growth & development 0-1 year and implications in the hospitalized child by prof. unn hidle...
Post on 19-Dec-2015
215 views
TRANSCRIPT

Growth & Development 0-Growth & Development 0-1 Year and Implications in 1 Year and Implications in
the Hospitalized Childthe Hospitalized Child
Growth & Development 0-Growth & Development 0-1 Year and Implications in 1 Year and Implications in
the Hospitalized Childthe Hospitalized ChildByBy
Prof. Unn HidleProf. Unn HidleUpdated 2010Updated 2010

* THE INFANT – STRONGLY RECOMMENDED
* PEDIATRIC ASSESSMENT - STRONGLY RECOMMENDED
* PROMOTING GROWTH OF THE HOSPITALIZED CHILD* (TODDLER / PRE-SCHOOL / SCHOOL AGE)
Recommended for Pediatric Growth & Development (Videos):

Biological development• During infancy, physical changes and developmental
achievements are tremendous• Acquisition of fine and gross motor skills occurs in an
orderly head-to-toe and center-to-periphery sequence (cephalocaudal-proximodistal)
• Increases in length occur in sudden spurts (growth spurts) rather than a slow, gradual pattern.
• Proportional changes: – by 6 months, the birth weight has at least doubled– by 1 year of age, the birth weight has tripled.– By 1 year of age, the birth length has increased by almost
50%.
• Head growth is also rapid and an important determinant of brain growth.
• By the age of 1 year, the head size has increased by almost 33%.
• Closure of the cranial sutures: – posterior fontanel fusing by 6-8 weeks– anterior fontanel closes by 12-18 months
• The infant growth is strongly influenced by genetic, metabolic, environmental, and nutritional factors

• Growth charts are extremely important
• By the end of the first year:– Brain has increased in weight approx. 2 ½
times– The primitive reflexes are replaced by
voluntary, purposeful movements, and new reflexes that influence motor development appear.

3 month old infant

8 month old infants

Sensory Changes• Visual acuity gradually improves with
binocular fixation:– Binocularity = fixation of two ocular images into
one cerebral picture (fusion) begins to develop by 6 weeks of age and should be well established by age 4 months. Lack of this results in strabismus and must be detected early to prevent permanent blindness
– Depth perception (stereopsis) begins to develop by age 7-9 months but may exist earlier as an innate safety mechanism.
– Visual preference for looking at the human face

Fine Motor Development
• Use of the hands and fingers in the prehension (grasp) of an object.
• Grasping occurs during the first 2-3 months as a reflex and gradually becomes voluntary
• The palmar grasp, using the whole hand, is replaced with a pincer grasp in which the infant uses the thumb and index finger– 8-9 months: crude pincer grasp (use parts of the
hand)– 10-11 months: neat pincer grasp (i.e. raisin)

1 year old infant
Gross Motor Development• Includes posture, head balance, sitting,
creeping, standing, and walking. • Primitive reflexes role in development of gross
motor skills. • Righting reflexes (new reflexes that
influence motor development) elicit certain postural responses, particular of flexion and extension– rolling over– crawl position– maintaining normal head-trunk-limb alignment
during all activities

• Head control: – Full-term newborn: Momentarily hold
the head in midline when prone. – By 3 months of age, infants can hold
their head well beyond the plane of the body.
– By 4-6 months head control is well established

• Rolling over: – From the abdomen to the back: 5 months– From the back to the abdomen occurs at 6 months
• The parachute reflex– Protective response to falling: 7 months
• Sitting: – Follows progressive head control and straightening
of the back. As the spinal column straightens, the infant can be propped in a sitting position.
– 7 months: sit alone, leaning forward on their hands for support.
– 8 months: sit unsupported. – 10 months: maneuver from a prone to a sitting
position.

• Crawling – 9 months: propelling forward with belly on
the floor, progresses to creeping on hands and knees (with belly off the floor)
• “Cruising”– ~11 months: walk while holding onto
furniture
• Infant who does not pull to a standing position by 11-12 months of age should be further evaluated for possible developmental dysplasia of the hip.

