healthcare benefit information for the diocese of … benefit information for the diocese of...
TRANSCRIPT

Healthcare Benefit Information
for
The Diocese of Virginia
St. Andrew’s – Sewanee School St. Andrew’s – Sewanee Sc

Contents
Network Access Directions Medical Plan Schedule of Benefits
• CIGNA HMO Plan • Empire BCBS EPO 90 Plan • Empire BCBS EPO 80 Plan • Kaiser EPO 80 Plan • UnitedHealthcare Choice 80 Plan • Empire BCBS High Option PPO Plan • Aetna Choice POS II Plan • Empire BCBS 80/60 PPO Plan • Empire BCBS HDHP/HSA II Plan
Medical Plan Design Comparison Medco Prescription Drug Summary Medco Fact Sheet EyeMed Vision Summary

Network Access Directions
How to find network providers & access your health plans online 1. Aetna 2. Go to www.aetna.com/docfind 3. Click on the “Continue to DocFind” icon 4. Complete the required items in General Search 5. In the Select a Plan drop-down window, Aetna’s
plans are sorted under sub-headings: a. For Aetna HMO, select HMO** under Aetna Standard Plans b. For Aetna Choice® POS II or Aetna Select® choose the plan under Aetna Open Access Plans sub-heading. c. Click Start Search
CIGNA Medical 1. Go to http://www.cigna.com 2. Click on Provider Directory (top of the screen) 3. Complete the information for provider type, enter
your zip code, city, state, how far you are willing to travel, and click next
4. Choose Network (HMO) Plans or Point of Service (POS) Plans, and select a network.
Empire BlueCross BlueShield 1. Go to http://www.empireblue.com/medicaltrust 2. Click on Find a Doctor 3. Click on Across the Country 4. A new window will open. Under Select a Plan,
choose the PPO/EPO option and continue with the directions on the screen, entering your geographic information
Kaiser Permanente 1. Go to http:/my.kp.org/ecmt 2. Click on Clinical Staff Directory in the Get
Started Now section. Select your region from the pull down menu and click Continue
3. Mid-Atlantic members only: Select Search for a doctor, hospital or other provider. Scroll down and select Kaiser Permanente Select HMO. Then select a search type, input your specifications and click on Find Providers
4. All other members: after selecting your region, select the criteria to use to begin your search for a provider (gender, specialty, etc). Then, if applicable, select the medical facility you prefer.
UnitedHealthcare 1. Go to http://www.myuhc.com 2. Under Links and Tools in the upper right of the
page, select Find a Physician or Facility.
3. Select Search for a Physician and click Continue 4. Select Search for a Physician by Name Location or
Specialty 5. For Select a Plan, choose: UnitedHealthcare
Choice or UnitedHealthcare Choice Plus 6. Enter your zip code and click Continue 7. Select a specialty and click Continue Medco 1. Go to www.medco.com
Follow the steps to register. (Note: Your benefits must be active in order to register. If your benefits are not yet active, log onto cpg.org/productsservices/pharmacy.cfm for participating pharmacies and formulary information)
2. Once registered, log on to price medications, view Medco’s formulary (list of preferred drugs), locate a participating pharmacy, etc.
EyeMed 1. Go to http://www.eyemedvisioncare.com 2. Go to the Locate a Provider window on the left
side of the page, and under Select Your Network, choose Access
3. Enter your zip code, and click Submit 4. A new window opens that requires you to enter
special text as a security feature. Enter the text and click Submit
CIGNA Behavioral Health & Employee Assistance Program (EAP) 1. Go to http://www.cignabehavioral.com 2. Click on Find a Therapist/Psychiatrist 3. Log in (on left) to review your EAP benefits.
“Episcopal” is the Employer ID. You do not need to log in to access the Provider Directory
4. Fill in the fields for seeking a provider under either Behavioral Health or EAP
5. Click Search 6. Or call (866) 395-7794 Health Advocate
1. Go to http://www.healthadvocate.com/ 2. Select the Members icon 3. Enter “Episcopal” in the Log in box, to view
information about your Health Advocate benefits.
4. Or call (8660 695-8622

SCHEDULE OF MEDICAL BENEFITSNETWORK PLAN (HMO)CIGNAPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Lifetime Benefit Maximum(Includes All Other Maximums)
None
You must receive services only from healthcare providers participating in the CIGNA network, or benefits will not be covered by theplan. Expenses for out-of-network providers will only be considered as specified in the Plan handbook.
The following schedule summarizes coinsurance amounts paid by the Plan, benefit maximums, and any additional explanationneeded for your benefits. The Plan’s coinsurance will be reduced if you do not follow the procedures outlined in the “ClinicalManagement” section of the Plan handbook. Please refer to the text for additional Plan provisions that may affect yourbenefits.
Our Benefits: Although a specific service may be listed as a covered expense, it may not be covered unless it is medicallynecessary for the prevention, diagnosis or treatment of an illness or condition.
COVERED HEALTHSERVICE
YOURCOST SHARE
Acupuncture Services $20 per visit
Allergy Testing
Ambulance Services - Emergency Only
Diagnostic Tests/X-Rayand Laboratory Services
Durable Medical
Emergency Room $50 per visit Services *
Home Health Care
Limited to 15 visits per year.
ADDITIONAL LIMITATIONS AND EXPLANATIONS
$20 per visit Benefit includes routine injections at PCP’s office, with or without a physician encounter.
No copay when medically necessary. Services for non-emergencies will not be covered.
No copay when medically necessary.
Must be precertified my CIGNA.
(Injections)
$0
$0
Equipment (DME)
Your $50 copay will be waived if you are admitted to the hospital.
Limited to 210 days per year.$0
$0

SCHEDULE OF MEDICAL BENEFITSNETWORK PLAN (HMO)CIGNAPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Hospice Care
Hospital Services
Hospital Services(Outpatient)
Maternity Services
Nutritional Counseling
Outpatient TherapyServices
Physician’s OfficeServices
Routine & PreventiveServices
COVERED HEALTHSERVICE
YOURCOST SHARE
ADDITIONAL LIMITATIONS AND EXPLANATIONS
$0
$20 for first visitonly
Benefits include, but are not limited to, hospital semi-private room, miscellaneous fees,anesthesia, surgeons’ fees, physician visits, x-ray, lab and therapy expenses. Follow theprocedures required by the Clinical Management Program.
Benefits include but are not limited to outpatient surgery, physician, anesthesiology, x-ray& laboratory, and therapy expenses in a hospital or ambulatory surgical center.
$350 per admission
$250
(Inpatient)
Limited to 6 visits per calendar year.$20 per visit
Benefits include physical, occupational, and speech therapy. Limited to: 120 dayscombined physical and pulmonary, 120 days combined speech and cognitive, and 60days occupational. There is no limit for cardiac rehabilitation.
$20 per visit
Your copay applies to the office visit only. To locate a network provider, contact CIGNAvia the toll-free number or check the web site.
$20 per visit
Benefits include the office visit and vaccinations, inoculations, and immunizations.Benefits include routine physicals, including gynecological exams, and digital rectal exam,well-child exams, X-Rays and laboratory tests related to the routine exam, baselinemammograms, PAP tests and PSA screenings. Age and frequency of services will followthe recommendations of the American Medical Association guidelines.
$0 per visit
Routine ExamsRoutine Exam X-Rays & Laboratory ServicesWell-Child CheckupsRoutine ColonoscopyRoutine SigmoidoscopyOther Routine Services

SCHEDULE OF MEDICAL BENEFITSCIGNA
PLAN IS EFFECTIVE AS OF JANUARY 1, 2011NETWORK PLAN (HMO)
Skilled Nursing Facility
Spinal Treatment
Surgical Treatment of Morbid Obesity
Urgent Care Services
COVERED HEALTHSERVICE
YOURCOST SHARE
ADDITIONALLIMITATIONS ANDEXPLANATIONS
Limited to 60 days per year
$20 per visit
$50 per visit
$350 per admission
$0
$15,000 maximum per lifetime. Must be preauthorized by CIGNA.
Please see your regular physician or practitioner for routine care. Services for non-emergencies will not be covered.
Limited to 20 days per year for spinal manipulation.
NOTES: The word “lifetime” refers to the period of time you or your eligible dependents participate in this plan or any other plan funded by the Medical Trust.
This benefit summary is provided for informational purposes, is not all-inclusive, and does not constitute an agreement. Additional limitations and explanations,including specific benefit maximums will be provided to eligible, enrolled members in the Plan Document Handbook. In the event of a conflict between thisdocument and the official plan documents, the official plan documents will govern. The Episcopal Church Medical Trust retains the right to amend, terminate ormodify the terms of the plan at any time, without notice and for any reason.
CIGNA Member Services toll-free number: (800) CIGNA-24 (800-244-6224)CIGNA Pre-Enrollment: (800) 401-4041
* You may visit out-of-network providers for these services and eligible expenses will be considered as specifiedon this schedule. You will be responsible for any deductible, coinsurance, and amount over the “reasonable andcustomary” amount. Please refer to the individual provisions under “Additional Limitations and Explanations”to see if there are any prior notification or prior authorization requirements or other limitations.

The following schedule summarizes your mental health and substance abuse benefits, coinsurance amounts, benefitmaximums, and any additional explanation needed for your benefits. Please refer to the Mental Health/SubstanceAbuse chapter for additional Plan provisions. All coinsurances apply to your health plan’s out-of-pocket maximums.
SCHEDULE OF MENTAL HEALTH/SUBSTANCE ABUSE BENEFITSCIGNA BEHAVIORAL HEALTH PLAN IS EFFECTIVE AS OF JANUARY 1, 2011
FOR MEMBERS ENROLLED IN THE CIGNA NETWORK (HMO) PLAN
Outpatient Mental Health/ There is no annual limit.
ADDITIONAL LIMITATIONS AND EXPLANATIONS
Network
Network
Out-of-Network
Network$20 per visit
Out-of-Network30%
All admissions must be precertified. There is no annual limit. Plan coverage isreduced to 50% if there is no precertification. Emergency room, ambulance,and lab work charges are covered by your medical plan.
Inpatient Mental Health/Substance Abuse $150 per admission
30%
Network
Out-of-Network
All programs must be precertified. There is no annual limit. Plan coverage isreduced to 50% if there is no precertification.
Benefits include (but are not limited to) unlimited telephonic and work/lifeservices, crisis intervention, referrals to community resources, legalconsultations, and a large online resource library. You may also receive up to10 face-to-face counseling sessions per issue, but they must be precertified byCIGNA Behavioral.
$150 per program,payable at admission
30%
$0
N/A
Intensive Outpatient MentalHealth/Substance Abuse
Employee Assistance Program(EAP)
Benefit is limited to 24 90-minute sessions per calendar year. Up to 12 of the24 sessions may be used for individual consultation. The Plan will reimburse70% up to $40.
Colleague Groups
Out-of-Network
YOUR COST SHARECOVERED HEALTH SERVICE
Substance Abuse
Everything you discuss with your counselor or care provider is kept in the strictest confidence in accordance withapplicable state and federal laws. Your employer is not notified of your visits or given specific information aboutyour treatment without your written permission. The general health privacy and security standards of theEpiscopal Church Medical Trust apply.
CIGNA Behavioral Health Member Services Toll-Free Number: (866) 395-7794

You must receive services only from healthcare providers participating in the Empire network, or benefits will not becovered by the plan. Expenses for out-of-network providers will only be considered as specified in the Plan handbook.
The following schedule summarizes coinsurance amounts paid by the Plan, benefit maximums, and any additionalexplanation needed for your benefits. The Plan’s coinsurance will be reduced if you do not follow the proceduresoutlined in the “Medical Management” section of the handbook. Please refer to the text for additional Planprovisions that may affect your benefits.
Our Benefits: Although a specific service may be listed as a covered expense, it may not be covered unless it ismedically necessary for the prevention, diagnosis or treatment of an illness or condition.
SCHEDULE OF MEDICAL BENEFITS90 EPO PLANEMPIRE BLUECROSS BLUESHIELDPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Lifetime Benefit Maximum
None
Annual Deductibles Annual Out-of-Pocket Maximums(Excludes Deductible)
Network $ 200 Individual $ 1,000 Individual$ 500 Family $ 2,000 Family
COVERED HEALTHSERVICE
YOUR COST SHARE
Acupuncture Services
Allergy Testing
Ambulance Services - Emergency Only
Diagnostic Tests/X-Rayand Laboratory Services
Durable Medical
Emergency Room
Home Health Care
Limited to 12 visits per calendar year.Acupuncture services received on an inpatientbasis are not covered.
Yes No
COPAY APPLYTO ANNUALOOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
$25 per visit NoNo
50% NoYes
Allergy treatment with no office visit billed iscovered at 100%.
The $50 copay wil be waived if you are admittedto the hospital within 24 hours.
(Injections)
20%
Yes No10%
10% No NoEquipment (DME)
No No$50
You should notify Empire by calling the toll-freenumber prior to receiving any home health care.Limited to 200 visits per calendar year.
Yes Yes10%
Services*
SCHEDULE OF MEDICAL BENEFITS90 EPO PLANEMPIRE BLUECROSS BLUESHIELDPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
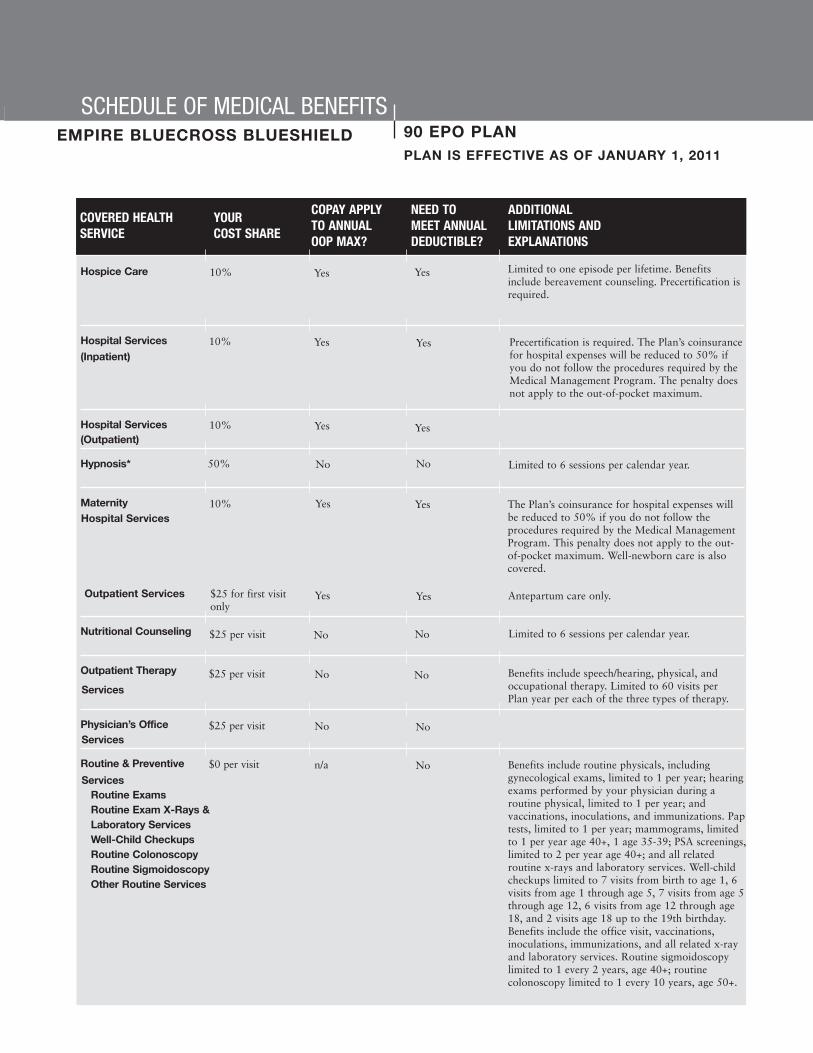
Hospice Care
Hospital Services
Hospital Services(Outpatient)
Hypnosis*
Maternity
Nutritional Counseling
Outpatient Therapy
Physician’s Office
Routine & Preventive
COVERED HEALTHSERVICE
YOURCOST SHARE
COPAY APPLYTO ANNUALOOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
Limited to one episode per lifetime. Benefitsinclude bereavement counseling. Precertification isrequired.
YesYes10%
YesYes Precertification is required. The Plan’s coinsurancefor hospital expenses will be reduced to 50% ifyou do not follow the procedures required by theMedical Management Program. The penalty doesnot apply to the out-of-pocket maximum.
10%
YesYes10%
NoNo50%
(Inpatient)
Antepartum care only.
Hospital Services
Outpatient Services
The Plan’s coinsurance for hospital expenses willbe reduced to 50% if you do not follow theprocedures required by the Medical ManagementProgram. This penalty does not apply to the out-of-pocket maximum. Well-newborn care is alsocovered.
10%
$25 for first visitonly
Yes Yes
Yes Yes
Limited to 6 sessions per calendar year.
Limited to 6 sessions per calendar year.
$25 per visit No No
Benefits include speech/hearing, physical, andoccupational therapy. Limited to 60 visits perPlan year per each of the three types of therapy.
Benefits include routine physicals, includinggynecological exams, limited to 1 per year; hearingexams performed by your physician during aroutine physical, limited to 1 per year; andvaccinations, inoculations, and immunizations. Paptests, limited to 1 per year; mammograms, limitedto 1 per year age 40+, 1 age 35-39; PSA screenings,limited to 2 per year age 40+; and all relatedroutine x-rays and laboratory services. Well-childcheckups limited to 7 visits from birth to age 1, 6visits from age 1 through age 5, 7 visits from age 5through age 12, 6 visits from age 12 through age18, and 2 visits age 18 up to the 19th birthday.Benefits include the office visit, vaccinations,inoculations, immunizations, and all related x-rayand laboratory services. Routine sigmoidoscopylimited to 1 every 2 years, age 40+; routinecolonoscopy limited to 1 every 10 years, age 50+.
$25 per visit No NoServices
$25 per visit No NoServices
$0 per visit n/a NoServices
Routine ExamsRoutine Exam X-Rays &Laboratory ServicesWell-Child CheckupsRoutine ColonoscopyRoutine SigmoidoscopyOther Routine Services

