full hsr proceedings vol. 2 - n. 4 2010 in pdf
TRANSCRIPT
proceedings
Editors
Alberto ZangrilloRoland Hetzer
in Intensive CareCardiovascular Anesthesia
Endorsed by
Vol. 2 · N° 4 · 2010
proceedingsIN THE NEXT ISSUES
• Epidural analgesia in cardiac surgery
• Neonatal surgery emergencies and peri-operative care
• Volatile anaesthetic preconditioning, oxidative stress and nitric oxide
• Radiological dilemma after central venous catheter positioning
• Non-invasive ventilation after cardiac surgery
• Imaging in cardiovascular medicine
• Papers, Posters, Presentations: communicating the biomedical sciences
ISSN: 2037-0504

Valutazione del paziente esorveglianza continua
Il monitoraggio incontinuo della saturazionevenosa centrale
SEDA S.P.A.Via Tolstoi, 720090 Trezzano sul Naviglio (Mi)
Telefono +39 02 48424.1Fax +39 02 48424290www.sedaitaly.it - [email protected] Certificato UNI EN ISO 9001:2000
Ogni onda è unica.La curva di pressione arteriosa è tutto ciò di cui MostCare® necessita per ottenere la Gittata Cardiaca ed altri parametri emodinamici.
• Campionamento della curva arteriosa a 1000Hz• Esclusivo rilevamento della pressione dicrota• Nessun consumabile dedicato• Non necessita di calibrazione iniziale mediante
nomogramma o diluizione di indicatori• Accesso radiale o femorale consentito• Non richiede cateterismo venoso
www.vytech.eu
Ogni paziente è unico.PRAM è il solo algoritmo in grado di
analizzare realmente la forma d’onda in tempo reale, battito per battito,
senza calibrazioni iniziali.

EditorS in chiEf
Alberto Zangrillo Università Vita-Salute San Raffaele
Milano, Italia
roland hetzer Deutsches Herzzentrum Berlin, Germany
Official Journal of School of Anesthesiology
and Intensive CareCattedra di Anestesia e Rianimazione Università Vita-Salute San Raffaele
Milano, Italia
Endorsed by
ITACTA(Italian Association
of Cardiothoracic Anaesthesiologists) www.itacta.org
Deutsches Herzzentrum Berlin, Germany
WEb Sitewww.itacta.org
SEction EditorSn intEnSivE cArE LucianoGattinoni Università degli Studi di Milano, Policlinico di Milano, Italia
n AnESthESiA FabioGuarracino Azienda Ospedaliera Universitaria Pisana, Pisa, Italia
n vASculAr SurgEry RobertoChiesa Università Vita-Salute San Raffaele, Milano, Italia
n cArdiAc SurgEry OttavioAlfieri Università Vita-Salute San Raffaele, Milano, Italia
n cArdiology GiuseppeBiondi-Zoccai Università degli Studi di Torino, Italia
n clinicAl cArdiology AlbertoMargonato Università Vita-Salute San Raffaele, Milano, Italia
n invASivE cArdiology StephanDreysse Deutsches Herzzentrum Berlin, Germany
n intErvEntionAl pEdiAtric cArdiology PeterEwert Deutsches Herzzentrum Berlin, Germany
n EchocArdiogrAphy MicheleOppizzi Università Vita-Salute San Raffaele, Milano, Italia
n mEtAboliSm DionisioColella Università degli Studi di Tor Vergata, Roma, Italia
n nEw tEchnologiES FedericoPappalardo Università Vita-Salute San Raffaele, Milano, Italia
n in hoSpitAl EmErgEnciES LucaCabrini Università Vita-Salute San Raffaele, Milano, Italia
n nurSing MarianoFichera Università Vita-Salute San Raffaele, Milano, Italia
n hEmAtology AndreasKoster Deutsches Herzzentrum Berlin, Germany
n pEEr-to-pEEr communicAtion MichaelJohn Università Vita-Salute San Raffaele, Milano, Italia
n imAging AntonioGrimaldi Università Vita-Salute San Raffaele, Milano, Italia
n futurE EvEntS GeorgeSilvay The Mount Sinai School of Medicine
ASSociAtE EditorSLucianoGattinoniUniversità degli Studi di Milano, Policlinico di Milano, Italia
MassimoAntonelliUniversità Cattolica Sacro Cuore, Policlinico Gemelli, Roma, Italia
AntonioPesentiUniversità degli Studi di Milano Bicocca, Ospedale San Gerardo, Italia
Edizioni Internazionali srlDivisione EDIMES
EDIzIonI MEDICo SCIEnTIfICHE - PAVIAVia Riviera 39 - 27100 Pavia
Tel. 0382526253 r.a. - fax 0382423120E-mail: [email protected]
Editore
vol. 2 • n° 4 • 2010
Segreteria di redazione
Lara SussaniCattedra di Anestesia e Rianimazione
Università Vita-Salute San Raffaele, MilanoVia olgettina, 60 - 20132 Milano
Tel. +39 02 26436158 fax +39 02 26436152
wEb Sitewww.itacta.org
direttore responsabilePaolo E. zoncada
Registrazione Tribunale di Milano n. 532 del 26 novembre 2009
The Journal is indexed inCInAHL, DoAJ, EBSCo,
GEnAMICS JoURnALSEEK, GooGLE SCHoLAR, HInARI,
InDEX CoPERnICUSISSn (onLInE): 2037-0512
ISSn (PRInTED): 2037-0504
Stampa
Jona Srl Paderno Dugnano (MI)
EXEcutivE Editor
MassimilianoNuzziUniversità Vita-Salute San Raffaele, Milano, Italia
EditorS
JohnT.ApostolakisCleveland Clinic, OH, US
ElenaBignamiUniversità Vita-Salute San Raffaele, Milano, Italia
TizianaBoveUniversità Vita-Salute San Raffaele, Milano, Italia
MariaGraziaCalabròUniversità Vita-Salute San Raffaele, Milano, Italia
NicolaColangeloUniversità Vita-Salute San Raffaele, Milano, Italia
MicheleDeBonisUniversità Vita-Salute San Raffaele, Milano, Italia
FrancescoDeSimoneUniversità Vita-Salute San Raffaele, Milano, Italia
GianFrancoGensiniUniversità degli Studi di Firenze, Italia
GiuseppeGiardinaUniversità Vita-Salute San Raffaele, Milano, Italia
JamesL.JanuzziHarvard University, Massachusetts General Hospital, US
GiovanniLandoniUniversità Vita-Salute San Raffaele, Milano, Italia
KevinLobdellSanger Heart and Vascular Institute, Charlotte, NC, US
GiovanniMarinoUniversità Vita-Salute San Raffaele, Milano, Italia
AndreaMorelliUniversità degli Studi “La Sapienza”, Roma, Italia
StefanoRomagnoliOspedale Careggi, Firenze, Italia
AntonioEmilioScalaDean, Università Vita-Salute San Raffaele, Milano, Italia
AnnaMaraScandroglioUniversità Vita-Salute San Raffaele, Milano, Italia
LuigiTritapepeUniversità degli Studi “La Sapienza”, Roma, Italia
EmilianoVitaliniOspedale San Camillo Forlanini, Roma, Italia
Edizioni Internazionali srlDivisione EDIMES
EDIzIonI MEDICo SCIEnTIfICHE - PAVIAVia Riviera 39 - 27100 Pavia
Tel. 0382526253 r.a. - fax 0382423120E-mail: [email protected]
Editore

241
proceedingsin Intensive Care
Cardiovascular Anesthesia
Endorsed by
proceedings
CONTENTS
nEditorial
Newfrontiersinaorticsurgeryandanesthesia...................................................................................................................................243 R.Chiesa,A.Zangrillo,O.Alfieri,G.Melissano
n iNvitEdEditorial
theissueoffluidbalanceandmortality...........................................................................................................................................................245 Z.Ricci,S.Romagnoli
nrEviEWartiClE
Cerebraloximetryincardiacandmajorvascularsurgery............................................................................................249 G.W.Fischer,G.Silvay
noriGiNalartiClE
Endovasculartreatmentofdescendingthoracicaneurysms........................................................................................261 R.Chiesa,E.Civilini,Y.Tshomba,E.M.Marone,L.Bertoglio,D.Baccellieri, G.Coppi,D.Logaldo,G.Melissano
transcatheteraorticvalvereplacementinhighriskpatients withdifferentanaesthetictechniques....................................................................................................................................................................273 I.MøllerNielsen,C.Andersen
Bystander-initiatedchestcompression-onlyCPrisbetterthanstandardCPr inout-of-hospitalcardiacarrest............................................................................................................................................................................................279 L.Cabrini,G.Biondi-Zoccai,G.Landoni,M.Greco,F.Vinciguerra,T.Greco,L.Ruggeri, J.Sayeg,A.Zangrillo
Highvolumesofintravenousfluidduringcardiacsurgeryareassociated withincreasedmortality.................................................................................................................................................................................................................... 287 A.Pradeep,S.Rajagopalam,H.K.Kolli,N.Patel,R.Venuto,J.Lohr,N.D.Nader
nCaSErEPort
leftdiaphragmaticherniaafterpneumonectomy............................................................................................................................ 299 E.Piraccini,V.Agnoletti,R.M.Corso,J.Chanis-Vargas,S.Gaetani,G.Gambale
nPaPErS,PoStErS,PrESENtatioNS:CommuNiCatiNG tHEBiomEdiCalSCiENCES
messageinabody:controllingyournervesduringanoralpresentation........................................ 303 M.John

Arresto cardiacoIctusHIE Encefalopatia Ischemica IpossicaDanno vertebrale traumaticoSepsiChirurgiaEmergenzaDanno celebrale traumaticoMantenimento organi per donazione
LA SOLUZIONE IDEALE PER:
SEDA S.P.A.Via Tolstoi, 720090 Trezzano sul Naviglio (Mi)
Telefono +39 02 48424.1Fax +39 02 48424290www.sedaitaly.it - [email protected]
Certificato UNI EN ISO 9001:2000

243
proceedingsin Intensive Care
Cardiovascular Anesthesia
Endorsed by
proceedings
The term “aortic pathology” includes a number of diseases ranging from the aortic valve to the abdominal tract. It represents not only one of the most prevalent affection of the human being, but also one of the most challenging fields in cardiovascular medicine.During the last 25 years, we witnessed a significant improvement in the results of treatment of this pathology. The important decrease in operative morbidity and mortality re-flects the ongoing experience of anesthesiologists and surgeons, the accuracy in patients selection and preoperative assessment, and the impact of advanced technology.Very few medical innovations had such an impact on the manage-ment of aortic disease as endovascular techniques. In appropriate patients, endovascular repair has reduced recovery times, major morbidity, and disease-related mortality, really transforming the care of patients with aortic valve disease, type A and type B dissec-tion, descending thoracic aortic aneurysm, penetrating ulcers, and traumatic aortic injury. However, these techniques still represent “a young therapy” and there is much to be learned about patient selection, specific indi-cations, contemporary advanced imaging, device design, procedural techniques, and follow-up. Now at its fourth edition, the International Congress Aortic Surgery and Anesthesia “How to do it” will have a new format in order to offer very intense, dynamic sessions of rapidly paced presentations. An international and truly multidisciplinary faculty has been selected to provide unparalleled expertise in both classical and innovative as-pects of aortic interventions. The meeting will have the privilege to bring together vascular, endovascular and cardiothoracic specialists as well as the anaesthesiologists that make surgical efforts possible every day.
Edi
tori
al New frontiers in aortic surgeryand anesthesiaR. Chiesa1, A. Zangrillo2, O. Alfieri3, G. Melissano1
1Department of Vascular Surgery; 2Department of Anesthesia and Intensive Care;3Department of Cardiac Surgery, Università Vita-Salute San Raffaele, Milan, Italy
Corresponding author:Roberto Chiesa, M.D.Chair of Vascular Surgery “Vita-Salute” University School of Medicine Scientific Institute San RaffaeleVia Olgettina, 60 - 20132 Milan, Italye.mail [email protected]
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010; 2: 243-244
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2

244
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
EDITORIAL
The mission of our “how to do it” meeting remains strictly practical. All the distinguished speakers will be asked to give very focused an-swers to particularly specific and relevant questions, including im-aging choices and interpretation, selection of patients, preoperative optimization, choice of procedure, technological innovations, tech-nical tips and tricks, bailout options and management of complica-tions, postoperative care and outcomes. The congress is designed for Vascular Surgeons, Cardiac Surgeons, Cardiovascular Anesthesiologists and Perfusionists. Its educational objectives include - the natural history, pathology and treatment options of aortic dis-
ease - updates on perioperative organ protection- the current surgical trends and treatment for, as well as recognise
the risk factors associated with, aneurysms and dissection - prevention and treatment of perioperative complications- the newest surgical and device treatments for aortic valve disease - anesthesiological techniques- the state-of-the-art in open surgery for aortic disease - definition of fit and unfit patients- the current endovascular treatments available for aortic disease - the latest in hybrid treatment for thoraco-abdominal and arch an-
eurysmsMoreover, a parallel Nursing Symposium will offer educational ses-sions to improve nursing practice in the management of critical aor-tic diseased patients also this year.We look forward to welcoming you to the 4th International Congress Aortic Surgery and Anesthesia “How to do it” to be held on December 17th-18th, 2010 at the San Raffaele Scientific Institute in Milano.

245
proceedingsin Intensive Care
Cardiovascular Anesthesia
Endorsed by
proceedings
Appropriate use of fluid infusion in cardiac surgery patients is of primary importance in the perioperative period in order to optimize cardiac output and oxygen delivery and to reduce the use of vas-pressors and inotropes. Fluid infusion is usually triggered by arte-rial hypotension, low urine output and signs of inadequate tissue oxygenation (e.g. hyperlactatemia). This general rule, however, may not be applied when the heart is working in the flat part of the Frank Starling curve, where hypervol-emia may cause excessive increase of filling pressures and tissue ede-ma. In this light, it is mandatory to carefully dose the exact amount of fluids to administer in order to avoid the risk of volume overload. In this issue of HSR Proceedings in Intensive Care and Cardiovascular Anesthesia, Arora and co-workers shed some light on the issue of perioperative fluid administration to cardiac surgery patients and its correlation to mortality (1). The authors clearly showed how the effects of intravascular filling correlates with mortality, especially if the amount of given fluids exceeded four litres in the perioperative period. This effect remained significant even after adjustment for the presence of acute kidney injury and/or hypotensive events.The authors did not specify if the nature of infused fluids had a role on patients outcomes nor if specific treatments such as early/aggres-sive perioperative ultrafiltration might inversely correlate with mor-tality. More than five years ago, data coming from the Prospective Pediatric Continuous Renal Replacement Therapy registry showed that survival rates in patients with multiorgan dysfunction syndrome were significantly better for patients with less than 20% fluid over-load (58% vs 40% survival rate) at continuous renal replacement therapy initiation (2). Fluid balance is probably underestimated in critically ill adults where a huge fluid volume amount is infused in order to target hypovolemia and organ perfusion. Few clinical inves-
Invi
ted
edit
oria
l The issue of fluid balance and mortalityZ. Ricci1, S. Romagnoli2 1Department of Pediatric Cardiac Surgery, Bambino Gesù Children’s Hospital, Rome, Italy;2Department of Cardiac and Vascular Anesthesia and Post-Surgical Intensive Care Unit, Careggi Hospital, Florence, Italy
Corresponding author:Zaccaria RicciDepartment of Pediatric Cardiac SurgeryBambino Gesù Chldren’s HospitalPiazza S.Onofrio, 4 - 00165 Rome, Italye.mail: [email protected]
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010; 2: 245-247
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2

246
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
InVITed edIToRIAl
tigations, until now, have evaluated the impact that fluid balance has on clinical outcomes in critically ill adults: the Sepsis Occurrence in Acutely Ill Patients (SOAP) study (3) and the PICARD (Program to Improve Care in Acute Renal Disease) study group (4) recently showed how critically ill patients with acute kidney injury and fluid overload experienced significantly higher mortality with respect of patients without fluid overload apart from the need for RRT. The work from Arora and co-authors seems to support, in the specific setting of cardiac surgery patients, the view that there might be a survival benefit from conservative approach to intra-operative in-travascular volume expansion. Early initiation of continuous renal replacement therapies to prevent fluid accumulation and overload in critically ill patients, once initial fluid resuscitative management has been accomplished might be an alternative approach (5) in this light, fluid overload is evolving as a primary trigger/indicator for extracorporeal fluid removal, and this may be independent of dose delivery or solute clearance. Another final aspect of the study from Arora must be highlighted: if it is true that extra volume provision was detrimental also in pa-tients without acute kidney injury and/or hemodynamic instability, it must be said that in these last patients correlation between fluid overload and mortality was exponentially higher. If it is evident that counterbalancing fluid accumulation, particularly in patients with oliguria or established acute kidney injury might be beneficial, on the other side it is also clear that more severely ill patients might often miss any active attempt of achieving a negative balance and we do not know if increasing vasopressors dose might really improve survival of such patients. Once a need for increased cardiac output is considered, it is helpful to have an indicator of fluid responsiveness. Central venous pressure and pulmonary artery occlusion pressure have limited predictive value as indicators of fluid responsiveness (with respect to volumetric-echocardiographic estimations) due to the existence of different conditions affecting the distribution of blood volumes (6). Normally, approximately 70% of the total blood resides in the small venules and veins (unstressed volume). Only the remaining 25-30% (1.2-1.4 l) of the total blood volume (stressed volume) determinates, with the elastic recoil of the vasculature, the mean systemic filling pressure that is, with the right atrial pressure , the main determinant of the venous return, and finally of the cardiac output (7). Cardiac surgery procedures and cardiopulmonary bypass deeply influence the venous return and the cardiac output by increasing the venous capacitance and right atrial pressure for different reasons (systemic inflammation, anesthetic drugs, mechanical ventilation). An in-crease in venous capacitance may cause a reduction in stressed vol-

The issue of fluid balance and mortality
247
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
ume and an increase in unstressed volume: the final result may be a reduction of cardiac output due to a relative hypovolemia. It seems that some patients (i.e. in case of bleeding) may actually benefit from an increase in mean systemic filling pressure (volume load) whereas in others a venous capacitance reduction (anti-inflam-matory strategies, vasopressors, conservative fluid infusion) should be encouraged. More recently, the use of respiratory variations of arterial pressure (systolic pressure variation, stroke volume variation, pulse pressure variation) to predict fluid responsiveness, have shown some inter-esting data in both operating theatres and intensive care units (8).Unfortunately, these dynamic indices, robust and reliable under spe-cific conditions (closed chest, controlled mechanical ventilation, si-nus rhythm) have not been validated during open chest settings. In this light, low cardiac output in cardiac surgery patients should be managed with a multimodal monitoring (echocardiography, cardiac and vascular filling pressures, dynamic indices of fluid responsive-ness) and treatment tailored to the single patient and clinical picture trying to obtain the best balance between fluids, inotropes and vaso-pressors during the whole intra and post-operative phase.
REFERENCES
1. A. Pradeep, S. Rajagopalam, HK Koll, et al. High volumes of intravenous fluid during cardiac surgery are associated with increased mortality. HSR Proceedings in Inten-sive Care and Cardiovascular Anesthesia 2010; 2: 287-296.
2. Foland JA, Fortenberry JD, Warshaw BL, et al. Fluid overload before continuous he-mofiltration and survival in critically ill children: a retrospective analysis. Crit Care Med. 2004; 32: 1771-1776.
3. Payen D, de Pont AC, Sakr Y, et al. Sepsis Occurrence in Acutely Ill Patients (SOAP) Investigators. A positive fluid balance is associated with a worse outcome in patients with acute renal failure. Crit Care 2008; 12: 169.
4. Bouchard J, Soroko SB, Chertow GM, et al. Program to Improve Care in Acute Renal Disease (PICARD) Study Group. Fluid accumulation, survival and recovery of kid-ney function in critically ill patients with acute kidney injury. Kidney Int 2009; 76: 422-427.
5. Rivers EP, Coba V, Whitmill M. Early goal-directed therapy in severe sepsis and sep-tic shock: a contemporary review of the literature. Curr Opin Anaesthesiol 2008; 21: 128-140.
6. Osman D, Ridel C, Ray P, et al. Cardiac filling pressures are not appropriate to pre-dict hemodynamic response to volume challenge. Crit Care Med 2007; 35: 64-68.
7. Maas JJ, Geerts BF, van den Berg PC, et al. Assessment of venous return curve and mean systemic filling pressure in postoperative cardiac surgery patients. Crit Care Med 2009; 37: 1-7.
8. Teboul JL, Monnet X. Detecting volume responsiveness and unresponsiveness in in-tensive care unit patients: two different problems, only one solution. Crit Care 2009; 13: 175.

Recordati è un gruppo farma-ceutico europeo fondato nel1926, quotato alla BorsaItaliana, con oltre 2800 dipen-denti, che si dedica alla ricer-ca, allo sviluppo, alla produ-zione e alla commercializza-zione di prodotti farmaceuticiin varie aree terapeutiche:antibioticoterapia e antivirali,broncopneumologia, cardiova-scolare, dermatologia, gastro-enterologia, ginecologia, neu-ropsichiatria, reumatologia eterapia del dolore, urologia,compresa un’attività specializ-zata nelle malattie rare.
I prodotti del GruppoRecordati sono presenti inoltre 100 Paesi.
La fiducia nel presenteLo sguardo nel futuro
200*270 2-07-2010 17:54 Pagina 1

249
proceedingsin Intensive Care
Cardiovascular Anesthesia
Endorsed by
proceedings
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
ReVIew ARtICle
Corresponding author:Gregory Fischer, M.D.Associate Professor, Department of AnesthesiologyThe Mount Sinai School of MedicineOne Gustave L. Levy Place, Box 1010e.mail: [email protected]
INtRODUCtION
Cardiac and major vascular surgery (CMVS) have entered their sixth decade of existence. During this time period, great strives have occurred towards increasing patient safety by developing and employ-ing reliable hemodynamic and respiratory monitors. Interestingly, the monitoring of cerebral function was slow to evolve and has only recently been able to keep pace with these other advances. The problem has not been lack of the interest, but rather the logistics of not having reliable technol-ogy for continuous monitoring of the cen-tral nervous system (CNS) in the operating room and intensive care unit.
Adverse CNS outcomes following CMVS are classified into two categories: Type I (cerebral death, non-fatal stroke, focal in-jury, stupor, encephalopathy, coma and new transient ischemic attack); Type II (deterioration in cognitive function, defi-cit in memory or seizures). The incidence of these complications varies according to type of surgery, co-morbidites and age. CNS complications are associated with increased mortality, length of hospitalization, and use of long-term facilities with substantial es-timated cost per year. Multiple approaches have been utilized to address neurological complications, though definitive therapeu-tic strategies are lacking.The etiology of these neurological com-plications is multifactorial. In operations without cardio pulmonary bypass (CPB): Hypotension, anemia, low oxygen satura-tion, genetic factors, anesthetic agents and previous neurological pathology, are the
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010; 2: 249-256
ABStRACt
We describe the development and current applications of cerebral oximetry (based on near-infrared reflectance spectroscopy) that can be used during cardiac and major vascular surgery to determined brain tissue oxygen saturation. There are presently three cerebral oximetry devices with FDA approval in the United States to measure and monitor cerebral tissue oxygen saturation. 1. INVOS (Somanetics Corporation, Troy, MI - recently COVIDIEN, Boulder, CO); FORE-SIGHT (CAS Medical Systems, Inc. Branford, CT); EQUANOX (Nonin Medical Inc. Minnesota, MN). All devices are portable, non-invasive and easy to use in operating room and intensive care unit. The data provided in these communication may provided information for improvement of perioperative neuromonitoring techniques, and may be crucial in the design of future clinical trials.
Keywords: cerebral oximetry, detection of cerebral hypopefusion or ischemia.
Cerebral oximetry in cardiac and major vascular surgeryG.W. Fischer, G. SilvayDepartment of Anesthesiology, Mount Sinai School of Medicine, New York, NY

