hot issues in health care focus on medicaid & schip april 2, 2005 martha king national...
TRANSCRIPT
Hot Issues in Health Hot Issues in Health CareCare
Focus on Medicaid & SCHIPFocus on Medicaid & SCHIP
April 2, 2005April 2, 2005
Martha KingMartha King
National Conference of State Legislatures National Conference of State Legislatures (NCSL)(NCSL)
Health Program DirectorHealth Program Director
303/856-1448303/856-1448
[email protected]@ncsl.org
2
“While I can explain the meaning of life, I don’t dare try to explain how the Medicaid system works.”
Medicaid “Experts”Medicaid “Experts”

3
Medicaid Made SimpleMedicaid Made Simple
4
Medicaid: Why Should You Medicaid: Why Should You Care?Care?
22% of average state’s total budget 22% of average state’s total budget Largest financing source for low-income Largest financing source for low-income
(43% of federal allocations to states)(43% of federal allocations to states) Pays half of U.S. nursing home costsPays half of U.S. nursing home costs Covers 31% of U.S. population 85+Covers 31% of U.S. population 85+ Funds about 35% of U.S. birthsFunds about 35% of U.S. births Subsidizes care for the uninsured Subsidizes care for the uninsured Subsidizes graduate medical educationSubsidizes graduate medical education
5
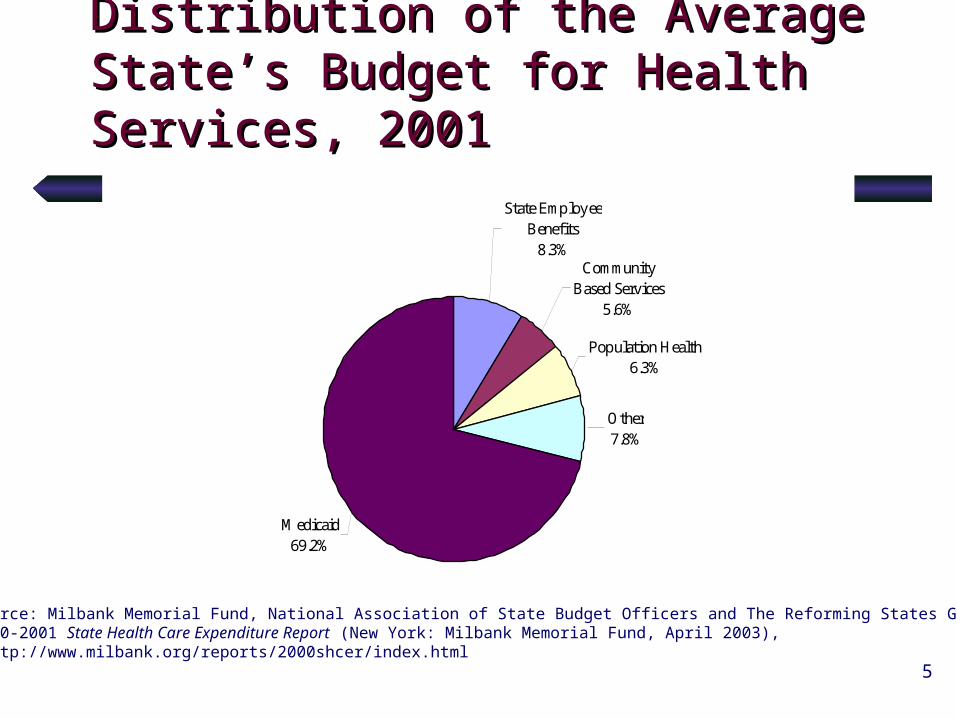
Distribution of the Average Distribution of the Average State’s Budget for Health State’s Budget for Health Services, 2001Services, 2001
Medicaid69.2%
Population Health 6.3%
Other7.8%
State Employee Benefits
8.3%Community
Based Services5.6%
Source: Milbank Memorial Fund, National Association of State Budget Officers and The Reforming States Group,2000-2001 State Health Care Expenditure Report (New York: Milbank Memorial Fund, April 2003), http://www.milbank.org/reports/2000shcer/index.html
6
Medicaid dominates the Medicaid dominates the health debatehealth debate
In 1985, Medicaid accounted for 8% of In 1985, Medicaid accounted for 8% of state budgets (total spending)state budgets (total spending)
In 2005, Medicaid accounts for 22% !!In 2005, Medicaid accounts for 22% !!(16.5% of state general funds)(16.5% of state general funds)
2/3 of spending is for optional people & 2/3 of spending is for optional people & servicesservices
42% of spending is for Medicare-42% of spending is for Medicare-covered recipientscovered recipients
35% of spending is for LTC services35% of spending is for LTC services
7
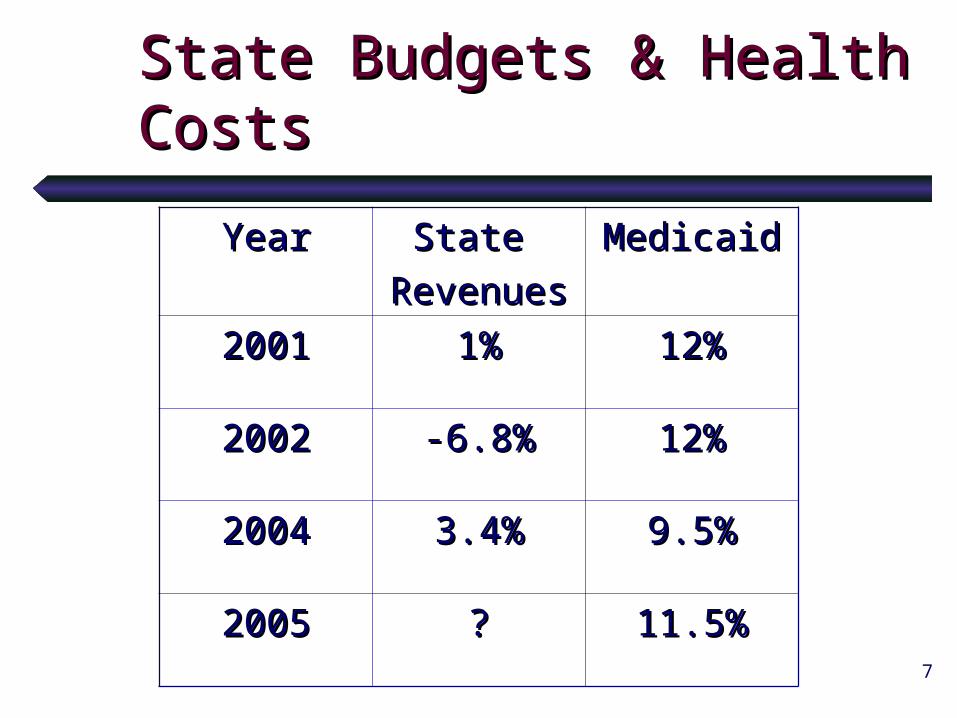
