document
DESCRIPTION
http://www.kirklees.nhs.uk/uploads/tx_galileodocuments/Wakefield__NK_Diabetes_guidelines_2007.pdfTRANSCRIPT

1 Diabetes Care : A Guide to Good Working Practice
Wakefield District and North Kirklees Diabetes Network : Diabetes Guidelines
Wakefield District and North Kirklees Diabetes Network Diabetes Care: A Guide to Good Working Practice
August 2007

2 Diabetes Care : A Guide to Good Working Practice
CONTENTS PAGE Introduction 4 Wakefield and District Diabetes Network Board Members 5 Wakefield and District Diabetes Network Terms of Reference 6 Core Guidelines for Diabetes Care 8 Early Identification of People with Type 2 Diabetes 10 Diagnosis of Diabetes 11 Management Guidelines for Impaired Glucose Tolerance and Fasting Glucose 14 Education of People with Diabetes 15
Dietary Management of Diabetes 21
Physical Activity in the Management of Diabetes : Benefits and Risks 27 Diabetes and Smoking 30 Management of Cardiovascular Risk 32 Stepwise Approach to the Treatment Management of Type 2 Diabetes 42 Insulin Therapy for Type 2 Diabetes 43 Retinopathy: Screening and Early Management 46 Integrated Care Pathway for Footcare in Diabetes 53 Care Pathway for the Management of Renal Disease in People With Diabetes 54 Management of Diabetes in Children : Good Practice Guidelines for Pontefract and Wakefield - Information for General Practitioners 56 Transitional Care 60

3 Diabetes Care : A Guide to Good Working Practice
Appendix I Classification and Terminology 61 Appendix II Guidelines for Screening and Diagnosis of Gestational Diabetes 62 Appendix III Recommended Testing for Individuals with Diabetes 64 Appendix IV Dietetic Guidelines for Children Newly Diagnosed With Diabetes 67 Appendix V Suggestions regarding Further Information for Individuals with Diabetes 69 References 71

4 Diabetes Care : A Guide to Good Working Practice
INTRODUCTION Guidelines for diabetes care were originally produced in 1991 and revised in 1997, 2001 and 2006 for the Wakefield area. Since this time there have been a number of changes to the diabetes service namely the development of the Wakefield District and North Kirklees Diabetes Network. There have also been changes affecting the clinical management of patients with Type 2 diabetes, including the publication of the diabetes National Service Framework (NSF) delivery strategy and NICE guidelines, and also the development of local integrated care pathways. We hope that the revised guidelines will continue to deliver the essential foundation of good quality diabetes care. It is anticipated that these guidelines will be reviewed periodically.

5 Diabetes Care : A Guide to Good Working Practice
WAKEFIELD DISTRICT AND NORTH KIRKLEES DIABETES NETWORK TITLE LEAD DEPUTY
Chair Dinesh Nagi
Clinical Lead (Pinderfields) Tara Kadis
Ryan Da Costa
Clinical Lead (Pontefract) Helen Dobson
Vicki Yates
Clinical Lead (Dewsbury) Ann Maria Wisher
Carol Wildey
Paediatric Lead Alison Grove Peter Mackay Brigid Allagoa Sheila Roberts
Network Manager Janet Wilson
Gill Day
Network Co-ordinator Kay Bellwood
Clinical Champion Mark Freeman
Amanda Rowley
Primary Care Clinical Lead Som de Silva (GP) Lesley Newland (GP) Tony Goodwin (GP)
Head of Public Health (Long Term Conditions) (Wakefield District PCT)
Jo Harcombe
Patient Representative(s) Anne Cooper Grahame Platt
Diabetes UK Regional Manager
Linda Wood
Commissioner(s) Richard Sewell (Wakefield District PCT)
Mid Yorkshire Hospitals NHS Trust General Manager
Shaun Garside

6 Diabetes Care : A Guide to Good Working Practice
WAKEFIELD DISTRICT AND NORTH KIRKLEES DIABETES NETWORK TERMS OF REFERENCE
Overall Purpose The purpose of the Wakefield District and North Kirklees Diabetes Network is to provide a structure for population based service planning across the ‘district’ by advising on targeting resources where they are most needed Aims and objectives • The multi-agency team’s strategic aim is to improve outcomes for adults and
children with diabetes in promoting models of self care. Patient empowerment within the context of the national targets and to ensure quality of life equitable to those patients without diabetes across the Wakefield District and North Kirklees Diabetes Network by securing a high equitable standard of care.
• Develop and agree a joint strategic plan, in order to modernise the delivery of
key national targets and local priorities, tackle health inequalities and improve the health experience of local people.
• Secure effective engagement with service users and carers to inform the
development of a modernised service plan. • To take the strategic lead on the national targets in the NSF, retinal screening,
diabetes registers and structured education programmes. • Prepare the Diabetes Network’s annual work programme, incorporating
specific objectives, targets and milestones to be achieved within the current planning year.
• It is a requirement of this group to review the annual public health report and
comment on its findings. • Undertake appropriate mapping work, to determine the current service model,
take stock of performance and identify existing financial resource commitment. • Re-engineer the service model, building on good practice and evidence where
appropriate. Consider ‘whole system solutions’ and the focus on health inequalities and health improvement
• Advice on and support appropriate commissioning arrangements to fulfill the
service and health improvement model.

7 Diabetes Care : A Guide to Good Working Practice
• Performance manages the annual work programme of the Diabetes Network to ensure improvement in key performance indicators (ie. Retinal screening targets, Quality Outcomes Framework Indicators). Review progress against work programmes and take action as appropriate.
• Ensure strategic links are established and maintained between relevant
strategic planning groups, in order to benefit from overlapping activities. • In conjunction with the District Workforce Development Group, determine the
workforce and capacity requirements necessary to achieve the strategic plan. • In conjunction with the District Local Information Strategy Group, determine the
IM and T requirements necessary to achieve the strategic plan. • To report annually to the PCTs and local people via the relevant channels. January 2007

8 Diabetes Care : A Guide to Good Working Practice
CORE GUIDELINES FOR DIABETES CARE A firm foundation for good quality diabetes care would incorporate a commitment to the following: 1. REGISTER To have and keep up to date a register for all people with diabetes 2. CALL AND RECALL To ensure that systematic call and recall of patients is taking place, for
regular surveillance for ongoing care and detection of complications. It is our aim that in future this will be done through electronic call and recall.
3. PERSON CENTRED / EMPOWERMENT
To empower the individual to adopt a healthy lifestyle and to manage their own diabetes, through education and support which recognises the importance of lifestyle, culture and religion, and which, where necessary, tackles the adverse impact of material disadvantage and social exclusion
4. STRUCTURED EDUCATION FOR NEWLY DIAGNOSED PATIENTS To ensure that all newly diagnosed patients receive appropriate structured
education and where appropriate attend the DESMOND (Diabetes Education and Self-management for Ongoing and Newly Diagnosed) education programme. Modules for ongoing care and for Black Minority and Ethnic (BME) groups are in development
To ensure that people who decline to attend the DESMOND education are
provided with structured education on an individual basis 5. CONTINUING EDUCATION FOR PATIENTS To ensure that all patients receive appropriate structured continuing
education following locally agreed guidelines 6. CLINICAL HISTORY AND TESTS To ensure that on initial diagnosis and at least annually, a full review should
be performed including the following: Measure: * weight and body mass index * blood pressure * Blood cholesterol HDL and LDL

9 Diabetes Care : A Guide to Good Working Practice
* microalbuminuria * glycosylated haemoglobin (HbA1C) * creatinine/eGFR Advise: * to stop smoking * to moderate alcohol consumption * to take as much physical activity as possible * regarding eye care in accordance with the retinal
screening programme * regarding foot care in accordance with Diabetes foot care
integrated care pathway Review patient's monitoring 7. REFERRAL POLICIES To refer patients promptly and appropriately to the relevant agencies using,
where issued, the appropriate referral guidelines 8. RECORD KEEPING To maintain adequate records of performance and outcomes of the above
procedures. 9. AUDIT To audit the care of patients with diabetes against the above criteria and to
audit the integrated care pathways as appropriate

EARLY IDENTIFICATION OF PEOPLE WITH TYPE 2 DIABETES EARLY IDENTIFICATION OF PEOPLE WITH TYPE 2 DIABETES
Diabetes Care : A Guide to Good Working Practice
10
Diabetes is becoming more common
• The prevalence of those over 30 years old is 10% and rises with age, • The prevalence will be doubled by 2025 • There is generally a long asymptomatic stage of up to 10 years
Risk Factors • Suggestive symptoms
o Polyuria, nocturia, excess thirst o Fatigue o Weight loss
o Neuropathic symptoms o Recurrent infections especially thrush o Changes in visual acuity
• Macrovascular disease (Ischaemic Heart Disease, Peripheral Vascular Disease, TIA/Stroke) • All women with a history of a large baby (>4kg) • History of diabetes in pregnancy • Overweight and sedentary lifestyle • South Asian or Afro-Caribbean
The risk of diabetes is increased X 5 (if not already present) in The Metabolic Syndrome
Of which the 2005 International Diabetes Federation definition is:
Central Obesity
Plus any two of
Waist circumference 1. Triglyceride>1.70mmol/L* Female >80cm (31.5 ins) 2. HDL-cholesterol<0.9mmol/L (M)*
<1.1mmol/L (F)* Europid Male >94cm (37 ins) 3. BP >130 systolic or >85 Diastolic* South Asian Male >90cm (35.5 ins) 4. Impaired fasting glycaemia or type 2 diabetes
* or on treatment for these
When to Screen
Targeted Opportunistic Screening • Routine health checks • Coronary heart disease clinics • Well women clinics • Health related events in the community
Annual Screening • Previous gestational diabetes • Impaired fasting glycaemia • Impaired glucose tolerance
Consider regular Screening (every 1 - 3 years) • Central Obesity* (ensuring waist measurements) • Macrovascular disease • Hypertension* • Hypertriglyceridaemia* *features of • Diabetes in a first degree relative metabolic • Long term steroid use syndrome • South Asian >30 years old
How to Test For initial routine screening of the asymptomatic young (<65 years)
• Test post-prandial urine for glucose For all others and if glycosuria
• Check fasting plasma glucose (but fasting normal glycaemia does not exclude diabetes)
If fasting plasma glucose is >7mmol/l refer to the Newly Diagnosed Diabetes Integrated Care Pathway

Newly Diagnosed DiabetesNewly Diagnosed DiabetesIntegrated Care PathwayIntegrated Care Pathway
Eastern W akefieldPrimary Care Trust
W akefield W estPrimary Care Trust
M id Yorkshire HospitalsNHS TrustReview date: 2.2.06
Enquiries to: gill.day@ wwpct.nhs.ukEndorsed by: Diabetes Strategic Partnership GroupGroup responsible for development: Diabetes Integrated Care Pathway Steering Group
Diabetes
SelfNHS Direct/W alk in Centre
Community PharmacistsOpticians
Opportunistic ScreeningHospital Outpatients/Inpatients
PresentationSymptoms, e.g. thirst, polyuria, weight loss, fatigue, visual disturbances
Diagnostic TestsPlasma Glucose (Laboratory Test)
(mmol/l)Random >11.1Fasting >7.0If asymptomatic, confirm diagnosis with repeat test on another dayTest urine for ketones
Diagnostic Guidelines
• Enter details onto practice register• Refer to DESMOND education programme for Type 2 diabetes (newly diagnosed module)• Refer to retinal screening programme
Implementation of self-management planReview according to individual needsConsider earlier intervention w ith tablet medication if symptomatic & Type 2 D iabetes
To Care Pathway for Continuing Diabetes Care
(In development)
North KirkleesPrimary Care Trust
•Discuss diagnosis and immediatepatient concerns
•Establish patients know ledge ofillness and education needs
•Give initial dietary lifestyle advice, including physical activity • Smoking cessation referral and
advice if required
Education
Negotiate and outline a self-management plan to include:-•Individual targets•Support and Monitoring•Named contact•Recall advice
Management
Type 2 Diabetes
Diagnosis
Follow ing D iagnostic Guidelines
Type 1 Diabetes
Assessment of the person w ith newly diagnosed diabetes by a member of the Primary Care Team•Physical examination to include
BMI waist measurement and BP• Urine for m icroalbum inuria• Take blood sample for glucose,
HbA1c, U&E, LFT’s, TFT’s Lipids• Examine feet
Clinical Examination
• Symptomatic and acutely ill• Ketonuria
Refer by:Telephone call followed by a fax to the appropriate Diabetes Centre
Referral
Same Day Admission
• Dehydrationrequiring IVfluids
• Requiringintensivemonitoring –ketotic
• Seriousintercurrent
problem
11 Diabetes Care : A Guide to Good Working Practice