250
G.W. Fischer, G. Silvay
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
main culprits. Operations utilizing CPB are associated with embolisation of gaseous and particulate emboli (arterial atheroma) from the surgical site as well as from place-ment and removal of the aortic cross clamp. Additionally, hypoperfusion resulting from loss of cerebral autoregulation, hypoten-sion or anemia can lead to water shed cere-bral hypoperfusion. In order to recognize cerebral ischemia in a timely manner, different monitoring mo-dalities have been introduced into clinical practice over the course of the last two de-cades. Electroencephalographic monitoring (EEG), serial measurements of jugular bulb saturations (jvSO2) and cerebral oximetry based on near infrared spectroscopy have all been reported to successfully identify cerebral ischemia (1-3). An institutional bias leads to heterogene-ity in regards on how to correctly monitor these patients in order to identify the onset of cerebral ischemia. Isoelectricity caused by deep hypothermia or excessive dosage of volatile anesthetic agents renders EEG monitoring useless. JvSO2 measurements require the invasive placement of a jugu-lar bulb catheter. Cerebral oximetry on the other hand is non-invasive, user friendly and not influenced by the depth of anesthe-sia. It can even be utilized as a monitor to detect ischemia in real-time during a circu-latory arrest period (4).This communication will review the devel-opment and current applications of cerebral oximetry that can be used during CMVS to improve peri-operative outcomes.
The evolution of cerebral oximetryJobsis first introduced the idea of using near infrared spectroscopy (NIRS) to non-invasively measure cerebral tissue oxygen-ation in 1977 (5). The principal of NIRS is based on the fact that near-infrared light passes through skin and skull readily and is absorbed by certain biological molecules in
the brain (6, 7). A “biological spectroscopic window” exists at the wavelength range 660-940 nm because only a few chromo-phores like Hb and HbO2 strongly absorb light in this spectra range, allowing light to penetrate tissue to a great distance. In this wavelength range, absorption of light due to other biological compounds and tis-sues such as water, lipids, skin, and bone is lower in magnitude, and these biological compounds generally have a flat absorption spectra when compared to Hb and HbO2. (Figure 1).Cerebral oximetry, based on near-infrared spectroscopy (NIRS) technology, provides information on the availability of oxygen in brain tissue. Cerebral oximetry measures regional cerebral tissue oxygen saturation (SctO2) at the microvascular level. Compli-mentary to the arterial oxygen saturation (SaO2) measured by pulse oximetry, SctO2 reflects regional cerebral metabolism and the balance of local cerebral oxygen sup-ply/demand, leading to the following clini-cal advantages:1. it provides SctO2 values continuously
and noninvasively;2. SctO2 is a sensitive index of cerebral
hypoperfusion, hypoxia and/or cere-bral ischemia, which is one of the main cause of brain injury during CMVS pro-cedures;
3. Cerebral oximeter is portable, easy to use in operating room or at the bedside.
In order to guarantee that only cerebral oxygen saturation is being measured most commercially available oximeters minimize extracerebral contamination by equipping the sensors with 2 light detectors located at fixed distances from the light source. The mean penetration depth of the photons is proportional to the distance between the emitting source and receiving detector. Consequently the detector (scalp or near detector) located closer to the light source measures saturations within the scalp,

Cerebral oximetry in cardiac and major vascular surgery
251
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
whereas the detector located further away measures both cerebral as well as scalp sat-urations (brain or far detector) (Figure 2). By simply subtracting the measurements obtained from the brain detector from the scalp detector, extracerebral contamination can be minimized. There are presently three non-invasive cerebral oximetry devices with FDA ap-proval to measure and monitor cerebral tissue oxygen saturation during the peri-operative period. 1. INVOS cerebral oxim-eter (Somanetics Corporation, Troy, MI). 2. FORE-SIGHT absolute cerebral oximeter (CAS Medical Systems, Branford, CT). 3. NONIN regional oximeter (Nonin Medical Inc. Minnesota, MN). A fourth device, the
Figure 1Near-infrared light passes through skin and skull readily and is absorbed by certain biological molecules in the brain. A “biological spectroscopic window” exists at the wavelength range 660 - 940 nm.
NIRO series near-infrared spectrophotom-eter (Hamamatsu, Photonic. Hamamatsu, Japan), is available in the Japanese and Eu-ropean markets.
INVOS® (Somanetics Corporation, Troy, MI)The INVOS Cerebral Oximeter (Somanet-ics Corporation, Troy, MI - from July 2010 COVIDIEN, Boulder, CO) (Figure 3) has been commercially available since 1993 and the sixth generation model is the only oximeter to display four channels simulta-neously, enabling the clinician to track ce-rebral as well as somatic (body) tissue oxy-gen saturations. The INVOS uses two wavelengths of infra-

252
G.W. Fischer, G. Silvay
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
red light (730 and 810 nm) from light-emit-ting diodes (LEDs) (8). The INVOS has dis-posable sensors, which contain LEDs and two light detectors at fixed distances from the light source. The device calculates and displays the value of regional cerebral oxy-gen saturation (rSO2). Most publications showing the benefit of using the Invos to monitor cerebral oxygenation during car-diac surgery have used it as a trend moni-
torErrore: sorgente del riferimento non tro-vata. This means that clinical interventions were based on changes of rSO2 from the initial baseline value, which was obtained at pre-induction of anesthesia (9).
FORE-SIGHT® (CAS Medical Systems, Inc. Branford, CT)The FORE-SIGHT® Absolute Cerebral Oximeter (Figure 4) has been commer-cially available since 2007 (10). The FORE-SIGHT monitor is a continuous wave (CW) spatially resolved near infrared spectrom-eter that measures absolute cerebral tissue oxygen saturation (SctO2%). This device has two channels for bilateral brain moni-toring. In contrast to the other devices cur-rently available, the FORE-SIGHT uses La-ser light at a FDA deemed safe level (Class I laser) to project four precise (bandwidth <1nm) wavelengths (690, 780, 805, & 850 nm) into the brain to capture information needed for the algorithm to calculate the absolute value of cerebral tissue oxygen saturation (SctO2). The advantage of add-ing additional wavelengths makes it pos-
Figure 3INVOS.
Figure 2By subtracting the measurements obtained from the brain detector from the scalp detector, extracererbal contamination can be minimized.

Cerebral oximetry in cardiac and major vascular surgery
253
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
sible to compensate for scattering losses, and to account for interference from other background light absorbers (11) (such as fluid, tissue and skin pigmentation). Con-sequently, the FORE-SIGHT is capable of measuring cerebral tissue oxygen satura-tion more precicely precisely than the IN-VOS (12). This advance in technology is the basis for enabling the device to reliably measure absolute values of SctO2. This, in turn, eliminates the need to establish pre-induction baseline measurements and en-ables the use of threshold values to guide clinical interventions.
EQUANOX® (Nonin Medical Inc. Minnesota, MN)The most recent device to emerge onto the market in the United States is the EQUAN-OX (Figure 5). FDA approval was granted in the summer of 2009. The EQUANOX uses LED technology to transmit three-wavelengths (730 nm, 810 nm and 880 nm) (13). The EQUANOX sensor differs from the INVOS and FORE-SIGHT sensors be-
cause it is equipped with dual emitter sites, enabling a crisscrossing in the transmission of the photons. According to the company this technology eliminates the challenges of surface variability by having the LEDs illuminate alternately leading to improved accuracy. Due to the novelty of the device studies confirming reliability and efficacy are not yet available. A calibration and vali-dation study from MacLeod and colleagues shows that the EQUANOX provides, simi-lar to the INVOS, an accurate measure of trends in cerebral oxygen saturation, how-ever falls short of obtaining absolute mea-surements (14).
Applications of cerebral oximetry monitoringAs previously described, commercially available cerebral oximetry devices have been available since the early 1990s, how-ever, most reports of the utility of cerebral oximetry during the early years focused on their ability to recognize catastrophic events. The literature is filled with such
Figure 4FORE-SIGHT.
Figure 5EQUANOX.

254
G.W. Fischer, G. Silvay
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
case reports (15-18). While the importance of a monitor that can alert the clinician to an otherwise unrecognized catastrophic event cannot be underscored the true sci-entific advances in the field started to take place during the last 5 years. Attempts at utilizing cerebral oximetry to improve clini-cal outcomes and shorten hospital length of stay are now the focus of most investigators within the field.Goldman and colleagues were the first to report that by optimizing cerebral oxygen-ation to maintain saturations around the pre-induction baseline that the treatment group demonstrated a significantly lower incidence of permanent stroke (19). This study however was not without undeniable weaknesses. The study was non-random-ized and retrospective in design. The con-trol group consisted of a historical cohort. Patients that underwent cardiac surgery 18 months prior to the introduction of cerebral oximetry at the author’s institution were subsequently compared with the treatment group which consisted of patients enrolled during the following 18 months. Addition-ally, the authors acknowledge that they were unable to determine how close rSO2 values were maintained to baseline val-ues during the course of surgery. Despite these shortcomings one could argue, as the authors pointed out, that better compli-ance with a predefined target value would translate into potentially better outcomes. The fact that the study group consisted of patients with more co-morbidities, yet had a lower incidence of permanent stroke, de-creased need for prolonged ventilation and shorter length of hospital stay is impressive.To date the best trial supporting the effi-cacy of monitoring and optimizing cerebral oxygenation was published by Murkin et al. in 2007. This randomized, blinded study of 200 CABG patients demonstrated pro-spectively that rSO2 (INVOS® Somanetics) monitoring is associated with a significant
improvement in overall outcome after car-diac surgery (20). Murkin utilized an intra-operative management protocol designed to maintain rSO2 values at or above 75% of the preinduction baseline. The results were associated with a significant improvement in overall organ function and decreased postoperative length of stay. While the study was underpowered to show signifi-cant difference in stroke rates between the intervention and control groups, the idea that cerebral oximetry could be used as a surrogate marker for overall organism well being was introduced. Slater and colleagues showed that an increase in post opera-tive neurocognitive dysfunction (POCD) was seen in patients with an increase in rSO2 desaturation score of greater than 3,000%-second (21). They also were able to associate a near threefold increase in risk of prolonged hospital stay. Unfortunately due to flawed study design no difference was seen between the intervention and control groups regarding outcome difference.In another randomized prospective study of elderly patients undergoing major ab-dominal surgery, Casati et al. (22) reported on improved mini mental scores (MMS), more rapid PACU discharge, and shortened length of hospital stay in 122 geriatric pa-tients after major abdominal surgery in which cerebral oximetry was monitored and optimized. While the utilization of the MMS to address postoperative cognitive impairment is crude, this study did demon-strate that 20% of all patients experienced a decrease in rSO2 (INVOS® Somanetics) below 75% of baseline without any change in systemic oxygenation (SpO2).In a recently published observational study of patients undergoing aortic arch surgery with hypothermic circulatory arrest (HCA) (Figure 6), Fischer and colleagues were able to support similar findings that other inves-tigators found in the CABG population (23). Time spent beneath threshold values as

Cerebral oximetry in cardiac and major vascular surgery
255
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
well as the area under the threshold (AUT) were significantly associated with adverse outcomes as well as time on ventilator, in-tensive care unit and hospital length of stay. In line with Casati’s findings, Fischer found that the risk of obtaining an adverse event doubled with ever decade of life. a finding that supports the overall belief that the ge-riatric population is more susceptible and prone to the effects of cerebral ischemia. Additionally, the investigators found that patients who spent more than 30 minutes under the threshold value of 60% had an in-creased cost of care of $8,300. Mathematical models, such as the one de-scribed by Fischer et al. (24) could potential-
ly make the technique of circulatory arrest safer and more predictable. Knowledge of the rate of cerebral desaturation can be used, in conjunction with the knowledge obtained from the threshold paper (23), to predict al-lowable duration of HCA prior to the occur-rence of adverse events. In summary, cere-bral oximetry is a non-invasive technology that has the potential to provide the clini-cian with information to tailor management during the perioperative period. Studies are emerging linking optimization of cerebral saturation with improved outcomes, short-ened length of stay and reduction in cost.
No conflict of interest is acknowledged by the authors.
Figure 6Intraoperative SctO2 course of a patient undergoing aortic arch surgery with hypothermic circulatory arrest. Note dependency of SctO2 to CO2. Insufflation of CO2 during endoscopic vein harvesting leading to increase in SctO2 as well as decline in SctO2 once mechanical ventilation was started.CPB = cardiopulmonary bypass; DHCA = deep hypothermic circulatory arrest.

256
G.W. Fischer, G. Silvay
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
ReFeReNCeS
1. Leggat CS, Fischer GW. Early detection of an acute cerebral event during cardiopulmonary bypass using a bispectral index monitor. Semin Cardiothorac Vasc Anesth 2008; 12: 80-82.
2. Reich DL, Horn LM, Hossain S, Uysal S. Us-ing jugular bulb oxyhemoglobin saturation to guide onset of deep hypothermic circulatory arrest does not affect post-operative neuropsy-chological function. Eur J Cardiothorac Surg 2004; 25: 401-406.
3. Fischer GW. Recent advances in application of cerebral oximetry in adult cardiovascular sur-gery. Semin Cardiothorac Vasc Anesth 2008; 12: 60-69.
4. Fischer GW, Benni PB, Lin HM, et al. Math-ematical model for describing cerebral oxy-gen desaturation in patients undergoing deep hypothermic circulatory arrest. Br J Anaesth 2010; 104: 59-66.
5. Jobsis FF. Noninvasive, infrared monitoring of cerebral and myocardial oxygen sufficiency-and circulatory parameters. Science 1977; 198: 1264-1267.
6. Silvay G, Weinreich A, Owitz S, et al. The ce-rebral function monitoring during open-heart surgery. Herz 1978; 3: 270-275.
7. McCormick PW, Stewart M, Ray P, et al. Mea-surement of regional cerebrovascular haemo-globin oxygen saturation in cats using optical spectroscopy. Neurological Res 1991; 13: 65-70.
8. Thavasothy M, Broadhead M, Elwell C, et al. A comparison of cerebral oxygenation as mea-sured by the NIRO 300 and the INVOS 5100 Near-Infrared Spectrophotometers. Anaesthe-sia 2002; 57: 999-1006.
9. Schell RM, Cole DJ. Cerebral monitoring: jugu-lar venous oximetry. Anesthesia & Analgesia 2000; 90: 559-566.
10. www.casmed.com11. Strangman G, Boas DA, Sutton JP. Non-inva-
sive neuroimaging using near-infrared light. Soc of Biol Psych 2002; 52: 679-693.
12. MacLeod D, Ikeda K, Vacchiano C. Simultane-ous comparison of FORE-SIGHT and INVOS cerebral oximeters to jugular bulb and arterial co-oximetry measurements in healthy volunteers. Anesth Analg 2009; 108 (SCA Suppl): SCA 56.
13. www.nonin.com14. MacLeod D, Ikeda K, Vacchiano C. Simultane-
ous Comparison of FORE-SIGHT and INVOS Cerebral Oximeters to Jugular Bulb and Arte-rial Co-Oximetry Measurements in Healthy Volunteers. ANESTH ANALG 2009; 108(SCA Suppl): 1-104.
15. Han SH, Kim CS, Lim C, Kim WH. Obstruc-tion of the Superior Vena Cava Cannula De-tected by Desaturation of the Cerebral Oxim-eter. J Cardiothorac Vasc Anesth. 2005; 19: 420-421.
16. Orihashi K, Sueda T, Okada K, Imai K. Malpo-sition of selective cerebral perfusion catheter is not a rare event. Eur J Cardiothorac Surg 2005; 27: 644-648.
17. Rodriguez RA, Cornel G, Semelhago L, et al. Cerebral effects in superior vena caval cannula obstruction: the role of brain monitoring. Ann Thorac Surg 1997; 64: 1820-1822.
18. Fischer GW, Stone ME. Cerebral air embolism recognized by cerebral oximetry. Semin Car-diothorac Vasc Anesth 2009;13:56-59.
19. Goldman S, Sutter F, Ferdinand F, Trace C. Optimizing intraoperative cerebral oxygen delivery using noninvasive cerebral oximetry decreases the incidence of stroke for cardiac surgical patients. Heart Surg Forum 2004; 7: 376-381.
20. Murkin JM, Adams SJ, Novick RJ, et al. Moni-toring brain oxygen saturation during coro-nary bypass surgery: a randomized, prospec-tive study. Anesth Analg. 2007; 104: 51-58.
21. Slater JP, Guarino T, Stack J, et al. Cerebral oxygen desaturation predicts cognitive decline and longer hospital stay after cardiac surgery. Ann Thorac Surg 2009; 87: 36-44.
22. Casati A, Fanelli G, Pietropaoli P, et al. Con-tinuous monitoring of cerebral oxygen satu-ration in elderly patients undergoing major abdominal surgery minimizes brain exposure to potential hypoxia. Anesth Analg 2005; 101: 740-747.
23. Fischer GW, Lin HM, Krol M, et al. Noninva-sive cerebral oxygenation may predict outcome in patients undergoing aortic arch surgery. J Thorac Cardiovasc Surg 2010. Epub ahead of print. PMID: 20579669.
24. Fischer GW, Benni PB, Lin HM, et al. Math-ematical model for describing cerebral oxy-gen desaturation in patients undergoing deep hypothermic circulatory arrest. Br J Anaesth 2010; 104: 59-66.


L’infezione sternale è uno dei principali rischi di morbidità e mortalità post operatorie in cardiochirurgia: il 4,7% dei pazienti sottoposti a sternotomia mediana soffre di infezione sternale durante e dopo l’ospe-dalizzazione (1). Il corsetto post-operatorio indossabile Posthorax® PRO M-XL stabilizza il torace del paziente generando una compressione dorso-ventrale e riducendo i movimenti relativi tra le due metà dello sterno, in partico-lar modo la rotazione.
Uno studio condotto su 586 pazienti dimostra che l’uso corretto di Posthorax® PRO M-XL abbatte l’incidenza delle complicanze dovute a instabilità sternale del 93,3% (2).
È nato prima l’uovo o la gallina?
È l’instabilità sternale a causare la deiscenza o viceversa?
È nato prima
LA RISPOSTA È:
Costi ospedalieri aggiuntivi (per paziente in €)Numero di complicanze (2)25
20
15
10
5
0
1
5
8
81
Senza Con Posthorax Posthorax
Deiscenza
Infezione super� ciale
Infezione profonda
Reintervento
400000
350000
30000
25000
20000
15000
10000
5000
0
35600
1590013200
37002800
Antibiotici
VAC
Reintervento
Degenza
Totale
PRO M-XL
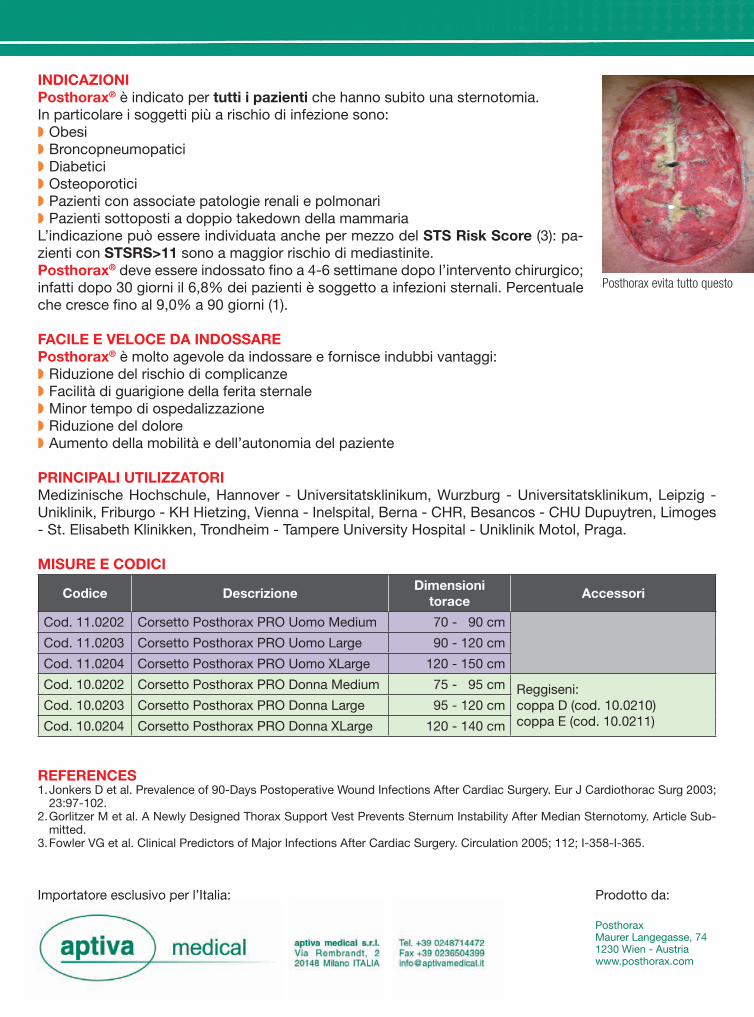
INDICAZIONIPosthorax® è indicato per tutti i pazienti che hanno subito una sternotomia.In particolare i soggetti più a rischio di infezione sono:◗ Obesi◗ Broncopneumopatici◗ Diabetici◗ Osteoporotici◗ Pazienti con associate patologie renali e polmonari◗ Pazienti sottoposti a doppio takedown della mammariaL’indicazione può essere individuata anche per mezzo del STS Risk Score (3): pa-zienti con STSRS>11 sono a maggior rischio di mediastinite.Posthorax® deve essere indossato � no a 4-6 settimane dopo l’intervento chirurgico; infatti dopo 30 giorni il 6,8% dei pazienti è soggetto a infezioni sternali. Percentuale che cresce � no al 9,0% a 90 giorni (1).
FACILE E VELOCE DA INDOSSAREPosthorax® è molto agevole da indossare e fornisce indubbi vantaggi:◗ Riduzione del rischio di complicanze◗ Facilità di guarigione della ferita sternale◗ Minor tempo di ospedalizzazione◗ Riduzione del dolore◗ Aumento della mobilità e dell’autonomia del paziente
PRINCIPALI UTILIZZATORIMedizinische Hochschule, Hannover - Universitatsklinikum, Wurzburg - Universitatsklinikum, Leipzig - Uniklinik, Friburgo - KH Hietzing, Vienna - Inelspital, Berna - CHR, Besancos - CHU Dupuytren, Limoges - St. Elisabeth Klinikken, Trondheim - Tampere University Hospital - Uniklinik Motol, Praga.
MISURE E CODICI
Codice DescrizioneDimensioni
toraceAccessori
Cod. 11.0202 Corsetto Posthorax PRO Uomo Medium 70 - 90 cm
Cod. 11.0203 Corsetto Posthorax PRO Uomo Large 90 - 120 cm
Cod. 11.0204 Corsetto Posthorax PRO Uomo XLarge 120 - 150 cm
Cod. 10.0202 Corsetto Posthorax PRO Donna Medium 75 - 95 cm Reggiseni:coppa D (cod. 10.0210) coppa E (cod. 10.0211)
Cod. 10.0203 Corsetto Posthorax PRO Donna Large 95 - 120 cm
Cod. 10.0204 Corsetto Posthorax PRO Donna XLarge 120 - 140 cm
REFERENCES1. Jonkers D et al. Prevalence of 90-Days Postoperative Wound Infections After Cardiac Surgery. Eur J Cardiothorac Surg 2003;
23:97-102.2. Gorlitzer M et al. A Newly Designed Thorax Support Vest Prevents Sternum Instability After Median Sternotomy. Article Sub-
mitted.3. Fowler VG et al. Clinical Predictors of Major Infections After Cardiac Surgery. Circulation 2005; 112; I-358-I-365.
Posthorax evita tutto questo
PosthoraxMaurer Langegasse, 741230 Wien - Austria www.posthorax.com
Importatore esclusivo per l’Italia:Importatore esclusivo per l’Italia: Prodotto da:


