hiatal herniashiatal hernias · hiatal herniashiatal hernias ... h l h t i ll i bdominal pressure...
TRANSCRIPT

Hiatal HerniasHiatal Hernias
Kiyanda Baldwin, MD
SUNY Downstate Medical CenterSUNY Downstate Medical Center
August 27, 2009
www.downstatesurgery.org

Case PresentationCase Presentation29 y/o male truck driver with intractable 29 y/o male truck driver with intractable hiccups since 8/2008
PMH: GERD
PSH: lap chole 2003
Meds: thorazine
All: NKDA
www.downstatesurgery.org
Case PresentationCase PresentationPhysical Exam:
Afebrile, hemodynamically normal, Ht: 5’, Wt: 86kg
Within normal limits includingWithin normal limits includingBreath sounds clear to auscultationCVS S1S2, no R/M/GAbd soft, no organomegaly, scars from lap chole
Labs: unremarkableLabs: unremarkable
www.downstatesurgery.org
Case PresentationCase PresentationCXR 8/08:CXR 8/08:
WNL
EGD 2/09: 1cm hiatal hernia1cm hiatal hernia
Esophageal Manometry 3/09: Esophageal Manometry 3/09: hypotensive LES with good relaxationlow amplitude peristaltic contractionsp p
www.downstatesurgery.org
Case PresentationCase PresentationCT abd/pelvis 5/09CT abd/pelvis 5/09
www.downstatesurgery.org
Case PresentationCase Presentation
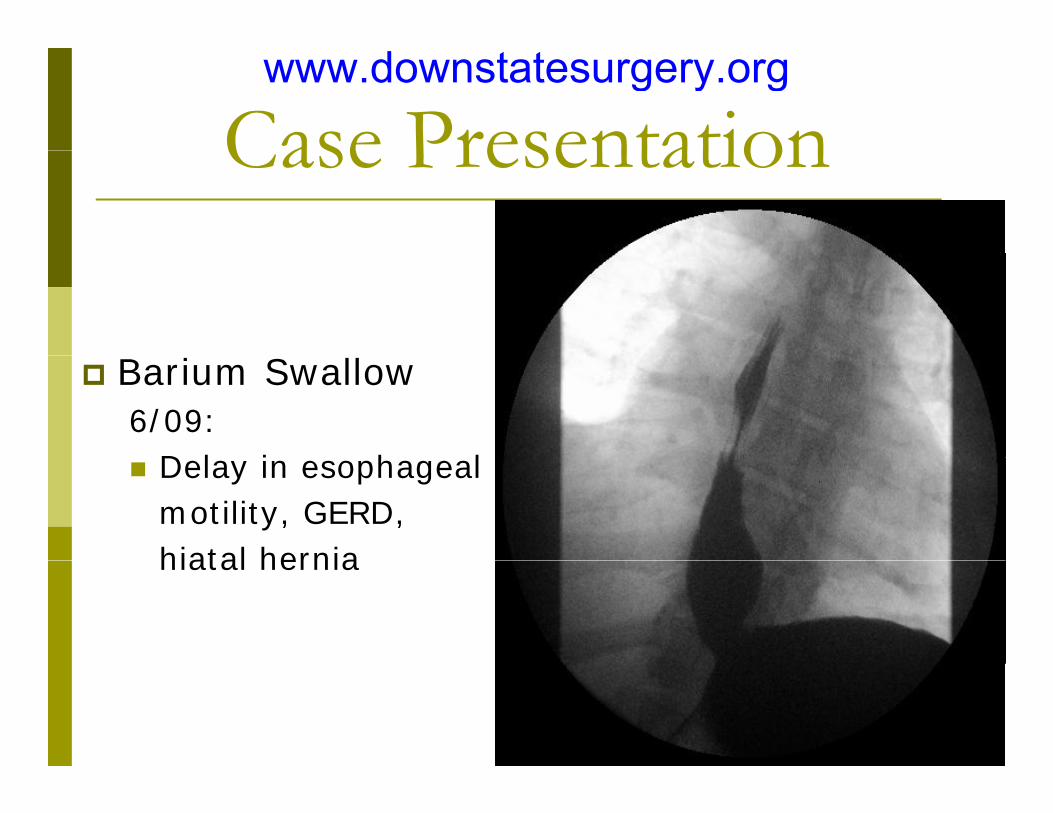
Barium Swallow 6/09:
D l i h l Delay in esophageal motility, GERD, hiatal herniahiatal hernia
www.downstatesurgery.org
Case PresentationCase Presentation6/26/09: laparoscopic converted to open Nissen f d li ti & t t h tfundoplication & emergent tracheostomy
POD #1: trach collar
POD #3: trach downsized
POD #4: trach capped
POD #5 b i ll l ll i POD #5: barium swallow: normal swallowing, normal motility, no delay, no reflux, no leak
Tolerated regular diet
POD #6: pt decannulated & discharged home
www.downstatesurgery.org
Case PresentationCase Presentation
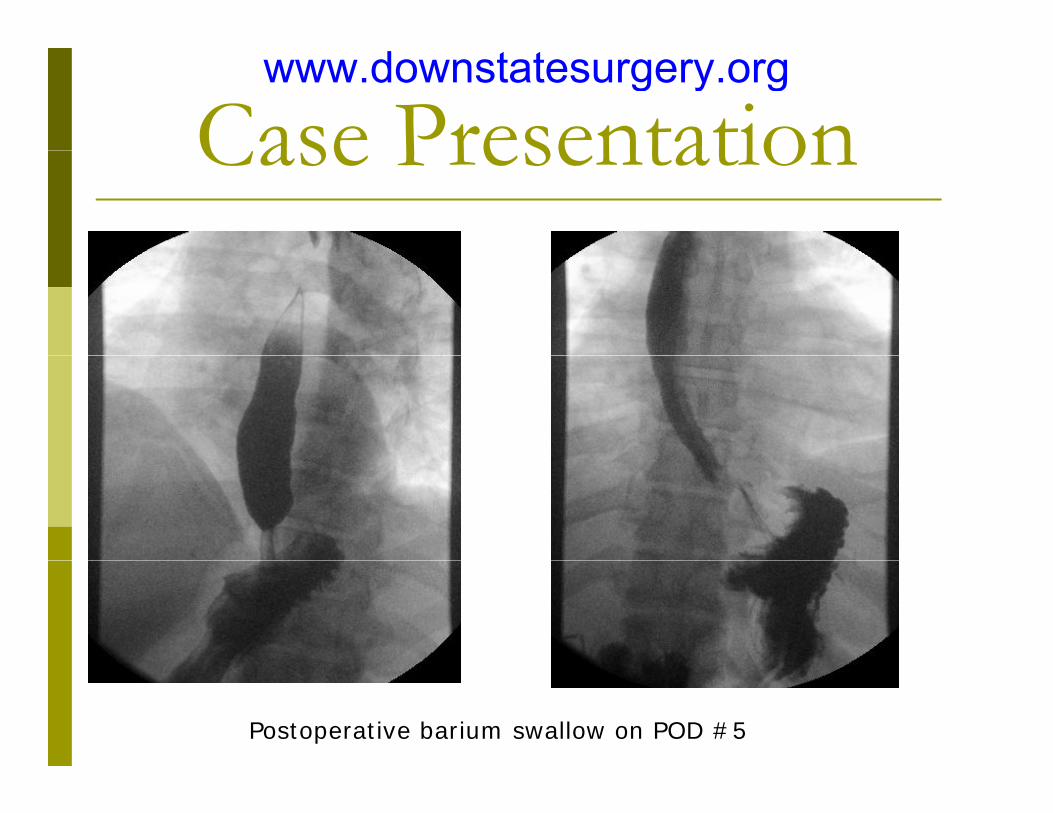
Postoperative barium swallow on POD #5
www.downstatesurgery.org