State Budgets & Health State Budgets & Health Costs Costs
YearYear State State
RevenuesRevenuesMedicaidMedicaid
20012001 1%1% 12%12%
20022002 -6.8%-6.8% 12%12%
20042004 3.4%3.4% 9.5%9.5%
20052005 ?? 11.5%11.5%
8
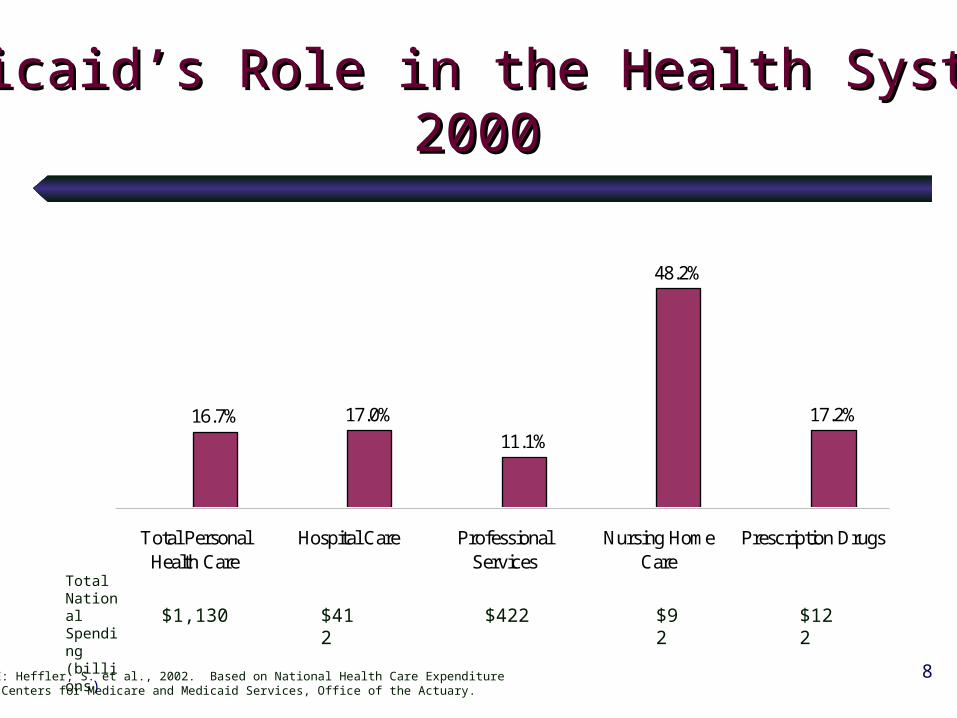
16.7% 17.0%
11.1%
48.2%
17.2%
Total PersonalHealth Care
Hospital Care ProfessionalServices
Nursing HomeCare
Prescription Drugs
TotalNationalSpending(billions)
$1,130 $412 $422 $92 $122
SOURCE: Heffler, S. et al., 2002. Based on National Health Care ExpenditureDate, Centers for Medicare and Medicaid Services, Office of the Actuary.
Medicaid’s Role in the Health System,Medicaid’s Role in the Health System,20002000
9
Medicaid at a GlanceMedicaid at a Glance
Federal/state program Federal/state program (55 variations)(55 variations)
Optional—large financial incentiveOptional—large financial incentiveFederal gov’t pays 50-80% of servicesFederal gov’t pays 50-80% of services
(Dollar for dollar match)(Dollar for dollar match)
10
Medicaid at a GlanceMedicaid at a Glance
Three programs in one:
A health insurance program for low-income parents (mostly mothers) and children
A funding source to provide services to people with significant disabilities
A long-term care program for the elderly““Medicaid makes Medicare work”Medicaid makes Medicare work”
11
Medicaid PerceptionsMedicaid Perceptions
One view:One view:
A black holeA black hole
Another view:Another view:
A cash cowA cash cow
12
People & ServicesPeople & Services
Entitlement: all who qualify are eligible
PEOPLE: Mandatory “categories” (e.g., children & PG women to 133% of poverty; SSI recipients)
Optional (e.g., additional children & PG women; “medically needy”)
SERVICES: Mandatory (e.g., hospital, nursing facility,physician, rural health clinics) Optional (e.g., Prescription drugs, hospice)
13
Who’s Not Covered?Who’s Not Covered?
Everybody else . . .Everybody else . . .Anyone not in a “category”Anyone not in a “category”
– 45 million uninsured Americans45 million uninsured Americans– Adults without children or SSI eligibilityAdults without children or SSI eligibility– Parents who makes more than about 40% of Parents who makes more than about 40% of
povertypoverty– Elderly or people with disabilities who don’t Elderly or people with disabilities who don’t
meet SSI or other criteriameet SSI or other criteria– High medical users who don’t meet criteriaHigh medical users who don’t meet criteria– etc.etc.
