heel pain
DESCRIPTION
MR imagingTRANSCRIPT

7/14/2019 Heel Pain
http://slidepdf.com/reader/full/heel-pain-56327df5543a9 1/11
AJR:200, April 2013 845
MRI of Heel Pain
David A. Lawrence1
Michael F. Rolen1
Khaled Abi Morshed2
Hicham Moukaddam1
Lawrence DA, Rolen MF, Morshed KA, Moukad-
dam H
1Department o Diagnostic Radiology, Yale University
School o Medicine, 333 Cedar St, PO Box 208 057,
New Haven, CT 065 20. Address correspondence to
H. Moukaddam ([email protected]).
2Department o Radiology, Beirut Arab University, Beirut,
Lebanon.
Musculoskeleta l Imaging • Review
CME/SAM
This article is available or CME/SAM credit.
AJR 2013; 200:845–855
0361–803X/13/2004–845
© American Roentgen Ray Society
Keywords: calcaneodynia, heel pain
DOI:10.2214/AJR.12.8824
Received February 28, 20 12; accepted ater revision
April 18, 2012.
Radiographs are oten obtained to exclude
acute causes o heel pain, such as calcaneal
racture; this has been well discussed in oth-
er articles and will not be urther addressed
here [2]. Some other causes o heel pain have
characteristic radiographic ndings, where-
as other causes have nonspecic ndings.
These will be discussed in this article.
MRI allows superior sot-tissue contrast
resolution, is noninvasive, and is widely avail-
able. It can be very helpul in equivocal cas-
es o heel pain. Additionally, some causes o
heel pain require surgical intervention (such
as an Achilles tendon tear), and the inorma-
tion gleaned rom MRI can infuence presur-
gical planning. In this article, we rst review
the normal anatomy o the posterior ankle and
hindoot and then review the causes o heel
pain, with attention to the clinical, radiograph-
ic, and MRI ndings.
Anatomy
Three ligamentous groups support the ankle:
the syndesmotic ligament complex, the lateral
collateral ligament, and the deltoid ligament.The syndesmotic ligament complex is com-
posed o the anterior and posterior tibiobular
(also known as the anterior inerior and posteri-
or inerior tibiobular) and interosseous liga-
ments. The lateral collateral ligament can be
subdivided into the anterior talobular, poste-
rior talobular, and calcaneobular ligaments.
The deltoid ligament contains the anterior and
posterior tibiotalar, tibiospring, tibiocalcaneal,
and tibionavicular ligaments.
Heel pain is a common problem that
may be due to a variety o sot-
tissue and osseous abnormalities.
Knowledge o the anatomy o the
posterior ankle and hindoot oers a useul way
to approach diagnosing the cause o the heel
pain: osseous, ligamentous, tendinous, and oth-
er sot-tissue structures. Some o the more com-
mon causes include Achilles tendinosis, Achilles
tendon tear, Achilles peritendinitis, Achilles
paratendinitis, insertional tendinitis o the Achil-
les tendon, retrocalcaneal bursitis, Haglund phe-
nomenon, plantar asciitis, plantar ascial tear,
calcaneal stress racture, calcaneal insuciency
racture, and Sever disease (in the pediatric
population). Radiographs are oten obtained
to exclude acute osseous abnormalities, such
as calcaneal ractures. MRI oers superior sot-
tissue contrast resolution and can be helpul
in diagnosis as well as in presurgical planning.
Heel pain, or calcaneodynia, is a common
problem, which may be present in up to 15%
o patients presenting to their primary care cli-
nician. Clinical examination is generally help-
ul in localizing the region o pain, which con-sequently can narrow the otherwise broad
dierential diagnosis (Table 1). Anatomical-
ly, heel pain may arise rom six structures: the
plantar ascia, tendons (e.g., Achilles, fex-
or digitorum longus), calcaneus, various bur-
sae, the tarsal tunnel, and the heel plantar at
pad [1]. Additionally, accessory muscles may
cause heel pain. The most common accessory
muscle is the accessory soleus muscle, which
may cause posteromedial ankle pain.
OBJECTIVE. The purpose o this article is to review the normal anatomy o the posterior
ankle and hindoot and review the causes o heel pain, with attention to the clinical, radio-
graphic, and MRI ndings.
CONCLUSION. Heel pain is a common problem that may be due to a variety o sot-
tissue and osseous abnormalities. Knowledge o the anatomy o the posterior ankle and hind-
oot oers a useul way in approaching heel pain. Some o the more common causes include
Achilles tendinosis, Haglund phenomenon, and plantar asciitis. MRI oers superior sot-tissue contrast resolution and can be helpul in diagnosis as well as in presurgical planning.
Lawrence et al.MRI o Heel Pain
Musculoskeletal ImagingReview

7/14/2019 Heel Pain
http://slidepdf.com/reader/full/heel-pain-56327df5543a9 2/11
846 AJR:200, April 2013
Lawrence et al.
These ligaments, as is true o ligaments
throughout the body, appear as thin linear hypo-
intense structures on both T1- and T2-weighted
images. Interposition o at between the liga-
ments can be seen in normal individuals [3].
The ligaments can routinely be evaluated on
three-plane MRI with a slice thickness o 3
mm or less.
Several ankle tendons are present in the
posterior ankle and hindoot. These include
the Achilles, posterior tibial, fexor digitorum
longus, fexor hallucis longus, and peroneal
tendons. Pathology o these tendons has been
well described in the radiology literature [3].
We will discuss the most common tendon to
be diseased: the Achilles tendon. The Achilles
tendon is ormed by the junction o the medial
and lateral heads o the gastrocnemius tendons
joining with the soleus tendon. The Achilles
tendon lacks a tendon sheath but is instead sur-
rounded by a peritenon (connective tissue also
called the paratenon), which is composed o
visceral and parietal layers. The vascular sys-
tem o the peritenon extends within and out-
side o the Achilles tendon. Importantly, 2–6
cm proximal to the calcaneal insertion there is
an area o diminished blood supply to the ten-
don, known as the “critical zone.” The poor
vascular supply to this area results in slow-
er tendon repair. Subsequently, this is where
most Achilles tendon disease occurs [4]. The
insertion site o the Achilles is an enthesis and
is intimately related to the retrocalcaneal bur-
sa [5]. Posterior to the tendon, there may be
an acquired or adventitial bursa, known as the
“retro-Achilles bursa.”
