healthy start · web viewapril 9, 2006 benita baker project officer division of healthy start and...
TRANSCRIPT

Tulsa Healthy Start Initiative 2001-2005
April 9, 2006
Benita BakerProject OfficerDivision of Healthy Start and Perinatal Services, Maternal and Child Health Bureau,Health Resources and Services Administration, US Public Health Service, Department of Health and Human Services Washington DC
Re: Eliminating Disparities in Perinatal Health: General Population
Dear Ms. Baker:
I submit to you the final version of the Tulsa Healthy Start Impact Report 2001-2005. The report contains data from grant years 2001-2005 and our perspective of the impact this program has made in our community. Also, you will find project accomplishments along with reports from local evaluations.
Tulsa Healthy Start appreciates the time and effort taken by HRSA to examine our report in its entirety. We welcome any recommendations you may have to us as it relates to our report. If additional information is needed or required, please do not hesitate to contact us.
Sincerely,
Corrina L. Jackson, MSMProject ManagerTulsa Healthy StartTulsa Health Department
1

Tulsa Healthy Start Initiative 2001-2005
HEALTHY START INITIATIVETulsa Healthy Start Initiative
TABLE OF CONTENTS
Letter of Transmittal 1 Table of Contents 2 Introduction 3
I. Overview of Racial and Ethnic Disparity Focused on By Project 3II. Project Implementation 34
III. Project Management and Governance 64 IV. Project Accomplishments 65
V. Project Impact 99 VI. Local Evaluation 104
VII. Fetal and Infant Mortality Review 105VIII. Products 106IX. Project Data
Form 1 MCHB Budget Forms 132Form 9 Tracking Discretionary Grant Healthy Start Specific Performance MeasuresForm 5 Number of Individuals ServedTable A Characteristics of Program ParticipantsTable B Risk Reduction/Prevention ServicesTable C Healthy Start Major Service Table
AppendicesAppendix A – Target Population and Tulsa County Specific DataAppendix B – Progress Report of Monitoring VisitAppendix C – Local Evaluation Appendix D – Products
Introduction
2

Tulsa Healthy Start Initiative 2001-2005
The purpose of Tulsa Healthy Start (THS) is to reduce the infant mortality and co-morbidity in Tulsa County, Oklahoma. This has been achieved by a continued emphasis on a community-based approach providing case management, education, counseling and support to women who are at most risk of poor birth outcomes. The strategies to achieve these outcomes include case management and care coordination, client recruitment and outreach and health education and training which began in l997 with the first four year cycle of Department of Health and Human Service, Health Resource Service Administration (DHHS, HRSA) funding. During the second four year cycle, a focus on interconceptional care and perinatal depression screening has been included in the case management and care coordination core services. These strategies fit into a well-conceived local health system action plan which has been developed by the Family Health Coalition (FHC) in conjunction with the Oklahoma State Department of Health, Title V (OSDH, Title V) and Tulsa Health Department (THD).
Pregnant and parenting women who consent for participation in the project are triaged through a risk assessment survey which weights the variables of race, economic status, zip code and medical and social risk factors into categories of high, moderate and low risk. Based on this risk designation, an individualized plan of care is established and reviewed periodically with the client through the pregnancy, birth and 2 year follow-up of women in THS.
Table 1 Core Services, Unduplicated Count and Contacts for 2001-2005 Calendar Years
Core Service Client Unduplicated Count 2001 2002 2003 2004
Contacts 2001 2002 2003 2004
Case Management Women Infants
Transportation
904827
244
834893
238
678882
228
604525
258
2,593
1,003
2,252
1,323
3,866
1,149
1,605
978Outreach Interconceptional Care Translation Home and community Babyline
170318246
4,423
325116712
4,604
286135578
4,795
60476
4554,659
1,4072,209
686 1,1321,761
Health Education and Training Presentations and events Learning Resource Center Training Institutes and Conference
3473412
5257715
9488514
53320921
6,15453
1,090
10,662300
1,159
20,113350633
10,874250
1,311
Depression Screening and Referrals
Not Offered
593 678 604 Not Offered
593 678 604
I. Overview of Racial and Ethnic Disparity Focused on by the Project
A. Community AssessmentData for the needs assessment has been garnered primarily from four sources, the 2000 U.S.
Census, the Oklahoma State Department of Health, Center for Vital Statistics (birth and death certificates) and the Family Health Service Division (Oklahoma Pregnancy Risk Assessment
3

Tulsa Healthy Start Initiative 2001-2005
Monitoring System and immunization data), the Tulsa Health Department (Tulsa Healthy Start data, Tulsa Fetal Infant Mortality Review, linked county birth and death certificates) and the Community Service Council of Greater Tulsa (Babyline/Planline data, Hispanic Study). The data has been provided for years 1999, 2000, 2001, 2002 and 2003 as data is available. No data is available for 2004 from the OSDH or THD. Segregation of data by race is cited as information is available.
Each data set has limitations which will be acknowledged at this time. The Oklahoma State Department of Health (OSDH) data for 1996 through 1998 has been aggregated at county level. Further reduction of the data to census tract analysis has been discontinued at the conclusion of l996. Data from 1997-2003 is aggregated at the county level and zip code level. However, due to OSDH computer conversions in l997 and data entry errors, the 1997 through 1999 data have notable error rates as high as 20%. As a result, this data has not been used by the Tulsa Healthy Start (THS) as comparative data for evaluation purposes until reviewed and corrected through a process at the Tulsa Health Department. The Pregnancy Risk Assessment Monitoring System (Oklahoma PRAMS) data for Tulsa County was aggregated for Tulsa County in l997 for the years 1988-1995. This timeframe was prior to the advent of Medicaid managed care and the family income eligibility for pregnant women increased from 100% to 185% of the federal poverty level (FPL). Newer data for Tulsa County is not available as Oklahoma PRAMS report has not been released from 1998 to July of 2005. New reports are beginning to be released.
The THD data does not aggregate Hispanic origin separately and includes this data in the category of "white". The THS data reflects services provided to women who consented to participation in the THS case management from January 1999 to December 2004. Footnotes will address which years of service are represented. The initial data set is representative of women in the 37 targeted census tracts of the first cycle THS grant from 1997 through 2000. 2001 through 2003 years represents data from the second cycle THS grant.
Community Service Council (CSC) aggregates data from the Babyline/Planline centralized appointment system. This data is representative of 44% of the total resident births in Tulsa County during 1996 through 2004.
PopulationThe total population of Tulsa County is 563,299 with 75% White, 10.9% Black, 5.2%
American Indian, 1.6 % Asian and 6.0% of Hispanic origin (U.S. Census 2000). The project area is a sub-area of Tulsa County. It represents the ten highest zip codes by race and ethnicity for infant mortality in our city at 14.2. This is a change from census tract tracking of the initial Tulsa Healthy Start grant cycle but is inclusive of the previous census tracts. It is estimated that there are 112,424 persons (2000 U.S. Census): 44,961 (39.9%) White, 50,615 (45%) Black, 6,375 (5.6%) Native American and 1,558 (1.3%) Asian/Other. There are 2,497 (2.2%) of Hispanic origin. It is estimated 15% are of Hispanic origin in this area but are undocumented in census information because of their illegal status. The estimate is based on known births from this area. Thirty per cent of children under 18 in families are below 100% Federal Poverty Level (FPL).
By race and ethnicity, there are 25,142 women of childbearing age (WCBA) in the project area (2000 U.S. Census): 9,552 (37.9%) White, 13,001 (51.7%) Black, 1,584 (6.3%) Native American, 358 (1.4%) Asian/Other. The Hispanic ethnicity is 584 (2.3%) It is
4

Tulsa Healthy Start Initiative 2001-2005
estimated 6% are of Hispanic origin in Tulsa County with an undocumented visitor rate 3 times that amount. Appendix A provides the Tulsa County and project area specific data.
Figure 1 Map of Tulsa County Highlighted By Zip Codes with 10.58 Infant Mortality 1999-2000
5

Tulsa Healthy Start Initiative 2001-2005
74070
74063
74008
74021
74055
74047
74127
74107
74011
74012
74073
74115
74037
74116
74132 74133
74033
74134
74108
7411774126
74136
74106
74105
74112
74145
74114 7412974119
7414674135
7412874104
74130
74110
7410374120
Infant Mortality RateBelow 10.5810.58 or higher
N
EW
S
Infant Mortality Rates3-Year Average 1999-2001Tulsa County, by Zip Code
Source: Tulsa City-County Health Dept. Prepared by the Family Health Coalition (12/04).
Behavioral and Environmental Factors Of the 7,398 Tulsa Healthy Start clients that were case managed from September
1998 to December 31, 2004, 632 (8.5%) were found to use illicit drugs.
Table 2 THS Client Illicit Drug Use by Race and Age for 1998-2004 Race Number Percentage Age Number Percentage
6

Tulsa Healthy Start Initiative 2001-2005
Hispanic 88 13.92% 9-14 years old 7 1.11%White 225 35.60% 15-17 years old 72 11.39%Black 173 27.37% 18-19 years old 93 14.72%American Indian 127 20.09% 20-35 years old 403 63.77%Asian 6 0.95% 36-44 years old 37 5.85%Hawaiian/Pacific 1 0.16% 45 years old and older 4 0.63%Unknown 12 1.90% Unknown 16 2.53%Total 632 100.00% Total 632 100.00%
Illicit drug use is underreported and poorly understood phenomena. Drug use is reported on birth certificate data but the significant unknown rate creates a validity failure for this question. In a 1992 study by the Community Service Council, it was noted that 10.9% of women giving birth at one hospital in Tulsa County had alcohol or illicit drugs in their blood at the time of delivery. In the THS results, illicit drug use was a co-factor in depression in 91 cases, and domestic violence in 133 cases. In 2001, 93 newborns from resident Tulsa County Births were referred to the Department of Human Services, Child Welfare Services with positive drug screens at birth (DHS, Child Welfare Services, 2002)
Of the 7,398 Tulsa Healthy Start clients that were case managed from September 1998 to December 31, 2004, 398 (5.3%) were found to drink alcoholic beverages.
Table 3 THS Client Alcohol Use by Race and Age for 1998-2004 Race Number Percentage Age Number Percentage
Hispanic 88 22.11% 9-14 years old 4 1.01%White 152 38.19% 15-17 years old 55 13.82%Black 3 23.37% 18-19 years old 60 15.08%American Indian 54 13.57% 20-35 years old 232 58.29%Asian 3 0.75% 36-44 years old 25 6.27%Hawaiian or other Pacific 0 0.00% 45 years old and older 1 0.25%Unknown 8 2.01% Unknown 21 5.28%Total 398 100.00% Total 398 100.00%
Alcohol consumption was a co-factor with depression in 68 cases, and domestic violence in 70 cases.
Table 4 Maternal Drinking (Alcohol) PatternsMaternal Demographic
Drinking 3 Mths Prior to Pregnancy-PRAMS
Drinking in the Last 3 Mths of Pregnancy-PRAMS
Age<20 years20-2930+
34.6%51.6%52.9%
3.7%8.8%
14.2%Education
7

Tulsa Healthy Start Initiative 2001-2005
<12 years12 years13+ years
36.6%48.9%55.1%
5.9%9.4%
12.0%RaceWhiteAfrican-AmericanAmerican IndianOther
51.8%40.6%51.4%21.7%
9.7%9.8%
14.3%1.1%
Marital StatusMarriedNot Married
51.4%45.5%
10.4%7.8%
FPL<100%100-184%185+%
42.6%53.2%58.4%
9.4%8.0%
11.0%
Factors associated with self-imposed risks arising from mothers’ behaviors or lifestyles place infants, neonates, and post-neonates at significant risk of mortality. The Oklahoma Pregnancy Risk Assessment Monitoring System (Oklahoma PRAMS), implemented through the Oklahoma State Department of Health in cooperation with the federal Centers for Disease Control, reports countywide and statewide results of interviews of samples of women after delivery.
Countywide survey data for 1988-95 indicate that 50.1% of 2,107 respondents reported drinking alcohol three months prior to pregnancy, 9.8% reported drinking alcohol in the last trimester of pregnancy (Oklahoma PRAMS, Maternal and Infant Health in Tulsa County). By comparison, statewide survey data for 1988-95 indicate that 42.4% of 11,107 respondents reported drinking alcohol during the three months before pregnancy (Oklahoma PRAMS, Trend Report). Results from the same survey indicate 7.4% of 11,209 respondents reported drinking alcohol during the final trimester before delivery. The survey data indicate that 34.6% of women under age 20 and 36.6% of women with less than a high school education reported drinking alcohol in the three months before pregnancy; 3.7% of women under age 20 and 5.9% of women with less than a high school education reported drinking alcohol in the last trimester of pregnancy.
Self-reported drinking rates among White women were within 2% of the overall Tulsa County rates of 50.1% before pregnancy and 9.8% during the last trimester of pregnancy. Drinking rates for Black women were 40.6% before pregnancy and 9.8% during the last trimester of pregnancy (Oklahoma PRAMS, Maternal and Infant Health in Tulsa County).
For women, drinking in the last trimester of pregnancy is most prevalent among American Indians. Countywide survey data for 1988-95 indicate that 51.4% reported drinking three months prior to pregnancy and 14.3% during the last trimester of pregnancy (Oklahoma PRAMS, Maternal and Infant Health in Tulsa County). Tulsa's Indian Health Care Resource Center (IHCRC) reports that acute drinking, adversely affecting pregnancy and other health outcomes, occurs among 24.3% of American Indian
8

Tulsa Healthy Start Initiative 2001-2005
females, while chronic drinking occurs among 73.3%. American Indian women have the highest rate for acute and chronic drinking among all races (IHCRC, 1995). The national rate of fetal alcohol syndrome (FAS) among American Indians is 6.1 per 1,000 live births, over four times the 1.3 per 1,000 rate in the general population (IHCRC, 1995).
Of the 7,398 Tulsa Healthy Start clients that were case managed from September 1998 to December 31, 2004, 1,167 (15.7%) were found to smoke.
Table 5 THS Client Smoking by Race and Age for 1998-2004 Race Number Percentage Age Number Percentage
Hispanic 139 11.91% 9-14 years old 12 1.03%White 499 42.76% 15-17 years old 122 10.45%Black 323 27.68% 18-19 years old 164 14.05%American Indian 191 16.37% 20-35 years old 773 66.24%Asian 6 0.51% 36-44 years old 65 5.57%Hawaiian or other Pacific 1 0.90% 45 years old and older 4 0.34%Unknown 8 0.69% Unknown 27 2.31%Total 1,167 100.00% Total 1,167 100.00%
Smoking was a co-factor with depression in 172 cases, and domestic violence in 204 cases.
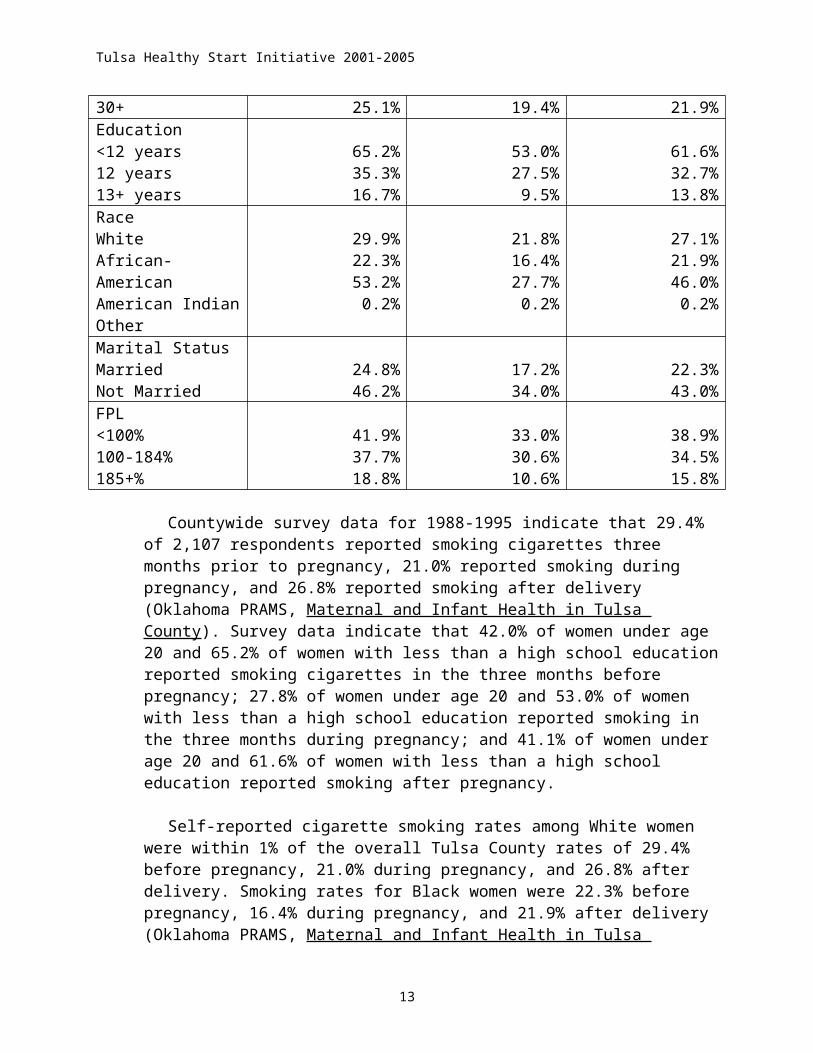
Table 6 Maternal Smoking PatternsMaternal Demographic
Smoking 3 Mths Prior to Pregnancy-PRAMS
Smoking During Pregnancy-PRAMS
Smoking After Delivery
Age<20 years20-2930+
42.0%29.1%25.1%
27.8%20.3%19.4%
41.1%26.4%21.9%
Education<12 years12 years13+ years
65.2%35.3%16.7%
53.0%27.5%9.5%
61.6%32.7%13.8%
RaceWhiteAfrican-AmericanAmerican IndianOther
29.9%22.3%53.2%0.2%
21.8%16.4%27.7%0.2%
27.1%21.9%46.0%0.2%
Marital StatusMarriedNot Married
24.8%46.2%
17.2%34.0%
22.3%43.0%
FPL<100%100-184%185+%
41.9%37.7%18.8%
33.0%30.6%10.6%
38.9%34.5%15.8%
9

Tulsa Healthy Start Initiative 2001-2005
Countywide survey data for 1988-1995 indicate that 29.4% of 2,107 respondents
reported smoking cigarettes three months prior to pregnancy, 21.0% reported smoking during pregnancy, and 26.8% reported smoking after delivery (Oklahoma PRAMS, Maternal and Infant Health in Tulsa County). Survey data indicate that 42.0% of women under age 20 and 65.2% of women with less than a high school education reported smoking cigarettes in the three months before pregnancy; 27.8% of women under age 20 and 53.0% of women with less than a high school education reported smoking in the three months during pregnancy; and 41.1% of women under age 20 and 61.6% of women with less than a high school education reported smoking after pregnancy.
Self-reported cigarette smoking rates among White women were within 1% of the overall Tulsa County rates of 29.4% before pregnancy, 21.0% during pregnancy, and 26.8% after delivery. Smoking rates for Black women were 22.3% before pregnancy, 16.4% during pregnancy, and 21.9% after delivery (Oklahoma PRAMS, Maternal and Infant Health in Tulsa County). By comparison, statewide survey data for 1988-95 indicate that 31.9% of 11,294 respondents reported smoking during the three months before pregnancy (Oklahoma PRAMS, Trend Report). Results from the same survey indicate 22.0% of 11,237 respondents reported smoking during the final trimester before delivery.
For women, cigarette smoking is most prevalent among American Indians. Countywide survey data for 1988-95 indicate that 53.2% reported smoking three months prior to pregnancy, 27.7% reported smoking during pregnancy, and 46.0% of American Indian respondents reported smoking cigarettes after delivery (Oklahoma PRAMS, Maternal and Infant Health in Tulsa County). Another source reports that among Oklahoma's American Indian women, 41.4% smoke, compared to 25.8% of all Oklahoma women and to 27.9% of all Oklahoma women of ages 18-44 (IHCRC, 1995).
Of the 7,398 Tulsa Healthy Start clients that were case managed from September 1998 to December 31, 2004, 740 (10.0%) were found to be in domestic violence.
Table 7 THS Client Domestic Violence by Race and Age for 1998-2004 Race Number Percentage Age Number Percentage
Hispanic 130 17.57% 9-14 years old 3 0.41%White 286 38.65% 15-17 years old 46 6.22%Black 189 25.43% 18-19 years old 79 10.68%American Indian 117 15.81% 20-35 years old 538 72.70%Asian 7 0.95% 36-44 years old 56 7.57%Hawaiian or other Pacific 1 0.14% 45 years old and older 4 0.54%Unknown 10 1.35% Unknown 14 1.89%Total 740 100.00% Total 740 100.00%
Of the 7,398 Tulsa Healthy Start clients that were case managed from September 1998 to December 31, 2004, 476 (6.4%) were found to have depression:
10

Tulsa Healthy Start Initiative 2001-2005
Table 8 THS Client Depression by Race and Age for 1998-2004 Race Number Percentage Age Number Percentage
Hispanic 101 21.22% 9-14 years old 2 0.42%White 175 36.76% 15-17 years old 36 7.56%Black 122 25.63% 18-19 years old 59 12.39%American Indian 74 15.55% 20-35 years old 314 65.97%Asian 0 0.00% 36-44 years old 51 10.71%Hawaiian or other Pacific 1 0.21% 45 years old and older 4 0.85%Unknown 3 0.63% Unknown 10 2.10%Total 476 100.00% Total 476 100.00%
Depression was a co-factor with domestic violence in 141 cases, illicit drug use in 91 cases, drinking in 68 cases, and smoking in 172 cases.
Table 9 Breastfeeding, Family Violence and Depression PatternsMaternal Demographic
Breastfeeding After Delivery-PRAMS
Physically Hurt by Their Partner12 Mths Before Delivery-PRAMS
Depression After Delivery-PRAMSNot Slight/ Very/ Moderate Sought Help
Age<20 years20-2930+
48.1%63.7%73.2%
10.9%6.6%1.7%
23.6% 57.5% 18.9%29.9% 59.4% 10.7%36.5% 56.7% 6.8%
Education<12 years12 years13+ years
45.7%58.3%76.6%
10.6%5.1%3.3%
35.9% 51.5% 14.5%33.7% 55.3% 11.0%30.8% 62.8% 6.9%
RaceWhiteAfrican-AmericanAmerican IndianOther
69.6%34.5%63.7%61.7%
4.2%15.4%7.3%0.0%
31.7% 30.5% 10.1%30.3% 59.4% 9.3%25.1% 64.5% 10.4%54.1% 45.5% 0.4%
Marital StatusMarriedNot Married
72.1%38.1%
3.2%14.4%
31.7% 60.4% 7.6%29.4% 51.1% 19.5%
FPL<100% 48.9% 9.4% 26.5% 60.4%
11

Tulsa Healthy Start Initiative 2001-2005
100-184%185+%
60.6%77.9%
7.4%1.3%
13.1%24.5% 63.5% 12.0%31.8% 59.9% 6.8%
Among other behavioral risk factors, countywide survey data for 1988-95 indicate that 36.4% of 2,107 respondents reported not breastfeeding after delivery (Oklahoma PRAMS, Maternal and Infant Health in Tulsa County). Not breastfeeding after delivery was more common among women under age 20 (51.9%) than among women ages 20-29 (36.3%), and was more common among women with less than a high school education (54.3%) than among those having 13 or more years of education (23.4%). Not breastfeeding was by far more common among Black women (65.5%) than among women of other races (range: 30.4% to 36.3%). Most behavioral risk factors are especially prevalent among low-income, minority, teenage women, many of whom live in the project area.
Factors associated with social variables of domestic violence, child abuse and neglect, and homelessness also adversely affect infant mortality rates in the project area. Countywide survey data for 1988-95 indicate that 5.7% of 2,107 respondents reported that they were physically hurt by their husband or partner in the 12 months prior to delivery (Oklahoma PRAMS, Maternal and Infant Health in Tulsa County). Domestic violence was much more prevalent among Black women (15.4%) and American Indian women (7.3%) and less prevalent among White women (4.2%). Domestic violence also was more prevalent among women under age 20 (10.9%) than those ages 20-29 (6.6%), and much more common among women with less than a high school education (10.6%) than with those having 13 or more years of education (3.3%) (Oklahoma PRAMS).
By comparison, statewide survey data for 1988-95 indicate that 8.7% of 11,457 respondents reported being involved in a physical fight during pregnancy, and that 5.9% of 11,452 respondents were physically hurt by a husband or partner (Oklahoma PRAMS, Trend Report). The 7-year data also indicate that 10.5% of 11,459 respondents either were involved in a physical fight or were physically hurt by the husband or partner during the 12 months before delivery (Oklahoma PRAMS, Trend Report).
Survey data for Tulsa County for 1988-95 indicate that among women giving birth, 2.4% reported being homeless in the 12 months before delivery (Oklahoma PRAMS data). Statewide survey data for 1988-95 indicate that among women giving birth 3.0% reported being homeless in the same time interval (Oklahoma PRAMS, Trend Report). Data by project area census tracts are not available.
There is an upward trend in confirmed child abuse cases in Tulsa County. From 1988-95, the rate of confirmed child abuse cases rose from 3.1 per 1,000 children to 7.7 per 1,000 children. In 2000, the Oklahoma State Department of Human Services (OSDHS) investigated 3,303 cases of child abuse and neglect in Tulsa County. It confirmed 1,347 cases, or 40.7% of those investigated, for a rate of 8.4 cases of abuse per 1,000 children in Tulsa County (ODHS, Annual Reports). In the same year, 10 children died of abuse and neglect in Tulsa County with over 50% less than one year old.
12
Tulsa Healthy Start Initiative 2001-2005
Healthy Start data prepared from the clients who received case management services from January 1998 to December 2001 and January 2003 to December 2004 amplifies the risk factors presented in the Oklahoma PRAMS data. The weighted risk assessment was reviewed in 2002 and additional family and women’s health factors were included in the survey.
Table 10 Risk Factors for THS Clients from 1998 – 2001 and 2003 -- 2004* means higher % than overall % on the 1998-2001
Risks Overall Scores1998-2001
Overall
Scores2003-2004
White Black Native Amer.
Asian Other Hisp.Origin
Less than high school ed
67% 54% 73%* 51% 75%* 71%* 72%* 85.5%
Lack of transportation
50% 60% 53%* 45% 30% 71.4%*
72.7%*
55.3%
Lack of one other adult to share with
42% 62.9% 46.6%* 34.2% 20% 80%* 90%* 45.2%
Lack of adequate, stable housing
34% 42.9% 38%* 28% 12.5% 57%* 54.5%*
6%
Smoking 28% 40.1% 28% 24.2% 24.2% 0 54.5%*
1.6%
Frequent crises 27% 35.9% 30%* 24% 2.5% 43%* 45.5%*
33.6%
Medical condition coexisting with pregnancy
23% 26.4% 29%* 18% 7.5% 14% 0 29.6%
Frequent conflict 22% 35.1% 26%* 17% 2.5% 43%* 45.5%*
27.6%
Hx of previous miscarriage
22% - 24%* 26%* 20% 0 18% 35%
Domestic violence
18% 36% 21.5%* 14.2% 6.6% 0 0 16.6%
Drug abuse 17% 17.6% 18.5%* 16.7% 18.6%*
0 0 5.6%
Psychiatric diagnosis
15.4% 29.8% 18.5%* 12.1% 4.6% 25%* 10% 13.5%
Low Birth Weight-below 2500 grams
15% 18.6% 13.4% 20%* 8.3% 0 0 9.4%
Ambivalence about pregnancy at 20 weeks
14% 9.5% 8% 9.3% 6.1% 0 16.7%*
8%
Hx of premature babies
13% 13% 12.3% 16.7%* 6% 0 0 13.7%
Current or past sexual abuse
11.1% 6.2% 12.5%* 9.9% 9.3% 0 0 7.7%
Current or past hx of children & DHS
11% 10.7% 12%* 11% 5% 14%* 0 .5%
Hx of abortions 11% 14.8% 12%* 9% 12%* 0 33%* 5.7%Drinking and 10% 20.3% 9.3% 11.7%* 9% 0 0 0%
13

Tulsa Healthy Start Initiative 2001-2005
pregnancyHIV+ or AIDS 7% 5.6% 10.6%* .8% 0 0 0 11.2%Incarceration or Probation
7% 6.8% 7% 9.6%* 2.5% 0 0 1.2%
Hx of death of child before age 1 year
6% 7.9% 5.3% 7.2%* 5.5% 0 0 6.4%
Eating disorder 4% 9.1% 4.7%* 3.1% 6.1%* 0 0 1.6%English as a Second Language
11.2%
Medical diagnosis co-existing with pregnancy that is uncontrolled
14.6%
Family member with illicit drug use
9.9%
Previous pregnancy with congenital anomaly
4.5%
Hx of special needs children
1.7%
Current alcohol use
3.4%
Ambivalence toward pregnancy initial reaction
26.5%
Work site risks 4.5%Family alcohol use
20.4%
Hx of depression 33.9%Current dx of depression
17.5%
Current periodontal infection
20%
Father involvement in pregnancy-None
20.2%
2-5 sexual partners in the last year
14.4%
Little or no exercise
18.2%
Family hx of breast cancer
1.2%
Fecal blood with no confirming test
15.8%
Gestational diabetes mellitus
22.5%
Analysis reveals in comparison to the overall total for 1998 to 2001, African-American women are more likely to have had a previous miscarriage, a low birth weight birth, history of premature birth, drinking with pregnancy, incarceration or probation
14

Tulsa Healthy Start Initiative 2001-2005
status, history of death of a child before age 1 year and eating disorder. The Native American women were more liking to smoke, have a history of miscarriage, drug abuse, low birth weight birth, history of premature babies, drinking while pregnant, incarceration or probation, history of death of child before age 1 year and eating disorder. The Asian population has a low population representation in this survey but reveal their risks to be lack of one other adult to share with, frequent crises, frequent conflict, psychiatric diagnosis, and current or past history of children in the Department of Human Services custody. The women of Hispanic Origin risks are frequent crisis, medical condition coexisting with pregnancy, frequent conflict, history of miscarriage, psychiatric diagnosis, ambivalence about pregnancy at 20 weeks, HIV or AIDS, and history of death of child before age 1 year. Consistent factors across racial and ethnic boundaries is poverty, less than high school education, lack of transportation and lack of adequate, stable housing. Smoking rate is at 28% of the total with the exception of Hispanic origin women who have a 1.6% smoking rate.
The 2003-2004 data has not been analyzed by race. Additional risk factors have been added to the weighted risk assessment which focus on family health and women’s health. Serious indicators of gestational diabetes mellitus (22.5%), history of depression (33.9%) and family alcohol use (20.4%) have demonstrated significant risk levels.
Poverty LevelIn the project area, in 2000, there was 30.5% of the total population living at or
below 100% of federal poverty level (2000 U.S. Census). The white population was 20.5%, Black 42.1%, Native American 17.0%, Asian/Other 18.7% and those with Hispanic origin of 17%. This is compared to Tulsa County at 16.1% with 9.4% white, 41.5% Black, 18.1% Native American, 21.0% Asian/Other and Hispanic origin of 25.7% for the same time period.
By way of comparison, in Tulsa County, 49.2% of 2,107 survey respondents from 1988-1995 reported they lived at or below 185% of federal poverty level (Oklahoma PRAMS, Maternal and Infant Health in Tulsa County). Among survey respondents, 78.2% of Black women lived at or below 185% of federal poverty level, compared to 60.6% of American Indian women, and 44.3% of White women. In addition, 93.1% of women under age 20 and 84.2% of women with less than a high school education lived at or below 185% of federal poverty level, compared to 48.3% of women ages 20-29 and 27.6% of women with 13 or more years of education.
Eligibility for Tulsa Healthy Start services are limited to women whose family incomes are 185% of the federal poverty level or less. All the women qualify for the SoonerCare (combined Medicaid managed care/State child health insurance program)
In 2005, there was an estimated 19% of Tulsa County person’s of all ages who were uninsured and 15% using Medicaid. (University of Oklahoma, 2005). Data by race, ethnicity and zip codes are not available. This estimate represents approximately 106,970 uninsured and 84,450 on Mediciad in Tulsa County. However, the Oklahoma Health Care Authority in March 2004 estimated the uninsured number to be 33% of the adult population (Tulsa World, 2004).
15

Tulsa Healthy Start Initiative 2001-2005
For FY 2005, there were 4,409 women and children receiving Temporary Assistance to Needy Families (TANF) in Tulsa County (14.3% of the state’s TANF cases) down from the 5,444 of November 2003.. By race, there were 27.1% White, 60.8% Black, 6.5% American Indian, 0.003% Asian, and 5.1% Hispanic. (Oklahoma State Department of Human Services, Family Support Services Division data 2005). Data by race in zip code is not available.
Statewide survey data for 1988-1995 indicate that 41.59% of 11,435 respondents reported paying for delivery by Medicaid (Oklahoma PRAMS, Trend Report). Medicaid was used as a method of payment for delivery for 29.9% of 2,107 women who gave birth in Tulsa County from 1988-1995 (Oklahoma PRAMS, Maternal and Infant Health in Tulsa County); it was used by 66.7% of women under age 20, 55.0% of women with less than a high school education, and was used by 54.2% of Black women, compared to 26.2% of White, 22.4% of American Indian, and 22.7% of other-race women. This number has grown to 46% of all births in Tulsa County are paid for by Medicaid in 2003 (OSDH, Perinatal Health Report, 2004). All births of THS case managed clients are paid for by SoonerCare, however, undocumented Hispanic women cannot receive Sooner Care for their prenatal care and must pay on a sliding scale.
Maternal Educational LevelIn Tulsa County (US Census 2000), there were 14.5% of person’s ages 25 and older
who had achieved less than a high school education. By race or ethnicity, there were 15.8% White, 28.0% Black, 23.7% American Indian, 47.6% of other races, and 35.6% of Hispanic Origin persons ages 25 and older who had achieved less than a high school education (U.S. Census 2000). Among persons ages 25 and older in census tracts in the project area, the comparable rates were 30.5% of total, 22.4% White, 49.2% Black, 42.4% other races, and 44.9% of Hispanic Origin persons. For all but other races, educational attainment is lower in the project area than in Tulsa as a whole. By comparison, in Tulsa County, 16.4% of 2,107 survey respondents who had given birth from 1988-95 had less than a high school education; among the Tulsa County survey respondents, 84.2% of those with less than a high school education lived at or below 185% federal poverty level (Oklahoma PRAMS, Maternal and Infant Health in Tulsa County). The January 1998 to December 2001 THS data indicated the 67% of the overall participants had less than a high school education with 73% White, 51% African-American, 75% Native American, 71% Asian and 72% of other. Women of Hispanic Origin indicate that 85.5% had less than a high school education and the education process was not in the United States. The January 2003 to December 2004 data indicates that 54% do not have a high school education. Data by race is not available.
Perinatal MeasuresThe OSDH reports that average for live births in the project area (1999-2001) was
1,779. There were an average 853 White live births, 971 Black live births, 94 Native American live births, 6 Asian live births and 74 Hispanic origin live births. (OSDH, MCH Planning and Evaluation Section, 2004).
The average for infant deaths (under 1 year of age) in project area (1999-2001) was 25.3 (14.2 IMR). There were an average 10 (11.7 IMR) White infant deaths, 19.7 (20.28 IMR) Black infant deaths, 2.3 Native American (24.28 IMR), 0.3 (47.37 IMR) Asian
16

Tulsa Healthy Start Initiative 2001-2005
infant death and 1.3 (17.7) Hispanic origin infant deaths. (OSDH, MCH Planning and Evaluation Section, 2004).
The average of births to teenagers 19 years of age or younger in the project area (1999-2001) was 326. There were an average 145 White births, 221 Black births, 20 Native American, 0 Asian and 15 Hispanic Origin. (OSDH, MCH Planning and Evaluation Section 2004). However, Babyline data for 2004 indicates that 25.1% of births to women 19 years of age or younger in the project area were to women of Hispanic origin compared to 74.9% for non-Hispanic (Babyline 2005).
For 1999-2001, the average births to women who received prenatal care during the first trimester in the project area were 1,169 (65.7%). There were an average 559 White births, 587 Black births, 58 Native American, 4 Asian births and 42 Hispanic origin. (OSDH, MCH Planning and Evaluation Section 2004). Babyline data for 2004 indicates that 51.9% (48.2% in 2003) of women of Hispanic origin compared to 68% (62.6% in 2003) non-Hispanic women entered prenatal care in the first trimester. In 2004, Babyline data indicated that 51.9% of Hispanic women received prenatal care in the first trimester with 76.6% seeking care in the first trimester. Many had to postpone their prenatal care until a sliding scale appointment was available or they had raised the initial visit fee (usually over $100). 27.5% (20.9% in 2003) waited one week or less for an appointment, 12.7% (8.1% in 2003) waited 2 weeks and 12.4% (14.2% in 2003) waited three weeks. Over 35% (57% in 2003) waited 5 weeks or more for an appointment compared to 11.3% for non-Hispanic women. 32.2% of all third trimester entries into prenatal care are women of Hispanic Origin. This trend to later entry into prenatal care is suggestive of both system and individual issues. The number of Hispanic clients has increased from 122 in 1998 to 1,302 in 2003 and 1,177 in 2004. Culturally competent services are located in two primary safety-net providers, the Tulsa Health Department and Planned Parenthood. As a result, some Hispanic women prefer to delay prenatal care rather than enter a clinic they feel less comfortable. (Babyline, 2005)
The average for births to women who received no prenatal care in the project area (1999-2001) was 39 (2.1%). There were 18 White births, 31 Black births, 4 Native American births, <1 Asian birth and Hispanic origin 3. (OSDH, MCH Planning and Evaluation Section, 2004). Babyline data for 2004 indicates that 4.5% (5.6% in 2003) of women of Hispanic origin received third trimester entry into prenatal care compared to 3.8% (4.8% in 2003) non-Hispanic women. THS statistics reflect the high risk nature of the women served in case management.
Table 11 THS Women in Case Management and Percent of First Trimester of Entry Into Prenatal Care 2001 -- 2004
Ethnicity 2001 2002 2003 2004
Hispanic 26.6% 24.7% 19.0% 19.6%
Non-Hispanic 40.2% 40.0% 25.0% 30.5%
17

Tulsa Healthy Start Initiative 2001-2005
Data for 1999-2003 on women with positive human immunovirus (HIV) screenings at the time of delivery, disaggregated by race, ethnicity, and census tract, are not available. In Tulsa County, HIV screening is not routinely conducted at the time of delivery. Tulsa Healthy Start data from January 1998 to December 2004 indicated that of 7,398, 4 women were positive.
Infant Mortality and Low Birth Weight Indicators
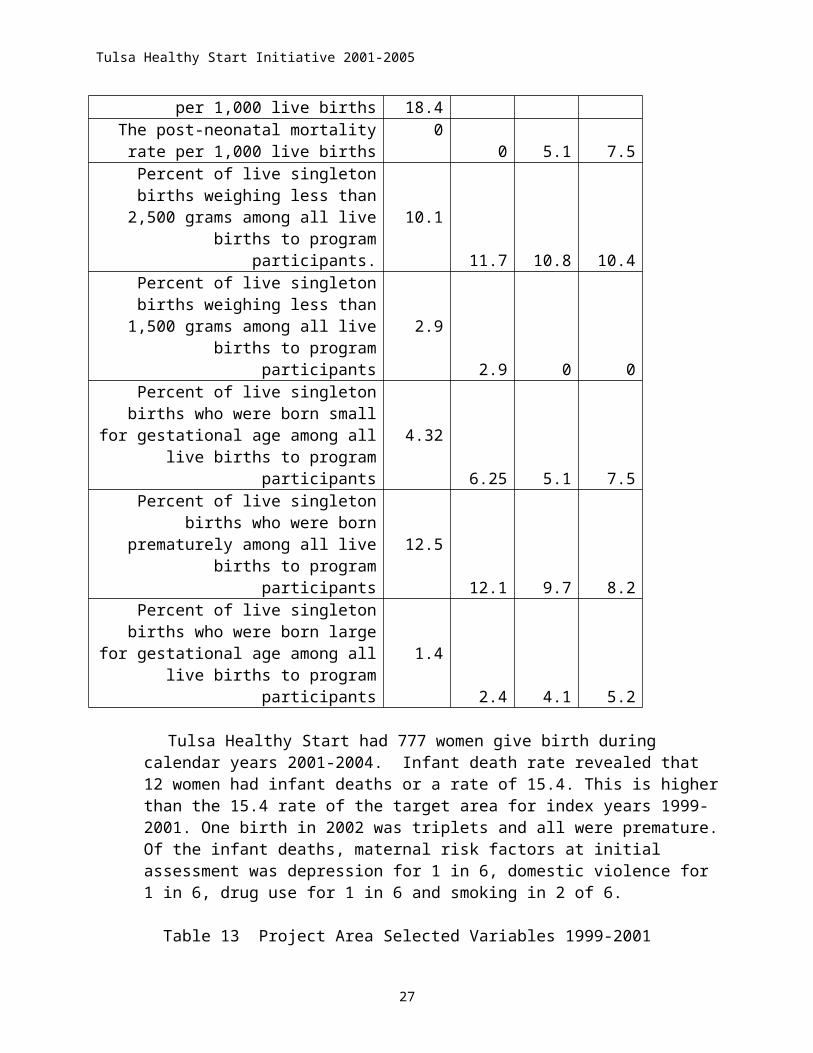
Table 12 THS Infant Mortality-Morbidity Data from 2001 -- 2004 2001 2002 2003 2004
The infant mortality rate per 1,000 live births
18.416.7 15.4 14.9
The neonatal mortality rate per 1,000 live births 18.4 16.7 10.3 7.5
The post-neonatal mortality rate per 1,000 live births
00 5.1 7.5
Percent of live singleton births weighing less than 2,500 grams among all live births
to program participants. 10.1 11.7 10.8 10.4Percent of live singleton births weighing
less than 1,500 grams among all live births to program participants 2.9 2.9 0 0
Percent of live singleton births who were born small for gestational age among all
live births to program participants 4.32 6.25 5.1 7.5Percent of live singleton births who were born prematurely among all live births to
program participants 12.5 12.1 9.7 8.2Percent of live singleton births who were born large for gestational age among all
live births to program participants 1.4 2.4 4.1 5.2
Tulsa Healthy Start had 777 women give birth during calendar years 2001-2004. Infant death rate revealed that 12 women had infant deaths or a rate of 15.4. This is higher than the 15.4 rate of the target area for index years 1999-2001. One birth in 2002 was triplets and all were premature. Of the infant deaths, maternal risk factors at initial assessment was depression for 1 in 6, domestic violence for 1 in 6, drug use for 1 in 6 and smoking in 2 of 6.
Table 13 Project Area Selected Variables 1999-2001
VARIABLE WHITE BLACK
NATIVE AMER.
ASIAN/ OTHER
(N) TOTA
L
HISP. ORIG.
3-Year Average: 1999-2001: # Live Births 853 971 94 6 1,779 74# Births to Teens 17 & younger 46 87 7 0 118 6# Births to Teens 18 & 19 99 134 13 0 208 9# Live Births with 1st Trimester entry 559 587 58 4 1,169 42
18

Tulsa Healthy Start Initiative 2001-2005
# Live Births with No Prenatal Care 18 31 4 0 39 3# Infant Deaths 10.0 19.7 2.3 0.3 25.3 1.3
Infant Mortality Rate (per 1,000 live births) 11.72 20.28 24.38 47.37 14.22 17.57
# Neonatal Infant Deaths (birth to 28 days)2 5.7 12.0 0.7 0.0 15.7 0.7
Neonatal Mortality Rate (per 1,000 live births)2 6.63 12.64 7.84 0.00 9.03 9.86
# Post-Neonatal Infant Deaths (29 to 365 days)2 6.3 8.3 0.7 0.3 9.0 0.3
Post-Neonatal Mortality Rate (per 1,000 live births)2 7.33 8.74 7.84 34.62 5.18 4.23
# Moderate Low Birth Weight (LBW) infants born with birth weight of 1501 to 2500 grams 49 101 3 1 130 3
Moderate Low Birth Weight Rates, % 5.8% 10.4% 3.5% 10.5% 7.3% 4.5%
# Very Low Birth Weight (VLBW) infants born with birth weight of 1500 grams or less 9 32 1 0 28 2
Very Low Birth Weight Rates, % 1.1% 3.3% 1.1% 0.0% 1.6% 2.3%Age Appropriate Immunization Rates
of Children from Birth to 2 Years3 NA NA NA NA NA
*Target population zip codes: For Whites: 74073 74106, 74107, 74116, 74126, 74127, 74146; For Blacks: 74012, 74104, 74105, 74106, 74107, 74110, 74112, 74113, 74116, 74126, 74128, 74130, 74133, 74134, 74135, 74145, 74146; For Native Americans: 74011, 74070, 74104, 74105, 74110, 74114; For Asians/Others: 74135; For all races combined: 74070, 74073, 74104, 74105, 74106, 74107, 74116, 74126; and For Hispanic origin: 74055, 74106, 74108 and 74114.
For the period 1996-1998 (index years for the second cycle), the average infant mortality rate per 1,000 live births within the project area was 14.5. There were an average 11 White infant mortalities, 15 Black infant mortalities, 3 Native American and 1 Asian infant mortality. The infant mortality rate was an average 14.50 for all races 13.69 White, 19.10 Black, 57.47 Native American and 27.52 Asian (OSDH 2000). The target population demographics for 1991-2001 have an overall infant mortality rate of 14.2 with White 11.7, Black 20.28, Native American 24.38, and Hispanic 17.57. The average number of deaths in the target zip codes by race per race is White 10, Black 9, Native American 2, Asian 0.3 and Hispanic origin 1.3. (OSDH, 2004)
Historically, the project area has had a variable history in infant mortalities. This variation can be attributed to mobility of the population in the project areas, a change in the health care delivery system (Medicaid managed care), an in-migration of women of Hispanic origin and data entry changes at the OSDH. In 1994, the infant mortality rate per 1,000 live births rose substantially among White infants and declined for all other races. There were an average of 17.0 infant mortalities among all races in the project area. There were an average 19.0 White infant mortalities, 14.1 Black infant mortalities, and 7.9 infant mortalities among other races. In 1995, the mortality rate among White infants fell to below the 1991-1993 averages; it rose again among Black infants, and more than tripled among infants of other races. Since 1988-90, the overall trend is higher infant mortality rates among all races in the total project area.
19

Tulsa Healthy Start Initiative 2001-2005
In Tulsa County, the disproportion share of infant deaths to births is in women under age 20, and minority heritage. Time of entry into prenatal care, economics and marital status show no correlation to infant mortality. This was documented through the 10 Year Analysis of Linked Birth and Death Certificates (THD, 2004), the Tulsa Healthy Start data analysis and the Pregnancy Periods of Risk Analysis 1996-2000 (TFIMR, 2004). However, fetal-infant mortality deaths are sharply higher among Hispanic women and represent factors in a lack of maternal care.
Table 14 Tulsa County 357 Feto-Infant Death Rates by Maternal Race and Pregnancy Period of Risk, 1996 – 2000
Maternal Health Prematurity
Maternal Care Newborn Care Infant Health
White Non-Hispanic 2.31 1.29 1.52 1.42African American 4.02 2.63 2.16 2.94Native American 2.18 1.82 1.09 2.54
Hispanic 4.65 9.00 0.87 1.74Other 0 3.62 2.41 1.21
For 1999-2001, the average neonatal mortality rate among all races in the project area was 9.03 per 1,000 live births. There were an average rate of 6.63 White neonatal mortalities, 12.64 Black neonatal mortalities, 7.84 Native American neonatal mortalities and 9.86 neonatal mortalities among women of Hispanic origin (OSDH, 2004). There is a strong correlation to the low birth weight and very low birth weight for White, Black and Native American infant deaths.
The average post-neonatal mortality rate among all races in the project area (1999-2001) was 5.18 per 1,000 live births. There were an average rate 7.33 White post-neonatal mortalities, 8.74 Black post-neonatal mortalities, 7.84 Native American 34.62 Asian and 4.23 post-neonatal mortalities among women of Hispanic origin. (OSDH, 2004). A strong correlation between race and post-neonatal rate for Black, and Native American exists. Although, the Asian rate was dramatic the population was <1 for the three year average.
For 1999-2001, the average low birth weight birth rate within the project area was 7.3%. There were an average percentage was 5.8% White low birth weight births, 10.4% Black low birth weight births, 3.5% Native American, 10.5% Asian and 4.5% low birth weight births among women of Hispanic origin (OSDH 2004).
Infant Health Status Measures
Table 15 Causes of Neonatal, Post-neonatal and Infant Deaths in Tulsa County by Healthy Start Index Years—1999-2002 Neonatal and Post-neonatal Causes Not Aggregated
Cause of Death 1988-1990
1991-1993
1994 1995 1996-1998
1999-2001
2002
Neonatal DeathsExtreme ImmaturitySIDS
6%2%
16%0%
7%4%
13%2%
19%1%
20

