head and neck 2 week wait referral - gpvts. · pdf filehead and neck 2 week wait referral...
TRANSCRIPT

Head and Neck 2 week wait referral
Richard Gracie
Lee Cooper

Aims
1. List the 2WW referral criteria for suspected head and neck cancer
2. Develop a differential diagnosis for cases of suspected head and neck cancer
3. Apply the criteria to clinical cases
4. Take into account patient risk factors
5. Know when to refer
6. Make a referral using the referral form
Introduction
• 15% GP consultations involve upper respiratory tract or head and neck
• Wide range of symptoms and conditions
– Minor to life threatening
• Minimal exposure to ENT as students/juniors
• How do you know what is serious?

Could it be Cancer?
• Hoarseness
• FB sensation in throat
• Epistaxis
• Otalgia
• Rhinorrhoea
• Hearing Loss
• Neck Lump
• Dysphagia
• Laryngitis
• Globus
• Anti-coagulants
• Otitis Media
• Allergy
• Age Related

How common is Head and Neck Cancer?
Type Incidence (cases/year)
Laryngeal 2360
Oral 6767
Tyroid 2727
Lung 44,488
Colorectal 41,581
http://www.cancerresearchuk.org/health-professional/cancer-statistics

GROUP WORK

1. What else would you like to know from the history and examination
2. What is your list of differential diagnoses
3. What would make you worry, and what would re-assure you?
4. Would you refer as a 2WW?

Case 1
• 45 year old female
• 6 weeks of hoarseness

History
• Onset, duration, progression
• Phonotrauma
• Reflux symptoms
• Recent/recurrent URTI
• Previous surgery
• Drugs – Steroid inhalers, ACEi
• Smoking
• Alcohol

Differential Diagnosis
• Muscle tension dysphonia
• Laryngitis
– Acute laryngitis
– Chronic laryngitis
– Reflux laryngitis
• Vocal fold nodule/cyst/polyp
• Vocal fold paralysis
• Leukoplakia
• Laryngeal Cancer

Polyp Reflux Laryngitis
Cancer

Laryngeal Cancer
• 25% of head and neck cancers
• M:F 4:1
• Risk Factors
– Smoking
– Alcohol
– Radiotherapy
– FH
– GORD (weak)

What does NICE say?
• Consider a suspected cancer pathway referral for laryngeal cancer in people aged 45 and over with
– persistent unexplained hoarseness
– or an unexplained lump in the neck
• Local referral criteria
– Hoarseness >3 weeks

ENT assessment
• FNE
• CT neck
• CT chest
• Biopsy

Case 2
42 year old lady presents with a swelling low down in the front of her neck .

Case 2
History • The lump - Where, how long, how big, getting
bigger, painful, one lump?
• Compressive symptoms - Swallowing or breathing difficulties
• Thyroid symptoms- most will be euthyroid
• Nerve palsy - hoarseness
• Smoker, drinker and family history of thyroid problems

Case 2
Differential • Reactive lymph node
• Autoimmune and inflammatory/infective
• Sebaceous cyst
• Benign disease, adenomas, multi-nodular, cysts.
• Thyroid cancer
• Lymphoma

Case 2
What would make you worry? • Rapidly increasing size
• Recurrent laryngeal nerve palsy
• Previous neck irradiation
• Extreme of age
• Compressive symptoms - Breathing/swallowing difficulties
• Smoker, drinker, positive family history for thyroid cancer/disease.

Case 2
Gloucestershire A thyroid swelling associated with any of, 1) Solitary nodule increasing in size 2) History of neck irradiation 3) Family history of endocrine tumour 4) Unexplained hoarseness or voice change 5) Pre-pubertal patient 6) Age 65 or over
NICE Consider a suspected cancer pathway referral (for an appointment within 2 weeks) for thyroid cancer in people with an unexplained thyroid lump
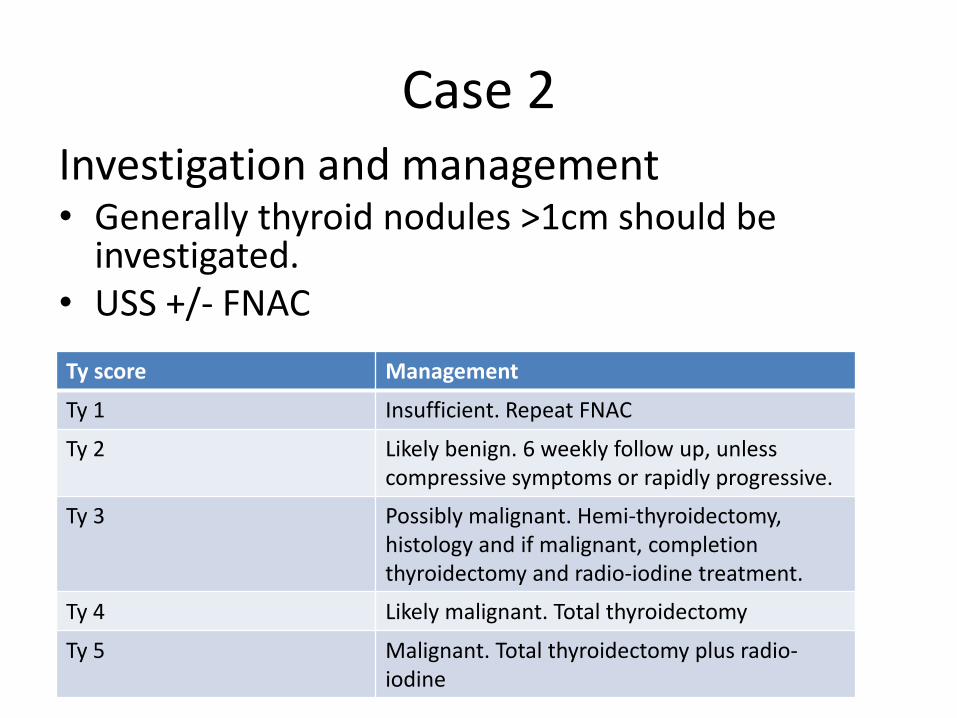
Case 2 Investigation and management • Generally thyroid nodules >1cm should be
investigated. • USS +/- FNAC
Ty score Management
Ty 1 Insufficient. Repeat FNAC
Ty 2 Likely benign. 6 weekly follow up, unless compressive symptoms or rapidly progressive.
Ty 3 Possibly malignant. Hemi-thyroidectomy, histology and if malignant, completion thyroidectomy and radio-iodine treatment.
Ty 4 Likely malignant. Total thyroidectomy
Ty 5 Malignant. Total thyroidectomy plus radio-iodine

