health, mortality, and longevity in china today
TRANSCRIPT

1
Health, Mortality, and Longevity in China Today
Presented at the XXVI IUSSP International Population Conference,
Marrakech, Morocco, September 2009
Judith Banister
The Conference Board
Executive Summary This paper on China health and mortality updates analysis of mortality levels, trends, and differentials through the 2005 by-census. Expectation of life at birth for China as a whole has risen further from the already-impressive level of 71 years achieved by 2000. During 2000-2005, infant and young child mortality rates declined greatly. Mortality rates continued dropping for females at all ages; maternal mortality was much reduced. Male death rates also declined in childhood and at ages 40+. But age-specific death rates rose slightly for men in the young working ages. The paper explores why. This paper also studies differentials in health status and health insurance coverage by urban or rural residence and by economic level. Poverty, inequality, and education statistics are updated; relationships with health and mortality differentials are assessed. The author discusses how China’s economy and businesses are affected by the evolving health insurance systems, changing health conditions, and mortality trends. The foundations of China’s strong showing today regarding survival and health of the population and workforce were laid down in the Maoist period 1949-1978. During the economic reform period since then, life expectancy has continued to increase, death rates have declined further, and health conditions (though more difficult to measure than mortality) have apparently continued to improve. The population has become more literate and numerate, and levels of education have steadily increased, factors that directly and indirectly contribute to improved health and survival of the total population and of the workers. The quality of China’s population has improved in step with the nation’s rapid economic development over the last three decades. Real economic growth of around 10 percent a year has raised consumption and living standards, driven down poverty levels, and helped pay the costs of improving survival and health and educating the population. By allowing the market to function more freely over time, the government has helped set the stage for the great economic and social progress that has taken place. Copyright 2009 Judith Banister [email protected]

2
The aggregate picture is favorable. Yet China is a vast country with major differences from place to place. Most available information shows that even the poorest places in China have gained in living standards, poverty decline, survival, health, literacy, and education. At the same time, disparities have widened between the most successful and the least successful regions, communities, families, and individuals. Today the people of China are enjoying the fruits of the country’s extraordinary economic, social, and demographic development over the last six decades. Challenges today include trying to further raise population and labor force quality to higher levels, and coping with the perceived unfairness of uneven development in order to make China a more harmonious society. This report gives an overview of the most recent three decades, highlighting the greatly improved food supply, reduced malnutrition and hunger, and significant mortality declines. Life expectancy increased from 60 years in the 1970s to about 74 years today. Survival gains have been strong everywhere in China, especially in the poorest counties and provinces from the 1970s to 2000. Since 2000, mortality decline has continued for females at all ages, for boys below the mid-teens, and for men ages 40 and older. But age-specific death rates stabilized or rose slightly for men in the young working ages 15-39. The report analyzes the likely causes of this break from the previous trends. This study focuses also on survival and health differentials between urban and rural China, in the context of continuing poverty and rising urban-rural inequality. Government initiatives to counteract continuing rural and urban poverty and to promote basic education in rural areas are noted. The report traces the collapse of rural medical insurance coverage and the reduced health insurance coverage in the cities during the economic reform period. Recent government policies to reinstitute a Rural Cooperative Medical Scheme are discussed. This report documents development of basic medical insurance systems for urban employees and other urban residents, and describes how these systems work. In addition to analysis of survival trends and causes of death, this study also reports the most recent data on the rates and causes of illness and disability in large and medium-sized cities, small cities, and rural areas.
3
Background
A population with good survival chances and reasonably robust health strengthens the economy. Investments in education, training, and health are not lost if children and then workers survive through the working ages and well into their sixties and seventies at least. Low rates of illness and disability of workers and their family members keep employees and laborers on the job and contribute to worker productivity.
China has unusually low mortality—death rates—for a developing economy, especially in comparison to poor developing countries in South Asia, Southeast Asia, and Africa. During the Maoist era from 1949 to the late 1970s, China’s government attempted to provide very basic health insurance coverage and access to preventive health care and curative medical treatment for the great majority of the people. By the mid-1970s, even though China’s village and city populations were still living at near-subsistence levels, life expectancy of the nation’s population had already reached about 60 years.1 This was far better than would have been expected given the rock-bottom living standards of the time. But city populations, who constituted only one-fifth of the population at that time, had a strong survival advantage compared to the rural majority.
After Mao’s death, China’s new government under Deng Xiaoping began in 1978 to
abandon the Marxist command economy and introduce market elements. In the early 1980s the government almost completely dismantled collective agriculture and gave farmers the right to grow crops on their assigned plots of land and to sell their surplus. In only 8 years from 1978 to 1986, China’s total agricultural output more than doubled, increasing by 118 percent in constant prices.2 As a result, the previous situation of widespread constant hunger of the majority of the population in the countryside and in urban areas greatly diminished, and poverty rates dropped steeply all over China.
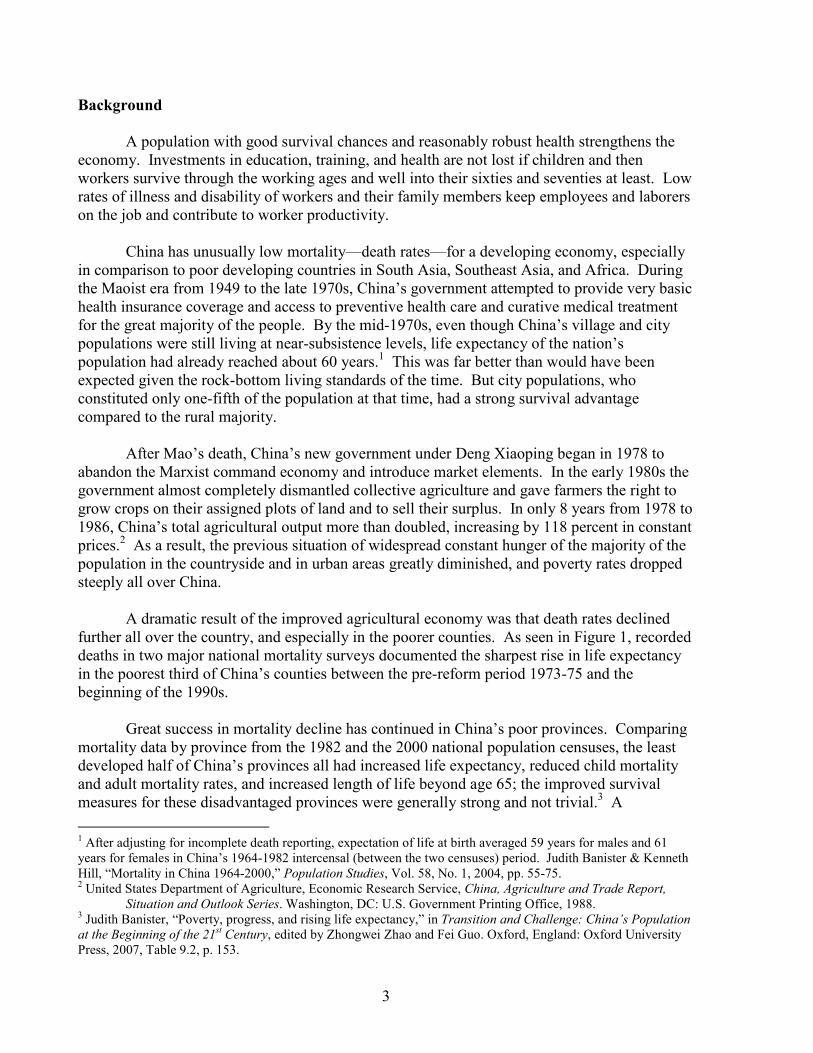
A dramatic result of the improved agricultural economy was that death rates declined
further all over the country, and especially in the poorer counties. As seen in Figure 1, recorded deaths in two major national mortality surveys documented the sharpest rise in life expectancy in the poorest third of China’s counties between the pre-reform period 1973-75 and the beginning of the 1990s. Great success in mortality decline has continued in China’s poor provinces. Comparing mortality data by province from the 1982 and the 2000 national population censuses, the least developed half of China’s provinces all had increased life expectancy, reduced child mortality and adult mortality rates, and increased length of life beyond age 65; the improved survival measures for these disadvantaged provinces were generally strong and not trivial.3 A
1 After adjusting for incomplete death reporting, expectation of life at birth averaged 59 years for males and 61 years for females in China’s 1964-1982 intercensal (between the two censuses) period. Judith Banister & Kenneth Hill, “Mortality in China 1964-2000,” Population Studies, Vol. 58, No. 1, 2004, pp. 55-75. 2 United States Department of Agriculture, Economic Research Service, China, Agriculture and Trade Report,
Situation and Outlook Series. Washington, DC: U.S. Government Printing Office, 1988. 3 Judith Banister, “Poverty, progress, and rising life expectancy,” in Transition and Challenge: China’s Population at the Beginning of the 21
st Century, edited by Zhongwei Zhao and Fei Guo. Oxford, England: Oxford University
Press, 2007, Table 9.2, p. 153.