The ankle tendons appear as hypointense
linear structures on T1- and T2-weighted im-
ages. T2-weighted images are helpul or show-
ing intratendinous or peritendinous edema, the
hallmark o tendinitis. It is important to note
the magic angle eect, which occurs at ap-
proximately 55° with the main magnetic vector
(B0) in sequences with TEs less than approx-imately 35 milliseconds and may produce in-
creased signal within normal structures [6].
Careul analysis o the tendon in question in
multiple planes and evaluation with prolonged
TE sequences (T2-weighted) will help avoid
this pitall. The Achilles tendon has a normal
thickness o 6 mm [4]. On axial images, the
anterior margin o the Achilles tendon should
be concave or most o its course.
The retrocalcaneal bursa should measure less
than 1–2 mm in anteroposterior dimension [7].
I enlarged, it may represent disease, especially
i surrounding edematous changes are present.
The subcutaneous at should be seen between
the Achilles tendon and the skin. I this at can-
not be seen on MRI, a blister or retro-Achil-
les bursitis may be present. In particular, retro-
Achilles bursitis is distinguished by edematous
changes without mass eect on the skin [4].
The plantar aponeurosis consists o medial,
central, and lateral bands. The plantar ascia
represents the thickest central band. The plan-
tar ascia is adherent to the underlying fexor
digitorum brevis muscle. The plantar ascia
originates rom the medial calcaneal tuberosity
and splits into ve bands that insert onto each
TABLE 1: Differential Diagnosis [62]
Category Dierential Diagnosis Considerations
Arthritic Gout, rheumatoid arthritis, seronegative arthropathy; primary or secondaryosteoarthritis
Inectious Diabetic ulcer, osteomyelitis, plantar warts
Mechanical Plantar—plantar asciitis, heel spur, calcaneal stress racture, medial or lateral
plantar nerve entrapment, heel pad syndrome, oreign body granulomatosisPosterior—Achilles tendinopathy, Haglund deormity, ret rocalcaneal bursitis, tarsal
coalition, accessory muscles, Sever disease (pediatrics)
Neuropathic Lumbar radiculopathy, nerve entrapment, neuroma, tarsal tunnel syndrome
Trauma
Tumor (rare) Ewing sarcoma, neuroma
Vascular (rare)
Fig. 1—60-year-old man with several months o posterior heel pain.A and B, Sagittal STIR image (A) and axial proton-density image (B) show thickening o distal Achilles tendon(arrows , A) with no evidence o tear, consistent with Achilles tendinosis. Note loss o normal concave shape oanterior aspect o Achilles tendon (arrowhead , B).
Fig. 2—45-year-old man with posterior heel andlower leg pain. Axial STIR image shows diuse
thickening o distal Achilles tendon (arrows ) withintratendinous small ocus o increased near-uidsignal intensity. Note that normal concavity alonganterior aspect o tendon has been los t (arrowhead ).Findings are consistent with distal Achilles tendinosisand small intrasubstance tendon tear.

7/14/2019 Heel Pain
http://slidepdf.com/reader/full/heel-pain-56327df5543a9 3/11
AJR:200, April 2013 847
MRI of Heel Pain
o the proximal phalanges. On MRI, the nor-
mal ascia appears 2- to 4-mm thick and hypo-
intense on T1- and T2-weighted sequences [8].
Osseous anatomy is primarily dened by the
calcaneus. The calcaneus is the largest tarsal
bone and is designed to bear the weight o the
body. Traction trabeculae radiate rom the in-
erior cortex, and compression trabeculae ra-
diate to the anterior and posterior articular ac-
ets. The lateral surace o the calcaneus is fat
with a central peroneal tubercle where the cal-
caneobular ligament attaches. The lateral talo-
calcaneal ligament attaches anterosuperior to
the peroneal tubercle. Medially, the interos-
seous and medial talocalcaneal ligaments hold
the talus and calcaneus in close apposition.
The plantar aponeurosis inserts on the calca-
neus along the anterior and plantar aspect. The
Achilles tendon inserts along the middle por-
tion o the posterior aspect o the calcaneus.
The calcaneus usually ossies by the third
month o gestation. There is a normal vari-
ant in which the calcaneus develops rom two
ossication centers with an apophysis devel-
oping along the posteroinerior aspect o the
calcaneus. This apophysis begins ossication
at 4–7 years in girls and 7–10 years in boys. It
uses with the calcaneus by 12–15 years [9].
This can be important to remember in pediat-
ric patients presenting with heel pain.
Causes of Heel Pain
Achilles Tendinosis
Achilles tendinosis is oten the common
precursor by which most Achilles tendon dis-
ease stems and reers to intratendinous de-
generation by one o our main mechanisms:
hypoxic-bromatosis, myxoid, lipoid, and os-
seous-calcic [10].
Hypoxic degeneration is the most requent
type seen in ruptured Achilles tendons and is
thought likely secondary to the relative hypo-
A
A
Fig. 3—60-year-old man with acute onset oposterior heel pain while playing tennis.A, Sagittal T2-weighted image with at-saturationshows complete discontinuity o distal Achilles
tendon (arrowheads ), consistent with completeAchilles tendon tear with tendon retraction. Noteassociated increased T2 signal intensity, which likelyrepresents combination o edema and hemorrhage.B, Axial proton-density image shows residual
plantaris tendon (arrow ).
Fig. 4—30-year-old man with acute onset oposterior heel pain while playing basketball.A and B, Sagittal T1-weighted image (A) andT2-weighted image with at-saturation (B) showdiscontinuity o Achilles tendon (arrows , A)approximately 2 cm rom distal insertion, consistentwith complete Achilles tendon rupture. Note thathemorrhage in distal gast rocnemius muscle is seenas areas o increased T1 and T2 signal (circles ).
B
B
7/14/2019 Heel Pain
http://slidepdf.com/reader/full/heel-pain-56327df5543a9 4/11
848 AJR:200, April 2013
Lawrence et al.
vascularity o the 2–6 cm area o the tendon
that lies proximal to the calcaneal insertion,
known as the “watershed area” or “critical
zone” [11, 12]. This type o degeneration o-
ten ollows multiple symptomatic episodes
[12]. Axial MRI shows usiorm thickening
o the tendon with loss o the normal concave
anterior margin (Fig. 1) but oten lacks theinternal increased signal intensity seen with
other types o tendinosis [4].