Case 2
5% chance of malignancy in a solitary nodule.
Types
• Epithelial - Papillary and follicular
• Poorly differentiated - Anaplastic
• Medullary - Calcitonin producing C-cells
• Others – SCC, sarcoma, lymphoma

Case 3
• 76 year old lady presents with swelling over the left cheek, and left facial droop

Case 3
History • The lump - Where, when, how long, rapidly
increasing, single lump, any others
• Infective symptoms - erythema, fevers, discharge in the mouth, punctum, is it painful
• Sialadenitis, sialolithiasis
• Nerve Palsy - Facial nerve
• Smoker, drinker family history

Case 3
Differential • Sialolithiasis
• Parotiditis
• Tumour Benign - Pleomorphic adenoma and Warthins
• Malignant – Many different types based on histology and grade.
Case 3
What would make you worry?
• Rapidly progressing mass in an elderly smoker with evidence of facial nerve palsy.

Case 3
Gloucestershire
• Swelling in the parotid or submandibular gland
NICE
?

Case 3
Investigation and management • USS and FNAC – 85% accurate
• CT scan to elucidate extent
• Benign 80% - Surgical excision
• Malignant – Surgical excision plus Chemo/radiotherapy

Case 4
• 62 year old man presenting with persistent right sided neck pain.

Case 4
History • Level of the pain - low middle or high. • Associated mass • Odynophagia and dysphagia. • Pain all the time • Stridor or SOB • Concurrent infective symptoms • Recurrent tonsillitis. • Smoker/drinker positive family history. • Trauma, previous surgery, head and neck irradiation

Case 4
Differential • Tumour
• Tonsillitis/quinsy/pharyngitis
• Neck space abscess
• Reactive lymph node
• Globus
• Foreign body

Case 4
What would make you worry • Unilateral persistent tonsillar swelling
• Persistent pain
• Associated mass
• Cranial nerve involvement i.e. glossopharyngeal leading to referred otalgia.
• Smoker drinker, family history, elderly.

Case 4
Gloucestershire
• Unilateral unexplained pain in the head and neck > 4weeks associated with otalgia and normal otoscopy.
NICE
?

Case 4
Investigation and management • FNE • CT, MRI • Examination under anaesthetic +/- biopsy, • PET
SCC most common pharyngeal malignancy • Surgery depending on site a multitude of surgical approaches. • Around the pharynx generally pharyngectomy and neck dissection. • Post nasal space and sinuses including FESS depending on stage, maxilla-
facial surgery • Radiotherapy.

NICE guidelines (NG12)
Laryngeal cancer • People aged 45 and over with:
– persistent unexplained hoarseness or – an unexplained lump in the neck.
Oral cancer • Unexplained ulceration in the oral cavity lasting for more than 3 weeks or • Persistent and unexplained lump in the neck. • Dental referral for
– a lump on the lip or in the oral cavity or – a red or red and white patch in the oral cavity consistent with erythroplakia or
erythroleukoplakia. – a lump on the lip or in the oral cavity consistent with oral cancer or
Thyroid cancer • Unexplained thyroid lump
Local policy
• Hoarseness >3 weeks
• Stridor
• Swelling in parotid/submandibular gland
• Persistent red and white patches of the oral mucosa
• Unexplained tooth mobility >3 weeks
• Unexplained persitant sore throat
• Progressive mouth, throat ulceration
• Persistent oral swelling/ulcer > 3 weeks
• Unilateral, unexplained pain in head >4 weeks, with otaligia and normal otoscopy
• Thyroid swelling with any of:
– Solitary nodule increasing in size
– History of neck irradiation
– FH of endocrine tumour
– Unexplained hoarseness/voice change
– Very young (pre-pubertal)
– > 65 years old

Conclusion
• Will see lots of ENT problems
• Head and neck cancer is rare but serious