Cognitive Development• Piaget’s Theory:
– Theory most commonly used to explain cognition or the ability to know
• Sensorimotor Phase: From birth to 24 months. It is composed of 6 phases.
• Importance of phases include:– Reflex behavior becoming simple repetitive acts– Separation from object or environment– Object permanence – Symbols or Mental representation
• Infant think of an object/situation without experiencing it


Psychosocial Development
• Erikson: – Developing a Sense of Trust (trust vs mistrust)
• Phase I (birth – 1 year) acquiring a sense of trust while overcoming a sense of mistrust.– The trust that develops is a trust of self, of others,
and the world (i.e. trust that they will be fed, comforted, stimulated etc.)
– The crucial element for the achievement of this task is the quality of both the parent/caregiver
– When this synchrony fails to develop, mistrust is the eventual outcome


ATTACHMENATTACHMENTT
ATTACHMENATTACHMENTT

Attachment• The importance of human physical
contact cannot be overemphasized• Attachment may not have a biological
significance since caretakers other than the biological parents can develop a stronger attachment to that child (i.e. adoption)
• If no attachment: ADHD, RAD (reactive attachment disorder, i.e. institutionalized)
• Feral Children: http://www.feralchildren.com/en/index.php

Separation Anxiety• Begins between the age of 4-8 months • Infant begins to have some awareness
of self and mother as separate beings • Object permanence is developing • Separation anxiety develops and is
manifested through a sequence of behaviors, beginning with protest

Separation Anxiety• Separation anxiety is a major stressor from
middle infancy (6 months) throughout the preschool years, which is also called anaclitic depression
• Preschoolers: Refusing to eat, difficulty in sleeping, crying quietly for their parents or withdraw from others
• School-age children: Better able to cope with separation in general, but the stress of hospitalization may regress them to an earlier stage where separation is more difficult.

Separation anxiety

Strategies to Make Separation Easier
• Primary nursing goal is to prevent separation, especially in children < 5 years
• Family-centered care: Collaboration between the health care provider, the child and the family. I.e., parent sleeping at the bedside, “parent tray”, parent’s active participation in the child’s care
• ROUTINE and NORMALIZE child’s day!

• Stranger fear – Sex, age, and size of the stranger – female,
younger age, and smaller size (including kneeling or sitting rather than standing) being less stressful
– Approach – loud, sudden, intrusive approach causing more distress
– Child’s proximity to parent – closer to parent (on parent’s lap rather than in infant seat) being less stressful

LANGUAGE LANGUAGE DEVELOPMENTDEVELOPMENT
LANGUAGE LANGUAGE DEVELOPMENTDEVELOPMENT

Language Development
• Sequence:– Crying: Distinguishing different– Vocalization: 5-6 weeks - small throaty sounds. Then
vowel sounds are added followed by consonants.• “Baby Language” based on crying sounds:
Christine Dunstan: http://www.dunstanbaby.com/cms/index.php?page=us-home
• “NO!” - The meaning is comprehended by 9-10 months
• By age 1 year, they can say 3-5 words with meaning and may understand as many as 100 words

A parent’s favorite…

PLAY• Infancy
– Activities are primarily narcissistic and revolves around their own body.
– Body parts are primarily objects of play and pleasure (think of Freud).
• 6 months to 1 year– Play involves sensorimotor skills. – Actual games such as peekaboo and pat-a-cake – Play is much more selective, not only in terms of
specific toys but also in terms of “playmates.”

• Stimulation is as important for psychosocial growth as food is for physical growth
• It is NOT sufficient to place a mobile over a crib and toys in a playpen for a child’s optimum social, emotional, and intellectual development

Solitary Play


Parallel Play



Appropriate Appropriate Developmental ToysDevelopmental Toys
Appropriate Appropriate Developmental ToysDevelopmental Toys
See Hand-Out!

TOYS• The types of toys given to the
child is much less important than the quality of personal interaction that occurs (i.e box).
• Always remember growth and development in terms of SAFETY!

Developmental Developmental AssessmentAssessment
Developmental Developmental AssessmentAssessment
Denver IIDenver II

Denver II

• Importance of distinguishing between DEVELOPMENTAL SCREENING (i.e. Denver II), and
• IQ test (Stanford-Binet)

Screening Procedures• Designed to identify quickly and reliably those
children whose developmental level is below normal for their age and who therefore may require further investigation
• Since the passage of P.L. 99-457, the Education of the Handicapped Act Amendment of 1986, much greater emphasis has been placed on developmental assessment of children with disabilities
• Nurses play a vital role in providing this service

Denver II• Denver Developmental Screening
Test (DDST) and its revision, the DDST-R have been revised, re standardized, and renamed the Denver II
• Before administering the Denver II, the examiner should be trained by and receive a certificate from a master instructor who has been trained by the Denver faculty

• Each item was evaluated to determine if significant differences exist on the basis of sex, ethnic group, maternal education, and place of residence
• When evaluating children who are delayed on one of these items, the examiner can look up norms for the subpopulations to consider if the delay may be caused by socio cultural or environmental differences
• Soap box: “Would we question the test?”

