houston we have a problem lessons learned from the …€¦ · houston we have a problem: lessons...
TRANSCRIPT

Houston We Have a Problem: Lessons Learned from the San
Francisco Plane Crash
André Campbell, M.D., F.A.C.S.,F.A.C.P.,F.C.C.M.Professor of Surgery, UCSF
San Francisco General HospitalNMA Honolulu Hawaii August 4, 2014

Nothing to disclose

The Response after Asiana


Overview
• I was the post call Trauma Surgeon who was present when the MCI was called.
• I noted what was happening on CNN and saw a twitter feed of actual video so I stayed.
• I spoke with Dr. Chin who verified that it was real
• A knock at the door and I was deeply involved.
• Many residents, faculty called in willing to help
• We had three trauma attending, two fellows, residents, ED staff, Radiology, Neurosurgery, Orthopedics, Anesthesia, Executive Staff, Nursing and Physician leaders and many more

Overview
• Largest mass casualty event in the history of SFGH Trauma Center
• Many systems worked really well overall
• Triage of the most severely injured patients is the key
• 67 victims were cared for at SFGH of the 308 crash victims
• Five patients received ICU care

Crash 11:28 am 7/6/13
122 mph196 kph



11:27 am…
• First report on twitter 30 seconds later
• “Code 33: Plane down”
• ‘small cargo plane’
• 11:29 am – 911 call
• 11:30 am – 1st ambulance
• 11:40 am San Mateo County disaster page
• 12:06 pm – SF red alert

SFO MCI Plan
• SFO is part of SF, but in San Mateo County
• Different SF & SM MCI Plans & Activation Levels
• Unified Command SFO

First beeper notification
12:03 am Mass Casualty Incidence Page(MCI)

“Code Triage”SFGH Mass Casualty Plan
• Clear ED – Expedited Admits & Discharges
• Radiology & EVS Move Available Gurneys to Ambulance Bay
• Prep OR & PACU for Rapid Turnover
• Open Inpatient Beds in Med-Surg
• Open & Expand Clinic Treatment Areas for Minor / Delayed Patients
Immediate Actions – Every Department Prepares for Surge:
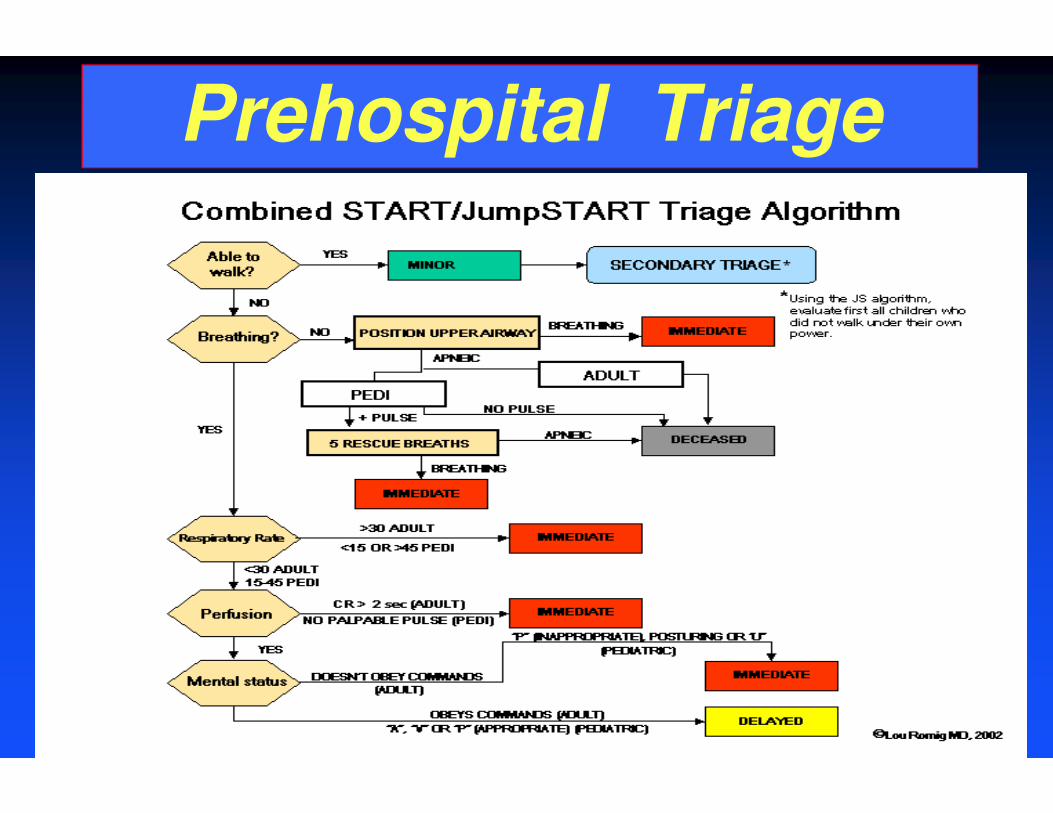
Prehospital Triage