Tulsa Healthy Start Initiative 2001-2005
Birth InjuriesCongenital Abn.Communicable DiseasesResp. Prob, other Perinatal Conditions
7%34%7%
42%
6%28%12%34%
6%24%15%44%
4%21%13%42%
4%25%14%37%
Post Neonatal DeathsPrematuritySIDSBirth DefectsCongenital Abn.Homicide and NeglectAccidentsCommunicable DiseasesOther prevalent factors
0%47%1%9%2%1%
13%23%
0%47%1%
11%0%6%
10%25%
4%31%0%8%4%8%
19%27%
4%35%0%
17%0%0%
13%30%
3%36%0%
12%0%0%5%
25%Infant MortalityPrematuritySIDSBirth DefectsCongenital Abn.Homicide and NeglectAccidentsCommunicable DiseasesOther prevalent factors
3%
23%4%
20%1%2%
10%22%
10%19%4%
21%0%2%
12%23%
6%
13%4%
21%0%2%
12%23%
11%12%3%
20%0%0%
13%32%
12%15%0%
20%0%0%2%
51%
14%8%0%
18%2%3%0%
55%
13%7%0%
24%0%0%0%
56%
Prematurity is a growing cause of neonatal infant deaths in Tulsa County. From 1988-1990, extreme immaturity accounted for 6% of causes of neonatal infant deaths in Tulsa County; from 1991-1993, it accounted for 16% of causes of neonatal infant deaths. In 1994, extreme immaturity accounted for 7% of causes of neonatal infant deaths in Tulsa County; in 1995, it accounted for 13% of causes of neonatal infant deaths in 1996-1998, it accounted for 19% and in 1999-2001 14% (OSDH, MCH Planning and Evaluation Section 1988-2001).
Sudden infant death syndrome (SIDS) is not a large cause of neonatal infant deaths in Tulsa County. From 1988-1990, SIDS accounted for 2% of causes of neonatal infant deaths; from 1991-1993, SIDS was not reported as a cause of neonatal infant deaths. In 1994, SIDS accounted for 4% of causes of neonatal infant deaths; in 1995, it accounted for 2% of causes of neonatal infant deaths. For 1996-1998, SIDS accounted for 1% of the neonatal infant deaths. There is no data available 1999-2001 at the time of this application. (OSDH, MCH Planning and Evaluation Section 1988-2001).
Birth defects are declining as a cause of neonatal infant deaths in Tulsa County. From 1988-1990, birth injuries (intracranial hemorrhage, severe/unspecified birth asphyxia) accounted for 7% of causes of neonatal infant deaths. From 1991-1993, birth injuries (intracranial hemorrhage, severe/unspecified birth asphyxia) accounted for 6% of causes of neonatal infant deaths. In 1994, birth injuries again accounted for 6% of causes of neonatal infant deaths, and in 1995, birth injuries (intracranial hemorrhage) accounted for 4% of causes of neonatal infant deaths. For 1996-1998, birth defects were not listed and
21

Tulsa Healthy Start Initiative 2001-2005
birth injuries were 4% of the neonatal infant deaths. No data is available for 1999-2001 (OSDH, MCH Planning and Evaluation Section, 1988-2001).
Congenital abnormalities are declining as a cause of neonatal infant deaths in Tulsa County. From 1988-1990, congenital abnormalities (compressed umbilical cord, circulatory, diaphragm, Edwards syndrome, multiple, nervous, Pataus syndrome, pulmonary, renal, placental abnormalities, incompetent cervix or premature rupture, and multiple pregnancy) accounted for 34% of causes of neonatal infant deaths. From 1991-93, congenital abnormalities (compressed umbilical cord, circulatory, diaphragm, Edwards syndrome, multiple, nervous, Pataus syndrome, pulmonary, renal, placental abnormalities, and incompetent cervix or premature rupture) accounted for 28% of causes of neonatal infant deaths. In 1994, congenital abnormalities (circulatory, multiple, nervous, pulmonary, renal, placental abnormalities, incompetent cervix or premature rupture) accounted for 24% of causes of neonatal infant deaths. In 1995, congenital abnormalities (circulatory, diaphragm, Edwards syndrome, nervous, other, pulmonary, and renal) accounted for 21% of causes of neonatal infant deaths. For 1996-1998 congenital abnormalities accounted for 25% of neonatal infant deaths. Data is not available for 1999-2001 (OSDH, MCH Planning and Evaluation Section, 1988-2001).
Neither homicide or neglect nor accidents were reported as a cause of neonatal infant deaths in Tulsa County for the periods 1988-1990 and 1991-1993 or for the years 1994 and 1995 or for 1996-1998. No data is available for 1999-2001 (OSDH, MCH Planning and Evaluation Section 1988-2001).
Other communicable diseases are generally increasing as a cause of neonatal infant deaths in Tulsa County. From 1988-1990, infections (chorioamnionitis, infectious and parasitic disease, necrotizing enterocolitis, and other perinatal infections) accounted for 7% of causes of neonatal infant deaths. From 1991-1993, infections (chorioamnionitis, infectious and parasitic disease, maternal infections, meningitis, necrotizing enterocolitis, and other perinatal infections) accounted for 12% of causes of neonatal infant deaths. In 1994, infections (necrotizing enterocolitis, respiratory infections, and other perinatal infections) accounted for 15% of causes of neonatal infant deaths in Tulsa County. In 1995, infections (chorioamnionitis, respiratory infections, and other perinatal infections) accounted for 13% of causes of neonatal infant deaths. For 1996-1998, infections accounted for 14% of neonatal infant deaths. No data is available for 1999-2001. (OSDH, MCH Planning and Evaluation Section 1988-2001).
Other prevalent factors are consistently a large cause of neonatal infant deaths in Tulsa County. From 1988-1990, respiratory problems, other perinatal conditions and other/unknown causes accounted for 42% of causes of neonatal infant deaths; from 1991-1993, they accounted for 34% of causes of neonatal infant deaths. In 1994, respiratory problems, other perinatal conditions and other/unknown causes accounted for 44% of causes of neonatal infant deaths in Tulsa County; in 1995, they accounted for 42% of causes of neonatal infant deaths and in 1996-1998 for 37%. No data is available 1999-2001. (OSDH, MCH Planning and Evaluation Section, 1988-2001).
Prematurity is a minimal but emerging cause of post-neonatal infant deaths in Tulsa County. From 1988-1990, and from 1991-1993, extreme immaturity is not reported as a
22

Tulsa Healthy Start Initiative 2001-2005
cause of post-neonatal infant deaths in Tulsa County. In 1994 and in 1995, extreme immaturity accounted for 4% of causes of post-neonatal infant deaths in Tulsa County and in 1996-1998, 3% (OSDH, MCH Planning and Evaluation Section data).
Sudden infant death syndrome (SIDS) is a large but declining cause of post-neonatal infant deaths in Tulsa County. From 1988-1990, and from 1991-1993, sudden infant death syndrome (SIDS) accounted for 47% of causes of post-neonatal infant deaths. In 1994, SIDS accounted for 31% of causes of post-neonatal infant deaths in Tulsa County; in 1995, it accounted for 35% of causes of post-neonatal infant deaths. For 1996-1998, SIDS accounted for 36% of post-neonatal infant deaths. No data is available for 1999-2001. (OSDH, MCH Planning and Evaluation Section, 1988-2001).
Birth defects are a small cause of post-neonatal infant deaths in Tulsa County. From 1988-1990, birth injuries (severe/unspecified birth asphyxia) accounted for 1% of causes of post-neonatal infant deaths in Tulsa County. From 1991-1993, birth injuries (intracranial hemorrhage) accounted for 1% of causes of post-neonatal infant deaths in Tulsa County. In 1994, 1995 and 1996-1998 birth injuries were not reported as a cause of post-neonatal infant deaths. No data is available for 1999-2001. (OSDH, MCH Planning and Evaluation Section 1988-2001).
Congenital abnormalities are a growing cause of post-neonatal infant deaths in Tulsa County. From 1988-1990, congenital abnormalities (circulatory, nervous) accounted for 9% of causes of post-neonatal infant deaths in Tulsa County. From 1991-1993, congenital abnormalities (circulatory, Edwards syndrome, Pataus syndrome, and pulmonary) accounted for 11% of causes of post-neonatal infant deaths. In 1994, congenital abnormalities (circulatory and diaphragm) accounted for 8% of causes of post-neonatal infant deaths in Tulsa County; in 1995, congenital abnormalities (circulatory) accounted for 17% of causes of post-neonatal infant deaths. For 1996-1998, congenital abnormalities (primarily circulatory) accounted for 12% of post-neonatal infant deaths. No data is available for 1999-2001 (OSDH, MCH Planning and Evaluation Section 1988-2001).
Homicide and neglect is a small cause of post-neonatal infant deaths in Tulsa County. From 1988-1990, homicide or neglect accounted for 2% of causes of post-neonatal infant deaths; from 1991-1993, homicide or neglect was not reported as a cause of post-neonatal infant deaths. In 1994, homicide or neglect accounted for 4% of causes of post-neonatal infant deaths in Tulsa County; in 1995 and 1996-1998 homicide or neglect was not reported as a cause of post-neonatal infant deaths. No data is available for 1999-2001 (OSDH, MCH Planning and Evaluation Section, 1988-2001).
Accidents are a small but tragic cause of post-neonatal infant deaths in Tulsa County. From 1988-1990, accidents (drowning, falls, fire, and suffocation) accounted for 1% of causes of post-neonatal infant deaths. From 1991-1993, accidents (drowning, falls, fire, suffocation, and unspecified) accounted for 6% of causes of post-neonatal infant deaths in Tulsa County. In 1994, accidents (drowning, falls, and unspecified) accounted for 8% of causes of post-neonatal infant deaths in Tulsa County. Beginning in 1995 and continuing through 1996-1998 accidents were not reported as a cause of post-neonatal
23

Tulsa Healthy Start Initiative 2001-2005
infant deaths. No data is available for 1999-2001 (OSDH, MCH Planning and Evaluation Section, 1988-2001).
Other communicable diseases are a large and growing cause of post-neonatal infant deaths in Tulsa County. From 1988-1990, infections (infectious and parasitic disease and respiratory infections) accounted for 13% of causes of post-neonatal infant deaths. From 1991-1993, infections (common cold, meningitis, necrotizing enterocolitis, respiratory infections, and other perinatal infections) accounted for 10% of causes of post-neonatal infant deaths. In 1994, infections (infectious and parasitic disease and respiratory infections) accounted for 19% of causes of post-neonatal infant deaths in Tulsa County. In 1995, infections (common cold and respiratory infections) accounted for 13% of causes of post-neonatal infant deaths; and for 1996-1998, 5% of causes of death. No data is available for 1999-2001 (OSDH, MCH Planning and Evaluation Section 1988-2001).
Other prevalent factors are a large and growing cause of post-neonatal infant deaths in Tulsa County. From 1988-1990, and from 1991-1993, respiratory problems, other perinatal conditions and other/unknown causes accounted for 25% of causes of post-neonatal infant deaths. In 1994, other/unknown causes accounted for 27% of causes of post-neonatal infant deaths in Tulsa County; in 1995, other/unknown causes accounted for 30% of causes of post-neonatal infant deaths. For 1996-1998, 25% other/unknown causes of post-neonatal infant death were reported. No data is available for 1999-2001.(OSDH, MCH Planning and Evaluation Section, 1988-2001).
Prematurity is a growing cause of infant deaths in Tulsa County. From 1988-1990, extreme immaturity accounted for 3% of causes of infant deaths in Tulsa County; from 1991-1993, it accounted for 10% of causes of infant deaths. In 1994, extreme immaturity accounted for 6% of causes of infant deaths in Tulsa County; in 1995, it accounted for 11% of causes of infant deaths, in 1996-1998, 12% and in 1999-2001, 14% (OSDH, MCH Planning and Evaluation Section, 1988-2001).
Sudden infant death syndrome (SIDS) is a large but declining cause of infant deaths in Tulsa County. From 1988-1990, sudden infant death syndrome (SIDS) accounted for 23% of causes of infant deaths; from 1991-1993, it accounted for 19% of causes of infant deaths, in 1994, SIDS accounted for 13% of causes of infant deaths, and in 1995, it accounted for 12% of causes of infant deaths. For 1996-1998, SIDS deaths were up to 15% of causes of infant death, 1999-2001 a drop to 8% and 2002 7% (OSDH, MCH Planning and Evaluation Section 1988-2002).
Birth injuries are a small and stable cause of infant deaths in Tulsa County. From 1988-1990, and from 1991-1993, birth injuries (intracranial hemorrhage, severe/unspecified birth asphyxia) accounted for 4% of causes of infant deaths in Tulsa County. Again in 1994, birth injuries accounted for 4% of causes of infant deaths, and in 1995, they accounted for 3% of causes of infant deaths. For 1996-1998, they accounted for 2% of causes of infant death, 1999-2002 were 0% (OSDH, MCH Planning and Evaluation Section, 1999-2002).
Congenital abnormalities are a large and stable cause of infant deaths in Tulsa County. From 1988-1990, congenital abnormalities (circulatory, diaphragm, Edwards
24

Tulsa Healthy Start Initiative 2001-2005
syndrome, multiple, nervous, Pataus syndrome, pulmonary, renal, placental abnormalities, incompetent cervix or premature rupture, and multiple pregnancy) accounted for 20% of causes of infant deaths. From 1991-1993, congenital abnormalities (circulatory, diaphragm, Edwards syndrome, multiple, nervous, Pataus syndrome, pulmonary, renal, placental abnormalities, and incompetent cervix or premature rupture) accounted for 21% of causes of infant deaths. In 1994, congenital abnormalities (circulatory, diaphragm, multiple, nervous, pulmonary, renal, placental abnormalities, and incompetent cervix or premature rupture) accounted for 19% of causes of infant deaths. In 1995, congenital abnormalities (circulatory, diaphragm, Edwards syndrome, nervous, other, pulmonary, renal) accounted for 20% of causes of infant deaths, in 1996-1998, 20% causes of infant death, in 1999-2001 18% and 2002 24%. A great deal of investigation through the TFIMR process is being conducted into the congenital anomalies ICD 10 designation. Many physicians, unwilling or unable to determine at death the cause of death related to genetics or interruptions in the fetal development process because of drug use, smoking or alcohol will cite congenital anomalies as the cause of death. (OSDH, MCH Planning and Evaluation Section, 1988-2002).
Homicide and neglect is a small and stable cause of infant deaths in Tulsa County. From 1988-1990, homicide or neglect accounted for 1% of causes of infant deaths in Tulsa County; from 1991-1993, homicide or neglect was not reported as a cause of infant deaths. In 1994, homicide or neglect accounted for 1% of causes of infant deaths in Tulsa County; in 1995 and 1996-1998, homicide or neglect was not reported as a cause of infant deaths (OSDH, MCH Planning and Evaluation Section data). While during the reporting period, 1988-1995, there were only 2 deaths from child abuse/neglect, these accounted for 7% of the 30 reported for all of Oklahoma compared to the 2 cited from 1999-2001 which represented 5.2% of all Oklahoma child abuse deaths for that period. No deaths were reported in 2002. (OSDH, Office of Child Abuse Prevention, 1988-2002).
Accidents are a small and stable cause of infant deaths in Tulsa County. From 1988-1990, accidents (drowning, falls, fire, suffocation) accounted for 2% of causes of infant deaths; from 1991-1993, accidents (drowning, falls, fire, suffocation, and unspecified) (drowning, falls, unspecified) accounted for 3% of causes of infant deaths in Tulsa County; in 1995, accidents were not reported as a cause of infant deaths. For 1996-1998, no deaths were reported by accidents; in 1999-2001, there were 3 and for 2002 0. (OSDH, MCH Planning and Evaluation Section, 1988-2002).
Other communicable diseases are a large and growing cause of infant deaths in Tulsa County. From 1988-1990, infections (chorioamnionitis, infectious and parasitic disease, necrotizing enterocolitis, respiratory infections, and other perinatal infections) accounted for 10% of causes of infant deaths. From 1991-1993, infections (chorioamnionitis, common cold, infectious and parasitic disease, maternal infections, meningitis, necrotizing enterocolitis, respiratory infections, and other perinatal infections) accounted for 12% of causes of infant deaths. In 1994, infections (infectious and parasitic disease, necrotizing enterocolitis, respiratory infections, and other perinatal infections) accounted for 10% of causes of infant deaths in Tulsa County. In 1995, infections (chorioamnionitis, common cold, respiratory infections, and other perinatal infections) accounted for 13% of causes of infant deaths. For 1996-1998, communicable diseases
25

Tulsa Healthy Start Initiative 2001-2005
accounted for 2% of infant deaths and 0% from 1999-2002. (OSDH, MCH Planning and Evaluation Section 1988-2002).
Other prevalent factors are a large and growing cause of infant deaths in Tulsa County. From 1988-1990, other perinatal conditions and other/unknown causes accounted for 22% of causes of infant deaths; from 1991-1993, they accounted for 23% of causes of infant deaths. In 1994, other perinatal conditions and other/unknown causes accounted for 36% of causes of infant deaths in Tulsa County; in 1995, they accounted for 32% of causes of infant deaths. For 1996-1998, 51% had other perinatal conditions or ill-defined health conditions reported for infant deaths; in 1999-2001 , 55% were reported and in 2002, 56%. (OSDH, MCH Planning and Evaluation Section, 1988-2002).
The Tulsa Fetal Infant Mortality Review (TFIMR) began in l999 through Title V and Tulsa Healthy Start collaboration. The TFIMR is the only operational FIMR in Oklahoma. The case review team has generated one complete year of reviews and the community action team began in January 2001. The results of the review indicate three areas of significance, women’s health, prenatal care and grieving. The community action team has focused on preconceptional and interconceptional women health, prenatal care access and grieving services for the Tulsa community.
Mortality data analyzed using the Perinatal Periods of Risk (PPOR) by Brian McCarthy of the Centers for Disease Control and the World Health Organization for the 1995-1997 3-year average reveals that the maternal risk factors is 4.3, maternal care system 3.3, neonatal risk factors 1.7, and post neonatal risk factors as 2.7. The implications of analysis are that preconception health plays a significant factor in the infant mortality rate of Tulsa County. PPOR was again analyzed in 2004 finding that that the maternal risk factors is 2.7, maternal care system 2.1, neonatal risk factors 1.5, and post neonatal risk factors as 1.8 for the 361 feto-infant deaths of the 44,365 fetal deaths and live births from 1996-2000 (THD, TFIMR, 2004). The infant mortality rates by race for this period was 6.54 for White, 11.75 for Black, 7.63 for Native Americans, 16.26 for the Hispanic Ethnicity and 7.24 Other.
Table 14 Feto-Infant Death Rates by Race 1996-2000 Using the Perinatal Periods of Risk
Maternal Health% No
Maternal Care % No
Neonatal Risk % No
Post-Neonatal % No
White-Non Hisp. 2.31 70 1.29 30 1.52 46 1.42 43Black 4.02 26 2.63 17 2.16 14 2.94 19Native American 2.18 6 1.82 5 1.09 3 2.54 7Hispanic 4.65 16 9.0 31 0.87 3 1.74 6Other - 0 3.62 3 2.41 2 1.21 1
Immunization rate data (ages 0-2) aggregated by the census tracts in the project area are not available. For Tulsa County the immunization rate was 76% for 1996, 74% for 1998 and 73% in 2000. The immunization rate is reported by OSDH from the immunization database. The information is collected from entries made by physicians and clinics that subscribe to the state immunization program. Physicians and clinics not
26
Tulsa Healthy Start Initiative 2001-2005
apart of the system are not included in the rate. As a result, the percentage may be lower than actual immunization rates. The 2001-2002 immunization rates may reflect decreased access to immunizations due to lack of MMR and H Influenza vaccine during a shortage period 2001 (70%) and 2002 (65.4%).
Cultural SensitivityThe preparation and implementation of the THS Initiative has been conducted with program
and community participants who are representative of the general population and target population of this grant. The Native American population is a substantial population in Tulsa County. Over 164 tribes are represented in northeast Oklahoma. All Native Americans are fully assimilated into the general population and are not restricted to tribal reservations or tribal health care. Indian Health Care Resource Center is a contractor for case management services for Native Americans who prefer bi-cultural care. The Hispanic population is the fastest growing population in Tulsa County and 73% of the non-English speaking population is of Mexican descent. Hispanic (bi-lingual and bi-cultural) case managers, outreach workers, health educators and telephone specialists are employed as personnel and on contract to THS.
Current Perinatal Health Care Delivery SystemThe public perinatal system in Tulsa County is focused on serving low-income women,
teens, and racial minorities. Since 1989, it has used voluntary free pregnancy testing and a centralized appointment system to effectively reach its targeted populations. Limited case finding and outreach to selected areas and through individual clinics, linked closely to the appointment setting process, was added in l993 through the Metropolitan Tulsa Urban League, Save Our Babies Program.
The American Red Cross’s Free Pregnancy Testing (FPT) program started in 1988 on a pilot basis at five public clinic sites to facilitate access to perinatal services among high risk women. The concept was spearheaded and funded initially by the Metropolitan Tulsa Chamber of Commerce’s Indigent Health Foundation and organized by the Family Health Coalition (FHC). From 1990 to 2002, the Tulsa Area United Way funded it through the Margaret Hudson Program (MHP). In 2002, MHP has conducted the FPT for teens and Planned Parenthood of Arkansas and Eastern Oklahoma (PPAEO) has conducted the adult FPT program. Currently, the program tests over 500 women monthly, including many teens, referring the 42.7% who are pregnant directly to clinics or the large majority to Babyline.
Babyline is the Tulsa area’s centralized source to call for information and referral and prenatal care appointments. Babyline’s typical client is young, single, unemployed, and uninsured. In 2004, Babyline scheduled 43% of initial prenatal appointments for resident births in Tulsa County, 65.5% of those for minorities, and 26.5% of those for teens. From 2004 data, 76.4% of callers to Babyline were uninsured. (Babyline Annual Data 2004)
Babyline also provides an array of useful information for both service and policy planning. Babyline’s service statistics indicate important shifts in client needs and service responses. One of the most critical shifts is the increase in calls from Hispanic women. In 2004, 26.6% of Babyline appointments were for Hispanic women, compared to 3% in 1990 and 14% in l996.
Women calling Babyline during the first trimester for 2004 were 75.2% which is up from 58% in 2003%, 71% of callers in 1996, and 57% at its inception in 1990. The growth in the
27

Tulsa Healthy Start Initiative 2001-2005
Hispanic population who more frequently enter prenatal care in the second trimester or later have caused a progressive lowering of the total percentage who access prenatal care in the first trimester. THS 1997-2001 project area specific indicates that 49.4% women enter prenatal care in the first trimester compared to non-Healthy start areas of 56.1%. These developments have prompted a focus on strategies to adjust the system’s response to changes in populations, location, living patterns, health behavior, methods of funding, and access to care due to Medicaid managed care, and opportunities to improve linkages with employment, family support, health care, and other critical assistance for women, their children, and their male partners.
In 1995, Planline, a new service provided in conjunction with Babyline, was initiated to set family planning appointments. Over 900 clients (1,300 in 2003) were assisted with appointments during 2004 working with two major provider clinic providing sliding scale or Title X family planning services. Information collected through Planline is used to help guide development of the overall perinatal system. In the fall of 1996, the Strategic Planning Committee of the Family Health Coalition conducted an assessment to determine the capacity of the public perinatal clinics to assist the Coalition’s overall planning activities in relation to changes associated with Medicaid managed care. The findings indicate the ability to pay is a huge barrier to care. SoonerCare does not extend beyond the 8 week postpartum period. Women who qualify and remain with TANF can continue family planning through SoonerCare. The vast majority of women do not have access to family planning services. With these findings, the Coalition has advocated for a “Family Planning Waiver” to pay for family planning for men and women whose family income do not exceed 185% of the FPL. The waiver was approved in November 2004 by Centers for Medicare and Medicaid (CMS) and was implemented in April 2005.
According to the Oklahoma State Medical Association (OSMA) Directory of Physicians and the Annual Directory of the Journal of the Oklahoma Osteopathic Association, there are 1,093 medical doctors and 255 osteopathic medicine doctors in the City of Tulsa, 5 of who have a specialty in the Neonatal/Perinatal Medicine. Of total physicians in Tulsa, 272 are listed as Primary Care Case Managers (PCCM) with the SoonerCare program and serve Medicaid Managed Care Clients. Primary care providers include: 110 Board certified Family Practice physicians and 45 Board certified Pediatricians. In addition, 62 Board certified Obstetrician-Gynecologists provide care in Tulsa County.
Data represent PCP’s throughout Tulsa. Most PCPs are located near local hospitals or in public clinics of the traditional providers of indigent care. In addition, PCPs see all clients, including the elderly or other populations that would not be considered when assessing the Maternal and Child Health target population. In the Tulsa area, average monthly enrollment in SoonerCare over the past 10 months has been 34,000. PCPs who are located at the traditional provider clinics of the University of Oklahoma College of Medicine at Tulsa (OU), Oklahoma State University College of Medicine (OSU), the Tulsa Health Department (THD), Planned Parenthood of Arkansas and Eastern Oklahoma (PPAEO), Morton Comprehensive Health Services (Morton), the Indian Health Care Resource Center (IHCRC), and the Margaret Hudson Program (MHP) are listed independently in the directories. There are no listings for the clinics.
28

Tulsa Healthy Start Initiative 2001-2005
211th St.
186th St. N.
181st St.
21st St.
46th St. N.
116th St. N.
Yal
e
Admiral Pl.
61st St.
101st St.
81s
t W. A
ve.
Utic
a
145
th E
. Ave
.
N
EW
S
Har
vard
** * **
**
****** **
Prepared by the Family Health Coalition (12/04).
OSU Houston Park
PPAEO - 51st & S. Union
OSU Family Medicine
Xavier Medical Clinic
PPAEO - 5780 S. Peoria
Morton
Morton East Satellite
OU - 28th & Sheridan
IHCRC
PPAEO - 10th & Peoria
TCCHD - 3rd & Utica
OU - 21st & Mingo
TCCHD - 51st & 129th
Day Center for Homeless
Morton Homeless
Tulsa County Safety Net Providers
According to the OHCA, a primary care provider may have no more than 2,500 clients on their caseload at any given time. Three studies have been conducted in Tulsa County by Community HealthNet (a non-profit corporation of safety-net providers). The first study looked at access of non-urgent care in Tulsa emergency rooms. The second was an intensive study of 1,000 emergency room (ER) goers in 5 hospitals regarding why they had chosen the emergency room for their care. A majority indicated they had contacted their physician prior to coming to the ER and either had been sent or chose to come to the ER because they could not get to their office in a timely fashion. The final study conducted by the University of Oklahoma College of Public Health examined the attitudes and behaviors of practices regarding Medicaid and uninsured populations. The pilot results revealed that most practices restrict the number of Medicaid and uninsured in their practice, and restrict the number of visits by both in any given week (Ehrlich, 2004). The intent is to reduce loss of income.
Covering Kids, a Robert Wood Johnson Foundation project, has focused on enrolling eligible children in SoonerCare. Covering Kids and the concurrent growth in the Department of Human Services enrollment outreach has increased the enrollment from 28% (November 1997) of the potential eligible children to 44% (September 2003) potential eligible children in Tulsa County. Despite this growth, women and children are accessing and utilizing SoonerCare at a low rate.
There have been a number of physicians who are reducing the percentage of their practice to SoonerCare eligible women and children. Most private practices do not exceed 6% of their total
29

Tulsa Healthy Start Initiative 2001-2005
practice for SoonerCare. The American Academy of Pediatrics cited in their Pediatrician Participation in Medicaid and SCHIP (2000) that Oklahoma is number one in the nation in physicians unwilling to participate in the program. The primary reason is poor reimbursement and paperwork. The Physicians Advocating To Children’s Health (PATCH) effort originating in Tulsa to address the poor reimbursement and inadequate number of specialty providers for women and children was successful in passing HB 2019 (May 2000) which increased funding for reimbursements overall by 18%. This effort fell short of the goal to index Medicaid services to Medicare rates for similar services. The reimbursement was distributed after rate hearings in a fashion which improved reimbursement to targeted ICD-9 codes and CPT codes. The physicians in the SoonerCare Plus market (urban MSAs of Tulsa, Oklahoma City and Lawton) which are fully capitated models have not benefited from this increase because rates are negotiated contractually and not as a fee for service reimbursement. As a result, there has been no improvement in the availability of providers. A lawsuit followed and challenged the Oklahoma Health Care Authorities’ delivery of health services to the indigent population of our state. After prolonged pressure and loss of participation of health maintenance organizations in the urban markets, the SoonerCare Plus system was discontinued on December 31, 2003 and SoonerCare Choice (primary care case management) model which had been offered in the rural areas was instituted in April 2004 in Tulsa County. The closure of SoonerCare Plus has resulted in more physicians participating in the Medicaid program. The lawsuit was successful in February 2005 with a judgement made to the physicians that the OHCA must pay fair market prices for the services. As a result, Medicaid reimbursement is indexed to Medicare rates.
The community response to lack of access for children has been the creation of Kidsline to identify first available appointments for children through a centralized telephone referral system and the creation of an on-going advocacy forum of the Coalition, the Preventive Health Task Force. The Task Force has successfully called for a greater state legislative oversight of the OHCA, indexing of provider rates to the Medicare rates and accountability of the health maintenance organization in accounting for their "ghost slots" of care.
Oklahoma State Department of Health identifies for deliveries by attendant and birth setting as follows for 2000. (Note that in the table "Other" may be an emergency medical technician, physician assistant, police, relative, and so on).
Table 17 Deliveries by Attendant and Birth Setting in 2000Birth Setting MD DO CN
MidwifeMidwife Other Unk Total
Hospital 6,873 1,148 127 2 4 0 8,154Birthing Center
0 0 0 1 0 0 1
Residence 3 1 4 29 4 0 41Other 4 2 5 1 7 0 19Unknown 0 0 0 0 0 0 0Total 6,880 1,151 136 33 15 0 8,215
Five hospitals or medical centers in Tulsa provided maternal child health services in 2000. No hospitals are at capacity. Tulsa Regional Medical Center has 462 beds, 19.5% Medicaid admissions; Hillcrest Medical Center has 446 beds, 19.2% Medicaid admissions; St. Francis
30

Tulsa Healthy Start Initiative 2001-2005
Hospital has 591 beds, 8.8% Medicaid admissions; and St. Johns Medical Center has 587 beds, 11.2% SouthCrest Hospital is a new addition in 1999 and its Medicaid admission rate is reported at 4%. The Hillcrest HealthCare System which has 14 hospitals in its system closed two hospitals in Tulsa during 2000, Doctor’s Hospital and Children’s Medical Center. They sold their interest in the SouthCrest venture to a Texas-based firm. Hillcrest HealthCare System is petitioned the legislature to provide a “charity” designation to the facility. This designation provided a formula reimbursement system (2.7 times) the regular reimbursement system. The $24 million annual cost allowed Tulsa Regional Medical Center to remain open and provide Tulsa parity with Oklahoma City who has the only other charity system in the state. Hillcrest Health Care System succumbed to hard economic times in July 2004 and was purchased by Ardent Inc.
One in three adults (19-64 years of age) are uninsured in Tulsa County (OHCA, 2004). The challenge of not having an indigent care facility in Tulsa has not been fully appreciated by the Oklahoma legislature and the OHCA. Graduate medical education of the University of Oklahoma Health Science Center and the Oklahoma State University College of Osteopathic Medicine are primarily located at Hillcrest Medical Center and Tulsa Regional Medical Center, respectively. No Tulsa hospital qualifies for Disproportionate Share for Medicaid and as a result each hospital sustains critical losses in delivery of services to the uninsured.
All hospitals provide delivery and emergency services for the uninsured; however, clients are billed for services rendered. St. Francis Hospital hosts the Eastern Oklahoma Perinatal Center which has 45 beds and remains at capacity. St. Johns Medical Center, Hillcrest Medical Center, and Tulsa Regional Medical Center each have neonatal intensive care units which serve their hospital and referrals from outlying affiliated hospitals. Hillcrest Medical Center hosts the Tulsa Center for Infertility and Women’s Health which conducts in vitro fertilization. The genetics counseling and testing program which served the Eastern half of the state was closed in July 2004 due to lack of funding leaving only Oklahoma City available for services to the state.
Within the project area and Tulsa County, the 7 agencies associated with the FHC are the primary means the uninsured access prenatal, family planning and pediatric services. Only THD, receive Title V Maternal Child Health and Title X funds contracted through the OSDH. The Title V and Title X funds have reduced by an annual $310,000 MCHB losses and state revenue deficits (2002-2004) were realized. Six clinics (OU, OSU, THD, Morton, PPAEO and IHCRC) provide services to the Medicaid clients through contracts as “safety-net providers” through SoonerCare. One clinic (MHP) provides niche services for family planning and wrap-around services to pregnant and parenting teens which are eluded to in the SoonerCare plan but criteria and a reimbursement system have not been established by OHCA to pay for these services. One clinic (Morton) is a federally qualified health center (FQHC). One clinic (IHCRC) is an urban Indian Health Service site. Most American Indians go to Claremore Indian Hospital in Rogers County or to W. W. Hastings Indian Hospital in Cherokee County for delivery services. No clinic is at capacity for low-risk obstetric services, however, high risk service capacity has reached maximum for the OU and OSU clinics.
Figure 2 Service Access Pattern of the Tulsa Perinatal System
31

Tulsa Healthy Start Initiative 2001-2005
Under the auspices of the Family Health Coalition (FHC), there are strong, ongoing linkages among different core services of the system. A free pregnancy testing program, centralized referral and appointment process, clinic services, and outreach are closely coordinated through the FHC’s Access Committee. During the emergence of Medicaid managed care (1996-2004), the Coalition worked closely with the new HMOs to assist in assuring both effective access and quality services to Medicaid clients. As the program deteriorated, FHC facilitated provider training and client information for enrollment in SoonerCare Choice (2004). Tulsa’s FHC provided leadership to form the Oklahoma Perinatal Coalition (OPC). The OPC has worked with the OHCA and OSDH to shape policies that better support an effective perinatal care program.
The FHC also is working closely with three professional (master of social worker, bachelor of counseling and/or registered nurse) case management programs. The Tulsa Alliance for Families Initiative is a collaborative effort among more than 60 organizations, including the Tulsa Health Department. The Alliance’s program partners are using federal funds from the Family Support and Preservation Act to establish decentralized support services in local neighborhoods (target zip code of 74127). Children First is a prenatal case management program based on the David Olds’ model. This OSDH project is statewide and administered through the county health departments. The model is most successful in reduction of child abuse. The OSDH Office of Child Abuse Prevention administers the Child Abuse Prevention grant fund which supports the Healthy Families Oklahoma project at the Parent-Child Center of Tulsa. The target population is families at high risk of child abuse. Tulsa Healthy Start, Tulsa Alliance for Families, Children First and Healthy Families Oklahoma jointly conduct triage of Babyline calls (semi-monthly) to prevent duplication of services and maximize program benefits. The range is 8.5 to 11% of the resident births annually have an opportunity to participate in any of these programs. Children First is the only case management program outside the physician’s care that has been allowed to bill OHCA for medical case management services. The OHCA has taken a limiting position on approval of case management for social health issues (i.e.,alcohol, illicit drugs, domestic violence).
The FHC sponsors and promotes the Community Health Action Team (CHAT) group. This sponsored group represents 75 outreach workers from numerous organizations. Networking and cross training have enabled outreach workers to collaborate in service delivery. Three major
32

Tulsa Healthy Start Initiative 2001-2005
outreach efforts have been developed through the FHC, Save Our Babies, Tulsa Healthy Start and Raising Educational Awareness for Community Health (REACH outreach). Common to all three programs is the focus on target communities, paraprofessional indigenous outreach workers and a focus on perinatal issues. A total of 5.0 FTEs conduct canvassing, follow-up on Free Pregnancy Testing results, follow-up on Babyline/Planline/Kidsline missed appointments and community surveillance. An estimated 3,600 canvass contacts are made per year.
In 1991, the FHC received a grant from the Kellogg Foundation to initiate the Save Our Babies Outreach Project (SOBOP), a community education and outreach program focused on six census tracts in north Tulsa. Its purpose was to engage a smaller community’s attention and involvement in achieving more positive birth outcomes. The program was fully operational under the auspices of the Metropolitan Tulsa Urban League in 1992. It featured extensive case finding and follow-up to assure access to care, as well as comprehensive health education. An advisory council of persons guided all activities primarily from the target community. Since its inception, referrals to Babyline from the area have increased significantly; infant mortality rates have decreased dramatically. After the end of Kellogg funding, the program has continued with reduced staff with funding from varied sources, including Community Development Block Grant funds and the OSDH. Implementing an enhanced version of the SOBOP concept became the focus of the initial THS outreach model and has been critical to improving health behavior and positive birth outcomes for a growing, mobile, target population migrating to housing and other opportunities throughout Tulsa.
REACH Outreach was a consolidation of outreach efforts from the Margaret Hudson Program, Planned Parenthood of Arkansas and Eastern Oklahoma and Save Our Babies. The OSDH consolidated funding and program administration at the Tulsa Health Department in l998. The REACH workers coordinate canvassing with the THS outreach workers and focus on target zip codes.
In addition to these linkages, the FHC works closely with Tulsa’s Community HealthNet (HealthNet) consortium, a group of Tulsa’s nonprofit “traditional/safety-net” community service providers formed in 1995 in response to the pending conversion of Oklahoma’s Medicaid program to managed care (SoonerCare). The eight member organizations of Community HealthNet work together to coordinate the delivery of primary health care and family planning and maternity care to Tulsa’s Medicaid, Medicare, medically indigent, and medically underserved populations.
All HealthNet clinics offer sliding fee adjusted rates for health services to persons without health insurance. Family planning and prenatal care are provided by all HealthNet clinics and all HealthNet clinics provide presumptive eligibility enrollment services for Medicaid Title XIX prenatal and postpartum care. All Community HealthNet members are also members of the FHC.
The HealthNet members include Tulsa Health Department, Morton Comprehensive Health Services (a PHS §330 federally qualified health center), Indian Health Care Resource Center (an Indian Health Services urban Indian health center and FQHC), the University of Oklahoma Health Sciences Center, Oklahoma State University College of Osteopathic Medicine, Planned Parenthood of Arkansas and Eastern Oklahoma, the Margaret Hudson Program (an alternative education and health care program for pregnant teens), and the Babyline/Planline/Kidsline
33

Tulsa Healthy Start Initiative 2001-2005
prenatal, family planning, child health appointment system within the Community Service Council’s Helpline system. The Babyline centralized telephone system makes prenatal and family planning appointments for the Community HealthNet clinics and has the potential to expand and provide other telephone-based client services.
One initial activity of Community HealthNet was to explore opportunities to work together and evaluate new organizational vehicles that might offer a greater competitive advantage when contracting with the SoonerCare Health Maintenance Organizations (HMOs). All of the Community HealthNet clinical providers are currently participating in the SoonerCare program and are vitally interested in continuing to serve the Medicaid population. The FHC’s Babyline and Planline program is HealthNet’s only non-clinical provider, yet it provides a key functional service to the HealthNet clinics though its centralized telephone appointment system (HealthLink). Babyline and Planline provide client follow-up to the Margaret Hudson Program free pregnancy testing program and make prenatal and family planning appointments for a large portion of clients at the HealthNet clinics.
Community HealthNet promotes collaboration among its member organizations to enhance the ability of each to deliver quality health care efficiently with special emphasis on primary care, disease prevention, health promotion, and family planning. The members have a common interest in working closely with each other to coordinate referrals, provide convenient access to health care, and reduce inappropriate utilization of specialist and hospital providers for both the insured and uninsured populations. Numerous ancillary services are provided by many of the HealthNet members, including lab, X-ray, pharmacy, WIC, and patient transportation. The two medical school members of Community HealthNet have established ties to all four of Tulsa’s major hospitals and have special, strategic linkages to the hospitals and their PHO organizations.
Of particular concern to Community HealthNet members is the large uninsured population which the clinics collectively serve. Oklahoma receives very little FQHC or PHS §330 support. In order to more efficiently and cost effectively serve Tulsa’s Medicaid and uninsured client population, the Community HealthNet was successful in achieving a Healthy Communities Access Program (HCAP) grant to improve community infrastructure. Two major needs assessments, expansion of the centralized appointment system to include adults and establishment of the Internet based case management system (CareLink) have been conducted through 3 years of the grant cycle. Three school based clinics, expansion of the community health center’s access point and an application for an additional community health center has been accomplished in 2004.
Community HealthNet member organizations have collaborated with the FHC to implement a comprehensive WIC social marketing campaign (1997), Smoking Cessation campaign (1999), Back to Sleep campaign (2001), Ask Me! (2002), Healthy You, Healthy Baby (2003-04). Collectively, 3 Health Summits, 2 Weeks of the Uninsured and 3 regional conferences.
Major gaps in the local perinatal health care system utilized by the target population relate to needed improvements in engaging its members in care at a time of a rapidly changing health care environment. Dramatic expansion needs to occur to improve health behavior, including an increased awareness and knowledge of how to access needed services given the changes in funding and service delivery approaches. Local experience indicates that increased consumer knowledge, awareness, and support can improve birth outcomes. Other more specific gaps in the
34

Tulsa Healthy Start Initiative 2001-2005
local system also include: (1) a lack of “enhanced care services” such as case management, nutrition, health education and outreach as an integral part of the SoonerCare system, (2) a lack of a mechanism to pay for prenatal and delivery services for uninsured women primarily Hispanic women, (3) a lack of a mechanism to pay for family planning for men and women, particularly tubal ligations and vasectomies, (4) limited dental services for uninsured women of childbearing age or their children, (5) a lack of PCP education on the SoonerCare system and the gate keeping (case management) activities of that role including referral for wrap-around services or family planning outside of the provider network and (6) a lack of specialty providers in the SoonerCare system for behavioral health and other specialties.
Tulsa Fetal Infant Mortality Review (TFIMR) was developed with Tulsa Healthy Start funding in l998. In 1999-2003, the OSDH wholly funded the project for Tulsa County. It is jointly funded by OSDH, THD and THS in 2004. This is the only active FIMR process in the state. A child death review process exists to determine criminality of children’s deaths age 2 through 18 years of age but the infant years are not included. The TFIMR examines the etiology and co-factors relating to fetal deaths after 28 weeks and before the infant’s first birth date. This is not a criminal review. The Tulsa Health Department administers TFIMR and members of the FHC are represented on the case review team and the community action team. A 10 Year Analysis of Linked Birth and Death Certificates 1991-2000, an analysis of fetal and infant deaths 1996-2000 using the Pregnancy Periods of Risk (PPOR) and the analysis of THS case management data has documented several interesting features. Trimester of entry into care, and adequacy of care (Kotelchuck or OSDH scale) do not correlate with poor birth outcomes. The implication is that quality of care is more essential to produce outcomes. The PPOR results indicate that white, Native American, and black are more like to have negative outcomes related to women’s health factors, while Hispanic women are more likely to have fetal death related to maternal care. There is no maternal death review board. One maternal death in the index years 1999-2001 was recorded and this was homicide.
II. Project Implementation The implementation of THS has been dynamic over the eight years of funding with changing expectation from the federal government and changing needs of the community. In 1997, THS proposed five of nine model services, Consortia, Case Management and Care Coordination, Outreach and Client Recruitment, Facilitating Services, and Health Education and Training. With the second cycle of funding, facilitation of services (transportation and translation) was absorbed in case management and outreach services respectively. As a result, Five Healthy Start Core Services were identified: Outreach and Client Recruitment, Case Management, Health Education and Training, Interconceptional Care and Depression Screening and Referral. These are accomplished through the processes of the Local Health System Action Plan, Consortium, Collaboration and Coordination with State Tivel V and Other Agencies and Sustainability.
The core services flow chart is depicted in Figure 3. This represents the core efforts of outreach, case management, health education, depression screening and referral and intraconceptional care. Details of each program are included in the Sections regarding each area.
35

Tulsa Healthy Start Initiative 2001-2005
/
Clinic/Case Manager Intake
Client Consent
Individual Plan of Care Based on Key Risk Factors: 1) Domestic violence 2) Substance abuse 3) Smoking 4) HIV/AIDS/STI 5) Depression 6) Nutrition 7) Prior pregnancy history
Weighted Assessment
Moderate Risk Outreach
Community Case
Management
Medium & High Risk Clinic Case
Management
Health Education For Prenatal and Parenting
Women
Community & Clinic Referrals: 1) High risk medical care 2) Substance abuse treatment 3) Domestic violence 4) Housing assistance 5) HIV/AIDS care 6) Save Our Babies outreach 7) Margaret Hudson Program 8) Govt. & CSC “Blue Book” social &
human service agencies 9) Tulsa Alliance for Families outreach 10) WIC and breastfeeding education 11) General Prenatal education 12) Baby skills and new parent class 13) Genetic testing 14) Pregnancy termination 15) Adoption 16) Translation 17) Transportation
Figure 3 Tulsa Healthy Start Core Services Flow Chart
Interconceptional Care for Women and their Infants
for 2 years
Free Pregnancy Testing
Self Referral Outreach
Canvassing Referral
BABYLINE
A. Outreach and Client RecruitmentOutreach is defined as the case finding and recruitment and community case management of
difficult to reach clients within Tulsa County. Outreach goals are to identify women in need of preventive care services (family planning), connecting women to early prenatal care as soon as possible, and delivering health messages to ensure healthy birth outcomes and prolonged interconceptional periods. The methods include door-to-door canvassing, home visit referrals from a communitywide centralized appointment line (Babyline), phone contact and the distribution of health education and parenting information. Outreach is part of the team effort to monitor and follow clients at low/moderate risk during pregnancy and during the interconceptional period.
Community Decision to Select This Approach. THS defined outreach approach was conceived as an outgrowth of successful programs in the Tulsa community including Babyline and Save Our Babies Outreach program (both described in detail in Section One). THS provided an opportunity to coordinate the efforts of existing program, and expand existing programs through the CHAT group of the Family Health Coalition.
Identify the Components. The Outreach Core Service includes 5.5 FTE on indigenous case workers and 1.5 FTE Babyline telephone referral specialists as described below. Supervision is conducted by the sub-contracting agencies and Kathy Kleine-Crabtree, MSW, the Outreach supervisor for THS.
The REACH outreach workers complement the number of outreach workers focusing on outreach efforts in the target communities. From 1997-2000, the target community was 37 census tracts. When it was clear limiting services to 37 census tracts was impossible because of the high mobility of most populations, the target was expanded to all of Tulsa County, with a weighted risk assessment tool providing greater weight in the risk analysis to target populations
36

Tulsa Healthy Start Initiative 2001-2005
and geographic locations (zip codes). This has served the project well from 2001 to 2004 as it has reduced the number of lost clients due to mobility or geographic limitations.
Table 18 THS Outreach Employees, Subcontractors, Caseload and Bilingual Status Title Location Caseload Bilingual2.0 FTE Outreach worker THD-employee 1:25 1.0 FTE1.0 FTE Outreach worker PPAEO-contract 1:25 1.0 FTE2.0 FTE Outreach worker MTUL 1:250.5 FTE Outreach worker Morton 1:123.0 FTE REACH outreach THD-employee
inkindNA 1.0 FTE
1.5 FTE Babyline telephone specialist CSC-contract NA 0.5 FTE1.5 FTE Babyline telephone specialist CSC-funded by
TAUWNA 0.5 FTE
Community case management is conducted by THS outreach workers for low and moderate risk program participants at a 1:25 case load (60% of scope of work). The initial assessment is conducted by THS clinic case managers, the plan of care is developed jointly with the program participant and case manager, staffings are conducted to review the progress as a team and data entry is maintained by the outreach worker. Services include: home visits for case management, information, referral and follow-up on prenatal, interconceptional and children’s care, prevention education (i.e., parenting education, risk reduction education) from the prenatal period through the first two years after birth scheduled every two months, documentation and data base entries to monitor client’s progress, and translation for health care services for Hispanic women receiving case management. (Bi-lingual outreach workers).
Outreach workers (employees and contractors) conduct follow-up of missed visits through telephone, mail and direct contact for Babyline and Free Pregnancy Testing (community participants) and community case managed clients in their caseload (program participants). Not all clients seen by the outreach workers from the Free Pregnancy Testing or Babyline become THS case managed clients due to limited capacity. Barriers are assessed at initial and follow-up visits. Barriers for the prenatal are usually transportation, insurability for health care and translation services. Of clients that do become case managed clients, transportation services for the uninsured through bus tokens and cab services are provided. Clients who are Medicaid enrolled received transportation through SoonerCare and THS case managers coordinate that service. Translation services for women of Hispanic Origin both uninsured and Medicaid eligible are provided through THS outreach translators if the clinic, lab or radiology center does not offer the service.
Interconceptional care clients attrition is contributed to high mobility of the population, often without leaving forwarding address or telephone number. This attrition can be contributed to by substance use and drug trafficking from the home, and domestic violence in which the families do not wish to have “strangers” in their home. Retention potential is being augmented by the transition of the Healthy Start database to an Internet based case management software called Service Point. The Internet based case management is the result of a community-wide effort which includes THS to create an access point for health and social services agencies for services rendered and follow-up conducted. Telephone and addresses can be updated as program
37

