heart failure in 2018 - totalcardiology
TRANSCRIPT

Click to edit Master title style
Heart Failure in 2018Sandeep Aggarwal MD FRCPC

Click to edit Master title styleFaculty Presenter Disclosure
Cardiology for the Non-Cardiologist
Faculty: Sandeep Aggarwal
Relationships with Financial Sponsors:
- Grants or Research Support: BI
- Speakers Honoraria: Bayer, Bristol-Meyers Squibb/Pfizer, Servier, Novartis, Amgen, AstraZeneca, BI, Merck, Sanofi, JnJ
- Consulting Fees: Bayer, Servier, Novartis, Amgen, Sanofi
- Patents: None
- Other: None

Click to edit Master title styleDisclosure of Financial Support
Cardiology for the Non-Cardiologist has received financial support from the following Pharmaceutical companies; Bayer, Bristol-Meyers Squibb/Pfizer, Servier, Novartis, Amgen, AstraZeneca and Merck in the form of unrestricted educational grants.
Potential Conflicts of Interest: None

Click to edit Master title styleMitigating Potential Bias
• While we have received unrestricted educational grants from several pharmaceutical companies, most presentations have no mention of specific products and are unrelated to the supporting companies or their products. No specific presentations will be supported or sponsored by a specific company.
• Information on specific products will be presented in the context of an unbiased overview of all products related to treating patients.
• All scientific research related to, reported or used in this CME activity in support or justification of patient care recommendations conforms to the generally accepted standards.
• Clinical medicine is based in evidence that is accepted within the profession.

Click to edit Master title styleOutline
• Epidemiology
• Case Presentation
• Key points
• HFpEF
• HFrEF
HFrEF = Heart Failure reduced EF
HFpEF = Heart Failure preserved EF

Click to edit Master title styleTypes of Heart Failure
• Systolic heart failure (HFrEF)• Ischemic
• Non-Ischemic
• Diastolic heart failure (HFpEF)
• Valvular heart failure
• Right sided heart failure
HFrEF = Heart Failure reduced EF
HFpEF = Heart Failure preserved EF

Click to edit Master title styleKey Points
1. SGLT2i prevents CHF in DM patients with cardiovascular disease
2. Maximize Triple Therapy (TT) – prevention and treatment of CHF
3. Entresto (Valsartan/Sacubitral) and Lancora (Ivabradine) after TT
4. Cardiac Rehabilitation for CHF
5. CRS (cardiorenal syndrome) – decongest if possible
6. IV Iron therapy improves CHF with IDA
7. HFpEF – Diuretics, ACE/ARBi, MRA and exercise

Click to edit Master title styleThe Burden
Age groupsBoth
sexesMen Women
≤ 69 years 1.9 3.7 0.9
70-79 years 2.5 3.5 1.3
≥ 80 years 6.0 7.4 5.0
Prevalence (%) heart failure by age and gender
ESC 2016
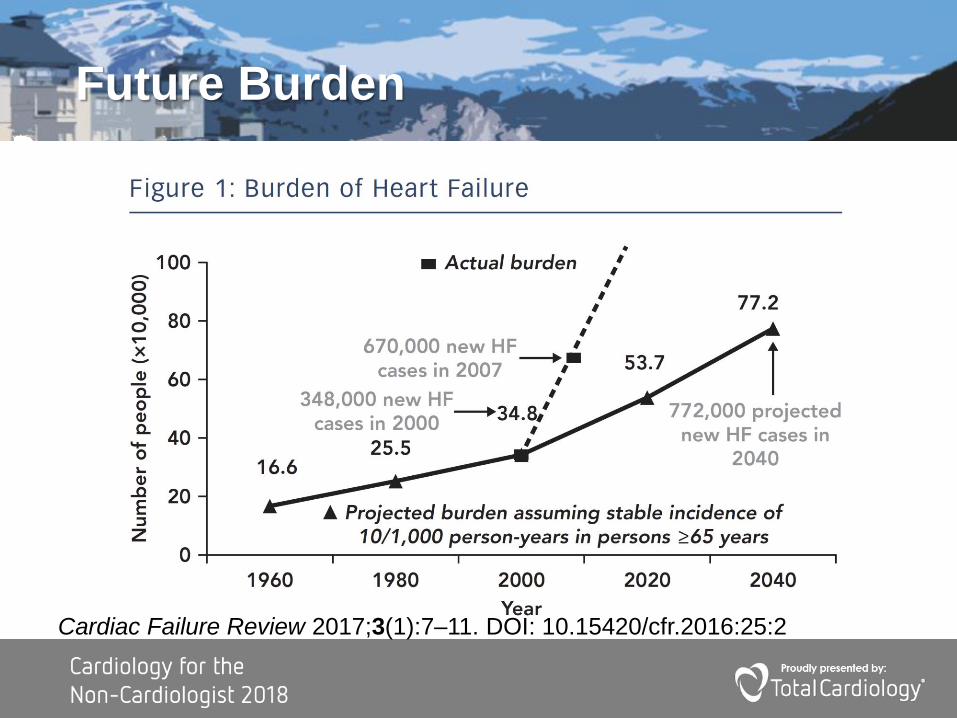
Click to edit Master title styleFuture Burden
Cardiac Failure Review 2017;3(1):7–11. DOI: 10.15420/cfr.2016:25:2

Click to edit Master title styleCanadian Data
Canadian Heart and Stroke 2016

Click to edit Master title styleWhat percent of CHF is treated by GP/FPs (2000 Canadian data)?
1. 33%
2. 50%
3. 66%
4. 75%

