gout a rapid review - rural primary care conference · the hyperuricemia cascade urate...
TRANSCRIPT

Gout
A rapid review
Jeremy Jones

The Hyperuricemia Cascade
Urate
Hyperuricemia
Overproduction Underexcretion
Associated
cardiovascular events
and mortality
Renal
manifestationsGout
Endogenous
purine synthesisDietary
purines
Tissue
nucleic acids
Silent
tissue
deposition
Main predisposing factors
1. Family history
2. Life style
• Inactive
• Obesity
• Wrong diet
• Alcohol
• etc

Hyperuricaemia
• Overproduction– Inherited tendency
– Severe enzyme deficencies
• Glucose 6 phosphatase
• Fructose 1 phosphatase aldolase
– Myeloproliferative
– Lymphoproliferative
– Polycythaemia
– Malignancy
– Psoriasis
– Drugs/dietary
• Alcohol, cytotoxic, DXT
• Undersecretors• Inherited
• Chronic renal failure
• Dehydration
• Starvation
• Drugs/dietary
• Alcohol,
• diuretics,
• aspirin,
• cyclosporin

Advanced
Gout
Long-term gouty
complications of
uncontrolled
hyperuricemia
Intercritical
Segments
The intervals
between
acute flares
Acute Flares
Acute inflammation
in the joint caused
by urate
crystallization
Asymptomatic
Hyperuricemia
Elevated serum urate
with no clinical
manifestations of gout
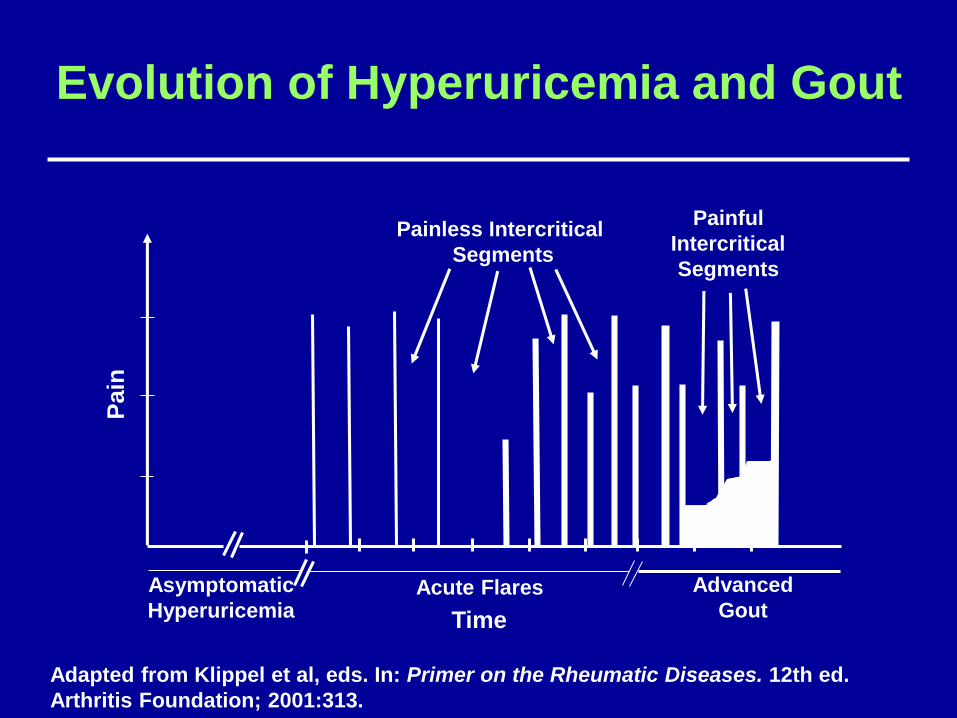
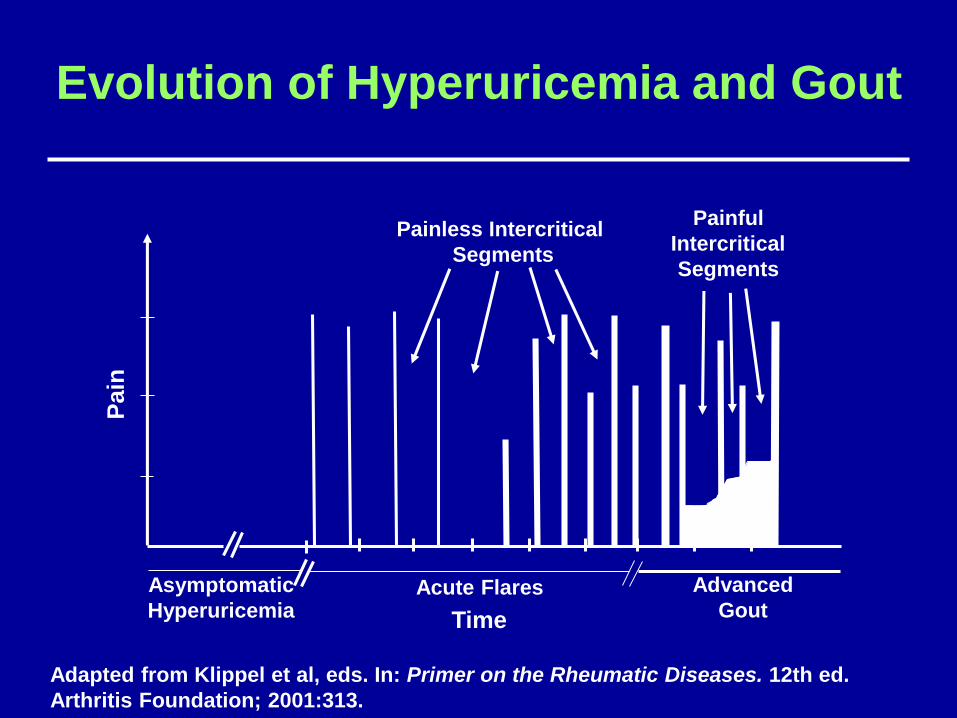
Uncontrolled Hyperuricemia