SCHEDULE OF MEDICAL BENEFITS90 EPO PLANEMPIRE BLUECROSS BLUESHIELDPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Skilled Nursing Facility/
Spinal Treatment
Surgical Treatment of
Urgent Care Services
Anesthesiology Services
Organ Transplants
COVERED HEALTHSERVICE
YOURCOST SHARE
COPAY APPLYTO ANNUALOOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
Yes Yes10% Limited to 60 days per year. Precertification isrequired.
No No$25 per visit Limited to 20 visits per year.
Yes Yes10%
Yes Yes10%
Yes Yes10%
Yes Yes10%
Limited to 1 procedure per lifetime.
For this benefit, “network plan” refers to theBCBS National Transplant Network.Precertification required. There is a $10,000travel and lodging limit.
Inpatient RehabilitationFacility Services
Morbid Obesity
Additional Benefits
Medical Management Program toll-free number: (800) 352-3152
*
NOTE:
You may visit out-of-network providers for these services and eligible expenses will be consideredas specified on this schedule. You will be responsible for any deductible, coinsurance, and amountover the “reasonable and customary” amount. Please refer to the individual provisions under“Additional Limitations and Explanations” to see if there are any prior notification or priorauthorization requirements or other limitations. For assistance in locating providers whoparticipate in the BlueCard PPO Network, contact Empire at the toll-free number (automatedservice is available 24 hours a day, 7 days a week; to speak with a representative, call between8:30 a.m. and 8:00 p.m., EST, Monday through Friday).
The word “lifetime” refers to the period of time you or your eligible dependents participate in thisplan or any other plan sponsored by the Medical Trust.
This benefit summary is provided for informational purposes, is not all-inclusive, and does not constitute an agreement. Additional limitations andexplanations, including specific benefit maximums will be provided to eligible, enrolled members in the Plan Document Handbook. In the event of aconflict between this document and the official plan documents, the official plan documents will govern. The Episcopal Church Medical Trust retains theright to amend, terminate or modify the terms of the plan at any time, without notice and for any reason.
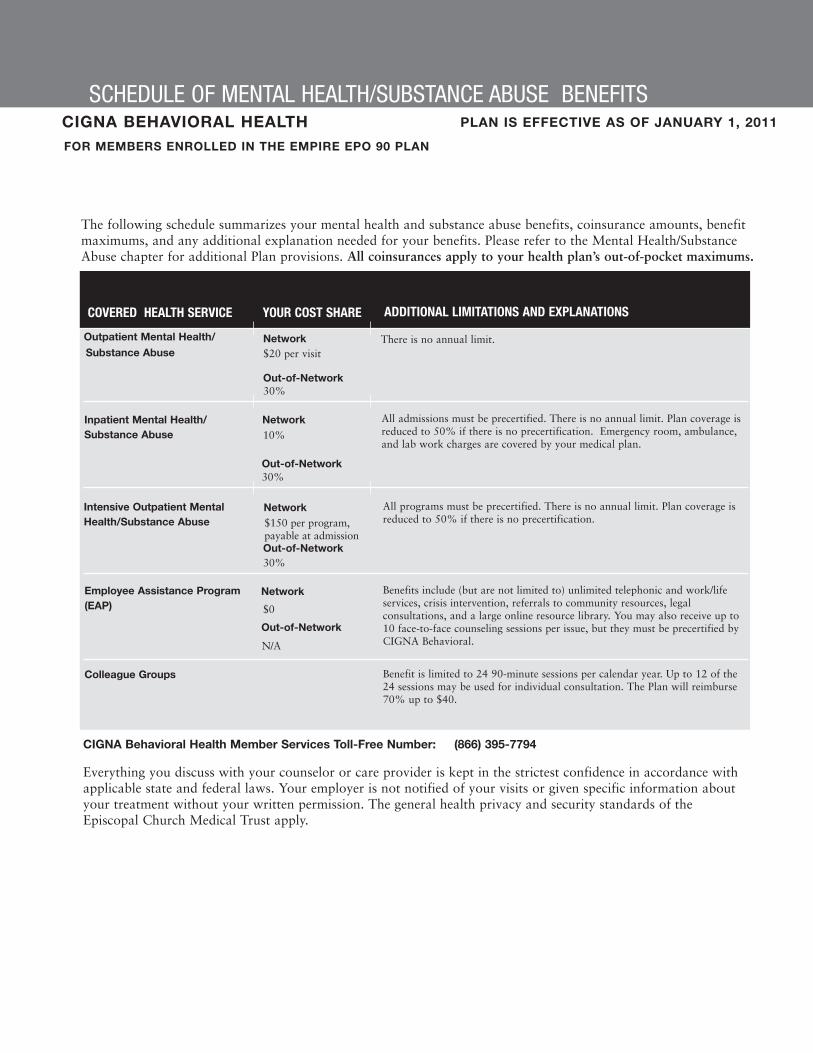
The following schedule summarizes your mental health and substance abuse benefits, coinsurance amounts, benefitmaximums, and any additional explanation needed for your benefits. Please refer to the Mental Health/SubstanceAbuse chapter for additional Plan provisions. All coinsurances apply to your health plan’s out-of-pocket maximums.
SCHEDULE OF MENTAL HEALTH/SUBSTANCE ABUSE BENEFITSCIGNA BEHAVIORAL HEALTH PLAN IS EFFECTIVE AS OF JANUARY 1, 2011
FOR MEMBERS ENROLLED IN THE EMPIRE EPO 90 PLAN
Outpatient Mental Health/ There is no annual limit.
ADDITIONAL LIMITATIONS AND EXPLANATIONS
Network
Network
Out-of-Network
Network$20 per visit
Out-of-Network30%
All admissions must be precertified. There is no annual limit. Plan coverage isreduced to 50% if there is no precertification. Emergency room, ambulance,and lab work charges are covered by your medical plan.
Inpatient Mental Health/Substance Abuse 10%
30%
Network
Out-of-Network
All programs must be precertified. There is no annual limit. Plan coverage isreduced to 50% if there is no precertification.
Benefits include (but are not limited to) unlimited telephonic and work/lifeservices, crisis intervention, referrals to community resources, legalconsultations, and a large online resource library. You may also receive up to10 face-to-face counseling sessions per issue, but they must be precertified byCIGNA Behavioral.
$150 per program,payable at admission
30%
$0
N/A
Intensive Outpatient MentalHealth/Substance Abuse
Employee Assistance Program(EAP)
Benefit is limited to 24 90-minute sessions per calendar year. Up to 12 of the24 sessions may be used for individual consultation. The Plan will reimburse70% up to $40.
Colleague Groups
Out-of-Network
YOUR COST SHARECOVERED HEALTH SERVICE
Substance Abuse
Everything you discuss with your counselor or care provider is kept in the strictest confidence in accordance withapplicable state and federal laws. Your employer is not notified of your visits or given specific information aboutyour treatment without your written permission. The general health privacy and security standards of theEpiscopal Church Medical Trust apply.
CIGNA Behavioral Health Member Services Toll-Free Number: (866) 395-7794
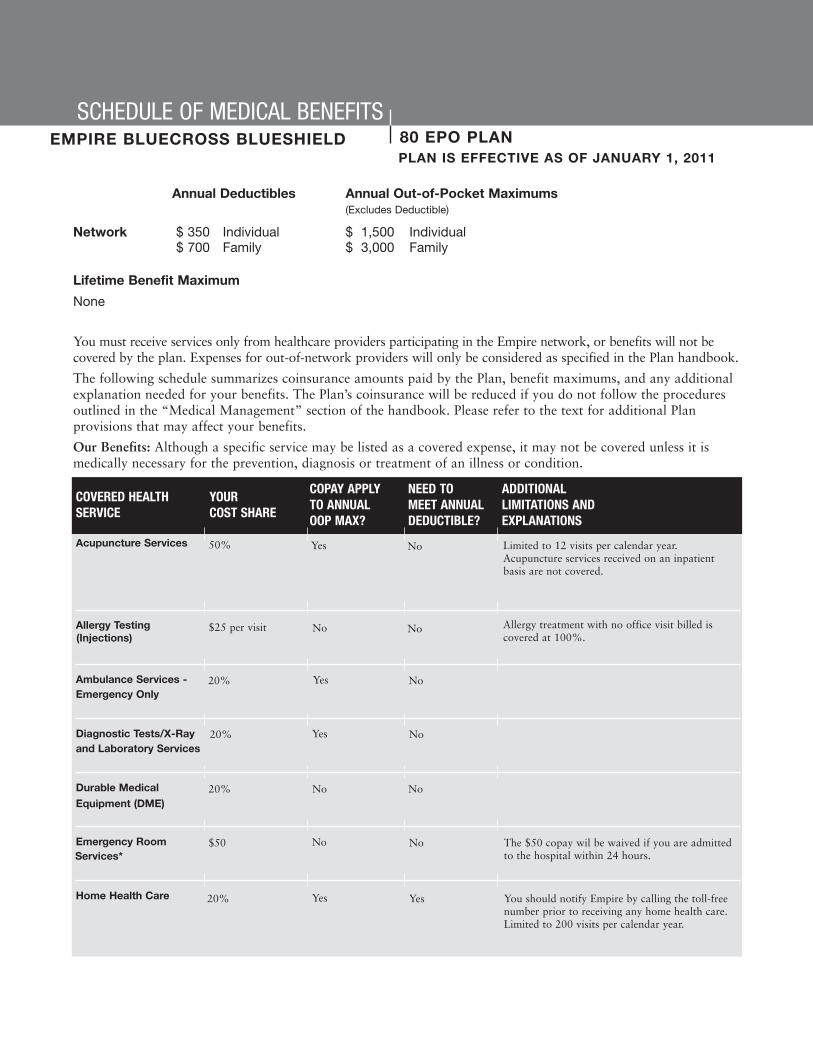
You must receive services only from healthcare providers participating in the Empire network, or benefits will not becovered by the plan. Expenses for out-of-network providers will only be considered as specified in the Plan handbook.
The following schedule summarizes coinsurance amounts paid by the Plan, benefit maximums, and any additionalexplanation needed for your benefits. The Plan’s coinsurance will be reduced if you do not follow the proceduresoutlined in the “Medical Management” section of the handbook. Please refer to the text for additional Planprovisions that may affect your benefits.
Our Benefits: Although a specific service may be listed as a covered expense, it may not be covered unless it ismedically necessary for the prevention, diagnosis or treatment of an illness or condition.
SCHEDULE OF MEDICAL BENEFITS80 EPO PLANEMPIRE BLUECROSS BLUESHIELDPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Lifetime Benefit Maximum
None
Annual Deductibles Annual Out-of-Pocket Maximums(Excludes Deductible)
Network $ 350 Individual $ 1,500 Individual$ 700 Family $ 3,000 Family
COVERED HEALTHSERVICE
YOUR COST SHARE
Acupuncture Services
Allergy Testing
Ambulance Services - Emergency Only
Diagnostic Tests/X-Rayand Laboratory Services
Durable Medical
Emergency Room
Home Health Care
Limited to 12 visits per calendar year.Acupuncture services received on an inpatientbasis are not covered.
Yes No
COPAY APPLYTO ANNUALOOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
$25 per visit NoNo
50% NoYes
Allergy treatment with no office visit billed iscovered at 100%.
The $50 copay wil be waived if you are admittedto the hospital within 24 hours.
(Injections)
20%
Yes No20%
20% No NoEquipment (DME)
No No$50
You should notify Empire by calling the toll-freenumber prior to receiving any home health care.Limited to 200 visits per calendar year.
Yes Yes20%
Services*
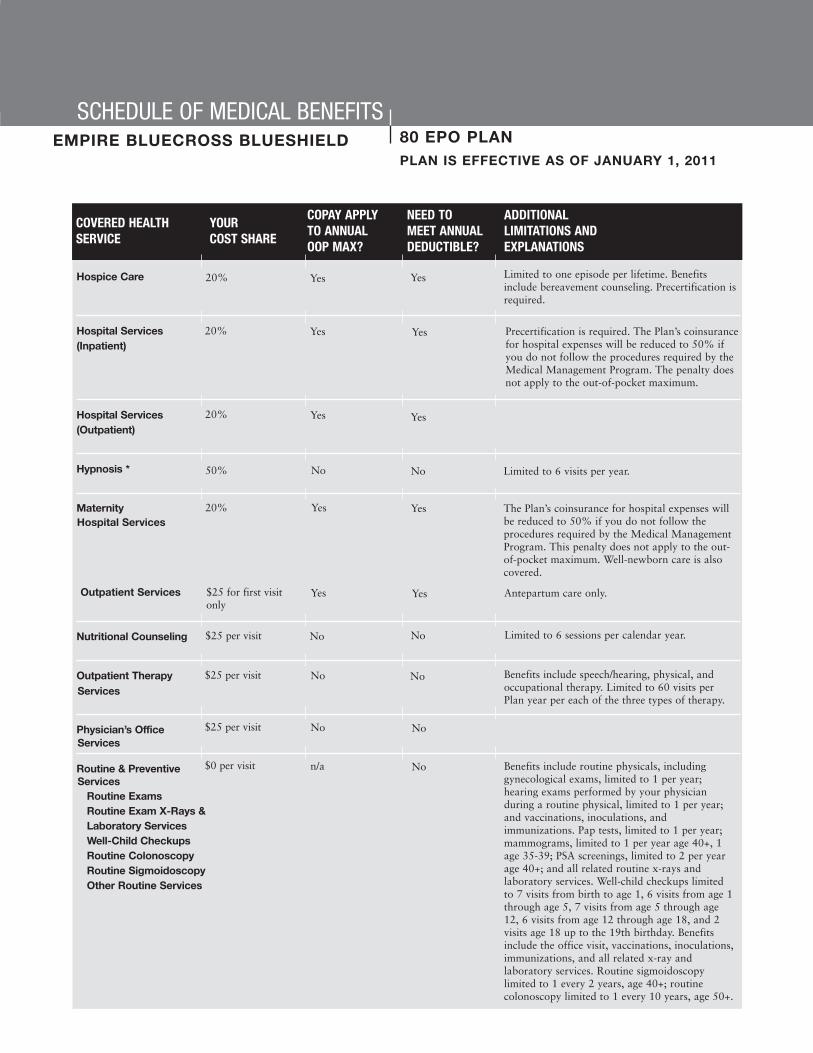
SCHEDULE OF MEDICAL BENEFITS80 EPO PLANEMPIRE BLUECROSS BLUESHIELDPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Hospice Care
Hospital Services
Hospital Services(Outpatient)
Hypnosis *
Maternity
Nutritional Counseling
Outpatient Therapy
Physician’s Office
Routine & Preventive
COVERED HEALTHSERVICE
YOURCOST SHARE
COPAY APPLYTO ANNUALOOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
Limited to one episode per lifetime. Benefitsinclude bereavement counseling. Precertification isrequired.
YesYes20%
YesYes Precertification is required. The Plan’s coinsurancefor hospital expenses will be reduced to 50% ifyou do not follow the procedures required by theMedical Management Program. The penalty doesnot apply to the out-of-pocket maximum.
20%
YesYes20%
(Inpatient)
Antepartum care only.
Hospital Services
Outpatient Services
The Plan’s coinsurance for hospital expenses willbe reduced to 50% if you do not follow theprocedures required by the Medical ManagementProgram. This penalty does not apply to the out-of-pocket maximum. Well-newborn care is alsocovered.
20%
$25 for first visitonly
Yes Yes
Limited to 6 visits per year.50% No No
Yes Yes
Limited to 6 sessions per calendar year.$25 per visit No No
Benefits include speech/hearing, physical, andoccupational therapy. Limited to 60 visits perPlan year per each of the three types of therapy.
Benefits include routine physicals, includinggynecological exams, limited to 1 per year;hearing exams performed by your physicianduring a routine physical, limited to 1 per year;and vaccinations, inoculations, andimmunizations. Pap tests, limited to 1 per year;mammograms, limited to 1 per year age 40+, 1age 35-39; PSA screenings, limited to 2 per yearage 40+; and all related routine x-rays andlaboratory services. Well-child checkups limitedto 7 visits from birth to age 1, 6 visits from age 1through age 5, 7 visits from age 5 through age12, 6 visits from age 12 through age 18, and 2visits age 18 up to the 19th birthday. Benefitsinclude the office visit, vaccinations, inoculations,immunizations, and all related x-ray andlaboratory services. Routine sigmoidoscopylimited to 1 every 2 years, age 40+; routinecolonoscopy limited to 1 every 10 years, age 50+.
$25 per visit No NoServices
$25 per visit No NoServices
$0 per visit n/a NoServices
Routine ExamsRoutine Exam X-Rays &Laboratory ServicesWell-Child CheckupsRoutine ColonoscopyRoutine SigmoidoscopyOther Routine Services

SCHEDULE OF MEDICAL BENEFITS80 EPO PLANEMPIRE BLUECROSS BLUESHIELDPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Skilled Nursing Facility/
Spinal Treatment
Surgical Treatment of
Urgent Care Services
Anesthesiology Services
Organ Transplants
COVERED HEALTHSERVICE
YOURCOST SHARE
COPAY APPLYTO ANNUALOOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
Yes Yes20% Limited to 60 days per year. Precertification isrequired.
No No$25 per visit Limited to 20 visits per year.
Yes Yes20%
Yes Yes20%
Yes Yes20%
Yes Yes20%
Limited to 1 procedure per lifetime.
For this benefit, “network plan” refers to theBCBS National Transplant Network.Precertification required. There is a $10,000travel and lodging limit.
Inpatient RehabilitationFacility Services
Morbid Obesity
Additional Benefits
Medical Management Program toll-free number: (800) 352-3152
You may visit out-of-network providers for these services and eligible expenses will be consideredas specified on this schedule. You will be responsible for any deductible, coinsurance, and amountover the “reasonable and customary” amount. Please refer to the individual provisions under“Additional Limitations and Explanations” to see if there are any prior notification or priorauthorization requirements or other limitations. For assistance in locating providers whoparticipate in the BlueCard PPO Network, contact Empire at the toll-free number (automatedservice is available 24 hours a day, 7 days a week; to speak with a representative, call between8:30 a.m. and 8:00 p.m., EST, Monday through Friday).
The word “lifetime” refers to the period of time you or your eligible dependents participate in thisplan or any other plan sponsored by the Medical Trust.
*
NOTE:
This benefit summary is provided for informational purposes, is not all-inclusive, and does not constitute an agreement. Additional limitations andexplanations, including specific benefit maximums will be provided to eligible, enrolled members in the Plan Document Handbook. In the event of aconflict between this document and the official plan documents, the official plan documents will govern. The Episcopal Church Medical Trust retainsthe right to amend, terminate or modify the terms of the plan at any time, without notice and for any reason.