Tulsa Healthy Start Initiative 2001-2005
participants access health and social services in the community. These universal records will allow THS to locate program participants who have moved but are still in the service area.
Attrition of program participants in Calendar Year 2003 was during pregnancy 12.16% (68), year one post partum was 11.45% (64), attrition during year two post partum was 9.66% (54), and 2 years after birth 16.64% (93) or a total of 279 of 559 clients (49.41%) leave the project over a 2 years period of time. It is anticipate a similar attrition pattern in the future.
Facilitating or detracting events. THS outreach and client recruitment funding for outreach workers is federal funding only. The federal funding has not expanded during this cycle, however, we have had excellent retention of outreach staff. Stagnant funding in the face of increased costs for supplies, gas and personnel costs has reduced the number of staff available for outreach services.
Three outreach workers with the REACH outreach program funded by the Oklahoma State Department of Health collaborate with THS outreach workers and are supervised by the same supervisor, Kathy Kleine-Crabtree. Babyline’s 1.5 FTE staff paid for through THS funding are complemented by 1.0 FTE staff funded through a Healthy Community Access Project (DHHS, HRSA, Healthy Communities Access) grant specifically for adult services, and 0.5 FTE from the Tulsa Area United Way for the conduct of children’s services. All funding has been tenuous. The state revenues have been lower than anticipated from 2002 to 2004 because of decreased oil prices with the first recovery seen in 2005. State agencies were reduced in funding from 12% to 18%. REACH matches state funds with county levy funds. When the county levy funds were decreased the impact was a loss of REACH outreach workers to begin in 2005. TAUW funding was reduced by 12% in 2004 and 2005 with the impact of a loss of Babyline staff by 0.5 FTE in 2004.
B. Case Management and Care CoordinationCare coordination/case management is referred to as “case management.” Case management
services are provided with the purpose of coordinating a highly specific, seamless continuum of care for Healthy Start case-managed program participants. This continuum of care is provided through client assessment, plan of care, referral, monitoring, facilitation and follow-up of needed services. Case management acuity and intensity of services are determined after a comprehensive weighted risk assessment. Through a team approach, an individualized plan of care is developed for the client. Monitoring and reassessment may change the risk acuity and precipitate a change in the plan of care. On-going team meetings with outreach and health education and training promote a smooth transition of services to meet the client needs.
Community decision to select this approach. FHC had identified case management as the most essential element in improving birth outcomes for women. Children First was identified (home visiting case management) as the strategy to reduce child abuse and neglect. Utilizing the David Olds’ Model, the case management was limited to first time mothers who start their prenatal care early in pregnancy. Although, this would be optimum; FHC members felt that infant mortality reduction could be well served by an interdisciplinary team with clinic based case management as a cornerstone.
The purpose of the case management is to coordinate the total care of pregnant and parenting women and their infants (0-2 years old) as an essential element of the THS. Case management
38

Tulsa Healthy Start Initiative 2001-2005
enrolls Healthy Start eligible families referred through Babyline to the clinics or internally referred by clinic staff. After informed consent, the voluntary enrollment is completed. Case management coordinates an agreed upon plan of care (signed by the client), specifically addressing the family’s individual needs. Case management facilitates interaction on behalf of their clients with medical service providers and community support services. The case manager documents assessments (including depression screening), interventions, referrals (and completions) and outcomes in a centralized THS chart and computerized database (ShareLink). This process measures the client’s progress toward their stated needs and goals.
The goal of case management is to make services and systems work by providing a broad scope of services including education, prevention and intervention. The education services provided by case managers include imparting information from the Healthy Start Resource Manual. The conceptual framework for the manual is based on client/family-centered services of health, nutrition, education, employment, housing and child care. Specific topics included in this manual include prenatal diet and exercise, delivery preparedness, newborn infant care and feeding, family planning alternatives, smoking cessation, budgeting and resume building.
Identify components of the intervention and resources. Services are conducted primarily
in the clinic setting. Home visiting is conducted on an as needed basis (client request, home assessment is necessary or unable to reach the client). Interconceptional care of program participants is coordinated by the case manager but if the risk level is low or moderate risk the client may be followed by an outreach worker in community-based or home-based services. It is estimated that 350 program participants are active in professional case management services at any given time, however, unduplicated count per year may be as high as 600 clients (attrition and new enrollment). The program participants seen by clinic case managers are high risk for infant mortality as determined by the weighted risk assessment scale.
Table 19 THS Case Management by Employee, Contractor, Caseload and Bilingual StatusTitle Location Caseload Bilingual3.0 FTE Case managers THD-employee 1:35 1.0 FTE2.0 FTE Case managers PPAEO-contractor 1:35 1.0 FTE2.0 FTE Case managers MHP-contractor 1:352.0 FTE Case managers PCCT-contractor 1:351.0 FTE Case managers IHCRC 1:35
The minimum education requirement for a case manager is a bachelor level in a social service field or registered nurse. The bachelor level case managers are supplied with additional support from the case manager coordinator who is a master prepared, Colleen Ayres-Griffin. The majority of case managers, including those assigned in the high-risk clinics are master level prepared social service providers or registered nurses. All case managers receive direct supervision from their respective subcontracting agencies in addition to on-going education through the THS Training Institute. Supervision and service protocols for the case managers assure that each client benefits from consistent assessment, intervention and monitoring.
Once a referral has been received by a THS case manager from a referral source (Babyline, traditional clinic, word of mouth or a self referral), the case manager meets with the client and/or family in their home or in the clinic. The case manager begins to gather baseline demographic
39

Tulsa Healthy Start Initiative 2001-2005
data, conduct standardized risk measurements and create a plan of care. All THS clients are assessed using the Tulsa Healthy Start Initiative Family/Risk Assessment. The assessment process may include the Babyline intake, the Beck Post Partum Depression tool (to be introduced Spring 2004) or the Quick Screen (Chasnoff’s 4P-Plus). When the client’s risk level has been identified the client is placed into one of three levels of risk: high, moderate or low. After the case manager and client have completed a plan of care the case manager presents the case to the Healthy Start team members. These team members include THS outreach workers, health education/trainers and case managers. The clinic-based services implies that clients have care coordination services at each visit and as needed in person or by phone in the intermediary times. Prenatal clients may have 7 to 10 visits, post-partum clients may have 2 visits in the first 8 weeks and quarterly thereafter, pediatric contacts are usually made with the post -partum contacts until the client is discharged. The initial visit, 36 weeks, after delivery, within 8 weeks post partum and quarterly during the interconceptional period are required contacts with reassessment using the weighted assessment scale.
The THS client voluntarily participates in the program and consents to services including participation in their plan of care. The individualized plan of care is created with the client based on their risk assessment and espoused needs, signed and a copy provided to the client, is documented in the client’s THS chart (began 2004), is reviewed periodically with the client as needs change and is reviewed at THS team staff meetings.
Multidisciplinary teams are made up of outreach workers, case managers and health/education trainers depending on the race, ethnicity and prevalent risk factors of the clients seen at the clinics. Each core service includes bi-lingual Hispanic staff and Asian language translators by contract. These teams are located at 2 providers in the Tulsa community: Oklahoma State University College of Osteopathic Medicine (OSUCOM) and the University of Oklahoma Women’s Clinic (OU Women’s). Morton Comprehensive Health Services (Morton), THD, PPAEO, and Indian Health Care Resource Center (IHCRC) are interdependent on services offered through their agencies and full THS sponsored teams are divided by the two locations. All THS teams work in collaboration with medical providers including hospital and clinic nurses, attending physicians, residents, medical students and hospital social workers. The case management team utilizes consultation with specialty care providers including referrals for substance abuse treatment, HIV/AIDS testing and counseling, depression and domestic violence counseling and support. The case manager through the THS subcontracting agencies can access many of these services. THS case management teams located in the high-risk medical clinics, OSUCOM and OU Women’s have access to nutritional and diabetic counseling and support. All case management teams have access to the nutritional program Women, Infants and Children (WIC) on site. Case managers coordinate transportation through SoonerCare (Medicaid managed care) services as well as THS transportation funds. Both services have had to reduce transportation services due to reduced funding. Child care resources are accessed through linkages with subcontracting agencies (i.e. Rainbow Care Room, Margaret Hudson Program (MHP) daycare, Childcare Resource Center and First Start program). In addition, teams access SoonerStart for infants with special needs. Each THS case management team has weekly staff meetings to present new client intakes and to monitor the risk status of all existing clients.
Facilitating or detracting events. Client barriers can be characterized as system barriers and personal barriers. System barriers include lack of access to care for women who are on Medicaid or uninsured, lack of transportation services, providers who are not culturally sensitive
40

Tulsa Healthy Start Initiative 2001-2005
and lack of bi-lingual professional staff. A limited number of physicians will provide Medicaid services to pregnant women and children because of the low reimbursement for care. As a result, Medicaid provider access is limited and women must wait 3 to 4 weeks to access initial care. Undocumented women must pay on a sliding scale at 2 provider locations and full price at all others to receive care. This inhibits early entry into care and continuity of care becomes dependent upon their ability to pay. Transportation is difficult because bus transportation is limited requiring the more costly taxi transportation ($28 round trip). Emergency scheduling of Medicaid transportation is impossible and waits for transportation may be as long as 2 hours which can result in appointments being rescheduled because of late arrival at the provider. Mental health and domestic violence service access is limited to both Medicaid and uninsured clients because of limited providers accepting low-income clients.
Client barriers can be characterized as motivation to participate and unhealthy lifestyles. Many clients have had unhealthy lifestyles (substance use, poor nutrition, obesity, smoking, domestic violence and behavioral problems) for a life time. Pregnancy is an additional stress “heaped” upon their current stressful lives. Although popular belief that women become highly motivated to improve their health for their baby during pregnancy, 76% of women in THS view their baby has mistimed or unintended. This ambivalence about the pregnancy does not inspire health improvements. Secondly, health care is expensive, and intimidating. Many women do not identify health promotion and disease prevention as a high priority. As a result, they may delay or avoid health care until acute symptoms promote their access to health care.
All of the case management programs in Tulsa County are at capacity. Collectively, the case managers have a caseload representative of 8-11% of the total resident births in Tulsa County each year. If risk was measured by women at 100% of the FPL, 33% of Tulsa County’s women would qualify. The county IMR cannot show dramatic improvements without additional case management services for the county. However, stable funding by THS at $1.07M (2000-2004) and reduced funding by 18% of all state funded (2002-2004) case management programs has reduced the number of clients that can be seen.
C. Health Education and Training The Health Education and Training Model is the provision of instructional activities and
other strategies to increase awareness and knowledge of an individual, group and/or community to change individual health behaviors. The Training Institute provides instructional activities planned and implemented to improve the knowledge and skills of the professional and paraprofessional staff of the THS. Community awareness and understanding of health-related issues are essential for reducing infant mortality. The strategies of the Health Education and Training Model include individual and group prenatal and parenting education for women at moderate and high risk (as deemed by the case manager), community presentations, consumer advocacy groups, THS newsletter, the Learning Resource Center and the Training Institute.
Community decision to select this approach. The Tulsa Healthy Start Health Education and Training Model have a multi-tiered function which includes client, paraprofessional and professional education. The FHC determined that enhancement of all three areas using a cost effective cross-program approach was the best practice for Tulsa County. The purpose of the Health Education and Training Model is to enhance the quality of service delivery through education and training, increase client participation in THS services and activities and increase knowledge, change attitudes, and reduce negative behaviors of the target population.
41

Tulsa Healthy Start Initiative 2001-2005
Identify components of the intervention and resources. The Health Education and Training Model is conducted by 3.0 FTE employees from the THD. Renetta Harrison supervised the staff from 2002 to 2004 and was health educator as well. At Ms. Harrison’s leaving and with anticipated changes in the 2005-2008 cycle, Corrina Jackson, the Program Manager served in this role.
Healthy Start clients in the case management model are referred to group training located in
their community and clinic. The series of trainings were developed after the 1998 THS assessment of health education needs and consumer health information gathering patterns. Five hospitals and two community agencies provide prenatal and parenting education on a monthly basis targeted but not limited to their clients. THS refers clients to these programs and documents by self-report the program participants participation in the activities.
Table 20 Summary of Health Education and Training Content and Audience
Content AudiencePregnant Postpartum Adolescent Community
Healthy Start X X Conflict Resolution X X X XAbstinence and Contraceptive Education X X X XAnger Management X X X XHIV/AIDS/STDS X X X XSmoking and Health X X X XFetal Alcohol Syndrome X X X XParenting Education X X X XDating Violence XFatherhood X X X XSelf Esteem X X X XRelationships X X X XFamily Violence X X X XStress Management X X X XNutrition X X X XLife Plans X X X XHealthy Start Sexuality Education X X X Physical Activity/Exercise X X X XPrenatal Care X XCommunicable Disease X X X X
THS sponsors monthly prenatal and parenting education programs, in English and in Spanish are offered at the THD 5051 S. 129th St and 315 S. Utica locations. Specialty programs are offered at the participating clinics—PPAEO, Morton, IHCRC, OU and OSU. Smoking cessation programs are offered in conjunction with the MATCH (Centers for Disease Control funded) through the THD. Family violence intervention programs are one-on-one and sponsored with Domestic Violence Intervention Services (DVIS). Substance use prevention is included in the prenatal and parenting programs, however, one-to-one and group intervention is referred to IHCRC, Twelve and Twelve, the Women and Children’s Residential Treatment Center and Palmer Continuum of Care (formerly Palmer Drug Abuse Services). Referral and follow-up is documented on the ShareLink system. Depression awareness and prevention is offered through the prenatal and parenting programs. Depression intervention education is offered one-on-one
42

Tulsa Healthy Start Initiative 2001-2005
and in group in collaboration with Family and Children’s Services and the Mental Health Association of Tulsa.
The prenatal and parenting programs include information on preterm labor (prenatal), smoking (second-hand smoke) avoidance, sexually transmitted disease (HIV/AIDs, syphilis, gonorrhea) prevention, child health and development and targeted risk reduction information (family violence, depression, alcohol use, illicit drug use and smoking). All programs have support materials collected eclectically from the March of Dimes, Parents As Teacher’s curriculum (Born Learning previously called the Minnesota Early Learning--MELD) and the American Lung Association. Materials were selected by committee to represent the most cultural appropriate and age appropriate materials. Baby Basics (2003) has been selected to become the universal resource manual for pregnant program participants and will be given to each program participant. This is being funded by the FHC through Smart Start Oklahoma and JumpStart Tulsa. All materials are in English and Spanish. A less than complete collection of Russian and Vietnamese translations are available. All programs have a pre and post test of knowledge which has been documented in outcome measures for the last eight years. However, behavior changes in smoking are documented comparatively from initial to 36 weeks for prenatal clients as a performance outcome. Depression is measured at initial, 36 weeks, postpartum and annually for program participants using the 4P+ (Chasnoff) and the Beck Postpartum Depression Scale (postpartum). Substance use and smoking are measured with 4P+ at each visit contact.
The scope of work for the Health Education and Training model includes community-based presentations to women of childbearing age and their significant others. Approximately 20% of the Scope of Work is dedicated to community-based presentations. The Health Education and Training model maintains relationships with social service agencies, juvenile agencies, Department of Human Services, Tulsa Housing Authority sites and public schools are on a recurring basis. An average of 550 participants per year are engaged in these programs. Programs are focused in 6 major topic areas: substance abuse, domestic violence, depression, nutrition and family planning and HIV/AIDS prevention.
Health educators present information about other topics such as parenting, sexually transmitted diseases, Fetal Alcohol Syndrome, effects of smoking, contraception, human growth and development, relationships, fathering, life plans and anger management in episodic programs on request. The average length of each presentation is two hours. Approximately 750 community participants are apart of these programs (which may be a duplicated count).
Health educators explore opportunities to reach high risk individuals that are not engaged in any social service agencies. Through health fairs and other agency promotion events, the health educators can make referrals and distribute brochures, pamphlets, and information on upcoming classes, while networking with other community agencies. These services are episodic focus on community participants. Health fairs engage approximately 10,000 people per year.
The scope of work for the health educator entails recruiting and training the consumer advocacy groups. Consumer advocacy groups participate on the FHC, support legislation involving perinatal care, provide feedback to the THS Executive Management Team concerning access to services and increase community knowledge of THS efforts.
43

Tulsa Healthy Start Initiative 2001-2005
The consumer advocates participate at the highest possible level in the structure of the FHC with mentoring from the Health Education and Training health educators. The goal is to have consumer advocates constitute 15% of the FHC, participating in meetings and committees. Consumer advocacy groups consist of women of childbearing age, their partners, leaders in housing complexes, leaders in faith-based communities, and members of the community at-large. The Health Education and Training staff recruit members for the consumer advocate groups by meeting with Resource Coordinators employed by the Tulsa Housing Authority. In addition, the Health Education and Training Team continue to maintain relationships with organizations such as the Department of Human Services, Welfare-to-Work programs and educational institutions such as Tulsa Community College and Tulsa Technology Center to recruit consumers for the advocacy groups.
In addition to the previously mentioned functions, the Health Education and Training Team spend approximately five percent (5%) of time publishing a newsletter. The goal of the newsletter is to provide education and information about THS. This newsletter is a tool to educate local and state legislators for sustainability as well as to:
share information with other Healthy Start programs, keep local subcontractors abreast of the project successes, and report data quarterly developed by the Tulsa Healthy Start evaluator.
Occasional papers are prepared and released annually for state-of-the-art information on risk related topics. Analysis of Teen Birth 1990-1999 (2001), Post-partum Depression (2002), Substance Use (2004), and Analysis of Ten Years of Linked Birth and Death Certificates 1991-2000 (2004). These papers are disseminated widely, and used as part of the local and state planning efforts.
Social marketing to the public and professional audiences have been conducted with FHC by the health educators. These campaigns include a comprehensive WIC social marketing campaign (1997), Smoking Cessation campaign (1999), Back to Sleep campaign (2001), Ask Me! (2002), Healthy You, Healthy Baby (2003-04) and the Father Involvement campaign of (2004-05). All campaigns include physician information, bill boards and incentive materials.
A Learning Resource Library is maintained at the Parent-Child Center of Tulsa (PCCT). This resource library includes table top displays, posters, brochures, and models which can be used in health education activities by case managers, health educators and outreach workers. The access to the materials are on a library check-out system for 3 days use. Over 200 check-outs were made in calendar year 2004.
For calendar years 2001 to 2004, 2,353 presentations and health fairs resulted in 48,803 participants. Of the total presentations, 2% presentations were related to Interconceptional Care and Family Planning content. The Training Institute conducted 62 workshops, and 6 statewide conferences. It co-sponsored 2 additional state wide conferences. The total professional and paraprofessional attendance was 4,193. Cultural competence content was included in each presentation.
Table 21 Tulsa Healthy Start Training Institutes and ConferencesProfessionals and Paraprofessionals 2000-2005
Education & Professional Paraprofessional General Total # Comments:
44

Tulsa Healthy Start Initiative 2001-2005
Training Event Evaluation ParticipationConsumer
Involvement: Making It
WorkJune 2001
11 11 A- 22 Sponsored with the DHHS,
HRSA, CISS/COG
Weapons, Violence and
DrugsJune 2001
A 82
Blue Print for Change:
Economic Issues
June 2001
A + 132 Joint conference
sponsored by Tulsa and
Oklahoma City Healthy Start Programs, the
Oklahoma State Dept. of
Health, Parent Child Center of
Tulsa and Turning Point
Blue Print for Change: Faith
IssuesJuly 2001
A- 99 Joint conference
sponsored by Tulsa and
Oklahoma City Healthy Start Programs, the
Oklahoma State Dept. of
Health, Parent Child Center of
Tulsa, Tulsa Metropolitan
Ministries and Turning Point
Blue Print for Change:
Future SearchAugust 2001
A 128 Joint conference
sponsored by Tulsa and
Oklahoma City Healthy Start Programs, the
Oklahoma State Dept. of
Health, Parent Child Center of
Tulsa, Tulsa Metropolitan
Ministries and
45

Tulsa Healthy Start Initiative 2001-2005
Turning Point and funded
through CISS/COG Technical Assistance
Mayor’s Summit on
Methamphe-tamine
September 2001
A 300 Joint conference
sponsored by the Mayor’s Office with
LLBG funds, Office of the US Attorney General and
Turning PointMELD
ConferenceOctober 2001
20 A 20 Joint conference
sponsored by Tulsa Healthy Start Programs
and Parent Child Center of
TulsaSmoking CessationDecember
2001
7 A 7 Joint conference
sponsored by Tulsa Healthy Start and Tulsa
Health Department
MATCH program
Cycle of Violence
January 2002
A- Joint conference with
Domestic Violence
Intervention Services
OHCA Reduction in
Service Response
February 2002
10 B 10
Gestational Diabetes
March 2002
15 20 A 35
Child Development MilestonesApril 2002
11 18 A+ 29
Health A 312 Sponsored by
46

Tulsa Healthy Start Initiative 2001-2005
SummitApril 2002
the Zarrow Family
Foundation, University of
OklahomaDrug Affected
Babies: Systems
Issues, May 2002
33 A 33 The Mayor’s Office
Substance Use, Domestic Violence and Depression:
Co-Factors in Infant
MortalityMay 2002
A 275 Joint conference with Title V, Central
Oklahoma Healthy Start,
March of Dimes, Parent-Child Center of Tulsa, Turning Points, Tulsa Health Dept
Uninsured, Medicaid
Eligible and Underinsured
Key Stakeholders
Meeting May 2002
55 A 55 Joint conference with
Community HealthNet
Sickle Cell Disease
July 2002
7 15 B 22 Sponsored with the National
Association for Sickle Cell
Disease, Oklahoma Chapter
Immigration and
Naturalization: What Health and Social
Service Professionals Should KnowAugust 2002
A- 42 Sponsored with Oklahoma
Institute for Child
Advocacy New Beginnings
Maltreatment and
Adolescent Pregnancy and
ParentingSeptember
2002
75 B 75 Teleconference with Tulsa
Health Department
47

Tulsa Healthy Start Initiative 2001-2005
Tulsa Summit on Health
October 2002
109 A 109 Sponsored with Community HealthNet
Region VI Healthy Start Partnerships: Interventions to Eliminate
Health DisparitiesNovember
2002
15 90 A 105 Sponsored with Region VI
Healthy Start programs in
New Mexico, Texas,
Louisiana, Arkansas and Oklahoma,
Title V Oklahoma and
DallasTulsa Healthy
Start Orientation December
2002
7 15 A 22
Learning Resource
Center 2002
77 contacts with 300
participantsHealthy
Lifestyles for Pregnant Women: Nutrition
January 2003
7 27 A 34 Sponsored with Tulsa Health Department
What Leads to Infant
MortalityFebruary 2003
8 13 A 21 Sponsored with Parent Child
Center of Tulsa and Tulsa Fetal Infant Mortality
ReviewHealthy
Lifestyles for Pregnant Women: Exercise
March 2003
10 5 A 15 Sponsored with Tulsa Health Department
HIPAA..What all frontline staff should
know? April 2003
A 45 Sponsored with the Tulsa
Health Department
Healthy Lifestyles
During Pregnancy—Pharmaco-
logy
17 10 A 24 Sponsored with the Tulsa
Health Department
48

Tulsa Healthy Start Initiative 2001-2005
May 2003 Family Support
ConferenceMay 2003
A 118 Sponsored with the Family
Support Association of
OklahomaOklahoma Fatherhood
SummitJuly 2003
A 85 Joint conference of the National Fatherhood Initiative, Oklahoma
Institute for Child
Advocacy, OSDH—CAP, Turning Points,
DHSMale
Involvement September
2003
20 15 A 35 Sponsored with Tulsa Health Department
Prematurity.It is a bigger
problem than you think.
October 2003
40 62 A 102 Sponsored with Tulsa Health Department,
March of Dimes
Oklahoma Chapter,
Oklahoma Institute for
Child Advocacy Healthy
BeginningsRegion VI
Healthy Start Title V
ConferenceLas Cruces,
NM October 2003
A 138 Region VI Healthy Starts and Region VI
Title V Directors
Healthy You Healthy Baby!
Infant Exercise
November, 2003
10 5 A 18 Sponsored with Tulsa Health Department
Healthy You..Healthy Baby! Breast
Health
22 10 A 32 Sponsored with the Tulsa
Health Department
49

Tulsa Healthy Start Initiative 2001-2005
December 2003
Learning Resource
Center 2003
85 contacts with 350
participantsHealthy
You..Healthy Baby!
Preconceptual Health Risk
January 2004
16 9 A 25 Sponsored with Tulsa Health Department
Community Indicator
SymposiumJanuary 2004
A 84 Sponsored with Community HealthNet,
Tulsa Health Department
ShareLink Training
January 2004
A 33 Sponsored with Community HealthNet
Health Summit III
Pre-conferenceJanuary 2004
A 154 Sponsored with Community HealthNet,
Vision 2025 and the
University of Oklahoma
ShareLink Training
February 2004
A 15 Sponsored with Community HealthNet
Men’s HealthFebruary 2004
A 39 Sponsored with the Tulsa
Health Department
Health Summit III
February 2004
A 154 Sponsored with Community HealthNet,
Vision 2025 and the
University of Oklahoma
Teen Pregnancy: A
New LookMarch 2004
A 33 Sponsored with Margaret Hudson Program
Conference on Infant
Mortality: Know the
Facts and Save Babies
April 2004
A 208 Sponsored with Tulsa Fetal
Infant Mortality Review, March of Dimes, Tulsa
Health Department,
Pediatric A 28 Sponsored with
50

Tulsa Healthy Start Initiative 2001-2005
Health: Special Needs
ChildrenMay 2004
SoonerStart
Pediatric Health:
Pediatric DentistryJune 2004
A 24 Sponsored with the Tulsa
Health Department
Oklahoma Fatherhood
SummitJuly 2004
B 81 Sponsored with COPE, Inc.
Tulsa Healthy Start
OrientationAugust 2004
A 32
Recognizing Arrested Prenatal
Development, September
2004
55 A 55 Pediatric Grand Rounds
Presentation. Dr. Ira
Chasnoff
Prenatal Risk Screening, September
2004
35 A 35 Sponsored by Hillcrest Women’s
Center. Dr. Ira Chasnoff
Together for Oklahoma’s
Children with Special Needs,
September 2004
A 114 Co-Sponsored by: Tulsa
Systems of Care, Care
Link, Associated Centers of Therapy,
Mental Health Association, Tulsa Area Alliance on
Disabilities and Tulsa Health
Dept.Childhood
Brain Development, October 2004
A 19 Co-sponsored with the Child Care Resource
CenterWelcoming Fathers Into the Picture, November,
2004
A- 133
51
Tulsa Healthy Start Initiative 2001-2005
How to Assist Families After Fetal or Infant
Loss, November,
2004
A 20 Co-Sponsored with FIMR and
the Tulsa Health Dept.
Helping Children Cope with Divorce,
December, 2004
A 25 Co-Sponsored with Family &
Children’s Services
Learning Resource
Center 2004
54 Check-outs with 200
participantsP.O.P.S.
Program for Teen Fathers, January 2005
A 19 Co-Sponsored with Margaret
Hudson Program
Fathers & Public
Housing, February 2005
A 28 Co-Sponsored with Tulsa Housing
AurthorityPaternity
Issues and DHS,
February 2005
A 29 Co-Sponsored with DHS
Cultural Considerations of Fatherhood March 2005
A 19
Child Custody Issues and
Fathers, April 2005
A 17
Bridges Out of Poverty, April
2005
A 64 Co-sponsored with the Tulsa
Health Department
HS Staff Training/new grant, May
2005
A 21
3 Consumer Focus Groups,
May 2005
A 38
Overview of the Ages &
Stages Questionnaire,
June 2005
A 20
52

Tulsa Healthy Start Initiative 2001-2005
Facilitating and detracting events. As sited in the outreach and case management core service sections, federal funding at a stand still level reduces the number of funded positions from 4.0 FTE in 2001 to 3.0 in 2004 FTE for health education and training. Client barriers include low motivation to participate in health education and training activities. Program participant audiences are difficult to engage and maintain particularly for the Advocacy Committee component. Clients who are dealing with the day to day frustrations of poverty and child rearing are not enthusiastic regarding group activities that the relevancy seems nebulous. Incentives have had a minor effect in engaging or retaining participation. The FHC received a DHHS, CISS grant relevant to this issue from 1999-2001. It was very successful in helping the providers to understand ways families can be engaged meaningfully on a limited engagement basis. These strategies have been most successful.
D. Interconceptional Care: Interconceptional care is defined as continuity of care from the conclusion of one pregnancy
to the onset of a second pregnancy has been included in the postpartum care description of case management services since the first cycle of THS funding. THS does not conduct interconceptional care as a separate model but it is included in the core services of case management and outreach.
Community decision to select this model. The FHC included interconceptional care as a core service of the case management and outreach components since the THS Initiatives inception in 1998. Clients who have participated in prenatal services are followed in case management (high risk) or outreach (moderate risk) during the 2 years after the baby is born. THS does not seek participation of new clients for case management that have not been a part of the THS case management prenatally. This decision was made based on the capacity of the case managers to accept new clients. In the build years of 1998-2000, caseloads were primary prenatal clients. From 2000-2005, caseloads of case managers are 1/3 pregnant and 2/3 parenting. Outreach workers from 1998-2004 have served interconceptional women only on their limited community case management caseloads. THS case managers incorporate interconceptional care interventions into the routine postpartum care for clients in case management at the time of delivery. Additional clients are not elicited into the program due to the capacity restraints of the current program. All professional case management programs which participate in the triage program previously described in Section One serves up to 2 years following the delivery of the baby.
Identify components of intervention and resources. Case managers have a caseload averaging 35 clients with 2/3 of clients in the post partum period. The visit patterns are dictated by the individual plan of care and the continuity of care affiliated with care transfers to primary care providers outside of the participating clinics. The THS protocols call for at least one visit in the postpartum period and then quarterly thereafter for the next two years or until discharge. Low risk and moderate risk clients may be seen by outreach workers in community case management. Moderate risk and high risk clients are followed by case managers.
THS case managers interconception services include: assessment, information and referral, education and reduction of barriers to services. Assessment for risks (weighted scale) is conducted during the initial prenatal, 36 week gestation, birth, with the post-partum and quarterly during the interconceptional period. The risk assessment is conducted to determine the level of intensity and amount of services from case managers is needed. The case managers may
53

Tulsa Healthy Start Initiative 2001-2005
counsel, education or refer clients for additional services. No direct medical services are provided
Health education and services may include but not limited to: nutrition, smoking cessation, alcohol cessation, substance use cessation, safe sex practices, family violence intervention, mental health interventions, family planning (spacing and contraception), establishment of medical home for mother and child, housing, education and career exploration, child care and family support. Barriers to services are minimized with referral for transportation, child care or translation supports.
Attrition is highest in the interconceptional period. Attrition slots are filled with high risk prenatal women. Hence, the average amount of unduplicated intraconceptional women per year is 300. Program participants who remain during the interconceptional period are affiliated with a medical home as a result of their continued service. Women who have been lost due to attrition by mobility, provider change, etc. may not be tracked adequately with phone or home visit. The ShareLink database is intended to improve the monitoring process of “community medical home” by providers having access to pertinent health information wherever the client may access services in Tulsa County.
Primary pediatric medical homes are established for infants and toddlers. Every effort is made to maintain the pediatrician that saw the infant at birth, frequently, OU/OSU residents see infants at delivery hospitals but may not assume their care after delivery. No direct medical care is provided to infants in the THS program. Maternal education, case management, well child services, acute care services, immunization, SoonerStart referrals are made in collaboration with the interconceptional care aspect of the case management program. Program participants who are low or moderate risk may be seen by the outreach worker in the home or community case management.
Intensity of care is determined by the risk level of the mother or if the child is identified as a special needs child. Frequency of visits for higher intensity infants and children vary by need and are expressed in the THS protocols.
Facilitating or detracting events. Interconceptional care services are offered as a continuum of services for program participants to reduce the likelihood of negative outcomes with higher order births. Fifty percent of clients will have a repeat pregnancy within two years even though they may deliver outside of the two year period. This high incidence of repeat is characteristic of high risk women (family violence, substance use, and depression). As a result of this continuity of care, an entry point for high risk infants not seen prenatally, or interconceptional high risk entry has not been a feature of the THS program. The Project Officers have acknowledged this discrepancy and have not pressed THS to create new entry points. The number of people that can be case managed has direct correlation to the amount of case managers which is driven by the amount of money available to support case management. It is not an infinite amount including all three professional case management programs (THS, Children First, and Healthy Families Oklahoma). THS is the only case management program that targets high risk women for services. Children First and Healthy Families Oklahoma target low and moderate risk. As a result, many high risk women are turned away from services because of a lack of capacity within THS.
54

Tulsa Healthy Start Initiative 2001-2005
Behavioral services for pregnant women are limited in Tulsa County and the state. Substance use services are not paid for by Medicaid unless the client has a presenting mental health problem. The mental health treatment services can be paid for by Medicaid while they have Medicaid coverage which concludes 8 weeks post-partum. The Oklahoma Department of Mental Health and Substance Abuse Services provides funding for treatment services for pregnant and parenting women. A Women and Children’s Residential Treatment Center was established in 2004 with 60 beds. These beds serve Eastern Oklahoma and have been at capacity since opening. They now restrict eligibility for inpatient services to intravenous abusers only. Undocumented women have no access to mental health or substance use service except on a sliding scale. This persistent lack of capacity in the face of such daunting numbers has reduced the likelihood of successful recovery from drug addiction or treatment of behavioral health conditions.
E. Depression Screening and ReferralThe purpose of this program is to more effectively screen, assess, refer, support and monitor
women experiencing depression during and around the time of pregnancy. For the purposes of this program a broad concept of depression is utilized which includes interrelated issues of substance use and abuse as well as domestic violence. Inherent in improving the treatment continuum is the need to provide greater education and collaboration with various providers and community organizations. Finally, this program seeks to impact these issues at a broader more global level by formulating a social marketing campaign to educate the community and legislators about the issues of depression and pregnancy.
Community decision to select this model. The FHC documented at the close of the first full year of THS operation a significantly high incidence of five factors which were often co-existing (Section One) depression, domestic violence, substance use, alcohol use and smoking. As a result, the focus of health education intervention changed to include these social factors. In 2004, the FHC was awarded a DHHS, HRSA, Women’s Behavioral Health grant to address the behavioral health issues as early in pregnancy as possible, beginning with the Free Pregnancy Test. October 2005 will be the first full year of operation of this grant program affiliated with THS.
Identify components of intervention and resources. The “Quick Screen” is used by the Outreach Workers, Babyline telephone staff, Free Pregnancy Testing staff, and case managers at each visit. The results are documented on ShareLink for comparison to previous screens. The information for physicians and community to understand the process, it’s implications and the intended follow through was part of the social marketing campaign “Ask Me!” where providers were prepared with the referral sites, treatment information and protocols to respond to positive screens.
Case manager and outreach workers (as previously described) are both employees of THS and subcontractor agencies. The scope of work and protocols are established by THD for the THS program staff and include use of screening at each visit. The Beck Postpartum Depression Scale is used at the post partum visit by the case manager and recorded in the client record and ShareLink data base.
Depression screening, assessment and referral are part of the case management services for prenatal and interconceptional care. Outreach workers can conduct screening for depression for
55
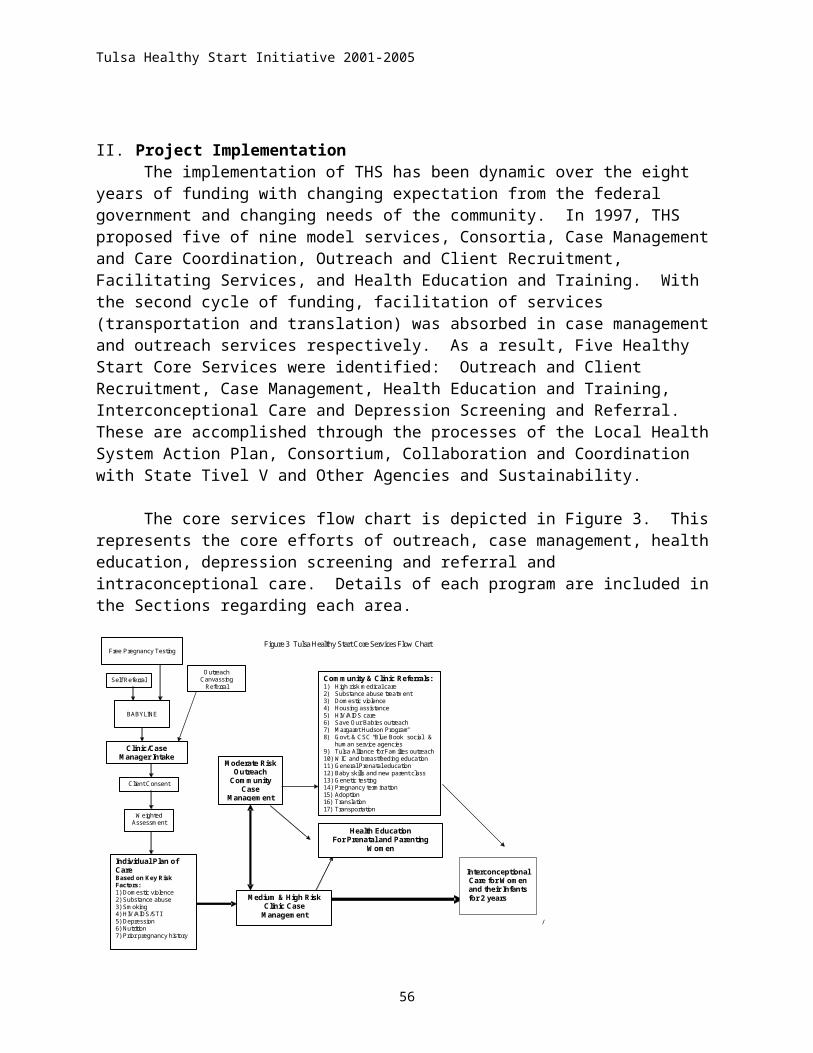
Tulsa Healthy Start Initiative 2001-2005
use in door-to-door canvassing (community participants) and community case management of low and moderate risk women using the “Quick Screen”. The “Quick Screen” uses the following questions: 1) Have you ever had problems or been treated for depression?, 2) Do you feel sad or depressed more often lately?, 3) Do you feel anxious more often lately?, 4.) Do you feel overwhelmed lately? Any of these questions answered positively require additional assessment. The “Quick Screen” and the Beck’s Postpartum Depression Scale have been validated for the multiple cultures. Both tools are translated into Spanish.
If the client screens positive than the outreach worker refers the client to the case manager for assessment. Assessment of depression is conducted with the Beck Postpartum Depression Scale (if appropriate) or the “Lethality” assessment included in the THS protocols. Appropriate referrals are made for treatment after this assessment is complete. The documented referral and completion of the referral is made through ShareLink. The mandatory schedule of documentation is Initial, 36 week visit, birth, post partum and quarterly during the interconceptional period. However, the screen is part of the Maternal/Ped form prompt screen for each visit and can be conducted as needed.
The Healthy You…Healthy Baby social marketing campaign was conducted in Fall 2002 and Spring 2003. Emphasis has been made on the risk factors which lead to infant mortality which include the co-factors of depression, family violence and substance use. Newspaper articles, special interest stories and television news features have been conducted regarding the co-factors.
Facilitating or detracting events. Case managers are frustrated due to the limited capacity and resources for mental health and substance use services. Additional resources, for assessment and diagnosis are located for each individual client in need of care through the Mental Health Association of Tulsa, Family and Children’s Services, University of Oklahoma College of Medicine Psychiatry, IHCRC, Associated Centers for Therapy, Parkside Behavioral Health Center and the Tulsa Behavioral Health Center. A Women’s Behavioral Health grant was funded to the FHC in 2004 to establish protocols for services especially for family violence, substance use and depression. Barriers to treatment include service capacity, stigma, transportation, affordability and culturally sensitivity. Medicaid (SoonerCare) will not pay for substance use services. They will pay for mental health services if the lead diagnosis is a mental health approved code. All services comes to a conclusion 8 weeks postpartum unless the client is concurrently enrolled in TANF Medicaid.
The serious lack of capacity and the overwhelming need for substance use services has become a mantle to address the co-factors of depression. The Oklahoma Institute of Child Advocacy and the Family Health Coalition joined efforts and through 3 legislative years and with pressure to the OHCA was instrumental in providing substance use services to women who qualify for Medicaid during the pregnancy. This service will begin July 2005.
F. ConsortiumThe Community Service Council of Greater Tulsa (CSC), a non-profit health and human
services research and planning organization founded the Tulsa Area Coalition on Perinatal Health in 1987 which in 2000 became the Family Health Coalition. For over 60 years, the CSC has provided leadership for addressing major social and health concerns in the Tulsa area. The FHC has been a CSC-sponsored group for 17 years. Historically, a Council volunteer board
56

Tulsa Healthy Start Initiative 2001-2005
member has provided leadership. The CSC has always provided the professional staff support for the FHC’s activities, funding during the last years has primarily been through the Tulsa Area United Way, Department of Human Services Developmental Disabilities Services, DHHS Healthy Communities Access Project and the DHHS Eliminating Disparities in Perinatal Health. The applicant, THD, has been an active FHC participant since its inception and has served as a working partner on several major initiatives.
Figure 4. Family Healthy Coalition Matrix
Task Forces-Youth Development Network (fomerly Teen Pregnancy)-Tulsa Hispanic Resource Association
Community Service Council Babyline/Planline/Kidsline
Metropolitan Tulsa Urban League, Save Our Babies
ProgramMargaret Hudson Program Tulsa Health Department,
Tulsa Healthy Start
-centralized appointments and follow-up
-door to door outreach workers in targeted area of Tulsa County
-school linked services for pregnant and parenting teens -free pregnancy testing program
-client recruitment & outreach -case coordination & case management -health education and training
Participating Clinics: Participating Hospitals:-Indian Health Care Resource Center -Claremore Indian Hospital-Morton Comprehensive Health Services -Hillcrest Medical Center-Oklahoma State University, College of Osteopathic Medicine -SouthCrest Medical Center-Planned Parenthood of Arkansas and Eastern Oklahoma -St. Francis Hospital-Tulsa Health Department -St. John Medical Center-University of Oklahoma, College of Medicine-Tulsa -Tulsa Regional Medical Center
Standing Committees -Steering Committee -Social Marketing -Access -System Evaluation
Family Health Coalition-sponsored by the Community Service Council of Greater Tulsa
-consists of business, consumers, health and social service providers
-target population: minority women, teens and low-income families
The FHC consists of 199 people representing 77 agencies and consumers. Active membership is defined as attending at least 50 percent of meetings of the full consortium: 20.2% have attended 3 of 6 meetings held annually, and 68.1% have participated in subcommittee activities and events.
13.1% public agencies or organizations 47.9% community-based organizations < 1.0% private agencies or organizations (not community-based) 2.0% providers contracting with the Healthy Start program
21.2% other providers 16.1% consumers
The racial and ethnic make up is as follows72.5% White23.3% Black 3.0% Native American 1.0% Asian, and 6.0% Hispanic ethnicity
Every effort is made to ensure the racial make-up of the FHC is representative of the community. However, representatives designated by the government and agency groups are as racially representative as the agency which selects them. Community representatives from
57

Tulsa Healthy Start Initiative 2001-2005
minority organizations (Tulsa Hispanic Resource Association or IHCRC) are recruited and encouraged to be active. Consumers (community participants) are self-selecting and courted by their interest in particular issues. Program participants are being developed through a Leadership Team process headed by the health educators in collaboration with the case managers and outreach workers. Program participants seldom indicate they have time or interest in participation on FHC committees except as appropriate for an event. Efforts are being reformulated to meet the performance requirement of the THS grant by developing a select group of advocates, receive training and mentoring and become active FHC representatives.
The FHC schedule of meeting is included in Table 22.
Table 22 Family Health Coalition Meeting ScheduleMeeting Number of Meetings FrequencyGeneral Coalition 6 Bi-monthlySteering Committee 11 MonthlyAccess and Strategic Planning 11 MonthlyTulsa Alliance for Families 12 MonthlySuccess By 6/Jump Start Tulsa 12 Monthly and as neededCommunity Home Access Team (CHAT)
6 Bi-monthly
Social Marketing 11 MonthlyExecutive Management Committee-THS
12 Monthly and as needed
Tulsa Hispanic Resource Association 6 Bi-monthly and as neededCase Manager Meeting-THS 12 Monthly and as neededOutreach/Education and Training Meeting-THS
12 Monthly and as needed
Subcontractors Meeting-THS 6 Bi-monthly and as neededSystems Development 10 Monthly and as neededAll Staff Meeting-THS 2 Ad hocFree Pregnancy Testing Meetings 4 Ad hocTFIMR-CRT 10 MonthlyTFIMR-CAT 10 Monthly
58

Tulsa Healthy Start Initiative 2001-2005
The strategic plan for the FHC is redeveloped every three to five years. The annual work plan for FHC is developed in committees and brought to the General Coalition for approval (usually January). A needs assessment is generated annually and is called the Community Profile. The Systems development committee compiles data from the projects sponsored by THS and incorporates this information in the data. The complete Community Profile is available at www.csctulsa.org under the Data button. From the workplan, the policy plan is developed and used to direct efforts with the public policy committees of the Oklahoma Institute for Child Advocacy, the Children’s Consortium and CSC. The plan is inclusive of maintaining outreach programs, case management, health education, social marketing, system evaluation and advocacy in the Tulsa community. THS sponsors the monthly Training Institute which is the interdisciplinary, interagency training center which provides state of the art information on health and social science topics. Continuing education credits are given for Licensed Professional Counselors and Social Workers through their state board of licensure for programs. Two state conferences and an annual regional conference are planned through FHC efforts.
Advocacy occurs on two levels, state and federal. Federal advocacy includes providing information to Congressional delegates regarding the needs of the health care system (Medicaid reform, Family Planning Waiver implementation, continuance of THS funding, TANF reauthorization). The State advocacy includes providing information to Legislative Senators and House members (expansion of case management funding for Children First and Healthy Families Oklahoma) and participation in the Oklahoma Institute of Child Advocacy policy forum which establishes the children’s agenda for the state (teen pregnancy prevention programs, adolescent health programs, expansion of SoonerCare to 12 month continuous eligibility).
The role of the program participant has been developed over the last eight years. Using the DHHS, Community Integrated Service Systems funding from 1998-2001, the FHC received technical assistance from Family Voices to better improve the recruitment and retention of consumers. A key lesson learned is that “consumers” are often temporarily engaged due to family and employment constraints. As a result, FHC reduces the barriers of participation by providing a role that is fluid, incentive payments for participation, transportation to events/meetings and allowing the children to remain with the families during the meetings (not child care). The consumers (community participants) participate on committees that are part of the work plan development, communication/media efforts and sustainability efforts. There is not a budget/finance committee as there are no assets to budget.
Program participants are high risk women, low socio-economic and struggling to survive. Very few indicate interest in participating in any governance activities during the highly stressful pregnancy and post partum period. However, every effort is being made to identify and recruit women who are interested in participation. A Leadership Training (modeled after the San Antonio Healthy Start) was implemented in November 2004 which includes 6 weeks of training 2 hours per week assisting the participant to be aware of advocacy techniques, governing skills, participation skills and self development strategies. A job description of future participation on specific THS activities has been constructed with a mentorship plan to be implemented which will allow case managers to mentor the first class into the community role and establish a mentorship capacity of future “leaders” to mentor the next class as part of their job description.
59