Q i ? ?Questions ? ?
www.downstatesurgery.org

HistoryHistoryHenry Ingersoll Bowditch
1846 hiatal hernias described at postmortem
Technically first description of paraesophageal hernia.
1898 Walter Cannon & Albert Moser: 1898 Walter Cannon & Albert Moser: anatomy & physiology of the cardia w/ contrast material
1904 Eppinger: hiatal hernia diagnosed in live pt Stylopoulos N, Rattner DW. The history of hiatal hernia surgery: from Bowditch
to laparoscopy. Ann Surg. 2005 Jan; 241(1):185-93
www.downstatesurgery.org

HistoryHistory1955: Rudolph Nissen 1955: Rudolph Nissen Nissen Fundoplication
1957: J. Leigh Collis gastroplastyg p y
1970’s Nissen 1970 s Nissen fundoplication widely acceptedaccepted
Stylopoulos N, Rattner DW. The history of hiatal herniasurgery: from Bowditch to laparoscopy. Ann Surg. 2005Jan; 241(1):185-93
www.downstatesurgery.org

Hiatal HerniasHiatal Hernias
Type I: sliding
Type II: paraesophageal (“rolling”)
Type III: combined I & II
classified according to the anatomic position of the GEJ in relationship to the diaphragmatic hiatus the composition of relationship to the diaphragmatic hiatus, the composition of the hernia sac, and the extent of herniated stomach
www.downstatesurgery.org

