holly wyatt, m.d. associate professor of medicine division of endocrinology, metabolism and diabetes...
TRANSCRIPT
Holly Wyatt, M.D.
Associate Professor of Medicine
Division of Endocrinology, Metabolism and Diabetes
Associate Director
Anschutz Health and Wellness Center
OBESITY TREATMENT: THE CUTTING EDGE
Dr. Wyatt has served as an advisor for Orexigen Pharmaceuticals, Arena Pharmaceuticals, Wellspring Camps, Retrofit Inc. and Eisai Inc.
She receives royalties from Up to Date and has received grant funding from the NIH, Orexigen, Norvo Nordisk and GI Dynamics.
She has ownership interests in Active Planet LLC and has co-ownership on a patent for a weight loss maintenance strategy.
DISCLOSURE SUMMARY
GAME PLAN
Current Treatment Guidelines
Advances in Diet
Advances in PA
New Medications
Surgery
New Areas- ahead of the curve
CURRENT APPROACH TO OBESITY TREATMENT
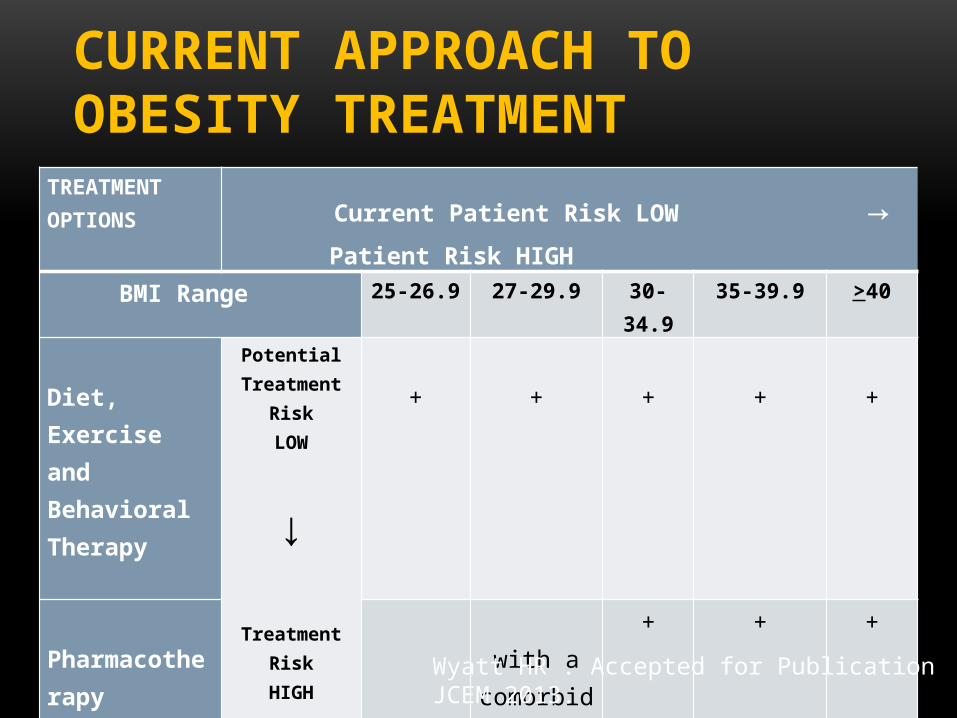
TREATMENT OPTIONS Current Patient Risk LOW → Patient Risk HIGH
BMI Range 25-26.9 27-29.9 30-34.9 35-39.9 >40
Diet, Exercise and Behavioral Therapy
Potential Treatment
RiskLOW
↓Treatment Risk
HIGH
+
+
+
+
+
Pharmacotherapy
with a
comorbidity
+ + +
Surgery
with a
comorbidity
+
Wyatt HR . Accepted for Publication JCEM 2013.

NEW OBESITY GUIDELINES IN 2013
• The NHLBI has announced that new Guidelines for Obesity, Hypertension and Lipids will be released jointly in 2013
• Guidelines for Lifestyle and for Risk Assessment will be released concomitantly. These new treatment guidelines will replace the older 1998 Guidelines and provide evidenced based approaches for obesity treatment for the practicing clinician.
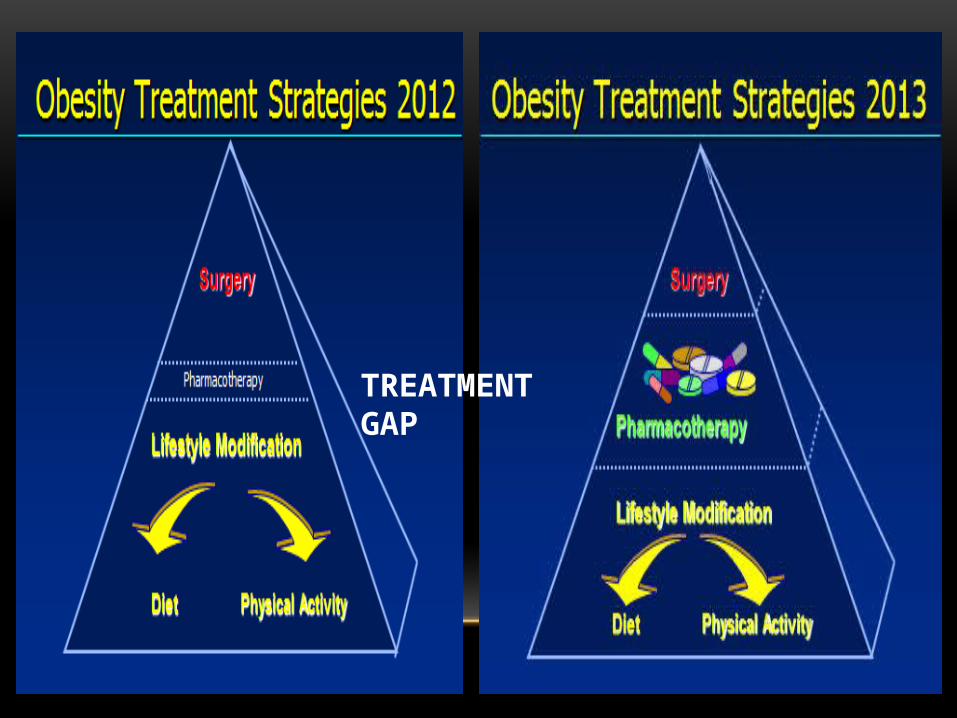
TREATMENT GAP
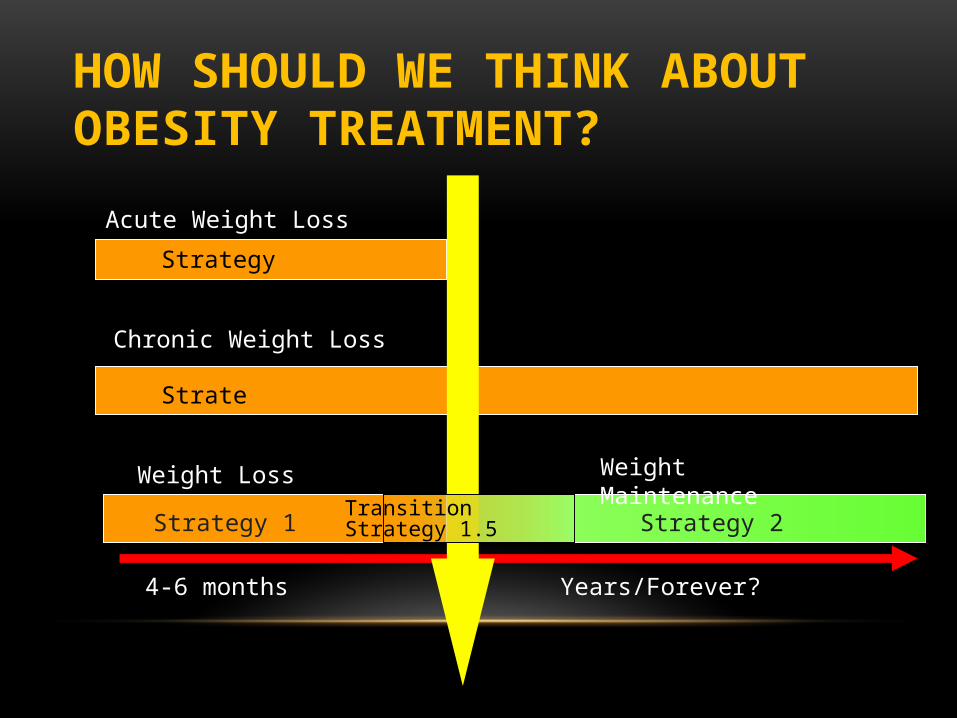
HOW SHOULD WE THINK ABOUT OBESITY TREATMENT?