Plane Crashes are Survivable
• 80% occur • 1st 3 mins/last 8 mins
• 1983 to 2000 • 95% of crashes survivable
• US: 1/11 million chance of dying in plane crash
• If fatality – 4% survivors

Plane Crash 101
• When a plane crashes there are huge forces that are exerted on the human body
• Typical injuries include fractured extremities, pelvic fractures, spinal fractures, smoke inhalation, cutaneous burns, toxin exposure, visceral injuries, sternal fracture, head injuries, neck injuries
• When people die it is usually massive blunt force trauma
J of Trauma; 47(4)1999:617


• 181 injured passengers
• 12 critical: 10 SFGH/2 Stanford
• 2 deaths at the scene
• 2 flight attendants ejected
• Found on the runway still in seats
• 9 hospitals admitted 182 pts.
Fate of the Passengers

• First wave of injured patients arrive
• Six critical condition
• “Burns and Inhalation injuries”?
• Severe blunt trauma
• Two very unstable: taken to the OR within minutes
First Wave of Patients arrive at 12:30 PM

“Prepare for the First, the Worst, & the Most”
12:30 – 1 pm: 10 patients
• 8 adults, 2 children
• 6 critical patients
• 4 serious

Initial Response
• 3 Attending Surgeon Led Teams
• Multiple ED teams
• 5 anesthesia teams
• Fellows
• Residents
• NPs
• Burns?
• Inhalation Injury?
• Industrial Hazards?
• Severe blunt trauma?

Lesson 2: ‘Dual Command’
Emergency Medicine MD
• Initial triage to Care areas
• Coordinates with RN leadership in ED
• Usually at ambulance entrances
Senior Trauma Surgeon
• Oversight of care plans
• Assign surgical workforce
• Remain in ED to coordinate
• Triages all resources (CT, OR, Blood products)
• Keep master list of all patient conditions
Rapid evaluation and dispositions

PATIENT INJURIES
#1 TBI, Facial Burns, Inhalation*, Spine
#2 Major intestinal, spine with paralysis; road burns
#3 Chest, intestinal, spine with paralysis,mandible, > 30% TBSA road burns
#4 Extremity injury with compartment Sx
#5 Severe TBI, spine, sternum, ribs
#6 TBI, spine, sternum, extremity fractures
First Wave Critical Injuries

Crash Related Other emergencies
Damage control laparotomy; burns Hand fracture
Reduction of fracture; fasciotomy Appendectomy
Damage control laparotomy; burns Stab wound to the abdomen
Laminectomy; spinal fusion Wrist fracture
Spinal decompression Craniotomy
Craniotomy Wound debridement
Spinal fusion Wound debridement
Take-back laparotomy Infection
Take-back laparotomy Fracture
Fracture
Operative Interventions First 48 hours

• Assess size & skillset
• Each MD group should have a plan
• Anticipate needs, but don’t cry wolf
• Central locations
• Comfort zone
“People didn’t stay at home to watch the news…they rushed to hospital to lend a hand.”
-Geoff Manley, MD
JAMA
Lesson #3: Assess workforce.Give people roles they are
capable of.

