and
writing and doing this or that…. it could be exciting by having a video.” The idea of using videos came up
in other groups as well: “For example, you are telling that you are going to prepare food. There should be
D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
35
in the video someone preparing the food in front of us. The way they show on T.” Similarly, another
participant recommended using slides to make the content more dynamic and visual:
For example, you are writing on the board. There are other things than writing on the board; the way of the presentation. Instead of writing it on the board, there are slides. Slides could be videos. You could know from the slides. A woman did a presentation for Rotary Club about Lebanon. She got the slides and the video about Lebanon. They were very impressed how she combined the slides with the video. Until now, people talk about the presentation. There are still things that make a person not to forget, other than the old way of writing only. Writing impacts but not a lot
Additional Health Experts
Another discussion on improvement centered on brining in additional experts. They liked having experts
visit to discuss health, nutrition and exercise: “the fact that you had a nutritionist, a health doctor, and a
variety of knowledgeable people here, they gave us a lot of information. We asked them and they were
very helpful.” Yet, it was noted that while the psychology of weight loss and lifestyle changes were talked
about, there was not a mental health expert present to address these issue as there was for other topics:
“You have the nutritionist. You have the health department doctor. We’re missing the psychiatrist.”
Cooking Classes
There was also significant discussion on the limited amount of time spent practicing and applying
lessons: “This program is not sufficient to be theoretical, it needs to be practical along with the
theoretical part….” Participants wanted more time to actually engage in application of the material. As
one said, “Even if there would be a small kitchen to cook a small dish.” This theme emerged in a later
group as well: “If one could do like a cooking class instead of using the video. I am not sure whether you
could do this here at the center. There isn’t a kitchen here. It helps if you can get someone to cook the
thing in front of you.”
More Time for Exercise
Similarly, many participants felt there were not enough exercise sessions to actually practice and refine
what they had learned: “Increase the exercise sessions. The time was not sufficient enough. They should
be more sessions.” This participant went on to say that there should be at least two exercise sessions per
D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
36
week. Another participant reasoned that at least half the program should be application of the exercise
lessons:
“If we consider that exercise has a role for about 50% [of reducing diabetes risk] in this aspect, we have to give educational sessions equal to the practical sessions. We are listening to 50 hours to theoretical subjects and learn them; however, practically I am not doing anything.”
Moreover, there was misunderstanding and confusion in one group over the provisions that were made
for exercising. Many thought they could only go to Bally Total Fitness. This was not acceptable for some
women who were unaware that Curves was also available to them:
I like that she got membership to all of us to go to the Bally fitness but as you know, a lot of sisters here are covered. They cannot go there. It’s mixed. I cannot go there. I personally don’t like to be in mixed area. I am not covered, but I do not feel comfortable. I wish you, because you know, most of the members they like that kind of environment. I wish you got membership or the deal, I don’t know if report or not, but I wish you got the membership with the gym that has this kind of privacy.
Calorie Count for Arab Foods
Most participants mentioned how much they liked the calorie counting book and materials. However,
there were also a few who suggested that it would be more useful if it better fit their ethnic cuisine and
the foodstuffs they commonly find in the grocery stores catering to the Arab community: “I would
suggest if you come up with the calorie content of things sold in the Arabic shops or sweet shops that we
buy from. For example, the sweet shops, if there would be a program to label how much calories or fat
each kind of stuff contains.”
More Training on How to Teach Others
Several participants felt that their role and purpose for being there was to eventually disseminate what
they had learned to the broader community. In particular they worked within their own families: “We
shared the things that we learned and implemented them together as a family.” While they clearly felt
they were making some impact (especially with the cooking in their own homes), they still felt limited.

