hum. reprod.-2003-haimov-kochman-990-3
DESCRIPTION
Hum. Reprod.-2003-Haimov-Kochman-990-3TRANSCRIPT

Intraperitoneal levonorgestrel-releasing intrauterine devicefollowing uterine perforation: the role of progestins inadhesion formation
Ronit Haimov-Kochman1,3, Victoria Doviner2, Hagay Amsalem1, Diane Prus2,Amiram Adoni1 and Yuval Lavy1
1Department of Obstetrics and Gynecology and 2Department of Pathology, Hadassah University Hospital, Jerusalem, Israel
3To whom correspondence should be addressed at: Department of Obstetrics and Gynecology, Hadassah University Hospital,
Mount Scopus, P.O.B 24035, il-91240, Jerusalem, Israel. E-mail: [email protected]
BACKGROUND: Intrauterine contraception is a widely used, highly effective means of birth control. Uterine
perforation is a serious, albeit rare, complication of intrauterine device (IUD) use. Although uterine perforation by
levonorgestrel-releasing (20 mg/day) intrauterine system (LNG-IUS) has already been reported, the peritoneal
adhesion potential of this IUD is unknown. METHODS: The medical ®les of all patients diagnosed with an
intra-peritoneal IUD between the years 1990±2002 at Hadassah Medical Center were reviewed. Histopathological
study of peritoneal adhesion tissue adjacent to levonorgestrel medicated IUD was conducted in one case. RESULTS:
Eight cases of dislocated IUDs were found. Four cases used LNG-IUS and four other cases used copper-IUD.
Laparoscopy for IUD removal disclosed mild local peritoneal adhesions between omentum and pelvic organs in all
cases. No difference was noted in the appearance of the peritoneum in the presence of either a copper-IUD or
LNG-IUS. Histological examination of peritoneal tissue encasing the levonorgestrel-intrauterine system revealed
loose connective tissue with aggregates of submesothelial cells with a pseudo-decidual change. Immunohistochemical
staining for progesterone receptor was negative. CONCLUSIONS: The peritoneal adhesions potential of LNG-IUS
is low, similar to that of the copper-bearing IUD.
Key words: adhesions/intrauterine device/levonorgestrel/perforation
Introduction
Intrauterine contraception is a widely used, highly effective
means of birth control. Uterine perforation is a serious, albeit
rare, potential complication of intrauterine device (IUD) use.
Copper-bearing IUD is known to cause local peritoneal
adhesions (Adoni and Ben Chetrit, 1991). Therefore its
removal from the peritoneal cavity is recommended once
perforation is diagnosed. Levonorgestrel-releasing (20 mg/day)
intrauterine system (LNG-IUS) (Mirenaâ, Schering AG,
Germany) was introduced to the market in Israel in 1998.
Although uterine perforation by this form of IUD has already
been reported (Andersson et al., 1998), the peritoneal adhesion
potential of the levonorgestrel-releasing intrauterine device is
unknown.
Materials and methods
The medical ®les of all patients diagnosed with an IUD in the
peritoneal cavity between the years 1990±2002 at Hadassah Medical
Center were reviewed. In case number 4 (Table I) peritoneal adhesions
encasing the IUD were separated, formalin ®xed and paraf®n
embedded. Sections of 4 mm thickness were stained with haema-
toxylin and eosin. Immunohistochemistry was performed using
antibodies to vimentin (clone Vim3B4; Dako, Glostrup, Denmark),
smooth muscle actin (clone 1A4; Dako), CD-68 (clone KP1; Dako),
caldesmon (clone h-CD; Dako), calretinin ([PAD:DC8]; Zymed, San
Francisco, CA, USA), cytokeratin (clone LP34; Dako), desmin (clone
NCL-DE-R-11; Ventana Medical Systems Inc., Harvard, MA, USA),
estrogen receptor (clone 6F11; Ventana Medical Systems Inc.) and
progesterone receptor (clone 1A6; Ventana Medical Systems Inc.).
