hospital consolidation and community benefit provision in
TRANSCRIPT

New Hampshire Center for Public Policy Studies
HospitalConsolidationandCommunityBenefit
Community Benefit and Market Changes in New Hampshire
July2017

2
Author
SteveNorton
ExecutiveDirector
AboutthispaperOneoftheCenter’sprojectsinrecentyearshasbeentoaddressissuesregardingchangesinthehealthcaresectorinNewHampshire.Thispaperisthelatestinourseriesofreportsonthattopic.ThisreportwasfundedinpartbytheStateofNewHampshireAttorneyGeneral’soffice,butthefindingsandrecommendationsarethoseoftheCenterandnotnecessarilythoseoftheStateofNewHampshireortheAttorneyGeneral’sOffice.
Thispaper,aswithalloftheCenter’spublishedwork,isinthepublicdomainandmaybereproducedwithoutpermission.Indeed,theCenterwelcomesindividuals’andgroups’effortstoexpandthepaper’scirculationandideas,withappropriateattribution.
Writeto:NHCPPS,OneEagleSquare,Suite510,Concord,NH03301

3
Executive Summary NewHampshirehospitalshavefinancialresponsibilityforalmost$5.7billionintotalassetsasof2014,themostrecentyearforwhichcompleteauditedfinancialdataisavailable.Ofthat$5.7billion,almost10%ofthoseassetshavebeenapartofhospitalmergeractivities(Memorial,UpperConnecticutValley,Weeks,Littleton,Androscoggin,AlicePeckDay,LakesRegionandFranklinhospitals).CatholicMedicalCenter,HugginsHospital,andMonadnockHospital(accountingforanother$500millionincommunityassets)andWentworthDouglassHospital($500million)recentlyhadmergerrequestsbeforetheAttorneyGeneral’soffice.[Otherconversations–principallyMaryHitchcockandElliotHospital–representmorethan$2billioninadditionalassetspotentiallyaffectedbymergeractivities.Together,theseaffiliationactivitiesaccountfor2/3rdsoftheassetsofNewHampshire’s24non-profithospitals.
TheCharitableTrustsUnitintheNewHampshireAttorneyGeneral’sofficehasresponsibilityformonitoringtheseaffiliationactivities,andisrequiredtoensurethat:
“Theassetsofthehealthcarecharitabletrustandanyproceedstobereceivedonaccountofthetransactionshallcontinuetobedevotedtocharitablepurposesconsistentwiththecharitableobjectsofthehealthcarecharitabletrustandtheneedsofthecommunitywhichitserves”-Section7:19-b
Tothatend,theAttorneyGeneral’sofficerequestedareviewofexistingdataandinformationonthetypesandlevelofcommunitybenefitcurrentlybeingprovidedinthestate,andbythe4hospitalscurrentlyengagedinmergerdiscussions–WentworthDouglass,CatholicMedicalCenter,MonadnockandHuggins.Inaddition,thisanalysisprovidesinformationonwhattheacademicliteraturesuggeststheimpactofhospitalconsolidationcouldbeoncommunitybenefit.
Major Findings TheNHDepartmentofJusticeandtheInternalRevenueServiceofferarich–ifrelativelyimprecise–bodyofdataoncommunitybenefitthatcouldbeusedtobothincreasethetransparencyofconversationsregardingcommunitybenefitandprovideameansforholdinghospitalsaccountableforboththelevelandtypeofcommunitybenefitprovided.However,hospitalsaregivenwidelatitudeinreportingcommunitybenefit,whichmakescomparisonacrosshospitalsandovertimedifficult.Providingclearerinstructionstohospitalsonreportingrequirementscouldresultindatawhichtheattorneygeneralcouldusetotrackcommunitybenefitacrossmerginghospitals.
Theliteratureregardinghospitalconsolidationsuggestspolicymakersshouldbecautiousaboutclaimsthatmergerswouldautomaticallyincreasevalueinthehealthcaresystem(eitherthroughimprovementsinprice,qualityorboth).Thereisarobust–albeitdated-literaturesuggestingthatreductionsincompetitionandhospitalconsolidationresultinincreasesinprice.
Morerecentresearch,however,suggeststhatnotallmergersarethesameandthatmorerecentmergersmaydifferinkeyrespectstothosethathavehistoricallybeenevaluated.Specifically,thenatureofthemarkets,clinicalservicechanges,andgeographymatterontheimpactonprice.Thisemergingliteraturesuggeststhatmergersinvolvinghospitalsindifferentmarketsandgeographicallyfarfromoneanotherhavenoimpactonprices.Theliteratureontheimpactofconsolidationonqualityandothercommunitybenefitprovisionislessrobust,generallysuggestingnorelationshipbetweenconsolidationandqualityorthelevelofoverallcommunitybenefitprovision.

4
Finally,specifictothemergerscurrentlybeforetheAttorneyGeneral’soffice,theCharitableTrustsUnitwillhaveadifficulttimeassessingtheimpactofmergerswithoutadditionalinformationnotcurrentlyprovided.Asmentioned,theliteratureregardinghospitalconsolidation–andassociatedchangesinmarketcompetition–suggeststhattheclaimsregardingsuchactivities–reductionsinpricesandincreasesinquality,forexample–aresensitivetodefinitionsofmarketsandservicesthatwouldbeaffected.ThesearenotcurrentlydefinedinthedocumentsprovidedtotheAttorneyGeneral’soffice.
Policymakersandboardsofdirectorswillhaveahardtimeunderstandingthepotentialimpactofamergerwithoutadditionalinformationontheactualplansforintegration,includingthedegreeofclinicalintegrationthatmightoccur.TheAttorneyGeneral’soffice,likewise,wouldfinditimpossibletojudge–asitisrequiredtodo–theimpactofmergerswithoutclearerinformationonhowthemergerwillactuallyimpactclinicalservices.
Recommendations Inwhatfollows,weprovideaseriesofrecommendationsfortheAttorneyGeneralandotherpolicymakersinterestedinunderstandingmoreclearlytheimpactofmergeractivityoncommunitybenefitprovisioninNewHampshire.
Community Benefit Provision BoththeNewHampshireAttorneyGeneral’sofficeandtheIRScollectdataontheprovisionofcommunitybenefitbyNewHampshire’shospitals.Littleanalysishasbeenconductedonthisdata,butitisausefulsourceofdatawithwhichtheAttorneyGeneral’sofficeandhospitalboardscouldmonitorchangesincommunitybenefitprovisionovertime.
InouranalysisofdatacollectedbytheAttorneyGeneral’soffice,wefoundsignificantvariationinthelevelofcommunitybenefitbyhospital,andsignificantchangeovertimeinthelevelofcommunitybenefitprovidedbyagivenhospital.Someofthisvariationisduetoinconsistenciesinthewayinwhichthedataisreported.TheseinconsistenciesstemfromthefactthatboththeNHAttorneyGeneral’sofficeandtheIRSgivehospitalsbroadlatitudeinreporting.Theliteratureonhospitalconsolidationandtheprovisionofcommunitybenefitsuggeststhathospitalconsolidationcould,insomeinstances,resultinincreasesincommunitybenefits,andpotentiallyshifthowthosebenefitsareprovided.
Asaresultofthesefindings,werecommend:
• TheAttorneyGeneral’sofficeconveneaworkgrouptodiscussclarifyingthedefinitionofwhatshouldandshouldnotbeincludedasacommunitybenefit,basedonguidancefromtheCatholicHospitalAssociation,whichhasbeenaleaderinthedevelopmentofcommunitybenefitreportingpractices.ThisworkgroupshouldalsodiscusswhetherthestateshouldcontinuerequiringhospitalstoreportcommunitybenefitsbothtotheAttorneyGeneral’sofficeandtotheIRS.
• ThestateandhospitalsshouldIncreasethetransparencyofdataontheprovisionofcommunitybenefitandchangesovertime.Suchaneffortcouldtakemanydifferentforms.Hospitalscould,aspartoftheircommunitybenefitplanefforts,provideananalysisofchangesinthelevelandtypeofcommunitybenefitovertime.Similarly,thelegislaturecouldrequiretheAttorneyGeneral’sofficetoprepareanannualreportoncommunitybenefitprovision.

