gastric giardiasis - jcp.bmj.com · gastric giardiasis cdoglioni, mdeboni, rcielo, llaurino,...
TRANSCRIPT
9 Clin Pathol 1992;45:964-967
Gastric giardiasisC Doglioni, M De Boni, R Cielo, L Laurino, P Pelosio, P Braidotti, G Viale
AbstractAims: To assess the prevalence of gastricgiardiasis in patients undergoing uppergastrointestinal endoscopy, and to definethe clinicopathological correlates of gas-tric Giardia lamblia infection.Methods: Consecutive gastric biopsyspecimens (n = 15 023) from 11 085patients, taken at Feltre City Hospital(north eastern Italy) from January 1986 toDecember 1991, were histologically andimmunocytochemically examined for theoccurrence of G lamblia trophozoites.Three gastric biopsy specimens frompatients harbouring G lamblia infection,who repeated endoscopy before treat-ment, were also examined electronmicroscopically.Results: Forty one patients (0.37% of thepopulation study) harboured gastric giar-diasis. All patients underwent upper gas-trointestinal endoscopy because ofdyspepsia, epigastric pain, or abdominaldistension. Only two patients had diarr-hoea at the time of investigation. Giardia-sis was clinically unsuspected in all cases,although the nine patients who also hadduodenal biopsies performed had con-comitant intestinal giardiasis. Gastricgiardiasis was invariably associated withchronic atrophic gastritis. Intestinalmetaplasia of the gastric mucosa andHelicobacter pylori infection were foundin 32 and 37 of the 41 patients with gastricgiardiasis, respectively.Conclusions:The invariable association ofgastric giardiasis with chronic atrophicgastritis, most often showing intestinalmetaplasia and H pylori infection, indi-cates that a decreased gastric acidity is aprerequisite for localisation of G lambliato the gastric mucosa. Though its possiblerole as a gastric pathogen remains to beelucidated, these findings suggest thattrophozoites should be carefully searchedfor when examining gastric biopsy speci-mens showing chronic atrophic gastritis.
(7 Clin Pathol 1992;45:964-967)
Giardia lamblia was the first intestinal protozoato be observed and described by Leeuwenhockin 1681, although it derives its name fromVilem Lambl, a Czech physician who identi-fied it in faeces in 1859, and was formallyconsidered its discoverer.The pathogenicity of G lamblia has been
controversial for a long time, but it is now
accepted that it causes disease in man.' Infec-tion is usually followed by an acute diarrhoealillness, after an incubation period of 12 to 19days; chronic giardiasis can also be accom-panied by ill defined gastrointestinal symp-toms.2 Diagnosis of infection relies on theidentification of trophozoites in duodenalaspirates or cysts in stool. Immunological andgenotypic assays have been introduced in
3 4clinical practice over the past few years.Histological examination of duodenal and jeju-nal biopsy specimens from patients with aclinical history of malabsorption permits directvisualisation of the trophozoites.
In infected patients G lamblia charac-teristically localises in the proximal smallintestine, but localisation in extraintestinalsites, including gall bladder,5 has also beenreported. However, no mention is made thatthe organism could possibly be identified ingastric biopsy specimens.
Following the first observation of G lambliatrophozoites in a gastric biopsy specimen, weundertook a prospective and retrospectiveanalysis for the presence of the organism inroutine gastric biopsy specimens taken at theendoscopic unit, Feltre City Hospital.