The most common asymptomatic type o de-
generation is myxoid, whereby mucoid patches
and vacuoles intersperse between thinned ten-
don bers [13]. These vacuoles then coalesce,
resulting in the ormation o interstitial tears
along the long axis o the tendon. Because o
the asymptomatic nature o myxoid degenera-
tion, it is not rare or patients to show an Achil-
les tendon tear at initial presentation. On MRI,
mucoid deposits will show linear areas o in-
creased signal on T1-weighted and proton den-
sity sequences. T2-weighted and STIR imaging
will show interrupted and irregular areas o in-
creased signal within the tendon [4].
Lipoid degeneration results in atty de-
posits within the tendon and is the most age
dependent o the our types o degeneration
[14]. Interestingly, lipoid degeneration does
not alter the structural properties o the ten-
don and thus, does not predispose the tendon
to tear [15, 16]. However, lipoid degeneration
is related to xanthobromatosis, which o-
ten shows nodular thickening o the Achil-
les tendon with low to intermediate signal on
all MRI sequences but enhances ater the ad-
ministration o gadolinium [17].
The ourth type o degeneration resulting
in Achilles tendinosis is calcic tendinopathy.
Although rare, dystrophic calcication o the
tendon can progress to the ormation o cor-tical bone and trabeculae within the aected
area o the tendon, which distinguishes this
type o degeneration on radiography, CT, and
MRI [18].
Achilles Tendon Tear
Tears o the Achilles tendon oten occur in
middle-aged men between 30 and 50 years old
who engage in leisure athletic activities that in-
volve concentric loading, such as basketball
and tennis, resulting in indirect trauma to the
tendon [19]. Although most o these types o
tears occur in the watershed region o the ten-
don, more proximal tears at the myotendinous
junction can also occur, which are more com-
mon in younger men and can result rom direct
trauma [20]. Systemic diseases, such as rheu-
matoid arthritis, gout, lupus, and diabetes mel-
litus as well as fuoroquinolone use have also
been implicated in tears o the Achilles [21–23].
In terms o tear severity, the spectrum in-
cludes microtears, interstitial tears, partial tears,
and complete tears or ruptures [24]. Microtears
are not visible on imaging but are oten the incit-
ing event that leads to tendinosis [25]. Increased
signal on T2-weighted sequences is the MRI
nding common to interstitial, partial, and
complete tears [26].
Interstitial tears are oten the sequelae o
myxoid degeneration o the tendon as previ-
ously described and are longitudinally ori-
ented [4]. On MRI, linear areas o increasedsignal are seen on T1-weighted, proton den-
sity, and fuid-sensitive sequences, but the
surrounding bers are intact. Treatment in-
volves surgical débridement o the mucoid
degenerative center with oversewing o the
peripheral bers o the tendon [27].
Partial tears show heterogeneous high sig-
nal intensity on fuid-sensitive MRI sequenc-
es, and there is incomplete interruption o
the tendon bers (Fig. 2). Involved bers can
partially retract and display a rayed or cork-
screw appearance. Complete tears are identi-
ed by their high signal intensity fuid-lled
tendinous gap, with either distracted or over-
lapping bers (Figs. 3 and 4). Intratendinous
or peritendinous edema and hemorrhage are
oten present in the acute setting [23].
Surgical repair o partial and complete tears
is determined using the our-stage Kuwada
classication system, which is based primar-
ily on the size o the gap between the retract-
ed ends o the torn tendon: type I, partial tear
involving 50% or less o the tendon; type II,
complete tear with a gap o less than 3 cm;
A
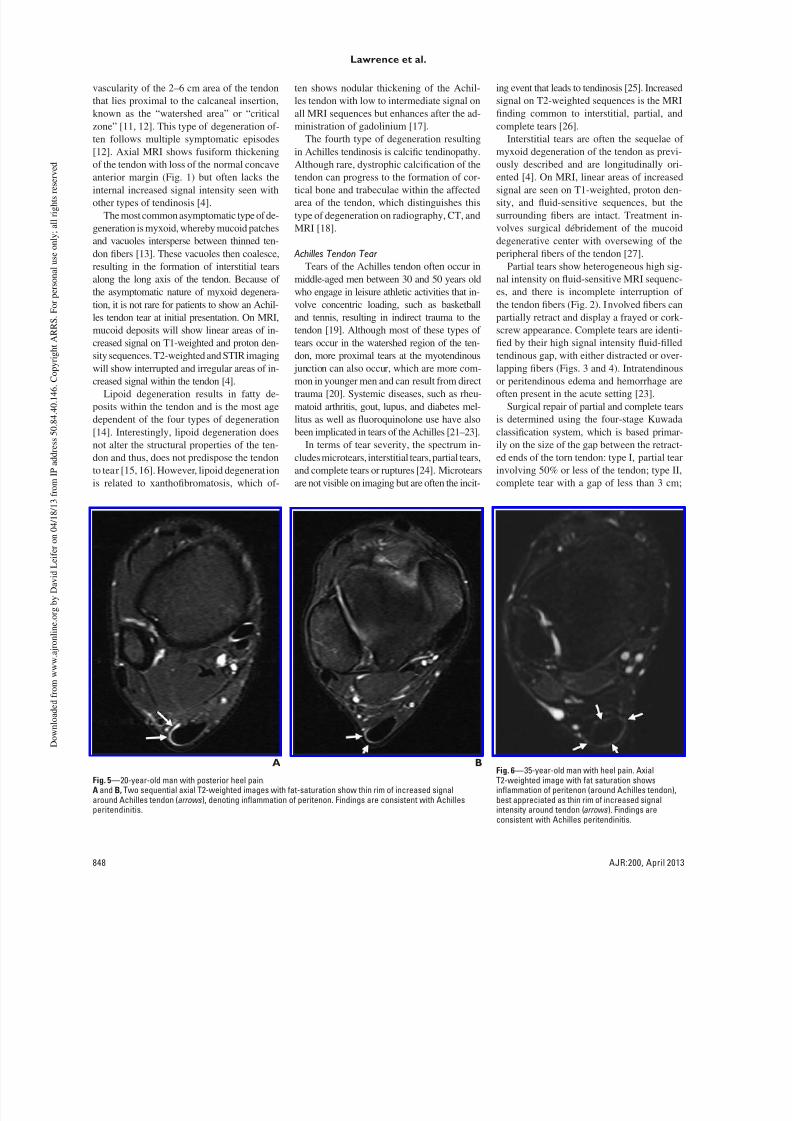
Fig. 5—20-year-old man with posterior heel pain.A and B, Two sequential axial T2-weighted images with at-saturation show thin rim o increased signalaround Achilles tendon (arrows ), denoting inammation o peritenon. Findings are consistent with Achillesperitendinitis.