4
sophisticated province-level analysis of mortality and survival patterns and trends from the 1990 to the 2000 census showed that “the largest improvements in mortality were experienced by the most backward provinces (Qinghai, Xinjiang, Sichuan, Ningxia, and Tibet).”4
Figure 1. China, Mortality Surveys, 1973-75 and 1990-92
Expectation of Life at Birth by Economic Level
56
58
60
62
64
66
68
70
72
74
76
1973-75 1990-92
Year
Expectation of Life at Birth
Poorer Middle Richer Urban
Notes: Calculated from 1973-75 and 1990-92 mortality data collected in the same whole counties and city districts covering 10 percent of China’s population; mortality surveys conducted by China’s Ministry of Health. Deaths have not been adjusted for underreporting; therefore, the life expectancies calculated from the collected data are higher than the true levels. Source: Judith Banister, Jun Gao, and Keqin Rao, “Survival and health in rapidly developing China,” presented at the Annual Meeting of the Population Association of America, Los Angeles, Mar. 2000.
4 Simona Bignami-Van Assche, “Province-specific mortality in China, 1990-2000,” presented at the annual meeting of the Population Association of America, Philadelphia, Mar.-Apr. 2005, p. 22.

5
Urbanization From the late 1980s to today, China has engineered a step-by-step transformation of the industrial and service economy from the command economy toward market socialism. Migration from rural to urban areas, which had been tightly restricted, has gradually been more tolerated. Even though fertility rates are much lower in urban than rural China, the urban population has been growing at 4-5 percent a year since 1978. Today, China’s population is officially 46 percent urban and 54 percent rural.5 Within the urban population, the national 1% sample population survey of 2005 reported that 62 percent of the urban population was in cities, which means that China’s city population is about 375 million today, and the population in urban towns (zhen) totals around 232 million.6 Meanwhile, as shown in Figure 2, China’s rural population has been dropping in absolute size since it peaked at 859 million in 1995, and now the rural total has declined to 721 million. Movement of workers from the villages to cities and towns has supplied the laborers needed to staff the explosive growth of China’s modern economy.
Source: China National Bureau of Statistics
5 China National Bureau of Statistics, China Statistical Abstract 2009. Beijing: China Statistics Press, 2009, p. 38. 6 China National Bureau of Statistics, 2005 National 1% Sample Survey Data. Beijing: China Statistics Press, 2007; China NBS CEIC database.

6
China National Mortality Trends
China has now experienced three decades of economic reform since 1978. During these decades, the national government has followed the policy of withdrawing from many of the spheres of the economy and of people’s lives that it had tried to micromanage in the pre-reform period. This disengagement has been extraordinarily beneficial to the economy. With markets functioning much more than before, and with the economy privatizing, official data show that China’s GDP has grown an average of 9.8 percent a year, and the per capita GDP has grown about 9 percent a year on average during 1978-2008.7 In these decades, China’s economy has been one of the fastest growing economies in the world. Not so beneficial has been the Chinese government’s withdrawal from the health and medical insurance system. In the 1980s, with the dismantling of agricultural collectives, China’s government also allowed the rural health insurance system to collapse. Since the 1980s, the government has also cut back on providing medical insurance in the cities. According to China’s 2003 National Health Services Survey, about 45 percent of the country’s urban population and almost 80 percent of the rural population as of that year had no medical insurance. Even in urban areas, coverage of social health and medical insurance declined during 1993-2003. For the urban poor, the coverage rate for the bottom quintile urban income group dropped from 37 percent to only 12 percent in that decade.8 Because of poor or nonexistent health insurance coverage and the high costs of medical care, especially for serious or catastrophic health problems, the people of China save as much money as possible against such medical contingencies: “A McKinsey survey indicates that the top two reasons for high savings rates in China are concerns about health care and retirement.”9 One way for China to lessen its dependence on export-led economic growth is to encourage greater domestic consumption, which has been an emphasis of government policy for some years. The New York Times describes the need this way:
Beijing must ease the emphasis on manufacturing exports and do more to expand domestic consumption. To start, it could spend a much larger share of its revenues on the threadbare systems of public health, education and pensions. The lack of an effective social safety net, which encourages the Chinese to save to the hilt, is one of the reasons China’s share of consumer spending is among the lowest in the world.10
7 China NBS, China Statistical Yearbook 2008, p. 41; China Statistical Abstract 2009, p. 12. 8 World Health Organization, Office of the WHO Representative in China, and China State Council, Development Research Center (DRC), Social Development Department, China: Health, Poverty, and Economic Development. Beijing: June 2006, p. 17. 9 Kevin P. Lane and Ian St-Maurice, “The Chinese consumer: To spend or to save?” The McKinsey Quarterly, 2006 No. 1, pp. 6-8 (www.mckinseyquarterly.com/links/21991); Diana Farrell, Ulrich A. Gersch, and Elizabeth Stephenson, “The value of China’s emerging middle class,” The McKinsey Quarterly, 2006, p. 66 (www.mckinseyquarterly.com/links/22060). 10 “Editorial: China’s economic puzzle,” New York Times, Oct. 19, 2007.