Click to edit Master title style
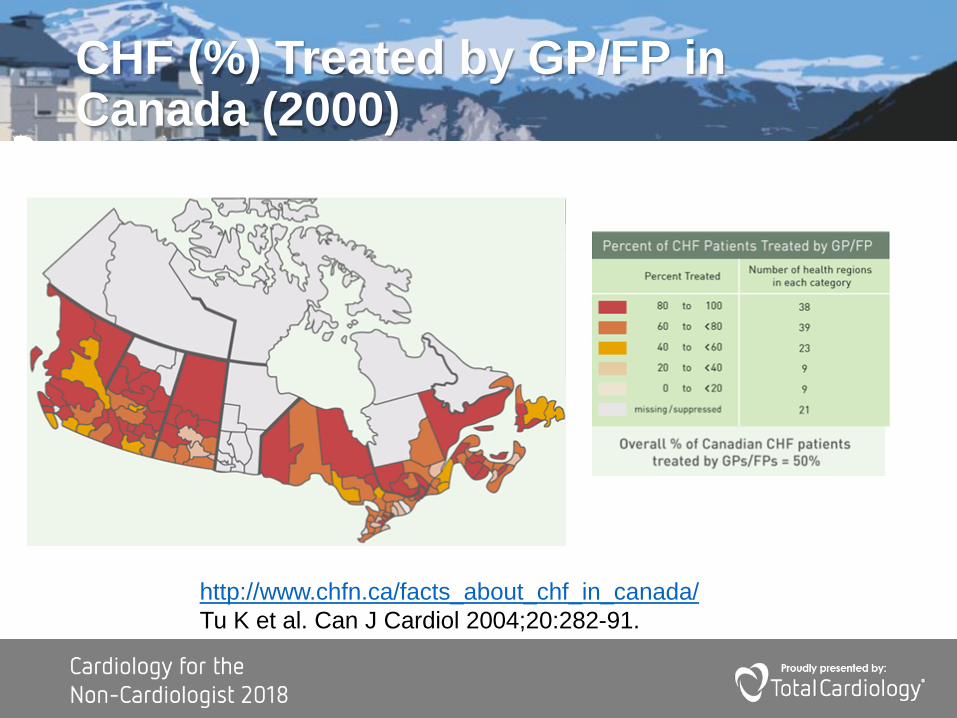
Click to edit Master title styleCHF (%) Treated by GP/FP in Canada (2000)
http://www.chfn.ca/facts_about_chf_in_canada/
Tu K et al. Can J Cardiol 2004;20:282-91.

Click to edit Master title stylePercent of CHF patients Treated by GP/FP
http://www.chfn.ca/facts_about_chf_in_canada/
Tu K et al. Can J Cardiol 2004;20:282-91.
Click to edit Master title styleMorbidity and Mortality
(1) Yeung., CMAJ, 2012, 184(14), E765-E773
(2) Stewart , Eur J Heart Fail, 2001, 3, 315
➢1-yr mortality rate after diagnosis:
OP:15% IP:35%
➢30d mortality rate after hosp.
15%
➢30d Readmit after CHF Admit
3-5% (CHF)
15% (Any cause)

Click to edit Master title styleWhich of the following statement is true about TT dosing?
1. Target dose is the same as blood pressure maximum dosage for all TT drugs
2. Carvedilol and ARB’s target dosage is maximum htn dosage
3. Target dose is ½ max htn dosage for all drugs
4. ACEi dosing is ½ max htn dosage
5. 2 and 4 are correct
6. All are correct
Click to edit Master title style

Click to edit Master title styleSystolic Heart Failure (HFrEF) Undertreated
Jhund ESC 2016
Click to edit Master title style
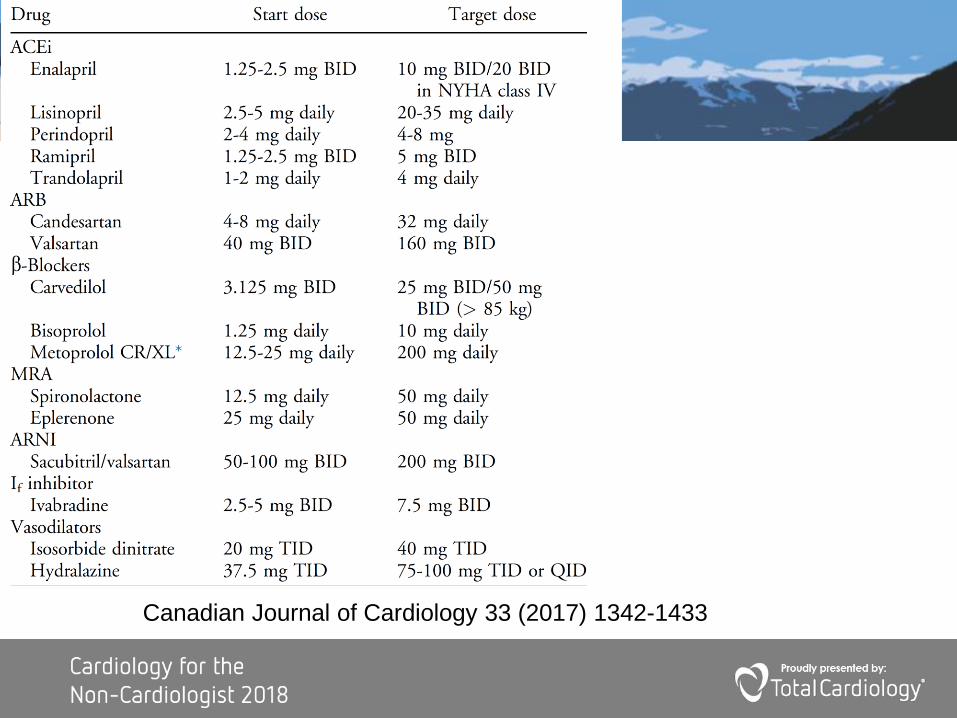
Canadian Journal of Cardiology 33 (2017) 1342-1433

Click to edit Master title styleTitration dosages
• ACEi – half max dosage
• ARB – max dosage
• B-blocker • Carvedilol 25 mg bid (max htn dosage)
• Bisoprolol 10 mg daily (1/2 max htn dosage)
• MRA (spironolactone and eplerenone)• 25 to 50 mg daily (1/4 to ½ max htn dosage)