Type IType IIntrathoracic GEJ, Contains gastric cardia and fundusContains gastric cardia and fundusNo true hernia sac
Most common of the 3 hiatal hernias
More common in women (4:1), 5th
& 6th decades, obese
Usually reducible but may become fixed above diaphragm
Attenuation of phrenoesophageal membrane (i e the subdiaphragmatic Attenuation of phrenoesophageal membrane (i.e., the subdiaphragmatic continuation of the transversalis fascia)
the phrenoesophageal membrane streches cranially due to intra-bd i l d th t f h l h t i ll i abdominal pressure and the tug of esophageal shortening on swallowing
Suggests acquired weakness of tissue secondary to aging and strain on diaphragm
www.downstatesurgery.org
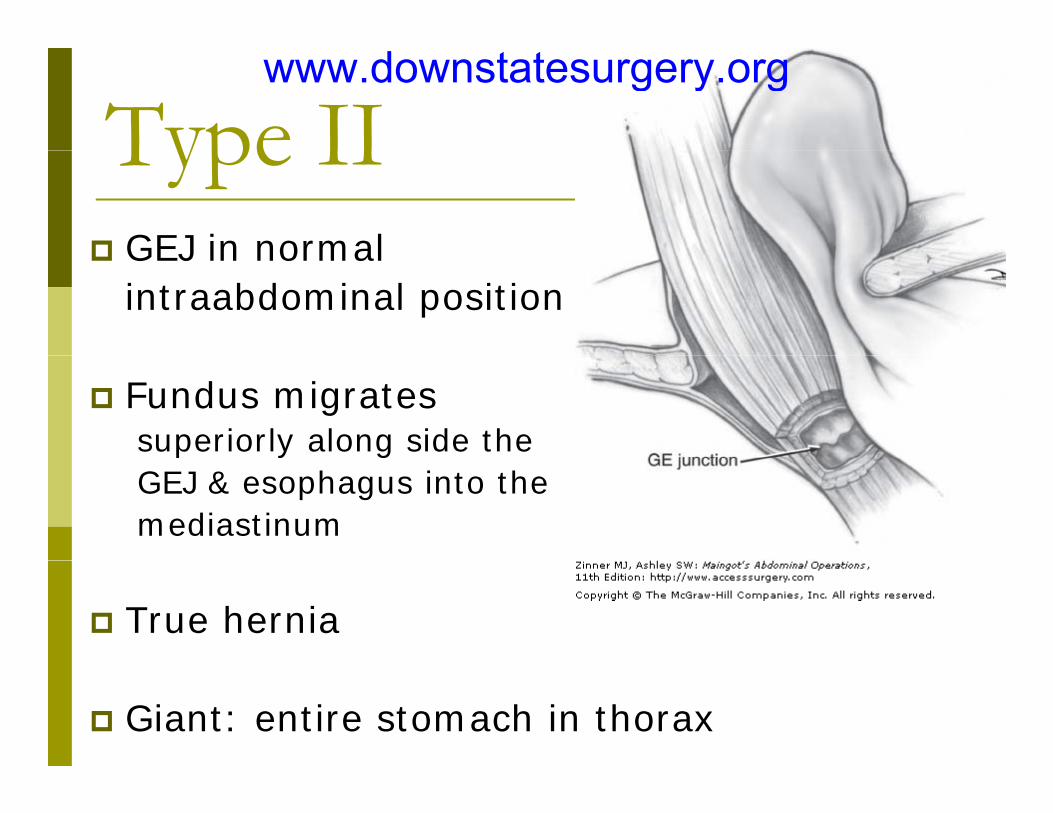
Type IIType IIGEJ in normal GEJ in normal intraabdominal position
Fundus migrates superiorly along side the GEJ & esophagus into the mediastinum
True hernia
Giant: entire stomach in thorax
www.downstatesurgery.org