7
Despite China’s poor medical insurance coverage during most of the economic reform period, survival chances have improved and mortality rates have declined for the country’s population as a whole. Until 2000, the best national mortality data, both before and after adjustments for incomplete death reporting, showed that death rates dropped continually for both sexes and for every age group, except for a possible rise in the infant mortality rate for girls in the 1990s caused by strong cultural discrimination against baby daughters when the fertility level is low.11 By the year 2000, expectation of life at birth for China was 69 years for males and 72 years for females, averaging about 70.6 years for the population as a whole.12 Why did mortality continue to decline in China, in spite of the government cutbacks in provision of medical insurance to the rural and urban populations since 1978? The main reasons have been the fabulous and sustained economic growth, along with steep declines in poverty, as well as reduced illiteracy and greatly increased educational attainment of the population.13 Education and literacy and greater financial resources all give people more options in their lives to improve their living environments, to fight illness, and to learn how to care for themselves and their children in ways that improve survival chances. The cutback in medical insurance coverage along with greater financial resources in urban and even rural households has caused this shift in household expenditures: The percent of household expenditures devoted to health care and medical services rose in the cities from 2.0 percent in 1990 to 7.0 percent in 2007, and in the villages from 3.3 percent in 1990 to 6.5 percent in 2007.14 McKinsey projects further increases in medical expenditures by urban families in particular:
Given the importance of health care to Chinese families, the country’s rapidly aging population, and the challenges facing the public health care system, we project that private health expenditures by urban consumers will grow at a rate of more than 11 percent annually over the next two decades. This increase in spending will create significant opportunities for health care providers, insurance companies, medical-equipment manufacturers, and pharmaceutical companies.15
The abandonment of collective agriculture and return to the family farm have been crucial during the economic reform period. Vastly increased food supply and much greater variety of foods have slashed hunger and undernutrition in China. A global study published in the British medical and health journal The Lancet contrasts China with most developing regions of the world:
But the study also pays tribute to China, saying it had achieved “a dramatic reduction” in hunger and undernourishment thanks to the economic reforms, initiated in 1978, that
11 Banister and Hill, “Mortality in China 1964-2000.” 12 Judith Banister, “Poverty, progress, and rising life expectancy,” in Transition and Challenge: China’s Population at the Beginning of the 21
st Century, edited by Zhongwei Zhao and Fei Guo. Oxford, England: Oxford
University Press, p. 146. 13 Judith Banister and Xiaobo Zhang, “China, economic development and mortality decline,” World Development, Vol. 33, No. 1, 2005, pp. 21-41. 14 China NBS, China Statistical Yearbook 2008, pp. 319, 343. 15 Farrell, Girsch, and Stephenson, 2006, pp. 66-67.

8
helped boost agricultural production and spurred economic growth. “In 1990-2, the number of undernourished people in China was 194 million, or 16 percent of the population, whereas in 2001-3, it was 150 million, or 12 percent, and the country is well on track for meeting the Millennium targets” on health and mortality set by the United Nations.16
Though survival improvement has been happening everywhere in China, the urban-rural gap remains large. As of the 2000 population census, the expectation of life at birth was almost six years more in urban than in rural China. The urban-rural disparity in life expectancy in the less developed western provinces of China is also much greater than in the far more developed eastern provinces.17 In addition, there is still some hunger and malnutrition in the poorest counties of China. If children are underweight for their age by more than a minimal degree, this is evidence that poor nutrition or food shortage persists. The World Health Organization estimated that in China as a whole, 10 percent of children under age 5 were underweight for their age in 2000; and in poor rural areas the proportion exceeded 20 percent.18
Poverty in China Estimates of the percent of China’s population living in poverty change from time to time as the World Bank re-estimates the purchasing power parity (PPP) of the Chinese currency compared to the US dollar, but the general trend is not in doubt. Looking first at the trend, China has seen a steep decline in poverty during the economic reform period. Until the end of 2007, when new estimates of China’s PPP were released, the World Bank’s estimates of China’s poverty levels and trends were as follows: Using the international standard measure of poverty as living on less than $1 per person per day measured at purchasing power parity, the World Bank previously estimated that in 1981, just after the beginning of economic reforms, 64 percent of China’s population was living in poverty. In only six years, by 1987, because of the near-complete abandonment of collective agriculture, the poverty proportion of China’s population was estimated to have dropped to 30 percent. Then from 1990 to 2004, China’s poverty rate had reportedly declined from about 30 percent to 10 percent of the total population.19 Most of this decline in poverty can be credited to the fact that China’s rapid economic growth has brought at least some measurable benefit to almost all areas of China and almost all subgroups in the population.
16 Agence France Presse, “Undernutrition kills 3.5 million children a year: researchers,” Yahoo News, Jan. 17, 2008. 17 UNDP, 2005, p. 9. 18 World Health Organization, The World Health Report 2004. Geneva: WHO; Rao Keqin and Liu Yuanli, “Study of health care systems and related policies in rural China” (in Chinese), in China Ministry of Health, Research on Health Reform Issues in China, 2003. Beijing: Zhongguo Xiehe Yike Daxue Chuban She, 2004; Zhongwei Zhao, “Income inequality, unequal health care access, and mortality in China,” Population and Development Review, Vol. 32, No. 3, Sept. 2006, p. 469. 19 David Dollar, “Poverty, inequality, and social disparities during China’s economic reform,” April 2007 manuscript, p. 31.
9
Recent re-estimation of the PPP between China’s Yuan or Renminbi (RMB) currency and the US dollar resulted in a new estimate for 2004 that 26 percent of China’s total population was still living below a poverty line of US$1 per day. This was 337 million people. If the poverty line were set at two-dollars-a-day, then in 2004, 54 percent of China’s population was still living in poverty, or 699 million people.20 If China today is actually much poorer than had earlier been estimated, this implies that the levels of poverty in 1981 and 1987-1990 were also much higher than previously thought. Whatever China’s current poverty level, it is certain that China has achieved a remarkably steep decline in poverty during the economic reform period of the last three decades. Because China includes one-fifth of the total global population, a steep drop in poverty in China means that global poverty levels have simultaneously been dramatically reduced.
Literacy When the People’s Republic of China was founded in 1949, the vast majority of men and nearly all women in China were illiterate. One of the great successes of the Maoist decades was to reduce the illiteracy rate, by promoting literacy classes for adults and by providing basic primary education to more and more children over time. By the 1964 census, the percent illiterate was reduced to 34 percent of the population age 13 and older. As of the early economic reform period, the 1982 census measured 23 percent of the population age 15 and older who could not read or write Chinese. Successive censuses in China have documented further declines in illiteracy.21 The lowest illiteracy rates in China’s history were recorded in the 2000 census.
The newest information on nationwide adult illiteracy, based on China’s 2005 nationally representative 1% sample survey of the population, shows that 11 percent of China’s population ages 15 and older is illiterate (6 percent of men and 16 percent of women).22 An illiterate adult in China’s cities and towns is defined as someone who recognizes fewer than 2,000 Chinese characters, and in the countryside recognizes fewer than 1,500 characters, and who cannot read and understand a simple book or write a short sentence. In spite of the more stringent criterion for urban literacy, today only 5 percent of China’s adult city population and 8 percent in towns is illiterate, in contrast to 15 percent in rural areas.
Before the Communist period in China, illiteracy was high among China’s population, and far higher among women than men. That historical legacy can be seen in illiteracy rates for today’s population ages 65 and older, as shown in Figure 3. Each successive younger cohort in the 2005 data reflects China’s gradual and continuing success against illiteracy in the 5 ½ decades after 1949. Now only 2 percent of the population ages 20-29 and merely 1 percent of
20 Albert Keidel and Yang Zhang, personal communication, computations based on “PovCal” from the World Bank, January 24, 2008; based on World Bank, 2005 International Comparison Program; Preliminary Results; December 2007. http://web.worldbank.org/WBSITE/EXTERNAL/DATASTATISTICS/ICPEXT/0,,menuPK:1973757~pagePK:62002243~piPK:62002387~theSitePK:270065,00.html 21 China NBS, China Statistical Yearbook 2006, p. 102. 22 China NBS, 2005 National 1% Sample Survey Data, p. 185.

10
those 15-19 is illiterate, which bodes very well for the future. We now see near-convergence of illiteracy rates among young men and women, only 1.0 percent illiterate for teenage women and 0.7 percent for teen men.
Source: China 2005 1% Population Survey.
Employers in China need workers at all skill levels who are at least literate and numerate, and the more educated the better. In the cities today, illiteracy is essentially zero among young adults of both sexes in their teens and twenties. In the countryside, illiteracy has not been completely overcome among all the youth. The United Nations Development Program calculates a Human Development Index (HDI) for each country, “a weighted index of three measures: life expectancy; level of education (measured by a combination of literacy rates and combined primary, secondary, and tertiary school enrollment ratios); and level of economic development (measured by GDP per capita).”23 According to the China Development Research Foundation which reports to China’s State Council, this UNDP concept of human development is consistent with the human-oriented approach to development put forth by the Chinese government and meshes with the government’s goal of building a harmonious society.24 China’s HDI has risen continuously. According to UNDP:
23 UNDP, 2005, p. 5. 24 Ibid., p. 6.