Acute Weight Loss
Chronic Weight Loss
Weight Loss Weight Maintenance
4-6 months Years/Forever?
Strategy
Strategy
Strategy 1 Strategy 2TransitionStrategy 1.5
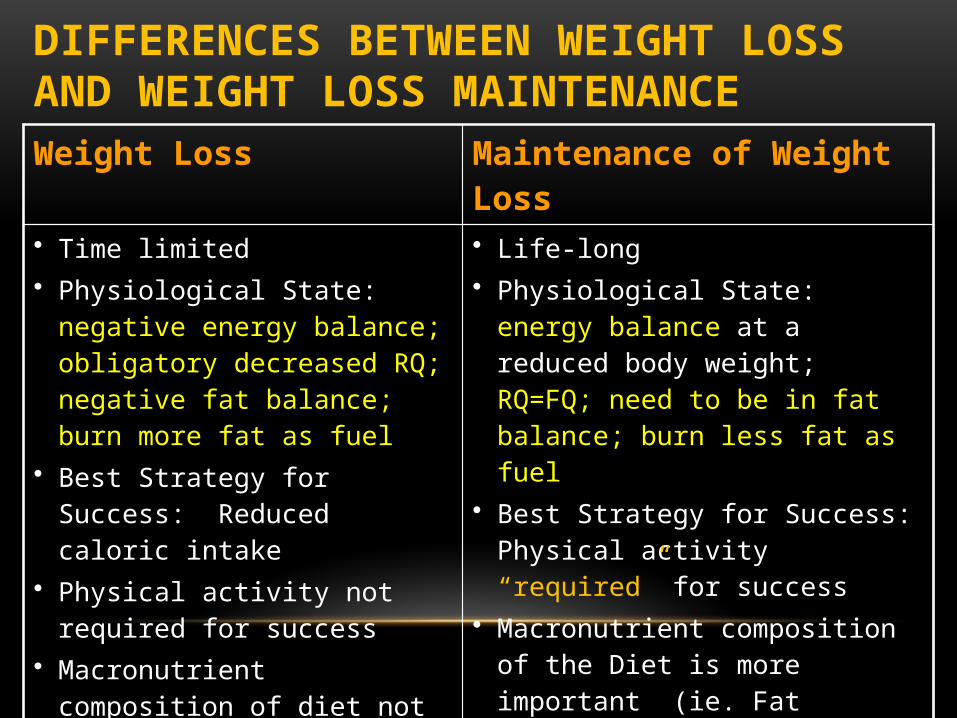
DIFFERENCES BETWEEN WEIGHT LOSS AND WEIGHT LOSS MAINTENANCE Weight Loss Maintenance of Weight Loss• Time limited• Physiological State: negative energy
balance; obligatory decreased RQ; negative fat balance; burn more fat as fuel
• Best Strategy for Success: Reduced caloric intake
• Physical activity not required for success• Macronutrient composition of diet not as
important• Common• Relatively easy• Multiple strategies have success• Exciting!
• Life-long• Physiological State: energy balance at a
reduced body weight; RQ=FQ; need to be in fat balance; burn less fat as fuel
• Best Strategy for Success: Physical activity “required” for success
• Macronutrient composition of the Diet is more important (ie. Fat balance is important)
• Rare• Harder/More elusive• Less strategies?• Longer-term health risk becomes an issue• Boring!
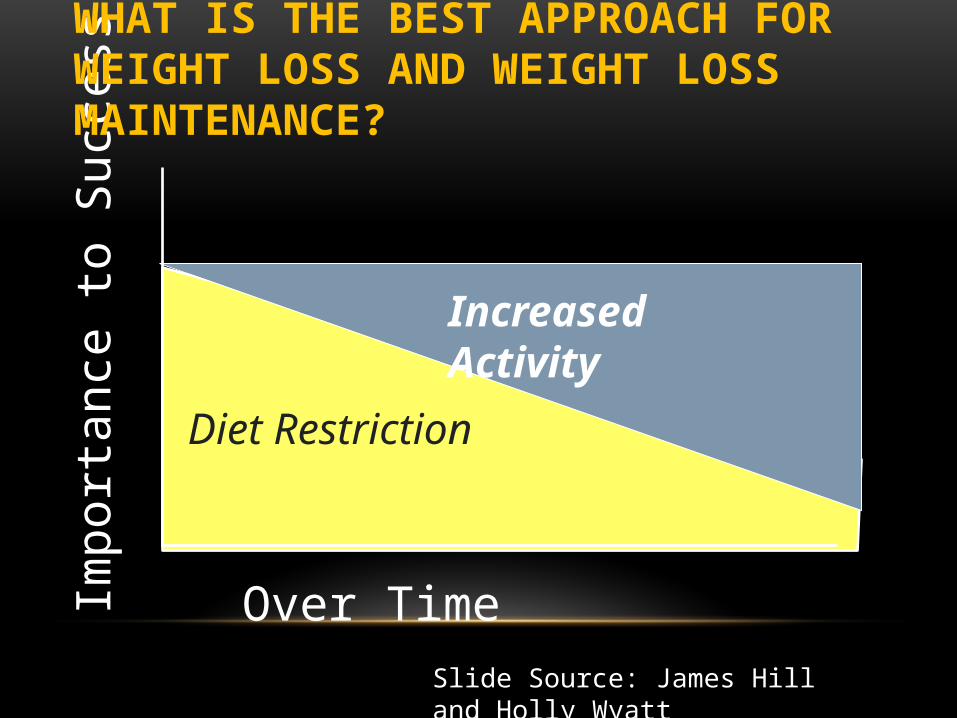
Impo
rtan
ce to
Suc
cess
Diet Restriction
Over Time
Increased Activity
Slide Source: James Hill and Holly Wyatt
WHAT IS THE BEST APPROACH FOR WEIGHT LOSS AND WEIGHT LOSS MAINTENANCE?