Keys to Our Success
• Formed ‘mini teams’
• Extend capabilities
• Senior members to areas where admitted
• Good team communication

• 1 – 5 pm: 25 patients Critical to good
• 5 – 7 pm: 18 patients – All minor category
53 Total Patients (36 Admitted) Day 1
#4 View everything as a potentially limited resource

Initial Distribution to Hospitals
Trauma Centers:
• SFGH – 53 (10 Critical)
• Stanford – 55 (2 Critical)
• Eden – 2
Other Hospitals:
Peninsula – 15
Kaiser RWC – 10
Sequoia – 5
UCSF – 15
CPMC – 9
St. Francis – 7
Kaiser SF – 5
St. Mary’s – 4

Stay Organized
• If you leave –leave someone in charge
• Master list
• Surgical team member assigned
• Reported to Trauma attending
• Direct hand offs

Physician Coordination
• EM
• Trauma
• Orthopedics
• Neurosurgery
• Radiology
• Interventional Radiology
Debrief on First 36 patients @ 17:30

Lesson 7: Don’t forget your other inpatients…they need care too.
• Dedicate a portion of the workforce
• These patients may be more ill
• Facilitate discharges

Lesson 8: Plan for the long haul
• Sunday - 8 adults & 1 child arrived at ED - all treated/released.
• Monday – 4 children Pediatric
Urgent Care
– 17 patients still admitted (6 in ICU)
• Wednesday – 1 adult
67 total patients

Lesson 9 – Think outside the Box
• Language Barriers
• Large number of children
• International Flight
• No identification
• Several unidentified
• Many agencies

Lesson 10 – Acknowledge contributions & Share Your
Experience
• Many people go far above the call of duty in disasters.

• Blood bank supply: >100 U
• Judicious monitored use
Other Unique Challenges

• Strange metabolic picture: acidosis, hypocalcemia; hypotension
• Persisted for days among survivors
• Toxic exposure: jet fuels, foam, cargo?
Potential Toxins Exposure

• 2 deaths at the scene
• Different Customs and Cultures and Languages
Emotional Distress Families

TYPES OF DISASTER TYPES OF DISASTER TYPES OF DISASTER TYPES OF DISASTER Natural
Disasters
Meteorological
Topographical
Environmental
Man-made Disasters
Technological
Industrial accidents
Security related


PHASES OF DISASTER MANAGEMENTPHASES OF DISASTER MANAGEMENTPHASES OF DISASTER MANAGEMENTPHASES OF DISASTER MANAGEMENT
Disaster Preparedness
Disaster impact
Disaster Response
Rehabilitation
Disaster Mitigation

Triage
• Goal: Identify minority of critically injured casualties requiring immediate treatment
• Secondary goal: prevent overwhelming primary receiving hospital with minor injuries(over triage)
• Fryberg and Tepas J of Trauma 1988
–Review of 14 bombing
–Inverse relationship between triage discrimination and critical mortality

Triage Methodology
• Goal: Triage accuracy
• Primary Triage: Institute near scene of the disaster
• Reinforce initial sorting at a second
designated triage area
• Triage areas should be separated from the hospital providing definitive care

Category Definition ExamplesExpectant Death expected if unlimited
resourcesGSW headProfound shockLarge burns + injuries
Urgent Will result in death unless urgently Rx’d
Tension PTXCardiac Tamponade
Immediate Life threatening but can survive if Rx’d
Open Fx’dVascular injury and ischemia
Delayed Injuries will tolerate a reasonable delay
Abdom inj (-) hemorrhageVascular inj w/o ischemia
Minimal/Ambulatory Minor, superficial wounds can be treated w/o GA
Burns < 15% TBSASuperficial lacerations
Triage DefinitionsNATO War Surgery Handbook-1988