SymptomsSymptomsType I:yp
HeartburnRegurgitation(loss of antireflux mechanism; goal is to restore physiology of ( ; g p y gycardia)
Type II: Type II: Epigastric painPostprandial fullnessDysphagiaDysphagiaAbdominal bloatingRespiratory symptomsAnemia (1/3 of pts)Anemia (1/3 of pts)Borchardt’s triad: chest pain, retching w/ inability to vomit, inability to pass NGT
www.downstatesurgery.org
Work UpWork UpPhysical Exam
CXR
EGDSee pathology
Barium swallowEvaluate dysphagia short esophagus guide endoscopistEvaluate dysphagia, short esophagus, guide endoscopist
24 hr pH monitoring 60% paraesophageal, 71% sliding p p g , g
Manometry Esophageal motility, LES function, LES position
CTHelps confirm extent of hernia
www.downstatesurgery.org
Indications for SurgeryIndications for SurgeryFailure of medications to control symptoms
(however, pts with good response to medical Tx often (however, pts with good response to medical Tx often have better surgical response)
Complications while on medications (ulceration, Barrett’s, t i t )stricture)
Noncompliance with medical treatment
Preference for surgery over lifelong medications(cost, inconvenience, side effects)
Severely incompetent LES
Paraesophageal herniap g1. Isolauri J, Luostarinen M, Viljakka M, et al. Long-term comparison of antireflux surgery versus
conservative therapy for reflux esophagitis. Ann Surg. 1997;225:295–299. 2. DeMeester TR, Stein HJ. Surgical treatment of gastroesophageal reflux disease. In: Castell DO, ed. The
Esophagus. Boston: Little, Brown; 1992:579–626.