11
Although it is still a low-income country, China’s achievements in literacy and life expectancy have placed it among the ranks of middle-income countries. China now no longer has a single province or autonomous region in the low human development category.25
Educational Attainment of the Working Age Population
Of those who got any education at all, the population’s educational attainment has improved over time. From 1978 to 2005, average years of schooling in the 15-64 age group rose from 5 to 9 years.26 As of 2002, China’s primary school enrollment rate was 11 percent higher than the average level of developing countries, and was at the same level as medium-income countries.27 By 2003, high school enrollment rates were much higher in all China’s provinces than had been the case in 1990. Table 1 shows the level of education reached by China’s adult working age population ages 15-64 in 1990, 2000, and 2005. The proportion of the population in that age group that had received any junior secondary schooling increased from 15 percent in 1978 to 33 percent in 1990 to 45 percent in 2005. By 2005, of the population ages 15-64, 16 percent had received some senior high school or specialty high school education, 5 percent had gone to a technical or professional college, 2 percent had attended university, and 0.2 percent had gone to graduate school. Those with senior secondary school and higher educational attainment are concentrated in China’s cities.
25 United Nations Development Program (UNDP), China Human Development Report 2005: Towards Human
Development with Equity, prepared by the China Development Research Foundation of the People’s Republic of China State Council Development Research Center (DRC), Foreword p. 3. http://hdr.undp.org/en/reports/nationalreports/asiathepacific/china/china_2005_en.pdf 26 WHO and China State Council DRC, China: Health, Poverty, and Economic Development, p. 2. 27 UNDP, 2005, p. 1.

12
Recent Mortality Trends
Since the late 1980s, China has paid particular attention to reducing maternal mortality
ratios (death rates of women associated with pregnancy, childbirth, and the immediate postpartum period), infant mortality rates, and death rates of children under age five. In 1989, a surveillance system was established in 247 cities and counties to monitor maternal mortality. The Ministry of Health set up the Child Mortality Surveillance System in 1991. These systems get much more complete reporting of child and maternal mortality rates than any other data sources. China’s maternal mortality ratio has declined from 95 maternal deaths per 100,000 live births in 1989 to 48 per 100,000 in 2004. The national infant mortality rate declined from 50 deaths of infants (children from the moment of birth to exact age one) per 1,000 live births in 1991 to 33 in 1997, 32 in 2000, and 19 in 2005. The probability of dying for China’s children from birth to exact age 5 declined from 61 per 1,000 live births in 1991 to 42 in 1997 to 23 in 2005. China’s current maternal and young child mortality rates are far lower than in the vast majority of developing countries and are comparable to those in middle-income countries. But the large differences between urban and rural mortality levels remain. For example, the infant mortality rate of China’s population outside the cities is 2.4 times the city IMR.28 The maternal mortality ratio in the countryside is twice the level in the cities.29
The release of data from China’s 2005 representative sample survey of 1% of the population, which serves as a by-census halfway between the decennial censuses, allows us to update mortality trends in China to 2005. Table 2 shows age-specific mortality rate trends from 2000 to 2005 as reported in the 2000 population census and the 2005 national survey. For females in all age groups, death rates declined from 2000 to 2005. These most recent data document the continuation of China’s spectacular record of strong survival improvements for girls and women at almost every age in each decade from the 1970s to today. At ages 0 (infancy) and ages 1-4, the 2005 death rates are still reported to be higher for girls than boys, an abnormal situation.30 But in this 5-year period, death rates of babies and young children reportedly dropped steeply for both boys and girls. This reported trend is consistent with the trend data from China’s Child Mortality Surveillance System.
28 China National Working Committee on Children and Women, Report of the People’s Republic of China on the
Development of Children in the 1990s—National Report on the Follow-up to the World Summit for Children. Beijing: China National Working Committee on Children and Women, 2001, pp. 28-29; WHO and China State Council DRC, China: Health, Poverty, and Economic Development, p. 5; China Ministry of Health, http://www.moh.gov.cn/open/2007tjts/P39.htm
29 UNDP, 2005, p. 3. 30 In normal populations without life-threatening discrimination against persons of either sex, female death rates are naturally lower than male death rates at every age.

13

14
For males, the unbroken mortality declines from the 1970s to 2000 continued to 2005 in childhood ages and in adult age groups 40-44 and older. However, young adult male age groups from the late teens through the thirties recorded a very slight rise in the death rates. Age-specific death rates remain very low at these ages, but a rise in the death rates was not expected. Could the data be incorrect? A close look at recorded death rates from the censuses of 1990 and 2000 and the by-census of 2005 confirm that the trend appears to be real. From 1989 to 2000, mortality declines slowed for young adult men; only tiny survival improvements were recorded in their twenties, thirties, and forties during that decade. The current reversal is believable considering the 1989-2000 recorded trends that showed male death rates almost stabilizing at young adult and young middle ages before the recent reversal.
Urban-Rural Inequality in China
During China’s three decades of economic reform, the rising tide has lifted all boats. But at the same time, disparities have widened between those who have benefited the most and those who have gained the least from the economic, social, and political transformations taking place. The most serious inequality is between urban and rural areas. Average per capita consumption expenditure in urban households is three times that of rural households, and this figure does not even capture all the financial advantages that China’s system gives to urbanites but not rural residents.31 The income ratio between urban and rural residents widened further by 2006 to 3.28:1.32 This urban-rural gap in living standards is far greater than in other Asian countries, where urban-to-rural income ratios are 1.3-2.2 to one.33 In China, if rural workers and families could more easily migrate to urban areas to live and work, this would help reduce the urban-rural gap in living standards. However, continuing rigidities in China’s household population registration system and discrimination against rural migrants into cities slows down this corrective mechanism.34 Given the continuing advantages for urban compared to rural people, we might hypothesize that perhaps the slight rise in young adult male death rates in China is a rural but not an urban phenomenon.
Recent Mortality Trends and Their Causes
Calculating the life tables separately for cities, urban towns, and rural China, the
following results emerge. In China’s cities, recorded male death rates dropped in all age groups from 2000 to 2005, except for an increase in the male death rates at ages 15-19 and 45-49. In the towns (zhen), male death rates dropped at all ages except for a notable increase in the death rate at ages 25-29, and very slight increases in the age groups 15-19, 20-24, and 35-39.
31 China NBS, China Statistical Yearbook 2006, pp. 350, 374; Banister, “Poverty, progress, and rising life expectancy,” pp. 145-148. 32 National Population and Family Planning Commission of China, “Rural-urban income gap still widening,” Xinhua News Service, Dec. 27, 2007. http://www.npfpc.gov.cn/en/en2007-12/news20071227.htm 33 Dollar, “Poverty, inequality, and social disparities,” pp. 10-11. 34 Maddison, Angus, Chinese Economic Performance in the Long Run, 2
nd Edition, Revised and Updated: 960-
2030 A.D. Paris: Organisation for Economic Co-operation and Development, OECD Development Centre, pp. 22, 99.

