hemodialysis vascular accessmorbidity1 - jasnjasn.asnjournals.org/content/7/4/523.full.pdf · ogous...
TRANSCRIPT
Journal of the American Society of Nephrology 523
Hemodialysis Vascular Access Morbidity1Harold I. Feldman,2 Sidney Kobrin, and Alan Wasserstein
In a whom radial arteriovenous fistula is a viable
HI, Feldman, S. Kobrin, A. Wasserstein, Department ofMedicine, Renal Electrolyte and Hypertension Divison,University of Pennsylvania School of Medicine, Phila-delphia, PA
HI, Feldman, Department of Biostatistics and Epidemi-ology, and Center for Clinical Epidemiology and Bio-statistics, Universily of Pennsylvania School of Medi-cine, Philadelphia, PA
(J, Am, Soc. Nephrol. 1996; 7:523-535)
ABSTRACTComplications associated with hemodialysis vascularaccess represent one ofthe most important sources ofmorbidity among ESRD patients in the United Statestoday. In this study, new data on the magnitude andgrowth of vascular access-related hospitalization inthe United States is presented, demonstrating that thecosts of this morbidity will soon exceed $1 billion peryr. This study also reviews published literature on themorbidity associated specifically with native arterio-venous fistulae, polytetrafluoroethylene bridge grafts,and permanent central venous catheters. Next, newinformation on the changing palterns of vascularaccess type in the United States is presented, demon-strating the continuing evolution of medical practiceaway from the use of arteriovenous fistulae in favor ofmore reliance on synthetic bridge grafts. Based onthese data, a discussion is provided of the tradeoffsamong the most commonly available modalities ofvascular access today. Although radial arteriovenousfistulae continue to represent the optimal access mo-dality, the appropriate roles for brachial arterio-venous fistulae, synthetic bridge grafts, and centralvenous catheters are less certain because of made-quate data on the long-term function of the first andthe high rates of complications associated with thelatter two. To reduce vascular access-related morbid-ity, strategies must be developed not only to preventand detect appropriately early synthetic vascularaccess dysfunction, but to better identify the patients
1 ReceIved June 2, 1995. Accepted January 3, 1996.
2 Correspondence to Dr. H.!. Feldman, Center for Clinical Epidemiology and
Biostatistics, University of Pennsylvania School of Medicine, 720 Blockley Hall, 423ServIce Drive, Philadelphia, PA 19104.6021.
104&667310704.0523$03.00/0Journal of the American Society of NephrologyCopyright C 1996 by the American Society of Nephrology
clinical option.
Key Words: Arteriovenous fistula, polytetrafluorene bridgegraft, permanent central venous catheter, hospitalization,
ESRD
C hronlc hemodialysis for patients with ESRD first
became technically feasible in 1960 with theintroduction of the Quinton-Scribner shunt (1). Al-
though this external arteriovenous (AV) shunt pro-vided, for the first time, direct access to the circulation
so that hemodialysis could be performed in the out-
patient setting, patient care was complicated by fre-
quent thrombosis and infection (1-3). Autologous ax-
teriovenous fistulae (A’IF’), introduced by Brescia and
Cimino in 1966, overcame many of the problems of
external dialysis shunts (4). Subsequent to this ad-
vance in dialysis vascular access surgery, AVF be-came the primary mode of achieving vascular access
for chronic hemodialysis. Once an AVF has maturedand been used for dialysis, the subsequent or second-
ary failure rate is low, with most patients enjoying
long-term fistula function lasting for many years (3-
5).Since the early 1970s, the rapid growth of the U.S.
ESRD Program has been accompanied by a diminu-
tion in the use ofAVF in favor ofalternative types of AV
bridge grafts and, more recently, permanent indwell-ing central venous catheters. This evolution has been
attributed to the growing primary failure rate of AVF,
often attributed to the increasing age and comorbidity
of the dialysis population, as well as the more rapidusabifity of alternative vascular accesses as compared
with AVF (6-1 1). Supporting this formulation is the
extensive change in the the demographics of the U.S.ESRD population over the past two decades. Although
only 6.6% ofESRD patients had diabetes in 1972 andfewer than 20% of ESRD patients were older than 65
yr of age, 36% of the ESRD population in 199 1 had
diabetes and nearly 1 in 2 (45%) was 65 yr of age or
older (12). It has been estimated that fewer than 25%
of incident ESRD patients successfully undergo theconstruction of a native AV fistula, an estimate re-
cently borne out by special studies conducted by the
U.S. Renal Data System (10,13,14).
Early alternative surgical techniques utilizing autol-
ogous saphenous vein grafts and implanted bovine
carotid heterografts to form bridge AV anastomoses
had unacceptably high rates of thrombosis and pseu-
doaneurysm (2,3,6, 15-17). In an attempt to achieve
better long-term success for dialysis vascular ac-
cesses, the same synthetic materials used for artery to
Hemodialysis Vascular Access Morbidily
524 Volume 7 ‘ Number 4 ‘ 1996
TABLE 1 . Hospitalization for vascular access morbidity, 1984 to 19860
Diagnosis/Hospital Stay 1984 1985 1986
Total number of ESRD hospital stays for any diagnosis 150,775 158,634 170,572Frequency of hospital stays with ICD-9 996. 1b 6,079 5,755 5,953Frequency of hospital stays with ICD-9 996.#{243}c 5,83 1 6,837 7,889Frequency of hospital stays with ICD-9 996#{149}7d 1 1 791 13,452 15,899Total number of stays with 996.1, 996.6, or 996.7 listed 23,701 26,044 29,741
as any diagnosisTotal number of stays with 996. 1 , 996.6, or 996.7 listed 9, 170 21 01 6 24,025
as first diagnosisAccess-related stays as percentage of Total 15.7 16.4 17.4Mean length of access-related stays 7.6 7.3 7.4
a Adapted from data presented in Reference 19: Feldman HI, Held PJ. Hutchinson 1. Stoiber E. Hartigan, MF, Berlin JA: Hemodialysis vascular accessmorbidity in the U.S. Kidney mt 1993:43:1091-1096.b Mechanical complication of vascular device, implant. and graft.C Infection and inflammatory reaction as a result of internal prosthetic device, implant. and graft.d Other complications of internal prosthetic device, implant, and graft.
artery vascular bypass procedures were implanted
into dialysis patients as bridging AV anastomoses.
Dacron#{174} (E.I. duPont de Nemours and Co. , Wilming-ton, DE) was used initially chosen for these access
devices but was rapidly replaced by polytetrafluoro-
ethylene (PTFE) (GoreTex#{174}, W.L. Gore and Assoc.,
Flagstaff, AZ: Impra#{174}, Impra, Inc. , Tempe, AZ) after
early experience suggested better short-term patency
rates with this newer synthetic material (10, 1 8). As
will be discussed below, the substitution of synthetic
access grafts for AVF has been accompanied by enor-
mous growth in the rate of secondary vascular access
failure, along with its attendant costs.
Below. we provide new data from Medicare’s ESRD
Program and summarize published research describ-
ing the morbidity associated with hemodialysis vascu-
lar accesses in current use today in the United States,
including AVF, PTFE bridge grafts, and indwelling
central venous catheters. We also provide recent data
from the U.S. Renal Data System on the continuing
transition from AVF to alternative synthetic access
devices. Finally, we present a discussion of the
tradeoffs involved in choosing a type of vascular ac-
cess in the clinical setting, and the data needed to
establish appropriate guidelines for making this
choice.
VASCULAR ACCESS COMPLICATIONS IN THEUNITED STATES
We have previously reported on the magnitude of
vascular access morbidity in the United States by
using hospitalization claims data from Medicare’s
End-Stage Renal Disease database, the ESRD Pro-
gram’s Medical Management Information System
(ESRD PMMIS) (19). Vascular access complications
were tabulated by counting the number of hospital
stays for one of three ICD-9 diagnosis codes recorded
as the first diagnosis in the hospitalization record of
PMMIS.*
Prevalent Medicare-entitled U.S. ESRD patients in
1984, 1985, and 1986 were studied (see Table 1).
Complications of vascular accesses alone accounted
for one of the most important causes of hospitalization
in the ESRD population. Between 1984 and 1986, the
number of hospitalizations for revision of dialysis
vascular accesses rose by 25.0% and represented
14. 1% of all ESRD hospitalizations that year.
Data recently published by Lazarus et at. (20) from
the network of dialysis units managed by National
Medical Care (NMC) also examined vascular access-
related morbidity as reflected in hospitalization forvascular access complication-related diagnoses by us-
ing a similar methodology. Between 1986 and 1990,
Lazarus et aL studied over 25,000 NMC patients who
were monitored for vascular access-related hospital-
ization. The authors reported that the proportion of all
hospital days related to vascular access dysfunctiongrew from about 6% in 1988 to nearly 1 1% by the end
of 1990, suggesting that vascular access-related hos-
pitallzation is growing faster than hospitalization for
other types of morbidity in the ESRD population.