MethodsThe first patient harbouring G lamblia tropho-zoites in the gastric mucosa was observed inDecember 1988. All subsequent gastric biopsyspecimens were routinely evaluated for thepresence of this parasite, and a retrospectiveanalysis was performed on all gastric biopsyspecimens dating back to 1986. Thus a total of15 023 specimens taken from 1986 to 1991from 11 095 patients were included in thecurrent investigation.When G lamblia was morphologically identi-
fied, additional sections were cut from paraffinwax blocks and immunostained with a 1 in10 000 dilution of anti-Giardia polyclonal anti-serum (Chemicon, Temecula, California,USA) and a standard avidin-biotin complex-peroxidase technique (reagents from Dako,Glostrup, Denmark), as previously reported.6All cases were also morphologically inves-tigated for Helicobacter pylon infection. Histo-pathological changes in the gastric mucosawere recorded according to the Sydney sys-tem.7Nine patients found to harbour gastric G
lamblia on initial examination, had a repeatendoscopy before treatment; at that time bothgastric and duodenal biopsy specimens weretaken from each patient. In three of these cases
Department ofSurgical Pathology,Ospedale Civile, FeltreC DoglioniL LaurinoP PelosioEndoscopy UnitM De BoniR CieloSecond Department ofPathology, Universityof Milan School ofMedicine, Milan, ItalyP BraidottiG VialeCorrespondence to:Dr C Doglioni, Departmentof Pathology, OspedaleCivile, 32032 Feltre (BL),ItalyAccepted for publication6 May 1992
964
on 19 October 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.45.11.964 on 1 Novem
ber 1992. Dow
nloaded from

Gastric giardiasis
part of the gastric samples were fixed in 2-5%glutaraldehyde in Millonig's phosphate bufferfor four hours and processed for electronmicroscopic examination. Seven patients had athird control endoscopy one to two monthsafter treatment.Symptoms leading to endoscopy, other per-
tinent clinical data, and the effects of treatment(metronidazole 250 mg three times a day for10 days often associated with antacid drugs) in24 patients who had been treated (patientsseen after December 1988) were retrievedfrom the clinical records of each patient.Twenty seven small bowel biopsy specimens,
taken from patients investigated for malabsorp-tion during the same period were alsoreviewed: 10 of these patients also had antraland fundic gastric biopsy specimens taken atthe same time.
Finally, to evaluate the prevalence of Glamblia in the population, we analysed duode-nal biopsy specimens and cytological brush-ings of a consecutive series of 110 patientsundergoing routine upper gastrointestinal tractendoscopic examination.
ResultsIDENTIFICATION AND LOCALISATION OF
TROPHOZOlTESForty one (0-37%) of the 11 085 patientsunder study harboured gastric G lamblia infec-tion. The trophozoites were identified at lightmicroscopy as pear-shaped structures with twosmall paired nuclei, or as concave diskswith thick outline (fig 1); thin flagella wereoccasionally seen. In all cases the immuno-cytochemical investigation provided con-firmatory evidence for the identity of thetrophozoites, which were strongly immuno-reactive to the anti-Giardia antiserum (fig 2).
In the three cases submitted for electronmicroscopic examination the trophozoites,
Figure I Light microscopic appearance of G lamblza tropnozo:tes overlytng tne
superficial and foveolar epithelium of the gastric mucosa.
_! t ~~~~~~~~~.'^....2.. X.
+.wX-94 _,2/- _ *AX i,&.kX
:: ::,:.. .. Y. ': c
*...... S.. i .... S fi r
4-Xo u T ^ . ..
7
*
. e.:i -:. o.Figure.2T.ophozites are immunoreactive to the
anti-ardi polyclonarantiserum. ,
.itiw . .;;'9S.,. ,
m\ ^'>A '&Y1'§
Figure 2 Trpozie ar immunoreactivet theanti-Gardia polyclonal antiserum.
