gastric adenocarcinoma ד"ר הוברט אילה מנהלת המרכז לגידולים...
TRANSCRIPT

GGastric adenocarcinomaastric adenocarcinoma
ד"ר הוברט אילהמנהלת המרכז לגידולים במערכת העיכולמכון שרתהדסה עין כרם

Gastric cancer epidemiology
• 4th most commonly diagnosed cancer
• Still the 2nd most common cause of cancer-related death globally
• Global incidence rates
• Almost 1,000,000 cases
• Nearly 700,000 deaths
• Global decline in mortality
• Incidence of gastro-oesophageal (GE) junction cancer rapidly increasing

Gastric Cancer – Epidemiological Trends
Reduction in gastric cancer mortality could be due to a number of factors– Earlier detection
– Improved understanding of the disease and associated improved treatments and clinical management
– Improvements in refrigeration
– Diet • Reduced intakes of salted, pickled, smoked, and other
chemically preserved foods
• Increased consumption of fresh fruit and vegetables
• Improved housing, sanitation and living standards with a resulting reduction in Helicobacter pylori

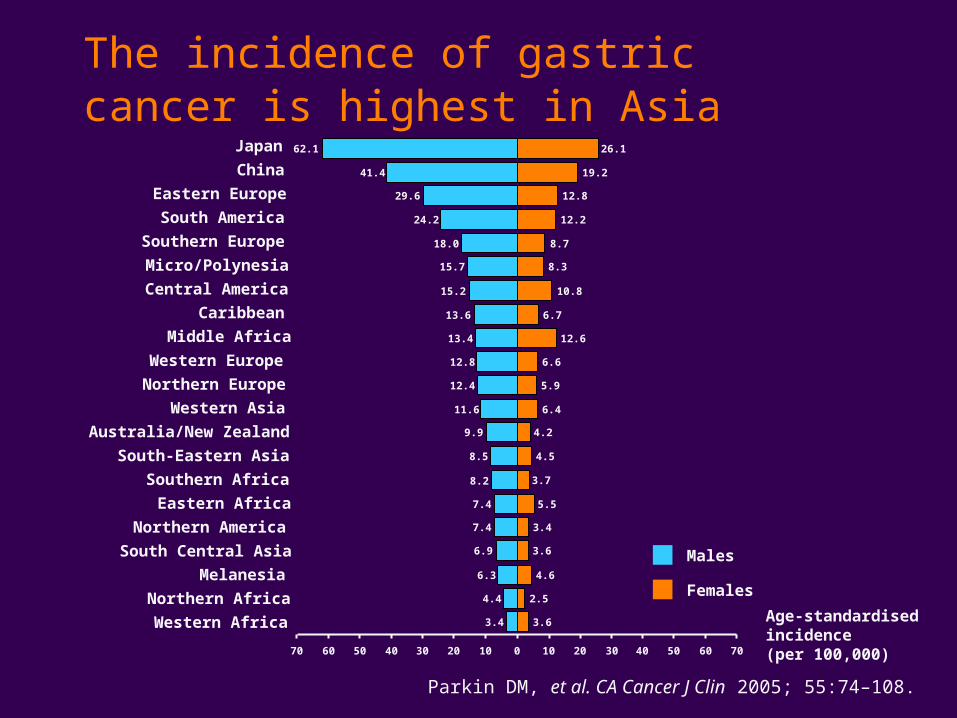
The incidence of gastric cancer is highest in Asia
Parkin DM, et al. CA Cancer J Clin 2005; 55:74–108.
Japan
China
Eastern Europe
South America
Southern Europe
Micro/Polynesia
Central America
Caribbean
Middle Africa
Western Europe
Northern Europe