5
Changes in Prices and Quality Associated with Consolidation Thebodyofliteraturethathasemergedoverthelast20yearslargelysuggeststhathospitalconsolidationneitherlowerscostsnorconsistentlyimprovesthequalityofthecareprovided.However,thereareimportantqualificationstothesefindings.
Withrespecttoprices,itisonlyrecentlythattheliteraturehasbeguntoexplorethepossibilitythatthetypeofconsolidation–whetherthetwoorganizationsarecompetitorsforcertainservicescomparedtonon-competitors–andthelevelofadministrativeandthereforeclinicalintegration–materiallyimpactsthedegreetowhichconsolidationcouldimpactprices.Themostrecentanalysis(Dafny,2015)confirmedthatashospitalcompetitiondeclines,pricesrise.However,italsosuggestedthatthemergersofhospitalsthataremoredistant–andpotentiallynotcompetingforthesamepatientsorservices–hadlittleimpactonprices.
Withrespecttoqualityofcare,theliteratureisweakerstill.Nationalstudies–withthebestcontrolsandmostgeneralizableresults–havelookedataverynarrowsetofservices(principallyforacutemyocardialinfarction),andnonehavelookedatgeographyanddifferenttypesofservicecompetition(forexample,forprimary,tertiaryorquaternaryservices).
Beyondthesegeneralizations,however,theabilitytounderstandhowtheproposedaffiliationswouldimpactpriceandqualityisextremelylimitedasaresultofthefactthattheaffiliationdocumentsprovidedtotheAttorneyGeneral’sofficedescribegovernancechangesassociatedwiththemergers,butdonotprovideanydetailontheintegrationplanforservices.
Asaresultofthesefindings,werecommend:
• Hospitalboardsengagedinmergeractivitiescoulddevelopqualityandcostmonitoringplansthatlinkqualityandcostwithspecificclinicalservices,identifiedasimportantinthedevelopmentoftheirintegrationplans.Thesecouldalsobecomepartofthecommunitybenefitplancommunicationeffortswiththelocalcommunity.
TheNHAttorneyGeneral’sofficecouldsimilarlymonitorchangesinpricesandquality,usingstandardnationalqualitymeasures,suchasreadmissionratesinthecaseofquality,andwithpricedatafromtheNewHampshireComprehensiveHealthInformationDatabase,whichhasbeenusedbytheNewHampshireDepartmentofInsurance.

6
Part 1 - Measuring Community Benefit
TheNewHampshireAttorneyGeneral’sofficehasledthenationindevelopingacommunitybenefitsreportingprocessthatrequireshealthcarecharitabletruststoassesstheircommunity’sneeds,andquantitativelydocumenthowthecharitabletrustisfocusingresourcesonthoseproblems.Eachyear,NewHampshire’shealthcarecharitabletrustsmustprovidetheAttorneyGeneralwithareportontheircommunitybenefitactivities.
WiththepassageoftheAffordableCareAct,thefederalgovernmentfollowedsuit.TheACAaddedSection501(r),whichrequirednon-profithospitalstomeetanewsetofobligationsregardingcommunitybenefitstoqualifyfortax-exemptstatusundersection501(c)(3).TheserequirementsweresimilartothosedevelopedbyNewHampshire.Non-profithospitalswererequiredto:
• Conductacommunityhealthneedsassessmentandprovideanimplementationplan• Documentwrittenfinancialassistancepolicyforfreecaretothemedicallyindigent• ReportontheresourcesdevotedtovariouscommunitybenefitactivitiesontheIRS990,
underscheduleH
RelativetoNewHampshire’sreportingefforts,theACAwasnarrowerinthesensethattheactrelatedsolelytonon-profithospitals,whereasNewHampshire’slawrelatestoallhealthcarecharitabletrusts.Inaddition,thedatacollectedundertheIRSForm990ScheduleHformislessdetailedthanNewHampshire’scollectioneffort.Forthepurposeofthisanalysis,wehavefocusedouranalysisonthedatacollectedbytheNewHampshireAttorneyGeneral’soffice.1
NH’sCommunityBenefitReportingandDataAsaresultofincreasingscrutinyregardingthecostsoftaxexemptionsforhealthcarecharitabletrustsandthepotentialbenefitstheyprovide,statesacrossthecountrybegandevelopinglegislationtotrackandassesscommunitybenefitsinthelate1990sandearly2000s.NewHampshireledthecountryindevelopinglawswhichrequiredhealthcarecharitabletrusts2inNewHampshiretoreportonthebenefitsprovidedtothecommunitytheyserve.
TheNewHampshireLegislaturepassedSB69-knownasNH’scommunitybenefitsstatute-in1999.EffectiveJanuary1,2000,thebillrequiredthatnon-profithospitalsinNewHampshiredevelopacommunitybenefitsplan,areportonthecommunitybenefitactivitiesundertakenbythehospital,andinformationdescribingtheresultsofthesecommunityinvestments.TheCharitableTrustsUnitissueditsfirstcommunitybenefitsreportingforminSeptemberof2001.
1We reviewed a sample of hospitals’ community benefit reporting in both the Schedule H from the IRS form 990 and the NH Attorney General’s community benefit forms. They were similar in most instances, with differences attributable to slight differences in the reporting requirements. We chose to use the NH DOJ data as it was more readily available for recent years. As we note, a more detailed analysis should be conducted to decide whether reporting of the state specific data is necessary, given the IRS 990 requirements. 2 "Health care charitable trust'' means a charitable trust organized to directly provide health care services, including, but not limited to, hospitals, nursing homes, community health services, and medical-surgical or other diagnostic or therapeutic facilities or services.
7
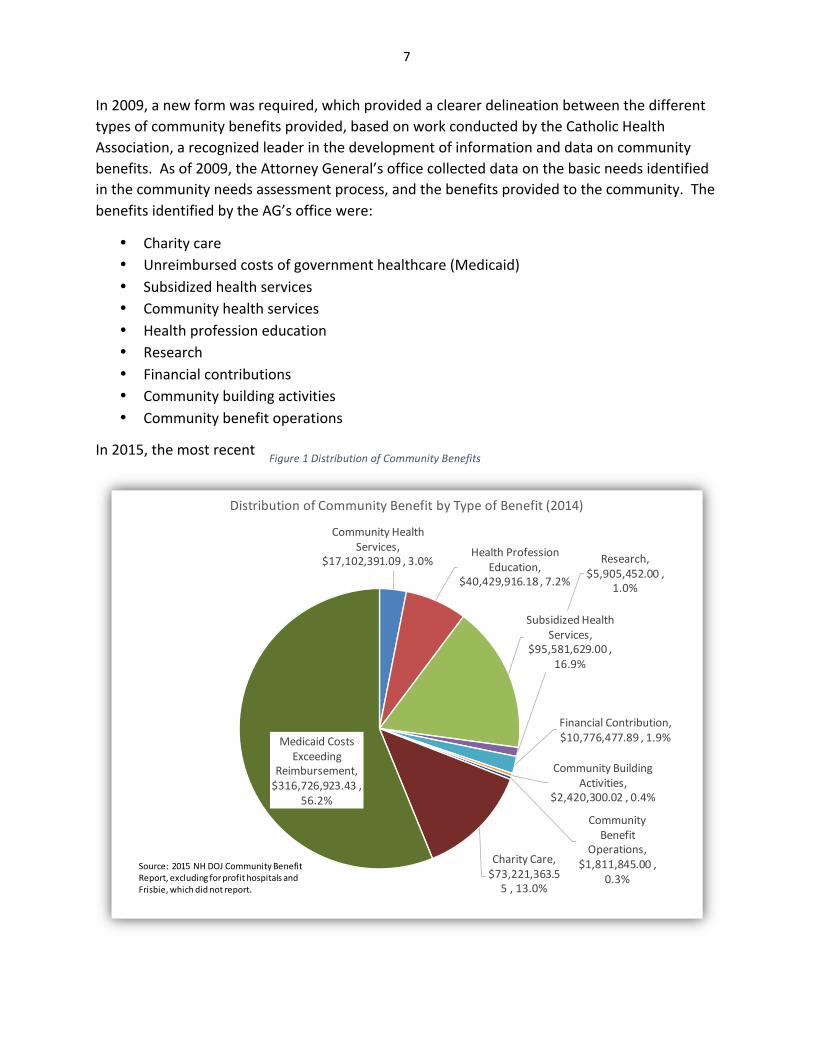
Figure1DistributionofCommunityBenefits
CommunityHealthServices,
$17,102,391.09,3.0%HealthProfession
Education,$40,429,916.18,7.2%
SubsidizedHealthServices,
$95,581,629.00,16.9%
Research,$5,905,452.00,
1.0%
FinancialContribution,$10,776,477.89,1.9%
CommunityBuildingActivities,
$2,420,300.02,0.4%
CommunityBenefit
Operations,$1,811,845.00,
0.3%
CharityCare,$73,221,363.55,13.0%
MedicaidCostsExceeding
Reimbursement,$316,726,923.43,
56.2%
DistributionofCommunityBenefitbyTypeofBenefit(2014)
Source:2015NH DOJCommunityBenefitReport,excludingforprofithospitalsandFrisbie,whichdidnotreport.
In2009,anewformwasrequired,whichprovidedaclearerdelineationbetweenthedifferenttypesofcommunitybenefitsprovided,basedonworkconductedbytheCatholicHealthAssociation,arecognizedleaderinthedevelopmentofinformationanddataoncommunitybenefits.Asof2009,theAttorneyGeneral’sofficecollecteddataonthebasicneedsidentifiedinthecommunityneedsassessmentprocess,andthebenefitsprovidedtothecommunity.ThebenefitsidentifiedbytheAG’sofficewere:
• Charitycare• Unreimbursedcostsofgovernmenthealthcare(Medicaid)• Subsidizedhealthservices• Communityhealthservices• Healthprofessioneducation• Research• Financialcontributions• Communitybuildingactivities• Communitybenefitoperations
In2015,themostrecent