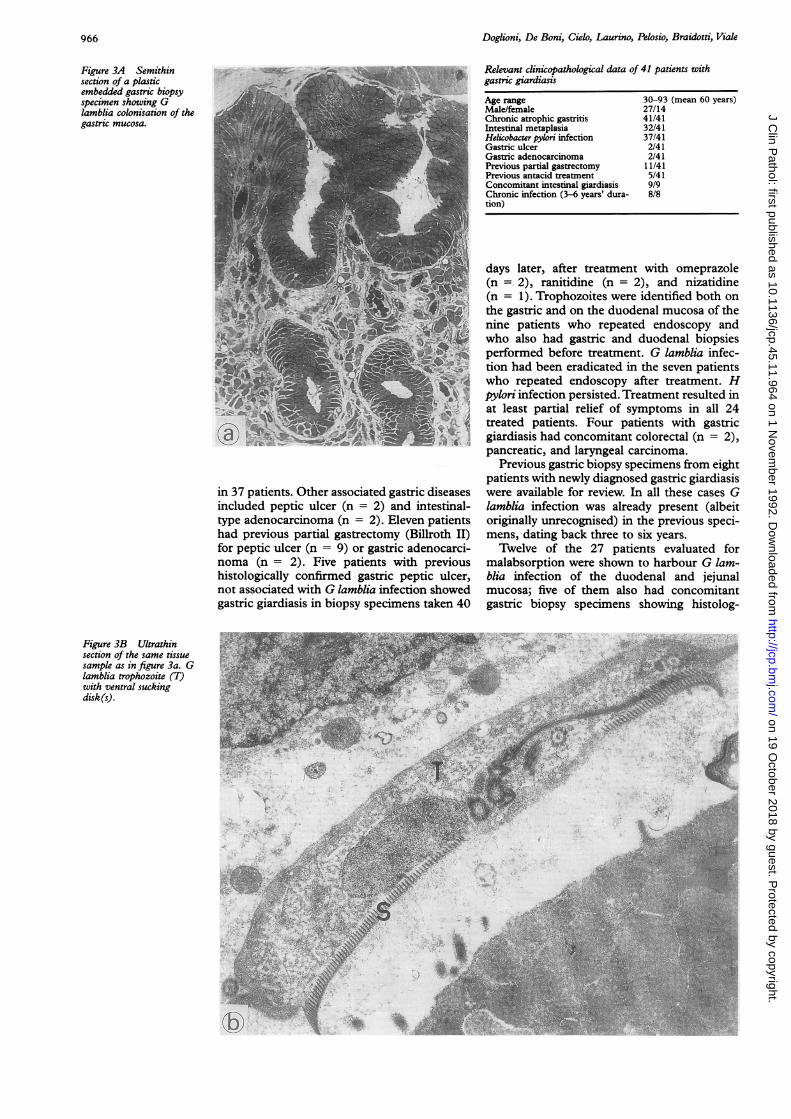
measuring 12-15 ,um in maximum diameter,showed the typical ultrastructural features of Glamblia,89 with a pair of ventral sucking disksand axostyles crossed by two parabasal bodies(fig 3). Four blepharoplasts and eight flagellawere clearly evident in step sections of thesame parasite.
Trophozoites were localised at the surfaceand at the base of foveolar pits, overlying thesuperficial and foveolar epithelium, and also inthe intestinal metaplastic epithelium. Theirnumber varied, ranging from five to more than100 in each biopsy specimen. In specimenstaken from gastric stumps, and includingjejunal mucosa, G lamblia was localised onboth gastric and intestinal epithelia. G lambliawas never observed over fundic-type gastricmucosa.
CLINICOPATHOLOGICAL DATA
Dyspepsia, epigastric pain, and abdominaldistension were the symptoms leading to endo-scopic examination of the upper gastrointesti-nal tract in the 41 patients with gastricgiardiasis. Only two patients had diarrhoea atthe time of endoscopy. Four patients hadrecently travelled abroad (Mexico, Turkey,former Yugoslavia, Greece). None had detect-able human immunodeficiency virus (HIV)serum antibodies; serological data available for13 patients did not indicate any abnormality inserum immunoglobulins.