www.downstatesurgery.org
Goals of SurgeryGoals of SurgeryReturn herniated content below diaphragm
Resect hernia sac
Establish adequate esophageal length
Repair hernia defect
www.downstatesurgery.org
Laparoscopic Paraesophageal Hernia R iRepair
Positioning:Positioning:Low lithotomy, Steep trendelenbergp gHands tucked5 ports
www.downstatesurgery.org
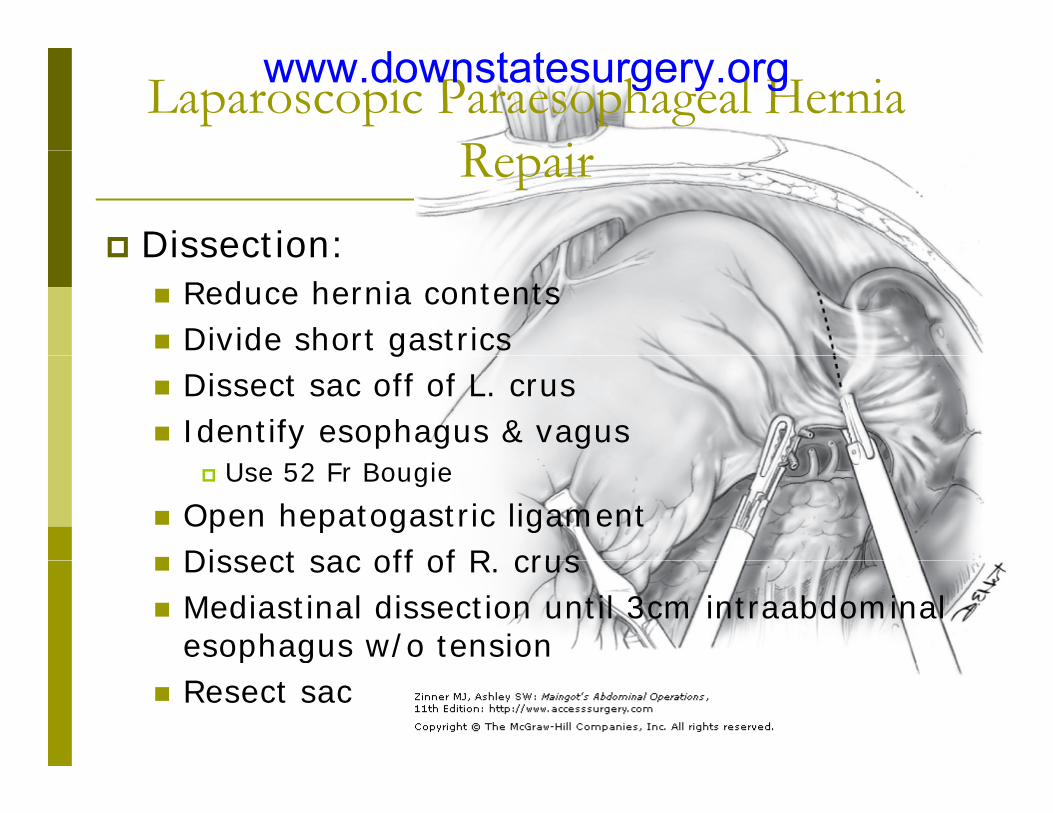
Laparoscopic Paraesophageal Hernia R iRepair
Dissection:Dissection:Reduce hernia contentsDivide short gastricsgDissect sac off of L. crusIdentify esophagus & vagus
Use 52 Fr Bougie
Open hepatogastric ligamentDissect sac off of R crusDissect sac off of R. crusMediastinal dissection until 3cm intraabdominal esophagus w/o tensiongResect sac
www.downstatesurgery.org
Laparoscopic Paraesophageal Hernia R iRepair
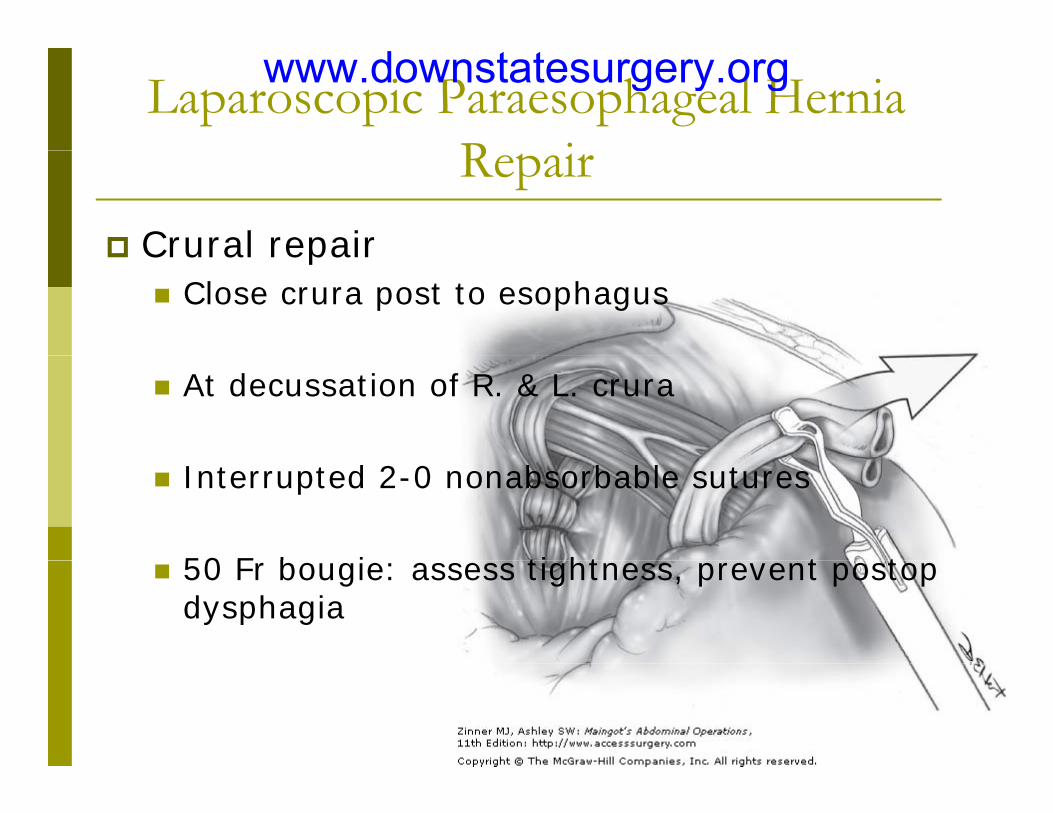
Crural repairCrural repairClose crura post to esophagus
At decussation of R. & L. crura
Interrupted 2-0 nonabsorbable sutures
50 F b i ti ht t t 50 Fr bougie: assess tightness, prevent postop dysphagia
www.downstatesurgery.org
Laparoscopic Paraesophageal Hernia R iRepair
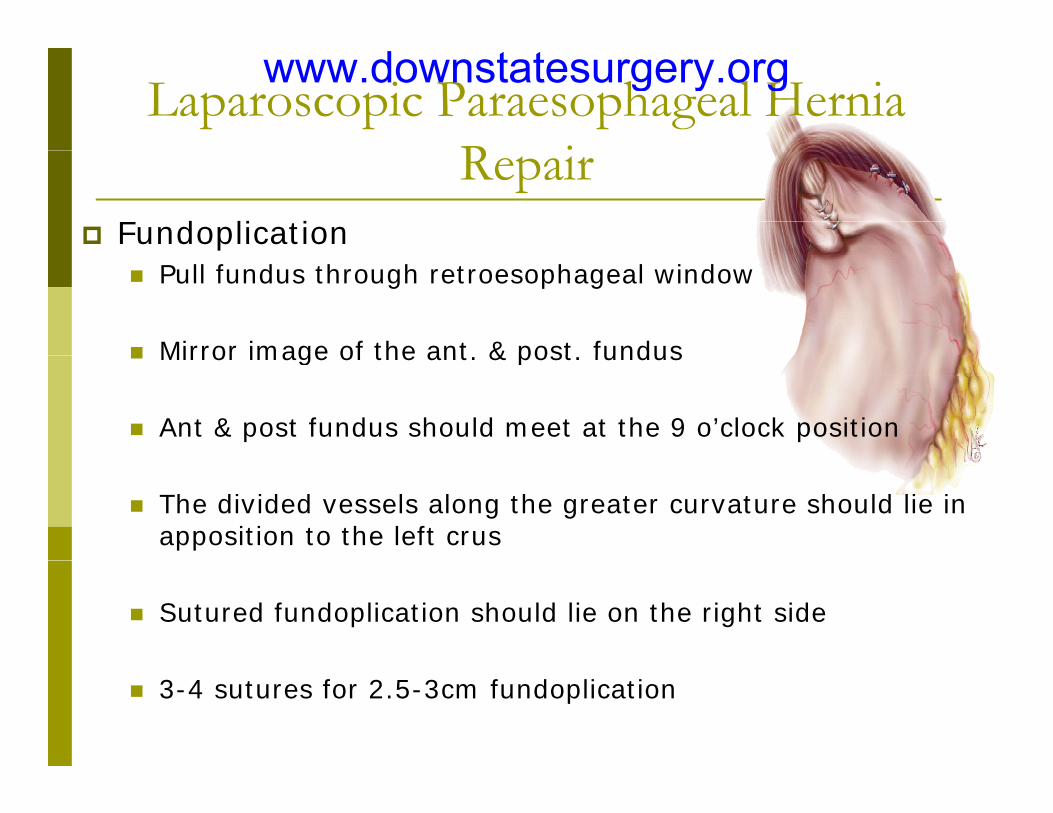
FundoplicationPull fundus through retroesophageal window
Mirror image of the ant & post fundusMirror image of the ant. & post. fundus
Ant & post fundus should meet at the 9 o’clock position
The divided vessels along the greater curvature should lie in apposition to the left crus
Sutured fundoplication should lie on the right side
3-4 sutures for 2.5-3cm fundoplication
www.downstatesurgery.org