8
yearforwhichcompletedataisavailable,NewHampshirecharitabletrustsprovidedalmost$564millionincommunitybenefit,accordingtoreportsfiledwiththeAttorneyGeneral’sCharitableTrustsUnit.Ofthattotalamount,56%resultedfromthefactthatMedicaidpayslessthantheexpensesassociatedwithprovidingservicestoMedicaidclients.Thesecondlargestshareresultedfromtheprovisionofsubsidizedhealthcareservices(17%).CharitableCare(at13%ofthetotal)cameinadistantthird.
Accordingtothesesamereports,theaveragehealthcarecharitabletrustprovidedalmost$22millionincommunitybenefit.MaryHitchcockprovidedover$180millionincommunitybenefit,withElliotandConcordhospitalprovidingmorethan$60million.Notsurprisingly,thelargerhospitalsaccountedforthelion’sshareofthecommunitybenefitprovided.
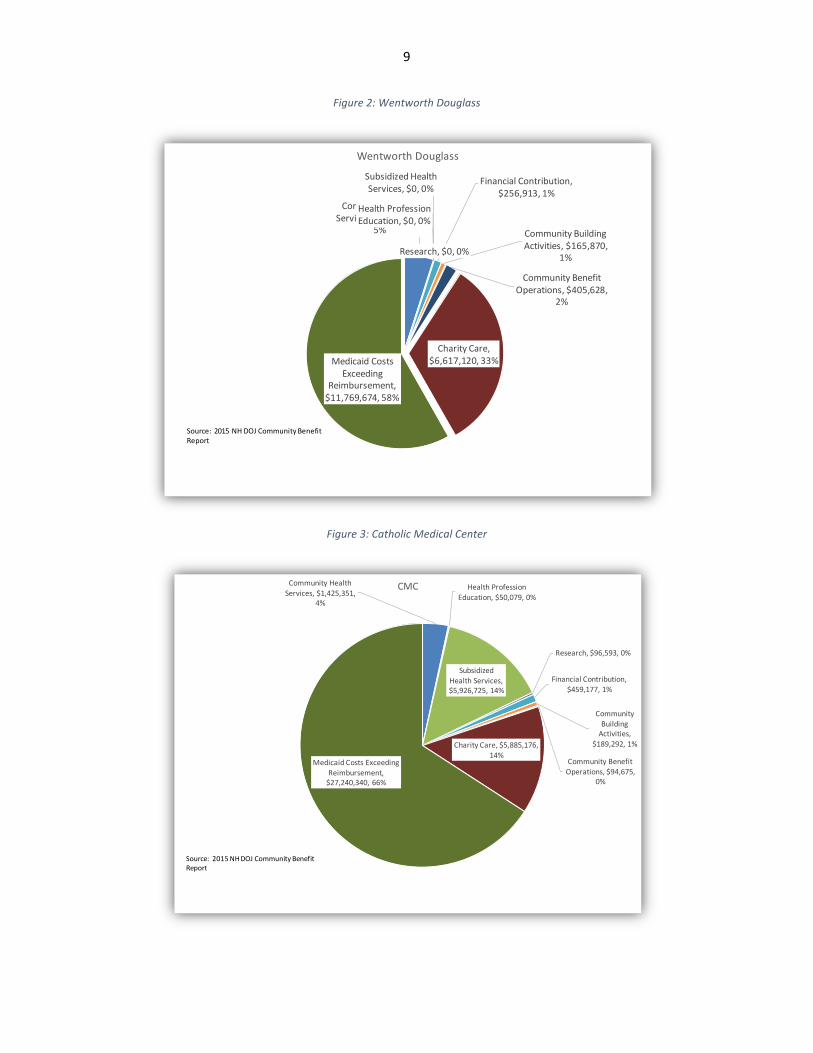
ThefiguresbelowincludedataforeachofthefourNHbasednon-profithospitalsthathavesoughtattorneygeneralapprovalformergeractivities.Whatisnotableaboutthisdataisthesignificantvariationinthedistributionofcommunitybenefitbytypebyhospital.Relativetotheotherhospitals,forexample,HugginsHospitalprovidedadisproportionateshareofitscommunitybenefitassubsidizedhealthservices.AreviewoftheunderlyingdatasuggeststhatHuggins3includedsubsidiesfortheirprimarycareservicesintheircommunitybenefitaccounting,somethingwhichonlyafewotherhospitalsdid,andwhichcouldarguablybeassumedtobeanormalcostofdoingbusiness.
3http://doj.nh.gov/charitable-trusts/community-benefits/documents/2015-huggins-hospital.pdf . This and all other data collected is available on the attorney general’s office website back to 2012.
9
Figure2:WentworthDouglass
Figure3:CatholicMedicalCenter
CommunityHealthServices,$1,005,764,
5%
HealthProfessionEducation,$0,0%
SubsidizedHealthServices,$0,0%
Research,$0,0%
FinancialContribution,$256,913,1%
CommunityBuildingActivities,$165,870,
1%
CommunityBenefitOperations,$405,628,
2%
CharityCare,$6,617,120,33%MedicaidCosts
ExceedingReimbursement,$11,769,674,58%
WentworthDouglass
Source:2015NH DOJCommunityBenefitReport
CommunityHealthServices,$1,425,351,
4%
HealthProfessionEducation,$50,079,0%
SubsidizedHealthServices,$5,926,725,14%
Research,$96,593,0%
FinancialContribution,$459,177,1%
CommunityBuildingActivities,
$189,292,1%
CommunityBenefitOperations,$94,675,
0%
CharityCare,$5,885,176,14%
MedicaidCostsExceedingReimbursement,$27,240,340,66%
CMC
Source:2015NHDOJCommunityBenefitReport