15
Table 3 shows China’s recorded rural death rates in 2000 and 2005, and the 5-year trend. A striking finding is that in rural China, girls and women at all ages experienced declining death rates in the latest half decade. Death rates also dropped for boys below age 10 and for men in their fifties and older. But rural death rates rose slightly for boys ages 10-14 and unmistakably for men from their late teens through young adulthood and up to age 50.
Separating the rural mortality data into the richer half of the provinces and the poorer half of the provinces, the rural populations in the richer provinces had increased male mortality from 10-14 through 35-39 and at 45-49. The poorer provinces showed tiny increases in rural male death rates in the teens (10-14 and 15-19), but strong increases in death rates of rural men in their twenties, thirties, and late forties. Rural men in the poorer provinces indeed seem to be the most affected. If inequalities between urban and rural households had widened so much in this half decade that they had led to an absolute decline in the quality of life for rural households, and if death rates rose as a result, we would expect that any such death rate increases would have affected all the household members—girls and boys, men and women. This is obviously not the

16
case. In addition, if environmental deterioration had caused rising death rates anywhere, we would also expect to see females as strongly affected as males. What then is the reason for rising death rates for rural males ages 10-14 through 45-49, town men ages 15-19 through 25-29 and 35-39, and city men 15-19 and 45-49? Why are the increases in rural male death rates most pronounced in the poorer half of the provinces in the twenties through the late forties? Some have predicted that death rates of Chinese men will rise because of the hugely increased rates of cigarette smoking in the economic reform period, due to the fact that men can afford to smoke heavily and they do. As of 2003, half of Chinese men and 3 percent of women smoked.35 The total number of smokers in China rose to 320 million in 2004, a 4 percent increase over 2003; China produces 39 percent of the world’s tobacco and exports 6 percent of world tobacco production, which means that the people of China who constitute 20 percent of the global population consume 33 percent of world tobacco production.36 Big increases in the incidence and prevalence of lung cancer, other tobacco-related cancers, emphysema, chronic obstructive pulmonary disease (COPD), heart and vascular diseases, and other severe illnesses are expected to follow rising tobacco use by several decades, so tobacco-related deaths may indeed be one of the causes of rising male death rates. In addition, increasing alcohol abuse leading to alcoholic liver disease is almost completely a male phenomenon in China. But if these male lifestyle issues are the cause of rising male death rates, why do we see no increase in death rates of men in their fifties and older? What has happened since the turn of the century, based on the data from the 2000 population census and the 2005 1% sample population survey, is that male death rates have risen slightly in prime working ages, particularly in rural China, especially rural areas of poor provinces, and to a lesser extent in towns and cities. Why? One possible cause is that, as men have moved out of labor-intensive agricultural work, many have shifted to work that involves increased risks, whether they have stayed in rural areas or moved to towns and cities—driving vehicles and riding in vehicles in their jobs, heavy construction work, coal mining and other kinds of mining, dangerous factory work, and riskier service jobs than those given to women. Observers in China and outside China have focused attention on the excess mortality of Chinese girls based on traditional strong son preference and exacerbated by the current low fertility rate. Indeed, both sex-selective abortion of female fetuses and excess female mortality after birth have led to the current situation that about 119-120 boys are born in China for every hundred girls and China now has a severe shortage of girls and women in all childhood ages and into adulthood.37
35 China National Health Services Survey 2003; WHO and China State Council DRC, China: Health, Poverty, and
Economic Development, p. 43. 36 Maggie Fox, Reuters, “Tobacco and poverty drive cancer in developing world,” Yahoo News, Dec. 20, 2007, based on a report from the International Agency for Research on Cancer and an interview with Dr. Tony Mok of the Chinese University of Hong Kong. 37 China National Bureau of Statistics, Tabulation on the 2000 Population Census of the People’s Republic of China. Beijing: China Statistics Press, 2002, Vol. 1, pp. 570; Vol. 3, p. 1883; China NBS, 2005 National 1%
Sample Survey Data, pp. 82, 147; Li Shuzhuo, Wei Yan, Jiang Quanbao, and Marcus W. Feldman, “Female child survival in China: past, present, and prospects for the future,” presented at the CEPED-CICRED-INED Seminar on Female Deficit in Asia: Trends and Perspectives, Singapore, Dec. 2005.

17
While not neglecting the continuing severity of the shortage of girls and young women in China, it is time to now focus on excess MALE mortality in China. Excess male mortality is common all over the world and it should be tackled not only in China but also in other countries. Mortality statistics everywhere confirm that natural male age-specific death rates are higher than natural female death rates in the same ages, but in addition, boys and men almost everywhere engage in behaviors that lead to their untimely deaths much more than girls and women do. Among these behaviors are high-risk vehicle driving, high-risk leisure activities and sports, violence, smoking, alcohol abuse, and neglect of their own health and safety. Societies also allocate to men jobs that are much more dangerous than women’s jobs—military jobs and warfare, driving vehicles, construction work, mining, and heavy labor. China has now entered the ranks of countries whose mortality is so low that many deaths are now caused by lifestyle, injuries and accidents, and occupational factors. Statistics on causes of death in China show that age-specific death rates are far higher for men than women from injuries and poisoning, cancer, digestive diseases, cardiovascular diseases, and respiratory diseases.38
China’s Mortality Today in International Perspective
Table 4 and Figure 4 show the long-term trends in expectation of life at birth (or life expectancy) for males and females in the mainland of China from the 1964-1982 intercensal period to 2005. Life expectancy for the Chinese population has continued to rise for this entire period, an outcome that is consistent with the country’s rapidly increasing living standards and rising educational attainment. Mortality statistics from the 2000 population census and the nationwide 1% sample population survey (or by-census) of 2005, after adjustment for underreporting of deaths in all age-sex groups, suggest that expectation of life at birth in China rose from 71 years in 2000 to 74 years in 2005. (If the underreporting of deaths was worse in the 2005 sample survey than in the 1990 and 2000 censuses, it is possible that actual life expectancy in 2005 was somewhat lower than estimated here.)39
38 Zhongwei Zhao, “Changing mortality patterns and causes of death,” in Transition and Challenge: China’s Population at the Beginning of the 21
st Century, edited by Zhongwei Zhao and Fei Guo. Oxford, England: Oxford
University Press, 2007, pp. 160-176, esp. pp. 174-175. 39 An attempt by Kenneth Hill and Judith Banister to estimate the completeness of death reporting for the 2000-2005 period was unsuccessful because of age structure data problems in the 2005 1% sample survey. Therefore, it was assumed that the sex-specific completeness of death reporting beyond young childhood for 2005 was the same as for 1990-2000. More accurate adjustment factors await data from the 2010 census of China.

18

19
Even though male death rates apparently stabilized or slightly increased in young adulthood and early middle age between 2000 and 2005, male life expectancy still rose from 69 years in 2000 to 72 years in 2005 because of sharply declining male infant, child, late middle age, and old age mortality rates. Data for females indicate a strong increase in life expectancy from 72 years in 2000 to 76 years in 2005. As shown in Table 4, females had a 3-year advantage in life expectancy over males during 1982-2000, and this survival advantage widened to 4 years by 2005.
China has achieved good survival conditions for a developing country. For example, life expectancy in China by 2004-2005 was about 11 years longer than in all the rest of the developing world combined (in particular, 12 years longer than in Africa, 10 years longer than in India, 5 years longer than in Southeast Asia and the Middle East, and at about the same level as the more urbanized Latin America and Caribbean region).40 Overall, child and infant mortality rates in China have been declining for six decades and are now at a low level compared to most developing countries. Though China is in the lead, it is part of a global trend toward reduced young child mortality in developing countries worldwide, caused primarily by improvements in health care and more access to safe drinking
40 United Nations Population Division, World Population Prospects: The 2006 Revision. New York: 2007. http://esa.un.org/unpp/p2k0data.asp ; World Health Organization, Mortality Country Fact Sheets 2006.