Click to edit Master title styleBNP and NTproBNP (NP’s)
Which of the following statements are true
1. NPs are useful to aid in diagnosis of CHF
2. NPs are useful to guide HF management
3. NPs are useful for prognosis
4. 1 and 2 are true
5. 1 and 3 are true
6. All statements are true
NP’s = Naturetic peptides
Click to edit Master title style
• Diagnosis • dyspnea and unclear etiology
• Dyspnea exacerbation known CHF
• Guiding HF therapy
• Pre-discharge to predict readmission
BNP and NTproBNP

Click to edit Master title style
Heart Failure Diagnosis – Acute and Ambulatory

Click to edit Master title stylePractical use of BNP Prevention and Management
CCS 2014 Heart Failure Guidelines
Click to edit Master title styleGuiding Therapy
• Inpatient Guided TherapyPRIMA II IP
• No reduced re-hosp. or mortality with guided therapy
• Discharge > 30% reduction lower readmission/Mortality
• Outpatient guided therapyGUIDE-IT Trial (NT-ProBNP)
• NT-ProBNP does NOT help to guide therapy
JAMA. 2017;318(8):713-720,
Circulation, July 17, 2018, Volume 138, Issue 3

Click to edit Master title styleNatiuretic Peptides - Pitfalls
• Falsely low BNP• Obesity
• Falsely high BNP• LVH and ischemia
• Tachycardia
• Hypoxia
• Pulmonary embolism
• Sepsis
• COPD
• Diabetes
• Liver cirrhosis
• Renal impairment

Click to edit Master title styleTreatment of HFpEF
CCS Heart Failure
Guidelines

Click to edit Master title style
CCS Heart Failure guidelines 2017

Click to edit Master title style
CCS Heart Failure
Guidelines

Click to edit Master title style
CCS Heart Failure
Guidelines

Click to edit Master title styleWhat Drugs to Avoid!!
•LVEF <40%
•NSAIDS or COX-2 inhibitors
•CCBs Diltiazem/Verapamil
•Amlodipine OK
•Triple RAAS therapy •ACEi, ARB and MRA

Click to edit Master title styleDiabetes and Heart Failure
• No trials in heart failure
• Probably not safe:• Glitazones, Saxigliptin (Onglyza)
• Safe:
• Sitagliptin (Januvia), Linagliptin (Trajenta)
• Liraglutide (Victoza)
• Helpful if CHF +DM, Possibly helpful even if not DM:
• SGLT2i’s

Click to edit Master title styleExercise Training
• Systolic Heart Failure• Cochrane review suggests reduction in Hospitalization for heart failure
• Diastolic Heart Failure• Improved exercise capacity
• Improved quality of life
• Improved echo parameter of diastolic function
http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD003331.pub4/full

Click to edit Master title styleNewer Drug Therapies
•Valsartan/sacubitril (Entresto)
•Ivabradine (Lancora)

Click to edit Master title style
VALSARTAN/SACUBITRIL(ENTRESTO)

Click to edit Master title styleEntresto – Improved outcomes
CV death or HF Hosp.
HR 0.80
NNT 21 over 2.25 yrs
p < 0.001
Overall Mortality
HR 0.84
NNT 36 over 2.25 yrs
p < 0.001
1.0
0.6
0.4
0.2
00 180 360 540 720 90010801260
1.0
0.6
0.4
0.2
00 180 360 540 720 900 10801260
NEJM 371;11 september 11, 2014
PARADIGM study

Click to edit Master title styleEntresto –Mechanism of Action
*Neprilysin substrates listed in order of relative affinity for neprilysin: ANP, CNP, Ang II, Ang I, adrenomedullin, substance P, bradykinin, endothelin-1, BNP
Ang=angiotensin; ANP=atrial natriuretic peptide; AT1=angiotensin II type 1; BNP=B-type natriuretic peptide; CNP=C-type natriuretic peptide; NEP=neprilysin; RAAS=renin-angiotensin-aldosterone system
Vasorelaxation
Blood pressure
Sympathetic tone
Aldosterone levels
Fibrosis
Hypertrophy
Natriuresis/diuresis
ANP, BNP, CNP,
other
vasoactive
peptides*
AT1 receptor
Vasoconstriction
Blood pressure
Sympathetic tone
Aldosterone
Fibrosis
Hypertrophy
Angiotensinogen
(liver secretion)
Ang I
Ang II
RAAS
Entresto
Sacubitril (AHU377; pro-drug)
InhibitingEnhancing
LBQ657
(NEP inhibitor)
OH
OHN
O
HO
O
Valsartan
N
NHN
N
N
O
OH
O
Inactive
fragments
15MDL099E
=Block
Schrier & Abraham. N Engl J Med
2009;341:577–85

Click to edit Master title style
39
• Symptomatic Systolic heart failure
• EF < 40%
• Maximum tolerated medical therapy
• ACEi or ARB + B-Blocker +/- MRA
• sBP > 100
• eGFR > 30
• K+ < 5.5 (caution when K+ 5-5.5)
Entresto –When to start
Click to edit Master title style
40
•Maximize triple therapy first
•Do not overlap the ACEi with ENTRESTO
•DO NOT PUT ON ACEi WITH ENTRESTO
•Titrate monthly
•Watch potassium and creatinine
•Watch fluid status
ENTRESTO KEY POINTS

Click to edit Master title style
41
• Stop ACE inhibitor > 36 hours pre
• Decrease diuretic dose if euvolemic
• Entresto 24/26 mg BID dose
• Titrate q 4 weeks
• Entresto 48/52 mg BID and Entresto 96/103 mg BID)
• Lytes, creatinine, urea 1 week and 3 weeks after first dose if K+≤5.1
• Lytes, creatinine, urea weekly x 3 after first dose if K+>5.1 but
K+<5.5.
HOW TO USE IT PRACTICAL SLIDES
PLUS GUIDELINES

Click to edit Master title style
42
• Hypotension SBP<90 mmHg with symptoms,
• Hypovolemic reduce/hold diuretics x 2-3 days
• If no improvement reduce or hold ENTRESTO for 1-2 weeks .
• Hypotension SBP<90 mmHg with symptoms,
• Euvolemic, reassess diuretic or vasodilator dose.
• Hypotension SBP<90 mmHg with symptoms,
• Hypervolemic, reduce/hold vasodilators +/- ENTRESTO for 1-2 weeks
HOW TO USE IT PRACTICAL SLIDES
PLUS GUIDELINES
Click to edit Master title style
IVABRADINE (Lancora)

