grey bruce health services - gbhs.on.ca accreditation report.pdf · grey bruce health services...
TRANSCRIPT

Accreditation Report
Grey Bruce Health Services
On-site Survey Dates:
Accredited by ISQua
Owen Sound, ON
Prepared for:
September 12, 2010 - September 17, 2010
October 1, 2010

Confidentiality
This Report is confidential and is provided by Accreditation Canada to Grey Bruce Health Services only. Accreditation Canada does not release the Report to any other parties.
In the interests of transparency, Accreditation Canada encourages the dissemination of the information in this Report to staff, board members, clients, the community, and other stakeholders.
About this Report
The results of this accreditation survey are documented in the attached report, which was prepared by Accreditation Canada at the request of Grey Bruce Health Services.
This report is based on information obtained from the organization. Accreditation Canada relies on the accuracy of this information to conduct the survey and to prepare the report. The contents of this report is subject to review by Accreditation Canada. Any alteration of this report would compromise the integrity of the accreditation process and is strictly prohibited.
Accreditation Report
© Accreditation Canada, 2010

Table of Contents
About the Accreditation Report........................................................................................................................ii
Accreditation Summary.................................................................................................................................1
Surveyor’s Commentary.................................................................................................................................3
Organization's Commentary.............................................................................................................................5
Overview by Quality Dimension.........................................................................................................................6
Overview by Standard Section..........................................................................................................................7
Overview by Required Organizational Practices (ROPs)..................................................................................................8
Detailed Accreditation Results........................................................................................................................9
Performance Measure Results...........................................................................................................................52
Instrument Results................................................................................................................................52
Indicator Results.................................................................................................................................63
Next Steps............................................................................................................................................70
Appendix A – Accreditation Decision Guidelines........................................................................................................71
QMENTUM PROGRAM
iTable of Contents
About the Accreditation Report
The accreditation report describes the findings of the organization's accreditation survey. It is Accreditation Canada's intention that the comments and identified areas for improvement in this report will support the organization to continue to improve quality of care and services it provides to its clients and community.
Legend
A number of symbols are used throughout the report. Please refer to the legend below for a description of these symbols.
Items marked with a GREEN flag reflect areas that have not been flagged for improvements. Evidence of action taken is not required for these areas.
Items marked with a YELLOW flag indicate areas where some improvement is required. The team is required to submit evidence of action taken for each item with a yellow flag.
Items marked with a RED flag indicate areas where substantial improvement is required. The team is required to submit evidence of action taken for each item with a red flag.
Leading Practices are noteworthy practices carried out by the organization and tied to the standards. Whereas strengths are recognized for what they contribute to the organization, leading practices are notable for what they could contribute to the field.
Items marked with an arrow indicate a high risk criterion.
Accreditation Report
About the Accreditation Reportii

QMENTUM PROGRAM
Accreditation Summary
Grey Bruce Health Services
On-site survey dates September 12 to 17, 2010
Accreditation with Condition (Report)Accreditation Decision
This section of the report provides a summary of the survey visit and the status of the accreditation decision.
Report Issue Date: October 1, 2010
The following locations were visited during this survey visit:
Locations
1 Lion's Head Hospital
2 Markdale Hospital
3 Meaford Hospital
4 Owen Sound Hospital
5 Southampton Hospital
6 Wiarton Hospital
The following service areas were visited during this survey visit:
Service areas
1 Ambulatory Care
2 Cancer Care
3 Diagnostic Imaging
4 Emergency Department
5 Intensive Care Unit/Critical Care
6 Maternal/Perinatal
7 Medicine
8 Mental Health
9 Operating Room
10 Rehabilitation
11 Sterilization and Reprocessing of Medical Equipment
Accreditation Summary 1
12 Surgical Care

QMENTUM PROGRAM
Surveyor’s Commentary
The following global comments regarding the survey visit are provided:
There is a strong Board of Directors with representation which reflects the community it serves. Its Bylaws are current and there are appropriate evaluation processes in place. There are board members with cross appointments on other boards for a period of one year and vice versa. For example, there is a member of the CCAC board on this board currently. The board, executive and other leaders value partnerships. There are many partnerships at the CEO level with other CEOs in the region, and the same occurs at the Chief of Medical Staff and Senior Nursing levels. There are quarterly Community Advisory committees representing each hospital community as well as annual forums in each community to update the specific community and educate them on health issues of the day. There is a patient-centred staff and group of service providers. There is low turnover with staff and so few vacancies. Many unique and varied programs for staff are in place to help support worklife balance such as work 4 days a week while protecting your pension. There are about eight hundred volunteers who support the organization. There is excellent educational support for staff.
There is an ethics framework and program in place and it is referred to frequently. The Board uses the values of the organization and the framework to assist them in decision-making.
The organization has balanced its operating budget for 2009-10 with no service cuts. Thirteen hospital sites in the area have integrated services such Lab, Diagnostic Imaging, Pharmacy and others. Using the same information system, they have been able to integrate patient information and thus are able to share this across sites which benefits patients physicians and staff. Client drug profiles have been implemented in the small rural sites as has the electronic medication administration record. The staff find this very helpful. There are many new patient risk assessment tools in place to assess for potential falls, skin and wound breakdown and others. Many new patient safety initiatives have occurred such as the use of two identifiers. Staff are very aware of the Required Organizational Practices (ROPs). and work to implement these. New systems have been introduced such as the Risk Monitor Pro, risk management system, the incident management system and others.
There are infrastructure issues which need to be addressed both at Markdale and Southampton hospital sites. Physician engagement is an issue for the organization. There are those physicians who wish to practice the historic rural style of medicine and those who wish to practice a more urban style. There seems to be a conflict based on these philosophies. Staff safety on weekends and the back shifts in small rural hospitals will always be an issue. Give the appropriate attention, scrutiny and actions taken to maximize staff safety at all times.
The CEO is in place for just over a year. At present there is an interim or temporary management structure. It has been found to be very confusing to staff and others. A review of the organizational structure is needed and a new structure developed which delineates clear lines of responsibility and accountability across the organization's 6 sites so that staff readily know to whom they report and thus avoiding the potential for confusion, gaps or duplication. There are clinical service teams whose roles need to be reviewed to ensure they are supportive of the new structure. The organization is encouraged to continue to educate staff, service providers and volunteers in their role in patient safety. They are encouraged to continue their quality and risk initiatives involving staff and educating staff about these initiatives as much as possible and feasible. The strategic plan was completed in 2005. There are plans to do another planning process in the fall to refresh and renew this plan. Currently there appears to be limited evidence of formal goals and objectives below the level of the executive committee. There is planning which occurs but it does not appear to be linked to the strategic goals and objectives. With
Surveyor’s Commentary2
the development of the new strategic plan there is an opportunity to correct this issue.

QMENTUM PROGRAM
Organization's Commentary
Organization's Commentary 3
The following comments were provided to Accreditation Canada post survey.
Grey Bruce Health Services welcomed our Accreditation Surveyors to our organization for the week of September 13th to 17th. During this time, the surveyors visited all of the Grey Bruce Health Services Hospitals and spoke with numerous patients, physician, volunteers and staff members through their use of the Qmentum tracers. It was felt to be a positive experience by all. Feedback received from the surveyors was consistent with the strengths and opportunities that the organization had identified through the self-assessment process. The surveyors found a very strong organizational engagement in patient safety activities. We look forward to moving ahead with our organizational strategic planning and aligning the work of our teams with these goals and objectives. This was the first time that the organization was assessed against specific accreditation standards within our SPD, Diagnostic Imaging, Medication Management and Infection Control Departments and gave these teams the opportunity to receive feedback. Recommendations received from Accreditation Canada will be integrated into the GBHS goals and objectives.
Accreditation Report
Overview by Quality Dimension
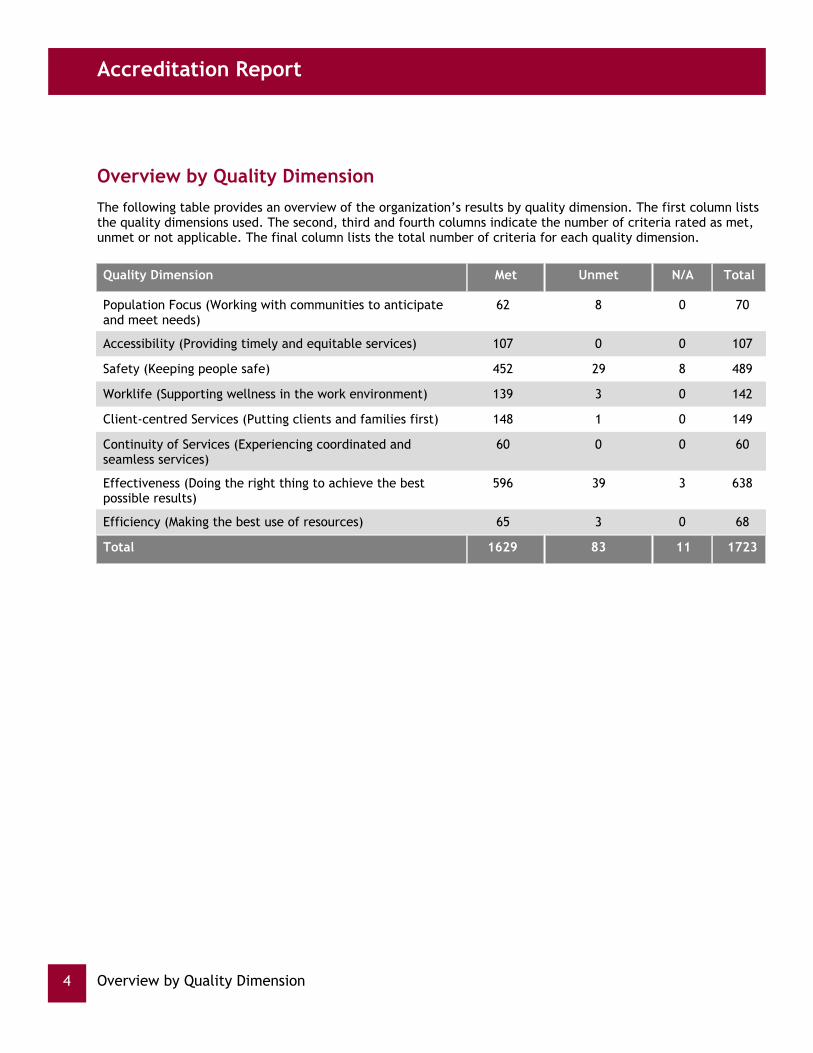
The following table provides an overview of the organization’s results by quality dimension. The first column lists the quality dimensions used. The second, third and fourth columns indicate the number of criteria rated as met, unmet or not applicable. The final column lists the total number of criteria for each quality dimension.
Quality Dimension Met Unmet N/A Total
Population Focus (Working with communities to anticipate and meet needs)
62 8 0 70
Accessibility (Providing timely and equitable services) 107 0 0 107
Safety (Keeping people safe) 452 29 8 489
Worklife (Supporting wellness in the work environment) 139 3 0 142
Client-centred Services (Putting clients and families first) 148 1 0 149
Continuity of Services (Experiencing coordinated and seamless services)
60 0 0 60
Effectiveness (Doing the right thing to achieve the best possible results)
596 39 3 638
Efficiency (Making the best use of resources) 65 3 0 68
Total 1629 83 11 1723
Overview by Quality Dimension4

QMENTUM PROGRAM
Overview by Standard Section
The following table provides an overview of the organization by standard section. The first column lists the standard section used. The second, third and fourth columns indicate the number of criteria rated as met, unmet or not applicable. The final column lists the total number of criteria for that standard section.
Standard Section Met Unmet N/A Total
Sustainable Governance 90 1 0 91
Effective Organization 100 5 0 105
Infection Prevention and Control 103 0 0 103
Ambulatory Care Services 106 13 1 120
Cancer Care and Oncology Services 104 5 1 110
Critical Care 103 6 0 109
Diagnostic Imaging Services 100 4 0 104
Emergency Department 101 6 0 107
Managing Medications 130 4 1 135
Medicine Services 96 8 0 104
Mental Health Services 99 12 0 111
Obstetrics/Perinatal Care Services 109 4 6 119
Operating Rooms 102 0 0 102
Rehabilitation Services 96 7 0 103
Reprocessing and Sterilization of Reusable Medical Devices 96 2 1 99
Surgical Care Services 94 6 1 101
Total 1629 83 11 1723
Overview by Standard Section 5

Accreditation Report
Based on the accreditation review, the table highlights each ROP that requires attention and its location in the standards.
Overview by Required Organizational Practices (ROPs)
Criteria Required Organizational Practices
The organization implements a formal and open policy and process for disclosure of adverse events to clients and families, including support mechanisms for clients, family, staff, and service providers involved in adverse events.
Effective Organization 6.5
The team reconciles medications with the client at referral or transfer, and communicates information about the client’s medications to the next provider of service at referral or transfer to another setting, service, service provider, or level of care within or outside the organization.
Ambulatory Care Services 12.2
The team reconciles medications with the client at referral or transfer, and communicates information about the client’s medications to the next provider of service at referral or transfer to another setting, service, service provider, or level of care within or outside the organization.
Critical Care 12.5
The team informs and educates its clients and families in writing and verbally about the client and family’s role in promoting safety.
Diagnostic Imaging Services 14.6
The organization removes concentrated electrolytes (including, but not limited to, potassium chloride, potassium phosphate, sodium chloride >0.9%) from client service areas.
Managing Medications 7.2
Staff and service providers receive ongoing, effective training on infusion pumps.
Mental Health Services 4.4
The team reconciles medications with the client at referral or transfer, and communicates information about the client’s medications to the next provider of service at referral or transfer to another setting, service, service provider, or level of care within or outside the organization.
Mental Health Services 11.3
The team reconciles medications with the client at referral or transfer, and communicates information about the client’s medications to the next provider of service at referral or transfer to another setting, service, service provider, or level of care within or outside the organization.
Rehabilitation Services 11.3
The team reconciles medications with the client at referral or transfer, and communicates information about the client’s medications to the next provider of service at referral or transfer to another setting, service, service provider, or level of care within or outside the organization.
Surgical Care Services 11.4
Overview by Required Organizational Practices (ROPs)6

QMENTUM PROGRAM
Detailed Accreditation Results
This part of the report speaks to the processes and infrastructure needed to support service delivery. In the regional context, this part of the report also highlights the consistency of the implementation and coordination of these processes across the entire system. Some specific areas that are evaluated include: integrated quality management, planning and service design, resource allocation, and communication across the organization.
Findings
System-Wide Processes and Infrastructure
Following the survey, once the organization has the opportunity to address the unresolved criteria and provide evidence of action taken, the results will be updated to show that they have been addressed.
Developing and implementing the infrastructure, programs and service to meet the needs of the community and populations served.
Planning and Service Design
There is a strategic plan in place which was created in 2005 with current goals and objectives for 2009 to 2011 which are monitored regularly by the board and executive committee. The board has 12 members with members who have cross-appointed board members from other boards such as CCAC. Some members of this board have cross-appointments with other boards as well. The board receives input from its rural communities from its community advisory committees, of which they is one in each of the 5 rural communities which meet quarterly. There is also an annual public forum in each of the 5 rural communities which have an educational component and an opportunity for input to the leadership team. The board receives information from a scorecard with performance indicators updated and analyzed. Areas to improve The board is encouraged to implement its strategic planning process as it plans for the fall involving a wide range and number of stakeholders to ensure the input from all stakeholders is gathered and analysed to create a comprehensive strategic plan to take the organization into future. The organizational structure is temporary at this time. The organization is encouraged to review the structure and make it permanent as soon as is feasible. The organization is encouraged to ensure that the reporting relationships and the resulting roles, responsibilities and accountabilities in the final structure are clearly defined and delineated so there is no possibility for confusion, gaps or duplication.
Surveyor Comments
No Unmet Criteria for this Priority Process.
Monitoring, administration, and integration of activities involved with the appropriate allocation and use of resources.
Resource Management
Detailed Accreditation Results 7

Accreditation Report
The organization is commended for balancing its budget for 2009-10 without service cuts. There are processes for developmenting, implementing and monitoring operating and capital budgets. There are processes in place to oversee the management of contracts. There are continguency funds available to manage unforeseen situations which arise
No Unmet Criteria for this Priority Process.
Developing the human resource capacity to deliver safe and high quality services to clients.
Human Capital
There is human resources plan and a manpower plan in place. A human resources scorecard has been introduced for reporting to executive team and the board on human resource issues regularly. There are appropriate processes to recruit board members, staff, physicians and volunteers. There are orientation programs designed to meet the needs of each group. Retention programs are in place as are wellness, and recognition programs. A management learning system for educating staff online at their convenience. A talent management program with the goal of developing new managers from within the organization is being implemented. Turnover is low and recruitment is not an issue currently. Worklife balance issues are addressed with programs into which staff have much input. There is an active Occupational Health and Safety team at all sites with certified members at each site. There are return to work programs which staff who are returning to work rate as good as do the staff on units where staff are returning. There is an organizational development program which assists with the implementation of educational programs such as the prevention of workplace violence. Quality improvement activities are in place and the use of best practice and evidenced based care are evident. The organization is commended for supporting four staff to attend the Executive Training in Research Application (EXTRA) at the Canadian Health Services Research Foundation. The Management Learning System has been implemented and is being used effectively . Areas to improve: Sicktime has increased in the last year and the team is encouraged to continue its rollout of the attendance management program. Staff are encouraged to be involved in human resource initiatives and they are engaged. The human resources team is encouraged to ensure that they keep staff informed of the changes made as a result of the input they provided. In this way they will continue to provide input knowing they can influence change. The team is encouraged to strengthen the role of staff in promoting patient safety as outlined in their job descriptions. The organization is encouraged to survey and/or discuss with staff regularly their preception of staff safety especially in the small rural hospitals where staff is limited in the off hours to ensure management is aware and takes action on any potential issues which may occur.
Surveyor Comments
No Unmet Criteria for this Priority Process.
Continuous, proactive and systematic process to understand, manage and communicate quality from a system-wide perspective to achieve goals and objectives.
Integrated Quality Management
Strengths. There is a board Quality Committee which receives regular updates on the quality management activities of the organization which includes patient safety activities. The executive team forms the membership of the Quality of Care Committee. There is a current Quality Workplan which has goals and objectives for the coming 3 years. A scorecard is provided regularly to the board members with information on selected indicators in a comprehensive fashion. There are patient safety walkabouts on all units at least twice each year attended by CEO, member of the executive team and others where patient safety issues are discussed with staff. Patients may be included in these safety conversations. Patient safety issues are placed at the beginning of the MAC agenda. The staff is aware of the importance of patient safety and their role in it. Areas to Improve There is a Utilization Management Committee with active physician engagement which functions effectively. The organization is encouraged to continue to try to bring it into the Quality Management framework in order that it is integrated into this framework with patient safety, quality improvement and risk management.
Surveyor Comments
Detailed Accreditation Results8
The organization is commended for balancing its budget for 2009-10 without service cuts. There are processes for developmenting, implementing and monitoring operating and capital budgets. There are processes in place to oversee the management of contracts. There are continguency funds available to manage unforeseen situations which arise
Surveyor Comments
regularly to the board members with information on selected indicators in a comprehensive fashion.