SCHEDULE OF MENTAL HEALTH/SUBSTANCE ABUSE BENEFITSCIGNA BEHAVIORAL HEALTH PLAN IS EFFECTIVE AS OF JANUARY 1, 2011
The following schedule summarizes your mental health and substance abuse benefits, coinsurance amounts, benefitmaximums, and any additional explanation needed for your benefits. Please refer to the Mental Health/SubstanceAbuse chapter for additional Plan provisions. All coinsurances apply to your health plan’s out-of-pocket maximums.
FOR MEMBERS ENROLLED IN THE EMPIRE EPO 80 PLAN
Outpatient Mental Health/ There is no annual limit.
ADDITIONAL LIMITATIONS AND EXPLANATIONS
Network
Network
Out-of-Network
Network$20 per visit
Out-of-Network30%
All admissions must be precertified. There is no annual limit. Plan coverage isreduced to 50% if there is no precertification. Emergency room, ambulance,and lab work charges are covered by your medical plan.
Inpatient Mental Health/Substance Abuse 20%
30%
Network
Out-of-Network
All programs must be precertified. There is no annual limit. Plan coverage isreduced to 50% if there is no precertification.
Benefits include (but are not limited to) unlimited telephonic and work/lifeservices, crisis intervention, referrals to community resources, legalconsultations, and a large online resource library. You may also receive up to10 face-to-face counseling sessions per issue, but they must be precertified byCIGNA Behavioral.
$150 per program,payable at admission
30%
$0
N/A
Intensive Outpatient MentalHealth/Substance Abuse
Employee Assistance Program(EAP)
Benefit is limited to 24 90-minute sessions per calendar year. Up to 12 of the24 sessions may be used for individual consultation. The Plan will reimburse70% up to $40.
Colleague Groups
Out-of-Network
YOUR COST SHARECOVERED HEALTH SERVICE
Substance Abuse
Everything you discuss with your counselor or care provider is kept in the strictest confidence in accordance withapplicable state and federal laws. Your employer is not notified of your visits or given specific information aboutyour treatment without your written permission. The general health privacy and security standards of theEpiscopal Church Medical Trust apply.
CIGNA Behavioral Health Member Services Toll-Free Number: (866) 395-7794

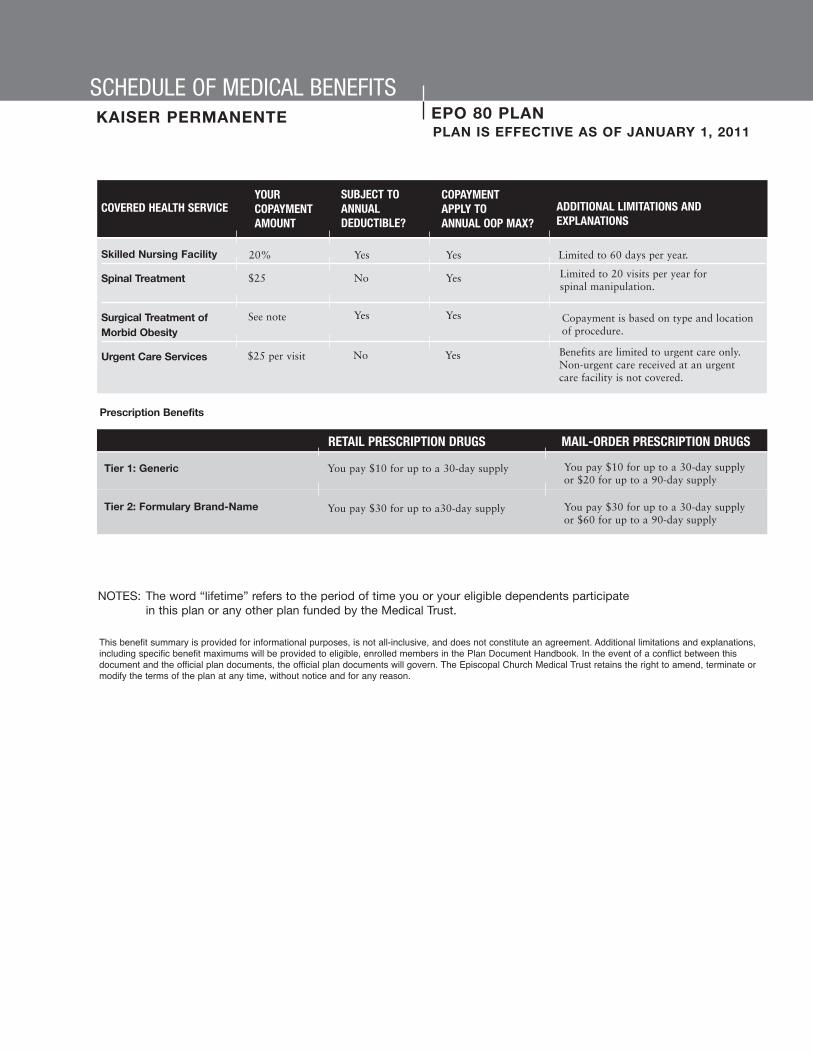
SCHEDULE OF MEDICAL BENEFITSEPO 80 PLAN
You must receive services only from healthcare providers participating in the Kaiser Permanente network, or benefits will not becovered by the plan. Expenses for out-of-network providers will only be considered as specified in this Handbook.
The following schedule summarizes coinsurance amounts paid by the Plan, benefit maximums, and any additional explanationneeded for your benefits. Please refer to the text for additional Plan provisions that may affect your benefits.The copayment refers to the copayment amount, whether it is expressed as a dollar amount (e.g. $20 per visit) or as apercentage (e.g. 10%).
Our Benefits: Although a specific service may be listed as a covered expense, it may not be covered unless it is medicallynecessary for the prevention, diagnosis or treatment of an illness or condition.
Annual Deductible
$ 500 Individual$1,000 Family
Annual Out-of-Pocket Maximums
$3,000 Individual$6,000 Family
KAISER PERMANENTEPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
COVERED HEALTH SERVICE
Acupuncture Services
Allergy Testing
Ambulance Services
Diagnostic Tests/X-Rayand Laboratory Services
Durable Medical
Emergency Room 20% Services
Home Health Care
Limited to 12 visits per calendar year.
COPAYMENTAPPLY TO ANNUAL OOP MAX?
SUBJECT TOANNUALDEDUCTIBLE?
YOURCOPAYMENTAMOUNT
ADDITIONAL LIMITATIONS ANDEXPLANATIONS
See note
$25
Yes
No
NoYou must pay a $25 PCP/$35 specialist copayper visit for allergy testing to a networkprovider if office visit charged. (Injections)
20% Yes
20%
Equipment (DME) 20%
Benefits include nurse visits (2 hours), aidevisits (4 hours), therapy visits, and supplies.Limited to 200 visits per calendar year.
$0 No
Yes
Yes
Yes
Yes
Yes
No No
N/A
Yes
Lifetime Benefit Maximum(Includes All Other Maximums)
None

Hospice Care
Hospital Services
Hospital Services(Outpatient)
Maternity Services
Mental Health/ Substance Abuse Services - Inpatient
Mental Health/ Substance AbuseServices - Outpatient
Nutritional Counseling
Outpatient TherapyServices
Physician’s OfficeServices
Routine & PreventiveServices
SCHEDULE OF MEDICAL BENEFITS EPO 80 PLAN
SCHEDULE OF MEDICAL BENEFITSKAISER PERMANENTE
PLAN IS EFFECTIVE AS OF JANUARY 1, 2011
COVERED HEALTH SERVICE COPAYMENTAPPLY TO ANNUAL OOP MAX?
YOURCOPAYMENTAMOUNT
ADDITIONAL LIMITATIONS ANDEXPLANATIONS
No$0
Yes
20%
Benefits include room and board for privateand semi-private rooms, ICU/CCU, acuterehab, inpatient professional services,medically necessary private duty nursing,ancillary services, and supplies.
Benefits include but are not limited tooutpatient surgery, physician, anesthesiology,x-ray & laboratory, and therapy expenses ina hospital or ambulatory surgical center. Allservices provided during the primaryprocedure are covered by the HospitalServices (Outpatient) copay.
Benefits include contracted birthing centers.
20%
Yes20%
(Inpatient)
Hospital Services
Outpatient Services $0 for all pre-natalvisits, includingpost partum
Yes
20% Yes
$25 per day forindividual visit;$12 for group visit
No
No
No$25 PCP/$35specialist per visit
Benefits include physical,occupational, and speech therapy.Limited to 60 visits each per year.
$25 per visit No
All services provided during the officevisit are covered under the Physician’sOffice Services copay.
No$25 PCP/$35specialist per visit
Benefits include the office visit andvaccinations, inoculations, andimmunizations. Well-Child checkupsare limited to those less than 24months old. Frequency and age limitsfor those age 24 months and older aremanaged by the KP provider. Benefitsinclude routine physicals, includinggynecological exams, digital rectalexams, mammograms, PAP tests, andPSA screenings.
No
N/A
Yes
Yes
Yes
Yes
Yes
N/A
Yes
Yes
Yes
n/a$0 per visit
Routine ExamsRoutine Exam X-Rays & Laboratory ServicesWell-Child CheckupsMammogramsRoutine ColonoscopyRoutine SigmoidoscopyOther Routine Services
SUBJECT TOANNUALDEDUCTIBLE?
SCHEDULE OF MEDICAL BENEFITSEPO 80 PLANKAISER PERMANENTEPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Skilled Nursing Facility
Spinal Treatment
Surgical Treatment of Morbid Obesity
Urgent Care Services
COVERED HEALTH SERVICE COPAYMENTAPPLY TO ANNUAL OOP MAX?
YOURCOPAYMENTAMOUNT
ADDITIONAL LIMITATIONS ANDEXPLANATIONS
Yes20% Limited to 60 days per year.
No$25
$25 per visit
YesSee note
No
Yes
Yes
Yes
Yes
Limited to 20 visits per year forspinal manipulation.
NOTES: The word “lifetime” refers to the period of time you or your eligible dependents participate in this plan or any other plan funded by the Medical Trust.
Benefits are limited to urgent care only.Non-urgent care received at an urgentcare facility is not covered.
This benefit summary is provided for informational purposes, is not all-inclusive, and does not constitute an agreement. Additional limitations and explanations,including specific benefit maximums will be provided to eligible, enrolled members in the Plan Document Handbook. In the event of a conflict between thisdocument and the official plan documents, the official plan documents will govern. The Episcopal Church Medical Trust retains the right to amend, terminate ormodify the terms of the plan at any time, without notice and for any reason.
SUBJECT TOANNUALDEDUCTIBLE?
Prescription Benefits
You pay $10 for up to a 30-day supply
You pay $30 for up to a30-day supply
You pay $10 for up to a 30-day supplyor $20 for up to a 90-day supply
You pay $30 for up to a 30-day supplyor $60 for up to a 90-day supply
Tier 1: Generic
Tier 2: Formulary Brand-Name
RETAIL PRESCRIPTION DRUGS MAIL-ORDER PRESCRIPTION DRUGS
Copayment is based on type and locationof procedure.

You must receive services only from healthcare providers participating in the UnitedHealthcare network, or benefits willnot be covered by the plan. Expenses for out-of-network providers will only be considered as specified in the Planhandbook.
The following schedule summarizes coinsurance amounts paid by the Plan, benefit maximums, and any additionalexplanation needed for your benefits. Please refer to the Coverage chapter for additional Plan provisions that mayaffect your benefits.
Our Benefits: Although a specific service may be listed as a covered expense, it may not be covered unless it ismedically necessary for the prevention, diagnosis or treatment of an illness or condition.
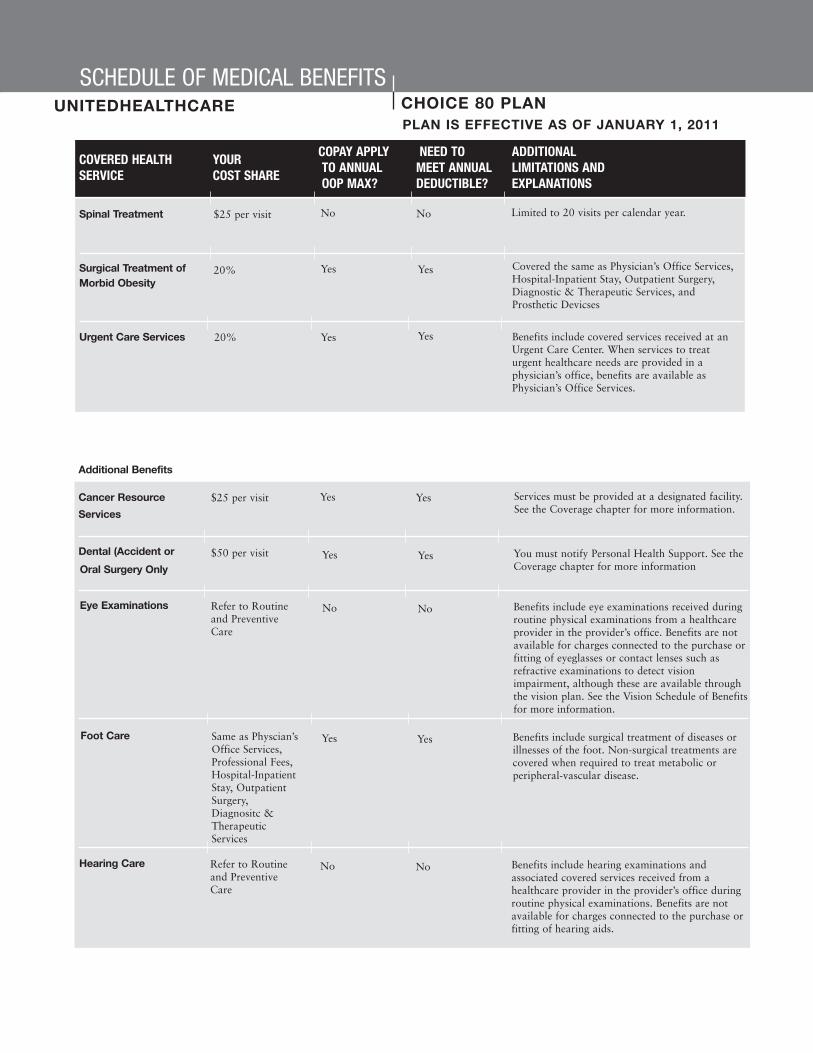
SCHEDULE OF MEDICAL BENEFITSCHOICE 80 PLANUNITEDHEALTHCAREPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Lifetime Benefit Maximum
(Includes All Other Maximums)
None
Annual Deductibles Annual Out-of-PocketMaximums
(Excludes Deductible)
Individual $1,000 Individual $1,500Family $2,000 Family $3,000
COVERED HEALTHSERVICE
YOUR COST SHARE
Acupuncture Services
Allergy Testing
Ambulance Services -
Diagnostic Tests/X-Rayand Laboratory Services
Durable Medical
Limited to 12 visits per calendar year.Acupuncture services received on an inpatientbasis are not covered.
Emergency ambulance transportation by a licensedambulance service to the nearest hospital whereemergency health services can be performed. Non-emergency amublance services are not covered.Services must be provided at a designated facility.Se the Coverage chapter for more details
Yes No
COPAY APPLYTO ANNUALOOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
$25 per visit
Ground or AirTrasportation20%
NoNo
$25 per visit NoNo
Benefits are available for injections received in aphysician’s office when no other health service isreceived, for example, allergy immunotherapy.Benefits include serum for allergy care.
(Injections)
20%
Yes Yes20%
Yes No
Equipment (DME)
Emergency Only

SCHEDULE OF MEDICAL BENEFITSCHOICE 80 PLANUNITEDHEALTHCAREPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Emergency Room Services
Home Health Care
Hospice Care
Hospital Services
Hospital Services(Outpatient)
Maternity Services
The $50 copay will be waived if you are admittedto the hospital. Hospital admission must beprecertified within 24 hours.
COVERED HEALTHSERVICE
YOURCOST SHARE
COPAY APPLYTO ANNUALOOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
YesYes Benefits limited to 210 visits per calendar year. Onevisit equals 4 hours of skilled care services. See theCoverage chapter for more details.
20%
NoNo$50
YesYes20%
YesYes
YesYes20%
Benefits are available for services and suppliesreceived during the inpatient stay and room andboard in a semi-private room (a room with two ormore beds).
20%
(Inpatient)
Antepartum care only.
Benefits are the same as Professional Fees,Hospital-Inpatient Stay, Outpatient Surgery, andDiagnostic & Therapeutic Services. See theCoverage chapter for more information.
Hospital Services
Outpatient Services
Benefits include covered health services receivedon an outpatient basis at a hospital or alternatefacility including: surgery and related services, laband radiology/x-ray, mammography testing, andother diagnostic tests and therapeutic treatments(including cancer chemotherapy or intravenousinfusion therapy). Benefits under this sectioninclude only the facility charge and the charge forrequired services, supplies, and equipment.Benefits for the professional fees related tooutpatient surgery, diagnostic, and therapeuticservices are described under Professional Fees forSurgical & Medical Services below. When theseservices are performed in a physician’s office,benefits are described under Physician’s OfficeVisits.
20%
$25 for first visitonly
No No
No No

SCHEDULE OF MEDICAL BENEFITSCHOICE 80 PLANUNITEDHEALTHCAREPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Nutritional Counseling
Outpatient TherapyServices
Physician’s OfficeServices
Routine & PreventiveServices
Skilled Nursing Facility/
COVERED HEALTHSERVICE
YOURCOST SHARE
COPAY APPLYTO ANNUALOOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
Beneifts include services provided by aregistered dietician in an individual session.Limited to 6 sessions per calendar year.
Benefits include hearing/speech, physical andoccupational therapy. Limited to 60 visits per planyear, combined facility and office, per each of thethree therapies.
No No$25 per visit
$25 per visit No No
Benefits include routine physicals, includinggynecological exams, limited to 1 per year; hearingexams performed by your physician during aroutine physical, limited to 1 per year; andvaccinations, inoculations, and immunizations.Pap tests, limited to 1 per year; mammograms,limited to 1 per year age 40+, 1 age 35-39; PSAscreenings, limited to 2 per year age 40+; and allrelated routine x-rays and laboratory services.Well-child checkups limited to 7 visits from birthto age 1, 6 visits from age 1 through age 5, 7 visitsfrom age 5 through age 12, 6 visits from age 12through age 18, and 2 visits age 18 up to the 19thbirthday. Benefits include the office visit,vaccinations, inoculations, immunizations, and allrelated x-ray and laboratory services. Routinesigmoidoscopy limited to 1 every 2 years, age 40+.Routine colonoscopy limited to 1 every 10 years,age 50+.
No No
n/a No
Yes Yes
$25 per visit
$0
20%
Routine ExamsRoutine Exam X-Rays & Laboratory ServicesWell-Child CheckupsRoutine ColonoscopyRoutine SigmoidoscopyOther Routine Services
Limited to 60 days per year. If you are transferredto a skilled nursing facility or inpatientrehabilitation facility directly from an acutefacility, any combination of copayments requiredfor the inpatient stay in a hospital and theinpatient stay in a skilled nursing facility orinpatient rehabilitation facility will apply to thestated maximum copayment per inpatient stay.
Inpatient RehabilitationFacility Services
SCHEDULE OF MEDICAL BENEFITSCHOICE 80 PLANUNITEDHEALTHCAREPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Spinal Treatment
Surgical Treatment of Morbid Obesity
Urgent Care Services
COVERED HEALTHSERVICE
YOUR COST SHARE
COPAY APPLYTO ANNUALOOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
No$25 per visit No
Yes20% Yes Covered the same as Physician’s Office Services,Hospital-Inpatient Stay, Outpatient Surgery,Diagnostic & Therapeutic Services, andProsthetic Devicses
Benefits include covered services received at anUrgent Care Center. When services to treaturgent healthcare needs are provided in aphysician’s office, benefits are available asPhysician’s Office Services.
Limited to 20 visits per calendar year.
20% YesYes
Cancer Resource
Dental (Accident or
Services must be provided at a designated facility.See the Coverage chapter for more information.
Yes Yes$25 per visit
You must notify Personal Health Support. See theCoverage chapter for more information
$50 per visit Yes Yes
Additional Benefits
Services
Oral Surgery Only
Benefits include eye examinations received duringroutine physical examinations from a healthcareprovider in the provider’s office. Benefits are notavailable for charges connected to the purchase orfitting of eyeglasses or contact lenses such asrefractive examinations to detect visionimpairment, although these are available throughthe vision plan. See the Vision Schedule of Benefitsfor more information.
Refer to Routineand PreventiveCare
No NoEye Examinations
Benefits include surgical treatment of diseases orillnesses of the foot. Non-surgical treatments arecovered when required to treat metabolic orperipheral-vascular disease.
Same as Physcian’sOffice Services,Professional Fees,Hospital-InpatientStay, OutpatientSurgery,Diagnositc &TherapeuticServices
Yes YesFoot Care
Benefits include hearing examinations andassociated covered services received from ahealthcare provider in the provider’s office duringroutine physical examinations. Benefits are notavailable for charges connected to the purchase orfitting of hearing aids.
Refer to Routineand PreventiveCare
No NoHearing Care
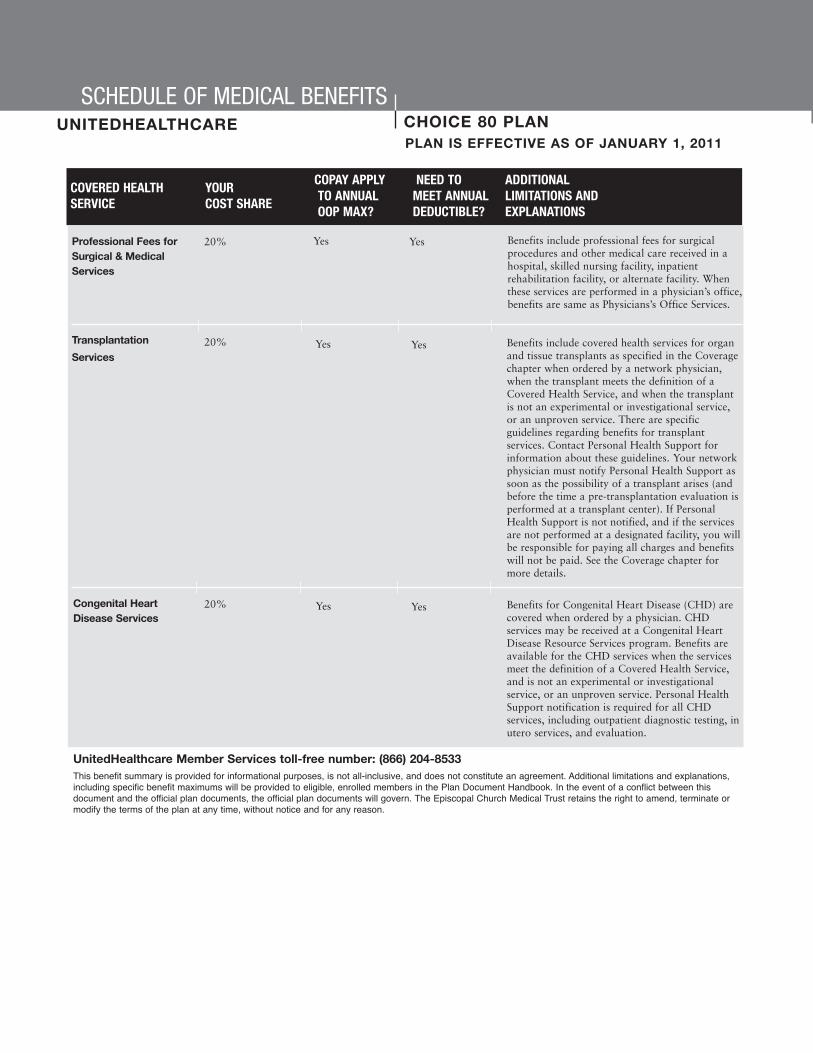
UnitedHealthcare Member Services toll-free number: (866) 204-8533This benefit summary is provided for informational purposes, is not all-inclusive, and does not constitute an agreement. Additional limitations and explanations,including specific benefit maximums will be provided to eligible, enrolled members in the Plan Document Handbook. In the event of a conflict between thisdocument and the official plan documents, the official plan documents will govern. The Episcopal Church Medical Trust retains the right to amend, terminate ormodify the terms of the plan at any time, without notice and for any reason.
Professional Fees for
Transplantation
Benefits include professional fees for surgicalprocedures and other medical care received in ahospital, skilled nursing facility, inpatientrehabilitation facility, or alternate facility. Whenthese services are performed in a physician’s office,benefits are same as Physicians’s Office Services.
Yes Yes20%
Benefits include covered health services for organand tissue transplants as specified in the Coveragechapter when ordered by a network physician,when the transplant meets the definition of aCovered Health Service, and when the transplantis not an experimental or investigational service,or an unproven service. There are specificguidelines regarding benefits for transplantservices. Contact Personal Health Support forinformation about these guidelines. Your networkphysician must notify Personal Health Support assoon as the possibility of a transplant arises (andbefore the time a pre-transplantation evaluation isperformed at a transplant center). If PersonalHealth Support is not notified, and if the servicesare not performed at a designated facility, you willbe responsible for paying all charges and benefitswill not be paid. See the Coverage chapter formore details.
20% Yes Yes
Surgical & MedicalServices
Services
Benefits for Congenital Heart Disease (CHD) arecovered when ordered by a physician. CHDservices may be received at a Congenital HeartDisease Resource Services program. Benefits areavailable for the CHD services when the servicesmeet the definition of a Covered Health Service,and is not an experimental or investigationalservice, or an unproven service. Personal HealthSupport notification is required for all CHDservices, including outpatient diagnostic testing, inutero services, and evaluation.
20% Yes YesCongenital HeartDisease Services
SCHEDULE OF MEDICAL BENEFITSCHOICE 80 PLANUNITEDHEALTHCAREPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
COVERED HEALTHSERVICE
YOURCOST SHARE
COPAY APPLYTO ANNUALOOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS

SCHEDULE OF MENTAL HEALTH/SUBSTANCE ABUSE BENEFITSCIGNA BEHAVIORAL HEALTH PLAN IS EFFECTIVE AS OF JANUARY 1, 2011
The following schedule summarizes your mental health and substance abuse benefits, coinsurance amounts, benefitmaximums, and any additional explanation needed for your benefits. Please refer to the Mental Health/SubstanceAbuse chapter for additional Plan provisions. All coinsurances apply to your health plan’s out-of-pocket maximums.
FOR MEMBERS ENROLLED IN THE UNITEDHEALTHCARE CHOICE 80 PLAN
Outpatient Mental Health/ There is no annual limit.
ADDITIONAL LIMITATIONS AND EXPLANATIONS
Network
Network
Out-of-Network
Network$20 per visit
Out-of-Network30%
All admissions must be precertified. There is no annual limit. Plan coverage isreduced to 50% if there is no precertification. Emergency room, ambulance,and lab work charges are covered by your medical plan.
Inpatient Mental Health/Substance Abuse 20%
30%
Network
Out-of-Network
All programs must be precertified. There is no annual limit. Plan coverage isreduced to 50% if there is no precertification.
Benefits include (but are not limited to) unlimited telephonic and work/lifeservices, crisis intervention, referrals to community resources, legalconsultations, and a large online resource library. You may also receive up to10 face-to-face counseling sessions per issue, but they must be precertified byCIGNA Behavioral.
$150 per program,payable at admission
30%
$0
N/A
Intensive Outpatient MentalHealth/Substance Abuse
Employee Assistance Program(EAP)
Benefit is limited to 24 90-minute sessions per calendar year. Up to 12 of the24 sessions may be used for individual consultation. The Plan will reimburse70% up to $40.
Colleague Groups
Out-of-Network
YOUR COST SHARECOVERED HEALTH SERVICE
Substance Abuse
Everything you discuss with your counselor or care provider is kept in the strictest confidence in accordance withapplicable state and federal laws. Your employer is not notified of your visits or given specific information aboutyour treatment without your written permission. The general health privacy and security standards of theEpiscopal Church Medical Trust apply.
CIGNA Behavioral Health Member Services Toll-Free Number: (866) 395-7794
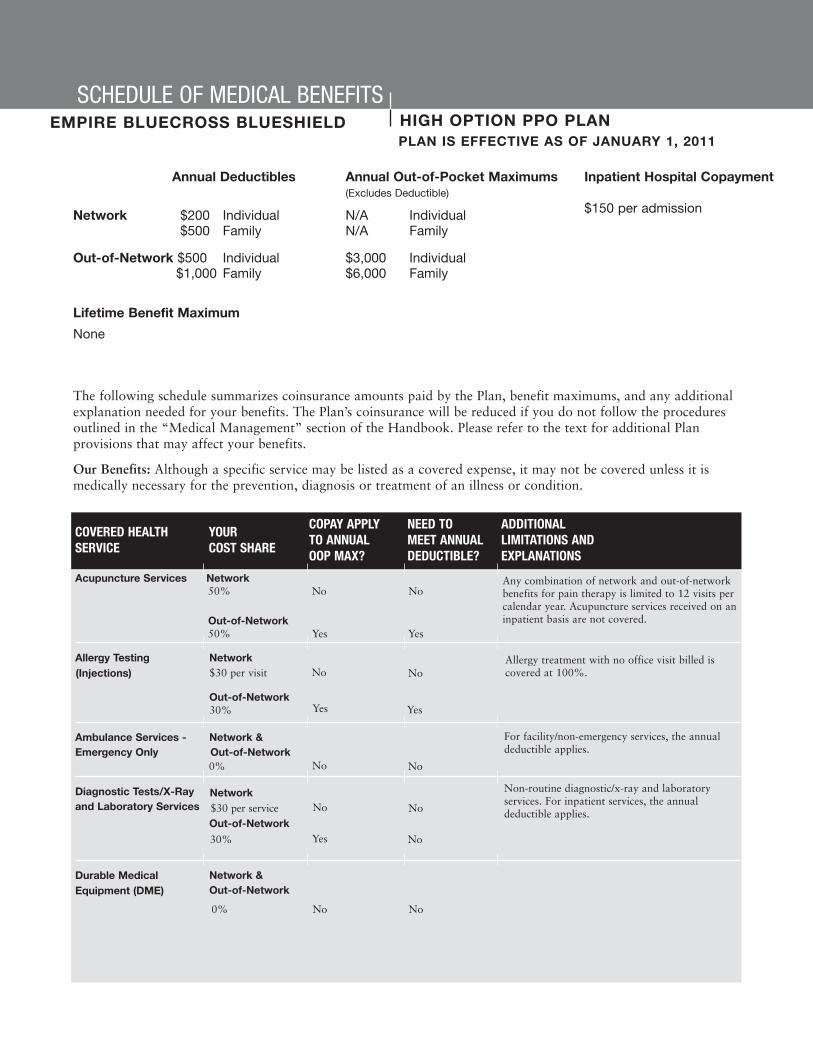
The following schedule summarizes coinsurance amounts paid by the Plan, benefit maximums, and any additionalexplanation needed for your benefits. The Plan’s coinsurance will be reduced if you do not follow the proceduresoutlined in the “Medical Management” section of the Handbook. Please refer to the text for additional Planprovisions that may affect your benefits.
Our Benefits: Although a specific service may be listed as a covered expense, it may not be covered unless it ismedically necessary for the prevention, diagnosis or treatment of an illness or condition.
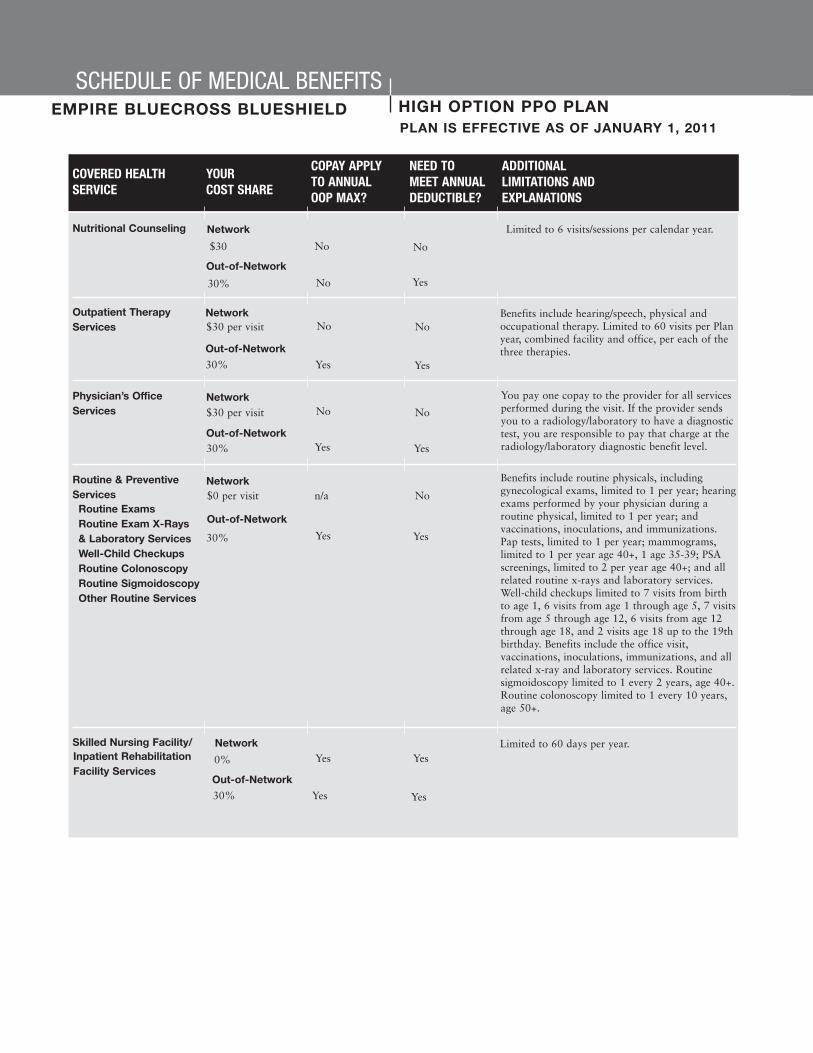
SCHEDULE OF MEDICAL BENEFITSHIGH OPTION PPO PLANEMPIRE BLUECROSS BLUESHIELDPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Lifetime Benefit Maximum
None
Annual Deductibles Annual Out-of-Pocket Maximums(Excludes Deductible)
Network $200 Individual N/A Individual$500 Family N/A Family
Out-of-Network $500 Individual $3,000 Individual$1,000 Family $6,000 Family
Inpatient Hospital Copayment
$150 per admission
COVERED HEALTHSERVICE
YOURCOST SHARE
Acupuncture Services Network50% No No
Out-of-Network50% Yes Yes
Allergy Testing
Ambulance Services - Network &Emergency Only Out-of-Network
Diagnostic Tests/X-Rayand Laboratory Services
Durable Medical
Any combination of network and out-of-networkbenefits for pain therapy is limited to 12 visits percalendar year. Acupuncture services received on aninpatient basis are not covered.
For facility/non-emergency services, the annualdeductible applies.
Non-routine diagnostic/x-ray and laboratoryservices. For inpatient services, the annualdeductible applies.
No No
Yes No
COPAY APPLYTO ANNUALOOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
Network
Network &Out-of-Network
Out-of-Network
Network$30 per visit
Out-of-Network30% Yes
No
Yes
NoAllergy treatment with no office visit billed iscovered at 100%.(Injections)
$30 per service
30%
No No0%
0% No No
Equipment (DME)

SCHEDULE OF MEDICAL BENEFITSHIGH OPTION PPO PLANEMPIRE BLUECROSS BLUESHIELDPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Emergency Room Network & Services Out-of-Network
$50 per visit No No
Home Health Care Network
Hospice Care Network
30% Yes Yes
Hospital Services Network
Hospital Services(Outpatient)
Hypnosis
Maternity Services
The $50 copay will be waived if you are admittedto the hospital. Hospital admission must beprecertified within 24 hours.
COVERED HEALTHSERVICE
YOUR COST SHARE
COPAY APPLYTO ANNUALOOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
Yes
No
Yes
Yes Yes
No
Limited to 200 visits per plan year; precertificationis required.
Limited to one episode per lifetime. Benefitsinclude bereavement counseling. Precertification isrequired.
0%
YesNo0%
NoNo
Out-of-Network
Out-of-Network
Out-of-Network
30%
Yes
Yes
Yes
No$150
Network
Network
Network
30%
The Plan’s coinsurance for hospital expenses willbe reduced to 50% if you do not follow theprocedures required by the Medical ManagementProgram. This penalty does not apply to the out-of-pocket maximum.
$150 copay perin-networkadmission
30%
(Inpatient)
Out-of-network
Yes
No
Yes
No50%
Network
50%
Out-of-network
Antepartum care only.
Limited to 6 visits per year.
Out-of-Network
Hospital Services
Outpatient Services
The Plan’s coinsurance for hospital expenses willbe reduced to 50% if you do not follow theprocedures required by the Medical ManagementProgram. This penalty does not apply to the out-of-pocket maximum. Well-newborn care is alsocovered, but is not subject to the inpatienthospital deductible.
$150 copay per in-network admission
$30 for first visitonly
30%
Out-of-Network30%
No No
Yes Yes
No No
Yes Yes
SCHEDULE OF MEDICAL BENEFITSHIGH OPTION PPO PLANEMPIRE BLUECROSS BLUESHIELDPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Nutritional Counseling
Outpatient TherapyServices
Physician’s OfficeServices
Routine & PreventiveServices
Skilled Nursing Facility/
COVERED HEALTHSERVICE
YOUR COST SHARE
COPAY APPLYTO ANNUALOOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
Limited to 6 visits/sessions per calendar year.
Benefits include hearing/speech, physical andoccupational therapy. Limited to 60 visits per Planyear, combined facility and office, per each of thethree therapies.
Out-of-Network
No No$30
30% No Yes
$30 per visit No No
Yes Yes
Out-of-Network
Network
Network
30%
You pay one copay to the provider for all servicesperformed during the visit. If the provider sendsyou to a radiology/laboratory to have a diagnostictest, you are responsible to pay that charge at theradiology/laboratory diagnostic benefit level.
Benefits include routine physicals, includinggynecological exams, limited to 1 per year; hearingexams performed by your physician during aroutine physical, limited to 1 per year; andvaccinations, inoculations, and immunizations.Pap tests, limited to 1 per year; mammograms,limited to 1 per year age 40+, 1 age 35-39; PSAscreenings, limited to 2 per year age 40+; and allrelated routine x-rays and laboratory services.Well-child checkups limited to 7 visits from birthto age 1, 6 visits from age 1 through age 5, 7 visitsfrom age 5 through age 12, 6 visits from age 12through age 18, and 2 visits age 18 up to the 19thbirthday. Benefits include the office visit,vaccinations, inoculations, immunizations, and allrelated x-ray and laboratory services. Routinesigmoidoscopy limited to 1 every 2 years, age 40+.Routine colonoscopy limited to 1 every 10 years,age 50+.
Yes Yes
No No
Out-of-Network
Network
Network
Network
Out-of-Network
30%
Yes Yes
n/a No
30%
Out-of-Network
Yes Yes
Yes Yes
30%
$30 per visit
$0 per visit
0%
Routine ExamsRoutine Exam X-Rays & Laboratory ServicesWell-Child CheckupsRoutine ColonoscopyRoutine SigmoidoscopyOther Routine Services
Limited to 60 days per year.Inpatient RehabilitationFacility Services

SCHEDULE OF MEDICAL BENEFITSHIGH OPTION PPO PLANEMPIRE BLUECROSS BLUESHIELDPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Spinal Treatment Network
Surgical Treatment of Network Morbid Obesity
Urgent Care Services
COVERED HEALTHSERVICE
YOURCOST SHARE
COPAY APPLYTO ANNUALOOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
No
30%
$30 per visit
$50 per visit
YesYes
No
No
30%
0%
YesYes
Yes
No No
Limited to 1 procedure per lifetime. Whensurgery is performed inpatient, $150 hospitalcopay applies.
The $50 copay will be waived if you areadmitted to the hospital. Hospital admissionmust be precertified within 24 hours.
Limited to 20 visits per year.
Out-of-Network
Network &Out-of-Network
Anesthesiology Services
Organ Transplants For this benefit, “network plan” refers to theBCBS National Transplant Network.Precertification required. There is a $10,000 traveland lodging limit.
YesYes
0%
0%
30%
No No
No No
No NoOut-of-Network
Network
0%
0%Out-of-Network
Network
YesYes30%
No Yes
Out-of-Network
Network
Professional
Facility
Additional Benefits
Medical Management Program toll-free number: (800) 352-3152NOTES: The word “lifetime” refers to the period of time you or your eligible dependents participate
in this plan or any other plan sponsored by the Medical Trust.
This benefit summary is provided for informational purposes, is not all-inclusive, and does not constitute an agreement. Additional limitations and explanations,including specific benefit maximums will be provided to eligible, enrolled members in the Plan Document Handbook. In the event of a conflict between thisdocument and the official plan documents, the official plan documents will govern. The Episcopal Church Medical Trust retains the right to amend, terminate ormodify the terms of the plan at any time, without notice and for any reason.
Out-of-Network