Results
Eight cases of dislocated IUDs were treated at Hadassah
Medical Center between the years 1990±2002 (Table I). Seven
of them were inserted within 3 months post-partum. Six of the
patients were breast-feeding at the time of IUD placement. In
four cases LNG-IUS (Mirena) was used and in four other cases
copper-IUD was inserted. The main reasons for investigation
of the IUD localization were mild abdominal pain and irregular
uterine bleeding. One patient was found to be 8 weeks
pregnant. The means for investigation were a transvaginal
ultrasonogram and an antero±posterior radiograph of the
pelvis. Diagnosis of dislocated IUD was made 12 days to 7
Human Reproduction Vol.18, No.5 pp. 990±993, 2003 DOI: 10.1093/humrep/deg203
990 ã European Society of Human Reproduction and Embryology
by guest on Novem
ber 14, 2015http://hum
rep.oxfordjournals.org/D
ownloaded from

months following insertion. Laparoscopy was performed
uneventfully in all patients. On laparoscopy, the perforation
site was noted in only four cases, when a relatively short time
had elapsed from insertion to laparoscopic removal. The IUD
was disclosed in ®ve cases encased in the omentum. Mild
peritoneal adhesions were reported between omentum and
pelvic organs in all eight cases. Lysis of peritoneal adhesions
was undertaken in only one case with a history of ®ve previous
Caesarean sections. No difference was noted in the appearance
of the peritoneum in the presence of either a copper-IUD or a
levonorgestrel-releasing intrauterine system.
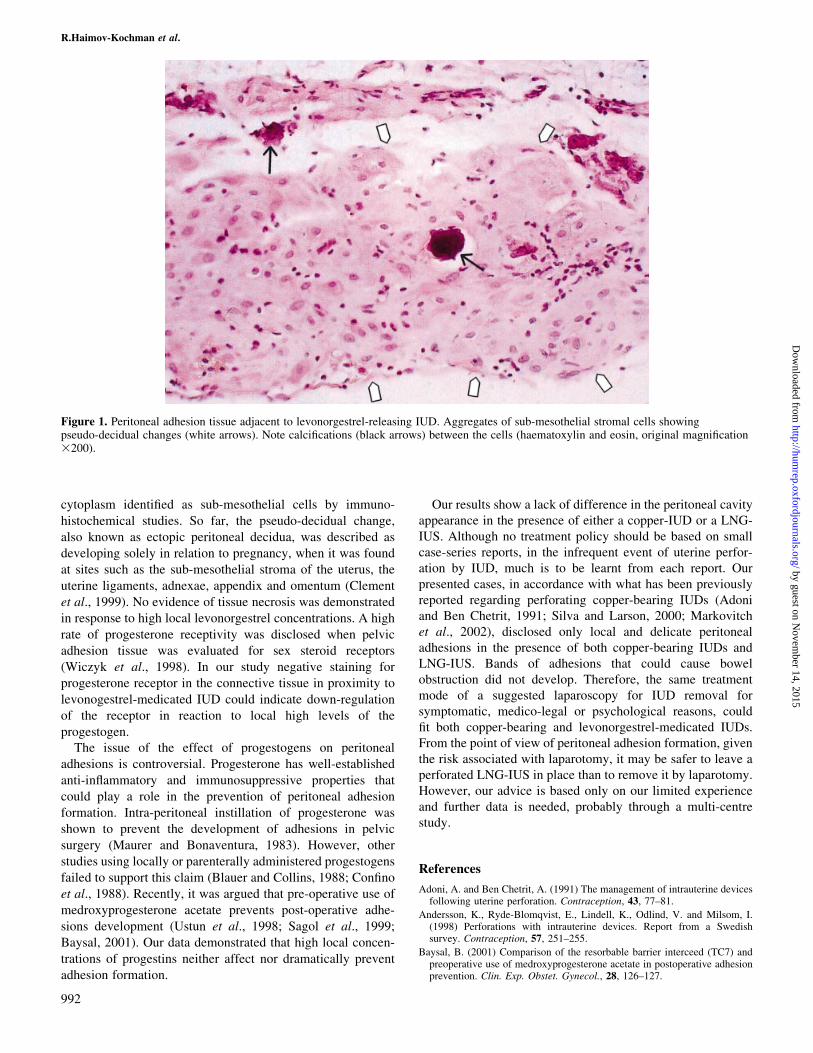
Histological examination of peritoneal tissue adjacent to
LNG-IUS (in case number 4), revealed richly vascularized
loose connective tissue with calci®cations and mild chronic
in¯ammation admixed with a few foreign body-type giant
cells. Aggregates of swollen cells with eosinophilic cytoplasm
and vesicular nucleus were found embedded in the tissue.