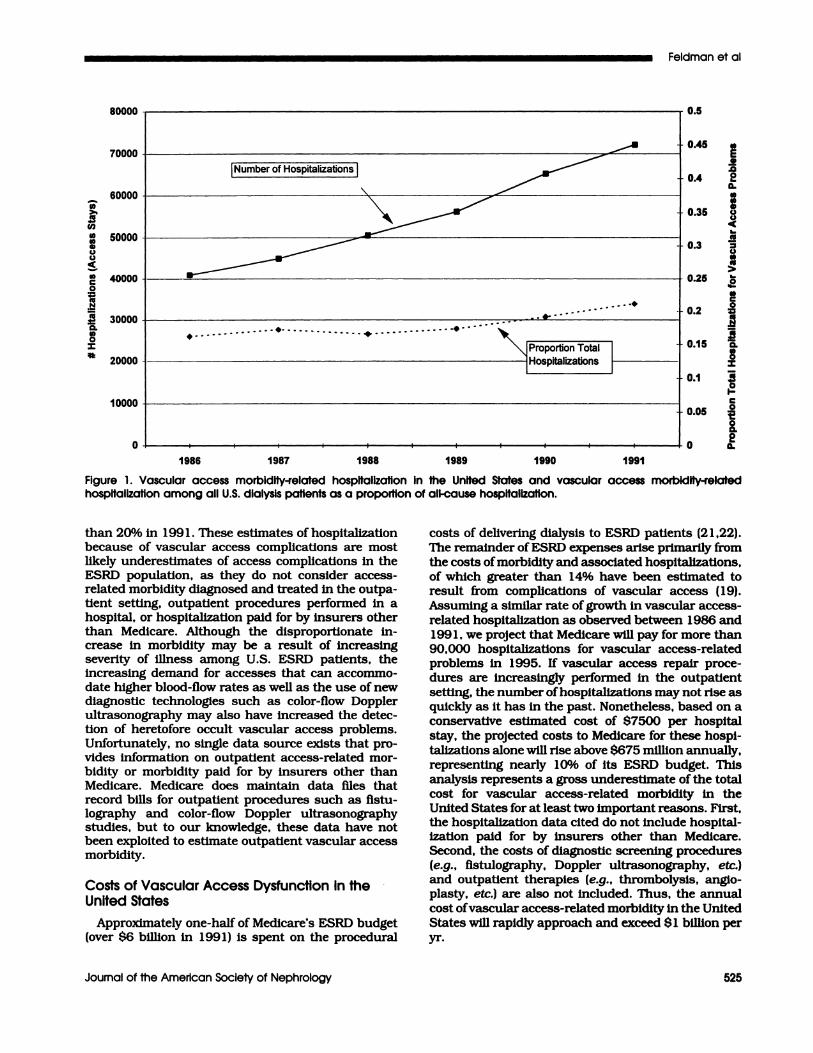
Recently we have extended our analyses character-
izing the burden of vascular access morbidity in the
United States between 1 986 and 1 99 1 on the basis ofdata from Medicare (see Figure 1). During this time
period, the number of vascular access-related stays
grew to over 70,000. Although this rise in access-related hospitalization emanates, in part, from the
growth in the U.S. ESRD population, Figure 1 alsodemonstrates that vascular access-related hospital-
ization as a percentage ofall-cause hospitalization has
also risen from approximately 1 7% in 1 986 to greater
* The three ICD-9 codes searched for included: 996.1, Mechanical complicationof vascular device, Implant, and graft 996.6, InfectIon and inflammatory reac-tion due to Internal prosthetic device, implant, and graft: and 996.7, Othercomplications of internal prosthetic device, Implant, and graft.
0.5
0.45
0.4
0.35
80000
70000
60000
50000
40000
30000
20000
10000
0
Figure 1 . Vascular access morbidity-related hospitalization In the United States and vascular access morbidity-relatedhospitalization among all U.S. dialysis patients as a proportion of all-cause hospitalization.
0.3
0.25
Cl,
E5,
.00a.(#5C’,4,UU
,(
CC’
U(I,CC’
>
0
CC,
0
CC’
.1:�
0.U,0
I
(C’
0I-C0
t00.0
0 a.
0.2
0.15
0.1
1986 1987 1988 1989 1990 1991
0.05
Feldman et al
Journal of the American Society of Nephrology 525
U,>.
U,‘I,U,0C.,U
U,
0
CUN
CU
0.U,0
I
than 20% in 199 1 . These estimates of hospitalization
because of vascular access complications are most
likely underestimates of access complications in theESRD population, as they do not consider access-
related morbidity diagnosed and treated in the outpa-
tient setting, outpatient procedures performed in a
hospital, or hospitalization paid for by insurers other
than Medicare. Although the disproportionate in-crease in morbidity may be a result of increasing
severity of illness among U.S. ESRD patients, the
increasing demand for accesses that can accommo-
date higher blood-flow rates as well as the use of new
diagnostic technologies such as color-flow Doppler
ultrasonography may also have increased the detec-
tion of heretofore occult vascular access problems.
Unfortunately, no single data source exists that pro-
vldes information on outpatient access-related mor-
bidity or morbidity paid for by insurers other than
Medicare. Medicare does maintain data ifies that
record bills for outpatient procedures such as fistu-lography and color-flow Doppler ultrasonography
studies, but to our knowledge, these data have notbeen exploited to estimate outpatient vascular access
morbidity.
Costs of Vascular Access Dysfunction in theUnited States
Approximately one-half of Medicare’s ESRD budget(over $6 billion in 199 1) is spent on the procedural
costs of delivering dialysis to ESRD patients (21,22).
The remainder of ESRD expenses arise primarily from
the costs ofmorbidity and associated hospitalizations,of which greater than 14% have been estimated to
result from complications of vascular access (19).
Assuming a similar rate of growth in vascular access-
related hospitalization as observed between 1986 and
199 1 , we project that Medicare will pay for more than
90,000 hospItalizations for vascular access-related
problems in 1995. If vascular access repair proce-
dures are increasingly performed in the outpatient
setting, the number ofhospitaJlzations may not rise as
quickly as it has In the past. Nonetheless, based on a
conservative estimated cost of $7500 per hospital
stay, the projected costs to Medicare for these hospi-talizations alone will rise above $675 million annually,representing nearly 10% of its ESRD budget. Thisanalysis represents a gross underestimate of the total
cost for vascular access-related morbidity in the
United States for at least two important reasons. First,
the hospitalization data cited do not include hospital-
ization paid for by insurers other than Medicare.
Second, the costs of diagnostic screening procedures(e.g., fistulography, Doppler ultrasonography, etc.)and outpatient therapies (e.g., thrombolysis, anglo-
plasty, etc.) are also not included. Thus, the annual
cost ofvascuiar access-related morbidity in the United
States will rapidly approach and exceed $ 1 billion per
yr.
Hemodlalysis Vascular Access Morbidity
526 Volume 7 . Number 4 ‘ 1996
ARTERIOVENOUS FISTULAE
Arteriovenous Fistula FunctionNumerous investigators have studied the likelihood
of successful maturation ofAVF into functional hemo-
dialysis vascular accesses (5,8, 17,23-32). Primary
failure of AVF is defined as insufficient dilation and
arterialization needed for function as a dialysis vascu-
lar access. The observed risk of primary failure of
these accesses has ranged from 9% (24) to 30% (1 7) in
surgical experience accumulated since the late 1960s.
Once AVF mature, numerous investigators have doc-
umented their excellent long-term function. Winsett
and Wolma reported the complication rates for 273AVF after successful maturation into functional vas-
cular accesses ( 1 7). After 2 yr of dialysis, 90% of these
accesses continued to function, with 80% still in use
after 3 yr. They observed a complication rate of five
events per 1000 patient-months of follow-up for AVF,which was considerably and statistically smaller than
the 37 events per 1000 patient-months observed in
recipients of PTFE synthetic dialysis grafts. Similar
fistula survival rates were also cited by Reilly and
colleagues in their report of 148 AVF created in En-gland between 1976 and 1981 (25) and more recently
by Kherlakian and colleagues (8). Bonalumi and co-
workers have reported the longest follow-up of AVF,
observing that 52% ofend-to-end radial artery fistulae
continued to be useful after 6.5 yr of hemodlalysis (5).
More recently, native AVF constructed using the
brachial artery have been evaluated as an alternative
access procedure when a radiocephalic fistula was not
able to be constructed (33-35). Although uncontrolled
studies have documented primary patency rates as
high as 86% at 2 yr of follow-up (33), the long-term
function of these accesses has not yet been evaluated.
Risk Factors for AVF DysfunctionDespite the excellent long-term function of fistulae
after successful maturation, little consensus has beenachieved regarding the predictors of the primary fail-
ure ofAVF. A number ofpotential risk factors, includ-
ing gender, vessel size, surgical technique, surgical
skill, and primary diagnosis have been postulated as
having an Important impact on the likelihood of suc-
cessful AVF maturation. Several studies in the early
1970s reported that women had a higher risk of
primary failure than men (24,26). Numerous otherreports (5,27-30) have looked for but failed to identify
specific risk factors of primary AVF failure. Many of
these studies were small in size and carried out lim-
ited analyses to control for potential confounding
factors.Reilly and coworkers presented one of the best
documented and one of the few prospective risk-factor
studies of dialysis fistula function published to date
(25). They studied 157 consecutive patients between
1 976 and 1 98 1 . Intraoperative data, including size
and type of anastomosis, size of vessels, suture mate-
rial, and adequacy of flow were recorded. Univariate
and multivariate analysis demonstrated that vein size
was an important predictor of long-term access com-
plications. The power of this study, however, was
limited because of its sample size, and no specific
analysis of the predictors of inadequate fistula matu-ration was performed.
Few recent data are available regarding the risk
factors for inadequate maturation ofAVF. Pourchez etaL reported that 4 1 of 47 French dialysis patients
older than 75 yr of age underwent successful con-struction of an AVF (36). Kobrin et al. evaluated 48
AVF constructed between 1989 and 199 1 at the Uni-versity of Pennsylvania (37). Overall, 44% ofAVF had
successfully matured at 3 months, whereas primaryfailure occurred in 56%. Although age, gender, loca-
tion of the AVF, and the presence of diabetes mellitus
did not affect AVF maturation, the small size of the
study limited statistical power to detect clinically rel-
evant differences in access function. Few investigators
have analyzed the impact of the use of recombinant
erythropoietin (EPO) on AVF function (38,39) but the
few data available seem to suggest that AVF thrombo-sis is not a very common complication. Neither Be-
sarab et aL (39) nor Tang et aL (40) found thrombosis
of AVF to be more common with EPO use.
Thus, extensive published experience with AVF’
demonstrate their long-term utility and low rate of
complications among patients in whom primary fis-
tula function is achieved. However, despite a large risk
of primary fistula failure, little is known about the
specific surgical, comorbidity, or demographic factorspredictive of primary fistula function. Although it is
probably true that an older and sicker ESRD popula-
tion may less commonly undergo successful AVF con-
struction, the subgroup of patients in whom fistulaeshould be created is poorly defined. Several recent
reports (23,33-37) suggest that despite the older age
and worse comorbidity of U.S. ESRD patients as com-
pared with two decades ago, a substantial number of
patients remain viable candidates for placement ofAVF. This is especially true if upper-arm fistulas such
as brachial artery-basilic vein fistulas are considered.
A review of alternatives to AVF readily demonstrates
that unnecessary substitution of synthetic grafts for
autologous AVF greatly enhances both the morbidity
of and costs for the U.S. ESRD population.