1 Diabetes Care : A Guide
Diagnosing Diabetes Diabetes is diagnosed on the basis of the following WHO criteria; Symptoms of hyperglycaemia (polyuria
polydipsia, unexplained weight loss. visual blurring, genital thrush, lethargy) plus raised venous plasma glucose level detected once fasting: 7.0mmol/L or higher or random 11.1 mmol/L or higher
OR In the absence of symptoms 2 abnormal
results are required for the diagnosis. A random glucose of 7 – 11 should be followed by a fasting blood glucose. If the result of the second test is not diagnostic, an oral glucose tolerance test (OGTT) should be performed
Impaired fasting glucose (FG >6.1mmol/l - 6.9mmol/l) should be followed by an OGTT to exclude a diagnosis of diabetes.
Impaired glucose tolerance (2 hour OGTT value of 7.8mmol/l – 11.1mmol/l) should be followed by lifestyle advice, education and repeat fasting blood tests in one year.
Initial Education and Management NICE guidelines (2003) recommend that
structured patient education is made available to all patients with diabetes at the time of initial diagnosis and then as required on an ongoing basis, based on a formal, regular assessment of need.
Initial education should include: lifestyle advice including healthy eating, physical activity, smoking cessation and alcohol.
Refer newly diagnosed to DESMOND programme if appropriate
Appropriate leaflets should be given to support the initial advice given eg. First steps and a healthy eating leaflet
An explanation of targets, stressing that a multifactorial approach (eg. looking at BP and cholesterol alongside blood glucose control) is required when negotiating a self-management plan with the patient.
Test urine for microalbuminuria in Type 2 diabetes
Ensure that the person with newly diagnosed diabetes is referred to the retinal screening programme.
Review dates should be agreed according to each patients individual needs.
Link to the single assessment process where appropriate when managing complex long term conditions.
Refer to specialist dietitian if appropriate ( see referral criteria in dietetic pathway in development) Ensure that a foot assessment takes place and appropriate education is given according to risk classification (see diabetic foot care ICP)
Referral Guidelines Admission
Admit to hospital if the person is at risk ofa hyperglycaemic emergency (vomiting, abdominal pain reduced conscious level, heavy ketonuria, dehydration requiring IVfluids, hypotension, serious intercurrent problem)
Same day referral Refer to be seen on the same day if the patient is acutely ill, consider Type 1 Diabetes if ketonuria present, the patient is slim and has a short history of marked symptoms (weight loss, thirst, polyuria)
Early Referral Diabetes and pregnancy requires referral to the hospital diabetes team please see pregnancy guidelines
2
to Good Working Practice

13 Diabetes Care : A Guide to Good Working Practice
Diagnosing Diabetes Diabetes is diagnosed on the basis of the following WHO criteria; • Symptoms of hyperglycaemia (polyuria polydipsia, unexplained weight loss.
visual blurring, genital thrush, lethargy) plus raised venous plasma glucose level detected once fasting: 7.0mmol/L or higher or random 11.1 mmol/L or higher
OR
• In the absence of symptoms 2 abnormal results are required for the diagnosis.
A random glucose of 7 – 11 should be followed by a fasting blood glucose. If the result of the second test is not diagnostic, an oral glucose tolerance test (OGTT) should be performed
• Impaired fasting glycaemia (FG >6.1mmol/l - 6.9mmol/l) should be followed by an OGTT to exclude a diagnosis of diabetes.
• Impaired glucose tolerance (2 hour OGTT value of 7.8mmol/l – 11.1mmol/l) should be followed by lifestyle advice, education and repeat fasting blood tests in one year.
A diagnosis of diabetes has important legal and medical implications for the patient and it is therefore essential to be secure in the diagnosis. A diagnosis should never be made on the basis of glycosuria or a stick reading of a finger prick blood glucose alone, although such tests may be useful for screening purposes. HbA1c measurement is also not currently recommended for the diagnosis of diabetes.

MANAGEMENT GUIDELINES FOR IMPAIRED GLUCOSE TOLERANCE AND IMPAIRED FASTING GLUCOSE
Previous gestational diabetes treated with insulin
Confirmed diagnosis of impaired glucose tolerance or impaired fasting glucose – refer to newly diagnosed diabetes ICP
OR
1. Advice regarding lifestyle modification
• Physical Activity • Healthy eating • No smoking
2. Cardiovascular risk factor
assessment
Annual fasting blood glucose
Diabetes Mellitus
Above or equal to 7.0 mmol/l x 2
14 Diabetes Care : A Guide to Good Working Practice

15 Diabetes Care : A Guide to Good Working Practice
EDUCATION OF PEOPLE WITH DIABETES The Diabetes National Service Framework (DH 2001) highlights structured education programmes as a key part of systematic care. It is recommended that structured patient education is made available to all people with diabetes at the time of initial diagnosis and then as required on an ongoing basis, based on a formal regular assessment of need. The aim of education for people with diabetes is to improve their knowledge and skills, enabling them to take control of their own condition and to integrate self management in their daily lives. The ultimate goal of education is improvement in the following areas: • Control of vascular risk factors, including blood glucose, blood lipids and blood
pressure • Management of diabetes associated complications, if and when they develop • Quality of life Education should be provided by an appropriately trained multidisciplinary team to groups of people with diabetes, unless group work is considered unsuitable for an individual. All people who are newly diagnosed with diabetes should be referred into the DESMOND programme if they are willing to participate in group education. The DESMOND Programme DESMOND (Diabetes Education and Self-Management for Ongoing and Newly Diagnosed) is a structured education programme for people with Type 2 diabetes. DESMOND provides 6 hours of structured group education over two half days no more than two weeks apart. Groups consist of 6 – 10 people newly diagnosed with Type 2 diabetes. The programme covers areas such as the patients’ story, main ways to manage diabetes, the risks and complications of diabetes, food choices and action planning. The philosophy underpinning DESMOND is essentially patient centred. Its aim is to support individuals to achieve their own goals for managing their diabetes. It is not about motivating people to do what health care professionals think they should do. Recognition that the person with diabetes is the expert in their own condition is therefore the driver for the programme and influences the style of how it is delivered. The style of delivery is crucial to enable all information to be made personally relevant and to promote individual problem solving and action planning which is then dovetailed with clinical management.

16 Diabetes Care : A Guide to Good Working Practice
The DESMOND programme should be ideally offered to people within two to three months of diagnosis. The overall aim is to ensure that people with diabetes are empowered to enhance their personal control over the day-to-day management of their diabetes in a way that enables them to experience the best quality of life. Carbohydrate Counting Group Education Group education sessions are provided for people with Type 1 diabetes and people with Type 2 diabetes who are using the basal bolus insulin regime and wish to control their blood glucose by carbohydrate counting. The session is run by both a Diabetes Specialist Nurse and a Specialist Dietician. There is individual carbohydrate counting education sessions available in Dewsbury. The education session helps the patient to understand how to adjust their own doses of insulin according to the amount of carbohydrate they are eating at each meal and also in relation to the amount and intensity of physical activity they are undertaking. Checklist For Diabetes Education The following checklists can be used as a helpful guide in covering the important points that an individual with diabetes and their family should know. Section One - Guidelines for all Individuals with Diabetes
Topic Date Discussed
Date(s) Reviewed
Comments
What is diabetes? o explanation of condition o symptoms o rationale of treatment Treatment Plan Dietary Requirements Physical Activity Oral hypoglycaemic agents o check patient knows: o type, length of action, dose,
when to take, side effects including hypoglycaemia

17 Diabetes Care : A Guide to Good Working Practice
Topic Date discussed
Date(s) Reviewed
Comments
Insulins (see section two) Warning signs of poor control Hyperglycaemia and ketoacidosis o symptoms o causes and prevention Hypoglycaemia o signs and symptoms o causes and prevention o carrying of glucose o patient identification o awareness of family/friends o Driving o need for glucagon/hypostop
Monitoring of condition * Importance of good control * Urine testing: technique why and when
to test significance record keeping * Urine testing: technique (ketones) why and when
to test * HbA1c What it means
Frequency of testing
* Blood testing: technique (self-monitoring why and when Of blood glucose) to test significance record keeping Safe disposal of sharps (Refer to Appendix III for

18 Diabetes Care : A Guide to Good Working Practice
recommended testing)
Topic Date Discussed
Date(s) Reviewed
Comments
Identification * Patient hand held record * Information regarding
talismans/medicalerts etc Illness and Diabetes * Never stop insulin/tablets * More frequent testing of
blood/urine for glucose (and ketones if appropriate)
* Vomiting * When to consult doctor/nurse Look After Yourself * Importance of regular diabetes
check ups * Effects of alcohol * Effects of smoking * Physical activity
Look After Yourself (continued) * Obesity * Holidays * Employment/jobs Eye Care * Importance of regular
retinal screening Foot Care * Importance of regularly
checking your feet Other possible Problems * Erectile Dysfunction * Neuropathy

19 Diabetes Care : A Guide to Good Working Practice
* Nephropathy Topic Date
Discussed Date(s) Reviewed
Comments
• CHD • Retinopathy Driving and Diabetes * Notify DVLC and Insurance* Dangers of hypoglycaemia Pregnancy and Diabetes * Preconception counselling * Contraception * Pregnancy advice Support Groups • Diabetes Focus Group • Diabetes UK Local branches • Expert patient programme • Local Support groups • PALS (Patient advice and
liaison service Prescription Charges/Benefits • Prescription exemption • Availability of benefits How to get Help * Contact numbers

20 Diabetes Care : A Guide to Good Working Practice
Section Two - Additional Information for Individuals with treated with Insulin
Topic Date Discussed
Date(s) Reviewed
Comments
Treatment Plan - Insulins The action of insulin injection techniques * Choice/use of pen * Name and type of insulin * Action of insulin * Timing of injections * Injection technique * Site rotation * Storage of insulin * Self adjustment of insulin Employment * Shift work adjustments * Counselling * Encouragement and
support

21 Diabetes Care : A Guide to Good Working Practice
DIETARY MANAGEMENT OF DIABETES
Diet remains the foundation of diabetes management. Everyone with diabetes should receive dietary information and support. State registered dietitians will provide specific, individual dietary advice that takes patient’s lifestyles and cultural preferences into account. Aims
• Abolish primary symptoms • Minimise fluctuations in blood glucose concentrations and improving
glycaemic control • Improve blood lipid profiles, minimising the long term macrovascular and
microvascular complications • Maintain a desirable body weight (BMI 20-25) • Encourage weight loss where appropriate
Dietary Management Of Type 1 Diabetes Dietary management of Type 1 diabetes focuses primarily on improvement of overall glycaemic control. Daily carbohydrate distribution, carbohydrate counting and glycaemic index may be discussed. Dietary Management Of Type 2 Diabetes Dietary management of Type 2 diabetes focuses on glycaemic control, cardioprotection and weight management. Carbohydrate Refined Sugars
These foods are digested very quickly and cause a rapid rise in the blood sugar levels. Diets should be low in sugar, but do not need to be sugar free. Some sugary foods can be eaten in moderation. Education should be given so that patients understand when refined sugars may be consumed. Intake of refined sugar foods should be reserved for:- • Special occasions • Occasionally following high carbohydrate fibre meal • Prior to vigorous exercise (mainly Type 1 diabetes) Refined sugars are also the first line treatment in the dietary management of hypoglycaemia, where rapidly available glucose is required to raise plasma glucose levels.

22 Diabetes Care : A Guide to Good Working Practice
However, it is paramount to follow this intake with • a complex carbohydrate to maintain the correct blood sugar levels and
prevent a rebound hypoglycaemic episode. Recommend These Instead of These Artificial sweeteners Sugar Reduced sugar jam Jams, marmalade, honey, syrup No added sugar squashes/diet fizzy drinks
Squashes, fizzy drinks, lucozade
Porridge, high fibre cereals Sugar/honey coated cereals Tinned fruit in juices/sugar free puddings Tinned fruit in syrup, puddings, jellies Diet yoghurt, diet fromage frais Low fat yoghurt, fromage frais Starches These are slowly broken down into sugar and can be used for energy. Always include a portion of one of these foods with each meal. Try high fibre varieties where possible.
Patients on sulphonylureas and insulins may require snacks and/or supper. These should be assessed individually. Those patients needing carbohydrate counting and dose adjustment should be referred to a specialist dietitian.
Starchy Carbohydrate Foods • Bread – preferably multigrain and granary • Naan bread, chapattis made with wholemeal or medium brown flour, pitta bread.
Try not to add any fat to chappatis. • Potato – boil, bake, mash and dry roast potatoes rather than cooking in fat or oil.
Oven chips are only slightly lower in fat than fried ones. • Rice, couscous, noodles. Boil rice rather than having it fried or pilau, or use only
1 teaspoon of vegetable oil for frying rice or curries. • Pasta – try wholemeal varieties • Cereals – especially porridge, Branflakes, Shredded Wheat, Weetabix, Allbran, Special K, Sultana Bran, Low Sugar Museli, Mini Wheats.
If the patient increases their intake of insoluble fibre ( e.g. cereal fibre such as wholemeal bread, wholewheat pasta, high fibre breakfast cereals, brown rice) they should be reminded to drink plenty of fluids – at least 6-8 cups per day.

