first re3ional working gpoup on...
TRANSCRIPT


FIRST RE3IONAL WORKING GPOUP ON r.::PROSY
sponsored
by
'!tIE WORU> HEALTH ORGANIZATION ItEGIONAL OFFICr: !o'OR TUE Wr:'S'l'I-:HN PAC H'IC
•
Manila, Philippines 1-12 December 19(8
F'HIAL REPOHT
Not for sale
Printed and dist.ributed
by the
Regional Office for the Western Pacific of the World Heal til Orr;1!.nlza tion
Manila, Phili ppines February 1979
~;L,c i'cTP..OL· 1dRi-U't·~ 1 ~;: ~ .. " ;; 1'-~'np;1

NO'm
The views expre •• ed in this report are those of the lIe",bars of t.\'le Work1n, Group and tile Gonsul tan til and do not necessarily reflect the policy of the World Health Organization.
Thia report wa. prepared by the Wcrld Health Organization Regional Office for the Western Pacific for Governllente of Member States and for members of the working Group on Lepro.y, held in Manila, Philippines, from 7 to 12 December 1~,8.
CONTENTS
1 • INTROD'Jr.TION ..•.......•.•••••••••••••.•••• , •••. , •••••••••••••.
2. R!V1EW OF THE REO tONAL LEPRO~Y CO~TPOI. PROr,~A!4!1'.:
3. REr.QMHENDATIONS OF THE RECENT nITERNA'l'T.ONAL LEPROSY WORKSHOPS !~ ASIA SPO~SORF.D RY THE
• ••••••••• t •• ,
SASAICAWA MI!MORUL HEALTH FOIINDA'l'mN ......... .. • • .. • .. • .. • .. .. • 4
4. ANAr.YSV~ OF ONGO!NG LEPROSY r.O~I'!'ROI. AC'!'tV'I;TtF.S IN THE r.OUNTRl ER •••••••••.••••••••••••••••••••••••••••• , ••••••
5. ~'JOOI.CJTtONS ANI) PJIOPOSALR TO IMPROVE THE 1I:"Ir.tIl!Nry or LIPJIOSY ~ONTROL ACTIVITIES AcrOWDlNO TO MATtf PRORlJJot AR!AS TN '.Aml mllNT"Y • • • • • • • • • • • • • • • • • • • • • • • • • • • • , 0
6. INTRODUCTION TO PLANNINO PROCESS •••••••••••••••••••••••••••••• "
'I.
8.
PftOORAtI4! PLANtmm AND IVALI'ATION JPnR I.I!!PROISY CON'!'ROt.
TlHTA'.I'TYI MODIL rOR A MRD111M.TIRM PROORAMMJI: Oil'
• ••••••••
t.I!lPROsY COtrl"ROL IN Tffl "'P!~"'RRN PACII":r,r. "lJ1tON •••••••••••••••••
'3
9. I!!MIHA'!'II!D ADDtTtONAI. RESOURCES R~"r.RJl:D BY r.OUNT"II~ tff ~H~ WESTERN PActFIC REorON •••••••••.•.•••••••• 18
10. THr.RAPIP.IJTTr. RF.OTMF.NIII R!COMMRNDRD '1'0 THI!: CUNICAl. r.LU~'f'T.CATtO~ A~n RA~TRR:rAL ~O~DTT10N • • • • • • • • • • • • • • • 20
11. METHODS AIM!D A'I' DETJI!RMTtmrO THE EXTENT OF DAMONP! RF!~T~TAN~~. 2~
12. MANAORMI!:N'I' OF LEPRA REAr-TTON TN THP! ,tELn •••••••••....••..•••. 24
13. CURRICUI.A PRIP.PARATION FOR TRAINtNO AND 'I'I!!ArH!~I('I PF.I!~ONNF.L ••••• 28
14. IVALUATION OF LIPROBY CONTROL PROOR~E ••••••••••••••••••••••• ~o
'S. LEPROSY MANAQBM!NT INII'ORMATION SYST!M •••••••••••••.•..••..••.. 32
16. RP!COMMINDATIOHS
ANNI!:X!S
...............................................
, - .......................................................... 2 - WORKSHOP ON EPIDEMIOLOGY AND CONTROL INCLUnU'G F'!ELD THERAPY
39
XI INTERNATIONAL L~PROSY CONGRE~~. MEXlnD CITY 1978 .••••.. 45
3 - AGENDA ........................ , •••• , •••••.••••.•.••••••••• , lJ 7
4 _ LIST OF MEMBERS, CONSIJLTANTS ANTl SECRE'l'ARtA'l' •••••••••••••• 51
5 - LIST OF WORKING PAPERS • • • • • • • • • • • • • • • • • • • •• • • • • • • • • • • • • • •• 55/56
6 - IfBFERBNr.B • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • 57

1. TNTROD!lC'T'ION
The First Re~ional Working r,roup on Lepro5Y W~5 h~lrl ~t the W40 Conference Room in Manila from 7 to 12 December 1978.
The objectives of the Workin~ Group were:
(a) to revi"lw ongoi.n~ leprosy control activ1t1.e~, 1nc111111nl1; (ll t.he magni tude of the problem, and (it) the pro/l:ra'mme management of lep,.osy control;
(b) to recommend to the Regional D1.,.ecto" stratellies fo,. the progrannne management of leprosy cont,.ol activities in the oount,.y tn Une with the proposed regional st"ate~YI including manpower traininll fo,. leprosy cont,.ol;
(c) to review all chemothe,.apeutic rell:imens cur,.ently betnll: used tn dfltermine the frequency of dapsone-resistant cases being encountered;
(d) to develop a system of l'Ionitor1.np: the spread of tiapsoM-"es1.stant leprosy and to propose effective oountermeasul"es to minimize this resistance.
The meetinll: was opened by PI" F.J. I)y, Relli"M1 01.!"ent('),. of t.he W~O Western Pacific Region. He sai.1i that the follow-up of the lonll;-term therapy has become a serious pl"oblem. T.rI"Ap;ula,.i.ty of trelltment and an increasing number of I"elapses are beinp; reported. The problem of dapsone resistance has a150 been reported from many parts of the world, and even though new drugs are ava1.lable to treat dapsone-resistant cBses, if regularity of drug intake is not obtainerl, the Doss1.bHtty arLses that i.n the future resistance to the new drugs will also appear. Or Oy als(') referred to the need for control measures to be t:leveloped ~m I'In l.ntep;l"al part of the general health services and the lIimpJ.e !lnli efrectlve tra1.nl.n/f of the general health worker. The substanUal rinancl'll oontrlbut1.ons bv many voluntary organizations w1.1l undoubtedly help lepr(')I"Y control acti v:1. ttes tn the Reg1.on.
01'" Fernando A. Jose, Jr. WI!S ~leoted liS nhlll.l"l'Ian, 01" On 1"1. ~111\, illS
vice-chairman and Dr W.R. Lang as rllpporteu,..
The agenda adopted is given :1.n Annex 3. There were 12 temporary Ildvisers from 10 different countries; their names togethfl!r wIth those of the oonsultant and seoretariat are listed in Annex 4.
This report aims to summarize the information pl"ovtded hy c~untl"v
reports, as well as the discussions on the different topics. The wo~king papers prepared by participants are available upon request fl'om the Regional Office; a list of the papers is given in Annex 5.

- 2 -
2. REVIEW OF THE REGIONAL LEPROSY r.ONTROL PROGR~F.
2.1 Introduotion
A review was made by Dr S. F.nrlo of the past An~ pre~ent WHO oollaborations with the Member Governments in the leprosy oontrol pro~rammes. He also mentioned the different voluntAry leprosy assooiations that 'lSsisted the prop;rammes 1.n oountries in the RI9p;1.on.
In 1965, the First Re~1.on!l1 ,C\eminar on I.eprosv r.ontrol was heIr! l.n Manila. Among the oonolusions drawn during the meetinp: the rollow1n~ were oonsidered as most relevant:
(1) tf the preval~noe or known oases t~ a oountry is around onp. per thousand population or higher, leprosy should be oOM1.dered as a pubHc health problem.
(2) The role of sanatorIa shoulr! be limiter! to the treatment of' cases with acute lepra reaction and other oomplioations, to surgery and rehabilitation anr! to serving as centres for researoh and tratn1.np;.
(3) The advantage of integration of leprosy control programmes into the general health services.
2.2 Size of the problem
Participants from six countries were requested to oomplete the questionnaire oonoerning the leprosy problem in the oountries ooncerned. The epidemj.ologioal profile is s\lIIIIIartzed in Table 1a (Annex 1). All oountries/areas have prevalence of one per thousand or higher with an average of 1.8 ranging from 1.1 in the Philippines to 7.0 in Papua New Guinea. The proportion for the registered oases of the estimated number of oases varies from 27.7. in Soctalist Republic of Viet Nam to 83.7. in New Caledonia.
The estimated prevalenoe of lepromatous oases varies from 0.5 per thousand in Malaysia to 3.2 in P~pua New GUinea.
All oountries exoept Malaysia (26.5~) have inpatients of 10_20~ of the total number of patients.
The Philippines anr! the Republio of ~orea depend on the v~rtlos1 programme; 1n other oountries, the programme is integrated into thf! p;ene"sl health services.
In summary in most oount"ies/areas the leprosy programmes have been conducted for more than ten years. rhe size of the problem is still oonsidered to be one of the public health problems and except for ijew Caledonia the proportion of patients under treatment is still far below the target.
- 3 -
2.3 Problem related to regional policy in leprosv control
The objectives or the regional lepros~ programme a"(> clearly tjef1nad 1 n the "egi.onal programme profi 1.e which has been approveti bv the Reglonal Programme Committee. However, the approaches to the obJectives arp. not clearly defined in dehiL For the effecUve i.mplemenhtton or the leprosv programme so as to achieve the regi.onaJ. objectives, more ()lelu'ly-defined approaches including control measures to be taken and the programme formulation must be worked out. The approaches should be practioable and flexible so th'!lt the~ could be adapted to the different condttl.ons of the health structure in the countries of the Region. The main sUb.1ects on which advice from the Workinp: Group is needed are the cont"01 mellsures to be taken and the programme rormulation. These are interrelated, and ma~ vary depending on the health structure of each countr~.
Attention is called to the following:
1. Whether the programme is inte~ratetj into the general healtl1 services 01" not, preliminary diagnostic services should depend on the non-medical allied personnel. Therefore, the t"1!.i.ning of he'llt.h workers 1n the diagnosis of lepros~ is verY important.
(a) What kind of workers aM QuaHfied ror the tr"lining?
(b) Who should be the trainer?
(c) How long should trlli.ntng be?
(ti) What is the curriculum?
(e) Where 1.s the p1 ace ror trai.n!.!'Ip;?
(r) After tra in1.ng can he/she make the riMl d1'lP;Msl.:'I t)r should he/she refer the patients to a med1.c'll off1.cer for confir!'!at,10"l?
(2) Bacteriological examination is an essenti.'ll tool for t1t'l~nosi.~ and review of progress of the disease. The gi.te of t,he skin from which l'Imear is to be takp.n, smear mal<i.ng, staininp: anci read1."I11: are very important subjects of training.
(3) What is the role of histologi.cal examination in lp.prosy control?
(4). The household contacts have a higher risk of contracttnp: leprosy than the general population. The present situation of contact examination is that even in a well-organized programme only 20% of the contacts are examined. On the other hand, there is some evidence that the contribution of the new cases detected by contact examination to the total new cases is low - around 20~ or less. Should ~e concentrate on oontacts who are deemed to be at higher risk?

- 4 -
(5) in many countries, the governments ~o not realiz~ the importance of the manlill!'ilment aspect or the prop;"anunp. SIIC" AS .,upe"vis:!.rln, rP..rres"er training and eVllluation. Tl1e mllin reason ror treatmE'!"t f'AHu"e !'lay I)", lack of thl~ mlin~II!"'ment; ~nd the expenses 1'or the improvement 01' manap;ement would be much cheAp'!r than thosF!ror procu"eme'lt of seco"dA"Y t!rulI!s.
3. Rl!:r.OMMENDA'l'IONS OF THE RE~P.NT iN'I'BRNA'I'TONAL LEPROSY ~ORKSHOPS IN A~iA SPONSOR"O BY THl!:
SASAI<AWA MEMORIAL HEAL'!'''' FO!lNDA"!O~J
3.1 Dr Y. YUIlsa co~p.nte~ on the recommendations of the internlltional leprosy workshops that "live bf'en held 1'1 Banll:koK, ~Ani1a "'n~ ,Ta\{'lrtl'l !jurin$!: . the years 1976_1977. 1
3.2 Meeting in Bangkok, November 1976
This worksl1op analysed tl1e problem roe' at ... d to t,"e trdn1np; or lepro!'l~ worke!"s in Asia and reconuner'll'led that Ii fact-rindi"l!; mission be cl'flate(f ion ol"dtu' to conduct an on-the-~pot study or existinp; institutions anl1 prograllllDes in seleoted oount .. t f!S of Ash, al'ld mllke a Cl"tt il'!d appl'''Ii ~'.I! of' these fI\CUtl:l8s. The ract.-f1nIEnp; Plt/ll'll.,n Sf'nt, to a '1umbflr of' cnuntl"ies recommended that the exist1n~ national centres shrluld b~ strenl!;thened possibly in cooper"lt1.on wU" ot" ... r medical lind educ3tlonal l.nstUut1oM to lIIeet nationAl needs and also to be user' from ttmOe to ttme for training on iDte,.national leval.
3.3 Meeting in Manila, January 1977
Th1!'1 worKshoD ma 1."ly stuMed the problems rellltel'l to the tre~tment or leprosy patients, particuhrlv in the light of the tncre'lsi.ng numbel" of oases reporter.! to be sulfone-"esistant.
The importance of conducting prevalp.nce surveys on dapsone ~-.stAtanc~ wa~ stl"essl'!if.
Specific recommenriations were p;ivlJn for t.he t!"t'latment ('If' patien!;s with multibaoillary forms of' leprosy.
it was also reconunenrlel1 tllal: health wO!"kBrs who a"e engag",d 1.., 1"'orosy control activities should reqeive app!"oprhte t!"atning in the I"ecol!~tti(,"
and treatment of dapsonF! resi.'!lt!lnt cast'l!l.
The need ror accurate treatment records, prefer'ibly st'indal"rlized, wa., elllphasized.
1Reference 3, 4 and 5 in Annex 6.

