from high dependency to self- responsibility the changing treatment model provided at the cassel...
TRANSCRIPT

From high dependency to self-responsibility
The changing treatment model provided at the Cassel Hospital specialist inpatient and outreach service
Dr Wilhelm Skogstad, Consultant Psychiatrist in Psychotherapy
Amanda MacKenzie, Senior Nurse
Julia Blazdell, Expert by Experience
Lesley Day, Head of Service
Cassel Hospital Specialist Personality Disorder Service

Cassel Hospital Specialist Personality Disorder Service
Psychotherapeutic and psychosocial inpatient, day patient and outpatient
treatment for people with severe personality disorders and complex needs
The Cassel - traditional and …

The Cassel - … modern

Traditional Model (1)
Inpatient
Treatment

Traditional Model (2)
Therapeutic Community
IndividualPsychotherapy
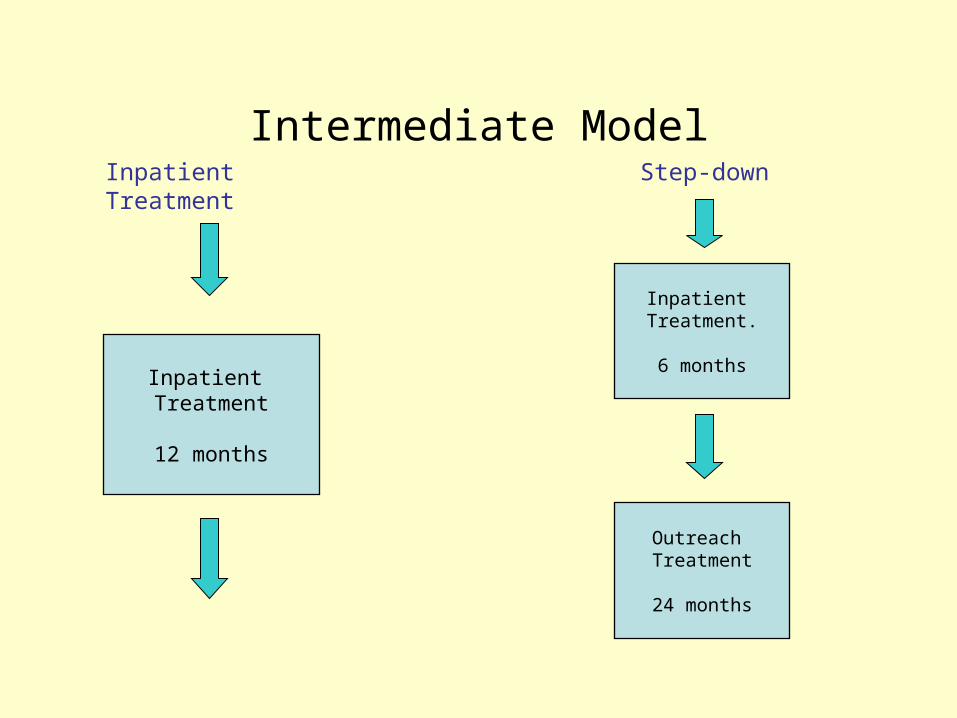
Intermediate Model
Inpatient Treatment
12 months
Inpatient Treatment.
6 months
Outreach Treatment
24 months
Inpatient Treatment Step-down
Cassel Research(M Chiesa et al)
• One stage programme– 12 months inpatient treatment at the Cassel– No follow-up treatment from the Cassel
• Step-down programme– 6 months inpatient treatment at the Cassel– 2 years outreach treatment: 2/wk group psychotherapy
+ psychosocial outreach nursing + working with local services
• Treatment as usual– General psychiatric care and management,with hospital
admissions, community support, psychotropic medication etc.

Change in number of symptoms
40
45
50
55
60
65
70
75
Intake 6 mo 12 mo 24 mo 72 mo
mean
InpatientStep downTAU

Change in symptom severity
0.8
1
1.2
1.4
1.6
1.8
2
2.2
Intake 6 mo 12 mo 24 mo 36 mo 72 mo
mean
InpatientStep downTAU
Chiesa et al. (2006). Six-year follow-up of three treatment programs to personality disorder Journal of Personality Disorders, 25, 493-509.