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
37
There was a feeling that the training was not sufficient for them to be able to go into the community and
train others:
We are going to be the pioneers in the community. Isn’t it right? Our aim is to learn and teach others as leaders. So, if the leaders/forerunners did not learn well, they will not be able to teach, otherwise, what the prophet can do in the جارعملاو ءارثإلا يف [Reference to the prophet way of teaching].
Alternatively, it was suggested that the Lifestyle Intervention program attempt to reach a broader
audience by using local the local imams, cultural and social institutions in the community, and the Arabic
language media:
I was surprised is that the community does not have sufficient information about what you are doing. It is important what you are doing, however, it is necessary there to be an advertising method to reach the community. I do not know how the advertisement method to be. For example, you could be on TV, or on satellite TV; LBC just to target the community. To speak what you are doing because it is an important thing what you are doing. The community is not aware of it. I was surprised to find out that there are a lot of information about food which I did not know, manner of exercising, and how to shop one’s food, the quality of food. This changed our home. It is important that it changed however, it is important that other people know about it. The advertisement should be more powerful than this.
Better Cultural Fit of the Intervention
Even though the materials were perceived to be culturally appropriate (97.6% agreed or strongly
agreed in the survey), a series of critiques in one early focus group (August 2008) revolved around
the question of a cultural match between the implementation and the Arab‐American community.
As one person put it, the intervention was “sensitive, but is it enough?” She went on to say, “It
lacked the cultural face of the Arab. It was purely scientific material. It was not crafted with Arabic
culture, even the terminologies… Even the suggested names, the examples were void of culture.
Relationship to the culture is weak. In particular, there was a feeling that the handouts and
examples should reflect the history, the diversity, and the religiosity of the Arab community. One
participant suggested:

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
38
Bring wise old Arabic sayings from the Chaldean culture in the Iraqi history to the Greek Arabic culture that was in Lebanon and all cultures. You can find subjects or stories about nutrition and medicine dealing with nutrition. All these, if we include, it will feel that this is a book automatically; a special book that includes ethnic matters.
Another participant commented on difficulty with the vocabulary on the handouts. She explained
that though she had been an English teacher, there were many words that she did not know used
in the handouts”
I wish opposite to the words to be written the meaning in Arabic. Khas [lettuce] is khas and not to say lettuce. Bamia [okra] is bamia. Our purpose is education. Science is good in the language of a person who understands it before implementing it….I wish that there were Arabic words next to the English words. It would have been simpler and easier for the student to understand. The purpose is the practical implementation.
Later focus groups (April 2009) did not feel the same about the cultural “fit” of the materials. In fact they
commented that the materials accurately reflected the cultural identity of the community: “…we, in
general, are a Middle Eastern society or even a religious society. You took into account this. You asked,
for example, Islamic quotes or “Alhadith” to include in that. It was good very much.” Yet the same
participant did note that the references to Arabic food were limited and perhaps more reflective of the
Lebanese community:
It was not sufficient, because, in general, the majority of the community here is Lebanese. However, it would have been good if there were examples from the Iraqi community or the Yemeni community. It was not sufficient. There should be more variety of the cuisine, because our Arabic community is large. There is a variety of cuisine.
These later groups did discuss the appropriateness of the mixed‐sex exercise sessions. Many felt it was
inappropriate for a female physical trainer to be teaching males and for males and females to exercise
together:
FGCompleters2.08: The only thing that was not appropriate was the exercise for men with Maysoon. It was inappropriate. Honestly, it was not appropriate. There is no hypocrisy.

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
39
Moderator: Can you repeat it?
FGCompleters2.08: It is necessary that you bring men to train and exercise men. A women standing in front of men and doing this or that movement was not appropriate.
The discussion of this issue extended to the topic of access to the exercise clubs. There was a clear
preference that women should not go mixed‐sex clubs, “Men train with men and women train with
women, because a woman whether covered or uncovered, it is not our custom. She will not be
comfortable in front of men.”

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
40
Conclusions and Recommendations Including the pilot focus groups, a total of 17 sessions were transcribed and analyzed for this report.
Additionally, 29 post‐focus pilot surveys, 42 pre‐focus group feedback surveys, and 121 post‐focus group
surveys were collected to help triangulate or “to confirm, cross‐validate, or corroborate findings”
(Creswell et al., 2003). As stated previously, there were three major objectives to these focus groups: 1)
to understand what factors influence participation in the lifestyle intervention; 2) to identify what
elements of the educational training which led to participation in the lifestyle intervention; and 3) to
identify barrier for those declined to participate in the intervention. Additionally, focus groups were used
to evaluate the outcomes of the lifestyle intervention.
Key factors which influenced participation
There are several key factors which influenced participation in both the educational sessions as well as
the intervention program. These factors are in part cultural and may be understood primarily as having
to do with preservation of self or as social obligations to family and community. Motivating factors
included:
Fears of becoming diabetic (self‐preservation)
Fears of family members becoming diabetic (self‐preservation/ social obligation)
Family history of diabetes (self‐preservation)
Desire to help the Arab‐American community or raise awareness among Arab‐Americans (social obligation)
Personal appeals from/ ties to project staff (social obligation)
Those who participated in the education program prior to the lifestyle intervention (education
conversion groups), also noted that their own personal awareness had to be heightened for them to see
the necessity of the lifestyle changes before they would commit to the program.
In developing health marketing for future programs it is recommended that organizers recognize the
key factors which influenced participation in this implementation. Future marketing should be
designed to make use of social obligations and emphasize the importance of lifestyle changes as a
means of improving health outcomes. However, there is a delicate balance in appealing to self‐
preservation and using fear as an appeal (see for example Witte and Allen 2000).