23 Diabetes Care : A Guide to Good Working Practice
Fats Reviewing the type and amount of dietary fat is an essential part of dietary advice for ‘heart health’ and weight management There are 4 types of dietary fats:- Omega 3 fatty acids Improves blood flow, makes blood less sticky, reduces risk of thrombosis and inflammation. Omega 3 Rich Foods Linseed, flaxseed oil Soya bean Tofu Oily fish (mackerel, herring, sardines, salmon, trout, pilchards) Monounsaturated Fats Can lower less beneficial types of cholesterol (LDL) but maintain “good cholesterol” (HDL).
Foods High in Monounsaturates: Olive, rapeseed, peanut, hazelnut, almond oils Almond, brazil, cashews, hazelnuts, peanuts Avacado pear, olive Olive and rapeseed spreads
Polyunsaturated Fats Can change chemically (oxidation) and contribute to atherosclerosis. Foods High in Polyunsaturates: Sunflower, corn, soya, sesame, grapeseed oil Pinenuts, walnuts, sesame and sunflower seeds Margarines and spreads labelled “high in Polyunsaturates”

24 Diabetes Care : A Guide to Good Working Practice
Saturated Fats Increase atherogenic LDL cholesterol. Foods High in Saturates: Butter, lard, suet, dripping Fatty cuts of meat, corn beef, chopped ham, sausages, burgers, pies and pasties Full fat milk, cream, cheeses Cakes, biscuits, chocolates, pastry, ice cream cream sauces Coconut, coconut oil, palm oil Fruit and Vegetables Patients should aim for five portions of fruit or vegetables daily. Excellent sources of soluble fibre and antioxidant vitamins which have beneficial effects on glycaemic control and lipid lowering. A Portion is: Apple/Orange/ Banana 1 fruit Melon/Pineapple 1 slice Plums, Kiwi, Satsumas 2 fruits Grapes, Raspberries 1 handful Vegetables 2 tablespoons
• Distribute fruit throughout the day (one portion at a time) • Choose tinned fruits in fruit juices • Limit dried fruit snacks • Limit quantities of unsweetened fruit juices to one small glass per day with
food • Include a wide variety of fruit and vegetables
Protein Sources include: meat, poultry, fish, eggs, nuts, beans and pulses, cheese, milk. Patients should limit their intake of meat products such as sausage rolls, meat pies, tinned meats and meat spreads. These are very high in fat. Patients should eat moderate amounts and choose lower fat versions whenever possible. They should avoid cooking with added fats. Remove visible fats from meats and skin from poultry.

25 Diabetes Care : A Guide to Good Working Practice
Patients should be encouraged to try low fat cooking methods including, grilling, baking, microwaving, steaming and poaching. Suggested portion sizes: 3-4oz (75-100g) cooked meat 4-5oz (100g-125g) cooked fish Alcohol Maximum daily intake Men 3 - 4 units Women 2 - 3 units 1 unit equals ½ pint of beer or lager (ordinary strength) 1 glass of wine (125 ml 9% alcohol) 1 glass of sherry 1 pub measure of spirit
• Distribute alcohol throughout the week (eg 2 units a day aim for at least 2 alcohol free days).
• Never drink on an empty stomach. Ensure regular CHO intake. • Alcohol may increase risk of hypoglycaemia. • Alcohol is high in calories. Consider weight management. • Advisable to avoid high alcohol content beers, lagers and alcopops above
5% volume.
(Department of Heath 2007) Diabetes Food Products These are not recommended. Often these foods are sweetened with sugar alcohols, which will act as a laxative and induce diarrhoea. Sugar alcohols, as sugar, contain 4 kcal/g and therefore such diabetes food products may be high in calories. This may promote weight gain or inhibit weight reduction. Weight Weight reduction, where appropriate, will improve glycaemic control, lipid profiles and blood pressure. It will decrease insulin resistance. Body mass index (BMI) can be used to assess the degree of obesity, however waist circumference is a more reliable clinical indicator of insulin resistance and, therefore cardiovascular risk.

26 Diabetes Care : A Guide to Good Working Practice
Waist circumference Europids: Male > 94cm Women > 80cm South Asians: Male >90cm Women > 80cm International Diabetes Federation definition of metabolic syndrome (April 2005) Weight loss expectations should be realistic, considering an individual’s ability to exercise and present medical history. Refer to weight management pathway for adults. Referral to Specialist Dietitian for diabetes
Pumps (via specialist insulin pump service) Pregnancy (via joint diabetic/antenatal clinic) Carbohydrate Counting Glycaemic Index Lipid Lowering Renal (see Integrated care pathway for Renal disease for people with diabetes) Resistant obesity (see weight management pathway) References M. Lean, 2003 Oct. Diabetic Medicine

27 Diabetes Care : A Guide to Good Working Practice
PHYSICAL ACTIVITY IN THE MANAGEMENT OF TYPE 2 DIABETES BENEFITS AND RISKS Physical activity is important in the management plan of Type 2 diabetes as it not only improves short and long term glycaemic control, but has beneficial effects on blood pressure and dyslipidaemia. In addition, regular physical activity helps to lose and maintain weight, improves physical and psychological well being and may enhance quality of life; it may also help to reduce long term mortality. Despite these potential benefits, compliance with physical activity remains discouragingly poor. At present there is little evidence to suggest how the exercise habits and barriers to physical activity are assessed in patients with Type 2 diabetes. To reap the multiple benefits of physical activity in patients with Type 2 diabetes, we need to educate our patients regarding the benefits of a healthy life style and being physically active. The brief guidelines which follow will help health professionals to understand the role of physical activity in the management of diabetes There is evidence, that regular physical activity benefits most patients with Type 2 diabetes and metabolic syndrome and the benefits generally far outweigh the risk associated with it. However, due to potentially detrimental effects of exercise on macro and micro vascular complications, careful selection of patients through a proper clinical evaluation and individualisation of exercise programmes is needed in those who wish to increase physical activity. Benefits Of Physical Activity The benefits are summarised in table 1: But remember • The best time to motivate your patients is around the time of diagnosis • Physical activity is much more likely to be beneficial during early years of Type 2
diabetes Risks Of Physical Activity The risks of physical activity need to be considered carefully as newly diagnosed subjects with Type 2 diabetes frequently have micro and macro vascular complications. All subjects with newly diagnosed Type 2 diabetes: • should routinely be assessed for their leisure time and occupational activity as is
the current practice for dietary assessment. • target those who currently take no or little exercise. • develop and disseminate information leaflets to highlight the health benefits of
exercise to subjects with Type 2 diabetes. • screen for complications of diabetes prior to the initiation of any formal exercise
program.

28 Diabetes Care : A Guide to Good Working Practice
• give individualised advice to those who are ready for action about the kind of activities they can choose.
• encourage patients to keep a log book of their activities, as a willingness to do so is associated with better compliance.
• education regarding exercise need to be reinforced and should form an essential part of any ongoing educational programmes.
• Minor musculo-skeletal injuries are common and depend upon the intensity and duration. Wearing proper fitting shoes and exercising in a proper environment can minimise these risks .
• Those treated with sulphonylureas or insulin are at risk of hypoglycaemia during and up to 24 hrs after exercise.
• Exercise may also cause transient or prolonged hyperglycaemia after strenuous exercise in those who are insulin deficient.
Effects on Specific Complications of Type 2 Diabetes Chronic complications of diabetes or other physical disabilities may be an impediment for exercise. However, none of these are an absolute contraindications for mild or moderate intensity exercise. • Sudden death is rare with an incidence of 0-2/1000,000 hours of exercise. • Precipitation of pre-existing CHD or unmasking of angina is another concern.
But, subjects should be carefully screened including a thorough history, a physical examination and a resting ECG should be considered. Follow safe tips for initiation of physical activity
Microvascular Complications Retinopathy: Moderate intensity physical activity has a no detrimental effect on non-proliferative retinopathy and the risk in those with proliferative retinopathy is low . • In those who have new vessel formation or vitreous haemorrhages, it is prudent
to avoid vigorous physical activities. • These include activities such pounding, repeated jarring, weight lifting, high
impact aerobics, and activities involving valsalva manoeuvre. Nephropathy: Exercise increases albumin excretion during and immediately after exercise although the long term implications on the natural history of diabetic nephropathy are unclear. Neuropathy: Patients with neuropathy and insensitive feet are more prone to foot ulceration and fractures. Therefore • screening for peripheral neuropathy, foot deformity or degenerative joint disease • limit or avoid weight bearing exercises such as step aerobics, prolonged jogging
or walking • Adequate advice about self foot care should be provided to all.

29 Diabetes Care : A Guide to Good Working Practice
• Subjects with autonomic neuropathy may have decreased exercise capacity. These subjects may be more prone to episodes of extreme hypo or hypertension following vigorous exercise.
Table 1: Rationale for promoting physical activity in Type 2 diabetes • As an adjunct to diet for initial weight loss • Aid to help maintain the weight loss • Loss and redistribution of abdominal fat • Favourable effect on glycaemic control • Management of hypertension in diabetes • Management of dyslipidaemia • Improvement in general well being
Table 2 : Potential benefits of regular exercise in Type 2 diabetes • Lowers blood glucose during and after exercise • Increases insulin sensitivity • Lowers basal and post prandial insulin levels • Lower glycated haemoglobin (HbA1c) over long term • Lowers systolic and diastolic blood pressures • Quantitative and qualitative changes in circulating lips
o Lower triglyceride, lower LDL cholesterol, higher HDL cholesterol o Beneficial effects on LDL density?
• Improves fibrinolysis lowers plasma fibrinogen • Other benefits
o Cardiovascular conditioning o Improves strength o Improves sense of well being (physical and psychological) o Better quality of life o Improves fibrinolysis, lowers plasma fibrinogen
Physical Activity – General Recommendations • Any new physical activity should be discussed with the individual’s diabetes
team. • When initiating physical activity, the amount and intensity of activity should be
increased gradually on an individual basis • People should aim to accumulate 30 minutes of moderate intensity physical
activity most days of the week, or at least five days a week. • A patient centred approach should be used to explore a person’s readiness to
adopt physical activity and to help the person formulate their personal physical activity strategies

30 Diabetes Care : A Guide to Good Working Practice
• Education on methods to prevent exercise induced hypoglycaemia should be provided, as well as information on hyperglycaemia and foot care.
Reference: Burr B, Nagi D (1999) DIABETES AND SMOKING Tobacco is harmful to health and is of particular danger to people with diabetes. All late complications of diabetes such as cardiovascular disease, foot problems, kidney and eye disease are worsened by smoking. There is growing evidence that cigarette smokers are more prone to developing Type 2 diabetes than the rest of the population. Smoking is associated with insulin resistance. While smoking, insulin absorption from subcutaneous tissue is delayed. In insulin treatment, smoking after meals will therefore be particularly untimely. When diabetes is already present, smoking increases the incidence of mortality and morbidity from cardiovascular and cerebrovascular complications such as myocardial infarction and stroke along with other complications that are explained in further detail below. Studies show that smoking shortens life on an average by 5 to 10 years; however this could be even more in people with diabetes. The effects of smoking on microvascular complications of diabetes The microvascular complications of diabetes include Nephropathy (kidney disease), neuropathy (nerve damage) and retinopathy (eye damage). These are strongly linked with metabolic control. However, it is likely that smoking increases the risk of microvascular complications. Nephropathy (kidney disease) has been shown to be common in type 1 diabetic patients who smoke and smoking increases the risk of microalbuminuria (the presence of protein in the urine which can indicate signs of kidney disease) in both type 1 and type 2 diabetes. Studies show that smoking cessation could slow the progression of kidney disease in people with diabetes. Smoking is also a risk factor for both the development and progression of various types of neuropathy (damage to the peripheral nervous system). A recent case study of Type 1 and Type 2 diabetic patients found that current or ex-smokers were significantly more likely to have neuropathy than diabetic patients that have never smoked. The study also found that cigarette smoking was associated with a 2-fold increase in risk of neuropathy. Generally, smoking has not been considered a serious risk factor for diabetes retinopathy. However, a number of studies involving people with Type 1 diabetes suggest that tobacco smoking predisposes these people to eye damage.