261
proceedingsin Intensive Care
Cardiovascular Anesthesia
Endorsed by
proceedings
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
ORIGINAL ARTICLE
Corresponding author:Prof. Roberto Chiesa, MDIRCCS H. San RaffaeleDepartment of Vascular SurgeryVia Olgettina, 60 e.mail: [email protected]
INTRODUCTION
Thoracic endovascular aortic repair (TE-VAR) could reduce perioperative mor-tality and pulmonary, cardiac and renal complications when compared to open re-pair. Furthermore, most of the past series
data included devices that will soon not be marketed anymore. In an ironic way, these data are loosing their value exactly in the moment they have the most to say. We therefore can speculate further TEVAR outcomes improvements with the newest updated devices. In this paper we present our experience in the management of patients with descend-ing thoracic aortic aneurysm undergoing TEVAR, including preoperative imaging modalities, endovascular procedures tech-niques, follow up, results and complica-tions.
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010; 2: 261-270
ABSTRACT
Introduction: Current strategies for repair of descending thoracic aortic aneurysms consist of open repair with surgical graft replacement or thoracic endovascular aortic repair. We review and update our overall experi-ence in aortic thoracic diseases and specifically analyzed our outcomes with thoracic endovascular aortic repair in patients with descending thoracic aortic aneurysms. Methods: From 1993 to present a total of 1144 patients were treated in our Center for pathology involving the thoracic aorta. Since 1998, 322 patients underwent thoracic endovascular aortic repair, and among this group, in 188 cases the descending aorta was involved. In 74% of patients treated for a descending thoracic aortic le-sion, a degenerative aneurysm was observed. Results: In patients with descending thoracic aortic aneurysms receiving thoracic endovascular aortic repair, our technical success rate, i.e. deployment of endograft with complete exclusion of the lesion/minimal en-doleak, was 99.5% (one case required emergent open conversion) with a perioperative mortality of 2.6% (five patients). The rate of spinal cord ischemia, manifesting either as paraplegia or paraparesis, was 4.7%. Delayed onset spinal cord ischemia ameliorated with adequate arterial pressure and cerebrospinal fluid drainage. Conclusions: Our experience of selected patients undergoing thoracic endovascular aortic repair of descend-ing thoracic aorta aneurysms is satisfactory with very low mortality and morbidity. A large use of thoracic endovascular aortic repair is foreseen in the next future.
Keywords: thoracic aortic aneurysm, endovascular aortic repair, aortic endoprostheses, thoracic aortic aneurysms, type B aortic dissection.
Endovascular treatment of descending thoracic aneurysmsR. Chiesa, E. Civilini, Y. Tshomba, E.M. Marone, L. Bertoglio, D. Baccellieri, G. Coppi, D. Logaldo, G. MelissanoDepartment of Vascular Surgery, Università Vita-Salute San Raffaele, Milan, Italy
262
R. Chiesa et al.
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
METHODS
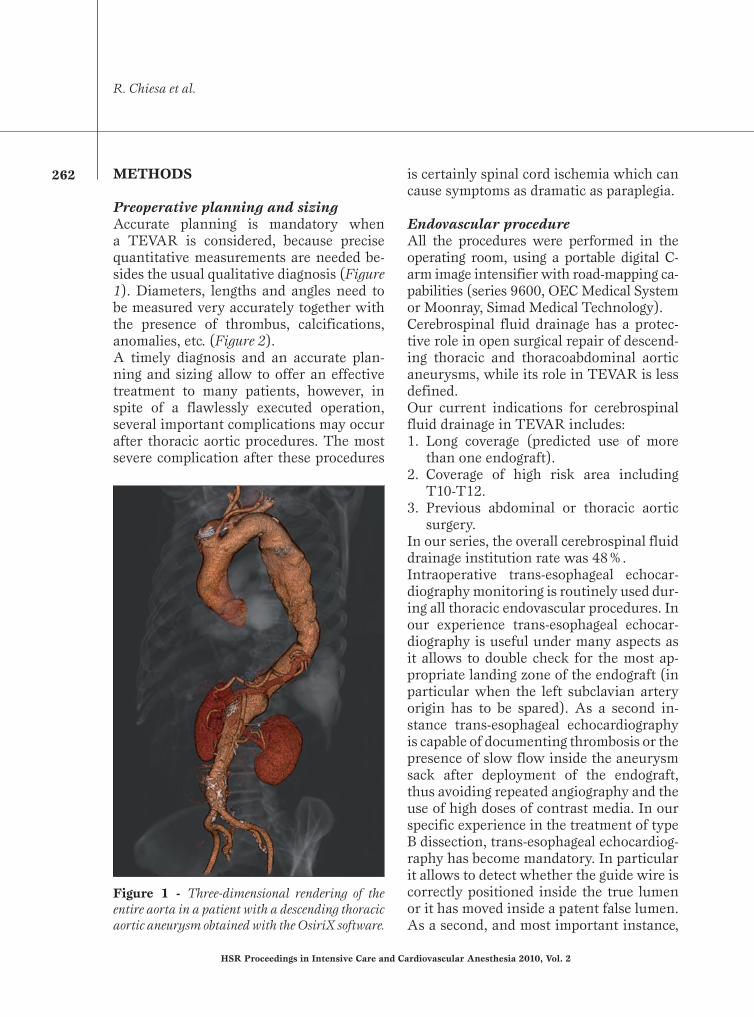
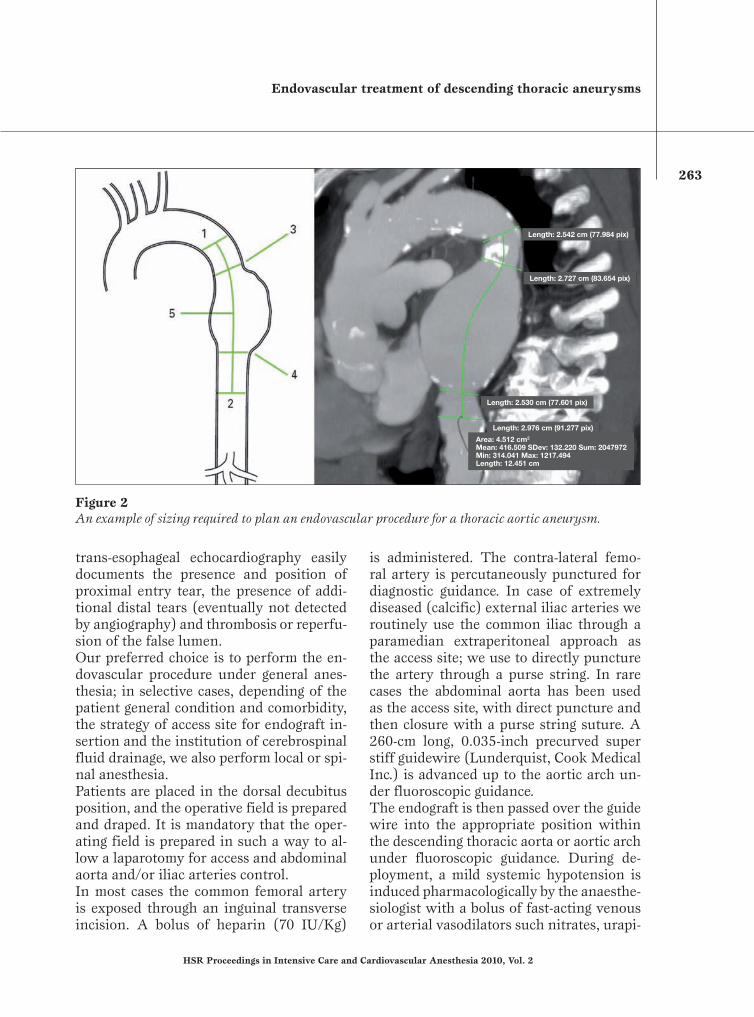
Preoperative planning and sizingAccurate planning is mandatory when a TEVAR is considered, because precise quantitative measurements are needed be-sides the usual qualitative diagnosis (Figure 1). Diameters, lengths and angles need to be measured very accurately together with the presence of thrombus, calcifications, anomalies, etc. (Figure 2).A timely diagnosis and an accurate plan-ning and sizing allow to offer an effective treatment to many patients, however, in spite of a flawlessly executed operation, several important complications may occur after thoracic aortic procedures. The most severe complication after these procedures
is certainly spinal cord ischemia which can cause symptoms as dramatic as paraplegia.
Endovascular procedureAll the procedures were performed in the operating room, using a portable digital C-arm image intensifier with road-mapping ca-pabilities (series 9600, OEC Medical System or Moonray, Simad Medical Technology).Cerebrospinal fluid drainage has a protec-tive role in open surgical repair of descend-ing thoracic and thoracoabdominal aortic aneurysms, while its role in TEVAR is less defined. Our current indications for cerebrospinal fluid drainage in TEVAR includes: 1. Long coverage (predicted use of more
than one endograft).2. Coverage of high risk area including
T10-T12.3. Previous abdominal or thoracic aortic
surgery.In our series, the overall cerebrospinal fluid drainage institution rate was 48%.Intraoperative trans-esophageal echocar-diography monitoring is routinely used dur-ing all thoracic endovascular procedures. In our experience trans-esophageal echocar-diography is useful under many aspects as it allows to double check for the most ap-propriate landing zone of the endograft (in particular when the left subclavian artery origin has to be spared). As a second in-stance trans-esophageal echocardiography is capable of documenting thrombosis or the presence of slow flow inside the aneurysm sack after deployment of the endograft, thus avoiding repeated angiography and the use of high doses of contrast media. In our specific experience in the treatment of type B dissection, trans-esophageal echocardiog-raphy has become mandatory. In particular it allows to detect whether the guide wire is correctly positioned inside the true lumen or it has moved inside a patent false lumen. As a second, and most important instance,
Figure 1 - Three-dimensional rendering of the entire aorta in a patient with a descending thoracic aortic aneurysm obtained with the OsiriX software.
Endovascular treatment of descending thoracic aneurysms
263
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
trans-esophageal echocardiography easily documents the presence and position of proximal entry tear, the presence of addi-tional distal tears (eventually not detected by angiography) and thrombosis or reperfu-sion of the false lumen. Our preferred choice is to perform the en-dovascular procedure under general anes-thesia; in selective cases, depending of the patient general condition and comorbidity, the strategy of access site for endograft in-sertion and the institution of cerebrospinal fluid drainage, we also perform local or spi-nal anesthesia. Patients are placed in the dorsal decubitus position, and the operative field is prepared and draped. It is mandatory that the oper-ating field is prepared in such a way to al-low a laparotomy for access and abdominal aorta and/or iliac arteries control.In most cases the common femoral artery is exposed through an inguinal transverse incision. A bolus of heparin (70 IU/Kg)
is administered. The contra-lateral femo-ral artery is percutaneously punctured for diagnostic guidance. In case of extremely diseased (calcific) external iliac arteries we routinely use the common iliac through a paramedian extraperitoneal approach as the access site; we use to directly puncture the artery through a purse string. In rare cases the abdominal aorta has been used as the access site, with direct puncture and then closure with a purse string suture. A 260-cm long, 0.035-inch precurved super stiff guidewire (Lunderquist, Cook Medical Inc.) is advanced up to the aortic arch un-der fluoroscopic guidance.The endograft is then passed over the guide wire into the appropriate position within the descending thoracic aorta or aortic arch under fluoroscopic guidance. During de-ployment, a mild systemic hypotension is induced pharmacologically by the anaesthe-siologist with a bolus of fast-acting venous or arterial vasodilators such nitrates, urapi-
Figure 2An example of sizing required to plan an endovascular procedure for a thoracic aortic aneurysm.
Length: 2.542 cm (77.984 pix)
Length: 2.727 cm (83.654 pix)
Length: 2.530 cm (77.601 pix)
Length: 2.976 cm (91.277 pix)
Area: 4.512 cm2
Mean: 416.509 SDev: 132.220 Sum: 2047972Min: 314.041 Max: 1217.494Length: 12.451 cm

264
R. Chiesa et al.
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
Figure 3Three-dimensional computed tomography angiography (3D CTA) of thoracic aortic aneurysm exclusion. In the box is visible the endoluminal reconstruction of 3D CTA: note that proximal stent lays at the origin of left carotid artery without covering it.

Endovascular treatment of descending thoracic aneurysms
265
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
dil. Nitroprusside or adenosine-induced asystole is never used. After deployment of the endograft on the selected location a completion angiogram is performed.The wounds are closed as our standard practice. Special care is mandatory when removing the introducer sheath, as rupture of the external iliac artery at its origin is more likely to happen with thoracic endo-grafts. It is particularly advisable to leave the guide wire in place until the sheath is completely removed in order to perform an emergent endoclamp in case of iliac rup-ture.
EndograftThe objective of a device intended for treat-ment of an aortic aneurysm is clear cut: it must prevent aneurysm rupture. This is achieved by effectively excluding the aneu-rismal sac from circulation, in the absence of blood flow and pressure within the sac, thrombus will form and with time the sac itself may regress or disappear altogether. For aortic dissection the degree of uncer-tainty is greater, in uncomplicated acute cases without dilatation of the aortic wall, closure of the proximal intimal tear may achieve healing of the aorta. However the device itself may produce additional tears at both the proximal and distal level of the fragile diseased aorta. Most currently avail-able endografts are not primarily intended for the treatment of this condition espe-cially if they carry proximal or distal un-covered stents, hooks or barbs. For chronic cases, closure of the intimal tear may pro-duce thrombosis of the false lumen. Stabi-lization of the flap and enlargement of the true lumen are also desirable. It must be re-membered that effective obliteration of the false lumen may compromises the circula-tion to arteries that arise from the false lu-men itself (i.e. left renal artery), flow to all important vessels must therefore be veri-fied and additional procedures (i.e. stent-
ing) may be necessary to restore flow in these vessels. In most other cases the use of aortic en-dografts is off label and experimental; for instance experience with endovascular treatment of traumatic lesions, penetrating ulcers, intra-mural hematoma is increasing and a few cases have been described in the literature.
Follow-up Once an endograft has been successfully implanted, the patients need to undergo fol-low up imaging to confirm that everything is working properly, and if something is wrong, to allow for a timely and safe proce-dure to fix the problem.The presence of metal parts (that are very radio-opaque) in the endovascular prosthe-ses makes the postoperative scans not only important for the patient’s safety but also fascinating to look at (Figure 3). Once again appropriate post-processing of the images is mission- critical for an accurate diagnosis.
RESULTS
Our experience with use of thoracic endo-vascular aortic repair started back in 1998. Since then we have performed a total of 322 procedures. Of these 116 involved the aortic arch with partial/total rerouting of the supra-aortic vessels, 172 involved the descending thoracic aorta, and 34 were hy-brid procedures for pathology of the thora-coabdominal district. A total of 126 proce-dures were conducted for degenerative an-eurysms of the descending thoracic aorta. Considering specifically the descending thoracic aorta our technical success rate, i.e. deployment of endograft with complete exclusion of the lesion/minimal endoleak, was 99.4% (with one case requiring emer-gent open conversion). Perioperative mor-tality was 2.9% (five patients).

266
R. Chiesa et al.
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
The rate of pulmonary complication, i.e. the need for more than 24 hours of me-chanical ventilation, was 1.2%. The rate of cardiac complication, i.e. new onset myo-cardial necrosis demonstrated by positive cardiac biomarkers tests, has been 0.6%. The rate of renal complication, i.e. the need for temporary or permanent renal replace-ment therapy, was 1.9%. Cerebrovascular accident, defined as a new neurologic defi-cit lasting more than 24 hours confirmed by imaging, occurred in 1.2% of patients. The rate of spinal cord ischemia, manifest-ing either as paraplegia or paraparesis, was 5.2%. We experienced an even distribution between early and delayed onset paraple-gia/paraparesis. Delayed onset spinal cord ischemia had a tendency towards ameliora-tion with adequate pressure support and cerebrospinal fluid drainage.
DISCUSSION
In spite of the great enthusiasm that endo-vascular techniques provoked and that are confirmed by the excellent results of our case series, it must be remembered that par-ticularly at the level of the thoracic aorta these techniques are by no means complete-ly safe. A significant mortality and morbid-ity is described in all published series. A French report from Ricco JB and coworkers for example, analyzed a countrywide expe-rience over two years and showed an high rate of complications (1).
Damage to access vesselsSeveral literature reports pointed out that serious and even fatal problems may arise from introduction of the device from the femoral artery. In particular rupture or avulsion of the external iliac artery have been reported, this usually becomes dra-matically evident only at the time the large introducer sheath used for endograft de-
livery is withdrawn. We therefore liberally switch to extra-peritoneal surgical expo-sure of the common iliac artery or even the distal aorta if it is difficult to advance the device through the femoral arteries.
StrokeCerebrovascular accidents are among the most common and dreaded complications of endovascular therapy of thoracic aor-tic disease. They are mainly linked to ath-eromatous embolization into the cerebral arteries caused by guide wires, catheters, introducer sheaths manipulation or the en-dograft itself (2). It should be remembered that angiography for diagnostic purposes alone carries a 1-2% risk of complications (3). Second generation commercial grafts are surely less prone to this complication than the home made devices used initially. This is due to the better flexibility of the grafts and sheaths and to the smaller pro-files, that results in improved navigability through the access vessels. Greater experi-ence of the operators may also play a role both in the selection of candidates with ad-equate anatomical characteristics and dur-ing the procedure itself. Anyhow, minimal manipulation of the wires and catheters and a meticulous technique do play a sig-nificant role in the prevention of periopera-tive stroke.
ParaplegiaEndoluminal repair allows the avoidance of aortic cross clamping and its sequelae; however, the intercostal arteries covered by the endograft cannot be reimplanted. The reported incidence of both immediate and delayed paraplegia in patients undergo-ing endovascular procedures of thoracoab-dominal aortic aneurysms can be as high as 12% of cases (4-6). The coverage of a long thoracic aortic segment has been reported to be a significant risk factor for spinal cord injury (7). Patients who have open abdomi-

Endovascular treatment of descending thoracic aneurysms
267
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
nal aortic aneurysms repair also appear to be prone to such a risk because of the marginal spinal cord collateral blood supply secondary to the ligation of lumbar arteries performed during the surgical procedure. Also, proximal collateral circulation of the spinal cord may be put at risk by the occlu-sion of the left subclavian artery (landing zone 2) that abolishes the contribution to the blood supply provided by the anterior spinal artery, a branch of the ipsilateral vertebral artery. Finally, spinal cord injury could be precipitated by the late sealing of a type II endoleak or late thrombosis of col-lateral pathways.In a recent study (8) we analyzed our most recent 5-year experience with repairs of thoracic aortic pathology to evaluate the incidence and investigate the determinants of spinal cord ischemia in endovascular procedures, identify patients at risk, and assess the role and efficacy of prophylactic adjuncts and therapeutic measures. Our data showed that the lack of collateral spi-nal cord blood supply through the lumbar arteries in patients with previous aortic repair appears to be a relevant risk factor even though it did not reach statistical sig-nificance in our series. The intentional oc-clusion of the left subclavian was not a pre-dictor of paraplegia and neither was the ex-clusion of an extensive thoracic aortic seg-ment. Among the perioperative variables, only a mean arterial pressure <70 mmHg was a statistically significant determinant of delayed neurologic deficit (P<.0001). A delayed neurologic deficit developed in four patients, completely resolved after the in-stitution of CSF drainage, steroids admin-istration, and arterial pressure pharmaco-logic adjustment.Our experience addresses the importance of hemodynamic control to prevent postop-erative neurologic deficits and encourages aggressive, postoperative care of these pa-tients. In our practice, we now try to main-
tain a perioperative mean arterial pressure of >90 mmHg and use cerebrospinal fluid drainage in patients deemed at high risk, including those who received abdominal aortic aneurysms repair. In this respect, patients with synchronous thoracic and ab-dominal aortic aneurysms, which we ear-lier treated simultaneously for both aneu-rysms, currently undergo staged procedures to better allow the development of collater-als for spinal cord blood supply. In the case of delayed paraplegia, prompt cerebrospinal fluid drainage, if not previously instituted, is also used to keep the cerebrospinal fluid pressure <10 mm Hg and possibly reverse the deficit.
Aorto-esophageal fistulaAs follow-up is becoming longer and the reported series larger, new serious compli-cations are emerging. One of the most omi-nous one is endograft infection (Figure 4), especially if sustained by an aortoesopha-geal fistula (Figure 5). There are at this time several reports in the literature. It may be caused by erosion of the endograft through the aortic wall into the esophagus, and we may speculate that excessive over-sizing may contribute. This complication does not seem to be specific to a single device. Sometimes it presents as a fatal hemorrhage however sometimes the presentation is less dramatic at it may be characterized by pain, dysphagia, he-matemesis, and septic symptoms. Treat-ment is very problematic and the outcome without treatment is invariably fatal.
MigrationSuccessful long term aneurysm exclusion requires the durability of proximal and dis-tal fixation sites against the bloodstream forces, the fatigue of the materials and the morphological behavior of the aneurysm. The Society for Vascular Surgery/Ameri-can Association for Vascular Surgery (SVS/

268
R. Chiesa et al.
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
Figure 4On the left: axial computed tomography scan of an infected thoracic endograft. Note the presence of air bubbles (arrows) clearly indicating the presence of bacterial flora. On the right: intraoperative picture showing the removal of the stent graft.
Figure 5Postoperative computed tomography showing endograft stent rupture leading to bleeding and aortoesophageal fistula.
AAVS) standards (9) defined endograft migration any movement relative to ana-tomical therapy. To address this problem, a variety of fixation methods such as hooks,
barbs, free-flows and longitudinal support devices have been developed (10) and each presented peculiar advantages and draw-backs. Due to the extreme friability of the

Endovascular treatment of descending thoracic aneurysms
269
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
aortic wall of a dissected aorta, the use of trans- rupture of the longitudinal support wire is a well known complication that af-fected the first generation thoracic Gore TAG device stressed by the bending forces arising in the arch or in kinked aneurysms.
CONCLUSION
The descending thoracic aorta is the ideal morphological site for application of en-dograft technology being the more large straight tubular arterial segment of human body. It has been the first site of aortic an-eurysm endograft exclusion as published by Volodos’ et al. yet in 1988 (11), 3 years be-fore Parodi et al. reported the first series of abdominal aortic aneurysm stent-graft re-pair (12). Since the pioneering experience of Volodos’ and the first renowned short series of thoracic aortic aneurysm endo-vascular repair published by Dake et al in ’94 (13), many series, registries and trials have confirmed feasibility and reduced in-vasivity of thoracic aortic aneurysms endo-vascular repair leading to a real worldwide revolution in the therapeutic approach to the descending aortic diseases. The endovascular era opened new attrac-tive scenarios with many hopes so that, currently, the open repair of an aneurysm limited to the descending aorta, especially to its middle part has became a really un-usual occurrence in the most of European vascular centers.Even in our Center, in the last years we ob-served a progressive shift in the selection of patients for TEVAR of the descending tho-racic aorta. At the beginning of our experi-ence (the first 4-5 years) TEVAR was lim-ited to those patients presenting with one or more serious comorbitidies, while open surgery remained the choice for those in fair clinical conditions. In particular TEVAR was the treatment of choice in the elderly
(>77 years), in patients with a depressed ejection fraction (<40%), in patients with severe pulmonary disease (home oxygen therapy, sever obstruction) and with a life expectancy of less than 5 years.Starting 3 years ago, mainly within investi-gational protocols and trials, we have grad-ually increased the rate of patients under-going TEVAR. Derived from this new at-titude, we experienced really appealing re-sults of TEVAR also in fit surgical patients, especially with critical intercostal arteries left uncovered.However, studies clearly addressing the respective roles of open and endovascular repair are still not available, and the world-wide spreading of expensive endovascular materials and facilities, with the extensive follow-up for endografting add to the cu-mulative escalation of overall health care costs.Furthermore the stents have been designed to have a durability of 10 years based on ISO (International Standardization Organiza-tion) stress testing and the series with the greatest number of patients reach maximum 5 years of follow-up, and are by now associ-ated to a high rate of reinterventions (14).In conclusion, in order to treat both pa-tients unfit for open surgery and patients with long life-expectancy especially with challenging anatomies for endograft de-ployment, both TEVAR and open repair (15) should be part of therapeutic arma-mentarium of every modern vascular sur-geon efficiently approaching thoracic vas-cular diseases.
REFERENCES
1. Ricco JB, Goeau-Brissonniere O, Rodde-Dunet MH, et al. Use of abdominal aortic endovascu-lar prostheses in France from 1999 to 2001. J Vasc Surg 2003; 38: 1273-1281.
2. Taylor PR, Gaines PA, McGuinness CL, et al. Thoracic aortic stent grafts - early experience from two centres using commercially available

270
R. Chiesa et al.
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
devices. Eur J Vasc Endovasc Surg 2001; 22: 70-76.
3. Willinsky RA, Taylor SM, TerBrugge K, et al. Neurologic complications of cerebral angiogra-phy: prospective analysis of 2,899 procedures and review of the literature. Radiology 2003; 227: 522-528.
4. Bell RE, Taylor PR, Aukett M, et al. Mid-term results for second-generation thoracic stent grafts. Br J Surg. 2003; 91: 811-817.
5. Criado FJ, Clark NS, Barnatan MF. Stent graft repair in the aortic arch and descending tho-racic aorta: a 4-year experience. J Vasc Surg 2002; 31: 1121-1128.
6. Greenberg R, Resch T, Nyman U, et al. Endo-vascular repair of descending thoracic aortic aneurysms: an early experience with inter-mediate-term follow-up. J Vasc Surg 2000; 31: 147-156.
7. Gravereaux EC, Faries PL, Burks JA, et al. Risk of spinal cord ischemia after endograft re-pair of thoracic aortic aneurysms. J Vasc Surg. 200; 34: 997-1003.
8. Chiesa R, Melissano G, Marrocco-Trischitta MM, et al. Spinal cord ischemia after elective stent-graft repair of the thoracic aorta. J Vasc Surg. 2005; 42: 11-17.
9. Chaikof EL, Blankensteijn JD, Harris PL, et al. Reporting standards for endovascular aortic an
eurysm repair. J Vasc Surg. 2002; 35: 1048-1060.10. Malina M, Lindblad B, Ivancev K, et al. En-
dovascular AAA exclusion: will stents with hooks and barbs prevent stent-graft migration? J Endovasc Surg 1998; 5: 310-317.
11. Volodos’ NL, Karpovich IP, Shekhanin VE, et al. A case of distant transfemoral endopros-thesis of the thoracic artery using a self-fixing synthetic prosthesis in traumatic aneurysm. Grudn Khir 1988; 84-86.
12. Parodi JC, Palmaz JC, Barone HD. Transfemo-ral intraluminal graft implantation for abdomi-nal aortic aneurysms. Ann Vasc Surg 1991; 5: 491-499.
13. Dake MD, Miller DC, Semba CP, et al. Trans-luminal placement of endovascular stent-grafts for the treatment of descending thoracic aortic aneurysms. N Engl J Med 1994; 331: 1729-1734.
14. Makaroun MS, Dillavou ED, Wheatley GH, et al; Gore TAG Investigators. Five-year results of endovascular treatment with the Gore TAG device compared with open repair of thoracic aortic aneurysms. J Vasc Surg. 2008; 47: 912-918.
15. R. Chiesa, Y. Tshomba, E. Civilini, et al. Open repair of descending thoracic aneurysms. HSR Proceedings in Intensive Care and Cardiovas-cular Anesthesia 2010; 3: 177-190.