Evolution of Hyperuricemia and Gout
Asymptomatic
HyperuricemiaAcute Flares Advanced
Gout
Painless Intercritical
Segments
Painful
Intercritical
Segments
Pain
Time
Adapted from Klippel et al, eds. In: Primer on the Rheumatic Diseases. 12th ed.
Arthritis Foundation; 2001:313.
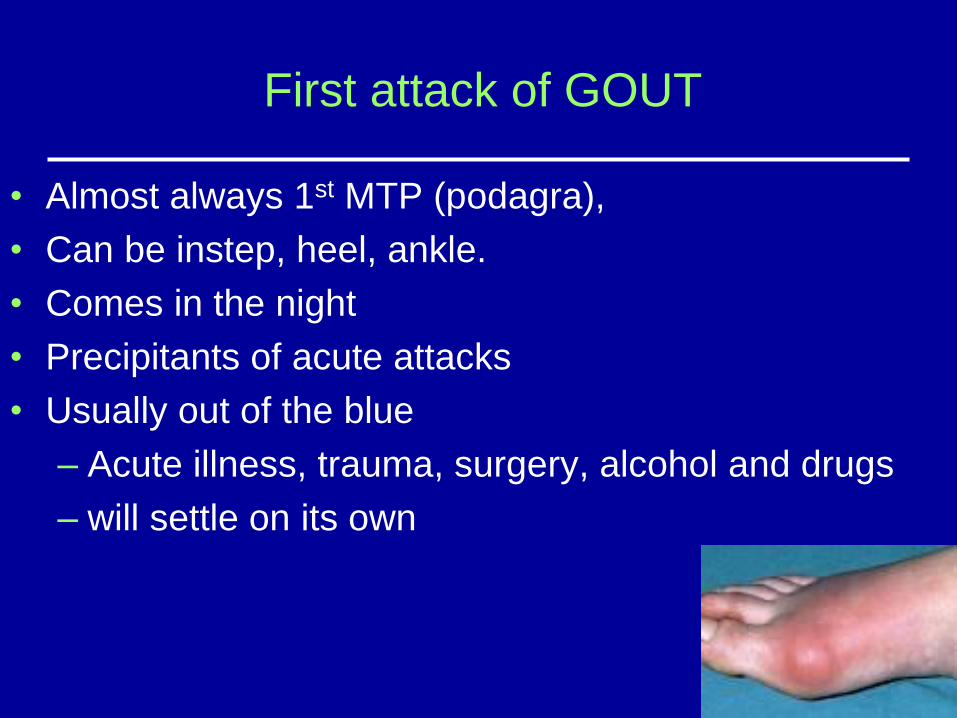
First attack of GOUT
• Almost always 1st MTP (podagra),
• Can be instep, heel, ankle.
• Comes in the night
• Precipitants of acute attacks
• Usually out of the blue
– Acute illness, trauma, surgery, alcohol and drugs
– will settle on its own