Testing• Adjusted age:
– Prior to the test, prematurely born children should be identified.
– Up to 24 months of age, allowances are made for prematurely born children by subtracting the number of weeks of missed gestation from their present age and testing them at adjusted age.

• Emphasize that the child is not expected to perform each item on the test
• It is the nurse’s responsibility to properly inform parents about any testing or screening procedure before its administration so that they are fully aware of its purpose and intent
• Prepare toddlers and preschoolers for the procedure by presenting it as a game

Categories tested• Personal-Social: getting along with
people and caring for personal needs• Fine Motor-Adaptive: eye-hand
coordination, manipulation of small objects and problem-solving
• Language: hearing, understanding and using language
• Gross Motor: sitting, walking, jumping, and overall large muscle movement

• Perform each item quickly and present only one toy from the kit at a time since children are easily distracted
• Temporary factors that may interfere with the child’s performance include:– Fatigue– Illness– Fear– Hospitalization– separation from the parent– general unwillingness to perform the activity

• In each sector, administer– 3 items nearest to and LEFT of the
age line– All items on (intersecting) the age
line– Continue until 3 “fails” occur (of
items)

• Following completion of the Denver II:– Ask the parent if the child’s performance
was typical of behavior at other times. – If it was not typical of usual behavior, it is
best to defer any scoring or discussion of results.
– The test should be rescheduled for a time when the child is more likely to cooperate

Denver II Scoring• Interpretation of Denver II scoring: (See Denver II
test booklet) 1) Advanced: Passed an item completely to the right of the age line (passed by fewer than 25% of children at an older than the child) 2) OK: Passed, failed, or refused an item intersected by the age line between the 25th and 75th percentiles 3) Caution: Failed or refused items intersected by the age line on or between the 75th and 90th percentiles 4) Delay: Failed an item completely to the left of the age line; refusals to the left of the age line may also be considered delays, because the reason for the refusal may be inability to perform the task

• Interpretation of test:
– Normal = No delays and a maximum of one caution
– Suspect = One or more delays and/or two or more cautions
– Untestable = Refusals on one or more items completely to the left of the age line or on more than one item intersected by the age line in the 75th to 90th percentile area

• Recommendations for referral (suspect & untestable:
• Re screen in 1-2 weeks to rule out temporary factors.
• If re screen is suspect or untestable, use clinical judgment based on the following:– number of cautions and delays– which item are cautions and delays– rate of past development– clinical examination and history– availability of referral sources (in community)

Delays• In explaining delays, carefully note the parent’s
response, especially indications of casual acceptance, such as “He’ll catch up,” or questions such as, “Does this mean my child is retarded?”
• Be aware of personal anxieties during these situations and refrain from giving reassurances such as “I’m sure he will do better the next time.” Instead, respond to parents’ questions honestly yet with appropriate flexibility and concern and stress the need for further developmental testing.

HEALTH PROMOTION HEALTH PROMOTION DURING INFANCYDURING INFANCY
HEALTH PROMOTION HEALTH PROMOTION DURING INFANCYDURING INFANCY

Teething• Eruption of the deciduous (primary
teeth); a very difficult period in the infant’s and parents’ life
• The age of tooth eruption shows considerable variation among children, but the order of their appearance is fairly regular and predictable


• Teething is a physiologic process; some discomfort is common as the crown of the tooth breaks through the periodontal membrane (pain is “remembered”).
• Varity in symptoms ranging from none to:– Drooling– Increased finger-sucking – Biting on hard objects– Irritability– Difficulty sleeping– Low grade fevers– Ear-rubbing– Decreased appetite for solid foods– Loose stools


Nutrition•First 6 months:
– Human milk is the most desirable complete diet for the infant during the first 6 months
– Iron by 4-6 months of age (when fetal stores are depleted).
– Breast-or bottle-fed infants do not require any additional fluids, especially water or juice, or solids during the first 4-6 months of life.