Transhiatal Hernia RepairTranshiatal Hernia RepairEsophagoscopy: extent of path, confirm absence of malignancy
L. posterolateral thoracotomy (6th or 7th
intercostal space)
Resect 1cm segement of rib below
www.downstatesurgery.org

Transhiatal Hernia RepairTranshiatal Hernia RepairMobilization of Esophagus & excision of hernia sac
Divide pulmonary ligament to inf pulmonary V
Incise mediastinal pleura to expose esophagus from carina to diaphragm
Watch out for vagus nervesWatch out for vagus nerves
Encircle esophagus w/ vagus nerves w/ penrose drain
Elevate esophagus and mobilize circumferentially toward diaphragm
Separate sac from pericardium anteriorly & aorta posteriorly
Dissect left to right, ant to post
www.downstatesurgery.org

Transhiatal Hernia RepairTranshiatal Hernia RepairDivision of Phrenoesopheal Membrane & pGastrohepatic ligament
h l h h lRetract esophagus anteriorly to expose phrenoesophageal membrane posteriorly
Divide membrane to allow entry into lesser sac
Divide esophageal branch of L. phrenic artery near the crusDivide esophageal branch of L. phrenic artery near the crus
Divide gastrohepatic ligament along undersurface of the R. crus & down to L gastric Acrus & down to L. gastric A
Visualize caudate lobe of the liver beneath the R. crus
www.downstatesurgery.org
Transhiatal Hernia RepairTranshiatal Hernia RepairMobilization of the stomachMobilization of the stomach
Ligate short gastrics (3-4)Elevate GEJ into chest & release any yorganoaxial rotation
Closure of cruraPlace 3-5 stitches at 1cm intervals post to ant in staggered fashionin staggered fashionAvoid spleen on L. & aorta on R.
www.downstatesurgery.org

Transhiatal Hernia RepairTranshiatal Hernia RepairAssesment of Esophageal length & removal of ant fat pad
If t h d t d il h t If stomach does not reduce easily = short esophagus
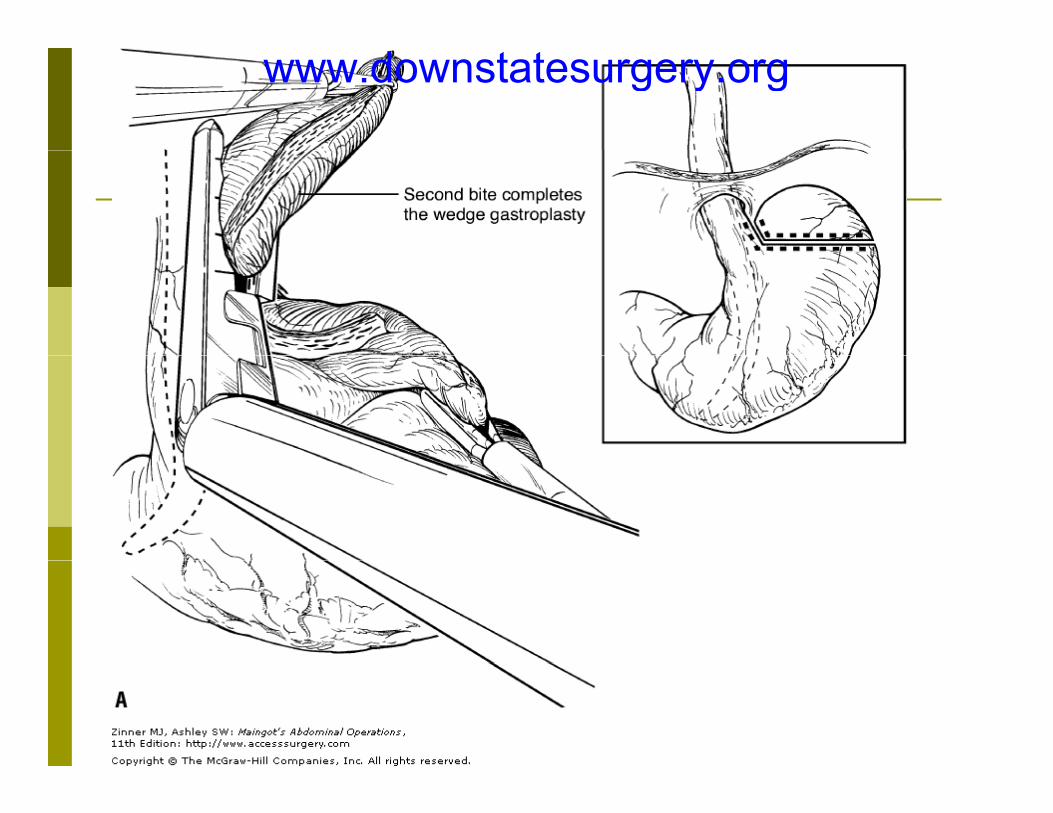
Collis gastroplasty54 Fr bougie for women, 56 for men into stomach past GEJGEJBougie held anteriorly against lesser curvature, fundus retracted away at a R. angle to the esophagus60mm GIA applied immediately alongside the bougie on pp y g gthe greater curvatureOversew staple line w/ nonabsorbable 4-0 monofilament suture
www.downstatesurgery.org
www.downstatesurgery.org