Western Asia
South-Eastern Asia
Southern Africa
Eastern Africa
Northern America
South Central Asia
Melanesia
Northern Africa
Western Africa
62.1 26.1
41.4 19.2
29.6 12.8
24.2 12.2
18.0 8.7
15.7 8.3
15.2 10.8
13.6 6.7
13.4 12.6
12.8 6.6
12.4 5.9
11.6 6.4
9.9 4.2
8.5 4.5
3.7
7.4 5.5
7.4 3.4
6.9 3.6
6.3 4.6
4.4 2.5
3.4 3.6
8.2
70 60 50 40 30 20 10 0 10 20 30 40 50 60 70
Age-standardised incidence(per 100,000)
Australia/New Zealand
Males
Females
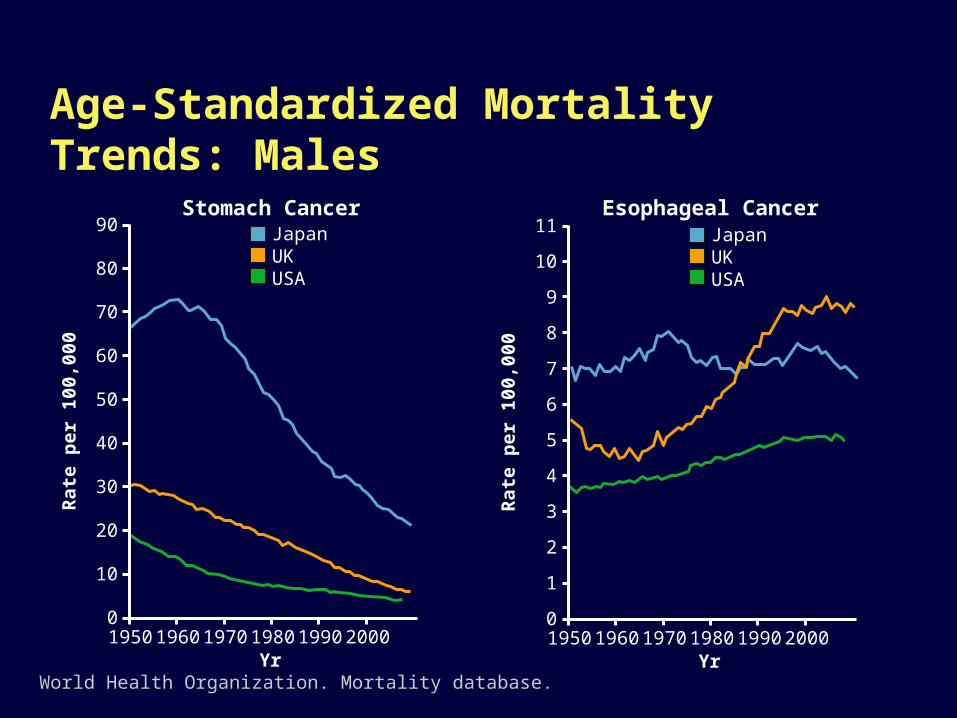
Stomach Cancer
World Health Organization. Mortality database.
Age-Standardized Mortality Trends: Males
JapanUKUSA
90
80
70
60
50
40
30
20
10
0
Rat
e p
er 1
00,0
00
1950 1960 1970 1980 1990 2000Yr
Esophageal CancerJapanUKUSA
11
10
7
6
5
4
3
2
1
0
Rat
e p
er 1
00,0
00
1950 1960 1970 1980 1990 2000Yr
9
8

Gastric cancer aetiology• Gastric cancer is a multifactorial disease
Environmental risk factors (~90%)
Genetic risk factors (8–10%) GE junction Body of stomach
Achlorhydria Gastro-oesophagealreflux disease (GERD)
Helicobacter pylori infection
Pernicious anaemia Obesity High dietary nitrate/ nitrite content
Blood group A Low consumption of fruit, vegetables
Tobacco use
Li-Fraumeni syndrome(p53 mutation)
High consumption ofred meat, alcohol
Tobacco use
Low consumption of fruit, vegetables