CV mortality and HF hospitalization benefits(primary endpoint)
• The curves for ivabradine and placebo begin to diverge at 3 months,
and the difference is statistically significant at 6 months
18%
HR = 0.82 (0.75–0.90)
p<0.0001
Standard
therapy
Standard therapy
& ivabradine
40
30
20
10
0
0 6 12 18 24 30
Cu
mu
lati
ve
fre
qu
en
cy,
%
Months
Swedberg et al. Lancet 2010; 376: 875-85.
NNT: 26
Early
No. at risk
Placebo
Ivabradine
3 264
3 241
2 868
2 928
2 489
2 600
2 061
2 173
1 089
1 191
439
447
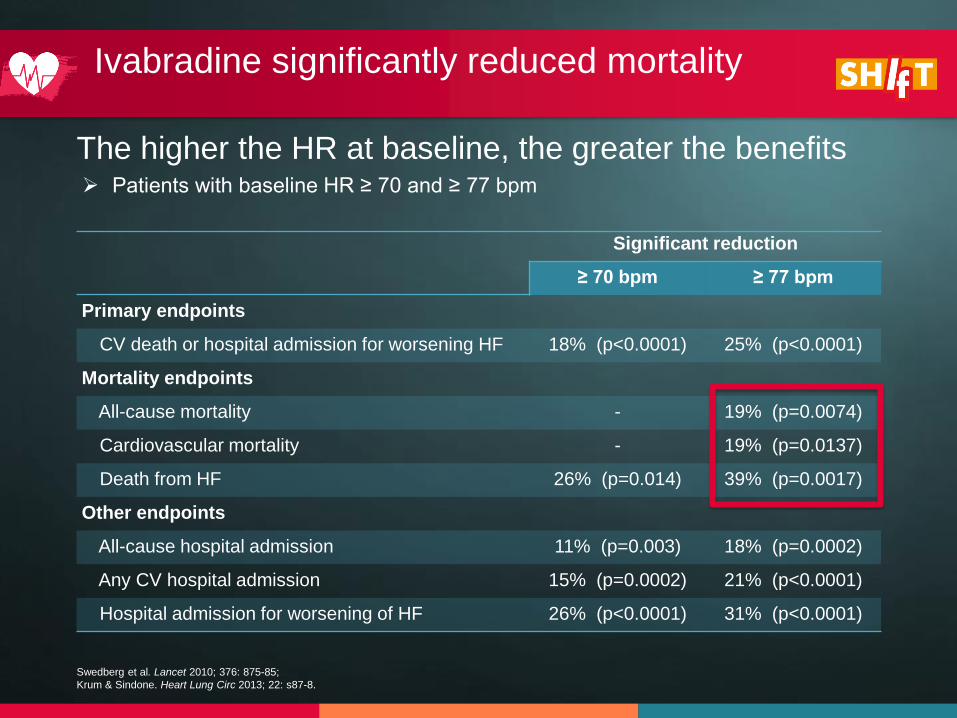
Significant reduction
≥ 70 bpm ≥ 77 bpm
Primary endpoints
CV death or hospital admission for worsening HF 18% (p<0.0001) 25% (p<0.0001)
Mortality endpoints
All-cause mortality - 19% (p=0.0074)
Cardiovascular mortality - 19% (p=0.0137)
Death from HF 26% (p=0.014) 39% (p=0.0017)
Other endpoints
All-cause hospital admission 11% (p=0.003) 18% (p=0.0002)
Any CV hospital admission 15% (p=0.0002) 21% (p<0.0001)
Hospital admission for worsening of HF 26% (p<0.0001) 31% (p<0.0001)
The higher the HR at baseline, the greater the benefits
Ivabradine significantly reduced mortality
Swedberg et al. Lancet 2010; 376: 875-85;
Krum & Sindone. Heart Lung Circ 2013; 22: s87-8.
➢ Patients with baseline HR ≥ 70 and ≥ 77 bpm
Click to edit Master title styleIvabradine – Mechanism of Action
• Slows action potential at sinus node
• Does not work on other parts of the conduction system• Sinus rhythm only (not atrial fib)
• Does NOT decrease BP
CCS 2014 Heart Failure
Guidelines

Click to edit Master title style
Ivabradine is safe to use and well tolerated by HF patients
Swedberg, Lancet, 2010, 376, 875-885
Safety
▪ Less serious adverse events cw
placebo
➢Explained by less cardiac events
▪ 1% Bradycardia (withdrawal)
▪ 3% transient phosphenes (visual)

Click to edit Master title styleIvabradine Practical Points
• Start at 5 mg po bid
• Sinus rhythm only
• After two weeks • HR > 60 7.5 mg bid
• HR < 50 2.5 mg bid
• No dosage adjustment for eGFR >15 or less than moderate hepatic disease

Click to edit Master title styleWhich is a true statement
1. A >20% improvement in renal function in CHF is associated with a good outcome
2. A > 20% worsening in renal function is CHF is associated with a good outcome
3. A >20% variability in renal function in either direction is associated with a bad outcome

Click to edit Master title style

Click to edit Master title styleRenal Failure
10
0
130
16
0

Click to edit Master title style
Click to edit Master title stylePractical Approach –CHF with Renal failure
• Like a skin lesion• 'If it's wet, dry it; if it's dry, wet it”
• Avoid hypovolemia• Avoid multiple diuretics or rapid diuresis
• Reduce diuretics during dehydrating illnesses

Click to edit Master title stylePractical Approach –CHF with Renal failure
• Volume overloaded• Diuresis without intravascular volume depletion
• Afterload reduction without hypotension
• Avoid nephrotoxins (NSAIDS)
• Hold RAAS agents, Use hydralazine nitrates
• 20-30% Δ acceptable
• Inotropes, Advanced support