- '5 -
3.4 Meeting in Jakarta, November-December 1977
At this workshop representat i ve::; from rlonor 'lp:enc i ",,,, unrler the'lll.'lp!.ce::; of ILEP (the Internati..onal Feder"lti.on of Anti-Lepro::;y AS30~iat.tonto) met witl1 government representa t i. vel'! and exehanp;ed vi <:!ws on f'urthe" 000per"l t i. on in tl1e future in the leprosy control prop,rammes.
Much more speCific recommendati.ons were marle on ehemot.l1erapy ann 'IS a result of the meetin!l: the SMHF has provi.rled cloflizimine to ::;evl"ral count.ries that have since accepted the offer marle by the "'oundl'ltton • rl-temot.herapy trials are also being sponsored by the Foundati.on Rinee the J"lka"ta workRl-top.
The workshop also recommencied that. an operFltional fea::;i.bl1 Hy Ilt.urly be made on the combined regimens of dapsone and other drugs stl()h as clofazimine, rifampici.n, etl-ttonamirle with parttcul"lr referencf'! t.o t.he availability of the tirugs in terms of eORt anti MceptabUUv oy t.he oat.tent.
4. ANALYSIS OF ONGOING LEPROSY rONTROL ACTIVTTTRS IN THE COlHJ'l'RIES
4.1 An epidemiolop:ical profile of leprosy for ~oIJrltl"te'l In the Rf'!p;l':m 1.3 given in Table 1 (Annex 1) and the m"lin problems f"ncoqntere(j in the orop;res:'l of leprosy control programmes are gi.ven in Table 2 (Annex 1). These problems by order of priority were discussed and confirmed by parti.ci.oants as they are shown in the mentioned Tahle 2.
4.2 Additional relevant informat1.on on count.ry leprnsv crml;r"l pI"op;"'ammeR given by partJ.cipants on their respect; ve cOlJntri.es wa~ ~:l fr,l.l o~,s:
4.2.1 Republic of Korea
The prevalence of leprosy is stearli.ly deer~'uli.np:. It '''CiS "'''oortF!d that about 1000 new cases are detected per year witl1 rlecrf'asing tenrlf'ncy (800 n~~ cases in 1977). There is a tendency of shU'tinp: of a~e of "i.":'lt '1ppearance of leprosy to older age grouos.
About 80% of leprosy cases are in the southe!'n part of the countrv. However there is evidence of the spread of leprosy to some vi.ll.ap;en not previously affected.
An increase in dapsone-resistant cases was noted. The Korean leprosy control programme is a vertical prog!'arnme depending mainly on mobile cli.nics and the Korean Leprosy Institute actively i.nvolved in the traini.n/l: of medical and auxiliary workers.

- 6 -
4.2.2 Philippines
Almost !'lll 74 provil'lces !'lrf! coverer! by the lepros" control Mrvices consisting of 8 lepros!'l!"i!'l, 15 mobilp. and 6 sti'lttona"y sktn .,1.1.1'11.0:::.
Leprosy still rem!'liM a major health problem in n1."e provinces. AbolJt 47~ of active cases are lapromatous.
Case-fint11nFt is dona through examinll.tton of pattent.:'I vis1.tin~ at ski n clinics. examination of household contact.'!. examination of :'Ichool cl'lildren (not important at prp.sent) and throu~h noUrteati!)n.
Since 1977 treatment with dapsone has been increasad to 50-100 m~ daily to conform with WHO recommendations.
Integration of leprosy cont.rol act.ivtties into the ~eMrf'l.l hMlt" services following the "ecommanrlat tOni! m'lde by T)r R. V. Wl!rllak'lr. WIiO consultant (1967) is stUl in progress - thp. results so far 'Ic"levad he'n~ rather unsatisfactory.
It was reported that "suspectell dapsone resistllnce" was or tht'! of 15.7% of LL and ~L cases for outpatients anr! 60% for l.no!'lt i.ents. estimate will probably be reducell H the sti'lnr!arrl olinil'!al c"iteria dapsone resistance is applier!.
Discussion
orrlar T",s
ror
It was suggested that the rather alarming statistics on rtapsoneresistant cases 1.n the Phi li.ppine might best he oonsidered as provistona 1 and subject to "eview. There should ba a cl!'lrifi.cation of whllt oeople mean by relapse and reactivation.
4.2.3 Socialist Republic of Viet Nam
The leprosy control activities are integratert into thp ~eneral healt" services at periphery levels with leprosy control centres supervtslng treatment of arounr! 800-1000 leprosy patients at ~~termed1ate levels. Difficulties arise from the existing prejudice a~ainst leprosy and the scarcity of speCialists.
A five-step met"od for the programme was descri_bed:
health education among the masses; training of cadres (average 7 days); mass examination, village by village in a "'lolling Mat" manner: conftrmat ion and classlficat ion of the patients; leprosy dossier for home treatment or hosptt'!l1.z'!tion.
- 7 -
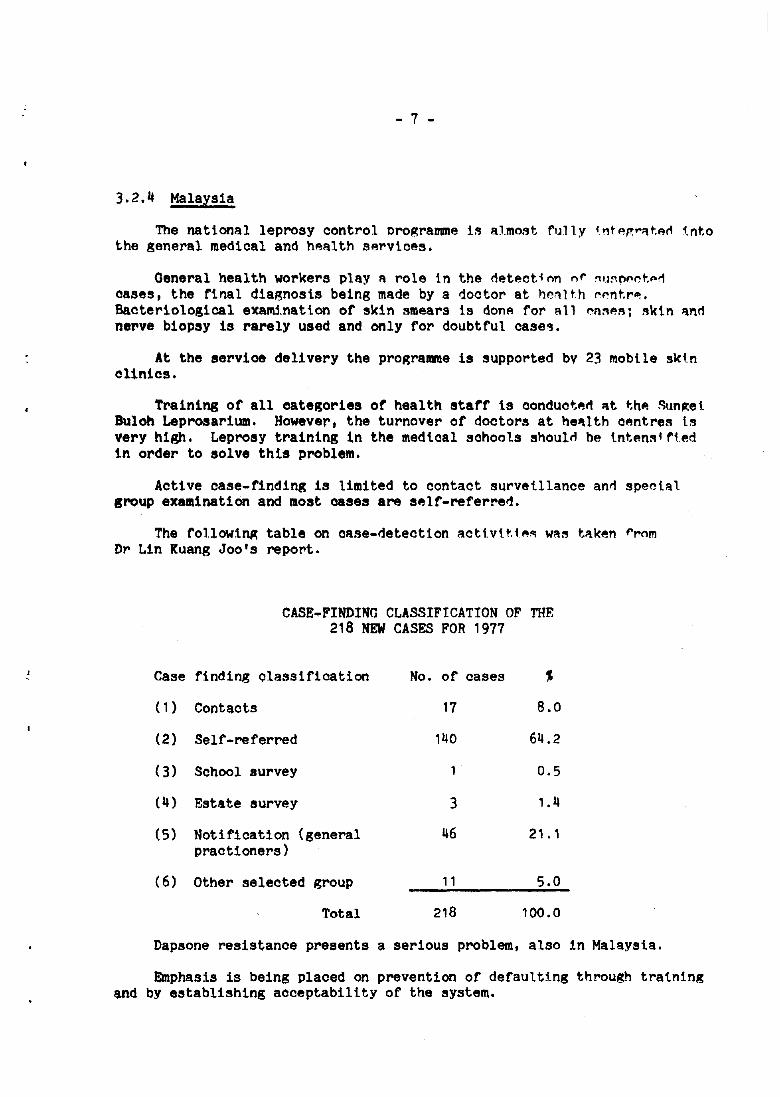
3.2.4 Malaysia
The national leprosy control programme is almost fully i !1tp,p: .. ~t.f!rl i.nto the general medical and hp.alth services.
General health wor~ers play A role in the detectinn nr ~lmD"~t.p,r1 cases, the rinal diagnosis being made by a doct.or at he~l t.h rl'!nt.r-.. Bacteriological exallU.nation of skin smears is donA for all I'nM~; skin ",,,d nerve biopsy is rarely used and only for doubtful cases.
At the service delivery the programme is supported bv 23 mobile skin olinics.
Training of all categories of health starf is conductjlld At t;hp. ~\lnp:e1. BUloh Leprosarium. However, the turnover of doctors at he~lth cp.ntres is very high. Leprosy training in the medi.oal schools shoulti be i.ntE!ns1rtE!d in order to solve this problem.
Aotive case-finding is limited to contact surveillance and special group examination and most cases are self-referred.
The fol1owl~ table on case-deteotion acti.vtt.1.M WM tl'lken r,.om D,. Lin Kuang Joo's report.
and
Case
(1)
(2)
(3)
(4)
(5)
(6)
CASE~FINDING CLASSIFICATION OF THE 218 NEW CASES FOR 1977
finding olassification No. of cases %
Contacts 17 8.0
Self-referred 140 64.2
Sohool survey 0.5
Estate survey 3 1.4
Notification (general 116 21.1 praotioners)
Other seleoted group 11 5.0
Total 218 100.0
Dapsone resistance presents a serious problem, also
Emphasis is being placed on prevention of defaulting by establish!ng acceptability of the system.
1n Malaysia.
through training
4.2.5 Papua New Guinea
Integration at ~ll throu~hout the country. special leprosy clinics or teaching.
Main problem are:
- 8 -
'_p.vels with the p;ener~l health servicp.sis Ilnrter1oJ'lY Thel"e ~I"e two majol" tl"f!atment l1ent r es an" ftve
and only a few speci.al1zel'1 personnel fol" t,1"p.~tment
training enough health workers at all levels of lI;eneral he"llth servl.cp.s to handle change-over fl"om institution1'!.l case to domicialiary cal"e:
drug supoly (drup; combination required): anri
drug resistance.
4.2.6 New Caledonia
Dr R. !"arrugta "eported that there wns a great need for trli tntn/!: ::t.nd health erlilcation. The stigma attacherl to leprosy is Ii ma,10r prt)hlem fo!" the detection and treatment of Ca::lP.S among the European popullitton, whtl.e IlmonR the native popuhtton thFlre was no fear of leprosy hut tp;norance.
As rliAgnosi.:'l of leprosy 1.s alwavs (10ne ]a~,e, chl'lmoprophyllixl s wi.t.n OAOOS (Hansolar ) intramusellhr in.1ectl.on 1.s given every 75 day:'!. Th1.s WAS started in July 1977. Adrlitional dose of dapsone 150 mg/week for adult:'! and a lower rlose for chUrlren is I\lso p;iven. The prophylact.ic treat.ment will last for three vears and i.s expecterl to cover a oopulAt1.0'l of 3000.
The number of cases detected last year was 58; 13 leprom'ltollll and 2 tuberculoid cases relapsed duri.ng the same veal".
Discussion
It was menttoned that the val tdtt" of the type of' proot,,,l'!.xt.'l indi.cated by Dr Farrugia may be qup.'3tioneci hecause it I'lIiY .1U'3t leari to suppression of leprosy HUt, subsequent emer~ence of cases.
4.2.7 South Pacific (see tables 1b and 2b Annex 1)
An account of the leprosy control activities in the ~outh Pacifjc was made by Dr L. Lopez-Bravo.
The activities of the WHO intercounty project called "Leorosy control advisory services" started in 1972 with the assistance of the Leprosy Trust Board (New Zealand) and was strengthened with assistance of the Jaoan Shipbuilding Industry Foundation, since 1977.

- 9 -
Training of health personnel is concentratp.d at Twomp.v Mp.mo,.i.'il Hospital, Suva, Fiji under an agreement between the Fi,it Governm ... nt, WHO and the Leprosy Trust Board (New Zp.aland). Two courses, each of one month's duration, will be held each vear. The Twomey Memorial Hospitlll haR been deSignated to be a rp.ferral cp.ntre for the South Pactfic. It 1.s proposed that upon the request of governments in the South Pacific:
(1) Members of an intercountry leprosy team should pay a follow-up visit of each country at least annually.
(2) Training and refresher courses for health personnel wi.! 1 be conducted.
(3) Training in reconstructive Rurgery will be provided.
(4) Health education material on leprosy will be prepared.
(5) Drugs will be provided to governments where other provisions Ilre not available.
Joint effort of the Leprosy Training and Referral r.entre and the intercountry leprosy team could do much for the control of leprosy in the South Pacific. It Reems to be the right approach to serve the needs in the field of leprosy of these scattered groups of country-islands.
Discussion
It was suggested that research studies should be taken into consideration. Studies in tmmunology and chemotherapy were also suggested. Small circumscribed areas were considered ideal for chemotherapy studies.
4.2.8 Fiji
Dr E. Karuru said that control activities are well integrated into the general health services. The final ~iagnosis of suspected case~ is done by the leprologist at the Twomey Memorial Hospital. The expenses for treatment including hospitalization and travel of patients to the medical institution are paid by the Government. The lepromatous rate among children (newly detected cases) is 21.4J and the incidence rate 0.6 per 1000 population (total population 600 000).
Discussion
It was noted that the proportion of lepromatous cases is very high in children, implying much transmission of the disease.

- 10 -
4.2.9 New Zealand
The Lepers' Trust Board Inc. (New Zealand) was fOllndl'ld hy MI" Twomey Chri.stchurch, New Zealand and is now ca U'ld r.eprosy TrlJ~t Boarr\ (New Zealand). With members drawn from influential ann puhlir.-mindF!d ci.tizens throughout the r.ountrv, non-governmental, voluntary RP,pn0. i es exist through subscripti.ons from the publ ic in response to I'Innu'l.l 'lPPM'.3. Income in excess of $300 000 per annum js mostly disbul'sen in the South Pacifi.c area after mini.m!!.l neduotion of expen:'les 1'01" On"! sellret.ary, one assistant secretary, OM typist. Donat.i.on to Leprosy St.Ut:!y Centr"!, London, $5000 per annum, to WHO Headquarters, Genp.va $10 000 pel" annum.
Medical Advisor Committee. r:hai.rmlln, secretary, treasurer, rt\ur doctors one from the Department of Health).
Fiji - P.J. TwomflY Memori.al flospH'll. Dr Karuru, and the "'1.1 1 Government as a partner with WHO and NZLTB f'unding.
WHO Regional Office for Western Pacific Region
One half of the sahrv of Dr Lopez-Bravo, intercountry 1 eprosy advisory services project (ICP/BVD/005) is funden by L'1'B.
r:ountr1 flS assisted by N~'f'LR: Samoa, New r:aledoni'l., ~flW Hebri. nee'!, French Polynesia, Solomon 1sl'lnds, Gi.lbert Islanns, and ethel' Po'yne::tlan countries/area (Tonga, Cook Islands, ~iue, etc.)
Leprosy control in New Zealand
Integrated with the general hea 1 th servi ces with free consultation advice, treatment and hospitalization where necessary.
Registration and follow up of the patients are the respr:msibiFty of the Department of Health.
Main prevalence is in Auckl.:md - 52 acti.ve cases; Welli.ngton - 12 or 15 active cases; elsehwere - a handful. Most cases fl'om Samol'!. anti a few from other island territories.
Biopsy specimens go to Leprosy Study "entrf! in London. I)ne r\efi.nH.e case of dapsone resistance has been seen.
5. SUGGESTIONS ANn PROPOSALS TO IMPROVE TH~ EFFICIENCY OF LEPROSY CONTROL ACTIVITIES ACCORDING TO THE
MAPl PROBLEM AREAS IN EACH COUNTRY
Dr F.M. Noussitou commented on Table 1a (see Annex 1) Epidemtologtc'll Profile. He stated that after 10-20 years of continuous control acttv1t.les in many countries probably only one half of the cases have been detected and most likely one half of the detected cases are not taking proper treatment. If it is considered essential to have at least 75% of positive cases under treatment in order to achieve a decltne in the inctdence of leprosY, the performance of the countries is much below target.
•

- 11 -
Based on his observations during his recent visits to Malaysia, Papua New Guinea and Philippines and his previous visit to the Republic of Korea, Dr Noussitou commented as follows:
The data obtained at ce"tral level has to be cross-checked with those at the periphery, as information provi1ed in official reports is usually overestimated, when comparect with that of the service delivery level. Consequently, there is an urgent need to finct out where the problems are and to make realistic changes in strategy when indicated.
Dr Noussitou presented the main problems by order of priori tv in each country which were corrected by the participants in the diSCUssion (Table 2a, Annex 1). Trainlng of health personnel at all levels was the first priority for all hut one of the countries represented at the meeting. Supervision was the second priority for most of them followed by drug supply, transport, physical rehabilitation, health education and information system as priorities, falling into a different order for each country.
Discussion
It was suggested that once priorUies anct targets were estabUstted for each country some broad proposals should be made for its planning of control activities.
6. INTRODUCTIO~ TO PLANNING PROCESS
Dr R. Mercado stated that the approach to a health problem in a communHy or a country needs to be very objective. The first step is the analysis of the situation which results in the identification of problems. The next step is the formulation of solutions to the identified problems. The third is implementation and the last is evaluation followed by reformulation.
In formulating the projects, the follQwing need to be tione:
(1) State in broad terms what shall be done and how it shall be done. There is need to be selective in this process, giving higher importance to actions which will give maximum returns. This part of the exercise is referred to as policy planni.ng, which consists of
- setting up of main objectives and establishing order of priority amongst them
- formulation of basis for specific strategy
To accomplish this, there is neect to refer to the final list of problems identifled, review the object! ves and prinCiples of the first national health plan, and interpret the implications on health and health services of the more recent policies of the country.