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
41
Barriers to participation
Barriers to participation may also be reduced to a few fundamental reasons: logistics, personal
characteristics, cultural impediments, and misperceptions or misunderstandings about healthcare.
According to participants, their obstacles to involvement may include:
Lack of time (logistics)
Transportation issues (logistics)
Lack of “will power” (personal characteristic)
“Laziness” (personal characteristic)
Myths about the causes of diabetes that are not influenced by lifestyle change, ie. ‘being startled’
(misperceptions)
Fear or mistrust of healthcare professionals (misperceptions)
Stigma of diabetes in community (misperceptions)
Mixed‐sex groups (cultural impediment)
Among intervention refusers, mixed‐sex groups was brought up as a barrier specifically for the Yemeni
and Iraqi communities, but was not necessarily an issue for those who did participate. Pilot group data as
well as exit surveys showed that about a quarter of participants (see Table 3) preferred single‐sex groups
particularly for exercise. It is recommended that 1) future program offer more timeslots on more days
(mornings and evenings, weekdays and weekends); 2) provide session in multiple venues or even in
some neighborhood homes; and 3) emphasize that exercise classes will be segregated by sex.
Overall Program Feedback
Participants were asked to provide suggestions for improving the programs. Those who attended the
educational session made a two recommendation that could be feasible in future implementations.
First, the program should explore alternative ways of communication (email groups, chats, or other
technologies) especially for younger participants. This could be used as a means of mutual support and
reinforcement between sessions. Also, the education information sessions should be redesigned for a
larger and broader audience in order to have a greater impact on the community and work as a more
effective recruitment tool for lifestyle implementation.