14
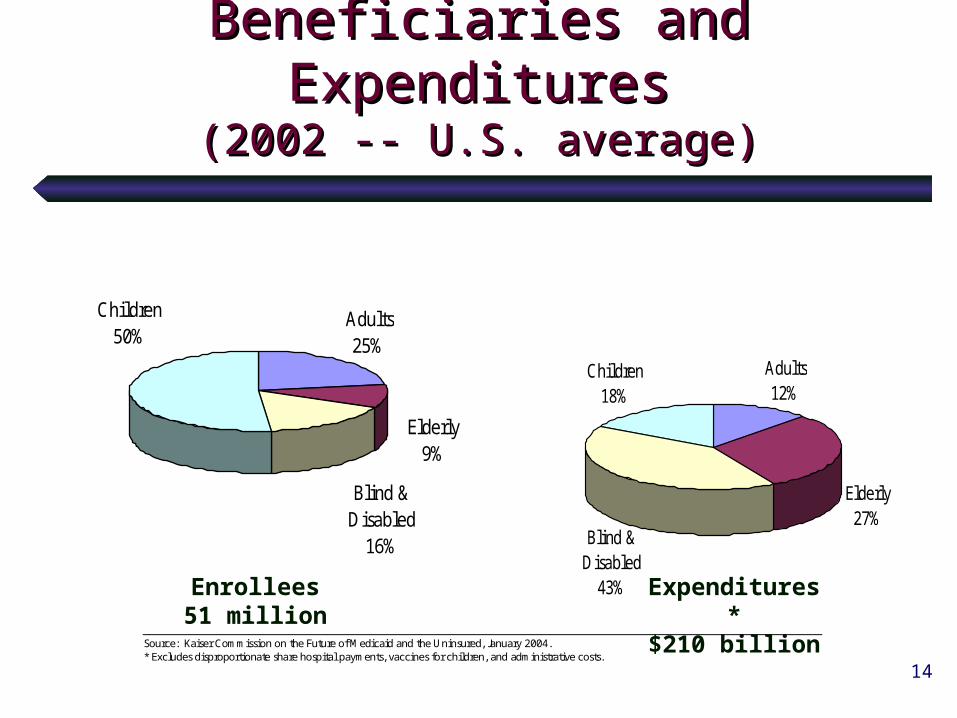
Beneficiaries and Beneficiaries and ExpendituresExpenditures
(2002 -- U.S. average)(2002 -- U.S. average)
Children50%
Adults25%
Elderly9%
Blind & Disabled
16%
Children18%
Adults12%
Elderly27%
Blind & Disabled
43%Enrollees51 million
Expenditures*$210 billion
Source: Kaiser Commission on the Future of Medicaid and the Uninsured, January 2004. * Excludes disproportionate share hospital payments, vaccines for children, and administrative costs.
15
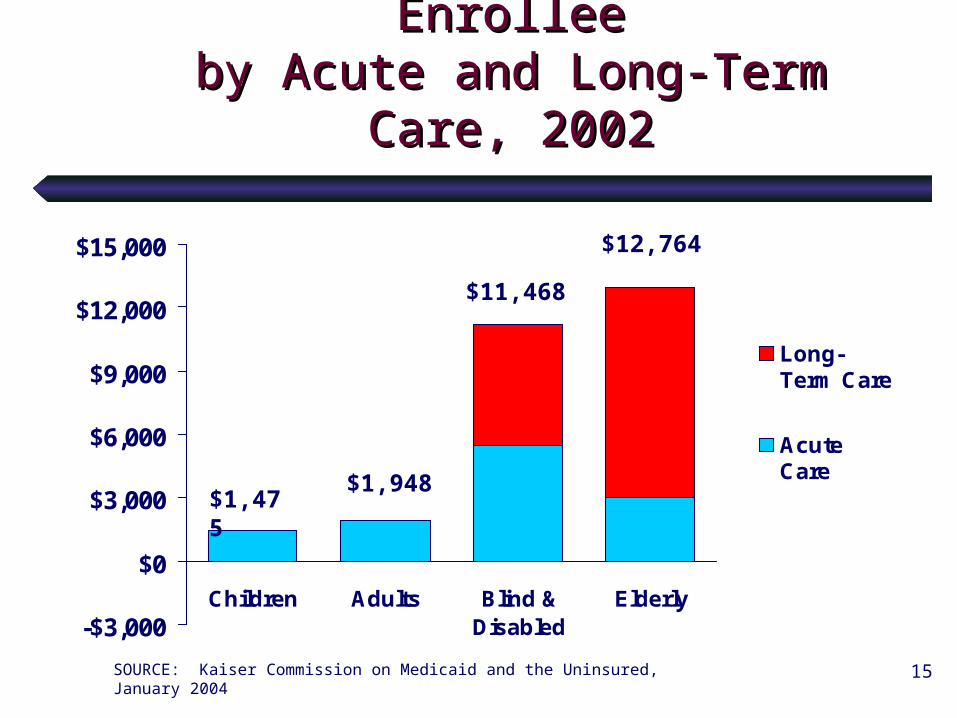
Medicaid Expenditures Per Medicaid Expenditures Per EnrolleeEnrollee
by Acute and Long-Term Care, by Acute and Long-Term Care, 20022002
-$3,000
$0
$3,000
$6,000
$9,000
$12,000
$15,000
Children Adults Blind &Disabled
Elderly
Long-Term Care
AcuteCare
$1,475$1,948
$11,468
$12,764
SOURCE: Kaiser Commission on Medicaid and the Uninsured, January 2004
16
““Waiver” OptionsWaiver” Options
Comprehensive health reform 1115 waiversComprehensive health reform 1115 waivers(e.g., DE, HI, MA, MN, OR, TN)(e.g., DE, HI, MA, MN, OR, TN)
New twist: Utah’s 1115 waiverNew twist: Utah’s 1115 waiverPrimary and preventive services only for adults to Primary and preventive services only for adults to 150% of poverty150% of poverty
Specialized 1115 waiversSpecialized 1115 waivers• ““Pharmacy Plus” — low-income senior Pharmacy Plus” — low-income senior
prescription drug benefit (only) up to 200% prescription drug benefit (only) up to 200% poverty (IL, SC, WI approved)poverty (IL, SC, WI approved)
• ““Discount-only” waiver — extend Medicaid drug Discount-only” waiver — extend Medicaid drug price reductions to other populations (ME price reductions to other populations (ME operating; court challenges)operating; court challenges)
• Family planning services — extend post-partum Family planning services — extend post-partum time for family planning (and primary care)time for family planning (and primary care)
17
Medicaid: New FlexibilityMedicaid: New Flexibility
HIFA (Health Insurance Flexibility & HIFA (Health Insurance Flexibility & Accountability initiative) —Accountability initiative) —6 approved6 approved
Special 1115 demonstration waiverSpecial 1115 demonstration waiver Purpose: to expand health Purpose: to expand health
insurance coverage to the insurance coverage to the uninsureduninsured
Targeted to people below 200% of Targeted to people below 200% of povertypoverty

18
Medicaid Expansions Medicaid Expansions Pros and ConsPros and Cons
ProsPros::• Federal share (50-80%) Federal share (50-80%) • Existing administration/provider networkExisting administration/provider network• New flexibility & optionsNew flexibility & options• ““Better than nothing” for uninsuredBetter than nothing” for uninsured
ConsCons::• Financing constraints Financing constraints (economy & budgets) (economy & budgets)
• Federal mandates (although getting better)Federal mandates (although getting better)• Potential “maintenance of effort” Potential “maintenance of effort”
requirementsrequirements• Political philosophy re less government rolePolitical philosophy re less government role
19
Cost-Saving StrategiesCost-Saving Strategies
Most typical cuts Most typical cuts Cut “optional” groups Cut “optional” groups (CO has limited (CO has limited
options)options) Cut or restrict “optional” servicesCut or restrict “optional” services
E.g., prescription drugs, hospice care, rehabilitative E.g., prescription drugs, hospice care, rehabilitative services, case management, etc.services, case management, etc.