- 12 -
(2) Health objectives '3.re realized through th" fOr!!1111'ltion 'lnrl implementation of progra!!1mes. There a~e three 0ategories of p~o~ram!!1es, namely: those which deliver tl1e promotive, prevenUvp., curati.ve ami rehabiltt'iti.ve servi,Jes, USII'illy referN!rl to as final p~o~rammes: tho<;e more technical activities which assist the final pro~rammes like X-rav, laboratory, health manpower development, statistics, I!!tc. call1!!d intermediate progr'immeSj and those essenti'il activities which support hoth fina land intermed iate pro~rammes like finance, personne l, Sllppl. v, etc. usually referred to as general administration. These p~o~rammes are of equal importance, and a breakdown in anyone of them wUl he felt by the whole system. The intermediate and general arlmi.nistration pro~rammes wOllld have for their objectives the provision of assistance anrt support to the final ones.
For final programmes, technica 1 tar~ets in terms of disease ~ertllct ion should be set up whenever at all possible, as well as in terms of health activitiesj identifying major ones, the population to which these shoulrt he directed, their frequency, morle of applications, and total numbe~. Another set of targets called administrative tar~el;s would be the changes 01'
additions/deleti.ons which should be made to make t,he prOl!;rl'lmme capable of carrying out its health ami activity tar~ets. They are based on tl1e identified problems in operations. Hence, the reason for asktnp; those i.n charge of programmes/services to make revi.ews, 1lsinp; as ba::tl::t the changes/constraints stated i.n the first nllt10nll' he~lth pl~n.
The targets of intermediate and general p~op;rammf'S are activi.ty targets in support of the technical. and adm1 n i.strati VP. tarp;ets of the f1 na 1 programmes. They themselves often requirf' changes/addttion/deletion:'l with corresponding resource reqlli.rements.
(3) To raise the capabi.lities of progrl'lmmes so that they ~an accomplish their targets, which taken together would lead to acl1ievement of' the national health object;ives, tntenstve, specinc, ti.me-Hm1.t:p.d acti.ons must be planned and carried out.
It will he noted that ~ll the preceding steps of p1l'lnntnp: thus far described, have only one purpose - the identification and formulation of projects. Without. the latter,. the pl.an would probably rel'1a1.n as an intellectual exercise at most, and not a tool. of nevelopment.
7.' Introduction
- 13 -
7. PROGRAMME PLANNING AND EVALUATION FOR LEPRO.')Y r.ONTROL
Dr J. Walter stressed the importAnce of pro~rame plll.nning to p;IJ1.l1e the programme in the right direction and improve its op~rational effioiencv.
Programme formulation provides a logical process for ensur1.n~ a fu1l analysis of the current epidem1.ological, operational, and mlina~er1.al problems.'
The formulation of deta1.led programing such as that for leprosy control is part of a much wider concept, country health programming (CHP) ann medium-term programming (MTP).
Country health programming is the systematic process of assessin~ Ii
country's health problems in their socioeconomic context, of identify1.ng areas susceptible to change, and of formulating priority programmes to induce such change.
The sum of these obJecUves and actiVities, their purpose top:ether with policy directives at country, regional or global levels, forms the basis of MTP.2
Taken in this context, MTP thus has general financial implications which have to be formulated into programme budgeting covering a five-year period. MTP should permit tentative budget forecasts needed for the planning of long-term country development, for external technical cooperation and for the attraction of financial assistance from external sources in general.
Medium-term programmes should be elaborated according to "clearly defined policy orientation".3 There are four main steps3 in the programming process:
Step 1 - Collection and collation of information Step 2 - Situation analysis of programme areas Step 3 - Formulation of broad programmes Step 4 - Formulation of detailed programmes
1WHO Technical Report Series No. 607, 1977 (Fifth Report of the Expert Committee on Leprosy).
2WHO Document PWG/3/15. Annex III (Revision of the Provisional Working Guidelines for WHO's Medi.um-Term Programming).
3WHO Document PWG/3/15, Annex III (Revision of the Provisional Working Guidelines for WHO's Medium-Term Programming).

- 14 -
Hence, the form'll::;tion of a leprosy progr~mme lIlust he 'tn 1 nte~rate(i part of the MTP and CHP.
Havin/l: out lined broad orogrammt np;, the purpose then is 1:0 rii vtrle thl'! broad programming are::;s i.nto programmes of lIl!'!.n'lge!'!.hle size !'!.nrl determi ne the vari.ous org!'!.nization'll levels.
The purpose of det!'!.i.led prop.;ramming is to '.ork ('lut. 't ph!'1 or 'tc~.ion
for the a tta tnment of the specUic ob.lecti ves of a suh-orop;r!'!.mme and i. ts implications (or interface) at 'Ill organiz!'!.tional levelfl.
7.2 The formulation of a detailed programme
When undertakin~ detai Toed programmtng, the prop;r~!'II!Ier wi 11 a lrp.!'!.dy bl'! in possession of the list of activities selected during the broad step. The process would thus conslst mainly of:
more det!'!.iled description of methods and approach:
detailed description of activities;
description of physical faci liUes !'!.nd manpower require'" to c;:trrv out the programe;
more preCise all ocat ion of resources th'ln i.n the case of' hroa'" programming;
a rlescripti.0n of interrel'1tionships with other prop:ral'lllles of' acti vities requi red for each step of ~.he acti. vitV;
output indicators for each activtty;
a detailed plan of acUon that correlates 'Inri coorrli"at.es all ~.he above elements."1
The outcome of detailed progra!'ll!les wD 1. be an individual. pllin of action for the implement!'!.tion of programmes in specific program~e areas.
Recalltnp.; steps 1 to 4 of the medi.um-term progr!'!.mmtng, p;ener'll 'tnfl speci fic informati on may he collected and collated, t. e. population d!'!.ta, the prevalence and public health importance of othe" rits~ases I!nd thetr planned control, the leprosy problem, its identtfication anI'! quantification. There are four commonly used 1.ndicators1 for rleHneating the nature of the leprosy endemicity in a given are~;
(1) The overall preval~nce rate (2) The lepromatous prevalence rate (3) The proportion of the different forms of leprosy (4) Age-specific rates.
1WHO Document PWG/3/15, Annex IrI (Review of the Provisional Working Guidelines for WHO's Medium-Term Programming).

- 15 -
The planni.ng for ""Asource requirements for two and preferablv, perl-taps tentati vely, for a five-veal" period, ;s another i.mportant ta!'!K to be included in the deta iJ ed programminl!:. The pri nctpal resource requt rements in leprosy control are:
manpower requirements with salary estimlites;
drul!:s and laboratory equipment ann estimated cost~;
transport need:'! with estimat.ed expenMture for capttaJ (\utlav ann running costs;
building and of'fj.ce nef'!ns inclut!ing maintenance costs.
7.3 EValuation
Indicators for the eVAluat"ton of pri.ncip'" 1 l'Iub.1ect arp.a:'l i.n 1 epro:'lV controJ have been defined in the 1966 ant! 1977 WHO Expert rommittee rp.po,.ts M well as by Bechelli and Mlirti.nez Domjnguez. 1
8. TENTATIVE MODEL FOR A M~DIUM-TERM PROGR~F. IN LEPROSY r.ON'l'ROL (1979-1983) IN THE WE~'l'F,RN PAr-':FIr REt'HON
(BY COUNTRY)
A theoretical m01e1 for a medium-term programme (5 years) for intensification of the programme currently being operated i.n leprosy control in "Lepra1and" with a detailed tahle (see TabJ e 3, A.nnex 1) was presented. Many bacillary positive cases and relapse cases have been accummulated as not properly treated. In the first year these cases have to be properly treated. This is the reason for the high expenditure in the first year.
The plan indi.cates costs. number of trainees, eqUipment, firllgs, etc. and the priorities expressed are the same as the ones previously di.:'lcussefi for each country as shown i.n table 2a (:'lee Annex 1). It I.s noted the tabl~ shows on1~ additional requirement for intensification of the programme being currently operated.
The model of information in "Leprosy information on Leora'.anfi" lists population statistiCS, type of programme planned anrt the requirements for the future.
The presentation \o/aS meant as an exercise in medi.um-term prop:""amming so that participants wi.ll in the future be in a position to prepare slmila" proRrammes to fit into the requirements and possi.bili.ties of each country.
1 BechelH, L.M. and Martinez Dominguez, V., Bull. WId. Hlth Org. , 42, 631 -634, (1970).
- 16 -
Discus!'!ion
A participant sllggestp.d 'inding to a f'inal plll.n til!" f"llo'~lnp.:
(1) rosts for planning process - t"atninp: of olanne ... s - oeriod or time neenp.d
(2) Technical justification
mlmber of patients, estimated
expected vea"ly increase of case!'!
case detecti.on l'lethods to he USI"d, i.ncorpor"lt!"d forms of registerp.d cases (LL BL BB 8'1' TT), adul ts, cl,) 1 rlr"'1 (proportinns of tl1ese), de form:l.tie!'!, et.c.
number of referral i.nstitutions, initial and mll.i.ntenlHlce costs.
(3) ~ number at various Ie-vels anrl costs per year.
same for mult i.pllrpose workerR in the pertpherv.
(4) Transport initial and maintenance costs.
(5) Laboratory faciliti.es for smear t::tl<tnp:, dapsone re!'!istance determination, etc. and mainten::tnce costR.
(6) Tot::t] aver'lge cost per pati.ent per year.
(7) Budget: state na tionaJ. budget, 'lnd expected i.nterface support such as WHO, UNICEF, voluntary organizations, n'ltional "lncl international.
(8) Optional - operati.onal studles: protocol, obiectives, metl1orl, start find expected completi.on.
Treatment
It was mentioned that the most important variable was going to he the number of drug-resistant cases.
A parttcipant suggested that once th.e acceptabil tty of the 1rug W"lS obtained, costs per patient should first he worked out and then budgeted accordinp:ly. Drug costs (::tnd regimens) have to be weighed (in te"m!'! of cost effectiveness) agai.nst the cost of the management of ca!!les suc" 'l.S
duration of treatment, transport costs fo" the fol1.o\o'-up, tl1e p::ltient's waste of drug from non-compliance, etc. - in other words, this meant improvement of operational efficiency; the use of combined rtru~ re~imp.n of dapsone and other effp.ctive but relatively expensive drug may reduce the cost for casp. mana~ement.

- 17 -
The possibH 1 ty of trell.tl.ng pure tubArculoirt p1'ltl.ent:'l "'ith rH':u'lpi.c i 11, so that they could he rti:'lch~rged rrom control, after a short period of treatment wa~ rai.sed. If thi:'l measure 1.s proved to be effective I!.
considerable worklolld could be rtischarged from the control act:!.v1tl.p.:'l. Tt. ,,'as noti.ced by many pllrtlci pants thRt the 11umber of pure 'l'T WI!.S not ve"'v common and mMY "tuberculoid" cases were actually BT. Lt was stressed t."Vlt the newly detected mu1.tlhacUlary cases should receive rtrst priorIty In treatment 1.n order to prevent. trl'!.nsmission of diseasF!.
Training
A wide-ranging discussion took place on the training or medical and auxiliary personnel deaJing with leprosy. It was obvious that job descriptions of heaU.h workers in leprosy l'Iervice vary p;reat 1y from one oountry to anot"ter depAnrting on the health servtce structure and type of leprosy control programme. Howevar, the .1ob description of the health workers at all levels and categorias involved in leprosy control ~ervices, includtng general he'lJth workers at the primary health ca"'e level, sl10ulti be clAarly delineated.
It was fully recognized by tl1e GrOIlP tl1at control of l.eprosv, be1.nll; a long-tel"1!l acti vi ty, will have to be an integr1'l ted acU v1ty at pel'ipher'l'., medi.1Jm and, to some extent, also at tl1e central levels.
Field workers can be trained to recognize leprosy, follow-up tha treatment of pat ients Md tR.kA skfn and nas'll smears including rt JCat ion; t"tey should be famiHar with reacti.ons and be ahle to promptly refer CMf's for hospital treatml'!nt if required. Duration of the trdning of this type of neld workers is one month. Since bacteriological finrting is very important to make diagnosis and evaluate the effect of treatment, trainj.np' of laboratol'Y technictan (mtcroscopist) should receive high pl'ioritv. '!'ha microscopy eX'imination shoulrl incl.ude not only findlnp; on posit5.ve/nep;'ltive but 'it least also bacter:l.ologicaJ. j.ndex.
Having agreed that the nrst priority in J.eprosv control progl'ammes was the tra:l.n1ng of hE'!alth personnel at all levels and echelons it was proposed that countries should have a full-Ume training officer, who must be knowledgeable in leprosy and trained in teaching methodology sincE'! he has to prepare the training programma of the wOl'kers at all levels.
There has been a problem in training of leprosy workers that trained workers often leave thE'! system clue to pl'omotion. This results in chl'oni.c shortage of key workers in leprosy control programme. The possibiHty of establishing career structures was considered as a solution that could attract good candi.dates to leprosy work.
The role of medical schools '.as stressed with emphasiS on more undergraduate exposure to leprosy as a subject and of leprosy being shown as a respectable study of great interest.