Click to edit Master title style
IRON DEFICIENCY

Click to edit Master title styleIron Deficiency (ID) in HF
• If anemia R/O other causes of IDA
• Anemia
• Definition
•Ferritin < 100
•Ferritin 100-200 with TSAT < 20%• Iron therapy improves outcomes
• improved QoL
• reduced hospitalization for HF 19.4/100 pts to 7.6/100 pts
•Mortality benefit not shown to dateEur Heart J. 2015 Mar 14;36(11):657-68.
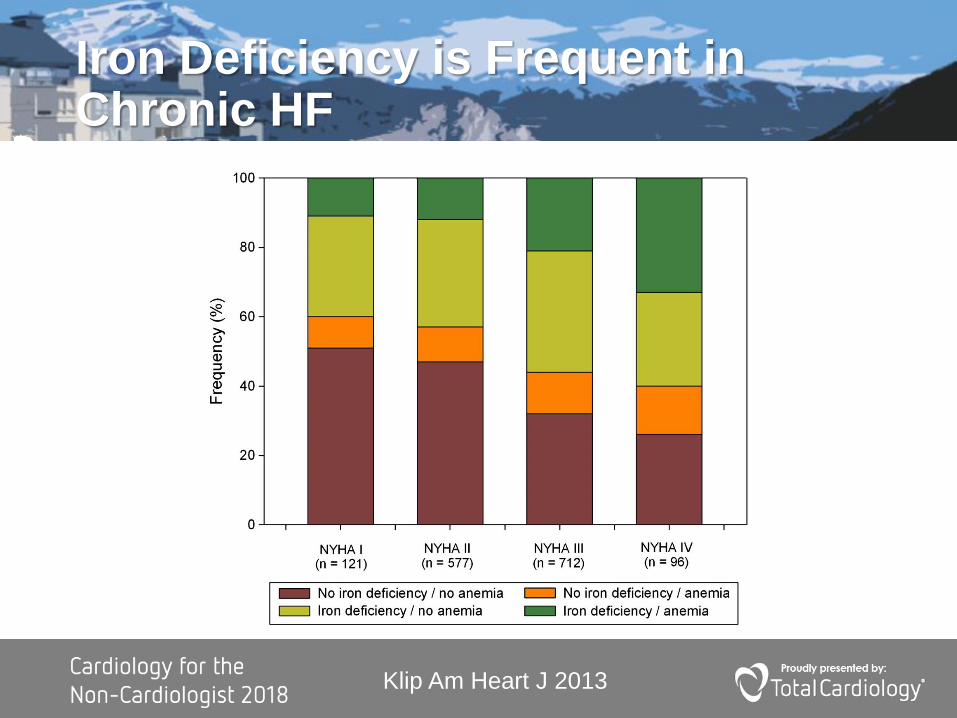
Click to edit Master title styleIron Deficiency is Frequent in Chronic HF
Klip Am Heart J 2013
Click to edit Master title styleIron Replacement in HF
• Oral iron is too slow!!!
• Start i.v. iron if max dose• 1000 to 2000 mg over 6 months
• Venofer 300mg q 2 months • FAIR-HF gave 200mg weekly
• Calculate deficiency • Ganzoni formula (link below)
• Ex.Target Hg 130, Current Hg 80, weight 80 kg• Deficiency 1460mg
http://www.al-nasir.com/www/PharmCalc/mob_exec_calc.php?ID=ganzoni

Click to edit Master title style
Heart Failure Preserved EF (HFpEF)
The disease formally known as diastolic heart failure

Click to edit Master title style
• Normal or near normal EF: • Heart Failure with preserved Ejection Fraction (HFpEF).
• Risk factors • advanced age, female gender, hypertension, obesity, chronic kidney
disease, diabetes mellitus, and coronary artery disease.
• Treatment difficult and not often very successful• Risk factor modification and diuretics.
• No therapy has been shown to improve survival in randomised control trials.
Heart Failure Preserved EF (HFpEF)

Click to edit Master title style
CCS 2014 Heart Failure Guidelines

Click to edit Master title styleHeart Failure Preserved EF (HFpEF)
• Symptoms ± signs
• LVEF >40-50%
• ↑BNP or NT-proBNP
• One of either• LVH or LAE
• Diastolic dysfx on imaging (ex echo)
LVH = Left ventricular hypertrophy, LAE = Left atrial enlargement, dysfx = dysfunction

JACC Vol. 62, No. 15,
2013

Click to edit Master title style
Total HF Hosp
Spiro : 394
Placebo: 475
P<0.01*
*poisson regression
245/1723 (14.2%)
206/1722 (12.0%)
TOPCAT Heart Failure Hospitalizations
Spironolactone
Placebo
HR = 0.83 (0.69 – 0.99)
p=0.042
Click to edit Master title style
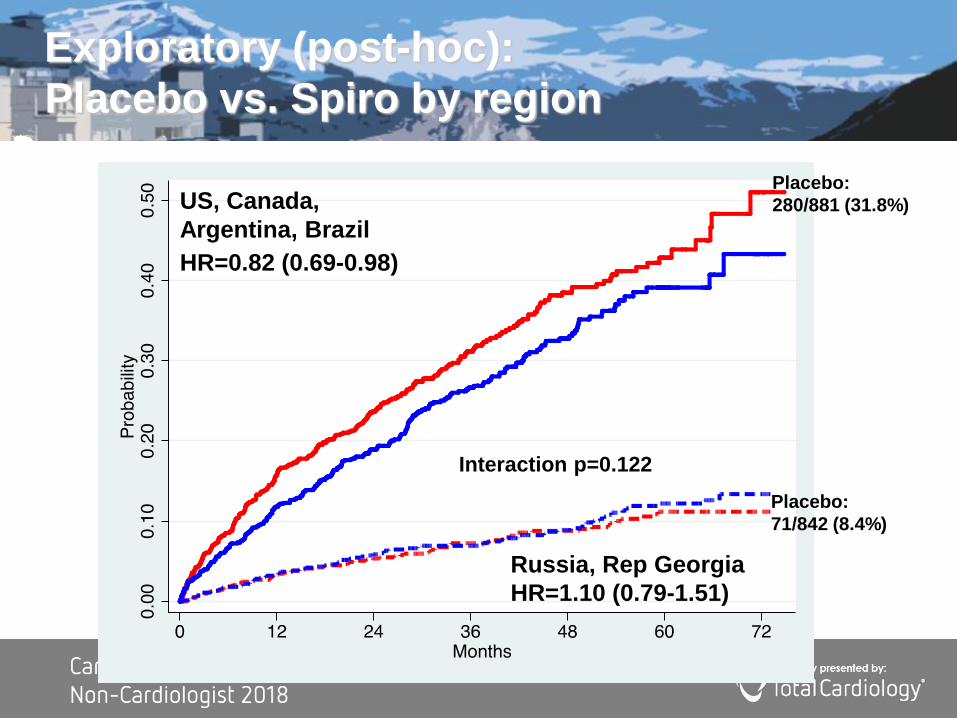
HR=0.82 (0.69-0.98)
HR=1.10 (0.79-1.51)
Interaction p=0.122
US, Canada,
Argentina, Brazil
Russia, Rep Georgia
Placebo:
280/881 (31.8%)
Placebo:
71/842 (8.4%)
Exploratory (post-hoc):
Placebo vs. Spiro by region