SCHEDULE OF MENTAL HEALTH/SUBSTANCE ABUSE BENEFITSCIGNA BEHAVIORAL HEALTH PLAN IS EFFECTIVE AS OF JANUARY 1, 2011
The following schedule summarizes your mental health and substance abuse benefits, coinsurance amounts, benefitmaximums, and any additional explanation needed for your benefits. Please refer to the Mental Health/SubstanceAbuse chapter for additional Plan provisions. All coinsurances apply to your health plan’s out-of-pocket maximums.
FOR MEMBERS ENROLLED IN THE EMPIRE PPO HIGH OPTION PLAN
Outpatient Mental Health/ There is no annual limit.
ADDITIONAL LIMITATIONS AND EXPLANATIONS
Network
Network
Out-of-Network
Network$20 per visit
Out-of-Network30%
All admissions must be precertified. There is no annual limit. Plan coverage isreduced to 50% if there is no precertification. Emergency room, ambulance,and lab work charges are covered by your medical plan.
Inpatient Mental Health/Substance Abuse $150 per admission
30%
Network
Out-of-Network
All programs must be precertified. There is no annual limit. Plan coverage isreduced to 50% if there is no precertification.
Benefits include (but are not limited to) unlimited telephonic and work/lifeservices, crisis intervention, referrals to community resources, legalconsultations, and a large online resource library. You may also receive up to10 face-to-face counseling sessions per issue, but they must be precertified byCIGNA Behavioral.
$150 per program,payable at admission
30%
$0
N/A
Intensive Outpatient MentalHealth/Substance Abuse
Employee Assistance Program(EAP)
Benefit is limited to 24 90-minute sessions per calendar year. Up to 12 of the24 sessions may be used for individual consultation. The Plan will reimburse70% up to $40.
Colleague Groups
Out-of-Network
YOUR COST SHARECOVERED HEALTH SERVICE
Substance Abuse
Everything you discuss with your counselor or care provider is kept in the strictest confidence in accordance withapplicable state and federal laws. Your employer is not notified of your visits or given specific information aboutyour treatment without your written permission. The general health privacy and security standards of theEpiscopal Church Medical Trust apply.
CIGNA Behavioral Health Member Services Toll-Free Number: (866) 395-7794
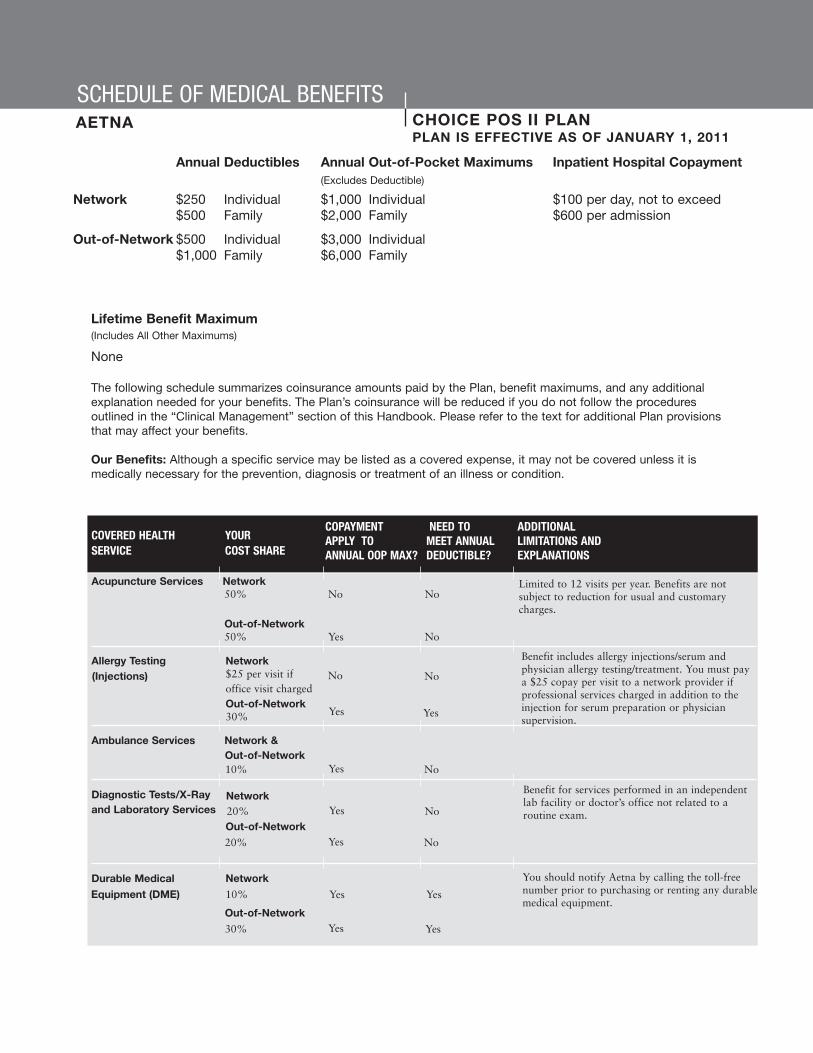
SCHEDULE OF MEDICAL BENEFITSCHOICE POS II PLANAETNAPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Lifetime Benefit Maximum(Includes All Other Maximums)
None
The following schedule summarizes coinsurance amounts paid by the Plan, benefit maximums, and any additionalexplanation needed for your benefits. The Plan’s coinsurance will be reduced if you do not follow the proceduresoutlined in the “Clinical Management” section of this Handbook. Please refer to the text for additional Plan provisionsthat may affect your benefits.
Our Benefits: Although a specific service may be listed as a covered expense, it may not be covered unless it ismedically necessary for the prevention, diagnosis or treatment of an illness or condition.
Annual Deductibles Annual Out-of-Pocket Maximums Inpatient Hospital Copayment(Excludes Deductible)
Network $250 Individual $1,000 Individual $100 per day, not to exceed $500 Family $2,000 Family $600 per admission
Out-of-Network $500 Individual $3,000 Individual$1,000 Family $6,000 Family
COVERED HEALTHSERVICE
YOUR COST SHARE
Acupuncture Services Network50% No No
Out-of-Network50% Yes No
Allergy Testing
Ambulance Services Network &Out-of-Network
Diagnostic Tests/X-Rayand Laboratory Services
Durable Medical
Limited to 12 visits per year. Benefits are notsubject to reduction for usual and customarycharges.
Yes No
Yes No
COPAYMENTAPPLY TO ANNUAL OOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
Network
Network
Out-of-Network
Network$25 per visit ifoffice visit chargedOut-of-Network30% Yes
No
Yes
No
Benefit includes allergy injections/serum andphysician allergy testing/treatment. You must paya $25 copay per visit to a network provider ifprofessional services charged in addition to theinjection for serum preparation or physiciansupervision.
Benefit for services performed in an independentlab facility or doctor’s office not related to aroutine exam.
You should notify Aetna by calling the toll-freenumber prior to purchasing or renting any durablemedical equipment.
(Injections)
20%
20%
Yes Yes
Out-of-Network
30%
Yes No10%
Equipment (DME) 10% Yes Yes

SCHEDULE OF MEDICAL BENEFITSCHOICE POS II PLANAETNAPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Emergency Room Network & Services Out-of-Network
$50 per visit No No
Home Health Care Network
Hospice Care Network
30% Yes Yes
Hospital Services Network
Hospital Services(Outpatient)
Hypnosis
Maternity Services
Your $50 copay will be waived if you areadmitted to the hospital. There is no coverage fornon-emergency treatment.
COVERED HEALTH SERVICE
YOUR COST SHARE
COPAYMENTAPPLY TO ANNUAL OOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Limited to 200 visits per plan year; precertificationis required. You should notify Aetna by calling thetoll-free number prior to receiving any homehealth care.
Limited to 210 visits per member. Benefits includebereavement counseling.
10%
YesYes10%
No
Out-of-Network
Out-of-Network
Out-of-Network
30%
Yes
Yes
Yes
Yes10%
Network
Network
Network
30%
The plan’s coinsurance for hospital expenses willbe reduced to 50% if you do not follow theprocedures required by the Clinical ManagmentProgram. This penalty does not apply to the out-of-pocket maximum. Benefits include, but are notlimited to, hospital semi-private room,miscellaneous fees, anesthesia, surgeons’ fees,physician visits, x-ray, lab and therapy expenses.
Benefits include but are not limited to outpatientsurgery, physician, anesthesiology, x-ray &laboratory, and therapy expenses in a hospital orambulatory surgical center.
10%
30%
(Inpatient)
Out-of-Network
Yes
No
No
No50%Network
50%
Limited to 6 visits per year.
Out-of-Network
Out-of-Network
Hospital Services
Outpatient Services
The Plan’s coinsurance for hospital expenses willbe reduced to 50% if you do not follow theprocedures required by the Medical ManagementProgram. This penalty does not apply to the out-of-pocket maximum.
10%
$25 for first visitonly
30%
Out-of-Network30%
No
Yes
Yes
Yes
No No
Yes Yes
$100 per daycopay, $600maximum perinpatient stay.
Subject to a $100copay per day,$600 maximumper inpatient stay
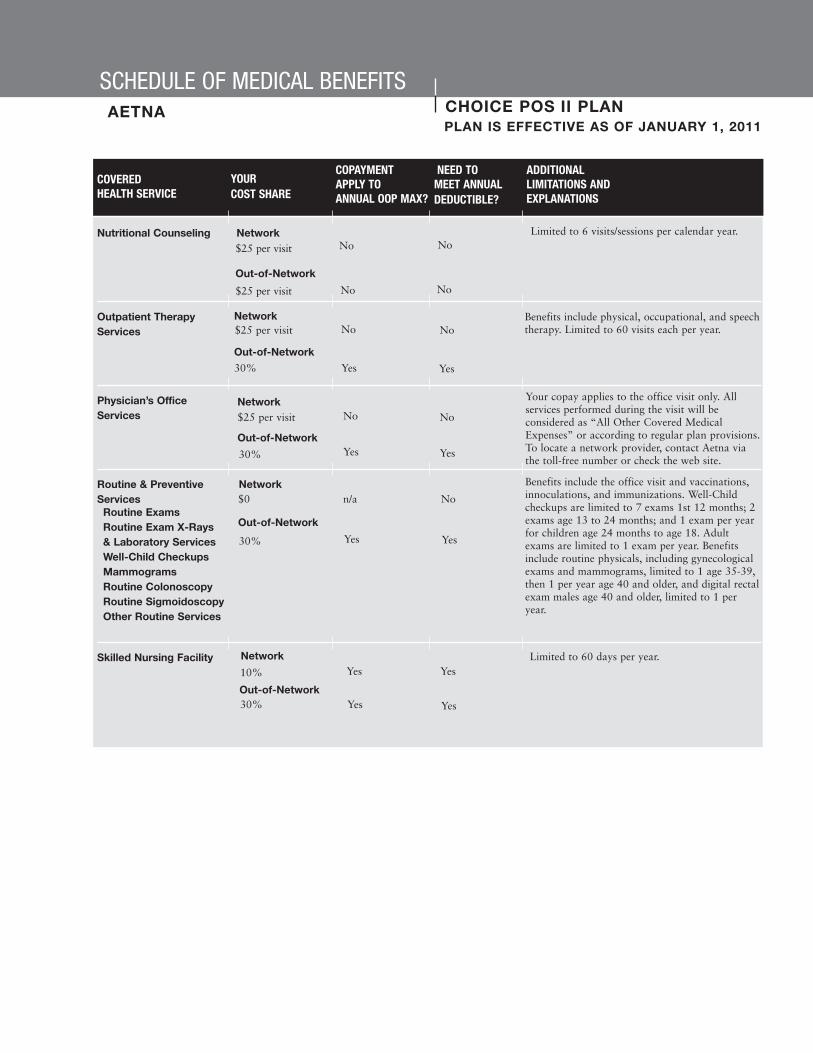
SCHEDULE OF MEDICAL BENEFITSCHOICE POS II PLANAETNAPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Nutritional Counseling Network
Outpatient TherapyServices
Physician’s OfficeServices
Routine & PreventiveServices
Skilled Nursing Facility
COVERED HEALTH SERVICE
YOUR COST SHARE
COPAYMENTAPPLY TO ANNUAL OOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
Limited to 6 visits/sessions per calendar year.
Benefits include physical, occupational, and speechtherapy. Limited to 60 visits each per year.
Out-of-Network
No No$25 per visit
$25 per visit No No
$25 per visit No No
Yes Yes
Out-of-Network
Network
30%
Your copay applies to the office visit only. Allservices performed during the visit will beconsidered as “All Other Covered MedicalExpenses” or according to regular plan provisions.To locate a network provider, contact Aetna viathe toll-free number or check the web site.
Benefits include the office visit and vaccinations,innoculations, and immunizations. Well-Childcheckups are limited to 7 exams 1st 12 months; 2exams age 13 to 24 months; and 1 exam per yearfor children age 24 months to age 18. Adultexams are limited to 1 exam per year. Benefitsinclude routine physicals, including gynecologicalexams and mammograms, limited to 1 age 35-39,then 1 per year age 40 and older, and digital rectalexam males age 40 and older, limited to 1 peryear.
Yes Yes
No No
Out-of-Network
Network
Network
Network
Out-of-Network
30%
Yes Yes
n/a No
30%
Out-of-NetworkYes Yes
Yes Yes
30%
$25 per visit
$0
10%
Routine ExamsRoutine Exam X-Rays & Laboratory ServicesWell-Child CheckupsMammogramsRoutine ColonoscopyRoutine SigmoidoscopyOther Routine Services
Limited to 60 days per year.

SCHEDULE OF MEDICAL BENEFITSCHOICE POS II PLANAETNAPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Clinical Management Program toll-free number: (877) 235-4005
NOTES: The word “lifetime” refers to the period of time you or your eligible dependents participate in this plan or any otherplan funded by the Medical Trust.
Spinal Treatment Network
Surgical Treatment of Network Morbid Obesity
Urgent Care Services
COVERED HEALTH SERVICE
YOUR COST SHARE
COPAYMENTAPPLY TO ANNUAL OOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
No
30%
$25 per visit
$25
YesYes
No
Yes
30%
10%
YesYes
Yes
No No
Limited to 1 procedure per lifetime. Must bepreauthorized by Aetna.
Benefits are limited to urgent care only. Non-urgent care received at an urgent care facility isnot covered.
Limited to 20 outpatient visits per year for spinalmanipulation.
Out-of-Network
Network & Out-of-Network
Out-of-Network
This benefit summary is provided for informational purposes, is not all-inclusive, and does not constitute an agreement. Additional limitations and explanations,including specific benefit maximums will be provided to eligible, enrolled members in the Plan Document Handbook. In the event of a conflict between thisdocument and the official plan documents, the official plan documents will govern. The Episcopal Church Medical Trust retains the right to amend, terminate ormodify the terms of the plan at any time, without notice and for any reason.

SCHEDULE OF MENTAL HEALTH/SUBSTANCE ABUSE BENEFITSCIGNA BEHAVIORAL HEALTH PLAN IS EFFECTIVE AS OF JANUARY 1, 2011
The following schedule summarizes your mental health and substance abuse benefits, coinsurance amounts, benefitmaximums, and any additional explanation needed for your benefits. Please refer to the Mental Health/SubstanceAbuse chapter for additional Plan provisions. All coinsurances apply to your health plan’s out-of-pocket maximums.
FOR MEMBERS ENROLLED IN THE AETNA CHOICE POS II PLAN
Outpatient Mental Health/ There is no annual limit.
ADDITIONAL LIMITATIONS AND EXPLANATIONS
Network
Network
Out-of-Network
Network$20 per visit
Out-of-Network30%
All admissions must be precertified. There is no annual limit. Plan coverage isreduced to 50% if there is no precertification. Emergency room, ambulance,and lab work charges are covered by your medical plan.
Inpatient Mental Health/Substance Abuse $100 per day, not to
exceed $600 peradmission
30%
Network
Out-of-Network
All programs must be precertified. There is no annual limit. Plan coverage isreduced to 50% if there is no precertification.
Benefits include (but are not limited to) unlimited telephonic and work/lifeservices, crisis intervention, referrals to community resources, legalconsultations, and a large online resource library. You may also receive up to10 face-to-face counseling sessions per issue, but they must be precertified byCIGNA Behavioral.
$150 per program,payable at admission
30%
$0
N/A
Intensive Outpatient MentalHealth/Substance Abuse
Employee Assistance Program(EAP)
Benefit is limited to 24 90-minute sessions per calendar year. Up to 12 of the24 sessions may be used for individual consultation. The Plan will reimburse70% up to $40.
Colleague Groups
Out-of-Network
YOUR COST SHARECOVERED HEALTH SERVICE
Substance Abuse
Everything you discuss with your counselor or care provider is kept in the strictest confidence in accordance withapplicable state and federal laws. Your employer is not notified of your visits or given specific information aboutyour treatment without your written permission. The general health privacy and security standards of theEpiscopal Church Medical Trust apply.
CIGNA Behavioral Health Member Services Toll-Free Number: (866) 395-7794

The following schedule summarizes coinsurance amounts paid by the Plan, benefit maximums, and any additionalexplanation needed for your benefits. The Plan’s coinsurance will be reduced if you do not follow the proceduresoutlined in the “Medical Management” section of the handbook. Please refer to the text for additional Planprovisions that may affect your benefits.
Our Benefits: Although a specific service may be listed as a covered expense, it may not be covered unless it ismedically necessary for the prevention, diagnosis or treatment of an illness or condition.
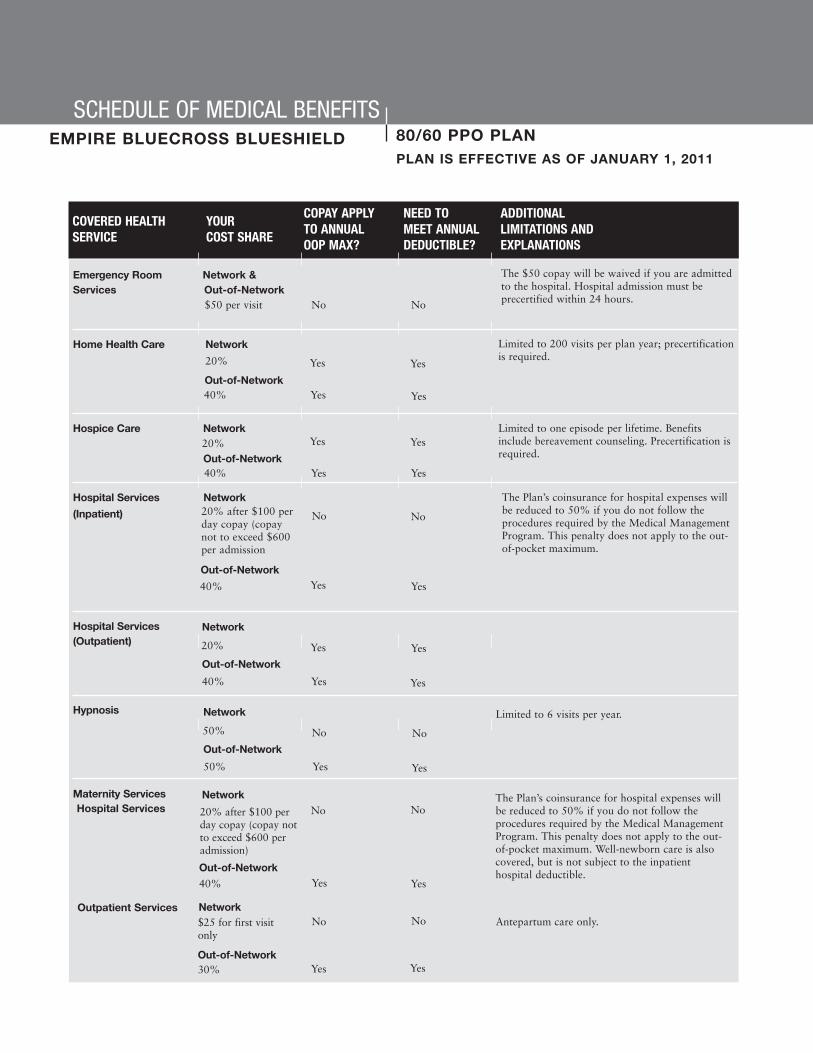
SCHEDULE OF MEDICAL BENEFITS80/60 PPO PLANEMPIRE BLUECROSS BLUESHIELDPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Lifetime Benefit Maximum
None
Annual Deductibles Annual Out-of-Pocket Maximums(Excludes Deductible)
Network $500 Individual $1,500 Individual$1,000 Family $3,000 Family
Out-of-Network $1,000 Individual $4,500 Individual$2,000 Family $9,000 Family
Inpatient Hospital Copayment
$100 per day, not to exceed$600 per admission
COVERED HEALTHSERVICE
YOUR COST SHARE
Acupuncture Services Network50% No No
Allergy Testing
Ambulance Services - Network &Emergency Only Out-of-Network
Diagnostic Tests/X-Rayand Laboratory Services
Durable Medical
Any combination of network and out-of-networkbenefits for pain therapy is limited to 12 visits percalendar year. Acupuncture services received on aninpatient basis are not covered.
For facility/non-emergency services, you will pay40% and the annual deductible applies.
Yes No
Yes Yes
COPAY APPLYTO ANNUALOOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
Network
Network
Out-of-Network
Network$25 per visit
Out-of-Network40% Yes
No
Yes
NoAllergy treatment with no office visit billed iscovered at 100%.(Injections)
20%
20%
Yes No20%
20% No No
20% Yes Yes
Equipment (DME)
Out-of-Network
Out-of-Network50%
SCHEDULE OF MEDICAL BENEFITS80/60 PPO PLANEMPIRE BLUECROSS BLUESHIELDPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Emergency Room Network & Services Out-of-Network
$50 per visit No No
Home Health Care Network
Hospice Care Network
40% Yes Yes
Hospital Services Network
Hospital Services(Outpatient)
Hypnosis
Maternity Services
The $50 copay will be waived if you are admittedto the hospital. Hospital admission must beprecertified within 24 hours.
COVERED HEALTHSERVICE
YOURCOST SHARE
COPAY APPLYTO ANNUALOOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
Yes
Yes
Yes
Yes Yes
Yes
Limited to 200 visits per plan year; precertificationis required.
Limited to one episode per lifetime. Benefitsinclude bereavement counseling. Precertification isrequired.
20%
YesYes20%
NoNo
Out-of-Network
Out-of-Network
Out-of-Network
40%
Yes
Yes
Yes
Yes20%
Network
Network
Network
40%
The Plan’s coinsurance for hospital expenses willbe reduced to 50% if you do not follow theprocedures required by the Medical ManagementProgram. This penalty does not apply to the out-of-pocket maximum.
20% after $100 perday copay (copaynot to exceed $600per admission
40%
(Inpatient)
Out-of-Network
Yes
No
Yes
No50%
Network
50%
Out-of-Network
Antepartum care only.
Limited to 6 visits per year.
Out-of-Network
Hospital Services
Outpatient Services
The Plan’s coinsurance for hospital expenses willbe reduced to 50% if you do not follow theprocedures required by the Medical ManagementProgram. This penalty does not apply to the out-of-pocket maximum. Well-newborn care is alsocovered, but is not subject to the inpatienthospital deductible.
20% after $100 perday copay (copay notto exceed $600 peradmission)
$25 for first visitonly
40%
Out-of-Network30%
No No
Yes Yes
No No
Yes Yes

