hernia | case study
TRANSCRIPT

HERNIAMOHAMMAD MATOUQ ALGHAMDI –PHARM.D INTERNSHIPSURGICAL ROTATION
HERNIA A hernia is a protrusion, bulge, or projection of an organ or part of an organ through the body wall that normally contains it, such as the abdominal wall. They are typically classified by etiology and location .[1]

SPECIFIC HERNIA SITES

Signs and symptomsPatients with significant symptoms attributable to an inguinal hernia should undergo elective surgical repair. Such symptoms typically include:I. Groin pain with exertion (eg, lifting) .II. Inability to perform daily activities due to pain or discomfort
from the hernia .III. Inability to manually reduce the hernia (ie, chronic
incarceration) . [2]

EtiologyHernias are classified by etiology depending upon whether the hernia is due to a congenital defect or is acquired. Congenital hernia – The defect in the abdominal wall is present from birth.Acquired hernia - The defect develops as the result of a weakening or disruption of the fibromuscular tissues of the abdominal wall due to connective tissue abnormalities, abdominal wall trauma.[3]
Overview of treatment for inguinal and femoral hernia in adultsThe definitive treatment of all hernias, regardless of origin or type, is surgical repair .Groin hernia repair is one of the most commonly performed operations. Over 20 million inguinal or femoral hernias are repaired every year worldwide including over 700,000 in the United States [4]

For patients with moderate to severe symptoms from an inguinal hernia, surgical repair is indicated. The only nonsurgical therapy for groin hernia in men is a truss. A truss is a strap similar to an athletic supporter with a metal or hard plastic plug positioned to lie over the hernia defect. [4]
Overview of treatment for inguinal and femoral hernia in adults

Truss

Preoperative prophylaxis Primary Regimens
Cefazolin 2 gm IV as a single dose If patient known to be colonized with MRSA, add Vancomycin to cefazolin. Postoperatively: Cefazolin 0.5-1 g IV q6-8hr for 24 hours [5]
Preoperative prophylaxis Alternative Regimens
Ampicillin-sulbactam 3 gm IV as a single dose, OR Clindamycin 900 mg IV as a single dose, OR Vancomycin 1 gm IV as a single dose; use 1.5 gm IV as a single dose if weight >90 kg [5]

Clinical Case

Demographic and Administrative InformationAge 35 Years
Gender Male
Nationality Saudi
Date of Administration 03 – 12- 2016
Date of Discharge 05 – 12- 2016
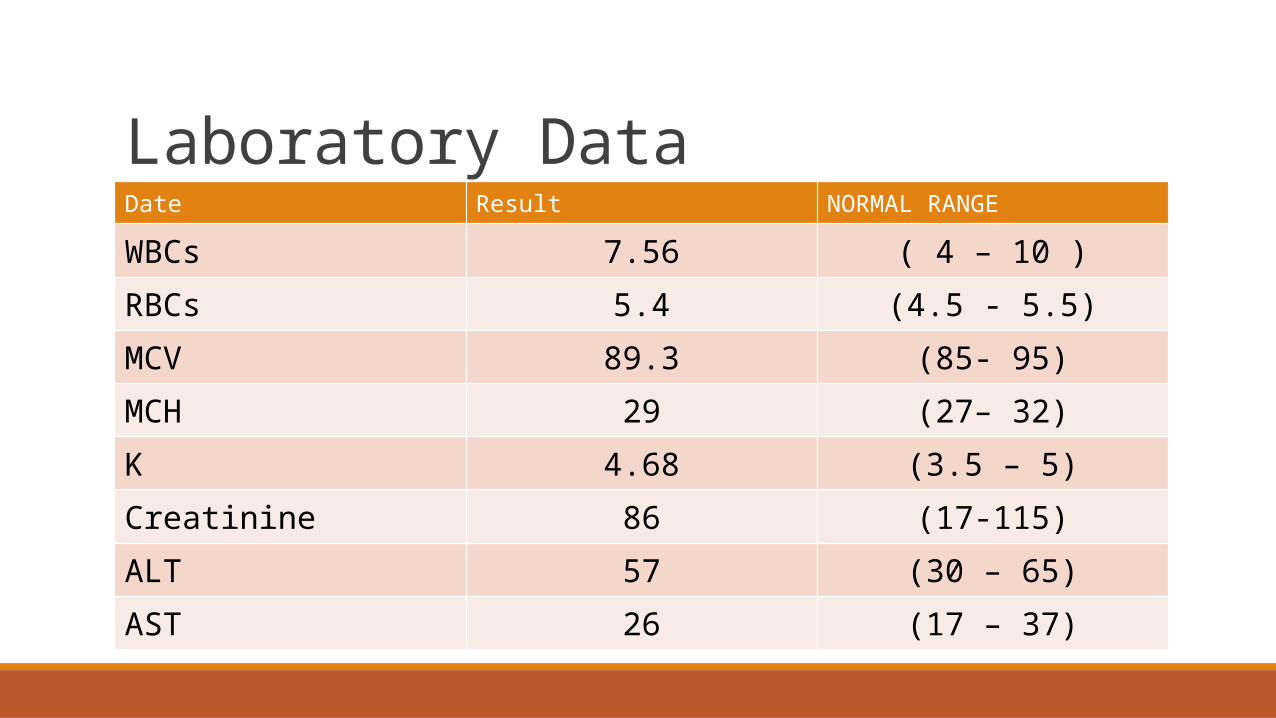
Laboratory DataDate Result NORMAL RANGE
WBCs 7.56 ( 4 – 10 )RBCs 5.4 (4.5 - 5.5)MCV 89.3 (85- 95)MCH 29 (27– 32)K 4.68 (3.5 – 5)Creatinine 86 (17-115)ALT 57 (30 – 65)AST 26 (17 – 37)
Chief Complaint Abdomen pain when coughing, exercising, or bending over