DIETS DON’T WORK? OR DO THEY ?
WHAT IS THE BEST DIET FOR WEIGHT LOSS?
WHAT IS THE BEST MACRONUTRIENT COMPOSITION OF A DIET FOR WEIGHT LOSS?
• Wadden et al presented a comprehensive review highlighting the randomized, controlled trials that have compared diets with varying macronutrient composition
• No single diet emerged as a clear winner despite a very robust number of clinical studies in this area
• TAKE AWAY: Impact of the caloric restriction that a diet produces outweighs the impact of the macronutrient composition of the calories consumed in that diet
Wadden TA, Webb VL, Moran CH, Bailer BA 2012 Lifestyle modification for obesity: new developments in diet, physical activity, and behavior therapy. Circulation 125:1157-1170
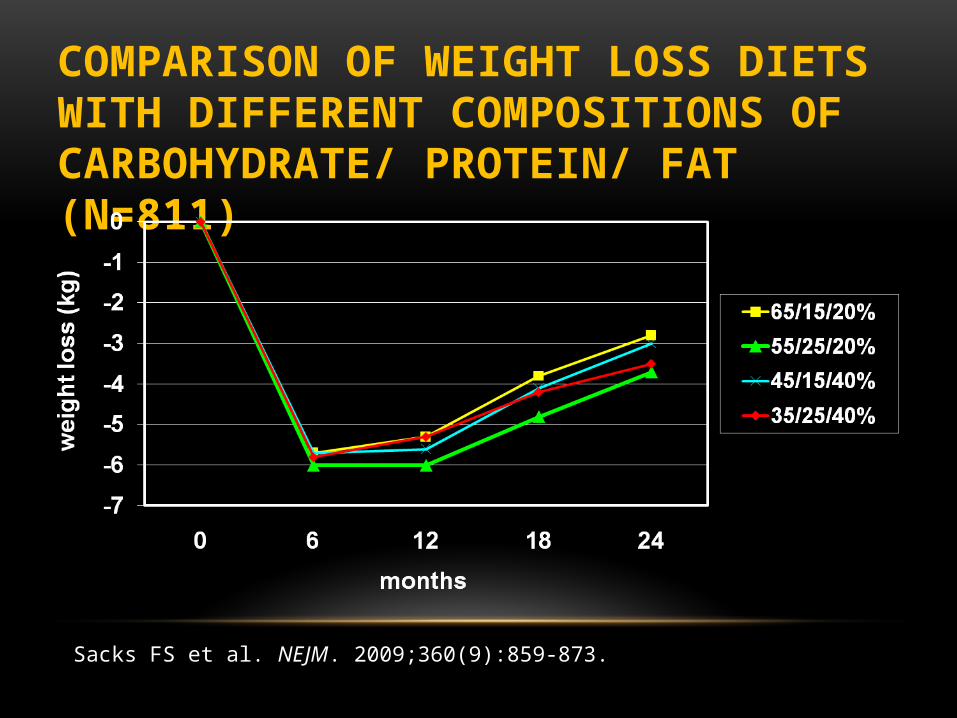
COMPARISON OF WEIGHT LOSS DIETS WITH DIFFERENT COMPOSITIONS OF CARBOHYDRATE/ PROTEIN/ FAT (N=811)
Sacks FS et al. NEJM. 2009;360(9):859-873.

WHAT DOES PREDICT DIETARY WEIGHT LOSS SUCCESS?

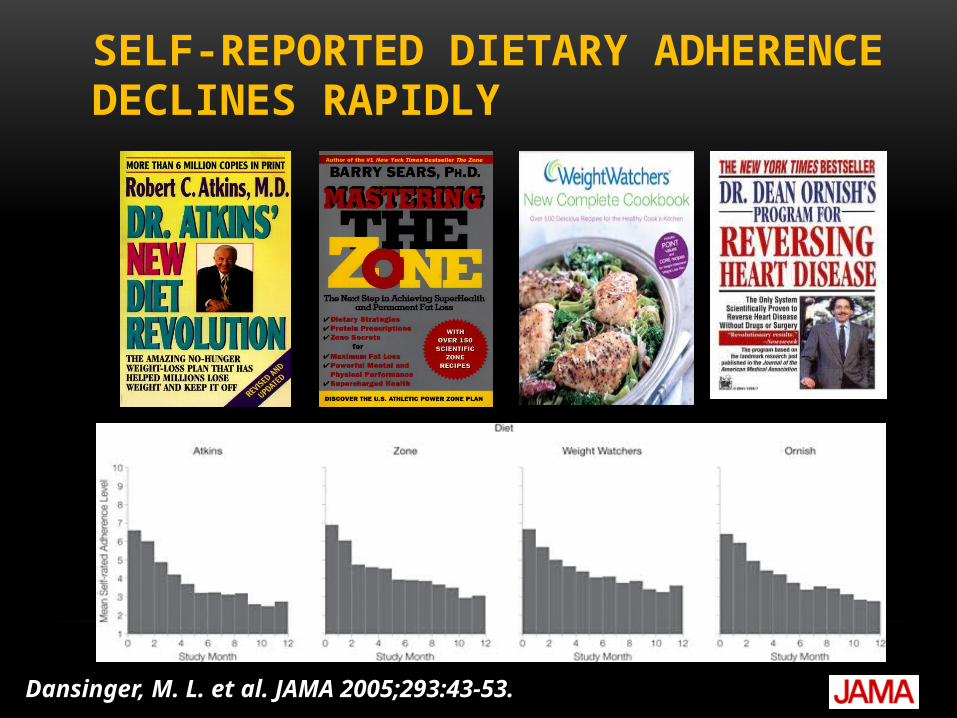
IT IS NOT WHAT YOU EAT BUT HOW LONG YOU CAN EAT IT
Dansinger, M. L. et al. JAMA 2005;293:43-53
Copyright restrictions may apply.
SELF-REPORTED DIETARY ADHERENCE DECLINES RAPIDLY
Dansinger, M. L. et al. JAMA 2005;293:43-53.

WHAT ARE THE BEST STRATEGIES TO MAXIMIZE WEIGHT LOSS ?
• Your physiology and environment can be overpowered by cognitive eating control strategies (diets)
• There are many diet strategies to reduce calories short-term
• Caloric restriction trumps macronutrient composition• Adherence is the key• Matching individuals to the “best” diet • Should the goal be too get off as much weight as
possible?