ABSTRACTIntroduction: Intra and inter-hospital transfer has become frequent in the care and even critical andshocked patients need to be transported. Extracorporeal Membrane Oxygenation (ECMO) represents animportant treatment option in these patients.Objectives: We describe our clinical experience with a new ECMO device: CARDIOHELP.Methods: Clinical trial was performed in three patients requiring cardiopulmonary support with ECMO.CARDIOHELP device was used as venous-arterial life support in patients affected by cardiogenic shock. Itis a light and portable device and it is provided with integrated sensors to monitorize the basic parameterssince ECMO activation.Results: Two patients had postoperative cardiogenic shock because of acute infarction or tamponadeand one patient had hemodynamic instability in our emergency department. They all underwent to ECMOimplantation with success. After adequate treatments two patients died and the other one was dismissed43 days after ECMO removal.Conclusion: Our first experience was carried out with success. A modified adult ECMO appears easierto implant and it permits an easy control since the activation of ECMO.Keywords: Extracorporeal Membrane Oxygenation; Cardiogenic Shock; Cardiopulmonary bypass.
INTRODUCTIONCardiovascular disorders are the first cause of death worldwide. Coronary artery disease has increasedduring last years and cardiogenic shock is the most important complication in patients admitted to hospi-tal because of acute myocardial infarction: it represents 7-10 % of all complications in these patients.Among all these patients, death occurs in 80% of all cases1.Extracorporeal life support (ECLS) using Extracorporeal Membrane Oxygenation (ECMO) was introducedinto clinical practice during the early 70s2 and it is now considered one of the fastest and cheapestmethods for biventricular and respiratory support in adult and paediatric populations. The main indicationto ECMO is the cardiogenic shock resistant to conventional critical care, including intra-aortic balloonpumps3. If a patient is quickly connected to an extracorporeal life support system such as ECMO, chanceof survival could be increased.A relative restriction to ECMO implantation is due to its difficult transport; sometimes these characteristicsmake the transport challenging especially in patients hemodinamically compromised4.Recently, a new miniaturized system for cardiopulmonary support has been introduced into the clinicalpractice: “CARDIOHELP” by Maquet Getinge Group. This paper describes 3 case reports treated with thisnew ECMO system at San Gerardo Hospital, Monza, Italy.
MATERIALS AND METHODSThe deviceThis “CARDIOHELP” device weighs just 10 kilos and it is compact enough to be carried by one person evenin a vehicle or in a helicopter; so even critical patients could be transported. The extracorporeal systemincludes a centrifugal pump (Rotaflow, MAQUET Cardiopulmonary AG, Hechingen, Germany) and a diffu-sion membrane oxygenator (Quadrox HLS Advanced, MAQUET Cardiopulmonary AG, Hechingen, Germany),both combined on a multifunctional and compact holder. The tubing circuit is characterized by a BIOLINEcoating, a minimized foreign surface and a small priming volume (about 600 ml); this particular device pre-vents blood-air contact.The peculiarity of this miniaturized system is that it is provided with integrated sensors for monitoring ofpressure (venous, arterial and integrated pressure), arterial and venous temperature, venous oxygen satu-ration, hematocrit and haemoglobin, blood flow and bubble transit.The system is also provided with a battery pack, in order to operate as a stand-alone device for 90 minu-tes with fully charged batteries. The device is approved for cardiac support and respiratory assistance fora period of up to 30 days.A cardiac surgeon, an anaesthetist, a nurse and a perfusionist form our ECMO équipe. Every member ofthis team received a training course. The trade company placed a device in our institution to improve ourlearning curve and a daily simluation was held in order to increase our perfusionists ability.
Technique of extracorporeal supportIn our experience, all patients treated with CARDIOHELP required venoarterial bypass. For outflow, femoralvein was cannulated with a 55 cm long and 21 French diameter cannula (MAQUET Cardiopulmonary AG,Hechingen, Germany) and for reinfusion, femoral artery was cannulated with a 15 cm long and 15 Frenchdiameter cannula (MAQUET Cardiopulmonary AG, Hechingen, Germany). Before cannulation, 5000 UIheparin were administrated in order to achieve an activated clotting time (ACT) value between 150-180seconds. The ECMO blood flow was adequately adjusted to maintain cardiac index of 2.6 L/min/m2.
PATIENTSFrom June 2010 to July 2010 three patients required cardiopulmonary support with ECMO in our hospi-tal. First patient was a 37-year-old male who previously underwent to cardiac surgery because of severecoronary disease and restrictive cardiomyopathy caused by radiotherapy; he was diagnosed with Hodgking
lymphoma in 1986 and he was treated with radiotherapy. During last six years he had developed sym-ptoms such as angor and dyspnoea related to chronic ischemic cardiac disease and he was treated withmedical therapy. The patient was evaluated as a stable NYHA class III in March 2010. In June 2010 medi-cal therapy was discontinueted because of a programmed dobutamine stress echo. He arrived in our emer-gency department three days after and he was diagnosed with acute pulmonary edema and hemodyna-mic instability which resulted in cardiac arrest. After adequate cardiopulmonary resuscitation, ECMOimplantation was decided. The patient underwent to surgical myocardial revascularization 24 hours lateand he required reexploration for bleeding and cardiac tamponade. On day 10, the patient was weanedfrom ECMO but his general conditions impaired and ECMO implantation was required five hours later. Afterfour days the patient died because of intracerebral hemorrhage.The second patient was a 49-year-old male referred to our department for acute myocardial infarction(AMI) to undergo an elective coronary artery bypass graft; he had a dilatative cardiomyopathy and a lowejection fraction. Three days after the operation, the patient had a cardiac arrest with ventricular fibrillationin our semi-intensive care unit. After 55-minutes cardiopulmonary resuscitation, ECMO was positioned andthe patient was transported to cardiac surgical ICU. Three days later, he underwent to a coronary angio-gram and a LIMA graft kinking was detected. For this reason the patient needed a surgical revision. Duringthe ICU stay there were some complications due to femoral bleeding so the patient was subjected to a localsurgical revision. On day 11, the ECMO system was removed successfully. On day 43 after ECMO remo-val, the patient was discharged.The third patient was a 75-year-old man with an history of ischemic heart disease, hypertension and noleft ventricular dysfunction. He was admitted to our cardiac surgical department to undergo a surgical myo-cardial revascularization and a left carotid endoarterectomy. During his fourth postoperative day, patienthad a cardiac arrest with pulseless electrical activity because of a left ventricular free wall rupture and anheart tamponade. After 45-minutes cardiopulmonary resuscitation, ECMO was implanted and the patientwas transferred to operating room to repair the free wall. The patient died two days after because of cere-bral post anoxic injury.
DISCUSSIONCritically ill patients with cardiopulmonary failure not responders to standard therapy frequently requireurgent intra or inter-hospital transfer to save their lives5,6. However, such patients cannot benefit of spe-cialized centers if they are considered too sick to be transferred. Our clinical experience with ECMO makeus point out all problems listed above. Conventional ECMO system used in our hospital is characterizedby three separate units: a console, a centrifugal pump and a oxygenator. It is not miniaturized, it is quiteheavy and it is not possible to carry it easily. Furthermore, this system doesn’t allow perfusionist to moni-torize the basic parameters (pressure, temperature, venous oxygen saturation, hematocrit, haemoglobin,blood flow and bubble transit). These are the most relevant restrictions to ECMO use out of cardiac sur-gical intensive care unit.A new miniaturized extracorporeal life support system appeared on the market six month ago: “CARDIO-HELP” Maquet GETINGE GROUP. During last June 2010, our hospital was selected by the trade companyin order to begin a clinical trial, part of an international project. We started our experience with CARDIO-HELP after adequate training.This portable device can be carried by one person, this characteristic allowed ECMO équipe to easilyimplant CARDIOHELP in intra or extra-hospital sceneries. CARDIOHELP system has also integrated para-meters monitoring so that medical staff can safely transport patients. This monitoring system is part of amore complex software that permits an easy control since the activation of ECMO device. We noticed thatthis system is characterized by a short preparation time and a user-friendly management.Since the most of ECMO implants is performed outside the ICU, the transfer is a crucial point and the avai-lability of a miniaturized device facilitate the execution of diagnostic exams even if the critical patient is jud-ged as not transportable.
REFERENCES1. Chen JS, Ko WJ, Yu H, et al. Analysis of the outcome for patients experiencing myocardial infarction
and cardiopulmonary resuscitation refractory to conventional therapies necessitating extracorporeal lifesupport rescue. Crit Care Med 34: 950-957, 2006.
2. Bartlett RH, Gazzaniga AB, Jefferies MR, et al. Extracorporeal membrane oxygenation (ECMO) cardio-pulmonary support in infants. ASAIO Trans 22: 80-93,1976.
3. Marasco SF, Lukas G, McDonald M, McMillan J, Ihle B. Review of ECMO (extra corporeal membraneoxygenation) support in critically ill adult patients. Heart Lung Circ17 Suppl 4:S41-7, 2008.
4. Matthias Arlt, Alois Philipp, Markus Zimmermann, Sabine Voelkel, Michael Hilker, Jonny Hobbhahna,Christof Schmidb. First experiences with a new miniaturised life support system for mobile percutane-ous cardiopulmonary bypass. Resuscitation 77: 345-350, 2008.
5. Smith I, Fleming S, Cernaiana A. Mishaps during transport from the intensive care unit. Crit Care Med18:278-81,1990.
6. Lovell MA, Mudaliar MY, Klineberg PL. Intrahospital transport of critically ill patients: complications anddifficulties. Anaesth Intensive Care 29:400-5, 2001.
A NEW MINIATURIZED ECMO SYSTEM: OUR FIRST EXPERIENCESM.C. Costa1, S. Mariani2, L. Avalli3, F. Formica2, R. Caruso1, S. Capalbi1, C. Gambarini1, G. Paolini2
1Perfusion service, 2Cardiac Surgical Department, 3Cardiac Surgical ICU, San Gerardo Hospital, Monza, Italy.
MAQUET Italia S.p.A. - Via Gozzano 14, 20092 Cinisello Balsamo (MI), ItalyPhone +39 (0) 2 6111 351 - Fax +39 (0) 2 6111 35 260/11 - E-mail: [email protected] - Internet: www.maquet.it
Correspondin Author:Maria Cristina Costa, Cheaf Perfusionist, Perfusion ServiceSan Gerardo Hospital - Via Pergolesi, 33 20052 Monza, ItalyE-mail: [email protected]
273
proceedingsin Intensive Care
Cardiovascular Anesthesia
Endorsed by
proceedings
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
ORIGINAL ARTICLE
Corresponding author:Ida Møller Nielsen, MDDepartment of Cardiothoracic Anesthesia, VOdense University Hospital Sdr. Boulevard 29DK-5000 Odense C - Denmarke.mail: [email protected]
INTRODUCTION
Age related aortic stenosis occurs in 2-3% of those over the age of 65. With the aging of the population in general, aortic valve disease is rapidly increasing. With only about 200,000 aortic valve re-placements (AVR) carried out worldwide per year, a large number of patients with
symptomatic aortic stenosis are not treated. Many of them are considered at too high risk to undergo open heart surgery due to age or comorbidity (1,2) and this led to a growing interest in the development of less invasive methods of AVR. In 1985, Cribier in Rouen (France) per-formed the first successful percutaneous aortic valvuloplasty, but before that, dur-ing the 80´s, Henning Rud Andersen in Aarhus (Denmark), actually experimented with expanding bioprosthetic stent valves implanted in pigs (3). In 2002, Cribier conducted the first percu-taneous AVR in a human.
(4-6).
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010; 2: 273-277
ABSTRACT
Introduction: Percutaneous retrograde transfemoral or transsubclavian aortic valve replacement is a mini-mally invasive method of aortic valve replacement in elderly and high-risk patients with symptomatic aortic stenosis considered too fragile to go through conventional heart surgery. The purpose of this study was to compare two different anaesthetic techniques for percutaneous retrograde transfemoral or transsubclavian aortic valve replacement in terms of anaesthetic depth, hemodynamic stability and need for vasoactive drugs.Methods: Forty-eight elderly or high risk patients, two third of them in their eighties, were scheduled for per-cutaneous retrograde transfemoral or transsubclavian aortic valve replacement. Anaesthetic induction was standardized, but anaesthesia was afterwards maintained alternately with either propofol infusion or sevo-flurane. Need for vasoactive drugs was recorded and anaesthetic depth was estimated from acoustic evoked potential measuring and clinical observation. Results: Twenty-eight percent of the patients in the sevoflurane group and 30% of the patients in the propo-fol group required vasoactive therapy (P=0.84). Forty-four percent of the patients in the sevoflurane group and 57% of the patients in the propofol group had episodes of superficial anaesthesia recorded (P=0.38). Conclusion: We found no significant difference in the use of vasoactive drugs or in anaesthetic depth between propofol and sevoflurane anaesthesia. Both can be recommended for percutaneous aortic valve replacement.
Keywords: PAVR, AVR, anaesthesia, trans catheter
Transcatheter aortic valve replacement in high risk patients with different anaesthetic techniquesI. Møller Nielsen, C. AndersenOdense University Hospital, Odense, Denmark

274
I. Møller Nielsen, C. Andersen
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
In our institution, patients considered for retrograde percutaneous aortic valve re-placement (PAVR) are patients with se-vere symptomatic aortic stenosis who are >75 years of age, or, are >65 years and either have a standard EUROscore (Euro-pean System Operation Risk Evaluation) >15% or at least one of the following risk factors: previous heart surgery, glass aorta, pulmonary disease, liver cirrhosis, right ventricular heart failure, thoracic trauma as from radiotherapy, cachexia or obesity (7). These factors must of course be considered individually according to their severity. The aim of this study was to compare an-aesthetic depth and hemodynamic stabil-ity between total intravenous propofol an-aesthesia and sevoflurane anaesthesia for PAVR.
METHODS
After Danish Committee in Biomedical Re-search Ethics approval and patient’s writ-ten consent, patients with severe, symp-tomatic aortic stenosis (AS) who were con-sidered at too high a risk for conventional surgery were included in the study. Patient characteristics including age, gender, sever-ity of aortic stenosis and comorbidity were collected as described in table 1. All under-went PAVR with the CoreValve® (Medtron-ic CV. Luxemburg) revalving system during a 22 months period from March 2008 till January 2010.All patients were anaesthetized with fen-tanyl (0.05-0.1 mg), etomidate (16-18 mg) and cisatracurium 0.2 mg/kg and endotra-cheally intubated. Patients were then as-signed to one of the two anaesthetic meth-ods, simply by using sevoflurane (MAC 0.8-1) in half of the cases and propofol (4-10 mg/kg/h) in the other half of the cases, this was done in a regular alternating manner.Our routine cardiac monitoring, consisting
of ECG, arterial, central venous and pulmo-nary artery pressure, cardiac index, arterial and mixed venous oxygen saturation, was supplemented with transesophageal echo-cardiography and anaesthetic depth moni-toring using the AEP Monitor/2™ (Danme-ter, Odense, DK), that measures and index-es acoustic evoked potentials.The anaesthesiologist was responsible for insertion of the temporary ventricular pace catheter and for operation of the pacemak-er when rapid ventricular pacing was de-manded. Dopamine was the drug of choice in hy-potension if there was a continuous mean arterial pressure under 60 mmHg (starting dose 5 mcg/kg/min), whereas norepineph-rine was chosen if the patient at the same time had relative tachycardia (starting dose 0.02 mcg/kg/min).Coughing or any other patient movements signalled by the interventional cardiolo-gist were recorded as well as rises in AEP signals. The cardiologist could not see and was not informed about the AEP monitor.PAVR was performed through either bilat-eral transfemoral, or combined transsub-clavian and transfemoral artery access (one access for the angiography and one access for the insertion of the stent valve device). Aortic valvuloplasty was performed during rapid ventricular pacing to minimize pul-sating transvalvular flow at the moment of dilation (8). The bioprosthetic valve, which had been shrinked in ice water to fit into an extendable stent, was then deployed
(9). Imaging of the procedure was provided by aortic angiography as well as by trans-esophageal echocardiography (10). Thus, the demands on anaesthesia were tolerance of bilateral inguinal catheterisation and tol-erance of the esophageal echocardiography probe. Quick recovery after rapid ventricu-lar pacing during valvuloplasty was espe-cially important (11-13).Statistics: Data are presented as mean,
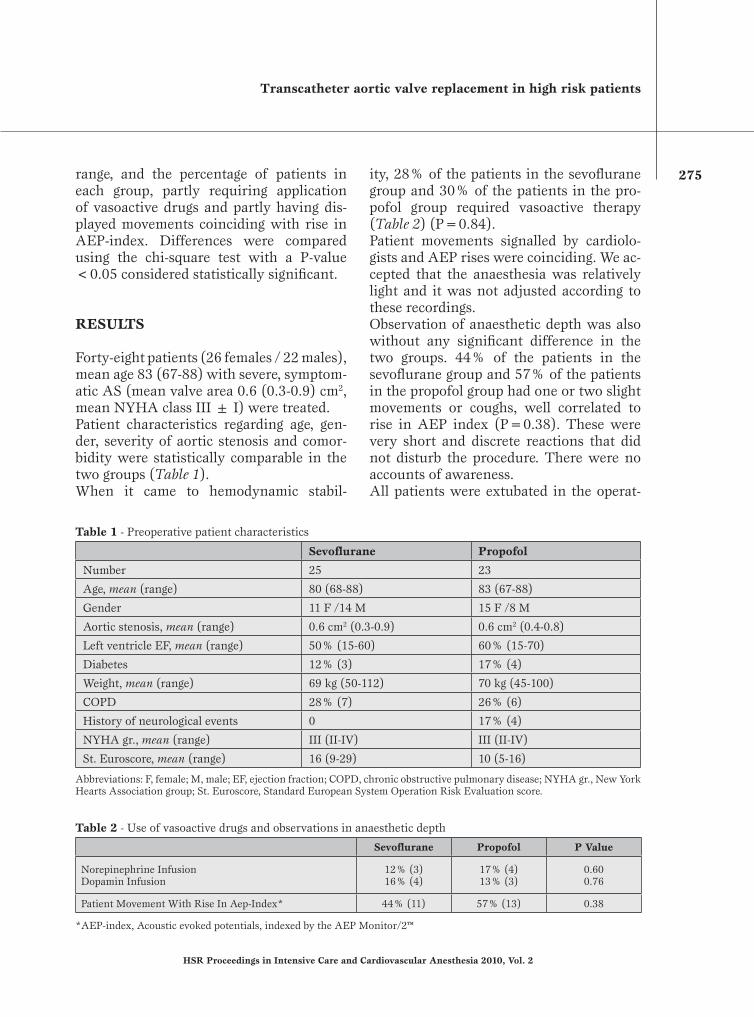
Transcatheter aortic valve replacement in high risk patients
275
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
range, and the percentage of patients in each group, partly requiring application of vasoactive drugs and partly having dis-played movements coinciding with rise in AEP-index. Differences were compared using the chi-square test with a P-value <0.05 considered statistically significant.
RESULTS
Forty-eight patients (26 females / 22 males), mean age 83 (67-88) with severe, symptom-atic AS (mean valve area 0.6 (0.3-0.9) cm2, mean NYHA class III ± I) were treated. Patient characteristics regarding age, gen-der, severity of aortic stenosis and comor-bidity were statistically comparable in the two groups (Table 1). When it came to hemodynamic stabil-
ity, 28% of the patients in the sevoflurane group and 30% of the patients in the pro-pofol group required vasoactive therapy (Table 2) (P=0.84). Patient movements signalled by cardiolo-gists and AEP rises were coinciding. We ac-cepted that the anaesthesia was relatively light and it was not adjusted according to these recordings. Observation of anaesthetic depth was also without any significant difference in the two groups. 44% of the patients in the sevoflurane group and 57% of the patients in the propofol group had one or two slight movements or coughs, well correlated to rise in AEP index (P=0.38). These were very short and discrete reactions that did not disturb the procedure. There were no accounts of awareness. All patients were extubated in the operat-
Table 2 - Use of vasoactive drugs and observations in anaesthetic depth
Sevoflurane Propofol P Value
Norepinephrine InfusionDopamin Infusion
12% (3)16% (4)
17% (4)13% (3)
0.600.76
Patient Movement With Rise In Aep-Index* 44% (11) 57% (13) 0.38
*AEP-index, Acoustic evoked potentials, indexed by the AEP Monitor/2™
Table 1 - Preoperative patient characteristics
Sevoflurane Propofol
Number 25 23
Age, mean (range) 80 (68-88) 83 (67-88)
Gender 11 F /14 M 15 F /8 M
Aortic stenosis, mean (range) 0.6 cm2 (0.3-0.9) 0.6 cm2 (0.4-0.8)
Left ventricle EF, mean (range) 50% (15-60) 60% (15-70)
Diabetes 12% (3) 17% (4)
Weight, mean (range) 69 kg (50-112) 70 kg (45-100)
COPD 28% (7) 26% (6)
History of neurological events 0 17% (4)
NYHA gr., mean (range) III (II-IV) III (II-IV)
St. Euroscore, mean (range) 16 (9-29) 10 (5-16)
Abbreviations: F, female; M, male; EF, ejection fraction; COPD, chronic obstructive pulmonary disease; NYHA gr., New York Hearts Association group; St. Euroscore, Standard European System Operation Risk Evaluation score.

276
I. Møller Nielsen, C. Andersen
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
ing theatre, before transferring to the in-tensive care unit (ICU), where the first 20 patients were monitored overnight, while it has now become standard to discharge the patients from the ICU after a six-hours monitoring.
DISCUSSION
In view of anaesthetic depth, hemodynamicstability and need for vasoactive drugs, ourresults showed no statistically significant difference between sevoflurane and propo-fol anaesthesia for PAVR. It should be notedthat all patients were extubated in the the-atre and then monitorized in ICU for a short period. Both anaesthetic techniques can be recommended for this procedure. We are conscious though, that a much larg-er sample size would probably have been needed to detect any difference. Potential advantages of general anaesthesia include, a part from hypnosis and analgesia, immo-bility and control of the patients cardiore-spiratory status. At our center however, cardiologists are getting more experienced in valve implan-tation, the duration of the procedure is get-ting shorter and the routine setting is be-coming one of local anaesthesia and light sedation. The same experience was previously de-scribed by other authors (14).There is nevertheless still still a role for theanaesthesiologist, just as much in taking part in the preprocedural evaluation of the patient as in providing appropriate moni-toring and early management of side effectsand complications.
LimitationsWe recognize a number of limitations with-in this study.There was no blind randomization of pa-tients to one group or the other; the patients
were never the less assigned in an alternat-ing manner without exception.Nobody in the theatre was blinded to the anaesthetic technique that had been chosen and the indication for starting vasopressor therapy, as well as the choice of drug, was not extremely precise.Only preoperative observations were reg-istered, we did not collect data on cardiac biomarker levels. Neither did we do any long term follow up on outcome.As already mentioned the study is probably underpowered as the number of patients may be too small to show any difference between techniques, if ever there was one.Our work should thus be considered a pilot study, as there has not yet been published any other works comparing terms methods for PAVR.
CONCLUSIONS
Successful management of these, generally very old or fragile patients, very much de-pends on a well coordinated interdisciplin-ary collaboration between interventional cardiologists and cardiovascular anaesthe-siologists.Clear understanding of the pathophysiol-ogy as well as knowledge of all technical aspects of the procedure is mandatory and good communication is momentous.Our work confirms that, once the decision of performing a general anaesthesia has been taken, the choice of anaesthetic drugs is not important in terms of anesthetic depth, hemodynamic stability and need for vasoactive drugs.
Acknowledgements: We thank Henrik Nissen and the rest of the interventional cardiology team as well as the nurse anaesthetists for good teamwork. Thanks to Chris Garcia for revision of the English manuscript.
No conflict of interest acknowledged by the authors.