Tulsa Healthy Start Initiative 2001-2005
Program participants and community participants are voting members of the General Coalition and committees. They are involved equally with providers and other representatives on the FHC with their recommendations included as appropriate in grant requests, planning, and implementation of programs. There suggestions are in all aspects of the FHC and THS programming..
Examples of the FHC successes for calendar year 2001-2004 are provided to give context to the work plan and local health planning.
In 2003, the FHC focused on maintaining the safety-net for families and children during a very turbulent time in Tulsa and Oklahoma. Due to unprecedented state revenue shortfalls, a sagging economic climate nationally and in the state, war and fear of terrorism, and massive lay-offs from the telecommunication industry locally, most philanthropic and government revenues were reduced from 12 to 18%. These reductions caused many health and social service agencies to reevaluate the eligibility and implementation of programs. With the increase in uninsured and the demands on a beleaguered SoonerCare system mounted, the Oklahoma Health Care Authority abandoned the SoonerCare Plus model in favor of Choice for the entire state. The fee for service health care delivery system is targeted for use during the Spring of 2004 as the urban areas of Tulsa, Oklahoma City and Lawton move toward a preferred provider system. As a result, the Coalition spent many meetings addressing the changes in the health care system and access to care to minimize barriers as they arose.
The TFIMR implemented the Infant Mortality Prevention Week. Activities included education programs and support services for women who are pregnant or have experienced a loss of an infant. The TFIMR website was inaugurated in 2003. An annual Infant Mortality Conference for professionals was implemented in May 2003. A study of trends in infant mortality was released in December 2004.
The Oklahoma Fatherhood Summit was conducted in Oklahoma City in July 2003. This national conference focused on male involvement and its importance in the success of the family and particularly prenatal outcomes. It was developed in collaboration with the Healthy Start of Central Oklahoma (Oklahoma City) and the OSDH. A male involvement social marketing campaign was executed in Fall 2004. A Fatherhood Expo was annualized beginning in 2004.
The Prematurity…It’s Bigger Than You Think! conference was held on October 7, 2003. The focus of the conference was infections which lead to premature birth. Over 100 physicians were reached through professional programs at Hillcrest Medical Center and the University of Oklahoma College of Medicine, Schusterman Campus. Two hundred case managers, nurses and outreach workers participated at the day long conference.
The Region VI conferences were held in New Orleans Louisiana in 2001, Tulsa Oklahoma in 2002, Las Cruces New Mexico in 2003 and San Antonio Texas in 2004. The focus of the regional conferences is to increase the collaboration between regional Healthy Start programs and the local Title V entities.
Babyline/Planline/Kidsline integrated into the HealthLink system in July 2003. This integration expanded services to non-elderly adults (19-64 years of age), improved the infrastructure of the program, and established a link with the Internet-base data system,
60

Tulsa Healthy Start Initiative 2001-2005
ShareLink funded through the DHHS, Community Access Project. Babyline data indicated a 4.9% growth in appointments for 2003 to 4,795 appointments for Tulsa County residents. The number was down a small amount in 2004 to 4,600 with a corresponding decrease in total births in the county. Babyline callers represents approximately 44% of first appointments for Tulsa County resident births.
The Free Pregnancy Testing Program was revamped when funding was dramatically reduced. The MHP has sponsored the program since 1997 for adult and teen women at 5 sites in Tulsa County for an average of 32 hours per week. The adult program was eliminated due to budget cuts imposed on the MHP. The FHC rallied support and created a joint effort between THS, PPAEO and the MHP to continue the program. The program conducts an average of 6,300 tests per year with 40-50% of the tests to teens less than 20 years of age. Forty percent of tests are positive and are referred to Babyline for first available appointment. The negative tests are referred to family planning services, THS outreach workers, at local clinics and Planline.
Community HealthNet developed its Community Access Project (CAP) work plan to address the comprehensive health needs of Medicaid and uninsured children and adults living in the metropolitan Tulsa statistical area (MSA). The plan addresses issues of infrastructure, access, utilization, continuity of care and financial stability. The plan was developed with collaboration of community leadership (Tulsa Mayor’s Office, Metropolitan Tulsa Chamber of Commerce, Metropolitan Human Services Commission), agency heads of key stakeholder health and social services agencies, grass roots forums, town hall meetings and focus groups. A synthesis of these visions generated a common community vision of an integrated system of care with identified client outcomes of 1) a better understanding of the clients’ needs, access and utilization patterns for the uninsured, underinsured and Medicaid eligible in the Tulsa MSA, 2) defined continuum of care (health, dental, mental health) from prevention to tertiary for clients who are uninsured, underinsured and Medicaid eligible, 3) a system of care that focuses on the right care for the right cost, 4) an easy to access continuum of care for the uninsured, underinsured and Medicaid eligible, and 5) improved health outcomes for children and non-elderly adults.
To achieve the improved client and system outcomes, the following objectives were developed to meet the needs of the uninsured, underinsured and Medicaid eligible. 1) Conduct a general community needs assessment of the user population for primary medical and dental and specialty care. (University of Oklahoma College of Public Health, ER Access Study, 2003, Tulsa Community Profile, Analysis of Tulsa County and Tulsa MSA for Selected Variables, 2003 and Survey of Safety-net Providers, 2003), 2) develop a business and strategic plan for the 24/7 care concept, 3) develop a Community Health Information System (CHIN) and establish other centralized Information Management systems. (renamed: ShareLink), 4) Expand and market Kidsline and Babyline to become “HealthLine” to assist clients select a medical home and make an appointment. (renamed: HealthLink), 5) Establish a comprehensive warm line/nurse line service and triage function. (renamed: NurseLink), 6) Address clinical system integration issues with an interagency task force, 7) develop a legal framework for an interagency nonprofit partnership and a community-based governance model, and 8) develop a financial plan for sustainability and continued funding. Community HealthNet was successful in securing successor funding to the CAP grant through a new categorical program Healthy Community Access Program (HCAP). This will allow the continuance of ShareLink, HealthLink and initiation of the NurseLink project. Additionally, the mental health and case management issues will be addressed.
61

Tulsa Healthy Start Initiative 2001-2005
Publication production and distribution for the Coalition was prolific from 2001-2005. The following reports were released and posted on the website: Analysis of Teen Birth in Tulsa Oklahoma for 2000 (2002) and annual updates were created in 2003, and 2004, Community Profile 2001, 2002, 2003 and 2004, Pregnancy and Depression (2002), Analysis of Divorce Indicators (2003) Analysis of Key Indicators from the US Census 2000 (2004), Substance Use in Pregnancy (2004) and Analysis of Parity (2004).. Additionally, 12 grant reports and 10 grant applications were prepared on behalf or with the Coalition.
Advocacy efforts included 1) support of the Family Planning Waiver submitted to DHHS, Centers of Medicaid and Medicare (CMS) and approved in 2005, 2) input into the state HIFA waiver, 3) analysis of state budget cuts on health, 4) analysis of health and human impact of SoonerCare eligibility reduction and SoonerCare Plus discontinuance, 5) analysis of the need for a children’s hospital, 6) promotion of tobacco tax to increase funding for Medicaid and smoking cessation programs and 7) eliminating indecency legislation regarding breastfeeding in public or breast feeding (pumping breasts) on the job.
Sustainability. Sustainability continues to be at the forefront of efforts with foundations, businesses and federal and state grant sources. The FHC has been successful in generating expansion and enhancement funding but few providers are interested in underwriting the continuation of federal programs. The OSDH has reduced or redirected funding to the community over the last four years due to significant state government revenues shortfalls and a decrease in Title V dollars. This has affected all state agencies and affiliated programs. As a result, the direction of the sustainment campaign has been directed toward state legislators and corporate appeals.
The FHC has complemented the THS grant with funding from federal and local resources: 2004 – current Title X federal grant for mobile family planning clinic for PPAEO. 1994 – current Healthy Families Oklahoma, OSDH Office of Child Abuse Prevention to
support the Parent Child Center of Tulsa in case management of pregnant and parenting families at risk for child abuse.
1997 -- current Free Pregnancy Testing Program, TAUW to support the free pregnancy testing program of MHP.
1998 -- current Save Our Babies, Community Development Block Grant to support the Metropolitan Tulsa Urban League’s infant mortality prevention program.
1998 – current Children First, David Old’s model of home visitation to reduce child abuse. 1994 – 2005 Enabling Services, OSDH to support the centralized appointment system
(Babyline/Planline) and Adolescent Pregnancy and Parenting services of the MHP. 1999 – 2005 REACH outreach, OSDH and THD levy funding to support family planning
outreach. 1994 – 2005 Title V and Title X services at PPAEO. 1999 -- 2004 Healthy Tomorrows, DHS, HRSA to support the development of the
Kidsline centralized appointment system for children uninsured and Medicaid eligible. 1999 – 2001 Covering Kids, Robert Wood Johnson Foundation through the Oklahoma
Institute for Child Advocacy to support a pilot in Tulsa to increase public awareness of the SoonerCare program.
2000 - current Kidsline Expansion, TAUW to support the expansion of the Kidsline services to after-hours and Saturday
62
Tulsa Healthy Start Initiative 2001-2005
2000 - 2003 Community Integrated Service Systems, DHS, HRSA to support the coalition in developing a stronger consumer involvement in health and social services.
2000 – current Success By 6, Bank of America and United Way of America to support the technical assistance for child care programs to implement the “Reach for the Stars” rating system, child care health program and expand services for Special Needs Children and non-English speaking children.
2001- current Healthy Beginnings, March of Dimes through the Oklahoma Institute for Child Advocacy to support professional education on infant mortality.
2001 – current It’s Your Future, Community Development Block Grant to support low income apartment community family enhancement and teen pregnancy prevention programs.
2001 -- 2005 MHP, DHS, Office of Adolescent Family Life to support a secondary prevention program for parenting teens and grandparent support program at the MHP.
THD is a contractor for a number of federal, federal pass through, state and local initiatives which support, collaborate or complement the THS contract. Recent contracts include:
1960 - current Maternal-Child Health Title V, OSDH for the provision of prenatal and children’s services.
1972 - current Title X funding, OSDH for the provision of family planning services. 1994 - current Ryan White funding, OSDH for the provision of HIV/AIDS services. 1995 - current SoonerCare (Medicaid managed care), OHCA for primary care provider
for women and children under the Medicaid managed care system of SoonerCare Plus. 1997 - current Turning Point Initiative, Robert Wood Johnson Foundation, a community
mobilization effort to prioritize health issues and design community coalitions and programs to address the priority areas. Three of the five priority areas (1997-2002) identified are substance use (reduction and prevention). infant and maternal issues and teen sexuality issues which are targets of THS. 2003 priority areas include access to care for the uninsured and other system improvements.
1997- current Children First, Oklahoma State Department of Health, a case management and outreach program designed to reduce infant mortality and child abuse through home-based services.
2000 - current MATCH, Centers for Disease Control, a model community mobilization effort to stop smoking based on four cornerstones: education, counter-marketing, surveillance and policy development.
2003 – current Healthy Community Access Project, DHHS, Bureau of Primary Care, a community infrastructure building project for the uninsured, underinsured and Medicaid eligible.
A sustainability plan for the perinatal system is fraught with gaps and failures due to poor economic times and high demand by consumers with inexhaustible needs. All efforts to include government and philanthropy in the continuum has been conceived and acted upon over the 8 years of THS and the 17 years of FHC. There are several realities of the funding system in Tulsa and most of Oklahoma: 1) philanthropy does not provide operative support, 2) the TAUW has its own agenda for funding which does not include replacing governmental funding but may leverage additional community funds on a project to complement efforts, 3) Medicaid is underfunded ($110 M in 2005) and does not desire to add any new programs no matter how valuable, 4) the state charter centralized funding of health at the state level, so the city and county government system provides no health support benefits beyond the county levy for the
63

Tulsa Healthy Start Initiative 2001-2005
THD, 5) the OSDH is centralized funding and planning and see their Title V and Title X money as “seed money” to start projects to meet federal priorities and do not provide long term funding, and 6) the community sees programs valuable if continued funding from federal or state sources and dispensable if requiring local funding only to sustain their efforts. These realities coupled with incredible tenacity of FHC stakeholders have maintained pressure on government and philanthropic sources to leverage funding from each other to sustain THS and other essential services within the safety-net.
Third party billing and managed care contracts have not been successful. SoonerCare Plus
was discontinued as of December 31, 2003. Prior to this time, the HMOs of the Medicaid managed care program refused to contract for care coordination and case management outside of their network of private providers. They insisted that telephone outreach (1:4,500 participants) was adequate. Children First, the state funded case management program, was the only contractor who was able to invoice for high risk case management prenatally. The relationship was enforced by the OHCA contracting language.
With the turbulent changes in the Medicaid/SCHIP’s system, and the discontinuance of the health maintenance organizations (2005), it is anticipated that current Medicaid providers such as PPAEO, Morton, the University of Oklahoma and Oklahoma State University will be able to invoice for case management services. A tremendous barrier to invoicing for services is the low reimburse of $15.00 per visit, hardly making worth the effort to meet the obligations of billing for case management services to the OHCA.
III. Project Management and GovernanceThe THS grant is administered by the applicant, THD, through Gary Cox, J.D., Executive
Director who is ultimately responsible for the project’s implementation. THD is a city-county health department; a government entity. As an MCH entity, it provides maternity services, child guidance, children’s services, WIC, immunization, Children First, and STD services.
The THD employs Corrina Jackson as Program Manager of THS to oversee the daily administrative operations, including the hiring of THD staff, development and monitoring of all subcontracts, working with the evaluator, providing technical assistance on administrative issues to facilitate smooth management of individual parts of the project, and to liaison closely with the lead staff of the FHC to support the Coalition’s activities as appropriate. A Project Assistant position assists with the overall program coordination and communications between the many partners on every day issues related to implementation, as well as report writing, data compilation and analysis and liaison with all the project participants. The THS project’s Chief Financial Officer, Renn LaCroix, handles the financial management responsibilities assisted by all the other project staff. The applicant contracts with a university-based evaluator to coordinate the evaluation process by Su Phipps, PhD RN of the University of Oklahoma, College of Nursing and Emma Kientz, MS, RN. All project management staff is housed at the applicant's (THD) administrative office at the James O. Goodwin, East Regional Health Center.
Figure 5. Tulsa Healthy Start Organizational Chart
64

Tulsa Healthy Start Initiative 2001-2005
TULSA HEALTHY START ORGANIZATIONAL CHARTTULSA CITY-COUNTY HEALTH DEPARTMENT
Gary Cox, Project DirectorRenn LaCroix, Project Financial Officer
Corrina Jackson, Project ManagerCheray Smith, Administrative AssistantKathy Rives, Grant Accounting Clerk
Bob Hines, Grant Auditor
COMMUNITY SERVICE COUNCILPhil Dessauer, Director
Jan Figart, Services Consultant
EVALUATORSu Phipps, PhD
TULSA HSI EXECUTIVE MANAGEMENT TEAM
Gary Cox, Project Director, TCCHDCorrina Jackson,, Project Manager,
Maria Palacios, CSCJan Figart, CSC
Su Phipps, PhD, OUEmma Kientz, OU
Leslie Shepher, BabylineKathy Kleine, TCCHD
Renetta Harrison, TCCHDAllen Baxter, TCCHDCheray Smith, TCCHD
Maria Palacios, CSC
CONSORTIUMJan Figart, Svcs Consultant
INDIAN HEALTH CARE RESOURCE CENTERDiane Hughes, SupervisorAnn Davis, Case Manager
MARGARET HUDSONDonna Walker, SupervisorKrystal Keener, Case MgrHilda Sanders, Case Mgr
MORTON HEALTH CLINICShirley Johnston-Horn RN,
SupervisorPagette Hill, Case Manager
PARENT CHILD CENTERBarbara Fyffe, Mgr/Supervisor
Michelle Evans, Case MgrTish DeHart, Case Manager
PLANNED PARENTHOODXan Blake, VP, Case Mgmt Supervisor
Tommie Chesbro, VP Ed., Outreach Supervisor
Alisha Artis, Case MgrAda Harwood, Case MgrAudra Farrow, Outreach
SAVE OUR BABIES/ URBAN LEAGUE
LaTonya Dement, Program Dir.Karon Allen, Outreach
Kassandra West, Outreach
TULSA CITY-COUNTY HEALTH DEPARTMENT
Kathy Kleine, Outreach CoordinatorPagette Hill, TFIMR
Lupe Diaz, Case ManagerGaby Carney, Case Manager
Annette Leon, EducatorRenetta Harrison, EducatorLeon Skillens III, EducatorClara E. Willis, Educator
BABYLINE/PLANLINELeslie Shepherd, Manager
Natsu Zurita, Svc SpecialistGinger Trender, Svc Specialist
Melanie Poulter, Data Specialist
OSU HEALTH CARE CENTER
(Clinic)
OU COLLEGE OF MEDICINE
(Clinic)
THS is fully intergrated into the THD communication and administrative chain. Communication between subcontractors is facilitated through Subcontractors meetings held bi-monthly at the conclusion of the bi-monthly FHC meeting. THS Program Management communicates through email and mail for formal communications. Key areas of focus annually are performance measures, quality assurance, submissions for applications for funding, new program development and program redirection. Evidence of satisfaction of the arrangement is noted in 8 years of continuous performance by all subcontractors.
All key personnel meet monthly, and are called the Executive Management Committee (EMT). At this meeting, an established agenda of committee reports, including program evaluation are provided. Solutions to problems are developed through a consensus method. Interagency commitment to the THS efforts are documented in scopes of work and protocols which are attachments on the subcontract.
All subcontracting is conducted according to current operating procedures and monthly program and financial reporting would be required in accord with DHHS, HRSA, HSI guidelines. The applicant works in partnership with the FHC and individual members and foster a spirit of consensus building on key decisions as currently occurs through the Executive Management Team. Support and guidance for implementation of each core service is provided through the FHC. Each core service is closely linked to one or more of the FHC’s current committees or task forces. Each group’s annual work plan includes active assistance for the project’s model. Final management decisions rest with the applicant. Obtaining feedback from
65

Tulsa Healthy Start Initiative 2001-2005
clients on their involvement and satisfaction with their experiences is coordinated by the Program Manager, the FHC staff and the Evaluator.
Quality assurance is measured externally and internally. Externally, the federal government receives program and financial performance reports. The county government has oversight of the fiscal compliance of the THD. Quality assurance is conducted internally three ways 1) review of program performance in comparison to the performance measures, 2) review of program performance by subcontractors to established scopes of work, protocols and financial audits, and 3) client satisfaction of services received in THS (translation, transportation, overall quality).
The external reviews are conducted by Region VI technical assistance (October 2004), HRSA project officer (Benita Baker), federal grants management officers and the Tulsa county government fiscal auditors. The internal audits are conducted by the independent evaluator (Su Phipps, PhD, RN), the Quality Assurance Review team and the THD fiscal auditors. All results are available for review and summary reports are prepared for the FHC.
IV. Project AccomplishmentsObjectives, Interventions and Indicators
Objectives, interventions and indicators are described per core service. Table 22 provides the objectives in table format. All THS indicators were developed from the performance measures established by the federal Healthy Start in 2003 grant cycle. These indicators are congruent with the OSDH 2004 Maternal Child Health Block Grant objectives and the FHC local health plan. The objectives and interventions were established with the Tulsa Healthy Start staff in collaboration with the Family Health Coalition.
No mentoring or technical assistance activities were conducted by other Healthy Start Initiatives during this period. THS is an active participant in the Region VI Title V/Healthy Start Initiative Partnership which conducts annual meetings. THS received a technical assistance review in October 2004 by the Region VI Office. The progress report of the monitoring is included in Appendix B.
66

Tulsa Healthy Start Initiative 2001-2005
Table 23: Model: ConsortiumProject Period Objective: By 5/31/05
Budget Year Objective: Strategy and Activities Progress
C-1 Increase the capacity (knowledge and skills) of consortium members through provided training.
Baseline: Number of trainings and retention of consumers.
Projected Number:Year 01 5 newYear 02 5 newYear 03 5 newYear 04 5 new
C-1 By 5/31/02 100% will report increased knowledge and skills of consortium members through provided training.
C-1 By 5/31/03 100% will report increased knowledge and skills of consortium members through provided training.
C-1 By 5/31/04 100% will report increased knowledge and skills of consortium members through provided training.
C-1 By 5/31/05 100% will report increased knowledge and skills of consortium members through provided training.
Strategy: Maintain the Community Involvement Team (CIT) approach to consumer engagement and training.Year 01 Activities:1. Provide training activities through the Training Institute to improve consumer knowledge of the issues, how to self-advocate.2. Evaluate CIT toward reaching objectives.Year 02 Activities:1. Mentor consumers by health educators to maintain participation in consortium events and committees.Year 03 Activities:1. Maintain the Client Advocates engage with bi-monthly meetings specifically to address their training and information needs. Year 04 Activities: 1. Measure satisfaction with mentoring of client advocates in FHC activities.
Year 01: Training Institutes were conducted monthly (6) focusing addressing racial and economic disparities in maternal and child health (statewide for July and August), and risk factors for infant mortality (smoking, methamphetamine use, etc). Family Health Coalition members participated with overall scores 4th quartile (agree, agree strongly).Year 02: Client Advocates conducted 8 meetings for orientation and training. Year 03: Client Advocates conducted 2 meetings for orientation and training. Fifteen new advocates were trained. 100% reported increased knowledge on pre and post test.Year 04: Client Advocates conducted 1 meeting for orientation and trained 9 new advocates.
CM-4 Increase the number of consumers participating in
CM-4 By 5/31/02, increase the number of consumers
Strategy: Identify key consumer
Year 01: Consortium participation by consumers was
67

Tulsa Healthy Start Initiative 2001-2005
consortium to 15% of consortium members. Score of 3 on Characteristics of Consumer Participation in HS (CCP).
Baseline: Number of consumers currently and number of consumers added.
participating in the consortium to 15% of consortium members.
CM-4 By 5/31/03, increase the number of consumers participating in the consortium to 15% of consortium members
CM-4 By 5/31/04, increase the number of consumers participating in the consortium to 15% of consortium membersCM-4 By 5/31/05, increase the number of consumers participating in the consortium to 15% of consortium members
leadership from the project area and begin to incorporate them into the EMT, FHC and THS programs and activities.Year 01 and Year 02 Activities1. Focus group participants, clients and residents of the project areas will be polled and encouraged to participate in CIT at the local level and in the FHC or subcommittees as interest develop.2. Clients in case management and outreach activities to be mentored by THS staff to participate in FHC and subcommittees.3. Survey will be conducted and results applied to reducing barriers (transportation, day care, meal offered, incentives, etc.) to increase participation.
Year 03 Activities:1. Create one coordinated campaign conducted by Client Advocates in their community.Year 04 Activities:
stable. No new participants were added from July to December 2001. The Health Educators began working with community groups to attract new participants to committee functions and planning opportunities. Year 02: Client Advocates participated in three presentations to community stakeholders and FHC meetings to highlight the needs of Medicaid eligible and uninsured in Tulsa. They attended a legislative day in OKC with state legislators regarding the issues. A grassroots conference was sponsored with To Your Good Health! in September 2002 where Client Advocates presented to other community members regarding the issues of health and insurability.Year 03: Fifteen new Client Advocates were trained with 2 trainings conducted. The Week of the Uninsured (March, 2003) was the large scale event with Client Advocates conducting a bus trip to OKC to talk with legislators, a letter writing campaign and participated in
68

Tulsa Healthy Start Initiative 2001-2005
the town hall event at the THD.Year 04: Nine new advocates participated in the Week of the Uninsured activities at the THD during the Community HealthNet meeting.
By 5/31/05 a FIMR process will be functioning for Tulsa County.
Baseline: TFIMR results at conclusion of 6/30/01.
Projected Numbers:Year 01 25 cases reviewedYear 02 25 cases reviewedYear 03 25 cases reviewedYear 04 25 cases reviewed
By 5/31/02, the FIMR process will have established a plan of action to reduce one of the determined causes of fetal infant mortality.
By 5/31/03, the FIMR process will have established a plan of action to reduce two of the determined causes of fetal infant mortality.
By 5/31/04, the FIMR process will have established a plan of action to reduce two of the determined causes of fetal infant mortality.
By 5/31/05, the FIMR process will have established a plan of action to reduce two of the determined causes of fetal infant mortality.
Strategy:Determine contributing factors to the cause of death of infants and children.Year 01 Activities:1. Sustain funding from OSDH.2. Conduct FIMR review of infant deaths in THS areas for 1 year.3. Streamline the process.4. Prepare baseline data report.Year 02 and Year 03 Activities:1. Recruit CRT and CAT participation from volunteers and consumers.2. Coordinate CAT social marketing with the FHC social marketing regarding women’s health, prenatal health and grief counseling.3. Conduct linked birth and death certificates for Healthy Start participants and the county within the capacity of the system.Year 04 Activities: 1. Conduct a statewide
Year 01: The Tulsa Fetal Infant Mortality Review continued with a second year of OSDH funding. The Case Review (CRT) and Community Action Teams (CAT) are active. The CRT sends analyzed results of the cases to the CAT. The CAT team has focused on women’s health, grieving and prenatal care. The TFIMR has conducted two community profiles regarding the results for the FHC at its General Coalition meeting. Pagette Hill from the CRT is a Steering Committee Member to the FHC.Year 02: The TFIMR reviewed 38 cases. CRT fully functioning. CAT implemented Infant Mortality Prevention Week for February 2002, supported a Miscarriage/Fetal Death/Infant Mortality Counseling Center (Tristee Center), plans a social marketing campaign, Get on
69
Tulsa Healthy Start Initiative 2001-2005
conference on the TFIMR results, and the PPOR method of analysis.2. Complete the 10 year analysis of the linked birth and death data for infant mortality analysis..
the Stick! to market healthy pregnancy information for women when they purchase at home pregnancy tests through selected pharmacy (Reasor’s).Year 03: Conducted the Infant Mortality Month campaign (April 2003). Co-sponsored the Prematurity Conference (October, 2003). Conducted 6 case reviews, 6 CRT meetings and 8 CAT meetings. Linked birth and death data was retrieved from the OSDH in 2003. Year 04: Released the study, Analysis of Ten Years of Linked Birth and Death Certificates 1991-2000. Key findings presented in a presentation to the FHC General Meeting. Re-organization of the TFIMR was conducted. PPOR analysis was conducted of data from 1996-2000. Findings released the FHC General Meeting. TFIMR received increased funding to add an epidemiologist. Sixteen cases were reviewed. CRT and CAT met regularly.
Strategy:Integrate THS into the Tulsa perinatal system.
Year 01: The Executive Management Team has conducted monthly meetings to
70

Tulsa Healthy Start Initiative 2001-2005
Year 01 and Year 02 Activities:1. Train staff and subcontracting agencies in the areas to be improved.2. Maintain communication with staff regarding quality improvement efforts. 3. Conduct quality review of the subcontracting agencies annually.Year 03 Activities:1. Continue Year 02 activities.2. Promote a sustainability plan with Title V/Children First.Year 04 Activities:1. Adapt FHC work plan to be inclusive of the National Healthy Start Evaluation effort.2. Advocate for expansion of the TFIMR.3. Conduct training for statewide Healthy Start effort for the new competition in 2005.
steer the THS activities. An orientation was conducted for new staff of THS. The THS Newsletter is slated to begin, Spring 2002. Monthly meetings are conducted with outreach workers and case managers. for administrative and communication purposes. The next quality review is to be conducted in the Spring 2002.Year 02: THS Newsletters, Special Deliveries and the Year 01-04 THS Report were released. State and federal legislative campaigns include infant mortality and early childhood messages. CQI review conducted in Spring 2003.Year 03: THS Newletters, Special Deliveries and the annual report were prepared. THS annual powerpoint was presented 3 times for FHC, THS subcontractors and THS staff. TFIMR funding was renewed by OSDH.Year 04: TFIMR was expanded. THS newsletters were released quarterly. THS was maintained in the annual workplan of activities for FHC.
71

Tulsa Healthy Start Initiative 2001-2005
Model: Education and TrainingProject Period Objective: By 5/31/05
Budget Period Objectives: Strategy and Activities Progress
ET1 The number of professional or paraprofessional trained in this model’s activities will be maintained at 100%.
Baseline: Current staff of THS and supervisors attend 100% of the Training Institute offerings.
Projected Numbers:Year 01 8 Trainings 150 participantsYear 02 8 Trainings 150 participantsYear 03 8 Trainings 150 participantsYear 04 8 Trainings 150 participants
ET1 By 5/31/02, the number of professional or paraprofessional trained in this model’s activities will be maintained at 100%.
ET1 By 5/31/03, the number of professional or paraprofessional trained in this model’s activities will be maintained at 100%.
ET1 By 5/31/04, the number of professional or paraprofessional trained in this model’s activities will be maintained at 100%.
ET1 By 5/31/05, the number of professional or paraprofessional trained in this model’s activities will be maintained at 100%.
Strategy:Establish Training Institute for professionals and paraprofessionals in Tulsa County.Year 01 Activities:1. Expand Training Institute services beyond THS staff. 2. Seek continuing education credits for programs offered to health professionals.3. Seek university or Vo-Tech credit toward applied learning for paraprofessional staff.Year 02 Activities:1. Establish link with Tulsa Community College for career ladder for outreach workers.2. Maintain quality cross training of case management and outreach workers in the community both with THS staff and other like programs. Year 03 and 04 Activities:1. Maintain career ladder with Tulsa Community College for outreach workers. 2. Continue interagency Training Institutes and conferences.
Year 01: From July to December 2001, 6 Training Institutes were conducted. All were attended by Tulsa Healthy Start staff and non-Healthy Start staff. Evaluations were conducted at all events with a standardized tool. Tulsa Community College was contacted and meetings have been contacted to establish a certification program for outreach workers.Year 02: The first group of 2 outreach workers participated in the Tulsa Community College Human Services certificate program Spring 2003. 12 Training Institutes, 2 statewide and 1 regional conferences was conducted in 2002. Year 03: 8 Training Institutes, 2 statewide conferences and 1 regional conference was conducted with 529 participants. 100% of paraprofessionals and professionals in THS participated in trainings.Year 04: The Tulsa
72

Tulsa Healthy Start Initiative 2001-2005
Community College connection continued to exist, but no outreach workers participated in Year 04. Fifteen Training Institutes were conducted with 516 attendants.
ET2 By 5/31/05 change in knowledge of risk behaviors such as smoking, substance use, domestic violence, fetal alcohol syndrome, depression, HIV/AIDS, family planning and behaviors that lead to poor perinatal outcomes after completion of training will be increased to 80% as measured by 1) decrease of women who smoke to 21% at 36 weeks of pregnancy,2) increase to 85% the number of women who score 80% or better on the Fetal Alcohol Syndrome Knowledge Instrument, 3) increase to 85% the number of women who score 80% or better on the Sexually Transmitted Infection Knowledge Instrument, 4) decrease to 26% the number of women who have interconceptional periods of less than 24 months and 5) 28% of target area will be reached with education, communication
ET2 By 5/31/02, change in knowledge of risk behaviors such as smoking, substance use, domestic violence, fetal alcohol syndrome, depression, HIV/AIDS, family planning and behaviors that lead to poor perinatal outcomes after completion of training will be increased to 80% as measured by 1) decrease of women who smoke to 27% at 36 weeks of pregnancy,2) increase to 70% the number of women who score 80% or better on the Fetal Alcohol Syndrome Knowledge Instrument, 3) increase to 70% the number of women who score 80% or better on the Sexually Transmitted Infection Knowledge Instrument, 4) decrease to 29% the number of women who have interconceptional periods of less than 24 months and 5) 28% of target area will be reached with education, communication
Strategy:Maintain a collaborative learning resource center.Year 01, Year 02, Year 03 and Year 04 Activities1. Assess the use of the learning resource center by THS and non-THS staff. 2. Identify new resources to be added to the resource center.
Strategy:Conduct risk reduction programs for consumers in the THS target areas.Year 01 Activities1. Develop and implement a social marketing approach regarding smoking and
Year 01: The Learning Resource Center at the Parent Child Center of Tulsa continues to be a viable avenue for release of books, table top displays and brochures for the agencies of THS with 34 unduplicated uses to 53 groups or individuals. Year 02: The Learning Resource Center had 77 contacts with over 300 participants using materials.Year 03: Learning Resource Center materials was offered to 85 groups. Year 04: Learning Resource Materials were to 54 groups.
Year 01: The Ask Me! Campaign has been established by the FHC Social Marketing Committee to focus on risk reduction. 150 physicians have received information by mail regarding the risk factors, with teaching materials, referral lists
73

Tulsa Healthy Start Initiative 2001-2005
or information on the importance of interconceptional care and family planning.
Baseline: Among the 1,679 women receiving case management services from September 1997 through August 2000, 28% smoke on entry into care and 30% of clients have an interconceptional care period of less than 24 months. No baseline exists for the score on the Sexually Transmitted Infection Knowledge Instrument or the Fetal Alcohol Syndrome Knowledge Instrument and will be established at the conclusion of the first year. There are 45,000 women of childbearing age in the target area to receive education, communication or information services.
Projected Numbers:Learning Resource CenterYear 01 50 accessYear 02 70 accessYear 03 75 accessYear 04 75 access
Social Marketing campaigns:
or information on the importance of interconceptional care and family planning.
By 5/31/03, the objective will be maintained.
By 5/31/04, the objective will be maintained.
By 5/31/05, the objective will be maintained.
substance use cessation interconceptional care and depression during pregnancy.2. Implement the Prochaska stages of change theory in the program design.3. Evaluate the results of the approach.4. Maintain HIV/AIDS programs with school based teen population and free pregnancy testing sites.Year 02 and Year 03 Activities:1. Maintain staff skills in the March of Dimes and MELD curriculum coordinated with case managers and outreach to provide in-home and community based risk reduction education for moderate and high risk women as determined by case manager.2. Maintain on-going social marketing programs for the public and the client regarding risk reduction activities (school, clinic, community-based). Year 04 Activities: 1. Conduct a social marketing campaign focusing on children with special health care needs and a second campaign on fatherhood.
and quick screens for office use. THS staff, Children First and Healthy Families OK have all been crossed trained in the materials. The initial results of the health education and training programs indicate:(1) Women who smoked at initial case management interview were 40% (158/395). Those active in THS and completed a 36 week follow-up assessment showed 30.4% (17/56) smoking.(2) Health Educators report a score of 80% or above on FASKI 67.3% for 35 of 52 participants. (3) Health Educators reports a scores of 80% or above on STIK 86.6% for 538 of 621 participants. (4) Women who were case managed and returned for THS services with their higher order births were 17 participants. 52.9% had an interconceptional period under 24 months (9/17). Of the 9, 6 were not discharged during that time and 3 were not discharged.(5) Target area reached with info on interconceptional care and family planning:
74

Tulsa Healthy Start Initiative 2001-2005
Year 01 2 campaigns Year 02 2 campaignsYear 03 2 campaignsYear 04 2 campaigns
Prevention EventsYear 01 120 events 1,200 participantsYear 02 120 events 1,200 participantsYear 03 120 events 1,200 participantsYear 04 120 events 1,200 participants
2. Engage Client Advocates in conducting the fatherhood campaign.
Total 19% participants participated in direct contacts or training which included family planning or interconceptional information (436/2,283). Of these 19.7% were active in THS (Mat/Ped form 119/603)and canvass/contact form was 18.9% (317/1,680). Presentations by health educators and outreach workers on interconceptional care and family planning represent 6.3% of presentations (20/318) reaching 776/5,367 participants. Year 02: The Ask Me! Risk Reduction and Ask Me! Healthy Lifestyle Campaigns have been established by the FHC Social Marketing Committee to focus on risk reduction. 250 physicians have received information by mail regarding the risk factors, with teaching materials, referral lists and quick screens for office use. (1) Women who smoked at initial case management interview were 40% (83/169). Those active in THS and completed a 36 week follow-up
75

Tulsa Healthy Start Initiative 2001-2005
assessment showed 22.9% (64/83) smoking.(2) Health Educators report a score of 80% or above on FASKI 94.1% for 63 of 67 participants.(3) Health Educators reports a scores of 80% or above on STIK 79.4% for 123 of 155 participants.(4) Women who were case managed and returned for THS services with their higher order births were 34 participants. 50% had an interconceptional period under 24 months (17/34). (5) Target area reached with info on interconceptional care and family planning: Total of 40.4% active THS clients participated in direct contacts or training which included family planning or interconceptional information (228/564). Others reached through canvas/contact form were 38.8% (457/1,176). Presentations by health educators and outreach workers on interconceptional care and family planning represent 11.6% of presentations (61/525) reaching 1,255/10,662
76

Tulsa Healthy Start Initiative 2001-2005
participants. Year 03: Healthy You…Healthy Baby! Healthy Lifestyle Campaigns have been established by the FHC Social Marketing Committee to focus on risk reduction in women’s health preconceptual and interconceptual. 250 physicians have received information by mail regarding the risk factors, with teaching materials, referral lists and quick screens for office use. (1) Women who smoked at initial case management interview were 47% (126/268). Those active in THS and completed a 36 week follow-up assessment showed 22.9% (47/126) smoking or a 63% decrease.(2) Health Educators report a score of 80% or above on FASKI: 2003 not calculated due to changing of tool.(3) Health Educators reports a scores of 80% or above on STIK 2003 not calculated due to changing of tool.(4) Women who were case managed and returned for THS services with their higher order births were 9 participants. 53%
77

Tulsa Healthy Start Initiative 2001-2005
had an interconceptional period under 24 months (9/17). (5) Target area reached with info on interconceptional care and family planning Total of 24% active THS clients participated in direct contacts or training which included family planning or interconceptional information (565/2,330).Year 04: Two social marketing campaigns were held, Healthy You ….Healthy Baby and the Fatherhood Involvement Campaign. Change in knowledge of risk behaviors (1) Decrease in smoking behavior by 30.6% (15/49)(2) Alcohol consumption (Fetal Alcohol Syndrome) scores 78% (32/41)(3) Interconceptional Periods Less than 24 months 61% (17/28)(4) Interconceptional care and family planning 77.3% (109/141)(5) Sexual behavior and HIV/AIDS 77.3% (109/141)
78

Tulsa Healthy Start Initiative 2001-2005
Model: Client Recruitment and OutreachProject Period Objective: By 5/31/05
Budget Period Objective: Strategy and Activities Progress
F-1 measure of client satisfaction with facilitating services will be increased to 97% for transportation services and 97% for translation services.
Projected Numbers:TransportationYear 01 250 participantsYear 02 200 participantsYear 03 175 participantsYear 04 175 participants
TranslationYear 01 250 participantsYear 02 250 participantsYear 03 250 participantsYear 04 250 participants
F-1 By 5/31/02, measure of client satisfaction with facilitating services will be increased to 91% for transportation services and 91% for translation services.
F-1 By 5/31/03, measure of client satisfaction with facilitating services will be increased to 93% for transportation services and 93% for translation services.
F-1 By 5/31/04, measure of client satisfaction with facilitating services will be increased to 95% for transportation services and 95% for translation services.
F-1 By 5/31/05, measure of client satisfaction with facilitating services will be increased to 97% for transportation services and 97% for translation services.
Strategy: Maintain transportation contract with taxi for urgent care and bus tokens to reduce no shows for transportation or appointments Year 01, Year 02, Year 03 and Year 04 Activities:1. Reexamine use of transportation services annually in comparison to alternative transportation (taxis or pay to client to buy gas).2. Determine client satisfaction with current system and solicit input to possible alternatives.3. Identify additional resources to pay for alternative approaches.Strategy:Broaden community awareness of need for translation services.Year 01, Year 02, Year 03 and Year 04 Activities1. Integrate translation services into the client recruitment and outreach model. 2. Identify need for clinics after hours answering services to have bi-lingual receptionists for emergency calls etc. for the
Year 01: The Transportation Survey revealed transportation satisfaction of 81.25% (satisfied or very satisfied). Year 02: The Transportation Survey revealed transportation satisfaction of 100% (satisfied or very satisfied). Year 03: The Transportation Survey revealed transportation satisfaction of 94.4% (satisfied or very satisfied). The areas of dissatisfaction was related to weight times.Year 04: The Transportation Survey revealed satisfaction in 88.8% of clients (8/9).Year 01: The Translation Survey revealed translation satisfaction of 100% (satisfied to very satisfied).Year 02: The Translation Survey once again revealed satisfaction of 100%.Year 03: The Translation Survey once again revealed satisfaction of 100%.Year 04: The Translation Survey revealed 100% satisfaction.
79

Tulsa Healthy Start Initiative 2001-2005
.clinics to be more responsive and less dependent on the THS outreach/translators.
Model: Outreach and Client RecruitmentProject Period Objective: By 5/31/05
Budget Period Objective: Strategy and Activities Progress
O-1 The number of infants two years of age or younger who have been recruited and receiving services will be increased to 90%.
Projected Number:Year 01 150 infantsYear 02 110 infantsYear 03 114 infantsYear 04 118 infants
O-1 By 5/31/02, the number of infants two years of age or younger who have been recruited and receiving services will be increased to 80%.
O-1 By 5/31/03, the number of infants two years of age or younger who have been recruited and receiving services will be increased to 82%.
O-1 By 5/31/04, the number of infants two years of age or younger who have been recruited and receiving services will be increased to 86%.
O-1 By 5/31/05, the number of infants two years of age or younger who have been recruited and receiving services will be increased to 90%.
Strategy:Enhance CHIPS awareness in community.Year 01 Activities:1. Participate in the Covering Kids program to enhance enrollment of infant and children in the SoonerCare program.2. Participate in the Immunization Coalition activities to promote immunizations.3. Participate with education and training model activities including health fairs, community meetings to promote enrollment to SoonerCare, immunizations, pediatric medical home.4. Improve documentation of outreach workers on the referral for services and the number of children receiving services.Year 02 Activities
Year 01: Infants recruited and receiving services by outreach staff were 67.9% (190/280) of infants reported on the canvass/contact form. This data is calculated from July 1 to December 31, 2001. Covering Kids was discontinued by the sponsoring agency due to outreach exceeding the ability of the DHS/OHCA SoonerCare program. DHS to discontinue outreach efforts on June 30, 2002 due to the same reason. FHC and THS are active on the Immunization Coalition and Community HealthNet to extend services to uninsured, underinsured and uninsurable.Year 02: Infants recruited and receiving services by outreach staff were 50% (164/328) of infants reported on the canvass/contact form. This data is calculated calendar year
80

Tulsa Healthy Start Initiative 2001-2005
1. Focus outreach activities on enrollment and utilization of SoonerCare services for the Medicaid eligible, immunizations, well-child appointments, WIC and other risk appropriate referrals.2. Conduct social marketing efforts to include legislators on the importance of pediatric medical, dental and behavioral health homes for children. Year 03 Activities:1. Continue Year 02 activities.2. Coordinate with Kidsline, Covering Kids and Families and Community HealthNet activities to increase pediatric medical homes.Year 04 Activities:1. Continue Year 02 and 03 activities.2. Coordinate with the Tulsa Alliance on Disabilities to establish a focus on pediatric medical homes for special needs children.
2002. Covering Kids and Families funded by Robert Wood Johnson Foundation and the Oklahoma Institute for Child Advocacy is the state leader. FHC has participated in the state planning for these activities. DHS to discontinued outreach efforts on June 30, 2002 due to lack of local resources to assume client care. FHC and THS are active on the Immunization Coalition and Community HealthNet to extend services to uninsured, underinsured and uninsurable. CAP grant application was successful with $880,000 received to improve infrastructure. Two stakeholder meetings and 2 health summits were conducted over the growing issues of uninsured and access. Client advocates participated in all events.Year 03: The collaboration with Covering Kids and Families established activities regarding the Week of the Uninsured (March 2003) including a bus trip to OKC and a a town hall meeting. The
81

Tulsa Healthy Start Initiative 2001-2005
Community HealthNet collaboration established an integrated Kidsline, Babyline/Planline, HealthLink system to be a one stop phone call for all health related appointments. The number of infants recruited was 255/405 or 70%. The loss between case managed mothers during prenatal care and infants connected to services falls within the number of women who stay with their private provider that delivered them (PPAEO, Morton, THD) that do not return to case management at their original clinic.Year 04: There were 398 of 764 infants who were recruited and now receive services or 52%. In September 2004, a conference was held which focused on Oklahoma’s Children in Special Needs. The focus was on developing a common language among disability, health, and mental health groups. As a result, an ongoing Early Intervention Committee has been established that as established Ages and Stages as the
82

Tulsa Healthy Start Initiative 2001-2005
universal screening tool.O-2 The number of pregnant women who have been recruited and receiving services will be increased to 50%.
Projected Number:Year 01 150Year 02 157Year 03 164Year 04 178
O-2 By 5/31/02, the number of pregnant women who have been recruited and receiving services will be increased to 42%.
O-2 By 5/31/03, the number of pregnant women who have been recruited and receiving services will be increased to 44%.
O-2 By 5/31/04, the number of pregnant women who have been recruited and receiving services will be increased to 46%.
O-2 By 5/31/05, the number of pregnant women who have been recruited and receiving services will be increased to 50%.
Strategy: Enhance THS awareness in community with door-to-door and school linked services.Year 01 Activities:1. Coordinated meetings with outreach workers and case managers to improve the transition of women from outreach into case management and the return to outreach at the conclusion of case management activities.2. Implement male involvement activities including inclusion in family planning and prenatal appointments and focus on interconceptional care.3. Implement smoking, alcohol and drug cessation and depression awareness regarding risk factors for mother and baby.4. Continue SoonerCare enrollment of women and children who are eligible.Year 02, Year 03 and Year 04 Activities:1. Analyze with Babyline and the triage participants, the number of women seeking care, the number of women
Year 01: On canvass contacts by outreach workers their were 692 women contacted of which 15% (104/692) were pregnant. Of the 588 women not in THS case management, 451 referrals for additional services were made. The high percent of pregnant women was due to the targeting of women from the free pregnancy testing and Babyline missed appointment follow-up. Of the 104 pregnant women 37 were recruited and received services from THS 35.5% (37/104).Year 02: On canvass contacts by outreach workers there were 337 pregnant women contacted of which 97.3% (328/337) received referrals. Of the 328 women not in THS case management, 1,148 referrals for additional services were made. The high percent of pregnant women was due to the targeting of women from the free pregnancy testing and Babyline missed appointment follow-up. Of the 337 pregnant women 7 were recruited and received services from THS 2.1% (7/337).
83

Tulsa Healthy Start Initiative 2001-2005
agreeing to participate in community triage and case management, the number of women referred to case management services in comparison to the number of women who engage case management services.2. Continue collaboration with Babyline and the Free Pregnancy Testing Program for follow-up of positive pregnancy tests or missed first appointments. 3. Conduct referrals for WIC, prenatal care, SoonerCare, male involvement and risk appropriate training or services.
Year 03: 650 women were referred from Babyline and 331 were referred from outreach services. 180/331 were recruited into THS case management services or 53.7%. Year 04: There were 199 of 268 women or 74.3% of pregnant women reached by outreach canvass recruited and receiving services.
84

Tulsa Healthy Start Initiative 2001-2005
Model: Care Coordination and Case ManagementProject Period Objective: By 5/31/05
Budget Year Objective: Strategy and Activities Progress
CMT-2-4.1 The percentage of completed referrals among infant participants will be 97%.
Projected NumberYear 01 189 birthsYear 02 193 birthsYear 03 197 birthsYear 04 201 births
CMT-2-4.1 By 5/31/02, the percentage of completed referrals among infant participants will be 91%.
CMT-2-4.1 By 5/31/03, the percentage of completed referrals among infant participants will be 93%.
CMT-2-4.1 By 5/31/04, the percentage of completed referrals among infant participants will be 95%.
CMT-2-4.1 By 5/31/05, the percentage of completed referrals among infant participants will be 97%.
Strategy:Incentives for parents to maintain infant health care.Year 01 and Year 02 Activities:1. Participate in the Covering Kids program to enroll children in SoonerCare and establish a pediatric medical home.2. Establish target community case management for high risk infants which are not maintaining clinic appointments.3. Maintain Kidsline for centralized appointment system for children.4. Improve documentation of referrals of infants for WIC, well child services and other risk based services.5. Improve follow-up for infants who were referred to see that the family completed the appointment.Year 03 and Year 04 Activities: 1. Continue Year 02 objectives.2. Define special needs children referral process and outcome expectations for low birthweight babies not
Year 01: Completed referrals: Infants 0-12 mths. 9.6% (15/155) There were 190 births in 2000. Of these 190, 121 were discharged from the program. Of the 155, 15 had referrals.Infants 13-24 mths. 4.2% (2/49)(to SoonerCare, WIC etc.). There were 117 births in 1999. Of these 77 were discharged in 2001. Of the remaining 2 had referrals in 2001.Year 02: Completed referrals: Infants 0-12 mths. 94.6% (331/350) were completed. .Infants 13-24 mths. 100% (18/18)(to SoonerCare, WIC etc.). Year 03: Completed referrals:among infants: 92.5% (381/412) were completed.Year 04: Completed referrals among infants was 76.5% or 127 of 166.
85