Fig. 6—35-year-old man with heel pain. AxialT2-weighted image with at saturation showsinammation o peritenon (around Achilles tendon),best appreciated as thin rim o increased signalintensity around tendon (arrows ). Findings areconsistent with Achilles peritendinitis.
B

7/14/2019 Heel Pain
http://slidepdf.com/reader/full/heel-pain-56327df5543a9 5/11
AJR:200, April 2013 849
MRI of Heel Pain
type III, complete tear with a gap o 3–6 cm;
and type IV, complete tear with a gap o great-
er than 6 cm. Type I and II tears are typically
repaired with end-to-end anastomosis, where-
as an autogenous tendon grat fap is used or
type III tears. Type IV tears usually require a
ree tendon grat or synthetic grat [28].
Chronic tears can result in varying degreeso muscle atrophy, which can be reversible
or irreversible [29]. Reversible atrophy is o-
ten seen in the acute setting and is character-
ized by diuse edema noted throughout the
muscle [30]. Over time, the muscle takes on
a more atty inltrated appearance, which o-
ten signals irreversible atrophy [31]. O note,
the soleus is more susceptible to atrophy than
the gastrocnemius secondary to its greater
proportion o slow twitch type I bers [32].
Thereore, imaging protocols should include
sagittal views o the distal soleus when evalu-
ating or Achilles tendon injury.
Achilles Peri tendiniti s and Paratendinitis
Achilles peritendinitis reers to infamma-
tion o the connective tissue peritenon that
surrounds the tendon. Clinically, this entity
is similar to synovitis or tenosynovitis that
is seen in sheathed tendons. MRI shows high
T2 signal intensity around the tendon, which
is partially circumerential and is most evi-
dent along the posterior surace o the ten-
don (Figs. 5 and 6). However, given that the
Achilles tendon lacks a true synovial mem-
brane, the high T2 signal intensity is not as
bright as that seen with synovial fuid [4].A related entity is Achilles paratendinitis,
which, although the term is oten used inter-
changeably with peritendinitis, more accurate-
ly describes infammation o the pre-Achilles
(Kager) at pad. Fat-suppressed fuid-sensitive
sequences show increased signal and edema
with irregularity o the at pad anterior to the
tendon. T1-weighted images show replace-
ment o the normal high-signal-intensity at
(Fig. 7). Both peritendinitis and paratendini-
tis can be ound in conjunction with tendinosis
but may also be isolated ndings.
Retrocalcaneal BursitisAnother common cause o posterior heel
pain is retrocalcaneal bursitis, which can be a
maniestation o Achilles tendinosis but can
also be a separate entity. Repetitive trauma is
the most common cause and is requently ound
in runners. Other causes include rheumatoid
arthritis and seronegative spondyloarthropa-
thies [33]. Treatment is usually conservative,
although corticosteroid injection is sometimes
A
C
B
B
A
Fig. 7—70-year-oldwoman with heel pain.A, Lateral radiograph oankle shows increasedsot-tissue density inregion o pre-Achilles atpad (arrow ).B and C, Sagittal T2-weighted image with
at-saturation (B) andT1-weighted image (C)show inammatorychanges (arrowhead,B)in pre-Achilles (Kager) atpad. Note replacemento normal at seen on T1-weighted image (curved arrow, C), consistent withAchilles paratendinitis.
Fig. 8—40-year-old man with right heel pain.A, Lateral radiograph shows increased sot-tissue density in region o pre-Achilles at pad (arrow ).B, Sagittal T2-weighted image with at saturation shows uid distended bursa (arrowhead ) and surroundingsot-tissue inammation, consistent with retrocalcaneal bursitis.

7/14/2019 Heel Pain
http://slidepdf.com/reader/full/heel-pain-56327df5543a9 6/11
850 AJR:200, April 2013
Lawrence et al.
used [34]. However, caution should be exer-
cised i there is coexisting Achilles tendino-
sis because steroids can urther weaken an al-
ready at-risk tendon, making the tendon more
susceptible to tear or rupture [35, 36].
Radiography can show obliteration o the
normal retrocalcaneal at by the enlarged fu-
id-lled bursa (Fig. 8A). On MRI, a fuid col-
lection between the posterior calcaneus and
the insertion o the Achilles tendon can be
seen, which shows low signal intensity on T1-
weighted sequences and high signal intensity
on T2-weighted and STIR sequences (Figs.
8B and 9). Enlargement o the normal bursal
sac is the hallmark MRI nding, with values
greater than 7 mm craniocaudal, 11 mm trans-
verse, and 1 mm anteroposterior considered
abnormal [7]. Additionally, adjacent sot-tis-
sue infammatory changes are common.
Insertional Tendinosis of the Achilles Tendon
Insertional Achilles tendinosis is one o the
main causes o posterior heel pain [37]. Gen-
erally, this condition is secondary to chronic
A
A
Fig. 9—43-year-old woman with chronic heel pain.A, Axial oblique T2-weighted image with at saturation shows abnormally increased signal in region oretrocalcaneal bursa (asterisk ) and in subcutaneous tissues between posterior aspect o Achilles tendon and
skin (arrow ), consistent with retrocalcaneal and adventitial bursitis, respectively.B, Sagittal T2-weighted image with at saturation shows abnormal increased intratendinous signal intensity indistal Achilles tendon at its insertion (arrow ), consistent with insertional Achilles tendinitis. Additionally, notereactive bone marrow edema along posterior superior calcaneal tuberosity (arrowhead ).
Fig. 11—60-year-old old woman with heel pain.A, Sagittal T1-weighted image shows osseous excrescence along posterosuperior aspect o calcaneal tuberosity (arrow ), consistent with Haglund deormity.B and C, Sagittal (B) and axial (C) T2-weighted images with at saturation show bone marrow edema in region o Haglund deormity (arrowhead , B). Additionally, there isabnormally increased T2 signal intensity in region o retrocalcaneal bursa (asterisk , C) as well as between tendon and sk in (arrow , C), consistent with retrocalcaneal andadventitial bursitis, respectively. Furthermore, region o insertion o Achilles tendon shows evidence o edema (arrow , B), consistent with insertional Achilles tendinosis.
These fndings o inammation taken together with Haglund deormity are consistent with Haglund syndrome.
Fig. 10—40-year-old man with heel pain. Normalcalcaneal tuberosity is present. Calcaneal pitchlines are created by frst drawing lower pitch line
tangent to anterior tubercle. Upper pitch line is then
drawn parallel to lower pitch line at level o subtalararticular acet. Calcaneal tuberosity is enlarged i itextends superior to upper pitch line.