These cells stained with vimentin only and were identi®ed as
sub-mesothelial stromal cells of the peritoneal cavity that
underwent pseudo-decidual changes (Figure 1). Immuno-
histochemical staining for estrogen receptor was positive, but
staining for progesterone receptor was negative.
Discussion
The most serious potential complication of IUD use is uterine
perforation, which has been reported to happen in 0±1.3 events
per 1000 insertions (Andersson et al., 1998; Markovitch et al.,
2002). Uterine perforation by a copper-bearing IUD, although
usually asymptomatic, could rarely entail severe morbidity
such as bowel obstruction and infection. This type of IUD is
known to cause local peritoneal adhesions. The process of
adhesion formation in reaction to copper-bearing IUD is self-
limited and stops after a short period of time (Adoni and
Ben Chetrit, 1991). The recommended treatment of a mis-
placed copper-bearing IUD is its removal from the abdominal
cavity by laparoscopy (Silva and Larson, 2000), although
recently conservative management of mislocated IUDs has also
been suggested (Markovitch et al., 2002). Laparotomy is
considered to be by far too dangerous a procedure for the
management of an ectopic asymptomatic copper-IUD (Adoni
and Ben Chetrit, 1991).
Levonorgestrel-releasing (20 mg/day) intrauterine system
(Mirena) is a relatively new form of contraception. Perforation
of the uterus during its insertion has been reported among other
IUD types in a Swedish survey (Andersson et al., 1998);
however, the abdominal cavity in its presence was not
described. The adhesion formation potential of LNG-IUD
remained largely unknown. Mirena, similar to copper-bearing
IUDs, consists of a plain plastic T-shaped frame. The
development of peritoneal adhesions in response to a non-
irritating plastic-made foreign body was described by
Echenberg and Ledger (1968). This process involves encase-
ment of the device in delicate peritoneal bands. The plastic
skeleton of Mirena carries a cylindric progestogen reservoir
that contains 52 mg levonorgestrel and is covered by a
polydimethylsiloxane membrane which regulates the release of
levonorgestrel. Local release of levonorgestrel by Mirena
results in very high tissue concentrations, ranging from
470±1500 ng/g wet weight. The endometrial changes seen in
the presence of LNG-IUD are: endometrial gland atrophy,
stromal decidualization, thickened arterial walls and endome-
trial capillary thrombosis. An in¯ammatory reaction involving
neutrophils, lymphocytes, plasma cells and macrophages is
described (Zhu et al., 1989), and focal stromal necrosis may
also occur (Silverberg et al., 1986). The local effect of high
levonorgestrel concentrations on the peritoneum involves a
pseudo-decidual change of swollen cells with rich eosinophilic
Table I. Data of eight patients with uterine perforation by an IUD
Patientno.
Age Lysis ofadhesions
Presenceofperitonealadhesions
Previousoperations
IUDlocationin theperitoneum
Perforationsite
Time ofremoval sinceinsertion indays/months
MainSymptom
Breastfeedingstatus
Time ofinsertionpost-partumin days
Year ofIUDinsertion
IUDtype
CS P G
1 32 + Mild CSx5 Rt gutter Broadligament
3 months Irregularbleeding
+ 75 2001 Mirena 5 5 6
2 32 ± Mild Laparoscopiccholecystectomy
Omentum Uterinefundus
12 days Pain uponinsertion.Irregularbleeding
+ 38 2000 Mirena 0 4 4
3 37 ± Mild Appendectomy Omentum Not seen 7 months None + 60 1999 Mirena 0 4 64 33 ± Mild Splenectomy.
