fuel poverty - engaging the nhs definitions of fuel poverty (10%) and “vulnerable” impact on...
TRANSCRIPT
Fuel Poverty - Engaging the NHS• definitions of fuel poverty (10%) and “vulnerable”
• impact on health and demand for health services
• win-win for health and sustainable development
• targeting the “financially and clinically vulnerable” populations responsively
• accessing the services – need for “front facing” services
• name of strategy = “Affordable warmth –avoidable ill health”
Fuel poverty – engaging the NHSOutline of approach
• Presenting information is a “health focused way”
• Analysis of data in a “health focused way”
- & attempt at sharing data
• Initiatives such as EAGA flu-mail out training of front-line staff
• Thermal energy survey (AM)
• Joint strategy (AM)
Health perspectives
• The term “fuel poverty” doesn’t engage the Health service very strongly
• Health care providers don’t see how they contribute to this
• What is in it for the NHS?• Concerns are about prevention and treatment of
ill-health (mostly the latter)• Local authority staff need to think about how to
“sell to NHS” including putting NI 187 in LAAs
Health effects• 24˚C and above there is a risk of
cardio vascular problems, strokes and heart attacks
• Indoor temp 18-24 ˚C no threat to health• Below 16˚ C reduced resistance to
respiratory infections• Below 12˚C core body temperature
drops- BP rises – risk of cardiovascular disease