SCHEDULE OF MEDICAL BENEFITS80/60 PPO PLANEMPIRE BLUECROSS BLUESHIELDPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Nutritional Counseling Network
Outpatient TherapyServices
Physician’s OfficeServices
Routine & PreventiveServices
Skilled Nursing Facility/
COVERED HEALTHSERVICE
YOURCOST SHARE
COPAY APPLYTO ANNUALOOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
Limited to 6 visits/sessions per calendar year.
Benefits include hearing/speech, physical andoccupational therapy. Limited to 60 visits per Planyear, combined facility and office, per each of thethree therapies.
Out-of-Network
No No$25 per visit
40% No No
$25 per visit No No
Yes Yes
Out-of-Network
Network
40%
You pay one copay to the provider for all servicesperformed during the visit. If the provider sendsyou to a radiology/laboratory to have a diagnostictest, you are responsible to pay that charge at theradiology/laboratory diagnostic benefit level.
Benefits include routine physicals, includinggynecological exams, limited to 1 per year; hearingexams performed by your physician during aroutine physical, limited to 1 per year; andvaccinations, inoculations, and immunizations.Pap tests, limited to 1 per year; mammograms,limited to 1 per year age 40+, 1 age 35-39; PSAscreenings, limited to 2 per year age 40+; and allrelated routine x-rays and laboratory services.Well-child checkups limited to 7 visits from birthto age 1, 6 visits from age 1 through age 5, 7 visitsfrom age 5 through age 12, 6 visits from age 12through age 18, and 2 visits age 18 up to the 19thbirthday. Benefits include the office visit,vaccinations, inoculations, immunizations, and allrelated x-ray and laboratory services. Routinesigmoidoscopy limited to 1 every 2 years, age 40+.Routine colonoscopy limited to 1 every 10 years,age 50+.
Yes Yes
No No
Out-of-Network
Network
Network
Network
Out-of-Network
40%
Yes Yes
n/a No
40%
Out-of-NetworkYes Yes
Yes Yes
40%
$25 per visit
$0 per visit
20%
Routine ExamsRoutine Exam X-Rays & Laboratory ServicesWell-Child CheckupsRoutine ColonoscopyRoutine SigmoidoscopyOther Routine Services
Limited to 60 days per year.Inpatient RehabilitationFacility Services

SCHEDULE OF MEDICAL BENEFITS80/60 PPO PLANEMPIRE BLUECROSS BLUESHIELDPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Spinal Treatment Network
Out-of-Network
Surgical Treatment of Network Morbid Obesity
Urgent Care Services
COVERED HEALTHSERVICE
YOUR COST SHARE
COPAY APPLYTO ANNUALOOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
No
40%
$25 per visit
YesYes
No
Yes
40%
20%
YesYes
Yes
Limited to 1 procedure per lifetime.
Limited to 20 visits per calendar year.
Out-of-Network
20% YesYesNetwork
40% YesYesOut-of-Network
Anesthesiology Services
Organ Transplants For this benefit, “network plan” refers to theBCBS National Transplant Network.Precertification required. There is a $10,000 traveland lodging limit.
YesYes
20%
20%
40%
No No
Yes No
Yes NoOut-of-Network
Network
20%
20%Out-of-Network
Network
YesYes40%
Yes Yes
Out-of-Network
Network
Professional
Facility
Additional Benefits
Medical Management Program toll-free number: (800) 352-3152NOTES: The word “lifetime” refers to the period of time you or your eligible dependents participate
in this plan or any other plan sponsored by the Medical Trust.
This benefit summary is provided for informational purposes, is not all-inclusive, and does not constitute an agreement. Additional limitations and explanations,including specific benefit maximums will be provided to eligible, enrolled members in the Plan Document Handbook. In the event of a conflict between thisdocument and the official plan documents, the official plan documents will govern. The Episcopal Church Medical Trust retains the right to amend, terminate ormodify the terms of the plan at any time, without notice and for any reason.

SCHEDULE OF MENTAL HEALTH/SUBSTANCE ABUSE BENEFITSCIGNA BEHAVIORAL HEALTH PLAN IS EFFECTIVE AS OF JANUARY 1, 2011
The following schedule summarizes your mental health and substance abuse benefits, coinsurance amounts, benefitmaximums, and any additional explanation needed for your benefits. Please refer to the Mental Health/SubstanceAbuse chapter for additional Plan provisions. All coinsurances apply to your health plan’s out-of-pocket maximums.
FOR MEMBERS ENROLLED IN THE EMPIRE PPO 80/60 PLAN
Outpatient Mental Health/ There is no annual limit.
ADDITIONAL LIMITATIONS AND EXPLANATIONS
Network
Network
Out-of-Network
Network$20 per visit
Out-of-Network30%
All admissions must be precertified. There is no annual limit. Plan coverage isreduced to 50% if there is no precertification. Emergency room, ambulance,and lab work charges are covered by your medical plan.
Inpatient Mental Health/Substance Abuse $100 per day to $600
maximum
30%
Network
Out-of-Network
All programs must be precertified. There is no annual limit. Plan coverage isreduced to 50% if there is no precertification.
Benefits include (but are not limited to) unlimited telephonic and work/lifeservices, crisis intervention, referrals to community resources, legalconsultations, and a large online resource library. You may also receive up to10 face-to-face counseling sessions per issue, but they must be precertified byCIGNA Behavioral.
$150 per program,payable at admission
30%
$0
N/A
Intensive Outpatient MentalHealth/Substance Abuse
Employee Assistance Program(EAP)
Benefit is limited to 24 90-minute sessions per calendar year. Up to 12 of the24 sessions may be used for individual consultation. The Plan will reimburse70% up to $40.
Colleague Groups
Out-of-Network
YOUR COST SHARECOVERED HEALTH SERVICE
Substance Abuse
Everything you discuss with your counselor or care provider is kept in the strictest confidence in accordance withapplicable state and federal laws. Your employer is not notified of your visits or given specific information aboutyour treatment without your written permission. The general health privacy and security standards of theEpiscopal Church Medical Trust apply.
CIGNA Behavioral Health Member Services Toll-Free Number: (866) 395-7794
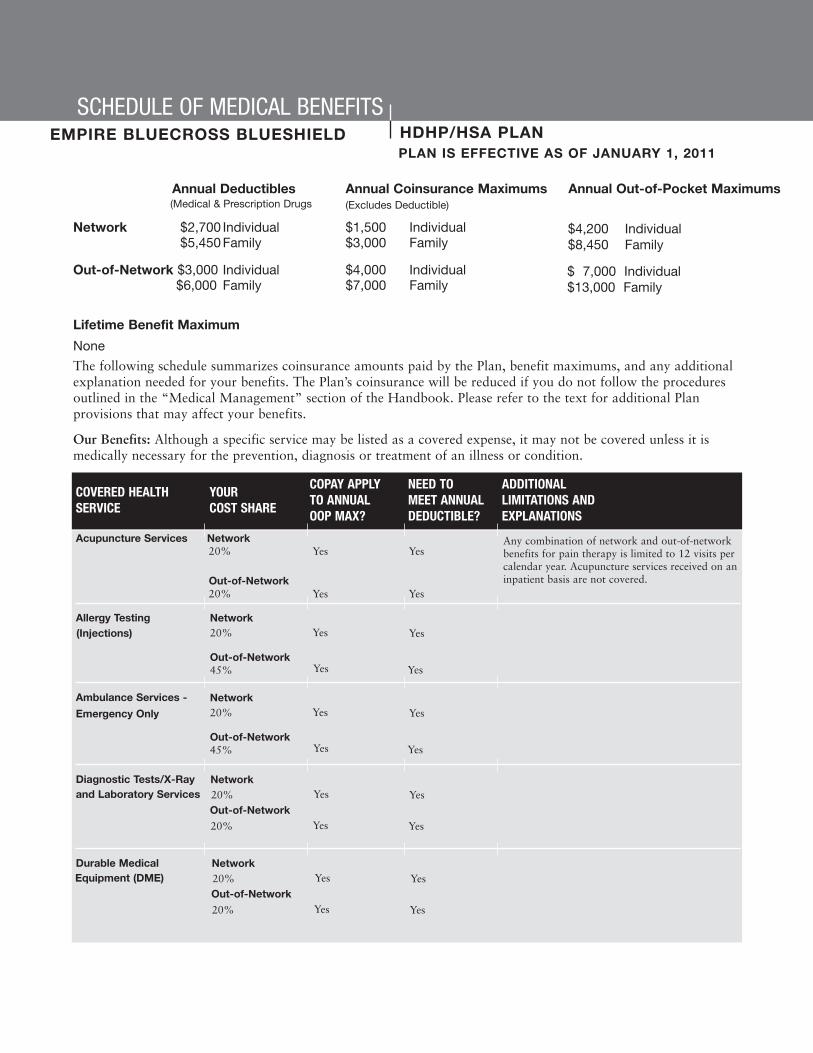
The following schedule summarizes coinsurance amounts paid by the Plan, benefit maximums, and any additionalexplanation needed for your benefits. The Plan’s coinsurance will be reduced if you do not follow the proceduresoutlined in the “Medical Management” section of the Handbook. Please refer to the text for additional Planprovisions that may affect your benefits.
Our Benefits: Although a specific service may be listed as a covered expense, it may not be covered unless it ismedically necessary for the prevention, diagnosis or treatment of an illness or condition.
SCHEDULE OF MEDICAL BENEFITSHDHP/HSA PLANEMPIRE BLUECROSS BLUESHIELDPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Lifetime Benefit Maximum
None
Annual Deductibles Annual Coinsurance Maximums(Excludes Deductible)
Network $2,700 Individual $1,500 Individual$5,450 Family $3,000 Family
Out-of-Network $3,000 Individual $4,000 Individual$6,000 Family $7,000 Family
Annual Out-of-Pocket Maximums
COVERED HEALTHSERVICE
YOURCOST SHARE
Acupuncture Services Network20% Yes Yes
Out-of-Network20% Yes Yes
Allergy Testing
Ambulance Services -
Diagnostic Tests/X-Rayand Laboratory Services
Durable Medical
Any combination of network and out-of-networkbenefits for pain therapy is limited to 12 visits percalendar year. Acupuncture services received on aninpatient basis are not covered.
Yes Yes
Yes Yes
COPAY APPLYTO ANNUALOOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
Network
Out-of-Network
Network20%
Out-of-Network45% Yes
Yes
Yes
Yes
Network20%
Out-of-Network45% Yes
Yes
Yes
Yes
(Injections)
20%
20%
Yes Yes
Yes Yes
Network
Out-of-Network20%
20%
Equipment (DME)
Emergency Only
(Medical & Prescription Drugs
$4,200 Individual$8,450 Family
$ 7,000 Individual$13,000 Family

SCHEDULE OF MEDICAL BENEFITSHDHP/HSA PLANEMPIRE BLUECROSS BLUESHIELDPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Emergency Room Network & Services Out-of-Network
20% Yes Yes
Home Health Care Network
Hospice Care Network
45% Yes Yes
Hospital Services Network
Hospital Services(Outpatient)
Hypnosis
Maternity Services
Mental Health/
Services for non-emergencies will not be covered.Hospital admission must be precertified within 24hours.
COVERED HEALTHSERVICE
YOUR COST SHARE
COPAY APPLYTO ANNUALOOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
Yes
Yes
Yes
Yes Yes
Yes
Limited to 200 visits per plan year; precertificationis required.
Limited to one episode per lifetime. Benefitsinclude bereavement counseling. Precertification isrequired.
20%
YesYes20%
YesYes
Out-of-Network
Out-of-Network
Out-of-Network
45%
Yes
Yes
Yes
Yes20%
Network
Network
Network
45%
The Plan’s coinsurance for hospital expenses willbe reduced to 50% if you do not follow theprocedures required by the Medical ManagementProgram. This penalty does not apply to the out-of-pocket maximum.
20%
45%
(Inpatient)
Out-of-network
Yes
Yes
Yes
Yes20%
Network
20%
Out-of-network
Antepartum care only.
Limited to 6 visits per year.
Out-of-Network
Hospital Services
Outpatient Services
The Plan’s coinsurance for hospital expenses willbe reduced to 50% if you do not follow theprocedures required by the Medical ManagementProgram. This penalty does not apply to the out-of-pocket maximum. Well-newborn care is alsocovered, but is not subject to the inpatienthospital deductible.
20%
20%
45%
Out-of-Network45%
Yes Yes
Yes Yes
Yes Yes
Yes Yes
Network Pre-authorization required. The Plan’s coinsurancefor hospital expenses will be reduced by 50% ifyou do not follow the procedures required by theMedical Management Program. This penalty doesnot apply to the out-of-pocket maximum.
20%
Out-of-Network45%
Yes Yes
Yes Yes
Substance AbuseServices - Inpatient

SCHEDULE OF MEDICAL BENEFITSHDHP/HSA PLANEMPIRE BLUECROSS BLUESHIELDPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Mental Health/
Nutritional Counseling
Outpatient TherapyServices
Physician’s OfficeServices
Routine & PreventiveServices
Skilled Nursing Facility/
COVERED HEALTHSERVICE
YOUR COST SHARE
COPAY APPLYTO ANNUALOOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
Limited to 6 visits/sessions per calendar year.
Benefits include hearing/speech, physical andoccupational therapy. Limited to 60 visits per Planyear, combined facility and office, per each of thethree therapies.
Out-of-Network
Yes Yes20%
45% Yes Yes
20% Yes Yes
Yes Yes
Out-of-Network
Network
Network
Out-of-Network
Yes Yes20%
45% Yes Yes
NetworkSubstance AbuseServices - Outpatient
45%
Benefits include routine physicals, includinggynecological exams, limited to 1 per year; hearingexams performed by your physician during aroutine physical, limited to 1 per year; andvaccinations, inoculations, and immunizations.Pap tests, limited to 1 per year; mammograms,limited to 1 per year age 40+, 1 age 35-39; PSAscreenings, limited to 2 per year age 40+; and allrelated routine x-rays and laboratory services.Well-child checkups limited to 7 visits from birthto age 1, 6 visits from age 1 through age 5, 7 visitsfrom age 5 through age 12, 6 visits from age 12through age 18, and 2 visits age 18 up to the 19thbirthday. Benefits include the office visit,vaccinations, inoculations, immunizations, and allrelated x-ray and laboratory services. Routinesigmoidoscopy limited to 1 every 2 years, age 40+.Routine colonoscopy limited to 1 every 10 years,age 50+.
Yes Yes
Yes Yes
Out-of-Network
Network
Network
Network
Out-of-Network
45%
Yes Yes
n/a No
45%
Out-of-Network
Yes Yes
Yes Yes
45%
20%
$0
20%
Routine ExamsRoutine Exam X-Rays & Laboratory ServicesWell-Child CheckupsRoutine ColonoscopyRoutine SigmoidoscopyOther Routine Services
Limited to 60 days per year.Inpatient RehabilitationFacility Services

SCHEDULE OF MEDICAL BENEFITSHDHP/HSA PLANEMPIRE BLUECROSS BLUESHIELDPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Spinal Treatment Network
Surgical Treatment of Network Morbid Obesity
Urgent Care Services
COVERED HEALTHSERVICE
YOURCOST SHARE
COPAY APPLYTO ANNUALOOP MAX?
NEED TO MEET ANNUALDEDUCTIBLE?
ADDITIONALLIMITATIONS ANDEXPLANATIONS
Yes
45%
20%
YesYes
Yes
Yes
45%
20%
YesYes
Yes
Limited to 1 procedure per lifetime.
Limited to 20 visits per year.
Out-of-Network
Anesthesiology Services
Organ Transplants For this benefit, “network plan” refers to theBCBS National Transplant Network.Precertification required. There is a $10,000 traveland lodging limit.
YesYes
20%
20%
20%
Yes Yes
Yes Yes
Yes YesOut-of-Network
Network
20%
20%Out-of-Network
Network
Yes Yes
Yes Yes20%
45%Out-of-Network
Network
YesYes45%
Yes Yes
Out-of-Network
Network
Professional
Facility
Additional Benefits
Medical Management Program toll-free number: (800) 352-3152NOTES: The word “lifetime” refers to the period of time you or your eligible dependents participate
in this plan or any other plan sponsored by the Medical Trust.
This benefit summary is provided for informational purposes, is not all-inclusive, and does not constitute an agreement. Additional limitations and explanations,including specific benefit maximums will be provided to eligible, enrolled members in the Plan Document Handbook. In the event of a conflict between thisdocument and the official plan documents, the official plan documents will govern. The Episcopal Church Medical Trust retains the right to amend, terminate ormodify the terms of the plan at any time, without notice and for any reason.
Out-of-Network

Coverage of Non-Sedating Antihistamines
Brand non-sedating antihistamine drugs are paid as Tier 3, regardless of the drug’s formulary status of preferred or non-preferred drug. For example, if you prefer to take the medication Clarinex rather than buying Claritin over the counter, youwill pay the Tier 3 copayment.
Retail Refill Limit
The Prescription Drug Program will maintain a Retail Refill Limit policy. The retail refill limit requires that you use the mail-orderpharmacy if you are prescribed a maintenance medication, rather than refilling multiple prescriptions for the same drug at aretail pharmacy. If you or a covered dependent receives a prescription for a maintenance medication and you do not use themail-order pharmacy, your prescriptions may not be covered.
In some circumstances, you may not be required to use the mail-order pharmacy. For example, there are several categoriesof medications that are uniquely appropriate for multiple refills at your local pharmacy (and are therefore exempt from themandatory mail-order provision, as outlined above). If you have a prescription for any of the following medications, thePrescription Drug Program allows you to receive multiple refills at your local retail pharmacy:
• Anti-infectives, including antibiotics (Amoxicillin, Biaxin), antivirals (Zovirax, Famvir), antifungals (Diflucan), and drops used in the eyes and ears (Polsporin Opth, Cipro Otic). Please note that drops must be prescribed specifically to treat infection. For example, glaucoma drops are not covered.
• Prescription cough medications, including Phenergan with Codeine, Tessalon, and Tussionex.
• Medications to treat acute pain, both narcotic (Vicodin, Percodan, etc.) and non-narcotic (Darvocet). Please note thatlong-term pain medications, such as NSAIDs, do not meet the necessary retail requirements.
• Medications that require a new written prescription each time you need them, as refills are prohibited by federal law (e.g., Percodan, Ritalin, and Nembutal).
• Medications used to treat both attention deficit disorder (Ritalin, Cylert) and narcolepsy (Dexedrine).
RETAIL PRESCRIPTION DRUGS MAIL-ORDER PRESCRIPTION DRUGS
Annual Prescription Deductible
Tier 1: Generic
Tier 2: Formulary Brand-Name
Tier 3: Non-Formulary Brand-Name andBrand Non-Sedating Antihistamines
Paper Claims Reimbursement
Dispensing Limits Per Copayment
Combined With Medical
15% (after deductible)
25% (after deductible)
50% (after deductible)
You must pay the full price at the pharmacyand file a claim for reimbursement, as
outlined in the “Pharmacy Benefits” sectionof this Handbook. You will be reimbursed
according to what the Plan would have paidat a participating pharmacy, less your
applicable copayment.
Up to a 90-day supply
Keep in mind, the retail pharmacy program allows for a total of three fills of a maintenance medication at a retailpharmacy (one original fill and two refills). Additional fills will not be covered by the Plan. Each fill can be for nomore than a 30-day supply. Note that you are allowed a total of three fills, even if each is for less than 30 days.
SCHEDULE OF MEDICAL BENEFITSHDHP/HSA PLANMEDCOPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Up to a 30-day supply.