D I A B E T E S P R E V E N T I O N I N A R A B A M E R I C A N S
42
Lifestyle completers also had a number of recommendations. The “hands‐on” elements of the program
were especially appealing and they would like for there to be more of these. In particular, the
participants wanted to spend more time cooking and engaging in exercise. At times they felt there was
too much “paper work” and wished for a variety of instructional material. They mentioned wanting
more multi‐media as well as additional visits from experts. Finally, while 97.6% agreed that the materials
were a cultural fit for the program, there were some elements that could use revision. First, participants
suggested that the calorie count information be provided with more Arab foods listed. Second, these
foods should include those for a pan‐Arab community (comments were made that the food references
were more reflective of Lebanese community).
Feedback from both the intervention and the educational components were positive. Intervention
participants indicated on the exit survey that they had increased their knowledge about diabetes (100%
agree), and changed the way they eat (100% agree) and exercise (97.5% agree). Overall they felt
healthier (97.6% agree) and believe their risk of diabetes has been reduced (97.6% agree). Participants
estimated that they attained 60% to 90% of their goals in weight reduction, cutting calorie intake, and
maintaining their exercise regimens. While many were aware of the necessity of lifestyle changes prior
to the intervention, they needed the structure and mutual support offered by the group to be able to
engage in making changes.
43
References Ajrouch, K. J. (2005). Arab‐american immigrant elders’ views about social support. Ageing &
Society, 25(5): 655‐673. Anderson, L. A., Satterfield D., German R., & Anderson, R. M . (1996). Using quantitative and
qualitative methods to pretest the publication Take Charge of Your Diabetes: A Guide for Care. The Diabetes Educator. 22(6):598‐604.
Anderson, R. M., Goddard C.E., Garcia R., Guzman J. R., & Vazquez F. (1998). Using focus groups to identify diabetes care and education issues for Latinos with diabetes. Diabetes Education. 24(5):618‐25.
Anderson, R. M. (2001) Qualitative research in diabetes: The role of stories in the culture of silence. The Diabetes Educator. 27(6):718‐808.
Arab American Institute (2009a). Arab Americans ‐ Demographics. Retrieved from http://www.aaiusa.org/arab‐americans/22/demographics
Arab American Institute (2009b). Arab American Population Highlights. Retrieved from http://aai.3cdn.net/9298c231f3a79e30c6_g7m6bx9hs.pdf
Bristol, T. (1999). Enhancing focus group productivity: new research and insights. Advances in Consumer Research. 26(1): 479‐482.
Conner, R. F. (2004). Developing and implementing culturally competent evaluation: A discussion of multicultural validity in two HIV prevention programs for Latinos. New Directions for Evaluation, 2004(102), 51‐65.
Creswell J. W., Plano Clark V. L., Guttman M., Hanson W. (2003). Advanced mixed methods research designs. In: Tashakkori A, Teddlie C, eds. Handbook on Mixed Methods in the Behavioral and Social Sciences. Thousand Oaks, Calif: Sage Publications:209–240.
de la Cruz, G. Patricia and Angela Brittingham. (2003). The Arab Population: 2000 Census 2000 Brief. United States Census Bureau. Retrieved from http://www.census.gov/prod/2003pubs/c2kbr‐23.pdf
Garfield S. A. , Malozowski S. , Chin M. H., Narayan K. M. V., Glasgow R. E., Green L. W., Hiss R. G., Krumholz H. M., (2003). The diabetes mellitus interagency coordinating committee (dmicc) translation conference working group. Considerations for diabetes translational research in real‐world settings. Diabetes Care. 26:2670‐2674.
Goldman, A. E., & Mcdonald, S. S. (1987). The Group Depth Interview: Principles and Practice. Englewood Cliffs, NJ: Prentice Hall.
Hollander, J. A. (2004). The Social Contexts of Focus Group. Journal of Contemporary Ethnography,.33(5), 602‐637.
Hosey, G. (1993). Talking circles: a community assessment method. Diabetes Educator. 19(4):351. Jaber, L. A., Brown M. B., Hammad A., Nowak S. N., Zhu Q., Ghafoor A., Herman W. H. (2003).
Epidemiology of diabetes among Arab Americans. Diabetes Care. 26:308‐313. Jaber L. A., Brown M. B., Hammad A., Q., Herman W. H. (2003). Lack of acculturation is a risk factor
for diabetes in Arab immigrants in the US. Diabetes Care. 26:2010‐4. Kayyali, Randa. 2006. The Arab Americans. Westport, Connecticut: Greenwood Press.