• FOODS TO AVOID BEFORE AGE 1 YEAR:– Honey: Risk of botulism (food
poisoning by Clostridium Botulinum– Whole milk (prior to age 1 year) can
cause iron deficiency anemia in infants
– Eggs = increase in allergic reaction– Strawberries = increase in alergic
reaction

Introducing Solid Foods

• Second 6 months:– Human milk or formula continues to be the primary
source of nutrition– Solid foods added: physiologically and
developmentally ready– Extrusion (protrusion reflex) disappears– GI tract has matured sufficiently to handle more
complex nutrition– Tooth eruption facilitates biting and chewing– Head control is well developed– Voluntary grasping and improved eye-hand
coordination allows the infant to pick up certain finger-foods and feed themselves


Selection of Solid Foods
In the correct order
• 1) CEREAL (rice)• 2) GREEN VEGETABLES• 3) YELLOW VEGETABLES• 4) FRUIT• 5) MEAT
Immunizations• Immunization = Inclusive term denoting the process of
inducting or providing active or passive immunity artificially by administering an immunobiologic Use vaccines.
• Active immunity = Immune bodies are actively formed against specific antigens, naturally by having had the disease or artificially by getting the vaccine
• Passive immunity = Temporary immunity by transfusing immune globulins or antitoxins either artificially from another human or from an animal that has been actively immunized against an antigen or naturally from the mother to the fetus via the placenta
• Acquired immunity = (Part of the “active immunity” category) Immunity from exposure to the invading agent, either bacteria, virus, or toxin.
• Vaccination = Originally meant inoculation with vaccinia smallpox virus to make a person immune to smallpox; currently denotes physical act of administering any vaccine or toxoid

Injury Prevention• Injuries are a major cause of death during
infancy, especially for children 6-12 months old
• Asphyxiation by foreign material in the respiratory tract, combined with mechanical suffocation, is one of the leading causes of fatal injury in children younger than 1 year.
• Food items are the second most common cause of aspiration. Small toys/items is the #1 cause.
• The size, shape, and consistency of foods or objects are important determinants of fatal obstruction, i.e. cut them into irregular shapes


Nurse’s Role in Injury Prevention
• Nurses must be aware of the possible causes of injury in each age-group in order for anticipatory preventive teaching to occur (see hand-out of anticipatory guidance)
• Preventive teaching ideally occurs during pregnancy (i.e. car-seats, child-proofing house)
• 2/3 of all injuries to children occur in the home and the importance of safety is crucial.


NEXT LAB NEXT LAB ……………………
NEXT LAB NEXT LAB ……………………

Growth & Growth & DevelopmentDevelopment
Growth & Growth & DevelopmentDevelopment
Infant, Infant, Toddler Through School AgeToddler Through School Age

Toddler (1-3 years)• Erikson: Autonomy versus doubt and shame
• Positive resolution: – Self control is learned and the extent to
which the environment can be influenced by direct manipulation
• Negative resolution: – Compulsive self-restraint or compliance.
The child becomes will-full and defiant

Pre-school (3-5 years)• Erikson: Initiative versus guilt
– Positive resolution: Learning the extent to which assertiveness and purpose will influence the environment. It is the beginning ability to evaluate one’s own behavior.
– Negative resolution: Lack of self-confidence and fear of wrong-doing

School-age child (6-12 years)
• Erikson: Industry versus inferiority– Positive resolution: The child achieve a
sense of accomplishment. Learning to use energies to create, develop and manipulate.
– Negative resolution: Disappointment in own abilities, loss of hope and a sense of inadequacy.

Adolescence
• Erikson: Identity versus role diffusion– Positive resolution: Integration of life
experiences into a coherent sense of self. One plans for actualizing one’s ability.
– Negative resolution: Doubt about sexual identity and ability to find an occupational identity. Also personality confusion.

Issues Related to the
Hospitalized Child

PAINPAINPAINPAIN
PAINFacts about Pain in Infants and Children:
Infants, regardless of age, feel pain. The youngest premature infant has the anatomic and physiologic components to perceive pain or “nociception” and demonstrates a severe stress response to painful stimuli.

Operational Definition of Pain
“Pain is whatever the experiencing person says it is, existing whenever he says it does.”
BELIEVE THE PATIENT! McCaffery and Pasero: Pain: Clinical Manual,
(1999).
Children Do Not Tolerate Pain Better Than Adults
• Children’s tolerance to pain actually INCREASES with age.

Children Can Tell You Where They Hurt
• Children beyond infancy can accurately point to the body area or mark the painful site on a drawing; children as young as 3 years can use pain scales.

Children Do Not Always Tell The Truth About Pain
• Children may not admit having pain to avoid an injection
QUESTT• Question the patient
• Use pain rating scale
• Evaluate behavior and physiologic signs
• Secure family’s involvement
• Take cause of pain into account
• Take action and assess effectiveness

Question the ChildVerbal Indications of Pain
• Much less common than in adults• May not understand term “pain”
(owie, boo-boo, ouch, hurt, ow ow) – Other languages!
• May speak globally, such as “I don’t feel good”
• Cries, screams, groans, moans

Have Child Locate Pain by:
• Marking body parts on a human figure drawing
• Point to area with one finger on self, doll, stuffed animal
• Point to “where mommy or daddy would put a bandage”

Use diagram to have child locate pain

Burn patient’s drawing

Use Pain Rating Scale
• In 2001 Joint Commission on Accreditation of Healthcare Organizations (JCAHO) published Pain Standards
• One of the standards is to make pain rating the 5th vital sign.