Freeze or cut provider Freeze or cut provider reimbursementsreimbursements
Eliminate the entire Medicaid Eliminate the entire Medicaid programprogram
Caveats: Caveats: Unintended consequencesUnintended consequences““Penny-wise and pound foolish”Penny-wise and pound foolish”Cuts often shift burden: needs don’t disappearCuts often shift burden: needs don’t disappear
20
Only so much to cutOnly so much to cut
PeoplePeople
ProvidersProviders
ServicesServices

21
22
Cost-Saving StrategiesCost-Saving Strategies
Other reform options Other reform options Evaluate & understand program & optionsEvaluate & understand program & options Study & reform long-term careStudy & reform long-term care Emphasize preventionEmphasize prevention Reduce prescription drugs costsReduce prescription drugs costs Take advantage of federal flexibilityTake advantage of federal flexibility Reduce fraud & abuseReduce fraud & abuse Use electronic recordsUse electronic records ID any services eligible for federal matchID any services eligible for federal match Make Medicaid the “payer of last resort”Make Medicaid the “payer of last resort”
23
Evaluation/Oversight/Evaluation/Oversight/ConsultationConsultation
24
Evaluation/Oversight/Evaluation/Oversight/ConsultationConsultation
Medicaid oversight committeesMedicaid oversight committees MassachusettsMassachusetts House created a Medicaid committeeHouse created a Medicaid committee WyomingWyoming's 's subcommittee on Medicaid cost control & subcommittee on Medicaid cost control &
content content OregonOregon Senate special committee on the Oregon Health Senate special committee on the Oregon Health
Plan Plan KentuckyKentucky Medicaid Managed Care Oversight CommitteeMedicaid Managed Care Oversight Committee
http://www.lrc.state.ky.us/Statcomm/Medicaid/homepage.htmhttp://www.lrc.state.ky.us/Statcomm/Medicaid/homepage.htm
Legislative auditsLegislative audits South Carolina’sSouth Carolina’s Legislative Audit Council recommended Legislative Audit Council recommended
$22.9 million in savings. $22.9 million in savings. Preferred drug list est. $12.8 milPreferred drug list est. $12.8 mil Medicaid enrollment fee est. $1.4 milMedicaid enrollment fee est. $1.4 mil
http://www.state.sc.us/sclac/Reports/2003/Medicaid.htmhttp://www.state.sc.us/sclac/Reports/2003/Medicaid.htm

25
Evaluation/Oversight/Evaluation/Oversight/ConsultationConsultation
External evaluation & consultantsExternal evaluation & consultants Idaho’sIdaho’s Office of Performance Evaluations 2000 report Office of Performance Evaluations 2000 report
"Idaho's Medicaid Program: The Department of Health and "Idaho's Medicaid Program: The Department of Health and Welfare Has Many Opportunities for Cost Savings.” Welfare Has Many Opportunities for Cost Savings.”
http://www2.state.id.us/ope/http://www2.state.id.us/ope/ WashingtonWashington State Institute for Public Policy State Institute for Public Policy
http://www.wa.gov/wsipphttp://www.wa.gov/wsipp// WashingtonWashington commissioned a Lewin Group study. commissioned a Lewin Group study.
http://www.leg.wa.gov/senate/scs/wm/publications/http://www.leg.wa.gov/senate/scs/wm/publications/
Additional resources:Additional resources:http://www.dpw.state.pa.us/omap/geninf/maac/http://www.dpw.state.pa.us/omap/geninf/maac/
022703CostContainment.asp022703CostContainment.asp
http://http://www.le.state.ut.us/lrgc/briefingpapers/medicaid.pdfwww.le.state.ut.us/lrgc/briefingpapers/medicaid.pdf
26
Understanding the CostsUnderstanding the Costs
Elderly & people with disabilitiesElderly & people with disabilities Qualify based on both income & disabilityQualify based on both income & disability Medicaid has become the nation’s LTC Medicaid has become the nation’s LTC
“program of last resort” “program of last resort” (pays for 60% of N.H. (pays for 60% of N.H. residents)residents)
Medicaid serves as the nation’s “high risk Medicaid serves as the nation’s “high risk pool” for low-income people with serious pool” for low-income people with serious disabilities and chronic conditionsdisabilities and chronic conditions
What other options exist?What other options exist?
27
Focus on Long-Term CareFocus on Long-Term Care
80% of LTC provided by informal caregivers80% of LTC provided by informal caregiversDoes/should the state provide assistance?Does/should the state provide assistance?Can the state prevent or delay NH placements?Can the state prevent or delay NH placements?
““Personal care option”Personal care option” (assistance with bathing, (assistance with bathing, dressing, feeding, housekeeping, shopping, etc.)dressing, feeding, housekeeping, shopping, etc.)
LTC insurance: LTC insurance: does/should the state promote?does/should the state promote?
Federal law encourages community careFederal law encourages community care Doubling of residential and assisted living Doubling of residential and assisted living
options in last decadeoptions in last decade
28
Long-Term CareLong-Term Care
Institutional vs. community-based careInstitutional vs. community-based care 25% vs. 75% of LTC recipients25% vs. 75% of LTC recipients 70% vs. 30% of LTC spending70% vs. 30% of LTC spending
(Source: Harrington & Kitchener, NCSL Annual Meeting, 2003)(Source: Harrington & Kitchener, NCSL Annual Meeting, 2003)
Screening programsScreening programs Prevention initiatives Prevention initiatives (e.g., disease management, (e.g., disease management,
Meals-on Wheels, etc.)Meals-on Wheels, etc.)