44
Knowler, W. C., Barrett‐Connor, E,. Fowler, S. E., Hamman, R.F., Lachin, J. M., Walker, E. A., & Nathan, D. M. (2002). Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. New England Journal of Medicine. 346:393‐403.
Kulwicki, A. D., Miller, J., Schim, S.M. (2000). "Collaborative Partnership for Culture Care: Enhancing Health Services for the Arab Community Journal of Transcultural Nursing," 11(1): 31‐39.
Morgan, D. L. (1988). Focus groups as qualitative research. Newbury Park, CA: Sage. Morgan, D. L. (1996). Focus Groups. Annual Review of Sociology. 22: 129‐152. Nassar‐McMillan, S. & Hakim‐Larson, J. (2003). Counseling Considerations among Arab Americans.
Journal of Counseling and Development. 81(2): 150‐159. Orlandi, M. A. ed. (1992). Cultural Competence for Evaluators: A Guide for Alcohol and Other Drug
Abuse Prevention Practitioners Working with Ethnic/Racial Communities. OSAP Cultural Competence Series. National Clearinghouse for Alcohol and Drug Information, Rockville, MD.
Peek, L. & A. Fothergill (2009). Using focus groups: lessons from studying daycare centers, 9/11, and Hurricane Katrina. Qualitative Research. 9(1): 31‐59.
Pew Hispanic Center. (2006). From 200 Million to 300 Million: The Numbers behind Population Growth. Fact Sheet. Washington, DC, Pew Hispanic Center. Retrieved from http://pewhispanic.org/files/factsheets/25.pdf
Pumariega, A. J. (1996). Culturally competent outcome evaluation in systems of care for children's mental health. Journal of Child & Family Studies, 5(4): 389‐397.
Quatromoni, P.A., Milbauer, M., Posner, B.M., Carballeira, N.P., Brunt M., & Chipkin, S.R. (1994). Use of focus groups to explore nutrition practices and health beliefs of urban Caribbean Latinos with diabetes. Diabetes Care. 17(8):869‐73.
Rice, V. H., Weglicki, L. S., Templin, T., Hammad, A., & Jamil, H. (2006) Predictors of Arab American Adolescent Tobacco Use. Merrill‐Palmer Quarterly 52(2): 327‐342.
Salend, S. J., & Taylor, L. S. (2002). Cultural Perspectives: Missing Pieces in the Functional Assessment Process. Intervention in School & Clinic, 38(2), 104.
Shah S. M., Ayash C., Pharaon N. A., Gany F. M. (2008). "Arab American immigrants in New York: health care and cancer knowledge, attitudes, and beliefs." Journal of Immigrant and Minor Health. 10(5):429‐36.
Smithson, J. (2000). Using and Analyzing Focus Groups: Limitations and Possibilities. International Journal of Social Research Methodology. 3(2): 103–19.
U.S. Census Bureau. (2008). Table B04003 Total Ancestry Categories Tallied For People with One or More Ancestry Categories Reported. 2008 American Community Survey.
U.S. Census Bureau (2009). U.S. POPClock Projection. Retrieved from http://www.census.gov/population/www/popclockus.html.
Vincent, D.; Clark L. ; Marquez‐Zimmer L.; & Sanchez J. (2006). Using focus groups to develop a culturally competent diabetes self‐management program for Mexican Americans. The Diabetes Educator. 32(1): 89‐97.
Witte, K. and Allen, M. (2000). A Meta‐Analysis of Fear Appeals: Implications for Effective Public Health Campaigns. Health Education & Behavior, 27(5) 591‐615.
Willgerodt, M. A. (2003). Using Focus Groups to Develop Culturally Relevant Instruments. Western Journal of Nursing Research. 25(7): 798‐814.

45
Appendix A Project Deliverables

46
Project timeline and products
1. June 2007 ‐ focus group protocol
2. October 2007 ‐ focus group facilitator training in Detroit
3. November 2007 ‐ pilot focus group scripts
4. November 2007 ‐ focus group survey
5. February 2008 ‐ focus group 1 & 2 scripts
6. February 2008 ‐ pilot focus group report
7. May 2008 ‐ focus group 3 script
8. August 2008 ‐ focus group 5 script
9. November 2008 ‐ presentation at 5th National Conference on Health Issues in the Arab American community
10. April 2009 ‐ presentation at the Southern Sociological Society Annual Meeting
11. February 2009 ‐ focus group 6 script
12. February 2009 ‐ preliminary focus group report
13. September 2009 – Post‐Ramadan focus group script
14. December 2009 ‐ paper submitted to Qualitative Health Research:
Sills, S., Pinelli, N. & Jaber, L. “Sex and self‐disclosure: methodological issues of mixed sex focus groups in Arab Americans”
15. December 2009 ‐ final focus group report
16. January/February 2010 ‐ paper preparation for Diabetes Care:
Sills, S., & Jaber, L. “Knowledge and perception of diabetes risk among Arab Americans”