Transhiatal Hernia RepairTranshiatal Hernia RepairFundoplication & reduction of wrap into abdomen
Fundus is passed posteriorly behind esophagus
Approximate fundus to esophagus or gastroplasty tube w/ 2 interrupted 2-0 silk sutures
Wrap should accommodate a finger alongside esophagusWrap should accommodate a finger alongside esophagus
2 clips placed at superior aspect of the wrap to confirm length & location of wrap on CXRg p
Remove bougie
Secure top of fundoplication to underside of diaphragm using 2 2-0 polypropylene mattress sutures
www.downstatesurgery.org

Types of FundoplicationTypes of FundoplicationNissen:
360 degrees360 degreesIncrease LES muscle pressurenormal esophageal length and normal motility
Toupet180 degreesNormal esophageal length and decreased motilityNormal esophageal length and decreased motility
Belsey Mark IV270 degrees through the chest270 degrees through the chest
Dor180 degree anterior wrap used w/ myotomy for achalasia180 degree anterior wrap used w/ myotomy for achalasia
www.downstatesurgery.org

Operative ManagementOperative ManagementOpen vs. Lap:
Minimal difference for experienced techniciansBenefits of Lap:
Improved visualization due to magnificationImproved visualization due to magnificationShorter hospital stay
Lap sometimes more difficult in obese pts
Indication for thoracic approachpplarger hernias w/ suspected esophageal shortening, allows maximal mobilization
i hi l h i i f di iPrior hiatal hernia repair, safer dissection
Current Surgical Therapy 9th Edition Cameron 2008
www.downstatesurgery.org

Operative ManagementOperative ManagementOutcomes:
Symptomatic: 88% have resolution for up to 4 yrs, 92% have resolution of anemia
Anatomic: 41% have recurrent hernia after 4 yrsAnatomic: 41% have recurrent hernia after 4 yrs
Long term success depends onLong term success depends on1. tension-free repair w/ 4cm intraabdominal esophagus 2. durable approximation of diaphragmatic crura3 t t hi f f d li ti t h i t th 3. correct matching of fundoplication technique to the peristaltic function of the esophagus
Current Surgical Therapy 9th Edition Cameron 2008
www.downstatesurgery.org

Ann Surg. 2006 July; 244(1): 42–51.
Repair of 104 Failed Anti-Reflux Operations
Atif Iqbal, MD,* Ziad Awad, MD, FRCSI,† Jennifer Simkins, MD,* Ricky Shah, BS,‡ Mumnoon Haider, MD,* Vanessa Salinas, MD,* Kiran Turaga, MD,* Anouki Karu, MS,‡ Sumeet K. Mittal, MD,* and Charles J. Filipi, MD, FACS*From the *Department of Surgery, Creighton University School of Medicine, Omaha, NE; †Department of Surgery, University of Missouri, Columbia, MO; and ‡Creighton
Objective: assess whether reoperative surgery for failed Nissen fundoplication is beneficial & classify mechanisms of failure
p g y, g y , , ; p g y, y , , ; gUniversity School of Medicine, Omaha, NE.
Study group: 104 pt’s w/ previous fundoplication for GERD who underwent reoperation
Failure Rate: Open fundoplication: 9% to 30%Laparoscopic: 2% to 17%Laparoscopic: 2% to 17%
58 Laparoscopic, 12 open, 34 thoracotomy
Included Nissen, Toupet, & Dor fundoplications, and Collis gastrostomy when indicated (surgeon’s discretion)
www.downstatesurgery.org

Ann Surg. 2006 July; 244(1): 42–51.
Repair of 104 Failed Anti-Reflux Operations
Atif Iqbal, MD,* Ziad Awad, MD, FRCSI,† Jennifer Simkins, MD,* Ricky Shah, BS,‡ Mumnoon Haider, MD,* Vanessa Salinas, MD,* Kiran Turaga, MD,* Anouki Karu, MS,‡ Sumeet K. Mittal, MD,* and Charles J. Filipi, MD, FACS*From the *Department of Surgery, Creighton University School of Medicine, Omaha, NE; †Department of Surgery, University of Missouri, Columbia, MO; and ‡Creighton
Mechanism of Failure
p g y, g y , , ; p g y, y , , ; gUniversity School of Medicine, Omaha, NE.
Crus closure failureHiatal stenosisFundoplication disruptionLoose or slipped fundoplicationShort esophagusShort esophagusGastroparesisWrong primary diagnosis
www.downstatesurgery.org