HOW MUCH PA DO WE PRESCRIBE TO PREVENT WEIGT REGAIN?
• The data consistently shows that for the majority of patients 60 minutes of moderate intensity activity most days of the week is an amount required to prevent or mitigate weight loss regain.
• A recent review of randomized trials and observational data by Donnelly et al in 2009 highlighted and confirmed this PA rec
• This high level of PA is also supported by self-reports and objective measures of individuals in the National Weight Control Registry (NWCR)
• As well as a recent prospective analysis in the Nurses’ Health Study published in 2010
Donnelly JE et al. 2009. Medicine and science in sports and exercise 41:459-471Mekary RA et al. 2010. Obesity 18:167-174
WE DO KNOW A LOT ABOUT WHAT WILL WORK !
BUT HOW DO WE GET OUR PEOPLE TO DO IT ?
MOST EXCITING RECENT ADVANCES IN OBESITY TREATMENT IN 2013 ARE IN DRUG THERAPY
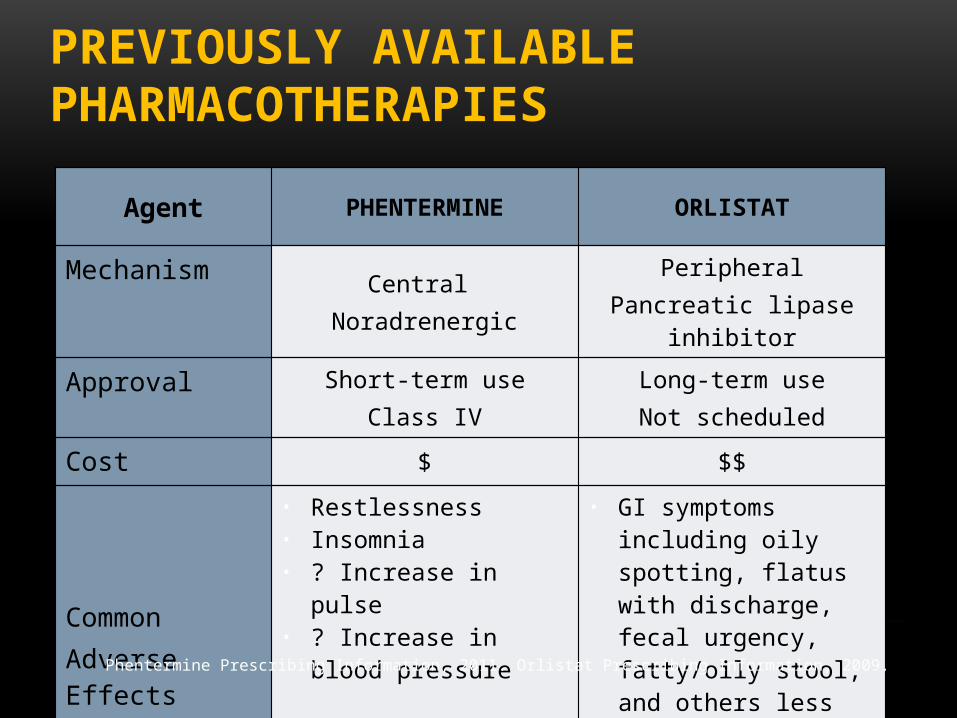
PREVIOUSLY AVAILABLE PHARMACOTHERAPIES
Agent PHENTERMINE ORLISTAT
Mechanism Central Noradrenergic
PeripheralPancreatic lipase inhibitor
Approval Short-term useClass IV
Long-term useNot scheduled
Cost $ $$
CommonAdverse Effects
• Restlessness• Insomnia• ? Increase in pulse• ? Increase in blood pressure
• GI symptoms including oily spotting, flatus with discharge, fecal urgency, fatty/oily stool, and others less frequently
• Increase in urinary oxalate
Phentermine Prescribing Information, 2011. Orlistat Prescribing Information, 2009.
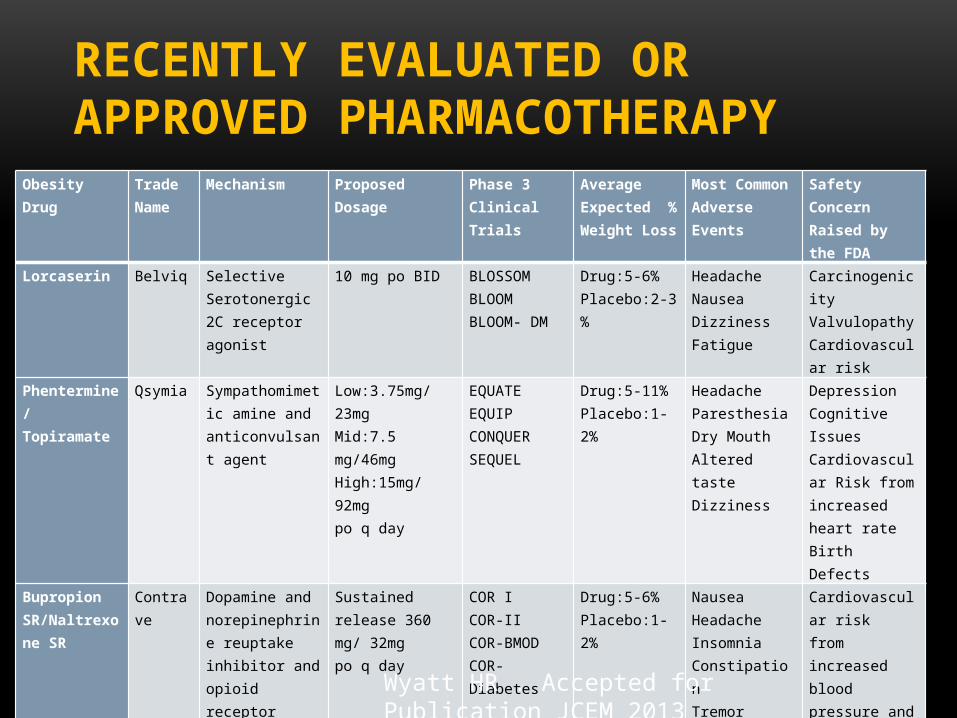
RECENTLY EVALUATED OR APPROVED PHARMACOTHERAPY
Obesity Drug Trade Name
Mechanism Proposed Dosage Phase 3 Clinical Trials
Average Expected % Weight Loss
Most Common Adverse Events
Safety Concern Raised by the FDA
Lorcaserin Belviq Selective Serotonergic 2C receptor agonist
10 mg po BID BLOSSOMBLOOMBLOOM- DM
Drug:5-6%Placebo:2-3 %
Headache Nausea Dizziness Fatigue
Carcinogenicity Valvulopathy Cardiovascular risk
Phentermine/Topiramate
Qsymia Sympathomimetic amine and anticonvulsant agent
Low:3.75mg/23mgMid:7.5 mg/46mgHigh:15mg/92mgpo q day
EQUATEEQUIPCONQUERSEQUEL
Drug:5-11%Placebo:1-2%
HeadacheParesthesiaDry MouthAltered tasteDizziness
DepressionCognitive IssuesCardiovascular Risk from increased heart rateBirth Defects
Bupropion SR/Naltrexone SR
Contrave Dopamine and norepinephrine reuptake inhibitor and opioid receptor antagonist
Sustained release 360 mg/ 32mgpo q day
COR ICOR-IICOR-BMODCOR-Diabetes
Drug:5-6%Placebo:1-2%
Nausea HeadacheInsomniaConstipationTremor
Cardiovascular riskfrom increased blood pressure and heart rate
Wyatt HR . Accepted for Publication JCEM 2013

LORCASERIN
• Selective serotonin 2C receptor agonist that works by decreasing food intake.