QMENTUM PROGRAM
There are patient safety walkabouts on all units at least twice each year attended by CEO, member of the executive team and others where patient safety issues are discussed with staff. Patients may be included in these safety conversations. Patient safety issues are placed at the beginning of the MAC agenda. The staff is aware of the importance of patient safety and their role in it. Areas to Improve There is a Utilization Management Committee with active physician engagement which functions effectively. The organization is encouraged to continue to try to bring it into the Quality Management framework in order that it is integrated into this framework with patient safety, quality improvement and risk management.
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
Effective Organization
The organization implements a formal and open policy and process for disclosure of adverse events to clients and families, including support mechanisms for clients, family, staff, and service providers involved in adverse events.
6.5
The disclosure policy includes support mechanisms for clients, families, staff and service providers.
6.5.2
The organization’s leaders, staff, service providers, volunteers, and students receive recognition for their quality improvement work.
7.5
The organization’s leaders require service or program areas to monitor their own process and outcome indicators, and monitor and support their efforts to do so.
14.6
Sustainable Governance
The governing body demonstrates a commitment to recognizing staff, service providers, volunteers, and students for their quality improvement work.
15.7
Identifying and decision making regarding ethical dilemmas and problems.
Principle Based Care and Decision Making
Strengths:
There is a defined framework, policies and procedures, committee structure, external Ethicist expertise when required and educational sessions to support the Grey Bruce hospital community
both groups worked through the fiscal challenges faced by the corporation to balance its financial position. Members of these groups articulated that the framework for decision making as well as revisiting the values of the corporation was very helpful in allowing them to make what they felt were responsible and defensible decisions to their many internal and external stakeholder groups. The framework has also helped the group with respect to the debate around the future of the thoracic surgery program at the Owen Sounds site.
The Grey Bruce Health Services organization has been highlighted in Accreditation Canada's 2009 conference for both its ethical framework as well as for its process for managing Research Ethics in a Rural Hospital setting. The processes developed for research ethics and the management of research projects in the rural environment are shared with Hanover & District Hospital as well as South Bruce Grey Health Centre. The Clinical Research Advisory Group (CRAG) is very responsive to research requests and do due diligence from the ethical, scientific and administrative aspects of each request that is received.
Areas for Improvement:
It is anticipated that with the potential growth in the oncology program as well as potential increase in requests for orthopaedic research that capacity building for the Clinical Research Advisory Group be considered especially when expedited reviews are requested. Currently, the workload for managing the infrastructure support for the Research function is manageable however, the organization needs to think about building capacity and succession planning to support the research agenda if there is a desire and ability to grow this capacity into the future.
The Clinical Research Advisory Group and the Ethics Committee have no formalized process in place for when an appeal is made with respect to a Research project being denied. Development of a formal appeal process is suggested as it will support transparent and objective decision making for the organization. Further, it is suggested that the Ethics Committee provide a status update on Research activities and their scope on a regular basis to the Board via the Board Quality Committee.
The area of Advanced Directives and their practical application at Grey Bruce Health Services has been identified as an area that needs to be revisited as it applies to acute care. Work on this initiative in the Long Term Sector, EMS and CCAC has occurred with resulting modifications in terms of how advanced directives are to be handled by hospital staff. Changes made appear to be problematic to implement and require review and adjustment so that advanced directives are followed and staff are comfortable doing so in a time efficient fashion.
One of the organization's strategic goals is to operationalize its ethics framework and ensure the informed consent process is hardwired in all clinical areas at the front line level. The organization is encouraged to implement educational and other strategies to ensure that front line staff do have a good understanding of the supports that are available to them for ethical issues as well as building awareness, capacity and understanding of ethical issues and how they can best be managed. Key areas that have surfaced where staff require more educational support are advanced directives, consents and elder abuse.
Surveyor Comments
Detailed Accreditation Results 9
on Ethical issues.

Accreditation Report
The framework was used by the Senior leadership level and by the Board as both groups worked through the fiscal challenges faced by the corporation to balance its financial position. Members of these groups articulated that the framework for decision making as well as revisiting the values of the corporation was very helpful in allowing them to make what they felt were responsible and defensible decisions to their many internal and external stakeholder groups. The framework has also helped the group with respect to the debate around the future of the thoracic surgery program at the Owen Sounds site.
The Grey Bruce Health Services organization has been highlighted in Accreditation Canada's 2009 conference for both its ethical framework as well as for its process for managing Research Ethics in a Rural Hospital setting. The processes developed for research ethics and the management of research projects in the rural environment are shared with Hanover & District Hospital as well as South Bruce Grey Health Centre. The Clinical Research Advisory Group (CRAG) is very responsive to research requests and do due diligence from the ethical, scientific and administrative aspects of each request that is received.
Areas for Improvement:
It is anticipated that with the potential growth in the oncology program as well as potential increase in requests for orthopaedic research that capacity building for the Clinical Research Advisory Group be considered especially when expedited reviews are requested. Currently, the workload for managing the infrastructure support for the Research function is manageable however, the organization needs to think about building capacity and succession planning to support the research agenda if there is a desire and ability to grow this capacity into the future.
The Clinical Research Advisory Group and the Ethics Committee have no formalized process in place for when an appeal is made with respect to a Research project being denied. Development of a formal appeal process is suggested as it will support transparent and objective decision making for the organization. Further, it is suggested that the Ethics Committee provide a status update on Research activities and their scope on a regular basis to the Board via the Board Quality Committee.
The area of Advanced Directives and their practical application at Grey Bruce Health Services has been identified as an area that needs to be revisited as it applies to acute care. Work on this initiative in the Long Term Sector, EMS and CCAC has occurred with resulting modifications in terms of how advanced directives are to be handled by hospital staff. Changes made appear to be problematic to implement and require review and adjustment so that advanced directives are followed and staff are comfortable doing so in a time efficient fashion.
One of the organization's strategic goals is to operationalize its ethics framework and ensure the informed consent process is hardwired in all clinical areas at the front line level. The organization is encouraged to implement educational and other strategies to ensure that front line staff do have a good understanding of the supports that are available to them for ethical issues as well as building awareness, capacity and understanding of ethical issues and how they can best be managed. Key areas that have surfaced where staff require more educational support are advanced directives, consents and elder abuse.
No Unmet Criteria for this Priority Process.
Communication among various layers of the organization, and with external stakeholders.
Communication
Detailed Accreditation Results10

QMENTUM PROGRAM
There appears to be effective communication with and among all levels in the organization. People state they are knowledgeable of what is happening. There is an inter net and intranet to help with this. There is Coffee with the President and opportunities to talk with CEO and executive team members such as when they do walkabouts. Relationship between the community and organization There were 13 people who contributed to the Community Partners discussion. They stated that they were pleased with their partnership with this organization and its members. They stated that even though they were the largest partner they acted as an equal partner. Integration has occurred successfully in several departments such as Pharmacy and Diagnostic Imaging across several hospital sites and the partners want these types of activities to continue. The partners believe that the organization seeks to have a seamless system for patients. They are seen as open and innovative. The partners asks that the organization put more emphasis on wellness and link this with them. The partners would like more partnering to address co-morbid conditions. One partner suggests that semi annual meetings with the municipalities, mayors and others should occur as they are pertinent issues to discuss. It is important that when input has been requested that the follow up is shared with those who provided input originally.
The communication plan is a flexible document that functions more as a yearly goals and objectives on communication issues. It is adaptable to changing environmental factors. Originally it focused on a worse case scenario for 2010 that fortunately did not materialize. It changed to changing needs. This document is a good plan but may need a underlying template that would function as a plan and then filled in on an ongoing basis. This template could talk about generalized strategies that can be adapted depending on the audience and the unique issues of the various communities.
The support for community advisory committees is very commendable. They function both as a source of information and public sentiment but also as a sounding board for new initiatives or changes in direction. They also allow for different messages with different focuses depending on the unique challenges in each community.
The advocacy of the Board and the CEO in their interaction with the community is noted favourably. This role should be expanded to include senior members of staff who can bring their unique skills into the public discussion. This is especially helpful in preventive health advocacy and responded to external pressures eg. H1N1
The Board is encouraged to expand its disclosure process to include discussion on governance process, decision making and the ethical framework used in decision making. This level of transparency will augment the communities faith in the governance model of public funding organizations.
The cross appointments with the other health and hospital boards is very commendable and is discussed under governance. This unique sharing of governance should be shared with the public to show the value of collaboration and the value of a different set of eyes.
The organization needs to periodically step back and determine the effectiveness of its communication philosophy both with internal and external stakeholders and be willing to adapt to this level of feedback.
The hospital's information management system is unique due to the background of the CIO.Unlike many organizations that are lead by formally trained information specialist, the present CIO has
able to rely on technical specialists when problems are identified and solutions need to be developed. He is able to evaluate the problem in context of the big picture and formulate a direction for the program based on his understanding of processes and the needs of the people in the middle of the process. The end result is a very impressive group of players and a very strong program
The Board will hold in-camera sessions to review the performance review of the Chief of Staff and the CEO and also the audit committee will function in an in-camera perspective. The Board should consider if more frequent or regular in-camera sessions would be of some assistance.
Surveyor Comments
Detailed Accreditation Results 11
evolved from a process management background and a long history with the organization.

Accreditation Report
He is able to rely on technical specialists when problems are identified and solutions need to be developed. He is able to evaluate the problem in context of the big picture and formulate a direction for the program based on his understanding of processes and the needs of the people in the middle of the process. The end result is a very impressive group of players and a very strong program.
The Board will hold in-camera sessions to review the performance review of the Chief of Staff and the CEO and also the audit committee will function in an in-camera perspective. The Board should consider if more frequent or regular in-camera sessions would be of some assistance.
No Unmet Criteria for this Priority Process.
Providing appropriate and safe structures and facilities to successfully carry out the mission, vision, and goals.
Physical Environment
This is a very proactive team that supports 7 sites (including Withdrawal Management Building) encompassing 720,000 sq. ft.
The organization has a formal process to ensure that applicable laws, regulations and codes are met, with the exception of the Markdale Site, which is waiting for MoHLTC approval to rebuild. There is evidence of consideration of staff and patient health and safety during periods of renovation and construction.
Back up systems are in place to reduce the impact of utilities failures.
The organization is involved in energy conservation and recycling activities
Preventive maintenance processes are in place and monitored closely.
Work Orders are generated electronically and turn around times are tracked and trended.
There has been several significant incidents (substation failure, water line break, boiler failures, and fires) that the Engineering Service has dealt with since the last survey which has lead to improvements in preventative maintenance and the acquisition of an infrared camera.
There are significant infrastructure challenges at the Markdale and the Southampton sites, and to the lesser degree at the other Rural sites. The organization is encouraged to continue to advocate for the Capital Projects needed for the Rural Sites (including the building of a new Hospital for Markdale).
Surveyor Comments
Detailed Accreditation Results12

QMENTUM PROGRAM
Criteria Location Priority forAction
Effective Organization
The organization’s physical space meets applicable laws, regulations, and codes.
10.1
Dealing with emergencies and other aspects of public safety.
Emergency Preparedness
The organization has identified potential risks for disasters and emergencies, prepared comprehensive plans, and defined responsibilities and communication plans. It is testing its fire and other emergency preparedness situations regularly and reporting appropriately. There is evidence that appropriate debriefing occurs following a disaster or emergency.
An outbreak protocol is in place. There is a contracted service with UHN for their Infection Control and Prevention expertise.
Of particular importance is the manner in which the Incident Management System is utilized for all of the Contingency Plans.
A detailed Pandemic plan is noted.
There are still hard copies of various Emergency Code Responses from 1992-1994 hanging in the Markdale Ultrasound Area, even though the most current versions are online.
Surveyor Comments
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
Effective Organization
When the organization uses an office in a public building to provide services, the organization’s leaders regularly verify fire safety precautions with the property manager, e.g. lighted exit signs, emergency lighting in stairwells, and regularly maintained fire extinguishers that are centrally located and well-marked.
11.7
Smooth and timely movement of clients and their families through appropriate service and care settings.
Patient Flow
Detailed Accreditation Results 13
The table below indicates the specific criteria that require attention, based on the accreditation review.

Accreditation Report
There is a very open and flexible system for booking diagnostic US, CT and MRI. The request is reviewed by the radiologist and a time is allotted based on the MD's indication of urgency. If the MD feels the test should be booked earlier, the MD can talk to the radiologist and negotiate an appropriate time. If the radiologist or even the technologist feels that an alternative test is more appropriate, the referring MD is contacted and a discussion occurs on the most appropriate test. At times a US is as effective as a CT or the wait for an US is too long and a MRI is quicker. The initial booking is returned to the MD quickly with the appointment and not delayed for weeks prior to informing the referring MD.
Urgent testing is available but if it can be deferred from nightime to the next AM, this will occur with CT and US as long as the referring physician agrees. This allows for a quick production of a written report. It was noted that the turn around time from procedure to written report is extremely short.
There are formal policies in place on managing overcrowding especially in the Emergency Department. In general, the department has the ability to find more space, find more doctors and nurses and increase its ability to admit to the inpatient beds. Diverting ambulances is not an option but decanting appropriate inpatients to the smaller hospitals can allow the Owen Sound site to increase its inpatient capacity.
There are department bullet rounds that allows the coordinator to fully understand the bed utilization challenges. This information is shared with a general bed meeting with the Admitting Department leading and having access to small hospital census information. This allows the various department to coordinate movement of patients and anticipate elective patient movement. In the reverse, each of the small hospitals is given bed availability of the various wards at Owen Sound and this is posted on the in-patient unit and will help guide transfer or potential repatriation of patients.
There is a formal process on utilization of surgical time. This involves block booking of patients for specific surgeons and a commitment that the block will be used 14 days prior and fully used 7 days prior. If this does not occur, the space will be offered to other surgeons of the same sub speciality and if still not utilized, available to all surgeons.
No Unmet Criteria for this Priority Process.
Machinery and technologies designed to aid in the diagnosis and treatment of healthcare problems.
Medical Devices and Equipment
The staff and its leadership have an unrelenting focus on trying to meet and exceed standards in this area. The team regularly scans the environment for standards that impact their operations Ie. CSA, Health & Welfare Canada/FDA, Accreditation Canada, Device guidelines, Association for the Advancement of Medical Instrumentation etc. The installation of a steam filtration system is an example where Grey Bruce has demonstrated it is ahead of the curve in meeting standards.
There is evidence that there is a strong program for both Preventative as well as Corrective Maintenance at Grey Bruce on equipment and medical devices. Examples were found that in some cases preventative maintenance processes exceed what is required by various standard setting groups Ie. In Owen Sound, new state of the art steam filtration system for the two vac sterilizers was installed, a proactive approach in advance of this being a required standard.
Corporate wide cleaning product improvement for detergents, enzymatic and instrument milk used in washer/disinfectors and sinks which has increased the efficacy rate and effectiveness in pathogen removal.
Design and introduction of a custom orthopaedic transport cart for the effective and save movement of all knee and hip instrumentation (Owen Sound).
In Markdale the design and outfit of a new decontamination area, given physical plant challenges at the site.
Virtually all of the SPD function has been centralized to the central SPD function at Owen Sound in a physical space that has been laid out to ensure that there is a barrier between the contaminated area to clean to sterility to high level clean storage. All areas have separate monitoring for temperature, humidity, ventilation and negative or positive air exchange depending on the area.
A variance reporting process has been established between the OR/SPD. The audit process allows real time corrective action to take place. Data from the variance reports is discussed at the OR/ SPD Sterilization Committee whose mission is to promote improvements and ensure standards compliance.
Staff are well trained; 100% have certification in Sterilization and Reprocessing as well as regular in servicing on endoscopy sterilization and infection prevention and control measures specific to their areas of responsibility.
Cystoscopy cleaning and sterilization is taking place in Ambulatory Care in Owen Sound and endoscopy reprocessing is taking place at rural sites. The space conditions for this cleaning is not ideal as clean and dirty are in the same physical space. Practical strategies have been put in place to ensure a separation of activity from clean and dirty. Trained SPD staff are the only personnel who handle the reprocessing of the equipment and ensure that it passes the various checkpoints for sterility. This situation needs to be constantly monitored, managed and factored into any future space planning.
A good evergreen strategy has been in place for some time. Major equipment has been replaced when it has reached end of life. The Cart Washer is now the only piece of original equipment in the SPD and as resources are available consideration needs to be given to planning for its replacement.
An instrument tracking system as well as the capacity to have computerized SOP's (standardized operating procedures) ideally projected on flat screens would enhance the work of the department. The latter would make document control less labour intensive and efficient.
As part of the roaming endocopy initiative, it is suggested that the temperature/humidity of the transport vehicle be monitored.
It is suggested that the team consider establishing a hand hygiene champion for the area that can help reinforce infection prevention and control practices as well as support the completion of regular on the spot hand hygiene audits that can be shared with staff in real time.
The separation of clean and dirty in a number of locations at the Southampton site needs to be high on the radar screen. The areas in question are known by the leadership.
Surveyor Comments
Detailed Accreditation Results14
There is a very open and flexible system for booking diagnostic US, CT and MRI. The request is reviewed by the radiologist and a time is allotted based on the MD's indication of urgency. If the MD feels the test should be booked earlier, the MD can talk to the radiologist and negotiate an appropriate time. If the radiologist or even the technologist feels that an alternative test is more appropriate, the referring MD is contacted and a discussion occurs on the most appropriate test. At times a US is as effective as a CT or the wait for an US is too long and a MRI is quicker. The initial booking is returned to the MD quickly with the appointment and not delayed for weeks prior to informing the referring MD.
Urgent testing is available but if it can be deferred from nightime to the next AM, this will occur with CT and US as long as the referring physician agrees. This allows for a quick production of a written report. It was noted that the turn around time from procedure to written report is extremely short.
There are formal policies in place on managing overcrowding especially in the Emergency Department. In general, the department has the ability to find more space, find more doctors and nurses and increase its ability to admit to the inpatient beds. Diverting ambulances is not an option but decanting appropriate inpatients to the smaller hospitals can allow the Owen Sound site to increase its inpatient capacity.
There are department bullet rounds that allows the coordinator to fully understand the bed utilization challenges. This information is shared with a general bed meeting with the Admitting Department leading and having access to small hospital census information. This allows the various department to coordinate movement of patients and anticipate elective patient movement. In the reverse, each of the small hospitals is given bed availability of the various wards at Owen Sound and this is posted on the in-patient unit and will help guide transfer or potential repatriation of patients.
There is a formal process on utilization of surgical time. This involves block booking of patients for specific surgeons and a commitment that the block will be used 14 days prior and fully used 7 days prior. If this does not occur, the space will be offered to other surgeons of the same sub speciality and if still not utilized, available to all surgeons.
Surveyor Comments