POLVTETRAFLUOROETHYLENE DIALYSIS ACCESS
Patency and Complications ofPolyfetrafluoroethylene Dialysis Access
PTFE was introduced as a material for vascular
bypass grafts in 1976 (10). Since that time, thismaterial has become the mainstay for dialysis vascu-
lax accesses when an autologous AVF is either be-
lieved to be technically impossible or has failed to
mature, or commonly when there is insufficient time
for an AVF to mature before the need for hemodialysis
because of the late presentation of a patient’s symp-
51).
Feldman et al
Journal of the American Society of Nephrology 527
tomatic advanced renal failure. PTFE dialysis grafts
are currently the most common type of dialysis ac-
cess, accounting for as many as 83% of access place-
ments among prevalent ESRD patients (38). A great
majority of hemodialysis patients undergo only PTFE
graft placement despite the high probability that a
significant proportion of them would have been able to
undergo successful AVF construction. However, few
data exist documenting the proportion of accesses
that are constructed of PTFE but that could have been
successfully created as a native AVF. Nonetheless, the
potential excess use of PTFE vascular accesses and
the protean complications possible after their place-
ment, including stenosis, occlusion, infection, aneu-
rysm and pseudoaneurysm formation, cardiovascular
instability, and nerve injury, are all potentially re-
sponsible for a large component of the high morbidity
in the U.S. ESRD population.
Numerous investigators have reported 1 -and 3-yr
patency rates for PTFE grafts. Between 63 and 90% of
grafts still function after 1 yr. whereas only 42 to 60%
remain patent after 3 yr (9, 13-15, 17,41-47). Most of
these reports defined patency as persistent graft func-
tion, regardless of treatment for access complications
such as thrombectomy or percutaneous angioplasty.
Complication-free graft survival has been reported by
a number of investigators (17,41,45). Sabanayagam
and colleagues (45) reported the complication-free
survival ofPTFE grafts to be 77. 1% at 1 yr; Palder and
colleagues reported complication-free PTFE graft sur-
vival to be 51% at 2 yr (41): and Winsett and Wolma
reported complication-free PTFE graft survival to be
39% at 3 yr (1 7). Outflow obstruction and thrombosis
accounted for the vast majority of the complications
observed. Unfortunately, none of these studies re-
ported the influence of patient comorbidity on access
dysfunction. By prospectively studying a subgroup of
52 healthier patients who lived longer than 3 yr on
dialysis, Schuman and colleagues grossly controlled
for comorbidity and observed one access complication
for every 5 1 5 patient-days of follow-up (14).
In recent years, increasing attention has been given
to the detection and repair of stenosis of PTFE grafts.
Color-flow Doppler ultrasonography and contrast fis-
tulography are widely utilized. Repair by transluminal
angioplasty or surgical vein-patch angioplasty may
promote delivery of adequate dialysis and prevent
graft thrombosis. Whether repair before thrombosis
extends the useful life of PTFE grafts has yet to be
proven. A large, but not precisely determined, cost is
incurred by these diagnostic tests and interventional
procedures, which are performed for the most part on
an outpatient basis. A detailed discussion of the diag-
nosis and therapy of stenosis of PTFE grafts is beyond
the scope of this paper, but the reader is referred
elsewhere for recent discussions of these issues (48-
Risk Factors for Complications from PTFEDialysis Access
Thromboses of VFFE access grafts have been
thought to result from a number of causes, including
venous outflow obstruction and inadequate arterial
inflow. Outflow obstruction has usually been attrib-
uted to neointimal hyperplasia (52-54) or central ye-nous stenosis/thrombosis from prior central venous
access (55). Inadequate arterial inflow has resulted
from a small or diseased arterial source as well as
from recurrent bouts ofintradialytic hypotension (56-
59). Postdialysis dehydration with increased blood
viscosity; low serum albumin; inadequate anticoagu-
lation; external compression either from perigraft he-
matomas, overly vigorous pressure at needle sites,
occlusive bandages, or inopportune arm positioning
during sleep; the presence of anticardiolipin antibod-
ies, diabetes mellitus, and high hematocrit with EPO
therapy have all been claimed, with varying justifica-
tion, to contribute to PTFE graft thromboses
(39,40,52,57,59-64).
Despite these numerous hypothetical risk factors,
few studies have examined specific risk factors in a
controlled fashion. Aman et aL reported on 9 1 PT’FE
grafts followed for 24 months and observed a signifi-
cantly increased graft patency rate with the use of
double-lumen dialysis needles (54). They were unable
to find a relationship between graft survival or com-
plication-free graft survival and sex, race, degree of
hypertension, heparin dosing, or intradialytic hypo-
tension, although the statistical power of their study
was limited. Munda and colleagues followed 67 PTFE
grafts for 2 yr and found that a forearm loop configu-ration had greater than twice the rate of secondary
patency of forearm straight grafts (57).Although controversial, several reports have sug-
gested an association between diabetes mellitus andPTFE graft thrombosis (19,65,66). Windus and col-
leagues observed a rate of PTFE graft thrombosis at 1
yr of 72% among patients with diabetes, compared
with a rate of 49% among patients without diabetes
(65). Data from Medicare and the U.S. Renal Data
System (19,66) have been consistent, demonstrating
higher rates of hospitalization for vascular access
problems among the subset of ESRD patients with
diabetes.
Several investigators have evaluated the impact of
therapy with recombinant EPO on synthetic vascular
access function and reported conificting results
(39,40,62). Besarab and colleagues compared the rateof thrombotic events in 164 patients receiving EPO for
at least 2 months with that among 142 patients
treated earlier, before the availability of EPO. Theywere unable to detect any differences in the rate of
thrombosis either for synthetic grafts or AVF (39).
Consistent with these findings have been a number ofother studies (67-70), each failing to note an increase
in access thrombosis with EPO.In contrast to these findings, Dy and colleagues
Hemodialysis Vascular Access Morbidity
528 Volume 7 ‘ Number 4 . 1996
performed a nonconcurrent cohort study of 46 dialy-
sis patients before and after treatment with EPO (62).They reported a greater incidence of graft thrombosis
in the EPO period. Similar findings were reported by
the Canadian Erythropoletin Study, a randomized
comparison between treatment with placebo (N = 40)
and treatment with EPO targeting either a hemoglobin
concentration of 9.5 to 1 1 .0 g/dL (N = 40) or 1 1 .5 to13.0 g/dL (N = 38). A 2.5% rate of access thrombosis
at 6 months was observed in the placebo group with a
mean hemoglobin of 7.4 g/dL. In contrast, the two
groups treated with EPO achieved mean hemoglobin
concentrations of 10.2 g/dL and 1 1.7 g/dL with
6-month thrombosis rates of 10% and 18%, respec-
tively (7 1). The low rate of thrombosis in the placebo
group was considerably lower than that published by
Eschbach and colleagues (67), making this study’s
findings difficult to interpret. Although several inves-
tigations reporting substantial thrombosis rates inpatients with PTFE grafts on EPO have recenfly been
reviewed (68), none of these studies have includedcontrol groups off EPO.
Thus, several investigators have independently con-
firmed the impression derived from the hospitalizationdata in Medicare’s ESRD database: the rate of compli-
cations, especially stenosis and thrombosis, arising
from synthetic dialysis vascular accesses is very large.
The mean duration of the complication-free accesssurvival appears to be between 9 and 16 months, with
a great majority of patients experiencing a complica-
tion by the end ofthe 3rd yr after graft placement. This
extraordinarily high complication rate, with its atten-dant suffering and high utilization of U.S. Dialysis
Program resources, makes the search for better strat-egies to improve outcomes among recipients of syn-
thetic vascular accesses urgent. Formulation of suchstrategies will require, in part, better delineation of the
risk factors for failure of PTFE access grafts.
INDWELLING CENTRAL VENOUS DIALYSISCATHETERS
Intended originally as a temporary measure, thesilicone double-lumen catheter with Dacron#{174}cuff hasinevitably come into long-term use in patients inwhom peripheral vascular access (fistula or graft) Is
unsuitable. The Dacron#{174} cuff decreases infection andmakes long-term use possible. When catheters are
intended for use for less than 1 month, a polyure-
thane, non-cuffed central venous access is normallyused. However, if catheter use is expected to exceed 1month, the cuffed SILASTIC (Dow Corning, Midland,
MI) catheter is preferred (73). The proportion of hemo-
dialysis patients in the United States in whom cuffed
SILASTIC� catheters provide long-term vascular ac-
cess is unknown. Based on data from the 1991 U.S.Renal Data System (USRDS) Special Study of CaseMix, It can be estimated that 4% ofU.S. ESRD patientsbegin dialysis with a permanent catheter. These data
underestimate the actual prevalence of catheter use,
as they do not account for usage after failure of more
traditional vascular accesses, AVF, or PTFE grafts. In
a survey of 1 7 dialysis units in the Chicago area, theproportion ofpatients using permanent double-lumencatheters ranged between 3.3 and 45%; of 1372 pa-
tients, 210 (15%) received or already had such cathe-
ters (74). Increasing long-term survival of the end-
stage renal population has enhanced the incidence of
depletion of potential sites for AV vascular access, and
the use of central venous catheters for permanentaccess is likely to be increasing.
A jugular vein has become the preferred site forpermanent central venous catheter insertion. Percu-
taneous jugular venous insertion is safer than in thesubclavian location. Subclavian catheters have
caused subclavian thrombosis and stenosis (75),
which can preclude creation of AV vascular access in
the ipsilateral ann, and there may be less mechanical
malfunction in catheters placed in the jugular rather
than subclavian location (76), partIcularly the right
jugular veins (77). Blood-flow rates of 200 to 300mL/min are routinely achieved (78-80); flows up to
400 mL/min can be achieved in some patients, but
sometimes not consistently. Recirculation in variousstudies has ranged from 5.5 to 8.6% (79-82). Unlike
AV fistulas and grafts, dialysis through central venous
catheters is not affected by cardiopulmonary recircu-lation.
Actuarial catheter survival at 12 months has ranged
from 30 to 65% (76,79,80,83). Catheter failure has
been the result primarily of malfunction (thrombosis
or poor blood flow) or to infection, in roughly equalproportions. Catheter malfunction can be reduced by
proper placement of the catheter tip in the right
atrium and by the use of chronic anticoagulation,beginning with aspirin and using warfarmn if necessary(74). Urokinase and streptokinase and mechanical
means have been used to open thrombosed catheters
and those with poor flow (74,78-80,84-86). Infection
with septicemia occurs with a frequency between 0.25and 1.0 infections per patient-year (76-79). Although
Gram-positive infections have been successfullytreated with antibiotics alone, many infections, espe-cially those resulting from Gram negative organisms,have required catheter removal.