SCHEDULE OF MEDICAL BENEFITSHDHP/HSA PLANMEDCOPLAN IS EFFECTIVE AS OF JANUARY 1, 2011
Generic Substitution RequirementGeneric medications and their brand-name counterparts have the same active ingredients and are manufactured accordingto the same strict federal regulations. Generic drugs may differ in color, size, or shape, but the U.S. Food and DrugAdministration (FDA) requires that the active ingredients have the same strength, purity, and quality as their brand-namecounterparts. For this reason, the Plan will cover the cost of the generic equivalent if you purchase a brand-namemedication when there is a generic available. You will be charged the generic copayment and the cost differencebetween the brand-name and the generic medication. If you have questions or concerns about generic medication,speak to your physician or your pharmacist, and he or she will be able to help you.
Refilling Mail-Order PrescriptionsSince your medication can take 7 to 11 days to be delivered, you should have at least a 14-day supply of that medicationon hand to hold you over. If you do not have enough medication, you may need to ask your doctor for another prescriptionfor a 14-day supply that you can fill at your local retail network pharmacy.
Prescriptions Filled At A Nonparticipating Pharmacy If you go to a retail pharmacy that is not part of the Medco network, you must pay the full cost of the prescription and thensubmit a direct reimbursement claim form to Medco. You will be reimbursed for the amount the medication would have costyour Plan at a participating pharmacy minus the copayment you would have paid.
Your Plan May Have Coverage LimitsYour plan may have certain coverage limits. For example, prescription drugs used for cosmetic purposes may not becovered, or a medication might be limited to a certain amount (such as the number of pills or total dosage) within a specifictime period.
If you submit a prescription for a drug that has coverage limits, your pharmacist will tell you that approval is needed beforethe prescription can be filled. The pharmacist will give you or your doctor a toll-free number to call. If you use Medco ByMail, your doctor will be contacted directly.
When a coverage limit is triggered, more information is needed to determine whether your use of the medication meets yourplan’s coverage conditions. We will notify you and your doctor of the decision in writing. If coverage is approved, the letterwill indicate the amount of time for which coverage is valid. If coverage is denied, an explanation will be provided, alongwith instructions on how to submit an appeal.
Medco toll-free number: (800) 841-3361
NOTES: Some prescriptions may require prior authorization. Please refer to the “Pharmacy Benefits” section of thisHandbook for further information.
Prescription deductibles and copayments do not apply to the medical plan deductibles or out-of-pocketmaximums.
This benefit summary is provided for informational purposes, is not all-inclusive, and does not constitute an agreement. Additional limitations and explanations,including specific benefit maximums will be provided to eligible, enrolled members in the Plan Document Handbook. In the event of a conflict between thisdocument and the official plan documents, the official plan documents will govern. The Episcopal Church Medical Trust retains the right to amend, terminate ormodify the terms of the plan at any time, without notice and for any reason.

CIGNAHMO
Empire BCBSEPO 90
Empire BCBSEPO 80
KaiserEPO 80
UnitedHealthcareChoice 80
Network Only Network Network Only Network Only Network OnlyAnnual Medical Deductible $0 per person
$0 per family$200 per person $500 per family
$350 per person$700 per family
$500 per person$1,000 per family
$1,000 per person$2,000 per family
Annual Out-of-Pocket Maximum(excludes deductible)
$0 per person$0 per family
$1,000 per person$2,000 per family
$1,500 per person$3,000 per family
$3,000 per person$6,000 per family
$1,500 per person$3,000 per family
Preventive CareRoutine and Preventive Services
Benefits include routine physicals, gynecological exams, hearing exams performed by your physician during a routine physical, and vaccinations, inoculations, and immunizations. Pap tests, mammograms, PSA screenings, and all related routine x-rays and laboratory services. Also includes routine sigmoidoscopy and colonoscopy. Please see the Schedules of Benefits for limitations on age and frequency for the related exams and lab services.
$0 copay $0 copay $0 copay $0 copay (Frequency and age limits for those age 24 months and older are managed by the KP provider)
$0 copay
Well-Child CareBenefits include the office visit, vaccinations, inoculations, immunizations, and all related x-ray and laboratory services. See the Schedules of Benefits for age and frequency limitations.
$0 copay $0 copay $0 copay $0 copay (Well-child checkups are limited to those less than 24 months old)
$0 copay
Physician ServicesOffice Visit $20 copay $25 copay $25 copay $25 copay $25 copayDiagnostic Services No copay You pay 20% You pay 20% 20% coinsurance You pay 20%Specialist Care $20 copay $25 copay $25 copay $35 copay $25 copayHospital ServicesInpatient Services Copay of $350 per
admissionYou pay 10% You pay 20% You pay 20% You pay 20%
Emergency Room Care $50 copay (waived if admitted)
$50 copay (waived if admitted within 24 hours)
$50 copay (waived if admitted within 24 hours)
You pay 20% $50 copay (waived if admitted within 24 hours)
Outpatient Surgery $250 copay You pay 10% You pay 20% You pay 20% You pay 20%Organ Transplants Copay of $350 per
admissionYou pay 10% You pay 20% You pay 20% You pay 20%
Anesthesiology Services Cost share based on service and provider type
Cost share based on service and provider type
Cost share based on service and provider type
Cost share based on service and provider type
Cost share based on service and provider type
Ambulance Services (emergency only)
No copay You pay 10% You pay 20% 20% coinsurance You pay 20%
Maternity ServicesPrenatal Care $20 for first visit only $25 copay for first
office visit only$25 copay for first visit only
$25 PCP/$35 specialist for visit to confirm pregnancy; $0 for initial pre-natal visit
$25 copay for first office visit only
Inpatient Services Copay of $350 per admission
You pay 10% You pay 20% You pay 20% You pay 20%
Plan
This chart is a general description and is provided for informational purposes only. It should not be viewed as an offer of coverage. In the event of a conflict between this chart and the official Plan documents, the official Plan documents will govern.
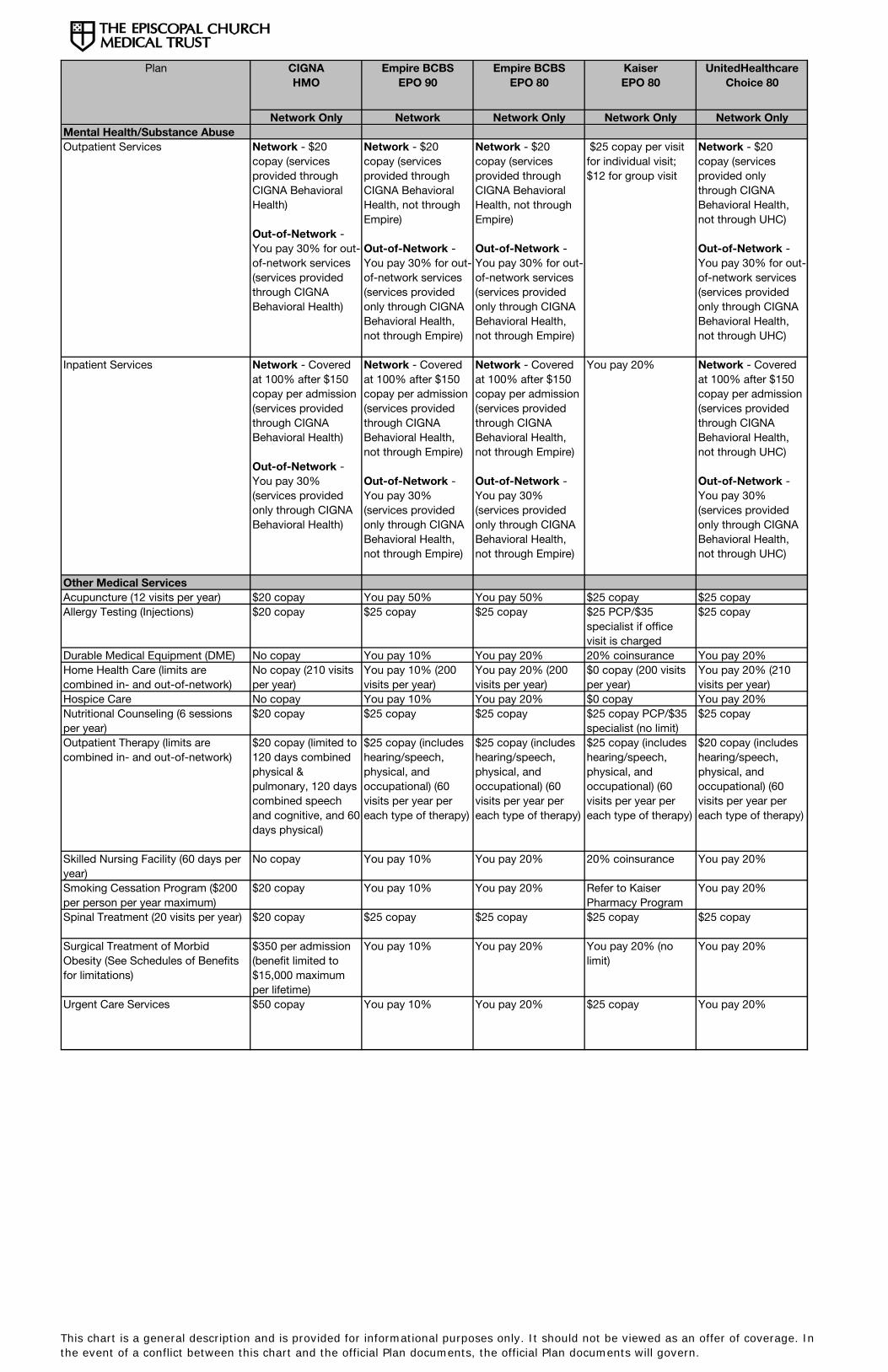
CIGNAHMO
Empire BCBSEPO 90
Empire BCBSEPO 80
KaiserEPO 80
UnitedHealthcareChoice 80
Network Only Network Network Only Network Only Network Only
Plan
Mental Health/Substance Abuse Outpatient Services Network - $20
copay (services provided through CIGNA Behavioral Health)
Out-of-Network - You pay 30% for out-of-network services (services provided through CIGNA Behavioral Health)
Network - $20 copay (services provided through CIGNA Behavioral Health, not through Empire)
Out-of-Network - You pay 30% for out-of-network services (services provided only through CIGNA Behavioral Health, not through Empire)
Network - $20 copay (services provided through CIGNA Behavioral Health, not through Empire)
Out-of-Network - You pay 30% for out-of-network services (services provided only through CIGNA Behavioral Health, not through Empire)
$25 copay per visit for individual visit; $12 for group visit
Network - $20 copay (services provided only through CIGNA Behavioral Health, not through UHC)
Out-of-Network - You pay 30% for out-of-network services (services provided only through CIGNA Behavioral Health, not through UHC)
Inpatient Services Network - Covered at 100% after $150 copay per admission (services provided through CIGNA Behavioral Health)
Out-of-Network - You pay 30% (services provided only through CIGNA Behavioral Health)
Network - Covered at 100% after $150 copay per admission (services provided through CIGNA Behavioral Health, not through Empire)
Out-of-Network - You pay 30% (services provided only through CIGNA Behavioral Health, not through Empire)
Network - Covered at 100% after $150 copay per admission (services provided through CIGNA Behavioral Health, not through Empire)
Out-of-Network - You pay 30% (services provided only through CIGNA Behavioral Health, not through Empire)
You pay 20% Network - Covered at 100% after $150 copay per admission (services provided through CIGNA Behavioral Health, not through UHC)
Out-of-Network - You pay 30% (services provided only through CIGNA Behavioral Health, not through UHC)
Other Medical ServicesAcupuncture (12 visits per year) $20 copay You pay 50% You pay 50% $25 copay $25 copayAllergy Testing (Injections) $20 copay $25 copay $25 copay $25 PCP/$35
specialist if office visit is charged
$25 copay
Durable Medical Equipment (DME) No copay You pay 10% You pay 20% 20% coinsurance You pay 20%Home Health Care (limits are combined in- and out-of-network)
No copay (210 visits per year)
You pay 10% (200 visits per year)
You pay 20% (200 visits per year)
$0 copay (200 visits per year)
You pay 20% (210 visits per year)
Hospice Care No copay You pay 10% You pay 20% $0 copay You pay 20%Nutritional Counseling (6 sessions per year)
$20 copay $25 copay $25 copay $25 copay PCP/$35 specialist (no limit)
$25 copay
Outpatient Therapy (limits are combined in- and out-of-network)
$20 copay (limited to 120 days combined physical & pulmonary, 120 days combined speech and cognitive, and 60 days physical)
$25 copay (includes hearing/speech, physical, and occupational) (60 visits per year per each type of therapy)
$25 copay (includes hearing/speech, physical, and occupational) (60 visits per year per each type of therapy)
$25 copay (includes hearing/speech, physical, and occupational) (60 visits per year per each type of therapy)
$20 copay (includes hearing/speech, physical, and occupational) (60 visits per year per each type of therapy)
Skilled Nursing Facility (60 days per year)
No copay You pay 10% You pay 20% 20% coinsurance You pay 20%
Smoking Cessation Program ($200 per person per year maximum)
$20 copay You pay 10% You pay 20% Refer to Kaiser Pharmacy Program
You pay 20%
Spinal Treatment (20 visits per year) $20 copay $25 copay $25 copay $25 copay $25 copay
Surgical Treatment of Morbid Obesity (See Schedules of Benefits for limitations)
$350 per admission (benefit limited to $15,000 maximum per lifetime)
You pay 10% You pay 20% You pay 20% (no limit)
You pay 20%
Urgent Care Services $50 copay You pay 10% You pay 20% $25 copay You pay 20%
This chart is a general description and is provided for informational purposes only. It should not be viewed as an offer of coverage. In the event of a conflict between this chart and the official Plan documents, the official Plan documents will govern.

Annual Medical Deductible
Annual Out-of-Pocket Maximum(excludes deductible)
Preventive CareRoutine and Preventive Services
Benefits include routine physicals, gynecological exams, hearing exams performed by your physician during a routine physical, and vaccinations, inoculations, and immunizations. Pap tests, mammograms, PSA screenings, and all related routine x-rays and laboratory services. Also includes routine sigmoidoscopy and colonoscopy. Please see the Schedules of Benefits for limitations on age and frequency for the related exams and lab services.
Well-Child CareBenefits include the office visit, vaccinations, inoculations, immunizations, and all related x-ray and laboratory services. See the Schedules of Benefits for age and frequency limitations.Physician ServicesOffice VisitDiagnostic ServicesSpecialist CareHospital ServicesInpatient Services
Emergency Room Care
Outpatient SurgeryOrgan Transplants
Anesthesiology Services
Ambulance Services (emergency only)Maternity ServicesPrenatal Care
Inpatient Services
Plan
Network Out-of-Network Network Out-of-Network$200 per person$500 per family
$500 per person$1,000 per family
$250 per person$500 per family
$500 per person$1,000 per family
$0 per person$0 per family
$3,000 per person$6,000 per family
$1,000 per person$2,000 per family
$3,000 per person$6,000 per family
$0 copay You pay 30% $0 copay You pay 30%
$0 copay You pay 30% $0 copay You pay 30%
$30 copay You pay 30% $25 copay You pay 30%$30 copay You pay 30% You pay 20% You pay 20%$30 copay You pay 30% $25 copay You pay 30%
Copay of $150 per admission
You pay 30% Copay of $100 per day not to exceed $600, then you pay 10%
You pay 30%
$50 copay (waived if admitted within 24 hours)
$50 copay (waived if admitted within 24 hours)
$50 copay (waived if admitted) (non-emergency services are not covered)
$50 copay (waived if admitted) (non-emergency services are not covered)
$150 copay You pay 30% You pay 10% You pay 30%No copay You pay 30% $100 per day copay,
not to exceed $600, then you pay 10%
You pay 30%
Cost share based on service and provider type
Cost share based on service and provider type
Cost share based on service and provider type
Cost share based on service and provider type
No copay No copay You pay 10% You pay 10%
$30 copay for first visit only
You pay 30% $25 copay for first visit only
You pay 30%
Copay of $150 per admission
You pay 30% Copay of $100 per day not to exceed $600, then you pay 10%
You pay 30%
AetnaChoice POS II
Empire BCBSPPO High Option
This chart is a general description and is provided for informational purposes only. It should not be viewed as an offer of coverage. In the event of a conflict between this chart and the official Plan documents, the official Plan documents will govern.