QMENTUM PROGRAM
Corporate wide cleaning product improvement for detergents, enzymatic and instrument milk used in washer/disinfectors and sinks which has increased the efficacy rate and effectiveness in pathogen removal.
Design and introduction of a custom orthopaedic transport cart for the effective and save movement of all knee and hip instrumentation (Owen Sound).
In Markdale the design and outfit of a new decontamination area, given physical plant challenges at the site.
Virtually all of the SPD function has been centralized to the central SPD function at Owen Sound in a physical space that has been laid out to ensure that there is a barrier between the contaminated area to clean to sterility to high level clean storage. All areas have separate monitoring for temperature, humidity, ventilation and negative or positive air exchange depending on the area.
A variance reporting process has been established between the OR/SPD. The audit process allows real time corrective action to take place. Data from the variance reports is discussed at the OR/ SPD Sterilization Committee whose mission is to promote improvements and ensure standards compliance.
Staff are well trained; 100% have certification in Sterilization and Reprocessing as well as regular in servicing on endoscopy sterilization and infection prevention and control measures specific to their areas of responsibility.
Cystoscopy cleaning and sterilization is taking place in Ambulatory Care in Owen Sound and endoscopy reprocessing is taking place at rural sites. The space conditions for this cleaning is not ideal as clean and dirty are in the same physical space. Practical strategies have been put in place to ensure a separation of activity from clean and dirty. Trained SPD staff are the only personnel who handle the reprocessing of the equipment and ensure that it passes the various checkpoints for sterility. This situation needs to be constantly monitored, managed and factored into any future space planning.
A good evergreen strategy has been in place for some time. Major equipment has been replaced when it has reached end of life. The Cart Washer is now the only piece of original equipment in the SPD and as resources are available consideration needs to be given to planning for its replacement.
An instrument tracking system as well as the capacity to have computerized SOP's (standardized operating procedures) ideally projected on flat screens would enhance the work of the department. The latter would make document control less labour intensive and efficient.
As part of the roaming endocopy initiative, it is suggested that the temperature/humidity of the transport vehicle be monitored.
It is suggested that the team consider establishing a hand hygiene champion for the area that can help reinforce infection prevention and control practices as well as support the completion of regular on the spot hand hygiene audits that can be shared with staff in real time.
The separation of clean and dirty in a number of locations at the Southampton site needs to be high on the radar screen. The areas in question are known by the leadership.
Detailed Accreditation Results 15

Accreditation Report
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
Reprocessing and Sterilization of Reusable Medical Devices
The team works with others in the organization to limit the use of flash sterilization to emergencies only, and never for complete sets or implantable devices.
1.3
Where reprocessing and sterilization services are contracted to external providers, the organization annually reviews each contract and records all aspects of the contract and negotiations in its files.
1.9
This part of the report provides information on the delivery of high quality, safe services. Some specific areas that are evaluated include: the episode of care, medication management, infection control, and medical devices and equipment.
Findings
Direct Service Provision
Following the survey, once the organization has the opportunity to address the unresolved criteria and provide evidence of action taken, the results will be updated to show that they have been addressed.
Ambulatory Care Services
Providing leadership and overall goals and direction to the team of people providing services.
Clinical Leadership
Experienced and well trained staff work in the ambulatory care program.
Instruments requiring sterilization have been centralized in SPD. Cystoscopy reprocessing takes place in Ambulatory care. Only trained SPD personnel undertake the cleaning and sterilizing of the scopes in ambulatory care and undertake their activities in a manner that clean and dirty are separated within the same geographic space. This situation needs to be under constant review to ensure performance levels for clean and sterile are maintained. Future space planning for ambulatory care should factor in how scopes are to be processed.
An internal review of the service has been started and some benchmarking work has been undertaken. Although there is a formal structure established called the Ambulatory Care Utilization Committee. It has not formally met for some time. There is an opportunity for both clinical and medical leadership within the program to meet to review the data that has been obtained to date and what other information may be required to help inform planning and decision making around what the kind and scope of service will be provided on a go forward basis particularly as there will be a need to align with the new strategic plan that the Board is spearheading.
A formal and regular review of Ambulatory care time utilization should be considered in light of ongoing requests for this resource, the need to maximize productivity and also support physician recruitment and retention. Benchmarking with other hospitals and reviewing best practices around ambulatory care programming may be helpful to the program.
Surveyor Comments
Detailed Accreditation Results16
particularly as there will be a need to align with the new strategic plan that the Board is spearheading.

QMENTUM PROGRAM
A formal and regular review of Ambulatory care time utilization should be considered in light of ongoing requests for this resource, the need to maximize productivity and also support physician recruitment and retention. Benchmarking with other hospitals and reviewing best practices around ambulatory care programming may be helpful to the program.
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
The team collects information about its clients and the community.
1.1
The team uses the information it collects about clients and the community to define the scope of its services and set priorities when multiple service needs are identified.
1.2
The team works together to develop goals and objectives. 2.1
The team’s goals and objectives for ambulatory care services are measurable and specific.
2.2
The team has an equipment log in which to record maintenance and downtime, and to identify problems.
13.2
Developing a highly competent interdisciplinary team with the knowledge, skills and abilities to develop, manage, and deliver effective and efficient programs, services, and care.
Competency
Performance appraisals of staff are up to date.
There is a good orientation program for new staff and access to in services for those staff who work in the area.
Staffing assignments are well coordinated.
Trained SPD staff are responsible for the cleaning and sterilization of the cystocopes that are located and used in the Ambulatory Care unit and for the ambulatory care services at the rural sites.
Inservicing on how the ROP's apply to the Ambulatory Care Unit would be helpful to the staff and serve as an ongoing reinforcement of these practices especially medication reconciliation and transfer of information.
Surveyor Comments
Detailed Accreditation Results 17
Accreditation Report
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
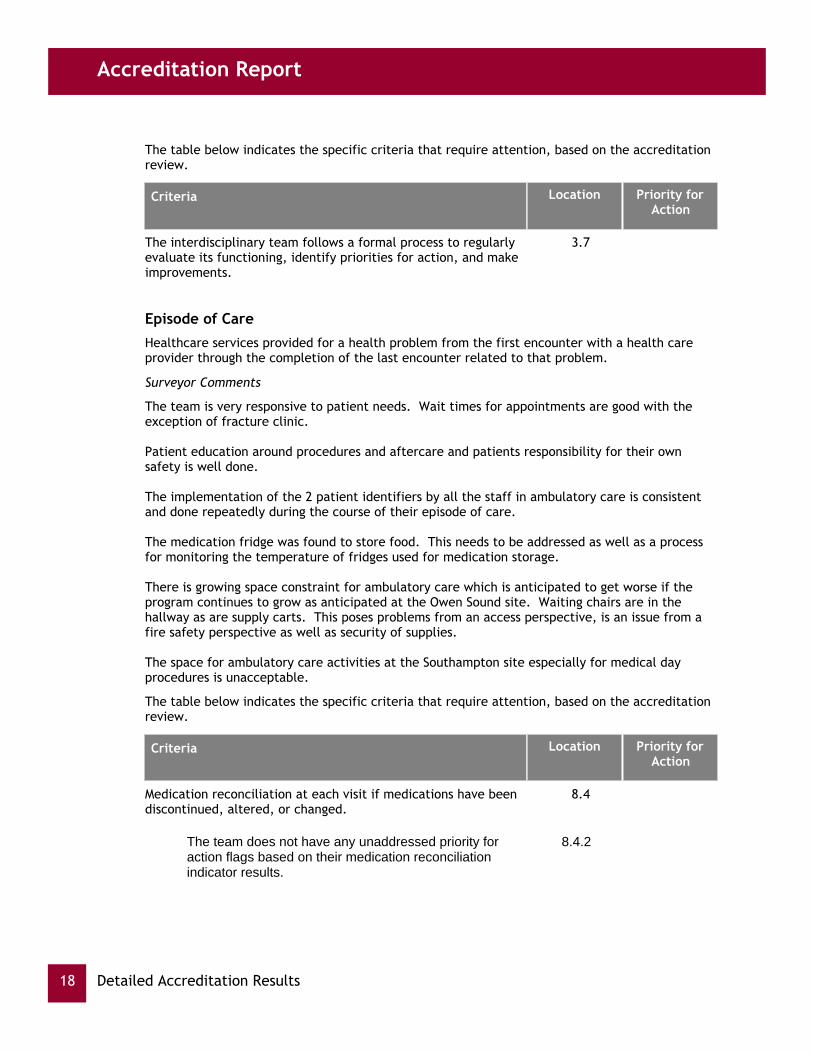
The interdisciplinary team follows a formal process to regularly evaluate its functioning, identify priorities for action, and make improvements.
3.7
Healthcare services provided for a health problem from the first encounter with a health care provider through the completion of the last encounter related to that problem.
Episode of Care
The team is very responsive to patient needs. Wait times for appointments are good with the exception of fracture clinic.
Patient education around procedures and aftercare and patients responsibility for their own safety is well done.
The implementation of the 2 patient identifiers by all the staff in ambulatory care is consistent and done repeatedly during the course of their episode of care.
The medication fridge was found to store food. This needs to be addressed as well as a process for monitoring the temperature of fridges used for medication storage.
There is growing space constraint for ambulatory care which is anticipated to get worse if the program continues to grow as anticipated at the Owen Sound site. Waiting chairs are in the hallway as are supply carts. This poses problems from an access perspective, is an issue from a fire safety perspective as well as security of supplies.
The space for ambulatory care activities at the Southampton site especially for medical day procedures is unacceptable.
Surveyor Comments
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
Medication reconciliation at each visit if medications have been discontinued, altered, or changed.
8.4
The team does not have any unaddressed priority for action flags based on their medication reconciliation indicator results.
8.4.2
Detailed Accreditation Results18

QMENTUM PROGRAM
The team follows the organization’s process to identify, address, and record all ethics-related issues.
9.8
The team reconciles medications with the client at referral or transfer, and communicates information about the client’s medications to the next provider of service at referral or transfer to another setting, service, service provider, or level of care within or outside the organization.
12.2
There is a demonstrated, formal process to reconcile client medications at referral or transfer.
12.2.1
The process includes generating a comprehensive list of all medications the client has been taking prior to referral or transfer.
12.2.2
The process includes a timely comparison of the prior-to-referral or prior-to-transfer medication list with the list of new medications ordered at referral or transfer.
12.2.3
The process requires documentation that the two lists have been compared; differences have been identified, discussed, and resolved; and appropriate modifications to the new medications have been made.
12.2.4
The process makes it clear that medication reconciliation is a shared responsibility involving the client, nursing staff, medical staff and pharmacists, as appropriate.
12.2.5
The organization has a documented plan to implement throughout the organization, and before the next accreditation survey, a medication reconciliation process at referral and transfer.
12.2.6
Information, research and evidence, data, and technologies that support and facilitate management and clinical decision-making.
Decision Support
Clinicians use contemporary guidelines to guide their practice. Input is sought from the key stakeholders in providing practice guidelines for various procedures.
Surveyor Comments
No Unmet Criteria for this Priority Process.
The identification and monitoring of process and outcome measures to evaluate and improve the quality of services to clients and the impact on client outcomes.
Impact on Outcomes
Despite limitations in the physical plants at the sites providing ambulatory care, the actual care delivered to patients is solid and patients are satisfied with the outcomes as well as the customer service they receive.
done in the Ambulatory Care area. Logs are maintained of the reprocessing activity and a mechanism to track for recall purposes should that be required is in place.
The new Patient identification system that has been introduced is in evidence at numerous contact points by staff who interact with the patient.
There is good understanding of the processes that need to be undertaken when there is an adverse event and the processes around disclosure.
There is good patient satisfaction with the service provided and good follow up arrangements are made if required with other providers.
Service planning is not formalized at the departmental level. Benchmarking and use of evidence based data are at the beginning stages of being utilized to look at service planning. Leadership in the area acknowledge that goal setting, planning and evaluation of the service is reactive rather than proactive and systematic. Further, in service planning physicians and physician leadership need to be actively engaged in the process. New clinics are in the process of being introduced Ie. Cardiology clinic and potentially additional clinics to support Oncology, Orthopaedics and Rheumatology. The team needs to look at a structure where utilization of clinic resources is monitored, adjusted/ reallocated based on the corporate clinical priorities identified by the organization and within its available financial envelope.
The program at Owen Sound is becoming space constrained and the physical layout from a patient flow perspective is not ideal Patient privacy and confidentiality will need to be on the program's radar screen in the registration and waiting area as the program's volumes continue to grow. As well, storage space for equipment and supplies has been taken over by other functions leaving supply carts in the corridors. This is not only posses an access barrier but also leaves supplies open to theft. The situation in Southampton is of concern and of higher urgency to address.
Storage and handling of medications requires review. It was observed that the medication fridge contained medications and food and there was no temperature monitor or logging of the temperature. The locked cupboard where medications are stored needs to be reviewed to ensure only appropriate inventory is stored in that location.
Surveyor Comments
Detailed Accreditation Results 19

Accreditation Report
A SPD staff member is assigned to do the scope cleaning, disinfecting and sterilization that is done in the Ambulatory Care area. Logs are maintained of the reprocessing activity and a mechanism to track for recall purposes should that be required is in place.
The new Patient identification system that has been introduced is in evidence at numerous contact points by staff who interact with the patient.
There is good understanding of the processes that need to be undertaken when there is an adverse event and the processes around disclosure.
There is good patient satisfaction with the service provided and good follow up arrangements are made if required with other providers.
Service planning is not formalized at the departmental level. Benchmarking and use of evidence based data are at the beginning stages of being utilized to look at service planning. Leadership in the area acknowledge that goal setting, planning and evaluation of the service is reactive rather than proactive and systematic. Further, in service planning physicians and physician leadership need to be actively engaged in the process. New clinics are in the process of being introduced Ie. Cardiology clinic and potentially additional clinics to support Oncology, Orthopaedics and Rheumatology. The team needs to look at a structure where utilization of clinic resources is monitored, adjusted/ reallocated based on the corporate clinical priorities identified by the organization and within its available financial envelope.
The program at Owen Sound is becoming space constrained and the physical layout from a patient flow perspective is not ideal Patient privacy and confidentiality will need to be on the program's radar screen in the registration and waiting area as the program's volumes continue to grow. As well, storage space for equipment and supplies has been taken over by other functions leaving supply carts in the corridors. This is not only posses an access barrier but also leaves supplies open to theft. The situation in Southampton is of concern and of higher urgency to address.
Storage and handling of medications requires review. It was observed that the medication fridge contained medications and food and there was no temperature monitor or logging of the temperature. The locked cupboard where medications are stored needs to be reviewed to ensure only appropriate inventory is stored in that location.
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
The team shares benchmark and best practice information with its partners and other organizations.
16.5
The team identifies and monitors process and outcome measures for its ambulatory care services.
18.1
The team compares its results with other similar interventions, programs, or organizations.
18.3
Detailed Accreditation Results20