• Below 9˚ C after two or more hours body temperature falls
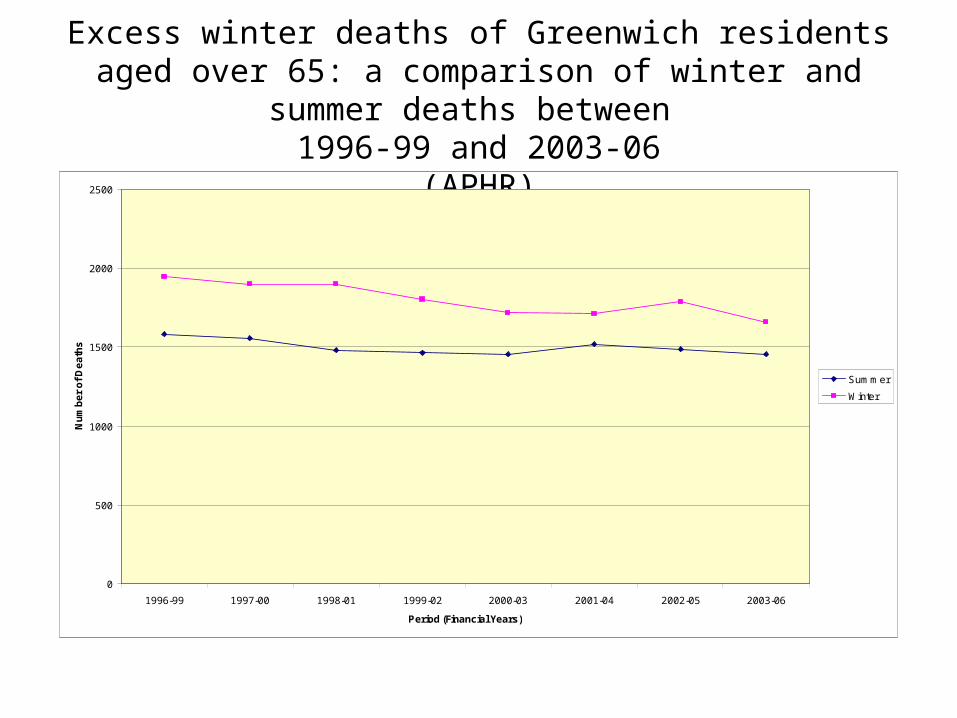
Excess winter deaths of Greenwich residents aged over 65: a comparison of winter and summer deaths between
1996-99 and 2003-06(APHR)
0
500
1000
1500
2000
2500
1996-99 1997-00 1998-01 1999-02 2000-03 2001-04 2002-05 2003-06
Period (Financial Years)
Nu
mb
er
of
De
ath
s
Summer
Winter
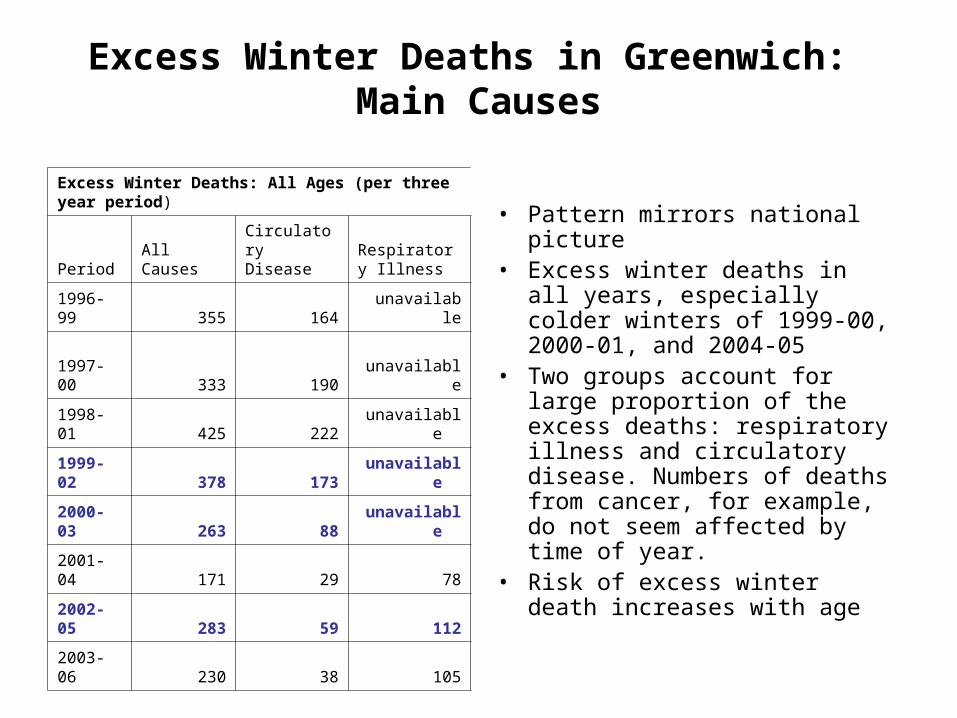
Excess Winter Deaths in Greenwich: Main Causes
Excess Winter Deaths: All Ages (per three year period)
Period All Causes Circulatory Disease
Respiratory Illness
1996-99 355 164 unavailable
1997-00 333 190 unavailable
1998-01 425 222 unavailable
1999-02 378 173 unavailable
2000-03 263 88 unavailable
2001-04 171 29 78
2002-05 283 59 112
2003-06 230 38 105
• Pattern mirrors national picture• Excess winter deaths in all
years, especially colder winters of 1999-00, 2000-01, and 2004-05
• Two groups account for large proportion of the excess deaths: respiratory illness and circulatory disease. Numbers of deaths from cancer, for example, do not seem affected by time of year.
• Risk of excess winter death increases with age
The benefits of affordable warmth:• Increases life expectancy and reduces inequalities
in health
• Promotes independent living and social well-being.
• Improves mental well-being
• Amongst children, improves educational achievement through providing warm space to study, and reduces non-attendance at school due to sickness.