Asset transfers/estate recoveryAsset transfers/estate recovery Family education/contributions?Family education/contributions? End-of-Life planning?End-of-Life planning?
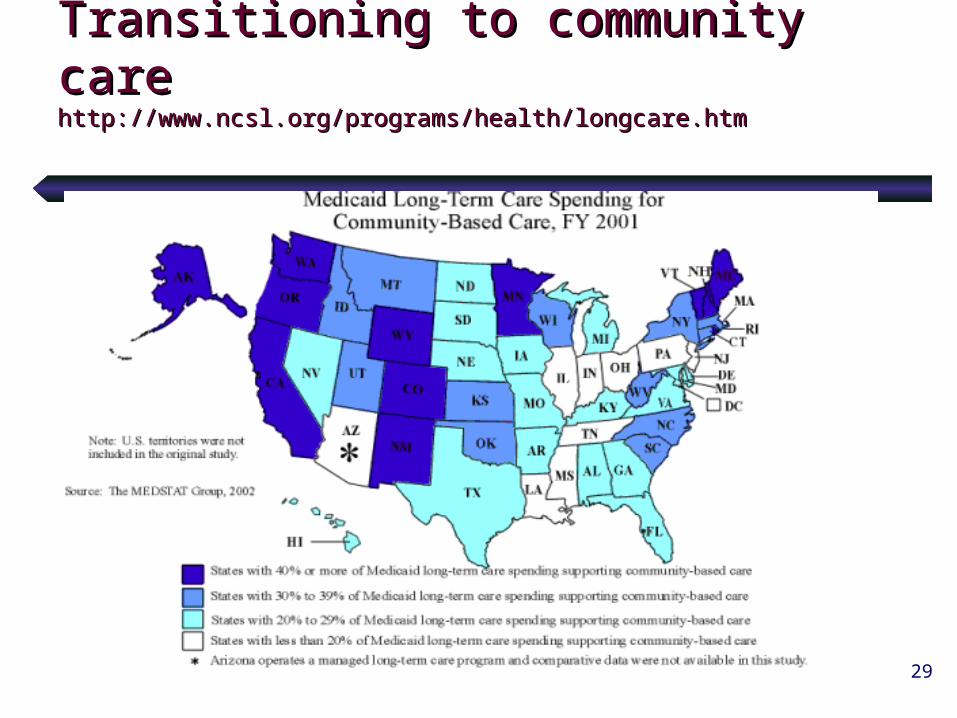
29
Transitioning to community careTransitioning to community carehttp://www.ncsl.org/programs/health/longcare.htmhttp://www.ncsl.org/programs/health/longcare.htm
30
Case Study: MaineCase Study: Maine
Target nursing home admissionsTarget nursing home admissions Medicare as first payerMedicare as first payer Legislative approval for nursing Legislative approval for nursing
home capacity changeshome capacity changes Stricter controls on asset transferStricter controls on asset transfer Expanded access to state and Expanded access to state and
Medicaid-funded home care services Medicaid-funded home care services
31
1995 MeCare program1995 MeCare program
Universal LTC pre-admissions screeningUniversal LTC pre-admissions screening Assessment costs = 1% of LTC spendingAssessment costs = 1% of LTC spending ““Case-mix” reimbursement for nursing Case-mix” reimbursement for nursing
homeshomes Nursing homes certify more Medicare Nursing homes certify more Medicare
bedsbeds Change in nursing facility Change in nursing facility
reimbursementreimbursement
32
Maine’s Cost SavingsMaine’s Cost Savings
Increased Medicare’s share of LTC (Medicaid’s Increased Medicare’s share of LTC (Medicaid’s share dropped 18% between 1995-2002)share dropped 18% between 1995-2002)
44% decline in Medicaid length of stay44% decline in Medicaid length of stay 26% decline in total nursing home days26% decline in total nursing home days # Nursing home beds: 10,207 (1994) 7,708 # Nursing home beds: 10,207 (1994) 7,708
(2002)(2002) % of LTC clients in nursing homes:% of LTC clients in nursing homes:
1995, 50%1995, 50%
2001, 33% 2001, 33% 12% decline in per-person spending12% decline in per-person spending
33
For More InformationFor More Information
Maine Resources:Maine Resources: Maine’s HCBS System Maine’s HCBS System
www.state.me.us/dhs/beas/ltc/www.state.me.us/dhs/beas/ltc/ Pre-Admission Screening Program Pre-Admission Screening Program
www.state.me.us/dhs/beas/ltc/2001/mecare2001.htmwww.state.me.us/dhs/beas/ltc/2001/mecare2001.htm
State and Medicaid LTC Expenditures: State and Medicaid LTC Expenditures: www.state.me.us/dhs/beas/ltc/ltc_exp_97_01.htwww.state.me.us/dhs/beas/ltc/ltc_exp_97_01.htmm
LTC status report, Dec. 2002: LTC status report, Dec. 2002: www.state.me.us/dhs/beas/ltc/2002/ltc_2002.htwww.state.me.us/dhs/beas/ltc/2002/ltc_2002.htmm
34
Case Study: MinnesotaCase Study: Minnesota
Pre-admission screening for nursing Pre-admission screening for nursing home carehome care
Community development grants NH Community development grants NH alternatives alternatives
Community services expansionsCommunity services expansions Closure of excess nursing home bedsClosure of excess nursing home beds Moratorium on new nursing home Moratorium on new nursing home
constructionconstruction

35
Minnesota Cost SavingsMinnesota Cost Savings
Eliminated 1,089 nursing home beds Eliminated 1,089 nursing home beds between Aug. 2001 and Jan. 2003between Aug. 2001 and Jan. 2003
Reduced nursing home beds per 1,000 Reduced nursing home beds per 1,000 elderly from 68 in 2000 to 64 in 2002elderly from 68 in 2000 to 64 in 2002
Decreased NH spending as % of public Decreased NH spending as % of public LTC spending from 86% in 2000 to 73% LTC spending from 86% in 2000 to 73% in 2002in 2002
Minnesota’s Long-term Care Task Force:Minnesota’s Long-term Care Task Force:
www.dhs.state.mn.us/agingint/ltctaskforce/default.htmwww.dhs.state.mn.us/agingint/ltctaskforce/default.htm

36
Case Study: WisconsinCase Study: Wisconsin
1995 Family Care Pilot Program (integrates county-level 1995 Family Care Pilot Program (integrates county-level LTC services through case management and managed LTC services through case management and managed LTC)LTC)
Single entry point for LTC services (assessment, Single entry point for LTC services (assessment, consultation, case management, individual service plans)consultation, case management, individual service plans)
Pre-admission counseling to LTC facilitiesPre-admission counseling to LTC facilities Savings:Savings:
LTC spending decreased by an average of $198/person/mo. LTC spending decreased by an average of $198/person/mo.