QMENTUM PROGRAM
The team shares evaluation results with staff, clients, and families.
18.5
Cancer Care and Oncology Services
Providing leadership and overall goals and direction to the team of people providing services.
Clinical Leadership
Clinical leadership is knowledgeable and committed and has good working relationships with London Health Sciences and CCO.
There is good physician support and coverage for the program from both the oncologists and hosptialists.
Strong community partnerships and support for the cancer program is in evidence.
Surveyor Comments
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
The team works together to develop goals and objectives. 2.1
The team’s goals and objectives for its cancer care and oncology services are clearly written, measurable, and directly linked to the organization’s strategic direction.
2.2
Developing a highly competent interdisciplinary team with the knowledge, skills and abilities to develop, manage, and deliver effective and efficient programs, services, and care.
Competency
All staff have specialized training and certification in oncology. Educational opportunities to maintain currency on oncology topics are available and are accessed by personnel.
The interdisciplinary team is cohesive, knowledgeable, experienced and responsive to individual client situations.
There is good case coordination for client care that also assists with the management of workload for the providers.
Surveyor Comments
The table below indicates the specific criteria that require attention, based on the accreditation review.
Detailed Accreditation Results 21

Accreditation Report
Criteria Location Priority forAction
The interdisciplinary team follows a formal process to regularly evaluate its functioning, identify priorities for action, and make improvements.
3.8
Healthcare services provided for a health problem from the first encounter with a health care provider through the completion of the last encounter related to that problem.
Episode of Care
The Oncology Patient Electronic referral to Home Care for newly diagnosed patients has been in place for about a year. Anecdotally, this practice which provides CCAC with a heads up on Oncology referrals so that they can mobilize their resources and establish a provider relationship with newly diagnosed cancer patients is noteworthy. It is anticipated that once this practice has been evaluated, metrics around process and outcomes indicators will demonstrate a positive impact.
There is evidence of a client centred and service excellence to care delivery by the team.
Patient education and involvement in the care process is noteworthy.
Improvements have been made to the distribution of cytotoxic medication to the clinic since the last survey. Pharmacy prepares the medication for administration in the main pharmacy and transports the product in a closed plastic container to the clinic so as to prevent any potential spillage or contamination.
There is a good process in place to handle patients presenting with febrile neutropenia.
The medication fridge needs to be monitored to ensure that the temperature is appropriate for the storage of chemotherapeutic medications. It was noted that the freezer section was frosted over and as such could potentially impact the stability/integrity of the medication products contained in the fridge.
The Cancer program is projected to expand; the volume of cases is increasing, there is no storage space for equipment or supplies necessitating they be kept in open corridors which creates other problems. Work space for the interdisciplinary team supporting the patients is limited. It is suggested that reviewing the space requirements for the program needs to be revisited.
Although there are many informal means of providing feedback to the staff of the Cancer program on how patients do when they transition to different providers there is no formal mechanism for evaluating the effectiveness of the transition for service planning or end of service planning. It is suggested that a formal evaluation and feedback mechanisms be developed to help inform transition planning.
The team make a point of having focused ethical discussions Ie. 3rd party payment for certain drug regimens etc. so that practice, policy and positions are well informed by open debate on these issues.
The team needs to continue to evolve its medication reconciliation practices.
Surveyor Comments
Detailed Accreditation Results22
these issues.

QMENTUM PROGRAM
The team needs to continue to evolve its medication reconciliation practices.
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
Medication Reconciliation at Admission 7.6
The team does not have any unaddressed priority for action flags based on their medication reconciliation at admission indicator results.
7.6.2
Information, research and evidence, data, and technologies that support and facilitate management and clinical decision-making.
Decision Support
Chemotherapy protocols are adhered to and are largely centrally dictated by Cancer Care Ontario and specifically London Health Sciences with whom the Grey Bruce program is affiliated.
There is good understanding of the protocols that are being used for the chemotherapy population.
Surveyor Comments
No Unmet Criteria for this Priority Process.
The identification and monitoring of process and outcome measures to evaluate and improve the quality of services to clients and the impact on client outcomes.
Impact on Outcomes
Staff are knowledgeable about sentinel and adverse events as well as the disclosure policy.
The team has a number of ways of monitoring clients and families perspectives on the quality of its cancer care and oncology service Ie. verbal feedback from families and patients, thank you notes etc. This is an area that the team should consider more formal and regular mechanisms of soliciting feedback.
Surveyor Comments
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
The team shares evaluation results with staff, clients, and families.
16.5
Detailed Accreditation Results 23

Accreditation Report
Critical Care
Providing leadership and overall goals and direction to the team of people providing services.
Clinical Leadership
The organization is well aware of its population that is getting older, more complex and in greater need of cardiac and respiratory care.This has resulted in a separation of services offered. There is a level 2 facility with 6 beds to provide cardiac monitoring and another level 3 ICU to handle serious, complex cases that may include ventilated patients. This is consistent with corporate and LHIN goals and has helped the internists focus the coverage as needed. There is a now a core of intensivists that cover the ICU and the monitored beds that are available to all the internists.
The Hospital should be commended by being creative in the selection of the unit manager. Often a senior nurse is selected but in this case, the most suitable candidate was a Respiratory Therapist and she appears to be doing a very good job.
Surveyor Comments
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
The team works together to develop goals and objectives. 2.1
The team’s goals and objectives for its critical care services are measurable and specific.
2.2
Developing a highly competent interdisciplinary team with the knowledge, skills and abilities to develop, manage, and deliver effective and efficient programs, services, and care.
Competency
The staff appear to be well trained and well supported. There are minimum educational criteria for both Level 2 and Level 3 services. Staff have been given various education opportunities and the option of providing mentoring support to students.
Daily rounds occur between the intensivist, the nursing staff, the coordinator or manager, social worker, RT and the resident NP. The latter has evolved an unique role of providing continuity for families and ongoing support and advocacy.
Surveyor Comments
No Unmet Criteria for this Priority Process.
Healthcare services provided for a health problem from the first encounter with a health care provider through the completion of the last encounter related to that problem.
Episode of Care
Detailed Accreditation Results24

QMENTUM PROGRAM
The Critical Care program has developed a two stream approach to delivery of care. The Level 2 Cardiac Monitoring Centre allows all the internists to participate in the care and monitoring of stable cardiac patients. The Level 3 ICU is supported by a core of talented specialists who function as intensivists. This group includes a surgeon, some anaesthetists and some of the internists. They have developed a creative schedule that allows for ongoing care on a weekly basis and support at night for new admissions.
The morning rounds bring together all the direct and indirect care givers to review the status, prognosis and plans for all the ICU patients. It is noted that one of the team members includes a nurse practitioner who adds continuity to the ongoing care of patients on longer term ventilators.
The team has developed a very good working relationship with St. Mary's for cardiac problems and London for complex surgical issues and this allows for rapid transfer to these sites.
Staff appear well supported and able to advocate for their patients. They find that they have a receptive ear in management. Collectively this supports a good working environment. The need to stay current and maintain competency is supported and encouraged by the team.
Overall, it appears to be a very impressive service.
Surveyor Comments
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
During the assessment, the team determines whether the client has an advance directive and records this in the client record.
7.3
Medication Reconciliation at Admission 7.7
The team meets Accreditation Canada’s recommended target for medication reconciliation at admission.
7.7.2
When clients are incapable of giving informed consent, the team refers to the client’s advance directives if available or obtains consent using a substitute decision maker.
9.7
The team reconciles medications with the client at referral or transfer, and communicates information about the client’s medications to the next provider of service at referral or transfer to another setting, service, service provider, or level of care within or outside the organization.
12.5
There is a demonstrated, formal process to reconcile client medications at referral or transfer.
12.5.1
The process includes a timely comparison of the prior-to-referral or prior-to-transfer medication list with the list of new medications ordered at referral or transfer.
12.5.3
Detailed Accreditation Results 25

Accreditation Report
The process requires documentation that the two lists have been compared; differences have been identified, discussed, and resolved; and appropriate modifications to the new medications have been made.
12.5.4
The process makes it clear that medication reconciliation is a shared responsibility involving the client, nursing staff, medical staff and pharmacists, as appropriate.
12.5.5
Information, research and evidence, data, and technologies that support and facilitate management and clinical decision-making.
Decision Support
No specific comments.
Surveyor Comments
No Unmet Criteria for this Priority Process.
The identification and monitoring of process and outcome measures to evaluate and improve the quality of services to clients and the impact on client outcomes.
Impact on Outcomes
No specific comment.
Surveyor Comments
No Unmet Criteria for this Priority Process.
Diagnostic Imaging Services
The identification and monitoring of process and outcome measures to evaluate and improve the quality of services to clients and the impact on client outcomes.
Impact on Outcomes
here is standard work done on the same or similar equipment throughout the sites, minimizing the risk for error while facilitating the moving of staff from one area to another as need arises.
The DI leadership team collects and reviews wait times on a weekly basis and service volumes on a monthly basis. CT and MRI wait times are tracked through the WTIS strategy. Currently the wait times for all modalities are below the Provincial averages.
The Team widely surveys the patients at all sites to ensure it is meeting the needs of the communities.
Risk Monitor Pro is utilized and widely known throughout the sites.
There was no evidence at any of the DI sites that information was given to patients in writing with regard to their role in promoting safety. DI Brochures were developed several years ago, but appear to have not been utilized of late.
Surveyor Comments
Detailed Accreditation Results26

QMENTUM PROGRAM
No Unmet Criteria for this Priority Process.
Availability of diagnostic imaging to provide health care practitioners with information about the presence, severity, and causes of health problems, and the procedures and processes used by these services.
Diagnostic Services - Diagnostic Imaging
The team has embarked on a very creative "Survivor" journey to prepare for accreditation. In addition, they have created a very detailed reference binder.
There is central booking for all DI procedures for all sites. Patients are given the opportunity to have their diagnostics performed closer to home, or within a shorter timeframe at another site.
The PACS system is fully implemented in all of the sites. There are very quick turnaround times for results (sometimes before the patient is returned back to the ER).
The organization has formed partnerships with the various educational facilities to ensure that the traditionally hard to recruit health care providers in the DI area are doing placements at the sites. This has resulted in no Human Resource shortages for DI, including Radiologists.
There is standard work and standard equipment for all of the DI areas throughout the Corporation, enabling staff to fill in for vacancies/sick calls seamlessly.
There is a very collaborative relationship between the Radiologists and Staff.
The Organization is encouraged to advocate for resources for digital Mammography as the fumes from the processor in the Mammography area are quite noticeable.
Surveyor Comments
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
All DI reprocessing areas are physically separate from client care areas.
7.5
All DI reprocessing areas are equipped with separate clean and decontamination work areas as well as separate storage, dedicated plumbing and drains, and proper air ventilation.
7.6
The staff member soaks, flushes, and cleans each DI device or piece of equipment in a timely way to remove inorganic and organic matter retained on the device.
7.9
Detailed Accreditation Results 27

Accreditation Report
The team informs and educates its clients and families in writing and verbally about the client and family’s role in promoting safety.
14.6
Written and verbal information is provided to clients and families about their role in promoting safety.
14.6.1
Staff uses written and verbal approaches to inform and educate clients about their role in promoting safety.
14.6.2
Clients indicate that they have received written and verbal communication about their role in promoting safety.
14.6.3
Emergency Department
Providing leadership and overall goals and direction to the team of people providing services.
Clinical Leadership
Thre is evidence of strong collaboration between the ER in Owen Sound and the local EMS services. This collaboration extends to include the Mental Health crisis team and the hospital based CCAC staff. Consideration was given for a GEM nurse and an ER based CCAC but the business case did not justify their inclusion in the ER.
The team and manager is well aware of the population is serves and the changing realities of age, economic instability and increasing co-morbidities. In response to external factors, they will often meet with police, fire and EMS to plan a response to an upcoming event such as a community concert in the summer time. Additional staff, availability of fluids and an awareness of possible drug reactions was discussed and prepared prior to the concert.
The ER department has recognized some challenges that it has with the wait times for CTAS 4 and 5 patients. It is about to explore via Kiazen events some modifications to its physical plant to allow for a fast tract or a see and treat environment that is more suitable for these types of patients. To help support this new model, it has embarked on the incorporation of physician assistants within the department. All these initiatives are creative approaches to help address this ongoing concern.
There is an excellent system in place to track patients within the department. It clearly outlines, bed availability, time within the department, lab and DI testing and when the results are available and plans for future management. There is also a clock system that becomes activated if the patients stays longer than provincial standards. An excellent use of the tracking system is an extra monitor that sits in the Manager's office and allows her to monitor ER volumes from her office.
There is a clear process on how to screen and identify patients with potential infectious diseases.
Consider reviewing the ambulatory care space at Southampton. Patients receive medical outpatient treatments Ie. blood transfusions in a lazy boy chair in a hallway close to the ER. The location of the chair blocks access to a fire extinguisher.
Grey Bruce leadership is aware of the situation and are doing what they can to manage the risks associated with providing care in such an environment.
Detailed Accreditation Results28
Surveyor Comments

QMENTUM PROGRAM
The leadership is encouraged to continue their efforts to work with the LHIN and MOHLTC to provide a longer term solution to the physical plant deficiencies. The leadership is also challenged to see what other creative alternatives can be developed to address the current state.
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
The team works together to develop goals and objectives. 2.1
The team’s goals and objectives are linked to benchmarking of bed availability in the Emergency Department, time to admission, client diversion to other facilities, and wait times.
2.2
The team has the workspace needed to deliver effective services in the Emergency Department.
2.8
Developing a highly competent interdisciplinary team with the knowledge, skills and abilities to develop, manage, and deliver effective and efficient programs, services, and care.
Competency
New staff has an orientation process on best to prepare them for the new work environment. Each of the locum physicians are given specific instruction on use of computer systems and utilization of the tracking system.
The organization has fully implemented a formal workplace violence program. The use of patient ALERTS at the time of triage; the willingness to call security and the willingness to trigger CODE WHITE appears to be working very well. There is adequate backups in place to call back up staff in setting where one triage nurse or one receptionist are alone with the patient.
There is a strong focus on supporting the educational needs of staff. Many of the required certifications are provided in house such as PALS, ACLS. There are also experience requirements for staff to fill certain roles such as the triage nurse.
There are formal processes in place to help the department respond to the high volume and surges in the ER. Extra staff can be accessed, extra spaces on the in-patient floor can be obtained and the ER physicians are potentially available 4 hours prior and 4 hours after their shifts.
Surveyor Comments
No Unmet Criteria for this Priority Process.
Healthcare services provided for a health problem from the first encounter with a health care provider through the completion of the last encounter related to that problem.
Episode of Care
Detailed Accreditation Results 29

Accreditation Report
The service is designed around a 24/7 model but has additional capacity during higher volume times. There is 32 hours a day of MD coverage. The triage RN service is available from 7 to 11 and triggered by receptionist during the night time hours. The triage nurse can be increased to two RNs if higher volume settings.
Since the door covering has been removed from the Ambulance entrance, there is no easy way to distinguish between the ambulance and the walking entrance. This has been recognized and signage is being developed to add clarity.
Ambulance off load time is almost non existence as the process allows for almost immediate placement and transfer of care to the hospital. It is monitored intermittently and times are always reasonable. In light of this, no change of practice has been initiated and is not planned. The EMS is very good in warning the hospital of incoming patients and their needs. If a CTAS 1 or 2 patient is coming in, the nurse is already setting up and the MD is alerted to the incoming patient prior to the patient arriving. This allows for urgent placement and only one transfer from EMS stretcher to the ER stretcher.
Monitoring of wait times for various CTAS classifications is ongoing and judged against LHIN and Provincial benchmarks as the organization is involved in the ER Pay for Performance initiative. Generally standards are very good except for the CTAS 4s and 5s. In light of these challenges, a number of initiatives are being explored and initiated.
The triaging process is very complete. The patient is quickly identified and checked against the hospital data base. If previously seen, important demographics including ALERTS pop up. A screen for febrile illness is done prior to evaluating the needs of the patients. A base set of vitals occurs at this stage and the collection of a Best Possible Medication is collected by the triage nurse. If needed, she will contact the community pharmacy. Then depending on need, the triage nurse will place the patient in an empty room (by using the patient tracker) and tell the primary nurse or place the patient in the waiting room. This process has the ability to have two triage nurses and this is triggered by the first triage nurse. The triage nurse is experienced with minimum years of experience to fulfil the role.
If the triage nurse identifies abnormal vitals, these are posted and high lighted on the patient tracker and this will trigger the primary nurse to repeat and monitor these vitals. This helps the primary nurse monitor changes or progression of the illness. If changes, this will trigger a revaluation of the CTAS scoring and engage the MD sooner.
The Best Possible Medication List is generated by the triage nurse using all relevant sources. This information is on the patient's chart including the drug allergies. This list is referred to by the MD during the patient's stay in the ER. If the decision to admit is made and the patient is being admitted by the ER doctor or the specialist. The BPMH sheet allows for the MD to order, discontinue or hold any of the medication on the list and add new meds. This sheet is signed by the MD and becomes a medication order that is shared with pharmacy. This process appears to be working well and is closely monitored by the department and organization.,
Lab services function well as a 24/7 service. DI is also functioning well as CT and basic radiology is available 24/7 and access to radiologist after hours is functioning well with the contracting out of this service to a radiologist in Austria for evenings and weekends.It was noted that one of the patients involved in a tracer had the CXR at 1330 and a typed report in the PACS system by 1415... very commendable. ER Doctors generally record their interpretations on the PACS system and any discrepancies are identified and it is the responsibility of the next day's MD to review and respond to the situation.
It should be noted favourably, they have in Owen Sound and high risk follow up system in place. If the MD or the RN is concerned, the patient or family is called the next day by the RN staff to inquire on their health status. This is very much appreciated by the families.
Issues with informed consent appear to be managed well and it is clearly the responsibility of the MD to obtain. If the RN feels that the patient does not understand or is potentially incapable, she will contact the MD. The role of the substitute decision maker is clearly outlined
However the use of advanced directives is not going well. The previous model of using the "purple sheet" had been replaced with a community document and it does appear to function well in the emergency department. This issue is identified in other areas of care within the organization and needs to be reviewed. Some areas such as surgery was happy with the new form as it was very clear on DNR status. Obviously this needs further review.
At the time of transfer the ER nurse will contact the inpatient nurse and share the relevant information and especially recent diagnostics, medication or other interventions. The ER nurse will document that the information has been shared,
The observations made in Markdale were very favourable. The staff is very creative in supporting each other .. from the ward clerk who manages patient flow, to the triage nurse and the primary nurse to move seamlessly from patient to patient and the doctor who has a clear understanding of the unique needs of his population. Patients are respected and receive quality care despite the physical space challenges.
Detailed Accreditation Results30
Surveyor Comments