- 18 -
Supervision
:'leveral participants referl'ed to the need of re~1I11\1' ana c('>nti.nUr')ll1'1 supervision, espectally at the peripheral level.
Without constant supervi.sion contl'01 activiti.AS '"apj <1lv dp.t"!l'ioratp. however well the prop,ra!lll!le may have been tntttaterl.
Supervision must he buB t into tl-)e i.nH i..al p"op;"amrnp a1'1 '\n i nteg"I\J part of H" The supervisor should be i.nv(')lv"!a 1.n the cont"'ol snheme, LO!. be the man to whom thp. P1.elrl workp.r refer cases an(! r"om w"om teohnical. ativice i.S expectl!!<1.
It was emphastzp.d that the sup"lrvision tioes not mean merelv lnvp.l'!tigation of the performance; the supervi.sor shou1.d bp. actiVp.l.v involved in on-the-spot t,raini.'lP, of the fie)rI workp.r!'!.
The government has to provirle !'!ufPicient fun<1ing and tl'ansport POI" the supervision, as in many countri.es supervisors rlo not go out 1).111'111; t.r') 11\01< of travel expen!'!es and transport.
Hel'llth education
In the fielrl of health educati.on, the use of' pa!"ticular methorl!'! and even the assistance of health educators should ba taken into consi.rterlition so as to avoid much misrlirected efforts.
9. ES'l'IMATED ADDIT1:0NAL l'lESOURr.ES RF.:QUIRED BY r.OIJ~'l'RTES pj THF. I.jESTERN PAr.TPTr. RErHO~1
Dr Endo presented an account of the regional resources "01" lepl"osv control as follows:
Regional resources fo!' lep!'osy control
9.1 Intercountry project Ir.P/BVDI005/VL
9.1.1 Personnel
(~) One medical officer - one half of the salary and +-ravel expenses are provj.ded by the Leprosy Trust Board (New 7.ealand); t,he ol",hp.r h:j1,f is provided by the rp.p,ular budgp.t, WHO Western Pacific ~eg1on.
(b) One technical officer - Salary and travel expenses are prov1de~ by Japan Shipbuilding Industry Foundation, through WHO voluntary fund for health promotion.
•

- 19 -
9.1.2 Expenditures from the JSIF cont~ibution to the intercountry lep~o~v control project, Iep/BVd/OOS in 1978
Balance at the end of 1977
E!xpendHu~es, including unliquidated obligations and additional requirements until the end of 1978
(a) Staff (technical officer) salary and travel expenses $ 27 400
(b) Short-term consultant . (c) Training cour~e tn Suva
(d) Leprosy Working Group
(e) Supplies and equipment (or leprosy training centre
(f) Supplies and equipment for Socialist Republic of Viet Nam
(g) Programme support cost
rotal requi. rement
Contribution from J~IF 1978
Balance at the end of 1978
9.1.3 Estimated expenses in 1979
(a) Leprosy training centre and intercountry leprosy team
(b) Papua New Guinea
(c) Philippines (two vehicles)
Balance
Sub-total
23 600
19 300
17 500
11 992
80 000
17 208
$197 000
$168 000
$ 50 000
$ 14 000
$232 000
$309 776
$219 500
$332 276
$100 276
The use of the balance ($100 276) should be discussed at meeting.
9.2 Japan Shipbuilding Industry Foundation contributed funds for the (ollowing in 1978:
(a) (b) (c)
The Republic of Korea Philippines Socialist Republic of Viet Nam
(to be used 1n 1979) (to be used in 1979) (to be used in 1979)
$65 000 $65 000 $50 000

- 20 -
Dr Endo reque:'lted the p~rt i.cip'mts to put forw;:trd sllgge"lt ions on the utiHzation of the balance (US$100 276) for 197Q.
The participantR were inforllIed that the recornJl'lendattons of tl-li'l meeting could form a basis on which each country could prepare a list or their requirement"l. This list cOlllti then be submttterl to WHO !\lon~ with full supporting documentat:lon.
r.ountries mav neerl to develop the:l.r own tel!.ching prol!;rammes. '1'0 flo this they may need hel.p in the preparatlon and develoPIDf'nt of svlll!.bu!! contents and 1n tl-le understanMnp; of teachinl!; methods. WHO may hfl able to help in this report, perhaps by means of a separate seminar.
10. THERAPF.lJTIr. RP,G TMF.NS RF.r:OMMENDEl) Ar.r.mmnm "'0 'rHF. CLINlr.AL CLASSIF'rr~ATION AND BAr.TERIOI.OGTr.AL r;ONIHTION OF CASES PRF.VENTION AND TRF.A'T'MP.N'r OF' DAPSOJ-.1E REC;TS'l'A~!r.P,
10.1 Introduction
Dr F.M.R. WaterR said t.l-lat the basic causes for the fA.i.1.ure or treA.tment pro~ramme could be summarized as the result of a widesprearl failure of drug delivery and drug acceptance, a shortage or !lertal.n necessary drugs and a failure to use t.hose available in '~"'at i.s now realized to be the most scientific way.
10.2 Drug acceptance
To achieve good drug acceptl!.nce it is essential to gain the confide~ce of the patient and to convince him that treatment is '.rorthwhile. To do this the control doctor mURt understand the disease and ita treatment. He must have available effective drugs which he knows how to IJS'!! oorrectly, both in combA.ting the infecti.on with Mycobacterium leprae and i.n controlling any complications, especially reactions, quickly and efficiently. In additi.on, he !!lust he provided with adequate speohll .. 'lt. support and facili.ties, including adequate raciliti.es for Rmflar-t.a\(ing anr! examination, and for testing urine ror the presence of dapsone.
This impEes better supplies of drup:~, anti involves good mer!ica1. training of control 1%rkers, especi.ally i.n the recent adv"lnoes in the chemotherapy of leprosy.
10.3 Available drugR
1)rugs availahle for treattng lflprosy have been revi.eweti by the Committee on Experimental r;hemotherapy appointed by the International Leprosv Association (Shepard ~., 1976), which recommender! the use of bactericidal rather than bacteriostatic substances. Such drug~ fa 1.1 i.nto four groups, namely thfl sulphones (and long-acti.ng sulphonamides), rifampicin, clofazimine. and ethionamide and prothionamide.

- 21 -
10.4 SU8§ested field regimens
Drug regimens must be effective. They shoulrl also be as sj.mple and as superovisable as possible, acceptable to patients, and relatively non-toxic and cheap.
In LL and BL leprosy there should be an initial intensive phase of c~bined chemotherapy.
Anti-leprosy treatment should not be altered or interrupted should a Patient develop a reaction (see: Working Paper on Treatment of Lepra Reactions in the Field).
Dr Waters presented the regimens recommended for the newly discovered oases without previous treatment and the dapsone resistant casps reoOllllllended by the workshop on epidemiology and control including neld therapy, the XI International Leprosy Congress held in Mexico r.t tv, Nove.ber 1978, shown in Annex 2 with his detailed explanat1.on on the .ft'1cient use of these regimens.
The choice of the second drug used in the initial phase will depp.nd 0"
a nUNber of factors, including skin colour (for clofazimine), live,. toxicity (for ethionamide and rifampicin), cost, culture, and incidence of other disease in the control area. It must be remembered that both rifampicin and ethionamide can cause liver damage, and speCial car .. should be taken to check liver function dUl"ing the first weeks of combined therapy with these two drugs.
Pre-programme studj.es of a new c!rug, particularly clofazimine and ethionamide, for acceptability by the patient and tOXicity should be oarried out in each country before the drug is introduced generally.
All suggested regimens for dapsone-resistant leprosy In Annex 2 are lIIoderately priced or very expensive. Therefore, possiblE'! "low-cost" regllllens which could undergo clinical trials are:
(a) Rifampicin 1500 mg, single dose on the first day of treatment, plus clofazlllline 100 mg daily for two months, then 100 mg three times weekly, indefinitely and ethionamide 375 mg daily for two months, then thiacetazone 150 mg daily, indefinitely.
(b) Rifampicin 600 mg daily for two weeks, then 600 mg on the first day of each month, indefinitely, plus et.hionamide 375 mg daily for two lIonths, then thiacetazone 150 mg daily indefinitely.
(c) Clofaztmine 100 mg daily for two months, then 100 mg three times weekly, indefinitely, plus ethionamide 375 mg daily for two months, then thiacetazone 150 mg daily, indefinitely.
- 22 -
10.5 Duration of therapy
More research is needed on the duration of treatment in non-lepromatous leprosy. It is proposed here to give simple recommendations, based on the date of commencement of treatment, or of ~ecommencement in the casp. of relapse through faUure to take treatment, or of change to effective treatment in the case of relRpse due to the emergence of dapsone resistance.
Type of leprosy
Duration of chemotherapy
Period of intensive follow-up (hecause of threat of reaction, etc.)
TT BT BB BL I.L
3 years 5 years
10 years 15 vears
At least 20 years ( li fe pre fer red )
0-3 months 0-4 lIIonths 0-6 months 0-12 months 0-1 years (subsequently, an annual complete check for relapse remai.ns essential, indefinitely
Indeterminate - treat for three years, and t.hen lepromin-test.
(a) tf lepromin postti.ve, stop at three years;
(b) if lepromin negative, continue for another three years (Le. total of Si_x years).
Discussion
It was mentioned that the Working Group should qualify its recommendations by saying that the regimens suggested must be ahle to be carried out thoroughly; otherwise, simpler but less effective alternatives may have to be used.
It was agreed that for practical purposes the recommendation of the XI International Leprosy r,on~ .. ess concerning chemother~py would be used for the Working Group's recommendation on the drug regimen in treatment of the disease (see Annex 2).
In general, only one or at most two regimens should be employed in a single control area in order to avoid unnecessary confusion among field workers in the selection of regimens.
A number of participants focused on the need of urine testing for dapsone, and qualtty control of smears in order to assess regularity of treament. New techniques for the testing for dapsone in urine have been developed that are good enough to suit this reQuirement. 1 It should be kept in mind when the drug regimen is selected that with no other drug bacterial resistance develops so quickly as with rifampicin.
lWPR/PWG/LepI18.4, p. 3.

- 23 -
A participant referred to the new problp.m of training both lp.prosy workers and patients in the treatment of leprosy with the new regim~ns of combined therapy.
11. METHODS AIMED AT DETERMINING THE EXTENT OF DAPSONE RESISTANr.E
Dr R.S. Guinto referred to the increasing number of sulfone-I"eslstant leprosy infections. Leprosy control is based entirely on chemotherapy with dapsone, and dapsone-resistant leprosy patients will require long-term treatment with expensive alternative drugs (rifampicin, clorazimine).
Primary dapsone resistance ts now a distinct possibiHty on a hrge soale in the near future. The problem can however be overemphasized and thus give rise to unnecessary fear.
Dr Guinto presented on the follOWing table showing the results or mouse footpad innoculation for secondary dapsone resistance in 30 relapsed oases with LL and BL leprosy.
Table
Summary of Thel"apy Histories, 30 relapsed cases
A. Dapsone-resistant relapses
Number of cases observed ........................... 26
Relapses, after therapy was stopped ..•.•............ 10
Relapses, during dapsone therapv ........••.•.••.•...•.•. 16
History, low dose and irregular t.herapy ....••.•••••• 26
Duration, from initial dapsone therapy to relapse
B. Dapsone-sensitive relapses
8 - 28 (average 18.7 yrs)
Number of cases observed •.....•.••..••.•.•••.•••.•.•• 4
Relapses, after therapy was stopped •.•.....•.•.•..•.. 4
Relapses, during dapsone therapy ..................... History, low dose and irregular therapy............. 4
Duration, from initial dapsone therapy to relapse ..............••..••••••.•...•••••••.••.• 7 - 20 Y1"S
(average 14.5 yrs)

- 24 -
Discussion
As stated by a part i .c1pant rlapsonf'! resistance must he dtagnosed mal.nlv by clinical mf'!ans b~cause of the difricultif'!s and f'!XpenSAS involvAd In thf'!' footplld 1nnocll1l1t1O'1. The ~linl.cal and b=ict,f'!riologic'i] "elliPses of LL 'ind LB cases on dapsone treatment could be used as in~icators or dllpsone resistance, and if no improvement is observed riuF'ing thF'ee to si.x months of supervtl'leri and conti.nuous dapsone therapy the clin:l.cal diagnosi.s of dapsoM resistance may be conftrmed. Bacterotological 1.ndex may help 1.n IISSl'!ssm"!nt of p"ogress of the (li.sease.
T.,eF'e was mention of the :I.mporhnce of knowing the magnitut1e of the dapsone !"eststancej attempts should be ma~e to estimate its prevalence.
Analysi'lg the correl"ltlon between thp. dillgnosis of r1ap!'lont'! resi.stance by clinical and mousp. footpad mAthods was suggp.steri, as clinical trials alt)ne may mis .. ~ eal"ly cases or cases of low or i.ntermediate r1l1psonf'! 1"t!sistanc~.
12. MANAGEMF;NT OF LEPRA REACTION T.N 'l'HF.: FIELD
12.1 Introduction
Dr WatArs started hots p"esf'!ntation by clearly riefi.ning and separating the two ma1.n types of lepra reaction: The e"ythema nodosum leprosum (Ti:NL) or 1 epromatous lepra reaction, and the reversal "eacti on (noT\-lepl"omatous or borderline 1~pra reacti.on).
The pl"acti ce of stoppi.ng dapsone during reactions "IrOse :!loon after the introduction of sulphone therapy when it was found that chronic ~NL gradually subsided when sulohones were "rested".
The tr!1.dition also a"ose that E~L was helpe!ri bv cuttin.a; the rll!.pMne dosage, although tl-tis hlid not been conf1.rmed in any double-blind contl"olled trial, and the recent study makes it theoretically most unlikeJ.v. Moreover, dapsone has no effect on ENL1 'I dapsone-resistant p"ltienti'! (Waters and Helmy, 1974), confirming that its FoNL-producing "Ictt vity 1.11 rellltet1 to its bacteri.cidal effect. In fact, any drug which results in death of ~. lepl"ae may precipitate Em.. The high dosage clor~zimine has an anti-inflammatl')rv ann therefore ENL-suppressive erfect. ""e shol"t-tt'!l"m benefit from stoppt1"\g treatment is grelltly outweighed by the lon~-term disadvant"lges, ~spectally the overall prolongation of E~ an~ the incl"eased tncidence of rirug l"esistance.