Tulsa Healthy Start Initiative 2001-2005
diagnosed with physical or mental disability at birth.
CMT-2-4.2 The percentage of completed referrals among prenatal clients will be 98%.
Projected Numbers:Births Est. 205 annuallyYear 01 189 birthsYear 02 193 birthsYear 03 197 birthsYear 04 201 births
CMT-2-4.2 By 5/31/02, the percentage of completed referrals among prenatal clients will be 91%.
CMT-2-4.2 By 5/31/03, the percentage of completed referrals among prenatal clients will be 93%.
CMT-2-4.2 By 5/31/04, the percentage of completed referrals among prenatal clients will be 95%.
CMT-2-4.2 By 5/31/05, the percentage of completed referrals among prenatal clients will be 98%.
Strategy:Maintain Babyline and triage process for the case management programs in Tulsa.Year 01 Activities:1. Expand awareness of Babyline number for women to access for prenatal care.2. Improve triage system with other area case management providers.3. Coordinate with HMO’s regarding case management services.StrategyDocument referral and reception of services by THS clients for targeted services.Year 02, Year 03 and Year 04 Activities:1. Maintain and expand the information management system which tracts referrals made and referrals received.2. Conduct training and education for all staff regarding the “warm-handoff” to facilitate the completion of referrals for WIC, risk appropriate education and service, SoonerCare, etc.
Year 01: THS case managers report 106 active prenatal clients in 2001. Of these 223 referrals were made. Of the 106 women, 35 were discharged in 2001. There were 154 completed referral done on 82 clients active during 2001 or 69.05% (154/223). The triage process is active with Children First, Healthy Families OK and THS. Babyline/Planline materials have been distributed to Human Resource Departments of area businesses and the temporary staffing agencies in Tulsa.Year 02: One thousand three hundred seventy-three (1,373) referrals were made for 324 prenatal women during 2002. Of these referrals, 47.5% were completed. (652/1,373). Two hundred twenty-five clients had at least one completed referral.Year 03: Of the 678 prenatal clients 1,682 referrals were made with 1,431 completing referrals for 85.1%. the tremendous jump was facilitated by an improved tracking system established on
86

Tulsa Healthy Start Initiative 2001-2005
the database in 2003.Year 04: There were 729 of 1,661 referrals completed among prenatal clients or 43.9%
CMT-2-4. The percentage of completed referrals among infant clients with special health care needs will be 74%.
Projected Number:Est 205 BirthsYear 01-04 6% of total births of that year
By 5/31/02, the percentage of completed referrals among infant clients with special health care needs will be 72.5%.
By 5/31/03, the percentage of completed referrals among infant clients with special health care needs will be 73%.
By 5/31/04, the percentage of completed referrals among infant clients with special health care needs will be 73.5%.
By 5/31/05, the percentage of completed referrals among infant clients with special health care needs will be 74%.
Strategy:Coordinate with area providers of health care, day care, education, social services for special needs children.Year 01 Activities:1. Coordinate services with SoonerCare and revise the protocol for referral of special needs children for care.2. Identify the issues regarding children not born in the United States and access to care for undocumented children who have special needs.3. Improve documentation by case manager of referrals made for special needs children to services.4. Document follow-up of referral completion.Year 02 and Year 03 Activities:1. Develop a special needs children review process to include assessment protocol, forms and follow-up for referrals.2. Identify system issues which are creating the lack of service
Year 01: Completed infant referrals:Infants 0-12 mths. 0% No babies of the 3 identified as in need of services received a referral of the 190 babies born to THS active clients in 2000.Infants 13-24 mths. 66% or 2 of 3 babies identified as in need of services received a referral of the 119 babies born to THS active clients in 1999.Total: 33% (2/6) of babies in need received and completed referrals.SoonerStart has closed its casefinding operations because of inadequate service availability. They are penalized for a waiting list…so no names are taken for a list. Perseverance is the only way special need services are available to children.Year 02: Completed infant referrals:Infants 0-12 mths. Twenty infants received 192 referrals. Of these referrals 63%
87

Tulsa Healthy Start Initiative 2001-2005
access.3. Analyze low birthweight and very low birthweight infants as to need for special need services.Year 04 Activities: 1. Coordinate services with the Tulsa Alliance for Families to identify a standard of definition, a continuum of care and referral points for newborns and infants.2. Collaborate on a conference to heighten physician and case management awareness of the issues of children with special health care needs.
(121/192) were completed. Infants 13-24 mths. 60% or 3 of 5 babies identified as in need of services had a completed referral Total: 62.9% (124/197) of referrals were completed for infants 1-2 years of age.Year 03: The definition of special health care needs for THS was established. There is not a uniform standard across the community. Most case managers had been using “a doctor’s diagnosis”. Any child diagnosed with a mental or physical disability and any child weighing less than 5.5 lbs. Not all children low birth weight are seen in NICU which is where most referrals for services are made. So an SGA or a low birth weight with no complications are retained in the regular nursery. 27 infants were identified as special needs with 17 completing referrals for services or developmental follow-up.Year 04: Among infants with special health care needs 62% or 13 of 21 clients completed referrals.
CMT-3 The percent of CMT-3 By 5/31/02, the percent Strategy: Year 01: Interconceptional
88

Tulsa Healthy Start Initiative 2001-2005
participating postpartum women who receive interconceptional services will be 83%.
Projected Number:Est 205 Postpartum Women annuallyYear 01 139Year 02 147Year 03 159Year 04 170
of participating postpartum women who receive interconceptional services will be 68%.
CMT-3 By 5/31/03, the percent of participating postpartum women who receive interconceptional services will be 72%.
CMT-3 By 5/31/04, the percent of participating postpartum women who receive interconceptional services will be 77%.
CMT-3 By 5/31/05, the percent of participating postpartum women who receive interconceptional services will be 83%.
Expand Planline and Free Pregnancy Testing ServicesYear 01, Year 02, Year 03 and Year 04 Activities:1. Establish a complete referral and follow-up system for women who access free pregnancy testing and are negative.2. Expand the number of free slots in Planline.3. FHC to collaborate with the OSDH and OHCA on a family planning waiver.4. Youth Resouce Network to identify strategy to reduce unintended pregnancy and produce information regarding implementation.5. Maintain the male involvement program to focus on interconceptional care especially spacing issues.6. Refer postpartum women to community based case manager and outreach workers who will target high risk women for interconceptional intensity and acuity of service increases.
services 50.2% (109/217) postpartum women in 2001 received interconceptional education or services. There were 217 births in 2001. 13 women did not return for a postpartum visit and 74 women were discharged from the program in 2001. Women who are calling Planline are receiving phone follow-up and outreach follow-up for missed appointments. Free pregnancy tests that are negative are being referred to Planline for follow-up by phone and outreach. FHC has supported the family planning waiver which was submitted by the OHCA/OSDH to DHHS, CMS. A letter of support was mailed to Tommy Thompson (DHHS). The response letter indicated that the waiver has been mailed to the state for additional information. The Teen Pregnancy Prevention Committee is now the Youth Resource Network. They have conducted an assessment of the types of pregnancy prevention programs in the community and compiled a list for release. Year 02: Interconceptional
89

Tulsa Healthy Start Initiative 2001-2005
services 97.5% (234/240) postpartum women in 2002 received interconceptional education or services.Year 03: Interconceptional services 93.8% (183/195) postpartum women in 2003 received interconceptional education or services.Year 04: Of participating postpartum women 100% received interconceptional services (133/133).
CM-1 The percentage of 1 year olds who have received the full schedule of age appropriate immunizations against measles, mumps, rubella, polo, diphtheria, tetanus, pertussis, H. Influenza and Hepatitis A & B will have increased to 77%.
Projected Number:Estimated 205 births annuallyYear 01 75Year 02 100Year 03 100Year 04 100
CM-1 By 5/31/02, the percentage of 1 year olds who have received the full schedule of age appropriate immunizations against measles, mumps, rubella, polo, diphtheria, tetanus, pertussis, H. Influenza and Hepatitis A & B will have increased to 74%.
CM-1 By 5/31/03, the percentage of 1 year olds who have received the full schedule of age appropriate immunizations against measles, mumps, rubella, polo, diphtheria, tetanus, pertussis, H. Influenza and Hepatitis A & B will have increased to 75%.
CM-1 By 5/31/04, the
Strategy:Coordinate effort of case management and outreach to emphasize immunization.Year 01 Activities:1. Implement Covering Kids project to enroll children in SoonerCare.2. Disburse client education calendar for appointments and information regarding importance of immunizations.3. Participate in Turning Point social marketing regarding infant-maternal health and particularly immunizations.4. Participate in the Immunization Coalition social marketing regarding immunizations and the Be Wise campaign.
Year 01: Full immunizations: Infants 0-12 mths. 46.3% (19/41) There has been an attrition on 21 of 62 infants from 2001 of the 190 that were born in 2000.Infants 13-24 mths. 25% (2/8) There has been an attrition of 2 clients in 2001 of the 119 babies born in l999. Kidsline conducted 36,648 out-going calls for 2001. The total consisted of THS-330, HMO-31,171 and Covering Kids-1,147.Year 02: Full immunizations: Twenty seven of eighty-six infants, or 31.4%, were reported by their mothers as having received the full schedule of immunizations.
90

Tulsa Healthy Start Initiative 2001-2005
percentage of 1 year olds who have received the full schedule of age appropriate immunizations against measles, mumps, rubella, polo, diphtheria, tetanus, pertussis, H. Influenza and Hepatitis A & B will have increased to 76%.
CM-1 By 5/31/05, the percentage of 1 year olds who have received the full schedule of age appropriate immunizations against measles, mumps, rubella, polo, diphtheria, tetanus, pertussis, H. Influenza and Hepatitis A & B will have increased to 77%.
5. Conduct follow-up phone calls on missed immunization appointments through outreach and Kidsline.Year 02 Activities:1. Maintain and expand the information management system to better track immunizations of infants in THS. 2. Examine impact of immunization shortage on maintaining the schedule.Year 03 and 04 Activities: 1. Maintain and expand follow-up tracking of immunizations on THS outreach and case management clients. 2. Conduct health fairs with the Tulsa Hispanic Resource Association to reach Hispanic clients.
The tardiness was enhanced by the lack of some immunizations due to shortage. Kidsline conducted 402 incoming and 3,040 out-going calls for 2002. Year 03: Full immunizations: One twenty infants, or 63%, were reported by their mothers as having received the full schedule of immunizations (120/191). The improvement was noted in more vaccination media available and additional tracking methods. Kidsline conducted 467 incoming and 3,700 out-going calls for 2003. Year 04: 85% of 2 year olds received the full schedule of age-appropriate immunizations (82/96).
CM-2 The percentage of pregnant Healthy Start participants who initiate prenatal care in the first trimester of pregnancy will be at least 66% for non-Hispanic and 55.6% for the Hispanic population.
Projected Numbers:Estimated 350 new clients
CM-2 By 5/31/02, the percentage of pregnant Healthy Start participants who initiate prenatal care in the first trimester of pregnancy will be at least 65% for non-Hispanic women and 54% for Hispanic women.
CM-2 By 5/31/03, the percentage of pregnant Healthy
Strategy:Continue THS social marketing campaign to address the Hispanic population.Year 01 and Year 02 Activities1. Coordinate with Turning Points to establish joint goals.2. Implement public relations strategy to increase awareness of Hispanic consumers and general community to good
Year 01: Of the 506 prenatal initial interviews conducted by THS 31% (157/506) were of Hispanic Origin. First trimester entry was 27% (42/157), 42.7% were second trimester entry (67/157) and 30% were third trimester entry (48/157). Non-Hispanic trimester of entry was 40.4% for first (141/349), 35% second
91

Tulsa Healthy Start Initiative 2001-2005
annuallyYear 01 80Year 02 80Year 03 80Year 04 80
Start participants who initiate prenatal care in the first trimester of pregnancy will be at least 65% for non-Hispanic women and 54% for Hispanic women.
CM-2 By 5/31/04, the percentage of pregnant Healthy Start participants who initiate prenatal care in the first trimester of pregnancy will be at least 65% for non-Hispanic women and 54% for Hispanic women.
CM-2 By 5/31/05, the percentage of pregnant Healthy Start participants who initiate prenatal care in the first trimester of pregnancy will be at least 66% for non-Hispanic women and 55% for Hispanic women. CM-2 By 5/31/04, the percentage of pregnant Healthy Start participants who initiate prenatal care in the first trimester of pregnancy will be at least 65% for non-Hispanic women and 54% for Hispanic women.
prenatal health equals good beginnings…..3. Evaluate increase use with increased public relations on the Hispanic media services, churches, chamber of commerce etc.Year 03 and Year 04 Activities1. Continue Year 01 and Year 02.2. Education OHCA and legislators regarding need for the SCHIPs funding to be extended to women of Hispanic Origin to encourage early entry into prenatal care.3. Support Community HealthNet providers to increase their cultural competence for women of Hispanic origin.4. Support Tulsa Hispanic Resource Association activities that promote health care.
(124/349) and third 24% (84/349). The Tulsa Hispanic Resource Association was an outgrowth of the bilingual services committee of THS.Year 02: First trimester entry of prenatal clients of Hispanic Origin was 24.7% (42/170), 44.7% were second trimester entry (76/170) and 30.5% were third trimester entry (52/170). Non-Hispanic trimester of entry was 35.5% for first (211/593), 35.5% second (257/593) and third 21% (125/593). The Tulsa Hispanic Resource Association was an outgrowth of the bilingual services committee of THS. They have conducted 2 town hall meetings, 1 health fair and developed an outreach directory for health professionals who serve Hispanic clients.Year 03: First trimester entry of prenatal clients of Hispanic Origin was 31.3% (32/102), 51% were second trimester entry (50/102) and 15.6% were third trimester entry (16/102). Non-Hispanic trimester of entry was 34.5% for first (126/365), 47.6% second
92

Tulsa Healthy Start Initiative 2001-2005
(174/365) and third 10.9% (40/365). The Tulsa Hispanic Resource Association was an outgrowth of the bilingual services committee of THS. They have conducted 1 town hall meetings, 1 health fair and developed an outreach directory for health professionals who serve Hispanic clients.Year 04: For non-Hispanic women it was 30.5% (60/197) and for Hispanic women it was 19.6% (22/112).
CM-3 Among women who prenatal received Healthy Start Services:3a. Percent of low birth weight babieswill be reduced to 7%3b. Percent of very low birth weight babies will be reduced to 1.2%.3c. Percent preterm will be reduced to 8.1%.3d. Percent small for gestational age will be reduced to 5.4%.3e. Percent large for gestational age will be no more than 6.4%
CM-3 By 5/31/02, among women who prenatal received Healthy Start Services:3a. Percent of low birth weight babieswill be reduced to 7.4%3b. Percent of very low birth weight babies will be reduced to 1.2%.3c. Percent preterm will be reduced to 9%.3d. Percent small for gestational age will be reduced to 6%.3e. Percent large for gestational age will be no more than 7%.
CM-3 By 5/31/03, among women who prenatal received
Strategy:Conduct assessment of infants who are born as to the demographics that lead to the low birth weight and prematurity.Year 01 and Year 02 Activities:1. Examine the relationship of poor infant outcomes with risk factors weight gain, smoking and drug or alcohol use, domestic violence etc.2. Continue to use information from the TFIMR to improve care.3. Implement Depression intervention plan with health educators for referral and intervention.
Year 01: 3a. Percent of low birth weight babieswere 10.1% (21/208)3b. Percent of very low birth weight babies were 2.9% (6/208).3c. Percent preterm were 12.5% (26/208)3d. Percent small for gestational age were 4.3% (9/208)).3e. Percent large for gestational age were 1.4% (3/208).Year 02:3a. Percent of low birth weight babieswere 11.7% (42/170)3b. Percent of very low birth
93

Tulsa Healthy Start Initiative 2001-2005
Healthy Start Services:3a. Percent of low birth weight babieswill be reduced to 7.2%3b. Percent of very low birth weight babies will be reduced to 1.4%.3c. Percent preterm will be reduced to 8.4%.3d. Percent small for gestational age will be reduced to 5.6%.3e. Percent large for gestational age will be no more than 6.6%.
CM-3 By 5/31/04, among women who prenatal received Healthy Start Services:3a. Percent of low birth weight babieswill be reduced to 7.3%3b. Percent of very low birth weight babies will be reduced to 1.2%.3c. Percent preterm will be reduced to 8.8%.3d. Percent small for gestational age will be reduced to 5.8%.3e. Percent large for gestational age will be no more than 6.8%.
CM-3 By 5/31/05, among women who prenatal received
4. Coordinate with outreach and community base case managers for the focus on interconceptional care.Year 02 Activities:1. Conduct a System Evaluation analysis on the relationship of race with outcomes, trimester of entry into care and risk factors at initial interview.Year 03 Activities:1. Conduct a System Evaluation analysis of low birth weight, very low birth weight and preterm for risk factors of the client.Year 04 Activities:1. Continue the survey of factors which lead to low birth weight, very low birth weight and preterm infants.
weight babies were 2.9% (7/240).3c. Percent preterm were 12.1% (29/240)3d. Percent small for gestational age were 6.25% (15/240).3e. Percent large for gestational age were 2.4% (10/240).Year 03: 3a. Percent of low birth weight babieswere 10.8% (21/195)3b. Percent of very low birth weight babies were 0% (0/195).3c. Percent preterm were 9.7% (19/195)3d. Percent small for gestational age were 5.1% (10/195). 3e. Percent large for gestational age were 6.4% (8/195).Year 04: 3a. Percent of low birth weight babieswere 10.4% (14/134)3b. Percent of very low birth weight babies were 0% (0/134).3c. Percent preterm were 8.2% (11/134)3d. Percent small for gestational age were 7.5% (10/134).3e. Percent large for gestational
94

Tulsa Healthy Start Initiative 2001-2005
Healthy Start Services:3a. Percent of low birth weight babieswill be reduced to 7%3b. Percent of very low birth weight babies will be reduced to 1.2%.3c. Percent preterm will be reduced to 8.1%.3d. Percent small for gestational age will be reduced to 5.4%.3e. Percent large for gestational age will be no more than 6.4%
age were 5.2% (7/134).
CM-6 Increase the percentage of clients who speak English as a second language who enter prenatal care in the first trimester to 51.5%.
CM-6 By 5/31/02, increase the percentage of clients who speak English as a second language who enter prenatal care in the first trimester to 46%.
CM-6 By 5/31/03, increase the percentage of clients who speak English as a second language who enter prenatal care in the first trimester to 47.5%.
CM-6 By 5/31/04, increase the percentage of clients who speak English as a second language who enter prenatal care in the first trimester to 50%.
CM-6 By 5/31/05, increase the percentage of clients who speak
Strategy:Hispanic targeted outreach.Year 01 Activities:1. FHC distribute results of Hispanic study to best identify barriers to service for undocumented Hispanic clients and documented Hispanic clients. 2. Identify resources to further expand translation services in clinics, hospitals, after hours answering services, etc.Year 02 Activities:1. Identify additional services for Non-Hispanic women with English as a second language.Year 03 and 04 Activities:1. Strategize with Community HealthNet providers for
Year 01: Women with English as a second language entering in the first trimester of prenatal care 25.5% (13/51). Four women were non-Hispanic. The Hispanic Study has been widely distributed and presentations are being conducted to community groups. Year 02: Women with English as a second language entering in the first trimester of prenatal care 10.7% (6/56). Four women were non-Hispanic. The Hispanic Study has been widely distributed and presentations are being conducted to community groups.
95

Tulsa Healthy Start Initiative 2001-2005
English as a second language who enter prenatal care in the first trimester to 51.5%.
improved cultural competence for clients who have English as a second language.
Year 03: Women with English as a second language entering in the first trimester of prenatal care 13.2% (7/53). Year 04: For women, with English as a second language 3.4% (1/29) received prenatal care in the first trimester.
Increase the percentage of perinatal clients who receive depression screening.
Baseline: Women are not routinely screened for depression.
By 5/31/03 increase the percentage of clients who have been screened for depression during and after pregnancy to 70%.
By 5/31/04 increase the percentage of clients who have been screened for depression during and after pregnancy to 80%.
By 5/31/05 increase the percentage of clients who have been screened for depression during and after pregnancy to 85%.
Strategy: Create a continuum of care for women who are depressed in the perinatal period.Year 02Activities:1. Empower the System Evaluation Committee of the FHC to establish a protocol for screening, assessment, documenting and referring women with depression.Year 03 and Year 04 Activities: 1. Pilot the Beck tool, and examine effectiveness in assessment.2. Continue to explore development of the continuum of care for services.
Year 02: 593 clients (100%) were screened and 115 (19.3%) were positive for depression screen. The case managers piloted the Edinburg assessment tool but were not satisfied with the tool. Beck is being examined as an alternative.Year 03: 356 clients (96.4%) were screened prenatally with 89 (25%) were positive for depression screen. 431 client (64.8%) were screened in the post partum. Beck Post Partum Depression Inventory scale has been selected for Year 04 use. Year 04: 191 clients (60%) were screened for depression in the prenatal period. 158 of 286 clients or 55% were screened for depression in the postpartum period.
Increase the percentage of perinatal clients who receive family violence screening.
By 5/31/03 increase the percentage of clients who have been screened for family
Strategy: Create a continuum of care for women who are in violent situations in the
Year 02: 593 clients (100%) were screen with 105 clients (17.7%) self reporting domestic
96

Tulsa Healthy Start Initiative 2001-2005
Baseline: Women are not routinely screened for family violence.
violence during and after pregnancy to 70%.
By 5/31/04 increase the percentage of clients who have been screened for family violence during and after pregnancy to 80%.
By 5/31/05 increase the percentage of clients who have been screened for family violence during and after pregnancy to 85%.
perinatal period.Year 02 Activities:1. Empower the System Evaluation Committee of the FHC to establish a protocol for screening, assessment, documenting and referring women with depression.Year 03 and Year 04 Activities:1. Continue to explore development of the continuum of care for services.
violence.Year 03: 356 clients (96.4%) were screened.Year 04: 178 of 318 (56%) of clients were screened for domestic violence prenatally.160 of 318 clients were screened for domestic violence postpartum.
Increase the percentage of perinatal clients who receive substance use screening.
Baseline: Women are not routinely screened for substance use.
By 5/31/03 increase the percentage of clients who have been screened for substance use during and after pregnancy to 70%.
By 5/31/04 increase the percentage of clients who have been screened for substance use during and after pregnancy to 80%
By 5/31/05 increase the percentage of clients who have been screened for substance use during and after pregnancy to 85%.
Strategy: Create a continuum of care for women who are substance users in the perinatal period.Year 02 Activities:1. Empower the System Evaluation Committee of the FHC to establish a protocol for screening, assessment, documenting and referring women with depression.Year 03 and Year 04 Activities: 1. Continue to develop the continuum of care for substance use services.2. Integrate findings from the Leadership Team into planning for Healthy Start.
Year 02: 593 clients (100%) were screened with 91clients (15.3%) positive for drug use and 181 (30.5%) positive for smoking.Year 04: 356 of 369 (96.4%) clients were screened for prenatal smoking with 47% positive for prenatal smoking at initial interview. 589 of 665 (88.5%) postpartum clients were screened with 13.3% positive.356 of 369 prenatal clients were screened for prenatal use of alcohol with 4.8% screening positive.589 of 665 (88.5%) of postpartum clients were screened for alcohol with 2.2%
97

Tulsa Healthy Start Initiative 2001-2005
screening positive.356 of 369 (96.4%) clients were screened for prenatal illicit drug use with 11.9% screening positive. 589 of 665 (88.5%) of postpartum clients were screened for illegal drug use with 9.9% screening positive.Year 04: 694 of 318 (61%) were screened for smoking prenatally. 265 of 286 (92.3%) were screened postpartum for smoking.195 of 318 (61.3%) were screened for drinking prenatally.254 of 286 (89%) were screened postpartum for drinking.180 of 318 (56.5%) were screened for illicit drug use prenatally.160 of 286 (56%) were screened postpartum for illicit drug use.
98

Tulsa Healthy Start Initiative 2001-2005
V. Project ImpactThe Tulsa Healthy Start Initiative focalized activities from prenatal care access to infant
mortality reduction or a change from process to outcome. THS in its initial funding cycle had three major impacts on the perinatal system in the Tulsa community: (1) brought theoretical framework to programs and projects funded in the community through other resources, (2) pressed an alignment of Title V and community goals through the common performance measurements, and (3) dispelled myths regarding risk factors and interventions in infant mortality. During the second cycle, a strong focus has been placed in validating and replicating the strategies that reduce infant mortality.
A. System of CareThe successes of Year 01-04 activities are not overshadowed by the stresses in developing
and implementing a vast change in the perinatal system. The FHC has very basic guiding principles that all women and children should have access, that community based organizations represent an important approach to accessing low-income families and that collaboration and consensus is the process by which organizations can work together.
Healthy Start has tested that commitment in Year 05-08. Intrinsic to the development of this program was that case management and outreach could be defined and conducted uniformly over multiple agencies. Although in form this can be accomplished, in practice it has been a challenge. To achieve uniformity, the subcontracting agencies committed contractually to a scope of work. Training was conducted with front line staff, front line supervisors and executive staff of the different agencies. Protocols were established for identifying clients, admitting them into the program, consent for service, quality assurance, transfer of clients, etc. Uniformity of reporting was developed though an independent data entry system to an on-line data entry system (ShareLink). Prenatal assessments were conduced using the POPRAS form initially but has been replaced with a uniform client assessment and progress notes were of subcontracting agencies in the style and form of that agency. Teach them and they will comply is a myth.
The majority of problems have been related to process and not quality of services. Quality of services has been exceptional with case managers and outreach workers embracing the Healthy Start philosophy. However, process has been more frustrating with data entry failures, conflict with agency process and service contracts.
Data gathering has been stymied by a myriad of software glitches which has created a lack of confidence with the system. Data has been requested in both disk version and paper version in order for the central office to be able to cross reference materials to assure accuracy in preparing reports. This “extra work” has kept data entry and recovery in arrears during the entire year. The expectations that case managers and outreach workers would conduct their data entry instead of a centralized data entry has been discussed and evaluated. However, if the goal is to achieve an on-line real time system, it is necessary for front line staff to be computer literate and able to insert and retrieve data in the system. Currently, the plan is to proceed with the evolution of software until we can achieve a stable data entry process which is workable across multiple agencies.
The conflict with agency processes has been based on the underlying FHC philosophy of “service to all”. The restriction of Healthy Start funding and services to 37 census tracts is very
99

Tulsa Healthy Start Initiative 2001-2005
problematic particularly when clinic sites may serve a broad catchment area of the city. For case managers who are working off-site of their agency such as the Parent-Child Center of Tulsa, case managers located at the University of Oklahoma College of Medicine, Women’s Clinic find that all women are high risk, and are expected to be seen by the case manager even though may are not in the target area. The case managers have difficulty segregating their caseload by high risk and low risk because of the rapid change in risk factors for low-income women. So caseloads continue to grow and the case managers become frustrated that “they can’t see everyone they want to….and their caseload is so high that they can’t see the ones they have!” This internal conflict poses the most significant threat to staff turnover that we face.The EMT has conducted several measures to attempt to define this stressor: 1) an all staff retreat in which philosophical conflicts have been discussed, 2) inclusion of representatives from the models in all decision-making areas regarding their model, 3) interaction with executives and front line supervisors regarding the expectations of service (staff and client rations, services areas) and 4) case management driven solutions to the risk triage and service delivery.Service contracts for translation and transportation services have been an area of frustration. Client satisfaction surveys regarding translation and transportation services document a very high satisfaction with the services. Yet in looking at the “no show” rate for appointments and the comments which are included in the surveys, one wonders if their satisfaction is just having the service. Translation demands outside the clinic are increasing particularly for laboratory services, ultrasound services and hospital services not located at the clinic site. This off placement of staff inhibits the ability of the primary clinic to have services. In looking at the philosophies of the ancillary and hospital services, the underlying belief is that “bring your own” or “take what we have”. Often clerical staff are brought in to translate regarding medical issues in which they do not have adequate familiarity to assure a quality translation. THS is leading the way in advocacy for non-English speaking clients in the medical community by support of the Hispanic Study and focus on this issue at FHC Access Committee meetings.Transportation for planned and urgent care has been a concern point. Expansion of the MTTA Medilift service time has been costly with any visit scheduled during that period whether Healthy Start or other contractors were being posted to the Healthy Start account. Additionally, little attempt beyond driving by the address and sounding the horn was made to assure the client achieved the ride. The lack of customer service has caused THS to discontinue this option and contract solely with cab companies for door-to-door services.This has not been without problems. Taxi drivers often seek additional payment from riders even though on the THS voucher system. One cab driver threatened to call the police when the rider would not pay the fee. The lack of customer service and poor communication with the cab companies has caused THS to continue to examine other alternatives. This area is resistant to a simple solution.
A hallmark of the Tulsa community is its collaboration. Tulsa is the largest community in the United States that does not have a public hospital, as a result, the provider system in Tulsa has frequently planned and implemented joint ventures. From this history, the Family Health Coalition which is staffed by the Community Service Council through funding from the Tulsa Area United Way, OSDH Title V, TCCHD and DHS, HRSA, Community Integrated Service System (CISS). The FHC is not a service provider and maintains a neutral position in conducting assessments of the community needs and programs to fill the gaps. FHC has been the grant developers, quality assurance, program evaluation for a number of community-based initiatives including the Free Pregnancy Testing Program (Margaret Hudson Program), Save Our Babies (Metropolitan Tulsa Urban League), Children First (TCCHD), School-linked Services for
100

Tulsa Healthy Start Initiative 2001-2005
Pregnant and Parenting Teens (Margaret Hudson Program) and Covering Kids (Community Action Project of Tulsa County).
The Tulsa community excels in the use of collaborations and strong working relationships. The THS has built on that tradition and created the largest collaboration the community has experienced to date. More than anything else, this may be Healthy Start’s greatest impact in Tulsa. Tulsa Healthy Start has successfully brought together governmental, non-profit agencies of various sizes and medical schools. This collaboration represents specialists in the areas of medicine, child abuse prevention, pregnant and parenting teens, public health, neighborhood organization, education and many others. Never before has a medical school had a case manager working in their clinic and with their clients who was actually employed by a non-profit organization, and supervised by someone in a third organization. Never before has a “management team” been made up of staff representing the THD, a non-profit planning agency and a major university. Never before have 8 different organizations brought together by complex subcontracting relationships met in a regular, ongoing manner to devise the best system possible for women and their children. Without this level of partnership, Tulsa Healthy Start would never have been able to reach and serve these extremely high-risk women and their children.
B. Impact to the CommunityThe Healthy Start program has also had a significant impact on the Tulsa community
through various community awareness and social marketing campaigns. Marketing campaigns have included; “Back to Sleep” (addressing sleep position and SIDS), “Ask Me” (encouraging providers to screen for depression, substance use and domestic violence), “Healthy You, Healthy Babies…Take Care of Yourself” (focusing on preconceptual women’s health), Father Involvement (engaging fathers in health care of mother and baby), and “The 2-Year Plan” (focusing on interconceptional family planning). The Social Marketing Committee has also been the organizing force for the various conferences that have been held such as Welcoming Fathers Into the Picture (2004), Together for Oklahoma’s Children with Special Needs (2004), Conference on Infant Mortality: Know the Facts..Save a Baby (2004), Prematurity It Is A Bigger Problem Than You Think (2003), the Oklahoma Fatherhood Summit (2003) and “Substance Abuse, Depression and Domestic Violence, Co-factors in Infant Mortality” in 2002. Tulsa was hosted the regional Healthy Start conference in November 2002, and collaborated on the 2003 and 2004 conferences which have included several nationally recognized presenters. Many of the education campaigns have been targeted to providers. The exciting part is that both traditional providers to the indigent as well as private doctors have received these messages.
Perhaps the truest form of a successful impact is when an idea or program need is identified that becomes independently supported. Such is the case with the Tulsa Fetal Infant Mortality Review program (TFIMR). This began as a program under Healthy Start and was sustained by the OSDH through the THD. Even though both programs are under the Health Department, each has separate funding and administration. TFIMR has two teams: a case review team and a community action team. The case review team receives confidential anonymous information about an infant death and looks for possible system changes that might have prevented that death. The community action team takes the recommendations from the review team and tries to implement needed changes. The review team has been active for approximately 7 years and the community action team for almost 5 years. The community action team has focused on preconception health, grief services and greater access to prenatal care.
101

Tulsa Healthy Start Initiative 2001-2005
THS has conducted in-state presentations for communities regarding addressing infant mortality and replicating the THS models. A state wide presentation was conducted as a Pre-Conference to the Conference on Infant Mortality (2004). Social marketing campaigns have been designed for corporate, community and legislative support. Public service announcements for radio and television have been disseminated throughout the state.
C. Impact on the StateAs has been previously described, THS collaborated with all state agencies to develop a
continuum of care for low-income women and children who are uninsured, underinsured and Medicaid eligible. THS has documented that adequacy of health care is not numbered in visits but in the quality of health care that is rendered by the service providers. THS has underscored the importance of state agency planning with communities and not for communities. As a result of this strong community voice, THS has been able to communicate effectively with data generated from the program the needs of women and children and the type of programs which best serve the Tulsa community.
As part of the state impact, the FHC has sponsored the Director’s Committee (1999-2001). This committee includes leadership from OSDH Title V and the OHCA. During these meetings, the Tulsa community and state officials discussed the unstable Medicaid managed care environment in Tulsa and its impact on quality care to low-income families. These discussions have enabled smooth transitions of families from health maintenance organizations no longer contracting in the Tulsa market. This group spawned two initiatives, the Covering Kids (Covering Kids and Families) and Preventive Health Task Force projects.
Covering Kids was a Robert Woods Johnson Foundation grant to the Institute of Child Advocacy in Oklahoma City to improve the access of eligible, uninsured children ages 0 through 17 to the Child Health Initiative Program (CHIP). Tulsa was a pilot site through the Community Action Project of Tulsa County. This effort engaged Tulsa Healthy Start outreach workers to assist families in enrolling in the SoonerCare program. The program was largely successful with over 2,500 children enrolled. It became the Covering Kids and Families project of which the FHC had representative members and conducted four successful Week of the Uninsured campaigns.
The Preventive Health Task Force analyzed the access and utilization of families and children of the SoonerCare program. Approximately 60% of the eligible population is enrolled in SoonerCare, yet, Early Periodic Diagnosis and Treatment (EPSDT) utilization rate is very low (62% has had at least one visit, OHCA, HCFA 416 Report, 2003). Oklahoma has the least number of pediatric providers participating in the Medicaid program (Academy of Pediatrics, Provider Survey, 2000). This Task Force successfully advocated for HB 2019 which improved reimbursement to SoonerCare providers to 90% of the 1999 Medicare reimbursement rate for the same service. It has also been successful in working with the OHCA and OSDH to initiate the Family Planning Waiver which has made family planning available for men and women whose family income does not exceed 185% FPL.
The THS subcontractors participated on a collaborative effort, Community HealthNet. The traditional providers have formalized their network by incorporating as a non-profit organization. The traditional providers of care include Morton Comprehensive Health Services (federally qualified health center), Indian Health Care Resource Center (federally qualified urban
102
Tulsa Healthy Start Initiative 2001-2005
Indian health center), the University of Oklahoma College of Medicine Tulsa, Oklahoma State University College of Osteopathic Medicine, Margaret Hudson Program (a niche service for pregnant and parenting teens) THD, Planned Parenthood of Arkansas and Eastern Oklahoma and the Community Service Council’s Babyline (centralized appointment system). The interaction with Community HealthNet providers and THS has made it possible to secure funding from the Medicare Outreach Project, the Healthy Communities Access Project and local foundations.
D. Local Government RoleLocal government has played a limited direct role in Tulsa Healthy Start. City and county
government do not have a role in health or social service development. This role is centralized in state agency budgets. The exception to this is the local offices of the THD and the Department of Human Services. THD has the administrative role of the THS and has been a long term member of the safety-net providers of care for the community. DHS participates in the Family Health Coalition and has played a role in the Covering Kids program.
THS and OSDH, Title V Program has collaborated in the development, implementation and sustainment of the Tulsa Healthy Start Initiative. The goals the federal MCHB and THS are consistent with the overall State effort to develop comprehensive community-based systems of services. It focuses on service needs identified in the State FY 2004-2006 Maternal Child Health (MCH) Services Title V Comprehensive Needs Assessment and Block Grant Plan. The mission of the Oklahoma MCH Block Grant is to improve the health of all mothers and children in Oklahoma. It is accomplished by six goals: (1) to improve the health of all mothers and children in Oklahoma families by providing and assuring women, mothers and children (particularly those with low income or with limited availability of health services) access to quality child health and women’s health (as related to pregnancy and prevention of unwanted pregnancies) services; (2) to reduce infant mortality and the incidence of preventable disease and handicapping conditions among children; (3) to promote the health of mothers-to-be and infants by providing preconception, prenatal and post-partum care for low-income, at-risk, pregnant women; (4) to promote the health of children by providing preventative and primary care services for low-income children; (5) to provide and facilitate community-based systems of family-centered, coordinated cares, especially for children with special health care needs and their families; and (6) to improve the health of all mothers and children consistent with the applicable status goals and national health objectives for the year 2010. The THS project advances the Title V objectives by strengthening community-based systems of maternal and infant care through efforts of the FHC to reduce infant mortality in the community and specifically the target areas of THS.
The linkage of the THS with the OSDH Title V MCH is evident in a number of ways. The applicant, Tulsa Health Department (THD), is a member of the FHC and is a Title V and Title X provider of services. The THD is the lead agency for the Turning Point Initiative and Tulsa Healthy Start Initiative which includes a number of community partners.
New Title V funding was received by the THD for the Fetal Infant Mortality Review (FIMR) process ($42,000) in Year 03. This funding supports the project established in Year 02 through THS funding and FHC planning and implementation.
The THD and the FHC have been striving for healthy citizens in our community by emphasizing exploration and development of strategic public and private partnerships. THS
103

Tulsa Healthy Start Initiative 2001-2005
staff have participated in Turning Point planning activities which has a very high visibility in the community with community and business leaders participating in the planning and implementation health system change. Maternal-infant health, substance use, and teen sexuality are 3 of 5 priorities. Over 200 presentations have been conducted to the general public, chambers of commerce in Tulsa County, social and civic agencies and public school setting to raise the awareness of community members in these areas. THS goals are included in the Turning Point social marketing, public policy, and health information and planning committee’s objectives.
Sustaining the THS models of client recruitment and outreach and case coordination and case management is directly dependent upon OHCA through the Medicaid managed care program, SoonerCare. The OHCA has been reluctant to pay for any services outside of the primary care provider’s fee. The changes made in FY04-05 to the OHCA has enabled PPAEO, OU and OSU to be reimbursed for a small amount of high risk case management services. The reimbursement is so low that it does not cover the cost of the personnel. Agencies that do not already have contracts as Medicaid providers are reluctant to increase their overhead costs to become a Medicaid agency and invoice for these services.
D. Lessons LearnedTHS has been a catalyst for the perinatal system to make changes in the
access and delivery of health and social services for women and infants. In order for Healthy Start to be effective it requires passionate commitment to the reduction of infant mortality by the staff, key leadership must be tenacious to keep the message before the public, professionals, agencies and legislators and data drives the system.
VI. Local Evaluation
HEALTHY STATE LOCAL EVALUATION REPORT
PROJECT NAME: Tulsa Healthy StartTITLE OF REPORT: Evaluation of Healthy Start Project 2001-2005 AUTHOR: Su An Phipps PhD, RN
IntroductionLocal Evaluation Component
The THS has had a well established performance measure and evaluation plan since its inception. The evaluation component of the Tulsa Healthy Start Initiative was developed in 1997 by Paulette Burns R.N., PhD as part of the grant application to the national organization. The evaluation plan was designed in a four column format which incorporates: 1) the project period objective; 2) the annual project objective; 3) strategy and activities to meet the objectives; and 4) progress (toward meeting the objectives). Dr. Burns, a faculty member of the University of Oklahoma College Of Nursing (OUCN), resigned her position in June 2001 and was replaced by Su An Phipps R.N., Ph.D., who is also affiliated with the College of Nursing. Emma Kientz
104

Tulsa Healthy Start Initiative 2001-2005
R.N., M.S., (OUCN), is the assistant evaluator whose responsibility is to develop and modify forms specific to the program objectives and new HRSA standards, train new employees in use of these forms, and participate in data analysis.
Healthy Start Case Manager and Outreach Coordinators have been instrumental in the development and modification of forms, as well as conducting internal audits and monitoring data collection by staff. Feedback from project staff (case managers, educators and outreach workers) regarding instrument efficacy and suggested modifications has been welcome, formally occurring through staff representation at System Evaluation Committee meetings.
HistoryThe client population served by Tulsa Healthy Start changed in 2001 from those women and
infants residing in “at risk” census tracks to women residing in certain Tulsa County zip codes determined to be at extreme high risk for a successful pregnancy outcome. This change was a result of the development of a weighted assessment system which recognized that in addition to medical factors, individual client social risk factors (e.g. substance use, smoking, depression, domestic violence) should be the focus of the determination of risk rather than environmental factors only (census track). Initial risk level is determined through screening conducted by Babyline, a community referral/triage service. The pregnant women at highest risk are referred to Healthy Start. Once assigned to a clinic and THS case manger, the woman’s prenatal social and medical risk is further defined using the THS Risk Assessment tool, with reassessment occurring at 36 weeks gestation, at 6-8 weeks postpartum , and for mother and infant during the interconceptional period.
Despite the change in risk level of program participants, the focus and structure of the 2001-2005 grant evaluation retained all components of the initial plan for each of the four THS models (consortium, education and training, client recruitment and outreach, care coordination and case management). The plan was expanded in 2003 to include the additional HRSA performance measures. More recent additions and modifications to the evaluation plan and related forms have been driven by performance measure requirements from the national organization. Revisions to the evaluation plan have resulted from the evaluation process, which typically is conducted quarterly
Type of StudyThe local evaluation process includes formative evaluation, process evaluation and outcome
evaluation. Formative evaluation is conducted through quarterly reports pertaining to the program’s annual objectives and reviewed by the Systems Evaluation Committee. Internal changes are made based on this information. Process evaluation occurs when data is presented which indicates program strengths and areas of improvement. This data based evaluation also occurs quarterly, or as questions arise from other models. An annual audit of selected areas is also conducted as part of the process evaluation. Outcome evaluation is conducted and a report submitted annually to National Healthy Start. This information is shared with other local organizations, such as the Family Health Coalition and the Tulsa Community Service Council. The THS evaluators are members of the Family Health Coalition and an annual report of performance standards and infant outcomes is routinely presented. The evaluators are also members the FHC Steering Committee which meets every other month. They are also members of Tulsa FIMR Community Action Team. Some community members of the FHC also serve on the Systems Evaluation Committee
105

Tulsa Healthy Start Initiative 2001-2005
Dr. Phipps is chairperson of the THS Systems Evaluation Committee and presents quarterly data and annual data for review and input. This committee publishes an annual newsletter, Special Delivery, which incorporates Healthy Start data in discussion of maternal-infant health care issues and health care provision aimed at the professional community. Dr. Phipps also writes an “article” discussing the outcome data for Great Beginnings, a Tulsa Healthy Start publication, which is distributed to providers of care, agencies and consumers.
Key Questions As a result of providing care to the “highest of the high risk” perinatal population, THS local evaluation has incorporated maternal prenatal, interconceptional, and infant risk assessment, and relates these risk factors to outcome measures of infant mortality and morbidity. Evaluation processes have also monitored temporary and permanent changes in maternal life style behaviors ( e.g. smoking, substance use, depression, domestic violence), health practices, use of consumer services (translation and transportation), and consumer and consortium education.
Key questions during 2001-2005 included: 1. What are the salient risks factors of Healthy Start clients in total, by race and ethnicity? 2. What factors are affecting THS client’s entry into care? How can THS address this problem in the community/ Family Health Coalition?3. How do the Tulsa Healthy Start models affect maternal risk, maternal-infant morbidity and infant mortality over time? 4. What is the incidence of completed referrals for women, infants, and children with special health care needs? How can we improve tracking of appointments and how can these rates be improved? 5. How does the THS definition of special needs children correspond with that of other agencies and how are services to them tracked?
ProcessProcedures and Data Sources
THS client information is obtained by THS outreach workers, case managers, and health educators through client self report, medical records, and pre-test/post-test methods (education). Previous to February, 2004, and the implementation of ServicePoint® there was no centralized data processing location. Allen Baxter, THS Data Coordinator, collected data from the case managers and outreach workers on site at the various clinic locations. Data is now entered at each clinic by the case managers and electronically transmitted to Mr. Baxter at the Health Department. Data is complied and analyzed quarterly and annually by the system evaluators, in conjunction with Mr. Baxter. Reports of the THS client population as a whole, rather than a sample, are prepared and provided to the Systems Evaluation Committee for review and discussion. Additional data review may be requested at these meetings. Reports are then presented at the EMT (Executive Management Tam) meetings by the System Evaluator, where recommendations are made. THS demographic and outcome data is compared with Tulsa County, State and national statistics when available. THS outcome trend data is also compared to determine program effectiveness.
Data reports are shared with the Tulsa Family Health Coalition (FHC) and their steering committee. The effectiveness of the FHC is central to the success of THS. The THS evaluators
106

Tulsa Healthy Start Initiative 2001-2005
attend all coalition meetings and review all coalition meeting minutes. The functions of the committee are to monitor the overall health care system for childbearing women, including free pregnancy testing services, Babyline/Planline/Kidsline, THS data, Tulsa City-County Health Department (TCCHD) county indicators and FIMR committee recommendations, and Oklahoma State Department of Health indicators.
InstrumentsThe local evaluation has two components. Outreach workers and case managers collect the
majority of data from community participants and THS clients via self report. Outreach workers survey prospective clients using the Outreach Contact Form to determine maternal-infant health care needs and connect clients to services. They canvass many areas in the community, including housing projects. Referrals to Healthy Start or other community organizations, such as WIC, Baby-Line or Kids-Line are also documented on this form. Each Healthy Start client is seen in one of seven health clinics by a case manager who completes a Client Intake/Prenatal Record, Client/ Family Risk Assessment, and Maternal/Pediatric Visit Record. The Client/ Family Risk Assessment Form is a weighted form assessing medical and social risk factors. Case managers also review a brochure “Before Baby Arrives” to new clients which describes possible maternal perinatal risk conditions and referral agencies. The brochure is used for screening purposes and is retained by the client for future reference. The Maternal/Pediatric Visit Record includes Ira Chasnoff’s 4 Ps + to further assess substance use, smoking/ tobacco use and domestic violence on admission and throughout clients’ participation in the program. Each subsequent client contact is documented on the Maternal/Pediatric Visit Record and incorporates the Intervention and Referral Guide. Following delivery, client information is gathered on the Labor, Delivery and Postpartum Record and the Maternal/Pediatric Visit Record. Women and infants are assessed using the Family/Client Risk Assessment Form within 8 weeks postpartum. Women who are assessed at high risk for depression are given Beck’s Postpartum Depression Scale and appropriate referral is made. Case managers review 2 brochures with clients during the interconceptional period, “Before You Become Pregnant” and “Healthy Baby” which are also used for screening and possible referral. The brochures are retained by the clients. Should an infant perinatal death occur, information is recorded on The Infant Death Form. The information is compared to that gathered by Tulsa FIMR. When clients are discharged or transferred from the program, case managers complete the Transfer/Discharge from Program Form.
Educational programs offered to clients are recorded on the Presentation/Event/Canvass Form. The effectiveness of client education programs concerning a specific to a health subject, such as sexually transmitted diseases (STDs), is assessed through content specific pre and posttests. Emma Kientz annually surveyed a convenience sample of consumers of translation and of transportation services to evaluate client satisfaction. This information was complied and reported through December, 2005. Consortium data is gathered at training institutes and community committee group meetings (roster of attendance, program evaluation).
107

Tulsa Healthy Start Initiative 2001-2005
Findings and Discussion
Findings from 2001-2005 (mid year) clearly demonstrate the change to an extremely high risk client population from the previous grant cycle. Demographics revealed a 1% increase in the number of teen clients under 15, and a 6.6% increase in women ages 35-44 years of age from 2001-2005. Both populations are considered higher risk for age. The percentage of women by race and ethnicity also changed from during these years. The percent of Caucasian women has slightly decreased. The Native American population has increased approximately 3%, with African American and Hispanic populations approximating 30% each of THS clientele. Most astonishing is the change in percent of clients living under the federal poverty level (FPL). The percent living <100% FPL in 2001 has increased to 81% in 2005, while those living 100-185% has slightly decreased. The combined percent increased annually from 39.8% in 2001 to 91.9% in 2005. Almost forty-three percent had a lack of adequate, stable housing in 2004 compared to 34% in the previous cycle. The percent without transportation increased from 50-60%. The percent experiencing frequent crises rose from 27% to 36%. The only risk factor that decreased from the previous cycle was a change in percent of women with less than a high school education (67& to 54%). As evident, women of lower socioeconomic status have numerous obstacles to overcome in order to gain ready access to perinatal health care in Tulsa County.
In addition to the maternal risks associated with living in poverty and being a member of a racial/ethnic minority, the percentage of clients experiencing behavioral lifestyle risks also increased from 1998-2001 to 2003-2004. The percent of women self reporting domestic violence increased from 18% to 36% in the previous grant cycle, and the percent of women at risk for drinking and pregnancy also doubled (10% - 20.3%). Twenty percent also reported family alcohol use in 2003-04. Approximately 17% reported current or past illicit drug use in both cycles. The percentage of women with a previous or current psychiatric diagnosis doubled. While not gathered in 1998-2001, earlier, thirty-three percent reported a history of depression and 17.5% reported current depression in 2003-04. Approximately 22% were at risk for gestational diabetes mellitus from a previous or current pregnancy. The percentage of women having had a previous LBW birth increased from 15% to 18.6%.
Many of these factors, plus Tulsa’s health care system and poor public transportation system contribute barriers to prenatal care. First trimester entry into care for THS clients has always been below that of Tulsa County, which has ranged from 78%in 1998 to approximately 72% in 2004.
108
0
20
40
60
80
1998 2000 2002 2004Healthy Start
Healthy Start
Tulsa County