Transcatheter aortic valve replacement in high risk patients
277
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
REFERENCES
1. Brown JM, O’Brien SM, Wu C, et al. Isolated aor-tic valve replacement in North America comprising 108,687 patients in 10 years: changes in risks, valve types, and outcomes in the Society of Thoracic Sur-geons National Database. J Thorac Cardiovasc Surg 2009; 137: 82-90.
2. Iung B, Baron G, Butchart EG, et al. A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. Eur. Heart J 2003; 24: 1231-1243.
3. Andersen HR, Knudsen LL, Hassenkam JM. Trans-luminal implantation of artificial heart valves. Dis-cription of a new extendable aortic valve and initial results with implantation by catheter technique in closed chest pigs. Eur Heart J 1992; 13: 704-708.
4. Cribier A, Eltchaninoff H, Bash A, et al. Percutane-ous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis: first human case description. Circulation 2002; 106: 3006-3008.
5. Cribier A, Eltcaninoff H, Tron C, et al. Early experi-ence with percutaneous transcatheter implantation of heart valve prosthesis for the treatment of end-stage inoperable patients with calcific aortic steno-sis. J Am Coll Cardiol 2004; 43: 698-703.
6. Cribier A, Eltchaninoff H, Tron C, et al. Treat-ment of calcific aortic stenosis with the percutane-ous heart valve: Mid-term follow-up from the initial feasibility studies: the french experience. J Am Coll Cardiol 2006; 47: 1214-1223.
7. Grube E, Schuler G, Buellesfeld L, et al. Percutane-ous aortic valve replacement for severe aortic ste-
nosis in high-risk patients using the second- and current third-generation self-expanding CoreValve prosthesis: device success and 30-day clinical out-come. J Am Coll Cardiol 2007; 50: 69-76.
8. Webb JG, Pasupati S, Achtem L, Thompson CR. Rapid pacing to facilitate transcatheter prosthetic heart valve implantation. Catheter Cardiovasc In-terv 2006; 68: 199-204.
9. Webb JG, Chandavimol M, Thompson CR, et al. Per-cutaneous aortic valve implantation retrograde from the femoral artery. Circulation 2006; 113: 842-850.
10. Berry C, Oukerraj L, Asgar A, et al. Role of trans-esophageal echocardiography in percutaneous aortic valve replacement with the CoreValve Revalving sys-tem. Echocardiography 2008; 25: 840-848.
11. Covello RD, Maj G, Landoni G, et al. Anesthetic management of percutaneous aortic valve implanta-tion: focus on challenges encountered and proposed solutions. J Cardiothorac Vasc Anesth 2009;23:280-285.
12. Basciani R, Henle S, Zobrist C, et al. Retrograde per-cutaneous aortic valve replacement in severe aortic valve stenosis: anesthesia management and short term outcome. Anesth Analg 2008; 106 (SCASuppl): 1-128
13. Meineri M, Wasowiez M, Vegas A, Karski J. Anes-thetic management for trans-catheter aortic valve implantation: Initial experience. Anest Analg 2008; 106 (SCASuppl): 1-128.
14. Covello RD, Ruggeri L, Landoni G, et al. Transcath-eter implantation of an aortic valve: anesthesiologi-cal management. Minerva Anestesiol. 2010; 76: 100-108.

Pfizer è da anni fortemente impegnata nella ricerca e sviluppo di molecole innovativecontro le malattie infettive, come gli attuali presidi antinfettivi salvavita:
• Zyvoxid® (linezolid)• VFend® (voriconazolo)• Ecalta® (anidulafungina)
Anti-Infectives
Depo
sita
to p
ress
o l’A
IFA
in d
ata
12/0
3/09
V 1.
0

279
proceedingsin Intensive Care
Cardiovascular Anesthesia
Endorsed by
proceedings
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
ORIGINAL ARTICLE
Corresponding author:Giovanni Landoni, M.D.Department of Anaesthesia and Intensive CareUniversita Vita-Salute San RaffaeleVia Olgettina, 60 - 20132 Milan, Italye.mail: [email protected]
INTRODUCTION
Out-of-hospital cardiac arrest is still a ma-jor public health issue (1), claiming hun-dreds of thousands of lives worldwide year-ly. Unfortunately, survival rate to hospital
discharge has improved little over the past decades (2). Bystander-initiated cardiopul-monary resuscitation (CPR) is essential to increase the chance of survival and neuro-logical recovery (3). Despite huge efforts to train laypeople to recognize and treat car-diac arrest, incidence of bystander CPR re-mains very low (4). Reluctance to perform mouth-to-mouth ventilation is one of the major reason (5, 6). Whereas CPR includ-ing ventilation is still considered the gold
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010; 2: 279-285
ABSTRACT
Introduction: Out-of-hospital cardiac arrest has a low survival rate to hospital discharge. Recent studies com-pared a simplified form of CPR, based on chest compression alone versus standard CPR including ventilation. We performed systematic review and meta-analysis of randomized controlled trials, focusing on survival at hospital discharge.Methods: We extensively searched the published literature on out-of hospital CPR for non traumatic cardiac arrest in different databases. Results: We identified only three randomized trials on this topic, including witnessed and not-witnessed car-diac arrests. When pooling them together with a meta-analytic approach, we found that there is already clinical and statistical evidence to support the superiority of the compression-only CPR in terms of survival at hospital discharge, as 211/1842 (11.5%) patients in the chest compression alone group versus 178/1895 (9.4%) in the standard CPR group were alive at hospital discharge: odds ratio from both Peto and DerSimonian-Laird methods =0.80 (95% confidence interval 0.65-0.99), p for effect =0.04, p for heterogeneity =0.69, inconsistency =0%).Conclusion: Available evidence strongly support the superiority of bystander compression-only CPR. Reasons for the best efficacy of chest compression-only CPR include a better willingness to start CPR by bystanders, the low quality of mouth-to-mouth ventilation and a detrimental effect of too long interruptions of chest com-pressions during ventilation. Based on our findings, compression-only CPR should be recommended as the preferred CPR technique performed by untrained bystander.
Keywords: cardiopulmonary resuscitation; meta-analysis; systematic review, cardiac arrest, randomized trials, compression-only.
Bystander-initiated chest compression-only CPR is better than standard CPR in out-of-hospital cardiac arrestL. Cabrini1, G. Biondi-Zoccai2, G. Landoni1, M. Greco1, F. Vinciguerra1, T. Greco1, L. Ruggeri1, J. Sayeg1, A. Zangrillo1
1Department of Anesthesia and Intensive Care, Università Vita-Salute San Raffaele, Milan, Italy; 2Interventional Cardiology, Division of Cardiology, Università di Torino, Tourin, Italy

280
L. Cabrini et al.
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
standard approach before advanced life sup-port can be instituted, a growing number of studies compared a simplified form of CPR, based on chest compression alone versus standard CPR including ventila-tion. Animal studies showed no difference in survival (7) or even worse outcomes (8) when ventilation was added to chest com-pressions; nevertheless, in animal models of cardiac arrest due to respiratory causes a positive effect of ventilations was demon-strated (9). In humans, observational stud-ies of bystander-initiated CPR comparing standard and compressions-only CPR re-ported similar survival rates (10-12); how-ever, interpretation of the results is made difficult due to the high heterogeneity of the causes of cardiac arrest and of the res-cue characteristics. Chest compression-only CPR is simpler than standard CPR to teach (during courses but even by dispatchers under real conditions), and likely a higher percentage of bystanders would accept to perform it while avoiding mouth-to-mouth contact (6): the demonstration that it is (at least) as effective as standard CPR can be crucial to improve survival rate in out-of-hospital cardiac arrest.With the underlying hypothesis that out-of-hospital cardiac arrest bystander–initi-ated compression-only CPR is equivalent to CPR including ventilation (standard CPR), we performed a comprehensive systematic review and meta-analysis of randomized controlled trials, focusing on survival at hospital discharge.
METHODS
Search strategyPertinent studies were independently searched in BioMedCentral, CENTRAL, and PubMed (updated September 1st , 2010) by several trained investigator. The full search strategies in Pubmed was “(cpr
OR resuscitation) AND compression AND breath* AND cardiac AND arrest AND survival)”. Further hand or computerized searches involved the recent (2008-2010) conference proceedings from the Interna-tional Anesthesia Research Society, Ameri-can Heart Association, American College of Cardiology, American Society of Anesthe-siology and European Society of Cardiology congresses. In addition, we employed back-ward snowballing (ie scanning of reference of retrieved articles and pertinent reviews) and contacted international experts for fur-ther studies. No language restriction was enforced, and non-English-language arti-cles were translated when appropriate.
Study selectionReferences obtained from database and lit-erature searches were first independently examined at the title/abstract level by sev-eral investigators with divergences resolved by consensus, and then, if potentially perti-nent, retrieved as complete articles.The following inclusion criteria were em-ployed for potentially relevant studies:a) random allocation to treatment;b) comparison of chest-compression-only
versus standard CPR.The exclusion criteria were:a) non-parallel design (ie cross-over) ran-
domized trials,b) duplicate publications (in this case only
the article reporting the longest follow-up was abstracted);
c) non-human experimental studies;d) no outcome data.Two investigators independently assessed compliance to selection criteria and selected studies for the final analysis, with divergenc-es finally resolved by consensus (Table 1).
Data abstraction and study characteristicsBaseline and outcome data were indepen-dently abstracted by several investigators
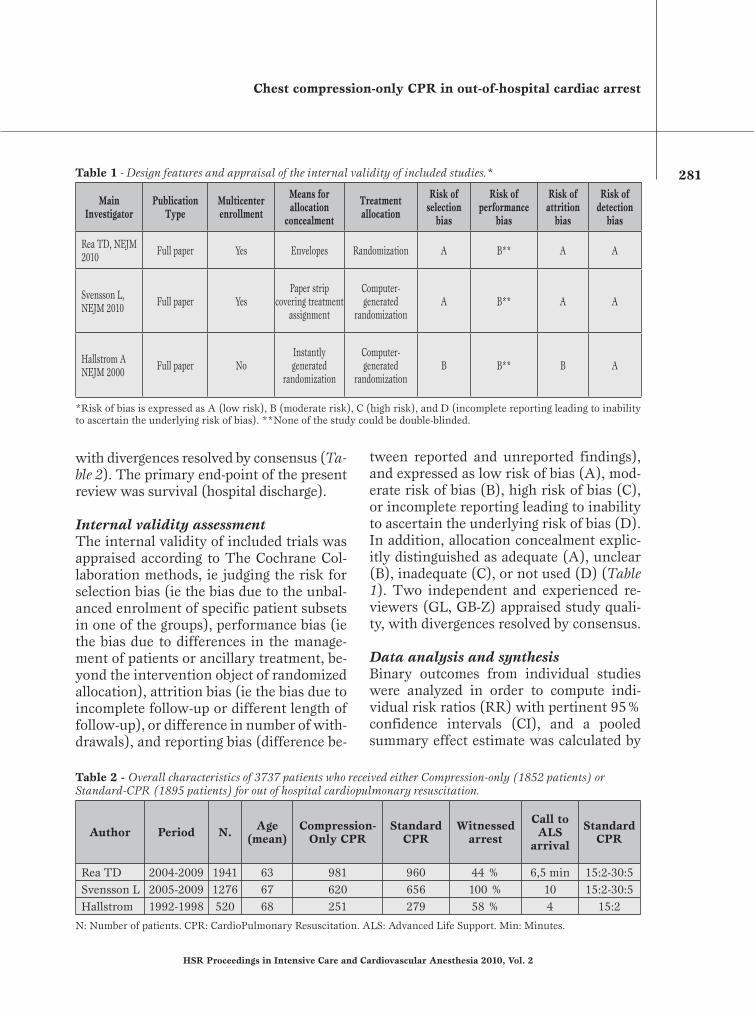
Chest compression-only CPR in out-of-hospital cardiac arrest
281
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
with divergences resolved by consensus (Ta-ble 2). The primary end-point of the present review was survival (hospital discharge).
Internal validity assessmentThe internal validity of included trials was appraised according to The Cochrane Col-laboration methods, ie judging the risk for selection bias (ie the bias due to the unbal-anced enrolment of specific patient subsets in one of the groups), performance bias (ie the bias due to differences in the manage-ment of patients or ancillary treatment, be-yond the intervention object of randomized allocation), attrition bias (ie the bias due to incomplete follow-up or different length of follow-up), or difference in number of with-drawals), and reporting bias (difference be-
tween reported and unreported findings), and expressed as low risk of bias (A), mod-erate risk of bias (B), high risk of bias (C), or incomplete reporting leading to inability to ascertain the underlying risk of bias (D). In addition, allocation concealment explic-itly distinguished as adequate (A), unclear (B), inadequate (C), or not used (D) (Table 1). Two independent and experienced re-viewers (GL, GB-Z) appraised study quali-ty, with divergences resolved by consensus.
Data analysis and synthesisBinary outcomes from individual studies were analyzed in order to compute indi-vidual risk ratios (RR) with pertinent 95% confidence intervals (CI), and a pooled summary effect estimate was calculated by
Table 1 - Design features and appraisal of the internal validity of included studies.*
Main Investigator
Publication Type
Multicenterenrollment
Means for allocation
concealment
Treatment allocation
Risk ofselection
bias
Risk ofperformance
bias
Risk ofattrition
bias
Risk ofdetection
bias
Rea TD, NEJM 2010 Full paper Yes Envelopes Randomization A B** A A
Svensson L, NEJM 2010 Full paper Yes
Paper strip covering treatment
assignment
Computer-generated
randomizationA B** A A
Hallstrom A NEJM 2000 Full paper No
Instantly generated
randomization
Computer-generated
randomizationB B** B A
*Risk of bias is expressed as A (low risk), B (moderate risk), C (high risk), and D (incomplete reporting leading to inability to ascertain the underlying risk of bias). **None of the study could be double-blinded.
Table 2 - Overall characteristics of 3737 patients who received either Compression-only (1852 patients) or Standard-CPR (1895 patients) for out of hospital cardiopulmonary resuscitation.
Author Period N. Age (mean)
Compression-Only CPR
Standard CPR
Witnessed arrest
Call to ALS
arrival
Standard CPR
Rea TD 2004-2009 1941 63 981 960 44 % 6,5 min 15:2-30:5Svensson L 2005-2009 1276 67 620 656 100 % 10 15:2-30:5Hallstrom 1992-1998 520 68 251 279 58 % 4 15:2
N: Number of patients. CPR: CardioPulmonary Resuscitation. ALS: Advanced Life Support. Min: Minutes.

282
L. Cabrini et al.
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
means of a fixed effects model. Statistical heterogeneity and inconsistency was mea-sured using, respectively, Cochrane Q tests and I2. The risk of small study bias was not assessed given the inclusion of 3 studies only. Statistical significance was set at the two-tailed 0.05 level. Computations were performed with RevMan 5.0 (The Cochrane Collaboration, Copenhagen, Denmark).
RESULTS
Database searches, snowballing and con-tacts with experts yielded a total of 32 citations (Figure 1). Excluding 29 non-pertinent titles or abstracts, we retrieved in complete form and assessed according to the selection criteria 3 studies (13-15).
which were included in the final analysis.
Study characteristicsThe 3 randomized controlled studies in-cluded 3737 patients (1895 to chest-com-pression-only and 1842 to the standard CPR group) (Table 2). All studies were per-formed in non-traumatic out of hospital pa-tients and stated that the updated interna-tional basic life support and advanced life support guidelines were strictly followed. All studies were of high quality (Table 1)
as testified by the details on the method used for randomized sequence generation and allocation, adequate allocation con-cealment and low risk of selection, perfor-mance, attrition and detection bias. One study employed a multicenter design, a fea-ture which does not strictly impact on in-ternal validity, but usually increases exter-nal validity of a trial. All studies reported on mortality.
Quantitative data synthesisOverall analysis showed that, in compari-son to standard CPR, chest-compression-only was associated to increased survival at hospital discharge (211/1842 [11.5%] vs 178/1895 [9.4%], RR=1.24 [1.01-1.54], p=0.04) (Figure 2). Similar results were obtained at sensitivity analyses using ran-dom-effect methods or risk differences (all p<0.05).Only one study (13) considered the favour-able neurological outcome suggesting better outcome in clinical subgroups of patients receiving chest-compression-only.
DISCUSSION
Available evidence from randomized con-trolled trials strongly supports the superior-
Figure 1Flow chart of the systematic review process (RCT=randomized clinical trial).

Chest compression-only CPR in out-of-hospital cardiac arrest
283
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
ity of bystander-initiated compression-only CPR, given that patients who experienced out-of-hospital cardiac arrest could be saved by limiting CPR to chest compres-sion. These results are crucial to signifi-cantly improve the first response to out-of-hospital cardiac arrests, a worldwide major public health problem. Previous findings from observational stud-ies in humans (11, 12, 16, 17) document-ed that spontaneously performed (i.e., not dispatcher instructed) compression-only CPR was as effective as standard CPR. In the SOS-KANTO study (10), including wit-nessed cardiac arrests, compression-only CPR resulted in a higher proportion of pa-tients with a favourable neurological out-come than standard CPR in patients with apnoea, shockable rhythm and resuscita-tion started within 4 minutes; ventilations did not add benefits in any subgroup. On the contrary, two recent nationwide obser-vational studies (18, 19) conducted in Ja-pan concluded that standard CPR should be preferred in out-of-hospital cardiac arrests of noncardiac origin, both in adults and in children; in this group, the two CPR tech-niques were similarly effective for arrests of cardiac origin. Among the tree randomized controlled studies included in this meta-analysis, only one study (15) included pae-diatric patients <8 years old, but results of this subgroup were not separately reported;
the study by Rea et coworkers reported a tendency towards a worse efficacy of com-pression-only CPR than standard CPR in cardiac arrests of noncardiac origin, and a tendency towards a better efficacy in shock-able rhythm and in rapid (<6 minutes) re-sponse by the Emergency medical System.The results of the present meta-analysis are consistent with the most recent obser-vational study on 4415 cardiac arrests not due to trauma or asphyxia, drug overdose or drowning (20), in which a 5-years data collection was accompanied by a statewide public education campaign aimed to in-crease bystander compression-only CPR. In this study, the incidence of bystander-ini-tiated CPR increased every year, as did the proportion of compression-only CPR; more importantly, overall survival increased sig-nificantly over time. Overall survival to hospital discharge was equal between the no bystander CPR and the standard CPR groups, while survival and neurological out-come were significantly better in the com-pression-only CPR group; compression-only CPR resulted particularly effective when the cardiac arrest was witnessed and presented with a shockable rhythm. In 1128 patients with cardiac arrest of presumed noncardiac origin, not included in the study, survival was lower and not different among the two technique and no bystander CPR. Several reasons could explain the best effi-
Figure 2Forest plot for the comparison of standard CPR vs compression-only CPR on hospital survival after cardiopulmonary resuscitation.
Study or Subgroup Compression-only CRP Standard CRP Peto Odds Ratio Peto Odds RatioStudy or Subgroup Events Total Events Total Weight Peto, Fixed, 95% CI Peto, Fixed, 95% CIHallstrom A et al. 2000 35 241 29 279 16.1% 1.46 [0.87, 2.47]Rea TD et al. 2010 122 981 105 960 57.8% 1.16 [0.88, 1.52]Svensson L et al. 2010 54 620 44 656 26.1% 1.33 [0.88, 2.00]
Total (95% CI) 1842 1895 100.0% 1.24 [1.01, 1.54]Total events 211 178
Heterogeneity: Chi2 = 0.73, df = 2 (P = 0.69); I2 = 0% 0.5 0.7 1 1.5 2Test for overall effect: Z = 2.04 (P = 0.04) Compression-only worse Standard worse