20
water.41 In the case of China, by the turn of the century, 93 percent of the rural population had benefited from water improvement projects, with a total of 50 percent of rural households having running water, and by 2003, sanitary toilets were in place for 21 percent of rural residents.42
Remaining Poverty and Worsening Inequality
The urban-rural divide is the most visible pattern of economic inequality in China. This is reflected in education, health, and environmental conditions. Rural youth receive 2-3 fewer years of schooling than urban youth. The proportion of the population with only unclean water to drink is nearly zero in urban areas but about 20 percent in rural areas and over 50 percent in the poorest rural areas. The prevalence of malnutrition, hunger, and food shortages is two to three times higher in rural than urban areas.43 In addition, inequalities in economic conditions and opportunities have widened within rural China and within urban China.
But the forces unleashed by reforms—namely economic liberalization with few provisions toward equity—have negatively affected the distribution of incomes and opportunities. Since the late 1990s, widening disparities in income and social development have started to overshadow the impressive performance in economic growth and poverty reduction. Liberalization and an unclear role of the Government in the social sector have contributed to significant income inequalities, and inequity in access to public services. Disparities in human development indicators have sharpened over the past few decades and China’s progress in social development has slowed down, particularly in poor rural areas.44
The very large proportion of China’s rural and urban populations who have no medical insurance coverage or very minimal coverage, coupled with rapidly rising costs of medical care, has meant that large percentages of the people do not get medical care when they need it. Based on successive China National Health Services Surveys conducted by the Ministry of Health, the percent of people in China who got sick but did not use outpatient medical services was 36 percent in 1993, 39 percent in 1998, and 49 percent in 2003. In addition, the percent of patients who were referred to hospitals for inpatient care but did not go into the hospital was 36 percent in 1993, 32 percent in 1998, and still 30 percent in 2003. As of 2003, of those who did not go into the hospital when referred by a doctor, 70 percent said that the reason was their inability to afford hospital costs. Similarly, among early hospital discharges that occurred against medical advice, 67 percent were reported to be associated with inability to pay any more.45 All these measures of inability to get access to or afford medical care are far worse in rural than urban
41 Agence France Presse, “Infant mortality rates declining around the globe: UNICEF,” Yahoo News, Dec. 9, 2007. 42 UNDP, 2005, p. 94. 43 WHO and China State Council DRC, China: Health, Poverty, and Economic Development, p. 10. 44 United Nations Development Program (UNDP), China Human Development Report 2005: Development with
Equity. Beijing: China Translation and Publishing Corporation; WHO and China State Council DRC, China: Health, Poverty, and Economic Development, p. 2. 45 China National Health Services Surveys 1993, 1998, 2003; WHO and China State Council DRC, China: Health,
Poverty, and Economic Development, p. 16.

21
areas.46 The majority of China’s population fully depends on out-of-pocket spending to cover the cost of health services. Remaining poverty in China is connected in part to the lack of medical insurance coverage: “Many farmers revert to poverty due to illness and the burden of medical treatment.”47 In 2007, nine doctors who were representatives at China’s National People’s Congress complained that China’s government spends too little on health, 2.7 percent of GDP, in contrast to many other developing countries at 6-8 percent of GDP and developed countries at around 10 percent of GDP. One of the doctors, a former president of the Chinese Academy of Medical Sciences, described organizational problems in China’s health system as follows:
The government department in charge of population is not responsible for health, the one in charge of medical treatment is not responsible for drugs, the one in charge of western drugs is not responsible for traditional Chinese medicine, and the one in charge of urban medical insurance is not responsible for rural insurance. This is not only inefficient, but also easily leads to buck-passing, malpractice and corruption.48
Illness and Injuries in China
As we have seen, China has mortality data of reasonably good quality from its successive censuses and by-censuses. But China does not gather enough good information on the health status of the population. So, until people die, we do not know enough about their health conditions. To improve this situation, it is important that China pay more attention to measuring the health and illness and disability of the people, not only to measuring whether they are alive or dead. It would also be helpful if the results of current studies on China’s health were made more readily accessible to a broad global audience.
A World Bank global study of the burdens of disease, disabilities, and premature deaths
focused on China as of 2001, with the cooperation of China’s Ministry of Health and the Chinese Center for Disease Control.49 This study estimated that over 70 percent of the disease and disability burden in China is now from non-communicable diseases and injuries, primarily stroke, chronic respiratory disease, cancer, perinatal conditions, unipolar depressive disorders, heart disease, accidents and injuries (especially road traffic and self-inflicted), age-related vision disorders, and lower respiratory infections. The main risk factors leading to China’s burden of disease are high blood pressure, alcohol, tobacco, indoor smoke from solid fuels (indoor air pollution from burning coal, biofuels, etc.), poor quality diet, poor sanitation, high cholesterol, overweight, undernutrition, and physical inactivity. The main causes of adult deaths in the
46 UNDP, 2005, p. 60. 47 Susan V. Lawrence, “The sickness trap,” Far Eastern Economic Review (Hong Kong), June 13, 2002. http://www.feer.com ; Baogang Guo, “Transforming China’s urban health-care system,” Asian Survey, Vol. 43, No. 2 (Mar.-Apr. 2003), pp. 385-403, esp. pp. 399-400. 48 Irene Wang, “Doctors decry mean medical care spending; only 2.7pc of GDP invested, well below emerging nations,” South China Morning Post (Hong Kong), Mar. 12, 2007. 49 World Bank, Burden of Disease in China in 2001. Washington, DC: World Bank, Disease Control Priorities Project, 2006. http://www.popline.org/docs/1724/311384.html See also relevant chapters in Global Burden of Disease and Risk Factors, edited by A.D. Lopez, C.D. Mathers, M. Ezzati, D.T. Jamison, and C.J.L. Murray. New York: Oxford University Press, 2006.
22
working ages 15-59 in China are cerebrovascular disease (stroke), road traffic accidents, suicide, liver cancer and cirrhosis of the liver, and stomach cancer. Many of these risk factors and premature deaths could, at least in theory, be greatly reduced by lifestyle changes, adequate medical monitoring, availability of affordable pharmaceuticals and health care, more attention to road traffic safety, better household energy sources, cleaner water, adequate quantity and quality of food, better sanitation, and availability of mental health services.
The Ministry of Health, in its national survey on health services and illness in 2003,
asked respondents if they or their household members had been ill or disabled in the two weeks immediately before the survey.50 In large cities, 6 percent of the population responded that they had been ill due to cardiovascular diseases (stroke, heart disease), 4 percent of the people were sick because of respiratory diseases, and 2 percent with digestive diseases—these conditions accounted for almost 70 percent of the total illness and disability. The situation was almost the same in medium-sized cities. In most rural areas, over 40 percent of the morbidity (disease and disability) was attributable to respiratory diseases. Digestive diseases were more prevalent and cardiovascular diseases far less prevalent in the countryside and small cities than in large and medium-sized cities.
Health and China’s Labor Force
One of the many reasons that China’s economy has grown so much faster than the
economies of other poor developing countries of Asia in the latest three decades is that China has had a better base of human capital. By the late 1970s and early 1980s, China had much lower death rates than did other poor Asian countries. China also had a better base of literacy and primary education. Further significant improvements since then have been noteworthy.
But weaknesses emerged in the economic reform period in monitoring the health of
China’s population and in preventing epidemics. These problems were highlighted at the start of the SARS epidemic in 2003. The successful struggle inside and outside China to stop that epidemic has led to renewed efforts to address health issues in China, with special emphasis on containing any future SARS outbreak and controlling various infectious diseases such as AIDS and avian flu, as well as vaccine-preventable diseases including tuberculosis and Hepatitis B.51 It is a continuing battle to control these illnesses. For example, inadequate treatment of tuberculosis can lead to drug-resistant strains; high rates of drug-resistant TB are found in China and India, which together are home to half the world’s cases of drug-resistant TB, according to the World Health Organization.52 Though communicable diseases remain important and worthy of constant surveillance in China, most of the burden of disease today is caused by chronic diseases and conditions. China’s poorly funded health system is not affordable for many millions who suffer from birth
50 China Ministry of Health, Center for Health Statistics and Information. 2004; Zhongwei Zhao, “Income inequality, unequal health care access, and mortality in China,” 2006, esp. p. 468. 51 WHO and China State Council DRC, China: Health, Poverty, and Economic Development, p. 37. 52 Maria Cheng, “WHO says drug-resistant TB spreads fast,” AP, Yahoo! News, Feb. 26, 2008.