- 25 -
12.2 SUllested field treatment regimens for reactions
~. Treatment of ENL
(1) Mild ENL, wMch clln bp. treated in the fielli, coni'li.i'lts or mUr! to moderate crops of ENL papules, with no more than mild fever anli malaise: nerves are not painful but may be slightly enlarged and tender, and voluntary muscle testing (VMT) reveals no increase in nerve dama~e.
(i) The antileprosy trAatment is conti.nued unchanged.
(t1) If there is any ne .. ve tenderness, rest the affecteli Hmb (s) •
(Ht) Give analges1.cs, either aspirin or paracetamol, as requi ... eti.
(iv) Give stibophen (Fouadin) by intramuscular lnjection, eVher 2-3 m' daily tor four to seven davs or 5 ml everv two to three davs fo.. ~h"ep or tour injeotions. The course may be repeated once after a week's rest: thereafter courses may be repeated after a fulJ two weeks' rest.
(v) The patient should be seen regularly, at least every two wee~s. In particular, the eyes shoulli 1)e checked at each visit to enl'lure that the patient is not developing iridocyclitii'l.
(2) Severe Em.. ENL is graded severe if there is hi.gh fever and severe general malaise, or if moderate fever lasts more than four weeks: if the papules ~come pustular and/or ulcerate, or if they coalesce to form I\ard tender sheets in the ski.n; tf the lymphnodes become very tende", and enlarged: if the nerves become painful or if there is any loss of nerve funotion; if there is any iridocyclitis, orchitis or joint swelling, or if urine ex~minations reveal·persistent albuminuria with red cells present on miorosoopy.
Tr.eatment of severe ENL must be commenced in hospital. Therefore:
(1) The patient is referred jmmediately to hospital, especially if the eyes, testis or nerves are involved.
(Ii) The anttleprosy treatment is continued unchanged.
It is suggested that a short-term course of prednisolone shoulli be first given:
prednisolone 10 mg three times a day for one week, the~ prednisolone 10 mg twice daily for one week, then prednisolone 10 mg daily for one week, then prednisolone, 5 mg daily for one week.
- 26 -
Tf thp. patient's skin lestons immedia!;131y I"p.lapse, 0'" jf F'NL iridocyclitis, orch l t 4 s, neuritis, arthriti.s ar nephrttts i~ nat camplpt~ly cured in a single course, t,hen Alternative OT'lII1;S should be emplovetl. POBsI.blp. CO'lT'SeS are:
either thalidomioe 200 mg twice dailv for three oavs, then thaUdomide 100 mg mane, 200 mg nocte for fnur OAV"I, t~en thalidomide 200 mg nocte for t.wo weeks, then thaHdami ne 200 mg nocte fol" eight weeks. (Do not give prednisolone wHh thal1tlomide).
Or clofaztmine 100 mg three times a day Por two months, then clofazimine 100 mg twice daily for one month, then clofaztmine 100 mg daily indef.'initely. Plus pl"erl'1isalone 10 mg twice daily for the rtrst two weeks, then prednisolone 10 mg once daily for the next two we~ks, t~en preclnisolone C; mg daily for the third two weeks (thf'ln stop
prF!dn i sol one) .
Pati. ents should be rF!vie\oled around eip;ht weeks bv the cnnt1"ol scheme lepl"osy speci ."llist. At his oiscretion, patients may be discharged i10me on clofazi.mi ne, subject to rev!.ew every thl"ee months. Out pat I. ent use of tha li.dom' d<>, '11 though bv and la1"ge cheap, simnle and ve"'y satisfa<'!tory, must be unrler tI-Je di"ect cont"'ol of the speCialist, 'In<l sUb.lect to any rep;u1aUn'1s i"1posed hy the nat; onal he<llth aut.ho .. i tv. Re/l:ulA1" ch"!cks I'll'''!
advis"lblp to qxclurle th"lidomlde neuropathy.
B. Treatment of reversal reactions
(1) !'Aild reactions consist of swe 1 U11g R"rl "'ertness of 0 1 -1 ,ski.n lesions ',JHh or without the appearance of new lesions, an<1/or some tenderness witl-Jout pain or loss of funcUon.
(;. ) The antUep1"osy treatment is continued unc"lanp:el"j.
(ii) Give analgesics, either aspi .. in 01" paracetamol, as "'equiretl
(i i i.) If there is ne!"ve tenderness, rest the affecte'" limb
(i v) The panent is seen at least every two weeks, 'lnr! asked to return at once if the reaction becomes more severe.
(2) Severe reversal reactions. Reacti.ons are grarled severe i.f.' there i.s marked feve .. and malaise, if there i.s oedema of hands I'lnd/or feet; if the skin 1pslons (threaten to) ulcerate, and/or if theroe is nerove p'!.i.n and tenderness or loss of nerve function, or if a mild rection last,'! fo1" more than six weeks without subsiding.
(U 'l'he patient. must be referred i.mmedtatelv to hospi.tal.
(ii) rontinue the antilep1"osy treatment unchanged.

- 27 -
In hospital:
(i) Rest painful nerve(s), splint".n,,; the I\ffectAd '''.mh(s) if' nseessary.
(11) Give prednisolone. Patients will v"try ~.n their -qllirementl'l, and a suggested average course is:
Weeks 1 and 2, prednisolone 10 mg, t"ree times a ~av; Weeks 3 and 4, prednisolone 15 mg mane, 10 mg nocte: Weeks 5 to 8, prednisolone 10 m~ twice ~aily; Weeks 9 to 16, prednisolone 10 mg daUv; Weeks 17 to 24, prednisolone 5 mg ~aHv:
Provi~ed that patients can be seen monthly hy a docto~, anrl have made a Sood response to therapy, they may be discharged home I\t Ilbout the end of th, seoond month, if necessary on a small dose of prednisolone, w.,ic" should be continued until the ~action subsides.
C. Treatment of down,rading reactions
These are seldom severe. However, if t"ere is marke1 lntla.matlon of the skin or undoubted nerve tenderness, a short course or pre~nisolone may be given, commencin~ on the dav befo~e or on the l'Illme dav as dapsone treatment. A possible course is:
prednisolone 10 rng twice daily for 2 days, then prednisolone 5 mg three times Il day f'or 3 days, then prednisolone 5 mg twice daily for 4 days, then prednisolone 5 mp; once daily for 5 ~ays,
D. Treatment of Lucio's phenomenon
This is relativelY a local proMem. Little has been ~itten oonoerning the use of either thalidomide 01" clofazimine. For the prellent, the two main points appear to be:
(i) commence antileprosy treatment with dapsone and a second antileprosy drug (rifampicin, clofazimine, ethionamide or prothionamide) ;
(i 1.) control the reaction with prednisolone for as long as is necessary.
12.3 Imellcatlons
The treatment of reactions, espeCially ENL oQIIIPl1oated and requires skill and experi.ence. outline here require:
and reversal, is therefore The sohemes of treatment
(1) dl~os1s reaotions
Better training of both doctors and other health workers in the and dlfferential diagnosis of reactions, in the anticipation or and of their complications, and in their treatment.

- 28 -
(;.1.) A specilili_zed referral centre for severe re!lction pati_ent,~ to hp attached to every control ~cheme. Such a centre should he 9taff",d by a leprolop,J.~t possessing the necessary rlrugs Ctncludinp; steroirls anrl clofazimine and/or thalidomide), tratni_np; (inclurlinp; tr'li.ninp, ion t,l1e use 0"
these rlrugs) anrl equipment. ~~e system of selection and referral of pl!tients to the centre should he well o"p;anized and care"ullv taup;~t to t.he neld workers.
(11i) Where traini.ng cannot be provided on a national h!lSiS, tt is recommended that WHO shoulrl help in the upgrading of t~e specialty of leprosy by prov:!_din~ regional traininll; in the treatment, of reacHon~. A detailed set of instructions, simi tar to that provtded by all Afrioa Leprosy and llehl!bUitation Training Centre, Ethj.opia or Us tr8 inee dootor~ (Pearson and Wheate, 1976) but giving more dl!tails of t.he 'lse (')f olofazimtne and of thalidomirle would be of gl"eat value to leor(')logists and should provide lI;uidance to national m1nistri.es of heAlth on the u~e of thalidomide in hospital and under field conditions.
12.4 Use of thalidomide
Most of the countries/areas in the Rep;ion orohthi,t thf'! manufactUrer and importation of thAlidomide because of l.ts posslblf! teratogf'!nlotty. Or NoussttOlJ warnf!d t"at once t.,is rlrug is introduoerl fC)r use in t'1l1! nelli, many patients become addicted to the drug and want to hke only thalidomide, givinll; up taking rlapsone.
There is I! mention in t,"e fi fth report of t"e WHO Expert r.ommittee on Leprosy as follows:
"For drllg sa fet y reA~ons WliO does not ass ist countries or proll;r!ll-"I111"~ in the purchase of thl!ltdomide. ResponsibUi ty for the use of the drup; must rest wi th prOIl;T'amme manap;er or hospital doctor. ~a HrJomide should b,. given to patiflnts only after they have been fully 'informed Ahout its possihle teratogenioity".
13. CllRRIr:ULA PREPARATION "'OR ~llATN,[N() AND TEACHING PERSONNEL
Dr D.A. Russell analysed t.he various fl!otors that hAve a bearing on the failure of control programmes: paHent factors U rregularHy of treatment), geographical factors (pOOT' communications, isol'lted unsupervised areas), chemotherapy factors (intolerance, drug resistance)
Leprosy is basically a rural disease and most oountries havetorfepend on t"e skills and services of auxiliary personnel.
Before p,oing into detaUs of the precise curricula of tra:!.ning it would be advisable to define some of the needs that would require more_ attenti.on and also to decide on the teaching materi.al and the level of workers to be trained.
- 29 -
Areas that require special attention are:
(~) b~810 leprosy information for village level worke~s,
(b) supervislo~,
(0) pro~~amme management ann evaluation,
(d) laboratory technology,
(e) suitable publications that prov~dp ongoi~g information ror leprosy workers.
With respect to p1'aotical teaching (lemon~trations i.n the cl1.n1.o Ilnl! the n.ell!. teaching mat'3l"ial is av"! nable in the form of'hanl!books, textbooks, oosters, pamphlets, oolour transparl!noil!S, fUms Ilncl .1ou""I\.1:'1.
App!'Oprlate syllabi w1.] 1 have to be deslgnet1 to ~each the level of' peJOaon to be taught, e.p;. general public, patient, various ll!veli'l of auxUtary medical field worker, sophistioated metiioallv-tr'!inet4 personnel, s\lCh 1115 doctorA, nurses, laboratory techntci ans Ilnl! eventlJalJ. v speoiali sts who 1n tum will be !"espons1.ble for teliChin~ and tl"atning.
The basic oontent of teaching should el'lhl"aoe Rnd stress the f'011ow1nll::
(a) support and sympathy ror the plltient,
(b) the keeping of prope~ records,
(c) the recognition of' early SvmptolllS of leproAv,
(d) the need to seek medi.cal advice at the elll"l1p.st opportun1.ty,
(e) the 01inica1 diagnosis and 01assifiollt1 on or the diseas'3,
(r) the treatment of leprosy,
(g) the takinp; of skin I'lmears and the interpretation of ~kin smears,
(h) the recognition and management of the oomplic.tions of leprosy suah as react1.on (Em.. and Reversal),
(i) the awareness of tt}e danger of DRTJr. l!E~I!3'1'A~r." ant! the ~ill:ns to look for to recognize this complication,
C1} the Qar'e of the hands and feet anr! the prevenUon ()f comp,i.cati.on due to nerve involvement and injury.
- 30 -
14. EVALUATION OF LEPRO~Y rO~"R()L P~O()RAMMP:<;
DI" Noul'Isl t(')u ref~l"l"ed t(') t,he 1mportanc~ or perl orlll' P.V~111::tt,1 on 1 n leprosy control progl"amm~s. He stresl!lfld the need for q'1::tnt1 ri.n~tl nn nf' targets, but to do so basl!l1.ne rlata must be taken into ::tonount ..
The collecti.on nr accurate data may not ",l.ways he DM~ibln anc1 rl\nrlom sample sUl"veys may have to be organized. JO.:ven thoup;h they Rrf'! expp.ni'l~. ve, periol:lic (every 5 to 10 years) epidemiological. su"vevs w1ll he the ""lat measu .. e to evaluate c(')ntrol programmes.
As operational and epidem1.ological indicators thos" p;1.v"n 1.n t,h~ report or the WHO Expert rommittee on leprosy (1977) are recnmmenrl"lrl ::Inr! the same are listed bel(')w:
Operational inrll.natol"s
Case-rinding
- Covel"age !"ate: '!'he proportion of the nopulat ion reacheti bv case-rindlng activities
- netect.i.on .. ate: Tnten:'lttv of case-r1.nrli.np; wH.hin t,hl.:'l sE\~f!nt, nf' the popul::ttinn in a given pel"iod or ti.me (usuallv onp. "eal")
It .1.1'1 us~ful to compare the y1elrl or different Cl\sp.-,.l.nd1.M metl1orll'l employed.
- DtsablHtv rate among ne\~ cases: Pel"mits an inriirect ::tI'lS "!slImen t, of' the delay in ctetecting the rl1.sease by provtdl.np; a measul"e 0" t,I1A number or old cases that have escaped case-finding service
- Proportion of cases wi.t11 si.ngle lesions: Among; the new.1.y rletecterl cases of tubel"culoirl leprosy. provirles an i.mportant ind1.~::tt,i "n of earlv detect,;. on.
- The p"'nporti.on of' lepromatous cases amonp; the total nllrt1hf'!'" nr CllS"''l
detected: During the fi.rst years of control acti.viti.es tl1i.s p"opol"t,.1.on is generally l1igh and tl1en gradually declines.
Treatment
- treatment cove"::tge: Tt should aoproac'" 100~. All lIcttVP. c~ses should be loc~ted and signed on at a treatment ~entre.
- Treatment attenctance: Refers to the percenta~e of treatment sessi.ons attended by the patient in one veal".
- The annual treatment defaulting !"ate: 1ndicates the numher of' patients who default from treatment each year in relation to the number of patients under treatment.
- 31 -
- The dose administered as percenta~e of the dose prescribed: ProVIdes an indication of the efficiency of' treatment activUi~s.
- The annual inactivation rate: Refers to the number of treateo patients who beoome 011nioa11y inactive eaoh year.
- The annual bacteriologically conversion-to-negative rate: Rerlects the proportion of baoterI010gically positive oases who have become bacterio10gioa1ly negative during the year.
- The annual relapse rate: Refers to the proportton of cases who present reaotivation among the inactive oases under su~vei11ance during the
. year.
BpideaI010gical Indioators
I.noidenoe: The number of new cases ocourri~ during Ii givl9n pertod (Ie"erally one year) in relation to the population. "'''h1.s i.s the only index tor measl.lring the efrioaoy of the meal'lures taken, Le. ~edlJction ot transmission".
lnoidenoe rates for ohildren: This indioator is of p,;l"f!at ~pit1emfolop:1.CI11 silftttloance as it indicates transmission of the disease.
Prevalenoe: Changes in prevalenoe are onlv indirectly indicattve of' thp. tapaot of the programme on the epidemiologioa1 situation. However, prevalence is needed for planning and organizational purposes.
Disoussion
Dr Noussitou said that the examination of contacts is essential and this can be done when the index case is diagnosed; later on programmes should conoentrate on the examination of contacts or hacterjologic~lly positive leproasatous cases. Lons-term examination of household contacts of' all registered cases ts not praoticable. Several partic1.pants a~reed with Dr Noussitou's sussestion.
Epidemiological survey among population ~ives useful information of the size of problems and repeated survey shows the impact of the programme on the leprosy problems. However, for the oountries with the prevalence of lesathan 10 per thousand, the large number of study population is required. Usually the repeated surveys do not show the significant difference owing to insuffioient size of study population. Anot.her diffioulty was the deoreasing trend of cooperation from the population. Therefore, the expeoted prevalence from the survey, cooperation from the popuation and expeoted change in the prevalenoe and t~e inte~val b~tw~en
two' surveys in case of repeated survey should be carefully taken into oonsideration when the survey is planned. It was suggested that survey should be conoentrated among the population in the hyperendemic area.