• Mechanism of action is similar to fenfluramine and dexfenfluramine except it is specific for the 2C serotonin receptor that is not found on the heart or heart valves.
• The result is a compound with a desirable increased satiety effect and no heart valve damage. Echo studies showed no increased incidence of FDA-defined cardiac valvulopathy. There is some concern the studies were not powered adequately for complete confidence because of a lower than expected event rate.
• The FDA advisory panel voted in favor of approval 18-4 in May 2012 and locaserin was officially approved by the FDA in June 2012.
• It should be available in 2013.
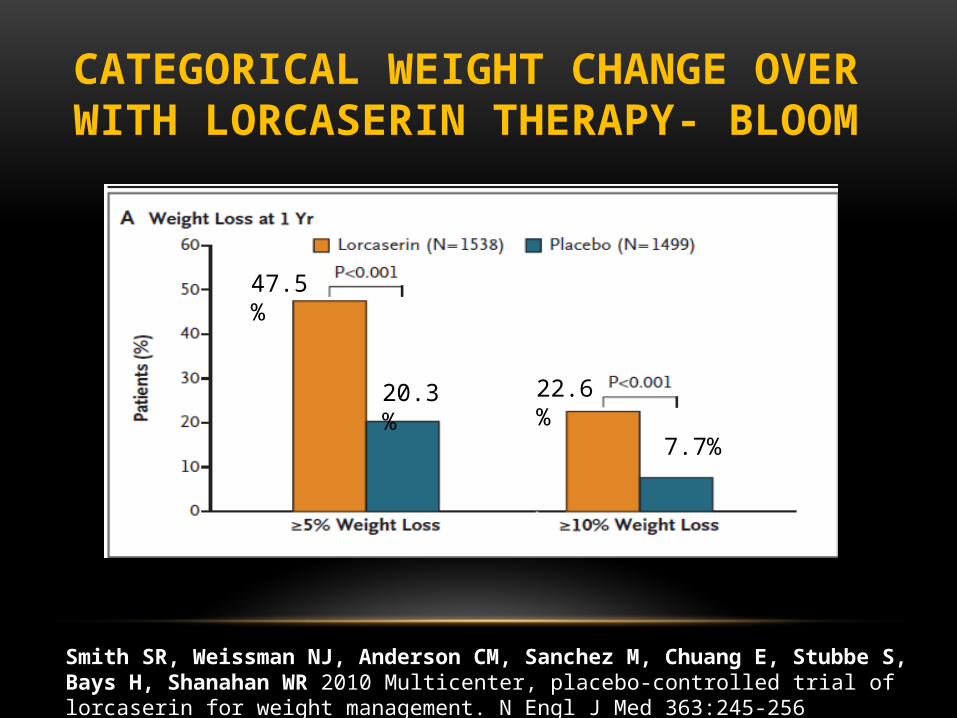
CATEGORICAL WEIGHT CHANGE OVER WITH LORCASERIN THERAPY- BLOOM
Smith SR, Weissman NJ, Anderson CM, Sanchez M, Chuang E, Stubbe S, Bays H, Shanahan WR 2010 Multicenter, placebo-controlled trial of lorcaserin for weight management. N Engl J Med 363:245-256
47.5%
20.3% 22.6%
7.7%
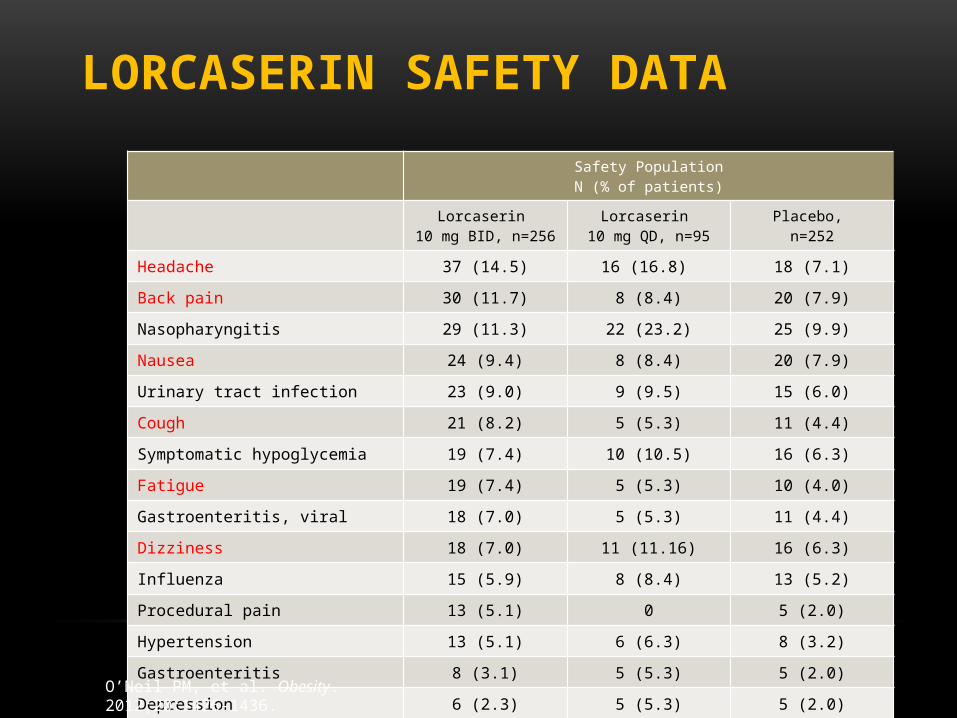
LORCASERIN SAFETY DATA
Safety PopulationN (% of patients)
Lorcaserin 10 mg BID, n=256
Lorcaserin 10 mg QD, n=95
Placebo, n=252
Headache 37 (14.5) 16 (16.8) 18 (7.1)
Back pain 30 (11.7) 8 (8.4) 20 (7.9)
Nasopharyngitis 29 (11.3) 22 (23.2) 25 (9.9)
Nausea 24 (9.4) 8 (8.4) 20 (7.9)
Urinary tract infection 23 (9.0) 9 (9.5) 15 (6.0)
Cough 21 (8.2) 5 (5.3) 11 (4.4)
Symptomatic hypoglycemia 19 (7.4) 10 (10.5) 16 (6.3)
Fatigue 19 (7.4) 5 (5.3) 10 (4.0)
Gastroenteritis, viral 18 (7.0) 5 (5.3) 11 (4.4)
Dizziness 18 (7.0) 11 (11.16) 16 (6.3)
Influenza 15 (5.9) 8 (8.4) 13 (5.2)
Procedural pain 13 (5.1) 0 5 (2.0)
Hypertension 13 (5.1) 6 (6.3) 8 (3.2)
Gastroenteritis 8 (3.1) 5 (5.3) 5 (2.0)
Depression 6 (2.3) 5 (5.3) 5 (2.0)
O’Neil PM, et al. Obesity. 2012;20:1426-1436.