10
Figure4:Huggins
Figure5:Monadnock
CommunityHealthServices,$260,885,
4%HealthProfession
Education,$181,659,2%
SubsidizedHealthServices,$4,875,230,
66%
FinancialContribution,$50,716,1%
CommunityBuildingActivities,
$92,792,1%
CommunityBenefitOperations,$3,200,
0%CharityCare,
$1,057,000,14%
MedicaidCostsExceeding
Reimbursement,$876,644,12%
Huggins
CommunityHealthServices,$815,547,
18.05%Health
ProfessionEducation,
$5,821,0.13%
SubsidizedHealthServices,$533,208,
11.80%
FinancialContribution,$157,940,3.50%
CharityCare,$1,238,335,27.41%
MedicaidCostsExceeding
Reimbursement,$1,767,178,39.11%
Monadnock

11
Theoveralllevelofcommunitybenefiteffortvariedconsiderablyaswell,asshowninFigure6whichprovidesinformationshowingcommunitybenefitrelativetothesizeoftheorganization,asmeasuredbyoperatingexpenses.LakesRegionHospitalandUpperConnecticutValleyHospitalprovidedcommunitybenefitthatwasapproximately20%ofoperatingexpenses,comparedtoSpeareMemorial,St.JosephHospitalandMemorialHospital,eachofwhichprovidedcommunitybenefitsatmuchlowerlevels(lessthan5%).
Figure6:LevelofEffort:CommunityBenefitasashareofOperatingExpenses
Unreimbursed Medicaid Expenses
Asnoted,unreimbursedMedicaidexpensesaccountforthesinglelargestshareofcommunitybenefitactivities,rangingfrom.1%ofexpensesin2015toalmost10%,asshowninFigure 7.NewHampshirepaysforbasepaymentratesthroughmanagedcarearrangementsforservicesprovidedtoMedicaidbeneficiaries.Thesepaymentsaregenerallymuchlowerthantheexpensesassociatedwithprovidingthatcare.Inaddition,paymentpoliciesintheMedicaidprogramhavegenerallyrecognizedthedifficultfinancialpositionofmanyruralhospitals.
8.7%
13.9%
13.2%12.5%
16.6%
7.3%
15.7%
7.5%
13.9%
20.4%
6.2%
14.0%
3.1%
6.1%
15.3%
9.7%
4.7%3.8%
19.9%
11.6%11.4%
7.0%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
CommunityBenefit(IncludingMedicaidShortfall)asShareofOperatingExpensein2014
StateAverage=12.1%