B
B C

7/14/2019 Heel Pain
http://slidepdf.com/reader/full/heel-pain-56327df5543a9 7/11
AJR:200, April 2013 851
MRI of Heel Pain
repetitive trauma with associated microtears
due to excessive use o the cal muscles. This
condition is most oten seen in ballet danc-
ers, runners, and athletes who participate in
jumping sports. Additionally, systemic con-
ditions, such as rheumatoid arthritis and se-ronegative spondyloarthropathies, are also
associated with the condition [37]. Infam-
mation o the peritenon may precede or be
associated with insertional Achilles tendino-
sis. Insertional Achilles tendinosis is also re-
quently associated with Haglund deormity
o the calcaneus.
MRI shows thickening o the tendon at its in-
sertion, with loss o the normal concavity o the
anterior margin o the tendon [37, 38]. Intraten-
dinous areas o increased signal may be seen
with some edema o the adjacent sot tissue
and possibly the adjacent calcaneal tuberosi-
ty at the level o the tendon insertion (Fig. 9).
Haglund Deformity and Syndrome
Haglund syndrome, rst described by Pat-
rick Haglund in 1927, is not an uncommon
cause o posterior heel pain and consists o a
constellation o sot-tissue and osseous abnor-
malities. The Haglund deormity is dened by
the presence o a prominent bursal bony pro-
jection o the calcaneus, which is generally as-
sociated with wearing low-back shoes. The
bony deormity, along with the shoes in ques-
tion, may lead to a mechanically induced in-
fammation o the supercial bursa, Achilles
tendinosis, and retrocalcaneal bursitis. These
infammatory changes in the presence o the
bony deormity are together known as Haglund
syndrome [9, 39]. Hindoot varus and pes ca-
vus are predisposing actors [40]. Most impor-tant is the presence o chronic stress.
On radiographs, the Haglund deormity is
maniested by a bony projection along the supe-
rior posterior aspect o the calcaneal tuberosity
on the lateral view (the radiographic equivalent
o the “pump bump”). Diagnosing an enlarged
calcaneal tuberosity is accomplished by draw-
ing parallel pitch lines along the superior and
inerior aspects o the calcaneus. The lower
pitch line is tangent to the anterior tubercle. The
upper pitch line is drawn parallel to the lower
pitch line and at the level o the subtalar articu-
lar acet (Fig. 10). The calcaneal tuberosity is
enlarged i it extends superior to the upper pitch
line [41]. Although radiography cannot be reli-
ably used to diagnose Haglund syndrome, loss
o the normal radiolucent retrocalcaneal recess
is important to note because it indicates retro-
calcaneal bursitis [1].
MRI may be required or ambiguous or
clinically equivocal cases. I present, a bony
bump along the superior posterior corner o
the calcaneal tuberosity is well visualized on
sagittal T1-weighted images (Fig. 11). T2-
weighted images will show excessive fuid
in the retrocalcaneal bursa and fuid in the
retro-Achilles bursa [4]. The presence o bone marrow edema in the calcaneal tuber-
osity supports the theory o the condition be-
ing caused by chronic repetitive mechanical
compression and infammation [42].
Plantar Fasciitis
Plantar asciitis is the most common cause
o inerior heel pain [43]. Plantar asciitis is
most commonly due to repetitive mechani-
cal stress, specically, prolonged pronation
stresses. This produces microtears and in-
fammation o the ascia and periascial sot
tissues. The condition is commonly seen in
runners and obese patients [44]. Additional-ly, it may be a result o an enthesopathy in
association with seronegative spondyloar-
thropathies, such as ankylosing spondylitis,
Reiter syndrome, or psoriatic arthritis [1].
Lateral radiographs oten show a calcaneal
spur, a very nonspecic nding [3].
MRI ndings include plantar ascial thick-
ening, intraascial edema on T2-weighted
images, edema surrounding the ascia on T2-
B
B
A
A
Fig. 13—52-year-old woman with plantar heel pain.A and B, Sagittal (A) and axial (B) T2-weighted images with at saturation show complete discontinuity oplantar ascia (arrow , A and B), consistent with ull-thickness tear o plantar ascia. Also note some uidsurrounding exor hallucis tendon sheath on axial image (arrowhead , B).
Fig. 12—42-year-old man with heel pain.A and B, Sagittal T2-weighted image with at-saturation (A) and T1-weighted image (B) show plantar ascia
thickening (arrows , B) and edema (arrowheads , A) along calcaneal insertion o plantar ascia, with reactivebone marrow edema. Findings are consistent with plantar asciitis. Also noted is small calcaneal bone spur,nonspecifc fnding.

7/14/2019 Heel Pain
http://slidepdf.com/reader/full/heel-pain-56327df5543a9 8/11
852 AJR:200, April 2013
Lawrence et al.
weighted images (primarily that the proxi-
mal aspect o the ascia is edematous), and in-
creased intraascial T1 signal [44] (Fig. 12).
Fascial thickening is dened as greater than 3
mm, with some cases thickening to 7–8 mm
[3]. The thickening is usually usiorm as op-
posed to the ocal nodular thickening o the as-
cia seen in plantar bromatosis. In addition, the
nodular thickening o plantar bromatosis oc-
curs distal to the calcaneal insertion at the lev-
el o the midoot. Furthermore, marrow edema
in the calcaneal tuberosity may be present [45].
Tear of the Plantar FasciaRupture o the plantar ascia is typically a
sports-related injury that is generally seen in
athletes engaged in running and jumping [46].
Additionally, it can be seen in patients with
chronic plantar asciitis receiving local corti-
costeroid injections [47]. Most cases o plan-
tar ascia rupture involve the proximal ascia
near its calcaneal insertion—similar to the lo-
cal edema seen in plantar asciitis. Distal (an-
terior) tears also may occur [37, 45].
Radiography has little role in diagnosing
plantar ascia rupture aside rom excluding
other causes o plantar heel pain. MRI nd-
ings are the same as would be seen in other
ascial or aponeurosis tears. Acute tears show
partial or complete disruption o the normallylow-signal-intensity ascia, with areas o ede-
ma and hemorrhage best seen on T2-weight-
ed or STIR sequences [1] (Fig. 13). Periascial
fuid accumulation is oten also seen. Further-
more, it is important to inspect the fexor digi-
torum brevis muscle because plantar ascia
rupture is commonly associated with tears o
the fexor digitorum brevis muscle [45]. Acute
and subacute muscle tears show intramuscu-
lar areas o increased signal on T1- and T2-
weighted images, representing bleeding and
edema within the muscle [1]. Less commonly,
strains o other plantar muscles may be pres-ent, such as the abductor halluces or quadratus
plantae muscles [45].