31 Diabetes Care : A Guide to Good Working Practice
The Effects Of Smoking On Macrovascular Complications Of Diabetes The multiple effects of smoking on the blood vessels have been established for several years. It seems that people with diabetes are particularly susceptible to some of these effects. In all people with diabetes, it has been shown that smoking is significantly associated with an increased risk of heart disease. The UK Prospective Diabetes Study clearly showed that in people with Type 2 diabetes, cigarette smoking is a significant and independent risk factor for heart disease, stroke and peripheral vascular disease. Generally, tobacco smokers show various aspects of the metabolic syndrome – a cluster of features including abdominal obesity, high blood pressure insulin insensitivity and glucose intolerance. While these metabolic changes, which are often precursors to Type 2 diabetes are generally correlated with the degree of nicotine use. Smoking Cessation There is overwhelming evidence that stopping smoking reduces the risk of cardiovascular disease, lung disease, cancer and stroke. A large number of clinical and experimental studies and surveys have found evidence for significant associations between tobacco use, blood glucose control and diabetes complications. In diabetes care, smoking cessation is of the utmost importance in order to facilitate the effective control of blood glucose, and to limit the development of diabetes complications. Nicotine Addiction Cigarettes and some other products containing tobacco are highly engineered so as to create and maintain dependence to nicotine. It is not nicotine itself which is the most dangerous agent of smoking, but the many compounds that these products contain and the smoke they produce that cause the most damage: they are pharmacologically active, toxic, mutagenic and carcinogenic. The tobacco industry’s artful marketing, advertising and promotion are another obstacle to smoking cessation. Therefore, it is advised that smokers enlist the help and support of a specialist stop smoking service to aid them with their quit attempt. The stop smoking service in your area will offer free and confidential advice and support. Guidance will be given about products such as nicotine replacement therapy (NRT) that can be used to aid your quit attempt. How to Access Support To be referred to the Wakefield stop smoking service please collect a referral form from the reception at your G.P. surgery, complete the form and return it to the following address:

32 Diabetes Care : A Guide to Good Working Practice
Stop Smoking Service, Pontefract health Centre, Trinity Street, Pontefract, WF8 1EY. Alternatively, please call 01977 465449 and one of our friendly staff will be happy to take your enquiry. If you do not live in the Wakefield area, to find your local NHS stop smoking service please call 0800 169 0 169. MANAGEMENT OF CARDIOVASCULAR RISK Introduction Patients with diabetes are generally a very high risk group for Cardiovascular (CVD) disease and its clinical manifestations. The risk of CVD in patients with Type 2 diabetes is higher than patients without diabetes who already have IHD. Smoking, hypertension, dyslipidaemia and physical inactivity are major modifiable risk factors for IHD in diabetes. . Nephropathy manifest as microalbuminuria and retinopathy are strong predictions of CVD and total mortality. What Are We Trying To Achieve? People with diabetes (Type1 or Type 2) are now all considered to be at high risk and therefore formal cardiovascular risk assessment is not required. The absolute risk can be effectively lowered by tackling multiple risk factors ie stopping smoking, treating hypertension adequately and lowering cholesterol levels.
Lifestyle and Risk Factor Targets
Discontinue smoking, make healthier food choices, increase physical activity and achieve optimal weight (BMI<25) and weight distribution (waist circumference <94cm in men [Asians <90cm] and <80cm in women Blood pressure target of <140mmHg systolic and <80 mmHg diastolic. In selected higher risk people (established atherosclerotic disease, diabetes and chronic renal failure) a new lower blood pressure target of< 130mmHg and, <75 mmHg may be more appropriate. A new lower total cholesterol target of <5.0 mmol/l and a new density lipoprotein (LDL) cholesterol < 3.0 mmol/l, or a 25% reduction in total cholesterol and a 30% reduction in LDL cholesterol, whichever gets the person to the lowest absolute level

33 Diabetes Care : A Guide to Good Working Practice
The optimal fasting glucose is < 5.6 mmol/l for all people. The optimal target for glycaemic control in people with diabetes is a fasting or pre-prandial glucose value of 4.0 – 6.0 mmol/l and a HbA1c < 6.5% The Management of Hypertension In Diabetes The treatment of hypertension is as important as good glycaemic control and all patients, irrespective of age, should have their blood pressure measured annually (hypertension, particularly systolic hypertension may be present from an early age). "At risk" patients, those with macro/microalbuminuria, established vascular disease, dyslipidaemia or smokers should be monitored at every clinic visit. In the case of proteinuria or microalbuminuria, it is reasonable to aim for a blood pressure of 130/75 mmHg. (NICE 2002) A diagnosis on hypertension is made if the blood pressure exceeds the criteria for that individual on three separate occasions. When treatment is initiated depends on the individual patient and the presence or absence of proteinuria/microalbuminuria, vascular disease or other risk factors. Treatment Non-pharmacological therapy: advice should be given, as appropriate, about smoking, diet, exercise, weight reduction, alcohol and salt intake and in those with borderline or mild hypertension this may be sufficient. Drug therapy: there are several classes of anti-hypertensive agents available. The choice of agent would depend upon the presence or absence of albuminuria or microalbuminuria for these patients consider the use of - ACE-inhibitors (or angiotensin II receptor antagonists if not tolerated) as the first choice irrespective of blood pressure (MEREC 2006). Some degree of patient profiling is necessary depending upon co-existing cardiac complications such as angina, due to ischaemic heart disease or cardiac failure.

MEDICINES GUIDELINE
Younger than 55yearsand non Afro Caribbean
55years or older or Afro Caribbean
patients of any age
Step 1
Step 2
Step 3
Step 4Resistant Hypertension
Add: further diuretic therapy or Beta-blocker, Alpha-blocker, or spironolactone. Consider seeking specialist advice
A: ACE Inhibitor or angiotensin receptor blockerC: Calcium Channel Blocker D: Diuretic (thiazide)
A +D
A
A
+ +C D
Refer to the management of renal disease in people with diabetes re ace inhibitors and angiotensin 11 receptors page 54
D
Targets for Blood Pressure Management The results of the UKPDS showed that aggressive management of blood pressure is more important than that of hyperglycaemia. Secondly, it was clear that for good blood pressure control most patients required two or more hypertensive agents. Target BP. No end organ damage aim for < 140/80 mm of Hg. End organ damage aim for < 130/75 mm of Hg The individual clinical situation may determine positioning
34 Diabetes Care : A Guide to Good Working Practice

35 Diabetes Care : A Guide to Good Working Practice
Detection And Management Of Lipid Disorders How to Screen Ideally all adults with diabetes should have their lipids checked at the time of diagnosis and, every year thereafter. Caution: Do not forget secondary causes of hyperlipidaemia in patients with diabetes ie • Hypothyroidism • Primary biliary cirrhosis • Alcohol excess • Nephrotic syndrome • Chronic renal failure • Drugs When to Treat All patients with Type 2 diabetes should have a statin over the age of 40 years unless there is a compelling reason for them not to. Each patient should be clinically assessed and their individual risk should be discussed. In people with diabetes statin therapy is recommended for: • All those who are aged 40 years or over with type 2 diabetes • For people who are aged 18 – 39 years with type 2 diabetes and who have at
least one of the following: • Retinopathy (pre-proliferative, proliferative, maculopathy) • Nephropathy, including persistent microalbuminuria • Poor glycaemic control (HbA1c >9.0%) • Elevated blood pressure requiring antihypertensive therapy • Raised total blood cholesterol (>6.0 mmol/l) • Features of metabolic syndrome (central obesity and fasting
triglyceride >1.7 mmol/l [non-fasting >2.0 mmol/l] and/or HDL cholesterol <1.0 mmol/l in men or <1.2 mmol/l in women)
• Family history of premature cardiovascular disease in a first degree relative.
Other classes of lipid lowering drugs (fibrates, bile acid sequestrants, cholesterol absorption inhibitors, nicotinic acid) should be considered in addition to a statin if the total and LDL cholesterol targets have not been achieved

36 Diabetes Care : A Guide to Good Working Practice

37 Diabetes Care : A Guide to Good Working Practice
Aspirin Aspirin 75mg daily is recommended for all people with type 2 diabetes who are aged 50 years or older, and selectively in younger people with one of the following criteria: people who have had the disease for more than 10 years, who are already receiving treatment for hypertension and who have target end organ damage in the form of retinopathy or nephropathy Before starting treatment ensure that the systolic blood pressure has been reduced to 145 mmHg or below and maintain while taking aspirin. If aspirin is contraindicated as per NICE which defines aspirin intolerance as: • proven hypersensitivity to aspirin-containing medicines • history of severe dyspepsia induced by low-dose aspirin, then clopidogrel 75mg could be considered as an alternative (NICE 2002)

Guidelines For The Management Of Diabetes And Cardiovascular Disease
Management of Blood Pressure and Lipids is fundamental to the treatment of Type 2 diabetes the aim is: to reduce the risk of coronary events and mortality. Each patient should be clinically assessed and their individual risk should be discussed
Lifestyle and risk factor targets
• Discontinue smoking • Make healthier food choices • Reduce alcohol intake
• Increase physical activity • Achieve optimal weight and weight
distribution
Lifestyle advice should be offered initially and then periodically throughout the patient journey
Lipids: target total cholesterol - <5.0mmol/l and low density lipoprotein (LDL) <3.0mmol/l
Blood Pressure: target – 140/80 130/75 may be more appropriate in selected people with chronic renal failure or established cardiovascular disease
When to screen The treatment of hypertension is as important as good glycaemic control and all patients irrespective of age should have their blood pressure measured annually
When to screen All people with diabetes should have their lipids checked at the time of diagnosis and yearly thereafter
Younger than 55yearsand non Afro Caribbean
55years or older or Afro Caribbean
patients of any age
Step 1
Step 2
Step 3
Step 4Resistant Hypertension
Add: further diuretic therapy or Alpha-blocker, Beta-blocker or spironolactone. Consider seeking specialist advice
A: ACE Inhibitor or angiotensin receptor blockerC: Calcium Channel Blocker D: Diuretic (thiazide)
A +D
A
A C or D
+ +C D
Refer to the management of renal disease in people with diabetes re ace inhibitors and angiotensin 11 receptors page 54
When to treat • All those who are 40 years or over with Type 1 or
Type 2 diabetes • For people who are 18 – 39 with either Type 1 or
Type 2 and have at least one of the following o Retinopathy o Nephropathy including persistent
microalbuminuria o Poor glycaemic control HbA1C > 9.0% o Elevated blood pressure requiring
therapy o Features of metabolic syndrome o Family history of premature
cardiovascular disease in first degree relative
38 Diabetes Care : A Guide to Good Working Practice
Aspirin Aspirin 75mg is recommended for all people with Type 2 diabetes who are aged 50 years or over, or younger if : • Had diabetes for more than 10 years • Receiving treatment for hypertension • Have retinopathy or nephropathy Caution Ensure that the systolic blood pressure is 150mmHg or below and maintain while taking aspirin If aspirin is contraindicated clopidogrel 75mg daily is an alternative.

39 Diabetes Care : A Guide to Good Working Practice
Oral Medication For Type 2 Diabetes Oral anti-diabetic drugs should usually be prescribed when diet and lifestyle change has proved inadequate in controlling plasma glucose, usually after at least one month's trial. The tablets should be used to supplement diet and not to replace it. Occasionally, tablet medication may be used at an early stage for symptom control. The list of oral medication below is not exhaustive and further up to date information can be accessed in a current BNF and summaries of product characteristics (SPC) www.emc.medicines.org. Metformin Metformin should be used as first line oral medication after lifestyle intervention in all patients, on the basis of evidence of beneficial clinical outcomes and cost effectiveness. It is particularly beneficial in overweight patients as it tends to facilitate weight reduction. Gastrointestinal symptoms, nausea, abdominal pain and diarrhoea are relatively common but can be minimised if taken at mealtimes and doses are initially low and increased in stages. Side effects tend to be dose dependent so where a higher dose causes symptoms, a lower dose may be tolerated. Metformin has an excellent safety record but caution must be used in patients with renal, hepatic or cardiac impairment because of the small risk of lactic acidosis. Sulphonylureas Sulphonylureas lower blood glucose by stimulating insulin release and therefore tend to encourage weight gain and hypoglycaemia. They should be used as first line for patients who are intolerant of metformin, not overweight and with a BMI of less than 25. It can be used as first line treatment in a person newly diagnosed with Type 2 diabetes who has severe osmotic symptoms. Caution is advised in the elderly and in those with hepatic or renal insufficiency because of the risks of hypoglycaemia. The longer acting agent Glibenclamide should be avoided in these populations. Side effects apart from hypoglycaemia are generally mild and infrequent and include gastrointestinal disturbances and headaches. The sulphonylureas preferred by the Diabetes Centres are listed below: • Gliclazide • Glimeperide

40 Diabetes Care : A Guide to Good Working Practice
HYPOGLYCAEMIC WARNING All patients prescribed sulphonylureas must be given advice regarding hypoglycaemic symptoms and management. Treatment should be adjusted if Hypoglycaemia is experienced.
Glitazones (Thiazolidinediones) The Glitazones: Rosiglitazone and Pioglitazone reduce peripheral insulin resistance, leading to a reduction in blood glucose but take 2 to 3 months for maximum effect. Liver function tests (LFTs) should be performed on all patients prior to commencing a Glitazone and periodically thereafter: see summaries of product characteristics (SPC) for frequency of further monitoring. It is important to discuss with patients, particularly those at risk of heart failure and/or reduced cardiac reserve to look out for signs and symptoms of adverse reactions relating to fluid retention and weight gain which can precipitate heart failure. There is a paucity of evidence that glitazones improve patient orientated outcomes. In addition, NICE advises that the use of Pioglitazone or Rosiglitazone as second line therapy added to either metformin or a sulphonylurea, is not recommended unless tolerance is an issue (BNF 2007, SPC 2007) • Pioglitazone • Rosiglitazone Meglitinides Nateglinide and repaglinide have a very similar action to sulphonylureas stimulation of pancreatic insulin release. Both drugs have a rapid onset of action and short duration of activity, and should be administered shortly before each meal to decrease postprandial blood glucose. They are beneficial to people with erratic meal schedules, but may limit compliance Repaglinide Repaglinide may be given as monotherapy for patients who are not overweight or for those in whom metformin is contra-indicated or not tolerated, or may be given with metformin. Nateglinide Nategilinide is licensed only for use with metformin