HOW I SEE THE FUTURE ROLE OF LOCASERIN
• While locaserin meets FDA weight loss criteria, the efficacy is modest, but the risk profile is also low.
• For this drug, it is important for clinicians to realize that certain individuals may respond more (have a significantly greater weight loss) than other individuals.
• This drug may be one that eventually will be helpful in a smaller subset of obese “responders”
• Locaserin’s reduction in HbA1c levels appears more substantial than the weight loss reduction in the BLOOM-DM study and therefore diabetics may also prove to be a subset that may have greater benefit
• Locaserin has not been studied in combination with other drugs such as phentermine. While combining the two drugs (phentermine and locaserin) may increase weight loss, the safety of the combination has not been evaluated
PHENTERMINE AND TOPIRAMATE (PHEN/TPM)
• Phentermine induces central NE release and promotes weight loss by decreasing food intake. It is currently approved as a monotherapy for only short-term use.
• Topiramate monotherapy (200-400 mg/day) was approved in 1996 for the treatment of seizures and in 2004 for migraine prophylaxis (100mg/day) and is currently not approved as a monotherapy for weight management.
• Topiramate exhibits a combination of properties such as effects on sodium channels, enhancements of GABA-activated chloride channels, and inhibition of carbonic anhydrase isoenzymes, but the specific mechanism promoting weight loss is unclear.
• In combination the drugs have shown greater weight reduction than either agent alone.
PHENTERMINE AND TOPIRAMATE (PHEN/TPM)
• Higher dose topiramate trials as a monotherapy were halted because of the cognitive and depressive side effects.
• The combination of PHEN/TPM allows a lower dose of controlled release topiramate to be used and therefore a more acceptable adverse events profile.
• The drug combination of phentermine and topiramate received a 20-2 in favor vote from the February 2012 FDA advisory panel and was FDA approved in July of 2012. It became available for use in late 2012.
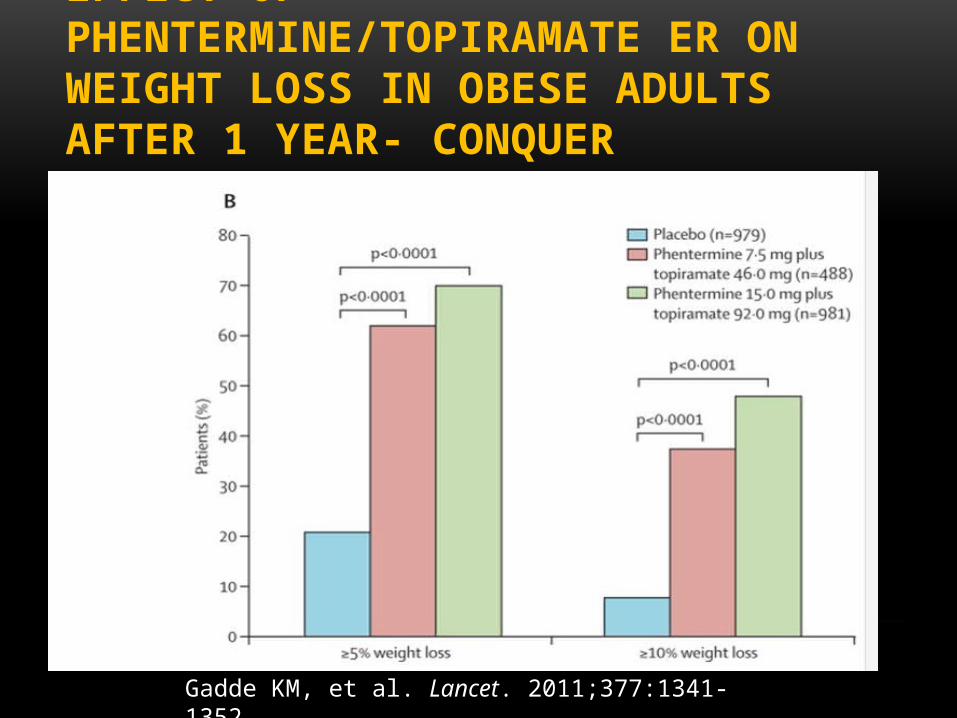
EFFECT OF PHENTERMINE/TOPIRAMATE ER ON WEIGHT LOSS IN OBESE ADULTS AFTER 1 YEAR- CONQUER
Gadde KM, et al. Lancet. 2011;377:1341-1352

PHENTERMINE/TOPIRAMATE ER SAFETY DATA
% Adverse Events
Placebo(n=993)
PHEN/TPM ER7.5/46 (n=498)
PValue
PHEN/TPM ER15/92 (n=994)
PValue
Dry mouth 2 13 <0.0001 21 <0.0001
Paraesthesia 2 14 <0.0001 21 <0.0001
Constipation 6 15 <0.0001 17 <0.0001
URI 13 12 0.7422 13 0.7906
Nasopharyngitis 9 11 0.2204 10 0.3947
Dysgeusia 1 7 <0.0001 10 <0.0001
Insomnia 5 6 0.3832 10 <0.0001
Headache 9 7 0.1983 10 0.4467
Dizziness 3 7 0.0005 10 <0.0001
Sinusitis 7 7 1.0000 9 0.1511
Back pain 5 6 0.6199 7 0.0386
Nausea 4 4 0.6754 7 0.0139
Fatigue 5 4 0.7010 7 0.1270
Diarrhoea 5 6 0.2229 6 0.3690
Blurred vision 4 4 0.7729 6 0.0157
UTI 4 5 0.1753 5 0.0855
Arthralgia 5 5 0.5373 4 0.3025
Bronchitis 4 4 1.0000 5 0.4004
GADDE KM, ET AL. LANCET. 2011;377:1341-1352. URI, UPPER RESPIRATORY INFECTION; UTI, URINARY TRACT INFECTION

HOW I SEE THE FUTURE ROLE OF PHEN/TPM
• Weight loss with the combination of PHEN/TPM is better than any of the obesity drugs in the pipeline at this time.
• Along with this increase in efficacy however comes a more troublesome risk profile that clinicians need to understand and actively address with their patients.
• Depression and cognitive issues have not been major issues in the more recent controlled release trials.
• Cardiovascular events and birth defects appear to be the issues that will need to be monitored closely.