B
B
A
A
Fig. 16—12-year-old boy who presented with posterior heel pain and ocal tenderness.A, Sagittal T2-weighted image with at saturation shows bone marrow edema in calcaneal apophysis (arrow ). Findings are consistent with calcaneal apophysitis (Severdisease).B, Follow-up sagittal T2-weighted MR image with at saturation obtained ater 5 months shows resolution o bone marrow edema in calcaneal apophysis with clinicalresolution o symptoms. Additionally, ollow-up examination shows aint bone marrow edema in talus (arrowheads ), nonspecifc fnding (normal signal on T1-weightedimage not shown).
Fig. 14—82-year-old woman with chronic poorly defned heel pain.A and B, Sagittal T2-weighted image with at saturation (A) and T1-weighted image (B) show ill-defned bonemarrow edema inerior to posterior subtalar articular acet (arrow ) and low-signal-intensity (nondisplacedracture) line just deep in relation to posterior articular acet (arrowhead ), consistent with calcaneal stress(insufciency) racture.
Fig. 15—38-year-old woman with posterior heelpain. Sagittal T2-weighted image with at saturationshows abnormal curvilinear area o decreased T2signal intensity (arrow ), consistent with racture oposterior calcaneal tuberosity. Increased T2 signalin region o retrocalcaneal bursa (arrowhead ) isindicative o associated retrocalcaneal bursitis
and inammatory changes in pre-Achilles at pad.Findings are consistent with calcaneus stress(atigue) racture.

7/14/2019 Heel Pain
http://slidepdf.com/reader/full/heel-pain-56327df5543a9 9/11
AJR:200, April 2013 853
MRI of Heel Pain
Calcaneal Stress Fracture
The calcaneus is the second most common
site o atigue stress ractures, ater the meta-
tarsal bones. Insuciency stress ractures may
be seen in patients with rheumatoid arthritis or
neurologic disorders. Stress ractures general-
ly involve the posterosuperior or posterior as-
pects o the calcaneus and are usually orientedvertically or perpendicular to the long axis o
the calcaneus [1]. Patients with diabetes mel-
litus are at increased risk o calcaneal insu-
ciency ractures, particularly those involving
avulsion o the posterior process o the calca-
neus [48]. Stress ractures o the anterior two
thirds o the calcaneus may be more requent
than previously thought [49].
Radiographs are insensitive or acute stress
ractures, appearing normal in more than 70%
o the cases in one series [2, 50]. Follow-up ra-
diographs are diagnostic in only 50% o cases
[51]. When abnormalities are present, a stress
racture will show incomplete linear sclerosis
running orthogonal to the major trabeculae,
best seen on lateral radiographs.
CT is occasionally used to diagnose cal-
caneal stress ractures because it will show
disruption o the bony cortex with surround-
ing periostitis. The sensitivity o CT is high-
er than radiography but poorer than MRI and
bone scanning.
MRI shows characteristic ndings, includ-
ing bandlike areas o low signal intensity in the
medullary space, surrounding marrow space
signal abnormalities with ill-dened areas o
T1 hypointensity and T2 hyperintensity that
represent medullary edema, and hemorrhage
[1, 51, 52] (Figs 14 and 15). Periosteal callus
ormation starts shortly ater the racture and
appears as a hypointense line running parallel
to the cortex, which represents the elevated
periosteum [48].
Sever Disease (Calcaneal Apophysitis)
Apophyseal injuries are unique to the im-
mature skeleton; traction apophyseal injuries
may occur acutely at the site o tendinous in-
sertion. Chronic apophysitis is caused by in-
fammatory changes at the site o tendinous
insertion into a bony prominence. When this
occurs at the calcaneal apophysis, the associ-
ated eponym is Sever disease, rst described
by J. W. Sever in 1912.
Several authors have argued that calcane-
al apophysitis is primarily a clinical diagno-
sis [53, 54]. However, oot radiographs are
oten obtained to exclude other causes. Unor-
tunately, there are no pathognomonic radio-
graphic ndings o calcaneal apophysitis [55,
56]. Nonspecic radiographic eatures include
increased density and greater ragmentation
o the apophysis, which may also be seen in
healthy children [55].
As might be expected, MRI will show edem-
atous changes within the calcaneal apophysis,
possibly extending into the adjacent calcane-
al tuberosity (Fig. 16). Furthermore, in equiv-
ocal cases, MRI can be helpul in excluding
other causes o heel pain.
Os Trigonum Syndrome
The posterolateral talus has a variety o ana-
tomic variants, including a normal tubercle; en-
largement o the lateral tubercle o the posterior
process o the talus, known as the “Stieda pro-
cess”; and a separate ossicle, known as an “os
trigonum,” which may or may not be used to
the posterior process o the talus. The os trigo-num is considered by some to represent a de-
velopmental anomaly analogous to a secondary
ossication center because it is ormed by en-
dochondral ossication within a cartilaginous
extension rom the talus [57]. The mineralized
os trigonum appears between the ages o 7 and
13 years and usually uses with the talus within
1 year. In approximately 10% o patients, it re-
mains as a separate ossicle [58].
Clinically, the os trigonum is asymptomatic
unless impingement occurs; hence, os trigonum
syndrome is also known as “posterior ankle
impingement syndrome.” Other osseous abnor-
malities o the posterior talus may also result in
posterior ankle impingement syndrome, such as
the Steida process [59]. Strenuous activities that
result in extreme plantar fexion can cause com-
pression o the adjacent synovial and capsular
tissue against the tibia [60]. Thus, the syndrome
is oten seen in athletes participating in ballet,
ootball, and soccer.
On radiography, the normal os trigonum
generally shows smooth margins. Repetitive
trauma to the os trigonum may result in a
racture o the ossicle.
On MRI, os trigonum syndrome shows ab-
normal signal intensity in the lateral talar tu-bercle, the os trigonum, or both because o
the bone impaction (Fig. 17). Furthermore, in-
fammatory changes will generally be present
in the sot tissues o the posterior ankle, es-
pecially in the posterior synovial recess o the
subtalar and tibiotalar joints [59]. Infamma-
tory changes aecting the fexor hallucis lon-
gus tendon sheath may variably be present.