Use of permanent central venous catheters hasimportant morbidity. Insertion can be complicated by
arterial puncture, pneumothorax, hemothorax, ar-rhythmia, and perforation or laceration of the brachial
plexus, trachea, superior vena cava, or myocardium.Jugular venous cannulation Is generally safer than
subclavian cannulation and the incidence of these
complications is low in experienced hands (73). Late
complications include catheter malfunction because
of thrombosis or malposition, infection, and subcla-
vian or superior vena cava thrombosis or stricture(73,87,88). The latter complications, which occur with
internal jugular as well as subclavian catheters, mayprevent subsequent use of the ipsilateral arm or of
both arms for AV access. Superior vena cava throm-
Feldman et al
Journal of the American Society of Nephrology 529
bosis may be more common than has been reported
(88), but the actual rates of occurrence of these mor-bidities are unknown.
Permanent dual-lumen central venous cathetershave some advantages over AV access, including easeof insertion, removal, and replacement, immediacy of
use, absence of hemodynamic stress or steal syn-
drome, absence of cardiopulmonary recirculation,
and avoidance of venipuncture. Indications for suchcatheters include loss of other vascular access sites,
prolonged period of maturation of other accesses
(usually AVF), cardiovascular instability or steal syn-
drome, and short expected duration of dialysis (e.g.,
malignancy, impending renal transplantation). If
rates of poor flow and thrombosis and infection are as
low as in some series, permanent catheters may even
be considered an acceptable alternative to PTFE grafts
in the general population of patients in whom creation
of an AVF is not feasible (80).
PATFERNS OF VASCULAR ACCESS UTILIZATION INTHE UNITED STATES
The only national data permitting study of specific
types of vascular access were collected as part of the
special studies of Case Mix conducted by the USRDS,
first for patients in 1986 and 1987, and subsequentlyfor patients in 1 99 1 . Although these data are older,
they provide us with an opportunity to examine the
evolution of the patterns of vascular access utilization
C4,C.,
4,a.
in the United States that have not been previously
published.
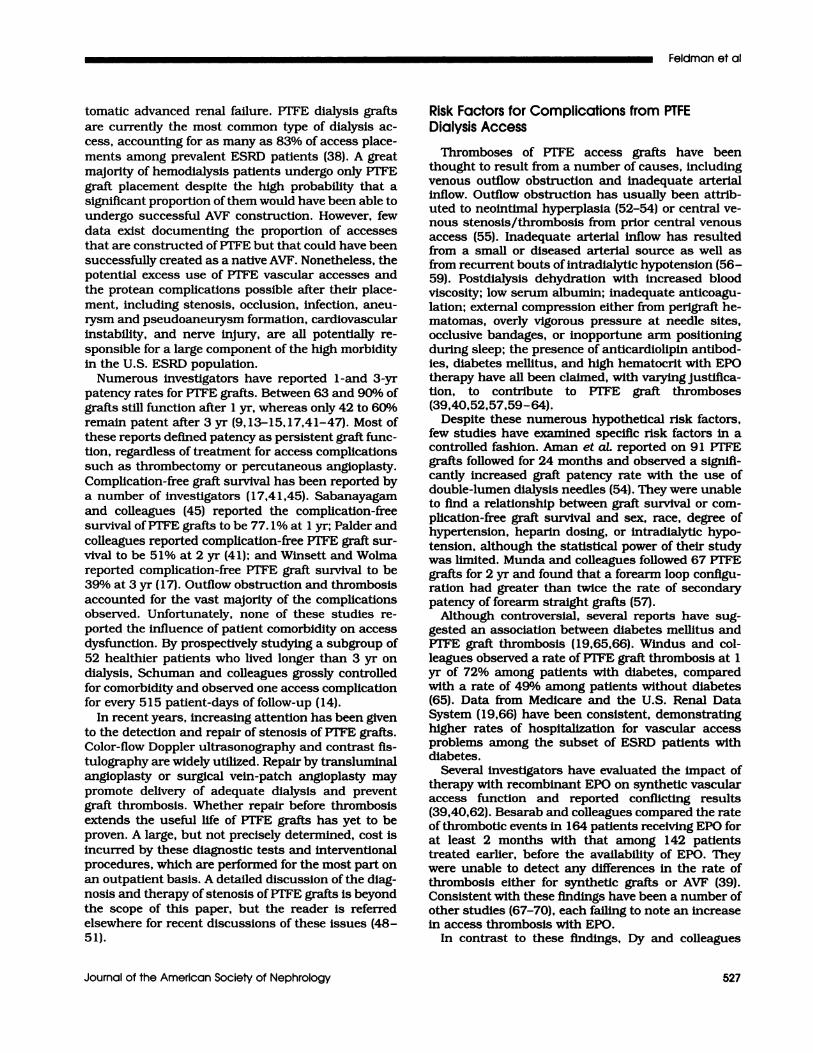
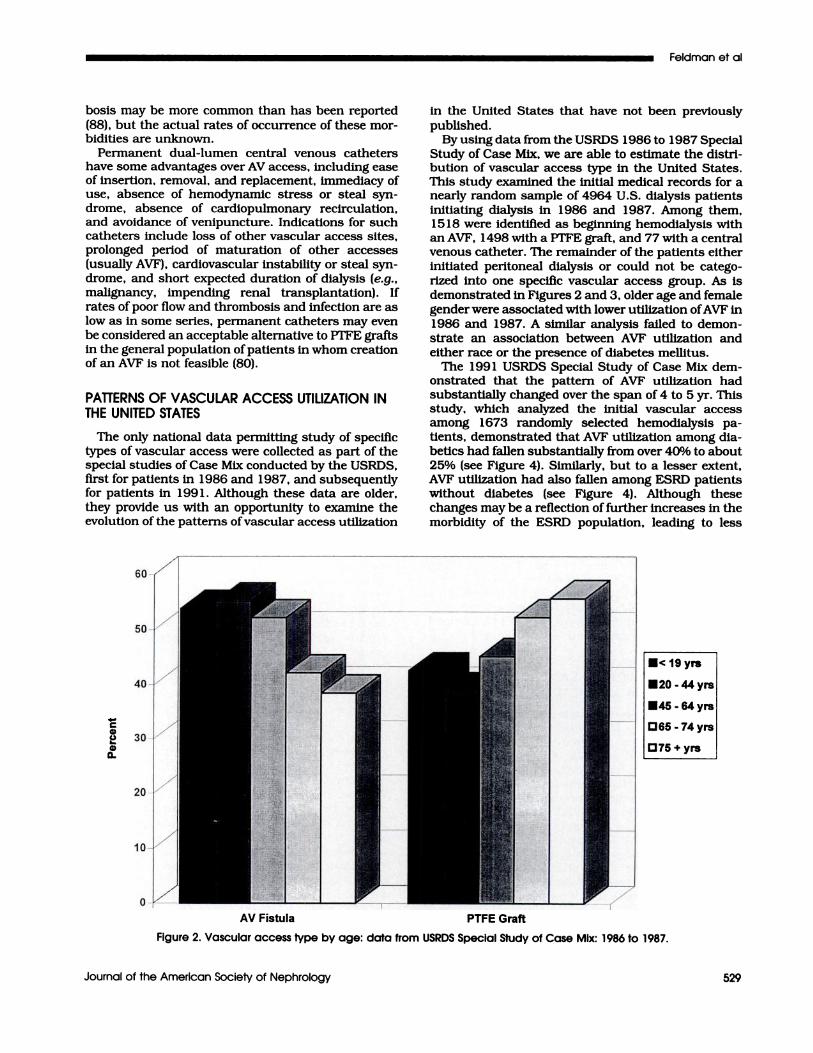
By using data from the USRDS 1 986 to 1 987 Special
Study of Case Mix, we are able to estimate the distri-bution of vascular access type in the United States.