Cases of gastric giardiasis were diagnosedsporadically all year long, without any apparentseasonal exacerbation of the infection. Fur-thermore, there did not seem to be anyclustering of the affected patients within spe-cific regional areas.The most relevant clinicopathological data
of the 41 patients with gastric giardiasis aresummarised in the table. All patients showedmoderate to severe chronic atrophic gastritiswith mild to severe activity, often associatedwith focal to extensive intestinal metaplasia.Concomitant H pylori infection was identified
965
on 19 October 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.45.11.964 on 1 Novem
ber 1992. Dow
nloaded from
Doglioni, De Boni, Cielo, Laurino, Pelosio, Braidotti, Viale
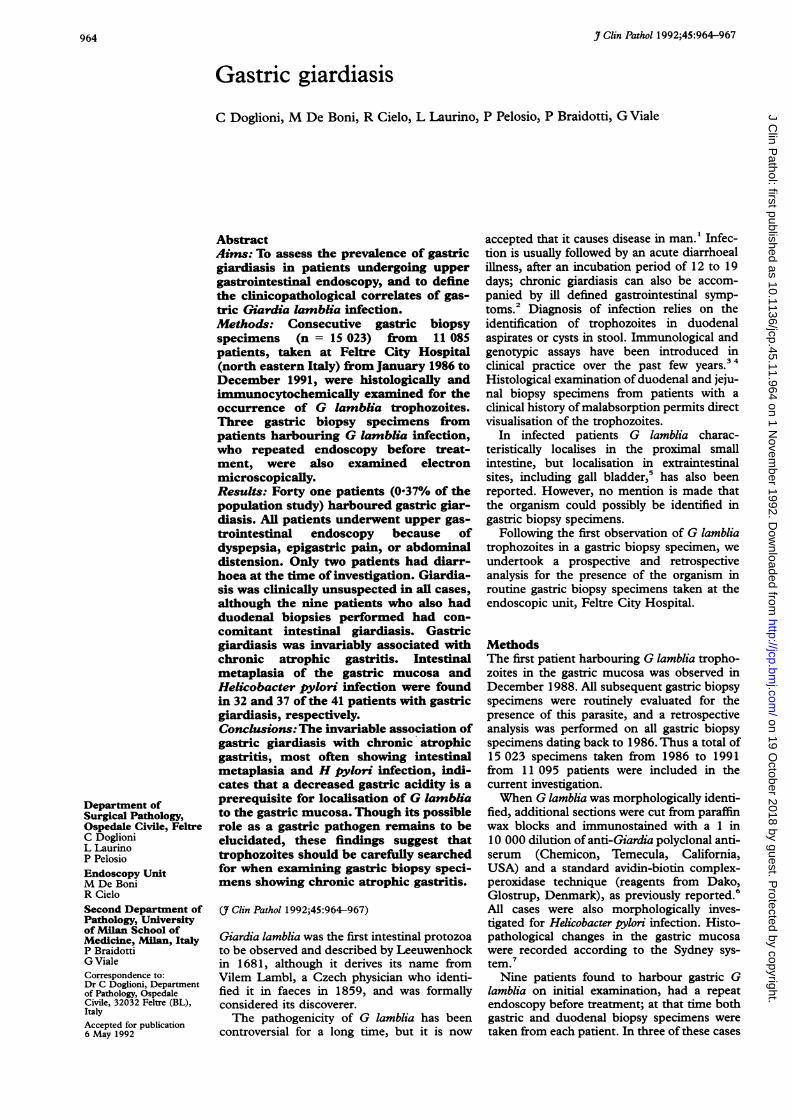
Figure 3A Semithinsection of a plasticembedded gastric biopsyspecimen showing Glamblia colonisation of thegastric mucosa.
Relevant clinicopathological data of 41 patients withgastric giardiasis
Age range 30-93 (mean 60 years)Male/female 27/14Chronic atrophic gastritis 41/41Intestinal metaplasia 32/41Helicobacter pylori infection 37/41Gastric ulcer 2/41Gastric adenocarcinoma 2/41Previous partial gastrectomy 11/41Previous antacid treatment 5/41Concomitant intestinal giardiasis 9/9Chronic infection (3-6 years' dura- 8/8tion)
in 37 patients. Other associated gastric diseasesincluded peptic ulcer (n = 2) and intestinal-type adenocarcinoma (n = 2). Eleven patientshad previous partial gastrectomy (Billroth II)for peptic ulcer (n = 9) or gastric adenocarci-noma (n = 2). Five patients with previoushistologically confirmed gastric peptic ulcer,not associated with G lamblia infection showedgastric giardiasis in biopsy specimens taken 40
days later, after treatment with omeprazole(n 2), ranitidine (n = 2), and nizatidine(n = 1). Trophozoites were identified both onthe gastric and on the duodenal mucosa of thenine patients who repeated endoscopy andwho also had gastric and duodenal biopsiesperformed before treatment. G lamblia infec-tion had been eradicated in the seven patientswho repeated endoscopy after treatment. Hpylon infection persisted. Treatment resulted inat least partial relief of symptoms in all 24treated patients. Four patients with gastricgiardiasis had concomitant colorectal (n = 2),pancreatic, and laryngeal carcinoma.