(9.6% less per Family Care enrollee than a similar population (9.6% less per Family Care enrollee than a similar population in a fee-for-service environment)in a fee-for-service environment)
Family Care Program: www.dhfs.state.wi.us/LTCare/index.htmFamily Care Program: www.dhfs.state.wi.us/LTCare/index.htm
37
LTC: Other IdeasLTC: Other Ideas Arizona, Texas, Arizona Arizona, Texas, Arizona
Managed LTC and integrated acute/LTC programsManaged LTC and integrated acute/LTC programs
Oregon:Oregon: expanded home & community services; reduced expanded home & community services; reduced NH beds (1981-95, Medicaid $ fell by 8.6%; nationwide NH beds (1981-95, Medicaid $ fell by 8.6%; nationwide increase of 19%)increase of 19%)
National Family Caregiver Program National Family Caregiver Program (funds to Area (funds to Area Agencies on Aging—86% participants say” enables home care Agencies on Aging—86% participants say” enables home care
for longer”) for longer”) Bush Admin. Systems Change Grants & Bush Admin. Systems Change Grants &
“Independence Plus Initiative” (D“Independence Plus Initiative” (Demo for family or emo for family or individual directed comm. Services)individual directed comm. Services)
““Aging in Place” initiatives (e.g., GA & NH)Aging in Place” initiatives (e.g., GA & NH)
38
Chronic Illness & Chronic Illness & DisabilitiesDisabilities
How much could be prevented/reduced?How much could be prevented/reduced? Access to insurance Access to insurance Medicaid “Ticket to Work” Buy-Medicaid “Ticket to Work” Buy-
in in http://www.ncsl.org/legis/health/medicaidbuyin.htm)http://www.ncsl.org/legis/health/medicaidbuyin.htm)
Access to preventive & primary careAccess to preventive & primary care Prenatal care & counselingPrenatal care & counseling Focus on wellness/health educationFocus on wellness/health education Smoking (est. 12% of costs for Medicaid in ’99)Smoking (est. 12% of costs for Medicaid in ’99) Obesity Obesity (estimated $21 billion in obesity-related (estimated $21 billion in obesity-related
conditions)conditions)
Disease Management/”Care Management”Disease Management/”Care Management”
39
Disease ManagementDisease Management
Top 1% of people account for 30% of health spendingTop 1% of people account for 30% of health spending Top 10% of people for 70% of spendingTop 10% of people for 70% of spending Bottom 50% of people for 3% of spendingBottom 50% of people for 3% of spending
(Source: Scott Leitz, Economist, Minnesota Department of Health)(Source: Scott Leitz, Economist, Minnesota Department of Health)
““Disease management” targets people with Disease management” targets people with chronic illness and provides more intensive chronic illness and provides more intensive services services Common targets: asthma, HIV/AIDS, cardiac diseases, Common targets: asthma, HIV/AIDS, cardiac diseases,
diabetes, hemophilia, depressiondiabetes, hemophilia, depression Leaders: FL, MD, MS, NCLeaders: FL, MD, MS, NC
““Care Management” focuses on people, not Care Management” focuses on people, not diseasedisease E.g., Lahey Clinic in Mass.: 50% of enrollees had 5+ E.g., Lahey Clinic in Mass.: 50% of enrollees had 5+
conditionsconditions
40
Disease ManagementDisease Management
Cost savings?Cost savings? Not a panacea, could help with longer-term Not a panacea, could help with longer-term
costscosts ER visits for patients reducedER visits for patients reduced Hospital costs reduced overall for participantsHospital costs reduced overall for participants
Resources:Resources: http://www.ncsl.org/programs/health/diseasemgmt.htmhttp://www.ncsl.org/programs/health/diseasemgmt.htm ““Contracting for Chronic Disease Management: The Florida Contracting for Chronic Disease Management: The Florida
Experience”Experience”
http://www.chcs.org/usr_doc/CDM-report.PDFhttp://www.chcs.org/usr_doc/CDM-report.PDF
41
Preventive & Primary CarePreventive & Primary Care
Appropriate preventive & acute care Appropriate preventive & acute care for Medicaid enrolleesfor Medicaid enrollees Plan/provider accountabilityPlan/provider accountability Outreach/TreatmentOutreach/Treatment Screening/educationScreening/education ImmunizationsImmunizations ““Medical home” for kids (avoid ER use)Medical home” for kids (avoid ER use)
(North Carolina Pilot Project)(North Carolina Pilot Project)
42
High-Value Preventive ServicesHigh-Value Preventive Services(for adults--Partnership for (for adults--Partnership for Prevention)Prevention)