12
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
UnreimbursedMedicaidExpenseas%ofOperatingExpense
Thosesmallruralhospitals–designatedcriticalaccesshospitals–incertaininstancesreceivedenhancedrates.4
Inaddition,NewHampshiremakessupplementalpaymentstohospitalstooffsetbothcharitycareandunreimbursedexpensesassociatedwithMedicaid.Nationally,allsupplementalMedicaidpaymentscombinedamountedto44percentofMedicaidfee-for-servicepaymentstohospitalsin2014.5ThesepaymentssignificantlyreducebothcharitycareandunreimbursedMedicaidexpenses.Similartothebasepayment,hospitalsreceivingcriticalaccessdesignationaretreateddifferently,withtheUncompensatedCareandMedicaidFundoffsettingupto75%ofthehospital’scharitycareandunreimbursedMedicaidexpenses,comparedto50%forallotherhospitals,aresultoflegislationpassedin2014.
4This includes Alice Peck Day, Androscoggin, Cottage, Franklin Regional, Huggins, Littleton, Memorial, Monadnock, New London, Speare, Upper Connecticut Valley, Valley Regional, and Weeks.] 5 https://www.macpac.gov/wp-content/uploads/2015/11/EXHIBIT-23.-Medicaid-Supplemental-Payments-to-Hospital-Providers-by-State-FY-2014-millions.pdf
Figure7:CommunityBenefitandMedicaid
13
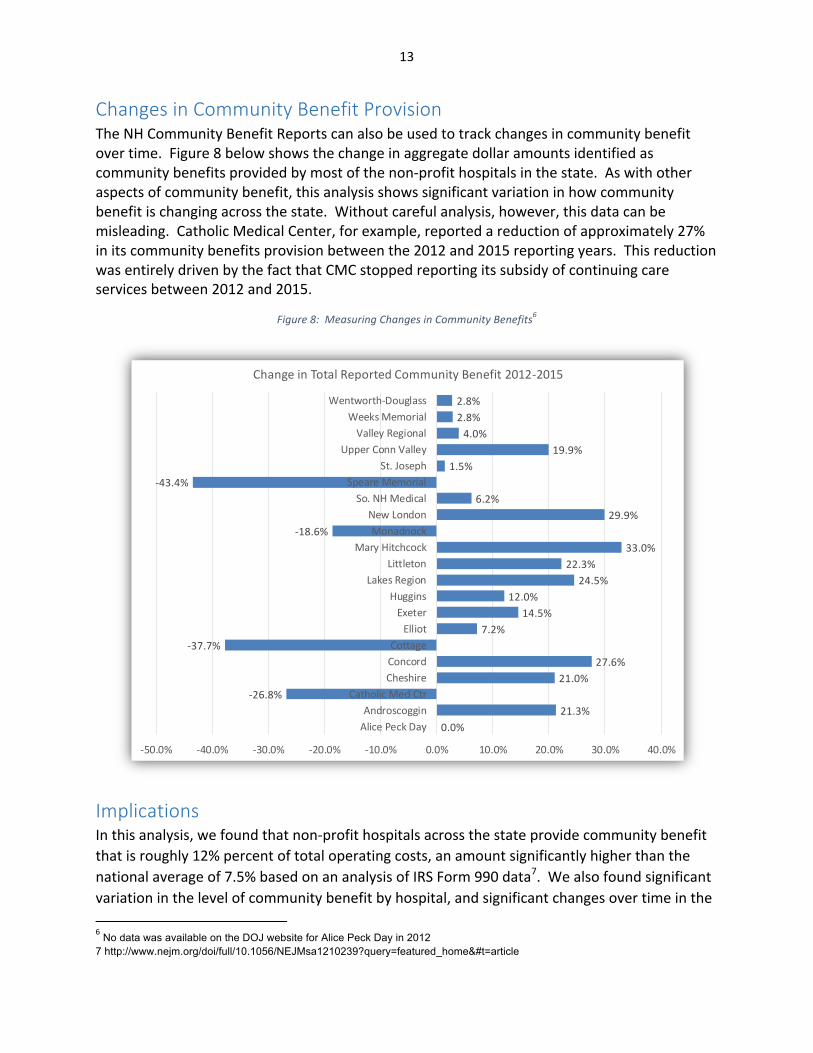
Changes in Community Benefit Provision TheNHCommunityBenefitReportscanalsobeusedtotrackchangesincommunitybenefitovertime.Figure8belowshowsthechangeinaggregatedollaramountsidentifiedascommunitybenefitsprovidedbymostofthenon-profithospitalsinthestate.Aswithotheraspectsofcommunitybenefit,thisanalysisshowssignificantvariationinhowcommunitybenefitischangingacrossthestate.Withoutcarefulanalysis,however,thisdatacanbemisleading.CatholicMedicalCenter,forexample,reportedareductionofapproximately27%initscommunitybenefitsprovisionbetweenthe2012and2015reportingyears.ThisreductionwasentirelydrivenbythefactthatCMCstoppedreportingitssubsidyofcontinuingcareservicesbetween2012and2015.
Figure8:MeasuringChangesinCommunityBenefits6
Implications Inthisanalysis,wefoundthatnon-profithospitalsacrossthestateprovidecommunitybenefitthatisroughly12%percentoftotaloperatingcosts,anamountsignificantlyhigherthanthenationalaverageof7.5%basedonananalysisofIRSForm990data7.Wealsofoundsignificantvariationinthelevelofcommunitybenefitbyhospital,andsignificantchangesovertimeinthe6No data was available on the DOJ website for Alice Peck Day in 2012 7 http://www.nejm.org/doi/full/10.1056/NEJMsa1210239?query=featured_home&#t=article
0.0%21.3%
-26.8%21.0%
27.6%-37.7%
7.2%14.5%
12.0%24.5%
22.3%33.0%
-18.6%29.9%
6.2%-43.4%
1.5%19.9%
4.0%2.8%2.8%
-50.0% -40.0% -30.0% -20.0% -10.0% 0.0% 10.0% 20.0% 30.0% 40.0%
AlicePeckDayAndroscoggin
CatholicMedCtrCheshireConcordCottage
ElliotExeter
HugginsLakesRegion
LittletonMaryHitchcock
MonadnockNewLondon
So.NHMedicalSpeareMemorial
St.JosephUpperConnValley
ValleyRegionalWeeksMemorial
Wentworth-Douglass
ChangeinTotalReportedCommunityBenefit2012-2015
14
levelofcommunitybenefitprovidedbyagivenhospital.Someofthisvariationislikelyduetoinconsistenciesinthewayinwhichthedataisreported.TheseinconsistenciesstemfromthefactthatboththeNHAttorneyGeneral’sofficeandtheIRSgivehospitalsbroadlatitudeinreporting.
Forpolicymakersinterestedinunderstandingthecommunitybenefitenvironment,thisdatawouldprovideagoodbenchmarkagainstwhichchangesgoingforwardcouldbeassessed.Thestateandhospitalboardscouldusethisdatatoincreasethetransparencyofconversationsaboutcommunitybenefitprovision,astheyhavedonewithconversationsabouthealthcarecosts.Thiscouldtakedifferentforms.Hospitalscould,aspartoftheirlocalcommunitybenefitplanefforts,provideananalysisofchangesinthelevelof,andtypeofcommunitybenefitovertime.Alternatively,thelegislaturecouldrequiretheAttorneyGeneral’sofficetoprepareanannualreportoncommunitybenefitprovision.
Tousethistooleffectively,however,wouldrequireadditionalstepstoensuretheaccuracyofthedata.First,amoreindepthanalysisoftheNewHampshireCommunityBenefitdatashouldbeconducted,whichincludesamoreindepthanalysisofthedataanddiscussionswithhospitalsregardingthedefinitionandcalculationofthequantitativemeasuresofcommunitybenefit.
Thevariationinwhatisincluded(ornot)ascommunitybenefitbyhospitalssuggeststhatmoreclarityislikelyneededindefiningwhatisandwhatisnotcommunitybenefit.TheCenterrequesteddatafromeachofthehospitalsrecentlyinvolvedinmergerdiscussionswiththeAttorneyGeneral’sofficeontwoareasthatsignificantlyimpacttheoverallestimatesoftheprovisionofcommunitybenefit.
First,weaskedhospitalswhethertheMedicaidlosswasnetofanyexpenses(associatedwiththeMedicaidEnhancementTax)andrevenues(intheformofpaymentsbythestateforahighshareofcostsassociatedwithMedicaidanduncompensatedcare)associatedwiththestate’sdisproportionateshareprogram.Thehospitalsvariedconsiderablyinhowtheyreportedthisinformationonthecommunitybenefitforms.
Second,werequesteddataonthedegreetowhichhospitalsincludedthesubsidizationofphysicianpractices.Arguably,ahospital’sdecisiontopurchaseaphysicianpracticeisabusinessdecisionandshouldthereforenotimmediatelybeconsideredacommunitybenefitunlessitisidentifiedspecificallyinthehospital’scommunitybenefitplanorlinkedwithsomespecialneedwithinthecommunity.Heretoo,therewassignificantvariationinwhatwasincluded,andtherationaleforitsinclusion.
AnydecisionabouthowtoproceedwiththisdatashouldalsoincludeafullcomparisonoftheresultsrelativetodatacollectedbytheIRS.Fromthisanalysis,hospitals,theAttorneyGeneral,andlegislatorscouldclarifyandtightenthedefinitionofwhatisincludedasacommunitybenefitornottoensurecomparabilityovertime(andalsoacrosshospitals),anddiscuss

15
whetherornotthestateshouldcontinuecollectingdatafromthecharitabletrustsinNewHampshire,ordefertothecollectionofdatafromtheIRS.
Part 2 - Hospital Consolidation’s Impact on Community Benefits IntheCenter’sreviewofaffiliationdocuments,it’sclearthatinadditionto‘communitybenefit’asdefinedbytheNHDepartmentofJusticeaswellastheIRSintheirinstructions,thehospitalsthemselvesidentifythetripleaimofloweringcosts,improvingpublichealthandimprovingquality.Thetheorybehindtheseclaimsisthatconsolidationwillhelpimprovecoordinationofcare(viascaleorbyallowingforinvestmentininformationtechnologysystemsandotherprocessimprovementefforts).Consolidationcouldalsoeliminateduplication.Finally,bothhospitalsthemselvesandtheAffordableCareActhavemadetheargumentthatsuchconsolidationwillhelpcreatescalesufficienttoimprovepublichealth.
Inwhatfollows,wereviewtheliteratureontheimplicationofhospitalmergersoncommunitybenefit,pricesandquality.Inthisanalysis,wereviewliteratureforthelast20years,whichlooksatthelargeincreaseinmergersandacquisitionsinthelate1990sandmorerecentlyinearlytothemid2010s.
Figure9:HospitalMergersandAcquisitions,1998-20148
8American Hospital Association, Trendwatch Chartbook 2015, Chart 2.9