Use Pain Rating Scale
• Select a scale that is suitable for the child’s age, abilities, and preferences
• Teach child to use scale before pain is expected, such as preoperatively
• Use same scale with child
• Ask child about acceptable or functional pain level

Types of Pain Rating Scales
• Numbers
• Visual analogue
• Words
• Colors
• Faces
• Behavior/physiologic
signs

No Pain Worst Pain
0 1 2 3 4 5 6 7 8 9 10
Numeric Scale

No Pain Mild Moderate Severe Very Severe Worst
Simple Descriptive Scale

No Pain Worst Pain
Visual-Analogue Scale*
Usually 0-10 cm long line.Placed either vertical or horizontal.

VAS: Coloured Analogue Scale(Ref: McGrath, PA, et al: Pain, 1996.)

Wong-Baker FACES Pain Rating Scale
0 2 4 6 8 10

Child’s FACES Pain Rating Scale

Child’s FACES and Body Outline
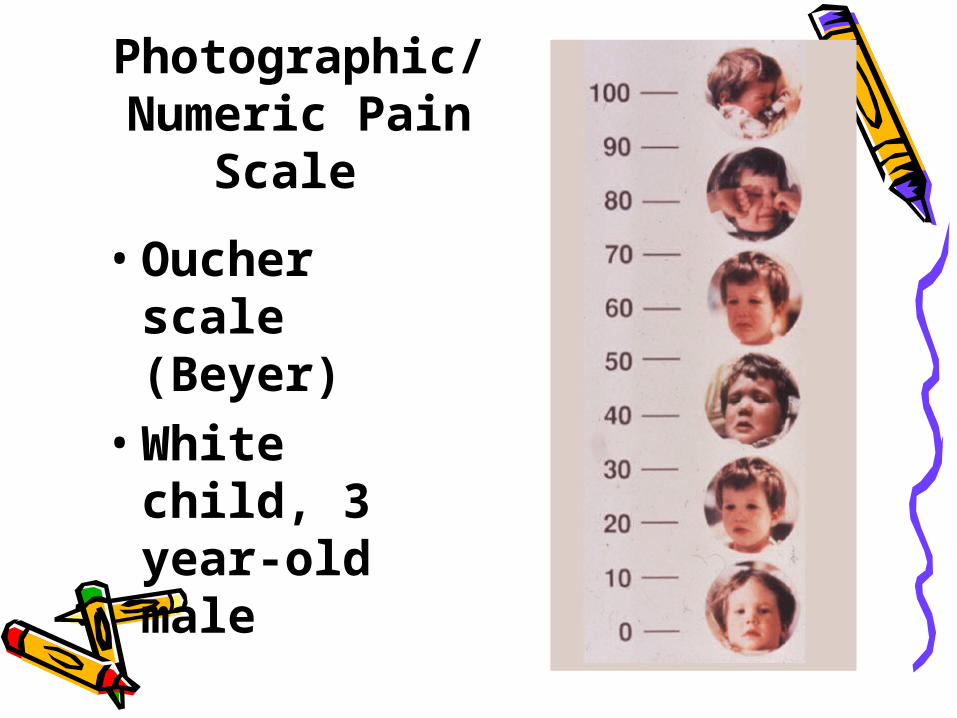
• Oucher scale (Beyer)
• White child, 3 year-old male
Photographic/Numeric Pain
Scale

• Oucher scale (Beyer)
• Black child, school age, male
Photographic/Numeric Pain Scale, cont.

Observe for Improvement in Behavior Following an Analgesic

Observe for Improvement in Behavior Following an Analgesic

The Golden Rule
What is painful to an adult is painful to an infant and child
unless proven otherwise.

PROCEDURES: Preparing the child
• Parental presence and support:– Presence = controversial! In regards to ROLE of parent.– The presence of a parent/caregiver during a procedure is
“usually” beneficial. • Involve the child as much as possible. Permitting them
to make choices whenever possible will give them some measure of control. (examples)
• Provide distraction – especially during painful procedures
• Allow expression of feelings: Anxiety, fear, frustration, crying etc.
• Use play in procedures• When to prepare:
– Growth and development

Questions, Comments, Concerns???