25% - 40% of patients during an acute
attack of gout will have normal levels of
urate
Evolution of Hyperuricemia and Gout
Asymptomatic
HyperuricemiaAcute Flares Advanced
Gout
Painless Intercritical
Segments
Painful
Intercritical
Segments
Pain
Time
Adapted from Klippel et al, eds. In: Primer on the Rheumatic Diseases. 12th ed.
Arthritis Foundation; 2001:313.
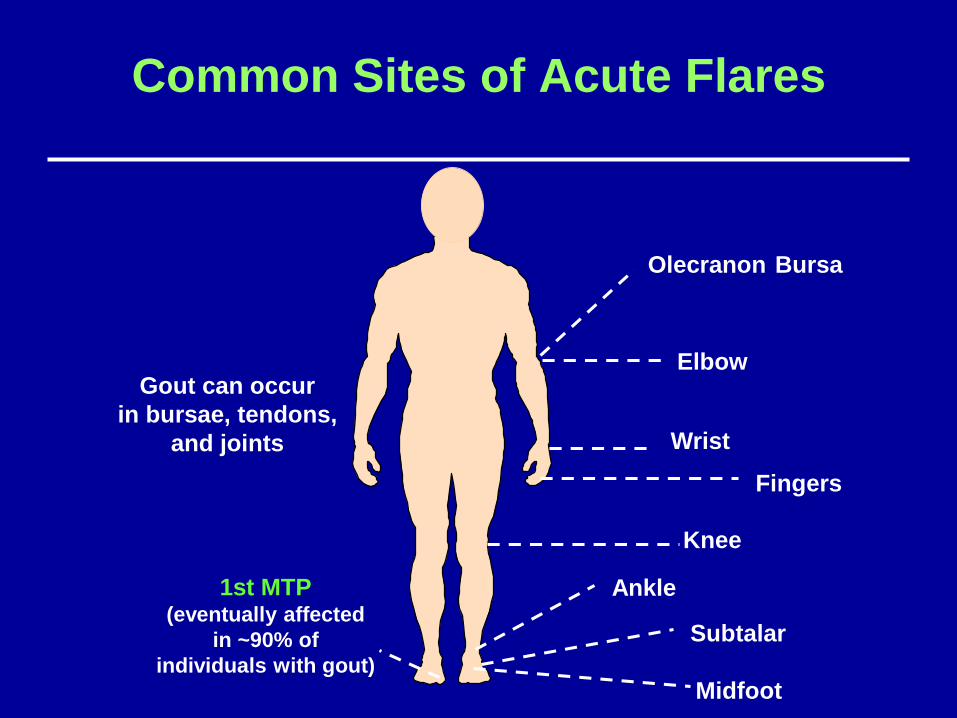
Common Sites of Acute Flares
Midfoot
Gout can occur
in bursae, tendons,
and joints
Olecranon Bursa
Elbow
Wrist
Knee
Ankle
Subtalar
1st MTP(eventually affected
in ~90% of
individuals with gout)
Fingers
Evolution of Hyperuricemia and Gout
Asymptomatic
HyperuricemiaAcute Flares Advanced
Gout
Painless Intercritical
Segments
Painful
Intercritical
Segments
Pain
Time
Adapted from Klippel et al, eds. In: Primer on the Rheumatic Diseases. 12th ed.
Arthritis Foundation; 2001:313.

Advanced GoutClinically Apparent Tophi
ACR Clinical Slide Collection on the Rheumatic Diseases, 1998.
Helix of the ear
Hands, fingers, and wrists