This study examined the initial medical records for a
nearly random sample of 4964 U.S. dialysis patients
initiating dialysis in 1986 and 1987. Among them,
1 5 1 8 were identified as beginning hemodialysis with
an AVF, 1498 with a VTFE graft, and 77 with a central
venous catheter. The remainder of the patients either
initiated peritoneal dialysis or could not be catego-
rized into one specific vascular access group. As is
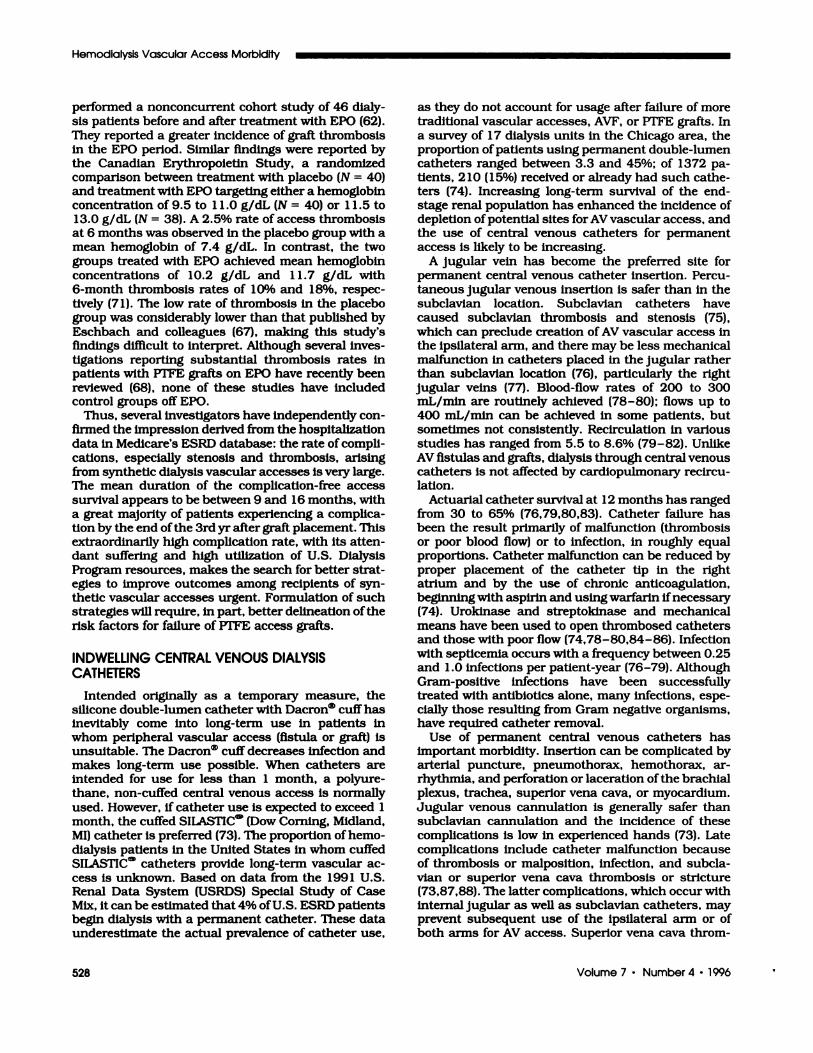
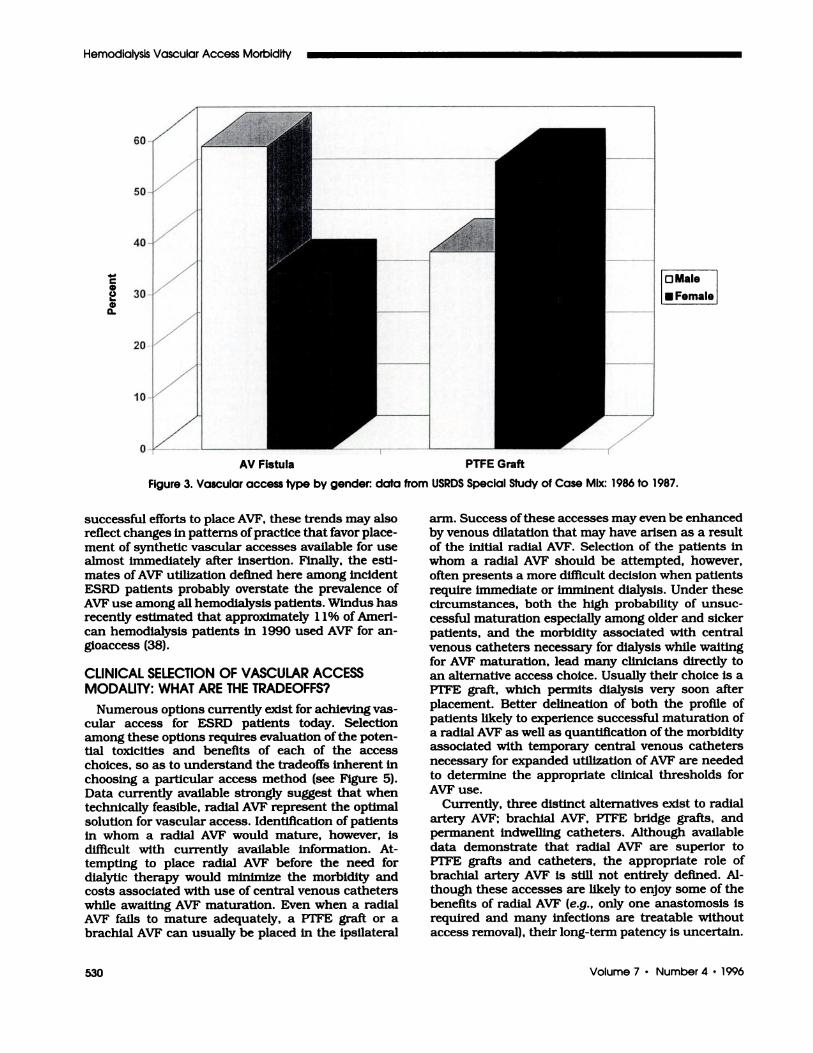
demonstrated in Figures 2 and 3, older age and female
gender were associated with lower utilization ofAVF in
1986 and 1987. A similar analysis failed to demon-
strate an association between AVF utilization and
either race or the presence of diabetes mellitus.
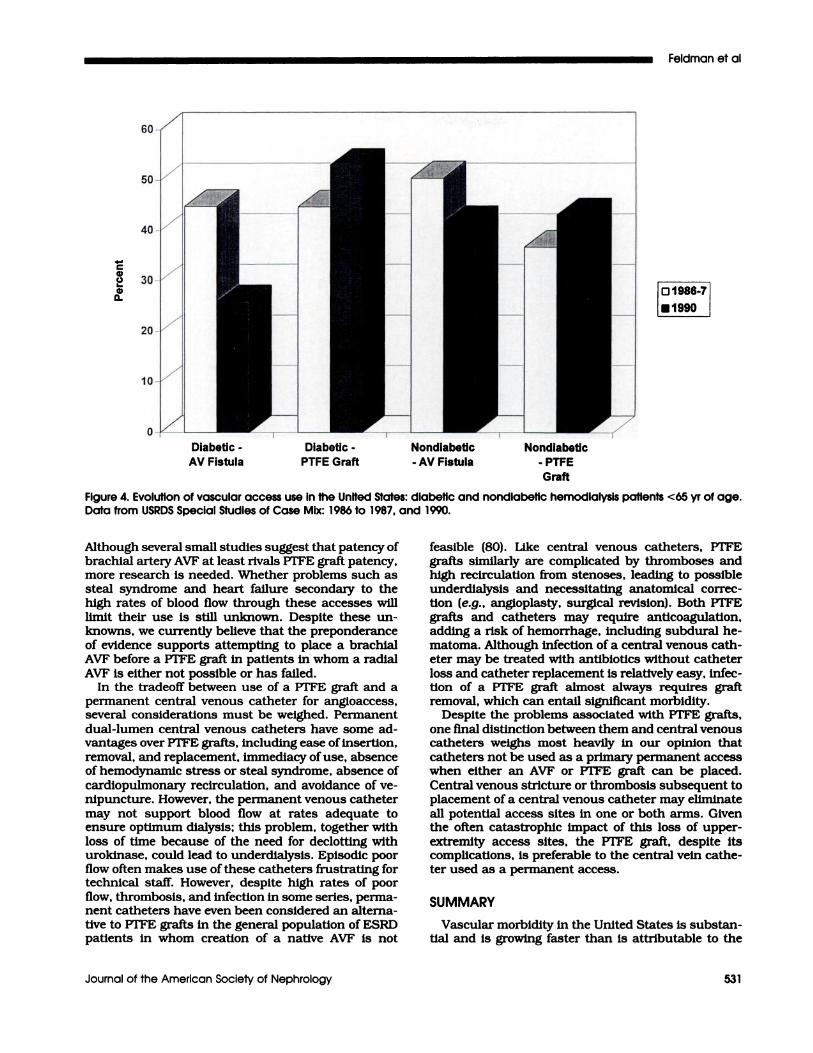
The 199 1 USRDS Special Study of Case Mix dem-onstrated that the pattern of AVF utilization had
substantially changed over the span of 4 to 5 yr. This
study, which analyzed the initial vascular access
among 1673 randomly selected hemodialysis pa-
tients, demonstrated that AVF utilization among dia-
betics had fallen substantially from over 40% to about
25% (see Figure 4). Similarly, but to a lesser extent,
AVF utilization had also fallen among ESRD patients
without diabetes (see Figure 4). Although these
changes may be a reflection of further increases in the
morbidity of the ESRD population, leading to less
.< 19 yrs
#{149}20-44yrs
�45-64yrs
D65-74yrs
D75 + yrs
AV Fistula PTFE Graft
Figure 2. Vascular access type by age: data from USRDS Special Study of Case Mix: 1986 to 1987.
Hemodialysis Vascular Access Morbidity
530 Volume 7 . Number 4 ‘ 1996
C4,
C.,I-
4,a.
AV Fistula PTFE Graft
OMale
#{149}Female
Figure 3. Vascular access type by gender: data from USRDS Special Study of Case Mix: 1986 to 1987.
successful efforts to place AVF, these trends may also
reflect changes in patterns ofpractice that favor place-
ment of synthetic vascular accesses available for usealmost Immediately after insertion. Finally, the esti-
mates of AVF utilization defined here among incident
ESRD patients probably overstate the prevalence of
AVF use among all hemodialysis patients. Windus hasrecently estimated that approximately 1 1% of Amen-
can hemodialysis patients in 1990 used AVF for an-
gioaccess (38).