41 Diabetes Care : A Guide to Good Working Practice
Acarbose Acarbose is an inhibitor of intestinal alpha glucoseidases and delays the absorption of simple sugars. It has a small but significant effect in lowering blood glucose, alone or in combination with other anti-diabetic agents. Flatulence is a frequent and troublesome side effect making it unpopular with most patients who have tried it. Newer Medications for People with Type 2 Diabetes These medications are currently under NPAG assessment and firmer guidance will be issued as an addendum Exenatide Exenatide is an injectable drug which reduces blood sugar in people with type 2 diabetes.Exenatide belongs to class of drugs called incretin mimetics such as human-glucagon-like-peptide 1 (GLP 1). GLP1 increases the secretion of insulin from the pancreas, slows the absorption of glucose from the gut and reduces the action of glucagon, GLP1 also reduces appetite therefore reducing blood glucose levels and also patients experience weight loss. The exenatide injection should be given 60 minutes before breakfast meals and should not be used for patients with Type 1 diabetes or as a substitute for insulin. Sitagliptin Sitagliptin is an oral drug which reduces blood glucose I Type 2 diabetes by inhibiting the enzyme dipeptidyl peptidase-4 (DPP-4) and increasing the the levels of GLP-1 and glucose-dependent insulinotropic polypeptide (GIP), GIP reduces blood glucose by increasing the production and release of of insulin from the pancreas. Sitagliptin can be taken with or without food once daily. Obesity Agents Orlistat Orlistat, a lipase inhibitor, reduces the absorption of dietary fat. It may be considered as an aid to weight reduction in conjunction with a hypocaloric diet in patients with Type 2 diabetes and a body mass index (BMI) of greater than 28. Treatment with orlistat should be discontinued after 12 weeks if patients have been unable to lose at least 5 % of the body weight as measured at the start of drug therapy (NICE 2006).It is not licensed for treatment longer than 2 years

42 Diabetes Care : A Guide to Good Working Practice
because of insufficient evidence for a longer treatment period. Sibutramine Sibutramine inhibits the re-uptake of noradrenaline and serotonin. It is used in the management of obesity in individuals with a BMI of 27 or more when associated with Type 2 diabetes Sibutramine is not licensed for use longer than 1 year; on stopping it, there may be a reversal of the weight loss. Sibutramine should only be prescribed for individuals who have attempted seriously to lose weight by diet, exercise, and other behavioural modification. Arrangements should exist for appropriate healthcare professionals to offer specific advice, support, and counseling on diet, physical activity, and behavioural strategies to those receiving sibutramine. Blood pressure should be monitored according to the SPC Rimonabant Rimonabant was launched in the July 2006 and is currently under NPAG assessment. Rimonobant is a cannabinoid receptor antagonist for the management of obesity in individuals with a BMI of 30 kg/m2 or more, or in individuals with a BMI of at least 27 kg/m2 in the presence of other risk factors such as Type 2 diabetes or dyslipidaemia. Rimonabant is not licensed for use for longer than 2 years; on stopping rimonabant, there may be a gradual reversal of weight loss Contraindications: Ongoing major depressive illness and/or ongoing anti depressive treatment

STEPWISE APPROACH TO THE TREATMENT MANAGEMENT OF TYPE 2 DIABETES
Confirmed diagnosis of Type 2 diabetes Target HbA1c between 6.5% and 7%
However all patients should be treated according to their individual needs
Step 1 • Refer to DESMOND structured education programme • Refer to Retinal Screening programme • Healthy Eating • Physical Activity • Weight Control • Stop Smoking • Reassess in 3 months • Consider early use of oral hypoglycaemic agent if symptomatic
Reassess patient 3 – 6 monthly if not controlled 12 monthly if controlled. Check compliance with lifestyle issues at each visit. Step 2: Monotherapy 1st Line
• Metformin
2nd Line • sulphonylurea • Optimise doses
Step 3: Dual Therapy
• Add sulphonylurea to metformin • In patients not at risk of heart failure or reduced cardiac
reserve consider adding pioglitazone to sulphonylurea if metformin intolerant
• Optimise doses
Notes • Consider Orlistat or sibutramine as adjunct to healthy eating advice for weight reduction in those with a BMI >28 • When the patient with diabetes is symptomatic consider introducing dual therapy earlier • The clinical need of the patient may result in entry into the pathway at any point
Step 5: Insulin Therapy • See guidelines
for insulin initiation in primary care
Step 4: Triple Therapy
If the patient is metformin tolerant
• Metformin, glitazone and sulphonylurea
• Optimise doses
Ensure compliance /concordance with lifestyle issues and oral therapy throughout the patient journey. Consider reassessment of patient’s blood glucose control at appropriate intervals throughout the patient’s journey
43 Diabetes Care : A Guide to Good Working Practice

Insulin Initiation Pathway for People with Type 2 Diabetes
Diff
Basal Insulinhypoglycaem
• Overweig• Reluctan• Unable to
themselv• The olde
complicahypoglycunaccept
When to initiate insulin
• The aim of the treatment is to improve glycaemic control and quality of life. • Oral hypoglycaemic agent (OHA) prescription is to the maximum tolerated dose and
desired HbA1c not achieved (< 8%) • OHA not tolerated/contra-indicated • Check concordance of medication (OHA) • Symptoms related to poor glycaemic control • Patient agrees to and understands the benefits of insulin therapy
Before insulin therapy • Reinforce dietary advice and discuss lifestyle issues and employment i.e. smoking
and physical activity • Check ability to administer own insulin / carers district nurse involvement • Patients should be taught home blood glucose monitoring advice to monitor blood
glucose at different times. • Refer to specialist diabetes dietitian if appropriate • Assess for diabetes related complications
erent regimes which may be considered when initiating insulin therapy in people with Type 2 diabetes
with oral ic agents
ht BMI >26 ce to start insulin inject es r person with no tions but where aemia is able
Twice daily pre-mixed insulin with oral hypoglycaemic agents
• Regular lifestyles • Eat similar amounts at
similar times of the day • OHAs are no longer
stimulating efficient insulin production leading to post prandial high blood glucose level
• Symptomatic
Basal Bolus consider referral to Diabetes specialist nurse to initiate this regime
• On daily/bd insulin regimes without optimal control
• Requiring flexibility due to an erratic lifestyle
• Shift work • Regular travel across time
zones • Regular sport • To optimise blood glucose
control because of complications
44
Diabetes Care : A Guide to Good Working Practice

Reasons for Resisting Commencing Insulin Therapy The decision when to start insulin therapy must be made in partnership with the patient keeping the Hba1c results in mind. Lifestyle and employment issues must discussed (HGV drivers may not wish or delay transfer to insulin as they will lose their HGV licence Needle phobia accurate information may help people with needle phobia for example people may think that they need to find a vein to inject into or that the needle may be large. A demonstration of the pen device is therefore useful People generally over estimate the risk of hypoglycaemia or be basing their ideas on stories on outdated treatments or equipment Some people may believe that if they have no symptoms their diabetes is well controlled and that they are not at risk of complications
Levels of Control Generally the target HbA1C is < 7.5% or < 7% if there are complications present however each person should be assessed on an individual basisand targets set accordingly Who may not benefit from insulin therapy The target of 7.5% may not be appropriate for all and the risk of hypoglycaemia must be balanced against the target. HbA1c is not always relevant if life expectancy is limited Some obese people may not benefit from insulin therapy because insulin can lead to further weightgain with little or no improvement in HbA1c. Couldlifestyle issues such as change in their diet, more exercise, or the use weight reducing agents like orlistat or sibutramine be explored? People whose oral hypoglycaemic therapy regimecould be improved and titrated to the maximum doses
Different Regimes There is no one ‘right’ choice and one regimen is not necessarily forever. If it unsuitable it should be changed. Negotiate with each individual the most appropriate form of treatment taking into consideration lifestyle and individual needs. Metformin should always be continued with all three regimes unless it is not tolerated or the patient has renal impairment and the serum creatinine is outside the normal range. Sulphonylurea should be discontinued after a period of six weeks when the dose of insulin has been titrated when using basal insulin
Training and Competencies Prior to initiating insulin in Primary Care it is essential that Providers have:
• A health care professional who has already completed ENB 928 or the Diabetes Diploma. • Undertaken Insulin initiation training either at The Crow Trees Centre, Idle, Bradford or by accessing locally
developed training with support from the Diabetes Specialist Nurses. Nurses involved in the initiation of insulin in primary care will be required to commit to attending at least 1 updatesession per year. The training for insulin initiation will take three months to complete with a case study forum to finish. A forum todiscuss case studies will be held six monthly to enable nurses to have regular updates particularly around newpen devices and insulin regimes and to share any problems they may be encountering in practice.
The training will be linked to the Skills for Health Diabetes competencies which in turn is linked to the knowledgeand skills framework Patients should be encouraged to take responsibility for their own care as far as possible. A good understandingof their own condition and how to treat it increases the chances of effective control of blood glucose levels, whichwill minimize the risk of complications. Educating people with diabetes, their carers, partners and families istherefore vitally important part of the nurse’s role
45 Diabetes Care : A Guide to Good Working Practice

46 Diabetes Care : A Guide to Good Working Practice
INSULIN INITIATION CHECKLIST 1. Aims of treatments Date 2. Oral Medication Date 3. Choice/use of pen Date 4. Name and type of insulin Date 5. Action of insulin Date 6. Timing of injections Date 7. Injection technique Date 8. Site rotation Date 9. Safe disposal of sharps Date 10. Storage of insulin Date 11. Self adjustment of insulin Date 12. Hypoglycaemia – cause/symptoms/treatment Date 13. Hyperglycaemia - Cause/symptoms/treatment Date 14. Ketone testing Date 15. Sick day rules Date 16. Meter used Date 17. Timing/frequency Date 18. Recording results Date 19. Interpreting results Date 20. Basic dietary advice Date 21. Alcohol Date 22. Dietitian referral Date 23. Physical Activity Date 24. Smoking Date 25. Driving-DVLA/insurance/hypoglycaemia Date 26. Employment Date 27. Prescription exemption Date 28. Footcare/podiatry referral Date 29. Contraception/pregnancy/pre-pregnancy counseling Date 30. Holidays/travel Date 31. ID card Date 32. Local support groups Date

47 Diabetes Care : A Guide to Good Working Practice
RETINOPATHY – SCREENING AND EARLY MANAGEMENT Introduction Diabetic retinopathy is the leading cause of blindness in people under the age of 60 in industrialised countries. It is also a major cause of blindness in older people. Many people will be asymptomatic until the disease is very advanced. After 20 years from the onset of diabetes, almost all people with Type 1 diabetes and more than 60% of people with Type 2 diabetes will have diabetic retinopathy. Nearly 1 in 5 people with type 2 diabetes will have a significant degree of diabetic retinopathy at the time when diabetes is diagnosed. The risk of visual impairment and blindness is substantially reduced by a care programme that combines methods for early detection with effective treatment of diabetic retinopathy. The key issue in screening for diabetic retinopathy is to identify those people with sight-threatening retinopathy who may require treatment to prevent visual loss. In 2001 the policy for screening for diabetic retinopathy was clearly set out in the National Service Framework for Diabetes with the introduction of a national screening programme. Within the local area retinal screening has been commissioned by the Wakefield and Kirklees PCTs to provide comprehensive coverage to the area served by the Diabetes Network.
Screening and treatment for diabetic retinopathy will not eliminate all cases of sight loss, but can play an important part in minimising the numbers of patients with sight loss due to retinopathy. Referral And Screening All people with diabetes aged 12 years and over should be referred into the screening programme using the appropriate referral form. These forms are available electronically on request to the programme administrators. However, in a small number of circumstances, it may be appropriate to decide that a patient is not suitable for screening. This should only be done after careful assessment of the person and their circumstances (see guidance notes). In all cases where patients are excluded from screening their details should still be provided to the retinal screening programme for reporting purposes with an indication of whether the exclusion is permanent or temporary. In all other circumstances, people with diabetes will be sent an annual invitation for screening and given the opportunity to make their own informed choice about whether to accept on each and every occasion that screening is offered. All screening is carried out by digital photography unless patients are referred by the screening programme into the biomicroscopy clinic where retinal examination is undertaken with a slit lamp.

48 Diabetes Care : A Guide to Good Working Practice
Screening takes place at fixed sites throughout the district by accredited retinal screeners. Patients are invited to attend the most convenient site to their registered General Practice. However, for those patients attending the diabetes clinics at Pontefract Hospital, retinal screening is integrated within the clinic visit.

