history of low back-pain
TRANSCRIPT

HISTORY OF
LOW BACK PAINDR. SAMSUL AREFIN
ResidentDept . of Anesthesia ,Analgesia &
Intensive careBSMMU

Common cause of low back pain• Myofascial lower back pain
HNP of lumber spineSpinal canal stenosisLumber spondylolysisSpondylolisthesisFacet SyndromeAdult kyphosis and scoliosisInfective pathology of spine eg. TB & osteomyelitisPrimary neoplasm of the neural tissue and MMMetastatic disease of spineRheumatic conditions eg. Ankylosing spondylitis and fibromyalgiaMetabolic causes of back painFBSS
Ref. Handbook of pain medicine / G. Dureja / 2nd ed

PAIN CLINIC ,BSMMU10 years old boy comes with low back pain
26 years old boy comes with low back pain
65 years old female comes with the low back pain

COMMON CAUSES OF BACK PAIN IN VARIOUS AGE GROUPSCHILDREN
ADOLESCENTS
YOUNG ADULTS
• scoliosis• Spondylolisthesis• Pyogenic or tuberculous infections• Calve’s disease
• Scheuermann’s disease• Scoliosis(idiopathic and postural)• Mechanical baack pain• Adolescent intervertebral disc syndrome• Pyogenic or tuberculous infection
• Prolapsed intervertebral disc• Spondylolidthesis• Spinal fracture• Ankylosing apondylitid• Coccydynia• Pyogenic or tuberculous infection• Spinal stenosis

MIDDLE – AGED
ELDERLY
• Mechanical back pain• Prolapsed intervertebral disc• Scheuermann’s disease and old
fracture• Spondylolisthesis• Rheumatoid arthritis• Spinal stenosis • Paget’s disease• Cocccydynia• Spinal metastases• Pyogenic osteitis of spine
• Osteoarthritis(primary or secondary)• True senile kyphosis• Osteoporosis(with or without fracture)• Osteomalacia(with or without fracture)• Spinal metastases.

• Site and nature of pain : localized of diffuse persistent or intermittent
• Onset of pain : When did the symptoms commence?
pattern of onset: slow and insidious rapid or sudden ( strongly suggestive of mechanical factor) history of an injury ( a sudden twist or strain or sneeze occurring when the patient was in a flexed position :a common history for intervertebral disc prolapse )
• Character of pain Usually described by adjectives like sharp, dull, burning, tingling, boring , stabing
Directly relevant previous history : Is there any history of previous similar attack? or any previous trouble with the spine ?
• Radiation of the pain : does the pain radiates to the legs ? how far down does the pain go & what are the area involved ? commonly affaected nerve root L 4,L 5 &S1
•

Associated any paresthesia
N.B. Pain radiates into legs is not necessarily due to nerve root compression. It seems that irritation of facet joints , ligaments and muscles may produce dull aching pain in the buttock and back of the thighs.Pain arising from nerve root is usually sharp and knief like
Back with without radiation Back pain with radicular lower extremity pain or weakness
Musculoskeletal lower back painSpondylosis Facet syndrome Adult scoliosis Adult kyphosisSpondylolisthesisInfectionFractureDislocationArthritisRheumatological conditionReffered pain from visera
HNPSpinal stenosisFractureDislocationCauda equina syndrome
Ref. Handbook of pain medicine / G. Dureja/ 2nd ed


•
Timing of pain Constant: back ache with spinal pathology ( tumour , infection or inflammation constant night pain , distinct short lived pain when turning in bed) > Sleep disturbance Episodic In particular day or part of whole day Any changes in severity as day progress Morning pain associated with stiffness Exacerbating and relieving factor Mechanical back pain bending or sudden movement may make the pain worse ,whereas lying flat , particularly on a hard surface or applying local heat or even sitting, may relieve pain. During rest pain increase or decrease?
•
•
• Motor involvement any weakness in the lower limbs or any muscle wasting or fibrillation? Any disturbance of gait or balance , any tendency to giving way of the legs , any sign of foot drop?
• Any constitutional symptoms : malaise , fever , weight loss
involvement of other joints associated GIT problems associated genitourinary symptoms respiratory difficulty major neurological disturbance