CSx1Pouch ofDouglas
Not seen 2 months Irregularbleeding
± 60 2002 Mirena 1 2 2
5 27 ± Mild Ovariancystectomy.Appendectomy
Omentum Not seen 5 months 8 weekpregnancy
+ 87 1996 CopperIUD
0 2 2
6 33 ± Mild None Omentum Uterinefundus
2 months Mild pelvicpain
+ 80 1997 CopperIUD
0 6 6
7 33 ± None CSx1 Pouch ofDouglas
Uterinefundus
2 days Mild pelvicpain
+ 38 1995 CopperIUD
1 5 8
8 39 ± None None Omentum Not seen 4 months Mild pelvicpain
± 100< 1994 CopperIUD
0 3 3
G = gravida; P = para; CS = Caesarean sections; IUD = intrauterine device.
Peritoneal adhesion potential of intrauterine device
991
by guest on Novem
ber 14, 2015http://hum
rep.oxfordjournals.org/D
ownloaded from
cytoplasm identi®ed as sub-mesothelial cells by immuno-
histochemical studies. So far, the pseudo-decidual change,
also known as ectopic peritoneal decidua, was described as
developing solely in relation to pregnancy, when it was found
at sites such as the sub-mesothelial stroma of the uterus, the
uterine ligaments, adnexae, appendix and omentum (Clement
et al., 1999). No evidence of tissue necrosis was demonstrated
in response to high local levonorgestrel concentrations. A high
rate of progesterone receptivity was disclosed when pelvic
adhesion tissue was evaluated for sex steroid receptors
(Wiczyk et al., 1998). In our study negative staining for
progesterone receptor in the connective tissue in proximity to
levonogestrel-medicated IUD could indicate down-regulation
of the receptor in reaction to local high levels of the
progestogen.
The issue of the effect of progestogens on peritoneal
adhesions is controversial. Progesterone has well-established
anti-in¯ammatory and immunosuppressive properties that
could play a role in the prevention of peritoneal adhesion
formation. Intra-peritoneal instillation of progesterone was
shown to prevent the development of adhesions in pelvic
surgery (Maurer and Bonaventura, 1983). However, other
studies using locally or parenterally administered progestogens
failed to support this claim (Blauer and Collins, 1988; Con®no
et al., 1988). Recently, it was argued that pre-operative use of
medroxyprogesterone acetate prevents post-operative adhe-
sions development (Ustun et al., 1998; Sagol et al., 1999;
Baysal, 2001). Our data demonstrated that high local concen-
trations of progestins neither affect nor dramatically prevent
adhesion formation.
Our results show a lack of difference in the peritoneal cavity
appearance in the presence of either a copper-IUD or a LNG-
IUS. Although no treatment policy should be based on small
case-series reports, in the infrequent event of uterine perfor-
ation by IUD, much is to be learnt from each report. Our
presented cases, in accordance with what has been previously
reported regarding perforating copper-bearing IUDs (Adoni
and Ben Chetrit, 1991; Silva and Larson, 2000; Markovitch
et al., 2002), disclosed only local and delicate peritoneal
adhesions in the presence of both copper-bearing IUDs and
LNG-IUS. Bands of adhesions that could cause bowel
obstruction did not develop. Therefore, the same treatment
mode of a suggested laparoscopy for IUD removal for
symptomatic, medico-legal or psychological reasons, could
®t both copper-bearing and levonorgestrel-medicated IUDs.
From the point of view of peritoneal adhesion formation, given
the risk associated with laparotomy, it may be safer to leave a
perforated LNG-IUS in place than to remove it by laparotomy.
However, our advice is based only on our limited experience
and further data is needed, probably through a multi-centre
study.
References
Adoni, A. and Ben Chetrit, A. (1991) The management of intrauterine devicesfollowing uterine perforation. Contraception, 43, 77±81.
Andersson, K., Ryde-Blomqvist, E., Lindell, K., Odlind, V. and Milsom, I.(1998) Perforations with intrauterine devices. Report from a Swedishsurvey. Contraception, 57, 251±255.