Tobacco cessation counselingTobacco cessation counseling Vision screening age 65+Vision screening age 65+ Cervical cancer screeningCervical cancer screening Colorectal cancer screeningColorectal cancer screening Hypertension screeningHypertension screening Influenza vaccinationInfluenza vaccination Chlamydia screeningChlamydia screening Cholesterol screeningCholesterol screening Problem drinking screening & counselingProblem drinking screening & counseling Pneumococcal vaccination age 65+Pneumococcal vaccination age 65+
43
Prescription Drug SavingsPrescription Drug Savings
Rx accounts for 12% of Medicaid costs (U.S.)Rx accounts for 12% of Medicaid costs (U.S.) Rapidly rising costs (17.3% in ’01; est. 12.9% in Rapidly rising costs (17.3% in ’01; est. 12.9% in
’04)’04) Valuable cost-saving tool Valuable cost-saving tool
Prevent hospital & nursing home costsPrevent hospital & nursing home costs Most common cost containment strategies:Most common cost containment strategies:
Prior authorization Prior authorization Preferred drug lists: 30+ states Preferred drug lists: 30+ states Supplemental rebates: 14+ statesSupplemental rebates: 14+ statesUse of genericsUse of generics
Caveat: Don’t be “penny wise & pound foolish”Caveat: Don’t be “penny wise & pound foolish”
44
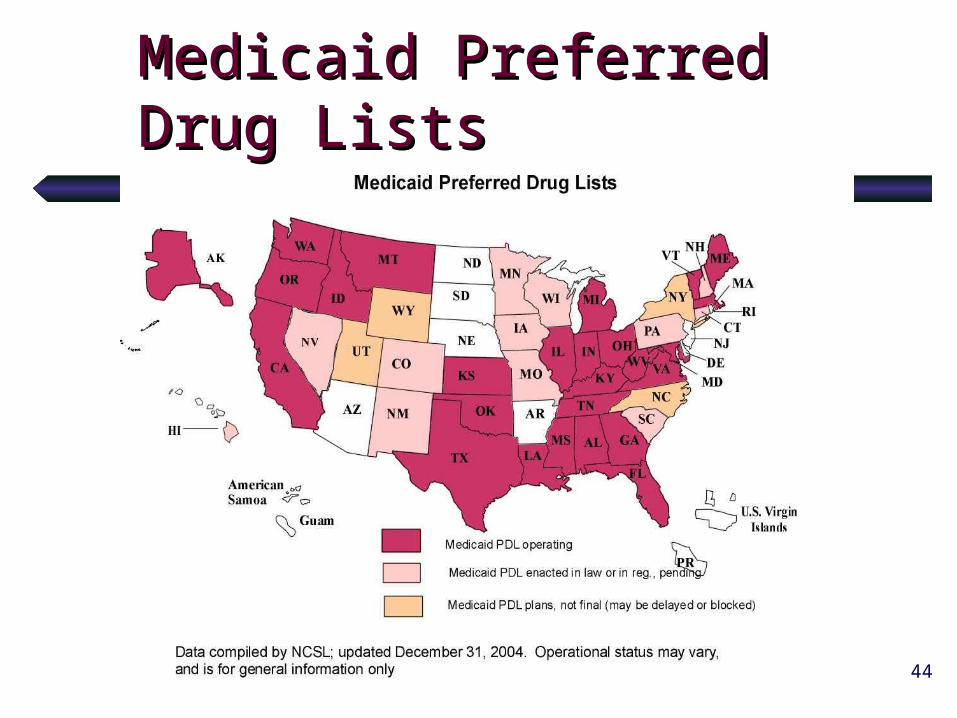
Medicaid Preferred Drug Medicaid Preferred Drug ListsLists
45
Prescription Drug SavingsPrescription Drug Savings
Other cost containment strategies:Other cost containment strategies: Step therapy or “fail first”Step therapy or “fail first” Disease managementDisease management Monthly Caps and limitsMonthly Caps and limits Adjust dispensing fees & ingredient Adjust dispensing fees & ingredient
reimbursementreimbursement Enrollee copaymentsEnrollee copayments Fraud & abuse investigationsFraud & abuse investigations Pharmaceutical managers or administratorsPharmaceutical managers or administrators Multi-state bulk purchasingMulti-state bulk purchasing
46
New Medicare Rx BenefitNew Medicare Rx Benefit
Medicaid has subsidized MedicareMedicaid has subsidized Medicare Est. 80-85% of Medicaid Rx costs for Est. 80-85% of Medicaid Rx costs for
elderly & people with disabilities elderly & people with disabilities (many (many of whom covered by Medicare)of whom covered by Medicare)
January 2006:January 2006:Medicare will cover outpatient Rx for Medicare will cover outpatient Rx for
Medicare/Medicaid “dually eligible”Medicare/Medicaid “dually eligible”States will pay under “claw back” States will pay under “claw back”
provisionprovision(90% of 2003 drug costs in ’06 & ’07)(90% of 2003 drug costs in ’06 & ’07)
47
New Federal FlexibilityNew Federal Flexibility
Most reforms intended to expand Most reforms intended to expand coveragecoverage
1115 Waivers1115 Waivers HIFA Waiver (a new 1115 type)HIFA Waiver (a new 1115 type) Premium assistance programsPremium assistance programs Modified benefit packagesModified benefit packages
48
Employer Premium Assistance Employer Premium Assistance Programs/Health Insurance Premium Programs/Health Insurance Premium Payment ProgramsPayment Programs
Public insurance subsidizes employer coverage for Public insurance subsidizes employer coverage for low-income working beneficiaries: Medicaid or SCHIP.low-income working beneficiaries: Medicaid or SCHIP.
15 states have programs -- different in intent and 15 states have programs -- different in intent and scope. scope.
Can be done through Medicaid or SCHIPCan be done through Medicaid or SCHIP Savings significant in states with eligibility to families Savings significant in states with eligibility to families
above 100% of povertyabove 100% of poverty
visit http://www.ncsl.org/programs/health/buyin03.htm visit http://www.ncsl.org/programs/health/buyin03.htm for a list of the states and few details of the programs.for a list of the states and few details of the programs.
49
Case Study: Utah’s Primary Case Study: Utah’s Primary Care Network (1115 Waiver Care Network (1115 Waiver program)program)
First state to offer a very basic benefit First state to offer a very basic benefit package (limited to preventive & primary package (limited to preventive & primary care) to an expansion population (adults up care) to an expansion population (adults up to 150%).to 150%).
Reduced benefits and increased cost Reduced benefits and increased cost sharing to some mandatory Medicaid clients sharing to some mandatory Medicaid clients (TANF parents) to help finance the program.(TANF parents) to help finance the program.