0
50
100
150
200
250
300
A 1
Glo
bal C
onne
ctio
nsA
2 C
ultu
ral L
eade
rshi
pA
3 C
orpo
rate
Chi
efta
ins
A 4
Gol
den
Em
pty
Nes
ters
A 5
Pro
vinc
ial P
rivile
geA
6 H
igh
Tec
hnol
ogis
tsA
7 S
emi-R
ural
Sec
lusi
onB
8 Ju
st M
ovin
g In
B9
Fle
dglin
g N
urse
ries
B10
Ups
cale
New
Ow
ners
B11
Fam
ilies
Mak
ing
Goo
dB
12 M
iddl
e R
ung
Fam
ilies
B13
Bur
dene
d O
ptim
ists
B14
In
Mili
tary
Qua
rter
sC
15 C
lose
to
Ret
irem
ent
C16
Con
serv
ativ
e V
alue
sC
17 S
mal
l Tim
e B
usin
ess
C18
Spr
awlin
g S
ubto
pia
C19
Orig
inal
Sub
urbs
C20
Asi
an E
nter
pris
eD
21 R
espe
ctab
le R
ows
D22
Aff
luen
t B
lue
Col
lar
D23
Ind
ustr
ial G
ritD
24 C
oron
atio
n S
tree
tD
25 T
own
Cen
tre
Ref
uge
D26
Sou
th A
sian
Ind
ustr
yD
27 S
ettle
d M
inor
ities
E28
Cou
nter
Cul
tura
l Mix
E29
City
Adv
entu
rers
E30
New
Urb
an C
olon
ists
E31
Car
ing
Pro
fess
iona
lsE
32 D
inky
Dev
elop
men
tsE
33 T
own
Gow
n T
rans
ition
E34
Uni
vers
ity C
halle
nge
F35
Bed
sit
Ben
efic
iarie
sF
36 M
etro
Mul
ticul
ture
F37
Upp
er F
loor
Fam
ilies
F38
Tow
er B
lock
Liv
ing
F39
Dig
nifie
d D
epen
denc
yF
40 S
harin
g a
Sta
ircas
eG
41 F
amili
es o
n B
enef