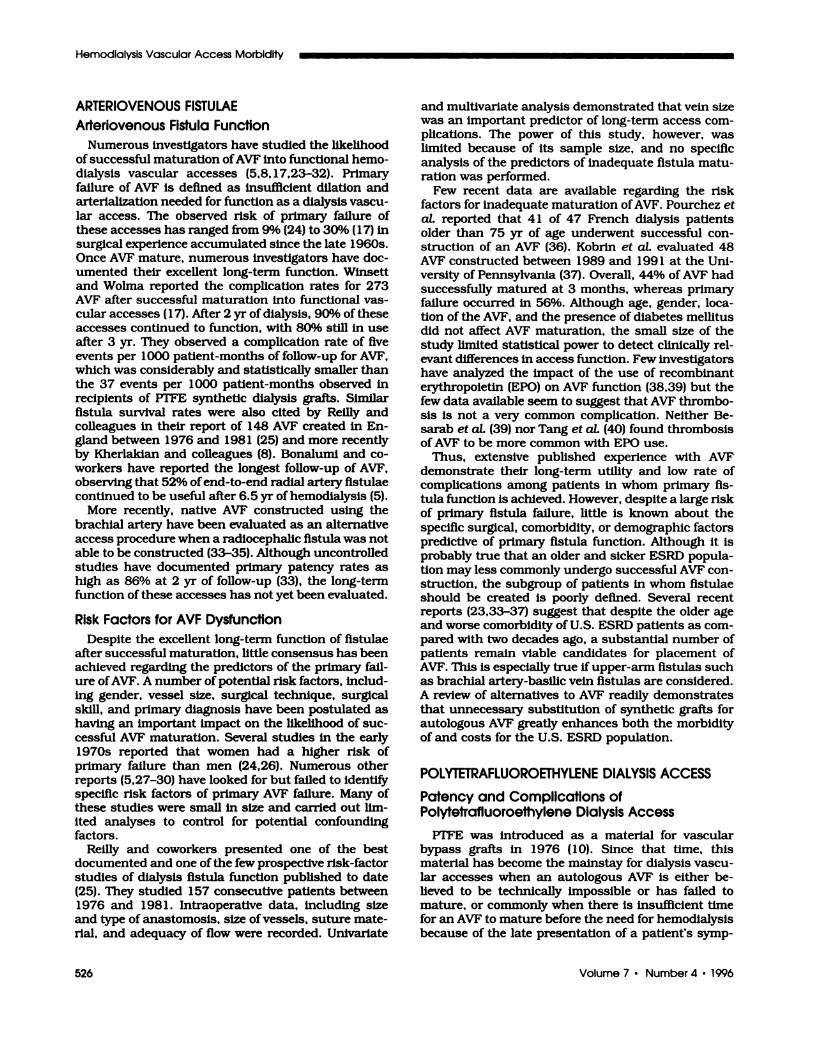
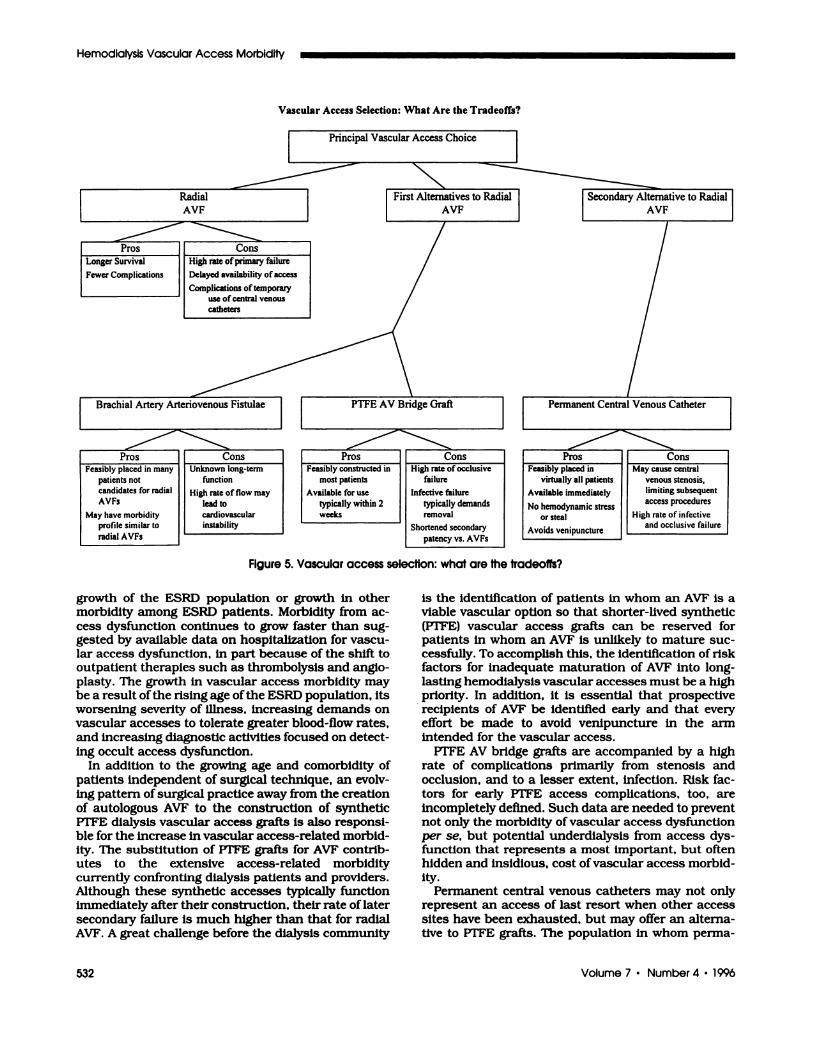
CLINICAL SELECTION OF VASCULAR ACCESSMODALITY: WHAT ARE THE TRADEOFFS?
Numerous options currently exist for achieving vas-
cular access for ESRD patients today. Selectionamong these options requires evaluation of the poten-
tial toxicitles and benefits of each of the access
choices, so as to understand the tradeoffs inherent in
choosing a particular access method (see Figure 5).
Data currently available strongly suggest that whentechnically feasible, radial AVF represent the optimalsolution for vascular access. Identification of patients
in whom a radial AVF would mature, however, isdifficult with currently available information. At-tempting to place radial AVF before the need fordialytic therapy would minimize the morbidity andcosts associated with use of central venous catheters
while awaiting AVF maturation. Even when a radialAVF falls to mature adequately, a VFFE graft or a
brachial AVF can usually be placed in the ipsilateral
ann. Success of these accesses may even be enhanced
by venous dilatation that may have arisen as a result
of the initial radial AVF. Selection of the patients in
whom a radial AVF should be attempted, however,
often presents a more difficult decision when patients
require immediate or imminent dialysis. Under thesecircumstances, both the high probabifity of unsuc-
cessful maturation especially among older and sicker
patients, and the morbidity associated with central
venous catheters necessary for dialysis while waiting
for AVF maturation, lead many clinicians directly toan alternative access choice. Usually their choice is aVrFE graft, which permits dialysis very soon after
placement. Better delineation of both the profile ofpatients likely to experience successful maturation of
a radial AVF as well as quantification of the morbidity
associated with temporary central venous catheters
necessary for expanded utilization of AVF are neededto determine the appropriate clinical thresholds for
AVF use.
Currently, three distinct alternatives exist to radialartery AVF; brachial AVF, VFFE bridge grafts, and
permanent indwelling catheters. Although availabledata demonstrate that radial AVF are superior toVT’FE grafts and catheters, the appropriate role of
brachial artery AVF Is still not entirely defined. Al-though these accesses are likely to enjoy some of the
benefits of radial AVF (e.g., only one anastomosis isrequired and many infections are treatable withoutaccess removal), their long-term patency is uncertain.
Graft
Figure 4. Evolution of vascular access use in the United States: diabetic and nondlabetic hemodlalysis patients <65 yr of age.Data from USRDS Special Studies of Case Mix: 1986 to 1987, and 1990.
Feldman et al
Journal of the American Society of Nephrology 531
C,U _________L. � � �
C, IO1986-7�a. � I
_0
Diabetic - Diabetic - Nondiabetic Nondiabetic
AV Fistula PTFE Graft - AV Fistula - PTFE
Although several small studies suggest that patency of
brachial artery AVF at least rivals VT’FE graft patency,more research is needed. Whether problems such as
steal syndrome and heart failure secondary to the
high rates of blood flow through these accesses will
limit their use is still unknown. Despite these un-
knowns, we currently believe that the preponderance
of evidence supports attempting to place a brachial
AVF before a PTFE graft in patients in whom a radial
AVF is either not possible or has failed.In the tradeoff between use of a PTFE graft and a
permanent central venous catheter for angloaccess,several considerations must be weighed. Permanent
dual-lumen central venous catheters have some ad-vantages over FTFE grafts, including ease of insertion,
removal, and replacement, immediacy ofuse, absenceof hemodynamic stress or steal syndrome, absence of
cardiopulmonary recirculation, and avoidance of ye-
nipuncture. However, the permanent venous catheter
may not support blood flow at rates adequate toensure optimum dialysis; this problem, together with
loss of time because of the need for declotting withurokinase, could lead to underdialysis. Episodic poorflow often makes use of these catheters frustrating for
technical staff. However, despite high rates of poor
flow, thrombosis, and infection in some series, perma-
nent catheters have even been considered an alterna-
tive to PTFE grafts in the general population of ESRDpatients in whom creation of a native AVF Is not
feasible (80). Like central venous catheters, PTFE
grafts similarly are complicated by thromboses and
high recirculation from stenoses, leading to possible
underdialysis and necessitating anatomical correc-
tion (e.g., angioplasty, surgical revision). Both PTFEgrafts and catheters may require anticoagulation,adding a risk of hemorrhage, including subdural he-
matoma. Although infection of a central venous cath-eter may be treated with antibiotics without catheter
loss and catheter replacement is relatively easy, infec-
tion of a PTFE graft almost always requires graftremoval, which can entail significant morbidity.
Despite the problems associated with PTFE grafts,
one final distinction between them and central venouscatheters weighs most heavily in our opinion that
catheters not be used as a primary permanent accesswhen either an AVF or VFFE graft can be placed.Central venous stricture or thrombosis subsequent toplacement of a central venous catheter may eliminate
all potential access sites in one or both arms. Giventhe often catastrophic impact of this loss of upper-
extremity access sites, the PTFE graft, despite itscomplications, is preferable to the central vein cathe-ten used as a permanent access.
SUMMARY
Vascular morbidity In the United States is substan-
tial and is growing faster than Is attributable to the
Principal Vascular Access Choice
Radial
AVF
I Pros �J Cons
NFirst Alternatives to Radial
AVF
Longer Survival � High rate ofprimary failure
Fewer Complications � Delayed availability of access
�J Complications of temporaryuse of central venous
catheters
Secondary Alternative to RadialAVF
Brachial Artery Arteriovenous Fistulae Permanent Central Venous Catheter
Pros Cons
Feasibly placed in
virtually all patients
Available immediately
No hemodynamic stressor steal
Avoids venipuncture
Hemodialysis Vascular Access Morbidity
532 Volume 7 ‘ Number 4 ‘ 1996
Vascular Access Selection: What Are the Tradeoffs?
Pros ConsFeasibly placed in many Unknown long-term
patients not function
candidates for radial High rate offlow may
AVFs lead to
May have nsorbidity cardiovascularprofile similar to instability
radial AVFs
PTFE AV Bridge Graft
Pros Cons
Feasibly constructed in High rate of occlusive
most patients failure
Available for use Infective failure
typically within 2 typically demandsweeks removal
Shortened secondary
patency vs. AVFs
May cause central
venous stenosis,limiting subsequent
access procedures
High rate of infectiveand occlusive failure
Figure 5. Vascular access selection: what are the tradeoffs?
growth of the ESRD population or growth in other
morbidity among ESRD patients. Morbidity from ac-
cess dysfunction continues to grow faster than sug-gested by available data on hospitalization for vascu-
lar access dysfunction, In part because of the shift tooutpatient therapies such as thrombolysis and anglo-
plasty. The growth in vascular access morbidity may
be a result ofthe rising age ofthe ESRD population, itsworsening severity of illness, increasing demands on
vascular accesses to tolerate greater blood-flow rates,
and increasing diagnostic activities focused on detect-
ing occult access dysfunction.