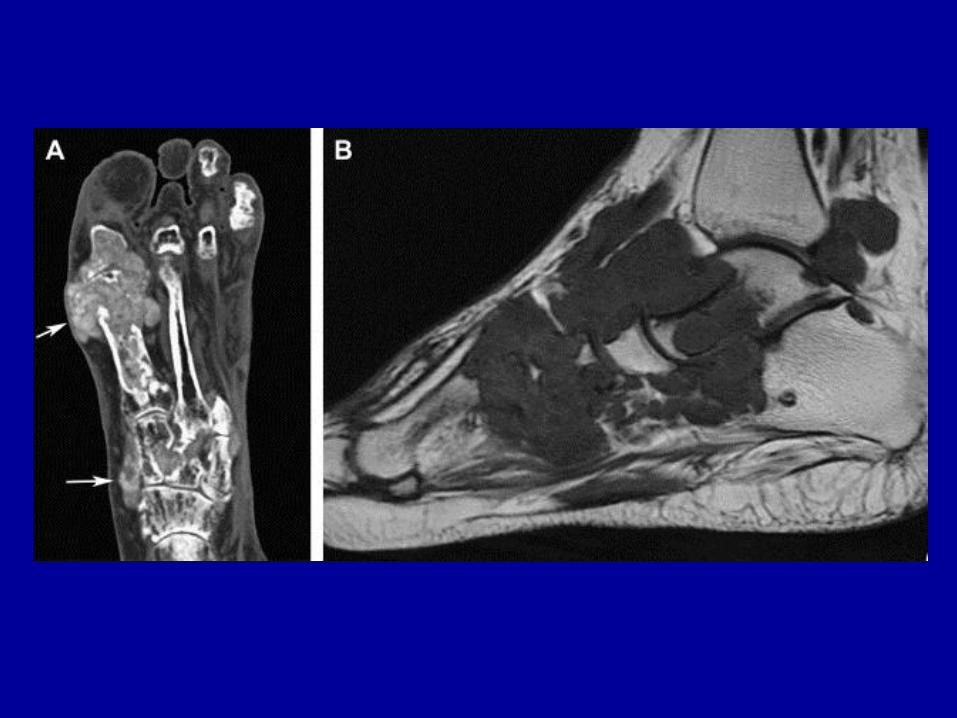

Gout kidney
Why treat gout?
• Prevent severe pain and disability of acute
attacks
• Present damage to joints from tophi
• Prevent tophi being deposited elsewhere
• Preserve kidney function

Treatment of gout
1. General
2. Acute gout
3. Lowering urate

Treatment of gout
General
• EDUCATION, EDUCATION, EDUCATION.
• LIFESTYLE MODIFICATION
• REVIEW DRUGS (Diuretics Especially)
• COMPLIANCE (it’s a man thing!)
Treatment of gout
Acute gout
NSAIDs
Colchicine
Steroids

NSAIDs
Colchicine
What is the dosing
regime of
colchicine?

Treatment of acute gout
Colchicine
• Therapeutic dose close to the toxic dose
So needs to be tailored to the patient
• Excreted by the kidney
So care in those with renal impairment
• Diarrhoea means too much drug, not that colchicine is contraindicated
• Therapeutic dose ranges from 0.5 mgs tds to 0.5 mg alternate days or even every third day
Treatment of acute gout
Steroids
• Useful in those unable to tolerate NSAIDs
and severe polyarticular gout
• Intra-articular will settle down a joint
• ACTH injection (Synacthen depot 1 mgs in
1 ml IMI) will settle polyarticular gout,
grumbling gout and the gouty grump.
• Intra-muscular steroids or tablets less
useful than ACTH
Treatment of gout
Lowering urate
• Do not start urate lowering drugs if there is
active gout
• It is likely to cause a flare and your patient will
lose faith in you and the drug
• If gout is a bit touchy, cover introduction of
urate lowering drug with Colchicine and/ or
NSAIDs.
• Treatment will be lifelong

Treatment of Gout
Lowering urate
ALLOPURINOL
• Competitively inhibits xanthine oxidases
• If there has been acute gout or poor renal function, start gingerly (100 mgs/day or alternate days)
• Cover with Colchicine/NSAID as necessary
• Dose must be tailored to individual; effective dose varies between 100-800mgs)
• Need to titrate to target urate level (<0.36 for gout; <0.30 for tophi resorption)

Treatment of gout
Lowering urate
Febuxostat– Nonpurine xanthine oxidase inhibitor– More selective than Allopurinol– Metabolised by the liver– Effective in moderate renal impairment– Very promising but ……– Used as second line to Allopurinol at the
moment

Treatment of gout
Lowering urate
Third LINE drugsPromote the clearance uric acid by inhibiting renal tubular
reabsorption
Probenecid
Sulphinpyrazone
Benzbromarone

New treatments
• Uricase
• Uricosuric
• Xanthine Oxidase
Inhibitors
• Biologic (IL6 inhibitor)
Pegloticase
Uricase PEG 20
Rasburicase
Lesinurad (Inhibits uric acid
resorption)
Oxpurinol
Anakinra

KEY MESSAGES
• Gout is very treatable disease and
should be treated seriously
• Must treat to target
• reduce SUA < 0.36mmol/l in all cases
• If tophi reduce SUA < 0.3 or under to
reabsorb them
• Treatment is lifelong

NZ atlas of health care variation• http://www.hqsc.govt.nz/our-programmes/health-quality-evaluation/projects/atlas-of-healthcare-variation/gout/