COMMON CAUSES OF LOW BACK PAIN
PATHOLOGY AGE PAIN NATURE ASSOCIATED PAIN
ASSOCIATED SYMPTOMS
Degenerative spondylosis
> 40 years Mechanical Distance claudication
Active patient
Spondylolisthesis
<20 years>40 years
Mechanical Extension Hyperextension on activity
Trauma Any age Mechanical _ Trauma
Infection Any age Non- mechanical Rest pain Fever
Mets >50 years Non-mechanical Rest pain Primary+LOWLOA
Osteoporosis >60 years Mechanical _ Trivial injury

Findings PID Lateral stenosis Central stenosis
Average age 43 41 65
Duration of symptoms Shortest
Pain at rest, at night and on coughing
+ Equal +
SLR +++ Sometimes Hardlyever
Motor disturbance Commonest specially knee jerk
Sensory changes Commonest
DIFFERENCE BETWEEN DISC PROLAPSE AND SPINAL STENOSIS

RED FLAG FEATURES
•Histosry• Age <20 years or >55 years• Recent significant trauma• Pain- thorasic (dissecting aneurysm)• non-mechanical
(infection/tumour/pathological fracture)• Fever(infection)• Difficulty in micturition• Faecal incontinence• Motor weakness• Sensory changes in the
perineum( saddle anesthesia)• Sexual dysfunction( erectile/ejaculatory
failure)• Gait change ( cauda equine syndrome)• Bilateral sciatica
•Past medical history
•Systemic review
• Cancer ( metastases)• Previous steroid use
(osteoporotic collapse)
• Weight loss/malaise without obvious cause

YELOOW FLAG features
These are psychosocial factors associated with greater likelihood of long term chronicity and disability
•A history of anxiety, depression chronic pain irritable bowel syndrome, chronic fatigue, social withdrawal.
•A belief that the diagnosis is severe such as cancer, faulty beliefs can lead to ‘catastrophisation’ and avoidance of activity.
•Lack of belief that the patient can improve leads to an expectation that only passive, rather than active, treatment will be active.
•Ongoing litigation or compensation claims such as work , road traffic accident.
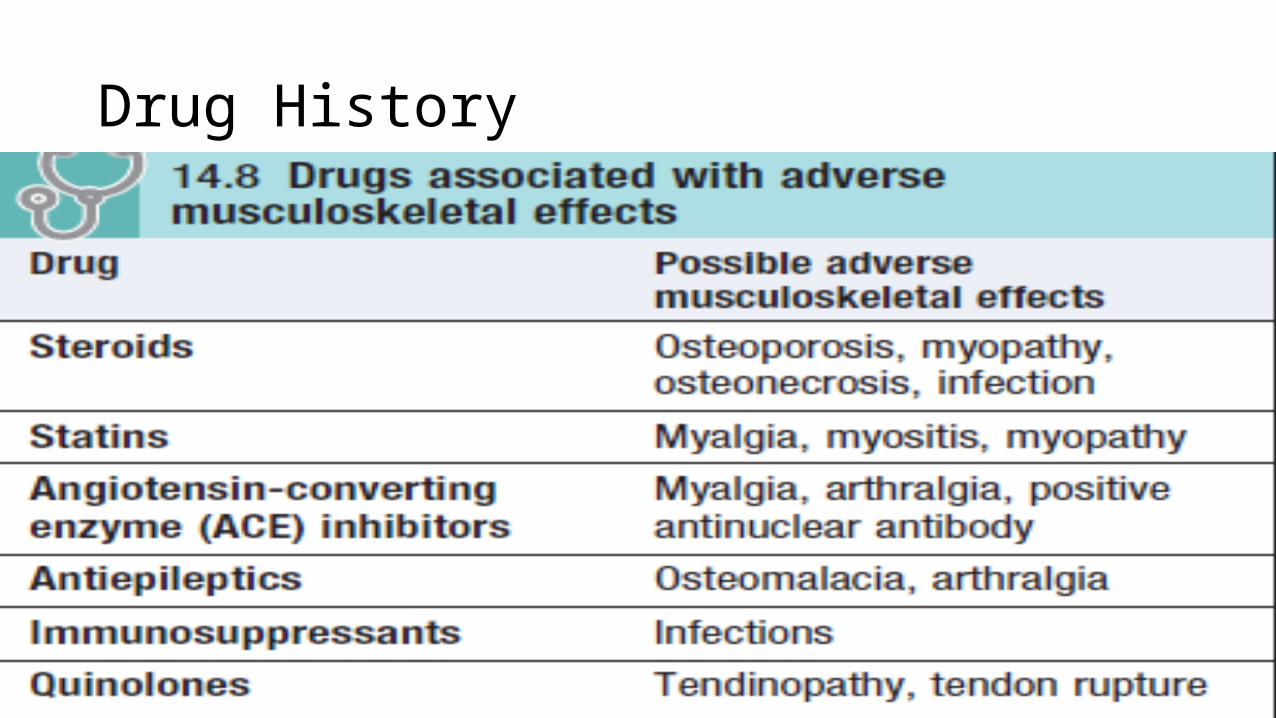
Drug History