In addition to the growing age and comorbidity of
patients independent of surgical technique, an evolv-
ing pattern of surgical practice away from the creation
of autologous AVF to the construction of syntheticPTFE dialysis vascular access grafts is also responsi-
ble for the increase in vascular access-related morbid-ity. The substitution of PTFE grafts for AVF contrib-utes to the extensive access-related morbiditycurrently confronting dialysis patients and providers.
Although these synthetic accesses typically functionimmediately after their construction, their rate of later
secondary failure is much higher than that for radialAVF. A great challenge before the dialysis community
is the identification of patients in whom an AVF is a
viable vascular option so that shorter-lived synthetic(VrFE) vascular access grafts can be reserved forpatients in whom an AVF is unlikely to mature suc-
cessfully. To accomplish this, the identification of riskfactors for inadequate maturation of AVF into long-
lasting hemodialysis vascular accesses must be a high
priority. In addition, it is essential that prospective
recipients of AVF be identified early and that everyeffort be made to avoid venipuncture in the arm
intended for the vascular access.
PTFE AV bridge grafts are accompanied by a high
rate of complications primarily from stenosis and
occlusion, and to a lesser extent, infection. Risk fac-
tons for early PTFE access complications, too, are
incompletely defined. Such data are needed to preventnot only the morbidity of vascular access dysfunction
per se, but potential undendialysis from access dys-
function that represents a most important, but oftenhidden and insidious, cost ofvascular access morbid-
ity.
Permanent central venous catheters may not onlyrepresent an access of last resort when other accesssites have been exhausted, but may offer an altenna-tive to PTFE grafts. The population in whom perma-
Feldman et al
Journal of the American Society of Nephrology 533
nent central venous catheters may be a superior
alternative to PTFE grafts, even when sites for grafts
have not been exhausted, needs to be better defmed incontrolled studies.
Clinical strategies to optimize the diagnosis andtherapy ofvascular access dysfunction also need to be
identified. These strategies must define the appropri-
ate threshold of abnormal morphology and functionthat justifies radiologic and/or surgical intervention.Clearly, early intervention may preserve the second-
ary patency of synthetic vascular access grafts. How-
ever, aggressive diagnostic activities plausibly may
lead to a higher rate of radiologic and surgical inter-ventions for detectable but not yet clinically important
stenoses. These interventions (e.g. , angioplasty or
surgical repair) themselves may reduce the feasibifity
of later interventions and may damage the vascularaccess directly, thereby shortening its long-term func-
tion.Finally, identification of the fundamental mecha-
nisms of vascular access dysfunction should also bethe focus of investigation so that specific therapies
and preventive strategies can be developed and imple-
mented.
ACKNOWLEDGMENTSThe authors gratefully acknowledge the assistance of the U.S. RenalData System for providing data from their Special Studies ofCase Mix.
This work was supported, in part. by a Cooperative Agreement withthe Health Care Financing Administration (HCFA).
REFERENCES1 . Quinton W, Dullard D, Scribner BH: Cannulation of blood
vessels for prolonged hemodlalysis. Trans Am Soc ArtifIntern Organs 19606:104-113.
2. Rosenthal JJ: Vascular access for hemodialysis. MajorProbl Clin Surg 198 1;4:455-468.
3. Wilson SE, Stabile BE, Williams RA, Owens ML: Currentstatus of vascular access techniques. Surg Clin NorthAm 1982;62:531-551.
4. Brescia MJ, Cimino JE, Appel K, Hurwich BJ: Chronichemodialysis using venipuncture and a surgically cre-ated arteriovenous fistula. N Engi J Med 1966;275:1089-1092.
5. Bonalumi U, Civalleri D, Rovida S, Adami GF, GianettaE, Griffanti-Bartoli F: Nine years’ experience with end-to-end artenlovenous flstula at the anatomical snufiboxfor maintenance haemodlalysis. BrJ Surg 1982;69:486-488.
6. Brems J, Castaneda M, Garvin PJ: A five-year experiencewith the Bovine Heterograft for vascular access. ArchSurg 1986:121:941-944.
7. Giacchino JL, Geis WP, Buckingham JM, Vertune LL,Bansal VK: Vascular access: Long-term results, newtechniques. Arch Sung 1979; 114:403-409.
8. Kherlakian GM, Roedersheimer LR, Arbaugh JJ, New-mark LI, King LR: Comparison of autogenous fistulaversus expanded polytetrafluoroethylene graft fistula forangioaccess in hemodialysis. Am J Surg 1986; 152:238-243.
9. Munda R, First MR, Alexander JW, Linnemann CC,FidlerJP, Kittur D: Polytetrafluoroethylene graft survivalin hemodialysis. JAMA 1983;249:219-222.
10. Rapaport A, Noon GP, McCollum CH: Polytetrafluoro-ethylene (VI’FE) grafts for haemodlalysis in chronic renalfailure: Assessment of durability and function at threeyears. Aust NZJ Surg 198 1:51:562-567.
1 1 . Veith FJ, Wilson SE, Hobson RW, Rosenthal JJ, TellisVA, Dagher FJ: Vascular access complications and new
methods. Trans Am Soc Artif Intern Organs 1982;28:647-657.
12. Office of Statistics and Data Management. End-stagerenal disease patient profile tables, 1987. Baltimore:Office of Statistics and Data Management, Health CareFinancing Administration; 1987.
13. Bell DD, Rosental JJ: Arteniovenous graft life in chronichemodlalysis. Arch Surg 1988; 123:1169-1172.
14. Schuman ES, Gross GF, Hayes JF, Standage BA: Long-term patency of polytetrafluoroethylene graft flstulas.AmJ Surg 1988:155:644-646.
15. Haimov M, Burrows L, Sclianzer H, et at.: Experiencewith arterial substitutes in the construction of vascularaccess for hemodialysis. J Cardiovasc Surg 1980:21:149-154.
16. Mohaideen AR, Mendivil J, Avram MM, Malnzer RA:Artenlo-venous access utilizing modified bovine arterialgrafts for hemodlalysis. Sung Clin North Am 1977:62:531-550.
17. Winsett OE, Wolma FJ: Complications of vascular ac-cess for hemodialysis. South Med J 1985:78:513-517.
18. Kester RC: Arteniovenous grafts for vascular access inhemodialysis. Br J Surg 1979;66:23-28.
19. Feldman HI, Held PJ, Hutchinson T, Stoiber E, HartiganMF, Berlin JA: Hemodialysis vascular access morbidityin the U.S. Kidney Int 1993:43:1091-1096.
20. Lazarus JM, Huang WI!, Lew NL, Lowrie EG. Contnibu-lion of vascular access-related disease to morbidity ofhemodlalysis. Vascular Access for Hemodialysis III. Chi-cago: WL Gore & Assoc. , Inc. , and Precept Press, Inc.:1993:3- 13.
2 1 . Held PJ, Pauly MV, Bovbjerg R, Diamond L: Large andsmall transplant programs: Implications for cost andoutcomes. IPublication No. 3293-22] WashIngton, DC:The Urban Institute; 1986.
22. US Renal Data System. USRDS 1994 Annual Data Re-port. Bethesda, MD: The National Institutes of Health,National Institute of Diabetes and Digestive and KidneyDiseases: 1994:23-42.
23. Churchill DN, Taylor DW, Cook RJ, LaPlante P, et at.:Canadian hemodialysis morbidity study. Am J KidneyDis 1992:19:214-234.
24. Kinnaert P. Vereerstraeten P, Toussaint C, Van Geer-truyden J: Nine years’ experience with internal artenio-venous fistulas for haemodialysls: A study of some fac-tors influencing the results. BrJ Surg 1977:64:242-246.
25. Reilly DT, Wood RFM, Bell PRF: Prospective study ofdialysis fistulas: Problem patients and their treatment.BrJ Surg 1982:69:549-553.
26. HIggins MR. Grace M, Bettcher KB, Silverberg DS,DossetorJB: Blood access In hemodialysis. Clint Nephrol1976:6:473-477.
27. Aim A, Lundberg M: Clinical experience with therapeuticarteriovenous flstulae. Scand J Urol Nephrol 1977; 1 1:53-57.
28. Rohr MS. Browder W, Frentz GD, McDonald JC: Arterio-venous flstulas for long-term dialysis. Arch Surg 1978;113:153-155.
29. Dunlop MG, Mackinlay JY, Jenkins AM: Vascular ac-cess: Experience with the brachiocephalic fistula. Ann RColl Sung Engl 1986:68:203-206.
30. ZIbari GB, Rohr MS. Landreneau MD, Bridges RM, etaL: Complications from permanent hemodialysis vascu-lar access. Surgery (St. Louis) 1988; 104:681-686.
3 1 . Bourquelot P, Cussenot 0, Corbi P, et at.: Microsurgicalcreation and follow-up of arteriovenous flstulae forchronic haemodialysis in children. Pediatr Nephrol1990:4:156-159.
32. Wehrli H, Chenevard R, Zaruba K: Chlrurgische Erfahr-ungen mit arterio-venosen Hamodialyse-Shunts (1970-1988). Helv Chir Acta 1989:56:621-627.
33. Coburn MC, Carney WI Jr: Comparison of basilic veinand polytetrafluorethylene for brachial arteriovenousfistula. J Vasc Surg 1994:20:896-902..
34. RIvers SP, Scher LA, Sheehan E, Lynn R, Veith FJ:Basific vein transposition: An underused autologousalternative to prosthetic dialysis angioaccess. J VaseSurg 18:391-396.
Hemodialysis Vascular Access Morbidity
534 Volume 7 . Number 4 . 1996
35. Bender MH, Bruyninckx CM, Genlag PG: The brachioce-phalic elbow fistula: A useful alternative angioaccess forpermanent hemodialysis. J Vase Surg 1994:20:808-813.
36. Pourchez T, Moriniere F, St Priest A, et at: Outcome ofvascular access for hemodialyses in the elderly (>75years) lAbstracti. Proc Eur Dial Transplant Assoc 1990:27: 160A.
37. Kobrln 5, Feldman H, Morley C, Deno M: Outcome ofarteniovenous fistula (AVF) placements (Abstract).ASAIO 38th Annual Meeting: 1992:84A.