Acute Medical Therapy :ParacetamolOmeprazole

Vital Signs Date 03-12 04-12 05-12
Temp 37.2 37.1 36.8
B.P 119/79 126/82 128/88
Pulse 82 84 85
R.R 20 20 20
Normal Vital Signs
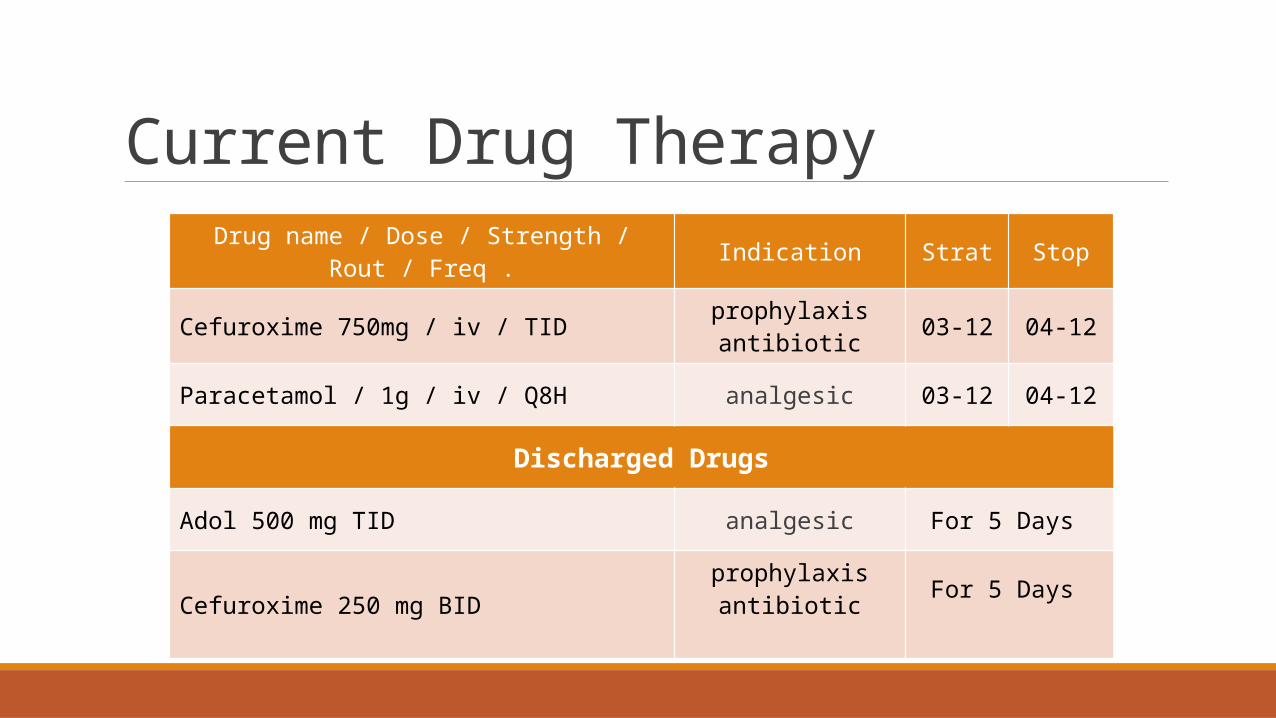
Current Drug Therapy Drug name / Dose / Strength / Rout / Freq . Indication Strat Stop
Cefuroxime 750mg / iv / TID prophylaxis antibiotic 03-12 04-12
Paracetamol / 1g / iv / Q8H analgesic 03-12 04-12
Discharged Drugs
Adol 500 mg TID analgesic For 5 Days
Cefuroxime 250 mg BID prophylaxis antibiotic For 5 Days