Previous gastric biopsy specimens from eightpatients with newly diagnosed gastric giardiasiswere available for review. In all these cases Glamblia infection was already present (albeitoriginally unrecognised) in the previous speci-mens, dating back three to six years.Twelve of the 27 patients evaluated for
malabsorption were shown to harbour G lam-blia infection of the duodenal and jejunalmucosa; five of them also had concomitantgastric biopsy specimens showing histolog-
Figure 3B Ultrathinsection of the same tissuesample as in figure 3a. Glamblia trophozoite (T)with ventral suckingdisk(s).
966
on 19 October 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.45.11.964 on 1 Novem
ber 1992. Dow
nloaded from

Gastric giardiasis
ically normal mucosa (n = 2) or H pyloriassociated chronic gastritis with mild atrophy(n = 3). Gastric giardiasis was absent in thesepatients.
Finally, only one of the 110 consecutivepatients undergoing upper gastrointestinaltract endoscopy showed evidence of G lambliainfection in the duodenal mucosa.
DiscussionTo the best of our knowledge, this is the firstreport on the localisation of G lamblia tro-phozoites to the gastric mucosa. The parasiteshave previously been identified in gastric lav-age fluids,'0 but contamination with duodenaljuice of these specimens cannot be precluded.The current study is based on a population ofalmost 80 000 inhabitants living in a restrictedarea of north eastern Italy, with a low preva-lence of giardiasis (less than 1% of the patientsundergoing upper gastrointestinal tract endo-scopy, as documented in the present series).Therefore, although our results do not comefrom a multicentre investigation, the reportedprevalence of G lamblia trophozoites in 0-37%of gastric biopsy specimens may well be con-sidered applicable to other areas with mediumto high socioeconomic standards.The small bowel mucosa is the expected area
of colonisation of G lamblia in infectedpatients; in this alkaline environment theorganism can complete its life cycle and exertits pathogenic effects." A significantlydecreased gastric acidity and modifications ofthe normal microenvironmental conditions ofthe gastric mucosa (becoming like those of thesmall bowel) may be essential prerequisites forG lamblia colonisation of the stomach. Indeed,we were unable to find any gastric infection inpatients with duodenal giardiasis and normalor slightly modified gastric mucosa. Con-versely, we identified G lamblia trophozoitesonly in the gastric biopsy specimens of patientswith chronic atrophic gastritis, most oftenassociated with Hpylori infection and showingintestinal metaplasia, and in gastric stumps.Both these conditions are known to reducesignificantly or completely abolish gastric acid-ity. Furthermore, five patients showed gastriccolonisation only after treatment with antacidsecreting drugs for peptic ulcer.