Gastric CancerPathogenesis
Karpeh MS, et al. Cancer: Principles & Practice of Oncology. 6th ed. 2001;1092-1126.
Mucosal Atrophy + Increased Gastric pH
Bacterial Overgrowth
Direct Bacteria-Induced Injury + Increased Production of Nitrites and N-nitroso compounds
Intestinal Metaplasia
Gastric Carcinoma
Anatomic classification
• Site of origin
• Proximal (incidence on the increase)
• GE junction = cardia
• Fundus
• Distal
• Corpus
• Antrum

Gastric CancerHistology
95% of gastric neoplasms are adenocarcinomas
Other subtypes include:
– Squamous cell carcinoma
– Adenoacanthoma
– Carcinoid tumors
– Gastric stromal tumor (leiomyosarcoma)
– Primary lymphoma
Karpeh MS, et al. Cancer: Principles & Practice of Oncology. 6th ed. 2001:1092-1126.

Microscopic histologic typesMicroscopic histologic types
The most widely used classification system is that of Lauren
• Intestinal: arises from precancerous lesions, more common in men, dominant type where gastric cancers are epidemic, differentiated, tends to form glands
• Diffuse: little cell cohesion, tendency for submucosal spread and early metastases, worse prognosis

0
50
100
150
200
250
300
350 IntestinalDiffuseMixed
Patients
Distribution of histological subtypes among countries
Bang YJ, et al. J Clin Oncol 2009.n=2759
TNMTNM Primary tumor (T)
Principal factor is degree of penetrationof stomach wall by carcinoma
Tx : Primary tumor cannot be assessed T0 : No evidence of primary tumor Tis : Carcinoma in situ : intraepithelial tumor without invasion of the lamina propria T1 : Tumor invades lamina propria or submucosa T2 : Tumor invades muscularis propria or the subserosa T3 : Tumor penetrates the serosa without invading adjacent structures T4 : Tumor invades adjacent structures
Nodal involvement (N)
Nx : Regional lymph nodes cannot be assessedN0 : No regional lymph nodes within 3 cm of
the edge of the primary tumorN1 : Metastasis in 1 to 6 regional lymph nodesN2 : Metastasis in 7 to 15 regional lymph nodesN3 : Metastasis in more than 15 regional lymph nodespN0 : histological examination of a regional lymphadenectomy specimen will ordinarily include 15 or more lymph nodes
TNMTNM

SubmucosapT1A
B
pT2A
B
pT3
pT4
Mucosa
Muscularispropria
Subserosa
Serosa
<5%20%
40%
70%
90%
Primary tumor Lymph nodes
Increased depth of penetration is associated Increased depth of penetration is associated with increased lymph node metastaseswith increased lymph node metastases

Increased depth of penetration is Increased depth of penetration is associated with a poor prognosisassociated with a poor prognosis
Penetration 5-yr survival
Mucosa 100%
Submucosa 92%
Muscularis propria 42-73%
Subserosa 29-55%
Serosa 0-7%

No nodes
5-yr surv
N1 1-6 46%
N2 7-15 30%
N3 >15 10%
Increased level of lymph node involvement is associated with decreased survival

Gastric cancer stageand survival rates
Disease Stage TMN 5-yr survival rates
Early 0 Tis, N0, M0 89%
IA T1, N0, M0 78%
IB T1, N1, M0 orT2a/b, N0, M0
58%
II T1, N2, M0 orT2a/b, N1, M0 or
T3, N0, M0
34%
Advanced IIIA T2a/b, N2, M0 orT3, N1, M0 or
T4, N0, M0
20%
IIIB T3, N2, M0 8%
IV T1–3, N3, M0 or T4, N1–3, M0 or
any T, any N, M1
7%