Family History
In a young man with gradual-onset chronic back pain, a positive family history for reactive arthritis, psoriasis or inflammatorybowel disease, and the presence of peripheral joint involvementor anterior uveitis all suggest a diagnosis of ankylosingspondylitis.
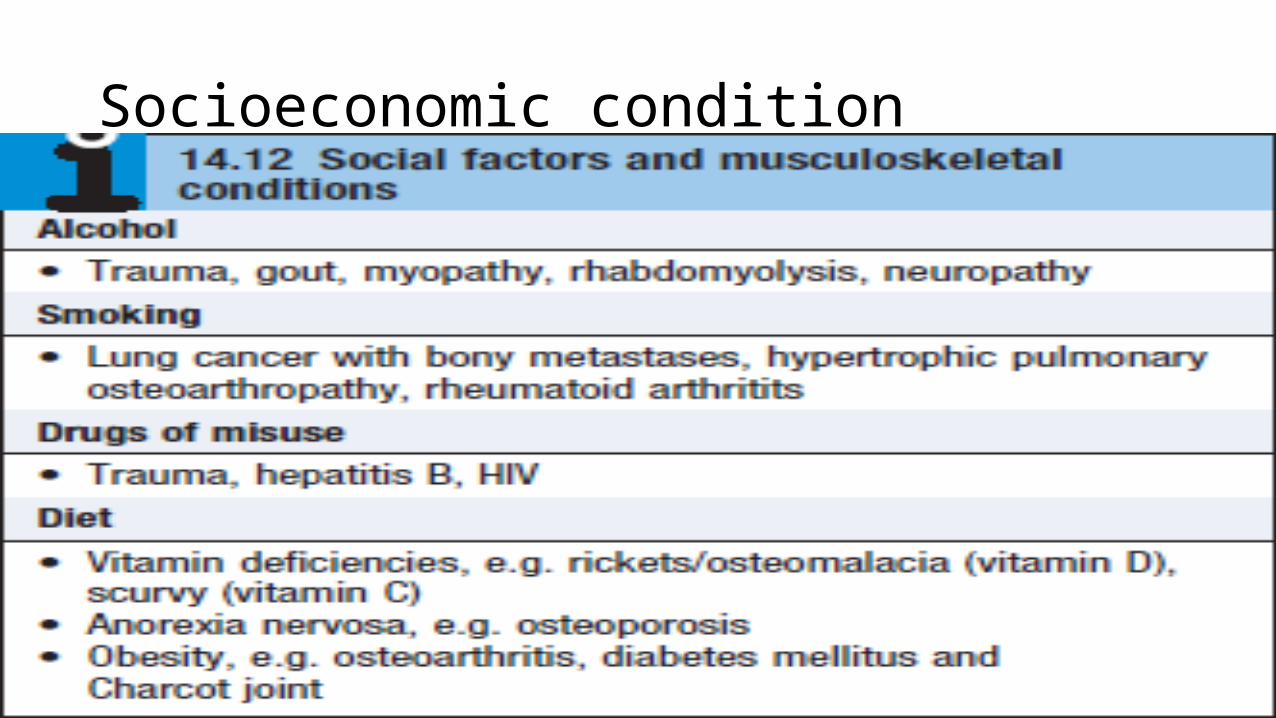
Socioeconomic condition

Occupational history• Longstanding sitting, standing
Constant exrtemitiesmovementWeight lifting
• Psychological historyDepressionUnemploymentJob satisfactionFamilial disharmony