Tulsa Healthy Start Initiative 2001-2005
THS clients’ percentage has steadily decreased from approximately 58% in 1998 to 27.5% in 2005. Besides community barriers to care, the decrease may be partially related to clarification of the THS definition of entry into care. Entry into care is based on when the woman had her first appointment with a health provider, rather than a first clinic appointment which could mean completing paperwork or becoming eligible for services. Percentages for all racial and ethnic groups show an increased percentage in second trimester entry and decreases in first and third trimester entry.
Despite the high risk of the mothers and barriers to health care, THS clients have experienced some improved birth outcomes. No VLBW infants were born during 2003 or 2004!! The percent of VLBW infants to total births has ranged from 1.2 to 2.4%. The majority of these births were to African American moms, with Hispanic mothers running second.
The percent of LBW infants has been higher than that of Tulsa County since THS began. Not surprisingly, the percentage of LBW births increased in 2001, concomitant to the elevated risk status of the mothers, and has fluctuated from 10.8 to 12.4%. However, when one considers the lack of, or low number of VLBW births, it may be that the reason for increased LBW is that babies are remaining in utero later. This rationale is supported by data reflecting a much lower percentage of pre-term births to THS clients that what occurs in Tulsa County.
County premature births have steadily increased from 15.9% in 1999 to 19.4 in 2003. Not only have THS premature birth percentages remained lower than the County, but after a rise to 12.5 in 2000 and 2001, they have steadily decreased.
THS preterm births were lower in 2004 and 2005, (8.2% for both years) than in all previous years, including the lower risk population years of 1998 (9.4%), 1999 (9.6%), and 2000 (12.5%). Preterm births in 2003, a high risk year, were 9.7%, a percentage close to that of THS starting years with a lower risk population.
THS infant mortality rates sharply increased with the increase in client population risk level. Prior to 2001, the THS infant mortality rate was below the Tulsa County level.
109
15.9 16.3 17.118.2 18.9 19.4
9.4 9.6
12.5 12.5 12.19.7
8.2 8.2
0
5
10
15
20
25
1998 1999 2000 2001 2002 2003 2004 2005
Tulsa County
Tulsa Healthy Start

Tulsa Healthy Start Initiative 2001-2005
IMR rose sharply in 2001, from 1.1 (1999) and 4.3 (2000) to 18.4 in 2001. However, the rate has decreased each successive year to no infant deaths in mid-2005!! Only neonatal deaths comprised the IMR until 2003. At that time, post-neonatal IMR was 5.1 and 7.5. Reasons for these deaths included congenital anomalies, SIDS, and bedding with a parent. Guidea, Fone, Dunstan, Sibert and Cartlidge (2001) reported that post-neonatal IMR in particular was strongly associated with maternal social deprivation, which may be another reflection of the high risk social and medical mothers THS serves. [ Guildea, ZES, Fone, DL, Dunstan, FD, Sibert, JR, Cartlidge, PHT. (2001). Social deprivation and the causes of stillbirth and infant mortality. Archives of Disease in Children. 84:307-310.]
Limitations of findingsSeveral factors have limited the evaluation process. Most stem from the transition from
the Microsoft Access database to a more sophisticated system of Internet-based information management system, known as ShareLink, initiated in 2002. This system, co-sponsored with the Community HealthNet’s Healthy Community Access Project, enables “real time” data entry and access. ServicePoint® is the software data entry system used in ShareLink. Limiting factors include the necessity of numerous additions and adjustments to the ServicePoint® system itself to accommodate THS program evaluation. Mr. Baxter and other data management persons at the TCCHD worked closely with ServicePoint® personnel to expand their existing data base to meet the needs of THS and other community agencies. Numerous additions,adjustments and revisions were made to the ServicePoint® data base over a period of 2 years in order to accommodate the different THS forms and collect data specific to performance measures. Several “glitches” were found when running THS data for the first time on the new system and THS went “back to the drawing board.” The change to ServicePoint® required case managers, outreach workers and educators to learn a new data entry system where data screens were reformatted, more numerous and very unfamiliar. Every glitch or revision required new training and delayed data entry. In addition, staff turn over and related orientation/ education to the data system, slowed down data entry, recovery and processing. THS data entry was attempted at different times, and was successfully conducted in April, 2005. To the credit of Mr. Baxter and the case managers, outreach workers and educators, evaluation determined that data was not lost in the process as data was maintained in hardcopy and later entered into ServicePoint®.
110
7.18.4
7.28.1 7.5
6.6
1.1
4.3
18.416.7
15.4
7.5
002468
101214161820
1999 2000 2001 2002 2003 2004 2005
Tulsa County
Tulsa Healthy Start

Tulsa Healthy Start Initiative 2001-2005
However, data conversion and subsequent cleansing of data delayed quarterly reports for 2005 and affected submission of the Impact Report. Plans are to continue with ServicePoint® and for the evolution of software to achieve a stable data entry process which is compatible with that of multiple community agencies.
The transient nature of the THS population also limits the completeness of data. It is not uncommon for women exit services without notice to the case manger resulting in early discharge with resultant gaps in services and data.
The self-report nature of the risk assessment may not accurately reflect actual risks of THS clients, particularly in relation to behavioral risks such as alcohol and drug use, smoking, eating disorders, or other risk factors that are known to be socially unacceptable during pregnancy. The risks of THS mothers may actually be higher than data shows.
The changes in the performance measures required by HRSA in 2003 were a challenge, which required numerous revisions of the existing THS evaluation plan, data collection and reporting forms. However, that challenge was met by THS staff and evaluators to the optimum improvement of the program and the local and federal level.
Recommendations and Future EvaluationSeveral recommendations/ changes have stemmed from the local evaluation. These
include the introduction of The Brief Acculturation Rating Scale (ARMSAII-SF) for use with the THS Hispanic mothers, to determine the relationship of level of acculturation to maternal/infant risk and infant outcome. ARMSAII-SF has been used with clients starting in October, 2005.
Ages and Stages Questionnaires® (ASQ), a reliable way to screen infants and young children for developmental delays during the first 5 years of life is being used by THS staff, as well as in other community childhood programs. Universal screening with the ASQ was a result of clarification of the definition of children with special health care needs in THS and FHC, which varied widely by agency. As of mid 2005, children are screened and referred for developmental delays much earlier.
The facilitating services of transportation and translation are no longer evaluated, because of the continued difficulty in locating transient clients after a period of time, and because services were always evaluated as very satisfactory (90-100% satisfaction).
Case mangers will continue to screen, and follow women more closely, for eating disorders and obesity. The percentage of LGA babies has increased steadily during 2001-2005. THS percentages are still below those of Tulsa County, but the rate of growth (4%) is twice that of the County (2.3%). It was initially thought that increase in LGA may be an increase in Native American and Hispanic clients, both populations at higher risk for GDM. However, the primary factor in THS LGA babies is the obesity of the mother, rather than race/ethnicity.
The Systems Evaluation Committee is in the process of further evaluating the weight of race, particularly African American, in the risk assessment. As is reflected in national and state
111

Tulsa Healthy Start Initiative 2001-2005
numbers, THS African American clients have higher percentages of VLBW, LBW and premature births than other racial and ethnic groups.
ImpactChanges in the perinatal system or community
THS and FHC have established a Fatherhood Involvement Coalition. The intent of the group is to conduct training with service providers to improve their father friendly environments, conduct training for fathers and interested providers. THS hosted an Oklahoma Fatherhood Summit during July 2003. A Tulsa conference is planned for April, 2006.
THS, in conjunction with FIMR and their use of PPOR, have worked with the FHC and other groups to improve access to care for different racial and ethnic groups. PPOR has demonstrated to the community that most races are at higher risk for poor infant outcome prior to pregnancy (prenatal health), than during or following pregnancy. Hispanic women in Tulsa County are at a much higher risk for poor outcome as a result of factors experience during pregnancy. As a result, women’s access to care is being addressed by an Access Committee of the FHC.
Changes in project implementation THS capacity to serve is now based on the number of slots available per case manager to
accept new clients. Every effort is being made by FHC and the THD to find additional monies to increase the number of case managers. The former outreach worker role has been transformed through education and supervision to the role of community case manager. These individuals now case manage lower risk women and families, opening more slots for higher risk clients.
THS and FHC brought Jerri Roberson for the THS annual meeting in August 2005. Technical assistance was received in developing a stronger consumer involvement. Consumer involvement in THS has increased. Consumers are planning to attend the National and Regional Healthy Start meetings this coming spring.
Publications
Publications resulting from the evaluation process or those containing information related to the evaluation process are:
Phipps, S. (2004). Progress in the Past, Challenges for the Future. Tulsa City County Health Department. Healthy Start. Great Beginnings. 2(2), 4.
Phipps, S. (2004). Let’s Celebrate: Data Report. Tulsa City County Health Department. Great Beginnings, 1(2), 3.
Phipps, S.A. (2003) Healthy Start Data Report. Tulsa City County Health Department, Great Beginnings. 2(1), 4.
Phipps, S.A. (2002). Mothers at risk. Tulsa Health Department, Great Beginnings, 1(3), 5.
Phipps, S.A. (2002). Who does Tulsa Healthy Start serve? Great Beginnings, 1(2), 4.
112

Tulsa Healthy Start Initiative 2001-2005
Kientz, E. (2002). Queries Used in the Evaluation Process, Tulsa Healthy Start: Tulsa.
Phipps, S.A., Smith, C. (2002). Data report: What did we do in 2002?, Great Beginnings, 2 (1), 5. Tulsa Health Department.
Phipps, S. & Kientz, E. (2002). Risks that affect Tulsa’s Moms-to be, in R. Ivey. (ed). Great Beginnings, 1 (1), Tulsa Healthy Start Initiative: Tulsa.
Phipps, S. (2002). Who does healthy start serve? In R. Ivey (ed). Great Beginnings 1(2), Tulsa Healthy Start Initiative: Tulsa.
Systems Evaluation Committee. (2002). Kientz, E. (ed). Special Delivery, 1 (2), Community Service Council: Tulsa.
Systems Evaluation Committee. (2001). Phipps. S (ed.). Special Delivery. 1(1), Community Service Council: Tulsa.
VII. Fetal and Infant Mortality Review (FIMR)The Tulsa Fetal Infant Mortality Review (TFIMR) was established in 1998 with THS
funding. In 1999-2001, it was primarily funded by OSDH. From 2002 to the present, it is a joint funding effort of THS and OSDH Title V. It is the only FIMR in Oklahoma; however, plans do exist for replicating the Tulsa model in Oklahoma City. It has a Community Review Team (CRT) that meets monthly, and a Community Action Team (CAT) that meets variably but usually every other month. Initially, the program had a Coordinator for the CRT which conducted the chart reviews and the home visitations. The CAT Coordinator conducted the CAT activities including the preparation for conferences and support of the work groups for Grieving. Social marketing campaigns were developed from this group. The activities of TFIMR were somewhat removed from the activities of the FHC.
In the second cycle of funding, a restructuring occurred which added a specific function for chart review separate from home visitation, and added time of an epidemiologist. The work of the CAT was a team effort and much of the conferencing and social marketing was returned to the FHC. This restructuring has allowed the opportunity for the myriad of data being produced to be analyzed and compiliated in two reports, Ten Year Analysis of Linked Birth and Death Certificates 1991-2000 and the Analysis of Feto-Infant Death 1996-2000 using the PPOR. The findings have been incorporated in the THS workplan and the FHC workplan.
Key implications from the THS, and TFIMR analysis of data are:(1) entry into prenatal care does not correlate to infant mortality, (2) adequacy of care does not correlate to infant mortality, (3) maternal risk factors prior to pregnancy (family violence, depression, smoking, alcohol and illicit drug use) does correlate to in infant mortality, (4) obesity correlates to large for gestational age babies (not race or ethnicity), (5) feto-mortality correlates strongly with the Hispanic ethnicity, and (6) marital status and income does not correlate strongly to infant mortality; however, maternal education level correlates strongly.
113

Tulsa Healthy Start Initiative 2001-2005
The Child Death Review is conducted by a statewide group. Report information is not disseminated but annually. The report is used to make FHC and THS workplans.
No maternal review is conducted at the state or local level.
VIII. ProductsThe Tulsa Healthy Start has been prolific and products related to the grant period. This is considered a partial list. Appendix D includes examples of materials created with THS funding.
Table 23. Itemized Product ListItem FunctionHealthy Start Database Microsoft Access database for the
information management of case management, outreach, education and training and facilitating services (translation and transportation services).
ShareLink database for information management using an Internet-based report system.
Case Management Intake Form Initial intake form for case management services.
Risk Scale Medical and social risk scale to determine level of infant mortality risk.
Case Management Maternal/Ped Form Form for documentation by case managers of phone/personal/mail contact.
Case Management Transfer Form Transfer form for continuum of care through client recruitment and outreach.
Case Management Discharge Form Discharge form for clients no longer in case management program.
Health Presentation Form Health educator and outreach worker form for the documentation of health education and health promotion events.
Canvas Form Outreach worker form used to document canvassing contacts in the home, community and school.
Translation Log Translator log of units of service.Transportation Schedule Outreach worker, case manager and
translator log of transportation scheduling.Healthy Start Orientation Manual 2003 Manual for pre-service orientation of staff
to the Healthy Start program. Content includes: Orientation to Healthy Start (federal and local), Orientation to the Tulsa Area Coalition on Perinatal Care, Talk It Up! (presentation guide), Life Patterns
114

Tulsa Healthy Start Initiative 2001-2005
Curriculum, Evaluation. Quality Assurance Protocols Protocols for case management, outreach
worker, facilitating services, health education and training with agency evaluation guide.
Service Protocols and Scope of Work Protocols for each service model for inter agency interdisciplinary service.
Healthy Start Contractual Agreement Tulsa Health Department contractual agreement, scope of work and recitals for sub-contracting agencies.
Smoking Cessation Campaign Manual for the implementation and training for the smoking cessation campaign.
Back to Sleep Campaign Manual for the implementation and training for the back to sleep campaign.
Face Up to Wake Up Campaign (collaborative with the CJ Foundation and the Child Care Resource Center of Tulsa)
Professional training materials for the SID syndrome campaign.
Healthy Start Promotion Year 05 VHS Video/CD of Tulsa Healthy Start focusing on the successes of the first cycle
Healthy Start Before You Become Pregnant Brochure
Brochure with all the pre-conceptional and interconceptional targets included. Spanish and English
Healthy Start After You Become Pregnant Brochure with all the pregnancy targets included. Spanish and English.
Healthy Start Pediatric Brochure Brochure with all the pediatric targets included. Spanish and English.
Healthy Start Refrigerator Magnet Promotion incentive for Babyline/Planline.Healthy Start Incentives for Participation Incentives include: camera, Nuk and
Regular pacifier and pacifier catch, bottles, tippy cup, snack carrier, medicine measurer, electrical covers.
Tulsa Fetal Infant Mortality Review Manual for Community Action Team
Orientation and progress manual for participation on the Tulsa Fetal Infant Mortality Review Community Action Team for health professionals and consumers.
Tulsa Fetal Infant Mortality ReviewCase Review Team
Orientation and progress manual for participation on the Tulsa Fetal Infant Mortality Review Case Review Team for health professionals.
Tulsa Healthy Start Logo Logo slicks in two color and mono-color format in multiple sizes.
Tulsa Healthy Start Learning Resource Center Directory
A complete listing of holdings of the Tulsa Healthy Start Learning Resource Center at the Parent-Child Center of Tulsa.
Tulsa Healthy Start Outreach Guide A quick reference guide for outreach
115
Tulsa Healthy Start Initiative 2001-2005
(Edition 1 and 2) workers to community services.Tulsa Healthy Start Hispanic Guide to Service
A quick reference guide for Spanish-speaking consumers to community services which provide bi-lingual services and services to the income eligible and uninsurable consumers.
Tulsa Healthy Start-Promotion Brochure Year 05-08
Tri-fold promotion brochure in Spanish and English which promotes Tulsa Healthy Start services for the consumer. The brochure highlight a telephone referral system.
Tulsa Healthy Start-Promotion Bus Placard Bus placard used for Metropolitan Tulsa Transit Authority bus system advertising insert for inside the bus.
Family Health Coalition By-laws Family Health Coalition (previously Tulsa Area Coalition on Perinatal Health) by-laws for conduct of the coalition.
Healthy You…Healthy Baby CampaignTake Care of Yourself!
Materials include bus placard, brochure, physician information sheet, referral sheet for information regarding, letter to the physician, and request for more materials.
Ask Me! Campaign Materials include bus placard, brochure, physician information sheets on depression, smoking cessation, family violence, alcohol use and drug use, letter to the physician and request for more materials.
Father Involvement CampaignWelcoming Fathers Into the Picture
Materials include bus placard, brochure, physician information sheets on creating a father friendly environment, letter to the physician and request for more materials.
The 2 Year Plan Materials include bus placard, brochure, physician information sheets, letter to the physician and request for more materials.
THS Five Year Report A synopsis of the first cycle of THS activities.
Tulsa Healthy Start8 Years of Service
A synopsis of the second cycle of THS activities.
IX. Project DataThe Healthy Start Data Reporting Requirements follow for each year. Grantee Name: Tulsa City County Health DepartmentGrantee Name: Tulsa City County Health DepartmentProject Name: Tulsa Healthy Start InitiativeProject Grant No.: H49CM00087
116

Tulsa Healthy Start Initiative 2001-2005
FORM 9TRACKING PERFORMANCE MEASURESAnnual Objective and Performance Data
Performance Measure #07Degree to which programs ensure family participation.
Baseline
7-12 2001
CY 2002 CY 2003 CY 2004 1-6 2005
2003
Annual Performance Objective na na 40% 45% 45%Annual Performance Indicator 33% 33% 33%
Numerator 6 6 6Denominator 18 18 18
Performance Measure #10Degree to which programs ensure Cultural Competency.
2003
Annual Performance Objective na na 65% 68% 68%Annual Performance Indicator 63.8% 69.6% 69.9%
Numerator 44 48 48Denominator 69 69 69
Performance Measure #14Degree to which morbidity/mortality review processes are used.
2001
Annual Performance Objective na na 44% 50% 50%Annual Performance Indicator 44% 44% 44% 56% 56%
Numerator 4 4 4 5 5Denominator 9 9 9 9 9
Performance Measure #17Percent of children 0-2 years of age with a medical home.
2002
Annual Performance Objective na 100% 100% 100% 100%Annual Performance Indicator 89% 96% 99% 100%
Numerator 571 616 372 227Denominator 610 645 376 227
117

Tulsa Healthy Start Initiative 2001-2005
FORM 9TRACKING PERFORMANCE MEASURESAnnual Objective and Performance Data
Performance Measure #20Percent of women participants who have an ongoing source of primary care.
Baseline
7-12 2001
CY2002 CY 2003 CY2004 1-6 2005
2002
Annual Performance Objective 100% 100% 100% 100% 100%Annual Performance Indicator 100% 100% 100% 100% 100%
Numerator 626 735 647 604 465Denominator 626 735 647 604 465
Performance Measure #22Degree to which programs facilitate screening for risk
factors.
2003
Annual Performance Objective na na 64% 70% 70%Annual Performance Indicator 85.4% 87.5% 87.5%
Numerator 41 42 42Denominator 48 48 48
Performance Measure #35Percent of communities having
comprehensive systems for women's health services.
2003
Annual Performance Objective na na 50% 55% 55%Annual Performance Indicator 52.4% 71.4% 71.4
Numerator 22 20 20Denominator 42 28 28
Performance Measure #36Percent of pregnant participants who have a prenatal visit in the
first trimester of pregnancy.
2001
Annual Performance Objective 59% 59% 59% 59% 59%Annual Performance Indicator 37.1% 35.6% 36.9% 26.1% 27.5%
Numerator 163 211 126 83 68Denominator 439 593 365 318 247
118
Tulsa Healthy Start Initiative 2001-2005
FORM 9TRACKING PERFORMANCE MEASURESAnnual Objective and Performance Data
Performance Measure #50Percent of very low birthweight (<1500 grams) infants among all live births
Baseline 7-12 2001
CY2002 CY 2003 CY2004 1-6 2005
2001
Annual Performance Objective 1.2% 1.2% 1.2% 1.2% 1.2%Annual Performance Indicator 2.5% 2.9% 0% 0% 2.4%
Numerator 4 7 0 0 1Denominator 163 240 195 134 41
Performance Measure #51Percent of live singleton births weighing < 2,500 grams among all live births
2001
Annual Performance Objective 7.4% 7.4% 7.4% 7.4% 7.4%Annual Performance Indicator 3.7% 11.7% 9.7% 9.7% 12.2%
Numerator 6 28 19 13 5Denominator 163 240 193 134 41
Performance Measure #52The infant mortality rate per 1,000 live births
2001
Annual Performance Objective na na na 11.2 11.2Annual Performance Indicator 18.4 16.7 15.4 14.9 0
Numerator 3 4 3 2 0Denominator 163 240 195 134 41
Performance Measure #53The neonatal mortality rate per 1,000 live births
2001
Annual Performance Objective na na na 7.0 7.0Annual Performance Indicator 18.4 16.7 10.3 7.5 0
Numerator 3 4 2 1 0Denominator 163 240 195 134 41
Performance Measure #54The post-neo-natal mortality rate per 1,000 live births
2001
Annual Performance Objective na na na 4.2 4.2Annual Performance Indicator 0 0 5.1 7.5 0Numerator 0 0 1 1 0Denominator 163 240 195 134 41
119

Tulsa Healthy Start Initiative 2001-2005
Performance Measure #55 The perinatal mortality rate per 1,000 live births
Baseline 7-12 2001
CY2002 CY 2003 CY2004 1-6 2005
2001Annual Performance Objective na na na 11.2 11.2Annual Performance Indicator 18.4 29.2 15.4 14.9 0Numerator 3 7 3 2 0Denominator 163 240 195 134 41
120

Tulsa Healthy Start Initiative 2001-2005
Grantee Name: Tulsa City County Health DepartmentProject Name: Tulsa Healthy Start InitiativeProject Grant #: H49CM00087
FORM 5 NUMBER OF INDIVIDUALS SERVED (UNDUPLICATED) Program Participants* By Type of Individual and Source of Primary Insurance Coverage
For Projects Providing Direct Health Care, Enabling or Population-based Services
Calendar Year July – December 2001
Table 1 (a) (b) (c) (d) (e) (f)Pregnant Women Served
Number
Served
TotalServed
Title XIX %
Title XXI %
Private/Other %
None%
Pregnant Women (All Ages)
439 67% N/A .4% 31%
10-14 515-19 11220-24 15525-34 13035-44 1945 + 1
Unknown 17
Table 2 (a) (b) (c) (d) (e) (f)Children Served
Number
Served
Total Served
Title XIX %
Title XXI %
Private/Other %
None %
Infants <1 166 95% N/A 2 % 3%Children 1 to 24 yr *
497 86% N/A .6% 11.9%
12-24 months
353
25 months-4 years
0
5-9 010-14 215-19 7320-23 64
Unknown 5
* Children and Interconceptional Women Under Age 24
121

Tulsa Healthy Start Initiative 2001-2005
122

Tulsa Healthy Start Initiative 2001-2005
NUMBER OF INDIVIDUALS SERVED (UNDUPLICATED) By Type of Individual and Source of Primary Insurance Coverage
For Projects Providing Direct Health Care, Enabling or Population-based ServicesCalendar Year July – December 2001
Table 3 (a) (b) (c) (d) (e) (f)
CSHCN Served
Number Served
Total Served
Title XIX %
Title XXI %
Private/Other %
None %
Infants <1 yr
14 93% N/A 0% 7%
Children 1 to 24 yr
3 100% N/A 0% 0%
12-24 months
3
25 months-4 yrs
0
5-9 010-14 020-24 0
Table 4 (a) (b) (c) (d) (e) (f)Women Served
Number
Served
TotalServe
d
Title XIX %
Title XXI %
Private/
Other %
None%
Women 24+
87 38% N/A 1% 61%
24-29 5330-34 2135-44 1345-54 055-64 0
65+ 0 * Interconceptional Women Over Age 23
Table 5 (a) (b) (c) (d) (e) (f)Other Number
Served TotalServed
Title XIX %
Title XXI %
Private/Other %
None %
N/A N/A N/A N/A N/A N/A
123

Tulsa Healthy Start Initiative 2001-2005
Table 6 (a) (b) (c) (d) (e) (f)TOTALS Number
Served TotalServed
Title XIX %
Title XXI %
Private/Other %
None %
Grantee Name: Tulsa Healthy StartGrantee Name: Tulsa City County Health DepartmentProject Name: Tulsa Healthy Start InitiativeProject Grant #: H49CM00087
FORM 5 NUMBER OF INDIVIDUALS SERVED (UNDUPLICATED) Program Participants* By Type of Individual and Source of Primary Insurance Coverage
For Projects Providing Direct Health Care, Enabling or Population-based Services
Calendar Year___2002_____
Table 1 (a) (b) (c) (d) (e) (f)Pregnant Women Served
Number Served
TotalServed
Title XIX %
Title XXI %
Private/Other %
None%
Pregnant Women (All Ages)
509 77.41% N/A 1.36% 21.61%
10-14 715-19 13720-24 17625-34 13435-44 3845 + 1
Unknown 16
Table 2 (a) (b) (c) (d) (e) (f)Children Served
Number Served
Total Served
Title XIX %
Title XXI %
Private/Other %
None %
Infants <1 219 93.15% N/A .46% 6.85%Children 1 to 24 yr
674 59.05% N/A .89% 38.43%
12-24 months 48025 months-
4 years0
5-9 010-14 215-19 8220-24 101
Unknown 9
124

Tulsa Healthy Start Initiative 2001-2005
FORM 5 Continued NUMBER OF INDIVIDUALS SERVED (UNDUPLICATED) By Type of Individual and Source of Primary Insurance Coverage
For Projects Providing Direct Health Care, Enabling or Population-based ServicesCalendar Year__2002___
Table 3 (a) (b) (c) (d) (e) (f)CSHCN Served
Number Served
Total Served
Title XIX %
Title XXI %
Private/Other %
None %
Infants <1 yr N/A N/A N/A N/A N/AChildren 1 to 24 yr
N/A N/A N/A N/A N/A
12-24 months N/A25 months-
4 yrsN/A
5-9 N/A10-14 N/A20-24 N/A
Table 4 (a) (b) (c) (d) (e) (f)Women Served
Number Served
TotalServed
Title XIX %
Title XXI %
Private/Other %
None%
Women 24+ 151 42.38% N/A .66% 58.28%24-29 8630-34 4335-44 2145-54 155-64 0
65+ 0
Table 5 (a) (b) (c) (d) (e) (f)Other Number
Served TotalServed
Title XIX %
Title XXI %
Private/Other %
None %
N/A N/A N/A N/A N/A N/A
Table 6 (a) (b) (c) (d) (e) (f)TOTA
LNumber Served
TotalServed
Title XIX %
Title XXI %
Private/Other %
None %
1553 68.25% N/A .97% 30.39%
125

Tulsa Healthy Start Initiative 2001-2005
Grantee Name: Tulsa City County Health DepartmentProject Name: Tulsa Healthy Start InitiativeProject Grant #: H49CM00087
FORM 5 NUMBER OF INDIVIDUALS SERVED (UNDUPLICATED) Program Participants* By Type of Individual and Source of Primary Insurance Coverage
For Projects Providing Direct Health Care, Enabling or Population-based Services
Calendar Year___2003_____
Table 1 (a) (b) (c) (d) (e) (f)Pregnant Women Served
Number Served
TotalServed
Title XIX %
Title XXI %
Private/Other %
None%
Pregnant Women (All Ages)
369 65% N/A 3% 33.60%
10-14 515-19 8920-24 12925-34 10835-44 3245 + 0
Unknown 6
Table 2 (a) (b) (c) (d) (e) (f)Children Served
Number Served
Total Served
Title XIX %
Title XXI %
Private/Other %
None %
Infants <1 188 95.20% N/A 1.60% 1.10%Children 1 to 24 yr
644 72.40% N/A 0.60% 11.30%
1-4 4585-9 0
10-14 815-19 7720-24 101
Unknown 0
126

Tulsa Healthy Start Initiative 2001-2005
FORM 5 Continued NUMBER OF INDIVIDUALS SERVED (UNDUPLICATED) By Type of Individual and Source of Primary Insurance Coverage
For Projects Providing Direct Health Care, Enabling or Population-based ServicesCalendar Year__2003___
Table 3 (a) (b) (c) (d) (e) (f)CSHCN Served
Number Served
Total Served
Title XIX %
Title XXI %
Private/Other %
None %
Infants <1 yr 23 87% N/A 0% 0%Children 1 to 22 yr
40 67.50% N/A 2% 4%
1-4 405-9 0
10-14 015-21 0
Table 4 (a) (b) (c) (d) (e)(f)
Women Served
Number Served
TotalServed
Title XIX %
Title XXI %
Private/Other %
None%
Women 22+ 181 44.20% N/A 1.70% 50.80%24-29 5630-34 5935-44 3545-54 2955-64 2
65+ 0
Table 5 (a) (b) (c) (d) (e) (f)Other Number
Served TotalServed
Title XIX %
Title XXI %
Private/Other %
None %
N/A N/A N/A N/A N/A N/A
Table 6 (a) (b) (c) (d) (e) (f)TOTAL Number
Served TotalServed
Title XIX %
Title XXI %
Private/Other %
None %
1445 56.30% N/A 0.69% 20.30%
127

Tulsa Healthy Start Initiative 2001-2005
Grantee Name: Tulsa City County Health DepartmentProject Name: Tulsa Healthy Start InitiativeProject Grant #: H49CM00087
FORM 5NUMBER OF INDIVIDUALS SERVED (UNDUPLICATED) Program Participants*
By Type of Individual and Source of Primary Insurance Coverage
For Projects Providing Direct Health Care, Enabling or Population-based Services
Calendar Year __2004_____
Table 1 (a) (b) (c) (d) (e) (f)PregnantWomenServed
NumberServed
TotalServed
Title XIX%
Title XXI%
Private/Other %
None%
PregnantWomen(All Ages)
318 73.0% na 0.3% 26.7%
10-14 915-19 8020-24 8425-34 11335-44 3245 + 0
Table 2 (a) (b) (c) (d) (e) (f)ChildrenServed
NumberServed
TotalServed
Title XIX%
Title XXI%
Private/Other %
None%
Infants <1 220 94% na 4.1% 1%Children 1 to 2 4 yr
305 81.3% na 5.2% 12.8%
12-24 months 13025 months- 4
years0
5-9 010-14 315-19 6220-24 110
Table 3 (a) (b) (c) (d) (e) (f)
CSHCNServed
NumberServed
TotalServed
Title XIX%
Title XXI%
Private/Other %
None%
Infants <1 yr 14 100 na 0 0Children 1 to 2 4 yr
12 100 na 0 0
12-24 months 1225 months- 4
years0
5-9 010-14 020-24 0
*CSNCN not duplicated in Table 2
128

Tulsa Healthy Start Initiative 2001-2005
FORM 5 ContinuedNUMBER OF INDIVIDUALS SERVED (UNDUPLICATED) Program Participants*
By Type of Individual and Source of Primary Insurance Coverage
For Projects Providing Direct Health Care, Enabling or Population-based Services
Calendar Year __2004_____
Table 4 (a) (b) (c) (d) (e) (f)WomenServed
NumberServed
TotalServed
Title XIX%
Title XXI%
Private/Other %
None%
Women 24+ 111 76.6% na 4.5% 18.9%24-29 5430-34 3235-44 2545-54 055-64 0
65+ 0
Table 5 (a) (b) (c) (d) (e) (f)Other Number
ServedTotal
ServedTitle XIX
%Title XXI
%Private/Other %
None%
NA
Table 6 (a) (b) (c) (d) (e) (f)TOTALS Number
ServedTotal
ServedTitle XIX
%Title XXI
%Private/Other %
None%
980
129

Tulsa Healthy Start Initiative 2001-2005
Grantee Name: Tulsa City County Health DepartmentProject Name: Tulsa Healthy Start InitiativeProject Grant #: H49MC00087
FORM 5 NUMBER OF INDIVIDUALS SERVED (UNDUPLICATED) Program Participants* By Type of Individual and Source of Primary Insurance Coverage
For Projects Providing Direct Health Care, Enabling or Population-based Services
Calendar Year_ January – June 2005
Table 1 (a) (b) (c) (d) (e) (f)Pregnant Women Served
Number Served
TotalServed
Title XIX %
Title XXI %
Private/Other %
None%
Pregnant Women (All Ages)
247 60.7% N/A 0.4% 40%
10-14 515-19 5820-24 4925-34 6835-44 2745 + 0
Unknown 2
Table 2 (a) (b) (c) (d) (e) (f)Children Served
Number Served
Total Served
Title XIX %
Title XXI %
Private/Other %
None %
Infants <1 37 91.9% N/A 2.7% 0%Children 1 to 24 yr
215 80.0% N/A .9% 19.1%
12-24 months 8725 months-
4 years0
5-9 010-14 315-19 5120-23 74
Unknown 0
* Children and Interconceptional Women Under Age 24
130

Tulsa Healthy Start Initiative 2001-2005
FORM 5 Continued NUMBER OF INDIVIDUALS SERVED (UNDUPLICATED) By Type of Individual and Source of Primary Insurance Coverage
For Projects Providing Direct Health Care, Enabling or Population-based ServicesCalendar Year_ January – June 2005
Table 3 (a) (b) (c) (d) (e) (f)CSHCN Served
Number Served
Total Served
Title XIX %
Title XXI %
Private/Other %
None %
Infants <1 yr 13 100% N/A 0% 0%Children 1 to 24 yr
18 88.9% N/A 0% 5.5%
12-24 months 025 months-
4 yrs0
5-9 010-14 020-24 0
Table 4 (a) (b) (c) (d) (e) (f)Women Served
Number Served
TotalServed
Title XIX %
Title XXI %
Private/Other %
None%
Women 24+ 90 56.7% N/A 0 43.3%24-29 4730-34 2535-44 1845-54 055-64 0
65+ 0 * Interconceptional Women Over Age 23
Table 5 (a) (b) (c) (d) (e) (f)Other Number
Served TotalServed
Title XIX %
Title XXI %
Private/Other %
None %
N/A N/A N/A N/A N/A N/A
Table 6 (a) (b) (c) (d) (e) (f)TOTAL
SNumber Served
TotalServed
Title XIX %
Title XXI %
Private/Other %
None %
620 70.3% N/A .6% 29.4
131

Tulsa Healthy Start Initiative 2001-2005
MCHB PROJECT BUDGET DETAILS FOR Budget Year (BY)2001-2005
132

Tulsa Healthy Start Initiative 2001-2005
133

Tulsa Healthy Start Initiative 2001-2005
Project Name: Tulsa Healthy Start Initiative City: Tulsa Project Grant #: H49MC00087 State: Oklahoma
DIVISION OF HEALTHY START AND PERINATAL SERVICES DATA SHEET Section A. Characteristics of Program Participants Page 1 - July - December 2001
Race (Indicate all that apply) ETHNICITYCharacteristics of Program Participants Page 1 of 3
American Indian
or Alaska Native
Asian Black or African America
n
Native Hawaiia
n or Other Pacific
Islander
Caucasian Unknown Total Hispanic or
Latino
Not Hispanic or Latino
Unknown Total
a. Number of Pregnant Women
Under age 15 0 0 3 0 2 0 5 1 4 0 5Aged 15-17 5 0 9 4 25 3 46 22 22 2 46Aged 18-19 12 0 14 0 39 1 66 22 43 1 66Aged 20-23 20 2 42 1 59 1 125 24 98 3 125Aged 24-34 16 0 34 0 106 4 160 65 88 7 160Aged 35-44 0 0 3 0 16 0 19 12 7 0 19
45+ 0 0 0 0 1 0 1 1 0 0 1Unknown Age 6 0 3 0 8 0 17 12 5 0 17
Total # of Pregnant Women 59 2 108 5 256 9 439 159 267 13 439
b. Number of Pregnant Women with Incomes:
Below 100 Percent Of the FPL 21 0 35 2 59 3 120 27 85 8 120
Between 100-185 Percent
Of the FPL 10 0 13 1 29 2 55 31 1 9 55c. Number of Pregnant Participants who Enter Prenatal Care:
During First Trimester 14 0 45 2 98 4 163 39 122 2 163During Second
Trimester 26 1 42 2 118 3 192 86 101 5 192
122

Tulsa Healthy Start Initiative 2001-2005
During Third Trimester 6 1 9 1 21 2 40 19 18 3 40
Receiving No Prenatal Care 0 0 0 0 0 0 0 0 0 0 0
Unknown 13 0 12 0 19 0 44 15 26 3 44Total 59 2 108 5 256 9 439 159 267 13 439
DIVISION OF HEALTHY START AND PERINATAL SERVICES DATA SHEET
Section A. Characteristics of Program Participants Page 2 -July - December 2001
Characteristics of Program Participants Page 2 of 3
American Indian
or Alaska Native
Asian Black or African America
n
Native Hawaiia
n or Other Pacific
Islander
Caucasian Unknown Total Hispanic or
Latino
Not Hispanic or Latino
Unknown Total
d. Adequate Prenatal Care
Number Pregnant Participants Receiving
Adequate Prenatal Care (Kotelchuck1,or
similar index)
3 1 19 1 52 1 77 36 38 3 77
Level of Adequate
Prenatal Care Unknown 0 0 4 0 3 0 7 3 4 0 7
e. Live Singleton Births to Participants
Number of live births to participants 17 1 37 2 112 3 172 76 92 4 172
Number of live singleton births
between 2499grams and 1500 grams to
program participants 0 0 2 0 3 1 6 2 3 1 6
123

Tulsa Healthy Start Initiative 2001-2005
Number of live singleton births less than 1499
grams to program participants 0 0 2 0 1 1 4 1 3 0 4
G. Infant/Child Health
ParticipantsProject Name: Tulsa Healthy Start Initiative City: TulsaProject Grant #: H49MC00087 State: Oklahoma
DIVISION OF HEALTHY START AND PERINATAL SERVICES DATA SHEET
Section A. Characteristics of Program Participants Page 3 - July - December 2001Characteristics of Program Participants Page 3 of 3
Race (Indicate all that apply) ETHNICITYAmeric
an Indian
or Alaska Native
Asian Black or
African Americ
an
Native Hawaiian or Other Pacific Islande
r
Caucasian
Unknown
Total Hispanic or Latino
Not Hispanic or Latino
Unknown Total
f. Number of Program Participates in Interconceptional Care/Women's Health Activities
Under age 15 0 0 2 0 0 0 2 0 2 0 2Aged 15-17 3 0 10 0 13 0 26 7 19 0 26Aged 18-19 6 0 10 0 30 1 47 19 27 1 47Aged 20-23 4 0 11 0 44 5 64 35 28 1 64Aged 24-34 3 3 13 1 52 2 74 46 28 0 74Aged 35-44 0 0 1 0 11 1 13 8 5 0 13 Aged 45 + 0 0 0 0 0 0 0 0 0 0 0
Unknown Age 1 0 2 0 2 0 5 1 4 0 5
125

Tulsa Healthy Start Initiative 2001-2005
Total 17 3 49 1 152 9 231 116 113 2 231g. Infant/Child Health Participants
Number of Infant Participants Aged 0 to 11 months 12 1 34 0 84 35 166 82 71 13 166Number of Child Participants aged 12 to 23 months 18 5 68 0 216 46 353 185 149 19 353
Total 30 6 102 0 300 81 519 267 220 32 519h. Male Support Services Participants
Number of Male Participants 17 years and under NA NANumber of Male Participants 18 years and older NA NA
Total NA NA
126

Tulsa Healthy Start Initiative 2001-2005
Project Name: Tulsa Healthy Start Initiative City: Tulsa Project Grant #: H49CM00087 State: Oklahoma
DIVISION OF HEALTHY START AND PERINATAL SERVICES DATA SHEET Section A. Characteristics of Program Participants Page 1 - 2002
Race (Indicate all that apply) ETHNICITYCharacteristics of Program Participants Page 1 of 3
American Indian or
Alaska Native
Asian Black or African
American
Native Hawaiian or Other Pacific
Islander
Caucasian Unknown Total Hispanic or Latino
Not Hispanic or
Latino
Unknown Total
a. Number of Pregnant Women
Under age 15 1 0 2 0 4 0 7 3 4 0 7Aged 15-17 14 0 20 1 35 1 71 15 56 0 71Aged 18-19 7 0 21 0 38 0 66 15 49 2 66Aged 20-23 22 1 50 2 59 0 134 29 98 7 134Aged 24-34 22 1 60 0 93 0 176 55 99 22 176Aged 35-44 3 0 8 0 26 1 38 20 10 8 38
45+ 0 0 0 0 1 0 1 0 0 1 1Unknown Age 6 0 5 0 5 0 16 7 8 1 16
Total # of Pregnant Women 75 2 166 3 261 2 509 144 324 41 509
b. Number of Pregnant Women with Incomes:
Below 100 Percent of the FPL 28 1 89 2 132 3 255 75 153 27 255Between 100-185 Percent of the FPL 10 0 16 1 49 0 76 33 37 6 76
c. Number of Pregnant Participants who
127

Tulsa Healthy Start Initiative 2001-2005
Enter Prenatal Care:During First Trimester 28 1 55 0 79 1 164 29 128 7 164
During Second Trimester 36 0 82 2 134 1 255 83 148 24 255
During Third Trimester 9 1 22 1 39 0 72 27 36 9 72
Receiving No Prenatal Care 0 0 0 0 0 0 0 0 0 0 0
Unknown 2 0 7 0 9 0 18 5 12 1 18Total
75 2 166 3 261 2 509 144 324 41 509
DIVISION OF HEALTHY START AND PERINATAL SERVICES DATA SHEET Section A. Characteristics of Program Participants Page 2 -2002
Characteristics of Program Participants Page 2 of 3
American Indian or
Alaska Native
Asian Black or African
American
Native Hawaiian or Other Pacific
Islander
Caucasian Unknown Total Hispanic or Latino
Not Hispanic or
Latino
Unknown Total
d. Adequate Prenatal Care
Number Pregnant Participants Receiving
Adequate Prenatal Care (Kotelchuck1,or
similar index) 1 0 18 0 28 0 47 18 24 5 47
Level of Adequate Prenatal Care
Unknown 0 0 0 0 0 0 0 0 0 0 0e. Live Singleton Births to Participants
Number of live births to participants 30 1 80 0 126 1 238 65 154 19 238
128

Tulsa Healthy Start Initiative 2001-2005
Number of live singleton births
between 2499grams and 1500 grams to
program participants3 0 11 0 14 0 28 6 20 2 28
Number of live singleton births less than 1499 grams to
program participants 0 0 4 0 3 0 7 2 5 0 7
G. Infant/Child Health Participants
Project Name: Tulsa Healthy Start Initiative City: TulsaProject Grant #: H49CM00087 State: Oklahoma
DIVISION OF HEALTHY START AND PERINATAL SERVICES DATA SHEET
Section A. Characteristics of Program Participants Page 3 - 2002Characteristics of Program Participants Page 3 of 3
Race (Indicate all that apply) ETHNICITYAmerican Indian
or Alaska Native
Asian Black or African
American
Native Hawaiian or Other Pacific
Islander
Caucasian Unknown Total Hispanic or Latino
Not Hispanic or
Latino
Unknown Total
f. Number of Program Participates in Interconceptional Care/Women's Health Activities
Under age 15 0 0 2 0 0 0 2 0 2 0 2Aged 15-17 2 0 13 1 16 0 32 10 21 1 32Aged 18-19 5 0 13 0 31 1 50 24 26 0 50Aged 20-23 6 1 12 0 59 3 81 45 36 0 81Aged 24-34 6 3 20 0 95 5 129 74 52 3 129Aged 35-44 1 0 0 0 19 1 21 15 6 0 21 Aged 45 + 0 0 0 0 1 0 1 1 0 0 1
Unknown Age 3 0 0 3 3 0 9 2 7 9
129
Tulsa Healthy Start Initiative 2001-2005
Total 23 4 60 4 224 10 325 171 150 4 325g. Infant/Child Health Participants
Number of Infant Participants Aged 0 to 11 months 27 1 70 0 70 51 219 66 130 23 219Number of Child Participants aged 12 to 23 months 41 5 116 0 221 97 480 206 233 41 480
Total 68 6 186 0 291 148 699 272 363 64 699h. Male Support Services Participants
Number of Male Participants 17 years and under NA Number of Male Participants 18 years and older NA
Total NA
130
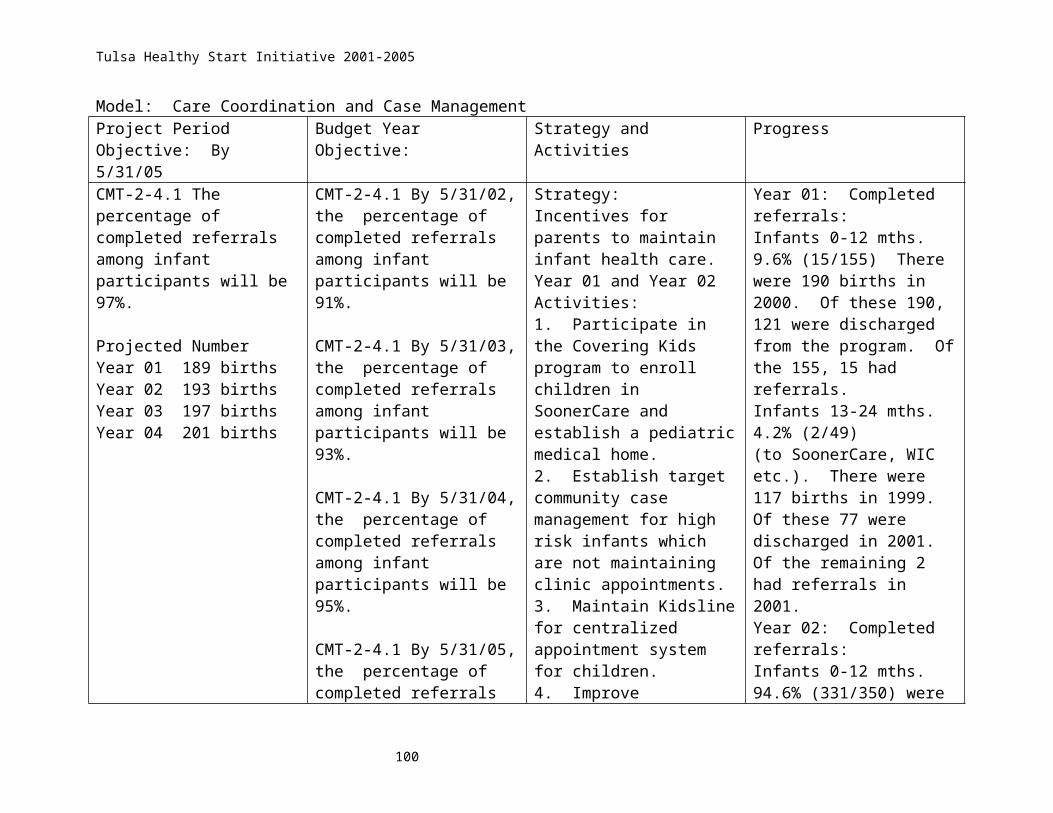
Tulsa Healthy Start Initiative 2001-2005
Project Name: Tulsa Healthy Start Initiative City: Tulsa Project Grant #: H49CM00087 State: Oklahoma
DIVISION OF HEALTHY START AND PERINATAL SERVICES DATA SHEET Section A. Characteristics of Program Participants Page 1 - 2003
Race (Indicate all that apply) ETHNICITYCharacteristics of Program Participants Page 1 of 3
American Indian
or Alaska Native
Asian Black or African America
n
Native Hawaiia
n or Other Pacific
Islander
Caucasian
Unknown Total Hispanic or
Latino
Not Hispanic or Latino
Unknown Total
a. Number of Pregnant Women
Under age 15 1 0 1 0 5 0 7 1 5 1 7Aged 15-17 14 0 7 0 16 0 37 9 28 0 37Aged 18-19 6 0 15 0 31 0 52 17 35 0 52Aged 20-23 25 1 54 3 45 1 129 30 90 9 129Aged 24-34 12 0 38 0 58 0 108 33 54 21 108Aged 35-44 4 0 8 0 20 0 32 12 14 6 32
45+ 0 0 0 0 0 0 0 0 0 0 0Unknown Age 0 0
Total # of Pregnant Women 62 1 123 3 175 1 365 102 226 37 365
b. Number of Pregnant Women with Incomes:
Below 100 Percent of the FPL 34 0 102 3 137 21 297 78 163 56 297
Between 100-185 Percent
of the FPL 2 4 11 0 20 0 37 14 23 0 37c. Number of Pregnant Participants who
131