Drug Interaction
No interactions of Risk Level A or greater identified.

Pharmacist’s care plan The recommended antibiotic prophylaxis Preoperatively: Cefazolin 2 gm IV as a single dose (may be repeated in 4 hours intra operatively) Postoperatively: 0.5-1 g IV q6-8hr for 24 hours [5]

Antimicrobial Prophylaxis The goal of antimicrobial prophylaxis is to prevent SSI by reducing the burden of microorganisms at the surgical site during the operative procedure. Preoperative antibiotics are warranted if there is high risk of infection or if there is high risk of deleterious outcomes should infection develop at the surgical site. [6]

Guideline recommendations For most surgical procedures, joint clinical practice guidelines from
the American Society of Health-System Pharmacists, Infectious Diseases Society of America, Surgical Infection Society, and Society for Healthcare Epidemiology of America (ASHP/IDSA/SIS/SHEA) recommend a dose of 2 g within 60 minutes prior to surgical incision (for nonobese patients weighing <120 kg).
Cefazolin doses may be repeated intraoperatively in 4 hours if procedure is lengthy or if there is excessive blood loss [7]
(2013 )
Guideline recommendations In general, repeat antimicrobial dosing following wound closure is not necessary and may increase antimicrobial resistance. For cases in which prophylaxis beyond the period of surgery is warranted, in general, the duration should be less than 24 hours. [8]

[1] Steinke W, Zellweger R. Richter's hernia and Sir Frederick Treves: an original clinical experience, review, and historical overview. Ann Surg 2000; 232:710.
[2] Rosenberg J, Bisgaard T, Kehlet H, et al. Danish Hernia Database recommendations for the management of inguinal and femoral hernia in adults. Dan Med Bull 2011; 58:C4243.
[3] http://emedicine.medscape.com/article/189563-treatment#showall
[4] McIntosh A, Hutchinson A, Roberts A, Withers H. Evidence-based management of groin hernia in primary care--a systematic review. Fam Pract 2000; 17:442.
Cheek CM, Williams MH, Farndon JR. Trusses in the management of hernia today. Br J Surg 1995; 82:1611.
[5] Antimicrobial prophylaxis for surgery. Treat Guidel Med Lett 2012; 10:73.
[6] Bratzler DW, Hunt DR. The surgical infection prevention and surgical care improvement projects: national initiatives to improve outcomes for patients having surgery. Clin Infect Dis 2006; 43:322.
[7] (Bratzler 2013).
[8]- Antimicrobial prophylaxis for surgery. Treat Guidel Med Lett 2012; 10:73. ◦ -Goldmann DA, Hopkins CC, Karchmer AW, et al. Cephalothin prophylaxis in cardiac valve surgery. A prospective, double-blind
comparison of two-day and six-day regimens. J Thorac Cardiovasc Surg 1977; 73:470.◦ -Harbarth S, Samore MH, Lichtenberg D, Carmeli Y. Prolonged antibiotic prophylaxis after cardiovascular surgery and its effect on
surgical site infections and antimicrobial resistance. Circulation 2000; 101:2916.

Thank You