However, it is important to remember that the
fexor hallucis longus tendon sheath normally
communicates with the tibiotalar joint in ap-
proximately 20% o normal individuals; there-
ore, fuid in the tendon sheath may be normal.
Septations, contour irregularities, and abruptcuto o the fuid at the level o the posterior
talus are helpul distinguishers in diagnosing
tenosynovitis o the tendon sheath [61].
Conclusion
There are a variety o causes o heel pain, and
we have reviewed the most common causes. We
have primarily reviewed mechanical causes, by
ar the most common; however, it is important
BA
Fig. 17—18-year-old man with posterior ankle and heel pain.A and B, Sagittal T1-weighted image (A) and T2-weighted image with at saturation (B) show os trigonum(arrow , A) with bone marrow edema (arrowhead , B), consistent with os trigonum syndrome.

7/14/2019 Heel Pain
http://slidepdf.com/reader/full/heel-pain-56327df5543a9 10/11
854 AJR:200, April 2013
Lawrence et al.
to remember that there may be other causes
o heel pain, such as osteomyelitis, which
will present with a much dierent clinical
picture. Although clinical examination is o-
ten useul, imaging the hindoot is helpul or
solving equivocal cases as well as or preop-
erative planning by showing the exact loca-
tion and extent o the pathology. MRI has su-perior sot-tissue contrast resolution to other
modalities; thereore, it can usually provide a
specic diagnosis.
References
1. Narváez JA, Narváez J, Ortega R, Aguilera C,
Sanchez A, Andia E. Painul heel: MR imaging
ndings. RadioGraphics 2000; 20:333–352
2. Datary A, Haims AH, Baumgaertner MR. Frac-
tures o the calcaneus: a review with emphasis on
CT. RadioGraphics 2005; 25:1215–1226
3. Rosenberg ZS, Beltran J, Bencardino JT; Radio-
logical Society o North America. From the
RSNA reresher courses: MR imaging o the an-
kle and oot. RadioGraphics 2000; 20(spec
no):S153–S179
4. Schweitzer ME, Karasick D. MR imaging o dis-
orders o the Achilles tendon. AJR 2000;
175:613–625
5. Frey C, Rosenberg Z, Shere MJ, Kim H. The
retrocalcaneal bursa: anatomy and bursography.
Foot Ankle 1992; 13:203–207
6. Erickson SJ, Cox IH, Hyde JS, Car rera GF,
Strandt JA, Estkowski LD. Eect o tendon orien-
tation on MR imaging signal intensity: a manies-
tation o the “magic angle” phenomenon. Radiol-
ogy 1991; 181:389–3927. Bottger BA, Schweitzer ME, El-Noueam KI, De-
sai M. MR imaging o the normal and abnormal
retrocalcaneal bursae. AJR 1998; 170:1239–1241
8. Berkowitz JF, Kier R, Rudicel S. Plantar asciitis:
MR imaging. Radiology 1991; 179:665–667
9. Kumar R, Matasar K, Stansber ry S, et al. The cal-
caneus: normal and abnormal. RadioGraphics
1991; 11:415–440
10. Józsa L, Balint BJ, Rey A, Demel Z. Hypoxic
alterations o tenocytes in degenerative tendinopa-
thy. Arch Orthop Trauma Surg 1982; 99:243–246
11. Fox JM, Blazina ME, Jobe FW, et al. Degenera-
tion and rupture o the Achilles tendon. Clin Or-
thop Relat Res 1975; 107:221–224
12. Leach RE, DiIorio E, Ha rney RA. Pathologic
hindoot conditions in the athlete. Clin Orthop
Relat Res 1983; 177:116–121
13. Kannus P, Jozsa L. Histopathological changes
preceding spontaneous rupture o a tendon: a con-
trolled study o 891 patients. J Bone Joint Surg
Am 1991; 73:1507–1525
14. Adams CW, Bayliss OB, Baker RW, Abdulla YH,
Hunter-Craig CJ. Lipid deposits in ageing human
arteries, tendons and ascia. Atherosclerosis 1974;
19:429–440
15. Bureau NJ, Roederer G. Sonography o Achilles ten-
don xanthomas in patients with heterozygous amil-
ial hypercholesterolemia. AJR 1998; 171:745–749
16. Dussault RG, Kaplan PA, Roederer G. MR imag-
ing o Achilles tendon in patients with amilial
hyperlipidemia: comparison with plain lms,
physical examination, and patients with traumatic
tendon lesions. AJR 1995; 164:403–407
17. Bude RO, Adler RS, Bassett DR. Diagnosis o
Achilles tendon xanthoma in patients with hetero-
zygous amilial hypercholesterolemia: MR vs so-
nography. AJR 1994; 162:913–917
18. Richards PJ, Braid JC, Carmont MR, Maulli N.
Achilles tendon ossication: pathology, imaging and
aetiology. Disabil Rehabil 2008; 30:1651–1665
19. Hattrup SJ, Johnson KA. A review o ruptures o
the Achilles tendon. Foot Ankle 1985; 6:34–38
20. Miller WA. Rupture o the musculotendinous
juncture o the medial head o the gastrocnemius
muscle. Am J Sports Med 1977; 5:191–193
21. Mahoney PG, James PD, Howell CJ, Swannell AJ.
Spontaneous rupture o the Achilles tendon in a
patient with gout. Ann Rheum Dis 1981; 40:416–
418
22. Rask MR. Achilles tendon rupture owing to rheu-
matoid disease: case report with a nine-year ol-
low-up. JAMA 1978; 239:435–436
23. Stoller DW. Magnetic resonance imaging in or-
thopaedics and sports medicine, 3rd ed. Philadel-
phia, PA: Wolters Kluwer/Lippincott Williams &
Wilkins, 2007:2161
24. Józsa L, Balint BJ, Rey A, Demel Z. Fine struc-
tural alterations o collagen bers in degenerativetendinopathy. Arch Orthop Trauma Surg 1984;