- 32 -
1'he Sll!"vey FJ.mong schoolchildren is easy to orp;antze and ft,iVf'S v"l1'lllh'''' lndex of the eptdemiolo/l:ical situFJ.ti,on iT' the community hut ('''In h" mi.slellrling as t.hi.s does not give i.nf'orm"ltion "Imong t" .. oth",.. .1F'." r:"('I'ln!'l. Tt ts expectf'ri thllt I;he serolop.:;rFJ.l test t.o rli"lp'1o!'le !'Illh!:!1;"i",,1 (>11"'''' would be de'felopeti.
In developing a management i.nformation system, a distinction shou'rib~ mAde between data which are rAW statements of facts and ~nf'ormatton whirh is data recorCied'- clllssified, processed, organized and I"'elated within context to convey meanin~.
utn i~at1 on 1.s the potnt of neparturE! for i.nfo!'mat.ton Rvst.~m
development. Information system provides ri~t i,nformatton to t."~ ri.ght per-son Ilt the right time in r1.p;ht form. The effectivene!ls anrleft't~lencv or the tnformlltton system depends on how far the system is used ann us~r-o"5.ent.~d. AIRO, i.t 5s 'mtir~ly dependent on the mllnall,ertl'l' !'It.v'" of programme m'lnFJ.p.:nme"t.
nata utilitv 1S both !'Ipace and Hme-1ependent. Tn the Ilhsel'l!:!p of l\
mf>.chan1 sm for dynllmi.sm in the svst.em, t.he present sit.uat.i.on l.S generFJ.ll.v such that there 1.s scarcity of relevant inf'ormR.tton but r.>verllbllndllnllp. ,.,r i rre levant O'1es.
The dat.a bllRe of' the information system contains "11\ data .. l.empnts as inputs t.o yip-l.r! i.'1formation as outputs to suppo,..t deci"lio,,-m"lktnl!; functil'll'ls for action. "'he actual process of transmutati.on in convert.ing ti"l.tll to information anr! t~chnologtcal support in terms of COIllP'Jte"'s to support thl.!'I proces.'3 are necp.:'l:'lary components of the i.nformat. 'ton svstem to he stllrlierl. Howev!!r, the primary conc!!rn in development of an inf'orm"ltton svstem 1'II,l'Iu11 be on "content" of' thp. system.
Inforlll"l.ti.on relevant to leprosy programme can he oatell:ortzerl llS technical, t!!chnirlll-support and management i.nformation. ~ven management information ha"l two aspects - those related to individual patt~mt management and those concerned with service management. to1hUe inrl1.vidual patient management informati.on is critical for service personnp.l, prograllllle managers are concerned with service or programme management infol"'ml!tion. A good proport.ion of' prop:ramm'3 management i'1fo"matton nep.rierl 1'01'" plal'ln1.I'Ip;, management cont"'ol and operational control can be obtained t.hrou/!:h perll'ld1.o reports based on patient management informat.ion usually containerl as rlata items in pattent ""ecords. Other relevant information can be obtainer! 1'l"om other sources - census, surveys, vital registration - or t"rough sp'!!cia'. extract1.on of data contained in the patient records. Since scarce 'IIal'lpower resources are neeried for Q;eneration of data and preparat.ion of routtne reports, every effort should be marle to reduce t"is 1I'1format~.on-""elaterl load on the health personnel.

- 47 -
ANNF.X 3
AGENDA
Thursday, 7 Decembe~
0830 - 0930 Opening ceremony
- Registration - Opening remarks by the Regional Director
0930 - 0945 Coffee break
0945 - 1100 Review of the reg.i.onlll leprosy oontrol prol':ramme - Dr ~. F.ndo
1100 - 1200 Reoommendations of the reoent international leprosy workshops in Asla sponsoreri by the Sasawaka Memorial Health Foundati.on -Dr Y. Yuasa .
1200 - 1330 Lunoh break
1330 - 1600 Analysis of ongoinll; leprosy ,control activities 1.n the oountries:
~lday, 8 December
Dr Do II Kim (Republic of Korea) Dr Fernando .Tose. .Jr (Phi Ii. ppines) Dr Le Kinh Tlue (Socialist Republic of Viet Nam) Dr Lim Kuan~ Joo (Malavsia) Dr D.A. Russell (for Papua New Guinea) Dr R. Farrugia (New Caledonia) Dr L. Lopez-Bravo (for the South Pacific) Dr W.R. Lang (New Zealand) Dr E. Karuru (Fiji)
0830 - 1000 Suggestions and proposals to improve the effioiency of J.eprosv control aotivities according t~ the main prob1ems areas in each country - Dr F.M. Noussitou
1000 - 1015
1015 _ 1200
1200 - 1330
1330 - 1415
Coffee break
Integration of leprosy control aotivities into the general health services and prel1rdnary evaluation of results -Dr F.M. Noussitou
Lunoh break
Introduotion of health planning process - Dr R.D. ~ercado. Director, Health Services Development and Planni.ng

- 48 -
Annex 3
Saturd~y, 9 December
1415 lIiOO
0830 - 1000
1000 - 1015
1015 - 2000
P"'op:"'a!l\llle planninll "lnd ev"lll~t ion 0" 1 "'PI'O:'IV ()ontl'o 1. -Dr .J. W"llter
TentatIve model for R. merHllm-tp.l'm pr-op;raJl!ll'llt'! I" leDl'osy contl"ol (1979-,Q83) in the We~tel"n Pacific RegIon (bv countrv) - Part T -Dr P.M. Noussitou
r.of"ee break
T~ntative model for ~ medium-term pl'O(framme 1" lepl"osv oont.ro1 (1979-1983) in the Western Pacific Region (bv countrY) - Part TI - l)r P.M. Noussitou - Dr L. Lopez-Bravo
Afternoon - F r e e
Sunday, 10 Decemher Free day
Monday, 11 December A
0830 - 1000 -:stimatFld atidHtonal l"eBources requireti by Muntries in t'1e Western Pactf1.c Region and suggesteti 'l11ocllUon to t"" diffel"ent component.~ of thetr respective medi.um-termleDI"osy control programme (1979-1983) - Dr ~. Endo
1000 - 1015 Coffee break
1015 - 1200 TherFlpelltic regimens recommended IiCcorMng to t"e cl tnical· clR.sst flcation and bacteriologic condition or casp.s. Prevention ~nr1 treatment of dapsone l"ei'l~.l'It.ance - 1\1" M. F. R. Watel"s
1200 - 1330 Lunc" break
1330 - 1430 Hethods aimed at determininp; the extent of dapsone-l"es1,stanoe -Dr R.S. Guinto
1430 - 1445 Coffee break
1445 - 1660 ~anagement of lepra ~actions in the rt~l~ - Dr ~.F.R. W~ters
Tuesd~y! 12 December
0830 - 1000
1000 - 1015
CU"'I";cula for teachin~ and training rlel~ personnel 1.n leprosy control - Dr D.A. Russell
Coffee break

- 49/50 -
Annex 3
1015 - 1200 Management information 1n leprosy control programmes -Mr M. Subramanian
1200 - 1330 Lunch break
1330 - 1500 Evaluation of leprosy oontrol progrAmmes - Dr F.M. Noussttou
1500 - 1515 Coffee break
1515 - 1600 Closing session

- 51 -
LIS'!' OF MEMBERS, rONSUL'I'A~'I' AND ~Er.RF.TARTAT
WHO Tempo~ary Advisers/Memners
Dr M.F.R. Waters MedIcal Institute ~or Medical Resea~ch The Ridgeway, Mn 1 Hill J~ondon , NW7 1 AA England
Dr Y. YUIlsa Medical Director Sasal(l\wl\ Memortlll Health Found1\ti.on Sabokaikan Bldg. 2-7-5 Hiral(1\wa-cho, r:h1.VOOl'l-ku Tokyo 102 Japan
Dr Ricardo S. Guinto Leonard Wood Memorial FoundatIon Cenu Skin 1"·11.nlc Cebu City Pbi lippinp.s
Dr W.R. Lanp; (Rapporteur) Senior PhysiCian Infectious Diseases nepartment Auckland Hospital Park Road, Grarton Auckland 1 New Zealand
Dr D. A. Russell Regional Medioal Adviser for South-East Asia The Leprosy Mission 22 Ijong Street Kenmore, Queensland 4069 Australia
Dr 1!:nele Karuru Med10al Superintendent P.J. Twomp.v Memorial Hospital Tamavu!\ Suva FrJf Dr Lim Kuan Joo Deputy Director National Leprosy r.ontrol Centre Sungei Buloh, Selangor Malaysia
ANNEX 4

Anne:< 4
r.onsultant
Secretariat
Dr R. Fl'Il'rugia Medecin
- 52 -
r.entrA Raoul Fol tel'eau Noumea Nouve Ue-r.aIedonie
1)1' Fernan(jo A. Jose, Jr. (rhail"lllan) Offt cP.-t n-charge Leprosv r.ontrol ~ervioe D1 vision of lH.!l8Ilse ~ontrol Bureau of Health and Medill'!l c;e"vioe!l Ministry of Helllth ManUIl P~il1.PPlnf!S
Dr 00-11 Kim (r.o-ohai~an) Di.rector Korpan Lp~rosy tnst1.tlJte Anvang P.O. Box 27 ~n 87, 0.1eon-r1, EUlAnp; I!\vun Sihung_gun, f{veonMi-do Republic of Korell
Dr Le l(inh Du'! Dtl'ecteur fiu Department Central "'e Dermato-venerolol':ie de l'Hoplta.1. Bach MIli Hanoi RepubHque soohl1ste du Viet: Nam
Mr Nguyen Quang Hoanh Ministere de 1a Sante llanoi iieiiii'blique socillltste du Vi"!t Na,,!
Dr Fernando M. NoussUou Callao 1829 Buenos Aires ArgenUna
Dr J. l4al tel" Medical Officer, Leprosv Ul'\it '. Division of COIIIIIIuntcahle Dise1'lses WHO Headquarters Geneva Swttze!"land
. ,

- 53/<;11 -
Dr Shotcht En<1o llep;;. ona 1. Anv i 3131" on r:hrol1 1 c ami Degenerattve THsAal'les WHO Reglonal ornce for the WAstern PliC 1. ftc Manil<l
Mr M. Subramanian Re~ional Advi.sl'lr on Hea lth 1:l'Iforlftat ion WHO Regi.onal OUlce for t.he Western Paci nc Manila
Dr Lliis Lopez-B1"llvo Medical. OfncA"/Leprolo~iet Int.ercDul'lt1"Y project, T~P/Bvn/005
Suva Fm
Annex II
- 5~/56 -
ANNEX r;
WORI<ING PAPEM
WPR/WO/LEPI78.2 - Progrl!.mme Planning an(1 IO;vl!.lllati.l)n ""1" I,ftpl"OSV I'l)nt 1"0 1 , Dr J. Walte ..
WPR/WG/LEPI78.3 Mana~fI",ent of' Le!'lra Reaotion 1.n t."fII F1.",'<1, Dr M.F.R. Watel""
WPR/WG/LEPI78.4 - F1.eld '1'heraJ'!V of I.eprosy, DI" N.F.~. W"tftrs
WPJt/WO/LEPI78.5 - Rftv1.ew of WHO Re~1.on"l Pl"op:rlllllllle on Leprosv, n" ~. "ndo ..-..... WPR/WG/LEP.78.6 - S~e8t1ons I!.nd Proposals to :T.lllprove ttlft P,f'f'i.c:!hnoy of
I.eprosy Contl"ol Activttif1!8 Aooort1i.n~ to Mlltn Prohlem Al"eas (By country', n" F.M. NI)uss1tou
WPRIWO/LEPI78.7 - Leprosy Cont!"ol tn the SOll".1'1 Paotrtc, [\1" L. l,oPft2l.Rl"avo
WPR/WG/LEPI78.8 - Leprosy Inform!\tl.on ~:vstA"', Nr M. ~ubrRmanhn
WPR/WG/LEPI78.9 - Introduction to I'·he Plann1"1I: P"ooeslI, n,. Fl. n. HerMcio
WPR/WG/LEPI78.10 - rUl"r1.o111.al" PI"eoAr!lHon fo .. TrI'l1.n1np: ant! '!'flA(!1o)1n~ P"I"sonnel, DI" n.A. ~USi"ll'!n
..
- 57 -
A"1"1P.Y. 6
REFERE~r,!=.:S
1. r.ulnto, R.S. et '11 (1978) Study of' t.~e Drey",l~n(')p. 'Inri 1'1il':"l1 f'i(,)'lnt, characteristics of Sulfone-rf>!'istant leoroy i.1'l Cebll, Phi.! tpptn'l1'1 (unpubl i shed docum'lnt).
2, Jlussell, D.A. (1978) Proposals for Operati.onal ReMllrch and-or epidemiologi.cal research (unDubl ;sl-)en documElnt.)
3. ~asllkawa Memoria.! He'llth Foundation (1976) Report on the First tnternati.onal Workshop on Trai.ni.nr, of Leprosv "'orke"s in Asi'l, Bangkok, and Patt'Iya, Thailand.
II. Sasa1<awa Memorial Health Foundation (1977) Report on the First Int.ernati.onal \·rorkshop on r,hemotherapv of' L",prosy tn As!.a, Manila, Philippine'!.
5. Sasakawa Memorial Hea1t~ Foundation (1977) Report on the First International Workshop on Leprosy Control i.n Asi'!., Jak'Irt'3., T"1oo"1e3ia.
6. Waters, M.F.R. (1976) ~hemotheraDeuttc Problems 1n Leprosv Control Programmes, (preparatory paper for the Expert r,ommittee on Leprosy, GenflVa 1976), LRP Il~P 17f.. 10.
7. WHO, A Gulde to Leprosy Control (1973), LEPI73.1.
8. WHO Expert Committee on Leprosy, Fourth Report (1C)70), WId. Inth. Org. Techn. Rep. Ser. No. 459.
9. WHO Rxpert CommUtee on Leprosy, I"Hth 'l~port (1977), ~1Jn. Hlth. Org. Techn. Rep. SeY'. No. 607.
10. WHO 'lepo!"t on the t-l~p.ti.ng on 1'ra1ninp: anti Institution StT'enp;thp.ning for Leprosy Resear(')h (1978), TDR/L8PI78. 1.
11. to/HO Regional Office for the Western Paci nc (1978) PT'Ol!:ramme P!"ofile 4.1.3(4), Lep!"osy .