Ann Surg. 2006 July; 244(1): 42–51.
Repair of 104 Failed Anti-Reflux Operations
Atif Iqbal, MD,* Ziad Awad, MD, FRCSI,† Jennifer Simkins, MD,* Ricky Shah, BS,‡ Mumnoon Haider, MD,* Vanessa Salinas, MD,* Kiran Turaga, MD,* Anouki Karu, MS,‡ Sumeet K. Mittal, MD,* and Charles J. Filipi, MD, FACS*From the *Department of Surgery, Creighton University School of Medicine, Omaha, NE; †Department of Surgery, University of Missouri, Columbia, MO; and ‡Creighton
Operative Approach for Failed Procedures
p g y, g y , , ; p g y, y , , ; gUniversity School of Medicine, Omaha, NE.
Open thoracotomyRecommended when > 2 cm of gastric tissue within thoracic cavity on esophagramy p gShort esophagus suspected
L tLaparotomyMultiple previous failed operations
LaparoscopyPatient did not meet above criteria
www.downstatesurgery.org

Ann Surg. 2006 July; 244(1): 42–51.
Repair of 104 Failed Anti-Reflux Operations
Atif Iqbal, MD,* Ziad Awad, MD, FRCSI,† Jennifer Simkins, MD,* Ricky Shah, BS,‡ Mumnoon Haider, MD,* Vanessa Salinas, MD,* Kiran Turaga, MD,* Anouki Karu, MS,‡ Sumeet K. Mittal, MD,* and Charles J. Filipi, MD, FACS*From the *Department of Surgery, Creighton University School of Medicine, Omaha, NE; †Department of Surgery, University of Missouri, Columbia, MO; and ‡Creighton
Pitfalls:p g y, g y , , ; p g y, y , , ; g
University School of Medicine, Omaha, NE.
Intraoperative perforations must be closed with sutures incorporating mucosa
Must have intraoperative EGD during surgery
Using a large bougie will allow a good asessment of the Using a large bougie will allow a good asessment of the mobility of the fundic wrap and secure an adequate fundoplication
Must ligate and divide short gastric vessels
Do not hesitate to convert from laparoscopy to open
www.downstatesurgery.org

ReferencesReferences1. Maingot’s Adominal Operations 11th Edition 20072. Schwartz’s Principles of Surgery, 8th Edition 20053. Current Surgical Therapy 9th Edition Cameron 20084. Stylopoulos N, Rattner DW. The history of hiatal hernia surgery: from Bowditch to
laparoscopy. Ann Surg. 2005 Jan; 241(1):185-935. Bombeck TC, Dillard DH, Nyhus LM: Muscular anatomy of the gastroesophageal
junction and role of the phrenoesophageal ligament. Ann Surg 164:643, 1966. 6. DeMeester TR, Stein HJ. Surgical treatment of gastroesophageal reflux disease. In:
Castell DO, ed. The Esophagus. Boston: Little, Brown; 1992:579–626.7. Isolauri J, Luostarinen M, Viljakka M, et al. Long-term comparison of antireflux
surgery versus conservative therapy for reflux esophagitis. Ann Surg. 1997;225:295–299.
8. Weber TR. Toupet fundoplication for gastroesophageal reflux in childhood.Arch Surg 1999 Jul;134(7):717 21 Surg. 1999 Jul;134(7):717-21.
9. Patti MG, Albanese CT, et al. Laparoscopic heller myotomy and dor fundoplication for esophageal achalasia in children. Journal of Pediatric Surg. 2001 Aug;36(8):1248-1251.
10 Terry M Smith CD Branum GD: Outcomes of laparoscopic fundoplication for 10. Terry M, Smith CD, Branum GD: Outcomes of laparoscopic fundoplication for gastroesophageal reflux disease and paraesophageal hernia. Surg Endosc 2001; 15:691.and others
11. Iqbal et al. Reoperation for failed anti-reflux surgery. Ann Surg 2006;244: 42-51.
www.downstatesurgery.org

CommentsComments
www.downstatesurgery.org
QuestionsQuestionsWhich is true?Which is true?
A) Type I hiatal hernia is a rolling herniaA) Type I hiatal hernia is a rolling hernia
B) Type II hiatal hernia is a sliding hernia
C) Type III hiatal hernia is a combined Type I lidi d T II h l h isliding and Type II paraesophageal hernia
D) None of the aboveD) None of the above
www.downstatesurgery.org
QuestionsQuestionsThe first to describe hiatal hernias in The first to describe hiatal hernias in postmortem pt’s was
a) Moser
b) Bowditch
c) Nissen
d) Belsey
www.downstatesurgery.org
QuestionsQuestionsBorchardt’s triad includes of the following except
a) chest pain
b) retching w/ inability to vomit
) i bilit t NGTc) inability to pass NGT
d) gastric distention
www.downstatesurgery.org
QuestionsQuestionsDuring hiatal hernia repair, all of the During hiatal hernia repair, all of the following are important except:
A) have intraoperative EGD
B) make the fundoplication as tight as possible
C) use a large bougie
D) dissect the short gastrics to obtain adequate D) dissect the short gastrics to obtain adequate intraabdominal esophageal length
www.downstatesurgery.org

www.downstatesurgery.org