16
Charity Care
Severalarticleswerepublishedregardingtherelationshipbetweentheprovisionofcharitycareandthelevelofcompetitioninthe1990sandearly2000s.TheseincludedFrankandSalkever(1991),Gruber(1994),Mannetal.(1995),Mannetal.(1997)andGarmin(2006).Thesestudiesinvariouswaysassessedthehypothesisthatincreasedcompetitionwouldinhibitaprovider’sabilitytooffercharitycare.Underthistheory,hospitalconsolidationcould,becauseoftheresultantreductionincompetition,resultinanincreaseinuncompensatedcareprovision.
Theresultsoftheliteraturearemixed,butgenerallysuggestthatreductionsincompetitioncouldleadtoincreasesincharitycareprovision,allotherfactorsbeingequal.Gruber(1994)andMannetal.(1995)foundthatwhenfacedwithsystem-widechangesinreimbursementsystems,hospitalsdecreasedtheircharitycarefasterinrelativelycompetitivemarketsthaninrelativelyuncompetitivemarkets.CuellarandGertler(2005)9andGarmin(2006)foundsimilarresults.However,noneofthesestudiesdirectlymeasuredtherelationshipbetweenhospitalconsolidationandcharitycareprovision.
Community Benefit Broadly Defined
Whilepolicymakersweregenerallyconcernedwiththeprovisionofcharitycare,overthecourseofthe2000s,states-andultimatelytheIRS-expandedthedefinitionofcommunitybenefittoincludeawholeseriesofcommunitybasedactivities,asdescribedelsewhere.This,alongwiththedataavailableasaresultoftheIRS’implementationofscheduleH,hasresultedinalimitednumberofstudiesassessingtheseothercommunitybenefitofferings.
Mostrecently,a2013articleintheNewEnglandJournalofMedicineusedscheduleHdatatodescribenon-profits’provisionofcharitablecare.Thatstudyfoundthathospitalsexpended7.5%oftheiroperatingexpensesforcommunitybenefitservices.Approximatelyhalfoftheseexpenditureswenttosubsidizingthecostofcareforpatientscoveredbymeans-testedprograms,primarilyMedicaid.10
Inadditiontodescribingthecharacteristicsoftheprovisionofcharitablecare,Younget.al.(2013)conductedregressionanalysestoassesstheimpactofvariousmarketcharacteristicsontheprovisionofcommunitybenefit.Forthisanalysis,theyanalyzeddirectpatientcareandcommunityservice.Theauthorsweretestingthehypothesisthatinstitutionalcharacteristics(solecommunityproviderstatus,amongothers)andmarketcharacteristics(includingmarketcompetition)wouldimpactthelevelsofcommunitybenefitprovision.
99How The Expansion Of Hospital Systems Has Affected Consumers Alison Evans Cuellar and Paul J. Gertler C 10 Gary J. Young, J.D., Ph.D., Chia-Hung Chou, Ph.D., Jeffrey Alexander, Ph.D., Shoou-Yih Daniel Lee, Ph.D., and Eli Raver N Engl J Med 2013; 368:1519-1527April 18, 2013
17
Forthemodelassessingdirectpatientcare,hospitalcommunitybenefitexpenditureswerepositivelyassociatedwithonlythestate-levelrequirementsforreportingcommunitybenefits.Thisresultsuggeststhatstateaccountabilitysystemsencouragetheprovisionofcommunitybenefits(andthatperhapsattorneysgeneralshouldincreasetheirreviewofthisimportanttrust).Forthemodelassessingcommunity-service,hospitalexpenditureswerepositivelyassociatedwithtwoinstitutional-levelcharacteristics—teachingstatusandsolecommunityproviderdesignation—andalsowithstate-levelreportingrequirementsforcommunitybenefits.Theresultsforteachingstatusarenotsurprisinggiventhefactthathealtheducationservicesareconsideredacommunitybenefit.Inbothmodels,theanalysisfoundnostatisticalrelationshipbetweenmarketcompetitionandthelevelofcommunitybenefit.
Public Health Improvement
Again,takingadvantageofdataavailablebecauseofstateandfederaleffortstomoreclearlydefinecommunitybenefits,avarietyofstudieshavesuggestedthatdeclinesincompetitioncouldlowertheprovisionofhealthimprovementactivitiesbecausehospitalsusetheseservicesasmarketingtools.C.Ginn,ShenandMoseley(2006),forexample,reviewedtheeffectofcommunitybenefitlaws,typeofownership,andcompetitiononhospital-basedhealthpromotionservices.Theyconcludedthatthehigherthelevelofcompetition–asmeasuredbytheHHI–themoresignificanttheprovisionofhospital-basedhealthpromotionservices,suggestingthathospitalsprovidetheseservicesatleastinpartforcompetitivereasons.D.GinnandMoseley(2009),andMoseley,Shen,andGinn(2010),E.Proenca,Rosko,andZinn(2000;2003)allsuggestthattheintensityofcompetitionissignificantlyandpositivelyassociatedwiththeprovisionofhospital-basedhealthpromotionservices.
Systems Vs. Mergers and Hospital Operating Expenses Intheory,hospitalmergerscanresultinefficienciesthroughtheeliminationofduplicativeactivities,includingtheintegrationofclinicalactivities.DranoveandLindrooth(2003)11attemptedtoassessthedegreeofintegrationthatoccursbydifferentiatingbetweensystemacquisitionsandmergers.Intheirdefinition,hospitalmergersinvolvethecombinationofseparatelicensesintoasinglefacilitylicense,withthehospitalsreportingasinglesetoffinancialandutilizationstatisticsandregulatedasasingleentity.Theoretically,theauthorsargue,amergerwouldallowformoreclinicalintegration,andtheauthorsconductapre-postanalysisofsystemconsolidationsandmergers,totestthehypothesisthatsuchintegrationlowersoperatingexpenses.
11Journal of Health Economics 22 (2003) 983–997

18
Theauthors’resultssuggestthatthegreatertheclinicalintegration,themorelikelyitisthattherewillbeoperatingexpensereductions.Theiranalysisofsystemconsolidations(comparingthosethatconsolidatedtothosethatdidn’t)showedaninsignificantimpactonoperatingexpenses.Theirre-analysisofsystemmergers,ontheotherhand,suggestedthatcontrollingforotherfactors,hospitalmergersresultedinareductionin14%ofoperatingexpensesandthatimpactremainedsignificantforfouryearspostthemerger.
PriceTheearlyliteratureonconsolidationthatoccurredinthe1990siswellsummarizedbyVogtandBrown(2006).Theyconductedameta-analysisofstudieslookingatvariousmethodsforunderstandingtheimpactofconsolidationonprices.Theresultsoftheirmeta-analysisledthemtotheconclusionthatthehospitalconsolidationinthe1990sraisedpricesbyatleastfivepercent,andlikelybysignificantlymore.
Thesinglelargestgroupofliteratureconductedwhattheauthorscallstructure-conduct-performanceanalysis,whichdonotanalyzeactualmergers,butlooksattheimpactofchangesinmarketstructure–usuallycompetitionasmeasuredbytheHerfindahlindex–anditsimpactonprices.Thefigurebelowshowstheauthors’selectionsofstudiesthatwerethemethodologicallymostsound12anddocumentsthevariationintheresults,allofwhichsuggestdeclinesinmarketcompetitionresultinincreasesinprices.
12Based on the definition of the market, controls for other factors which could impact prices, and the measure of price.