PATHWAY OF CARE Patients registered within the retinal screening programme follow the pathway of care outlined below by the National Screening Committee (NSC). This links with the NSC and NICE guidelines for the early treatment of diabetic retinopathy from the identification of the presence of diabetes through to referral into a screening programme, grading and referral for treatment or back into the screening programme.
On Diagnosis of type 1 or type 2 diabetes, examine eyes: • Record best corrected visual acuity, with spectacles or pinhole as appropriate• Dilate pupils with Tropicamide • Examine for diabetic retinopathy using 2-field digital photography
• Optomise diabetes control • Manage retinopathy according to
severity:
• • • •
49 Diabetes Care : A Guide to Good Wo
Background Retinopathy R1 • Microaneurysm • Retinal haemorrhage (s)
RoutinArrang
Pre-proliferative retinopathy R2 • Venous beading, venous loop or reduplication • Intraretinal microvascular abnormality (IRMA) • Multiple deep, round or blot haemorrhages • (CWS – careful search for above features)
Achiev 95% Minim 70%
Maculopathy M1 • Exudates within 1 disc diameter (DD) of the centre
of the fovea • Circinate or group of exudates within the macula • Retinal thickening within 1DD of the centre of the
fovea (if stereo available) • Any microaneurysm of haemorrhage within 1DD of
the fovea only if associated with a best VA of ≤ 6/12 (if no stereo)
Achiev 95% Minim 70%
Proliferative retinopathy / rubeosis iridis R3 • New vessels on disc (NVD) • New vessels elsewhere (NVE) • Pre-retinal or vitreous haemorrhage • Pre-retinal fibrosis ± tractional retinal
detachment
Achiev 95% s Minimu70% s
Very Urgent • Sudden loss of vision • Retinal detachment
Emergday)
Routine diabetes care Maintain good blood glucose control Maintain good blood pressure controlAnnual screening
rking Practice
e diabetes Care e annual screening
able standard seen by ophthalmologist in <13 weeks
um Standard seen by ophthalmologist in <13 weeks
able standard seen by ophthalmologist in <13 weeks
um Standard seen by ophthalmologist in <13 weeks
able Standard een by Ophthalmologist in < 2 weeks
m Standard een by ophthalmologist in < 2 weeks
ency referral to ophthalmologist (same

50 Diabetes Care : A Guide to Good Working Practice
Ungradable Images In a small minority of patients attending for retinal photography, it may not be possible to obtain clear images of their eyes and these patients are categorised as “technical failures”. Reason may include inadequate dilation, dense cataract etc. In such cases patients will be referred into the dedicated biomicroscopy clinic where examination with a slit lamp will be carried out by an experienced member of the retinal screening team. Feedback Full disease grading is carried out by the dedicated team of retinal screener/graders overseen by internal and external quality assurance. Patients and health care providers should expect to receive written feedback within approximately 2 weeks of attendance. Medical Treatment Blood pressure Tight blood pressure control is particularly important in retarding the development and progression of eye disease and the prevention of visual impairment. The minimum target for blood pressure should be <140/80 mm.Hg but ideally <130/75 mm.Hg.
Glycaemic control
Tight glycaemic control also has a beneficial effect on the development and progression of eye disease and the prevention of visual impairment. The minimum target for HbA1c should be <7.5% or ideally lower than 7%. It is important to note that in patients with severe background or significant retinopathy rapid tightening of glycaemic control can lead to rapid progression to high risk proliferative retinopathy.
• In a patient with unknown retinopathy status and poor glycaemic control, retinal screening should be performed before tightening up glycaemic control.
• As it takes years for the complications of diabetes to occur, it would seem prudent for glycaemic control to be improved gradually over 6-12 months in such at risk patients.
Laser treatment
Laser treatment is an effective treatment for proliferative retinopathy and will prevent the majority of people developing significant visual impairment.
However the outcome of laser treatment is dependent upon the severity of retinopathy and its impact on vision. For example if people enter into laser treatment with poor vision the likelihood of visual improvement is greatly reduced.

Wakefield District & North KirkleesRetinal Screening Programme
Wakefield Primary Care Trust Kirklees Primary Care Trust
Retinal Screening Department
Clayton Hospital Wakefield WF1 3JS
Tel: 01924 213656
Retinal Screening Referral Form Name (attach demographic printout if available)
Mr / Mrs / Ms / Master / Miss / Dr
D.O.B
Address
Postcode
Telephone number
NHS Number
Registered GP/ Practice
Diabetes Type / Diagnosed Type 1 Type 2 Date Diagnosed:
………… Suitable for retinal photography (see
exclusion notes) YES NO If NO state reason:
………………………………………. ……………………………………………………… Permanent exclusion Temporary exclusion commence recall
Date of last Retinal examination
Any other comments (Please supply any known dates patient unable to attend, i.e. holidays)
51 Diabetes Care : A Guide to Good Working Practice

Please complete and return this form to the above address. (Please photocopy this form as required Wakefield District & North Kirklees Retinal Screening Programme
SCREENING / REFERRAL CRITERIA
WHO : All people with diabetes aged 12 years and over WHEN : Refer at diagnosis Screening will be performed at least annually PATIENTS REQUIRING SPECIAL CONSIDERATION In a small number of circumstances it may be appropriate to decide that a patient is not suitable for diabetic retinopathy screening. This should only be done after a careful assessment of the person and their circumstances.
Learning & mental disabilities Every effort should be made with the carers and relatives to facilitate the explanation of the procedure. However, some patients may become distressed when the procedure is attempted. In these circumstances the screening activity will cease and the GP informed and the situation reconsidered at the next screening interval. Mental disability may be a temporary condition and this should be taken into account when considering
Patients receiving specialist eye care These patients may be exempt from screening once it has been established that they are attending ophthalmology and it has been identified that retinal examination has been carried out there. In such cases these patients should be identified to the screening programme as under ophthalmology care and the responsibility will fall with the screening programme to liaise with ophthalmology regarding continuing care.
Diabetes Ca
Physical disabilities Some patients with physical disabilities may prevent them from achieving a position where a diagnostic image of the eye can be obtained. This may include medical conditions which prevent the head from being steady for sufficiently long to assess the eyes properly. In these circumstances the situation should be explained to the patientand should only be excluded if their disabilities are unlikely to improve.
exempting the patient.
52
re : A Guide to Good Working Practice

Note of caution! Screening outside the NHS programme Patients who have their eyes screened outside the NHS should not be excluded from the programme. Patients will continue to receive an invitation for screening at the routine interval so they can decide whether or not to attend.
For detawith
Terminal illness Patients should be referred and invited foras long as they are able to participate in screening. Discretion should be exercised by the GP/Practice Nurse referring the patient as to not causeundue distress. Registered blind Patients who are registered blind or partially sighted may still have some residual vision and should only be excluded if they have no perception of light in both eyes.
reporting purposes, where patieils should still be provided to the the reason for exclusion clearly
Diabetes Care :
Informed choice If a patient requests to be withdrawn from the screening programme permanently, the healthcare professional receivingthis information should ensure the patient has had sufficient information to make informed choice. That person should inform the programme of their decision in writing. Consider asking whether the patient would want to be invited in future.
nts fall into any of the above categories, their retinal screening programme on a referral form stated.
53
A Guide to Good Working Practice

THE DIABETIC FOOT DIABETES FOOTCARE INTEGRATED CARE PATHWAY
Wakefield District and North Wakefield District and North KirkleesKirklees
Diabetes Diabetes Foot CareFoot Care Integrated Integrated Care PathwayCare Pathway
Review date:3.5.06Enquiries to: gill.day@ wwpct.nhs.ukEndorsed by:Diabetes Strategic Partnership GroupGroup responsib le for developm ent:Diabetes Foot Care ICP S teering Group
Managem ent by prim ary care team3-6 m onthly review sEnhanced foot care education
Managem ent by prim ary care teamAgree m anagem ent plan inc luding foot care educationArrange call and recallAnnual review
Absent foot pulses Start secondary
prevention i.e. statin and aspirin
Norm al sensation and pulses
Absent pulse or sensation
No callous deform ity or redness
Foot ulcer presentIf previous ulceror
as Am ber p lus deform ity
Prim ary Care TeamAssessm ent to inc lude:• testing of foot sensation• palpation of foot pulses• inspection for deform ity• inspection of footwear
Increased riskAMBER
High RiskRED
Low riskGREEN
Managem ent and frequent review by com m unity pod iatrist1-3 m onthlyEnhanced foot care education
Refer prom ptly to foot clinic/d iabetes centre w ithin 24 hours if a new ulcer
Sym ptom atic e.g. interm ittent c laudicationor rest pain NO
YESVascular surgery
referra l
54 Diabetes Care : A Guide to Good Working Practice

CARE PATHWAY FOR THE MANAGEMENT OF RENAL DISEASE IN PEOPLE WITH DIABETES
Microalbuminuria in diabetes is a key marker of cardiovascular risk
All newly diagnosed Type 2 patients Type 1 patients 5 years following diagnosis
Test urine for microalbuminuria annually Screen for microalbuminuria by measuring the
albumin/creatinine ratio on overnight first void samples type If positive, confirm by demonstrating at least 2 positive of 3
tests in 1 month. Exclude other causes i.e. urinary tract infections, other
kidney disease etc.
No Is microalbuminuria present?
Routine care Arrange recall and annual review
Yes
55 Diabetes Care : A Guide to Good Working Practice
Consider Referral to Diabetes Specialist
Diabetic Nephropathy with one of the following • eGFR < 30 • Plasma creatinine >200 mcmol/l or plasma urea>20
mmol/l • Plasma potassium>6 mmol/l on a non-haemolysed
(hospital ) sample • Hyperphosphataemia or hypocalcaemia • Heavy proteinuria (1g in 24 hours) • Renal impairment with haemoglobin<10g/dl and normal
haematinic values • Uncontrollable hypertension (>150/90 on 3 agents) • Suspected non-diabetic renal disease • Suspected renal artery stenosis
Following reassessment • Blood pressure targets not
achieved • Glycaemic control remains poor • Creatinine levels are elevated
and rising
Refer to Nephrologists
Dr Richard Baker (DDH) Dr Graham Woodrow Dr Alex Brownjohn
If targets are not reached • Intensify treatment • Consider insulin therapy if HbA1c >7.5mmol/l and rising • Reassess in 3 – 6 months
• Document it and identify the patient as high cardiovascular risk • Aim for a blood pressure of 130/75 mmHg (accepting that many patients are unable to
achieve this target) by using aggressive blood pressure lowering medication - ACE-inhibitors (or angiotensin II receptor antagonists if not tolerated) as the first choice irrespective of blood pressure
• Tighten glycaemic control (below 7% HbA1c according to individual’s target) • Stop metformin if creatinine > 140 mcmol/l • Intensive management of cardiovascular risks smoking cessation, weight management,
dyslipidaemia and physical inactivity
It is important in this group of people especially at the first detection of any diabetic nephropathy, that any risk factors should be addressed ie: Glycaemic
control (HbA1c<7%)
Control of hypertension (<130/75 mmHg)
Lipid assessment Total Cholesterol <5, LDL <3
Smoking cessation (advised)

Screening for Nephropathy • Screen when free of acute, intercurrent
illness • Collect an early morning urine sample • Check for protein using a dipstick
o Check for urinary tract infection o Obtain a laboratory urine protein :
creatinine ratio (PCR) If dipstick negative
o Check for microalbuminuria using laboratory urine albumin : creatinine ratio (ACR)
o If positive, confirm by demonstrating at 2 positive of 3 tests in 1 month
Definitions Diabetic Renal Disease The presence of raised urine albumin levels or raised serum creatinine in Type 2 diabetes indicates an increased risk of premature cardiovascular events and, to a lesser extent, end stage renal disease. If the person has also signs of retinopathy, it is likely that the raised urine albumin and raised serum creatinine is resulting from diabetes-related renal disease. If retinopathy is not present, the probability of another renal disease increases. Lower-risk urine albumin excretion People who have levels of microalbuminuria and/or proteinuria lower than those indicated below. Higher-risk urine albumin excretion Microalbuminuria – albumin:creatinine ratio greater than orequal to 2.5mg/mmol (men) or 3.5mg/mmol (women), or albumin concentration greater than or equal to 20mg/l and/or Proteinuria – albumin; creatinine ratio greater than or equal to 30mg/mmol or albumin concentration greater than or equal to 200mg/l.
56 Diabetes Care : A Guide to Good Working Practice
Calculating Glomerular Filtration Rate The National Service Framework for Kidney Disease (2005) recommends the use of a formula-based estimation of glomerular filtration rate (GFR) Estimation of GFR using the MDRD study equation eGFR = 186 x (Pcr/88)-1.154 x (age)-0.203 x (0.742 if female) x (1.210 if black) This equation uses serum creatinine in combination with age, sex and race to estimate GFR and therefore improves upon several of the limitations with the use of serum creatinine. Plasma creatinine levels may rise by more than 30% after a meat – containing meal. To use the creatinine level for one of these calculations a sample after a 10 hour fast is recommended.
Stages of Chronic Kidney Disease Stage Description GFR 1 Kidney damage with normal or increased GFR >90 2 Mild renal impairment 60-89 3 Moderate renal impairment 30-59 4 Severe renal impairment 15-29 5 Established Kidney Failure <15
Management of diabetic renal disease Lifestyle, tight control of blood sugar and blood pressure, and regular monitoring of kidney function are key management approaches that aim to minimise the progression of diabetic renal disease. Most recommendations are covered by existing guidance, particularly the Diabetes NSF and NICE guidance.