QMENTUM PROGRAM
It should be noted favourably, they have in Owen Sound and high risk follow up system in place. If the MD or the RN is concerned, the patient or family is called the next day by the RN staff to inquire on their health status. This is very much appreciated by the families.
Issues with informed consent appear to be managed well and it is clearly the responsibility of the MD to obtain. If the RN feels that the patient does not understand or is potentially incapable, she will contact the MD. The role of the substitute decision maker is clearly outlined
However the use of advanced directives is not going well. The previous model of using the "purple sheet" had been replaced with a community document and it does appear to function well in the emergency department. This issue is identified in other areas of care within the organization and needs to be reviewed. Some areas such as surgery was happy with the new form as it was very clear on DNR status. Obviously this needs further review.
At the time of transfer the ER nurse will contact the inpatient nurse and share the relevant information and especially recent diagnostics, medication or other interventions. The ER nurse will document that the information has been shared,
The observations made in Markdale were very favourable. The staff is very creative in supporting each other .. from the ward clerk who manages patient flow, to the triage nurse and the primary nurse to move seamlessly from patient to patient and the doctor who has a clear understanding of the unique needs of his population. Patients are respected and receive quality care despite the physical space challenges.
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
Medication reconciliation for clients with a decision to admit. 8.4
The team does not have any unaddressed priority for action flags based on their medication reconciliation indicator results.
8.4.2
During registration, an appropriate team member explains to the client, and family if available, the anticipated sequence of events, locations where services will be provided, and by whom.
10.1
When clients are incapable of giving informed consent, the team refers to the client’s advance directives if available or obtains consent using a substitute decision maker.
10.3
Information, research and evidence, data, and technologies that support and facilitate management and clinical decision-making.
Decision Support
The information collected in the ER is a blend of written documents including MD and primary nurse assessments, triage's Best Possible Medication History, triage assessment, demographics and lab and DI reports. This repository of information is readily available for all care givers and moves with the patient. There is some trailing of expanding the computer generated material as the organization moves towards a paperless solution.
The ER in Wiarton was also reviewed. It obviously has a modern, expansive physical site and follows a similar system to care for their patients as we witnessed in Owen Sound and Markdale. The triage phase includes a two step registration process that involved a private telephone conservation with the receptionist. The nurse triage is a large well equipped site with adequate privacy and protection for the staff. The tracking system exists and supports patient flow. The med cupboard and refrigerator is well secured and appropriately monitored. The department is very well supported by the local family physicians who have a common belief that working in the local ER is part of the mandate of being a rural family MD.
The ER service in Meaford was also reviewed and again, generally running well. It was noted that there was some inconsistent application of the allergy bands for admitted patients. Although the triage area is well identified, there was some concern about the lack of privacy or maintenance of confidentiality at triage and the receptionist site. It was also noted that the medication door in the ER was not always closed or locked. Although there are cameras and locked doors, there still is some concern around staff safety especially at night. This issue exists to varying degree in many of the small facilities. It is worthwhile to review this issue from a collective perspective. The risk may be real or just a confidence issue, but it is worth reviewing.
THe ER at Lion's Head is also working hard to deal with the issue of confidentiality in the triaging process.
The ER at Southampton is obviously challenged with its limited spaces and expanding needs especially in the summer time. The challenges of balancing staff to the seasonal changes is noted and may require further review. It was also noted that the cameras give relatively limited pictures due to the short range of the camera.
Detailed Accreditation Results 31

Accreditation Report
The information collected in the ER is a blend of written documents including MD and primary nurse assessments, triage's Best Possible Medication History, triage assessment, demographics and lab and DI reports. This repository of information is readily available for all care givers and moves with the patient. There is some trailing of expanding the computer generated material as the organization moves towards a paperless solution.
The ER in Wiarton was also reviewed. It obviously has a modern, expansive physical site and follows a similar system to care for their patients as we witnessed in Owen Sound and Markdale. The triage phase includes a two step registration process that involved a private telephone conservation with the receptionist. The nurse triage is a large well equipped site with adequate privacy and protection for the staff. The tracking system exists and supports patient flow. The med cupboard and refrigerator is well secured and appropriately monitored. The department is very well supported by the local family physicians who have a common belief that working in the local ER is part of the mandate of being a rural family MD.
The ER service in Meaford was also reviewed and again, generally running well. It was noted that there was some inconsistent application of the allergy bands for admitted patients. Although the triage area is well identified, there was some concern about the lack of privacy or maintenance of confidentiality at triage and the receptionist site. It was also noted that the medication door in the ER was not always closed or locked. Although there are cameras and locked doors, there still is some concern around staff safety especially at night. This issue exists to varying degree in many of the small facilities. It is worthwhile to review this issue from a collective perspective. The risk may be real or just a confidence issue, but it is worth reviewing.
THe ER at Lion's Head is also working hard to deal with the issue of confidentiality in the triaging process.
The ER at Southampton is obviously challenged with its limited spaces and expanding needs especially in the summer time. The challenges of balancing staff to the seasonal changes is noted and may require further review. It was also noted that the cameras give relatively limited pictures due to the short range of the camera.
No Unmet Criteria for this Priority Process.
The identification and monitoring of process and outcome measures to evaluate and improve the quality of services to clients and the impact on client outcomes.
Impact on Outcomes
The staff are versed on the issue of near misses and critical incidents. There are processes of documentation that will go to the risk manager and the unit manager. It will be the responsibility of the unit manager to document her/her review and action plan and indicate this to the quality / risk manager who will review the proposed action.
Information on performance such as hours worked, volumes of patients, wait times, budget implications and left without being seen are reviewed regularly and shared up and down the information and corporate ladder.
Surveyor Comments
No Unmet Criteria for this Priority Process.
Detailed Accreditation Results32
The information collected in the ER is a blend of written documents including MD and primary nurse assessments, triage's Best Possible Medication History, triage assessment, demographics and lab and DI reports. This repository of information is readily available for all care givers and moves with the patient. There is some trailing of expanding the computer generated material as the organization moves towards a paperless solution.
The ER in Wiarton was also reviewed. It obviously has a modern, expansive physical site and follows a similar system to care for their patients as we witnessed in Owen Sound and Markdale. The triage phase includes a two step registration process that involved a private telephone conservation with the receptionist. The nurse triage is a large well equipped site with adequate privacy and protection for the staff. The tracking system exists and supports patient flow. The med cupboard and refrigerator is well secured and appropriately monitored. The department is very well supported by the local family physicians who have a common belief that working in the local ER is part of the mandate of being a rural family MD.
The ER service in Meaford was also reviewed and again, generally running well. It was noted that there was some inconsistent application of the allergy bands for admitted patients. Although the triage area is well identified, there was some concern about the lack of privacy or maintenance of confidentiality at triage and the receptionist site. It was also noted that the medication door in the ER was not always closed or locked. Although there are cameras and locked doors, there still is some concern around staff safety especially at night. This issue exists to varying degree in many of the small facilities. It is worthwhile to review this issue from a collective perspective. The risk may be real or just a confidence issue, but it is worth reviewing.
THe ER at Lion's Head is also working hard to deal with the issue of confidentiality in the triaging process.
The ER at Southampton is obviously challenged with its limited spaces and expanding needs especially in the summer time. The challenges of balancing staff to the seasonal changes is noted and may require further review. It was also noted that the cameras give relatively limited pictures due to the short range of the camera.
Surveyor Comments
QMENTUM PROGRAM
Measures practiced by healthcare personnel in healthcare facilities to decrease transmission and acquisition of infectious agents.
Infection Prevention and Control
The infection prevention and control department is an excellent service with strong local leadership. They have evolved a number of very good partnerships such as public health and the consultative arrangement with the University Health Network. They have been very active in responding to a number of ARO outbreaks in a number of sites. This has forced them to develop responses quickly to isolate, close selectively or restrict admissions in an attempt to control. The infection disease prevention team has been very well supported by leadership especially by using the Incident Management Service of senior leadership. This has allowed them to focus on the outbreak and delegate the political issues to the senior management.
Unfortunately the response to outbreaks has made the ongoing maintenance and scanning more difficult from a time challenge but our observations were very positive. The facilities are very clean and very focused on preventive practices.
THe review in the OR and in the central sterilization departments of the various sites were in full compliance with the standards. The leadership in the various sites are well aware of the implication of letting something fall thru the system and are very focused and committed to ensure safe and detailed practices to ensure sterility, careful separation of clean and dirty and ensuring staff compliance with the standards.
There were a few minor issues such as food being kept in some of the medication and vaccination fridges.
Surveyor Comments
No Unmet Criteria for this Priority Process.
Managing Medications
Interdisciplinary provision of medication to clients.
Medication Management
In the Rural Sites, they have implemented Electronic Documentation and have patient education and reference material for medications via Lexi-Comp right at point of care. The Medication Management System (Pharmacy in particular) is very efficient whereby there is a central fax service for the entire region (12 sites), and a Pharmacy Technician performing order entry 24/7 at varying sites, depending on the day of the week. There is a Pharmacist on-site at the Owen Sound Site for 12 hours during the day doing order verification, and there is one Pharmacist On-Call for the 12 hours overnight. There is a Clinical Pharmacist that is on site one day a week at each of the Rural Sites.
A Pharmacist partakes in the Patient Safety Walkabouts. There is a Multidisciplinary Safe Medications Committee, which is completing the implementation of the 183 recommendations from the ISMP Safe Medications Practice Review.
not in use. During this survey, this was not consistently met.
The organization is encouraged to advocate for Electronic Medication Management (eMar) implementation at the Owen Sound Site. In addition, the Rural Sites do not have Unit Dose, which is inconsistent with Best Practice.
In addition, it was noted in several areas (NICU/OBS, Ambulatory Care, Mental Health (inpatient)) that the Medication Carts were not locked.
There continues to be Magnesium Sulphate and Calcium Gluconate in the night/weekend cupboards at the Rural sites. This appears to be more historical, than of necessary.
Surveyor Comments
Detailed Accreditation Results 33
Infection Prevention and Control

Accreditation Report
access to the medication cart in the step down area and that the medication cart be locked when not in use. During this survey, this was not consistently met.
The organization is encouraged to advocate for Electronic Medication Management (eMar) implementation at the Owen Sound Site. In addition, the Rural Sites do not have Unit Dose, which is inconsistent with Best Practice.
In addition, it was noted in several areas (NICU/OBS, Ambulatory Care, Mental Health (inpatient)) that the Medication Carts were not locked.
There continues to be Magnesium Sulphate and Calcium Gluconate in the night/weekend cupboards at the Rural sites. This appears to be more historical, than of necessary.
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
The organization removes concentrated electrolytes (including, but not limited to, potassium chloride, potassium phosphate, sodium chloride >0.9%) from client service areas.
7.2
There are no concentrated electrolytes stored in client service areas.
7.2.1
Medications for client service areas are stocked in ready-to-use formats, where available.
7.3
The pharmacy and other service providers accept verbal orders for medication only in emergencies.
10.9
The pharmacy dispenses medications in unit dose packaging. 13.3
Medicine Services
Providing leadership and overall goals and direction to the team of people providing services.
Clinical Leadership
Based on a number of infectious outbreaks that impacted medical beds, the clinical leadership of the program at Owen Sound has redesigned the capacity of the medical program. 28 medical beds have been increased to 32 beds. The medical unit was relocated in a more spacious area thereby allowing us to increase the volume of private rooms and reducing our use of "ward" room to 1, which houses a maximum of 2 patients. As well, ALC patients have to a large extent be localized in one geographic area. A number of other changes such as enhanced cleaning, more detailed standard work for housekeeping for rooms requiring two cleans and changes in practice have occurred. All of the initiatives have all contributed to improving the medical programs performance with respect to nosocomial transmission.
Care of the medical patients in the rural hospitals was client centred and solid.
All medical programs are working on strategies to facilitate patient flow, Bullet rounds, case conferencing, flex clinics and the One Number to Call initiative
Goals for the Medical Programs need more specificity and to be measurable as well as demonstrate clear alignment with the corporate strategic directions. Physician engagement in goal setting and planning for the Medical Service is important and the medical teams across the corporation are encouraged to find ways to engage them in the planning and goal setting process.
Staffing and staff safety need to be reviewed at the Southampton site. The activity in the ER in the past two years has had a higher seasonal surge according to both management and staff. Concurrently, within the past two years capacity for 5 telemetry beds has been added on 2east. The staff on 2east back up the ER staff particularly on the off shift hours. Between activity in ER, higher acuity on the medical unit and staff being regularly diverted to support patients during transport for diagnostic or other reasons the existing situation needs to be re-examined. Serious consideration needs to be provided to re-examining the staffing model particularly during the peak season of patient activity.
Surveyor Comments
Detailed Accreditation Results34
There was a recommendation from the last accreditation survey to develop a process to restrict

QMENTUM PROGRAM
Care of the medical patients in the rural hospitals was client centred and solid.
All medical programs are working on strategies to facilitate patient flow, Bullet rounds, case conferencing, flex clinics and the One Number to Call initiative
Goals for the Medical Programs need more specificity and to be measurable as well as demonstrate clear alignment with the corporate strategic directions. Physician engagement in goal setting and planning for the Medical Service is important and the medical teams across the corporation are encouraged to find ways to engage them in the planning and goal setting process.
Staffing and staff safety need to be reviewed at the Southampton site. The activity in the ER in the past two years has had a higher seasonal surge according to both management and staff. Concurrently, within the past two years capacity for 5 telemetry beds has been added on 2east. The staff on 2east back up the ER staff particularly on the off shift hours. Between activity in ER, higher acuity on the medical unit and staff being regularly diverted to support patients during transport for diagnostic or other reasons the existing situation needs to be re-examined. Serious consideration needs to be provided to re-examining the staffing model particularly during the peak season of patient activity.
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
The team works together to develop goals and objectives. 2.1
The team’s goals and objectives for its medicine services are measurable and specific.
2.2
Developing a highly competent interdisciplinary team with the knowledge, skills and abilities to develop, manage, and deliver effective and efficient programs, services, and care.
Competency
There is evidence of a good interdisciplinary team functioning within the Medical Programs. Bullet rounds are conducted daily with good hospitalist participation at Owen Sound. Bullet rounds are also conducted at the rural sites with participation of the available core interdisciplinary team members available at the site. It is noted that if required at the rural sites, interdisciplinary expertise such as social work or others can be accessed by phone as may be required. CCAC representation was noted in all of the bullet rounds attended.
Staff working on the medical units are experienced and have had further training and exposure to dealing with the acute care medical population. They have access to regular inservices and CME. All staff interviewed commented on the fact that they felt that the organization supported their educational needs as funding permitted.
Program.
Performance appraisals for all front line staff in Medicine have been 95%- 100% completed depending on the site. The clinical leadership of the Medical Program have also had their performance appraisals completed.
Given the organizations focus on patient flow and the high number of ALC patients, it is suggested that consideration be given to training managers and staff in the Medical Program in Lean methodology to facilitate their being able to initiate process improvements that will help with patient flow as well as access to medical inpatient beds.
Surveyor Comments
Detailed Accreditation Results 35