itsG
42 L
ow H
oriz
ons
G43
Ex-
indu
stria
l Leg
acy
H44
Rus
tbel
t R
esili
ence
H45
Old
er R
ight
to
Buy
H46
Whi
te V
an C
ultu
reH
47 N
ew T
own
Mat
eria
lism
I48
Old
Peo
ple
in F
lats
I49
Low
Inc
ome
Eld
erly
I50
Car
ed f
or P
ensi
oner
sJ5
1 S
epia
Mem
orie
sJ5
2 C
hild
free
Ser
enity
J53
Hig
h S
pend
ing
Eld
ers
J54
Bun
galo
w R
etire
men
tJ5
5 S
mal
l Tow
n S
enio
rsJ5
6 T
ouris
t A
tten
dant
sK
57 S
umm
er P
layg
roun
dsK
58 G
reen
belt
Gua
rdia
nsK
59 P
aroc
hial
Vill
ager
sK
60 P
asto
ral S
ymph
ony
K61
Upl
and
Hill
Far
mer
s
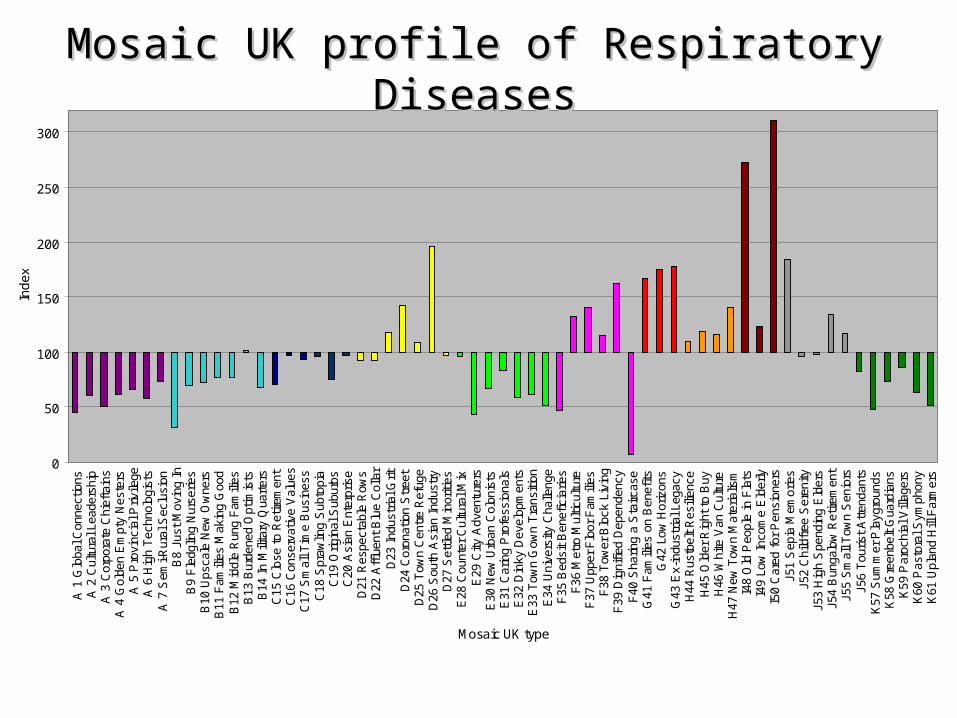
Mosaic UK type
Ind
ex
Mosaic UK profile of Respiratory DiseasesMosaic UK profile of Respiratory Diseases
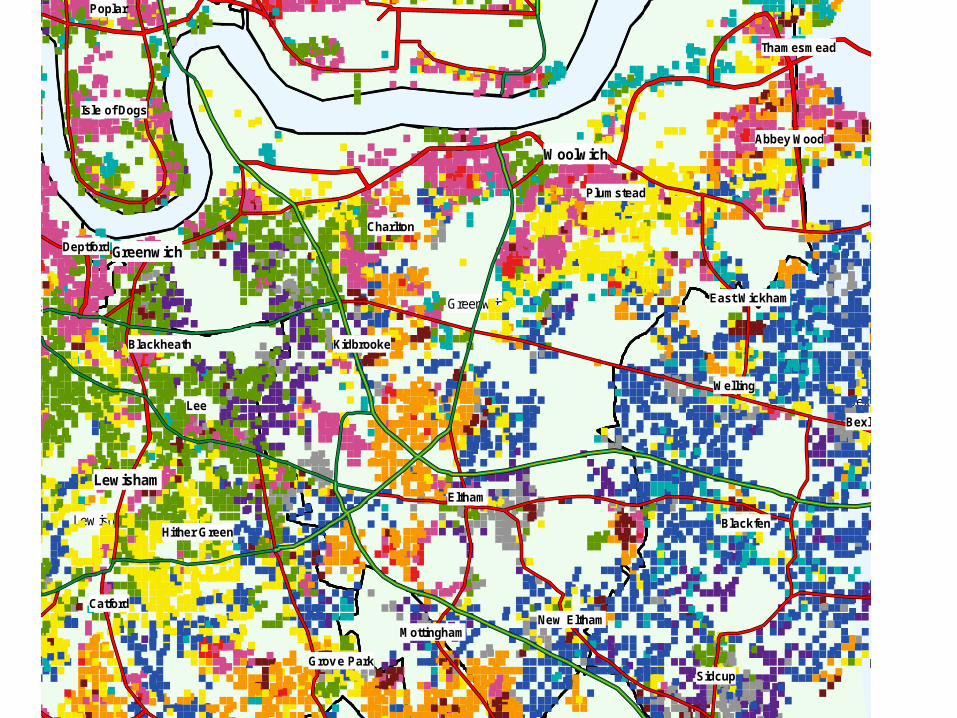
Greenwich
Bexley
Greenw ich
Lew isham
Abbey Wood
Bexleyheath
Blackfen
Blackheath
Canning Town
Catford
Charlton
Deptford
Downham
East Wickham
Eltham
Forest Hill
Greenwich
Grov e Park
Hither Green
Isle of Dogs
Kidbrooke
Lee
Lewisham
Mottingham
New Cross
New Eltham
North Cray
Plumstead
Poplar
Sidcup
Sydenham
Thamesmead
Welling
Woolwich
North Cray
Abbey Wood
Bexleyheath
Blackfen
Blackheath
Canning Town
Catford