57 Diabetes Care : A Guide to Good Working Practice
MANAGEMENT OF DIABETES IN CHILDREN : GOOD PRACTICE GUIDELINES FOR PONTEFRACT AND WAKEFIELD - INFORMATION FOR GENERAL PRACTITIONERS Introduction This paper is intended to outline the current practice for the management of children with diabetes in this district. As diabetes occurs in only about 1 in 1000 children, most practices will have very few children with this condition and treatment and follow up is largely hospital based. The General Practitioner however, is the key figure in the initial recognition of the condition and may be called upon for advice about complications or incurrent illness. The family doctor is also responsible for much of the ongoing prescribing for the life long condition. One purpose of this paper is to improve liaison between primary and secondary health care. Our philosophy of care is to deliver children to the care of the adult physicians in their late teens as healthy individuals. Our aim is that they should have a comprehensive understanding of all aspects of diabetes, normal growth and development, good biochemical control and be free of complications including emotional and psychological disturbance. To achieve this we believe requires the efforts of a multidisciplinary team providing care to a high standard in a supportive and educational environment. Diagnosis Diabetes in childhood can present in a number of ways: • Classical symtoms of polydipsia, polyuria, weight loss and lethargy. New onset
of bedwetting is not uncommon. Remember diabetes in children cam present at any age. In infants and toddlers the diagnosis may not be obvious in the early stages and these children therefore often present in DKA.
• Diabetic ketoacidosis – while often obvious, this diagnosis shoulsd be
considered in cases of vomiting, dehydration, drowsiness, tachypnoea. Ketosis frequently causes abdominal pain. Consequently diabetes appears in the differential diagnosis of gastroenteritis, pneumonia, appendicitis, meningitis etc.
• sometimes parents make the diagnosis by testing themselves when another
family member has diabetes • sometimes the diagnosis is fortuitous when blood or urine is tested for another
reason Whenever diabetes mellitus is suspected check an instant blood sugar with a

58 Diabetes Care : A Guide to Good Working Practice
blood glucose meter or dipstick urine for glucose and ketones. Referral Same day referral to the paediatric diabetes team (on call team if out of hours) is important, however well the child is, as children can decompensate rapidly. Urgent referral will enable them to be seen within 24 hours of presentation and minimize hospital stay. Early Management The child may be admitted for a few days but, if well, may be discharged early and, in some cases, treatment may be initiated without overnight stay. Initiating treatment without formal admission is the preferred option as there is some evidence that families learn to cope better and are less likely to require re-admission to hospital at a later date. This approach, however, is very dependent on adequate staff availability to provide the necessary support at home. During this time there will be close liaison with members of the Paediatric Diabetes Team. Longer Term Management And Liaison Out-patient appointments are scheduled 3 monthly. Children with problems may be seen in clinic more frequently or be reviewed by the paediatric diabetes specialist nurse (PDSN) between clinic appointments. Families who fail to attend clinic appointments are contacted by the PDSN either by telephone call or home visit. Trouble Shooting All families are given contact numbers for the paediatric diabetes team and emergency pager to enable emergency advice to be sought. Please feel free to use the contact numbers provided for advice about a particular patient, or diabetes in children in general. Protocols for illness management and hypoglycaemia are outlined below. Illness Management During illness blood sugars tend to rise in response to increased metabolic demands. Consequently, it is often necessary to take more insulin during illness than usual. Many children are reluctant to eat when they are unwell but must be encouraged to take at least as much carbohydrate as on a normal day. Basic advice should therefore be as follows: • never stop insulin even during illness • drink plenty of fluids • If reluctant to eat usual diet give carbohydrate in alternative form – eg lucozade,
milk, fruit juice, soup, jelly, yoghurt, biscuits, toast etc.

59 Diabetes Care : A Guide to Good Working Practice
• test the blood sugar at least four times each day more frequently if necessary • test the urine also for ketones even if blood sugars acceptable • if the blood glucose is 20 mmol/l or higher with moderate or large ketones give
extra soluble or rapid acting insulin. Dose is approximately one-tenth of normal total daily insulin.
• Extra insulin may need to be repeated after a few hours ( 3-4 hours if soluble
insulin, ~2 hours if rapid acting insulin) if high sugars or ketones persist. • Family to contact diabetes team for further advice at this stage if not already
done so • Refer to hospital if:
o Urine remains strongly positive for ketones o Vomiting o Troublesome hypoglycaemia (typically in younger children with D&V) o Depressed conscious level
Hypoglycaemia • In a co-operative child, give oral glucose or other sugar eg three dextrose
tablets, a cup of Lucozade (50 mls), a non diet cola, Glucogel (previously Hypostop) (one vial) or table sugar (two teaspoons).
• Glucogel (hypostop) can be used in the less co-operative or drowsy child as it
can be rubbed into the buccal mucosa • In an unconscious child give glucagon IM – 1mg (one unit) for children over 8
years and adults, 0.5mg for children under 8 years • On recovery, oral glucose must be followed by more starchy carbohydrate such
as a sandwich, a packet of crisps or biscuits to prevent rebound hypoglycaemia. Hospital admission is not necessary if there is full recovery and a normal diet can be tolerated. Admission for IV glucose infusion may be required if there is an ongoing problem such as gastroenteritis.
Prescribing Initial treatment and equipment will be provided from the hospital along with educational literature. If changes of treatment need to be initiated promptly, the new drugs or formulations will also be provided from out-patients. If the GP agrees with the recommended treatment, we would be grateful if they would accept responsibility for prescribing ongoing therapy.

60 Diabetes Care : A Guide to Good Working Practice
Paediatric Diabetes Team Contacts PGI Diabetes Pager Sheila Roberts(Diabetes Specialist nurse) Dr Allison Grove (Consultant) Dr Sue Gardiner (Consultant) Rosie Booth (Dietitian) Hydes Ward
07699 782555 7am-8pm every day 01977 606854 mobile 07899 901169 01977 606468 01977 606466 01977 606919 01977 606293/4
PGH Diabetes Pager Vanessa Parkin (Diabetes Specialist Nurse) Dr Steve Jones (Consultant) Dr Samka Gakenyi (Consultant) Nicky Godley (Dietitian) A Ward (>8 years) B Ward (<8 years)
07699 782555 7am-8pm every day 01977 606854 mobile 07785 760095 01924 212279 01924 212092 01924 213640 01924 212277 01924 212278
DDH Eileen Wilkinson (Diabetes Specialist Nurse) Dr Peter Mackay (Consultant) Dr Brigid Allagoa (Consultant) Childrens ward DDH
01924 512000 ext 4604 01924 816147 01924 512050 01924 816007

THE PHILOSOPHY OF TRANSITIONAL CARE A transitional care clinic is a flexible 3 – 4 monthly clinic which is run jointly with both the paediatric and adult services to ensure that a smooth transition between the services is facilitated. The clinic will: • Provide comprehensive, coordinated and uninterrupted health-care that is age appropriate and
developmentally appropriate with respect to all persons involved • Promote skills in communication, decision-making, assertiveness and self-care
DRAFT Algorithm for diabetes transitional care from paediatric to adult services
The concept of transitional care should be introduced during year 10 or 11 of the school years
Attend the first transition clinic Clinic: • Led by the paediatric consultant and paediatric diabetes specialist nurse (PDSN) • Adult consultant and adult diabetes specialist nurse (DSN) present • Patient introduced to the adult team • Paediatric dietitian present • If patient DNAs paediatric team to follow up
Attend second transition clinic 3 – 4 months later Clinic: • Led by the PDSN and adult consultant • Paediatric consultant may be present if patient not ready to move over to adult at this time • Adult DSN present • Paediatric dietitian present • If patient DNAs paediatric team to follow up • If admission to hospital at 16+ years adult team to follow up and refer to transition clinic led be adult
team
Third clinic: 3 - 4 months • Led by adult consultant and adult DSN • Paediatric support • Assessment by the adult diabetes team regarding the readiness of the patient to attend the young
person’s clinic • No dietitian available at each clinic appointment in young person clinic • If patient DNAs adult team to follow up
Attend young persons clinic/adult clinic unless special requirements (age 18 – 25 years)
If pregnant refer straight to adult services (young person’s clinic) and specialist antenatal clinic
Attend further transition clinics if patient not ready to progress to young person’s clinic
References: • Type 1 diabetes: diagnosis and management of Type 1 diabetes in children, young people and
adults NICE (2004) • Adolescent transition care guidance for nursing staff RCN (2004) • Getting the right start: the National Service Framework for children, young people and maternity
services part 1 DH (2003) • National Service Framework for children and young people DH (2006)
61 Diabetes Care : A Guide to Good Working Practice

62 Diabetes Care : A Guide to Good Working Practice
APPENDIX I CLASSIFICATION AND TERMINOLOGY • Impaired Glucose Tolerance (IGT) is a stage of impaired glucose regulation
(Fasting plasma glucose less than 7.0 mmol/l and OGTT two hour value greater than or equal to 7.8 mmol/l but less than 11.1 mmol/l)
• Impaired Fasting Glycaemia (IFG) has been introduced to classify individuals
who have fasting glucose values above the normal range but below those diagnostic of diabetes. (Fasting plasma glucose greater than or equal to 5.6 mmol/l but less than 7.0 mmol/l). Diabetes UK recommends that all those with IFG should have an OGTT to exclude the diagnosis of diabetes.
• Gestational diabetes is retained but now encompasses the groups formerly
classified as Gestational Impaired Glucose Tolerance (GIGT) and Gestational Diabetes Mellitus (GDM). Diabetes UK endorses the use of the World Health Organisation definition to allow for comparative studies. However, since glucose tolerance changes with the duration of pregnancy, the gestation at which the diagnosis was made should be recorded and, if made in the third trimester, the clinician should be cautious about the clinical implication of impaired glucose tolerance.
• It should be noted that children usually present with severe symptoms and
diagnosis should then be based on a single raised blood glucose result, as above. Immediate referral to a Paediatric Diabetes Team should not be delayed.
IGT and IFG are not clinical entities in their own right but rather risk categories for cardiovascular disease (IGT) and/or future diabetes (IFG). A diagnosis of diabetes has important legal and medical implications for the patient and it is therefore essential to be secure in the diagnosis. A diagnosis should never be made on the basis of glycosuria or a stick reading of a finger prick blood glucose alone, although such tests may be useful for screening purposes. HbA1c measurement is also not currently recommended for the diagnosis of diabetes. Diabetes UK recommends that the diagnosis is confirmed by a glucose measurement performed in an accredited laboratory on a venous plasma sample.
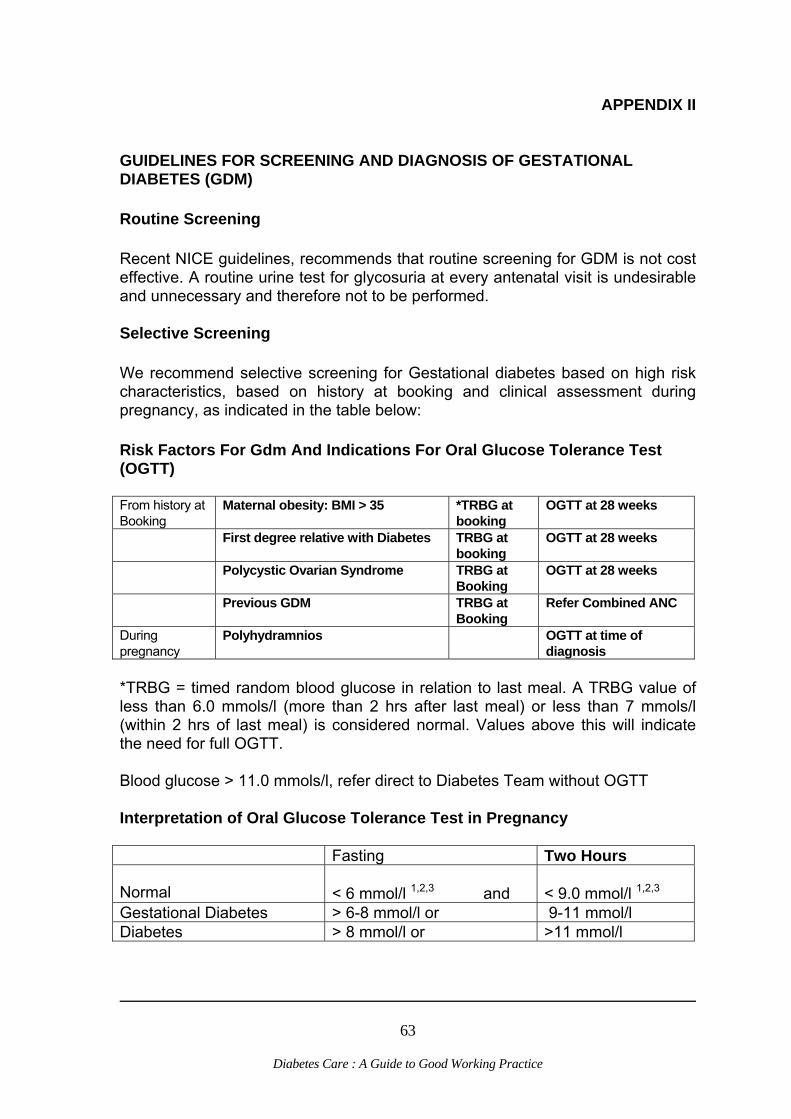
63 Diabetes Care : A Guide to Good Working Practice
APPENDIX II
GUIDELINES FOR SCREENING AND DIAGNOSIS OF GESTATIONAL DIABETES (GDM)
Routine Screening Recent NICE guidelines, recommends that routine screening for GDM is not cost effective. A routine urine test for glycosuria at every antenatal visit is undesirable and unnecessary and therefore not to be performed. Selective Screening We recommend selective screening for Gestational diabetes based on high risk characteristics, based on history at booking and clinical assessment during pregnancy, as indicated in the table below: Risk Factors For Gdm And Indications For Oral Glucose Tolerance Test (OGTT) From history at Booking
Maternal obesity: BMI > 35
*TRBG at booking
OGTT at 28 weeks
First degree relative with Diabetes
TRBG at booking
OGTT at 28 weeks
Polycystic Ovarian Syndrome TRBG at Booking
OGTT at 28 weeks
Previous GDM
TRBG at Booking
Refer Combined ANC
During pregnancy
Polyhydramnios OGTT at time of diagnosis
*TRBG = timed random blood glucose in relation to last meal. A TRBG value of less than 6.0 mmols/l (more than 2 hrs after last meal) or less than 7 mmols/l (within 2 hrs of last meal) is considered normal. Values above this will indicate the need for full OGTT. Blood glucose > 11.0 mmols/l, refer direct to Diabetes Team without OGTT Interpretation of Oral Glucose Tolerance Test in Pregnancy Fasting Two Hours Normal
< 6 mmol/l 1,2,3 and
< 9.0 mmol/l 1,2,3
Gestational Diabetes > 6-8 mmol/l or 9-11 mmol/l Diabetes > 8 mmol/l or >11 mmol/l