19
Figure10:Summaryofstructure-conduct-performanceliterature
Inthisanalysis,astheauthorsnote,therelationshipbetweenmarketcompetitionandpricesisusedtocalculatethelistedmergereffect,whichistheeffectonpricepredictedbythestudyfortheconsolidationfromfiveequallysizedhospitalstofourhospitalsinthemarket.Theimpactrangesfromaslightreductiontoa17%increase.
Recentanalyseshavebecomemoresophisticatedandrefinedintheirapproachtobothmarketdefinitionandmeasuresofprice.Thesestudiesgenerallyconfirmthefindingsofpreviousauthors.AkosaAntwietal.(2009),Dranoveet.al.,MelnickandKeeler(2007),andWU(2008)allindicatedthatincreasesinmarketpowerresultedinincreasesinprice.Cooperet.al.(2015)13analyzedclaimsdatabetween2007and2011tolookatavarietyoffactors,includingtheimpactofmarketpoweronprices.Theauthorsfoundthatevenaftercontrollingfordemandandforothercostmeasures,hospitalpricesinmonopolymarketswere15%percenthigherthanthosemarketswithfourormorehospitals.
Thereviewofstudiesofactualmergersislessrobust,butstillsuggeststhathospitalconsolidationcouldresultinpriceincreases,butmarketstructureandcompetitionforspecificservicesplayakeyrole.Onestudy(Dafny,2005)–whichlookedatmerginghospitalswithin3
13Zack Cooper, Stuart Craig, Martin Gaynor, John Van Reened. The Price Ain’t Right? Hospital Prices and Health Spending on the Privately Insured. December, 2015.

20
milesofeachother–showeda40percentincreaseinpricesoverthelongrun.14Ontheotherhand,Connor(1997),andConnorandFeldman(1998)foundthatpricesrosemoreslowlyinmergerthaninnon-mergermarkets,exceptinthoseareaswheremarketcompetitionwaslowalready.Theauthorsarguethattheirmarketdefinitionwasoverlybroad(amongotherconcerns)buthighlightthefactthatmarket(andpotentiallyproduct)definitionisveryimportanttounderstandingthepriceimpactsofhospitalconsolidation.
Whilemoststudieshavelookedathorizontalmergersinthesamegeographicarea,Dafnyet.al.(2016)15tooktheliteratureastepfurtherandlookedatboththosehospitalsthatmergedwithinthesamestate,andthosethatmergedacrossstatelines.Similartoworkpreviouslyconducted,Dafny(2005)foundthathospitalsgainingmemberswithinastatesawpriceincreasesof6-10percent,whilehospitalsgainingsystemmembersout-of-stateexhibitnostatisticallysignificantchangesinprice.
Quality of Care Thereislittleevidencetosuggestthatqualityimproveswithincreasinghospitalconcentration.KesslerandMcClellan(2000),Mukameletal.(2002),Shen(2003),andKesslerandGeppert(2005)allusedMedicaredatatoassessvariousmeasuresofmortality,principallywithafocusonacutemyocardialinfarction.Thesestudiesfoundthattherewaseithernoimpact,oraslightdecreaseinthequalityofcareasmeasuredbyAMImortalityassociatedwithincreasinghospitalconcentration.MorerecentstudiesoftheNationalHealthServiceshowsimilarresults(Cooperetal.2011,Gaynoretal,2010,Bloometal.2010).
StudiesonthefullpopulationoftheU.S.showsimilarresults(Mukameletal.2001;GowrisankaranandTown,2003;Volpetal.,2005).Cuellaretal.(2003)lookatmorebroadmeasuresofqualityofcare,includingratesofreadmission,adversepatientsafetyevents,andmortality,andfoundweakresults,withonlyonemeasure–ratesofoverusedprocedures–decliningassociatedwithincreasingmarketconcentration.
14Dafny L. Estimation and Identification of Merger Effects: an Application to Hospital Mergers. 2005, Mimeo, Northwestern University.15Leemore Dafny, Kate Ho, Robin Lee. The Price Effects of Cross-Market Hospital Mergers.” March, 2016.

21
Bibliography
HospitalConsolidationandHealthcareMarketsCuellar,AlisonEvansandPaulJ.Gertler.“TrendsInHospitalConsolidation:TheFormationOfLocalSystems.HealthAffairs22,no.6,2003Dafny,LeemoreS.2014.“HospitalIndustryConsolidation-StillMoretoCome?"NewEnglandJournalofMedicine,370,2014Ramirez,Edith.2014.“AntitrustEnforcementinHealthCare-ControllingCosts,ImprovingQuality."NewEnglandJournalofMedicine,(374)KilaruAS,WiebeDJ,KarpDN,LoveJ,KallanMJ,CarrBG.“Dohospitalserviceareasandhospitalreferralregionsdefinediscretehealthcarepopulations?”
MedicalCare,53(6),2015.
GeneralLiteratureonCommunityBenefitBarnett,K.,&Somerville,M.HospitalcommunitybenefitaftertheACA:ScheduleHandhospitalcommunitybenefit–Opportunitiesandchallengesforthestates(IssueBrief).Baltimore,MD:TheHilltopInstitute,UMBC,2012Bazzoli,GloriaJ.,JanP.Clement,andHui-MenHsieh,“CommunityBenefitActivitiesofPrivate,NonprofitHospitals,”JournalofHealth,Politics,andLaw,35(6),2010.
Corrigan,Janet,ElliottFisher,andScottHeiser,“HospitalCommunityBenefitPrograms:IncreasingBenefitstoCommunities,”JournaloftheAmericanMedicalAssociation313,no.12,2015
Ferdinand,AlvaO.,PatienJosueEpane,andNirMenachemi,"CommunityBenefitsProvidedbyReligious,OtherNonprofit,andFor-ProfitHospitals:ALongitudinalAnalysis,"HealthCareManagementReview;2013.GarmonChristopher.“HospitalCompetitionandCharityCare.”FTCBureauofEconomicsWorkingPaperNo.285,2006
Ginn,GregoryO.,JayJ.Shen,andCharlesB.Moseley,"TheImpactofStateCommunityBenefitLawsontheCommunityHealthOrientationandHealthPromotionServicesofHospitals,"JournalofHealthPolitics,PolicyandLaw,Volume31,Number2,2006