Lessons for other states:Lessons for other states: Does investment in primary care reduce uncompensated Does investment in primary care reduce uncompensated
care $$?care $$? Will people be interested in a very limited benefit package Will people be interested in a very limited benefit package
over time? So far, enrollment steady over time with the over time? So far, enrollment steady over time with the number at 18,910 as of 1-8-05number at 18,910 as of 1-8-05
50
Utah’s Primary Care Network Utah’s Primary Care Network BenefitsBenefits
Primary/preventive care by physicians and Primary/preventive care by physicians and mid-level professionals enrolled in the mid-level professionals enrolled in the networknetwork
Adult immunizationsAdult immunizations Urgent care & ER visits when appropriateUrgent care & ER visits when appropriate Lab, x-ray, medical equipment, medical Lab, x-ray, medical equipment, medical
supplies, oxygen, ambulancesupplies, oxygen, ambulance Basic dental, hearing tests, vision screening Basic dental, hearing tests, vision screening
but not glasses.but not glasses. Prescription drugs [Limit of 4 per month]Prescription drugs [Limit of 4 per month]
51
Other State Medicaid Other State Medicaid ProposalsProposals
FloridaFlorida and and South CarolinaSouth Carolina• Revamp to resemble private managed care Revamp to resemble private managed care
plansplans• Assign a “premium” per person (risk Assign a “premium” per person (risk
adjusted)adjusted)• Cap the “premium”Cap the “premium”• Give Medicaid recipients HSAsGive Medicaid recipients HSAs• Focus on prevention (reward it)Focus on prevention (reward it)
52
Reducing Medicaid Fraud and Reducing Medicaid Fraud and AbuseAbuse
Billing for services not renderedBilling for services not rendered Billing for unnecessary servicesBilling for unnecessary services substitutions of generic drugssubstitutions of generic drugs KickbacksKickbacks Double billingDouble billing Other unauthorized billing such as charging a Other unauthorized billing such as charging a
customer for service covered by Medicaidcustomer for service covered by Medicaid

53
Case Study: Florida Case Study: Florida
Florida: 1996 enacted two laws to strengthen Florida: 1996 enacted two laws to strengthen anti-fraud and abuse activitiesanti-fraud and abuse activities
Identifies providers with aberrant billing patternsIdentifies providers with aberrant billing patterns Conducts provider investigationsConducts provider investigations Recommends administrative sanctionsRecommends administrative sanctions Permits Florida’s Medicaid Fraud Control Unit to Permits Florida’s Medicaid Fraud Control Unit to
become law enforcement officersbecome law enforcement officers Florida AG’s Office reports the Medicaid Fraud Florida AG’s Office reports the Medicaid Fraud
Control Unit recovered $17.5 million in cash and Control Unit recovered $17.5 million in cash and made 158 arrests in 2001made 158 arrests in 2001
54
Case Study: TexasCase Study: Texas
1995 Medicaid Fraud and Prevention Act1995 Medicaid Fraud and Prevention Act AG’s office investigates and prosecutes Medicaid AG’s office investigates and prosecutes Medicaid
fraudfraud Provider exclusion listsProvider exclusion lists Inpatient screening criteriaInpatient screening criteria Medicaid fraud training to health care professionalsMedicaid fraud training to health care professionals Medicaid fraud and abuse reportsMedicaid fraud and abuse reports In the second fiscal quarter of 2003, 1,435 fraud In the second fiscal quarter of 2003, 1,435 fraud
cases identified and $14.5 million was recoveredcases identified and $14.5 million was recovered Recently, 2 Rx companies paid $45 million to settle Recently, 2 Rx companies paid $45 million to settle
fraud charges (accused of falsely reporting inflated fraud charges (accused of falsely reporting inflated prices)prices)
55
Electronic Billing, Data Electronic Billing, Data Collection and Eligibility Collection and Eligibility DeterminationDetermination
Arkansas saved about $30 million in 17 Arkansas saved about $30 million in 17 months:months: Drop in emergency room useDrop in emergency room use Reduced claims processing timeReduced claims processing time Virtually eliminated collection expenseVirtually eliminated collection expense Lessened claim denialsLessened claim denials Increased efficiency in data analysis Increased efficiency in data analysis
and report productionand report production
Arkansas Medicaid: Arkansas Medicaid: http://www.medicaid.state.ar.ushttp://www.medicaid.state.ar.us

56
Combination InitiativesCombination Initiatives
E.g., OregonE.g., Oregon Government’s role:Government’s role:
Insure the uninsured up to the poverty Insure the uninsured up to the poverty levellevel
Provide subsidies for some othersProvide subsidies for some others Employers’ roles:Employers’ roles:
Cover employees with incomes above Cover employees with incomes above poverty via “play or pay” requirementpoverty via “play or pay” requirement
Other: Other: Prioritize publicly funded health Prioritize publicly funded health servicesservices
57
Opportunities & ChallengesOpportunities & Challenges
What are your goals?What are your goals? Universal coverage? Universal access?Universal coverage? Universal access? Healthy population?Healthy population? More personal responsibility?More personal responsibility?
What is the appropriate role of What is the appropriate role of government?government?
The private sector?The private sector? Individuals?Individuals?
Are you getting what you pay for?Are you getting what you pay for? Services, quality, health status improvements?Services, quality, health status improvements?
How can you control (not shift) costs?How can you control (not shift) costs?
58
SCHIPSCHIP
State Children’s Health Insurance State Children’s Health Insurance ProgramProgram
Non-Medicaid insurance optionNon-Medicaid insurance option More flexibility than Medicaid expansionMore flexibility than Medicaid expansion Higher federal matching rateHigher federal matching rate Cover kids under 200% of povertyCover kids under 200% of poverty Waivers possible Waivers possible
59
FY 2006 Proposed Health FY 2006 Proposed Health BudgetBudget
President’s FY 2006 Budget President’s FY 2006 Budget Proposal for Selected Health Proposal for Selected Health ProgramsPrograms
http://www.ncsl.org/print/health/06HltBgtPrhttp://www.ncsl.org/print/health/06HltBgtProps.pdfops.pdf
60
MedicaidMedicaid
CMS revised baseline for annual CMS revised baseline for annual Medicaid growth rate over next 10 Medicaid growth rate over next 10 years: from 7.8 % to 7.6%years: from 7.8 % to 7.6%
Result: $73 billion reduction in Result: $73 billion reduction in spendingspending
With FY06 Budget Proposals the With FY06 Budget Proposals the baseline for growth would be 7.3%baseline for growth would be 7.3%
61
Proposed Administrative Proposed Administrative ChangesChanges
Payment ReformsPayment Reforms Program AdministrationProgram Administration Prescription Drug Program ReformsPrescription Drug Program Reforms