Click to edit Master title styleMRA (aldactone or eplerenone)
• HFpEF• elevated NP level (ex. BNP)
• eGFR > 30
• K+ <5.0
• Dose• 25 to 50 mg/day
• Watch K (especially if borderline elevated already)

Click to edit Master title styleOther Therapies
• ACEi & ARB – CCS but not ESC
• Await Paragon HF (2018)
• Await SGLT2i Dapa and Empa studies

Click to edit Master title styleKey Points
1. SGLT2i prevents CHF in DM patients with cardiovascular disease
2. Maximize Triple Therapy (TT) – prevention and treatment of CHF
3. Entresto (Valsartan/Sacubitral) and Lancora (Ivabradine) after TT
4. Cardiac Rehabilitation for CHF
5. CRS (cardiorenal syndrome) – decongest if possible
6. IV Iron therapy improves CHF with IDA
7. HFpEF – Diuretics, ACE/ARBi, MRA and exercise

Click to edit Master title style
Questions?

Click to edit Master title style
Implantable defibrillator (ICD)Cardiac resychronization (CRT)
Click to edit Master title style

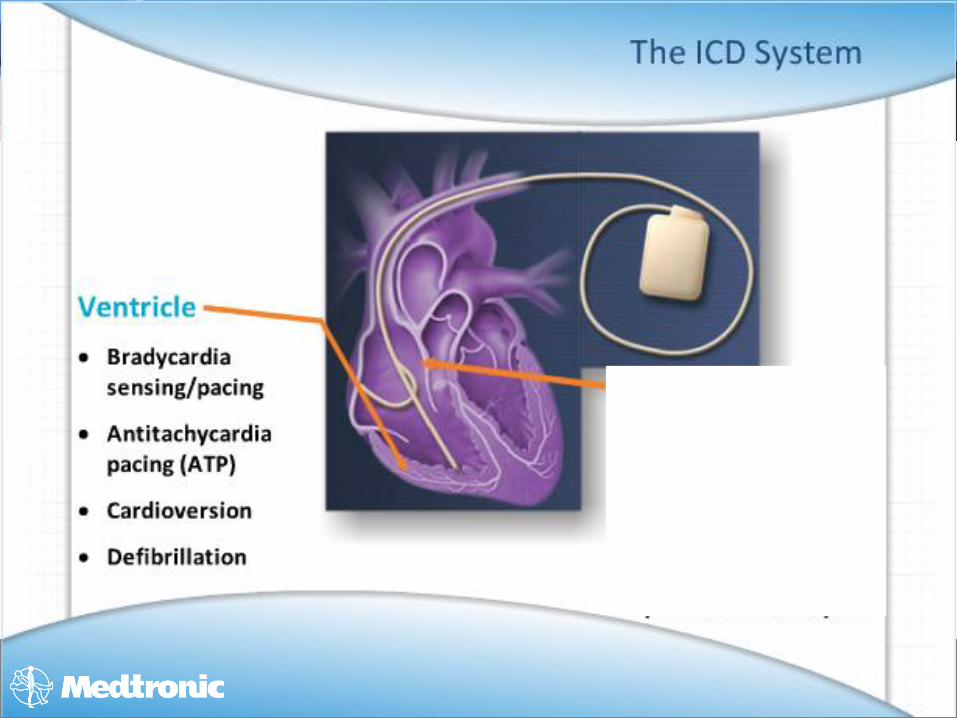
Click to edit Master title styleImplantable Cardioverter Defibrillator (ICD)
• Primary prevention• 2 deaths per year for every 100 devices
• Indications:• Ischemic CM:
• 3 mo. OMT persistent LVEF <30-35%
• Non-ischemic CM: • OMT with persistent NYHA ≥ II and
LVEF < 30-35%
• Cardiac Arrest
OMT – Optimal Medical Therapy CM - Cardiomyopathy

Click to edit Master title styleWhat is new in ICD therapy?
• ICD in non-ischemic CM• Possibly not beneficial (DANISH trial)
• Well treated population (titrated meds)
•96% on ACEi (91% of dose)
•92% on B-blocker (86% of dose)
•59% on MRA
•58% on CRT
•Subgroup < 60 y.o. (NNT 10 over 5.6 yrs)
NEJM Sept 6, 2016

Click to edit Master title styleCardiac Resynchronization Therapy (CRT)
Organized activation
Coordinated
contraction
Improved efficiency
Bi-ventricular
StimulationMimics normal
AV conduction

Click to edit Master title styleCardiac Resychronization Therapy (CRT)
• Pace RV and LV• Improve hearts coordination of contraction
• EF
• Mitral regurgitation.
• Improves heart failure symptoms
• Reduces mortality
OMT – Optimal Medical Therapy

Click to edit Master title styleCardiac Resychronization Therapy (CRT)
• Indication: • Persistent systolic HF (EF <30-35%)
• Optimal Medical Therapy
• QRS > 130 ms
• Ideal: LBBB with QRS > 150 ms
OMT – Optimal Medical Therapy