Accreditation Report
A good orientation program and buddy system is available to staff who newly join the Medical Program.
Performance appraisals for all front line staff in Medicine have been 95%- 100% completed depending on the site. The clinical leadership of the Medical Program have also had their performance appraisals completed.
Given the organizations focus on patient flow and the high number of ALC patients, it is suggested that consideration be given to training managers and staff in the Medical Program in Lean methodology to facilitate their being able to initiate process improvements that will help with patient flow as well as access to medical inpatient beds.
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
The interdisciplinary team follows a formal process to regularly evaluate its functioning, identify priorities for action, and make improvements.
3.7
Healthcare services provided for a health problem from the first encounter with a health care provider through the completion of the last encounter related to that problem.
Episode of Care
The team provides good assessment and management of pain.
Patient satisfaction with the care providers and the care processes delivered within the Medical Programs is high across all sites of the corporation.
There is evidence that clinical practice guidelines are in use and clinicians are using them.
The medical programs has been able to purchase some equipment to be able to manage morbidity obese patients. This has made a difference to both the patients and the staff looking after them. At the rural sites a number of high low beds have been purchased which has made a difference in the management of patients at risk for falls.
Across all sites, there has been a concerted effort to ensure that the ROP for two patient identifiers be hardwired. The attention to this ROP was readily apparent in every interaction observed between staff and patients.
A plan for bed replacement and acquisition of more high low beds will need to be considered pending financial and approval authorizations over the next 3 - 5 years.
The 2 East medical unit at Southampton is space challenged on may fronts; storage, medication room, patient rooms, nursing station etc. Despite the limitations of the physical plant the staff provide good care to the clients they serve.
temperature monitoring. Food and open cans of ensure were found in the fridges inspected in Owen Sound.
Medication Administration at Admission, Transfer and Discharge is at the beginning stages of implementation across most of the medical programs. All the programs are in various stages of implementation and are encouraged to continue to roll out this ROP in its entirety. The Southampton site was observed to have medication reconciliation on admission, transfer and discharge.
All of the medical programs are challenged with facilitating patient flow and the appropriate management of ALC patients. The teams are encouraged to learn from other organizations who are experiencing the same issues and have had a longer period of experience with Lean methodology. There are lessons that can be learned and incorporated to help manage the ALC issues faced by the corporation.
It is suggested that planning and benchmarking at the service level is an area of improvement across all the medical programs. It is further suggested that benchmarking should occur not only externally but internally.
Surveyor Comments
Detailed Accreditation Results36

QMENTUM PROGRAM
It is suggested that audits of medication fridges be undertaken on a regular basis along with temperature monitoring. Food and open cans of ensure were found in the fridges inspected in Owen Sound.
Medication Administration at Admission, Transfer and Discharge is at the beginning stages of implementation across most of the medical programs. All the programs are in various stages of implementation and are encouraged to continue to roll out this ROP in its entirety. The Southampton site was observed to have medication reconciliation on admission, transfer and discharge.
All of the medical programs are challenged with facilitating patient flow and the appropriate management of ALC patients. The teams are encouraged to learn from other organizations who are experiencing the same issues and have had a longer period of experience with Lean methodology. There are lessons that can be learned and incorporated to help manage the ALC issues faced by the corporation.
It is suggested that planning and benchmarking at the service level is an area of improvement across all the medical programs. It is further suggested that benchmarking should occur not only externally but internally.
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
Medication Reconciliation at Admission 7.6
The team does not have any unaddressed priority for action flags based on their medication reconciliation at admission indicator results.
7.6.2
When clients are incapable of giving informed consent, the team refers to the client’s advance directives if available or obtains consent using a substitute decision maker.
8.4
Information, research and evidence, data, and technologies that support and facilitate management and clinical decision-making.
Decision Support
An MRS research study was conducted on the unit by researcher from University of Guelph. Clinical Research Advisory Committee oversees all research and ethics approvals for studies.
There is evidence that there is good sharing of information amongst the interdisciplinary team as well as other providers who are involved in the care of the patient . Coordination of care although not without its challenges in specific case situations by and large is seamless. Complex client situations involve focused interdisciplinary discussions with the intent of having the patient discharged to the right continuum of care as quickly and safely as possible.
Surveyor Comments
No Unmet Criteria for this Priority Process.
Detailed Accreditation Results 37

Accreditation Report
The identification and monitoring of process and outcome measures to evaluate and improve the quality of services to clients and the impact on client outcomes.
Impact on Outcomes
The team has a good focus on safety. Safety walk about have been conducted on the unit. It was observed that staff were compliant in consistently following the two patient identifier policy when doing medication administration as other activities where it is important to ensure that the procedure or treatment is client specific.
Patient satisfaction is monitored via NCR Picker and is reviewed on a regular basis. It was reported that many thank you's to staff come in the newspaper especially from family whose relative has passed on the medical units.
Good, solid work is being done by the medical team.
The team needs to work on more clearly identifying what metrics it is monitoring that is aligned to the corporate scorecard but is relevant at the program/service level for medicine. It is suggested that the team can benefit from being more proactive in its benchmarking activities and in comparing itself with peer groups around its performance on metrics that are relevant to the medical population.
Surveyor Comments
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
The team identifies and monitors process and outcome measures for its medicine services.
16.1
The team compares its results with other similar interventions, programs, or organizations.
16.3
The team shares evaluation results with staff, clients, and families.
16.5
Mental Health Services
Providing leadership and overall goals and direction to the team of people providing services.
Clinical Leadership
There are very experienced and supportive staff that have worked together for a considerable amount of time at the Owen Sound Site.
The Clinical Service team meets regularly with a good representation from the various service providers.
The Outpatient Mental Health Team should be commended for all of the programs and services they are provided to the community, especially since there is a significant wait list to be seen at the Urgent Clinic or by a Psychiatrist.
There is a 2008-2010 workplan for the Clinical Service team, but actual goals and objectives, that are aligned with the Strategic Plan are not present.
The Outpatient Mental Health team are encouraged to advocate for the continuation of the Community Mental Health Common Assessment project.
Surveyor Comments
Detailed Accreditation Results38

QMENTUM PROGRAM
The Outpatient Mental Health Team should be commended for all of the programs and services they are provided to the community, especially since there is a significant wait list to be seen at the Urgent Clinic or by a Psychiatrist.
There is a 2008-2010 workplan for the Clinical Service team, but actual goals and objectives, that are aligned with the Strategic Plan are not present.
The Outpatient Mental Health team are encouraged to advocate for the continuation of the Community Mental Health Common Assessment project.
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
The team’s scope of services is aligned with the organization’s strategic direction.
1.3
The team works together to develop goals and objectives. 2.1
The team’s goals and objectives for its mental health services are measurable and specific.
2.2
Developing a highly competent interdisciplinary team with the knowledge, skills and abilities to develop, manage, and deliver effective and efficient programs, services, and care.
Competency
There are a number of programs utilizing a multidisciplinary team approach.
Staff should be encouraged to take part in the hospital sponsored education on Infusion pumps. Despite being told that they rarely get a patient with an IV, there was one patient admitted to PICU with an IV during the survey.
Staff members were not aware of their right nor the process to refuse work, if ever faced with an unsafe work environment.
Surveyor Comments
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
The organization provides sufficient workspace to support interdisciplinary team functioning and interaction.
3.5
Detailed Accreditation Results 39

Accreditation Report
The interdisciplinary team follows a formal process to regularly evaluate its functioning, identify priorities for action, and make improvements.
3.7
Staff and service providers receive ongoing, effective training on infusion pumps.
4.4
There is documented evidence of ongoing, effective training on infusion pumps.
4.4.1
The team is aware of the process to initiate the work refusal policy.
5.5
Healthcare services provided for a health problem from the first encounter with a health care provider through the completion of the last encounter related to that problem.
Episode of Care
There a number of programs and services that are available to the community that the team serves. The organization has created a directory of services outlining all that is available, with clear and concise wording as to what each service entails (Who are we?, What do we do?, Who do we serve?, Can we help you?).
There are separate information folders for both patients in the inpatients areas and one for their families/friends. The informationoutlines various safety initiatives (Top 10 Tips to Reduce Your Chance of Having a Fall) and privacy issues (Circle of Care).
There are a multitude of services available to the client upon discharge, including the COT making contact with the client within 24 hours of discharge.
The organization is highly encouraged to advocate for the redesign of the PICU.
Sprinkler System heads and ventilation grates that are seen in all of the client rooms of the Acute and PICU units are a safety risk and should be replaced with those appropriate for mental health clients.
Surveyor Comments
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
Medication Reconciliation at Admission 7.7
The team does not have any unaddressed priority for action flags based on their medication reconciliation at admission indicator results.
7.7.2
Detailed Accreditation Results40

QMENTUM PROGRAM
The team reconciles medications with the client at referral or transfer, and communicates information about the client’s medications to the next provider of service at referral or transfer to another setting, service, service provider, or level of care within or outside the organization.
11.3
There is a demonstrated, formal process to reconcile client medications at referral or transfer.
11.3.1
The process includes generating a comprehensive list of all medications the client has been taking prior to referral or transfer.
11.3.2
The process includes a timely comparison of the prior-to-referral or prior-to-transfer medication list with the list of new medications ordered at referral or transfer.
11.3.3
The process requires documentation that the two lists have been compared; differences have been identified, discussed, and resolved; and appropriate modifications to the new medications have been made.
11.3.4
The process makes it clear that medication reconciliation is a shared responsibility involving the client, nursing staff, medical staff and pharmacists, as appropriate.
11.3.5
The organization has a documented plan to implement throughout the organization, and before the next accreditation survey, a medication reconciliation process at referral and transfer.
11.3.6
Information, research and evidence, data, and technologies that support and facilitate management and clinical decision-making.
Decision Support
There is great collaboration with a number of Community Partners.
Documentation is still paper-based, and the team is encouraged to advocate for Electronic Documentation in order to facilitate collaboration, and efficiencies.
The Clinical Support team is encouraged to include more front-line staff when decisions are made about forms/processes that affect them. The Suicide Risk Assessment Tool is being modified by the front-line staff who is using it, in order for it to be of value to them.
Surveyor Comments
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
Team members receive education and training on information systems and other technology.
13.2
Detailed Accreditation Results 41
Accreditation Report
The team’s process includes seeking input from staff and service providers about the applicability of the guidelines and their ease of use.
14.3
The identification and monitoring of process and outcome measures to evaluate and improve the quality of services to clients and the impact on client outcomes.
Impact on Outcomes
The Community Mental Health Teams in Grey Bruce ensure that people in need of mental health services get the necessary care, as close to their home as possible, and in a timely manner. As a result of the various outpatient programs, there is documented admission avoidance to the Owen Sound Site.
Although generally the mental health services are effective and coordinated, there should be a set of common goals and objectives that all the programs can work collectively towards.
Surveyor Comments
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
The team identifies the resources needed to achieve its goals and objectives.
2.3
Obstetrics/Perinatal Care Services
Providing leadership and overall goals and direction to the team of people providing services.
Clinical Leadership
The clinical services team which is interdisciplinary in composition meets regularly to plan scope of services and discuss and address issues. There are goals and objectives in place which are current, specific and measurable.
Surveyor Comments
No Unmet Criteria for this Priority Process.
Developing a highly competent interdisciplinary team with the knowledge, skills and abilities to develop, manage, and deliver effective and efficient programs, services, and care.
Competency
The team is commended for its implementation of the MORE-OBS program. There are many opportunities for education as well. The staff have appropriate certifications to support their work such as NPR.
Surveyor Comments
No Unmet Criteria for this Priority Process.
Detailed Accreditation Results42

QMENTUM PROGRAM
Healthcare services provided for a health problem from the first encounter with a health care provider through the completion of the last encounter related to that problem.
Episode of Care
This team does 750 births per year with a 20 percent c-section rate. They do C-sections in the Operating room. They are midwives and obstetrics and family physicians who deliver babies. They are criteria in place for who can be delivered and who can be cared for in the NICU. Anaesthesia coverage is available for epidurals. There is an antenatal program in place where moms see obstetrics and a nurse who do assessments for patients which ensures comprehensive information on the mother is available when she arrives to deliver. The team works closely with community organizations to ensure their is a continuum of care and follow up before and post delivery. The team members relate well to one another.The team is encouraged to regularly review safety of staff on the night shifts which is always a potential risk when there are few staff on a unit and a large space to cover.
Surveyor Comments
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
Medication Reconciliation at Admission. 7.13
The team does not have any unaddressed priority for action flags based on their medication reconciliation at admission indicator results.
7.13.2
The team follows the organization’s established policies on storing and disposing of medications safely and securely.
9.7
Following transition or end of service, the team contacts clients, families, or referral organizations to evaluate the effectiveness of the transition, and uses this information to improve its transition and end of service planning.
11.5
Information, research and evidence, data, and technologies that support and facilitate management and clinical decision-making.
Decision Support
The team has vaginal deliveries, C-section and newborn guidelines.
Surveyor Comments
No Unmet Criteria for this Priority Process.
The identification and monitoring of process and outcome measures to evaluate and improve the quality of services to clients and the impact on client outcomes.
Impact on Outcomes
Detailed Accreditation Results 43
quality of services to clients and the impact on client outcomes.

Accreditation Report
The clinical service team meets regularly and reviews issues and concerns and monitors process and outcomes. There are many sources of data such as the NIDAY data and patient satisfaction information which is benchmarked appropriately.
Surveyor Comments
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
The team shares evaluation results with staff, clients, and families.
17.5
Rehabilitation Services
Providing leadership and overall goals and direction to the team of people providing services.
Clinical Leadership
There are recovered stroke patients that now serve as volunteers for the current stroke patients, which has proven to be very beneficial.
The team has many community partnerships which they utilize to their fullest. in particular, there is a "Community of Practice" team that collaborates with all providers quarterly, including a Rehab Facilitator from LHSC.
There is a shared manager for Rehab and the District Stroke Strategy.
The team needs to have current goals and objectives that are aligned with the Organization's Strategic Plan. The goals and objectives need to be specific and measurable.
Surveyor Comments
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
The team’s scope of services is aligned with the organization’s strategic direction.
1.3
The team works together to develop goals and objectives. 2.1
The team’s goals and objectives for rehabilitation services are measurable and specific.
2.2
Detailed Accreditation Results44

QMENTUM PROGRAM
Developing a highly competent interdisciplinary team with the knowledge, skills and abilities to develop, manage, and deliver effective and efficient programs, services, and care.
Competency
There is a well defined, interdisciplinary team that meets weekly for case conferencing.
There is a new manager to the Rehab Unit, and she is advocating for the RPNs/RNs to work to their full scope of practice.
The majority of the team members have been on the team for many years and work well together.
Since the majority of the nursing staff have been on the team for many years, any changes to upgrade/change/add services have been a challenge (TPN for patients, RN/RPN Scope of Practice, changes to the Admission Criteria as occupancy rates are low).
Surveyor Comments
The table below indicates the specific criteria that require attention, based on the accreditation review.
Criteria Location Priority forAction
Team members have position profiles that define roles, responsibilities, and scope of practice.
3.2
The team orients new team members about their roles and responsibilities, the team goals and objectives, and the organization as a whole.
4.2
Healthcare services provided for a health problem from the first encounter with a health care provider through the completion of the last encounter related to that problem.
Episode of Care
There is an Improvement Project Charter underway for an "Integrated Interdisciplinary Stroke Team Model for Acute Care".
Patients are very satisfied with the care that they have received by this team.
The organization is increasing their efforts to make their services known to the community.
Patients are involved in their care planning to some extent, but would greatly benefit from visual reminders of the plan of care with the use of white boards in their rooms.
The team is encouraged to continue to advocate for the acquisition of Hi Lo Beds for the clients.
Surveyor Comments
The table below indicates the specific criteria that require attention, based on the accreditation review.
Detailed Accreditation Results 45

Accreditation Report
Criteria Location Priority forAction
Medication Reconciliation at Admission 7.5
The team does not have any unaddressed priority for action flags based on their medication reconciliation at admission indicator results.
7.5.2
The team reconciles medications with the client at referral or transfer, and communicates information about the client’s medications to the next provider of service at referral or transfer to another setting, service, service provider, or level of care within or outside the organization.
11.3
There is a demonstrated, formal process to reconcile client medications at referral or transfer.
11.3.1
The process includes generating a comprehensive list of all medications the client has been taking prior to referral or transfer.
11.3.2
The process includes a timely comparison of the prior-to-referral or prior-to-transfer medication list with the list of new medications ordered at referral or transfer.
11.3.3
The process requires documentation that the two lists have been compared; differences have been identified, discussed, and resolved; and appropriate modifications to the new medications have been made.
11.3.4
The process makes it clear that medication reconciliation is a shared responsibility involving the client, nursing staff, medical staff and pharmacists, as appropriate.
11.3.5
Information, research and evidence, data, and technologies that support and facilitate management and clinical decision-making.
Decision Support
The active Rehabilitation program is a high functioning, multidisciplinary team. There is an extensive occupational, physiotherapy, speech-language pathology, recreation, social work, dietician, pharmacy, and nursing components.
Surveyor Comments
No Unmet Criteria for this Priority Process.
The identification and monitoring of process and outcome measures to evaluate and improve the quality of services to clients and the impact on client outcomes.
Impact on Outcomes
There is extensive use of FIM (functional independence measure) scores at the appropriate times.The use of key performance indicators was not identified.
Surveyor Comments
Detailed Accreditation Results46