38. Windus DW: Permanent vascular access: A nephrolo-gist’s view. Am J Kidney Dis 1993:21:457-471.
39. Besarab A, Medina F, Musial E, et aL: Recombinanthuman erythropoietin does not increase clotting in vas-cular accesses. ASAIO (Am Soc Artif Intern Organs)Trans 1990;36:M749-M753.
40. Tang TY, Vrahnos D, Valaitis D, Lau AR: Vascular accessthrombosis during recombinant human erythropoietintherapy. ASAIO J 1992:38:M528-M531.
4 1 . Palder SB, Kirkman RL, Whittenmore AD, Hakim RM,Lazarus JM, Tilney NL: Vascular access for hemodialy-sis. Ann Surg 1985:202:235-239.
42. Tauches LA: Immediate, safe hemodialysis with arterio-venous fistulas created with a new tunneler. Ann Sung1985:150:212-215.
43. Raju 5: PTFE grafts for hemodlalysis access. Ann Surg1987:206:73, 206-266.
44. Mandel SR. Martin PL, Blumoff RL, Mattern WD: Vas-cular access In a university transplant and dialysisprogram. Arch Surg 1977:112:1375-1380.
45. Sabanayagam P. Schwartz AR, Soricelli RR, Chinitz JL,Lyons P: Experience with one hundred reinforced ex-panded PTFE grafts for angioaccess in hemodialysis.Trans Am Soc Artif Intern Organs 1980:26:582-583.
46. Kraev Z, Kirjakov Z, Antonov S. Stantchev I, ZlatarskaS, Sofia: Polytherafluoroethylene graft’s complications inpatients on hemodialysis. Przegl Lek 1985:42:442-443.
47. Tellis VA, Kohlberg WI, Bhat DJ, Dniscoll B, Veith FJ:Expanded polytetrafluoroethylene graft fistula forchronic hemodialysis. Ann Surg 1979: 189: 10 1-105.
48. Beathard GE: Percutaneous transvenous angioplasty inthe treatment of vascular access stenosis. Kidney mt1992:42:1390-1397.
49. Schwab SJ, Raymond JR, Saeed M, Newman GE, Den-nis PA, Bollinger RR: Prevention of hemodialysis fistulathrombosis. Early detection of venous stenoses. Kidneymt 1989:36:707-711.
50. Windus DW, Audrain J, Vanderson R, Jendnisak MD,Picus D, Delmez JA: Optimization of high-efficiencyhemodialysis by detection and correction of fistula dys-function. Kidney Int 1990:38:337-441.
5 1 . Sands J, Young 5, Miranda C: The effect of Doppler flowscreening studies and elective revisions on dialysis ac-cess failure. ASAIO (Am Soc Artif Intern Organs) Trans1992:38:M524-M527.
52. Bell DD, Rosental JJ: Arteriovenous graft life in chronichemodlalysis. Arch Surg 1988:123:1169-1172.
53. Haimov M, Burrows L, Schanzer H, Neff M, Baez A,Kwun K, Slkfkin R: Experience with arterial substitutesin the construction of vascular access for hemodialysis.J Cardiovasc Surg 1980:21:149-154.
54. Aman LC, Levin NW, Smith DW: Hemodialysis accesssite morbidity. Proc Clin Dial Transplant Forum 1980:10:277-284.
55. Schwab SJ, Quarles D, Middelton JP, Cohan RH, SaeedM, Dennis VW: Hemodialysis-associated subclavian veinstenosis. Kidney Int 1988:33:1156-1159.
56. Kherlakian GM, Roedersheimer LR, Arbaugh JJ, New-mark KJ, King LR: Comparison of autogenous fistulaversus expanded polytetrafluoroethylene graft fistula forangloaccess in hemodialysis. Am J Sung 1986:152:238-243.
57. Munda R, First MR Alexander JW, Linnemann CC,Fidler JP, Kittur D: Polytetrafluoroethylene graft sur-vival in hemodialysis. JAMA 1983:249:219-222.
58. Winsett OE, Wolma FJ: Complications of vascular ac-cess for hemodialysis. South Med J 1985:78:513-517.
59. Kraev Z, Kirjakov Z, Antonov 5, Stantchev I, Zlatarska5, Sofia: Polytherafluoroethylene graft’s complications inpatients on hemodialysis. Przegl Lek 1985:42:442-443.
60. Rosenthal JJ: Vascular access for hemodialysis. MajorProbl Clin Surg 198 1:4:455-468.
6 1 . Tellis VA, Kohlberg WI, Bhat DJ, Driscoll B, Veith FJ:Expanded polytetrafluoroethylene graft fistula forchronic hemodialysis. Ann Sung 1979: 189: 10 1-105.
62. Dy GR, Bloom EJ, Ijelu GK, Merritts GW, Kramer MS,Raja RM: Effect of recombinant human erythropoietin onvascular access. ASAJO (Am Soc Artif Intern Organs)Transactions 199 1 ;37:M274-M275.
63. Garcia-Martin F, DeArriba G, Carrascosa T, et at.: Anti-cardiolipin antibodies and lupus anticoagulant in end-stage renal disease. Nephrol Dial Transplant 1991:6:543-547.
64. Page B, ZingraffJ, Houhou 5, et at.: Clotting of vascularaccess in dialysis patients associated to anticardiolipinantibodies lAbstracti. J Am Soc Nephrol 1992;3:385A.
65. Windus DW, Jendrisak MD, Dalmez JA: Prosthetic fis-tula survival and complications in hemodialysis pa-tients: Effects of diabetes and age. Am J Kidney Dis1992:20:448-452.
66. US Renal Data System. USRDS 1991 Annual Data Re-port. Bethesda, MD: The National Institutes of Health,National Institute of Diabetes and Digestive and KidneyDiseases; 1991.
67. Eschbach JW, Abdulhadi MH, Browne JK, et at.: Re-combinant human erythropoietin in anemic patientswith end-stage renal disease. Ann Intern Med 1989: 1 1:992-1000.
68. Sundal E, Businger J, Kappeler A: Treatment of trans-fusion dependent anemia of chronic renal failure withrecombinant human erythropoietin. Nephrol Dial Trans-plant 1991:6:955-965.
69. Bennett WM: A multicenter clinical trial of epoetin betafor anemia of end-stage renal disease. J Am Soc Nephrol1991; 1:990-998.
70. Kawalski EA, Trenkle JA, Natke E, et aL: The effect oferythropoietin on the incidence of chronic vascularthrombosis (Abstracti. J Am Soc Nephrol 1991:2:380.
7 1 . Canadian Erythropoietin Study Group. Association be-tween recombinant human erythrepoietin and qualityof life and exercise capacity of patients receiving hemo-dialysis. BMJ 1990;300:573-579.
72. Muirhead N: Erythropoietin as a cause of access throm-bosis. Semin Dial 1993:6:184-188.
73. Bander SJ, Schwab SJ: Central venous angioaccess forhemodialysis and its complications. Semin Dial 1992:5:12 1-128.
74. Uldail R, Besley ME, Thomas A, Salter S, Nuezca LA,Vas M: Maintaining the patency of double-lumen silasticjugular catheters for haemodialysis. mt j Artif Organs1993; 16:37-40.
75. Fant GF, Dennis V, Quarles LD: Late vascular complica-tions of the subclavlan dialysis catheter. Am J KidneyDis 1986:7:225-228.
76. Swartz RD, Messana JM, Boyer CJ, Lunde NM, WeitzelWF, Hartman TL: Successful use of cuffed central ye-nous hemodialysis catheters inserted percutaneously. JAm Soc Nephrol 1994:4: 17 19-1725.
77. Dc Meester J, Vanholder R, De Reese J, Ringoir 5:Factors and complications affecting catheter and tech-nique survival with permanent single-lumen dialysiscatheters. Nephrol Dial Transplant 1994:9:678-683.
78. Uldall R, DeBruyne M, Besley M, McMillan J, Simons M,Francoeur R: A new vascular access catheter for hemo-dialysis. Mn J Kidney Dis 1993:21:270-277.
79. Shusterman NH, Kloss K, Mullen JL: Successful use ofdouble-lumen, silicone rubber catheters for permanenthemodialysis access. Kidney mt 1989:35:887-890.
80. Moss AH, Vasilakis C, Holley JL, Foulks CJ, Pillal K,McDowell DE: Use ofa silicone dual-lumen catheter witha Dacron cuff as a long-term vascular access for hemo-dialysis patients. Am J Kidney Dis 1990: 16:21 1-2 15.
8 1 . Blake PG, Huraib 5, Wu G, Uldall PR: The use of duallumen jugular venous catheters as definitive long term
Feldman et al
Journal of the American Society of Nephrology 535
access for haemodialysis. IntJ ArtifOrgans 1990:13:26-31.
82. Schanzer H, Kaplan 5, Bosch J, Glabman 5, Burrows L:Double-lumen, silicone rubber, indwelling venous cath-eters. A new modality for angioaccess. Arch Surg 1986:121:229-232.
83. Shaffer D, Madras PN, Williams ME, D’Elia JA, KaldanyA, Monaco AP: Use ofDacron cuffed silicone catheters aslong-term hemodialysis access. ASAIO J 1992:38:55-58.
84. Dunea G, Domenico L, Gunnerson P, Winston-Willis F:A survey of permanent double lumen catheters in hemo-dialysis patients. ASAIO (Am Soc Artif Intern Organs)Trans 1991:37:M276-M277.
85. Schwab SJ, Buller GL, McCann RL, Bollinger RR,Stickel DL: Prospective evaluation of a Dacron cuffed
hemodialysis catheter for prolonged use. Am J KidneyDis 1988:11:166-169.
86. Shrivastava D, Lundin AP, Dosunmu B, Rae TKS, BeyerMM, Friedman EA: Salvage of clottedjugular vein hemo-dialysis catheters. Nephron 1994:68:77-79.
87. Caruana RI, Raja RM, Zeit RM, Goldstein SJ, KramerMS: Thrombotic complications of indwelling centralcatheters used for chronic hemodialysis. Am J KidneyDis 1987:9:497-501.
88. Grote J, Luift V. Nikkuta PVD, Lieth H, Bahlmann J,Daniel WG: Transesophageal echocardiographic assess-ment of superior vena cava thrombosis in patients withlong-term central venous hemodialysis catheters. ClinNephrol 1994:42:183-188.