Click to edit Master title stylePractical Application of Guidelines -2015 update
• Referral timelines
• Frequency of visits
• Discharging criteria from HF clinic
• Titration order
• New therapies
• Medication titration app
• When to measure lytes, creatinine, BUN
• Hyper and Hypokalemia measurement
• How to manage increased creatinine
• Diuretic resistance and hyponatremia
• BP and HR targets
• When to re-measure EF
• When to measure BNP and NT-proBNP
• When can HF meds be stopped
• HFpEF
• How to manage an acute episode of gout
• Is my patient a candidate for heart surgery
• Management of the older patient with HF
CCS 2015 Heart Failure Guidelines


Click to edit Master title styleAcute Heart Failure - Precipitants
• Medication non-compliance
• Dietary non-compliance
• Acute illness (ex. Pneumonia)
• Increased BP
• Worsening primary/secondary disease (ex recurrent MI, worsening MR)

Click to edit Master title styleAcute Heart Failure - CHAMP
•Acute Coronary Syndrome
•Hypertension
•Arrhythmia
•Acute Mechanical Cause
•Pulmonary Embolism

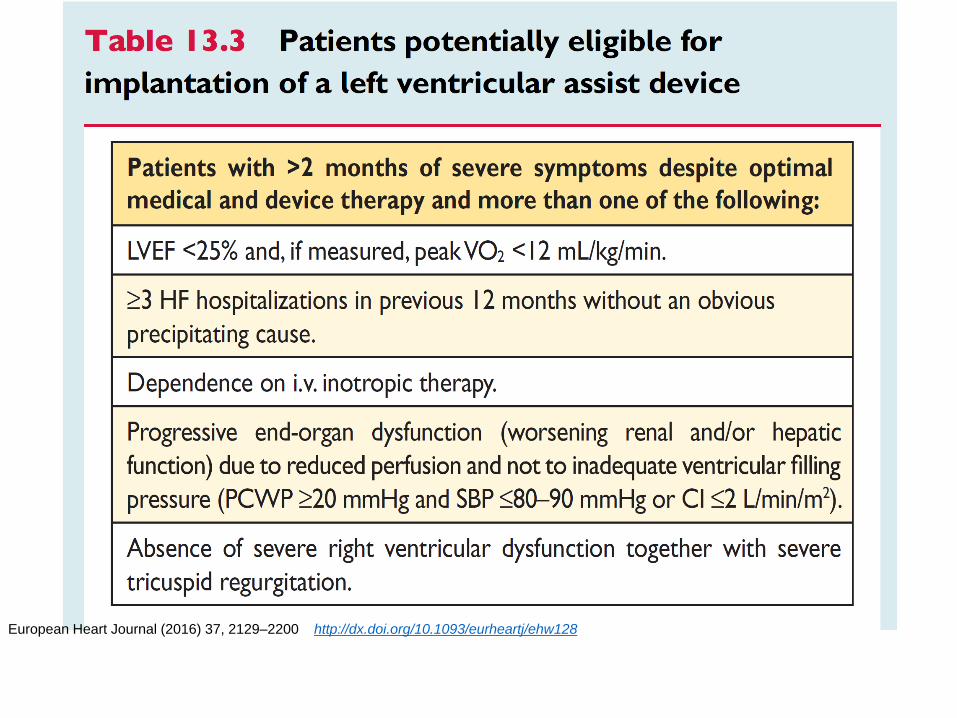
Click to edit Master title styleAdvanced Therapies
• Heart Failure clinics
• Advanced Heart Failure Teams• Acute Mechanical Circulatory Support
• Transplantation
• Destination therapy with implantable assist devices

Palliative Care
European Heart Journal (2016) 37, 2129–2200 http://dx.doi.org/10.1093/eurheartj/ehw128

Click to edit Master title styleNew Frontiers in TreatmentChronic Heart Failure
• Omecamtiv mecarbil (inotrope)• Cardiac Myosin activator
• Improves contractility without increasing O2 demand
• Finerenone (MRA)• Non-steroidal MRA, Less accumulation in kidney, Less hyper K
• FINESSE-HF (Phase III - hold)
• Vericiguat (bypass NO)• sGC stimulator
• VICTORIA 4900 pts – Jan 2020

Click to edit Master title styleDiastolic Heart Failure – New Frontiers
• Sildenefil
• Vericiguat
• Iron therapy
• Creating PFO shunt
• External and Internal devices to assist diastolic function
• Entresto (PARAGON-HF)
• Exercise / resistance training
Click to edit Master title styleKey Points
1. Heart failure incidence Increasing
2. BNP and NTproBNP
3. Maximize proven therapies
4. Entresto and Ivabradine
5. Cardiac Rehabilitation
6. ICD and CRT
7. i.v. Iron for low ferritin/Tsat
8. Goals of Care and Palliative care
Click to edit Master title styleUseful Links
• CCS Guidelines
• http://www.ccs.ca/en/guidelines/guidelines-library
• CCS Mobile Apps
• http://www.ccs.ca/index.php/en/apps
• Includes guidelines and titration apps
• ESC
• European Heart Journal (2016) 37, 2129–2200
• http://dx.doi.org/10.1093/eurheartj/ehw128

Click to edit Master title styleFluid Management
• Weigh Daily at same time in AM
• If weight increases/decreases by 1kg (2lb) over 2 days or 2.5kg (5lb) over a week
• Use Furosemide titration (up or down)
• Consider Metolazone
• Consider Tolvaptan
http://www.rxfiles.ca/rxfiles/modules/miscellaneous/search.aspx?for=furosemide+sliding
+scale
Click to edit Master title stylePotassium Management
• 5-5.5• Carry on and monitor closely
• 5.5-6.0• Stop one RAAS agent and recheck in 72 hours
• >5.9• Stop all RAAS agents
• Proceed to Urgent care/Emerg

Click to edit Master title styleGout
• Acute• Colchicine (usual dosage)
• Prednisone (does not appear to worsen HF)
• IA steroids
• Chronic (adjust as per renal disease)• Colchicine 0.6 mg bid
• Allopurinol
• Febuxostat
• Probenecid

Click to edit Master title styleSleep Disordered Breathing
• Central Sleep Apnea• Cheyne Stokes Respiration
• Do not use Adaptive Servo Ventilation (ASV)
• ASV worsens outcomes
• Obstructive Sleep Apnea (OSA)• CPAP, BiPAP or ASV
• Improved EF and 6 min. walk test
• No improvement in hospitalization or prognosis
N Engl J Med 2015;373:1095–1105
N Engl J Med 2005;353:2025–2033.