284
L. Cabrini et al.
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
cacy of chest compression-only CPR. It is well documented that both interruptions of chest compressions during ventilation and positive -pressure ventilations have detri-mental effects on survival rate (8). Oxygen-ation and ventilation could be allowed - at least initially- by passive ventilation during chest compressions, by spontaneous gasp-ing and by the lungs capacity to act as a res-ervoir (21) In addition, compression-only CPR is easier to teach, to remember and to perform, and it does not require mouth-to-mouth contact, so resulting in a better will-ingness to start CPR by bystanders (20). It is worth noting that in two of the three ana-lyzed studies (13, 15) bystanders randomly assigned to standard CPR were significant-ly more likely to withhold CPR than callers assigned to compression-only group.Based on our findings, compression-only CPR should be considered as the preferred bystander CPR technique, even if ventila-tions still have a crucial role in cardiac ar-rests of presumed noncardiac origin (18), in children (19) and when resuscitation is started more than 4 minutes after the ar-rest. (10). However, it should be consid-ered that most victims of cardiac arrest are adults, and the cause is cardiac in about 2/3 of cases (20). The importance of ventilations in cardiac arrests lasting more than 3-4 minutes is more controversial, as two recent studies in a porcine models reported contradictory results (22, 23). Likely laypersons training on CPR should be simplified to privilege compression-only CPR; in 2008 the American Heart Associa-tion already recommended that untrained bystanders should provide compression-only CPR for adults with sudden cardiac arrest (24). However, fatigue can be a rel-evant problem decreasing the quality of compressions and a change of CPR provid-ers every one minute instead of every two minutes has been suggested. (25)
CONCLUSIONS
Available evidence from randomized con-trolled trials suggests that compression-on-ly CPR is superior to standard CPR at least when performed by untrained bystander. These results have relevant implications on teaching, and if adequately publicized they should favour a crucial increase in the rate of bystanders performed CPR.
Acknowledgment: We thank Lara Sussani, RA, Zuppelli Paola, RA for the support in data collection and data entry and for revising the manuscript.
Funding Sources: None. The study was supported by departmental funds only.
No conflict of interest acknowledged by the authors.
REFERENCES
1. Lloyd-Jones D, Adams R, Carnethon M, et al. Heart disease and stroke statistics - 2009 update: a report from the American Heart As-sociation Statistics Committee and Stroke Sta-tistics Subcommittee. Circulation 2009; 119: 21-181.
2. Sasson C, Rogers MA, Dahl J, Kellermann AL. Predictors of survival from out-of-hospital car-diac arrest: a systematic review and meta-ana-lysis. Circ Cardiovasc Qual Outcomes 2010; 3: 63-81.
3. Stiell I, Nichol G, Wells G, et al. Health-rela-ted quality of life is better for cardiac arrest survivors who received citizen cardiopulmo-nary resuscitation. Circulation 2003; 108: 1939-1944.
4. Abella BS, Aufderheide TP, Eigel B, et al. Re-ducing barriers for implementation of bystan-der-initiated cardiopulmonary resuscitation. A scientific statement from the American Heart Association for healthcare providers policyma-kers, and community leaders regarding the ef-fectiveness of cardiopulmonary resuscitation. Circulation 2008; 117: 704-709.
5. Locke CJ, Berg RA, Sanders Ab, et al. Bystan-der cardiopulmonary resuscitation. Concerns about mouth-to-mouth contact. Arch Intern Med 1995; 155: 938-943.
Chest compression-only CPR in out-of-hospital cardiac arrest
285
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
6. Cho GC, Sohn YD, Kang KH, at al. The effect of basic life support education on laypersons’ willingness in performing bystander hands only cardiopulmonary resuscitation. Resusci-tation 2010; 81: 691-694.
7. Berg RA, Kern KB, Hilwig RW, et al. Assisted ventilation does not improve outcome in a por-cine model of single-rescuer bystander cardio-pulmonary resuscitation. Circulation 1997; 95: 1635-1641.
8. Ewy GA, Zuercher M, Hilwig RW, et al. Im-proved neurological outcome with continuous chest compressions compared with 30:2 com-pressions-to-ventilations cardiopulmonary re-suscitation in a realistic swine model of out-of-hospital cardiac arrest. Circulation 2007; 116: 2525-2530.
9. Dorph E, Wik L, Stromme TA, et al. Oxygen delivery and return of spontaneous circula-tion with ventilation: compression ratio 2:30 versus chest compressions only CPR in pigs. Resuscitation 2004; 60: 309-318.
10. SOS-KANTO study group. Cardiopulmonary resuscitation by bystanders with chest com-pression only (SOS-KANTO): an observatio-nal study. Lancet 2007; 369: 920-926.
11. Bohm K, Rosenqvist M, Herlitz J, et al. Sur-vival is similar after standard treatment and chest compression only in out-of-hospital bys-tander cardiopulmonary resuscitation. Circu-lation 2007; 116: 2908-2912.
12. Iwami T , Kawamura T, Hiraide A, et al. Effec-tiveness of bystander-initiated cardiac-only re-suscitation for patients with out-of-hospital car-diac arrest. Circulation 2007; 116: 2900-2907.
13. Rea TD, Fahrenbruch C, Culley L, et al. CPR with chest compression alone or with rescue breathing. N Engl J Med 2010; 363: 423-433.
14. Svensson L, Bohm K, Castren M, et al. Com-pression-only CPR or standard CPR in out-of-hospital cardiac arrest. N Engl J Med 2010; 363: 434-442.
15. Hallstrom A, Cobb L, Johnson E, Copass M. Cardiopulmonary resuscitation by chest com-pression alone or with mouth-to-mouth venti-lation. N Engl J Med 2000; 342: 1546-1553.
16. Ong ME, Ng FS, Anushia P, et al. Comparison of chest compression and standard cardiopul-monary resuscitation for out-of-hospital car-
diac arrest in Singapore. Resuscitation 2008; 78: 119-126.
17. Waalewijn RA, Tijssen JG, Koster RW. Bys-tander initiated actions in out-of-hospital cardiopulmonary resuscitation: results from the Amsterdam Resuscitation Study (ARRE-SUST). Resuscitation 2001; 50: 273-279.
18. Kitamura T, Iwami T, Kawamura T, et al. By-stander initiated rescue breathing for out-of-hospital cardiac arrests of noncardiac origin. Circulation 2010; 122: 293-299.
19. Kitamura T, Iwami T, Kawamura T, et al. Conventional and chest-compression-only cardiopulmonary resuscitation by bystanders for children who have out-of-hospital cardiac arrests: a prospective nationwide population-based cohort study. Lancet 2010; 375: 1321-1322.
20. Bobrow BJ, Spaite DW, Berg RA, et al. Chest compression-only CPR by lay rescuers and survival from out-of-hospital cardiac arrest. JAMA 2010; 304: 1447-1454.
21. Berg RA, Nadkarni VM. Hands-only cardio-pulmonary resuscitation: bench-to-bedside or bedside-to-bench? Crit Care Med 2010; 38: 2073-2075.
22. Yannopoulos D, Matsuura T, McKnite S, et al. No assisted ventilation cardiopulmonary re-suscitation and 24-hour neurological outcomes in a porcine model of cardiac arrest. Crit Care Med 2010; 38: 254-260.
23. Wang S, Li C, Ji X, et al. Effect of continuous compressions and 30:2 cardiopulmonary re-suscitation on global ventilation/perfusion va-lues during resuscitation in a porcine model. Crit Care Med 2010; 38: 2024-2030.
24. Sayre MR, Berg RA, Cave DM, et al. Hands-only (compression-only) cardiopulmonary resuscitation: a call to action for bystander response to adults who experience out-of-hos-pital sudden cardiac arrest: a science advisory for the public from the American Heart Asso-ciation Emergency Cardiovascular Care Com-mittee. Circulation 2008; 117: 2162-2167.
25. Nishiyama C, Iwami T, Kawamura T, et al. Quality of chest compressions during conti-nuous CPR: comparison between chest com-pression-only CPR and conventional CPR. Re-suscitation 2010; 81: 1152-1155.
DIVISIONE OSPEDALIERA: Viale Europa, 28 - Milano Oltre 2 - 20090 Segrate Tel. 02.26.92.70.11 - Fax 02.21.39.000
http://www.cea-spa.it/ - E-mail: [email protected]
C E APRESIDI MEDICO-CHIRURGICIPRESIDI MEDICO-CHIRURGICI
SPA
20133 Milano - Piazza Carlo Donegani, 1
287
proceedingsin Intensive Care
Cardiovascular Anesthesia
Endorsed by
proceedings
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
ORIGINAL ARTICLE
Corresponding author:Pradeep Arora, MD Assistant Professor University at Buffalo (SUNY) Veterans Hospital3495 Bailey AveBuffalo, NY 14215e.mail: [email protected]
INTRODUCTION
Cardiac surgery, primarily coronary-artery bypass grafting (CABG), is commonly per-formed on a worldwide basis. The unad-justed mortality in the United States has decreased from last decade, however still remains high at 2.2% according to the So-ciety of Thoracic Surgeons. A number of risk factors are associated with increased
surgical mortality: age, female gender, se-rum creatinine, extra cardiac arteriopathy, chronic airway disease, severe neurological dysfunction, previous cardiac surgery, re-cent myocardial infarction, left ventricular ejection fraction, chronic congestive cardi-ac failure (CHF), pulmonary hypertension, active endocarditis, unstable angina, proce-dure urgency, critical preoperative condi-tion (1). Intra-operative hemodynamic ab-normalities, including hypotension during and post cardiac surgery, pulmonary dia-stolic hypertension have also been shown to be independently associated with increased morbidity and mortality (2, 3). Most of the factors associated with increased mortality
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010; 2: 287-296
ABSTRACT
Introduction: Positive fluid balance during abdominal surgery has been associated with increased morbidity. We hypothesized that administration of large volumes of intravenous fluids in cardiac surgery is associated with increased mortality.Methods: Retrospective analysis of data on 1358 patients who underwent cardiac surgery from 2001 to 2005 at two major hospitals in Western New York. Patients were divided in to those who received intravenous fluids above the median volume (3.9L) and those who received less than the median volume of intra-operative fluid. Acute Kidney Injury Network criteria based on serum creatinine were used to define Acute Kidney injury.Results: Logistic regression and Cox-proportional models showed increased 90 day mortality (HR -2.8, 95% CI -1.16-7.01) in those patients who received greater than the median volume of intravenous during cardiac surgery. This was confirmed with propensity score analysis. Furthermore, the marginal effects analysis re-vealed that after about 4.0 liters of intravenous fluid, the survival probability falls significantly in cardiac surgery patients.Conclusions: Administration of large volumes of intra-operative intravenous fluid is independently associated with an increase in 90 day mortality in cardiac surgery.
Keywords: cardiac surgery, perioperative mortality, outcomes,i fluids, renal dysfunction.
High volumes of intravenous fluid during cardiac surgery are associated with increased mortalityA. Pradeep1, S. Rajagopalam2, H.K. Kolli1, N. Patel1, R. Venuto1, J. Lohr1, N.D. Nader1
1University at Buffalo (SUNY); 2Med. Data Analytics, Buffalo, NY

288
A. Pradeep et al.
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
after cardiac surgeries are non-modifiable. Increased Intravenous Fluid (IVF) in non-cardiac surgery has been shown to be asso-ciated with increased morbidity and com-plications (4). However, controversy still surrounds the type and regimen of fluids to be administered during cardiac surgery. Highly positive intra-operative fluid bal-ance during cardiac surgery has been corre-lated with increased length of hospital stay and increased rates of Intensive Care Unit (ICU) readmission and blood transfusion
(5). We hypothesized that large adminis-tration of intravenous fluid during cardiac surgery is associated with increased 90 day mortality.
METHODS
The study population was drawn from pa-tients who underwent cardiac surgery at 2 tertiary care hospitals affiliated with SUNY at Buffalo: Buffalo Veterans Administration Medical Center (VAMC) and Erie County Medical Center (ECMC). A list of patients who had undergone surgery between Janu-ary 2001 and January 2006 was generated through the hospital record system. This research protocol was approved by the Buf-falo VAMC and SUNY at Buffalo Institu-tional Review Boards. Clinical data was collected using a standard-ized form. Baseline data collection included demographics (age, gender, race, weight, height, BMI, smoking history), co-morbid conditions including congestive heart fail-ure (shortness of breath or weakness with concomitant decreased ejection fraction (<50%) on two dimensional echocardiog-raphy, Anesthesia risk category was deter-mined from American Society of anesthesi-ologist criteria (ASA). Intra-operative data collection included blood pressure, use of vasopressors, IV fluids and urine output. However dose and type of pressors were
not recorded. Postoperatively serial serum creatinine levels, blood pressure, use of va-sopressors, and dialysis requirement were recorded. The total intra-operative IV fluids included Cardiopulmonary bypass (CBP) prime, cardioplegic fluid, crystalloids, col-loids and blood transfusions. Urine output was then deducted from above number. Before 2006, ultrafiltaration was not being performed during surgery.
DefinitionsAcute kidney injury was defined using the Acute Kidney Network (AKIN) criteria: increase in serum creatinine of ≥0.3 mg/dl (25 μmol/l) or an increase of 50-200% from baseline (6). We did not use urine out-put criteria in defining AKI.Race was categorized as Caucasian, African American, or other based on what patient noted in his medical record. Type of surgery was defined as elective or emergency as per surgical attending note. Hypotension was defined as Systolic Blood pressure less than 90 for more than 15 min-utes during the surgery.ASA was determined from preoperative anesthesia records and stratified into 5 cat-egories. ASA 1 was defined as a healthy in-dividual; ASA 2-patient with mild systemic disease; ASA 3-patient with severe systemic disease; ASA 4-patient with severe system-ic disease with constant threat to life; ASA 5-moribund patient who is not expected to survive without surgery. The incidence of all cause mortality was recorded 90 day pe-riod from the date of surgery.
Statistical analysisPatients were divided into those who re-ceived above median intra-operative IVF (>3.9 liters) and those intra-operative IVF was at or below median (≤3.9 liters). The reason to use median to estimate the risk is based on logistic regression analysis showing increasing risk with increasing

Intravenous fluids during cardiac surgery
289
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
IVF especially after 4 liters. Descriptive statistics and/or frequency distributions was obtained for age, gender, body mass in-dex (BMI), preoperative use of angiotensin converting enzyme inhibitors (ACEI) and NSAIDS, preoperative presence of cardiac failure, hypertension, diabetes mellitus, chronic obstructive pulmonary disease, gas-trointestinal disorder diseases, liver disease and neurological disease, intra-operative vasopressors and hypotension, and postop-erative hypotension, vasopressors use and development of acute kidney injury for all patients. The comparison of continuous variables for patients in the above-median and below-median intra-operative IVF groups was performed using Wilcoxson rank sum test and the comparison of pro-portions was done using the Chi-square test or the Fisher exact test. We used logistic regression and Cox pro-portional models to determine the effect of intra-operative IVF on mortality. For both logistic regression and Cox proportional methods, we constructed several models. First, intra-operative IVF was included as a continuous variable in a stepwise selec-tion model along with other factors. Next we included intra-operative IVF as a di-chotomous variable using median value as the separation point as described above, in a stepwise selection along with other variables. Further, we matched the below-median and above-median groups using propensity score. The propensity score was calculated from a stepwise selection logistic model that included all pre-operative vari-ables. The matching was done using the nearest neighbor algorithm with a caliper of 0.01. A final logistic model of mortality was based on the matched sample that in-cluded only those variables that were not balanced and the dichotomous indicator for above or below median. We were also inter-ested in identifying the marginal effect of IVF on mortality from the logistic regres-
sion model. The marginal effect of a predic-tor is defined as the partial derivative of the event probability with respect to the predic-tor of interest. A more direct measure is the change in predicted probability for a unit change in the predictor from one level to another and can be directly computed by estimating pxi-pxj, the difference in event probabilities at levels i and j of the predic-tor, here a unit change in IVF (measured in liters). Note that the marginal effect is not constant and depends on the level of the predictor variable. We calculated the pre-dicted probability for unit change in IVF at different values of IVF and plotted them for various combinations of other binary predictors. Finally we also derived KM curves for cumulative probability of sur-vival for different values of IVF. Model fit was assessed with the Hosmer-Lemeshow goodness-of-fit test. SAS 9.1.3 was used to estimate the KM survival function and the Cox models.
RESULTS
Thirteen hundred and fifty eight patients over the age of 18 years who underwent cardiac surgery at two major hospitals in Western New York between 01/1/2001 to 12/31/2005 were the subjects of study. The mean age of patients was 65.9 (+11.4) years. The majority of the patients were Caucasians (86%) and were male (79.2%). The mean BMI was 29.3 (±5.9). 33.7% had diabetes, 80% had hypertension, 20% had CHF and 18% had COPD. The mean baseline serum creatinine was 0.96 (±0.21) mg/dl and the majority of the surgery was CABG alone (87%) and done electively (91%) with cardiopulmonary bypass pump (69%). The mean use of IV fluids during surgery was 3910 ml (±2121). 44.6% de-veloped hypotension during operation and 13% developed hypotension after opera-

290
A. Pradeep et al.
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
tion. The mean length of hospital stay of all patients was 8 (±10.4) days. The distribution of demographic variables, co-morbidities, intra- and post-operative risk factors across the 2 groups of IVF ad-ministration are shown on Table 1. Factors associated with increased intra-operative IVF administration were: male gender, cau-casian race, ASA risk of 4/5, combined sur-gery, higher preoperative serum creatinine level, CHF, COPD, hypotension during sur-gery, use of intra-operative vasopressors, on-pump surgery, and non elective surgery. Thirty seven patients died within 90 days of surgery. The mortality among patients who received greater than the median amount of IVF was 5.12/10,000 patient-year compared to 1.15 in patients who received less than the median volume of IVF. Univariate analysis showed that administration of greater than median volume of intra-operative IVF was significantly associated with higher 90 days mortality (p-0.002) (Figure 1). In addition,
univariate analysis also showed that higher age, CHF, anesthesia risk category 4 and 5, intra- or post-operative hypotension and higher baseline serum creatinine were sig-nificantly associated with 90 days mortality. Several adjusted Cox proportional hazard models and logistic models were built and the effect of demographic variables, anes-thesia risk category 4/5, intra-operative risk factors and postoperative risk factors were included. After including the effect of all sig-nificant variables administration of greater than the median amount of IVF intra-oper-atively remained an independent risk factor for the 90 days mortality after cardiac sur-gery (Table 2). The unmatched models of mortality with IVF as a continuous variable and as a binary variable indicate that high levels of IVF increased the risk of mortality. For every liter of IVF given during surgery the odds of death increased by 27%. Simi-larly for patients who receive above median IVF the odds of mortality were 3.6 times
Table 1 - Frequency distribution and Univariate Statistics of Variables by IVF administrat
Variable IVF < Median (%) IVF > Median (%) P§
Age* 65.4 (+11.9) 66.4 (+12.0) 0.1
Female 174 (25.5%) 109 (89.0) 0.008
White 574 (84.0) 600 (89.0) <.0001
Body Mass Index* 29.31 (+5.99) 29.31 (+6.21) 0.9
Diabetes 157 (28.34%) 141 (32.87%) <.0001
Hypertension 417 (75.27%) 351 (81.82%) 0.0001
CHF 80 (14.44%) 75 (17.48%) <.0001
COPD 75 (13.54%) 85 (19.81%) 0.001
Serum Creatinine at Baseline* 0.94 (+0.19) 0.94 (+0.21) <.0001
Anesthesia Risk Category ≥4 129 (23.29%) 140 (32.63%) <.0001
Elective/Urgent Surgery 519 (93.68%) 391 (91.14%) 0.002
Surgery Type - CABG 510 (92.06%) 380 (88.58%) <.0001
On Pump Surgery 342 (61.84%) 295 (68.93%) <.0001
Intra-operative Hypotension 204 (36.82%) 198 (46.15%) <.0001
Intra-operative IVF use* 3701 (+1996) 3960 (+2302) 0.0001
Post-operative Hypotension 56 (10.11%) 56 (13.05%) 0.004*Value expressed in Mean (+ SD); §p-value calculated by CMH Test for fixed variables and by Kruskal-Wallis Test for con-tinuous variables. IVF - Intravenous fluids. Note: Conversion factors for units: serum creatinine in mg/dL to mol/L, ×88.4

Intravenous fluids during cardiac surgery
291
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
Figure 1Univariate analysis showing risk of mortality and IVF.
Table 2 - Analysis of Maximum Likelihood Estimates.
Variable Parameter Estimate
Standard Error Chi-Square Pr > ChiS Hazard
Ratio95% Confidence
Limits
IVF ≥ Median 0.96 0.42 5.01 0.025 2.61 1.12 6.06
Anesthesia Risk Category ≥4 1.26 0.35 12.31 0.0004 3.53 1.74 7.14
Post-operative Hypotension 1.51 0.34 18.89 <.0001 4.56 2.30 9.06
Intra-operative Hypotension 0.71 0.40 3.18 0.075 2.05 0.93 4.52
Change in Peak creatinine* 0.76 0.13 34.44 <.0001 2.15 1.66 2.78
On/OffPump -0.88 0.36 6.03 0.014 0.41 0.20 0.83
Table 3 - Odds Ratio Estimates (Multivariate Analysis).
Effect Point Estimate 95% Wald Confidence Limits
IVF ≥ median Vs < Median 3.61 1.54 8.43
Intra-operative Hypotension 3.27 1.49 7.17
AKI 2.61 1.28 5.30
Off –Pump 0.42 0.21 0.87IVF = Intravenous fluids. AKI = Acute Kidney Injury.

292
A. Pradeep et al.
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
higher than those for patients at or below median (Table 3). Sensitivity analysis was done for intra-operative IVF administration based on BMI and weight and no difference was noted.The propensity score model could match only 494 patients from each group. The outcome model after matching also estab-lished increased risk of mortality with ad-ministration of higher volume of IVF al-though the odds were reduced to 2.86 (CI 1.16-7.01) (Table 4).The predicted probability increased at every level of IVF. The marginal effects further
Table 4 - Odds ratio estimates based on propensity score matched patients
Effect Point Estimate
95% Wald Confidence Limits
Age 1.04 1.0 1.09IVF ≥ than Median 2.85 1.16 7.01
Intra-operative Hypotension 3.25 1.35 7.82
ASA risk 2.74 1.20 6.25
AKI 2.69 1.08 6.69
Off -Pump 0.37 0.16 0.88IVF = Intravenous fluid. AKI = Acute Kidney Injury. ASA = American Society of Anesthesiologists.
Figure 2Survival Probability Vs IVF.
Figure 3Predicted Effect of IVF for Different Intra-operative Hypotension and AKI.

Intravenous fluids during cardiac surgery
293
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
demonstrate that change in the probability for unit change in IVF also increases at ev-ery level of IVF. Finally the survival curves indicate that after about 4.0 liters of IVF, the survival probability falls and drastically changes above 9 liters (Figure 2). Mortality was further increased with presence of in-traoperative hypotension and later develop-ment of AKI (Figure 3).
DISCUSSION
We found that administration of greater than the median amount of IV fluid during cardiac surgery was associated with a great-er than three-fold increase in mortality. In univariate analysis, preoperative variables that were significantly associated with mortality included increasing age, com-bined valve surgery and CABG compared to CABG alone, ASA category 4/5 compared to 2/3, intra- and post- operative hypoten-sion, CHF, and change in serum creatinine and more than median IVF. Adjusting for these factors in logistic and Cox models confirmed the association of greater than the median amount of intravenous fluid with increased mortality. Furthermore, propensity score analyses confirmed the re-sults (HR 2.86).Currently, the practice of giving IV fluids is often dictated by a non evidence based approach, taking account of pre-operative deficit, maintenance requirements, and extrapolated third space losses (7). There is a perception that patients who are un-dergoing cardiac surgery require liberal fluid replacement, there are no evidence based guidelines on how much fluid to give. Moreover evidence suggests that extracel-lular volume is well maintained after sur-gery due to the neuro endocrine responses
(8). There may be a tendency to use more IVF during cardiac surgery especially in patients who develop hypotension. Intra-
operative hypotension is an independent predictor of death in cardiac surgery pa-tients. We adjusted our analysis with intra-operative hypotension in the model, the ef-fect of IVF remain significant on mortality (Figure 3). Although data is lacking on the association of IVF amount and mortality in cardiac surgery patients, Toraman et.al showed that increased intra-operative flu-id balance in cardiac surgery is associated with increased length of hospital stay (5). The study did not show significant increase in mortality with increased IVF. However, this study only examined patients who had more than 500 cc of positive fluid balance. In addition, studies of patients undergoing colorectal and abdominal surgeries ran-domized to restrictive and standard fluid IV fluid administration showed an increase in postoperative morbidity and longer hos-pital stay in the latter group (9, 10). Increas-ing weight, indicative of water and salt retention, has been shown to correspond with increased mortality while achieving a negative balance within the first 72 hours of ICU admission has been postulated as an independent predictor of survival (11). Indeed, sepsis trials have shown an asso-ciation between volume overload and ad-verse clinical outcomes (12-15). Recently, Bouchard et al showed that fluid accumula-tion (defined by increase of more than 10% weight from baseline) among 618 critically ill patients with AKI was associated with higher odds of death (16). In our study, we showed that a patient who receives higher than median IVF during cardiac surgery had significantly higher 90 day mortality. However the use of median is only an ar-bitrary number as there is no data in the literature to show what the optimum IVF is. Now a day, ultrafiltration is being em-ployed during surgery, the effect of which on mortality is not studied so far. We did not use ultrafiltration during surgery in our patients.