103:47–51
25. Enwemeka CS, Spielholz NI, Nelson AJ. The e-
ect o early unctional activities on experimen-
tally tenotomized Achilles tendons in rats. Am J
Phys Med Rehabil 1988; 67:264–269
26. Aström M, Gentz CF, Nilsson P, Rausing A, Sjo-
berg S, Westlin N. Imaging in chronic Achilles
tendinopathy: a comparison o ultrasonography,
magnetic resonance imaging and surgical nd-
ings in 27 histologically veried cases. Skeletal
Radiol 1996; 25:615–620
27. Carden DG, Noble J, Chalmers J, Lunn P, Ellis J.
Rupture o the calcaneal tendon: The early and
late management. J Bone Joint Surg Br 1987;
69:416–420
28. Kuwada GT. Classication o tendo Achillis rup-
ture with consideration o surgical repair tech-
niques. J Foot Surg 1990; 29:361–365
29. Fleckenstein JL, Weatherall PT, Bertocci LA, et
al. Locomotor system assessment by muscle mag-
netic resonance imaging. Magn Reson Q 1991;
7:79–103
30. Rolle WA Jr, Herbison GJ, Wapner KL, Schweitzer
ME. Traumatic ocal posterior tibialis muscle de-
nervation. Foot Ankle Int 1995; 16:363–367
31. Fleckenstein JL, Peshock RM, Lewis SF, Haller
RG. Magnetic resonance imaging o muscle inju-
ry and atrophy in glycolytic myopathies. Muscle
Nerve 1989; 12:849–855
32. Booth FW. Time course o muscular atrophy dur-
ing immobilization o hindlimbs in rats. J Appl
Physiol 1977; 43:656–661
33. Gerster JC, Vischer TL, Bennani A, Fallet GH.
The painul heel: comparative study in rheuma-
toid arthr itis, ankylosing spondylitis, Reiter’s syn-
drome, and generalized osteoarthrosis. Ann
Rheum Dis 1977; 36:343–348
34. Yates DA. Use o local steroid injections. BMJ
1977; 1:495–496
35. Kleinman M, Gross AE. Achilles tendon rupture
ollowing steroid injection: report o three cases. J
Bone Joint Surg Am 1983; 65:1345–1347
36. Hugate R, Pennypacker J, Saunders M, Juliano P.
The eects o intratendinous and retrocalcaneal
intrabursal injections o corticosteroid on the bio-
mechanical properties o rabbit Achilles tendons.
J Bone Joint Surg Am 2004; 86-A:794–801
37. DiMarcangelo MT, Yu TC. Diagnostic imaging o
heel pain and plantar asciitis. Clin Podiatr Med
Surg 1997; 14:281–301
38. Kier R. Magnetic resonance imaging o plantar
asciitis and other causes o heel pain. Magn Re-
son Imaging Clin N Am 1994; 2:97–107
39. Pavlov H, Heneghan MA, Hersh A, Goldman AB,
Vigorita V. The Haglund syndrome: initial and di-
erential diagnosis. Radiology 1982; 144:83–88
40. Stephens MM. Haglund’s deormity and retrocal-caneal bursitis. Orthop Clin North Am 1994;
25:41–46
41. Chauveaux D, Liet P, Le Huec JC, Midy D. A new
radiologic measurement or the diagnosis o Ha-
glund’s deormity. Surg Radiol Anat 1991; 13:39–44
42. Hung EHY, Kwok WK, Tong MMP. Haglund syn-
drome: a characteristic cause o posterior heel
pain. 2009; 11:183–185
43. DeMaio M, Paine R, Mangine RE, Drez D Jr.
Plantar asciitis. Orthopedics 1993; 16:1153–1163
44. Grasel RP, Schweitzer ME, Kovalovich AM, et al.
MR imaging o plantar asciitis: edema, tears, and
occult marrow abnormalities correlated with out-
come. AJR 1999; 173:699–701
45. Roger B, Grenier P. MRI o plantar asciitis. Eur
Radiol 1997; 7:1430–1435
46. Leach R, Jones R, Silva T. Rupture o the plantar
ascia in athletes. J Bone Joint Surg Am 1978;
60:537–539
47. Sellman JR. Plantar ascia rupture associated
with corticosteroid injection. Foot Ankle Int 1994;
15:376–381
48. Kathol MH, el-Khoury GY, Moore TE, Marsh JL.

7/14/2019 Heel Pain
http://slidepdf.com/reader/full/heel-pain-56327df5543a9 11/11
AJR:200, April 2013 855
MRI of Heel Pain
Calcaneal insuciency avulsion ractures in pa-
tients with diabetes mellitus. Radiology 1991;
180:725–729
49. Sormaala MJ, Niva MH, Kiuru MJ, Mattila VM,
Pihlajamaki HK. Stress injuries o the calcaneus
detected with magnetic resonance imaging in
military recruits. J Bone Joint Surg Am 2006;
88:2237–2242
50. Greaney RB, Gerber FH, Laughlin RL, et al. Distri-
bution and natural history o stress ractures in U.S.
Marine recruits. Radiology 1983; 146:339–346
51. Anderson MW, Greenspan A. Stress ractures.
Radiology 1996; 199:1–12
52. Lee JK, Yao L. Stress ractures: MR imaging. Ra-
diology 1988; 169:217–220
53. Micheli LJ, Ireland ML. Prevention and manage-
ment o calcaneal apophysitis in children: an over-
use syndrome. J Pediatr Orthop 1987; 7:34–38
54. Manusov EG, Lillegard WA, Raspa RF, Epperly
TD. Evaluation o pediatric oot problems. Part II.
The hindoot and the ankle. Am Fam Physician
1996; 54:1012–1026, 1031
55. Schar billig RW, Jones S, Scutter SD. Sever’s dis-
ease: what does the literature really tell us? J Am
Podiatr Med Assoc 2008; 98:212–223
56. Kose O. Do we really need radiographic assess-
ment or the diagnosis o non-specic heel pain
(calcaneal apophysitis) in children? Skeletal Ra-
diol 2010; 39:359–361
57. Karasick D, Schweitzer ME. The os trigonum syn-
drome: imaging eatures. AJR 1996; 166:125–129
58. Lawson JP. Clinically signicant radiologic anatom-
ic variants o the skeleton. AJR 1994; 163:249–255
59. Cerezal L, Abascal F, Canga A, et al. MR imaging
o ankle impingement syndromes. AJR 2003;
181:551–559
60. Wredmark T, Carlstedt CA, Bauer H, Saartok T.
Os trigonum syndrome: a clinical entity in ballet
dancers. Foot Ankle 1991; 11:404–406
61. Lo LD, Schweitzer ME, Fan JK, Wapner KJ,
Hecht PJ. MR imaging ndings o entrapment o
the fexor hallucis longus tendon. AJR 2001;
176:1145–1148
62. Tu P, Bytomski JR. Diagnosis o heel pain. Am
Fam Physician 2011; 84:909–916
F O R Y O U R I N F O R M A T I O N
Thi s a rt icle is ava ila ble for CME /SAM cre dit . To access the e xam for this ar tic le, fol low the prompts ass oci ate d
with the online version of the article.