Gastric giardiasis may be chronic: eightpatients in our series had previous gastricbiopsy specimens (dating back three to sixyears) which already harboured G lambliainfection. At that time, however, we wereunaware of the possible occurrence of gastricgiardiasis and the presence of the trophozoiteswas therefore overlooked.The pathogenic effects of G lamblia on
gastric mucosa are difficult to evaluate, espe-cially because the histopathological changeswe observed were probably attributable toconcomitant H pylori infection. Specific mor-phological changes due to G lamblia colonisa-tion, however, have not been identified even inthe small bowel mucosa.'2 Furthermore, Glamblia infection was clinically unsuspected inall the 41 patients with gastric giardiasis. They
mostly complained of dyspepsia, epigastricpain, or abdominal distension, although arecent study refuted G lamblia as a cause ofnon-ulcer dyspepsia.. In any case the abovesymptoms are not specific and may well be dueto the underlying chronic atrophic gastritis andto H pylori infection. 3Treatment with metronidazole and antacid
drugs resulted in at least partial relief of thesymptoms, but it was impossible to evaluateseparately the effects of these medications.Metronidazole in the doses used, however, wasineffective at eradicating H pylori infection.Although the possible role of G lamblia as a
gastric pathogen remains to be clarified, webelieve that a careful search for trophozoitesshould become part of the routine histopath-ological examination of gastric biopsy speci-mens, with particular care given to thoseshowing chronic atrophic gastritis, and ofgastric stumps. Because gastric giardiasis isinvariably associated with intestinal giardiasis,the identification of G lamblia in gastric biopsyspecimens allows the infection to be diagnosedeven if clinically unsuspected (symptomsrelated to G lamblia infection are often atypical,as pointed out in recent studies,'4 and diversestrains of this parasite may exert differentpathogenic effects'5) and for appropriate treat-ment to be given.The demonstration of the actual capability
of G lamblia to colonise chronically the gastricmucosa might well stimulate further investiga-tions aimed at better defining the interactionsbetween man and this most common para-site.
1 WHO Expert Committee. Intestinal protozoan and helmin-tic infections. WHO Technical Report Series 666. Geneva:World Health Organization, 1981.
2 Chester AC, MacMurray FG, Restifo MD, Mann 0.Giardiasis as a chronic disease. Dig Dis Sci1985;30:215-8.
3 Green EL, Miles MA, Warhurst DC. Immunodiagnosticdetection of Giardia antigen in faeces by a rapid visualenzyme-linked immunosorbent assay. Lancet 1985;ii:691-3.
4 Butcher PD, Farthing MJG. DNA probes for the faecaldiagnosis of Giardia lamblia infections in man. BiochemSoc Trans 1989;17:363-4.
5 Goldstein F, Thomton JJ, Szydlowski T. Biliary tractdysfunction in giardiasis. Am Jf Dig Dis 1978;23:559-60.
6 Doglioni C, Dell'Orto P, Coggi G, luzzolino P, BontempiniL, Viale G. Choroid plexus tumors. An immunocyto-chemical study with particular reference to the coexpres-sion of intermediate filaments. Am Y Pathol1987;127:519-29.
7 Misiewicz nI, Tytgat GNJ, Goodwin CS, et al. The Sydneysystem: a new classification of gastritis. In: Working PartyReport. Melbourne: Blackwell Scientific Publications,1990:1-10.
8 Morecki R, Parker JG. Ultrastructural studies of the humanGiardia lamblia and subjacent jejunal mucosa in a subjectwith steatorrheoea. Gastroenterology 1967;52:151-64.
9 Brookes SEH, Audretsch J, Muller CG, Sparke B. Electronmicroscopy of Giardia lamblia in human jejunal biopsies.J Med Microbiol 1970;3: 196-9.
10 Koss LG. The gastrointestinal tract. In: Diagnostic cywlogyand its histopathological bases. Philadelphia: JB Lippincott,1979:834-5.
11 Ferguson A, Gillon J, Munro G. Pathology and pathogene-sis of the intestinal mucosal damage in the giardiasis. In:Meyer EA, ed. Giardiasis. Amsterdam: Elsevier,1990:155-95.
12 Oberhuber G, Stolte M. Giardiasis: analysis of histologicalchanges in biopsy specimens of 80 patients. J Clin Pathol1990;43:641-3.
13 Carr MF, Ma J, Green PHR. Giardia lamblia in patientsundergoing endoscopy: Lack of evidence for a role innon-ulcer dyspepsia. Gastroenterology 1988;95:972-4.
14 Gillon J. Clinical studies in adults presenting with giardiasisto a gastro-intestinal unit. Scot Med J 1985;30:89-95.
15 Nash TE, Herrington DA, Losonsky GA, Levine MM.Experimental human infections with Giardia lamblia. JInfect Dis 1987;156:974-84.
967
on 19 October 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.45.11.964 on 1 Novem
ber 1992. Dow
nloaded from