Tulsa Healthy Start Initiative 2001-2005
Enter Prenatal Care:During First Trimester 25 1 41 1 58 0 126 32 83 11 126
During Second Trimester 19 0 65 2 88 1 175 51 105 18 174
During Third Trimester 6 0 11 0 23 0 40 16 17 7 40
Receiving No Prenatal Care 0 0 0 0 0 0 0 0 0 0 0
Unknown 12 0 6 0 6 0 24 3 21 1 25Total
62 1 123 3 175 1 365 102 226 37 365
DIVISION OF HEALTHY START AND PERINATAL SERVICES DATA SHEET Section A. Characteristics of Program Participants Page 2 - 2003
Characteristics of Program Participants Page 2 of 3
American Indian
or Alaska Native
Asian Black or African America
n
Native Hawaiia
n or Other Pacific
Islander
Caucasian
Unknown Total Hispanic or
Latino
Not Hispanic or Latino
Unknown Total
d. Adequate Prenatal Care
Number Pregnant Participants Receiving
Adequate Prenatal Care (Kotelchuck1,or
similar index) 6 0 16 0 23 0 45 12 29 4 45
Level of Adequate Prenatal Care
Unknown 0 0 0 0 0 0 0 0 0 0 0e. Live Singleton Births to Participants
Number of live births to participants 22 1 69 3 85 0 180 41 122 17 180
132

Tulsa Healthy Start Initiative 2001-2005
Number of live singleton births
between 2499grams and 1500 grams to
program participants4 0 4 0 10 2 20 6 12 2 20
Number of live singleton births less than 1499 grams to
program participants 0 0 0 0 0 0 0 0 0 0 0
G. Infant/Child Health Participants
Project Name: Tulsa Healthy Start Initiative City: TulsaProject Grant #: H49MC00087 State: Oklahoma
DIVISION OF HEALTHY START AND PERINATAL SERVICES DATA SHEET
Section A. Characteristics of Program Participants Page 3 - 2003Characteristics of Program Participants Page 3 of 3
Race (Indicate all that apply) ETHNICITYAmerican Indian
or Alaska Native
Asian Black or African America
n
Native Hawaiia
n or Other Pacific
Islander
Caucasian
Unknown Total Hispanic or
Latino
Not Hispanic or Latino
Unknown Total
f. Number of Program Participates in Interconceptional Care/Women's Health Activities
Under age 15 4 0 8 0 8 0 20 4 15 1 20Aged 15-17 10 0 20 2 34 0 66 17 49 0 66Aged 18-19 8 0 24 0 52 0 84 25 57 2 84Aged 20-23 24 2 75 3 90 0 194 59 125 10 194Aged 24-34 13 2 48 0 121 1 185 74 91 20 185Aged 35-44 2 0 9 0 41 1 53 29 17 7 53 Aged 45 + 0 0 1 0 1 0 2 1 0 1 2
Unknown Age 0 0
133

Tulsa Healthy Start Initiative 2001-2005
Total 61 4 185 5 347 2 604 209 354 41 604g. Infant/Child Health Participants
Number of Infant Participants Aged 0 to 11 months 22 1 72 3 69 23 190 52 116 22 190Number of Child Participants aged 12 to 23 months 31 3 216 6 189 15 460 211 214 35 460
Total 53 4 288 9 258 38 650 263 330 57 650h. Male Support Services Participants
Number of Male Participants 17 years and under 0 0 0 0 0 0 0 0 0 0 0Number of Male Participants 18 years and older 0 0 0 0 0 0 0 0 0 0 0
Total 0 0 0 0 0 0 0 0 0 0 0
134

Tulsa Healthy Start Initiative 2001-2005
Project Name: Tulsa Healthy Start City: Tulsa Project Grant #: H49CM00087 State: Oklahoma
DIVISION OF PERINATAL SYSTEMS AND WOMEN’S HEALTH DATA SHEET Section A. Characteristics of Program Participants Page 1 2004
Race (Indicate all that apply) ETHNICITYCharacteristics of Program Participants Page 1 of 3
American
Indian or
Alaska Native
Asian Black or
African Americ
an
Native Hawaiia
n or Other Pacific Islande
r
Caucasian
Unknown
Total Hispanic or
Latino
Not Hispanic or Latino
Unknown Total
a. Number of Pregnant Women
Under age 15 1 0 2 1 5 0 9 4 5 0 9Aged 15-17 11 0 7 0 21 0 39 15 22 2 39Aged 18-19 9 0 10 0 22 0 41 15 26 0 41Aged 20-23 16 0 25 0 43 0 84 24 57 3 84Aged 24-34 15 0 37 2 57 2 113 41 70 2 113Aged 35-44 3 0 5 1 23 0 32 13 17 2 32
45+ 0 0 0 0 0 0 0 0 0 0 0Total # of
Pregnant Women 55 0 86 4 171 2 318 112 197 9 318b. Number of Pregnant Women with Incomes:
Below 100 Percent 44 0 79 3 138 2 266 87 170 9 266of the FPL .
Between 100-185 Percent 9 0 3 0 27 0 39 25 14 0 39
of the FPL
135

Tulsa Healthy Start Initiative 2001-2005
c. Number of Pregnant Participants who Enter Prenatal Care:
During First Trimester 22 0 22 0 39 0 83 22 60 1 83
During Second Trimester 29 0 51 1 95 2 178 67 107 4 178
During Third Trimester 4 0 11 2 35 0 52 21 21 3 52
Receiving No Prenatal Care 0 0 0 0 0 0 0 0 0 0 0
Unknown 0 0 2 1 2 0 5 2 2 1 5Total 55 0 86 4 171 2 318 112 197 9 318
DIVISION OF PERINATAL SYSTEMS AND WOMEN’S HEALTH DATA SHEET
Section A. Characteristics of Program Participants Page 2 2004
Characteristics of Program Participants Page 2 of 3
American
Indian or
Alaska Native
Asian Black or
African Americ
an
Native Hawaiian or Other Pacific Islande
r
Caucasian
Unknown
Total Hispanic or Latino
Not Hispanic or Latino
Unknown Total
d. Adequate Prenatal Care
Number Pregnant Participants
Receiving Adequate Prenatal
Care (Kotelchuck1,or
similar index)
2 0 6 0 11 0 19 5 14 0 19
Level of Adequate 0 0 0 0 0 0 0 0 0 0 0
136

Tulsa Healthy Start Initiative 2001-2005
Prenatal Care Unknown
e. Live Singleton Births to Participants
Number of live births to
participants 16 0 32 1 74 0 123 46 72 5 123Number of live
singleton births between
2499grams and 1500 grams to
program participants 1 0 8 0 4 0 13 4 9 0 13
Number of live singleton births less than 1499
grams to program participants 0 0 0 0 0 0 0 0 0 0 0
Project Name: Tulsa Healthy Start City: Tulsa Project Grant #: H49CM00087 State: Oklahoma DIVISION OF PERINATAL SYSTEMS AND WOMEN’S HEALTH DATA SHEET
Section A. Characteristics of Program Participants Page 3 2004Characteristics of Program Participants Page 3 of 3
Race (Indicate all that apply) ETHNICITYAmeric
an Indian
or Alaska Native
Asian Black or
African Americ
an
Native Hawaiian or Other Pacific Islande
r
Caucasian
Unknown
Total Hispanic or Latino
Not Hispanic or Latino
Unknown Total
f. Number of Program Participants in Interconception
137
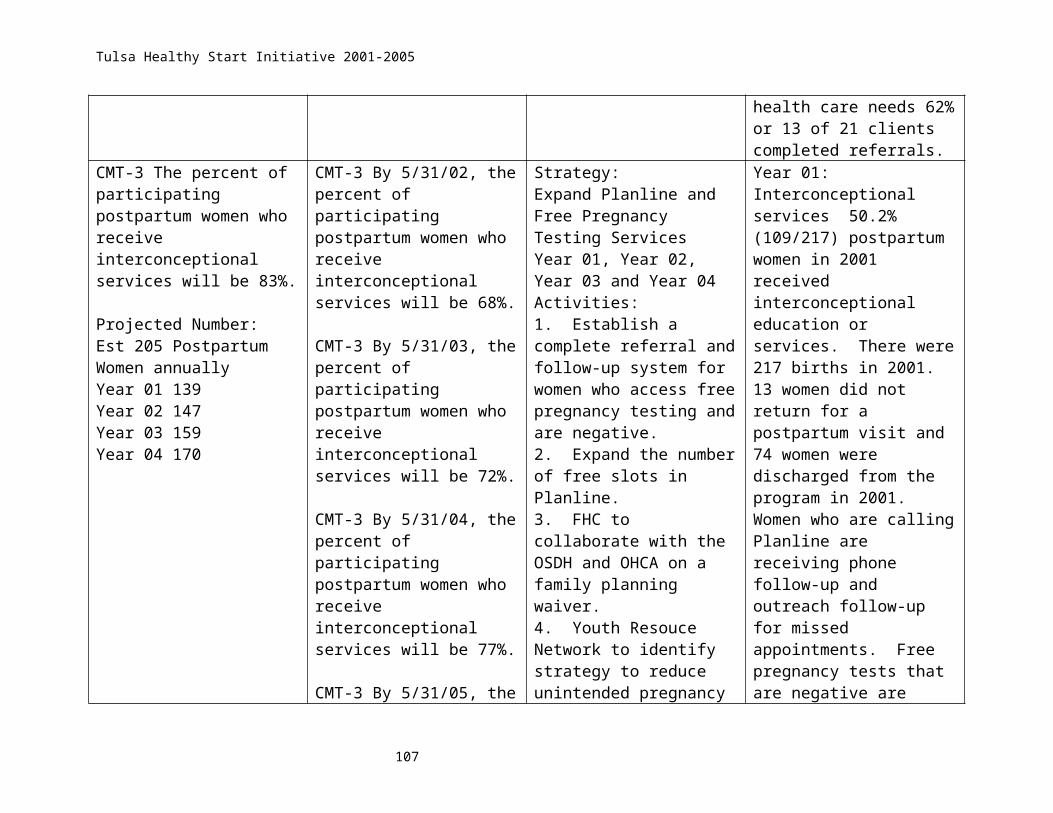
Tulsa Healthy Start Initiative 2001-2005
al Care/Women's Health Activities
Under age 15 0 0 1 0 2 0 3 1 2 0 3Aged 15-17 7 0 7 0 17 0 31 7 24 0 31Aged 18-19 4 0 7 0 20 0 31 7 24 0 31Aged 20-23 15 1 36 2 31 0 85 17 68 0 85Aged 24-34 13 0 38 0 60 0 111 37 74 0 111Aged 35-44 1 0 8 0 15 1 25 12 13 0 25 Aged 45 + 0 0 0 0 0 0 0 0 0 0 0
Total 40 1 97 2 145 1 286 81 205 0 286g. Infant/Child Health Participants
Number of Infant Participants Aged 0 to 11 months 38 3 81 0 88 24 234 72 151 11 234Number of Child Participants aged 12 to 23 months 30 1 44 0 47 20 142 36 100 6 142
Total 68 4 125 0 135 44 376 109 251 17 376h. Male Support Services Participants
Number of Male Participants 17 years and under 0 0 0Number of Male Participants 18 years and older 0 0 0
Total 0 0 0
138

Tulsa Healthy Start Initiative 2001-2005
Project Name:Tulsa Healthy Start Initiative City: Tulsa
Project Grant #: H49CM00087 State: Oklahoma
DIVISION OF HEALTHY START AND PERINATAL SERVICES DATA SHEET Section A. Characteristics of Program Participants Page 1 - Jan - June 2005
Race (Indicate all that apply) ETHNICITYCharacteristics of Program Participants Page 1 of 3
American
Indian or
Alaska Native
Asian Black or African America
n
Native Hawaiian or Other Pacific Islande
r
Caucasian
Unknown
Total Hispanic or
Latino
Not Hispanic or Latino
Unknown Total
a. Number of Pregnant Women
Under age 15 0 0 3 0 2 0 5 2 3 0 5Aged 15-17 8 0 6 0 13 3 30 8 16 6 30Aged 18-19 6 0 8 0 14 0 28 9 19 0 28Aged 20-23 7 0 22 0 36 1 66 13 50 3 66Aged 24-34 16 0 30 0 40 3 89 29 59 1 89Aged 35-44 2 0 3 0 21 1 27 10 16 1 27
45+ 0 0 0 0 0 0 0 0 0 0 0Unknown Age 0 0 0 0 2 0 2 2 0 0 2
Total # of Pregnant Women 39 0 72 0 128 8 247 73 163 11 247
b. Number of Pregnant Women with Incomes:
Below 100 Percent of the FPL 32 0 64 0 99 5 200 52 143 5 200
Between 100-185
139
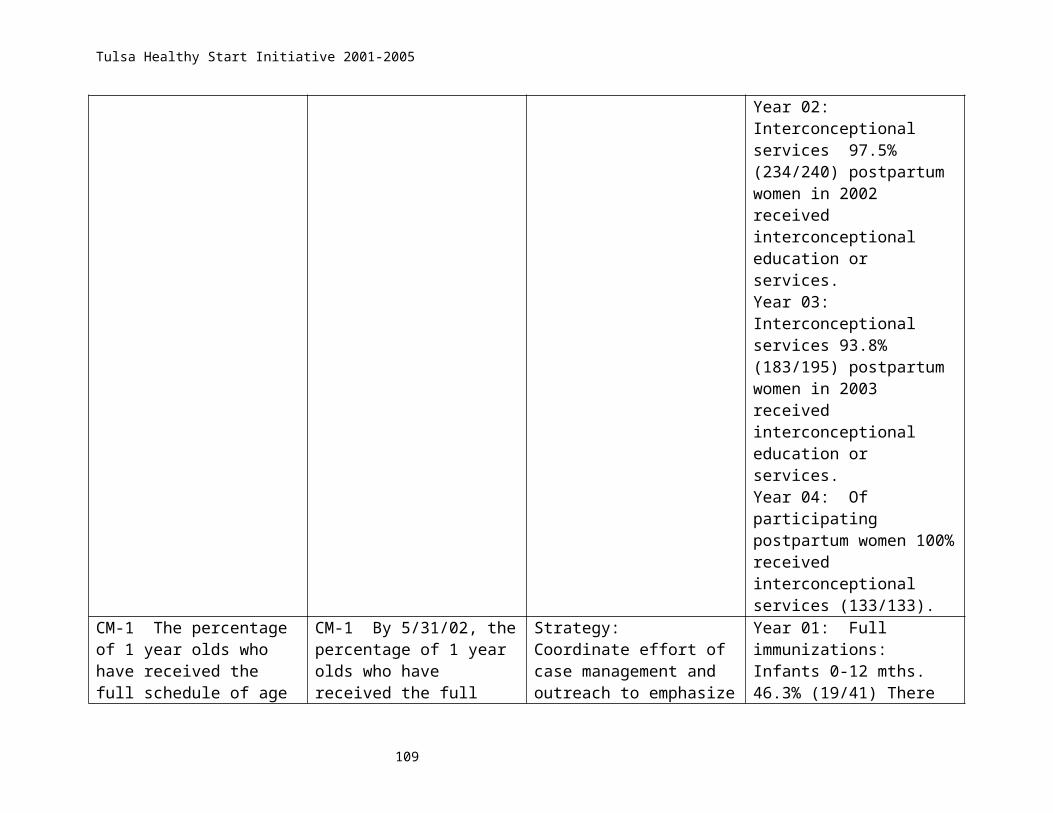
Tulsa Healthy Start Initiative 2001-2005
Percentof the FPL 2 0 3 0 22 0 27 20 7 0 27
c. Number of Pregnant Participants who Enter Prenatal Care:
During First Trimester 13 0 22 0 33 0 68 14 53 1 68
During Second Trimester 23 0 41 0 73 4 141 48 91 2 141
During Third Trimester 1 0 7 0 20 1 29 10 17 2 29
Receiving No Prenatal Care 0 0 0 0 0 0 0 0 0 0 0
Unknown 0 0 2 0 1 6 9 0 2 7 9Total 37 0 72 0 127 11 247 72 163 12 247
DIVISION OF HEALTHY START AND PERINATAL SERVICES DATA SHEET
Section A. Characteristics of Program Participants Page 2 - Jan - June 2005
Characteristics of Program Participants Page 2 of 3
American
Indian or
Alaska Native
Asian Black or African America
n
Native Hawaiian or Other Pacific Islande
r
Caucasian
Unknown
Total Hispanic or
Latino
Not Hispanic or Latino
Unknown Total
d. Adequate Prenatal Care
Number Pregnant Participants
Receiving Adequate Prenatal
Care (Kotelchuck1,or
2 0 9 0 12 2 25 3 20 2 25
140

Tulsa Healthy Start Initiative 2001-2005
similar index)Level of Adequate
Prenatal Care Unknown 1 0 2 0 2 0 5 1 4 0 5
e. Live Singleton Births to Participants
Number of live births to
participants 7 0 11 1 19 3 41 11 28 2 41Number of live
singleton births between
2499grams and 1500 grams to
program participants 1 0 1 0 3 0 5 2 3 0 5
Number of live singleton births less than 1499
grams to program participants 0 0 2 0 1 0 3 1 2 0 3
G. Infant/Child Health
ParticipantsProject Name: Tulsa Healthy Start Initiative City: TulsaProject Grant #: H49CM00087 State: Oklahoma
DIVISION OF HEALTHY START AND PERINATAL SERVICES DATA SHEET
Section A. Characteristics of Program Participants Page 3 - Jan - June 2005Characteristics of Program Participants Page 3 of 3
Race (Indicate all that apply) ETHNICITYAmeric
an Indian
or Alaska Native
Asian Black or African America
n
Native Hawaiian or Other Pacific Island
Caucasian
Unknown
Total Hispanic or
Latino
Not Hispanic or Latino
Unknown Total
141
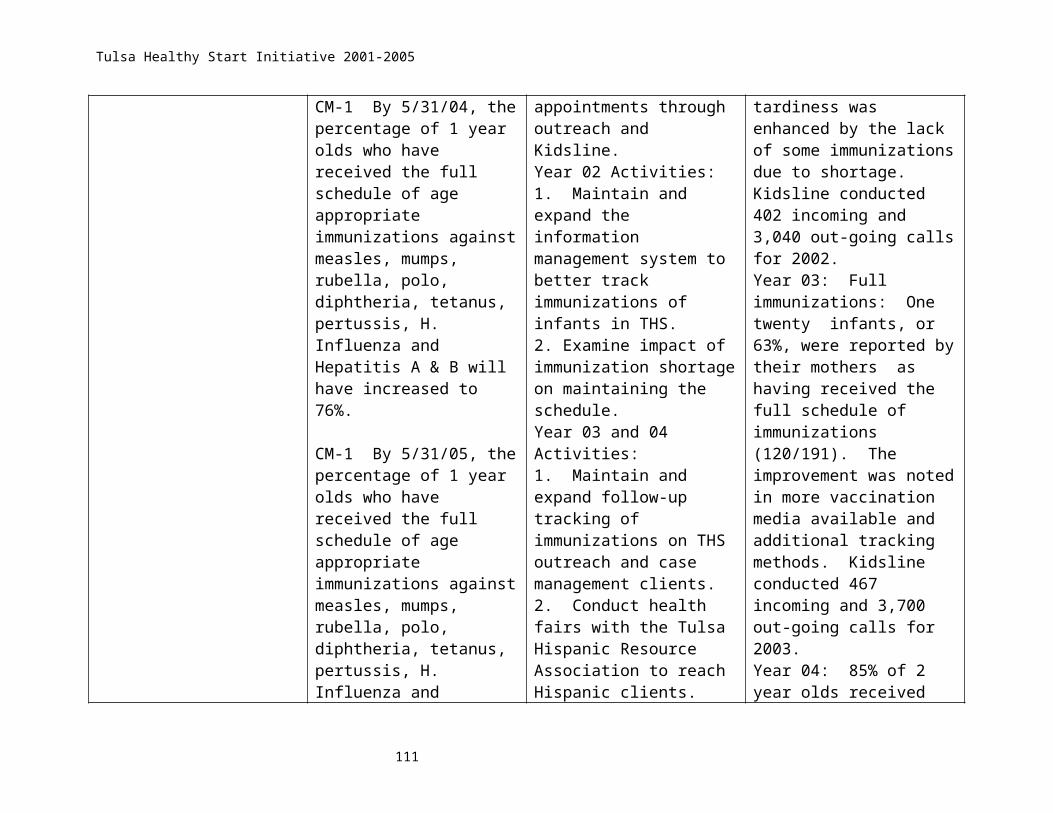
Tulsa Healthy Start Initiative 2001-2005
erf. Number of Program Participates in Interconceptional Care/Women's Health Activities
Under age 15 0 0 1 0 2 0 3 1 2 0 3Aged 15-17 4 0 5 0 13 1 23 9 13 1 23Aged 18-19 4 0 6 0 17 1 28 10 17 1 28Aged 20-23 11 1 29 2 30 1 74 16 55 3 74Aged 24-34 8 0 25 0 39 0 72 24 40 8 72Aged 35-44 0 0 3 1 14 0 18 11 5 2 18 Aged 45 + 0 0 0 0 0 0 0 0 0 0 0
Unknown Age 0 0 0 0 0 0 0 0 0 0 0Total 27 1 69 3 115 3 218 71 132 15 218
g. Infant/Child Health Participants
Number of Infant Participants Aged 0 to 11 months 6 0 11 0 16 4 37 9 26 2 37Number of Child Participants aged 12 to 23 months 11 2 24 0 45 5 87 38 45 4 87
Total 17 2 35 0 61 9 124 47 71 6 124h. Male Support Services Participants
Number of Male Participants 17 years and under NA NA
142

Tulsa Healthy Start Initiative 2001-2005
Number of Male Participants 18 years and older NA NA
Total NA NA
143

Tulsa Healthy Start Initiative 2001-2005
144

Tulsa Healthy Start Initiative 2001-2005
Project Name: Tulsa Healthy Start InitiativeProject Grant #: H49CM00087City: TulsaState: Oklahoma
B. RISK REDUCTION/PREVENTION SERVICES Page 1
(For Program Participants) July - December 2001
RISK FACTORS Page 1 of 3
Number Screene
d
Number Receiving Risk
Prevention Counseling and/or Risk Reduction Counseling
Number whose
Treatment is
Supported by Grant
Number Referred
for Further Assessmen
t and/or Treatment
a. PRENATAL PROGRAM PARTICIPANTS Group B Strep or Bacterial Vaginosis N/A N/A N/A N/A
HIV/AIDS N/A N/A N/A 2
Other STDs N/A N/A N/A 2
Smoking N/A N/A N/A 4
Alcohol N/A N/A N/A 0
Illicit Drugs N/A N/A N/A 0
Depression N/A N/A N/A 3Other Mental Health Problem N/A N/A N/A 1
Domestic Violence N/A N/A N/A 2
Homelessness N/A N/A N/A N/A
Overweight & Obesity N/A N/A N/A 0
Underweight N/A N/A N/A N/A
Hypertension N/A N/A N/A N/A
Gestational Diabetes N/A N/A N/A 5
Peridontal Infection N/A N/A N/A N/A
143
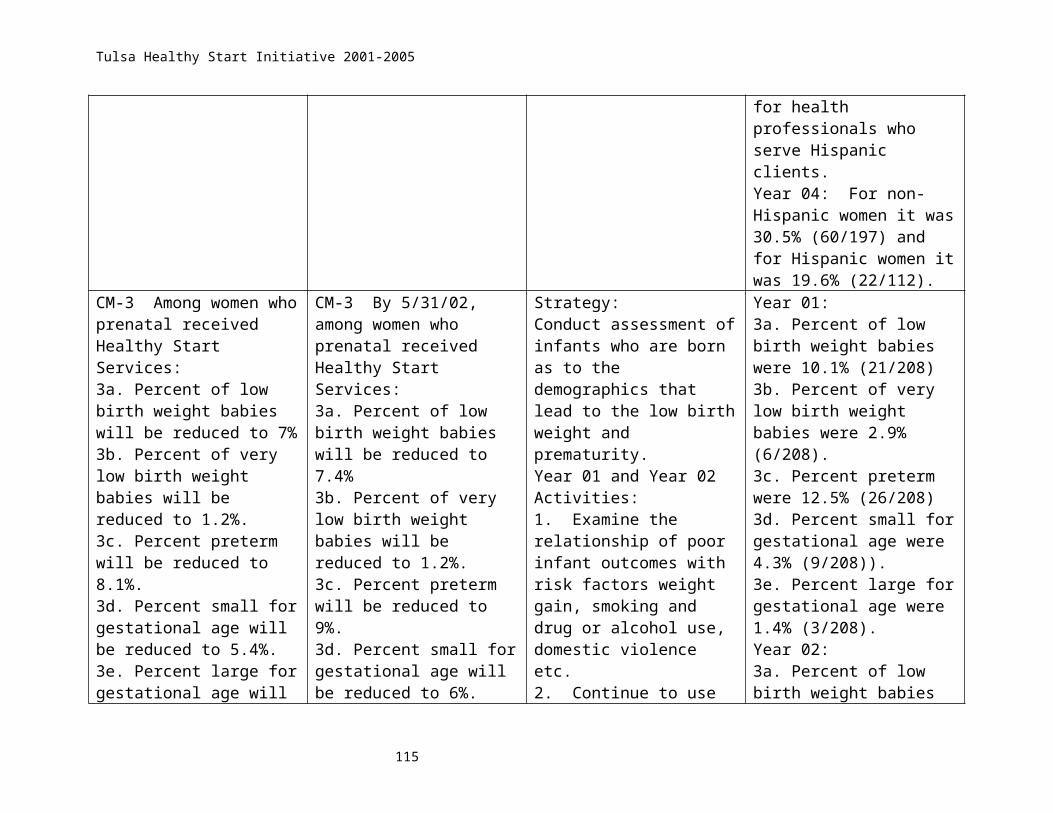
Tulsa Healthy Start Initiative 2001-2005
Asthma N/A N/A N/A N/A Project Name: Tulsa Healthy Start InitiativeProject Grant #: H49CM00087City: Tulsa State: Oklahoma
B. RISK REDUCTION/PREVENTION SERVICES Page 2(For Program Participants) July - December 2001
RISK FACTORS Page 2 of 3
Number Screene
d
Number Receiving Risk
Prevention Counseling and/or Risk Reduction Counseling
Number whose
Treatment is
Supported by Grant
Number Referred
for Further Assessmen
t and/or Treatment
b. INTERCONCEPTIONAL WOMEN PARTICIPANTS Group B Strep or Bacterial Vaginosis N/A N/A N/A N/A
HIV/AIDS N/A N/A N/A 0
Other STDs N/A N/A N/A 0
Smoking N/A N/A N/A 0
Alcohol N/A N/A N/A 0
Illicit Drugs N/A N/A N/A 0
Depression N/A N/A N/A 0Other Mental Health Problem N/A N/A N/A 1
Domestic Violence N/A N/A N/A 3
Homelessness N/A N/A N/A N/A
Overweight & Obesity N/A N/A N/A 0
Underweight N/A N/A N/A N/ALack of Physical Activity N/A N/A N/A N/A
Hypertension N/A N/A N/A N/A
144

Tulsa Healthy Start Initiative 2001-2005
Cholesterol N/A N/A N/A N/A
Diabetes N/A N/A N/A N/AFamily History of Breast Cancer N/A N/A N/A N/A
Fecal occult blood test N/A N/A N/A N/A
Asthma N/A N/A N/A N/A
Peridontal Infection N/A N/A N/A N/A
B. RISK REDUCTION/PREVENTION SERVICES Page 3(For Program Participants) July - December 2001
RISK FACTORS Page 3 of 3
Number Screene
d
Number Receiving Risk
Prevention Counseling and/or Risk Reduction Counseling
Number whose
Treatment is
Supported by Grant
Number Referred
for Further Assessmen
t and/or Treatment
c. INFANT CHILD (0-23 mths) Prenatal Drug Exposure N/A N/A N/A 0Prenatal Alcohol Exposure N/A N/A N/A 0Mental Health Problems N/A N/A N/A N/AFamily Violence Intentional Injury N/A N/A N/A 0
Homelessness N/A N/A N/A N/ANot Attaining Appropriate Growth N/A N/A N/A 14
Developmental Delays N/A N/A N/A N/A
Asthma N/A N/A N/A N/A
HIV/AIDS N/A N/A N/A 0Other Special Health Care Needs N/A N/A N/A N/A
145

Tulsa Healthy Start Initiative 2001-2005
Project Name: Tulsa Healthy Start InitiativeProject Grant #: H49MC00087City: TulsaState: Oklahoma
B. RISK REDUCTION/PREVENTION SERVICES Page 1
(For Program Participants) 2002
RISK FACTORS Page 1 of 3
Number Screene
d
Number Receiving Risk
Prevention Counseling and/or Risk Reduction Counseling
Number whose
Treatment is
Supported by Grant
Number Referred
for Further Assessmen
t and/or Treatment
a. PRENATAL PROGRAM PARTICIPANTS Group B Strep or Bacterial Vaginosis N/A N/A N/A N/A
HIV/AIDS N/A N/A N/A 2
Other STDs N/A N/A N/A 5
Smoking N/A N/A N/A 13
Alcohol N/A N/A N/A 1
Illicit Drugs N/A N/A N/A 4
Depression N/A N/A N/A 7Other Mental Health Problem N/A N/A N/A 5
Domestic Violence N/A N/A N/A 14
Homelessness N/A N/A N/A N/A
Overweight & Obesity N/A N/A N/A 2
Underweight N/A N/A N/A N/A
Hypertension N/A N/A N/A N/A
Gestational Diabetes N/A N/A N/A 10
Peridontal Infection N/A N/A N/A N/A
146

Tulsa Healthy Start Initiative 2001-2005
Asthma N/A N/A N/A N/A Project Name: Tulsa Healthy Start InitiativeProject Grant #: H49CM00087City: Tulsa State: Oklahoma
B. RISK REDUCTION/PREVENTION SERVICES Page 2
(For Program Participants) 2002RISK FACTORS Page 2 of 3
Number Screene
d
Number Receiving Risk
Prevention Counseling and/or Risk Reduction Counseling
Number whose
Treatment is
Supported by Grant
Number Referred
for Further Assessmen
t and/or Treatment
b. INTERCONCEPTIONAL WOMEN PARTICIPANTS Group B Strep or Bacterial Vaginosis N/A N/A N/A N/A
HIV/AIDS N/A N/A N/A 0
Other STDs N/A N/A N/A 2
Smoking N/A N/A N/A 0
Alcohol N/A N/A N/A 0
Illicit Drugs N/A N/A N/A 1
Depression N/A N/A N/A 3Other Mental Health Problem N/A N/A N/A 3
Domestic Violence N/A N/A N/A 0
Homelessness N/A N/A N/A N/A
Overweight & Obesity N/A N/A N/A 1
Underweight N/A N/A N/A N/ALack of Physical Activity N/A N/A N/A N/A
Hypertension N/A N/A N/A N/A
147

Tulsa Healthy Start Initiative 2001-2005
Cholesterol N/A N/A N/A N/A
Diabetes N/A N/A N/A N/AFamily History of Breast Cancer N/A N/A N/A N/A
Fecal occult blood test N/A N/A N/A N/A
Asthma N/A N/A N/A N/A
Peridontal Infection N/A N/A N/A N/A
B. RISK REDUCTION/PREVENTION SERVICES Page 3
(For Program Participants) 2002RISK FACTORS Page 3 of 3
Number Screene
d
Number Receiving Risk
Prevention Counseling and/or Risk Reduction Counseling
Number whose
Treatment is
Supported by Grant
Number Referred
for Further Assessmen
t and/or Treatment
c. INFANT CHILD (0-23 mths) Prenatal Drug Exposure N/A N/A N/A 0Prenatal Alcohol Exposure N/A N/A N/A 0Mental Health Problems N/A N/A N/A N/AFamily Violence Intentional Injury N/A N/A N/A 3
Homelessness N/A N/A N/A N/ANot Attaining Appropriate Growth N/A N/A N/A 15
Developmental Delays N/A N/A N/A N/A
Asthma N/A N/A N/A N/A
HIV/AIDS N/A N/A N/A 0Other Special Health Care Needs N/A N/A N/A N/A
148
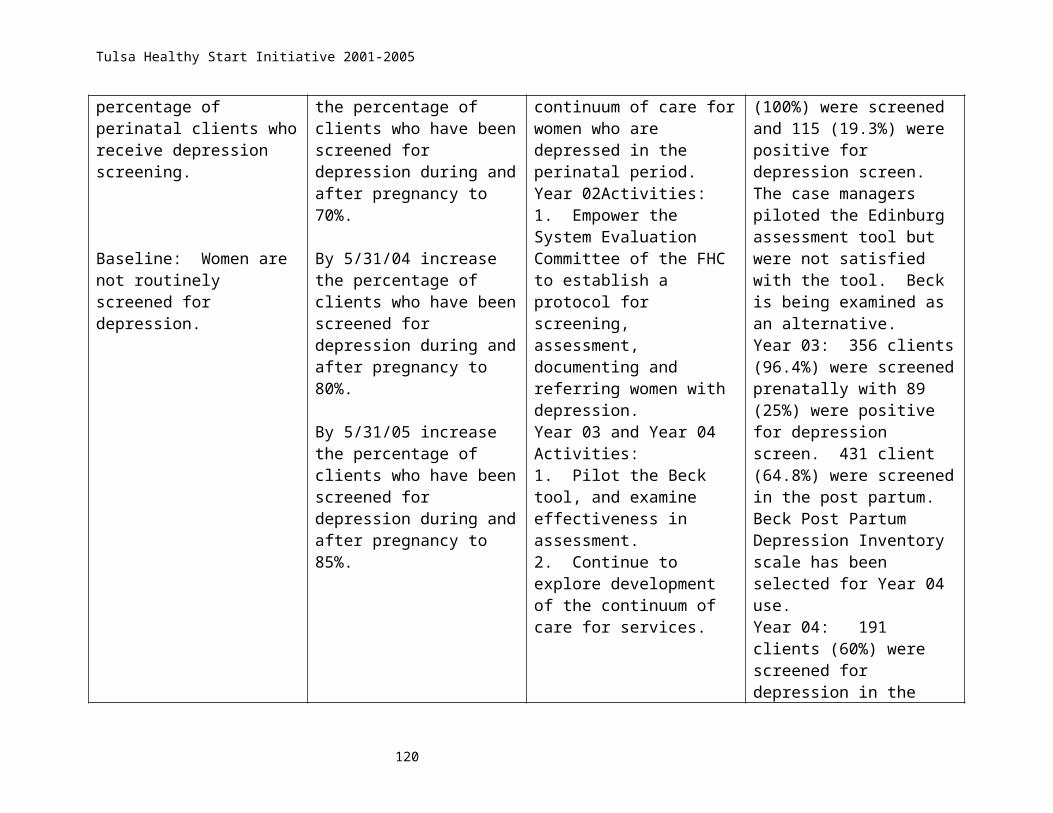
Tulsa Healthy Start Initiative 2001-2005
Project Name: Tulsa Healthy Start InitiativeProject Grant #: H49MC00087City: TulsaState: Oklahoma
RISK REDUCTION/PREVENTION SERVICES 2003
RISK FACTORS Number Screene
d
Number Receiving Risk
Prevention Counseling and/or Risk Reduction Counseling
Number whose
Treatment is
Supported by Grant
Number Referred
for Further Assessmen
t and/or Treatment
PRENATAL PARTICIPANTSGroup B Strep or Bacterial Vaginosis 40 0 0 0
HIV/AIDS 40 0 0 0
Other STDs 40 0 0 0
Smoking 40 0 0 4
Alcohol 40 6 0 0
Illicit Drugs 40 5 0 0
Depression 40 16 0 1Other Mental Health Problem 40 4 0 0
Domestic Violence 40 6 0 1
Homelessness 40 8 0 5
Overweight & Obesity 40 6 0 2
Underweight 40 1 0 0
Hypertension 40 3 0 0
Gestational Diabetes 40 1 0 1
Peridontal Infection 40 0 0 0
Asthma 40 0 0
149

Tulsa Healthy Start Initiative 2001-2005
Project Name: Tulsa Healthy Start InitiativeProject Grant #: H49MC00087City: Tulsa State: Oklahoma
RISK REDUCTION/PREVENTION SERVICES
RISK FACTORS Number Screene
d
Number Receiving Risk
Prevention Counseling and/or Risk Reduction Counseling
Number whose
Treatment is
Supported by Grant
Number Referred
for Further Assessmen
t and/or Treatment
INTERCONCEPTIONAL WOMEN PARTICIPANTSGroup B Strep or Bacterial Vaginosis 26 0 0 0
HIV/AIDS 26 0 0 0
Other STDs 26 1 0 1
Smoking 26 2 0 1
Alcohol 26 0 0 0
Illicit Drugs 26 0 0 0
Depression 26 5 0 0Other Mental Health Problem 26 2 0 0
Domestic Violence 26 3 0 1
Homelessness 26 1 0 1
Overweight & Obesity 26 1 0 1
Underweight 26 0 0 0Lack of Physical Activity 26 3 0 1
Hypertension 26 0 0 0
Cholesterol 26 0 0 0
Diabetes 26 0 0 0Family History of Breast Cancer 26 0 0 0
150

Tulsa Healthy Start Initiative 2001-2005
Fecal occult blood test 26 0 0 0
Asthma 26 0 0 0
Peridontal Infection 26 0 0 0
RISK REDUCTION/PREVENTION SERVICES
RISK FACTORS Number Screene
d
Number Receiving Risk
Prevention Counseling and/or Risk Reduction Counseling
Number whose
Treatment is
Supported by Grant
Number Referred
for Further Assessmen
t and/or Treatment
INFANT CHILD (0-24 mths)Prenatal Drug Exposure 56 0 0 0Prenatal Alcohol Exposure 56 0 0 0Mental Health Problems 56 5 0 0Family Violence Intentional Injury 56 4 0 1
Homelessness 56 0 0 0Not Attaining Appropriate Growth 56 2 0 1
Developmental Delays 56 3 0 0
Asthma 56 1 0 0
HIV/AIDS 56 0 0 0Other Special Health Care Needs 56 2 0 1
151

Tulsa Healthy Start Initiative 2001-2005
Project Name: Tulsa Healthy StartProject Grant #: H49MC00087City: TulsaState: Oklahoma
RISK REDUCTION/PREVENTION SERVICES 2004
RISK FACTORS Number Screene
d
Number Receiving Risk
Prevention Counseling and/or Risk Reduction Counseling
Number whose
Treatment is
Supported by Grant
Number Referred
for Further Assessmen
t and/or Treatment
PRENATAL PARTICIPANTS
NA
Group B Strep or Bacterial Vaginosis 97 31 1
HIV/AIDS 97 45 1
Other STDs 97 58 9
Smoking 183 87 8
Alcohol 183 68 1
Illicit Drugs 183 57 4
Depression 181 95 16Other Mental Health Problem 97 55 7
Domestic Violence 183 76 7
Homelessness 97 46 3
Overweight & Obesity 97 48 1
Underweight 97 45 1
Hypertension 97 56 0
Gestational Diabetes 97 47 5
Peridontal Infection 97 53 9
Asthma 97 42 0
152
Tulsa Healthy Start Initiative 2001-2005
Project Name: Tulsa Healthy StartProject Grant #: H49MC00087City: TulsaState: Oklahoma
RISK REDUCTION/PREVENTION SERVICES
RISK FACTORS Number Screene
d
Number Receiving Risk
Prevention Counseling and/or Risk Reduction Counseling
Number whose
Treatment is
Supported by Grant
Number Referred
for Further Assessmen
t and/or Treatment
INTERCONCEPTIONAL WOMEN PARTICIPANTS NAGroup B Strep or Bacterial Vaginosis 33 2 0
HIV/AIDS 33 2 0
Other STDs 33 12 6
Smoking 133 29 5
Alcohol 133 7 1
Illicit Drugs 133 8 1
Depression 136 123 90Other Mental Health Problem 33 11 2
Domestic Violence 133 18 2
Homelessness 33 2 0
Overweight & Obesity 33 12 2
Underweight 33 5 0Lack of Physical Activity 33 25 1
Hypertension 33 15 2
Cholesterol 33 0 0
Diabetes 33 0 0Family History of Breast Cancer 33 0 1
153
Tulsa Healthy Start Initiative 2001-2005
Fecal occult blood test 33 0 0
Asthma 33 0 0
Peridontal Infection 33 3 2
RISK REDUCTION/PREVENTION SERVICES
RISK FACTORS Number Screene
d
Number Receiving Risk
Prevention Counseling and/or Risk Reduction Counseling
Number whose
Treatment is
Supported by Grant
Number Referred
for Further Assessmen
t and/or Treatment
INFANT CHILD (0-21 mths) NAPrenatal Drug Exposure 48 2 1Prenatal Alcohol Exposure 48 9 0Mental Health Problems 48 3 0Family Violence Intentional Injury 48 10 2
Homelessness 48 4 0Not Attaining Appropriate Growth 48 11 2
Developmental Delays 48 23 6
Asthma 48 12 1
HIV/AIDS 48 1 0Other Special Health Care Needs 48 21 15
154
Tulsa Healthy Start Initiative 2001-2005
Project Name: Tulsa Healthy Start InitiativeProject Grant #: H49CM00087City: TulsaState: Oklahoma
B. RISK REDUCTION/PREVENTION SERVICES Page 1 (For Program Participants) January - June 2005
RISK FACTORS Page 1 of 3
Number Screened
Number Receiving Risk Prevention
Counseling and/or Risk Reduction
Counseling
Number whose
Treatment is Supported by
Grant
Number Referred for
Further Assessment
and/or Treatment
a. PRENATAL PROGRAM PARTICIPANTS Group B Strep or Bacterial Vaginosis 49 25 NA 0
HIV/AIDS 49 17 NA 1
Other STDs 49 28 NA 2
Smoking 72 43 NA 6
Alcohol 72 26 NA 0
Illicit Drugs 72 28 NA 3
Depression 71 40 NA 12Other Mental Health Problem 49 25 NA 2
Domestic Violence 72 32 NA 7
Homelessness 49 15 NA 2
Overweight & Obesity 49 20 NA 0
Underweight 49 18 NA 1
Hypertension 49 28 NA 0
Gestational Diabetes 49 28 NA 1
Peridontal Infection 49 25 NA 3
Asthma 49 11 NA 0
155

Tulsa Healthy Start Initiative 2001-2005
Project Name: Tulsa Healthy Start Initiative
Project Grant #: H49CM00087City: Tulsa State: Oklahoma
B. RISK REDUCTION/PREVENTION SERVICES Page 2(For Program Participants) January - June 2005
RISK FACTORS Page 2 of 3
Number Screened
Number Receiving Risk Prevention
Counseling and/or Risk Reduction
Counseling
Number whose
Treatment is Supported by
Grant
Number Referred for
Further Assessment
and/or Treatment
b. INTERCONCEPTIONAL WOMEN PARTICIPANTS Group B Strep or Bacterial Vaginosis 10 1 NA 0
HIV/AIDS 10 2 NA 0
Other STDs 10 5 NA 0
Smoking 32 14 NA 2
Alcohol 32 4 NA 0
Illicit Drugs 32 2 NA 0
Depression 32 15 NA 9Other Mental Health Problem 10 4 NA 0
Domestic Violence 32 6 NA 0
Homelessness 10 2 NA 1
Overweight & Obesity 10 4 NA 1
Underweight 10 3 NA 0
Lack of Physical Activity 10 7 NA 1
Hypertension 10 5 NA 0
Cholesterol 10 0 NA 0
Diabetes 10 2 NA 0Family History of Breast Cancer 10 3 NA 0
156

Tulsa Healthy Start Initiative 2001-2005
Fecal occult blood test 10 2 NA 0
Asthma 10 2 NA 0
Peridontal Infection 10 6 NA 2
B. RISK REDUCTION/PREVENTION SERVICES Page 3
(For Program Participants) January - June 2005RISK FACTORS Page 3 of 3
Number Screened
Number Receiving Risk Prevention
Counseling and/or Risk Reduction
Counseling
Number whose
Treatment is Supported by
Grant
Number Referred for
Further Assessment
and/or Treatment
c. INFANT CHILD (0-23 mths)
Prenatal Drug Exposure 19 3 NA 0
Prenatal Alcohol Exposure 19 6 NA 0
Mental Health Problems 19 2 NA 0Family Violence Intentional Injury 19 2 NA 0
Homelessness 19 0 NA 0Not Attaining Appropriate Growth 19 4 NA 0
Developmental Delays 19 10 NA 1
Asthma 19 8 NA 1
HIV/AIDS 19 1 NA 0Other Special Health Care Needs 19 16 NA 10
157

Tulsa Healthy Start Initiative 2001-2005
Project Name: Tulsa Healthy Start Initiative Project Grant #: H49CM00087 City: Tulsa State: Oklahoma C. HEALTHY START MAJOR SERVICE TABLE* - July - Dec
2001* When data is collected on both program participant and community participants, please report data separately for each category of participant.
PP=Program Participant CP= Community Participant
a. DIRECT HEALTH CARE SERVICES Prenatal Clinic Visits:
NANumber of Medical Visits
by All Prenatal ParticipantsPostpartum Clinic Visits
NANumber of Medical Visits
by All Postpartum ParticipantsWell Baby/ Pediatric Clinic Visits
NANumber of Any Provider Visitsby All Infant/Child Participants
Adolescent Health Services
NANumber of any Provider Visitsby Participants age 17 and under
Family Planning
pp 194Number of Participants Receiving
Family Planning ServicesWomen’s Health
NANumber of Participants Receiving
Women’s Health Services b. ENABLING SERVICES
Total Number of Families Servedpp 670 cp 695
Number of Families in the Prenatal Period
pp 439
158

Tulsa Healthy Start Initiative 2001-2005
Assisted by Case Management
Number of Families in the Interconceptional Period Assisted by
Case Management pp 231
Number of Families in the Prenatal Period
cp 114Assisted by Outreach
Number of Families in the Interconceptional
cp 122Period Assisted by Outreach
Number of Families in the Prenatal Period pp 35 cp
49Receiving Home Visiting
Number of Families in the Interconceptional pp 72 cp
20Period Receiving Home Visiting
Number of Participants Age 17 and Under who participated in Adolescent Pregnancy
Prevention Activities NA
Number of Families who participated in
cp 0
Pregnancy/Childbirth Education Activities
Number of Families who
participated in
cp 80Parenting Skill
Building/Education
Number of Participants in
NA
Youth Empowerment/Peer Education/
Self-Esteem/Mentor Programs
Number of Families Who Received Transportation Services
159

Tulsa Healthy Start Initiative 2001-2005
Includes Tokens, Taxis and Vans
Number of Families Who Receivepp 69Translation Services
Number of Families Receiving
NAChild Care Services
Number of Participants Who Received
NABreastfeeding Education ,
Counseling and Support
Number of Participants Who Received Nutrition Education
and Counseling Services including WIC Services
pp 280 cp 0
Number of Participants in
NAMale Support Services:
Number of Participants Referred for pp 21
cp 0Housing Assistance
Total Participants assisted with pp 34 cp 23 Jobs/Jobs Training
Total Participants served in
NAPrison/Jail Initiatives
c. POPULATION
Number Of Immunizations NAProvided
Public Information/Education:
cp 1705
Number of Individuals Reached
d. INFRASTRUCTURE BUILDING
160

Tulsa Healthy Start Initiative 2001-2005
Consortia Training
53Number of Individual Members
Trained
Provider Training
654Number of Individual Providers
Trained
161

Tulsa Healthy Start Initiative 2001-2005
Project Name: Tulsa Healthy Start Initiative Project Grant #: H49CM00087 City: Tulsa State: Oklahoma
C. HEALTHY START MAJOR SERVICE TABLE* - 2002* When data is collected on both program participant and community participants, please report data separately for each category of participant.
PP=Program Participant CP= Community Participant
a. DIRECT HEALTH CARE SERVICES Prenatal Clinic Visits:
NANumber of Medical Visits
by All Prenatal ParticipantsPostpartum Clinic Visits
NANumber of Medical Visits
by All Postpartum ParticipantsWell Baby/ Pediatric Clinic Visits
NANumber of Any Provider Visitsby All Infant/Child Participants
Adolescent Health Services
NANumber of any Provider Visitsby Participants age 17 and under
Family Planning
pp 513Number of Participants Receiving
Family Planning ServicesWomen’s Health
NANumber of Participants Receiving
Women’s Health Services b. ENABLING SERVICES
Total Number of Families Servedpp 834 cp 1181
Number of Families in the Prenatal Period
pp 509Assisted by Case Management
162