Click to edit Master title styleWho can stop HF meds
•Tachycardia related CM
•Alcoholic CM
•Chemotherapy CM
•Peripartum CM
•Valve replacement Surgery

Click to edit Master title styleDiagnosis in Office Setting
• Clinical Hx, PEx, ECG• If all normal HF ruled out
• One element abn check BNP
• Echocardiogram if• NT-proBNP >125 or
• BNP >35 or
• NP levels cannot be measured

Click to edit Master title styleTreatment Options
Treatment benefit CV
Mortality
HF Hosp QoL
Exercise Early ? ? +++
Aldactone Late +++ ++ ?
Ivabradine Acutely ? ? +
Statin Unknown +/- ? ?
B-Blocker No No No No
Statins Possible + ? ?

European Heart Journal (2016) 37, 2129–
2200
http://dx.doi.org/10.1093/eurheartj/ehw128

Click to edit Master title style
CCS 2014 Heart Failure Guidelines

Click to edit Master title style

Click to edit Master title styleWhat is next?
• Inotropes• All current inotropes increase mortality
• omecamtiv mecarbil• improves systolic function
• increasing the systolic ejection duration/stroke volume, without consuming more ATP energy
• Renal Vasodilatation• Seralaxin

CCS 2014 Heart Failure Guidelines

Click to edit Master title styleIvabradine Practical Points
•Food delays absorption
•CYP3A4 – avoid Azole, Macrolide, Protease inhibitor, Rate limiting CCB
•Avoid QT prolonging drugs
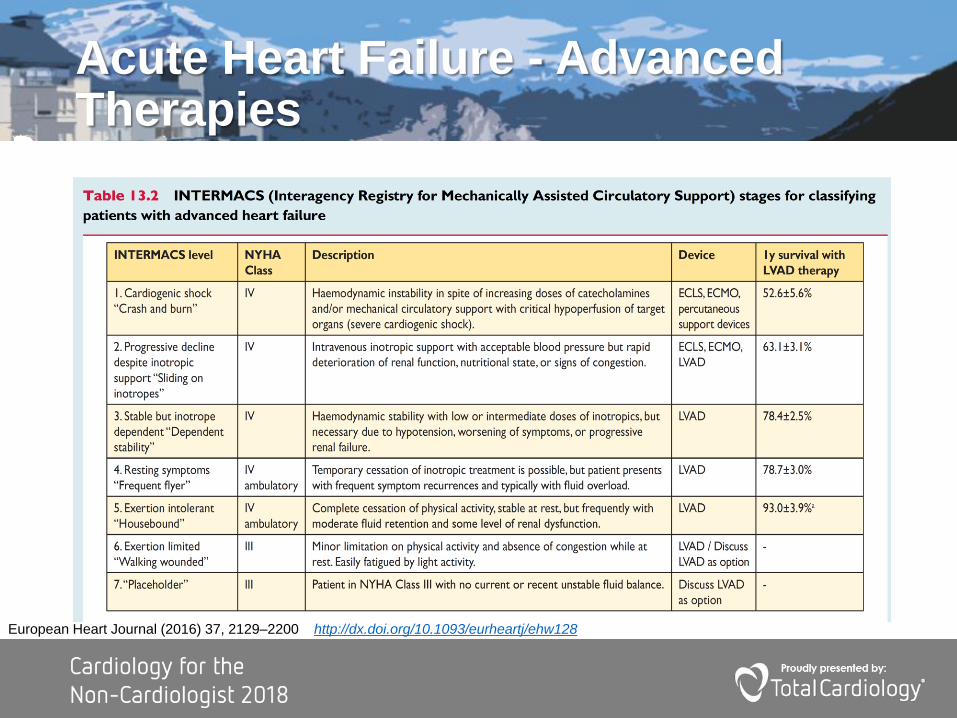
Click to edit Master title styleAcute Heart Failure - Advanced Therapies
European Heart Journal (2016) 37, 2129–2200 http://dx.doi.org/10.1093/eurheartj/ehw128

Click to edit Master title styleCHF – Next Frontiers
• Systolic Heart failure• Ulartide
• Nitric Oxide donors (Riociguat, sildenefil)
• MRA (Finerenone)
• B3 antagonist to inhibit sympathetic tone
• Serelaxin
• OMecaMtiv (inotrope)
• Anti-inflammation (Anakura)
• Mitrochondrial activation
• Pharmacogenetics
CCS 2014 Heart Failure
Guidelines

European Heart Journal (2016) 37, 2129–
2200
http://dx.doi.org/10.1093/eurheartj/ehw128
European Heart Journal (2016) 37, 2129–2200 http://dx.doi.org/10.1093/eurheartj/ehw128

Click to edit Master title styleWhen to use Tolvaptan
• Fluid overloaded
• Low sodium (Na < 130)
• 60mg/day
• Ongoing trials to assess outcome improvements

Click to edit Master title styleDiagnostic tests
•CBC, Electrolytes, Creatinine, LFTs, Glucose and HbA1c, Lipid profile, TSH, Iron Studies, (nt-pro)BNP
•ECG, CXR
•Echocardiogram
• Ischemic Test (angiogram, MPI, cMRI)
•Non-ischemic test (cMRI)
MPI – Myocardial perfusion test, cMRI – Cardiac MRI

Click to edit Master title styleDiuretic Resistance
• Loop Diuretics• Double oral dose
• Add IV
• Add Metolozone
• Consider Tolvaptan if Na < 130
• Aim for 0.5kg/day
• Restrict fluid to 2000 mL/day