23
defects, cancers, heart diseases or defects, stroke, high blood pressure, diabetes, anemia, occupational diseases, or the effects of air or water pollution, contaminated food, or fake medicines. People confronting AIDS, malaria, tuberculosis, or chronic Hepatitis B or other types of hepatitis also have difficulty affording care.
Current Drive to Expand Medical Insurance Coverage
China is trying to improve medical insurance coverage in cities. In 1998, the government promulgated the “Decision on establishing a basic medical insurance system for urban employees.”53 It is supposed to cover all employers and employees in urban areas. Businesses are to pay monthly into a social medical insurance pool that is designed to cover hospital expenses, while employees pay (through payroll deduction) a small percent of their monthly wage for a personal medical account to pay for outpatient treatment fees. When workers see a doctor or go to a hospital, part of the cost is supposed to be covered by these urban medical insurance schemes. By the end of 2003, about 80 million urban employees (only 31 percent of the reported total number of urban employees that year54) and 29 million urban retirees were reportedly covered by the scheme. The state encourages enterprises to establish supplementary medical insurance for their employees, mainly for settling medical expenses not covered by the enterprise employees’ basic medical insurance. Some multinational companies do supplement the municipal medical insurance system for their employees. The government reported that coverage of “urban basic medical insurance” was greatly expanded in 2008, and hundreds of cities are working on providing medical insurance to non-working urban residents.55
Since 2002, China’s government has begun to recreate a Rural Cooperative Medical
Scheme to help rural people pay for some medical costs; the system has reportedly been set up in at least 80 percent of rural counties.56 Participation is voluntary and the schemes vary by locality, but the per capita amounts of money allocated to the scheme have been tiny, at least so far.57 In 2007, “China allocated 11.38 billion yuan to promote a new rural cooperative medical care system and 27.98 billion yuan to support the new compulsory education mechanism in rural areas to ensure that all citizens shared the fruits of China’s reform and opening up,” according to the Minister of Agriculture Sun Zhengcai.58 Further assistance was planned for 2008:
53 Details in this paragraph are from Xinhua News Agency, “China improves medical insurance system,” Sept. 7, 2004, distributed by BBC Monitoring Asia Pacific—Political, of BBC Worldwide Monitoring. 54 China NBS, China Statistical Yearbook 2007, p. 127. 55 China National Development and Reform Commission, “Report on the implementation of the 2008 plan for national economic and social development and on the 2009 draft plan for national economic and social development,” Mar. 2009. http://www.cctb.net 56 “Missing the barefoot doctors,” The Economist, Oct. 13, 2007, pp. 27-30. 57 UNDP, 2005, pp. 65-68. 58 National Population and Family Planning Commission of China, Dec. 27, 2007.

24
China will improve its work on social security Wang Jun, vice minister of finance, says the government will double its contributions to the cooperative health program for rural and urban areas. The program is aimed at helping farmers and the jobless in cities. Authorities have decided to increase subsidies from the central and local governments to RMB80 for each recipient for medical costs.59 The government reported the following major progress in extending at least minimal
medical insurance during the year 2008: At the end of 2008,….a total of 316.98 million people participated in the urban basic health insurance program, an increase of 93.87 million….A total of 2,729 counties (cities, districts) conducted the new cooperative medical care system in rural areas, with a participation rate of 91.5 percent. The total expenditure of the new cooperative medical care system in rural areas reached 42.9 billion yuan, benefiting 370 million people.60 China has a serious problem with the safety of foods and pharmaceuticals. The people
of China are accustomed to taking both traditional Chinese and modern Western medicines, often at the same time. The opportunity for exploitation is enormous; China’s people can almost never be sure whether the medical drug they are purchasing is genuine, or a worthless fake, or downright dangerous.
Fake or bad drugs have killed dozens in China in recent years and raised questions about safety. Public fears grew in 2004 when at least 13 babies died of malnutrition in Anhui province after being fed fake milk powder with no nutritional value.61
Government Anti-poverty Programs
The government is also alarmed by growing inequality in China and has numerous
programs to reverse this trend: Western and northeastern initiatives: In the late 1990s, the national government began promoting preferential policies to develop the poor western half of China’s territory that has included fiscal transfers and infrastructure projects. This was followed by targeted policies to revitalize the northeastern rust belt of China. Promotion of rural education: “After years of focus on urban schools and higher education, basic schooling in rural areas has finally become a priority for a government trying to address a rural-urban wealth gap in China that is contributing to social unrest.”62 Effective in early 2007, all students in rural areas are now supposed to be exempt from paying tuition fees for the
59 “China will improve its work on social security.” www.sohu.com , Jan. 16, 2008. 60 China National Bureau of Statistics, “Statistical communique of the People’s Republic of China on the 2008 national economic and social development,” Feb. 26, 2006 broadcast. 61 Reuters, “Government takes aim at fake dangerous drugs,” Feb. 9, 2007, also in the China Daily. 62 Reuters, “Govt struggles to bridge rural education gap,” Feb. 28, 2007; based on China Daily, Feb. 28, 2007.

25
statutory nine years of compulsory education. In some of the poorest rural areas, government provides subsidies for textbooks and boarding expenses for needy students.63 Minimum living standard scheme for urban residents: In 1999, China’s State Council issued rules allowing all persons with city residence permits to apply for public assistance in their city of residence registration; as of 2002-2003, 22 million urban residents received some social assistance payment.64 This scheme is not designed to benefit migrants from rural areas who still have a village residence registration. In 2004, of China’s urban population of 543 million, 160 million did not hold urban residence registration.65
What Can Business Do?
Businesses operating in China have greatly contributed to improving the living standards of China’s people during the reform decades, simply by doing what they do best—investing, increasing production, creating jobs in the modern economy, and competing for market share and sales. Rising per capita income has reduced mortality and increased educational opportunities. Today, business has important roles to play in helping to sustain and to improve the human capital, including health status and educational level, of China’s workforce and population. At the same time, these business initiatives and ongoing business processes can benefit their own company profit bottom line while serving employers and employees and their families, as well as the wider Chinese society. What else can businesses do and are they doing?
1. Support employees to receive legal health insurance and medical benefits.
In most of China’s cities and many urban towns, businesses are required to pay to the local government each month some proportion of their total wage bill for the municipal medical insurance program. A small percent of salary is also deducted from each employee’s wage and forwarded to the municipal government each month for this health insurance scheme. When these employees have medical needs, at least some of the costs are supposed to be covered by the municipal health insurance system. However, this system is still under development and varies enormously from one urban area to another. In some cities, this scheme works reasonably well serving the health needs of workers and sometimes of their families. But in other places, factories employing rural-to-urban migrant workers are exempted by the municipality from paying into the health insurance scheme for those employees, and then the workers have no medical coverage when illness or injury strikes. Some other businesses simply do not comply with the legal requirements in the urban areas where they operate. Some cities have had the money in their health insurance funds stolen through official corruption, and then the money is not there when workers need it. In some places, the system does not work as well as intended and employee health benefits from the program are inadequate or not provided after the employers and employees paid into the system.
63 UNDP, 2005, p. 90. 64 UNDP, 2005, p. 69. 65 UNDP, 2005, p. 102.