294
A. Pradeep et al.
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
The mechanisms by which increased ad-ministration of intravenous fluid may re-sult in increased mortality are unclear. Two mains factors that may contribute are: 1) development of congestive heart failure;
and 2) hemodilution. Hemodilution has been linked to decreased oxygen delivery, increased lactate produc-tion and increased risk of AKI and mortal-ity (17-19). Indeed, Lassnigg et. al showed a significant increase in mortality in the group of patients with the most pronounced fall in postoperative serum creatinine (≥0.3 mg/dl) (20). Patients who had less than a 0.3 mg/dl drop in serum creatinine had bet-ter outcomes compared to those who had a decrease greater than 0.3 mg/dl. Cardio-pulmonary bypass (CPB) may cause sys-temic inflammatory response syndrome (SIRS) (21, 22). leading to third space fluid loss. Contact of blood components with the artificial surface of the bypass circuit, ischemia-reperfusion injury, endotoxemia, operative trauma, and non-pulsatile blood flow, are possible causes of SIRS in this sit-uation (1, 23). This inflammatory response and increased vascular permeability in con-junction with massive intravenous fluid ad-ministration leads to extravascular fluid ac-cumulation and pulmonary edema and pro-longs the stay in the hospital (24). In one study interstitial fluid volume increased by an average of 14% during coronary artery bypass graft surgery (25).. During cardiac surgery, the patient is exposed to the ad-ministration of a considerable amount of intravenous fluids. Such fluids include the preoperative period, intra-operative period including CPB pump prime, the fluids used for cardioplegia and fluids given to deal with hypotensive episodes and in the post-operative period (26, 27). This increased fluid overload burdens a heart which often is weakened by the original pathology for which surgery is being done. Often it leads
to fluid overload which may participates in the pathogenesis of postoperative hypox-emia, myocardial edema and organ edema leading to a delay in recovery. Myocardial edema has been implicated as the cause of an increase in left ventricle stiffness and a decrease in the LV volume (28). This can lead to vicious cycle of hypotension and administration of more IVF further exacer-bating the edema. Our study has several strengths. We includ-ed all patients who had undergone cardiac surgery in 2 different academic medical centers in with different demographics and clinical condition, increasing the gener-alizability of our results. Furthermore we used propensity score analysis adjust for confounding by indication. There are im-portant limitations to our study. We did not distinguish whether IVF was crystalloid or colloid,or CBP prime. We did not account for the variability of IVF administration based on surgeon or the anesthesiologist. Since this being a retrospective study we do not have a data on why increased IVF were used in some patients and what in-traoperative techniques were used to deter-mine it. Our results could be confounded by other factors such as renal dysfunction events. However adjusting for AKI in our study, effect of increased IVF on mortality remains significant. Since this is a retro-spective study, even with various logistic models, we cannot truly evaluate the ef-fect of intravenous fluid on mortality as we could in prospective randomized trial. Al-though propensity score model can adjust for confounding by indication, it may not eliminate residual unobserved factors.
LimitationsIn the median number of 3.9 liters is ar-bitrary cut off and cannot be established. However, marginal effects analyses further confirm that above 4.0 liters of IVF, the sur-vival probability falls and drastically chang-

Intravenous fluids during cardiac surgery
295
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
es above 9 liters. Since this is a retrospec-tive study, even with various logistic mod-els, we cannot truly evaluate the effect of intravenous fluid on mortality as we could in prospective randomized trials. Further studies are needed to confirm these results.
CONCLUSIONS
We have shown an association between administering increasing volumes of in-travenous fluid during cardiac surgery and increased risk of mortality at 90 days. We suggest a more judicious and conservative approach to intra-operative intravascular volume expansion for all patients.
Funding Sources: This study was partially funded by an Evidence Based Medicine Quality Improvement Proj-ect Award from the Donald W. Reynolds Foundation.
No conflict of interest acknowledged by the authors.
REFERENCES
1. Roques F, Nashef SA, Michel P, et al. Risk fac-tors and outcome in European cardiac surgery: analysis of the EuroSCORE multinational da-tabase of 19030 patients. Eur J Cardiothorac Surg 1999; 15: 816-822.
2. Reich D, Bodian C, Krol M, et al. Intraopera-tive hemodynamic predictors of mortality, stroke, and myocardial infarction after coro-nary bypass surgery. Anesth Analg 1999; 89: 814-820.
3. Kuralay E, Demirkilic U, Oz BS, et al. Primary Pulmonary hypertension and coronary artery bypass surgery. J Cardiac Surg 2002; 17: 79-80.
4. Rahbari NN, Zimmermann JB, Schmidt T, et al. Meta-analysis of standard, restrictive and supplemental fluid administration in colorec-tal surgery. British Journal of Surgery 2009; 96: 331-341.
5. Toraman F, Evrenkaya S, Yuce M, et al. Highly positive intraoperative fluid balance during cardiac surgery is associated with adverse out-come. Perfusion 2004; 19: 85-91.
6. Mehta RL, Kellum JA, Shah SV, et al. Acute Kidney Injury Network (AKIN): report of an initiative to improve outcomes in acute kidney injury. Crit Care 2007; 11: 31.
7. Shields CJ. Towards a new standard of peri-operative fluid management. Ther Clin Risk Manag 2008; 4: 569-571.
8. Brandstrup B, Svenson C, Engquist A. Hemor-rhage and operation cause a contraction of the extracellular space needing replacement-evi-dence and implications? A systematic review. Surgery 2006; 139: 419-432.
9. Brandstrup B, Tonnesen H, Beirer-Holgersen R, et al. Effects of intravenous fluid restric-tion on postoperative complications; compa-rision of two perioperative fluid regimens. A randomized assessor-blinded multicenter trial. Ann Surg 2003; 238: 641-648.
10. Holte K, Klarskov B, Christensen DS, et al. Liberal versus restrictive fluid administration to improve recovery after laparoscopic chole-cystectomy: a randomized, double-blind study. Ann Surg 2004; 240: 892-899.
11. Lowell JA, Schifferdecker C, Driscoll DF, et al. Postoperative fluid overload: not a benign problem. Crit Care Med 1990; 18: 728-733.
12. Simmons RS, Berdine GG, Seidenfeld JJ, et al. Fluid balance and the adult respiratory distress syndrome. Am Rev Respir Dis 1987; 135: 924-929.
13. Sakr Y, Vincent JL, Reinhart K, et al. High tidal volume and positive fluid balance are associ-ated with worse outcome in acute lung injury. Chest 2005; 128: 3098-3108.
14. Wiedemann HP, Wheeler AP, Bernard GR, et al. Comparison of two fluid-management strat-egies in acute lung injury. N Engl J Med 2006; 354: 2564-2575.
15. Van Biesen W, Yegenaga I, Vanholder R, et al. Relationship between fluid status and its man-agement on acute renal failure (ARF) in inten-sive care unit (ICU) patients with sepsis: a pro-spective analysis. J Nephrol 2005; 18: 54-60.
16. Bouchard J, Soroko SB, Chertow GM, et al. Fluid accumulation, survival and recovery of kidney function in critically ill patients with acute kidney injury. Kidney International 2009; 76: 422-427.
17. Swaminathan M, Phillips-Bute BG, Conlon PJ, et al. The association of lowest hematocrit dur-ing cardiopulmonary bypass with acute renal

296
A. Pradeep et al.
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
injury after coronary artery bypass surgery. Ann Thorac Surg 2003; 76: 784-792.
18. Johannes T, Mik EG, Nohé B, et al. Acute de-crease in renal microvascular PO2 during acute normovolemic hemodilution. Am J Physiol Re-nal Physiol 2007; 292: 796-803.
19. Rosner MH, Okusa MD. Acute kidney injury associated with cardiac surgery. Clin J Am Soc Nephrol 2006; 1: 19-32.
20. Lassnigg A, Schmidlin D, Mouhieddine M, et al. Minimal changes of serum creatinine pre-dict prognosis in patients after cardiothoracic surgery: a prospective cohort study. J Am Soc Nephrol 2004; 15: 1597-1605.
21. Cremer J, Martin M, Redl H, et al. Systemic in-flammatory response after cardiac operations. Ann Thorac Surg 1996; 61: 1714-1720.
22. Taylor K. SIRS-The systemic inflammatory response syndrome after cardiac operations. Ann Thorac Surg 1996; 61: 1607-1608.
23. Butler R, Rocker GM, Westaby S. Inflamma-
tory response to cardiopulmonary bypass. Ann Thorac Surg 1993; 55: 552-559.
24. Holte K, Sharrock NE, Kehlet H. Pathophysil-ogy and clinical implications of perioperative fluid excess. Anaesth 2002; 89: 622-632.
25. Olthof CG, Jansen PG, Vries JP, et al. Intersti-tial fluid volume during cardiac surgery mea-sured by means of a non-invasive conductivity technique. Acta Anaesthesiol Scand 1995; 39: 508-512.
26. Boldt J. Volume therapy in cardiac surgery. An-nals of Cardiac Anaesthesia 2005; 8: 104-116.
27. Bellomo R, Raman J, Ronco C. Intensive care unit management of the critically ill patient with fluid overload after open heart surgery. Cardiology 2001; 96: 169-176.
28. Amirhamzeh MM, Hsu DT, Cabreriza SE, et al. Myocardial edema: comparison of effects on filling volume and stiffness of the left ventricle in rats and pigs. Ann Thorac Surg 1997; 63: 1293-1297.

Nei nostri farmaci equivalentic’è tanta scienzaquanta negli originatori.

Nei nostri farmaci equivalentic’è tanta scienzaquanta negli originatori.

299
proceedingsin Intensive Care
Cardiovascular Anesthesia
Endorsed by
proceedings
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
CASE REPORT
Corresponding author:Emanuele Piraccini, MDAnaesthesia and Intensive Care Unit, Ospedale “G.B. Morgagni-Pierantoni” Viale Forlanini, 34 - 47100 Forlì, Italye-mail: [email protected]
INTRODUCTION
The altered postoperative physiology after pneumonectomy interventions can cause severe implications, especially in patients receiving adjuvant therapy for advanced lung cancer (1). We report a case of left diaphragmatic her-nia after left pneumonectomy.
CASE REPORT
A 60 year-old man with malignant pleural mesothelioma underwent a thoracotomy through double incision (5th and 7th in-tercostal spaces) for left pleuro-pneumo-nectomy and diaphragmatic resection af-ter chemotherapy. The pre operative chest computed tomography scan showed a pat-
tern of centrolobular emphysema. Forced expiratory volume was 82% preoperatively and 70% as predictive post operative value. Cardiac function was assessed by an echo-cardiogram which showed an ejection frac-tion of 64%. A thoracic epidural catheter was placed before anaesthesia induction and a mixture of ropivacaine 0.375% and fentanyl was used during the intervention and postoperative period.Parietal pleural dissection produced a sig-nificant blood loss and red blood cells and fresh frozen plasma transfused. Recon-struction was obtained with a pericardial patch, diaphragm plastic and suture. Chest drains were placed and not connected to suction. The patient did not meet the ex-tubation criteria and was transferred to the intensive care unit. On intensive care unit admission the pa-tient was hypotensive (blood pressure= 90/60 mmHg) and treated with fluids. Chest X-ray was normal (Figure 1) and the patient was extubated 40 minutes thereaf-ter. An hypotensive episode (blood pres-
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010; 2: 299-300
ABSTRACT
Patients undergoing pneumonectomy can suffer by cardiovascular and respiratory postoperative complica-tions that can affect patient’s outcome by increasing morbidity and mortality.We describe a diaphragmatic hernia occurring after pneumonectomy. with late presentation and with epidural analgesia confusing the scenario suggesting that anesthesiologists should remain aware on this complication even in the late post operative period.
Keywords: thoracic surgery, cardiothoracic intensive care, diaphragmatic hernia.
Left diaphragmatic hernia after pneumonectomyE. Piraccini, V. Agnoletti, R.M. Corso, J. Chanis-Vargas, S. Gaetani, G. Gambale Anaesthesia and Intensive Care Unit, “G.B. Morgagni-Pierantoni” Hospital, Forlì, Italy

300
E. Piraccini et al.
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010, Vol. 2
sure 60/40 mmHg) and tachypnea (respi-ratory rate =32 breaths per minute) were treated with fl uids, dopamine (5 mcg/kg/min)And interruption of the epidural in-fusion. A transesophageal echocardiogram and cardiac troponin were normal. A chest X-ray with contrast administration trough nasogastric tube was performed. Respira-tory arrest and asytolia were treated fol-lowing advanced life support guidelines including chest compressions, atropine e.v. bolus and tracheal intubation. The chest X-
ray showed gastric and spleen herniation through a diaphragmatic breach (Figure 2). Gastric hernia was surgically reduced and the diaphragm repaired with a prothesis. Dopamine infusion was interrupted during the operation, the patient was extubated in the intensive care unit six hours later dis-charged from the hospital on the 6th post op-erative day without further complications.
DISCUSSION
The mortality rate after pneumonectomy is 6%, the major causes of death being pneu-monia, pulmonary edema, pulmonary em-bolism, myocardial infarction, empyema and bronchopleural fi stula. Gastric hernia is a rare postoperative complication usually diagnosed at the fi rst postoperative chest Xray (1,2).In our case the diagnosis was challenging because the hernia became evident only after intensive care unit admission and be-cause the epidural analgesia confused the clinical scenario: this technique was con-sidered the cause of persistent hypotension. The left pneumonectomy likely created a vacant space into which the stomach acute-ly herniated compressing the heart and cre-ating a cardiac tamponade.
CONCLUSIONS
In patients with hypotension after left pneumonectomy a high index of suspicion should be observed for diaphragmatic her-nia during the whole postoperative period.
No confl ict of interest acknowledged by the authors.
REFERENCES
1. Tsukada G, Stark P. Postpneumonectomy complica-tions. Am J Roentgenol 1997;169:1363-1370.
2. Blum MG, Sundaresan RS. Giant hiatal hernia with gastric volvolus complicating pneumonectomy. Ann Thorac Surg 2006; 81:1491-2
Figure 1 - This figure shows the first chest X-ray (immediately after the admission in the intensive care unit).
Figure 2 - This figure shows the diaphragmatic herniation (the chest Xray was performed immedi-ately before cardirespiratory arrest).

LA STESSA COMPROVATA VALUTAZIONE DELLO STATO DI COSCIENZA DELLA TECNOLOGIA BIS, MIGLIORATA CON FUNZIONALITÀ DI MONITORAGGIO SUI DUE EMISFERI CEREBRALI.
Il sistema di monitoraggio bilaterale BIS VISTA e il sensore bilaterale BIS consentono di effettuare il rilevamento delle differenze di attività EEG tra gli emisferi cerebrali, utile per le applicazioni di monitoraggio avanzate.
TRA LE FUNZIONI BILATERALI AVANZATE:
• Monitoraggio EEG a 4 canali• Indicatore asimmetria (ASYM)• Density Spectral Array (DSA)
Sistema di monitoraggio bilaterale BIS VISTA™
Un metodo completamente nuovo per la valutazione di entrambi gli emisferi cerebrali

Sistema di monitoraggio bilaterale BIS VISTA™
Un metodo completamente nuovo per la valutazione di entrambi gli emisferi cerebrali
INDICATORE ASIMMETRIA (ASYM)
Indicatore delle differenze dell’attività EEG emisferica
EEG 4 CANALIMigliore comprensione dell’attività EEG del paziente
DENSITY SPECTRAL ARRAY (DSA)
Rappresentazione grafica delle differenze della frequenza EEG tra i due emisferi
INFORMAZIONI PER L’ORDINAZIONE
Codice prodotto Descrizione
186-1015KIT
Il sistema di monitoraggio bilaterale BIS VISTA comprende:
• Monitor BIS VISTA
• BISx4™ con cavo PIC-4
186-0224-AMS BISx4 con cavo PIC-4186-0212 Sensore bilaterale BIS
COVIDIEN, COVIDIEN con logo, il logo Covidien e “positive results for life” sono marchi registrati di Covidien AG negli Stati Uniti e/o in altri paesi.Altri marchi appartengono a una delle società Covidien. © 2010 Covidien. Tutti i diritti riservati. - C-MN-BISBilateral/IT - 06/2010
www.covidien.comCovidien Italia SpA
Via Rivoltana, 2/d I-20090 Segrate (Mi) Italia
+39 02 703171 [t] +39 02 703 173 17 [f]
Covidien Switzerland Ltd.
Roosstrasse 53 CH-8832 Wollerau Switzerland
+41 (0) 44 786 50 50 [t] +41 (0) 44 786 50 10 [f]

303
PaPers, Posters, Presentations: communicating the biomedical sciences
proceedingsin Intensive Care
Cardiovascular Anesthesia
Endorsed by
proceedings
hsr Proceedings in intensive care and cardiovascular anesthesia 2010, Vol. 2
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010; 2: 303-305
Corresponding author:Prof. Michael JohnUniversità Vita-Salute San Raffaele, Milan, ItalyVia Olgettina, 48 - 20132 Milan, Italye.mail: [email protected]
in the allotted time, having too much to say in the allotted time, feeling inadequate (especially linguistically inadequate) and a general dislike of being ‘put under the mi-croscope’. Body language is a very important part of a presentation. A good way to study body language is by turning down the volume of your TV to watch newsreaders, actors and talk-show hosts who are able to use fa-cial expressions, head nodding, smiles and frowns to convey a million emotions.
People often ask me what they should do with their hands during a presentation. Well, what you shouldn’t do is probably easier to describe:• do not play with things in your pockets,
such as coins or keys• never put both hands into your pockets
- this is just too casual • do not fold your arms across your chest• do not wave your arms around so you
seem like a windmill• avoid playing excessively with your hair
and your spectacles
You can move your hands around a bit to add some kind of dramatic and theatrical effect to what you are saying. You do not need to keep your arms vertical and rigid, as if you are a soldier standing to attention. In any case, your hands will be necessary to hold your laser pointer, or eventually change slides on your computer, so it will
According to ‘The Book of Lists’, which, as you might be able to understand from its title, is not exactly the type of publication you will find on Pubmed, the fear of speak-ing in public is second only to being burnt alive! Statistically speaking, this means that a certain number of people might even seriously consider being burnt alive rather than have to face the torment and ordeal of speaking before an audience. A peer audi-ence at that. Yet, it has to be said that ner-vousness before a presentation is more than normal. Unfortunately, it is a problem that causes not only suffering for the speaker, but can also destroy even a well-prepared presentation. A good rush of adrenalin can, of course, be used to your advantage and give you a push in the right direction. The secret is knowing how to conceal and con-trol your nervousness. Most congress speakers worry about being judged negatively by others. People don’t want to look stupid and, moreover, don’t wish to fail to deliver the correct answers during ‘question time’ (which we spoke about in detail last time). Other reasons why people are nervous during oral presen-tations involve such things as fear of failure and fear of the unknown, forgetting what you have to say, not having enough to say
message in a body: controlling your nerves during an oral presentationM. JohnProfessor of Applied English, Faculty of Medicine, Università Vita-Salute San Raffaele Milan, Italy
304
M. John
hsr Proceedings in intensive care and cardiovascular anesthesia 2010, Vol. 2
be impossible to keep them in the same po-sition throughout your talk. Then we have the so-called ‘pause noises’, such as ums and ers, which should never become too noticeable (a teacher at school was so boring that we students would pre-fer to count his ums and ers rather than lis-ten to his excruciatingly tedious lessons). Don’t speak too quickly or too quietly, drink water if your throat goes dry and try to control your breathing. Taking one or two deep breaths before speaking will gen-erally make you feel more relaxed. Correct breathing patterns will also enhance voice volume and projection, which will no doubt be appreciated by your audience. Eye contact is fundamental. Scan the au-dience and involve everyone present in your presentation, whether they are ten or a thousand. Never stare at people for too long as you might intimidate them, and also avoid private conversations with friends or members of the audience that look nice be-cause they are nodding at everything you say and seem to agree with you all the time.
Of course, the main thing to remember when you are speaking in public is that you have to at least give the impression, even when it might not be absolutely true, that you are enjoying yourself and wish for nothing more than to communicate your fascinating data to the gathered peer audi-ence. When speakers are too worried about not being able to tell their story they some-times disengage and don’t seem interested in communicating at all. This is, of course, a defence mechanism, but flat uninterest-ing and, what is more serious, uninter-ested voices are the sad result. The overall impression is that they couldn’t care less about speaking to the audience: not a good tactic to use. Remember that successful communication is always a two-way matter. Even though you are talking to the audience, you should still sense their reaction to what you are saying. Work on all these things, and not only on your PowerPoint slides and data, if you want your presentation to be memo-rable.
Questions from the readers
1 how long should you spend on each slide so as not to bore the audience?
This depends on the type of slide you are describing. Simple slides can be presented in 30 seconds, while more complex ones can take up a minute or more. In any case, as a rule you should never spend more than two minutes on any slide.
2 considering the fluctuating atten-tion of the audience, and the im-portance to transmit certain fun-
damental data, should we aim to transmit our key points when the audience is fully concentrated? can we use intermediate-conclu-sion terms such as ‘to summarise’ or ‘in conclusion’ to focus drifting audience attention, and how often might we do so without losing the audience’s respect and trust? is it absolutely wrong to transmit im-portant data when the audience is not 100% concentrated and can this type of phrase help regain au-dience attention?
If you are a dynamic speaker and give the impression that what you are speaking

message in a body: controlling your nerves during an oral presentation
305
hsr Proceedings in intensive care and cardiovascular anesthesia 2010, Vol. 2
‘This is the eighth of a series of articles on this topic.Send any questions to [email protected] who will answer them as part of this column’
about is fundamental for the audience’s professional future, then there is no reason they will not listen to you, with or without intermediate conclusions, as long as your data are valid.
3 how should a case report be set out?
A case description is generally told in chronological order:• patient’s presenting signs and symptoms
and chief complaint(s)• medical history e.g. family diseases such
as heart disease or diabetes• social history such as alcohol, drugs, to-
bacco• medications being used• results from physical examination and
laboratory tests• differential diagnosis• final diagnosis (es)• treatment and follow-upDifferent journals have different styles. Each journal will make it clear if they want or not a brief introduction, a presentation of the case report and a discussion/conclu-sion. The above described order/check list applies to the case report paragraph.
4 While presenting a poster, should we follow the standard imrad (introduction, methods, results and discussion) scheme?
A poster generally follows the standard IM-RAD format, although there is usually no abstract, methods are kept to a minimum
and, most importantly, there is no long Discussion section. A poster should fo-cus mainly on the principal results of the study being presented and should use as many images (graphs, tables, photographs) as possible to stimulate interest and attract viewers. You can change the order around to make things ‘more interesting’ if you think this will do the job.
5 Which is the best way to use a mi-crophone during public speaking?
A microphone needs to be held close to your mouth so that it actually picks up your voice. Cable microphones can be an-noying (due to the cable); radio frequency microphones give you more freedom to move around. Be sure to give a microphone to questioners so the rest of the audience can actually hear the question before you answer.
6 how can you effectively commu-nicate orally during a slide pre-sentation when your audience is divided into two different catego-ries (e.g. nurses and doctors or surgeons and anesthesists)?
Who is in the audience will determine the type of presentation you give. Find out be-forehand.

For more information, visit www.proactivecounterpulsation.com or call 1-866-699-IABP (4227) (United States)/1-610-655-8520 (International).
INTRA-AORTIC BALLOON CATHETER
Introduced in 2003 and proven in thousands of patient procedures in more than 45 countries, Arrow FiberOptix, the world’s firstfiber optic IAB catheter, is an essential element of ProActiveCounterPulsation. Delivering 98% timing accuracy even duringsevere arrhythmias, ProActive CounterPulsation offers the uniqueability to anticipate and adjust to individual AV closures within eachand every cardiac cycle, increasing the time for coronary perfusionand decreasing afterload. Proven performance and greater peace of mind—ProActive CounterPulsation is achieved through:
• FiberOptix technology
• Aortic flow timing
• WAVE® software
• AutoPilot™ mode of operation
Get proactive…with Arrow FiberOptix.
Only the Arrow FiberOptix™ catheter delivers…
ProActive CounterPulsation™
Caution: U.S. Federal law limits this device to sale by or on order of a physician. Contents of unopened, undamaged package are sterile.Disposable. Refer to package insert for current warnings, indications, contraindications, precautions, and instructions for use. Patent Nos. 6,258,035, 6,569,103, 6,887,206, and 5,913,814; additional patents pending.© 2007 Arrow International, Inc. U.S.A. All rights reserved. 2/07 CRB-07-0066
www.teleflexmedical.com