Treatment

Treatment options according to TNM status
T1–2, N0, M0• Early stage ,Surgery alone
• Locally advanced :Risk of relapse is high after surgery alone• Adjuvant/neoadjuvant chemotherapy and radiation followed by
attempt at curative surgery
• Metastatic : Chemotherapy• Palliative surgery and/or radiation if indicated
Curative care options
• Surgery is the only curative therapy for gastric cancer (curative surgical resection, R0)
• Total gastrectomy or oesophagogastrectomy
• Subtotal gastrectomy
• Lymphadenectomy
• Debate regarding the most appropriate surgical procedures
(D2 vs. D1 resection)
• Irrespective of the surgical procedure, high recurrence rate
after surgery


Lymph nodes N1groupes 1-6
Lymph nodes N2groupes 7-11 (13)
Lymph node dissection extension : D1 vs D2
Curative care options
• Pre-operative (neoadjuvant) therapy• Downstaging of disease may
facilitate resection
• Post-operative (adjuvant) therapy

SWOG 9008/INT 0116RESECTED GASTRIC CANCER
RESECTED
STAGE IB-IV (M0)
GASTRIC
ADENOCARCINOMA
R
A
N
D
O
M
OBSERVATION
5-FU/LV RADIATION 5- FU/LV X2
5-FU/LV 5-FU/LV
SCHEMA
Macdonald et al, N Engl J Med 2001

INT 0119 - SWOG 9008
Surgery Surgery chemo RT
p-value
Median DFS 19 months 30 months p=0.001
3y survival Med. Survival
40% 28 months
50% 35 months
p=0.03
J McDonald et al, NEJM 2001
Gastric Cancer: Postoperative Adjuvant Chemoradiotherapy
Gastric Cancer: Neoadjuvant Chemo in Locally Advanced Disease
• Data from non-randomized phase II and small randomized trials show feasibility of chemotherapy followed by surgery.
• Rationale:• gastric cancer is chemosensitive
downstaging is realistic• eradication of microscopic metastases?• better tolerance of pre- than postoperative chemotherapy• selection of patients who benefit from adjuvant treatment
Curative treatment programs
Neoadjuvant (Chemotherapy)
SURGERY
Adjuvant (Chemotherapy and Radiation therapy)

MAGIC trial
503 patients 503 patients with gastric with gastric
cancercancer
Surgery only (S)Surgery only (S)
ECFx3ECFx3surgery surgery ECFx3 (CSC)ECFx3 (CSC)
Allum WH, et al. Proc Am Soc Clin Oncol 2003;22:2493 (abst 998)Cunningham et al. Proc Am Soc Clin Oncol 2005;308s (abst 4091)
R
S CSC
Curative resection 69% 79% p=0.02pT1-2 36% 54% p=0.01pN0-1 71% 80% p=0.10PFS (mo) 14 20 p=0.0001MS (mo) 20 24 p=0.009