Charlton
Deptford
Downham
East Wickham
Eltham
Forest Hill
Grov e Park
Hither Green
Isle of Dogs
Kidbrooke
Lee
Mottingham
New Cross
New Eltham
Plumstead
Poplar
Sidcup
Sydenham
Thamesmead
Welling
Greenwich
Lewisham
Woolwich
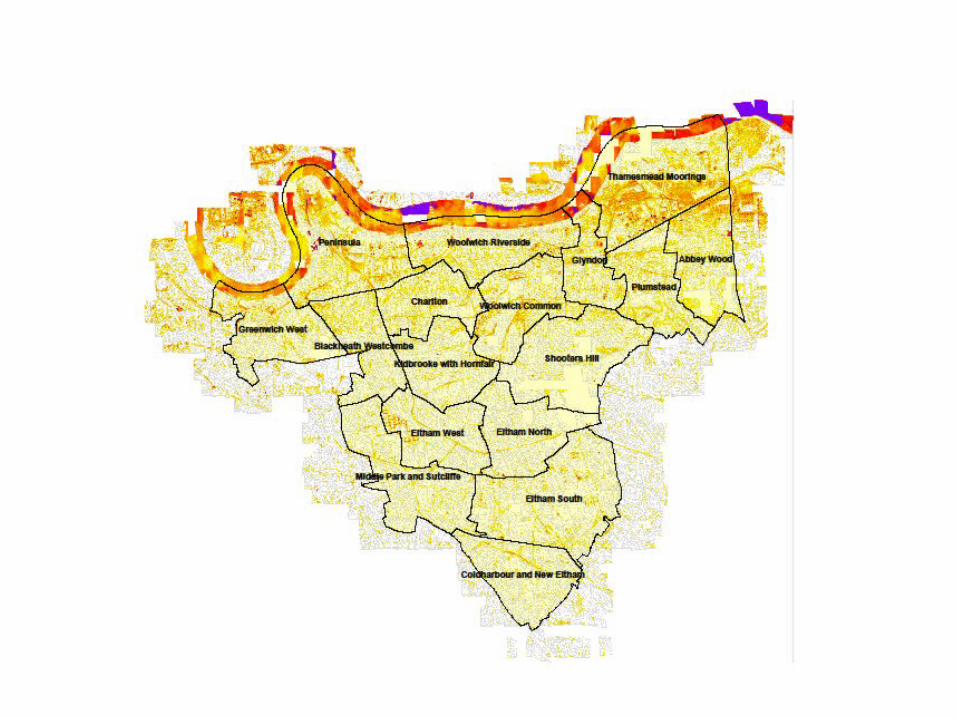
Fuel poverty – local information
• SAP ratings for types of properties
• Census information on heating
• Thermal survey
• Location of grant uptake
• Local knowledge
• Local estates surveys (damp)
SAP Rating* - Greenwich
• 43 = private sector = average
• 47 = RSL = average
• 48 = private rented = average
• 62 = council = Good
*2002 stock conditions survey – council property now 72 private sector little investment since
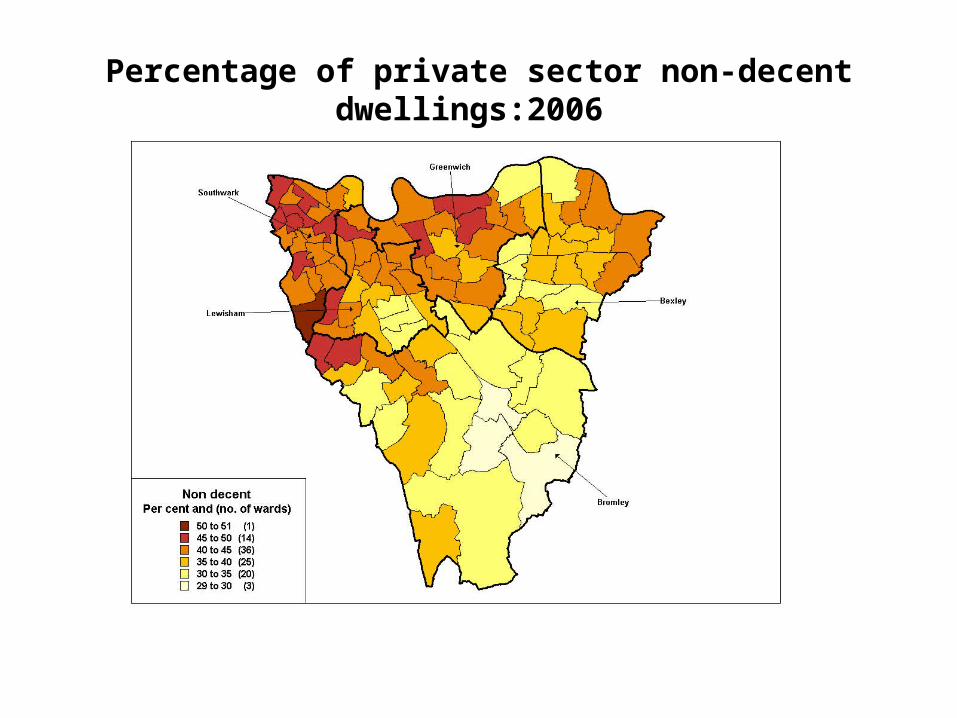
Percentage of private sector non-decent dwellings:2006
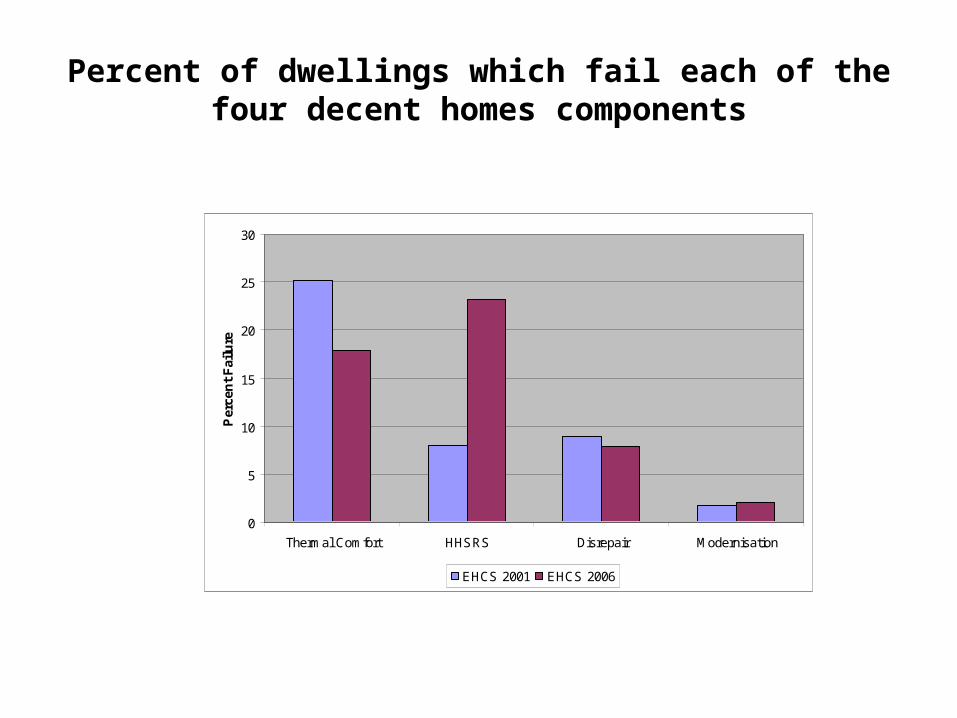
Percent of dwellings which fail each of the four decent homes components
0
5
10
15
20
25
30
Thermal Comfort HHSRS Disrepair Modernisation
Per
cen
t F
ailu
re
EHCS 2001 EHCS 2006

Flu mail out – private sector