•
- 33 -
Given that certain i.nformation is nf~erled more rrequentlv, sav on a monthly basis, and other inf'ormatton less frequentlv, ::lay on annual 01" "as they ooour/arise" basis, inf(')rmat ion lI;enerat ~.(')n and transmisl'lion l'Iod"! has to be different.
When inform~t 1.l)n is use<l or \Iser-or1 entert anti i. f' mndl'! of' p;enp.r~ t ; on and transmiss~.on is efficiently ident 1 f'1ed based on t.he f'requency wi th wtlioh they are needer! and p~ ... entatton of il'lr"rmatton e~fecti.vl!!'.y rll'!:'Ii.lI;neri then an extremely valuable information system can exist to sllpport pro8ra~e management functions.
In the case of lepr(')sy prop:ramme manap:emenl:., neerlerl i.nf/)rmatton can l-)"! obtained through:
(a) pfllr.1.odic monthly report based on indivtduaJ. patient cal"t1s;
(b) periotiic (annual)/ad hoc extraction of relevant elata rrom individual patient cards:---
(c) an :I,n(lex carel with criti.cal and H!I11,t.ed patient i.nr(')rl'lati.on.
Based on the above principles, the roUowing sources have been proposed:
- At tl1e service delivery point, ror Dat i p.nt-l'Ianap:p.ment purposp.:'I, there will be "Individual patient carel". In aeltiition, tl1el"e will be a ·oontinuou!9 care register" with relevant dl'lta to monitor 'mel Hnk pattent IIIanagement with service managemAnt. A "monthly report" IJsing th"! oontinuous care register as a basis will be preparerl hy the service delivery point for submiss:l.on to highel" levels.
To supply most of the informatton needed on an RnnlJal b:asis at t"'e national level, this continuous care register itself will be submitted liS
an additional report to the nl'ttional level annuany.
Dooument WPRIWGILEPI78.8 gives Ii rlescripUon or the cont.inuous care register and or t"'e monthly report for~.
- At the national level there will be, tn addition, a case 1.ndex e!lrti with information on age, sex, form of leprosy an<1 disab1.lity and baoiloscopy results as well as geogl't'.phiCRI location of i'.he patient.
It should be emphasized that the contents of these records and rflports are oountry dependent, may vary rrom country to oountry and thus have to be determined at country level.
Dr Lopez-Bravo w:tll test practi.cability of the forms mentione(\ in dooument WPRIWG/Lep/18.8 in the fi.eld condition •

- 34 -
16. RECOMMENnATtoNS
Rri'!lf t"tp. ... 1m rMommencilll;tonl'l l'Iufu~ested by a l'Iu1:l-01)11II'I1 t,t~e of t.l,,, meettnp,.
'1"1-)" pl'lrttc1Mnt.1'I I'lt, the mMtl!'l~ /1~rnd to thll! ro'lnw.!'IR p;8M1'''' ~n~lv~1B of thA ~ttuatlon:
Prop:ramme and planning i!'lclud1.ng manpower fOl"lllllt1l)1'1 in tepl"l)l!Sv Mntrl'lJ
(1) In the countrtf'll'l of the Western Pacific Regton len~av h~1'I h~en recop:nizF!11 9l'1 a rna.1I)!" !)uhHc hell1.l;h p~hlem I'lnd ant1-1epl"0l'lY act1.vlHel'l /11'1' h~ing carl"ied out.
HFlV11'l1l; ana 1 vsp.d the (lve!rall I'FJ8ul ts of l.epl"osy control t!'l the! , asl; 17 yellrs durtng which W~O has been involved it ~ppeal"! I;hFlI; t.he numh'!!!'" of registered C~Sfl.~ repre'!lents onlv 421 (Tahtt' 1Fll nr t.he IIJst1l'lRt.fld tntll.'. I\n<1 this rtgure Is l~ell below t./lrg4t. Some 161 of 1'flp;1.!ltflred oP.S~1'I art st1.11 1nstttlltioMliZf'Jd. r:oneerninp; trFJatmenl; and 1n J)l\rttouta1' rep;u1al" treatment, lilthoup;h dllta al"e dtrrtoutt to obtain, ft l.e obvious thAt regulal"ity of attenda1'lce for treatment p;enel"ally hilS not I"eaohed R~Oe"t.n I'Itan"'l'1rl1l'1.
(2) The p!'ol:llt'!ml'! in lAp"'o~v oontrol " •• fully 1"OMntz.~ _ the l"elattvAly htll:h propor-tion of multi,bao111ary pattent!'! I"epl""enttng " potential "MAI"VOll" fol" oontinued sprear1 of the lii.IIIIUII, e.R •• ,1'1 "t,j1 nv~l" 20 per oent of lepl"omatolls calles 1\1"8 I3hUdren and ~I)un. "dults. Oth,,1" problema .... "., rlirrtoultle~ 1.1'1 aue det.oHon, oOmlllul'I1.oaUt')n pl"ohleml, Axi!!t 1 ng pre,lud ices R~aln!!t leprosy I eta. tn spit., "f thflU dHfi oult 1 "'/1 pl"oP:l"eSII hll/l been marle notahtv tn the 1' .. Her of 1.",d~ V1.r1Ulll l'Il/rr"l"tn~ or pI'ltientl' and thAi.!' fami11.es. It- now !"OmAtna to analvl" ~,hl'l f.lalJMI Of the preSl'lnt unsatisfactory situation. ~elt aauses a"'8 App,,"ent on 8tudv of indi viduRl country rAports /lnd the raot.rindin« of thfl WHO Clonl'luU .. nt. These appl'il!\1" t.o hI'! 1 n the IlI"M.!'I of:
(b) supervi.9ion
(0) dru~s and equipment
(ci) trans port and commun 1 ea t.1 on
(e) physical rehabtlitation
(f) hea lth f'duca tion
(g) leprosy l.nformati.on system and evaluation
(11.) b1.ldil;et1np;.
,
- 35 -
Note:
Many of the impli.ed rteftcienci'!,':! ~re due to insuf'fi.cient p1.;'lnni.l1~ and management. A further complication is the now widely recol!;nized phAnomenl)n of dapsone reststance albeit the extent of this problem is unknown. '!'hA sum of these factors may be expressed in increastng relapse rates.
Following on these considerations the 1"0I"king Group m~kes tl1e following broad recommendations:
(1) Countri.es should consirier developinp; lonp;-term Dro!,:rll.mme plll.nninp: (formulation) with improved management techniqu'!s.
(2) Countries ShOll11 realize that it is eS!genti.al for t;he implementation of programme planning that full attention be given to training involvil1g the rttfferent levels anti catAQ;ories of heaH'" workers.
(3) Priority should also be gi.ven to consideration of ~hm!e ot.hp.r sectors outlined in the list (b) to (h) above.
~ote: -The Group is of the opil1ion that attention to the ahove
reoommendations would go some consit1erablA way tOWBl"tiS achi."!ving morA success than has been the case 111 t;he past; in the treatment 0" the ma.iori.ty of cases of leprosy.
As cOl"ollaries to the above general recommendations the Group adds the following machinery clauses:
(1) Problem identification and quantification
The extent of the leprosy pl"oblem should be stated 5.n terms of numbers and types of patients and any special circumstances bearing on rtifftcult:l.es in delivery of leprosy control measures.
(2) Pl"ogramme planning
A carefully chosen and speCially trained person in pro~ramme planning should assist the programme manager in planning, implementation and evaluation. He need not necessarily be medically-traineti,
3. Leprosy training
Precise job descripttons of health workers involv"!d in leprosy cont.rol including workers at the primary health care level. shou111 be formulated by each country according to Us needs. r.ollntries in which leprosy ts a public health problem should, h'herever possible, have a "ull-time lepl"osy teacher and make the necessary budgetary provisi.ons for such a post. The teacher should be also well versed in teaching methodology.

- 36 -
(4) For the effici_ent training of the heal th worker~ cons1.c1eratton shoulrl bEl givEln to:
Note:
(a) sEllection of tra;_nee~ (b) number of trainees (c) cat,ep;o"ie~ of trainees (d) ba~ic refresher courses (e) duration of teaching tim"'!.
The extent of training activtUes should b"! correlaterl with the healtl, serv.ice development of the country concerned.
(5) Adequate steps should be taken to maintain adequate supervision, bearing in mind that without vigilance and constant supervil!1.on hy a .fielt1 office,., leprosy control >"apilily lieteriorates.
(6) Details of the methods of supervision to be used shoulrl be an integral part of the in1.tial programme planning.
(7) Supervisors should be int~atelv i~volved in control schemes, e.g. t,o thf! "!xtent, that they may be the source of refe'"ence for r 1 e'li workers.
(8) Tran,'lport and travel costs for ~upel"v1.sion should I)e sufrtc1.ently provided.
(9) Estimates of needs for drugs and equipment should be made accurately enough to provide budgetal"Y fOl"ecasts 1"01" at lellst two, and pl"ef'erably flV"! years ahead.
(10) The lO/1:istics and costs of transport and cOllll'lllnicl\t:ton~ shoulrl be Similarly assesl'ed, nottng that bot,h initial and maintenance costs near! to be estim::tteo.
(11) 'T'he resources for physical rehabilitation should be lieterminetj by patients' needs.
(12) 'T'he ~equirements for health education - stafr, literature, teaching flie t Ii ties - should be f'lSt1mated and costs prerH.cted.
(13) '!'he requirements for a silllple but sufficJently comprehp.l'lsi ve leprosy infor'matlon system l'Ihould be determ1.ned and data presented on printing of record and report forms with thetr costs.
(14) Budgetary estimates should also be made for the planning procp.ss itself, 1. e. the tra i_ning of planners and the time needed to train them.
(15) T~e number of referral institutions and their initial and maintenance costs should be documented together with staff requ~rements.

- 37/38 -
(16) Laboratory facilit~es ror bacteriolo~ical exam~nation, determination of dapsone resistance, etc. to~ether with maintenance costs for equipment should be delineated.
(17) Information should be made avaUl'lble concerninp: the size ()f the national budget and expected interface support f .. om such sources as WHO, UNICEF and voluntary organizations, both national and international.
Evaluation
Operational evaluation must be a built-in feature of the initi.al programme planning. The basis for evaluating progress is an improved leprosy information system taking into account the special condttions of the countries of the Region. The outcome of ".hese evaluations requires a careful analysis of the system wUh the i.ntroduction of chanp:es as needed.
Research
The need for more managerial experience in leprosy control was clea .. lv expressed by members of the Working Group. Protocols particularly on operational and epidemiological studies are of p:reat importance. '!'hetr objectives and the expected benefit ror control activities should be stated. Suh,1ect to the avai.labi.Htv of funds, WHO ~hould endelivour to provide technical cooperation in the preparation of protocols and their implementation on a varietv or subjects. These protocols would "lnclude chemotherapeutic invel'ltigations which should be aimed at developing I'Ihorter periods of treatment and the p"evention of drug resistance.
Programme expenditure
Programme expend1.ture shoulrl be determined by each countrv' " accepted priorities. In the majority of countri.es these priori t tes wUl be assessahle in terms of the following:
programme formula t i .. on I'lnd management;
improved training, the results o~ which must reach the peripheral worker and motivate him sufficiently.
Chemotherapy
There is an urgent need to use combined therapy to prevent ~apsone resistance. However, action in this direct~on should be preceded by sho .. t pre-programme trials to evaluate drug tolerance under field conditions. Suoh trtals should also be used for training of staff in each country. Concerning the choice of drug combinations reference is made to t~e recommendations of the workshop on e idemiolo an1 control includin therapy, XI lnternational Leprosy Congress, Mexico CIty,

•
TABlE la. EPI DEMIOLOGI CAL PROFILE
Estimatm Total estimated No. r~stered Total estimated No. inpatients Cou ntry/Area population in cases (prevalence cases (of number of lepro- (% of registered
thousands(1978) rate per 1000) estimated cases) matous cases cases) (% of total estima-ted cases)
Malaysia 12999 15 000(1. 15) 7550 (50.3) 7650 (51. Q) 2000 (26.5)
New Cal monia 142 700 (4.9) 586 (83.7) 332 (47.4) 83 U4. 2) (\)
Papua New Guinea 2959 20 713 (7. Q) 8 019 (38. 7) 9523 (46. Q)
Philippines 46 145 50 000 U. I) 32 340 (64. 7) 23 800 (47.6) 4 353 U3. 5)
Republic of Korea 36 487 50000 U. 4) 28 000 (56. Q) 30 150 (60. 3) 5 032 U8. Q)
Socialist Republic of Viet Nam 51 699 130 000 (2. 4) 36 600 (27. 7) 38 6\0 (29. 7) 6495 (17.7)
Total I~ 431 266 413 (I. 8) 113 095 (42.45) 110 070 (41. 3) 17 954 (\5. 9)
mAli leprosy hospitals were closed by 1974
(2'Prior to the implementation of the National Health Plan (1974-78) leprosy control was conducted by regional leprosy control teams.
(3) I = I ntegrattlf; V = Vertical
Annex 1
Type of Year ~rogra~me of I or V) inception
V
V
1969
1913
1974(2)
1954
1964
1954
"" '"
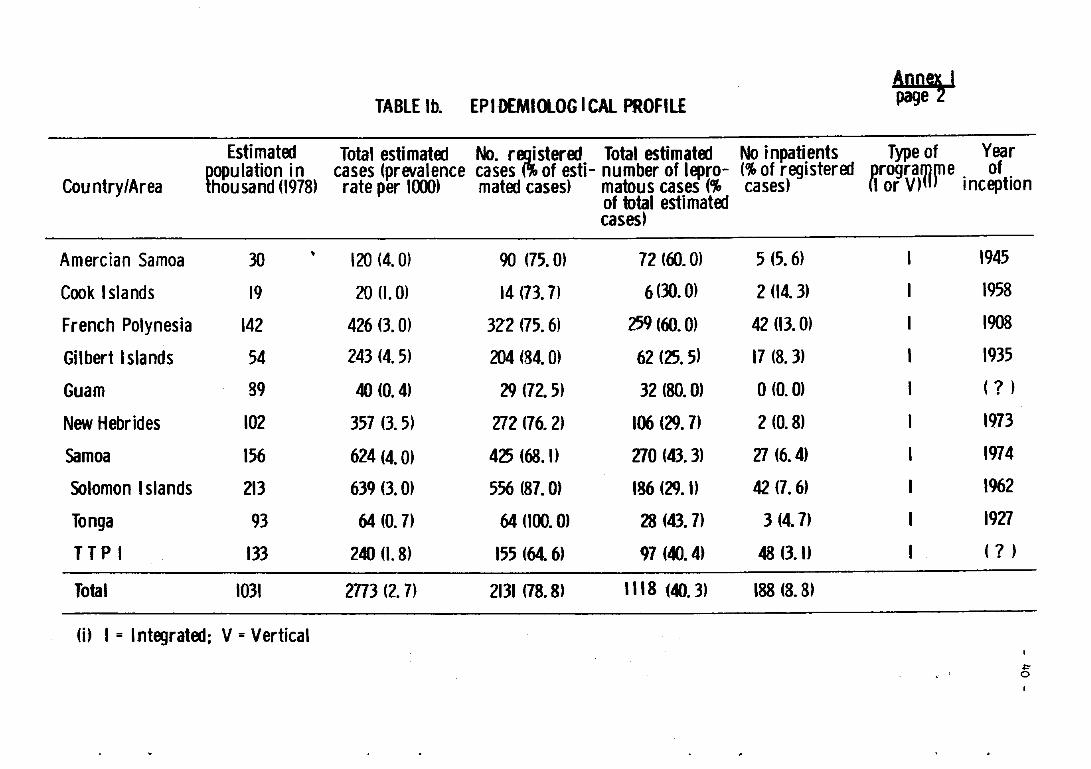
TABLE lb. EPIDEMIOlOG I CAl PROFILE ~ Estimatoo Total estimatoo No. r~steroo Total estimatoo No inpatients Type of Year
Country/Area ~ulation incases (prevalence cases of esti- number of lepro- (% of registeroo 8rogra~fe. of. housand (1978) rate per 1000) matoo cases) matous cases (% cases) I or V) inception
of total estimatoo cases)
Amercian Samoa 30 • 120 (4. Q) 90 (75. Q) 72 (60. Q) 5 (5.6) 1945
Cook Islands 19 20 (I. Q) 14 (717) 6 (30. Q) 2 (14.3) 1958
French Polynesia 142 426 (1 Q) 3Z2 (75.6) 259 (60. Q) 42 (11 Q) 1908
Gilbert Islands 54 243 (4.5) 204 (84. Q) 62 (25.5) 17 (8. 3) 1935
Guam 89 40 (0.4) 29 (72.5) 32 (SO. 01 o (0. Q) ( ? )
New Hebrides 102 357 (15) 272 (76.2) 106 (29.7) 2 (0.8) 1973
Samoa 156 624 (4. Q) 425 (68.1) 270 (413) 27 (6.4) 1974
Solomon Islands 213 639 (3. Q) 556 (87.01 136 (29. I) 42 (7.6) 1962
Tonga 93 64 (0.7) 64 (100.01 28 (43. 7) 3 (4.7) 1927
TTPI 133 240 (I. 8) 155 (64.6) 97 (40.4) 48 (11) ( ? )
Total 1031 2n3 (2.7) 2131 (78.8) "18 (40.3) 188 (8.8)
m I = Integratoo; V = Vertical ~ 0