QMENTUM PROGRAM
No Unmet Criteria for this Priority Process.
Delivery of safe surgical care to clients, from preparation and the actual procedure in the operating room, to the post-recovery area and discharge.
Surgical Procedures
The two managers have been jointly supporting the program due to a vacancy in the director's position. Each is very well versed in their different responsibilities and have been able to collaborate with the medical leadership in the surgical program. There is a easy flow of information and patients from the preop area, to the day and same day surgery areas, to the OR and eventually home or to the inpatient area. Documentation flows easily and the patient has a clear sense of what is next and who will look after them. Some patients are under diagnosis specific clinical pathways and this results in a formal plan of action that supports the patient and relevant care givers such as physio and expected date of discharge. This information is clearly shared with the patient via a white board in each patient room.
Most conflicts are dealt with at the personal or department level. However there is a clear understanding that chronic bad behaviour that includes verbal abuse, badgering or disrespect is not to be tolerated and would result in quick referral to senior team members to initiate changes and reviews. Simply put, bad behaviour is not tolerated within the organization.
There are specific educators on both the OR and the surgical floor that helps with mentoring, orientation and education of staff as needed.
There are some challenges with use of physical space. Generally there is plenty of rooms but the space is relatively limited. Space for storage of surgical equipment is limited and all the pre-op bundles congregate together. The organization has started to look at what changes to the physical plant could be considered in a period of economic difficulties. The team looks at the impacts on staff, physicians and patients and patient safety in recommending change.
There is a very good electronic tracking system that is available in a modified form for the waiting family to see. The patients is identified by a number and not name and family was given access to this number.
The surgical check list was most impressive when witnessed by the surveyor and occurred with each family.
The clinical pharmacist supports the medication reconciliation process for same day admit surgical patients. The day prior, the pharmacist will review the pre operative assessment and build the Best Possible Medication List (if necessary, will consult the community pharmacy and family MD) and have it available prior to the procedure. This list is consulted by the anaesthetist and used by the surgeon to create post operative orders by using the OK, hold or discontinue component of the list and then sign the order.
The anaesthetic hand over in the recovery room is clearly verbalized by the anaesthetist to the PACU staff. The anaesthetist remains until the patient is safely breathing and allows the PACU staff to extubate if defined criteria are meet.
The clean equipment comes from SPD via a dumb weigher and nothing is returned via that pathway. Dirty equipment returns to the SPD appropriated prepared via the general service elevator.
The pre operative assessment is detailed and allows for appropriate referral to the anaesthetists. The team is working on a medical directive to allow the pre op assessment nurses to refer directly to the anaesthetists. All same day admits are processed thru this process and some selected day surgery patients. The template is completed by the patient and forwards to the pre op clinic for review and for making an appointment with the service.
Consent is the responsibility of the surgeon and the team or nurse are responsible to verify that the informed consent is documented and that the patient understands the nature of the consent. IF the nurse is concerned that the patient does not understand, the surgeon is engaged prior to surgery.
The surgical program observed in Markdale was very impressive. The entire process from preop to anaesthetic assessment to the surgical check list and pause and eventual return to the recovery room followed the same high standards as witnessed in Owen Sound. The involvement and support of family was noted. Each staff member knew their job and completed it is a very professional way. Patient's family felt very reassured and comforted by the whole procedure.
Although the surgical program was not evaluated at Wiarton, it was noted that the programs has excellent support from the volunteers as they helped patients move from site to site as needed.
The surgical service at Meaford was active and functioning well. It was however noted that the orthopaedic surgeons have different processed for marking R and L and there is value in trying to standardize the process.
The surgical program is utilizing a template for nurse to nurse transfer at the end of the end of a shift. It is called the Transfer Accountability Template and it outlines what information is to be shared. What is most impressive is that it occurs in the presence of the patient and / or family. This process was most impressive and should be expanded to all areas of the hospital.
The surgical team does monitor a variety of outcomes and blends this with patient satisfaction data. This information does collectively influence the improvement activities taken within the program. There are minor inconsistencies between the various sites practicing surgery and it is worth reviewing and benchmarking internally to strive for more standardization. It is also important to share the evaluation information broader than just with management. We could not find any real connecting between the improvement activities and the corporate goals and objectives. It may be worthwhile to ensure that the programs use the guidance of goals and objectives to help direct the quality initiative within the organization.
Surveyor Comments
Detailed Accreditation Results 47

Accreditation Report
The clean equipment comes from SPD via a dumb weigher and nothing is returned via that pathway. Dirty equipment returns to the SPD appropriated prepared via the general service elevator.
The pre operative assessment is detailed and allows for appropriate referral to the anaesthetists. The team is working on a medical directive to allow the pre op assessment nurses to refer directly to the anaesthetists. All same day admits are processed thru this process and some selected day surgery patients. The template is completed by the patient and forwards to the pre op clinic for review and for making an appointment with the service.
Consent is the responsibility of the surgeon and the team or nurse are responsible to verify that the informed consent is documented and that the patient understands the nature of the consent. IF the nurse is concerned that the patient does not understand, the surgeon is engaged prior to surgery.
The surgical program observed in Markdale was very impressive. The entire process from preop to anaesthetic assessment to the surgical check list and pause and eventual return to the recovery room followed the same high standards as witnessed in Owen Sound. The involvement and support of family was noted. Each staff member knew their job and completed it is a very professional way. Patient's family felt very reassured and comforted by the whole procedure.
Although the surgical program was not evaluated at Wiarton, it was noted that the programs has excellent support from the volunteers as they helped patients move from site to site as needed.
The surgical service at Meaford was active and functioning well. It was however noted that the orthopaedic surgeons have different processed for marking R and L and there is value in trying to standardize the process.
The surgical program is utilizing a template for nurse to nurse transfer at the end of the end of a shift. It is called the Transfer Accountability Template and it outlines what information is to be shared. What is most impressive is that it occurs in the presence of the patient and / or family. This process was most impressive and should be expanded to all areas of the hospital.
The surgical team does monitor a variety of outcomes and blends this with patient satisfaction data. This information does collectively influence the improvement activities taken within the program. There are minor inconsistencies between the various sites practicing surgery and it is worth reviewing and benchmarking internally to strive for more standardization. It is also important to share the evaluation information broader than just with management. We could not find any real connecting between the improvement activities and the corporate goals and objectives. It may be worthwhile to ensure that the programs use the guidance of goals and objectives to help direct the quality initiative within the organization.
Detailed Accreditation Results48

QMENTUM PROGRAM
Criteria Location Priority forAction
Surgical Care Services
The team works together to develop goals and objectives. 2.1
The team’s goals and objectives for its surgical care services are measurable and specific.
2.2
The team identifies the resources needed to achieve its goals and objectives.
2.3
Medication Reconciliation at Admission 7.13
The team does not have any unaddressed priority for action flags based on their medication reconciliation at admission indicator results.
7.13.2
The team reconciles medications with the client at referral or transfer, and communicates information about the client’s medications to the next provider of service at referral or transfer to another setting, service, service provider, or level of care within or outside the organization.
11.4
The process includes a timely comparison of the prior-to-referral or prior-to-transfer medication list with the list of new medications ordered at referral or transfer.
11.4.3
The process requires documentation that the two lists have been compared; differences have been identified, discussed, and resolved; and appropriate modifications to the new medications have been made.
11.4.4
The process makes it clear that medication reconciliation is a shared responsibility involving the client, nursing staff, medical staff and pharmacists, as appropriate.
11.4.5
The team shares evaluation results with staff, clients, and families.
16.5
Detailed Accreditation Results 49
The table below indicates the specific criteria that require attention, based on the accreditation review.

Accreditation Report
Performance Measure Results
The following section provides an overview of the performance measures collected for the entire organization. These measures consist of both instrument and indicator results, which are valuable components of evaluation and quality improvement.
The instruments are questionnaires completed by a representative sample of clients, staff, leadership and/or other key stakeholders that provide important insight into critical aspects of the organization’s services. The following tables summarize the organization’s results and highlight each item that requires attention. Results are presented in three main areas: governance functioning, patient safety culture and worklife.
Instrument Results
Performance Measures (Instruments and Indicators): Instrument Results50

QMENTUM PROGRAM
Governance Functioning ToolThe Governance Functioning Tool is intended for members of the governing body to assess their own structures and processes and identify areas for improvement. The results reflect the perceptions and opinions of the governing body regarding the status of its internal structures and processes.
Summary of Results
Governance Structures and Processes % Agree % Neutral % Disagree
Organization Organization Organization
Priorityfor Action
1 We actively recruit, recommend and/or select new members based on needs for particular skills, background, and experience.
100 0 0
2 We have explicit criteria to recruit and select new members.
100 0 0
3 Our renewal cycle is appropriately managed to ensure continuity on the governing body.
100 0 0
4 The composition of our governing body allows us to meet stakeholder and community needs.
100 0 0
5 Clear written policies define term lengths and limits for individual members, as well as compensation.
100 0 0
6 We regularly review, understand, and ensure compliance with applicable laws, legislation and regulations.
92 0 8
7 Governance policies and procedures that define our role and responsibilities are well-documented and consistently followed.
100 0 0
8 We review our own structure, including size and sub-committee structure.
92 0 8
9 We have sub-committees that have clearly-defined roles and responsibilities.
100 0 0
10 Our roles and responsibilities are clearly identified and distinguished from those delegated to the CEO and/or senior management. We do not become overly involved in management issues.
100 0 0
11 We each receive orientation that helps us to understand the organization and its issues, and supports high-quality decision-making.
100 0 0
Performance Measures (Instruments and Indicators): Instrument Results 51

Accreditation Report
12 Disagreements are viewed as a search for solutions rather than a “win/lose”.
92 0 8
13 Our meetings are held frequently enough to make sure we are able to make timely decisions.
100 0 0
14 Individual members understand and carry out their legal duties, roles and responsibilities, including sub-committee work (as applicable).
100 0 0
15 Members come to meetings prepared to engage in meaningful discussion and thoughtful decision-making.
83 0 17
16 Our governance processes make sure that everyone participates in decision-making.
83 0 17
17 Individual members are actively involved in policy-making and strategic planning.
92 0 8
18 The composition of our governing body contributes to high governance and leadership performance.
92 0 8
19 Our governing body’s dynamics enable group dialogue and discussion. Individual members ask for and listen to one another’s ideas and input.
92 0 8
20 Our ongoing education and professional development is encouraged.
100 0 0
21 Working relationships among individual members and committees are positive.
100 0 0
22 We have a process to set bylaws and corporate policies.
100 0 0
23 Our bylaws and corporate policies cover confidentiality and conflict of interest.
100 0 0
24 We formally evaluate our own performance on a regular basis.
92 0 8
25 We benchmark our performance against other similar organizations and/or national standards.
92 0 8
26 Contributions of individual members are reviewed regularly.
92 0 8
27 As a team, we regularly review how we function together and how our governance processes could be improved.
92 0 8
28 There is a process for improving individual effectiveness when non-performance is an issue.
75 0 25
Performance Measures (Instruments and Indicators): Instrument Results52

QMENTUM PROGRAM
29 We regularly identify areas for improvement and engage in our own quality improvement activities.
83 0 17
30 As a governing body, we annually release a formal statement of our achievements that is shared with the organization’s staff as well as external partners and the community.
75 0 25
31 As individual members, we receive adequate feedback about our contribution to the governing body.
92 0 8
32 We have a process to elect or appoint our chair. 100 0 0
33 Our chair has clear roles and responsibilities and runs the governing body effectively.
100 0 0
Performance Measures (Instruments and Indicators): Instrument Results 53

Accreditation Report
Patient Safety Culture SurveyThe patient safety culture survey results provide valuable insight into staff perceptions of patient safety, as well as an indication of areas of strength, areas of improvement, and a mechanism to monitor changes within the organization.
Number of survey respondents = 501 respondents
Summary of Results
A. Patient Safety: Activities to avoid, prevent, or correct adverse outcomes which may result from the delivery of health care
% Disagree % Neutral % Agree
Organization Organization Organization
Priorityfor Action
1 Patient safety decisions are made at the proper level by the most qualified people
9 25 66
2 Good communication flow exists up the chain of command regarding patient safety issues
16 27 58
3 Reporting a patient safety problem will result in negative repercussions for the person reporting it
74 18 8
4 Senior management has a clear picture of the risk associated with patient care
19 29 52
5 My unit takes the time to identify and assess risks to patients
5 17 78
6 My unit does a good job managing risks to ensure patient safety
5 15 81
7 Senior management provides a climate that promotes patient safety
14 26 61
8 Asking for help is a sign of incompetence 88 8 5
9 If I make a mistake that has significant consequences and nobody notices, I do not tell anyone about it
92 4 3
10 I am sure that if I report an incident to our reporting system, it will not be used against me
24 23 53
11 I am less effective at work when I am fatigued 7 10 83
12 Senior management considers patient safety when program changes are discussed
13 37 49
13 Personal problems can adversely affect my performance
24 20 56
14 I will suffer negative consequences if I report a patient safety problem
78 15 7
Performance Measures (Instruments and Indicators): Instrument Results54
Used with permission from York University. All Rights Reserved.
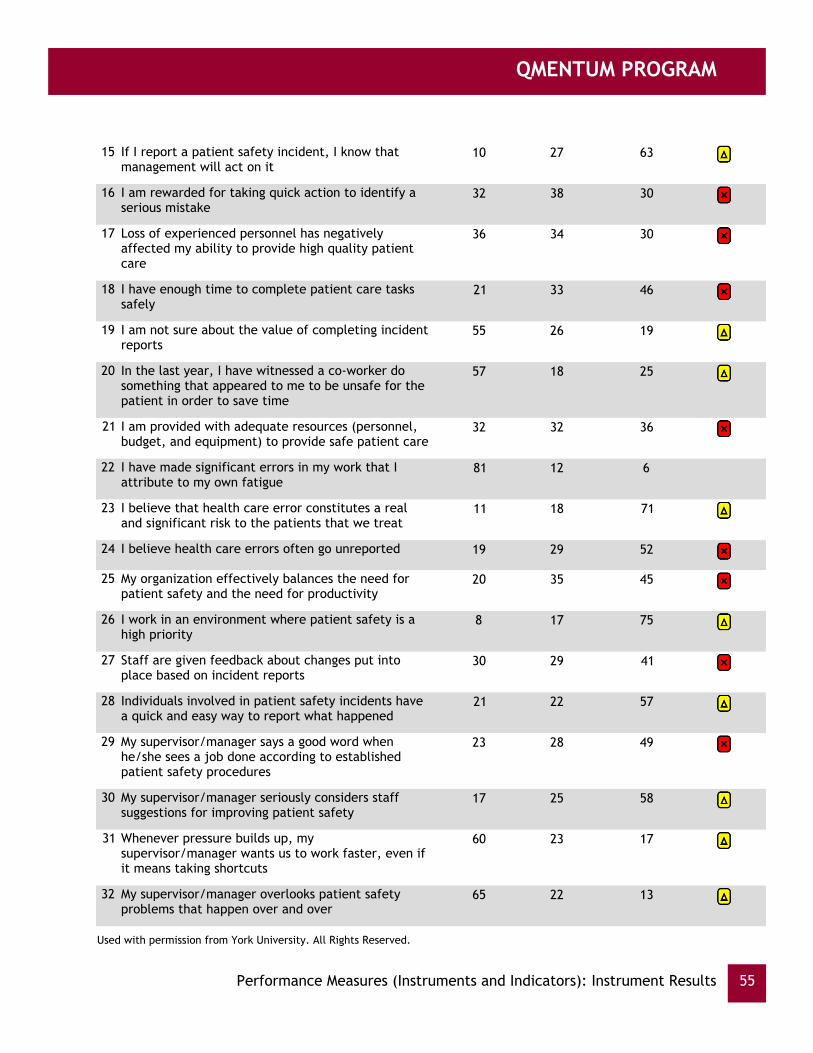
QMENTUM PROGRAM
15 If I report a patient safety incident, I know that management will act on it
10 27 63
16 I am rewarded for taking quick action to identify a serious mistake
32 38 30
17 Loss of experienced personnel has negatively affected my ability to provide high quality patient care
36 34 30
18 I have enough time to complete patient care tasks safely
21 33 46
19 I am not sure about the value of completing incident reports
55 26 19
20 In the last year, I have witnessed a co-worker do something that appeared to me to be unsafe for the patient in order to save time
57 18 25
21 I am provided with adequate resources (personnel, budget, and equipment) to provide safe patient care
32 32 36
22 I have made significant errors in my work that I attribute to my own fatigue
81 12 6
23 I believe that health care error constitutes a real and significant risk to the patients that we treat
11 18 71
24 I believe health care errors often go unreported 19 29 52
25 My organization effectively balances the need for patient safety and the need for productivity
20 35 45
26 I work in an environment where patient safety is a high priority
8 17 75
27 Staff are given feedback about changes put into place based on incident reports
30 29 41
28 Individuals involved in patient safety incidents have a quick and easy way to report what happened
21 22 57
29 My supervisor/manager says a good word when he/she sees a job done according to established patient safety procedures
23 28 49
30 My supervisor/manager seriously considers staff suggestions for improving patient safety
17 25 58
31 Whenever pressure builds up, my supervisor/manager wants us to work faster, even if it means taking shortcuts
60 23 17
32 My supervisor/manager overlooks patient safety problems that happen over and over
65 22 13
Performance Measures (Instruments and Indicators): Instrument Results 55
Used with permission from York University. All Rights Reserved.