47
Appendix B Transcript Concordance
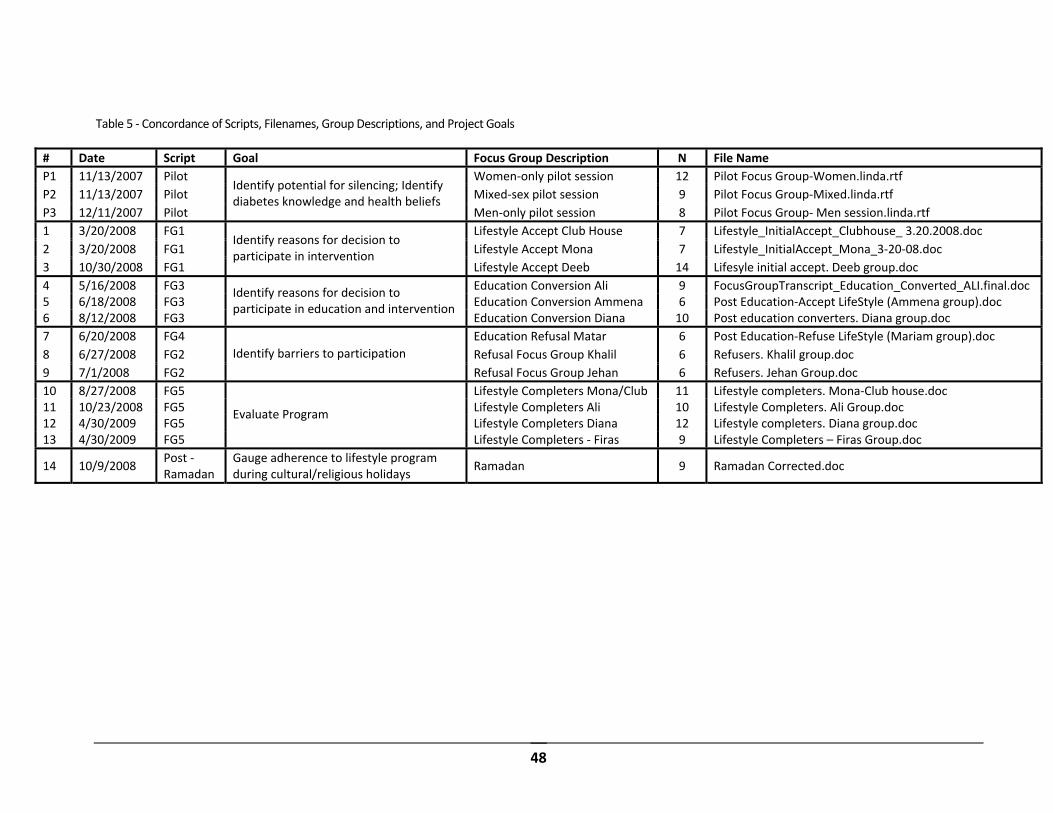
48
Table 5 ‐ Concordance of Scripts, Filenames, Group Descriptions, and Project Goals
# Date Script Goal Focus Group Description N File Name
P1 11/13/2007 Pilot Women‐only pilot session 12 Pilot Focus Group‐Women.linda.rtf
P2 11/13/2007 Pilot Mixed‐sex pilot session 9 Pilot Focus Group‐Mixed.linda.rtf
P3 12/11/2007 Pilot
Identify potential for silencing; Identify diabetes knowledge and health beliefs
Men‐only pilot session 8 Pilot Focus Group‐ Men session.linda.rtf
1 3/20/2008 FG1 Lifestyle Accept Club House 7 Lifestyle_InitialAccept_Clubhouse_ 3.20.2008.doc
2 3/20/2008 FG1 Lifestyle Accept Mona 7 Lifestyle_InitialAccept_Mona_3‐20‐08.doc
3 10/30/2008 FG1
Identify reasons for decision to participate in intervention
Lifestyle Accept Deeb 14 Lifesyle initial accept. Deeb group.doc
4 5/16/2008 FG3 Education Conversion Ali 9 FocusGroupTranscript_Education_Converted_ALI.final.doc 5 6/18/2008 FG3 Education Conversion Ammena 6 Post Education‐Accept LifeStyle (Ammena group).doc 6 8/12/2008 FG3
Identify reasons for decision to participate in education and intervention
Education Conversion Diana 10 Post education converters. Diana group.doc
7 6/20/2008 FG4 Education Refusal Matar 6 Post Education‐Refuse LifeStyle (Mariam group).doc
8 6/27/2008 FG2 Refusal Focus Group Khalil 6 Refusers. Khalil group.doc
9 7/1/2008 FG2
Identify barriers to participation
Refusal Focus Group Jehan 6 Refusers. Jehan Group.doc
10 8/27/2008 FG5 Lifestyle Completers Mona/Club 11 Lifestyle completers. Mona‐Club house.doc 11 10/23/2008 FG5 Lifestyle Completers Ali 10 Lifestyle Completers. Ali Group.doc 12 4/30/2009 FG5 Lifestyle Completers Diana 12 Lifestyle completers. Diana group.doc 13 4/30/2009 FG5
Evaluate Program
Lifestyle Completers ‐ Firas 9 Lifestyle Completers – Firas Group.doc
14 10/9/2008 Post ‐Ramadan
Gauge adherence to lifestyle program during cultural/religious holidays
Ramadan 9 Ramadan Corrected.doc

49