, .
Problems Training
MALAYSIA
NEW CALEDONIA
PAPUA NEW GUINEA I
PHILIPPINES
REPUBLIC OF KOREA
SOC1 All ST REPUBlI C OF VIET NAM
2
TABlE la. MAIN PROBlEMS BY ORDER OF PRIORITY U£~I
Supervision
2
3
2
3
2
Drugs and Equipment
4
2
5
3
Transport and Physical Communication rehaf:lilitation
5
2 7
3 5
4
7 5
Health Education
3
2
5
6
3
6
Leprosy Information
System
4
4
6
4
Note: Regularity of treatrre nt and case-finding were not tonsideroo as they are directly related to the above-mentioned factors.
~ .....

TABlE 2b. MAIN PROBLEMS BY ORDER OF PRIORITY
Training Supervision Dru9s and EqUipment
Transport and Communication
Ph~sical reha ilitation
A. SMNJA 2 3
COOK ISLANDS
F I J I 2 3
GILBERT ISlANDS 2 3 4 7
GUAM
NEW HEBR 1 DES 2 3 4
SAMOA 2 5 1 4
SOLO.wlN ISLAND S 2 5 3
IDNGA 2 6 5 1
T T P I 2 3 6
...
Health Education
6
6
3
6
3
5
AQ0r\ I page
Lepros6' I nforma Ion
System
4
5
5
6
4
4
4
~ I\)

Annex I page 5
P R I 0
TRAINING
SUPERVISION
DRUGS &
EQUIPMENT
TRANSPORT &
•
R
COMMUNICA TIONS
PHYSICAl REHABILITATION
HEAlTli EDUCATION
LEPROSY INFORMATION SYSTEM
TOTAL ESTIMATED
I T
ADDITIONAL EXPENDITURE FOR THE YEAR
TENTATIVE MODEL FOR A A'lDIUM-TERM~ROGRAMME IN LEPROSY CONTROl-lEPRALAND
S P E C I F I C T A I E S
1979 1980 1981
Category M.O. A.N. l.A. M.O. A.N. L.A. M.O. A.N. LA.
Number of trainees 3 10 8 6 6 2 6 6 2
Number of courses I 2 4 I 2 4 I 2 4
Duration (in days) 14 14 7 2 14 7 2 14 7 IUS$ 135701 IUS$ II 496) IUS$ II 496)
II To divide the country into three operational Periodic su~ervision of regions each of them under a medical officer the mobile eams b~ the responsible for the general supervision of regional medical 0 ic:) leprosy control programme. supervision according 0
2) To designate one health officer in each area th e preval ence rate in to supervise all tixa! and mobile activities. the area.
Rifampicin,3OOmg 54 000 caps. IU S$17 S2O) ISO cap~IUS$ 4455) ISO caps. (U S$4 455) Ciofazimine,6OOmgl 630 000 caps.IUS$75 6(0) 73 000 caps. (U 5$S 856) 73 000 caps. I U S$8 8561 Microscopes I ~ 438 140 ca~s. (US$525601
3 (US$ 0001 laboratory material (US$ I 000)
Total cases to receive combina! therapy· 3500
landrover ITo~tal 3 IUS$21 000) Motorcycles 5 (U 5$10 000) 5 IUS$12oool Outboard motors 5 IUS$ 3000)
US$2000 US$ 2000 US$ 3000
Printa! materials US$25OO US$25OO US$ 1000 for leprosy patients
Printing of recording US$ I 000 U5$ 500 and reporting forms
US$t5249O US$41807 US$28 SOl or ( U5$129 4501
R G
M. O .• Medic.al officer A. N. • Assistant nurse l. A. • Laboratory assistant
E T S
1982 1983
M.O. A.N. l.A. M.O. A.N. l. A.
6 6 2 6 6 2
I 2 4 I 2 4
2 14 7 2 14 7 (US$ 11496) IUS$ II 496)
same as in same as in previous year previous year
ISO caps. I U S$ 4 455) 180 caps. (U S$ 4 455) 73 000 caps. IU S$ S S561 73 000 caps. IUS$ 8 856)
, .. ~ .. ... ,
US$ 3000 US$ 3000
US$ 1000 US$ I 000
US$28 807 U5$28 807
\

txplanatory Note - LEPROSY I NFORMA TlON ON LEPRALAND
Total popu lation
Estimated number of leprosy cases
Total number of registered cases
10 million
20 000 (8000 L + B; 12 000 NU
L + B 6000 NL 6000
Total 12000
Multlbacillary reglster.t cases 3500 (of which 300 are clinically dapsone-resistant cases)
Type ot programme Fully Integrated
Responsible for leprosy control
Training facilities
Case-finding and treatment facilities
Full-time medical officer (Leprologist)
Fu Ily equ ifPed central I nstltutlon with a permanen clinical material of 400 cases of all forms of leprosy.
(a) all existing health centres covering the whole country;
(b) 23 mobile skin clinics operating to improve case-finding and treatment in hyperendemic areas.
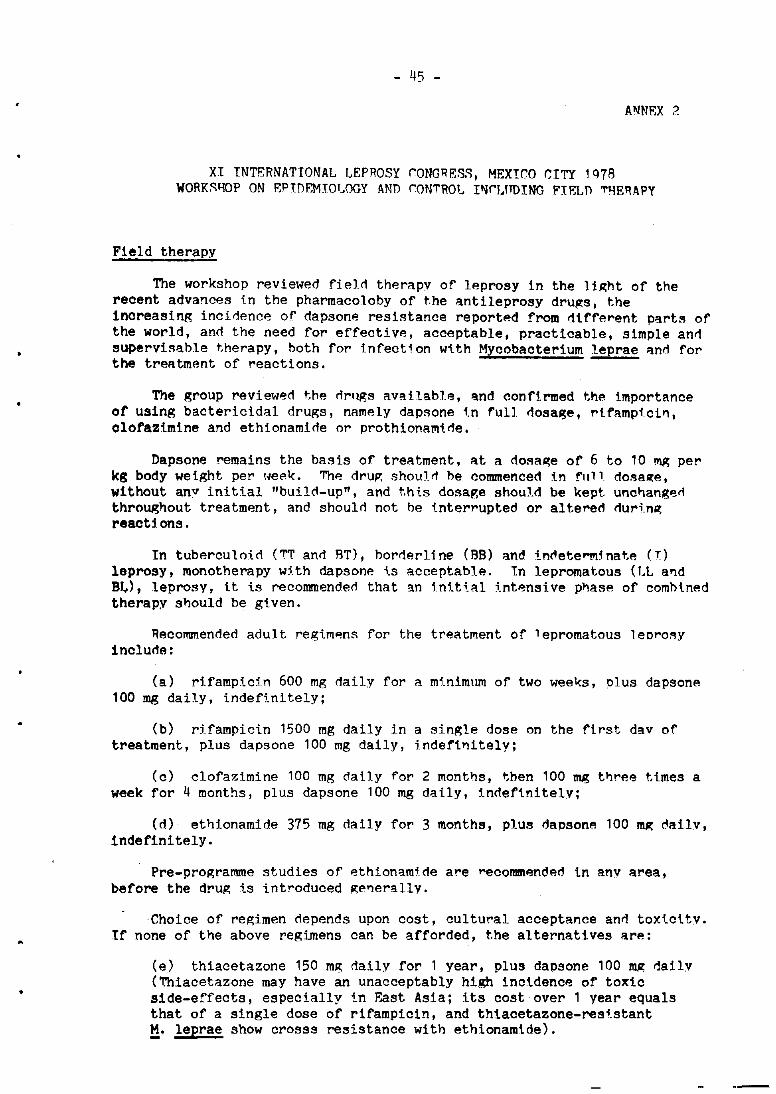
•
- 45 -
ANNEX ?
XI INTERNATIONAL LEPROSY rONGIlES~, MEXICO CITY 1Q78 WORK~I-IOP ON EPInEMIOI.OGY AND rON'l'ROt I"IrJ.tTDING FIEL!) 'l'I-IEIlAPY
Field therapy
The workshop reviewed fieIr! therapy of leprosy in the lip;ht of the recent advances tn the pharmacoloby of the antileprosy drup;s, the increasing incidence of dapsone resistance reported from different parts of the world, and the need for effective, acceptable, practicable, simple and supervisable therapy, both for tnfection w'l.th Mycobacterium leprae ant1 for the treatment of reactions.
The group reviewed the t1rllgs available, and conftrmed thl'! importance of using bactericidal drugs, nalllely dapsone 1.n full dosall;e, ri famplci", clofazimine and ethionamide or prothlonalll'l.de.
Dapsone remains the basis of treatment, at a dosap;e of 6 to 10 ~ per kg body weight per l,eel{. The drup, shoulfi be commenced in fllll dosaQ;e, without anv initial "buil<:l-up", and t.hts dosage should be kept unct)angen throughout treatment, and shoulr! not be i.nterrupted or altere<:l rluri.np; reactions.
In tuberculoid ('I'[ and BT), borderline (BB) and in~etel"!l]5nate (r) leprosy, monotherapy w5.th dapsone ls acceptable. In lepromatous (LL a'ld BI.) , leprosv, it ts recommendefi that an tnit ial lntensi va phase of combined therapy should be gtven.
Recommended adult regimens for the treatment of lepromatous leorosy inclurle:
(a) rtfampicin 600 mg rlaily for a minimum of two weel{s, plus dapsone 100 mg daily, indefinitely;
(b) rHampicin 1500 mg daily in a single dose on the first day of treatment, plus dapsone 100 mg daily, indefi'litely;
(c) clofazimine 100 mg dany for 2 months, then 100 mg three times a week for 4 months, plus dapsone 100 mg daily, 1n~ef'l.nitely;
(~) ethionamide 375 mg ~aily for 3 months, plus dapsone 100 ~ ~ailv, indefinitely.
Pre-programme studies of ethionamt~e are recommended in any area, before the drug is introduced p;e~erallv.
·Choice of regimen depends upon cost, cultural acceptance an~ toxtcity. If none of the above regimens can be afforded, the alternatives are:
(e) thiacetazone 150 mg daily for 1 year, plus dapsone 100 mp; ~aily (~iacetazone may have an unacceptably high incidence of toxic side-effects, espeCially in F~st Asia; its cost over 1 year equals that of a single dose of rifampiCin, and thiacetazone-resi.stant M. leprae show crosss resistance with ethionamide).

- 46 -
Annex 2
(fl o'lpsone 100 mg rI::lilv inrlRfi"ttelv, ~msul"i"g rp.I"ull!.l"i.tv of treatment.
nl!psone resi.stl'lnce. Secrmrlarv dapsonE'! I"esj.st./mce hits to tiltte onl v been reported in lRprom8.tous (LL and Bt) leprosy. The rl1ap;nos1s shoulrl be confirmed by a medi.ca] offieRr. Tt is appreciated that mouse footpad oonfirl'lI'ttton is not wirlely ::iva i.lable. However, random spectlllens of thp. patient's urine shoulrl normally be tested to confirm the presence of dapsone. Further informat 1. on is needed on the j.ncidence anrl preva] ance or dapsone-resistant leorosy in rltffRrent geographical areas.
Recomm~mrle<i 'idu'.t. regimf!n3 for the treatment of dapsone-rt'ststan t •
patients include:
(a) rifampi.cin 600 mg rlail.v for 1 month, plus clofllztm1ne 100 mp: daily for 6 mont.hs, t.hen lOa m~ th"'~F! tl.mes a week 1.nrtp.f1.nitelYi
(b) rifampicin 600 m. rlallv fnr 1 month, plus ethionamide ~7~ mp; daily, indef'init.?lv;
(c) et.htonamtrlp 37'i "II': rlai lv for "1 months, pllls cl.of'l'Izi.me 100 "Ill:
daily for 6 months, then 100 mg three times a week jndefinttelv;
(d) clofa70tme 100 m!2: dal.l.V f'or 6 months, plus ethlonamfde 375 mg datly indefinitRly.
Primary dapsone ~esi~tance may occur in any type of leprosy, anrl this possibility should always he kept in minrl, especi'llly "Imon.!!; contacts of known caS8S of SBCOnO'Irv r8sist'lnce.
•
. -