Accreditation Report
33 On this unit, when an incident occurs, we think about it carefully
5 25 70
34 On this unit, when people make mistakes, they ask others about how they could have prevented it
14 22 64
35 On this unit, after an incident has occurred, we think about how it came about and how to prevent the same mistake in the future
8 18 74
36 On this unit, when an incident occurs, we analyze it thoroughly
14 27 58
37 On this unit, it is difficult to discuss errors 58 22 20
38 On this unit, after an incident has occurred, we think long and hard about how to correct it
13 31 57
B. These questions are about your perceptions of overall patient safety
% Good/Excellent
%Acceptable
% Poor/Failing
Organization Organization Organization
Priorityfor Action
39 Please give your unit an overall grade on patient safety
64 32 4
40 Please give the organization an overall grade on patient safety
46 46 8
C. These questions are about what happens after a Major Event
% Disagree % Neutral % Agree
Organization Organization Organization
Priorityfor Action
41 Individuals involved in major events contribute to the understanding and analysis of the event and the generation of possible solutions
8 28 64
42 A formal process for disclosure of major events to patients/families is followed and this process includes support mechanisms for patients, family, and care/service providers
10 39 51
43 Discussion around major events focuses mainly on system-related issues, rather than focusing on the individual(s) most responsible for the event
10 43 47
44 The patient and family are invited to be directly involved in the entire process of understanding: what happened following a major event and generating solutions for reducing re-occurrence of similar events
14 55 30
Performance Measures (Instruments and Indicators): Instrument Results56
Used with permission from York University. All Rights Reserved.

QMENTUM PROGRAM
45 Things that are learned from major events are communicated to staff on our unit using more than one method (e.g. communication book, in-services, unit rounds, emails) and / or at several times so all staff hear about it
17 26 57
46 Changes are made to reduce re-occurrence of major events
8 27 66
Performance Measures (Instruments and Indicators): Instrument Results 57
Used with permission from York University. All Rights Reserved.

Accreditation Report
Worklife PulseThe concept of ‘quality of worklife’ is central to Accreditation Canada’s accreditation program. The Pulse Survey enables health service organizations to monitor key worklife areas. The survey takes the ‘pulse’ of quality of worklife, providing a quick and high level snapshot of key work environment factors, individual outcomes, and organizational outcomes. Organizations can then use the findings to identify strengths and gaps in their work environments, engage stakeholders in discussions of opportunities for improvement, plan interventions to improve the quality of worklife, and develop a clearer understanding of how quality of worklife influences the organization’s capacity to meet its strategic goals.
Number of survey respondents = 609 respondents
Summary of Results
How would you rate your work environment % Disagree % Neutral % Agree
Organization Organization Organization
Priorityfor Action
1 I am satisfied with communications in this organization.
29 27 44
2 I am satisfied with communications in my work area. 25 19 56
3 I am satisfied with my supervisor. 15 17 68
4 I am satisfied with the amount of control I have over my job activities.
17 18 64
5 I am clear about what is expected of me to do my job.
5 11 84
6 I am satisfied with my involvement in decision making processes in this organization.
32 27 42
7 I have enough time to do my job adequately. 26 22 52
8 I feel that I can trust this organization. 28 35 37
9 This organization supports my learning and development.
20 26 54
10 My work environment is safe. 12 18 70
11 My job allows me to balance my work and family/personal life.
13 16 71
Performance Measures (Instruments and Indicators): Instrument Results58

QMENTUM PROGRAM
Individual Outcomes % NotStressful
% A bitStressful
% Quite orExtremelyStressful
Organization Organization Organization
Priorityfor Action
12 In the past 12 months, would you say that most days at work were…
18 48 34
% VeryGood/
Excellent
% Good % Fair/ Poor
Organization Organization Organization
Priorityfor Action
13 In general, would you say your health is… 62 33 5
14 In general, would you say your mental health is… 62 31 7
15 In general, would you say your physical health is… 54 37 9
% VerySatisfied
% SomewhatSatisfied
% NotSatisfied
Organization Organization Organization
Priorityfor Action
16 How satisfied are you with your job? 87 10 3
% < 10 % 10 - 15 % > 15
Organization Organization Organization
Priorityfor Action
17 In the past 12 months, how many days were you away from work because of your own illness or injury? (counting each full or partial day as 1 day)
89 3 8
18 During the past 12 months, how many days did you work despite an illness or injury because you felt you had to (counting each full or partial day as 1 day)?
89 6 5
% Never/Rarely
%Sometimes
% Often/Always
Organization Organization Organization
Priorityfor Action
19 How often do you feel you can do your best quality work in your job?
2 18 79
Performance Measures (Instruments and Indicators): Instrument Results 59

Accreditation Report
% Disagree % Neutral % Agree
Organization Organization Organization
Priorityfor Action
20 Overall, I am satisfied with this organization. 15 32 53
21 Working conditions in my area contribute to patient safety.
11 24 65
Performance Measures (Instruments and Indicators): Instrument Results60

QMENTUM PROGRAM
Indicators collect data related to important aspects of patient safety and quality care. The tables in this section show the indicator data that has been submitted by the organization.
Indicator Results
Medication Reconciliation at Admission
Transition points in the care continuum are particularly prone to risk, and the communication of medication information has been identified as a priority area for improving the safety of healthcare service delivery. This performance measure will provide a practical guide for organizations as medication reconciliation is conducted more widely throughout the organization.
Team Name(standard section)
Medication Reconciliation at Admission
Dates(dd/mm/yyyy)
LocationFlag % Formal medicationreconciliation at
admission
4301/01/201031/03/2010
Critical Care (Critical Care Services)
Owen Sound HospitalRED
4801/04/201030/06/2010
Critical Care (Critical Care Services)
Owen Sound HospitalRED
2501/01/201031/03/2010
Medical (Medicine Services)
Owen Sound HospitalRED
5001/04/201030/06/2010
Medical (Medicine Services)
Owen Sound HospitalRED
4601/01/201031/03/2010
Mental Health Services (Mental Health Services)
Owen Sound HospitalRED
4401/04/201030/06/2010
Mental Health Services (Mental Health Services)
Owen Sound HospitalRED
6601/01/201031/03/2010
Surgical (Surgical Care Services)
Owen Sound HospitalRED
5901/04/201030/06/2010
Surgical (Surgical Care Services)
Owen Sound HospitalRED
3301/01/201031/03/2010
Women & Child Care (Obstetrics/Perinatal Care Services)
Owen Sound HospitalRED
4801/04/201030/06/2010
Women & Child Care (Obstetrics/Perinatal Care Services)
Owen Sound HospitalRED
Performance Measures (Instruments and Indicators): Indicator Results 61

Accreditation Report
Team Name(standard section)
Medication Reconciliation at Admission
Dates(dd/mm/yyyy)
LocationFlag % Formal medicationreconciliation at
admission
1201/01/201031/03/2010
Medical (Medicine Services)
Southampton HospitalRED
3301/04/201030/06/2010
Medical (Medicine Services)
Southampton HospitalRED
Threshold for FlagsRED: < 75/100YELLOW: >= 75/100 AND < 90/100GREEN: >= 90/100
Performance Measures (Instruments and Indicators): Indicator Results62

QMENTUM PROGRAM
Surgical Site Infection
Post-surgical infection rate is a key outcome measure that reflects process interventions.
The thresholds for this performance indicator are currently in development. Performance ratings will be provided when the thresholds are finalized.
Team Name(standard section)
Surgical Site Infection: Post-Surgical Infection - Total Joint Arthroplasty
Dates(dd/mm/yyyy)
LocationFlag % post-surgicalinfections
1.601/01/201031/03/2010
Infection Control (Infection Prevention and Control)
Owen Sound Hospital
1.901/04/201030/06/2010
Infection Control (Infection Prevention and Control)
Owen Sound Hospital
Performance Measures (Instruments and Indicators): Indicator Results 63

Accreditation Report
Surgical Site Infection
Timeliness of administering antibiotic prophylaxis is a universal process measure applicable to many surgical procedures and with widely recognized benefits in reducing post-surgical infections in selected high risk procedures.
Team Name(standard section)
Surgical Site Infection: Prophylactic Antibiotics - Total Joint Arthroplasty
Dates(dd/mm/yyyy)
LocationFlag % timelyadministrations of
antibiotics
10001/01/201031/03/2010
Infection Control (Infection Prevention and Control)
Owen Sound HospitalGREEN
9701/04/201030/06/2010
Infection Control (Infection Prevention and Control)
Owen Sound HospitalGREEN
Threshold for FlagsRED: < 80/100YELLOW: >= 80/100 AND < 90/100GREEN: >= 90/100
Performance Measures (Instruments and Indicators): Indicator Results64

QMENTUM PROGRAM
Health Care Associated Infection Rates
Health care associated C. difficile and MRSA infections represent a significant risk to the individuals receiving care and are a substantial resource burden to organizations and the health care system. Measuring infection control performance measures has the additional benefit of informing and shaping the staff's view of safety. Evidence suggests that as staff become more aware of infection control rates and the evidence related to infection control there is a change in behaviour to reduce the perceived risk.
Team Name(standard section)
Health Care-Associated MRSA & C. difficile - C. difficile
Dates(dd/mm/yyyy)
LocationFlag # cases of infection /10,000 patient days
001/01/201031/03/2010
Infection Control (Infection Prevention and Control)
Lion's Head HospitalGREEN
001/04/201030/06/2010
Infection Control (Infection Prevention and Control)
Lion's Head HospitalGREEN
001/01/201031/03/2010
Infection Control (Infection Prevention and Control)
Markdale HospitalGREEN
001/04/201030/06/2010
Infection Control (Infection Prevention and Control)
Markdale HospitalGREEN
001/01/201031/03/2010
Infection Control (Infection Prevention and Control)
Meaford HospitalGREEN
001/04/201030/06/2010
Infection Control (Infection Prevention and Control)
Meaford HospitalGREEN
1.701/01/201031/03/2010
Infection Control (Infection Prevention and Control)
Owen Sound HospitalGREEN
2.501/04/201030/06/2010
Infection Control (Infection Prevention and Control)
Owen Sound HospitalGREEN
001/01/201031/03/2010
Infection Control (Infection Prevention and Control)
Southampton HospitalGREEN
Performance Measures (Instruments and Indicators): Indicator Results 65

Accreditation Report
Team Name(standard section)
Health Care-Associated MRSA & C. difficile - C. difficile
Dates(dd/mm/yyyy)
LocationFlag # cases of infection /10,000 patient days
001/04/201030/06/2010
Infection Control (Infection Prevention and Control)
Southampton HospitalGREEN
001/01/201031/03/2010
Infection Control (Infection Prevention and Control)
Wiarton HospitalGREEN
001/04/201030/06/2010
Infection Control (Infection Prevention and Control)
Wiarton HospitalGREEN
Threshold for FlagsRED: > 80/10,000YELLOW: <= 80/10,000 AND > 60/10,000GREEN: <= 60/10,000
Team Name(standard section)
Health Care-Associated MRSA & C. difficile - MRSA
Dates(dd/mm/yyyy)
LocationFlag # cases of infection +colonization / 10,000
patient days
001/01/201031/03/2010
Infection Control (Infection Prevention and Control)
Lion's Head HospitalGREEN
001/04/201030/06/2010
Infection Control (Infection Prevention and Control)
Lion's Head HospitalGREEN
001/01/201031/03/2010
Infection Control (Infection Prevention and Control)
Markdale HospitalGREEN
5901/04/201030/06/2010
Infection Control (Infection Prevention and Control)
Markdale HospitalGREEN
001/01/201031/03/2010
Infection Control (Infection Prevention and Control)
Meaford HospitalGREEN
Performance Measures (Instruments and Indicators): Indicator Results66

QMENTUM PROGRAM
Team Name(standard section)
Health Care-Associated MRSA & C. difficile - MRSA
Dates(dd/mm/yyyy)
LocationFlag # cases of infection +colonization / 10,000
patient days
701/04/201030/06/2010
Infection Control (Infection Prevention and Control)
Meaford HospitalGREEN
1.701/01/201031/03/2010
Infection Control (Infection Prevention and Control)
Owen Sound HospitalGREEN
1101/04/201030/06/2010
Infection Control (Infection Prevention and Control)
Owen Sound HospitalGREEN
8.701/01/201031/03/2010
Infection Control (Infection Prevention and Control)
Southampton HospitalGREEN
001/04/201030/06/2010
Infection Control (Infection Prevention and Control)
Southampton HospitalGREEN
001/01/201031/03/2010
Infection Control (Infection Prevention and Control)
Wiarton HospitalGREEN
8.601/04/201030/06/2010
Infection Control (Infection Prevention and Control)
Wiarton HospitalGREEN
Threshold for FlagsRED: > 80/10,000YELLOW: <= 80/10,000 AND > 60/10,000GREEN: <= 60/10,000
Performance Measures (Instruments and Indicators): Indicator Results 67

Accreditation Report
Next Steps
Congratulations! You have just completed your Qmentum on-site survey visit. Please note the following check list items that you need to attend to in the coming days and months.
We ask that you review this report within the next five days for errors in titles of names of services. This will help ensure the report and our records are accurate. Once you have reviewed, please send your requested changes to your Accreditation Specialist.
In 10 business days, a letter outlining your accreditation decision and requirements will be e-mailed to your Chief Executive Officer. If revisions to the report were required, a copy of a revised report will be sent along with that letter.
You are required to submit your quarterly reports on indicators on May 31st, every year. If you have any questions regarding this submission, please contact your Accreditation Specialist.
Next Steps68

QMENTUM PROGRAM
Appendix A – Accreditation Decision Guidelines
Quality improvement continues to be a key principle of Accreditation Canada’s Qmentum program.Accreditation Canada’s standards assess the quality of services provided by an organization and areconstructed around eight dimensions of quality:
1. Population focus2. Accessibility3. Safety4. Worklife5. Client-centred services6. Continuity of services7. Effectiveness8. Efficiency
Each standard criterion is related to a quality dimension. Organizations participating in AccreditationCanada’s Qmentum program are eligible for the recognition awards: Accreditation; Accreditation withCondition (Report and/or Focused Visit) and Non-accreditation.
Under the Qmentum accreditation program, Accreditation Canada High Priority Criteria and RequiredOrganization Practices (ROPs) are the two main factors that are considered in determining the appropriaterecognition award.
Accreditation Canada High Priority Criteria
Accreditation Canada identifies high priority criteria by their alignment with several key areas:
• Quality Improvement• Safety• Risk• Ethics
Required Organization Practices (ROPs)
A Required Organizational Practice is defined as an essential practice that organizations must have inplace to enhance patient/client safety and minimize risk. It is a specific requirement for healthcareorganizations in the accreditation program.
Based on the above, the three accreditation decisions for 2010 Qmentum surveys are:
Appendix A – Accreditation Decision Guidelines 69

Accreditation Report
Option 1: AccreditationAn organization is eligible for full accreditation (with a resurvey in three years) if all of thefollowing criteria are met:
(a) 90% or more of high priority criteria met per standard section, AND(b) Compliance with all of the Required Organizational Practices, AND(c) Compliance with collection of all the performance measures,
If the organization is a CSSS, participating in the Joint Program with Conseil québecois d’agrément(CQA) and Accreditation Canada, the following additional criteria are required, which are specificCQA indicators relating to customer service and worklife:
(d) Compliance with ≥66.6% of Client Satisfaction Indicators AND(e) Compliance with ≥66.6% of Employees Mobilization Indicators
Option 2: Accreditation with Condition: Report and/or Focused VisitAn organization will receive Accreditation with Condition: Report and/or Focused Visit if any offollowing criteria is met:
(a) More than 10% and less than 30% of high priority criteria unmet in any standard section,OR(b) Non-compliance with any one of the Required Organizational PracticesOR(c) Non-compliance with the collection of any one of the performance measures
If the organization is a CSSS, participating in the Joint Program with CQA and Accreditation Canada,the following addition criteria apply:
(d) Compliance with less than 66.6% of Client Satisfaction Indicators, OR(e) Compliance with less than 66.6% of Employees Mobilization Indicators
The condition, i.e. submission of a report or focused visit; and timeframe, i.e. 6 months or 12 months; isbased upon the nature of the recommendations. If the organization is a CSSS, and their compliance withthe Client Satisfaction Indicators OR Employees Mobilization Indicators is less than 66.6%, they mustconduct the survey(s) again within 18 months following the onsite visit as a condition of accreditation.
Organizations are required to submit follow-up reports as a condition of maintaining accreditation status.If a satisfactory report is not submitted within the required timeline, Accreditation Canada may grant aone-time extension of 6 months, based on surveyor input, proof of progress, and a plan to meet theconditions. Failure to comply with these requirements within the maximum allotted time extension willresult in removal of accreditation status, at the discretion of Accreditation Canada.
For organizations that fail to complete a satisfactory focused visit within the required timeline,Accreditation Canada may grant a one-time extension of 6 months, based on surveyor input, proof ofprogress and a plan to meet the conditions. Failure to comply with these requirements within themaximum allotted time extension will result in removal of accreditation status, at the discretion ofAccreditation Canada.
Appendix A – Accreditation Decision Guidelines70

QMENTUM PROGRAM
Option 3: Non-accreditationAn organization will NOT be accredited if the following conditions exist:
(a) One or more ROPs not in placeAND(b) 30% or more high priority criteria unmet in one or more standards sectionsAND(c) 20% or more criteria unmet overall for all standards applied to the organization
Should an organization wish to have their non-accreditation status reviewed within 6 months post survey,they are required to complete a focused visit within 5 months. Organizations that fail to complete asatisfactory focused visit within the required timeframe will maintain a non-accreditation status.
If the organization is a CSSS, and their compliance with the Client Satisfaction Indicators OR EmployeesMobilization Indicators is less than 66.6%, they must conduct the survey(s) again within 18 monthsfollowing the onsite visit as a condition of accreditation.
Appendix A – Accreditation Decision Guidelines 71