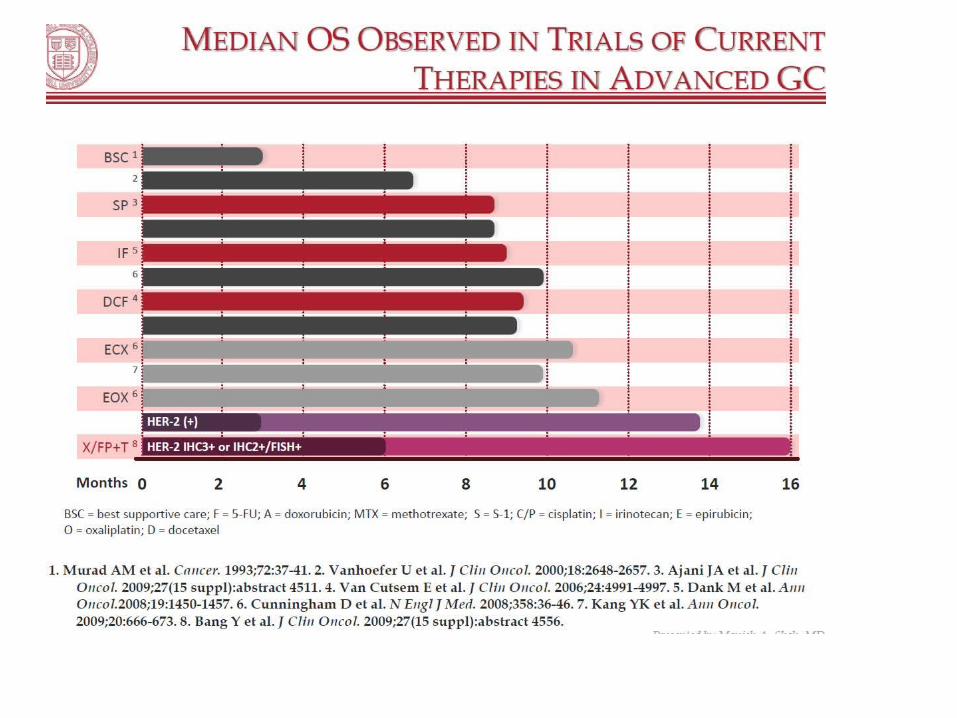
Palliative care options
• The objective is to manage symptoms, improve QoL and prolong life
• Chemotherapy• Multiple drug chemotherapy regimens are used• Response rates 30–50%; median OS ≤1 year
• Surgery• Palliative resection of affected gastric component may be
indicated (i.e. if risk of obstruction is high)
• Radiotherapy• Palliative radiotherapy to reduce pain or symptoms
AGENTS
• Cisplatine• Anthracyclines• 5FU(xeloda,S1) • Mitomycine C• Etoposide• Methotrexate• Taxanes• Campto• Oxaliplatine• Herceptin• Rmucirumab



Potential predictive factors of efficacy
TS DPD Topo I MSI ERCC-1 EGF

HER2 in gastric cancer
• Approximately 16% of patients with advanced adenocarcinoma of the stomach or GE junction have HER2-positive disease
• HER2 has predictive value in gastric cancer
• Accurate HER2 testing is essential to identify patients who may benefit from treatment with trastuzumab
1. Bang YJ, et al. J Clin Oncol 2009; 27:Abstract 4556.2. van Cutsem E, et al. J Clin Oncol 2009; 27:Abstract LBA4509.

IHC negative (0)
No staining or membrane staining in <10% of cells
IHC negative (1+)
Faint/barely perceptible membrane staining in >10% of cells; cells only stained in part of membrane
IHC equivocal (2+)
Weak to moderate complete or basolateral membrane staining in >10% of cells
IHC positive (3+)
Strong complete or basolateral membrane staining in
• >10% of cells in resection specimens or
• cohesive IHC 3+ clones irrespective of size (i.e.<10%) in biopsy samples
IHC scoring criteria forgastric cancer