Baysal, B. (2001) Comparison of the resorbable barrier interceed (TC7) andpreoperative use of medroxyprogesterone acetate in postoperative adhesionprevention. Clin. Exp. Obstet. Gynecol., 28, 126±127.
Figure 1. Peritoneal adhesion tissue adjacent to levonorgestrel-releasing IUD. Aggregates of sub-mesothelial stromal cells showingpseudo-decidual changes (white arrows). Note calci®cations (black arrows) between the cells (haematoxylin and eosin, original magni®cation3200).
R.Haimov-Kochman et al.
992
by guest on Novem
ber 14, 2015http://hum
rep.oxfordjournals.org/D
ownloaded from

Blauer, K.L. and Collins, R.L. (1988) The effect of intraperitonealprogesterone on postoperative adhesion formation in rabbits. Fertil.Steril., 49, 144±149.
Clement, P.B., Young, R.H. and Scully, R.E. (1999) The Peritoneum. InSternberg, S.C. (ed) Diagnostic Surgical Pathology, Vol. 2, 3rd edn.Lippincott Williams and Wilkins, USA. p. 2437.
Con®no, E., Friberg, J., Vermesh, M., Thomas, W. and Gleicher, N. (1988)Effects of progesterone on postoperative adhesion formation inhysterectomized rabbits. Int. J. Fertil., 33, 139±142.
Echenberg, R. and Ledger, W.J. (1968) Peritoneal response to polyethyleneforeign bodies. Obstet. Gynecol., 31, 795±798.
Markovitch, O., Klein, Z., Gidoni, Y., Holzinger, M. and Beyth, Y. (2002)Extrauterine mislocated IUD: is surgical removal mandatory?Contraception, 66, 105±108.
Maurer, J.H. and Bonaventura, L.M. (1983) The effect of aqueousprogesterone on operative adhesion formation. Fertil. Steril., 39, 485±489.
Sagol, S., Ozsener, S., Dincer, O. Yilmaz, H. and Karadadas, N. (1999) Theeffect of medroxyprogesterone acetate and heparin in the prevention ofpostsurgical adhesion formation in the rat uterine model. J. Obstet. Gynecol.Res., 25, 287±293.
Silva, P.D. and Larson, K.M. (2000) Laparoscopic removal of a perforated
intrauterine device from the perirectal fat. J. Soc. Laparosc. Surg., 4,159±162.
Silverberg, S.G., Haukkamaa, M., Arko, H., Nilsson, C.G. and Luukkainen, T.(1986) Endometrial morphology during long-term use of levonorgestrel-releasing intrauterine devices. Int. J. Gynecol. Pathol., 5, 235±241.
Ustun, C., Yanik, F.F., Kocak, I., Canbaz, M.A. and Cayli, R. (1998) Effectsof Ringer's lactate, medroxyprogesterone acetate, gonadotropin-releasinghormone analogue and its diluent on the prevention of postsurgical adhesionformation in rat models. Gynecol. Obstet. Invest., 46, 202±205.
Wiczyk, H.P., Grow, D.R., Adams, L.A., O'Shea, D.L. and Reece, M.T.(1998) Pelvic adhesions contain sex steroid receptors and produceangiogenesis growth factors. Fertil. Steril., 69, 511±516.
Zhu, P.D., Luo, H., Xu, R.H., Cheng, J., Wu, S.C., Chen, J.H., Wu, M.Z. andWang, X.P. (1989) The effect of intrauterine devices, the stainless steel ring,the copper T220, and releasing levonorgestrel, on the bleeding pro®le andthe morphological structure of the human endometrium±a comparativestudy of three IUDs. A morphometric study of 96 cases. Contraception, 40,425±438.
Submitted on September 13, 2002; resubmitted on December 12, 2002;accepted on January 14, 2003
Peritoneal adhesion potential of intrauterine device
993
by guest on Novem
ber 14, 2015http://hum
rep.oxfordjournals.org/D
ownloaded from