Changes in global functioning
42
46
50
54
58
62
Intake 6 mo 12 mo 24 mo 36 mo 72 mo
mean
InpatientStep downTAU

Change in social adaptation
1.8
2
2.2
2.4
2.6
2.8
3
Intake 6 mo 12 mo 24 mo 36 mo 72 mo
mean
InpatientStep downTAU

Parasuicidal Behaviour
2
12
22
32
42
52
62
%
InpatientStep downTAU

Hospitalisation
0
10
20
30
40
50
60
%
InpatientStep downTAU

Work on patients’ transitions
• Joint work with professionals and patient towards admission
• Written information for patients
• Pre-admission day visits to the Cassel
• Pre-admission planning meetings
• Buddy system for new patients
• Special structures for new patients
• Long anticipation of leaving
• Transition phase with shorter weeks or as day patient
• Working towards discharge with patient and local service
• Consulting to local professionals
• Setting up treatment and support for after discharge

Working with local services
• Liaison with local professionals prior to referral
• Working jointly with professionals and patient towards admission
• Pre-admission planning meetings
• Treatment reviews
• CPA meetings
• Frequent contact with local professionals to update and discuss
• Joint work towards discharge back to local services
• Pre-discharge planning meetings
• Follow-up meetings with patient and/or professionals

Pathways through the CasselIntensive
Community care - Revolving door
NHS or Private Sector Acute Unit
NHS or Private Sector Low/Medium Secure Unit
Psychosocial Assessment at the Cassel
Residential treatment at the Cassel
Joint workby Cassel and local services
Transitional phase e.g. shorter weeks, day patient - involving local
services
Cassel Outreach in cooperation with
local services
Outpatient treatment through
local services

Cassel Multidisciplinary Team
Dance Movement Therapist
CommunityDoctor(SHO)
SpRs Psychotherapy
PsychotherapistsAdult and Adolescent
SocialWorker
PsychosocialNurses
Consultant Psychiatrist, Psychoanalyst
MultiDisciplinary Team

New Treatment Model
Psychosocial Practice
Community meetingsWork GroupsPhysical and Social ActivitiesSpecial Interest GroupsParents GroupPsychosocial EducationCommunity Management Meeting
Psychotherapy
Individual psychotherapyGroup Psychotherapy
Dance Movement TherapyCouples/ Family sessions
MDT staff meetings.
Planning meetings
Reviews
CPA/ Professionals
Reflective practice
Supervision Groups

Why specialist residential treatment?
• Significant risk (self-harm, suicide) - not manageable as outpatient
• Long hospital admissions with failure to discharge/revolving door
• Step-down from more secure setting
• Local treatment resources exhausted
• Change only possible through intensive treatment
• No local specialist treatment available
• Treatment only possible away from home

Current Model
INCAMHS, CMHT/
Family/Carers/ Friends/ PsychiatricForensic Services (wards)
Psychosocial Practice
Community meetingsWork GroupsPhysical and Social ActivitiesSpecial Interest GroupsParents GroupPsychosocial EducationCommunity Management Meeting
Psychotherapy
Individual psychotherapyGroup Psychotherapy
Dance Movement TherapyCouples/ Family sessions
Family/carers/ friends, Voluntary sector, CMHT, Outreach
OUT
MDT staff meetings.
Planning meetings
Reviews
CPA/ Professionals
Reflective practice
Supervision Groups
Shared living-learning Environment
‘Alongside’ rather than ‘for’ the patient

The process of change
• Relationships as central focus
• Helping develop an internal container through an external container
• Linking ‘understanding’ and ‘doing’
• Fostering responsibility for themselves and others
• Enabling supportive relationships between patients
• Dealing with self-harm in a holistic way: challenging + understanding and support + emphasis on relationships (impact on others)
• Taking measured risks: tolerating anxiety
• Team work: bringing split-off aspects together in the staff team

References
• Chiesa, M. (2000) Hospital adjustment in personality disorder patients admitted to a therapeutic community milieu. British Journal of Medical Psychology 73: 259-267.
• Chiesa, M., Fonagy, P., Holmes, J. & Drahorad, C. (2004) Residential versus community treatment of personality disorders; a comparative study of three treatment programs. American Journal of Psychiatry, 161(8), pp 1463-1470.
• Chiesa, M., Fonagy, P. & Holmes, J. (2006) Six-year follow-up of three treatment programs to personality disorder. Journal of Personality Disorders, 20(5), pp 493-509.
• Chiesa, M. & Healy, K. (2009) The struggle to establish a research culture in the psychotherapy hospital: Reflections from the Cassel Hospital experience. Bulletin of the Menninger Clinic 73, 3: 157-175.
• Day. L. & Flynn, D. (Eds) (2003) The internal and external worlds of children and adolescents; collaborative therapeutic care (Cassel Hospital Monograph Series No. 3 ) London: Karnac
• Drahorad, C (1999) Reflections on being a patient in a therapeutic community. Therapeutic Communities, 20, 3: 195-215.
• Griffiths, P. & Pringle, P. (Eds) (1997) Psychosocial practice within a psychosocial setting (Cassel Hospital Monograph Series No. 1), Karnac Books, London
• Hinshelwood, R. D. & Skogstad, W. (1998) The hospital in mind; the setting and the internal world. In: Pestalozzi, J. et al. (Eds) Psychoanalytic psychotherapy in institutional settings, London: Karnac pp 59-73.
• Skogstad, W. (2003) Internal and external reality in in-patient psychotherapy; working with severely disturbed patients at the Cassel Hospital. Psychoanalytic Psychotherapy, 17 (2), pp 97-118.