307
proceedingsin Intensive Care
Cardiovascular Anesthesia
Endorsed by
proceedings
Calendar for future meetingsIntensive Care, Surgery and Cardiovascular Anesthesia
2010
December 17-18. 4th International Congress: Aortic Surgery and Anesthesia “How to do it”. Milano, Italy. For information, contact: S. Grassi, San Raffaele Congress Centre, Via Olgettina 58 20132 Milano, Italy. E.mail: [email protected]; Website: www.aorticsurgery.it
2011
January 12-15. Annual Meeting Society January 12-15. Annual Meeting Society for Technology in Anesthesia. Las Vegas, Ne-vada. For information, contact: Society For Technology in An-esthesia, 6737 W. Washington Street, Suite 1300, Milwaukee, WI 53214. Email: [email protected]
January 16-21. 29th Annual Symposium: Clinical Update in Anesthesiology, Surgery and Perioperative Medicine with International Faculty and Industrial Exhibits. St. Martin, French West Indies. For information, Contact: Helen Phillips, The Mount Sinai School of Medicine, One Gustave L. Levy Place, Box 1010, New York, NY 10029. Email: [email protected]
January 31 - February 2. 47th Annual Meeting Society of Tho-racic Surgeons. San Diego, CA. For information, contact: Email: [email protected]
February 10 -13. 11th Annual International Symposium on Con-genital Heart Disease. St. Petersburg, Florida. For information, Website: www.aats.org
February 13 -16. 40th Annual Meeting of the German Society. For Thoracic and Cardiovascular Surgery. Stuttgart, Ger-many. For information, contact: Executive Secretary GSTCVS Langerbeck-Virchou Haus Luisenstr 58/59, 10117 Berlin, Ger-many. Email: [email protected]
February 24-27. International Conference on Pre-Hypertension and Cardio Metabolic Syndrome. Vienna, Austria. For informa-tion, contact: Paragon Conventions, 18 Avenue Louis-Casai, 1209 Geneva, Switzerland. Email: [email protected]
March 22-25. 31st International Symposium on Intensive Care and Emergency Medicine. Brussels, Belgium. For informa-tion, contact: Eramus University Hospital, Route de lennick 808, B-1070 Brussels, Belgium, Email: [email protected], Website: www.intensive.org
March 31 – April 2. 3rd World Congress of Total Intravenous Anesthesia. Singapore. For information, Website: www.kenes.com/tivia-tci.
April 29 – May 1. 6th World Congress of Pain. Seoul, Korea. For information, contact: Kenes Int. 1-3, Rue de Chantepoulet, Ch-1211 Geneva, Switzerland.
April 29 – May 4. 33rd Annual Meeting and Workshops Society of the Cardiovascular Anesthesiologists. Savannah, GA. For information, contact: SCA, PO Box 11086, 2209 Dickens Road, Richmond, VA 23230. Website: www.scahq.org
May 5-6. Mitral Conclave 2011. New York, NY. For information, Website: www.AATS.org/Mitral
May 7-11. American Association of Thoracic Surgeons 91st Annual Meeting. Philadelphia, PA. For information, Website: www.aats.org
May 11-15. 58th Annual Meeting Association of University Anesthesiologists. Philadelphia, PA. For information, contact: AUA, 520 N. Northwest Highway, Park Ridge, IL 60068. Email: [email protected]
May 21-24. International Anesthesia Research Society IARS Annual Meeting. Vancouver, British Columbia, Canada. For in-
formation, contact: IARS 100 Pine Street, Suite 230, San Fran-cisco, CA 94111. Email: infoGIARS.org, Website: www.iars.org
May 26-29. The First Conjoint Meeting of ATCSA and ASCVTS Bangkok. For information, contact: Email:[email protected]
June 1-4. 26th Annual Meeting European Association of Car-diothoracic and Vascular Anesthesia and Intensive Care. Vienna, Austria. For information, Website: www.eacta.org
June 5-8. 19th European Conference on General Thoracic Sur-gery. Vienna, Austria. For information, contact: Email: [email protected]
June 11-14. Euroanesthesia. Amsterdam, The Netherlands. For in-formation, contact: Europaplain 2-22, 1078 GZ Amsterdam, The Netherlands. Website: www.euroanesthesia.org
June 15-18. 14th European Congress on Extracorporeal Circula-tion Technology. Dubrovnik, Croatia. For information, contact: Email: [email protected], Website: www.moonencongreson-ga-nisatie.nl
June 24-28. Annual Meeting of the Canadian Anesthesiolo-gist’s Society. Toronto, ON, Canada. For information, contact: Email: [email protected]
September 13-5. The 22nd International Congress of the Israeli Society of Anesthesiologists. For information, contact: Email: [email protected]
September 29 - October 2. 9th Asian Meeting of the Society of Cardiothoracic Anesthesia 7th International Chinese Car-diovascular Anesthesia Forum. Taipei, Taiwan. For informa-tion, Website: www.asca2011.org
October 15-19. American Society of Anesthesiologists An-nual Meeting. Chicago, IL. For information, contact: ASA, 520 N. Northwest Highway, Park Ridge, IL 60068. Website: www.ASAhq.org
November 7-8. Surgery of the thoracic aorta. Bologna, Italy. For information, contact: Noema, Via Orefici 4, 40124 Bologna, Italy. Email: [email protected], Website: www.noema-congressi.it
December 9-11. 65th Postgraduate Assembly, New York State Society of Anesthesiologists. New York, NY. For information, contact: NYSSA, 85 Fifth Avenue, New York, NY 10003. Email: [email protected]
2012
March 25-30. 15th World Congress of Anesthesiologists. Buenos Aires, Argentina. For information, Website: www.wca2012.coms
April 28 – May 2 . 34th Annual Meeting & Workshops Soc. Car-diovascular Anesthesiologists. Boston, MA.For information: SCA OO Box 11086, 2209 Dickens Road, Rischmond, VA 23230. Website: www.scahq.org
April 28 – May 2. 92nd Annual Meeting American Association for Thoracic Surgery. Moscone West Convention Center, San Francisco, CA. For information, Website: www.aats.org/annual meeting
June 10-13. 20th European Congress on General Thoracic Sur-gery. Essen, Germany. Email: [email protected]
November 14-17. 13th International Meeting of Cardiothoracic and Vascular Anesthesia and the New Zealand Anesthesia Annual Scientific Meeting. Auckland, New Zealand. For infor-mation, Website: www.iccva2012.com
December. 5th International Congress: Aortic Surgery and An-esthesia “How to do it”. Milano, Italy. For information, Web-site: www.aorticsurgery.it
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia welcomes announcements of interest to physicians, re-searchers and others concerned with cardiothoracic and vascular anesthesiology, medicine, pharmacology and related areas. All copies are reviewed and edited for style, clarity and length. Information should be addressed to: George Silvay, M.D., Ph.D., Editor, Professor of Anesthesiology, Department of Anesthesiology, Mount Sinai Medical Center, 1 Gustave L. Levy Place, Box 1010, New York, NY USA 10029-6574. E-mail: [email protected]
FUTURE EVENTS

308
proceedingsin Intensive Care
Cardiovascular Anesthesia
Endorsed by
proceedings
Acknowledgements
lIst oF gUest ReVIeweRsWe would like to thank the following referees who kindly gave of their time
with one or more papers.
HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010; 2(4): 308
M. AgostoniV. AjelloL. Barile
L. BerettaG. Bertarelli
C. BiselliL. BurattiM. Caldi
C. CarielloG.M. Casiraghi
F. CislaghiM. ComisL. Corno
R.D. CovelloF. Deni
L. De Giudici E. Frati
A. FumeroA. Galanti
A. GiacominiL. GottinP. GrassiM. GrecoT. Greco
M.F. GemmaA. GuidottiY. Hayashi
G. IaciS. Joseph C. Lazzeri
Y. Le Manach R. Lembo
G. MajG. MelisurgoM. Messina
E. MoizoF. MonacoG MontiP. MylesA OrianiP.S. PagelG. Pala
D. PaseroG. Paternoster
F. PiccioniF. Pinelli
E. PiracciniD. PittarelloM. Ponschab
P. PratiM. RanucciM. Renzini
Z. RicciA. Rigamonti
A. RoasioL. RuggeriF. Sangalli
J. SayegA. Scatto
S. Scolletta L. SeveriP. Silvani
M. TaramassoI. TosettiS. Turi
F. VinciguerraA. VittorioP. Zanatta
M. Zambon

309
BOOK REVIEW
proceedingsin Intensive Care
Cardiovascular Anesthesia
Endorsed by
proceedings
the final section of the book help the reader to understand common presentations of drug in-teractions with blood test.You may found this book useful in a clinical situation where an altered laboratory test is en-countered, and you wonder if some of the thera-pies your patient is on could be the culprit:in this book the reader can quickly find all thedrugs that can interfere with a test. The draw-backs are that: no frequency of effects is de-scribed and is not possible to differentiate com-mon alterations from rare hypothesis; no mech-anism of interference is reported; no references for the curious reader are reported; the book is in Italian, limiting its diffusion.In conclusion, given the complexity of drug in-teractions, this small handbook can be useful for consultation in clinical practice.
Farmaci e parametri chimico-clinicidi Achille Patrizio Caputi, Giuseppina FavaEd. SEEd, 2010, pagine 240
Massimiliano Greco, MDGiovanni Landoni, MD
In the book by Caputi AP and Fava G entitled “Farmaci e parametri chimico-clinici”, the au-thors present a complete and schematic list of laboratory tests that are modified by drugs: they describe for each routinely assessed metabolite all the drugs known to elevate or to decrease laboratory results. While common clinical side effects of drug therapy are well known, the action of drugs on blood test is far reaching and often underrated. Indeed many blood test alterations commonly encountered in clinical practice can be attrib-uted to drugs, but they often are overlooked or regarded as unexplained alterations.The book is organized in chapters, where me-tabolites are grouped referring to major clinical areas (e.g.: cardiovascular, renal). It then proceeds with a simple schematic order that, together with its pocket size, make it a use-ful manual for ready consultation more than a book to study on. Every metabolite is shortly described with its diagnostic importance, its normal reference val-ues, and the drugs that interferes with its test result. Last but not least some case reports in

310
proceedingsin Intensive Care
Cardiovascular Anesthesia
Endorsed by
proceedings
ERRATA
The previous issue of “HSR Proceeding in Intensive Care and Cardiovascular Anesthesia” appeared in the printed version as volume 3, 2010. The volume number was incorrect and should read 2, 2010. Thus, the citation of the articles published was incorrect and should read as follows:
Lurati Buse GA, Devereaux PJ. Anesthesia needs large international clinical trials. HSR Proceed-ings in Intensive Care and Cardiovascular Anesthesia 2010; 2: 153-155.
John M, Zangrillo A. ‘A trouble shared is a trouble halved’: how the Medical Humanities can help doctors to care while they cure. HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010; 2:157-159.
Jaffer U, Wade RG, Gourlay T. Cytokines in the systemic inflammatory response syndrome: a re-view. HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010; 2: 161-175.
Chiesa R, Tshomba Y, Civilini E, Marone EM, Bertoglio L, Baccellieri D, Coppi G, Logaldo D, Melis-sano G. Open repair of descending thoracic aneurysms. HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010; 2: 177-190.
Tran DTT, Badner NH, Nicolaou G, Sischek W. Arterial pCO2 changes during thoracoscopic sur-gery with CO2 insufflation and one lung ventilation. HSR Proceedings in Intensive Care and Car-diovascular Anesthesia 2010; 2: 191-197.
Picariello C, Lazzeri C, Chiostri M, Gensini GF, Valente S. Kinetic of procalcitonin in patients with cardiogenic shock following acute myocardial infarction: preliminary data. HSR Proceedings in In-tensive Care and Cardiovascular Anesthesia 2010; 2: 201-207.
Grassi P, Leone D, Vassallo C. Erroneously low continuous ScvO2 reading due to red blood cells transfusion. HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010; 2: 209-211.
Piraccini E, Agnoletti V, Corso R, Maitan S, Gambale G. The use of methylene blue in abdominal aortic surgery: a case report. HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010; 2: 215-218.
Berlot G, Vergolini A, Calderan C. Early and prolonged ECG alterations resembling a myocardial injury after severe amitriptyline poisoning. HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010; 2: 221-224.
Collu E, Grimaldi A, Benussi S, Castiglioni A, Bignami E, Rizzo N, De Bonis M, Melisurgo G, La Canna G, Alfieri O. A rare case of unexpected cardiac incidentaloma causing syncope. HSR Proceed-ings in Intensive Care and Cardiovascular Anesthesia 2010; 2: 225-227.
Franzoni I, Baratto F, Macchi A, Rosa I, Buzzetti F, Margonato A. Coronary angiography and angi-oplasty in a patient with an iliac artery volvolus. HSR Proceedings in Intensive Care and Cardiovas-cular Anesthesia 2010; 2: 229-230.
John M. When a question becomes a nightmare: surviving the most difficult part of your presenta-tion. HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 2010; 2: 233-234.
How to prepare a manuscript for submission toHSR Proceedings in Intensive Care and Cardiovascular Anesthesia
English language is the only language allowed for manuscripts submitted to “HSR proceed-ings in Intensive Care and Cardiovascular Anesthesia” from November 1st 2009. You can choose between American or British English, but be consistent.
“HSR proceedings in Intensive Care and Cardio-vascular Anesthesia” offers a “fast track” oppor-tunity: we’ll send you an editorial decision within 7 days if you submit a manuscript through email with the comments of previous reviewers of other journals who evaluated your paper. If you ask for a fast track review and send us comments of previ-ous reviewer you’ll not have to arrange the refer-ences or the layout according to the below cited journal guidelines.
Manuscripts must be double-spaced on A4 pages. A margin of at least 3 cm should be provided on all sides. All type should be 12 points in size. Pages must be numbered. Word limits are not imposed on any manuscript types, but all papers should be as concise as possible.
Please send your manuscript to [email protected] The Editorial Office will send by e-mail to the corre-sponding author all communications related to the status of a submission, including the final decision and the scheduled date of publication.
Different manuscripts could be submitted to “HSR proceedings” including: Original articles; Teach-ing articles; Brief reports; Review; Editorial; Case series; Letters to the Editor; Case reports; Images in clinical medicine. The peer-review process is ap-plied to all submissions, including appraisal by at least 2 peer-reviewers.
COVER LETTER. Please also send us a cover letter addressed to the Editor in Chief. The letter must include at the end a list of all authors as if for signature. The cover letter must state that the authors agree with and are responsible for the data presented. The letter should also acknowledge or deny any potential conflicts of interest.
MANUSCRIPT. Our preferred file type for new manuscript submissions is a single Microsoft Word Doc with all figures embedded in the same document. In the manuscript provide the title of the paper on the first page (TITLE PAGE); the title should be concise. Also list the name of each author, including the first name and the highest
graduate degree; the department and institutional affiliation of each author and the name, address, telephone number, fax number, and e-mail address of the author to whom correspondence should be addressed. ABSTRACT. Provide an abstract of not more than 250 words and without abbreviations. If possible, it should consist of four paragraphs, labelled Background, Methods, Results and Dis-cussion. They should briefly describe, respectively, the problem being addressed in the study, how the study was performed, the salient results and what the authors conclude from the results. The manuscript itself should be possibly divided into 4 sections: Introduction, Methods, Results, and Dis-cussion. Please refrain from using automatic refer-ence list software because its features are often lost during the publication process. Simply insert the reference number in parentheses in the text (after any punctuation mark) and type the reference list. References must be numbered with Arabic numer-als and cited in the text in numerical order. The reference list at the end of the article must also be in numerical order. The list headed “REFERENC-ES” should begin on a new page of the main text document and be double-spaced. Abbreviations for titles of medical periodicals must conform to those used in Index Medicus (http://www.nlm.nih.gov/tsd/serials/lji.html ). References to abstracts, sup-plements and letters to editors must be identified as such. Inclusive page numbers of references are required.
DETAILS. “HSR proceedings in Intensive Care and Cardiovascular Anesthesia” will consider for publication suitable articles on all topics related to intensive care and to anesthesia for cardiac, tho-racic and vascular surgery. The aim of “HSR pro-ceedings” is to contribute to the spread of knowl-edge in the field of intensive care, emergencies and major surgical operations.
Manuscripts are examined by members of the edi-torial staff and then sent to outside reviewers. We encourage authors to suggest the names of possible reviewers, but we reserve the right of final selec-tion. Communications about manuscripts will be sent after the review and then the editorial deci-sion-making process is complete.
All articles represent the opinion of the authors and do not necessarily reflect the opinion of the Editor, Editorial Board or Publisher. The Editors and Publisher deny any responsibility or liability for statements and opinions expressed by the au-

312 rationale for their approach, and demonstrate that the institutional review body explicitly approved the doubtful aspects of the study. When reporting experiments on animals, authors should be asked to indicate whether the institutional and national guide for the care and use of laboratory animals was followed.If photographs of patients are used, either they should not be identifiable or the photographs should be accompanied by written permission to use them. Patients have a right to privacy that should not be infringed without informed con-sent. Identifying information, including patients’ names, initials, or hospital numbers, should not be published in written descriptions, photographs, and pedigrees unless the information is essential for scientific purposes and the patient (or parent or guardian) gives written informed consent for publication. Informed consent for this purpose re-quires that a patient who is identifiable be shown the manuscript to be published. Authors should identify Individuals who provide writing assis-tance and disclose the funding source for this as-sistance. Identifying details should be omitted if they are not essential. Complete anonymity is dif-ficult to achieve, however, and informed consent should be obtained if there is any doubt. For ex-ample, masking the eye region in photographs of patients is inadequate protection of anonymity. If identifying characteristics are altered to pro-tect anonymity, such as in genetic pedigrees, au-thors should provide assurance that alterations do not distort scientific meaning and editors should so note. The requirement for informed consent should be included in the journal’s instructions for authors. When informed consent has been obtained it should be indicated in the published article.
All text, references, figure legends and tables should be in one double-spaced electronic docu-ment (Word Doc). You may either insert figures in the text file or upload your figures separately. We prefer the former but this may not work well for complicated graphics, which should be sent separately. It is permissible to send low-resolution images for peer review, although we may ask for high-resolution files at a later stage. Legends for all figures should be included in the file with the text (on a new page after the references list) and should not appear on the figures. Acceptable formats for pictures, photos and figures are PDF, DOC, PPT, JPG, TIF. Please send TIF not inferior to 300 DPI when your paper is accepted for publication.
thors. Neither the Editor nor the Publisher guar-antee, warrant or endorse any product or service advertised in this publication, nor do they guaran-tee any claim made by the manufacturer of such product or service.
Manuscripts containing original material are ac-cepted for consideration if neither the article nor any part of its essential substance, tables, or fig-ures have been or will be published or submitted elsewhere before appearing in “HSR proceedings”. This restriction does not apply to abstracts or press reports published in connection with scien-tific meetings.
Authors of all types of articles should follow the general instructions. These guidelines are in ac-cordance with the “Uniform Requirements for Manuscripts Submitted to Biomedical Journals,” published by the International Committee of Medical Journal Editors at http://www.icmje.org. Papers reporting human experimentation will be reviewed in accordance with the precepts estab-lished by the Helsinki Declaration (available at http://www.wma.net/e/policy/b3.htm ). Copies of this declaration may also be obtained by writing to the American Medical Association, 515 N State St, Chicago, IL 60610.
As stated in the Uniform Requirements, credit for authorship requires substantial contributions to (a) the conception and design of the protocol or analysis and interpretation of the data and (b) the drafting of the article or critical revision for important intellectual content. Each author must sign a statement attesting that he or she fulfills the authorship criteria of the Uniform Requirements. Any change in authorship after submission must be approved in writing by all authors.
In appropriate places in the manuscript, please provide, if applicable, a statement that the re-search protocol was approved by the relevant in-stitutional review boards or ethics committees and that all human participants gave written in-formed consent. When reporting experiments on human subjects, authors should indicate whether the procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and na-tional) and with the Helsinki Declaration of 1975, as revised in 2000. If doubt exists whether the re-search was conducted in accordance with the Hel-sinki Declaration, the authors must explain the

313journals helps shape diagnostic and therapeutic decisions. For a journal to be of value, it must publish authoritative, up-to-date information that is free of commercial influence. Because relation-ships between authors and biomedical companies are growing, we want to ensure that the articles we publish are not influenced by financial inter-ests.Authors should disclose any financial arrange-ment they may have had in the last 3 years or in the foreseeable future with a company whose product is pertinent to the submitted manuscript or with a company making a competing product. Such information will be held in confidence while the paper is under review and will not influence the editorial decision but if the article is accepted for publication, a disclosure statement will appear with the article. Here are some examples: Dr. “A” reports having served as a consultant to “A1”. Dr. “B” reports having been paid lecture fees by “B1”, “B2” and “B3” Drs. “C, D, E” report having re-ceived grant support from “C1” Neither Dr. “F”A nor Dr. “G” has any financial interest in the pat-ent. Dr. “H” and Dr. “I” are consultants to “H1” Dr. “L” reports having received consulting fees from “I1” Dr. “M” reports having been a member of speakers’ bureaus sponsored by “M1”
COPYRIGHT. “HSR proceedings” is the owner of all copyright to any published work. “HSR pro-ceedings” and its licensees have the right to use, reproduce, transmit, derive works from, publish and distribute the contribution, in the “HSR pro-ceedings” or otherwise, in any form or medium. Authors may not use or authorize the use of the contribution without the “HSR proceedings” written consent.
EDITING SERVICES“HSR proceedings in Intensive Care and Car-diovascular Anesthesia” offers a service of English language revision and methodologi-cal support to authors that wish to publish in peer-reviewed journals. For information and tariffs please contact [email protected]
Please direct any questions to [email protected] or visit www.itacta.org “HSR proceedings in Intensive Care and Car-diovascular Anesthesia” editorial offices are lo-cated in the Department of Anesthesia and In-tensive Care at 60 Via Olgettina, Milano, Italy 20132, telephone (+39) 02.26437164, fax (+39) 02.26437178, email [email protected]
References. References must be double-spaced and numbered consecutively as they are cited. Possibly list all authors when there are four or fewer; when there are five or more, list the first three, followed by “et al.” Abbreviations. Except for units of measurement, abbreviations are strongly discouraged. Except for units of measurement, the first time an abbrevia-tion appears, it should be preceded by the words for which it stands.Drug Names. Generic names should be used. When proprietary brands are used in research, in-clude the brand name and the name of the manu-facturer in parentheses after the first mention of the generic name in the Methods section.
Instructions for Submitting a Revised Manuscript. We require two versions of the revised manu-script, one with “tracked” or highlighted changes and one without. Please double-space. Include your response to the reviewers as a separate file. If a submitted article is accepted for publication, editorial revisions may be made to aid clarity and understanding without altering the meaning.
CONFLICT OF INTEREST. Public trust in the peer review process and the credibility of pub-lished articles depend in part on how well conflict of interest is handled during writing, peer review, and editorial decision making. Conflict of interest exists when an author (or the author’s institu-tion), reviewer, or editor has financial or personal relationships that inappropriately influence (bias) his or her actions (such relationships are also known as dual commitments, competing interests, or competing loyalties). These relationships vary from those with negligible potential to those with great potential to influence judgment, and not all relationships represent true conflict of interest. The potential for conflict of interest can exist whether or not an individual believes that the re-lationship affects his or her scientific judgment. Financial relationships (such as employment, consultancies, stock ownership, honoraria, paid expert testimony) are the most easily identifiable conflicts of interest and the most likely to under-mine the credibility of the journal, the authors, and of science itself. However, conflicts can occur for other reasons, such as personal relationships, academic competition, and intellectual passion.“HSR proceedings” expects that all authors ac-knowledge financial associations with a company (or its competitor) that makes a product discussed in the article. Information published in medical

Edizioni Internazionali Srl
La divisione EDIMES pubblica 16 riviste (7 uffi ciali di Società Scientifi che) e tiene in catalogo circa 100 titoli di volumi riguardanti la Medicina e la Comunicazione Medico Scientifi ca.
27100 PAVIA · VIA RIVIERA 39 · TEL. 0382526253 R.A. · FAX 0382423120 · E-MAIL: [email protected]
VISCONTEATIPOGRAFIA EDITORIALE
pubblica prevalentemente libri di “storia regionale e locale”
Alcuni titoli:
• “FIGURE E FIGURI” DEL RISORGIMENTO IN LOMBARDIAa cura di I. Montanelli e Coll.Si racconta di vita, fatti e misfatti di personaggi del risorgimento Lombardo
• PAVIA CISALPINA E NAPOLEONICAa cura di G.E. de PaoliDescrive con precisione il periodo napoleonico a Pavia
Alcune riviste:
• NEW MICROBIOLOGICA (et Infettivologica)Rivista con Impact Factor (Rivista Uffi ciale S.I.V.I.M. - Società Italiana Virologia Medica) · A. Lazzarin editor
• REUMATISMO(Rivista Uffi ciale S.I.R. - Società Italiana Reumatologia)L. Punzi editor
• INFETTIVOLOGIA PEDIATRICA(Rivista Uffi ciale Società Italiana Infettivologia Pediatrica)N. Principi editor
• PERIMED - Medicina Perioperatoria(Rivista Uff. ESRAT-CIAO-SARNePI-FOAP) G. Fanelli editor
• HSR PROCEEDINGS IN INTENSIVE CARE & CARDIOVASCULAR ANESTHESIA A. Zangrillo, R. Hetzer editors
• HEPATITIS WORLD · A. Craxì editor
• EMATOLOGIA ONCOLOGICAG. Lambertenghi Deliliers editor
• LE INFEZIONI IN MEDICINA · S. Esposito editor
Alcuni titoli di volumi pubblicati:
• SENOLOGIAa cura di U. Veronesi e G. Coopmans
• LO SCOMPENSO CARDIACOcura di P.L. Malini, E. Perugini, C. Rapezzi, B. Magnani
• PSA - ANTIGENE PROSTATICO SPECIFICOa cura di P. Rigatti, V. Scattoni
• PROLEGOMENI - STUDIO DELLA FISICA DEL FEGATOa cura di N. Dioguardi
• LE ARITMIE CARDIACHEa cura di L. dei Cas
• LA TERAPIA DELL’INSUFFICIENZA CARDIACAa cura di M. Volpe
La divisione EDINT pubblica in preferenza libri per ragazzi
Alcuni titoli:
• ORBITAL HOTELVolume scritto da Claudio Apone, presentato da Max Pezzali e “disegnato” da Marco LodolaAmbientato e “vissuto” nello spazio
• DOTTORE! DOTTORE!Volume scritto da Paolo Zanocco (medico). Racconta con sonetti e dialoghi ironici la professione di un Medico Pediatra di provincia
Il PPI differente dall’origine
Dep
osi
tato
pre
sso
l’A
IFA
in
data
26/0
1/2
010
PANTORC ADV 210X297 STP 27-01-2010 14:30 Pagina 1