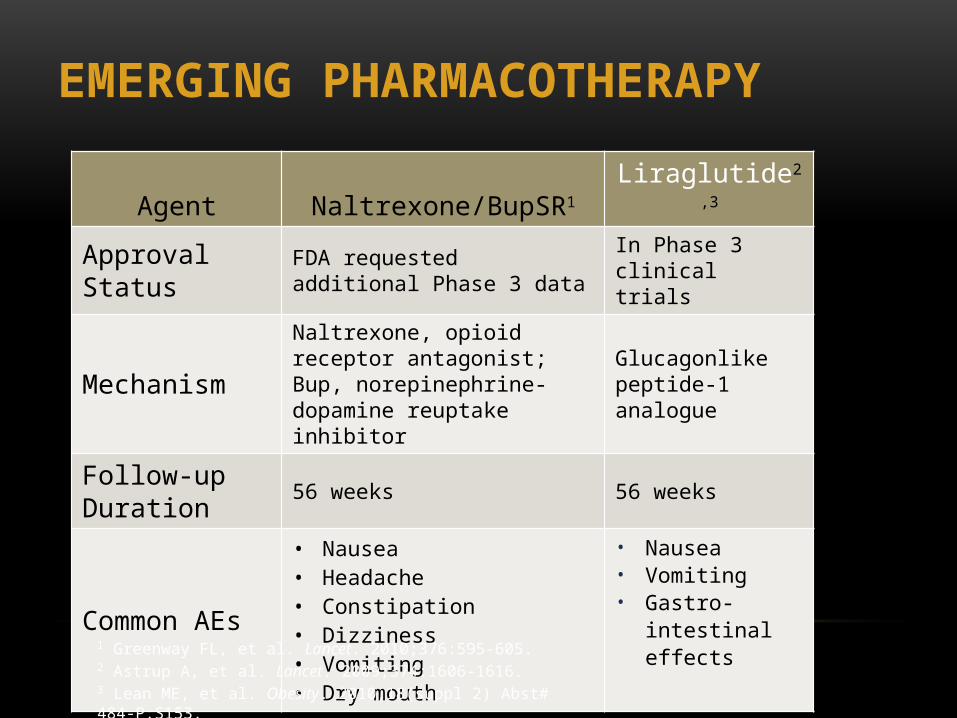
EMERGING PHARMACOTHERAPY
Agent Naltrexone/BupSR1 Liraglutide2,3
Approval Status FDA requested additional Phase 3 data In Phase 3 clinical trials
MechanismNaltrexone, opioid receptor antagonist; Bup, norepinephrine-dopamine reuptake inhibitor
Glucagonlike peptide-1 analogue
Follow-up Duration 56 weeks 56 weeks
Common AEs
• Nausea • Headache• Constipation• Dizziness• Vomiting• Dry mouth
• Nausea• Vomiting• Gastro-intestinal
effects
1 Greenway FL, et al. Lancet. 2010;376:595-605. 2 Astrup A, et al. Lancet. 2009;374:1606-1616. 3 Lean ME, et al. Obesity. 2010;18(suppl 2) Abst# 484-P:S153.
NALTREXONE AND BUPROPION (NAL/BUP)
• The Naltrexone SR/Bupropion SR combination functions as an opioid receptor antagonist combined with a norepinephrine and dopamine receptor reuptake inhibitor.
• Bupropion has neuronal effects that lead to reduced energy intake and increased energy expenditure.
• Naltrexone was chosen as a complement to bupropion in order to block compensating mechanisms that attempt to prevent long-term, sustained weight loss.
• The FDA advisory panel voted in favor of approval (13-7) of this combination in December of 2010 however the FDA declined to approve the drug in early 2011 going against the advisory panel recommendation
NALTREXONE AND BUPROPION (NAL/BUP)
• The FDA is requiring large scale safety study evaluating cardiovascular events. This was an interesting decision by the FDA given buproprion which is the drug potentially associated with the increase in cardiovascular risks, is currently available and used by millions of Americans for the treatment of mild depression or to stop smoking.
• Blood pressure and pulse were slightly increased indicating the potential for an increased cardiovascular events. Increased risk of seizures as well as syncope in the treatment group was also a safety concern that was noted.
• A study of this size and scope will take tremendous resources and time to complete. The earliest this drug could be approved is late 2014 or early 2015.-
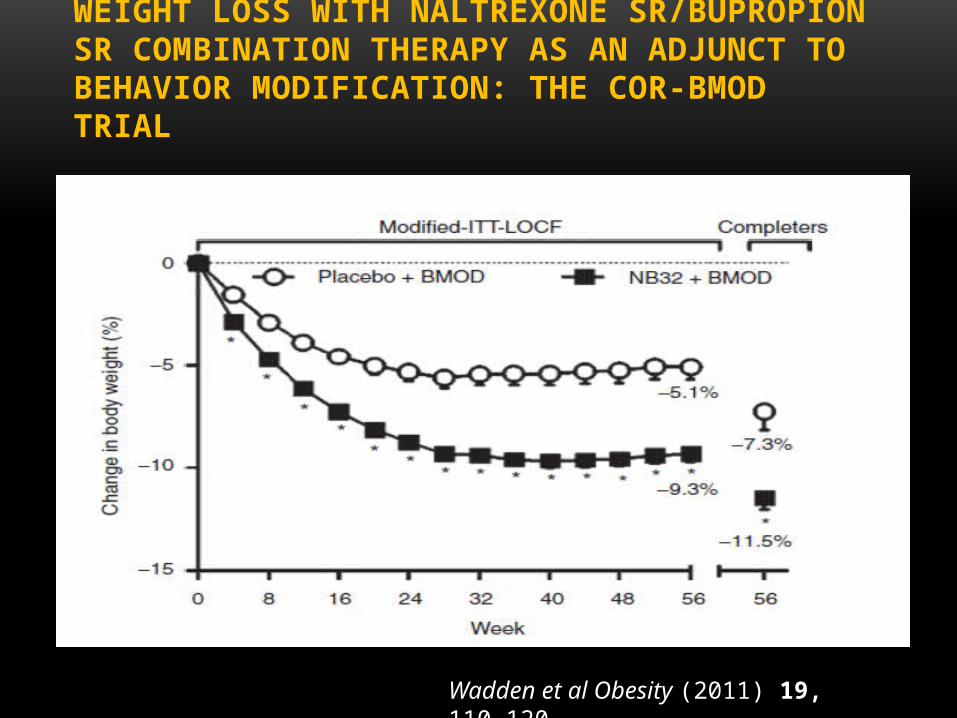
WEIGHT LOSS WITH NALTREXONE SR/BUPROPIONSR COMBINATION THERAPY AS AN ADJUNCT TOBEHAVIOR MODIFICATION: THE COR-BMOD TRIAL
Wadden et al Obesity (2011) 19, 110–120.