Ten Golden Rules for Urban Mass Casualty Management
• Try to follow day-to-day routines
– incorporate MCI terms and procedure into daily routines
• Do what will save lives in the long term
–balance immediate nears with survival
• Quickly establish a centralized easy to identify command post and incident commander
• Communicate succinctly in a Clear Zone
–free from surrounding noise; allows radio or phone signal
Pepe et al., Prehosp & Disaster Management, 1989

• Remember fewer knowledge rescuers do better than volunteers
• Emphasize central controlled evacuation
–BLS: first aid and transport
–ALS: secondary triage and accompany critical patients
• Triage and evaluate all patients to the usual receiving facilities
–Send to trauma centers even if numbers are large
Ten Golden Rules for Urban Mass Casualty Management
Pepe et al., Prehosp & Disaster Management, 1989

• Log events chronologically and centralize the media
–Use media to notify the public and dispel unnecessary fears: make request public
• Always provide post-incident care for rescuers and victims
– Both immediate and subsequent debriefings
• Train and test all potential rescuers
Ten Golden Rules for Urban Mass Casualty Management
Pepe et al., Prehosp & Disaster Management, 1989

Media
• Big media event from day one
• Many distractions from the care of the patients
• Must be careful in address the media in the setting of a dynamically changing situation

Instantaneous News
• They come quick and stay a long time…

Set Expectations
• Early announcement
• 1st press conference 2-3 hours after crash
• Set plans for next gathering

Keep Distance
• Privacy
• Secure Patient Areas
• Allow movement of medical teams around hospital
• NO PATIENT ACCESS DAY 1

Build Trust
• Media have a purpose
• VITAL in disasters
• Public are very influenced by EARLY information

Staff communication
• Helps to clarify role in disasters
• Call-in hotlines
• Refrain from boosting of early success
• Recognize contributions

Be Fair, Consistent, and Don’t Over promise
• Journalist do not like uncertainty.
• DO NOT BECOME THE SOURCE OF SCOOPED INFORMATION
oImmediately remind employees to direct ANY and ALL media requests to your PIO.
• Non-negotiable

• Combination of intestinal injuries and spine fractures
• Most commonly seen with lap-belt use
• Severe flexion over a fixed object
• Most common injuries:spine;chest
Chance Fractures after back injury

• Ruptured diaphragms
• “Road Burns”: wound care/skin grafts
• Cardiac arrhythmias, low Ca++, low platelets
• Renal failure: CVVH
• Intestinal Fistulas
• Intra-abdominal infections
• Open abdomens from damage control surgery
Other Challenges

Other Challenges
• Dealing with critically ill patients
• Cross cultural issues were really a challenge
• Months of care for some individuals
• Single event changed lives permanently
• Three deaths of the 308 passengers and crew that were on the plane two at the scene
• One died at SFGH

Caring for Our Caregivers
• Team Debriefings
• Open Debriefings in Wellness Center
• Open Chapel Times
• Active “Surveillance” for Issues
• Separate Operational Debriefing
• Schwartz Center Roundshttp://www.theschwartzcenter.org/ViewPage.aspx?pageId=20
• Recognition
• PTSD

Team Effort!



What Worked Well
• Surge Preparation – Drill, Drill, Drill
• Patient Assessment & Treatment
• Kept Families Together
• “Wrap Around Care” & 3-Step Check-Out
• Media Relations
• Sharing Patient Names with Red Cross
• Collaboration Throughout - “Yes We Can”
• Staff Care / Schwartz Center Rounds

Improvements Needed
• Redundant HICS Team Notifications
• Patient Tracking Dashboard
• Management of Phone Calls
• Volunteers / Press / Lawyers
• Call US State Department for Support
• Notify CDPH Earlier re: Use of Tent
• Further Integration of Mental Health
• Patient Decontamination

Conclusions
• Outstanding response from the entire area
• Biggest challenge in the history of the hospital
• I received emails, calls, texts from all around the world
• Everyone chipped in and helped
• Discharges done and transfers happened
• Pre-hospital, ED, OR, ICU and all the services worked together
• Our finest hour