22
Ginn,GregoryO.andCharlesB.Moseley,"CommunityBenefitLaws,HospitalOwnership,CommunityOrientationActivities,andHealthPromotionServices,"HealthCareManagementReview,34(2),2009.Ginn,GregoryO.andCharlesB.Moseley,"CommunityHealthOrientation,Community-basedQualityImprovement,andHealthPromotionServicesinHospitals,"JournalofHealthcareManagement,49(5),2004.
Young,Gary,Chia-HungChou,JeffreyAlexander,Shoou-YihDanielLee,andEliRaver,“ProvisionofCommunityBenefitsbyTax-ExemptU.S.Hospitals,”NewEnglandJournalofMedicine368,no.16,2013.
InternalRevenueService,ReporttoCongressonPrivateTax-Exempt,Taxable,andGovernment-OwnedHospitals(Washington,DC:DepartmentoftheTreasury,2015.
Moseley,CharlesB.,Jay,J.Shen,andGregoryO.Ginn,“TheLong-termCoerciveEffectofStateCommunityBenefitLawsonHospitalCommunityHealthOrientation,”NevadaJournalofPublicHealth,7(1),2010.
Rubin,DanielB,SimoneSingh,andGaryYoung.“TaxExemptHospitalsandCommunitybenefit:NewDirectionsinPolicyandPractice.”Annu.Rev.PublicHealth,36,2015.
Somerville,MarthaH.,GayleD.Nelson,CarlH.Mueller,andCynthiaL.Boddie-Willis,“HospitalCommunityBenefitsaftertheACA:PresentPosture,FutureChallenges”,Baltimore,MD:HilltopInstitute,2013.
Somerville,MarthaH.,GayleD.Nelson,CarlH.Mueller.“HospitalCommunityBenefitsaftertheACA:TheStateLawLandscape”TheHilltopInstitute,IssueBrief.2013.Schlesinger,MarkandBradfordH.Gray.“HowNonprofitsMatterInAmericanMedicine,AndWhatToDoAboutIt”HealthAffairs25,no.4,2006
Young,Gary,Chia-HungChou,JeffreyAlexander,Shoou-YihDanielLee,andEliRaver,“ProvisionofCommunityBenefitsbyTax-ExemptU.S.Hospitals,”NewEnglandJournalofMedicine368,no.16,2013.
Price–CappsC,DranoveD.“HospitalConsolidationandNegotiatedPPOPrices.”HealthAffairs,vol.23,no.2,2004.

23
Cooper,Zack,StuartCraig,MartinGaynor,JohnVanReened.ThePriceAin’tRight?HospitalPricesandHealthSpendingonthePrivatelyInsured.NationalBureauofEconomicResearch,2015.Cuellar,AlisonEvansandPaulJ.Gertler“HowTheExpansionOfHospitalSystemsHasAffectedConsumers.”HealthAffairs24,no.1,2005.Cutler,DavidM.,andFionaScott-Morton.“Hospitals,MarketShareandConsolidation."JournalofAmericanMedicalAssociation,310(18),2013.Dafny,Leemore,KateHoandRobinLee.“ThePriceEffectsofCross-MarketHospitalMergers.”NationalBureauofEconomicsWorkingPaper,2016.DafnyLeemore.“EstimationandIdentificationofMergerEffects:AnApplicationtoHospitalMergers.”JournalofLawandEconomics,vol.52,no.3,2009.Dranove,David,RichardLindrooth.“HospitalConsolidationandcosts:anotherlookattheevidence.”JournalofHealthEconomics22,2003.Gaynor,Martin,andRobertTown.“TheImpactofHospitalConsolidation:Update."Princeton,NJ:RobertWoodJohnstonFoundation.2012.Haas-WilsonD.GarmonC.“HospitalMergersandCompetitiveEffects:TwoRetrospectiveAnalyses.”InternationalJournaloftheEconomicsofBusiness,vol.18,no.1,2011.MelnickG,KeelerE.“TheEffectsofMulti-HospitalSystemsonHospitalPrices.”JournalofHealthEconomics,vol.26,no.2,2007.MoriyaAS,VogtWB,GaynorM.“HospitalPricesandMarketStructureintheHospitalandInsuranceIndustries.”HealthEconomics,PolicyandLaw,vol.5,no.4,2010.PropperC,BurgessS,GreenK.“DoesCompetitionbetweenHospitalsImprovetheQualityofCare?HospitalDeathRatesandtheNHSInternalMarket.”JournalofPublicEconomics,vol.88,no.7–8,2004.ThompsonE.“TheEffectofHospitalMergersonInpatientPrices:ACaseStudyoftheNewHanover-CapeFearTransaction,”InternationalJournaloftheEconomicsofBusiness,vol.18,no.1,2011.VogtWB,TownRJ.HowHasHospitalConsolidationAffectedthePriceandQualityofHospitalCare?ResearchSynthesisReportNo.9.Princeton,NJ:RobertWoodJohnsonFoundation,2006..

24
QualityBloomN,PropperC,SeilerS,VanReenenJ.“TheImpactofCompetitiononManagementQuality:EvidencefromPublicHospitals.”WorkingPaperNo.16032.NationalBureauofEconomicResearch,2010.
CooperZ,GibbonsS,JonesS,McGuireA.“DoesHospitalCompetitionSaveLives?EvidencefromtheEnglishNHSPatientChoiceReforms.”TheEconomicJournal,vol.121,no.554,2011.
CutlerDM,HuckmanRS,KolstadJT.“InputConstraintsandtheEfficiencyofEntry:LessonsfromCardiacSurgery.”AmericanEconomicJournal:EconomicPolicy,vol.2,no.1,2010.
Gaynor,Martin,R.Moreno-Serra,andC.Propper,DeathbyMarketPower:Reform,CompetitionandPatientOutcomesintheNationalHealthService,WorkingPaperNo.16164,NationalBureauofEconomicResearch,2010.
GowrisankaranG,TownR.“Competition,PayersandHospitalQuality.”HealthServicesResearch,vol.38,no.6PartI,2003.
HoV,HamiltonB.“HospitalMergersandAcquisitions:DoesMarketConsolidationHarmPatients?”JournalofHealthEconomics,vol.19,no.5,2000.
KesslerD,McClellanM.“IsHospitalCompetitionSociallyWasteful?”QuarterlyJournalofEconomics,vol.115,no.2,2000.
KesslerD,GeppertJ.TheEffectsofCompetitiononVariationintheQualityandCostofMedicalCare.NationalBureauofEconomicResearch,NBERWorkingPaper#11226,2005.
MukamelD,ZwanzigerJ,TomaszewskiK,“HMOPenetration,Competition,andRisk-AdjustedHospitalMortality.”HealthServicesResearch,vol.36,no.6,2001.
MukamelD,ZwanzigerJ,BamezaiA.“HospitalCompetition,ResourceAllocationandQualityofCare.”BMCHealthServicesResearch,vol.2.no.10,2002.
MutterR,WongH.TheEffectsofHospitalCompetitiononInpatientQualityofCare.AgencyforHealthCareResearchandQuality,2004.
RogowskiJ,JainAK,EscarceJJ.“HospitalCompetition,ManagedCare,andMortalityafterHospitalizationforMedicalConditionsinCalifornia.”HealthServicesResearch,vol.42,no.2,2007.
SariN.“DoCompetitionandManagedCareImproveQuality?”HealthEconomics,vol.11,no.7,Oct2002.

25
ShortellS,HughesE.“TheEffectsofRegulation,Competition,andOwnershiponMortalityRatesAmongHospitalInpatients.”NewEnglandJournalofMedicine,vol.318,no.17,1988.
ShenYC.“TheEffectofFinancialPressureontheQualityofCareinHospitals.”JournalofHealthEconomics,vol.22,no.2,2003.
VolppK.KetchamJ,EpsteinA,WilliamsS.“TheEffectsofPriceCompetitionandReducedSubsidesforUncompensatedCareonHospitalMortality.”HealthServicesResearch,vol.40,no.4,2005.