Tulsa Healthy Start Initiative 2001-2005
Number of Families in the Interconceptional Period Assisted by
Case Management pp 325
Number of Families in the Prenatal Period
cp 315Assisted by Outreach
Number of Families in the Interconceptional
cp 397Period Assisted by Outreach
Number of Families in the Prenatal Period pp 46 cp
338Receiving Home Visiting
Number of Families in the Interconceptional pp77 cp
477Period Receiving Home Visiting
Number of Participants Age 17 and Under who participated in Adolescent Pregnancy
Prevention Activities NA
Number of Families who participated in
cp 65
Pregnancy/Childbirth Education Activities
Number of Families who participated in
cp 825Parenting Skill
Building/Education
Number of Participants in
NA
Youth Empowerment/Peer Education/
Self-Esteem/Mentor Programs
Number of Families Who Received
pp Transportation Services
Includes Tokens, Taxis and Vans
163

Tulsa Healthy Start Initiative 2001-2005
Number of Families Who Receivepp 47Translation Services
Number of Families ReceivingNAChild Care Services
Number of Participants Who Received
NABreastfeeding Education ,
Counseling and Support
Number of Participants Who Received Nutrition Education
and Counseling Services including WIC Services pp 594
Number of Participants inNAMale Support Services:
Number of Participants Referred for pp 76
cp 34Housing Assistance
Total Participants assisted with pp 101 cp 40 Jobs/Jobs Training
Total Participants served inNAPrison/Jail Initiatives
c. POPULATION
Number Of Immunizations NAProvided
Public Information/Education: cp 16,142
Number of Individuals Reached
d. INFRASTRUCTURE BUILDING
Consortia Training 28/200 active members
164

Tulsa Healthy Start Initiative 2001-2005
Number of Individual Members Trained
Provider Training
839Number of Individual Providers
Trained
165

Tulsa Healthy Start Initiative 2001-2005
Project Name: Tulsa Healthy Start InitiativeProject Grant #: H49CM00087City: TulsaState: Oklahoma
C. HEALTHY START MAJOR SERVICE TABLE* 2003* When data is collected on both program participant and community participants, please report data separately for each category of participant.
PP=Program Participant
CP= Community Participant
DIRECT HEALTH CARE SERVICES Prenatal Clinic Visits:
NANumber of Medical Visits
by All Prenatal ParticipantsPostpartum Clinic Visits
NANumber of Medical Visits
by All Postpartum ParticipantsWell Baby/ Pediatric Clinic Visits
NANumber of Any Provider Visitsby All Infant/Child Participants
Adolescent Health Services
NANumber of any Provider Visitsby Participants age 17 and under
Family PlanningPP-201 CP-402
Number of Participants ReceivingFamily Planning Services
Women’s Health
NANumber of Participants Receiving
Women’s Health Services ENABLING SERVICES
Total Number of Families ServedPP-678 CP-1,369
Number of Families in the Prenatal Period
PP-369Assisted by Case Management
166

Tulsa Healthy Start Initiative 2001-2005
Number of Families in the
Interconceptional Period Assisted by Case Management PP-604
Number of Families in the
Prenatal PeriodPP-155Assisted by Outreach
Number of Families in the
InterconceptionalPP-300Period Assisted by Outreach
Number of Families in the
Prenatal PeriodPP-85Receiving Home Visiting
Number of Families in the
Interconceptional PP-122Period Receiving Home Visiting
Number of Participants Age 17 and Under who participated in
Adolescent Pregnancy Prevention Activities NA
Number of Families who
participated inNA
Pregnancy/Childbirth Education Activities
Number of Families who
participated in
CP-580Parenting Skill
Building/Education
Number of Participants in
CP-3,564
Youth Empowerment/Peer Education/
Self-Esteem/Mentor Programs
Number of Families Who Received
PP-258Transportation Services
167

Tulsa Healthy Start Initiative 2001-2005
Includes Tokens, Taxis and Vans
Number of Families Who ReceivePP-76Translation Services
Number of Families Receiving
NAChild Care Services
Number of Participants Who Received
NABreastfeeding Education ,
Counseling and Support
Number of Participants Who Received Nutrition Education
and Counseling Services including WIC Services PP-240
Number of Participants in
NAMale Support Services:
Number of Participants Referred for PP-51
CP-58Housing Assistance
Total Participants assisted with PP-22 CP-0 Jobs/Jobs Training
Total Participants served in
NAPrison/Jail Initiatives
POPULATION
Number Of Immunizations NAProvided
Public Information/Education:
15,895 Number of Individuals
Reached
INFRASTRUCTURE BUILDING
168
Tulsa Healthy Start Initiative 2001-2005
Consortia Training
32Number of Individual Members
Trained
Provider Training
529Number of Individual Providers
Trained
169

Tulsa Healthy Start Initiative 2001-2005
Project Name: Tulsa Healthy Start Project Grant #: H49CM00082 City: Tulsa State: Oklahoma
C. HEALTHY START MAJOR SERVICE TABLE* 2004* When data is collected on both program participant and community participants, please report data separately for each category of participant.
PP=Program Participant CP= Community Participant
a. DIRECT HEALTH CARE SERVICES Prenatal Clinic Visits:
NANumber of Medical Visits
by All Prenatal ParticipantsPostpartum Clinic Visits
NANumber of Medical Visits
by All Postpartum ParticipantsWell Baby/ Pediatric Clinic Visits
NANumber of Any Provider Visitsby All Infant/Child Participants
Adolescent Health Services
NANumber of any Provider Visitsby Participants age 17 and under
Family Planning PP 430 CP 309
Number of Participants ReceivingFamily Planning Services
Women’s Health
NANumber of Participants Receiving
Women’s Health Services b. ENABLING SERVICES
Total Number of Families Served PP604 CP 888
Number of Families in the Prenatal
Period318Assisted by Case Management
170

Tulsa Healthy Start Initiative 2001-2005
Number of Families in the
Interconceptional Period Assisted by Case Management 286
Number of Families in the Prenatal
Period269Assisted by Outreach
Number of Families in the
Interconceptional309Period Assisted by Outreach
Number of Families in the Prenatal
Period104Receiving Home Visiting
Number of Families in the
Interconceptional 133Period Receiving Home Visiting
Number of Participants Age 17 and
Under who participated in Adolescent Pregnancy
Prevention Activities NA
Number of Families who participated in
NAPregnancy/Childbirth Education
Activities
Number of Families who participated in
CP 305Parenting Skill
Building/Education
Number of Participants in
CP 595
Youth Empowerment/Peer Education/
Self-Esteem/Mentor Programs
Number of Families Who Received
228Transportation Services
Includes Tokens, Taxis and Vans
171

Tulsa Healthy Start Initiative 2001-2005
Number of Families Who Receive
18Translation Services
Number of Families ReceivingNAChild Care Services
Number of Participants Who
Received
NABreastfeeding Education ,
Counseling and Support
Number of Participants Who Received Nutrition Education
and Counseling Services including WIC Services PP 420
Number of Participants in
NAMale Support Services:
Number of Participants Referred for
PP 99 CP 54Housing Assistance
Total Participants assisted withPP 80 CP 2 Jobs/Jobs Training
Total Participants served in
NAPrison/Jail Initiatives
c. POPULATION
Number Of Immunizations NAProvided
Public Information/Education:
CP 10,563
Number of Individuals Reached
d. INFRASTRUCTURE BUILDING
Consortia Training 106
172

Tulsa Healthy Start Initiative 2001-2005
Number of Individual Members Trained
Provider Training
1311Number of Individual Providers
Trained
173

Tulsa Healthy Start Initiative 2001-2005
Project Name: Tulsa Healthy Start Project Grant #: H49CM00082 City: Tulsa State: Oklahoma C. HEALTHY START MAJOR SERVICE TABLE* - Jan - July
2005* When data is collected on both program participant and community participants, please report data separately for each category of participant.
PP=Program Participant CP= Community Participant
a. DIRECT HEALTH CARE SERVICES Prenatal Clinic Visits:
NANumber of Medical Visits
by All Prenatal ParticipantsPostpartum Clinic Visits
NANumber of Medical Visits
by All Postpartum ParticipantsWell Baby/ Pediatric Clinic Visits
NANumber of Any Provider Visitsby All Infant/Child Participants
Adolescent Health Services
NANumber of any Provider Visitsby Participants age 17 and under
Family Planning
PP 274 CP 312Number of Participants Receiving
Family Planning ServicesWomen’s Health
NANumber of Participants Receiving
Women’s Health Services b. ENABLING SERVICES
Total Number of Families Served PP 465 CP 347
Number of Families in the Prenatal
PeriodPP 247
174

Tulsa Healthy Start Initiative 2001-2005
Assisted by Case Management
Number of Families in the Interconceptional Period Assisted by
Case Management PP 218
Number of Families in the Prenatal Period
CP 118Assisted by Outreach
Number of Families in the Interconceptional
CP 234Period Assisted by Outreach
Number of Families in the Prenatal Period
PP 33 CP 62Receiving Home Visiting
Number of Families in the Interconceptional
PP 105 CP 107Period Receiving Home Visiting
Number of Participants Age 17 and Under who participated in Adolescent Pregnancy
Prevention Activities NA
Number of Families who participated in
NAPregnancy/Childbirth Education
Activities
Number of Families who participated in
CP 15Parenting Skill
Building/Education
Number of Participants in
NA
Youth Empowerment/Peer Education/
Self-Esteem/Mentor Programs
Number of Families Who Received NATransportation Services
175

Tulsa Healthy Start Initiative 2001-2005
Includes Tokens, Taxis and Vans
Number of Families Who ReceiveNATranslation Services
Number of Families Receiving
NAChild Care Services
Number of Participants Who Received
NABreastfeeding Education ,
Counseling and Support
Number of Participants Who Received Nutrition Education
and Counseling Services including WIC Services PP 242 CP 0
Number of Participants in
NAMale Support Services:
Number of Participants Referred for
PP 64 CP 0Housing Assistance
Total Participants assisted withPP 43 CP 0 Jobs/Jobs Training
Total Participants served in
NAPrison/Jail Initiatives
c. POPULATION
Number Of Immunizations NAProvided
Public Information/Education:
CP 139
Number of Individuals Reached
d. INFRASTRUCTURE BUILDING
176

Tulsa Healthy Start Initiative 2001-2005
Consortia Training
30Number of Individual Members
Trained
Provider Training
255Number of Individual Providers
Trained
177

Tulsa Healthy Start Initiative 2001-2005
Appendix A Target Population and Tulsa County Specific Data
178

Tulsa Healthy Start Initiative 2001-2005
PROJECT AREA DEMOGRAPHIC AND STATISTICAL DATA TABLEGrantee: Tulsa Healthy Start________________________________
VARIABLE WHITE BLACK OTHER (N)1TOTAL
HISPANIC ORIGIN
Year 2000 Census Data:Population by Racial Distribution (number) 422,581 61,656 79,062 563,299 33,616# Women of Child-bearing Age (WCBA) 90,798 15,748 18,933 125,479 7,868% Children under 18 in families with incomes below Federal Poverty Level (FPL) 9.4% 41.5% 39% 16.1% 25.7%Year 1998: (Selected Zip Codes) initial project area
# Live Births 903 880 106 1,743 NA# Births to Teens 17 years and younger 57 77 10 145 NA# Births to Teens 18 and 19 119 125 7 233 NA# Live Births with 1st Trimester entry 623 545 78 1,125 NA# Live Births with No Prenatal Care 10 12 1 21 NA# Infant Deaths 8 16 6 20 NA Infant Mortality Rate (per 1,000 live births) 8.9 18.2 103.3 11.5 NA# Infant deaths (birth to 28 days) 3 7 1 8 NA Neonatal Mortality Rate (per 1,000 live births) 3.3 8.0 16.1 4.6 NA# Infant Deaths (29 days to 365 days) 5 9 5 12 NA Post-Neonatal Mortality Rate (per 1,000 live births) 5.5 10.2 87.2 6.9 NA# Moderate Low Birth Weight (LBW) infants born with birth weight of 1501 to 2500 grams)
51 92 10 121 NA
Moderate Low Birth Weight Rates, % (birth weight 1501 to 2500 grams)
5.6% 10.5% 17.4% 6.9% NA
# Very Low Birth Weight (VLBW) Infants born with birth weight of 1500 grams or less
14 19 0 28 NA
Very Low Birth Weight Rates, % (birth weight of 1500 grams or less)
1.6% 2.2% 0 1.6% NA
Age Appropriate Immunization Rates of Children From Birth to 2 years
NA NA NA 73% NA
Year 1999 : ( Tulsa County) new/current project area# Live Births 7,023 1,356 729 9,185 743# Births to Teens 17 years and younger 240 113 42 401 63# Births to Teens 18 and 19 537 183 80 805 71# Live Births with 1st Trimester entry 5,428 877 499 6,857 456# Live Births with No Prenatal Care 66 37 19 122 8# Infant Deaths 43 17 5 65 3 Infant Mortality Rate (per 1,000 live births) 6.1 12.5 17.3 7.1 4.0# Infant deaths (birth to 28 days) 27 7 1 35 3 Neonatal Mortality Rate (per 1,000 live births) 3.8 5.2 6 3.8 4.0# Infant Deaths (29 days to 365 days) 16 10 4 30 0 Post-Neonatal Mortality Rate (per 1,000 live births) 2.3 7.4 11.3 3.3 0.0# Moderate Low Birth Weight (LBW) infants born with birth weight of 1501 to 2500 grams)
405 140 30 577 39
Moderate Low Birth Weight Rates, % (birth weight 1501 to 2500 grams)
5.8% 10.3% 7.9% 6.3% 5.2%
# Very Low Birth Weight (VLBW) Infants born with birth weight of 1500 grams or less
81 39 9 130 7
Very Low Birth Weight Rates, % (birth weight of 1500 grams or less)
1.2% 2.9% 2% 1.4% 0.9%
Age Appropriate Immunization Rates of Children From Birth to 2 years
NA NA NA 70.4% NA
179

Tulsa Healthy Start Initiative 2001-2005
PROJECT AREA DEMOGRAPHIC AND STATISTICAL DATA TABLEPage 2
VARIABLE WHITE BLACK OTHER (N)1TOTAL
HISPANIC
ORIGINYear 2000: (Tulsa County)# Live Births 7,064 1,429 814 9,346 964# Births to Teens 17 years and younger 280 112 44 422 74# Births to Teens 18 and 19 553 224 85 864 96# Live Births with 1st Trimester entry 5,415 851 552 6,843 578# Live Births with No Prenatal Care 74 44 14 132 21# Infant Deaths 54 27 3 84 7 Infant Mortality Rate (per 1,000 live births) 7.6 18.9 5.0 9.0 7.3# Infant deaths (birth to 28 days) 37 16 2 55 2 Neonatal Mortality Rate (per 1,000 live births) 5.2 11.2 3.4 5.9 2.1
# Infant Deaths (29 days to 365 days) 17 11 1 29 5 Post-Neonatal Mortality Rate (per 1,000 live births) 2.4 7.7 1.7 3.1 5.2# Moderate Low Birth Weight (LBW) infants born with birth weight of 1501 to 2500 grams)
374 153 34 562 35
Moderate Low Birth Weight Rates, % (birth weight 1501 to 2500 grams)
5.3% 10.7% 8.1% 6.0% 3.6%
# Very Low Birth Weight (VLBW) Infants born with birth weight of 1500 grams or less
79 44 15 141 10
Very Low Birth Weight Rates, % (birth weight of 1500 grams or less)
1.1% 3.1% 3.4% 1.5% 1.0%
Age Appropriate Immunization Rates of Children From Birth to 2 years
NA NA NA 68.3% NA
Year 2001: (Tulsa County)# Live Births 7,160 1,327 794 9,285 1,124# Births to Teens 17 years and younger 239 112 48 399 71# Births to Teens 18 and 19 571 169 95 837 133# Live Births with 1st Trimester entry 5,231 792 521 6,546 614# Live Births with No Prenatal Care 83 46 17 146 27# Infant Deaths 37 23 5 65 3 Infant Mortality Rate (per 1,000 live births) 5.2 17.3 11.5 7.0 2.7# Infant deaths (birth to 28 days) 25 15 2 42 2 Neonatal Mortality Rate (per 1,000 live births) 3.5 11.3 3.5 4.5 1.8# Infant Deaths (29 days to 365 days) 12 8 3 23 1 Post-Neonatal Mortality Rate (per 1,000 live births) 1.7 6.0 8 2.5 0.9# Moderate Low Birth Weight (LBW) infants born with birth weight of 1501 to 2500 grams)
401 143 31 576 40
Moderate Low Birth Weight Rates, % (birth weight 1501 to 2500 grams)
5.6% 10.8% 8.2% 6.2% 3.6%
# Very Low Birth Weight (VLBW) Infants born with birth weight of 1500 grams or less
73 48 14 135 5
Very Low Birth Weight Rates, % (birth weight of 1500 grams or less)
1.0% 3.6% 3.3 1.5% 0.4%
Age Appropriate Immunization Rates of Children From Birth to 2 years
NA NA NA 70% NA
180
Tulsa Healthy Start Initiative 2001-2005
PROJECT AREA DEMOGRAPHIC AND STATISTICAL DATA TABLEPage 3
VARIABLE WHITE BLACK OTHER (N)1TOTAL
HISPANIC
ORIGINYear 2002: (Tulsa County)# Live Births 7,212 1,255 811 9,288 1,218# Births to Teens 17 years and younger 272 104 35 411 80# Births to Teens 18 and 19 526 151 68 746 105# Live Births with 1st Trimester entry 5,137 735 577 6,453 544# Live Births with No Prenatal Care 119 30 9 159 40# Infant Deaths 60 21 1 82 15 Infant Mortality Rate (per 1,000 live births) 8.3 16.7 1.8 8.8 12.3# Infant deaths (birth to 28 days) 43 12 1 56 12 Neonatal Mortality Rate (per 1,000 live births) 6.0 9.6 1.8 6.0 9.9# Infant Deaths (29 days to 365 days) 17 9 0 26 3 Post-Neonatal Mortality Rate (per 1,000 live births) 2.4 7.2 0 2.8 2.5# Moderate Low Birth Weight (LBW) infants born with birth weight of 1501 to 2500 grams)
385 132 56 569 73
Moderate Low Birth Weight Rates, % (birth weight 1501 to 2500 grams)
5.3% 10.5% 13.4% 6.1% 6.0%
# Very Low Birth Weight (VLBW) Infants born with birth weight of 1500 grams or less
77 33 15 126 17
Very Low Birth Weight Rates, % (birth weight of 1500 grams or less)
1.1% 2.6% 3.8% 1.4% 1.4%
Age Appropriate Immunization Rates of Children From Birth to 2 years
NA NA NA 65.3% NA
Year 2003: (Tulsa County)# Live Births 7,195 1,292 854 9,357 1,361# Births to Teens 17 years and younger 236 103 34 373 68# Births to Teens 18 and 19 522 158 77 757 151# Live Births with 1st Trimester entry 4,872 627 577 6,070 670# Live Births with No Prenatal Care 104 43 16 163 30# Infant Deaths NA NA NA NA NA Infant Mortality Rate (per 1,000 live births) NA NA NA NA NA# Infant deaths (birth to 28 days) NA NA NA NA NA Neonatal Mortality Rate (per 1,000 live births) NA NA NA NA NA# Infant Deaths (29 days to 365 days) NA NA NA NA NA Post-Neonatal Mortality Rate (per 1,000 live births) NA NA NA NA NA# Moderate Low Birth Weight (LBW) infants born with birth weight of 1501 to 2500 grams)
380 119 56 557 53
Moderate Low Birth Weight Rates, % (birth weight 1501 to 2500 grams)
5.3% 9.0% 15% 6.0% 4.7%
# Very Low Birth Weight (VLBW) Infants born with birth weight of 1500 grams or less
72 36 8 116 13
Very Low Birth Weight Rates, % (birth weight of 1500 grams or less)
1.0% 2.7% 1.4% 1.2% 1.2%
Age Appropriate Immunization Rates of Children From Birth to 2 years
NA NA NA NA NA
181
Tulsa Healthy Start Initiative 2001-2005
Appendix B Progress Report Monitoring Visit
182

Tulsa Healthy Start Initiative 2001-2005
183

Tulsa Healthy Start Initiative 2001-2005
Health Resources and Services AdministrationOffice of Performance Review
Dallas Regional Division
Performance Report
Tulsa City-County Health Department5051 S. 129th E. Ave
Tulsa, OK 74134-7004EIN#-1736006419A1
Prepared by: Carol Sherman, D.M.D. (Team Leader)
Lynda Marquardt, M.S.W.Carla Parker
Site Visit Date: October 19-21, 2004
Report Date:November 30, 2004
Progress Report Date:September 2005
Grantee Summary
178

Tulsa Healthy Start Initiative 2001-2005
Tulsa City-County Health Department 4616 East 15th Street Tulsa, OK, 74112
Executive Director: Gary Cox, J.D.(918) 595-4400FAX (918) 595-4374 [email protected]
The City of Tulsa, OK, has a Metropolitan Statistical Area (MSA) population of 563,299, with an estimated 160,000 non-elderly that are uninsured. The Tulsa City-County Health Department (TCCHD) is a tax-supported branch of government and a health care provider. With an annual budget of approximately $14, the Health Department has a staff of over 300 full and part-time employees, who work throughout the county at ten clinical health centers and one regional office. TCCHD is the recipient of two grants from the Health Resources and Services Administration (HRSA): 1. Healthy Start Program, HRSA/MCH Bureau; and, 2. Healthy Community Access Program (CAP), HRSA/BPHC.
The Tulsa MSA currently faces several major challenges related to Medicaid and uninsured health care: a statewide budget deficit; Medicaid cuts; and, a recent conversion of the only non-profit hospital to for-profit status. In Tulsa, 46% of deliveries are paid for by Medicaid; 65% of deliveries are to families that would qualify at 185% ($18,000) of the Federal Poverty Level (FPL); and, 33% of resident births in the county are to families at 100% FPL or less.
Healthy Start-Health Center Cluster H49-MC-00087;CFDA# 93.926 Project Period 6/01/01-5/31/05; Funding Level - $1,114,695Program/Project Director: Corrina Jackson (918) 595-4460, [email protected] Project Officer: Benita Baker, Project Officer (301) 443-1461;[email protected] HRSA Grant Mgmt. Specialist: Shelia Burks, GMO (301)594-6452; [email protected]
During the performance review the OPR team and the Tulsa City-County Health Department staff focused on the following programs and major activities:
I. Low Birth Weight (LBW) and Very Low Birth Weight (VLBW) Infants
A. Program Summary
Population: Low birth weight (LBW) and Very Low Birth Weight (VLBW) infants born to pregnant and parenting women enrolled in Tulsa Healthy Start (THS).
Services: Outreach, case management, health education, depression screening, and interconceptional care for pregnant and postpartum women and infants to two years of age.
179

Tulsa Healthy Start Initiative 2001-2005
B. Performance Review Measure
Low Birth Weight (LBW) Infants Born to Healthy Start Clients
Number of LBW Infants Born 2001 2002 2003Healthy Start 21 28 21Tulsa County 615 608 623State of Oklahoma 3,234 3,372 3,312
180
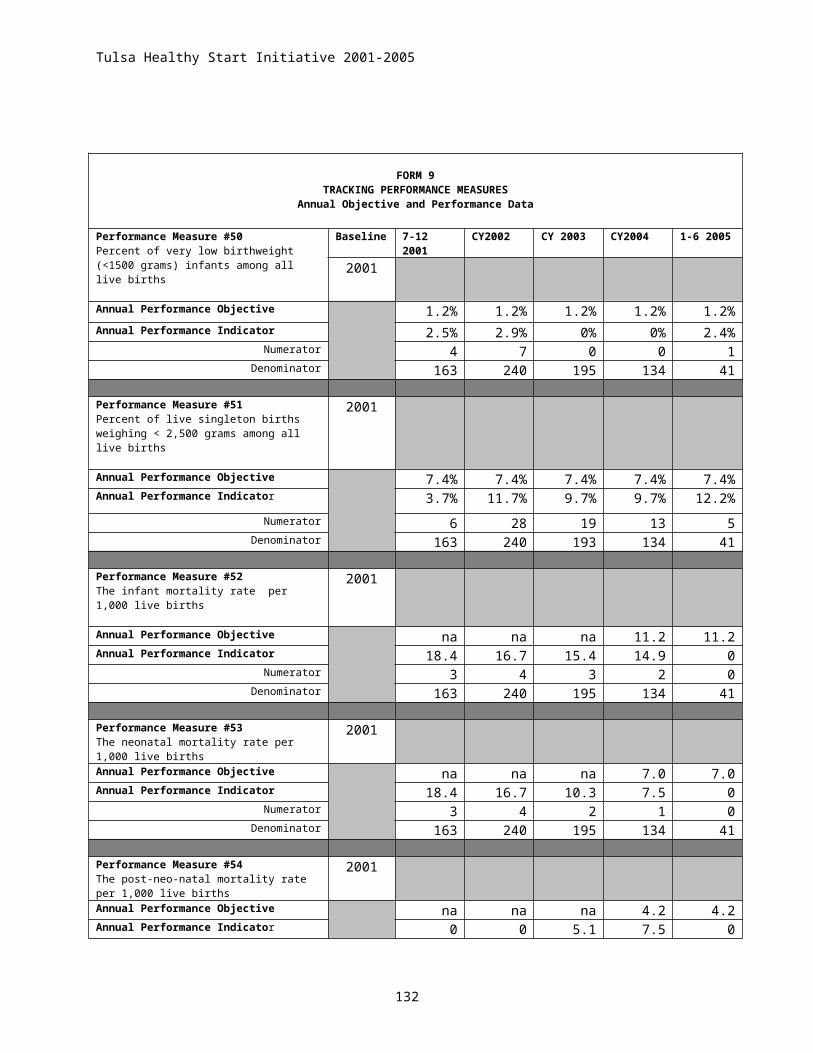
Tulsa Healthy Start Initiative 2001-2005
Very Low Birth Weight (VLBW) Infants Born to Healthy Start Clients
Data Sources: THS fiscal year (FY) 2001 competitive and FY 2002-2004 continuation funding applications, and input from staff.
The measures were selected because they: (1) incorporate a Government Performance Results Acts (GPRA) measure, HRSA/Maternal and Child Health Bureau (MCHB) program measures, and THS objectives; (2) meet OPR criteria for measure selection: data, communication, and proxy (importance); and, (3) illustrate grantee efforts to serve the needs of the target population.
C. Performance Analysis
Both THS LBW and VLBW percentages are higher than those reflected for Tulsa County and State of Oklahoma. THS LBW performance objective is 7.4%, but 10.1% in 2001 is the lowest percentage achieved to date. Tulsa County’s LBW percentage increased slightly from 6.5% in 2002 to 6.7% in 2003, while State of Oklahoma percentages decreased slightly from 6.7% in 2002 to 6.5% in 2003. Grantee will have a difficult time reaching their 7.4% LBW performance objective by the end of the May 2005 project
period.
181
Number of VLBW Infants Born
2001 2002 2003
Tulsa Healthy Start 21 28 21Tulsa County 615 608 623State of Oklahoma 3,234 3,372 3,312
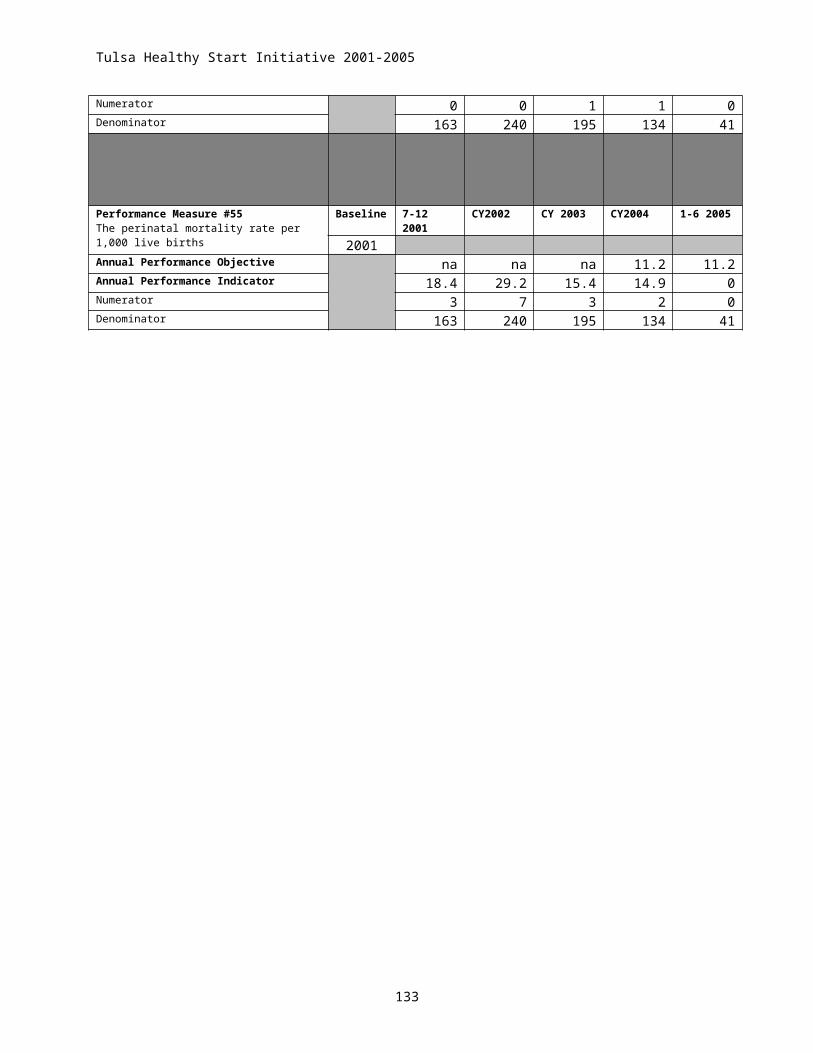
Tulsa Healthy Start Initiative 2001-2005
THS VLBW percentages decreased steadily from 2.9% in 2001-02 to 1.6% in 2002-03. THS performance objective is 1.2%. No VLBW infants have been born to women served by THS from January-June 2004. This stellar performance may be the result of risk screening and targeting of case management and care coordination services to pregnant and postpartum women at highest risk for LBW, thus further reducing VLBW births. Tulsa County percentages improved slightly from 1.4% in 2001-02 to 1.3% in 2002-03, while State percentages remained at 1.3%.
Difficult and persistent root causes impact the high-risk target population served by THS. These may include poverty, unemployment, family violence, pregnant and parenting adolescents, mental health and substance abuse, unstable housing/homeless, language literacy, education, and lack of health insurance, primary health care, transportation and child care services. Pregnant and postpartum women and infants served by THS are, based on identified risk screening, intervention and tracking, at highest risk for poor perinatal outcomes. Trends represent consistent progress, against difficult odds, in serving high-risk pregnant and postpartum women and infants through THS.
Factors Contributing to Performance (In Priority Order)
1. Early Identification of Risk Factors : Pregnant and parenting women seeking services are triaged, using a weighted risk assessment survey to identify medical and social risks, into categories of high, moderate, and low risk to expedite entry into care. Risk factors affecting birth outcomes include family income of less than 185% of poverty, Tulsa County residence, racial or ethnic minority heritage, below 18 or greater than 35 years of age, domestic violence, child abuse and neglect, pre-existing mental health disorder, depression, tobacco, drug and alcohol use, homelessness and previous birth history. Based upon risk designation, women are referred for case management and care coordination services to encourage early and continuous care with minimal duplication. Women designated as high-risk are referred to THS for follow-up, and those identified moderate to low risk are referred to one of three alternate case management programs available to serve Tulsa County.
2. Care Coordination and Case Management : THS is the only case management program in Tulsa County with primary focus on reduction of infant mortality. Case management facilitates interactions with high-risk medical providers, social service agencies, and support services; improves program retention rates and compliance with medical and social service information; and, increases access to care for high- risk populations. During calendar year 2003, 678 high-risk women and 474 infants received case management and care coordination services through THS.
3. Centralized Appointment System : Babyline, a centralized telephone appointment line serving Tulsa County, improved pregnancy outcomes through increased access for uninsured, underinsured, and Medicaid eligible pregnant and postpartum women and infants. Services included information on pregnancy testing, family planning and prenatal care resources; pregnancy risk screening, assessment, and referral; Medicaid eligibility determination; and, medical home selection. THS funds three (1.5 FTE) half-time telephone referral specialists, and one part-time (.5 FTE) coordinator to
182

Tulsa Healthy Start Initiative 2001-2005
provide outreach and client recruitment services. Babyline provided services to 4,795 unduplicated THS clients in 2003. 413 appointments for prenatal care were scheduled monthly during January-June, 2003; appointments scheduled for family planning averaged 104; and scheduled child health appointments averaged 39.
4. State and Regional Partnerships : THS collaborates with Oklahoma State Department of Health Title V Program on Tulsa Fetal Infant Mortality Review (TFIMR) to review deaths of infants less than one year of age, and identify system changes to prevent or reduce infant deaths. Transportation services for THS clients are coordinated through SoonerCare, Oklahoma Medicaid managed care. THS is an active member of the Region VI Healthy Start - Title V Partnership. The Partnership consists of HRSA/MCHB funded Healthy Start projects and state Title V leadership. THS hosted the annual Region VI Partnership meeting in November 2002 focused on interventions to eliminate health disparities in perinatal outcomes. These important partnerships represent a targeted approach to risk reduction for high-risk pregnant and postpartum women and infants.
Factors Restricting Performance (In Priority Order)
1. Program Capacity : Finances, language, and caseload restrictions limit service availability for high-risk bi-lingual women. Hispanic population growth (14.7% in 2002 and 15% in 2003) and growing high-risk service demands exceed THS case management and outreach program capacity. Four call center case managers, two bilingual, responded to 48,000 calls in 2003, and high-risk pregnant women eligible for THS case management services were referred to alternate services designed to serve less restrictive moderate to low risk women. Bilingual staff is difficult to attract and retain due to high community demand for translation skills.
2. Health Care Resources : First trimester entry into prenatal care for THS women dropped from 59.8% in 2000 to 35.6% in 2003. The impact of increased appointment wait times for entry into care, precipitated by dramatic increases in uninsured women seeking to access care, resulted in the dramatic decline. THS is able to identify and refer high-risk women, through outreach and case management activities, earlier than they can access prenatal care services. High-risk prenatal care appointment wait times average eight (8) weeks. Demand for prenatal, labor and delivery, and postpartum care exceeds available resources and services.
3. Adolescent Health : Adolescents represented 25.1% of active THS clients served in 2002, and 26.3% in 2003. There is no program emphasis or focus on delivery of comprehensive perinatal services for high-risk pregnant and parenting adolescents and their infants.
D. Performance Improvement Options
183

Tulsa Healthy Start Initiative 2001-2005
1. Program Capacity : Complete an analysis of THS program encounter data to assess demand for services (waiting lists, waiting time for appointments), most requested services, completed referrals, and staff and space capacity. The analysis may serve as an opportunity to prioritize and target available program and staff resources to better serve the needs of the target population.
Monitor the Health and Human Services (HHS) and Health Resources and Services Administration (HRSA) websites, http://www.hhs.gov and http://www.hrsa.gov, for current information on funding opportunities available to expand services and access to care for the THS population.
2. Health Care Resources : Continue to partner with Community HealthNet, Inc. participant agencies (Community Service Council of Greater Tulsa, Indian Health Care Resource Center of Tulsa, Margaret Hudson Program, Morton Comprehensive Health Services, Oklahoma State University College of Osteopathic Medicine, Planned Parenthood of Arkansas and Eastern Oklahoma, Tulsa City-County Health Department, and University of Oklahoma College of Medicine) to advocate for expanded program services, improved health care financing, and increased community resources to ensure access to care for high-risk pregnant and postpartum women and families.
Initiate partnerships with the Oklahoma Primary Care Association (OPCA) and state Primary Care Office (PCO) to address unmet health care access needs and health disparities for pregnant and postpartum women and families in Tulsa County. Ms. Greta Shepherd, Executive Director, OPCA, may be contacted at (405) 424-2282 or by e-mail at [email protected]. Mr. Mike Brown, PCO point of contact, may be contacted at (405) 271-8428, or by e-mail at [email protected].
Initiate a partnership with the HRSA/MCHB funded Healthy Start Project located in Oklahoma City to network, share information, and develop partnership strategies to address issues and concerns facing pregnant and postpartum women and families served by Healthy Start throughout Oklahoma. Dr. Donna Neal Thomas, Executive Director, Community Health Centers, Inc. Healthy Start, may be contacted at (405) 769-3301. Partnership strategies may reflect the successful partnership model demonstrated by Catholic Charities Healthy Start Project in working with Texas Healthy Start projects and the Texas Title V Program. Seek consultation and technical assistance from Francesca Pinto, Healthy Start Program Manager at Catholic Charities Diocese of Forth Worth (CCDOFW) for assistance with partnership identification and development strategies. Ms. Pinto may be reached at (817) 413-3923, or by e-mail at [email protected].
3. Adolescent Health : Consider an identified service focus for pregnant and parenting
adolescents and their families, and target outreach efforts to attract and retain high-risk teens in THS services. Partner with Oklahoma Maternal and Child Health (Title V) adolescent health program coordinator to explore funding opportunities for adolescent health services, and alliances with agencies and groups serving pregnant and parenting teens.
184

Tulsa Healthy Start Initiative 2001-2005
Explore development of comprehensive health initiatives to identify and address primary care, mental health, substance abuse, and psychosocial needs of adolescents served by THS. Please contact Dr. Wendy Adam, Baylor College of Medicine Leadership Education in Adolescent Health (LEAH) Program for consultation and technical assistance. Dr. Adam may be contacted at (832) 822-4004, or by e-mail at [email protected].
September 2005 Progress Report
LBW 1999 2000 2001 2002 2003 2004Tulsa Healthy Start 8.3 5.8 10.8 11.7 10.5 12.1Tulsa County 6.3 6.6 6.5 6.6 6.5 7.2
VLBW 1999 2000 2001 2002 2003 2004Tulsa Healthy Start 1.3 2.2 1.2 2.9 0 0Tulsa County 1.4 1.5 1.4 1.4 1.2 1.2
Findings:The Low Birth Weight (LBW) continues to be elevated above the Tulsa County percentages per year. The Very Low Birth Weight (VLBW) numbers are below the Tulsa County percentages per year with the exception of 2002. The implication is that many infants that would have been VLBW are in the LBW categories.
Program Capacity: The waiting lists have been analyzed. The capacity to serve is based on the number of slots available per case manager to accept new clients. Every effort is made by FHC and the THD to find additional dollars to expand case managers, however, in the current funding recession by the State it is unlikely to program funding will be available.
Health Care Resources: THS continues to partner with the Community HealthNet (CHN) providers of care with the intent of expanding high risk case management services to include both OU and OSU.
The Primary Care Association participates with CHN and has assisted Community Health Connections to make an FQHC application in 2005. THS has had a long standing partnership with the Central Oklahoma Healthy Start. We also have developed in collaboration with the Oklahoma Institute for Child Advocacy a Healthy Mothers, Healthy Baby project for the state engagement of rural areas of Oklahoma.
Adolescent Health: THS addresses adolescent health through the collaboration with Margaret Hudson Program. The Free Pregnancy
185
Tulsa Healthy Start Initiative 2001-2005
Testing program is an example of collaboration with THS to identify pregnant teens and teens in need of family planning services. OSDH Title V has had reduced funding from MCHB and has not initiated any new adolescent program expansions.
II. Preterm Births A. Program Summary
Population: Preterm (less than 37 weeks gestation) infants born to pregnant and postpartum women enrolled in THS.
Services: Outreach, case management, health education, depression screening, and interconceptional care for pregnant and postpartum women and infants to two years of age.
B. Performance Review Measure
Preterm (less than 37 weeks gestation) Births to Healthy Start Clients
Data Sources: THS FY 2001 competitive and FY 2002-2004 continuation funding applications, and
input from staff.
186
Number of Preterm Births 2001 2002 2003Tulsa Healthy Start 26 29 19Tulsa County 1,691 1,751 1,794State of Oklahoma 5,885 6,121 NA

Tulsa Healthy Start Initiative 2001-2005
The measure was selected because it: (1) incorporates a GPRA measure, HRSA/MCHB program measure, and THS objective; (2) meets OPR criteria for measure selection: data, communication, and proxy (importance), and, (3) illustrates grantee efforts to serve the needs of the target population.
C. Performance Analysis:
The grantee project performance objective is reduction of preterm birth to 9.0%. Preterm births to THS clients declined steadily from 12.5% in 2001, when Healthy Start received funding, to 9.7% in 2003. In the period January- June 2004, preterm births to pregnant women served by THS reached 0%. THS performance is well below the 2003 Tulsa County percentage (19.4%) and the 2002 State of Oklahoma (12.7%) percentage. TSH program components of outreach, case management, health education, depression screening, and interconceptional care impacted the target population, reduced barriers to care, and improved performance. THS staff is proud of program performance, and their performance trend is on track to reduce preterm birth percentages to 9.0% by conclusion of the project period.
Factors Contributing to Performance (In Priority Order)
1. Integrated Service Model : THS developed and utilizes integrated service delivery models to improve infant mortality rates and birth outcomes for preterm infants. Models include community-based consortium; care coordination and case management; outreach and client recruitment; facilitation services; education and training; depression screening; and interconceptional care. The models encompass a network of six clinic sites (Indian Health Care Resource Center, Morton Comprehensive Health Services, Oklahoma State University College of Osteopathic Medicine, Planned Parenthood of Arkansas and Eastern Oklahoma, Tulsa Health Department, and University of Oklahoma College of Medicine-Tulsa) focused on one common goal – reducing infant deaths.
2. Community Partnerships : THS successfully created strong collaborations and
working relationships with non-profit agencies (Community Service Council, Metropolitan Tulsa Urban League, Margaret Hudson Program, Tulsa Health Department) and local medical schools, Oklahoma State University College of Osteopathic Medicine and University of Oklahoma College of Medicine-Tulsa, to coordinate community activities and services. Representatives include consumers and specialists in medicine, child abuse prevention, pregnant and parenting teens, public health, neighborhood organizations, and education.
3. Social Marketing : THS has impacted the Tulsa community through sponsorship and coordination of community awareness and education campaigns. Marketing campaigns have targeted consumers and safety net and private care providers, and included information on Sudden Infant Death Syndrome (SIDS), lack of infant mortality funding, depression and impact of chronic depression, substance abuse, and
187

Tulsa Healthy Start Initiative 2001-2005
domestic violence as co-factors in infant mortality, and pre-conceptional care for women.
Factors Restricting Performance (In Priority Order)
1. Mental Health and Substance Abuse : In 2002 Tulsa County ranked second in the U.S. in illegal drug usage. Youth Risk Behavior Survey (YRBS) data from Tulsa public schools indicated high adolescent rates of depression, alcohol, burned and smokeless tobacco, and increased use of cigars soaked in liquid cocaine and marijuana solutions. Depression, family violence, and substance abuse are key factors impacting infant mortality, preterm births, and LBW and VLBW infants.
Pregnant and postpartum women served by THS are screened for depression at three intervals throughout the perinatal period. Positive screens result in further assessment, evaluation and referral for treatment. Community-based mental health and substance abuse treatment services, available free of charge or on a sliding fee scale to high-risk pregnant and postpartum women, operate at capacity and care is difficult to access. Language requirements create an additional barrier to care.
2. Health Care Environment : State of Oklahoma and Tulsa County has suffered from the economic downturn of past years. SoonerCare, Oklahoma Medicaid managed care, experienced a $50,000,000 deficit in 2003 and has implemented recovery measures. SoonerCare authorizes up to six thousand ($6,000) dollars to cover costs for prenatal care, labor and delivery, and postpartum services. One in three pregnant women in Tulsa County is uninsured, and SoonerCare paid for 46% percent of births to Oklahoma women in 2002. Restricted reimbursement rates result in fewer providers accepting pregnant women served by Medicaid, delayed entry into prenatal care, and a reduced quantity and quality of care. High-risk pregnant women face an even shorter available supply of providers and services.
3. Male Services : THS hosted an Oklahoma Fatherhood Summit during July 2003, and a conference for professionals, “Welcoming Fathers into the Picture,” is planned during November 2004. These conferences focus on male involvement and its importance in the success of families and prenatal outcomes. Despite these important education and training opportunities, THS does not have a male outreach and recruitment campaign or program to attract and involve male partners of pregnant and postpartum women, and fathers of infants. Lack of male participation and support for pregnant and parenting women may contribute to delayed entry into prenatal care; impact compliance with efforts to reduce/eliminate risk factors such as alcohol, tobacco, and illegal drugs; and, discourage effective use of community resources and services. Participation of males may also increase access to health care and social services for men, and improve participation and retention rates in THS programs and services that focus on the health and psychosocial needs of families.
4. Consumer Involvement : THS consortium, known as the Family Health Coalition (FHC), membership includes 199 persons from 77 community agencies and groups. Consumer advocates represent 16.1% of FHC members. While 68.1% of FHC
188

Tulsa Healthy Start Initiative 2001-2005
consumer members participate in episodic subcommittee and event planning activities, just 20.2% of consumer advocates attend half or more regularly scheduled consortium meetings. There is no strategic process in place to ensure consumer advocates reflect the racial/ethnic breakdown of the THS population.
D. Performance Improvement Options
1. Mental Health and Substance Abuse:
Seek information through the U.S. Department of Health and Human Services (HHS) Substance Abuse and Mental Health Services Administration (SAMHSA) website, http://www.samhsa.gov, for current information on prevention and treatment strategies for children, adolescents, and families, and funding opportunities available to expand services and access to care for the high-risk population served by THS.
Explore partnership opportunities with the HRSA MCHB funded Center for School Mental Health Assistance (CSMHA) for development of youth and adolescent services. The Center strives to support schools and communities in the development of mental health programs that are accessible, family-centered, culturally competent, and responsive to local needs. CSMHA offers a forum for training, the exchange of ideas, and promotion of coordinated systems of care that provide a continuum of services to enhance mental health, development, and learning. CSMHA may be contacted through the University of Maryland School of Medicine, Department of Psychiatry, 680 West Lexington Street, 10th floor, Baltimore, Maryland 21201; by phone at (410) 706-0980; or by e-mail at [email protected]. Their web site may be found at http://csmha.umaryland.edu.
2. Health Care Environment : Explore funding opportunities available through federal, state, and private sources to supplement and expand THS program goals and objectives to serve high-risk pregnant and postpartum women and infants. Additional federal funding opportunities may be available at www.grants.gov. Please contact Cedar Jackson, Director, Women’s Health Division, Oklahoma State Department of Health, to discuss opportunities for state maternal and child health funding, training and technical assistance to assist in expansion of access to care efforts for pregnant and parenting women and their infants. Ms. Jackson may be contacted at (405) 271-4476 or by e-mail at [email protected]. Private sources for consideration include Robert Wood Johnson Foundation (http://www.rwif.org) and W. K. Kellogg Foundation (http://www.wkkf.org).
3. Male Services : Consider development and implementation of a male services
initiative to serve and support male partners of pregnant and postpartum women, and fathers of infants served by THS. Please contact Ms. Vivian Gettys at Family Road of Greater Baton Rouge Health Start, 323 Airport Avenue, Baton Rouge, Louisiana 70806 for consultation and technical assistance. She may be contacted at (225) 201-8888 to discuss their successful fatherhood program.
189

Tulsa Healthy Start Initiative 2001-2005
4. Consumer Involvement : Key THS leadership should consider partnering with FHC to provide ongoing training, technical assistance, and support for consumer advocates, provide incentives for consumers to develop and improve advocacy skills and apply them toward efforts to increase access to care for the high-risk populations served by THS. Develop strategies to recruit and retain minority/ethnic consumer advocates skilled in languages other than English. Please seek consultation from Jerry Roberson at Catholic Charities Healthy Start in Fort Worth, Texas. Jerry may be contacted at (817) 524-0814, or by mail at 2001 Beach Street, Suite 800, Fort Worth, Texas 76015 to discuss their successful consortium model.
September 2005 Progress Report
Preterm Births 1998 1999 2000 2001 2002 2003 2004Tulsa Healthy Start 9.4 9.6 12.5 12.5 12.1 9.7 8.2Tulsa County 15.9 16.3 17.1 18.2 18.9
Findings: The Preterm births are lower than the Tulsa County statistics. Data is not available for 2003 and 2004 for Tulsa County at present.
Mental Health and Substance Abuse: The FHC has been successful in receiving a Women’s Behavioral Grant to assist in identifying women in need of family violence, depression, smoking, alcohol and illegal drug use.
Health Care Environment: Ms. Cedar Jackson participates on the FHC. We are using her services as needed. Male Services: FHC and THS have established a Fatherhood Involvement Coalition. The intent of the group is to conduct training with service providers to improve their father friendly environments, conduct training for fathers and interested providers which is scheduled for October and conduct a Father EXPO to attract men to an event they can participate with their children.
Consumer Involvement: THS and FHC brought Jerri Roberson for the THS annual meeting in August 2005. Technical assistance was received in developing a stronger consumer involvement.
190

Tulsa Healthy Start Initiative 2001-2005
191