Plan
Mental Health/Substance Abuse Outpatient Services
Inpatient Services
Other Medical ServicesAcupuncture (12 visits per year)Allergy Testing (Injections)
Durable Medical Equipment (DME)Home Health Care (limits are combined in- and out-of-network)Hospice CareNutritional Counseling (6 sessions per year)Outpatient Therapy (limits are combined in- and out-of-network)
Skilled Nursing Facility (60 days per year)Smoking Cessation Program ($200 per person per year maximum)Spinal Treatment (20 visits per year)
Surgical Treatment of Morbid Obesity (See Schedules of Benefits for limitations)
Urgent Care Services
Network Out-of-Network Network Out-of-Network
AetnaChoice POS II
Empire BCBSPPO High Option
$20 copay (services provided only through CIGNA Behavioral Health, not through Empire)
You pay 30% (services provided only through CIGNA Behavioral Health, not through Empire)
$20 copay (services provided only through CIGNA Behavioral Health, not through Aetna)
You pay 30% (services provided only through CIGNA Behavioral Health, not through Aetna)
Covered at 100% after $150 copay per admission (services provided through CIGNA Behavioral Health, not through Empire)
You pay 30% (services provided only through CIGNA Behavioral Health, not through Empire)
Covered at 100% after $150 copay per admission (services provided through CIGNA Behavioral Health, not through Aetna)
You pay 30% (services provided only through CIGNA Behavioral Health, not through Aetna)
You pay 50% You pay 50% You pay 50% You pay 50%$30 copay You pay 30% $25 copay You pay 30%
No copay No copay You pay 10% You pay 30%No copay (200 visits per year)
You pay 30% (200 visits per year)
You pay 10% (200 visits per year)
You pay 30% (200 visits per year)
No copay You pay 30% You pay 10% You pay 30% $30 copay You pay 30% $25 copay $25 copay
$30 copay (includes hearing/speech, physical, and occupational) (60 visits per year per each type of therapy)
You pay 30% (includes hearing/speech, physical, and occupational) (60 visits per year per each type of therapy)
$25 copay (includes hearing/speech, physical, and occupational) (60 visits per year per each type of therapy)
You pay 30% (includes hearing/speech, physical, and occupational) (60 visits per year per each type of therapy)
No copay You pay 30% You pay 10% You pay 30%
No copay You pay 30% No copay No copay
$30 copay You pay 30% $25 copay You pay 30%
No copay You pay 30% Copay of $100 per day not to exceed $600, then you pay 10%
You pay 30%
$50 copay $50 copay $25 copay (non-urgent care is not covered)
You pay 30% (non-urgent care is not covered)
This chart is a general description and is provided for informational purposes only. It should not be viewed as an offer of coverage. In the event of a conflict between this chart and the official Plan documents, the official Plan documents will govern.
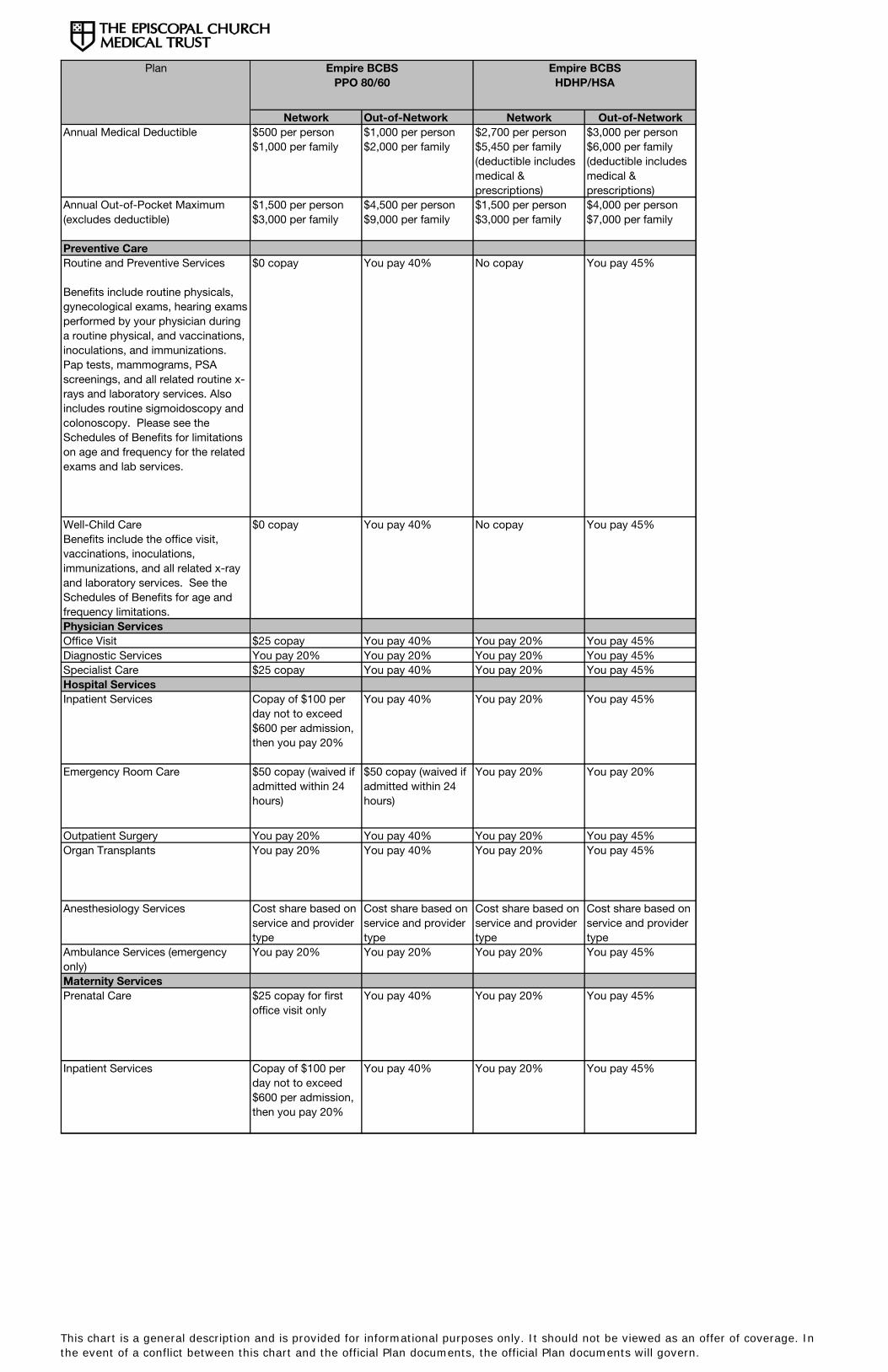
Annual Medical Deductible
Annual Out-of-Pocket Maximum(excludes deductible)
Preventive CareRoutine and Preventive Services
Benefits include routine physicals, gynecological exams, hearing exams performed by your physician during a routine physical, and vaccinations, inoculations, and immunizations. Pap tests, mammograms, PSA screenings, and all related routine x-rays and laboratory services. Also includes routine sigmoidoscopy and colonoscopy. Please see the Schedules of Benefits for limitations on age and frequency for the related exams and lab services.
Well-Child CareBenefits include the office visit, vaccinations, inoculations, immunizations, and all related x-ray and laboratory services. See the Schedules of Benefits for age and frequency limitations.Physician ServicesOffice VisitDiagnostic ServicesSpecialist CareHospital ServicesInpatient Services
Emergency Room Care
Outpatient SurgeryOrgan Transplants
Anesthesiology Services
Ambulance Services (emergency only)Maternity ServicesPrenatal Care
Inpatient Services
Plan
Network Out-of-Network Network Out-of-Network$500 per person$1,000 per family
$1,000 per person$2,000 per family
$2,700 per person$5,450 per family(deductible includes medical & prescriptions)
$3,000 per person$6,000 per family (deductible includes medical & prescriptions)
$1,500 per person$3,000 per family
$4,500 per person$9,000 per family
$1,500 per person$3,000 per family
$4,000 per person$7,000 per family
$0 copay You pay 40% No copay You pay 45%
$0 copay You pay 40% No copay You pay 45%
$25 copay You pay 40% You pay 20% You pay 45%You pay 20% You pay 20% You pay 20% You pay 45%$25 copay You pay 40% You pay 20% You pay 45%
Copay of $100 per day not to exceed $600 per admission, then you pay 20%
You pay 40% You pay 20% You pay 45%
$50 copay (waived if admitted within 24 hours)
$50 copay (waived if admitted within 24 hours)
You pay 20% You pay 20%
You pay 20% You pay 40% You pay 20% You pay 45%You pay 20% You pay 40% You pay 20% You pay 45%
Cost share based on service and provider type
Cost share based on service and provider type
Cost share based on service and provider type
Cost share based on service and provider type
You pay 20% You pay 20% You pay 20% You pay 45%
$25 copay for first office visit only
You pay 40% You pay 20% You pay 45%
Copay of $100 per day not to exceed $600 per admission, then you pay 20%
You pay 40% You pay 20% You pay 45%
Empire BCBSHDHP/HSA
Empire BCBSPPO 80/60
This chart is a general description and is provided for informational purposes only. It should not be viewed as an offer of coverage. In the event of a conflict between this chart and the official Plan documents, the official Plan documents will govern.

Plan
Mental Health/Substance Abuse Outpatient Services
Inpatient Services
Other Medical ServicesAcupuncture (12 visits per year)Allergy Testing (Injections)
Durable Medical Equipment (DME)Home Health Care (limits are combined in- and out-of-network)Hospice CareNutritional Counseling (6 sessions per year)Outpatient Therapy (limits are combined in- and out-of-network)
Skilled Nursing Facility (60 days per year)Smoking Cessation Program ($200 per person per year maximum)Spinal Treatment (20 visits per year)
Surgical Treatment of Morbid Obesity (See Schedules of Benefits for limitations)
Urgent Care Services
Network Out-of-Network Network Out-of-Network
Empire BCBSHDHP/HSA
Empire BCBSPPO 80/60
$20 copay (services provided only through CIGNA Behavioral Health, not through Empire)
You pay 30% (services provided only through CIGNA Behavioral Health, not through Empire)
You pay 20% You pay 45%
Covered at 100% after $150 copay per admission (services provided through CIGNA Behavioral Health, not through Empire)
You pay 30% (services provided only through CIGNA Behavioral Health, not through Empire)
You pay 20% You pay 45%
You pay 50% You pay 50% You pay 20% You pay 20%$25 copay You pay 40% You pay 20% You pay 45%
You pay 20% You pay 20% You pay 20% You pay 20%You pay 20% (200 visits per year)
You pay 40% (200 visits per year)
You pay 20% (200 visits per year)
You pay 45% (200 visits per year)
You pay 20% You pay 40% You pay 20% You pay 45%$25 copay You pay 40% You pay 20% You pay 45%
$25 copay (includes hearing/ speech, physical, and occupational) (60 visits per year per each type of therapy)
You pay 40% (includes hearing/speech, physical, and occupational) (60 visits per year per each type of therapy)
You pay 20% (includes hearing/speech, physical, and occupational) (60 visits per year per each type of therapy)
You pay 45% (includes hearing/speech, physical, and occupational) (60 visits per year per each type of therapy)
You pay 20% You pay 40% You pay 20% You pay 45%
You pay 20% You pay 40% You pay 20% You pay 45%
$25 copay You pay 40% You pay 20% You pay 45%
You pay 20% You pay 40% You pay 20% You pay 45%
You pay 20% You pay 40% You pay 20% You pay 45%
This chart is a general description and is provided for informational purposes only. It should not be viewed as an offer of coverage. In the event of a conflict between this chart and the official Plan documents, the official Plan documents will govern.

Standard
$50 per individual
You pay up to $10
You pay up to $30
You pay up to $50
Up to a 30-day supply
N/A
You pay up to $25
You pay up to $70
You pay up to $120
Up to a 90-day supply
Annual Prescription Deductible
Tier 1: Generic
Tier 2: Formulary Brand-Name
Tier 3: Non-Formulary Brand-Nameand Brand Non-SedatingAntihistamines
Dispensing Limits Per Copayment
RETAIL PRESCRIPTION DRUGS MAIL-ORDER PRESCRIPTION DRUGS
The HDHP/HSA Plans
Network Prescription Deductible (combined with Medical Deductible)
Tier 1: Generic Drugs 15% after deductible
Tier 2: Brand-Name Drugs Included 25% after deductible on the Medco Formulary
Tier 3: Brand-Name Drugs Not Included on the Medco Formularyand All Non-Sedating Antihistamines
$2,700/$5,450
RETAIL AND MAIL-ORDER PRESCRIPTION DRUGS
50% after deductible
For Kaiser plans, prescription drug benefits are embedded in the medical plan. Please refer to the Kaiser PlanSchedule of Medical Benefits for prescription drug benefit details.
PRESCRIPTION DRUG BENEFITS
When you enroll in one of our medical Plan options for Empire BCBS, CIGNA, Aetna, or UnitedHealthcare,you’ll automatically have prescription drug coverage through the Medco Prescription Drug Program. Thisprogram includes a Formulary Management Program, which uses a “three-tier” copayment approach tocovered drugs and is designed to control costs for you and the Plan. The formulary includes all FDA-approveddrugs, which have been placed in tiers based on their clinical effectiveness, safety, and cost.
• Tier 1 includes primarily generic drugs (smallest copayment)
• Tier 2 includes preferred drugs (middle copayment)
• Tier 3 includes non-preferred drugs and all non-sedating antihistamines (highest copayment)

PRESCRIPTION DRUG BENEFITS
Your Plan May Have Coverage Limits
Your Plan may have certain coverage limits. For example, prescription drugs used for cosmetic purposes may not be covered,or a medication might be limited to a certain amount (such as the number of pills or total dosage) within a specific time period.
If you submit a prescription for a drug that has coverage limits, your pharmacist will tell you that approval is needed before theprescription can be filled. The pharmacist will give you or your doctor a toll-free number to call. If you use Medco By Mail, yourdoctor will be contacted directly.
When a coverage limit is triggered, more information is needed to determine whether your use of the medication meets yourPlan’s coverage conditions. We will notify you and your doctor of the decision in writing. If coverage is approved, the letter willindicate the amount of time for which coverage is valid. If coverage is denied, an explanation will be provided, along withinstructions on how to submit an appeal.
Additional Information
It is always up to you and your doctor to decide which prescriptions are best for you. You are never required to use genericdrugs or drugs that are on the Medco formulary list. If you prefer, you can use non-formulary brand-name drugs and pay ahigher copayment.
It is also important to note that drugs included on the formulary list are routinely updated. To find the most up-to-date list ofcovered drugs, visit Medco at www.medco.com, or call their member services department at (800) 841-3361. It should benoted that all drugs listed on the formulary may not be covered due to Plan exclusions and limitations. You can also useMedco’s website or member services telephone number to locate the retail pharmacy nearest you.
Paper Claim Reimbursements
If you use a non-participating pharmacy, you must pay the full price and file a claim for reimbursement. You will be reimbursedaccording to what the Plan would have paid at a participating pharmacy, less your applicable copayment. See the “PharmacyBenefits” section of your Plan Handbook for more information about filing claims for reimbursement for prescription drugspurchased at non-participating retail pharmacies.

The Episcopal Church Medical Trust Prescription Drug Benefit Fact Sheet
Administered by Medco
With The Episcopal Church Medical Trust Prescription Drug Benefit, members and their dependents covered by this prescription benefit can use either retail or Medco’s mail service pharmacies. The benefit covers most prescription drugs plus insulin and some over-the-counter (OTC) diabetic supplies. Certain prescription medications are subject to quantity limitations or require prior authorization for continued use. Retail pharmacy service: Retail pharmacy service is most convenient when filling short-term prescription needs. For example, if you need an antibiotic to treat an infection, you can go to one of the many pharmacies that participate in the Medco network. − Up to a 30 day supply of medication can be obtained from retail pharmacies. − Find a participating pharmacy at www.medco.com or by calling 800-841-3361. Medco mail service: Members that need medication on an ongoing basis, such as to treat asthma or diabetes, can ask their doctor to prescribe up to a 90 day supply, plus refills. These medications can be supplied by Medco’s mail service pharmacy. Medications are shipped to you by standard delivery at no additional cost. − You can track your prescription online and order
refills at www.medco.com or by calling 800-841-3361.
− Registered pharmacists are available around-the-clock for medication consultations.
Member co-payments for prescriptions Episcopal Church Medical Trust members pay the following co-payments for prescriptions.
$50 Annual Retail Individual Deductible Retail Pharmacies Medco By
Mail Generic drugs $10 $25 Formulary or plan-preferred brand drugs $30 $70 Non-formulary or non-preferred brand drugs $50 $120
Limitations and prior authorization requirements: Some medications are covered by your benefit only for certain uses or in certain quantities. For example, a medication may not be covered when it is used for cosmetic purposes or a quantity may be limited to certain amounts over certain time periods. The pharmacy will let you know if additional information is required to authorize coverage of your prescription. Retail Refill Allowance: For a prescription that you take on a long-term basis (3 months or more), you may use a participating retail pharmacy for up to three refills (the original fill and two refills), for up to a 30 day supply each time. If you remain on that medication, you must order subsequent fills through Medco By Mail, or pay the entire cost of the medication at the retail pharmacy.
Up to a 90 day supply of
medication from Medco’s mail service
Prescriptions filled for 3 month supplies at mail only need to be refilled every 90 days

Member Pays the Difference: If a brand name prescription drug is dispensed when a generic drug version of the same drug is available, the member will be required to pay the generic co-pay plus the difference in the cost between the brand name drug and the generic. How can members get more information about their Rx benefit? 1. Call the Medco member services at 800-841-3361. Visit
www.medco.com on the Internet o Register using your member ID, which is on your
prescription ID card. o Order and track status of mail service prescriptions o Compare pricing for brand and generic drugs o Review your prescription history & expenses o Look up Episcopal Church Medical Trust specific
benefit guidelines o Print mail service order forms o Locate participating retail pharmacies o Get information from Medco’s health and wellness information, tools and resources o Shop for non-prescription (OTC) and other drugstore items
Medco’s Specialty Pharmacy Service: The Medco specialty pharmacy service is designed to help Episcopal Church Medical Trust members and dependents meet the particular challenges of using certain medications, many of which require injection or special handling. Examples of specialty medications include Betaseron, Avonex, Copaxone, Enbrel, Humira, Rebetrol, Peg-Intron, and others. If you are on one of these or another specialty medication, you can receive additional services when you fill your specialty prescriptions via the Medco specialty pharmacy service, including: − Support and guidance from Medco nurses and pharmacists who are trained in these
medications, their side effects, and the conditions they treat. − Expedited delivery of all your specialty prescription medications to your home or if needed,
doctor's office. − Supplemental supplies, such as needles and syringes that are required to administer the
medication, at no additional charge. − Scheduling of refills and coordination of services with home care providers, case managers,
and doctors or other healthcare professionals. Common questions: − What is a formulary?
A formulary is a list of generic and brand-name drugs that are preferred by your plan. This list offers you choice while helping to keep the cost of your prescription drug benefit affordable.
− Are generic drugs safe?
Generic drugs may have unfamiliar names, but they are safe and effective. Be assured that generic drugs and their brand-name counterparts have the same active ingredients and are manufactured according to the same strict federal regulations. Prescriptions filled with generic drugs often have lower co-payments. Ask your doctor or pharmacist whether a generic version of your medication is available and whether it would be right for you.

VISION BENEFITS
If you enroll in one of the Medical Trust’s Plans, you’ll receive vision benefits through EyeMed Vision Care. The visioncare benefits include an annual eye examination with no copay when you use a network provider, and prescriptioneyewear or contact lenses offered through a broad-based network of ophthalmologists, optometrists, and opticians atretail chains and independent provider locations.
EyeMed gives you the choice of using network or non-network providers, but you will have higher out-of-pocket costsout-of-network.
The services described in the following chart are covered once every calendar year. The chart below is for descriptivepurposes only. For more complete information regarding your vision coverage, please refer to the official Plan DocumentHandbook.
The benefits described in this chart do not apply to regional and local medical plans offered by your group.
When you use EyeMed network providers, you don’t need to submit a claim. Your EyeMed provider will submit claimsfor you. You’re responsible for the copayment and any noncovered expenses at the time you receive services.
Please keep in mind that many plans may offer limited vision coverage through their networks. Check with your Plan fordetails.
For more information about EyeMed, and to see a list of EyeMed providers, visit www.enrollwitheyemed.com/accessor call EyeMed toll-free at (866) 723-0596.
Eye Examinations
Lenses*
Lens OptionsUV CoatingTint (Solid and Gradient)Standard Scratch ResistanceStandard PolycarbonateStandard Anti-Reflective CoatingStandard Progressive (Add-On to Bifocal)
Other Add-Ons and Services
Frames*
Contact Lenses*
Conventional
Disposable
You pay $0
You pay $10 for single,bifocal or trifocal
You pay up to $15You pay up to $15You pay up to $15You pay $0You pay up to $45You pay up to $6520% off retail price
$130 allowance, 20% off balance over $130
$130 allowance, 15% offbalance over $130
$130 allowance, then youpay balance over $130
* You are eligible to receive lenses and frames or contact lenses once per calendar year.
Network Benefit Description Out-of-Network Plan pays up to $30 forophthalmologistsor optometrists
Plan pays up to: $32—single vision$46—bifocal$57—trifocal
You are responsible forthe cost of any lensoptions that you electfrom out-of-networkproviders
Plan pays up to $47
Plan pays up to $100
Plan pays up to $100