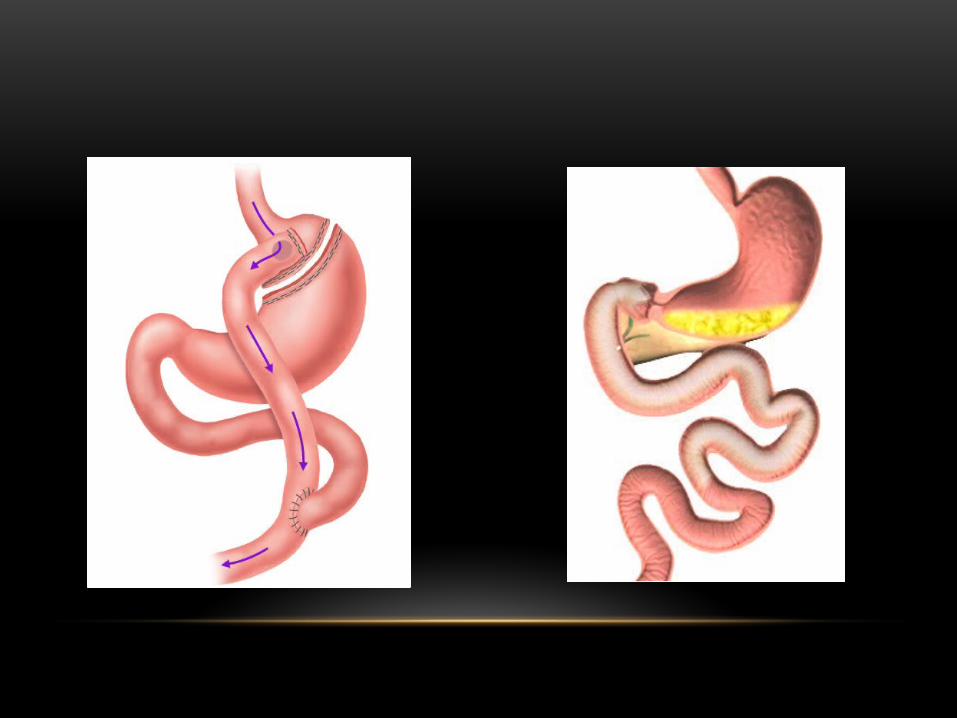
SURGICAL TREATMENT OF OBESITY
• The use of bariatric surgery as a treatment for obesity has grown dramatically over the last several years.
• The International Diabetes Federation recommended consideration of bariatric surgery as an accepted treatment option in patients with a BMI 30 to 35 when DM cannot be adequately controlled by traditional medical management
• In 2011 the FDA expanded approval of the LAP-BAND adjustable gastric banding system to be used in patients with a BMI of 30-34 with an existing condition related to their obesity.

WHAT IS NEW FOR THE FUTURE?
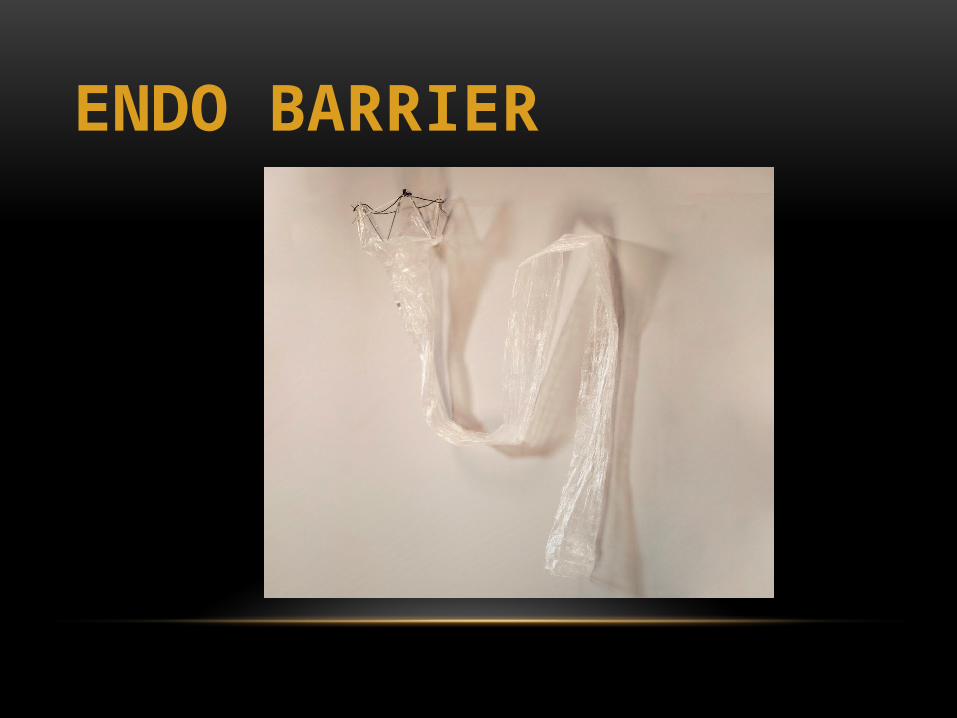
ENDO BARRIER
HOW DO WE GET PEOPLE TO DO IT?
• Motivation/Priorities • Carrot or Stick• Purpose/Mindset
• Skill Building • Rituals and Routines• Create New Environments

MAKE HEALTHY DECISIONS AUTOMATIC
• In todays world healthy behaviors takes planning and choices
• It’s not the default
• Sticking to your intentions requires willpower
BUILDING YOUR WILLPOWER MUSCLE
• Willpower is like a muscle
• It fatigues over the day
• You use it all day long
• Finite resource make it strong and use it wisely
• Examples of ways to use it efficiently
• Planning ahead
• Morning exercise

HABITS, ROUTINES AND RITUAL
• Patterns of behavior that are subconscious• Regular courses of action• Routines that have a deeper meaning
• Make the behaviors more likely to happen
HEALTHY DIET ROUTINES AND RITUALS
• Never go down the chip aisle in the grocery store
• Eat Starbucks oatmeal for breakfast when traveling
• Only buy single serving snacks
• Never bring ice cream home- always go out for it
• Prepare food on Sunday afternoon for the week
• Buy precut prewashed veggies
• Always order Grilled Teriyaki chicken, sauce of the side, only half the brown rice at my favorite Chinese restaurant
• Decline bread basket
• Always order dressing or sauce on the side
• Start with a veggies at dinner

HIGH ACTIVITY ROUTINES AND RITUALS • Only watch TV after exercise
• Always stand or walk on the cell phone
• Sleep by 10pm
• Prepack Gym bag
• Schedule working out on Sunday
• Meet friends
• Sign up for events
• Walk for 10 minutes at noon

CREATE A SUPPORTIVE ENVIRONMENT
• You want your relationships and surroundings to work for you not against your efforts
• Reengineer your environment
• Physical
• Social
• Make healthy the default when possible
• Push back against the environment

THE IMPORTANCE OF YOUR SOCIAL NETWORK
• The people you interact with at work, home and in your community have a tremendous influence over your behavior
• Join a group or develop new circles of friends that are doing the behavior you want to do