26
Businesses in China, whether they are state-owned, private, foreign-domestic joint ventures, or wholly owned foreign enterprises, should comply with the law and pay into the medical insurance scheme for all their employees, including migrant employees who are by law supposed to be included in this program. If employees have difficulty getting paid out of the insurance pool for legitimate and reasonable medical expenses, companies could give them assistance in accessing these benefits.
2. Supplement the official medical insurance and health benefits if needed.
Some multinationals in China provide supplemental health and medical benefits. According to the Watson Wyatt 2005 Compensation and Benefit Survey in China, of the foreign-invested enterprises they surveyed in 2005, 64 percent provided supplementary medical insurance, 43 percent provided medical insurance for children of employees, and 42 percent offered personal accident insurance.66 This is an added cost for the company, but it is also a selling point in attracting and retaining workers. Because companies in China are competing with each other for employees, especially talented and educated employees, benefits that the workers see as important can minimize employee turnover and thus help strengthen the viability of the company.
3. Provide company wellness programs.
Multinational and domestic businesses in China have a strong interest in minimizing illness and absenteeism among their employees. Simple and inexpensive programs could encourage workers to emphasize good health. For example, companies could occasionally provide free blood pressure and cholesterol screening onsite or offsite. Wellness presentations could be provided to employees. Smoking at work could be banned indoors, and heavy drinking as well as smoking could be discouraged at business functions.
4. Corporate Social Responsibility.
Many businesses in China, both domestic and multinational, have active, effective, and visible programs of Corporate Social Responsibility (CSR). Many focus attention on helping orphanages, clinics, poor rural schools, migrant families, and other needy groups who are benefiting the least from China’s growing economy. These CSR programs benefit Chinese society and help ameliorate inequality and improve social welfare in small ways; they also engage concerned employees and promote public acceptance of the businesses.
5. Financial institutions can develop innovative ways to provide credit for small and
informal businesses.
In China, one of the biggest barriers to employment generation and poverty alleviation is the difficulty experienced by small and medium-sized enterprises and by the informal sector in obtaining credit.67 This reflects China’s long-standing bias of extending credit preferentially to
66 “China’s tight talent market,” China Business Review, Mar.-Apr. 2006, p. 27. www.chinabusinessreview.com 67 UNDP, 2005, pp. 104-105.

27
state-owned enterprises. As the financial sector opens up to foreign participation, and competition intensifies in this sector, banks and other financial institutions can move toward providing credit to the huge underserved proportion of China’s businesses and employers, while still using sound financial guidelines for determining good credit risks.
6. Link up with technical schools and universities to make curriculum more relevant to the
actual demands of your business.
There is fierce competition for talent in China’s working world today. Domestic
businesses, multinational companies, universities, government, research institutes, and entrepreneurial start-ups all want the same limited supply of highly educated, qualified, and talented individuals with the right skill sets. One way to benefit your own business and Chinese society at the same time is to set up cooperative relationships with selected higher educational institutions to improve the relevance of the curriculum to your business and to provide internships to highly able students.68 This can contribute to improving the quality of China’s higher education, at least in those universities where your company recruits, and leads to a win-win situation for your business and for university graduates seeking good jobs.
7. Pharmaceutical and biotech companies can develop, test, and sell high quality
pharmaceuticals in China.
Western companies are discovering the cost advantages of developing pharmaceutical
products in China.69 China is a low-cost center for biotechnical research, because of its large numbers of scientists and engineers who work for low salaries by global standards. In addition, China has a huge and comparatively homogeneous population suitable for running modern clinical trials at much lower expense than in developed countries.70 These new drugs can benefit China’s people as well as the global market.
8. Occupational safety and health.
A sociologist at the Chinese Academy of Social Sciences reported that the government of China is troubled by the country’s “grim workplace safety record.”71 According to a study by the World Health Organization and China’s State Council,
Workplace risks are a major source of disease, injury, and death in China. China’s occupational accident rate in 2003 was estimated at 1.3 accidents per 1,000 in the
68 See also Judith Banister and David Learmond, Bridging China’s Talent Gap, The Conference Board Executive Action Series, No. 221, Jan. 2007; Leslie Raymond, “Fit for purpose: Are China’s graduates ready to work?” The Conference Board webcasts, Apr. 2008. 69 Details in this paragraph are from Jane Spencer, “Lilly, China firm to develop drugs,” Wall Street Journal, Aug. 21, 2007, p. A11. See also International Federation of Pharmaceutical Manufacturers Associations, Accelerating Innovative Pharmaceutical Research and Development in China: A Case Study. Geneva: IFPMA, 2003. 70 China’s population is 91 percent Han Chinese, with ethnicity, culture, customs, lifestyles, and diet that are similar though not identical in most of the nation. This makes it possible to conduct clinical trials in which most important variables can be held constant or statistically controlled, with the key distinguishing factor between groups being use or non-use or different doses of the pharmaceutical or medical procedure being tested. 71 Fu Jing, “Gov’t focuses on broader benefits,” China Daily, Mar. 1, 2006.

28
workforce with 15.4 fatalities per 100,000 in the workforce….In China, the cause of 85% of all occupational diseases and injuries is coal mining.72
Accidents, injuries and deaths associated with road traffic and manufacturing operations are also problematic. Businesses in China can help prevent occupational injuries by emphasizing driver safety training and good vehicle maintenance, use of safety protective gear at work, and training of employees in accident prevention.
Conclusions
China’s population and workforce are characterized by high human capital in comparison to most of the developing world. With regard to health and survival, China is more similar to middle-income countries than to the other poor countries. This enormous population, constituting 20 percent of the global total, has achieved the high life expectancy of approximately 74 years, reasonably good health conditions, widespread literacy and numeracy skills, and a moderately high level of basic educational attainment. The Maoist decades from 1949 to 1978 laid the groundwork for today’s comparatively good health and survival conditions, the popularization of literacy and primary education, and remarkably reduced inequality between males and females. Much of the progress achieved in the most recent three decades can be attributed to the booming economy of the economic reform period. Domestic and multinational businesses in China can legitimately claim some of the credit for China’s impressive human development to date. In turn, the moderately high quality of China’s population and workforce continues to directly benefit companies operating in China. Poverty has declined steeply in China. A majority, probably a very large majority, of the total population was still living in poverty in the late 1970s. The World Bank estimates that by 2004, 26 percent of the population was still living below a poverty line of US$1 per day, and 54 percent of the people below US$2 per day. As the economy has developed, inequality has risen dramatically, especially inequality between urban and rural areas, and also within the urban populations and within the rural populations. Though continuing poverty and increasing inequality are genuine problems that the government is addressing today, China’s exceptional economic performance has basically lifted all boats for more than a quarter century. People in the poorest third of counties in China experienced greater improvements in survival from the 1970s to the early 1990s than did middle-income counties, richer counties, and urban areas. In the 1990s decade, China’s poorest provinces made greater mortality gains than better-off provinces. Nevertheless, mortality and health differentials remain large today, especially between urban and rural areas. China’s government is trying to ameliorate some of the inequality and disparities between the urban and rural populations, and between those who have benefited most during the economic reform period and those who have been, comparatively speaking, left behind. The
72 WHO and China DRC, 2006, p. 44.

29
global economic crisis is making all such goals more difficult to attain. Nevertheless, China’s achievements in raising life expectancy and improving health are impressive in the context of developing and middle income countries.