• PCT does a central mail-out• EAGA partnerships provided materials• PALS notified• response good – 2% uptake from 27,000• 483 grants taken up (2004-5) and repeated since• 2301 grants between 4/5 & 8/9• Linked in Welfare benefits review at same time• LA staff provide training to front line profs and guidance
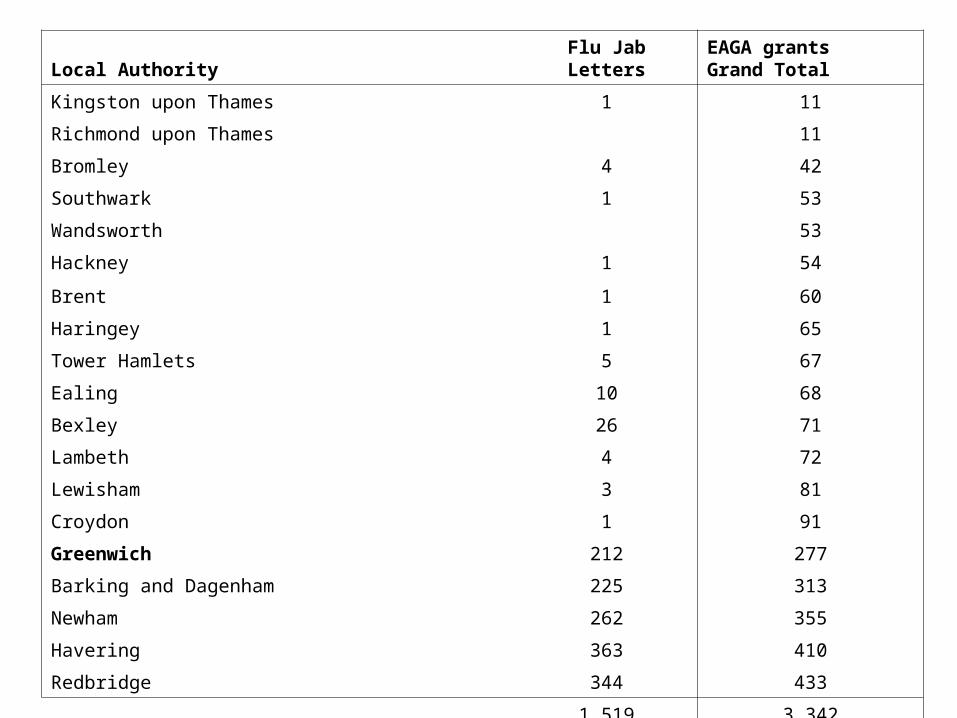
Local Authority Flu Jab LettersEAGA grants Grand Total
Kingston upon Thames 1 11
Richmond upon Thames 11
Bromley 4 42
Southwark 1 53
Wandsworth 53
Hackney 1 54
Brent 1 60
Haringey 1 65
Tower Hamlets 5 67
Ealing 10 68
Bexley 26 71
Lambeth 4 72
Lewisham 3 81
Croydon 1 91
Greenwich 212 277
Barking and Dagenham 225 313
Newham 262 355
Havering 363 410
Redbridge 344 433
1,519 3,342
Aims of the training session (eg from Scotland)
Aims of the session
To raise the awareness of front line health professionals to the health implications of cold, damp and mouldy housing.
To alert these front line health staff to the various sources of help, advice and financial assistance that are available to combat these problems.
Objectives
To outline the condition of the housing stock in Scotland and its financial implications for householders.
To review the research to date linking ill health with cold, damp and mouldy housing conditions.
To highlight the range of initiatives available to the householder to improve the energy efficiency of their home.
Learning outcomes
The participant will be able to identify householders vulnerable to fuel poverty.
The participant will be able to alert the client to sources of free and independent help and advice.
The participant will be able to inform the client of the range of financial assistance that is available.
2
What next• Ideal = one stop shop – accessible for “users”-
overcome tenure specific grants and action (eg multi - occupancy)
• Clear criteria with priority across groups for “vulnerable” people most in need
• Training for front-line staff (next slide)
• Analysis of survey and census info to identify areas and practices with greatest need (2011)
• Monitor progress as part of fuel poverty strategy - tbc
Conclusions
• Joint working requires joint understanding of different perspectives
• Moaning about “them” wont help – “understanding them” will help
• Start simple and build on the opportunities
• Better analysis of the issues helps
• Be aware of sensitivities
• Keep going