64 Diabetes Care : A Guide to Good Working Practice
Two-hour blood glucose – 7.8-8.9mmol/l please send diet sheet and letter to GP to request postnatal OGTT Post-Delivery: All women with two-hour blood glucose >7.8mmol/l should have OGTT performed approximately six weeks post-delivery. Management Of Gestational Diabetes During Pregnancy • Refer to Diabetes Specialist Nurse and to be seen within five days of OGTT: • for explanation of results, • dietary advice • Commence blood glucose monitoring. • HbA1c measured. • Transfer to Joint Antenatal clinic. • Review by Dietician ASAP post diagnosis (target within two weeks) • Bloods sugars recorded pre-prandially up to four times per day acceptable
range 4-6mmols. • Two hour post-prandial blood glucose target < 7.5 mmols. • Insulin therapy to be commenced, if after 4-5 days on modified diet home
blood sugars done pre-prandially are consistently above 6 mmol Intrapartum • CTG monitoring during labour • For the women who required insulin therapy antenatally follow guidelines for
management of labour in women receiving Insulin Treatment. Postpartum • Discontinue insulin immediately post delivery. • Blood sugars checked 6 hourly for 24 hours in women who required insulin
treatment. Contact diabetes specialist nurses if blood sugars above 9mmols otherwise discontinue.
• OGTT should be performed at six weeks post delivery on all women who had a 2 hr reading above 7.8mmols during the original OGTT during pregnancy – arrange via Diabetes Centre ext. 3904 (PGH), ext. 6212 (PGI) or ext. 4604 (DDGH).
• All women to be given an appointment with the Diabetes Specialist Nurse to discuss results of OGTT.
• GP to be informed of results by letter, including all lifestyle advice given and recommendations for subsequent screening (Annual fasting blood glucose).

65 Diabetes Care : A Guide to Good Working Practice
APPENDIX III
RECOMMENDED TESTING FOR INDIVIDUALS WITH DIABETES
TYPE 1 Blood glucose monitoring should be seen as an integral part of treating people with type 1 diabetes
Maximum Testing
Medium Testing
Basal bolus regime New transfer to insulin Pregnancy All children
Others
Ketostix also required for episodes of illness and high blood sugar readings where these patients will need to test for ketones in their urine. It is unlikely that this group will need testing strips for glycosuria.
TYPE 1
Frequency of Monitoring
Blood
Urine
Maximum Testing four times a day Strip requirement – three boxes a month
Ketostix Available as required
Medium Testing twice a day Strip requirements – three boxes every two months
Ketostix Available as required

66 Diabetes Care : A Guide to Good Working Practice
RECOMMENDED TESTING FOR INDIVIDUALS WITH DIABETES TYPE 2 The Freemantle study (Davis et al 2006) concluded that neither blood glucose monitoring nor it’s frequency was associated with glycaemic benefit in type 2 diabetes regardless of treatment. A better approach is to consider monitoring as one component of self -management education. If the patient has been properly educated in how to use the information they obtain from their meter, then he or she are much more likely to derive benefit from monitoring. Self monitoring of glucose levels can be important at diagnosis when used as part of patient education programme, however it is important in the longer term that the method of glucose monitoring is tailored to the current treatment regimen and the individual patients needs. (Regional drug and therapeutics centre 2007) Treatment Group
Self monitoring of Blood Glucose
Conventional insulin therapy or • Maximum oral therapy • Poorly
controlled/irregular blood sugar readings
• People with Type 2 diabetes who are using a conventional insulin regimen and who have stable control should SMBG two or three times per week
• People who have less stable control should SMBG at least once daily, varying the time of testing between fasting, premeal and postmeal.
• Testing twice a day for those requiring twice-daily insulins Strip requirement – three boxes every two months
Combined insulin and oral antidiabetic therapy
• Test once per day during insulin titration, at different times of
the day to identify hypoglycaemia • Test at other times of the day if feeling unwell • People who have unstable glycaemic control may require more
frequent testing • The frequency of monitoring can be reduced (but not
abandoned) when blood sugars and HbA1c targets are reached.
Diet, physical activity and oral antidiabetic therapy • Stable/controlled
glycaemia by diet and physical activity or diet physical activity and oral medication
• People with Type 2 diabetes who have good control on diet,
physical activity and oral hypoglycaemic agent do not need self-monitoring of blood glucose (SMBG) unless they are destabilized by other factors.
• Glycaemic control managed through diet and physical activity in people with Type 2 diabetes is best monitored through Hba1c. However the GP may wish to start SMBG at times of severe illness or poor control
67 Diabetes Care : A Guide to Good Working Practice
References: Diabetes and Primary Care: The continuing debate on self-monitoring of blood glucose in diabetes Owens et al. 2005 Diabetes guidelines: South Cambridgeshire Diabetes Network (2006) Position statements: Home monitoring of blood glucose levels Diabetes UK (2003) Drug Update Self-monitoring of Blood Glucose Regional Drug and Therapeutic Centre ( 2007) Davis WA, Bruce DG, Davis TME: Is self monitoring og blood glucose appropriate for all type 2 diabetic patients? The Freemantle Diabetes Study. Diabetes Care 29: 1764 -1770, 2006

68 Diabetes Care : A Guide to Good Working Practice
APPENDIX IV DIETETIC GUIDELINES FOR CHILDREN NEWLY DIAGNOSED WITH DIABETES All paediatric patients newly diagnosed with diabetes mellitus will have an initial visit from a State Registered Dietitian within 24 hours of receipt of referral (except weekends and Bank Holidays) Initial Interview * The Dietitian will introduce herself/himself and check identity of patient * A brief explanation of role in diet in diabetes will be provided * At the initial visit, a complete diet history will be taken * The importance of regular carbohydrate containing meals and snacks will be
explained and a list of suitable/unsuitable sources will be provided * Suitable alternatives will be suggested for cases of meal refusal - snacks, etc,
eg, milk, plain biscuit, crisps * A mention of treatment of hypos/illness exercise will be made * A sample meal plan may be provided as necessary * A brief discussion of school meal provision * Follow up will be offered within seven days or as necessary Second Interview * Further explanation of the role of diet in diabetes will be provided * Review their understanding of diabetes * Assess blood monitoring in relation to diet history and advice will be provided
as appropriate * Further information on school meal provision, meal refusal and other relevant
concerns will be provided

69 Diabetes Care : A Guide to Good Working Practice
Subsequent Interviews Further information will be provided as appropriate in relation to: * blood sugar carbohydrate and effect * reason for reducing sugar intake * importance of fibre - soluble - insoluble * different types of fat * effect of insulin/medication on blood sugar * illness * exercise * diabetic products * alcohol Written information and advice on the above will be provided as appropriate. These are only brief guidelines, each patient is treated as an individual.

70 Diabetes Care : A Guide to Good Working Practice
APPENDIX V
SUGGESTIONS REGARDING FURTHER INFORMATION FOR INDIVIDUALS WITH DIABETES The provision of background reading and information are important aids in reinforcing verbal advice and increasing patient awareness. Below are some suggestions of resources that are currently available. LITERATURE Balance for Beginners
• Type 2 diabetes • Type 1 diabetes
Available from Diabetes UK - currently at a charge of £3.00 Balance Magazine Bi-monthly "news and views" publication by Diabetes UK to subscribing members. Diabetes UK also produce a vast selection of leaflets and information which are listed in their catalogue and order form booklet. Can be ordered and purchased at Newsagents. Books Living with Diabetes for those treated with insulin) Dr JL Day ) Susan Brenchley Living with Diabetes for those treated with diet ) and Suzanne Redmond And Tablets ) Medicos 1992 British
Diabetic Association Diabetes at your fingertips Peter Sonksen, Charles
Fox and Sue Judd 1991, Class Publishing Ltd, cost approx £10.00
Diabetes in the Real World Charles Fox and Anthony
Pickering, Class Publishing Understanding your Diabetes for People with PH Wise, Foulsham the Type 1 Diabetes Publishing House Understanding your Diabetes for People with PH Wise Type 2 Diabetes

71 Diabetes Care : A Guide to Good Working Practice
Recipes for Health Diabetes Azhina Gouindji and Jill Myers published with BDA Support Group Diabetes UK 10 Parkway LONDON NW1 7AA Telephone: 020 7323 1531 Local branches of Diabetes UK are active in Wakefield. Further details are available from the Diabetes Centres in Wakefield. Diabetes Focus Group Local Support Groups currently running in: • Pontefract • Hemsworth • Castleford Diabetes CD Rom for Health Care Professionals and Multi-ed Medical Patients 0113 223 7428 www.multi-ed.co.uk
72 Diabetes Care : A Guide to Good Working Practice
REFERENCES UK Prospective Diabetes Study Group (1998) Intensive blood-glucose control with sulponylurea or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33) The Lancet 352 837-851 UK Prospective Diabetes Study Group (1998) tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes (UKPDS 38) British Medical Journal 317 703-713 Diabetes National Service Framework Delivery Strategy 2002 Department of Health Joint British Societies’ Guidelines on Prevention of Cardiovascular Disease in Clinical Practice (2005) Heart British Cardiac Society 91 supplement V The National Service Framework for Renal Services 2005 Part two: Chronic Renal Failure and End of Life Care Department of Health Management of Type 2 Diabetes Renal Disease – prevention and early management Clinical Guideline F (2002) National Institute for Clinical Excellence (NICE) Type 2 Diabetes Prevention and Management of Foot Problems Clinical Guideline 10 (2004) NICE Anglo Scandinavian Cardiac Outcomes (ASCOT) trial 2003……………………. Type 1 Diabetes: Diagnosis and Management of Type 1 Diabetes in Children, Young People and Adults Clinical Guideline 15 (2004) NICE Management of Type 2 Diabetes: Retinopathy – screening and early management Clinical Guideline E (2002) NICE Management of Type 2 Diabetes: Management of Blood Pressure and Blood Lipids Clinical Guideline H (2002) NICE Type 1 Diabetes: Diagnosis and Management of Type 1 Diabetes in Adults Clinical Guideline 15 (2004) NICE Guidance on the use of Patient Education Models for Diabetes: Technology Appraisal Guidance (TAG) – No.60 (2003) NICE Management of Type 2 Diabetes: Management of Blood Glucose Clinical Guideline G (2002) NICE

73 Diabetes Care : A Guide to Good Working Practice

74 Diabetes Care : A Guide to Good Working Practice
Guidance on Rosigltazone for Type 2 Diabetes Mellitus: TAG – No. 9 (2000) NICE Guidance on the use of Long-acting Insulin Analogues for the Treatment of Diabetes – Insulin Glargine: TAG – No. 53 (2002) NICE Recommendations of the St Vincent Task Force for the Management of Diabetes Pregnancies – 1996 (September 1999) International Diabetes Federation; new worldwide definition of metabolic syndrome (April 2005) British National Formulary; British Medical Association, Royal Pharmaceutical Society of Great Britain ( 2007) F:\cndh\J Wilson\Guidelines\Diabetes Guidelines A guide to good working practice revision 06-07\Current document\Approved Diabetes guidelines 2007.doc