ToGA trial design
HER2-positiveadvanced GC
(n=584)
5-FU or capecitabinea + cisplatin(n=290)
R
aChosen at investigator’s discretion GEJ, gastroesophageal junction
5-FU or capecitabinea + cisplatin
+ trastuzumab(n=294) Stratification factors
− advanced vs metastatic − GC vs GEJ− measurable vs non-measurable− ECOG PS 0-1 vs 2− capecitabine vs 5-FU
Phase III, randomized, open-label, international, multicenter study
1Bang et al; Abstract 4556, ASCO 2009
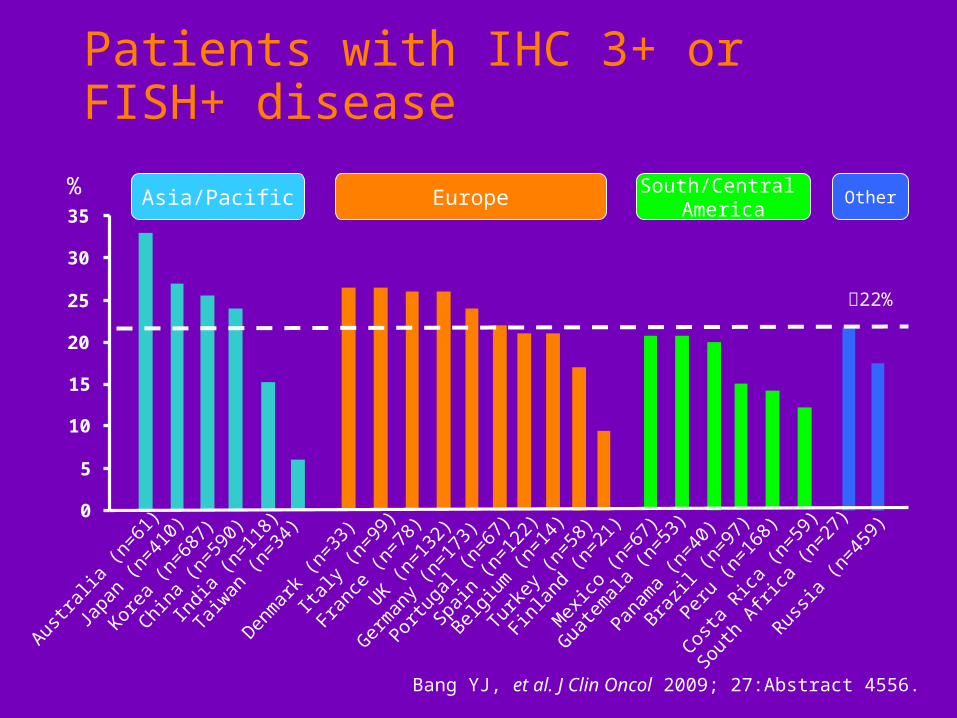
3807 patients screened1
810 HER2-positive (22.1%)

113
OS in IHC2+/FISH+ or IHC3+ (exploratory analysis)
1.0
0.8
0.6
0.4
0.2
0.0
363432302826242220181614121086420
Time (months)
11.8 16.0
FC + H
FC
Events
120136
HR
0.65
95% CI
0.51, 0.83
MedianOS
16.011.8
Event
0.1
0.3
0.5
0.7
0.9
218 198
40
53
124
2011
228 218
196 170
170 141
142 112
12296
10075
8453
6539
5128
10
00
No. at risk
3920
2813
Sout
h Af
rica
(n=27
)
Guate
mal
a (n
=53
)Cos
ta R
ica
(n=59
)
Aust
ralia
(n=61
)
Japa
n (n
=41
0)
Kore
a (n
=68
7)
China
(n=59
0)
Russia
(n=45
9)
Turk
ey (n
=58
)
Indi
a (n
=11
8)
Taiw
an (n
=34
)
Denm
ark
(n=33
)
Italy (n
=99
)
Fran
ce (n
=78
)
UK (n
=13
2)
Germ
any
(n=17
3)
Portug
al (n
=67
)
Belg
ium
(n=14
)
Spai
n (n
=12
2)Finl
and
(n=21
)
Mex
ico
(n=67
)
Pana
ma
(n=40
)
Braz
il (n
=97
)
Peru
(n=16
8)
%
0
5
10
15
20
25
30
35
22%
Asia/Pacific EuropeSouth/Central
AmericaOther
Patients with IHC 3+ or FISH+ disease
Bang YJ, et al. J Clin Oncol 2009; 27:Abstract 4556.

Ramucirumab (IMC-1121B; RAM) is a recombinant human IgG1 monoclonal antibody receptor antagonist designed to bind the extracellular domain of VEGF Receptor-2, thereby blocking the binding of VEGF ligands and inhibiting receptor activation










Novel Methods for Molecular Assessment
Analysis of circulating tumor cells
– Currently limited by technology (~ 50% of patients)
– New platforms in development
– Suitable for all biomarker analysis
– Potential to replace tissue biopsy
Analysis of circulating tumor DNA
– Tumor DNA mutational testing
– Potential for broader role?
